Spinal Nerves
Spinal Nerve Roots
Spinal Cord
Neuralgia
Spinal Cord Injuries
Injections, Spinal
Sciatic Nerve
Peripheral Nerves
Hyperalgesia
Nerve Fibers
Ganglia, Spinal
Peripheral Nervous System Diseases
Rats, Sprague-Dawley
Pain
Optic Nerve
Radiculopathy
Spinal Cord Neoplasms
Nerve Compression Syndromes
Mononeuropathies
Pain Measurement
Posterior Horn Cells
Neuritis
Axotomy
Peripheral Nervous System Neoplasms
Hyperesthesia
Lumbar Vertebrae
Spinal Cord Diseases
Cyclohexanecarboxylic Acids
Sciatica
Nerve Block
Peripheral Nervous System Agents
Intercostal Nerves
Nerve Fibers, Myelinated
Nerve Endings
Sural Nerve
Tibial Nerve
Disease Models, Animal
Lumbosacral Plexus
Median Nerve
Spinal Diseases
Spinal Cord Compression
Facial Nerve
Spinal Neoplasms
Ulnar Nerve
Femoral Nerve
Sciatic Neuropathy
Spinal Fusion
Neural Conduction
Nerve Fibers, Unmyelinated
Sensory Receptor Cells
Thoracic Vertebrae
Amines
Infusions, Spinal
Nociceptors
Nerve Growth Factors
Cervical Vertebrae
Phrenic Nerve
Trigeminal Nerve
Nerve Growth Factor
Cauda Equina
Myelography
Wallerian Degeneration
Hindlimb
Cranial Nerves
Muscular Atrophy, Spinal
Radial Nerve
Afferent Pathways
Nerve Degeneration
Nerve Tissue
Peripheral Nervous System
Brachial Plexus
Loperamide
Spinal Cord Ischemia
Action Potentials
Immunohistochemistry
Ophthalmic Nerve
Mandibular Nerve
Medulla Oblongata
Anesthetics, Local
Dose-Response Relationship, Drug
Cervical Plexus
Rats, Wistar
Clonidine
Dissection
Neurilemmoma
Splanchnic Nerves
Paraplegia
Lidocaine
Thoracic Nerves
Morphine
Cochlear Nerve
Magnetic Resonance Imaging
Tuberculosis, Spinal
Ligaments
Laminectomy
Low Back Pain
Glossopharyngeal Nerve
Intervertebral Disc Displacement
Neurons
Electroacupuncture
Intervertebral Disc
Microglia
Optic Nerve Injuries
Electrophysiology
Nervous System
Analgesics, Opioid
Spinal Curvatures
Optic Nerve Diseases
Astrocytes
Sympathetic Nervous System
Hematoma, Epidural, Spinal
Neuroglia
Chick Embryo
Nerve Tissue Proteins
Cats
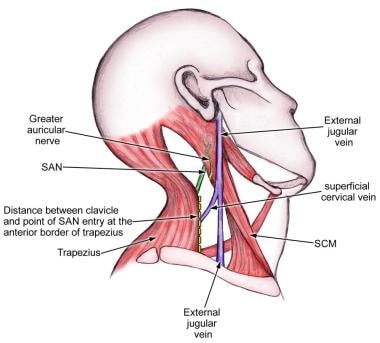
Accessory Nerve
Reflex
Naloxone
Abducens Nerve
Oculomotor Nerve
Cranial Nerve Neoplasms
Facial Nerve Injuries
Spinal Muscular Atrophies of Childhood
Olfactory Nerve
Facial Nerve Diseases
Recurrent Laryngeal Nerve
Hypoglossal Nerve
Lingual Nerve
Skin
Spinal Cord Regeneration
Electromyography
Uninjured C-fiber nociceptors develop spontaneous activity and alpha-adrenergic sensitivity following L6 spinal nerve ligation in monkey. (1/562)
We investigated whether uninjured cutaneous C-fiber nociceptors in primates develop abnormal responses after partial denervation of the skin. Partial denervation was induced by tightly ligating spinal nerve L6 that innervates the dorsum of the foot. Using an in vitro skin-nerve preparation, we recorded from uninjured single afferent nerve fibers in the superficial peroneal nerve. Recordings were made from 32 C-fiber nociceptors 2-3 wk after ligation and from 29 C-fiber nociceptors in control animals. Phenylephrine, a selective alpha1-adrenergic agonist, and UK14304 (UK), a selective alpha2-adrenergic agonist, were applied to the receptive field for 5 min in increasing concentrations from 0.1 to 100 microM. Nociceptors from in vitro control experiments were not significantly different from nociceptors recorded by us previously in in vivo experiments. In comparison to in vitro control animals, the afferents found in lesioned animals had 1) a significantly higher incidence of spontaneous activity, 2) a significantly higher incidence of response to phenylephrine, and 3) a higher incidence of response to UK. In lesioned animals, the peak response to phenylephrine was significantly greater than to UK, and the mechanical threshold of phenylephrine-sensitive afferents was significantly lower than for phenylephrine-insensitive afferents. Staining with protein gene product 9.5 revealed an approximately 55% reduction in the number of unmyelinated terminals in the epidermis of the lesioned limb compared with the contralateral limb. Thus uninjured cutaneous C-fiber nociceptors that innervate skin partially denervated by ligation of a spinal nerve acquire two abnormal properties: spontaneous activity and alpha-adrenergic sensitivity. These abnormalities in nociceptor function may contribute to neuropathic pain. (+info)The response of the brachial ventral horn or Xenopus laevis to forelimb amputation during development. (2/562)
The normal development of the brachial ventral horn of the frog Xenopus laevis and the response of the brachial ventral horn to complete forelimb extirpation at five developmental stages were assessed histologically. Differentiation of brachial ventral horn neurons occurred in pre-metamorphic tadpoles between stages 52/53 and 57. Mean cell number in the brachial ventral horn reached a peak of 2576 (S.E.M. equals +/- 269, N equals 2) per side of the spinal cord at stage 55 and decreased to 1070 (S.E.M. equals +/- 35, n equals 7) by the end of metamorphosis. Cell degeneration was presumed to be the mode of cell loss since it was most prevalent during the period of rapid decrease in cell numbers. The response of the ventral horn to forelimb removal varied with the stage of the animal at amputation. Following amputation at stage 52/53 or 54 the ipsilateral ventral horn neurons appeared less differentiated than those on the control side and a rapid cell loss of about 80% occurred on the operated side. These effects occurred more rapidly after ablation at stage 54 than at stage 52/53. Amputation at stage 58, 61, or 66 caused chromatolysis in the ventral horn, a period of relative cell excess on the operated side, and a delayed neuronal loss of 32-66%. It was concluded that excess cell degeneration accounted for cell loss and that suppression of normal neuronal degeneration caused the relative cell excess on the operated side. The data indicate that the brachial ventral horn was indifferent to the periphery before stage 54, was quickly affected by limb removal between stages 54 and 58, and by stage 58 had entered a phase in which a delay preceded cell death. No forelimb regeneration occurred. (+info)Receptor subtype mediating the adrenergic sensitivity of pain behavior and ectopic discharges in neuropathic Lewis rats. (3/562)
Receptor subtype mediating the adrenergic sensitivity of pain behavior and ectopic discharges in neuropathic Lewis rats. We attempted to identify the subtype of alpha-adrenergic receptor (alpha-AR) that is responsible for the sympathetic (adrenergic) dependency of neuropathic pain in the segmental spinal injury (SSI) model in the Lewis strain of rat. This model was chosen because our previous study showed that pain behaviors in this condition are particularly sensitive to systemic injection of phentolamine (PTL), a general alpha-AR blocker. We examined the effects of specific alpha1- and alpha2-AR blockers on 1) behavioral signs of mechanical allodynia, 2) ectopic discharges recorded in the in vivo condition, and 3) ectopic discharges recorded in an in vitro setup. One week after tight ligation of the L5 and L6 spinal nerves, mechanical thresholds of the paw for foot withdrawals were drastically lowered; we interpreted this change as a sign of mechanical allodynia. Signs of mechanical allodynia were significantly relieved by a systemic injection of PTL (a mixed alpha1- and alpha2-AR antagonist) or terazosin (TRZ, an alpha1-AR antagonist) but not by various alpha2-AR antagonists (idazoxan, rauwolscine, or yohimbine), suggesting that the alpha1-AR is in part the mediator of the signs of mechanical allodynia. Ongoing ectopic discharges were recorded from injured afferents in fascicles of the L5 dorsal root of the neuropathic rat with an in vivo recording setup. Ongoing discharge rate was significantly reduced after intraperitoneal injection of PTL or TRZ but not by idazoxan. In addition, by using an in vitro recording setup, spontaneous activity was recorded from teased dorsal root fibers in a segment in which the spinal nerve was previously ligated. Application of epinephrine to the perfusion bath enhanced ongoing discharges. This evoked activity was blocked by pretreatment with TRZ but not with idazoxan. This study demonstrated that both behavioral signs of mechanical allodynia and ectopic discharges of injured afferents in the Lewis neuropathic rat are in part mediated by mechanisms involving alpha1-ARs. These results suggest that the sympathetic dependency of neuropathic pain in the Lewis strain of the rat is mediated by the alpha1 subtype of AR. (+info)Characterization of antiallodynic actions of ALE-0540, a novel nerve growth factor receptor antagonist, in the rat. (4/562)
There is growing evidence that nerve growth factor (NGF) may function as a mediator of persistent pain states. We have identified a novel nonpeptidic molecule, ALE-0540, that inhibits the binding of NGF to tyrosine kinase (Trk) A or both p75 and TrkA (IC50 5.88 +/- 1. 87 microM, 3.72 +/- 1.3 microM, respectively), as well as signal transduction and biological responses mediated by TrkA receptors. ALE-0540 was tested in models of neuropathic pain and thermally-induced inflammatory pain, using two routes of administration, a systemic i.p. and a spinal intrathecal (i.th.) route. Morphine was also tested for comparison in the antiallodynia model using mechanical stimuli. We show that either i.p. or i.th. administration of ALE-0540 in rats produced antiallodynia in the L5/L6 ligation model of neuropathic pain. The calculated A50 values (and 95% confidence intervals) for ALE-0540 administered i.p. and i. th. were 38 (17.5-83) mg/kg and 34.6 (17.3-69.4) microgram, respectively. ALE-0540 given i.th., at doses of 30 and 60 microgram, also blocked tactile allodynia in the thermal sensitization model. Although morphine displayed greater potency [A50 value of 7.1 (5.6-8. 8) mg/kg] than ALE-0540 in anti-allodynic effect when given i.p. to L5/L6-ligated rats, it was not active when administered i.th. These data suggest that a blockade of NGF bioactivity using a NGF receptor antagonist is capable of blocking neuropathic and inflammatory pain and further support the hypothesis that NGF is involved in signaling pathways associated with these pain states. ALE-0540 represents a nonpeptidic small molecule which can be used to examine mechanisms leading to the development of agents for the treatment of pain. (+info)The structural effect of systemic NGF treatment on permanently axotomised dorsal root ganglion cells in adult rats. (5/562)
The effect of systemic NGF treatment on loss and shrinkage of dorsal root ganglion cells was studied in adult male rats after permanent axotomy. Nineteen 16 to 18-wk-old rats had their right 5th lumbar spinal nerve ligated and cut approximately 7 mm peripheral to the ganglion. Two days before the operation, treatment with subcutaneous injections of human recombinant NGF (1.0-0.5 mg/kg/day) was started in 9 test rats; 10 controls were given saline injections. After 1 mo the levels of substance P (SP) and calcitonin gene related peptide (CGRP) were significantly increased in intact sciatic nerve. The number and mean volume of perikarya were estimated using assumption-free stereological techniques including vertical sections, the Cavalieri principle, optical disectors, the planar rotator and systematic sampling techniques. Systemic NGF administration had no influence on survival of primary sensory neurons after axotomy. The number of perikarya was 14300 (S.D. = 1800) in axotomised ganglia in control rats versus 14700 (S.D. = 2100) in axotomised ganglia of NGF treated rats. The reduction of perikarya volume after axotomy was significantly less after NGF treatment (11600 microm3 in the control group versus 8000 microm3 in the NGF treated group). However, the apparent protection of NGF-treatment on perikaryal volume is explained by a hitherto unrecognised size effect on nonaxotomised dorsal root ganglion cells. The untreated rats had a mean volume of 24700 microm3 (S.D. = 2700 microm3) whereas rats treated with NGF had a volume of 20400 microm3 (S.D. = 1700 microm3) on the nonaxotomised side. In conclusion, systemic NGF treatment in adult rats has no effect on dorsal root ganglion cell loss in permanent axotomy whereas perikaryal size of intact nonaxotomised cells is reduced. (+info)External oblique abdominal muscle: a new look on its blood supply and innervation. (6/562)
Numerous reports have discussed the use of the external oblique abdominal muscle as a pedicled or a free flap for defect coverage. A detailed description of the supplying vessels and nerves is a prerequisite for successful tissue transfer but so far is not available in the literature. A study of the arteries and nerves supplying the external oblique abdominal muscle was carried out in 42 cadavers after injection of a mixture of latex and bariumsulfate. In seven fresh cadavers the motor branches were identified with the Karnovsky technique. Three different groups of arteries were identified as the nurturing vessels. The cranial part of the muscle is supplied by two branches of the intercostal arteries. While the lateral branches run on the outer surface of the muscle together with the nerves, the anterior branches enter the muscle from its inner surface. The caudal part of the muscle derives its main blood supply from one or two branches of the deep circumflex iliac artery (94.7%) or the iliolumbar artery (5.3%). The external oblique abdominal muscle is innervated by motor branches of the lateral cutaneous branches of the anterior spinal nerves in a segmental pattern. With the exception of the subcostal nerve the motor branches enter the outer surface of the muscle digitation arising from the rib above. The results show that the cranial half of the external oblique abdominal muscle has a strictly segmental blood and nerve supply while the caudal half of the muscle derives its main blood supply from one artery but still shows a segmental innervation. (+info)Neuronal nitric oxide synthase mRNA upregulation in rat sensory neurons after spinal nerve ligation: lack of a role in allodynia development. (7/562)
Pharmacological evidence suggests a functional role for spinal nitric oxide (NO) in the modulation of thermal and/or inflammatory hyperalgesia. To assess the role of NO in nerve injury-induced tactile allodynia, we examined neuronal NO synthase (nNOS) expression in the spinal cord and dorsal root ganglia (DRG) of rats with tactile allodynia because of either tight ligation of the left fifth and sixth lumbar spinal nerves or streptozotocin-induced diabetic neuropathy. RNase protection assays indicated that nNOS mRNA (1) was upregulated in DRG, but not spinal cord, neurons on the injury side beginning 1 d after nerve ligation, (2) peaked (approximately 10-fold increase) at 2 d, and (3) remained elevated for at least 13 weeks. A corresponding increase in DRG nNOS protein was also observed and localized principally to small and occasionally medium-size sensory neurons. In rats with diabetic neuropathy, there was no significant change in DRG nNOS mRNA. However, similar increases in DRG nNOS mRNA were observed in rats that did not develop allodynia after nerve ligation and in rats fully recovered from allodynia 3 months after the nerve ligation. Systemic treatment with a specific pharmacological inhibitor of nNOS failed to prevent or reverse allodynia in nerve-injured rats. Thus, regulation of nNOS may contribute to the development of neuronal plasticity after specific types of peripheral nerve injury. However, upregulation of nNOS is not responsible for the development and/or maintenance of allodynia after nerve injury. (+info)Sex differences in cholinergic analgesia II: differing mechanisms in two models of allodynia. (8/562)
BACKGROUND: Cholinergic agents reduce allodynia after nerve injury in animals and may be useful in the treatment of neuropathic pain. Intrathecally administered neostigmine and neuronal nicotinic agonists are more potent in female than in male rats against acute thermal noxious stimuli. The purpose of this study was to determine whether there is also a sex difference in the antiallodynic effects of intrathecal cholinomimetic agents in two models of allodynia and to test their pharmacologic mechanisms. METHODS: Male and female rats with indwelling intrathecal catheters received injections of neostigmine, bethanechol (muscarinic agonist), RJR-2403 (neuronal nicotinic agonist) alone or with atropine (muscarinic antagonist), mecamylamine (nicotinic antagonist), phentolamine (alpha-adrenergic antagonist), or saline control. The effect of these agents was determined on mechanical allodynia produced by either intraplantar injection of capsaicin or ligation of spinal nerves. RESULTS: Neostigmine and RJR-2403 but not bethanechol were more potent in female than in male rats in reducing allodynia after nerve injury, and antagonist studies were also consistent with a nicotinic component to explain this sex difference. Phentolamine did not reverse neostigmine's effect. In contrast, for capsaicin-induced allodynia, neostigmine plus mecamylamine but not neostigmine or RJR-2403 was more potent in female than in male rats. CONCLUSIONS: These data demonstrate a sex difference of intrathecal neostigmine after nerve injury-induced allodynia similar to that observed in normal animals that received acute noxious thermal stimulation. However, this sex difference is not universal to all pain models because it was not present after intradermal capsaicin injection, nor is its interaction with spinal noradrenergic mechanisms consistent in all models. (+info)Spinal nerves are the bundles of nerve fibers that transmit signals between the spinal cord and the rest of the body. There are 31 pairs of spinal nerves in the human body, which can be divided into five regions: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve carries both sensory information (such as touch, temperature, and pain) from the periphery to the spinal cord, and motor information (such as muscle control) from the spinal cord to the muscles and other structures in the body. Spinal nerves also contain autonomic fibers that regulate involuntary functions such as heart rate, digestion, and blood pressure.
Spinal nerve roots are the initial parts of spinal nerves that emerge from the spinal cord through the intervertebral foramen, which are small openings between each vertebra in the spine. These nerve roots carry motor, sensory, and autonomic fibers to and from specific regions of the body. There are 31 pairs of spinal nerve roots in total, with 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal pair. Each root has a dorsal (posterior) and ventral (anterior) ramus that branch off to form the peripheral nervous system. Irritation or compression of these nerve roots can result in pain, numbness, weakness, or loss of reflexes in the affected area.
The spinal cord is a major part of the nervous system, extending from the brainstem and continuing down to the lower back. It is a slender, tubular bundle of nerve fibers (axons) and support cells (glial cells) that carries signals between the brain and the rest of the body. The spinal cord primarily serves as a conduit for motor information, which travels from the brain to the muscles, and sensory information, which travels from the body to the brain. It also contains neurons that can independently process and respond to information within the spinal cord without direct input from the brain.
The spinal cord is protected by the bony vertebral column (spine) and is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each segment corresponds to a specific region of the body and gives rise to pairs of spinal nerves that exit through the intervertebral foramina at each level.
The spinal cord is responsible for several vital functions, including:
1. Reflexes: Simple reflex actions, such as the withdrawal reflex when touching a hot surface, are mediated by the spinal cord without involving the brain.
2. Muscle control: The spinal cord carries motor signals from the brain to the muscles, enabling voluntary movement and muscle tone regulation.
3. Sensory perception: The spinal cord transmits sensory information, such as touch, temperature, pain, and vibration, from the body to the brain for processing and awareness.
4. Autonomic functions: The sympathetic and parasympathetic divisions of the autonomic nervous system originate in the thoracolumbar and sacral regions of the spinal cord, respectively, controlling involuntary physiological responses like heart rate, blood pressure, digestion, and respiration.
Damage to the spinal cord can result in various degrees of paralysis or loss of sensation below the level of injury, depending on the severity and location of the damage.
Neuralgia is a type of pain that occurs along the pathway of a nerve, often caused by damage or irritation to the nerve. It is typically described as a sharp, stabbing, burning, or electric-shock like pain that can be severe and debilitating. Neuralgia can affect any nerve in the body, but it most commonly occurs in the facial area (trigeminal neuralgia) or in the nerves related to the spine (postherpetic neuralgia). The pain associated with neuralgia can be intermittent or constant and may be worsened by certain triggers such as touch, temperature changes, or movement. Treatment for neuralgia typically involves medications to manage pain, as well as other therapies such as nerve blocks, surgery, or lifestyle modifications.
Spinal cord injuries (SCI) refer to damage to the spinal cord that results in a loss of function, such as mobility or feeling. This injury can be caused by direct trauma to the spine or by indirect damage resulting from disease or degeneration of surrounding bones, tissues, or blood vessels. The location and severity of the injury on the spinal cord will determine which parts of the body are affected and to what extent.
The effects of SCI can range from mild sensory changes to severe paralysis, including loss of motor function, autonomic dysfunction, and possible changes in sensation, strength, and reflexes below the level of injury. These injuries are typically classified as complete or incomplete, depending on whether there is any remaining function below the level of injury.
Immediate medical attention is crucial for spinal cord injuries to prevent further damage and improve the chances of recovery. Treatment usually involves immobilization of the spine, medications to reduce swelling and pressure, surgery to stabilize the spine, and rehabilitation to help regain lost function. Despite advances in treatment, SCI can have a significant impact on a person's quality of life and ability to perform daily activities.
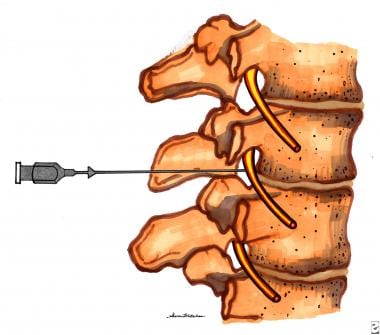
Spinal injections, also known as epidural injections or intrathecal injections, are medical procedures involving the injection of medications directly into the spinal canal. The medication is usually delivered into the space surrounding the spinal cord (the epidural space) or into the cerebrospinal fluid that surrounds and protects the spinal cord (the subarachnoid space).
The medications used in spinal injections can include local anesthetics, steroids, opioids, or a combination of these. The purpose of spinal injections is to provide diagnostic information, therapeutic relief, or both. They are commonly used to treat various conditions affecting the spine, such as radicular pain (pain that radiates down the arms or legs), disc herniation, spinal stenosis, and degenerative disc disease.
Spinal injections can be administered using different techniques, including fluoroscopy-guided injections, computed tomography (CT) scan-guided injections, or with the help of a nerve stimulator. These techniques ensure accurate placement of the medication and minimize the risk of complications.
It is essential to consult a healthcare professional for specific information regarding spinal injections and their potential benefits and risks.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
Ligation, in the context of medical terminology, refers to the process of tying off a part of the body, usually blood vessels or tissue, with a surgical suture or another device. The goal is to stop the flow of fluids such as blood or other substances within the body. It is commonly used during surgeries to control bleeding or to block the passage of fluids, gases, or solids in various parts of the body.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
Hyperalgesia is a medical term that describes an increased sensitivity to pain. It occurs when the nervous system, specifically the nociceptors (pain receptors), become excessively sensitive to stimuli. This means that a person experiences pain from a stimulus that normally wouldn't cause pain or experiences pain that is more intense than usual. Hyperalgesia can be a result of various conditions such as nerve damage, inflammation, or certain medications. It's an important symptom to monitor in patients with chronic pain conditions, as it may indicate the development of tolerance or addiction to pain medication.
Nerve fibers are specialized structures that constitute the long, slender processes (axons) of neurons (nerve cells). They are responsible for conducting electrical impulses, known as action potentials, away from the cell body and transmitting them to other neurons or effector organs such as muscles and glands. Nerve fibers are often surrounded by supportive cells called glial cells and are grouped together to form nerve bundles or nerves. These fibers can be myelinated (covered with a fatty insulating sheath called myelin) or unmyelinated, which influences the speed of impulse transmission.
Spinal ganglia, also known as dorsal root ganglia, are clusters of nerve cell bodies located in the peripheral nervous system. They are situated along the length of the spinal cord and are responsible for transmitting sensory information from the body to the brain. Each spinal ganglion contains numerous neurons, or nerve cells, with long processes called axons that extend into the periphery and innervate various tissues and organs. The cell bodies within the spinal ganglia receive sensory input from these axons and transmit this information to the central nervous system via the dorsal roots of the spinal nerves. This allows the brain to interpret and respond to a wide range of sensory stimuli, including touch, temperature, pain, and proprioception (the sense of the position and movement of one's body).
The lumbosacral region is the lower part of the back where the lumbar spine (five vertebrae in the lower back) connects with the sacrum (a triangular bone at the base of the spine). This region is subject to various conditions such as sprains, strains, herniated discs, and degenerative disorders that can cause pain and discomfort. It's also a common site for surgical intervention when non-surgical treatments fail to provide relief.
Peripheral Nervous System (PNS) diseases, also known as Peripheral Neuropathies, refer to conditions that affect the functioning of the peripheral nervous system, which includes all the nerves outside the brain and spinal cord. These nerves transmit signals between the central nervous system (CNS) and the rest of the body, controlling sensations, movements, and automatic functions such as heart rate and digestion.
PNS diseases can be caused by various factors, including genetics, infections, toxins, metabolic disorders, trauma, or autoimmune conditions. The symptoms of PNS diseases depend on the type and extent of nerve damage but often include:
1. Numbness, tingling, or pain in the hands and feet
2. Muscle weakness or cramps
3. Loss of reflexes
4. Decreased sensation to touch, temperature, or vibration
5. Coordination problems and difficulty with balance
6. Sexual dysfunction
7. Digestive issues, such as constipation or diarrhea
8. Dizziness or fainting due to changes in blood pressure
Examples of PNS diseases include Guillain-Barre syndrome, Charcot-Marie-Tooth disease, diabetic neuropathy, and peripheral nerve injuries. Treatment for these conditions varies depending on the underlying cause but may involve medications, physical therapy, lifestyle changes, or surgery.
Sprague-Dawley rats are a strain of albino laboratory rats that are widely used in scientific research. They were first developed by researchers H.H. Sprague and R.C. Dawley in the early 20th century, and have since become one of the most commonly used rat strains in biomedical research due to their relatively large size, ease of handling, and consistent genetic background.
Sprague-Dawley rats are outbred, which means that they are genetically diverse and do not suffer from the same limitations as inbred strains, which can have reduced fertility and increased susceptibility to certain diseases. They are also characterized by their docile nature and low levels of aggression, making them easier to handle and study than some other rat strains.
These rats are used in a wide variety of research areas, including toxicology, pharmacology, nutrition, cancer, and behavioral studies. Because they are genetically diverse, Sprague-Dawley rats can be used to model a range of human diseases and conditions, making them an important tool in the development of new drugs and therapies.
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. It is a complex phenomenon that can result from various stimuli, such as thermal, mechanical, or chemical irritation, and it can be acute or chronic. The perception of pain involves the activation of specialized nerve cells called nociceptors, which transmit signals to the brain via the spinal cord. These signals are then processed in different regions of the brain, leading to the conscious experience of pain. It's important to note that pain is a highly individual and subjective experience, and its perception can vary widely among individuals.
The optic nerve, also known as the second cranial nerve, is the nerve that transmits visual information from the retina to the brain. It is composed of approximately one million nerve fibers that carry signals related to vision, such as light intensity and color, from the eye's photoreceptor cells (rods and cones) to the visual cortex in the brain. The optic nerve is responsible for carrying this visual information so that it can be processed and interpreted by the brain, allowing us to see and perceive our surroundings. Damage to the optic nerve can result in vision loss or impairment.
Radiculopathy is a medical term that refers to the condition where there is damage or disturbance in the nerve roots as they exit the spinal column. These nerve roots, also known as radicles, can become damaged due to various reasons such as compression, inflammation, or injury, leading to a range of symptoms.
Radiculopathy may occur in any part of the spine, but it is most commonly found in the cervical (neck) and lumbar (lower back) regions. When the nerve roots in the cervical region are affected, it can result in symptoms such as neck pain, shoulder pain, arm pain, numbness, tingling, or weakness in the arms or fingers. On the other hand, when the nerve roots in the lumbar region are affected, it can cause lower back pain, leg pain, numbness, tingling, or weakness in the legs or feet.
The symptoms of radiculopathy can vary depending on the severity and location of the damage to the nerve roots. In some cases, the condition may resolve on its own with rest and conservative treatment. However, in more severe cases, medical intervention such as physical therapy, medication, or surgery may be necessary to alleviate the symptoms and prevent further damage.
Pain threshold is a term used in medicine and research to describe the point at which a stimulus begins to be perceived as painful. It is an individual's subjective response and can vary from person to person based on factors such as their pain tolerance, mood, expectations, and cultural background.
The pain threshold is typically determined through a series of tests where gradually increasing levels of stimuli are applied until the individual reports feeling pain. This is often used in research settings to study pain perception and analgesic efficacy. However, it's important to note that the pain threshold should not be confused with pain tolerance, which refers to the maximum level of pain a person can endure.
Spinal cord neoplasms refer to abnormal growths or tumors within the spinal cord. These can be benign (non-cancerous) or malignant (cancerous). They originate from the cells within the spinal cord itself (primary tumors), or they may spread to the spinal cord from other parts of the body (metastatic tumors). Spinal cord neoplasms can cause various symptoms depending on their location and size, including back pain, neurological deficits, and even paralysis. Treatment options include surgery, radiation therapy, and chemotherapy.
Nerve compression syndromes refer to a group of conditions characterized by the pressure or irritation of a peripheral nerve, causing various symptoms such as pain, numbness, tingling, and weakness in the affected area. This compression can occur due to several reasons, including injury, repetitive motion, bone spurs, tumors, or swelling. Common examples of nerve compression syndromes include carpal tunnel syndrome, cubital tunnel syndrome, radial nerve compression, and ulnar nerve entrapment at the wrist or elbow. Treatment options may include physical therapy, splinting, medications, injections, or surgery, depending on the severity and underlying cause of the condition.
Nerve regeneration is the process of regrowth and restoration of functional nerve connections following damage or injury to the nervous system. This complex process involves various cellular and molecular events, such as the activation of support cells called glia, the sprouting of surviving nerve fibers (axons), and the reformation of neural circuits. The goal of nerve regeneration is to enable the restoration of normal sensory, motor, and autonomic functions impaired due to nerve damage or injury.
Mononeuropathy is a medical condition that refers to damage or dysfunction affecting a single peripheral nerve, outside of the brain and spinal cord. This can result in weakness, numbness, or pain in the area served by that specific nerve. Mononeuropathies can occur due to various reasons such as trauma, compression, infection, or systemic diseases like diabetes. The symptoms and severity may vary depending on the type and location of the affected nerve.
Pain measurement, in a medical context, refers to the quantification or evaluation of the intensity and/or unpleasantness of a patient's subjective pain experience. This is typically accomplished through the use of standardized self-report measures such as numerical rating scales (NRS), visual analog scales (VAS), or categorical scales (mild, moderate, severe). In some cases, physiological measures like heart rate, blood pressure, and facial expressions may also be used to supplement self-reported pain ratings. The goal of pain measurement is to help healthcare providers better understand the nature and severity of a patient's pain in order to develop an effective treatment plan.
Posterior horn cells refer to the neurons located in the posterior (or dorsal) horn of the gray matter in the spinal cord. These cells are primarily responsible for receiving and processing sensory information from peripheral nerves, particularly related to touch, pressure, pain, and temperature. The axons of these cells form the ascending tracts that carry this information to the brain for further processing. It's worth noting that damage to posterior horn cells can result in various sensory deficits, such as those seen in certain neurological conditions.
Neuritis is a general term that refers to inflammation of a nerve or nerves, often causing pain, loss of function, and/or sensory changes. It can affect any part of the nervous system, including the peripheral nerves (those outside the brain and spinal cord) or the cranial nerves (those that serve the head and neck). Neuritis may result from various causes, such as infections, autoimmune disorders, trauma, toxins, or metabolic conditions. The specific symptoms and treatment depend on the underlying cause and the affected nerve(s).
Axotomy is a medical term that refers to the surgical cutting or severing of an axon, which is the long, slender projection of a neuron (nerve cell) that conducts electrical impulses away from the cell body and toward other cells. Axons are a critical component of the nervous system, allowing for communication between different parts of the body.
Axotomy is often used in research settings to study the effects of axonal injury on neuronal function and regeneration. This procedure can provide valuable insights into the mechanisms underlying neurodegenerative disorders and potential therapies for nerve injuries. However, it is important to note that axotomy can also have significant consequences for the affected neuron, including changes in gene expression, metabolism, and overall survival.
Peripheral nervous system (PNS) neoplasms refer to tumors that originate in the peripheral nerves, which are the nerves outside the brain and spinal cord. These tumors can be benign or malignant (cancerous). Benign tumors, such as schwannomas and neurofibromas, grow slowly and do not spread to other parts of the body. Malignant tumors, such as malignant peripheral nerve sheath tumors (MPNSTs), can invade nearby tissues and may metastasize (spread) to other organs.
PNS neoplasms can cause various symptoms depending on their location and size. Common symptoms include pain, weakness, numbness, or tingling in the affected area. In some cases, PNS neoplasms may not cause any symptoms until they become quite large. Treatment options for PNS neoplasms depend on several factors, including the type, size, and location of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Hyperesthesia is a medical term that refers to an increased sensitivity to sensory stimuli, including touch, pain, temperature, or sound. It can affect various parts of the body and can be a symptom of several different conditions, such as nerve damage, multiple sclerosis, or complex regional pain syndrome. Hyperesthesia can cause discomfort, pain, or even intense pain in response to light touch or other stimuli that would not normally cause such a reaction. Treatment for hyperesthesia depends on the underlying cause and may include medications, physical therapy, or other interventions.
Physical stimulation, in a medical context, refers to the application of external forces or agents to the body or its tissues to elicit a response. This can include various forms of touch, pressure, temperature, vibration, or electrical currents. The purpose of physical stimulation may be therapeutic, as in the case of massage or physical therapy, or diagnostic, as in the use of reflex tests. It is also used in research settings to study physiological responses and mechanisms.
In a broader sense, physical stimulation can also refer to the body's exposure to physical activity or exercise, which can have numerous health benefits, including improving cardiovascular function, increasing muscle strength and flexibility, and reducing the risk of chronic diseases.
Afferent neurons, also known as sensory neurons, are a type of nerve cell that conducts impulses or signals from peripheral receptors towards the central nervous system (CNS), which includes the brain and spinal cord. These neurons are responsible for transmitting sensory information such as touch, temperature, pain, sound, and light to the CNS for processing and interpretation. Afferent neurons have specialized receptor endings that detect changes in the environment and convert them into electrical signals, which are then transmitted to the CNS via synapses with other neurons. Once the signals reach the CNS, they are processed and integrated with other information to produce a response or reaction to the stimulus.
The lumbar vertebrae are the five largest and strongest vertebrae in the human spine, located in the lower back region. They are responsible for bearing most of the body's weight and providing stability during movement. The lumbar vertebrae have a characteristic shape, with a large body in the front, which serves as the main weight-bearing structure, and a bony ring in the back, formed by the pedicles, laminae, and processes. This ring encloses and protects the spinal cord and nerves. The lumbar vertebrae are numbered L1 to L5, starting from the uppermost one. They allow for flexion, extension, lateral bending, and rotation movements of the trunk.
Analgesics are a class of drugs that are used to relieve pain. They work by blocking the transmission of pain signals in the nervous system, allowing individuals to manage their pain levels more effectively. There are many different types of analgesics available, including both prescription and over-the-counter options. Some common examples include acetaminophen (Tylenol), ibuprofen (Advil or Motrin), and opioids such as morphine or oxycodone.
The choice of analgesic will depend on several factors, including the type and severity of pain being experienced, any underlying medical conditions, potential drug interactions, and individual patient preferences. It is important to use these medications as directed by a healthcare provider, as misuse or overuse can lead to serious side effects and potential addiction.
In addition to their pain-relieving properties, some analgesics may also have additional benefits such as reducing inflammation (like in the case of nonsteroidal anti-inflammatory drugs or NSAIDs) or causing sedation (as with certain opioids). However, it is essential to weigh these potential benefits against the risks and side effects associated with each medication.
When used appropriately, analgesics can significantly improve a person's quality of life by helping them manage their pain effectively and allowing them to engage in daily activities more comfortably.
Spinal cord diseases refer to a group of conditions that affect the spinal cord, which is a part of the central nervous system responsible for transmitting messages between the brain and the rest of the body. These diseases can cause damage to the spinal cord, leading to various symptoms such as muscle weakness, numbness, pain, bladder and bowel dysfunction, and difficulty with movement and coordination.
Spinal cord diseases can be congenital or acquired, and they can result from a variety of causes, including infections, injuries, tumors, degenerative conditions, autoimmune disorders, and genetic factors. Some examples of spinal cord diseases include multiple sclerosis, spina bifida, spinal cord injury, herniated discs, spinal stenosis, and motor neuron diseases such as amyotrophic lateral sclerosis (ALS).
The treatment for spinal cord diseases varies depending on the underlying cause and severity of the condition. Treatment options may include medication, physical therapy, surgery, and rehabilitation. In some cases, the damage to the spinal cord may be irreversible, leading to permanent disability or paralysis.
Cyclohexanecarboxylic acids are a type of organic compound that consists of a cyclohexane ring, which is a six-carbon saturated hydrocarbon, substituted with a carboxylic acid group (-COOH). This group contains a carbon atom double bonded to an oxygen atom and single bonded to a hydroxyl group (-OH).
The cyclohexane ring can be in various forms, including the chair, boat, or twist-boat conformations, depending on the orientation of its constituent atoms. The carboxylic acid group can ionize to form a carboxylate anion, which is negatively charged and has a deprotonated hydroxyl group.
Cyclohexanecarboxylic acids have various applications in industry and research, including as intermediates in the synthesis of other chemicals, solvents, and pharmaceuticals. They can also be found naturally in some plants and microorganisms.
Spinal anesthesia is a type of regional anesthesia that involves injecting local anesthetic medication into the cerebrospinal fluid in the subarachnoid space, which is the space surrounding the spinal cord. This procedure is typically performed by introducing a needle into the lower back, between the vertebrae, to reach the subarachnoid space.
Once the local anesthetic is introduced into this space, it spreads to block nerve impulses from the corresponding levels of the spine, resulting in numbness and loss of sensation in specific areas of the body below the injection site. The extent and level of anesthesia depend on the amount and type of medication used, as well as the patient's individual response.
Spinal anesthesia is often used for surgeries involving the lower abdomen, pelvis, or lower extremities, such as cesarean sections, hernia repairs, hip replacements, and knee arthroscopies. It can also be utilized for procedures like epidural steroid injections to manage chronic pain conditions affecting the spine and lower limbs.
While spinal anesthesia provides effective pain relief during and after surgery, it may cause side effects such as low blood pressure, headache, or difficulty urinating. These potential complications should be discussed with the healthcare provider before deciding on this type of anesthesia.
Motor neurons are specialized nerve cells in the brain and spinal cord that play a crucial role in controlling voluntary muscle movements. They transmit electrical signals from the brain to the muscles, enabling us to perform actions such as walking, talking, and swallowing. There are two types of motor neurons: upper motor neurons, which originate in the brain's motor cortex and travel down to the brainstem and spinal cord; and lower motor neurons, which extend from the brainstem and spinal cord to the muscles. Damage or degeneration of these motor neurons can lead to various neurological disorders, such as amyotrophic lateral sclerosis (ALS) and spinal muscular atrophy (SMA).
Rhizotomy is a surgical procedure where the root(s) of a nerve are cut. It is often used to treat chronic pain, spasticity, or other neurological symptoms that have not responded to other treatments. In some cases, only a portion of the nerve root may be severed (selective rhizotomy), while in others the entire root may be cut (root transaction). The specific nerves targeted during a rhizotomy depend on the individual patient's condition and symptoms.
This procedure is typically performed by a neurosurgeon, and it can be done through an open surgical approach or using minimally invasive techniques such as endoscopic or percutaneous approaches. After the surgery, patients may require physical therapy to help regain strength and mobility in the affected area. Potential risks of rhizotomy include numbness, weakness, and loss of reflexes in the areas served by the severed nerves.
Sciatica is not a medical condition itself but rather a symptom of an underlying medical problem. It's typically described as pain that radiates along the sciatic nerve, which runs from your lower back through your hips and buttocks and down each leg.
The pain can vary widely, from a mild ache to a sharp, burning sensation or excruciating discomfort. Sometimes, the pain is severe enough to make moving difficult. Sciatica most commonly occurs when a herniated disk, bone spur on the spine, or narrowing of the spine (spinal stenosis) compresses part of the nerve.
While sciatica can be quite painful, it's not typically a sign of permanent nerve damage and can often be relieved with non-surgical treatments. However, if the pain is severe or persists for a long period, it's essential to seek medical attention as it could indicate a more serious underlying condition.
A nerve block is a medical procedure in which an anesthetic or neurolytic agent is injected near a specific nerve or bundle of nerves to block the transmission of pain signals from that area to the brain. This technique can be used for both diagnostic and therapeutic purposes, such as identifying the source of pain, providing temporary or prolonged relief, or facilitating surgical procedures in the affected region.
The injection typically contains a local anesthetic like lidocaine or bupivacaine, which numbs the nerve, preventing it from transmitting pain signals. In some cases, steroids may also be added to reduce inflammation and provide longer-lasting relief. Depending on the type of nerve block and its intended use, the injection might be administered close to the spine (neuraxial blocks), at peripheral nerves (peripheral nerve blocks), or around the sympathetic nervous system (sympathetic nerve blocks).
While nerve blocks are generally safe, they can have side effects such as infection, bleeding, nerve damage, or in rare cases, systemic toxicity from the anesthetic agent. It is essential to consult with a qualified medical professional before undergoing this procedure to ensure proper evaluation, technique, and post-procedure care.
Peripheral nervous system (PNS) agents are a category of pharmaceutical drugs that act on the peripheral nervous system, which includes all the nerves outside the central nervous system (the brain and spinal cord). These agents can be further classified into various subgroups based on their specific mechanisms of action and therapeutic effects. Here are some examples:
1. Local anesthetics: These drugs block nerve impulses by inhibiting the sodium channels in the neuronal membrane, thereby preventing the generation and transmission of nerve impulses. They are commonly used to provide local or regional anesthesia during surgical procedures or to manage pain. Examples include lidocaine, bupivacaine, and prilocaine.
2. Neuropathic pain agents: These drugs are used to treat neuropathic pain, which is caused by damage or dysfunction of the peripheral nerves. They can act on various targets, including sodium channels, N-methyl-D-aspartate (NMDA) receptors, and voltage-gated calcium channels. Examples include gabapentin, pregabalin, duloxetine, and amitriptyline.
3. Muscle relaxants: These drugs act on the skeletal muscle to reduce muscle tone and spasticity. They can be classified into two main categories: centrally acting muscle relaxants (e.g., baclofen, tizanidine) and peripherally acting muscle relaxants (e.g., cyclobenzaprine, carisoprodol).
4. Cholinergic agents: These drugs act on the cholinergic receptors in the PNS to modulate nerve impulse transmission. They can be further classified into muscarinic and nicotinic agonists or antagonists, depending on their specific mechanism of action. Examples include neostigmine, pyridostigmine, and physostigmine.
5. Sympathomimetic agents: These drugs stimulate the sympathetic nervous system, which is part of the PNS that regulates the "fight or flight" response. They can be used to treat various conditions, such as hypotension, bronchospasm, and nasal congestion. Examples include epinephrine, norepinephrine, phenylephrine, and pseudoephedrine.
6. Sympatholytic agents: These drugs block the sympathetic nervous system to reduce its activity. They can be used to treat various conditions, such as hypertension, tachycardia, and anxiety. Examples include beta-blockers (e.g., propranolol, metoprolol), alpha-blockers (e.g., prazosin, doxazosin), and combined alpha-beta blockers (e.g., labetalol, carvedilol).
7. Neuropathic pain agents: These drugs are used to treat neuropathic pain, which is caused by damage or dysfunction of the nervous system. They can act on various targets in the PNS, such as sodium channels, N-methyl-D-aspartate (NMDA) receptors, and opioid receptors. Examples include lidocaine, capsaicin, tramadol, and tapentadol.
8. Antiepileptic drugs: These drugs are used to treat epilepsy, which is a neurological disorder characterized by recurrent seizures. They can act on various targets in the PNS, such as sodium channels, calcium channels, and GABA receptors. Examples include phenytoin, carbamazepine, valproate, lamotrigine, topiramate, and levetiracetam.
9. Antidepressant drugs: These drugs are used to treat depression, which is a mental disorder characterized by persistent low mood and loss of interest in activities. They can act on various targets in the PNS, such as serotonin receptors, norepinephrine receptors, and dopamine receptors. Examples include selective serotonin reuptake inhibitors (SSRIs) (e.g., fluoxetine, sertraline), serotonin-norepinephrine reuptake inhibitors (SNRIs) (e.g., venlafaxine, duloxetine), tricyclic antidepressants (TCAs) (e.g., amitriptyline, imipramine), and monoamine oxidase inhibitors (MAOIs) (e.g., phenelzine, selegiline).
10. Antipsychotic drugs: These drugs are used to treat psychosis, which is a mental disorder characterized by hallucinations, delusions, and disordered thought processes. They can act on various targets in the PNS, such as dopamine receptors, serotonin receptors, and histamine receptors. Examples include typical antipsychotics (e.g., haloperidol, chlorpromazine) and atypical antipsychotics (e.g., clozapine, risperidone).
11. Anxiolytic drugs: These drugs are used to treat anxiety disorders, which are mental disorders characterized by excessive fear, worry, or nervousness. They can act on various targets in the PNS, such as GABA receptors and benzodiazepine receptors. Examples include benzodiazepines (e.g., diazepam, alprazolam), buspirone, and hydroxyzine.
12. Sedative drugs: These drugs are used to induce sleep or reduce excitement. They can act on various targets in the PNS, such as GABA receptors and histamine receptors. Examples include barbiturates (e.g., phenobarbital, secobarbital), benzodiazepines (e.g., diazepam, temazepam), and antihistamines (e.g., diphenhydramine, doxylamine).
13. Hypnotic drugs: These drugs are used to induce sleep. They can act on various targets in the PNS, such as GABA receptors and benzodiazepine receptors. Examples include benzodiazepines (e.g., triazolam, flunitrazepam) and non-benzodiazepine hypnotics (e.g., zolpidem, eszopiclone).
14. Antidepressant drugs: These drugs are used to treat depression, which is a mental disorder characterized by persistent feelings of sadness, hopelessness, or worthlessness. They can act on various targets in the PNS, such as serotonin receptors and norepinephrine transporters. Examples include selective serotonin reuptake inhibitors (e.g., fluoxetine, sertraline), tricyclic antidepressants (e.g., amitriptyline, imipramine), and monoamine oxidase inhibitors (e.g., phenelzine, selegiline).
15. Anxiolytic drugs: These drugs are used to reduce anxiety, which is a feeling of fear, worry, or unease. They can act on various targets in the PNS, such as GABA receptors and benzodiazepine receptors. Examples include benzodiazepines (e.g., alprazolam, lorazepam), buspirone, and hydroxyzine.
16. Antipsychotic drugs: These drugs are used to treat psychosis, which is a mental disorder characterized by hallucinations, delusions, or disordered thinking. They can act on various targets in the PNS, such as dopamine receptors and serotonin receptors. Examples include typical antipsychotics (e.g., haloperidol, chlorpromazine) and atypical antipsychotics (e.g., risperidone, olanzapine).
17. Mood stabilizers: These drugs are used to treat mood disorders, such as bipolar disorder or major depressive disorder. They can act on various targets in the PNS, such as sodium channels and GABA receptors. Examples include lithium, valproic acid, and carbamazepine.
18. Stimulants: These drugs are used to treat attention deficit hyperactivity disorder (ADHD) or narcolepsy. They can act on various targets in the PNS, such as dopamine transporters and norepinephrine transporters. Examples include amphetamine, methylphenidate, and modafinil.
19. Antihistamines: These drugs are used to treat allergies or symptoms of the common cold. They can act on various targets in the PNS, such as histamine receptors and muscarinic acetylcholine receptors. Examples include diphenhydramine, loratadine, and cetirizine.
20. Antiemetics: These
The spinal canal is the bony, protective channel within the vertebral column that contains and houses the spinal cord. It extends from the foramen magnum at the base of the skull to the sacrum, where the spinal cord ends and forms the cauda equina. The spinal canal is formed by a series of vertebral bodies stacked on top of each other, intervertebral discs in between them, and the laminae and spinous processes that form the posterior elements of the vertebrae. The spinal canal provides protection to the spinal cord from external trauma and contains cerebrospinal fluid (CSF) that circulates around the cord, providing nutrients and cushioning. Any narrowing or compression of the spinal canal, known as spinal stenosis, can cause various neurological symptoms due to pressure on the spinal cord or nerve roots.
Intercostal nerves are the bundles of nerve fibers that originate from the thoracic spinal cord (T1 to T11) and provide sensory and motor innervation to the thorax, abdomen, and walls of the chest. They run between the ribs (intercostal spaces), hence the name intercostal nerves.
Each intercostal nerve has two components:
1. The lateral cutaneous branch: This branch provides sensory innervation to the skin on the side of the chest wall and abdomen.
2. The anterior cutaneous branch: This branch provides sensory innervation to the skin on the front of the chest and abdomen.
Additionally, each intercostal nerve also gives off a muscular branch that supplies motor innervation to the intercostal muscles (the muscles between the ribs) and the upper abdominal wall muscles. The lowest intercostal nerve (T11) also provides sensory innervation to a small area of skin over the buttock.
Intercostal nerves are important in clinical practice, as they can be affected by various conditions such as herpes zoster (shingles), rib fractures, or thoracic outlet syndrome, leading to pain and sensory changes in the chest wall.
An axon is a long, slender extension of a neuron (a type of nerve cell) that conducts electrical impulses (nerve impulses) away from the cell body to target cells, such as other neurons or muscle cells. Axons can vary in length from a few micrometers to over a meter long and are typically surrounded by a myelin sheath, which helps to insulate and protect the axon and allows for faster transmission of nerve impulses.
Axons play a critical role in the functioning of the nervous system, as they provide the means by which neurons communicate with one another and with other cells in the body. Damage to axons can result in serious neurological problems, such as those seen in spinal cord injuries or neurodegenerative diseases like multiple sclerosis.
Myelinated nerve fibers are neuronal processes that are surrounded by a myelin sheath, a fatty insulating substance that is produced by Schwann cells in the peripheral nervous system and oligodendrocytes in the central nervous system. This myelin sheath helps to increase the speed of electrical impulse transmission, also known as action potentials, along the nerve fiber. The myelin sheath has gaps called nodes of Ranvier where the electrical impulses can jump from one node to the next, which also contributes to the rapid conduction of signals. Myelinated nerve fibers are typically found in the peripheral nerves and the optic nerve, but not in the central nervous system (CNS) tracts that are located within the brain and spinal cord.
Nerve endings, also known as terminal branches or sensory receptors, are the specialized structures present at the termination point of nerve fibers (axons) that transmit electrical signals to and from the central nervous system (CNS). They primarily function in detecting changes in the external environment or internal body conditions and converting them into electrical impulses.
There are several types of nerve endings, including:
1. Free Nerve Endings: These are unencapsulated nerve endings that respond to various stimuli like temperature, pain, and touch. They are widely distributed throughout the body, especially in the skin, mucous membranes, and visceral organs.
2. Encapsulated Nerve Endings: These are wrapped by specialized connective tissue sheaths, which can modify their sensitivity to specific stimuli. Examples include Pacinian corpuscles (responsible for detecting deep pressure and vibration), Meissner's corpuscles (for light touch), Ruffini endings (for stretch and pressure), and Merkel cells (for sustained touch).
3. Specialised Nerve Endings: These are nerve endings that respond to specific stimuli, such as auditory, visual, olfactory, gustatory, and vestibular information. They include hair cells in the inner ear, photoreceptors in the retina, taste buds in the tongue, and olfactory receptors in the nasal cavity.
Nerve endings play a crucial role in relaying sensory information to the CNS for processing and initiating appropriate responses, such as reflex actions or conscious perception of the environment.
The sural nerve is a purely sensory peripheral nerve in the lower leg and foot. It provides sensation to the outer ( lateral) aspect of the little toe and the adjacent side of the fourth toe, as well as a small portion of the skin on the back of the leg between the ankle and knee joints.
The sural nerve is formed by the union of branches from the tibial and common fibular nerves (branches of the sciatic nerve) in the lower leg. It runs down the calf, behind the lateral malleolus (the bony prominence on the outside of the ankle), and into the foot.
The sural nerve is often used as a donor nerve during nerve grafting procedures due to its consistent anatomy and relatively low risk for morbidity at the donor site.
The Tibial nerve is a major branch of the sciatic nerve that originates in the lower back and runs through the buttock and leg. It provides motor (nerve impulses that control muscle movement) and sensory (nerve impulses that convey information about touch, temperature, and pain) innervation to several muscles and skin regions in the lower limb.
More specifically, the Tibial nerve supplies the following structures:
1. Motor Innervation: The Tibial nerve provides motor innervation to the muscles in the back of the leg (posterior compartment), including the calf muscles (gastrocnemius and soleus) and the small muscles in the foot (intrinsic muscles). These muscles are responsible for plantarflexion (pointing the foot downward) and inversion (turning the foot inward) of the foot.
2. Sensory Innervation: The Tibial nerve provides sensory innervation to the skin on the sole of the foot, as well as the heel and some parts of the lower leg.
The Tibial nerve travels down the leg, passing behind the knee and through the calf, where it eventually joins with the common fibular (peroneal) nerve to form the tibial-fibular trunk. This trunk then divides into several smaller nerves that innervate the foot's intrinsic muscles and skin.
Damage or injury to the Tibial nerve can result in various symptoms, such as weakness or paralysis of the calf and foot muscles, numbness or tingling sensations in the sole of the foot, and difficulty walking or standing on tiptoes.
Animal disease models are specialized animals, typically rodents such as mice or rats, that have been genetically engineered or exposed to certain conditions to develop symptoms and physiological changes similar to those seen in human diseases. These models are used in medical research to study the pathophysiology of diseases, identify potential therapeutic targets, test drug efficacy and safety, and understand disease mechanisms.
The genetic modifications can include knockout or knock-in mutations, transgenic expression of specific genes, or RNA interference techniques. The animals may also be exposed to environmental factors such as chemicals, radiation, or infectious agents to induce the disease state.
Examples of animal disease models include:
1. Mouse models of cancer: Genetically engineered mice that develop various types of tumors, allowing researchers to study cancer initiation, progression, and metastasis.
2. Alzheimer's disease models: Transgenic mice expressing mutant human genes associated with Alzheimer's disease, which exhibit amyloid plaque formation and cognitive decline.
3. Diabetes models: Obese and diabetic mouse strains like the NOD (non-obese diabetic) or db/db mice, used to study the development of type 1 and type 2 diabetes, respectively.
4. Cardiovascular disease models: Atherosclerosis-prone mice, such as ApoE-deficient or LDLR-deficient mice, that develop plaque buildup in their arteries when fed a high-fat diet.
5. Inflammatory bowel disease models: Mice with genetic mutations affecting intestinal barrier function and immune response, such as IL-10 knockout or SAMP1/YitFc mice, which develop colitis.
Animal disease models are essential tools in preclinical research, but it is important to recognize their limitations. Differences between species can affect the translatability of results from animal studies to human patients. Therefore, researchers must carefully consider the choice of model and interpret findings cautiously when applying them to human diseases.
The lumbosacral plexus is a complex network of nerves that arises from the lower part of the spinal cord, specifically the lumbar (L1-L5) and sacral (S1-S4) roots. This plexus is responsible for providing innervation to the lower extremities, including the legs, feet, and some parts of the abdomen and pelvis.
The lumbosacral plexus can be divided into several major branches:
1. The femoral nerve: It arises from the L2-L4 roots and supplies motor innervation to the muscles in the anterior compartment of the thigh, as well as sensation to the anterior and medial aspects of the leg and thigh.
2. The obturator nerve: It originates from the L2-L4 roots and provides motor innervation to the adductor muscles of the thigh and sensation to the inner aspect of the thigh.
3. The sciatic nerve: This is the largest nerve in the body, formed by the union of the tibial and common fibular (peroneal) nerves. It arises from the L4-S3 roots and supplies motor innervation to the muscles of the lower leg and foot, as well as sensation to the posterior aspect of the leg and foot.
4. The pudendal nerve: It originates from the S2-S4 roots and is responsible for providing motor innervation to the pelvic floor muscles and sensory innervation to the genital region.
5. Other smaller nerves, such as the ilioinguinal, iliohypogastric, and genitofemoral nerves, also arise from the lumbosacral plexus and supply sensation to various regions in the lower abdomen and pelvis.
Damage or injury to the lumbosacral plexus can result in significant neurological deficits, including muscle weakness, numbness, and pain in the lower extremities.
The median nerve is one of the major nerves in the human body, providing sensation and motor function to parts of the arm and hand. It originates from the brachial plexus, a network of nerves that arise from the spinal cord in the neck. The median nerve travels down the arm, passing through the cubital tunnel at the elbow, and continues into the forearm and hand.
In the hand, the median nerve supplies sensation to the palm side of the thumb, index finger, middle finger, and half of the ring finger. It also provides motor function to some of the muscles that control finger movements, allowing for flexion of the fingers and opposition of the thumb.
Damage to the median nerve can result in a condition called carpal tunnel syndrome, which is characterized by numbness, tingling, and weakness in the hand and fingers.
Spinal diseases refer to a range of medical conditions that affect the spinal column, which is made up of vertebrae (bones), intervertebral discs, facet joints, nerves, ligaments, and muscles. These diseases can cause pain, discomfort, stiffness, numbness, weakness, or even paralysis, depending on the severity and location of the condition. Here are some examples of spinal diseases:
1. Degenerative disc disease: This is a condition where the intervertebral discs lose their elasticity and height, leading to stiffness, pain, and decreased mobility.
2. Herniated disc: This occurs when the inner material of the intervertebral disc bulges or herniates out through a tear in the outer layer, causing pressure on the spinal nerves and resulting in pain, numbness, tingling, or weakness in the affected area.
3. Spinal stenosis: This is a narrowing of the spinal canal or the neural foramen (the openings where the spinal nerves exit the spinal column), which can cause pressure on the spinal cord or nerves and result in pain, numbness, tingling, or weakness.
4. Scoliosis: This is a curvature of the spine that can occur in children or adults, leading to an abnormal posture, back pain, and decreased lung function.
5. Osteoarthritis: This is a degenerative joint disease that affects the facet joints in the spine, causing pain, stiffness, and decreased mobility.
6. Ankylosing spondylitis: This is a chronic inflammatory disease that affects the spine and sacroiliac joints, leading to pain, stiffness, and fusion of the vertebrae.
7. Spinal tumors: These are abnormal growths that can occur in the spinal column, which can be benign or malignant, causing pain, neurological symptoms, or even paralysis.
8. Infections: Bacterial or viral infections can affect the spine, leading to pain, fever, and other systemic symptoms.
9. Trauma: Fractures, dislocations, or sprains of the spine can occur due to accidents, falls, or sports injuries, causing pain, neurological deficits, or even paralysis.
Spinal cord compression is a medical condition that refers to the narrowing of the spinal canal, which puts pressure on the spinal cord and the nerves that branch out from it. This can occur due to various reasons such as degenerative changes in the spine, herniated discs, bone spurs, tumors, or fractures. The compression can lead to a range of symptoms including pain, numbness, tingling, weakness, or loss of bladder and bowel control. In severe cases, it can cause paralysis. Treatment options depend on the underlying cause and may include physical therapy, medication, surgery, or radiation therapy.
A nerve crush injury is a type of peripheral nerve injury that occurs when there is excessive pressure or compression applied to a nerve, causing it to become damaged or dysfunctional. This can happen due to various reasons such as trauma from accidents, surgical errors, or prolonged pressure on the nerve from tight casts, clothing, or positions.
The compression disrupts the normal functioning of the nerve, leading to symptoms such as numbness, tingling, weakness, or pain in the affected area. In severe cases, a nerve crush injury can cause permanent damage to the nerve, leading to long-term disability or loss of function. Treatment for nerve crush injuries typically involves relieving the pressure on the nerve, providing supportive care, and in some cases, surgical intervention may be necessary to repair the damaged nerve.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
Spinal neoplasms refer to abnormal growths or tumors found within the spinal column, which can be benign (non-cancerous) or malignant (cancerous). These tumors can originate in the spine itself, called primary spinal neoplasms, or they can spread to the spine from other parts of the body, known as secondary or metastatic spinal neoplasms. Spinal neoplasms can cause various symptoms, such as back pain, neurological deficits, and even paralysis, depending on their location and size. Early diagnosis and treatment are crucial to prevent or minimize long-term complications and improve the patient's prognosis.
'Animal behavior' refers to the actions or responses of animals to various stimuli, including their interactions with the environment and other individuals. It is the study of the actions of animals, whether they are instinctual, learned, or a combination of both. Animal behavior includes communication, mating, foraging, predator avoidance, and social organization, among other things. The scientific study of animal behavior is called ethology. This field seeks to understand the evolutionary basis for behaviors as well as their physiological and psychological mechanisms.
The Ulnar nerve is one of the major nerves in the forearm and hand, which provides motor function to the majority of the intrinsic muscles of the hand (except for those innervated by the median nerve) and sensory innervation to the little finger and half of the ring finger. It originates from the brachial plexus, passes through the cubital tunnel at the elbow, and continues down the forearm, where it runs close to the ulna bone. The ulnar nerve then passes through the Guyon's canal in the wrist before branching out to innervate the hand muscles and provide sensation to the skin on the little finger and half of the ring finger.
Spinal stenosis is a narrowing of the spinal canal or the neural foramina (the openings through which nerves exit the spinal column), typically in the lower back (lumbar) or neck (cervical) regions. This can put pressure on the spinal cord and/or nerve roots, causing pain, numbness, tingling, or weakness in the affected areas, often in the legs, arms, or hands. It's most commonly caused by age-related wear and tear, but can also be due to degenerative changes, herniated discs, tumors, or spinal injuries.
The femoral nerve is a major nerve in the thigh region of the human body. It originates from the lumbar plexus, specifically from the ventral rami (anterior divisions) of the second, third, and fourth lumbar nerves (L2-L4). The femoral nerve provides motor and sensory innervation to various muscles and areas in the lower limb.
Motor Innervation:
The femoral nerve is responsible for providing motor innervation to several muscles in the anterior compartment of the thigh, including:
1. Iliacus muscle
2. Psoas major muscle
3. Quadriceps femoris muscle (consisting of four heads: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius)
These muscles are involved in hip flexion, knee extension, and stabilization of the hip joint.
Sensory Innervation:
The sensory distribution of the femoral nerve includes:
1. Anterior and medial aspects of the thigh
2. Skin over the anterior aspect of the knee and lower leg (via the saphenous nerve, a branch of the femoral nerve)
The saphenous nerve provides sensation to the skin on the inner side of the leg and foot, as well as the medial malleolus (the bony bump on the inside of the ankle).
In summary, the femoral nerve is a crucial component of the lumbar plexus that controls motor functions in the anterior thigh muscles and provides sensory innervation to the anterior and medial aspects of the thigh and lower leg.
Sciatic neuropathy is a condition that results from damage or injury to the sciatic nerve, which is the largest nerve in the human body. The sciatic nerve originates from the lower spine (lumbar and sacral regions) and travels down through the buttocks, hips, and legs to the feet.
Sciatic neuropathy can cause various symptoms, including pain, numbness, tingling, weakness, or difficulty moving the affected leg or foot. The pain associated with sciatic neuropathy is often described as sharp, shooting, or burning and may worsen with movement, coughing, or sneezing.
The causes of sciatic neuropathy include compression or irritation of the nerve due to conditions such as herniated discs, spinal stenosis, bone spurs, tumors, or piriformis syndrome. Trauma or injury to the lower back, hip, or buttocks can also cause sciatic neuropathy.
Diagnosing sciatic neuropathy typically involves a physical examination and medical history, as well as imaging tests such as X-rays, MRI, or CT scans to visualize the spine and surrounding structures. Treatment options may include pain management, physical therapy, steroid injections, or surgery, depending on the severity and underlying cause of the condition.
Electric stimulation, also known as electrical nerve stimulation or neuromuscular electrical stimulation, is a therapeutic treatment that uses low-voltage electrical currents to stimulate nerves and muscles. It is often used to help manage pain, promote healing, and improve muscle strength and mobility. The electrical impulses can be delivered through electrodes placed on the skin or directly implanted into the body.
In a medical context, electric stimulation may be used for various purposes such as:
1. Pain management: Electric stimulation can help to block pain signals from reaching the brain and promote the release of endorphins, which are natural painkillers produced by the body.
2. Muscle rehabilitation: Electric stimulation can help to strengthen muscles that have become weak due to injury, illness, or surgery. It can also help to prevent muscle atrophy and improve range of motion.
3. Wound healing: Electric stimulation can promote tissue growth and help to speed up the healing process in wounds, ulcers, and other types of injuries.
4. Urinary incontinence: Electric stimulation can be used to strengthen the muscles that control urination and reduce symptoms of urinary incontinence.
5. Migraine prevention: Electric stimulation can be used as a preventive treatment for migraines by applying electrical impulses to specific nerves in the head and neck.
It is important to note that electric stimulation should only be administered under the guidance of a qualified healthcare professional, as improper use can cause harm or discomfort.
Spinal fusion is a surgical procedure where two or more vertebrae in the spine are fused together to create a solid bone. The purpose of this procedure is to restrict movement between the fused vertebrae, which can help reduce pain and stabilize the spine. This is typically done using bone grafts or bone graft substitutes, along with hardware such as rods, screws, or cages to hold the vertebrae in place while they heal together. The procedure may be recommended for various spinal conditions, including degenerative disc disease, spinal stenosis, spondylolisthesis, scoliosis, or fractures.
The spine, also known as the vertebral column, is a complex structure in the human body that is part of the axial skeleton. It is composed of 33 individual vertebrae (except in some people where there are fewer due to fusion of certain vertebrae), intervertebral discs, facet joints, ligaments, muscles, and nerves.
The spine has several important functions:
1. Protection: The spine protects the spinal cord, which is a major component of the nervous system, by enclosing it within a bony canal.
2. Support: The spine supports the head and upper body, allowing us to maintain an upright posture and facilitating movement of the trunk and head.
3. Movement: The spine enables various movements such as flexion (bending forward), extension (bending backward), lateral flexion (bending sideways), and rotation (twisting).
4. Weight-bearing: The spine helps distribute weight and pressure evenly across the body, reducing stress on individual vertebrae and other structures.
5. Blood vessel and nerve protection: The spine protects vital blood vessels and nerves that pass through it, including the aorta, vena cava, and spinal nerves.
The spine is divided into five regions: cervical (7 vertebrae), thoracic (12 vertebrae), lumbar (5 vertebrae), sacrum (5 fused vertebrae), and coccyx (4 fused vertebrae, also known as the tailbone). Each region has unique characteristics that allow for specific functions and adaptations to the body's needs.
Neural conduction is the process by which electrical signals, known as action potentials, are transmitted along the axon of a neuron (nerve cell) to transmit information between different parts of the nervous system. This electrical impulse is generated by the movement of ions across the neuronal membrane, and it propagates down the length of the axon until it reaches the synapse, where it can then stimulate the release of neurotransmitters to communicate with other neurons or target cells. The speed of neural conduction can vary depending on factors such as the diameter of the axon, the presence of myelin sheaths (which act as insulation and allow for faster conduction), and the temperature of the environment.
Unmyelinated nerve fibers, also known as unmyelinated axons or non-myelinated fibers, are nerve cells that lack a myelin sheath. Myelin is a fatty, insulating substance that surrounds the axon of many nerve cells and helps to increase the speed of electrical impulses traveling along the nerve fiber.
In unmyelinated nerve fibers, the axons are surrounded by a thin layer of Schwann cell processes called the endoneurium, but there is no continuous myelin sheath. Instead, the axons are packed closely together in bundles, with several axons lying within the same Schwann cell.
Unmyelinated nerve fibers tend to be smaller in diameter than myelinated fibers and conduct electrical impulses more slowly. They are commonly found in the autonomic nervous system, which controls involuntary functions such as heart rate, blood pressure, and digestion, as well as in sensory nerves that transmit pain and temperature signals.
Sensory receptor cells are specialized structures that convert physical stimuli from our environment into electrical signals, which are then transmitted to the brain for interpretation. These receptors can be found in various tissues throughout the body and are responsible for detecting sensations such as touch, pressure, temperature, taste, and smell. They can be classified into two main types: exteroceptors, which respond to stimuli from the external environment, and interoceptors, which react to internal conditions within the body. Examples of sensory receptor cells include hair cells in the inner ear, photoreceptors in the eye, and taste buds on the tongue.
The thoracic vertebrae are the 12 vertebrae in the thoracic region of the spine, which is the portion between the cervical and lumbar regions. These vertebrae are numbered T1 to T12, with T1 being closest to the skull and T12 connecting to the lumbar region.
The main function of the thoracic vertebrae is to provide stability and support for the chest region, including protection for the vital organs within, such as the heart and lungs. Each thoracic vertebra has costal facets on its sides, which articulate with the heads of the ribs, forming the costovertebral joints. This connection between the spine and the ribcage allows for a range of movements while maintaining stability.
The thoracic vertebrae have a unique structure compared to other regions of the spine. They are characterized by having long, narrow bodies, small bony processes, and prominent spinous processes that point downwards. This particular shape and orientation of the thoracic vertebrae contribute to their role in limiting excessive spinal movement and providing overall trunk stability.
Amines are organic compounds that contain a basic nitrogen atom with a lone pair of electrons. They are derived from ammonia (NH3) by replacing one or more hydrogen atoms with alkyl or aryl groups. The nomenclature of amines follows the substitutive type, where the parent compound is named as an aliphatic or aromatic hydrocarbon, and the functional group "amine" is designated as a suffix or prefix.
Amines are classified into three types based on the number of carbon atoms attached to the nitrogen atom:
1. Primary (1°) amines: One alkyl or aryl group is attached to the nitrogen atom.
2. Secondary (2°) amines: Two alkyl or aryl groups are attached to the nitrogen atom.
3. Tertiary (3°) amines: Three alkyl or aryl groups are attached to the nitrogen atom.
Quaternary ammonium salts have four organic groups attached to the nitrogen atom and a positive charge, with anions balancing the charge.
Amines have a wide range of applications in the chemical industry, including pharmaceuticals, dyes, polymers, and solvents. They also play a significant role in biological systems as neurotransmitters, hormones, and cell membrane components.
Spinal infusions, also known as intrathecal infusions, refer to the administration of medications directly into the spinal canal through a surgically implanted device. This device typically consists of a pump and a catheter. The pump is a small reservoir that contains the medication, while the catheter is a thin tube that delivers the medication to the intrathecal space, which is the area surrounding the spinal cord.
This route of administration is often used for the management of chronic pain, as well as for the treatment of certain neurological disorders such as spasticity and severe muscle spasms. The medications that are commonly administered through spinal infusions include local anesthetics, opioids, and muscle relaxants.
The main advantage of spinal infusions is that they allow for the delivery of medication directly to the site of action, which can result in more effective pain relief and fewer systemic side effects compared to systemic administration. However, there are also potential risks associated with this procedure, including infection, bleeding, and mechanical failure of the device. Therefore, spinal infusions should only be performed by trained medical professionals in a controlled clinical setting.
Nociceptors are specialized peripheral sensory neurons that detect and transmit signals indicating potentially harmful stimuli in the form of pain. They are activated by various noxious stimuli such as extreme temperatures, intense pressure, or chemical irritants. Once activated, nociceptors transmit these signals to the central nervous system (spinal cord and brain) where they are interpreted as painful sensations, leading to protective responses like withdrawing from the harmful stimulus or seeking medical attention. Nociceptors play a crucial role in our perception of pain and help protect the body from further harm.
Nerve Growth Factors (NGFs) are a family of proteins that play an essential role in the growth, maintenance, and survival of certain neurons (nerve cells). They were first discovered by Rita Levi-Montalcini and Stanley Cohen in 1956. NGF is particularly crucial for the development and function of the peripheral nervous system, which connects the central nervous system to various organs and tissues throughout the body.
NGF supports the differentiation and survival of sympathetic and sensory neurons during embryonic development. In adults, NGF continues to regulate the maintenance and repair of these neurons, contributing to neuroplasticity – the brain's ability to adapt and change over time. Additionally, NGF has been implicated in pain transmission and modulation, as well as inflammatory responses.
Abnormal levels or dysfunctional NGF signaling have been associated with various medical conditions, including neurodegenerative diseases (e.g., Alzheimer's and Parkinson's), chronic pain disorders, and certain cancers (e.g., small cell lung cancer). Therefore, understanding the role of NGF in physiological and pathological processes may provide valuable insights into developing novel therapeutic strategies for these conditions.
The cervical vertebrae are the seven vertebrae that make up the upper part of the spine, also known as the neck region. They are labeled C1 to C7, with C1 being closest to the skull and C7 connecting to the thoracic vertebrae in the chest region. The cervical vertebrae have unique structures to allow for a wide range of motion in the neck while also protecting the spinal cord and providing attachment points for muscles and ligaments.
The phrenic nerve is a motor nerve that originates from the cervical spine (C3-C5) and descends through the neck to reach the diaphragm, which is the primary muscle used for breathing. The main function of the phrenic nerve is to innervate the diaphragm and control its contraction and relaxation, thereby enabling respiration.
Damage or injury to the phrenic nerve can result in paralysis of the diaphragm, leading to difficulty breathing and potentially causing respiratory failure. Certain medical conditions, such as neuromuscular disorders, spinal cord injuries, and tumors, can affect the phrenic nerve and impair its function.
The trigeminal nerve, also known as the fifth cranial nerve or CNV, is a paired nerve that carries both sensory and motor information. It has three major branches: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic branch provides sensation to the forehead, eyes, and upper portion of the nose; the maxillary branch supplies sensation to the lower eyelid, cheek, nasal cavity, and upper lip; and the mandibular branch is responsible for sensation in the lower lip, chin, and parts of the oral cavity, as well as motor function to the muscles involved in chewing. The trigeminal nerve plays a crucial role in sensations of touch, pain, temperature, and pressure in the face and mouth, and it also contributes to biting, chewing, and swallowing functions.
Nerve Growth Factor (NGF) is a small secreted protein that is involved in the growth, maintenance, and survival of certain neurons (nerve cells). It was the first neurotrophin to be discovered and is essential for the development and function of the nervous system. NGF binds to specific receptors on the surface of nerve cells and helps to promote their differentiation, axonal growth, and synaptic plasticity. Additionally, NGF has been implicated in various physiological processes such as inflammation, immune response, and wound healing. Deficiencies or excesses of NGF have been linked to several neurological disorders, including Alzheimer's disease, Parkinson's disease, and pain conditions.
The Cauda Equina refers to a bundle of nerves at the lower end of the spinal cord within the vertebral column. It originates from the lumbar (L1-L5) and sacral (S1-S5) regions and looks like a horse's tail, hence the name "Cauda Equina" in Latin. These nerves are responsible for providing motor and sensory innervation to the lower extremities, bladder, bowel, and sexual organs. Any damage or compression to this region can lead to serious neurological deficits, such as bowel and bladder incontinence, sexual dysfunction, and lower limb weakness or paralysis.
Myelography is a medical imaging technique used to examine the spinal cord and surrounding structures, such as the spinal nerves, intervertebral discs, and the spinal column. This procedure involves the injection of a contrast dye into the subarachnoid space, which is the area surrounding the spinal cord filled with cerebrospinal fluid (CSF). The dye outlines the spinal structures, making them visible on X-ray or CT scan images.
The primary purpose of myelography is to diagnose various spinal conditions, including herniated discs, spinal stenosis, tumors, infection, and traumatic injuries. It can help identify any compression or irritation of the spinal cord or nerves that may be causing pain, numbness, weakness, or other neurological symptoms.
The procedure typically requires the patient to lie flat on their stomach or side while the radiologist inserts a thin needle into the subarachnoid space, usually at the lower lumbar level. Once the contrast dye is injected, the patient will be repositioned for various X-ray views or undergo a CT scan to capture detailed images of the spine. After the procedure, patients may experience headaches, nausea, or discomfort at the injection site, but these symptoms usually resolve within a few days.
Wallerian degeneration is a process that occurs following damage to the axons of neurons (nerve cells). After an axon is severed or traumatically injured, it undergoes a series of changes including fragmentation and removal of the distal segment of the axon, which is the part that is separated from the cell body. This process is named after Augustus Waller, who first described it in 1850.
The degenerative changes in the distal axon are characterized by the breakdown of the axonal cytoskeleton, the loss of myelin sheath (the fatty insulating material that surrounds and protects the axon), and the infiltration of macrophages to clear away the debris. These events lead to the degeneration of the distal axon segment, which is necessary for successful regeneration of the injured nerve.
Wallerian degeneration is a crucial process in the nervous system's response to injury, as it enables the regrowth of axons and the reestablishment of connections between neurons. However, if the regenerative capacity of the neuron is insufficient or the environment is not conducive to growth, functional recovery may be impaired, leading to long-term neurological deficits.
A hindlimb, also known as a posterior limb, is one of the pair of extremities that are located distally to the trunk in tetrapods (four-legged vertebrates) and include mammals, birds, reptiles, and amphibians. In humans and other primates, hindlimbs are equivalent to the lower limbs, which consist of the thigh, leg, foot, and toes.
The primary function of hindlimbs is locomotion, allowing animals to move from one place to another. However, they also play a role in other activities such as balance, support, and communication. In humans, the hindlimbs are responsible for weight-bearing, standing, walking, running, and jumping.
In medical terminology, the term "hindlimb" is not commonly used to describe human anatomy. Instead, healthcare professionals use terms like lower limbs or lower extremities to refer to the same region of the body. However, in comparative anatomy and veterinary medicine, the term hindlimb is still widely used to describe the corresponding structures in non-human animals.
Cranial nerves are a set of twelve pairs of nerves that originate from the brainstem and skull, rather than the spinal cord. These nerves are responsible for transmitting sensory information (such as sight, smell, hearing, and taste) to the brain, as well as controlling various muscles in the head and neck (including those involved in chewing, swallowing, and eye movement). Each cranial nerve has a specific function and is named accordingly. For example, the optic nerve (cranial nerve II) transmits visual information from the eyes to the brain, while the vagus nerve (cranial nerve X) controls parasympathetic functions in the body such as heart rate and digestion.
Spinal injuries refer to damages or traumas that occur to the vertebral column, which houses and protects the spinal cord. These injuries can be caused by various factors such as trauma from accidents (motor vehicle, sports-related, falls, etc.), violence, or degenerative conditions like arthritis, disc herniation, or spinal stenosis.
Spinal injuries can result in bruising, fractures, dislocations, or compression of the vertebrae, which may then cause damage to the spinal cord and its surrounding tissues, nerves, and blood vessels. The severity of a spinal injury can range from mild, with temporary symptoms, to severe, resulting in permanent impairment or paralysis below the level of injury.
Symptoms of spinal injuries may include:
- Pain or stiffness in the neck or back
- Numbness, tingling, or weakness in the limbs
- Loss of bladder or bowel control
- Difficulty walking or maintaining balance
- Paralysis or loss of sensation below the level of injury
- In severe cases, respiratory problems and difficulty in breathing
Immediate medical attention is crucial for spinal injuries to prevent further damage and ensure proper treatment. Treatment options may include immobilization, surgery, medication, rehabilitation, and physical therapy.
Spinal muscular atrophy (SMA) is a genetic disorder that affects the motor neurons in the spinal cord, leading to muscle weakness and atrophy. It is caused by a mutation in the survival motor neuron 1 (SMN1) gene, which results in a deficiency of SMN protein necessary for the survival of motor neurons.
There are several types of SMA, classified based on the age of onset and severity of symptoms. The most common type is type 1, also known as Werdnig-Hoffmann disease, which presents in infancy and is characterized by severe muscle weakness, hypotonia, and feeding difficulties. Other types include type 2 (intermediate SMA), type 3 (Kugelberg-Welander disease), and type 4 (adult-onset SMA).
The symptoms of SMA may include muscle wasting, fasciculations, weakness, hypotonia, respiratory difficulties, and mobility impairment. The diagnosis of SMA typically involves genetic testing to confirm the presence of a mutation in the SMN1 gene. Treatment options for SMA may include medications, physical therapy, assistive devices, and respiratory support.
The Radial nerve is a major peripheral nerve in the human body that originates from the brachial plexus, which is a network of nerves formed by the union of the ventral rami (anterior divisions) of spinal nerves C5-T1. The radial nerve provides motor function to extensor muscles of the upper limb and sensation to parts of the skin on the back of the arm, forearm, and hand.
More specifically, the radial nerve supplies motor innervation to:
* Extensor muscles of the shoulder (e.g., teres minor, infraspinatus)
* Rotator cuff muscles
* Elbow joint stabilizers (e.g., lateral head of the triceps)
* Extensors of the wrist, fingers, and thumb
The radial nerve also provides sensory innervation to:
* Posterior aspect of the upper arm (from the lower third of the humerus to the elbow)
* Lateral forearm (from the lateral epicondyle of the humerus to the wrist)
* Dorsum of the hand (skin over the radial side of the dorsum, including the first web space)
Damage or injury to the radial nerve may result in various symptoms, such as weakness or paralysis of the extensor muscles, numbness or tingling sensations in the affected areas, and difficulty with extension movements of the wrist, fingers, and thumb. Common causes of radial nerve injuries include fractures of the humerus bone, compression during sleep or prolonged pressure on the nerve (e.g., from crutches), and entrapment syndromes like radial tunnel syndrome.
Denervation is a medical term that refers to the loss or removal of nerve supply to an organ or body part. This can occur as a result of surgical intervention, injury, or disease processes that damage the nerves leading to the affected area. The consequences of denervation depend on the specific organ or tissue involved, but generally, it can lead to changes in function, sensation, and muscle tone. For example, denervation of a skeletal muscle can cause weakness, atrophy, and altered reflexes. Similarly, denervation of an organ such as the heart can lead to abnormalities in heart rate and rhythm. In some cases, denervation may be intentional, such as during surgical procedures aimed at treating chronic pain or spasticity.
Afferent pathways, also known as sensory pathways, refer to the neural connections that transmit sensory information from the peripheral nervous system to the central nervous system (CNS), specifically to the brain and spinal cord. These pathways are responsible for carrying various types of sensory information, such as touch, temperature, pain, pressure, vibration, hearing, vision, and taste, to the CNS for processing and interpretation.
The afferent pathways begin with sensory receptors located throughout the body, which detect changes in the environment and convert them into electrical signals. These signals are then transmitted via afferent neurons, also known as sensory neurons, to the spinal cord or brainstem. Within the CNS, the information is further processed and integrated with other neural inputs before being relayed to higher cognitive centers for conscious awareness and response.
Understanding the anatomy and physiology of afferent pathways is essential for diagnosing and treating various neurological conditions that affect sensory function, such as neuropathies, spinal cord injuries, and brain disorders.
Nerve degeneration, also known as neurodegeneration, is the progressive loss of structure and function of neurons, which can lead to cognitive decline, motor impairment, and various other symptoms. This process occurs due to a variety of factors, including genetics, environmental influences, and aging. It is a key feature in several neurological disorders such as Alzheimer's disease, Parkinson's disease, Huntington's disease, and multiple sclerosis. The degeneration can affect any part of the nervous system, leading to different symptoms depending on the location and extent of the damage.
Nerve tissue, also known as neural tissue, is a type of specialized tissue that is responsible for the transmission of electrical signals and the processing of information in the body. It is a key component of the nervous system, which includes the brain, spinal cord, and peripheral nerves. Nerve tissue is composed of two main types of cells: neurons and glial cells.
Neurons are the primary functional units of nerve tissue. They are specialized cells that are capable of generating and transmitting electrical signals, known as action potentials. Neurons have a unique structure, with a cell body (also called the soma) that contains the nucleus and other organelles, and processes (dendrites and axons) that extend from the cell body and are used to receive and transmit signals.
Glial cells, also known as neuroglia or glia, are non-neuronal cells that provide support and protection for neurons. There are several different types of glial cells, including astrocytes, oligodendrocytes, microglia, and Schwann cells. These cells play a variety of roles in the nervous system, such as providing structural support, maintaining the proper environment for neurons, and helping to repair and regenerate nerve tissue after injury.
Nerve tissue is found throughout the body, but it is most highly concentrated in the brain and spinal cord, which make up the central nervous system (CNS). The peripheral nerves, which are the nerves that extend from the CNS to the rest of the body, also contain nerve tissue. Nerve tissue is responsible for transmitting sensory information from the body to the brain, controlling muscle movements, and regulating various bodily functions such as heart rate, digestion, and respiration.
The Peripheral Nervous System (PNS) is that part of the nervous system which lies outside of the brain and spinal cord. It includes all the nerves and ganglia ( clusters of neurons) outside of the central nervous system (CNS). The PNS is divided into two components: the somatic nervous system and the autonomic nervous system.
The somatic nervous system is responsible for transmitting sensory information from the skin, muscles, and joints to the CNS, and for controlling voluntary movements of the skeletal muscles.
The autonomic nervous system, on the other hand, controls involuntary actions, such as heart rate, digestion, respiratory rate, salivation, perspiration, pupillary dilation, and sexual arousal. It is further divided into the sympathetic and parasympathetic systems, which generally have opposing effects and maintain homeostasis in the body.
Damage to the peripheral nervous system can result in various medical conditions such as neuropathies, neuritis, plexopathies, and radiculopathies, leading to symptoms like numbness, tingling, pain, weakness, or loss of reflexes in the affected area.
The brachial plexus is a network of nerves that originates from the spinal cord in the neck region and supplies motor and sensory innervation to the upper limb. It is formed by the ventral rami (branches) of the lower four cervical nerves (C5-C8) and the first thoracic nerve (T1). In some cases, contributions from C4 and T2 may also be included.
The brachial plexus nerves exit the intervertebral foramen, pass through the neck, and travel down the upper chest before branching out to form major peripheral nerves of the upper limb. These include the axillary, radial, musculocutaneous, median, and ulnar nerves, which further innervate specific muscles and sensory areas in the arm, forearm, and hand.
Damage to the brachial plexus can result in various neurological deficits, such as weakness or paralysis of the upper limb, numbness, or loss of sensation in the affected area, depending on the severity and location of the injury.
Loperamide is an antidiarrheal medication that works by slowing down the movement of the intestines. This helps to increase the time between bowel movements and reduces the amount of liquid in stools, thereby helping to relieve diarrhea. It is available over-the-counter (OTC) and by prescription, depending on the strength and formulation.
Loperamide works by binding to opioid receptors in the gut, which helps to reduce the contractions of the intestines that can lead to diarrhea. It is important to note that loperamide should not be used for longer than 2 days without consulting a healthcare professional, as prolonged use can lead to serious side effects such as constipation, dizziness, and decreased alertness.
Loperamide is also known by its brand names, including Imodium, Pepto-Bismol Maximum Strength, and Kaopectate II. It is important to follow the instructions on the label carefully when taking loperamide, and to speak with a healthcare provider if you have any questions or concerns about using this medication.
Spinal cord ischemia refers to a reduction or interruption of blood flow to the spinal cord, leading to insufficient oxygen and nutrient supply. This condition can cause damage to the spinal cord tissue, potentially resulting in neurological deficits, such as muscle weakness, sensory loss, or autonomic dysfunction. Spinal cord ischemia may be caused by various factors, including atherosclerosis, embolism, spinal artery stenosis, or complications during surgery. The severity and extent of the neurological impairment depend on the duration and location of the ischemic event in the spinal cord.
An action potential is a brief electrical signal that travels along the membrane of a nerve cell (neuron) or muscle cell. It is initiated by a rapid, localized change in the permeability of the cell membrane to specific ions, such as sodium and potassium, resulting in a rapid influx of sodium ions and a subsequent efflux of potassium ions. This ion movement causes a brief reversal of the electrical potential across the membrane, which is known as depolarization. The action potential then propagates along the cell membrane as a wave, allowing the electrical signal to be transmitted over long distances within the body. Action potentials play a crucial role in the communication and functioning of the nervous system and muscle tissue.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
The ophthalmic nerve, also known as the first cranial nerve or CN I, is a sensory nerve that primarily transmits information about vision, including light intensity and color, and sensation in the eye and surrounding areas. It is responsible for the sensory innervation of the upper eyelid, conjunctiva, cornea, iris, ciliary body, and nasal cavity. The ophthalmic nerve has three major branches: the lacrimal nerve, frontal nerve, and nasociliary nerve. Damage to this nerve can result in various visual disturbances and loss of sensation in the affected areas.
Gamma-Aminobutyric Acid (GABA) is a major inhibitory neurotransmitter in the mammalian central nervous system. It plays a crucial role in regulating neuronal excitability and preventing excessive neuronal firing, which helps to maintain neural homeostasis and reduce the risk of seizures. GABA functions by binding to specific receptors (GABA-A, GABA-B, and GABA-C) on the postsynaptic membrane, leading to hyperpolarization of the neuronal membrane and reduced neurotransmitter release from presynaptic terminals.
In addition to its role in the central nervous system, GABA has also been identified as a neurotransmitter in the peripheral nervous system, where it is involved in regulating various physiological processes such as muscle relaxation, hormone secretion, and immune function.
GABA can be synthesized in neurons from glutamate, an excitatory neurotransmitter, through the action of the enzyme glutamic acid decarboxylase (GAD). Once synthesized, GABA is stored in synaptic vesicles and released into the synapse upon neuronal activation. After release, GABA can be taken up by surrounding glial cells or degraded by the enzyme GABA transaminase (GABA-T) into succinic semialdehyde, which is further metabolized to form succinate and enter the Krebs cycle for energy production.
Dysregulation of GABAergic neurotransmission has been implicated in various neurological and psychiatric disorders, including epilepsy, anxiety, depression, and sleep disturbances. Therefore, modulating GABAergic signaling through pharmacological interventions or other therapeutic approaches may offer potential benefits for the treatment of these conditions.
The mandibular nerve is a branch of the trigeminal nerve (the fifth cranial nerve), which is responsible for sensations in the face and motor functions such as biting and chewing. The mandibular nerve provides both sensory and motor innervation to the lower third of the face, below the eye and nose down to the chin.
More specifically, it carries sensory information from the lower teeth, lower lip, and parts of the oral cavity, as well as the skin over the jaw and chin. It also provides motor innervation to the muscles of mastication (chewing), which include the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles.
Damage to the mandibular nerve can result in numbness or loss of sensation in the lower face and mouth, as well as weakness or difficulty with chewing and biting.
The medulla oblongata is a part of the brainstem that is located in the posterior portion of the brainstem and continues with the spinal cord. It plays a vital role in controlling several critical bodily functions, such as breathing, heart rate, and blood pressure. The medulla oblongata also contains nerve pathways that transmit sensory information from the body to the brain and motor commands from the brain to the muscles. Additionally, it is responsible for reflexes such as vomiting, swallowing, coughing, and sneezing.
Local anesthetics are a type of medication that is used to block the sensation of pain in a specific area of the body. They work by temporarily numbing the nerves in that area, preventing them from transmitting pain signals to the brain. Local anesthetics can be administered through various routes, including topical application (such as creams or gels), injection (such as into the skin or tissues), or regional nerve blocks (such as epidural or spinal anesthesia).
Some common examples of local anesthetics include lidocaine, prilocaine, bupivacaine, and ropivacaine. These medications can be used for a variety of medical procedures, ranging from minor surgeries (such as dental work or skin biopsies) to more major surgeries (such as joint replacements or hernia repairs).
Local anesthetics are generally considered safe when used appropriately, but they can have side effects and potential complications. These may include allergic reactions, toxicity (if too much is administered), and nerve damage (if the medication is injected into a nerve). It's important to follow your healthcare provider's instructions carefully when using local anesthetics, and to report any unusual symptoms or side effects promptly.
A dose-response relationship in the context of drugs refers to the changes in the effects or symptoms that occur as the dose of a drug is increased or decreased. Generally, as the dose of a drug is increased, the severity or intensity of its effects also increases. Conversely, as the dose is decreased, the effects of the drug become less severe or may disappear altogether.
The dose-response relationship is an important concept in pharmacology and toxicology because it helps to establish the safe and effective dosage range for a drug. By understanding how changes in the dose of a drug affect its therapeutic and adverse effects, healthcare providers can optimize treatment plans for their patients while minimizing the risk of harm.
The dose-response relationship is typically depicted as a curve that shows the relationship between the dose of a drug and its effect. The shape of the curve may vary depending on the drug and the specific effect being measured. Some drugs may have a steep dose-response curve, meaning that small changes in the dose can result in large differences in the effect. Other drugs may have a more gradual dose-response curve, where larger changes in the dose are needed to produce significant effects.
In addition to helping establish safe and effective dosages, the dose-response relationship is also used to evaluate the potential therapeutic benefits and risks of new drugs during clinical trials. By systematically testing different doses of a drug in controlled studies, researchers can identify the optimal dosage range for the drug and assess its safety and efficacy.
The cervical plexus is a network of nerves that arises from the ventral rami (anterior divisions) of the first four cervical spinal nerves (C1-C4) and a portion of C5. These nerves form a series of loops and anastomoses (connections) that give rise to several major and minor branches.
The main functions of the cervical plexus include providing sensory innervation to the skin on the neck, shoulder, and back of the head, as well as supplying motor innervation to some of the muscles in the neck and shoulders, such as the sternocleidomastoid and trapezius.
Some of the major branches of the cervical plexus include:
* The lesser occipital nerve (C2), which provides sensory innervation to the skin over the back of the head and neck.
* The great auricular nerve (C2-C3), which provides sensory innervation to the skin over the ear and lower part of the face.
* The transverse cervical nerve (C2-C3), which provides sensory innervation to the skin over the anterior and lateral neck.
* The supraclavicular nerves (C3-C4), which provide sensory innervation to the skin over the shoulder and upper chest.
* The phrenic nerve (C3-C5), which supplies motor innervation to the diaphragm, the major muscle of respiration.
Overall, the cervical plexus plays a crucial role in providing sensory and motor innervation to the neck, head, and shoulders, allowing for normal movement and sensation in these areas.
"Wistar rats" are a strain of albino rats that are widely used in laboratory research. They were developed at the Wistar Institute in Philadelphia, USA, and were first introduced in 1906. Wistar rats are outbred, which means that they are genetically diverse and do not have a fixed set of genetic characteristics like inbred strains.
Wistar rats are commonly used as animal models in biomedical research because of their size, ease of handling, and relatively low cost. They are used in a wide range of research areas, including toxicology, pharmacology, nutrition, cancer, cardiovascular disease, and behavioral studies. Wistar rats are also used in safety testing of drugs, medical devices, and other products.
Wistar rats are typically larger than many other rat strains, with males weighing between 500-700 grams and females weighing between 250-350 grams. They have a lifespan of approximately 2-3 years. Wistar rats are also known for their docile and friendly nature, making them easy to handle and work with in the laboratory setting.
Clonidine is an medication that belongs to a class of drugs called centrally acting alpha-agonist hypotensives. It works by stimulating certain receptors in the brain and lowering the heart rate, which results in decreased blood pressure. Clonidine is commonly used to treat hypertension (high blood pressure), but it can also be used for other purposes such as managing withdrawal symptoms from opioids or alcohol, treating attention deficit hyperactivity disorder (ADHD), and preventing migraines. It can be taken orally in the form of tablets or transdermally through a patch applied to the skin. As with any medication, clonidine should be used under the guidance and supervision of a healthcare provider.
In medical terms, dissection refers to the separation of the layers of a biological tissue or structure by cutting or splitting. It is often used to describe the process of surgically cutting through tissues, such as during an operation to separate organs or examine their internal structures.
However, "dissection" can also refer to a pathological condition in which there is a separation of the layers of a blood vessel wall by blood, creating a false lumen or aneurysm. This type of dissection is most commonly seen in the aorta and can be life-threatening if not promptly diagnosed and treated.
In summary, "dissection" has both surgical and pathological meanings related to the separation of tissue layers, and it's essential to consider the context in which the term is used.
A neurilemmoma, also known as schwannoma or peripheral nerve sheath tumor, is a benign, slow-growing tumor that arises from the Schwann cells, which produce the myelin sheath that surrounds and insulates peripheral nerves. These tumors can occur anywhere along the course of a peripheral nerve, but they most commonly affect the acoustic nerve (vestibulocochlear nerve), leading to a type of tumor called vestibular schwannoma or acoustic neuroma. Neurilemmomas are typically encapsulated and do not invade the surrounding tissue, although larger ones may cause pressure-related symptoms due to compression of nearby structures. Rarely, these tumors can undergo malignant transformation, leading to a condition called malignant peripheral nerve sheath tumor or neurofibrosarcoma.
The splanchnic nerves are a set of nerve fibers that originate from the thoracic and lumbar regions of the spinal cord and innervate various internal organs. They are responsible for carrying both sensory information, such as pain and temperature, from the organs to the brain, and motor signals, which control the function of the organs, from the brain to the organs.
There are several splanchnic nerves, including the greater, lesser, and least splanchnic nerves, as well as the lumbar splanchnic nerves. These nerves primarily innervate the autonomic nervous system, which controls the involuntary functions of the body, such as heart rate, digestion, and respiration.
The greater splanchnic nerve arises from the fifth to the ninth thoracic ganglia and passes through the diaphragm to reach the abdomen. It innervates the stomach, esophagus, liver, pancreas, and adrenal glands.
The lesser splanchnic nerve arises from the tenth and eleventh thoracic ganglia and innervates the upper part of the small intestine, the pancreas, and the adrenal glands.
The least splanchnic nerve arises from the twelfth thoracic ganglion and innervates the lower part of the small intestine and the colon.
The lumbar splanchnic nerves arise from the first three or four lumbar ganglia and innervate the lower parts of the colon, the rectum, and the reproductive organs.
Paraplegia is a medical condition characterized by partial or complete loss of motor function and sensation in the lower extremities, typically affecting both legs. This results from damage to the spinal cord, often due to trauma such as accidents, falls, or gunshot wounds, or from diseases like spina bifida, polio, or tumors. The specific area and extent of the injury on the spinal cord determine the severity and location of paralysis. Individuals with paraplegia may require assistive devices for mobility, such as wheelchairs, and may face various health challenges, including pressure sores, urinary tract infections, and chronic pain.
Lidocaine is a type of local anesthetic that numbs painful areas and is used to prevent pain during certain medical procedures. It works by blocking the nerves that transmit pain signals to the brain. In addition to its use as an anesthetic, lidocaine can also be used to treat irregular heart rates and relieve itching caused by allergic reactions or skin conditions such as eczema.
Lidocaine is available in various forms, including creams, gels, ointments, sprays, solutions, and injectable preparations. It can be applied directly to the skin or mucous membranes, or it can be administered by injection into a muscle or vein. The specific dosage and method of administration will depend on the reason for its use and the individual patient's medical history and current health status.
Like all medications, lidocaine can have side effects, including allergic reactions, numbness that lasts too long, and in rare cases, heart problems or seizures. It is important to follow the instructions of a healthcare provider carefully when using lidocaine to minimize the risk of adverse effects.
Thoracic nerves are the 12 paired nerves that originate from the thoracic segment (T1-T12) of the spinal cord. These nerves provide motor and sensory innervation to the trunk and abdomen, specifically to the muscles of the chest wall, the skin over the back and chest, and some parts of the abdomen. They also contribute to the formation of the sympathetic trunk, which is a part of the autonomic nervous system that regulates unconscious bodily functions such as heart rate and digestion. Each thoracic nerve emerges from the intervertebral foramen, a small opening between each vertebra, and splits into anterior and posterior branches to innervate the corresponding dermatomes and myotomes.
Morphine is a potent opioid analgesic (pain reliever) derived from the opium poppy. It works by binding to opioid receptors in the brain and spinal cord, blocking the transmission of pain signals and reducing the perception of pain. Morphine is used to treat moderate to severe pain, including pain associated with cancer, myocardial infarction, and other conditions. It can also be used as a sedative and cough suppressant.
Morphine has a high potential for abuse and dependence, and its use should be closely monitored by healthcare professionals. Common side effects of morphine include drowsiness, respiratory depression, constipation, nausea, and vomiting. Overdose can result in respiratory failure, coma, and death.
The cochlear nerve, also known as the auditory nerve, is the sensory nerve that transmits sound signals from the inner ear to the brain. It consists of two parts: the outer spiral ganglion and the inner vestibular portion. The spiral ganglion contains the cell bodies of the bipolar neurons that receive input from hair cells in the cochlea, which is the snail-shaped organ in the inner ear responsible for hearing. These neurons then send their axons to form the cochlear nerve, which travels through the internal auditory meatus and synapses with neurons in the cochlear nuclei located in the brainstem.
Damage to the cochlear nerve can result in hearing loss or deafness, depending on the severity of the injury. Common causes of cochlear nerve damage include acoustic trauma, such as exposure to loud noises, viral infections, meningitis, and tumors affecting the nerve or surrounding structures. In some cases, cochlear nerve damage may be treated with hearing aids, cochlear implants, or other assistive devices to help restore or improve hearing function.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Xanthines are a type of natural alkaloids that are found in various plants, including tea leaves, cocoa beans, and mate. The most common xanthines are caffeine, theophylline, and theobromine. These compounds have stimulant effects on the central nervous system and are often used in medication to treat conditions such as asthma, bronchitis, and other respiratory issues.
Caffeine is the most widely consumed xanthine and is found in a variety of beverages like coffee, tea, and energy drinks. It works by blocking adenosine receptors in the brain, which can lead to increased alertness and reduced feelings of fatigue.
Theophylline is another xanthine that is used as a bronchodilator to treat asthma and other respiratory conditions. It works by relaxing smooth muscles in the airways, making it easier to breathe.
Theobromine is found in cocoa beans and is responsible for the stimulant effects of chocolate. While it has similar properties to caffeine and theophylline, it is less potent and has a milder effect on the body.
It's worth noting that while xanthines can have beneficial effects when used in moderation, they can also cause negative side effects such as insomnia, nervousness, and rapid heart rate if consumed in large quantities or over an extended period of time.
Tuberculosis (TB) of the spine, also known as Pott's disease, is a specific form of extrapulmonary tuberculosis that involves the vertebral column. It is caused by the Mycobacterium tuberculosis bacterium, which primarily affects the lungs but can spread through the bloodstream to other parts of the body, including the spine.
In Pott's disease, the infection leads to the destruction of the spongy bone (vertebral body) and the intervertebral disc space, resulting in vertebral collapse, kyphosis (hunchback deformity), and potential neurological complications due to spinal cord compression. Common symptoms include back pain, stiffness, fever, night sweats, and weight loss. Early diagnosis and treatment with a multidrug antibiotic regimen are crucial to prevent long-term disability and further spread of the infection.
Capsaicin is defined in medical terms as the active component of chili peppers (genus Capsicum) that produces a burning sensation when it comes into contact with mucous membranes or skin. It is a potent irritant and is used topically as a counterirritant in some creams and patches to relieve pain. Capsaicin works by depleting substance P, a neurotransmitter that relays pain signals to the brain, from nerve endings.
Here is the medical definition of capsaicin from the Merriam-Webster's Medical Dictionary:
caпсаісіn : an alkaloid (C18H27NO3) that is the active principle of red peppers and is used in topical preparations as a counterirritant and analgesic.
Ligaments are bands of dense, fibrous connective tissue that surround joints and provide support, stability, and limits the range of motion. They are made up primarily of collagen fibers arranged in a parallel pattern to withstand tension and stress. Ligaments attach bone to bone, and their function is to prevent excessive movement that could cause injury or dislocation.
There are two main types of ligaments: extracapsular and intracapsular. Extracapsular ligaments are located outside the joint capsule and provide stability to the joint by limiting its range of motion. Intracapsular ligaments, on the other hand, are found inside the joint capsule and help maintain the alignment of the joint surfaces.
Examples of common ligaments in the body include the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) in the knee, the medial collateral ligament (MCL) and lateral collateral ligament (LCL) in the elbow, and the coracoacromial ligament in the shoulder.
Injuries to ligaments can occur due to sudden trauma or overuse, leading to sprains, strains, or tears. These injuries can cause pain, swelling, bruising, and limited mobility, and may require medical treatment such as immobilization, physical therapy, or surgery.
A laminectomy is a surgical procedure that involves the removal of the lamina, which is the back part of the vertebra that covers the spinal canal. This procedure is often performed to relieve pressure on the spinal cord or nerves caused by conditions such as herniated discs, spinal stenosis, or tumors. By removing the lamina, the surgeon can access the affected area and alleviate the compression on the spinal cord or nerves, thereby reducing pain, numbness, or weakness in the back, legs, or arms.
Laminectomy may be performed as a standalone procedure or in combination with other surgical techniques such as discectomy, foraminotomy, or spinal fusion. The specific approach and extent of the surgery will depend on the patient's individual condition and symptoms.
Low back pain is a common musculoskeletal disorder characterized by discomfort or pain in the lower part of the back, typically between the costal margin (bottom of the ribcage) and the gluteal folds (buttocks). It can be caused by several factors including strain or sprain of the muscles or ligaments, disc herniation, spinal stenosis, osteoarthritis, or other degenerative conditions affecting the spine. The pain can range from a dull ache to a sharp stabbing sensation and may be accompanied by stiffness, limited mobility, and radiating pain down the legs in some cases. Low back pain is often described as acute (lasting less than 6 weeks), subacute (lasting between 6-12 weeks), or chronic (lasting more than 12 weeks).
The glossopharyngeal nerve, also known as the ninth cranial nerve (IX), is a mixed nerve that carries both sensory and motor fibers. It originates from the medulla oblongata in the brainstem and has several functions:
1. Sensory function: The glossopharyngeal nerve provides general sensation to the posterior third of the tongue, the tonsils, the back of the throat (pharynx), and the middle ear. It also carries taste sensations from the back one-third of the tongue.
2. Special visceral afferent function: The nerve transmits information about the stretch of the carotid artery and blood pressure to the brainstem.
3. Motor function: The glossopharyngeal nerve innervates the stylopharyngeus muscle, which helps elevate the pharynx during swallowing. It also provides parasympathetic fibers to the parotid gland, stimulating saliva production.
4. Visceral afferent function: The glossopharyngeal nerve carries information about the condition of the internal organs in the thorax and abdomen to the brainstem.
Overall, the glossopharyngeal nerve plays a crucial role in swallowing, taste, saliva production, and monitoring blood pressure and heart rate.
A cadaver is a deceased body that is used for medical research or education. In the field of medicine, cadavers are often used in anatomy lessons, surgical training, and other forms of medical research. The use of cadavers allows medical professionals to gain a deeper understanding of the human body and its various systems without causing harm to living subjects. Cadavers may be donated to medical schools or obtained through other means, such as through consent of the deceased or their next of kin. It is important to handle and treat cadavers with respect and dignity, as they were once living individuals who deserve to be treated with care even in death.
Intervertebral disc displacement, also known as a slipped disc or herniated disc, is a medical condition where the inner, softer material (nucleus pulposus) of the intervertebral disc bulges or ruptures through its outer, tougher ring (annulus fibrosus). This can put pressure on nearby nerves and cause pain, numbness, tingling, or weakness in the affected area, often in the lower back or neck. The displacement may also lead to inflammation and irritation of the surrounding spinal structures, further exacerbating the symptoms. The condition is typically caused by age-related wear and tear (degenerative disc disease) or sudden trauma.
Neurons, also known as nerve cells or neurocytes, are specialized cells that constitute the basic unit of the nervous system. They are responsible for receiving, processing, and transmitting information and signals within the body. Neurons have three main parts: the dendrites, the cell body (soma), and the axon. The dendrites receive signals from other neurons or sensory receptors, while the axon transmits these signals to other neurons, muscles, or glands. The junction between two neurons is called a synapse, where neurotransmitters are released to transmit the signal across the gap (synaptic cleft) to the next neuron. Neurons vary in size, shape, and structure depending on their function and location within the nervous system.
Electroacupuncture is a form of acupuncture where a small electric current is passed between pairs of acupuncture needles. This technique is used to stimulate the acupoints more strongly and consistently than with manual acupuncture. The intensity of the electrical impulses can be adjusted depending on the patient's comfort level and the desired therapeutic effect. Electroacupuncture is often used to treat conditions such as chronic pain, muscle spasms, and paralysis. It may also be used in the treatment of addiction, weight loss, and stroke rehabilitation.
An intervertebral disc is a fibrocartilaginous structure found between the vertebrae of the spinal column in humans and other animals. It functions as a shock absorber, distributes mechanical stress during weight-bearing activities, and allows for varying degrees of mobility between adjacent vertebrae.
The disc is composed of two parts: the annulus fibrosus, which forms the tough, outer layer; and the nucleus pulposus, which is a gel-like substance in the center that contains proteoglycans and water. The combination of these components provides the disc with its unique ability to distribute forces and allow for movement.
The intervertebral discs are essential for the normal functioning of the spine, providing stability, flexibility, and protection to the spinal cord and nerves. However, they can also be subject to degeneration and injury, which may result in conditions such as herniated discs or degenerative disc disease.
Microglia are a type of specialized immune cell found in the brain and spinal cord. They are part of the glial family, which provide support and protection to the neurons in the central nervous system (CNS). Microglia account for about 10-15% of all cells found in the CNS.
The primary role of microglia is to constantly survey their environment and eliminate any potentially harmful agents, such as pathogens, dead cells, or protein aggregates. They do this through a process called phagocytosis, where they engulf and digest foreign particles or cellular debris. In addition to their phagocytic function, microglia also release various cytokines, chemokines, and growth factors that help regulate the immune response in the CNS, promote neuronal survival, and contribute to synaptic plasticity.
Microglia can exist in different activation states depending on the nature of the stimuli they encounter. In a resting state, microglia have a small cell body with numerous branches that are constantly monitoring their surroundings. When activated by an injury, infection, or neurodegenerative process, microglia change their morphology and phenotype, retracting their processes and adopting an amoeboid shape to migrate towards the site of damage or inflammation. Based on the type of activation, microglia can release both pro-inflammatory and anti-inflammatory factors that contribute to either neuroprotection or neurotoxicity.
Dysregulation of microglial function has been implicated in several neurological disorders, including Alzheimer's disease, Parkinson's disease, multiple sclerosis, and Amyotrophic Lateral Sclerosis (ALS). Therefore, understanding the role of microglia in health and disease is crucial for developing novel therapeutic strategies to treat these conditions.
Optic nerve injuries refer to damages or trauma inflicted on the optic nerve, which is a crucial component of the visual system. The optic nerve transmits visual information from the retina to the brain, enabling us to see. Injuries to the optic nerve can result in various visual impairments, including partial or complete vision loss, decreased visual acuity, changes in color perception, and reduced field of view.
These injuries may occur due to several reasons, such as:
1. Direct trauma to the eye or head
2. Increased pressure inside the eye (glaucoma)
3. Optic neuritis, an inflammation of the optic nerve
4. Ischemia, or insufficient blood supply to the optic nerve
5. Compression from tumors or other space-occupying lesions
6. Intrinsic degenerative conditions affecting the optic nerve
7. Toxic exposure to certain chemicals or medications
Optic nerve injuries are diagnosed through a comprehensive eye examination, including visual acuity testing, slit-lamp examination, dilated fundus exam, and additional diagnostic tests like optical coherence tomography (OCT) and visual field testing. Treatment options vary depending on the cause and severity of the injury but may include medications, surgery, or vision rehabilitation.
Electrophysiology is a branch of medicine that deals with the electrical activities of the body, particularly the heart. In a medical context, electrophysiology studies (EPS) are performed to assess abnormal heart rhythms (arrhythmias) and to evaluate the effectiveness of certain treatments, such as medication or pacemakers.
During an EPS, electrode catheters are inserted into the heart through blood vessels in the groin or neck. These catheters can record the electrical activity of the heart and stimulate it to help identify the source of the arrhythmia. The information gathered during the study can help doctors determine the best course of treatment for each patient.
In addition to cardiac electrophysiology, there are also other subspecialties within electrophysiology, such as neuromuscular electrophysiology, which deals with the electrical activity of the nervous system and muscles.
The nervous system is a complex, highly organized network of specialized cells called neurons and glial cells that communicate with each other via electrical and chemical signals to coordinate various functions and activities in the body. It consists of two main parts: the central nervous system (CNS), including the brain and spinal cord, and the peripheral nervous system (PNS), which includes all the nerves and ganglia outside the CNS.
The primary function of the nervous system is to receive, process, and integrate information from both internal and external environments and then respond by generating appropriate motor outputs or behaviors. This involves sensing various stimuli through specialized receptors, transmitting this information through afferent neurons to the CNS for processing, integrating this information with other inputs and memories, making decisions based on this processed information, and finally executing responses through efferent neurons that control effector organs such as muscles and glands.
The nervous system can be further divided into subsystems based on their functions, including the somatic nervous system, which controls voluntary movements and reflexes; the autonomic nervous system, which regulates involuntary physiological processes like heart rate, digestion, and respiration; and the enteric nervous system, which is a specialized subset of the autonomic nervous system that controls gut functions. Overall, the nervous system plays a critical role in maintaining homeostasis, regulating behavior, and enabling cognition and consciousness.
Analgesics, opioid are a class of drugs used for the treatment of pain. They work by binding to specific receptors in the brain and spinal cord, blocking the transmission of pain signals to the brain. Opioids can be synthetic or natural, and include drugs such as morphine, codeine, oxycodone, hydrocodone, hydromorphone, fentanyl, and methadone. They are often used for moderate to severe pain, such as that resulting from injury, surgery, or chronic conditions like cancer. However, opioids can also produce euphoria, physical dependence, and addiction, so they are tightly regulated and carry a risk of misuse.
Spinal curvatures refer to the normal or abnormal curvature patterns of the spine as viewed from the side. The human spine has four distinct curves that form an "S" shape when viewed from the side: cervical, thoracic, lumbar, and sacral. These natural curves provide strength, flexibility, and balance to the spine, allowing us to stand upright, maintain proper posture, and absorb shock during movement.
Abnormal spinal curvatures are often referred to as spinal deformities and can be classified into two main categories: hyperkyphosis (increased kyphosis) and hyperlordosis (increased lordosis). Examples of such conditions include:
1. Kyphosis: An excessive curvature in the thoracic or sacral regions, leading to a hunchback or rounded appearance. Mild kyphosis is common and usually not problematic, but severe cases can cause pain, breathing difficulties, and neurological issues.
2. Lordosis: An abnormal increase in the curvature of the lumbar or cervical spine, resulting in an exaggerated swayback posture. This can lead to lower back pain, muscle strain, and difficulty maintaining proper balance.
3. Scoliosis: A lateral (side-to-side) spinal curvature that causes the spine to twist and rotate, forming a C or S shape when viewed from behind. Most scoliosis cases are idiopathic (of unknown cause), but they can also be congenital (present at birth) or secondary to other medical conditions.
These abnormal spinal curvatures may require medical intervention, such as physical therapy, bracing, or surgery, depending on the severity and progression of the condition.
Optic nerve diseases refer to a group of conditions that affect the optic nerve, which transmits visual information from the eye to the brain. These diseases can cause various symptoms such as vision loss, decreased visual acuity, changes in color vision, and visual field defects. Examples of optic nerve diseases include optic neuritis (inflammation of the optic nerve), glaucoma (damage to the optic nerve due to high eye pressure), optic nerve damage from trauma or injury, ischemic optic neuropathy (lack of blood flow to the optic nerve), and optic nerve tumors. Treatment for optic nerve diseases varies depending on the specific condition and may include medications, surgery, or lifestyle changes.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
Astrocytes are a type of star-shaped glial cell found in the central nervous system (CNS), including the brain and spinal cord. They play crucial roles in supporting and maintaining the health and function of neurons, which are the primary cells responsible for transmitting information in the CNS.
Some of the essential functions of astrocytes include:
1. Supporting neuronal structure and function: Astrocytes provide structural support to neurons by ensheathing them and maintaining the integrity of the blood-brain barrier, which helps regulate the entry and exit of substances into the CNS.
2. Regulating neurotransmitter levels: Astrocytes help control the levels of neurotransmitters in the synaptic cleft (the space between two neurons) by taking up excess neurotransmitters and breaking them down, thus preventing excessive or prolonged activation of neuronal receptors.
3. Providing nutrients to neurons: Astrocytes help supply energy metabolites, such as lactate, to neurons, which are essential for their survival and function.
4. Modulating synaptic activity: Through the release of various signaling molecules, astrocytes can modulate synaptic strength and plasticity, contributing to learning and memory processes.
5. Participating in immune responses: Astrocytes can respond to CNS injuries or infections by releasing pro-inflammatory cytokines and chemokines, which help recruit immune cells to the site of injury or infection.
6. Promoting neuronal survival and repair: In response to injury or disease, astrocytes can become reactive and undergo morphological changes that aid in forming a glial scar, which helps contain damage and promote tissue repair. Additionally, they release growth factors and other molecules that support the survival and regeneration of injured neurons.
Dysfunction or damage to astrocytes has been implicated in several neurological disorders, including Alzheimer's disease, Parkinson's disease, amyotrophic lateral sclerosis (ALS), and multiple sclerosis (MS).
The sympathetic nervous system (SNS) is a part of the autonomic nervous system that operates largely below the level of consciousness, and it functions to produce appropriate physiological responses to perceived danger. It's often associated with the "fight or flight" response. The SNS uses nerve impulses to stimulate target organs, causing them to speed up (e.g., increased heart rate), prepare for action, or otherwise respond to stressful situations.
The sympathetic nervous system is activated due to stressful emotional or physical situations and it prepares the body for immediate actions. It dilates the pupils, increases heart rate and blood pressure, accelerates breathing, and slows down digestion. The primary neurotransmitter involved in this system is norepinephrine (also known as noradrenaline).
An epidural spinal hematoma is a rare but potentially serious medical condition characterized by the accumulation of blood in the epidural space of the spinal canal. The epidural space is the outermost layer of the spinal canal and it contains fat, blood vessels, and nerve roots.
In an epidural spinal hematoma, blood collects in this space, often as a result of trauma or injury to the spine, or due to complications from medical procedures such as spinal taps or epidural anesthesia. The buildup of blood can put pressure on the spinal cord and nerves, leading to symptoms such as back pain, muscle weakness, numbness, or paralysis below the level of the hematoma.
Epidural spinal hematomas require immediate medical attention and may necessitate surgical intervention to relieve the pressure on the spinal cord and prevent further nerve damage. Risk factors for developing an epidural spinal hematoma include bleeding disorders, anticoagulant medication use, and spinal trauma or surgery.
Neuroglia, also known as glial cells or simply glia, are non-neuronal cells that provide support and protection for neurons in the nervous system. They maintain homeostasis, form myelin sheaths around nerve fibers, and provide structural support. They also play a role in the immune response of the central nervous system. Some types of neuroglia include astrocytes, oligodendrocytes, microglia, and ependymal cells.
A chick embryo refers to the developing organism that arises from a fertilized chicken egg. It is often used as a model system in biological research, particularly during the stages of development when many of its organs and systems are forming and can be easily observed and manipulated. The study of chick embryos has contributed significantly to our understanding of various aspects of developmental biology, including gastrulation, neurulation, organogenesis, and pattern formation. Researchers may use various techniques to observe and manipulate the chick embryo, such as surgical alterations, cell labeling, and exposure to drugs or other agents.
Analgesia is defined as the absence or relief of pain in a patient, achieved through various medical means. It is derived from the Greek word "an-" meaning without and "algein" meaning to feel pain. Analgesics are medications that are used to reduce pain without causing loss of consciousness, and they work by blocking the transmission of pain signals to the brain.
Examples of analgesics include over-the-counter medications such as acetaminophen (Tylenol) and nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve). Prescription opioid painkillers, such as oxycodone (OxyContin, Percocet) and hydrocodone (Vicodin), are also used for pain relief but carry a higher risk of addiction and abuse.
Analgesia can also be achieved through non-pharmacological means, such as through nerve blocks, spinal cord stimulation, acupuncture, and other complementary therapies. The choice of analgesic therapy depends on the type and severity of pain, as well as the patient's medical history and individual needs.
Nerve tissue proteins are specialized proteins found in the nervous system that provide structural and functional support to nerve cells, also known as neurons. These proteins include:
1. Neurofilaments: These are type IV intermediate filaments that provide structural support to neurons and help maintain their shape and size. They are composed of three subunits - NFL (light), NFM (medium), and NFH (heavy).
2. Neuronal Cytoskeletal Proteins: These include tubulins, actins, and spectrins that provide structural support to the neuronal cytoskeleton and help maintain its integrity.
3. Neurotransmitter Receptors: These are specialized proteins located on the postsynaptic membrane of neurons that bind neurotransmitters released by presynaptic neurons, triggering a response in the target cell.
4. Ion Channels: These are transmembrane proteins that regulate the flow of ions across the neuronal membrane and play a crucial role in generating and transmitting electrical signals in neurons.
5. Signaling Proteins: These include enzymes, receptors, and adaptor proteins that mediate intracellular signaling pathways involved in neuronal development, differentiation, survival, and death.
6. Adhesion Proteins: These are cell surface proteins that mediate cell-cell and cell-matrix interactions, playing a crucial role in the formation and maintenance of neural circuits.
7. Extracellular Matrix Proteins: These include proteoglycans, laminins, and collagens that provide structural support to nerve tissue and regulate neuronal migration, differentiation, and survival.
In a medical context, "hot temperature" is not a standard medical term with a specific definition. However, it is often used in relation to fever, which is a common symptom of illness. A fever is typically defined as a body temperature that is higher than normal, usually above 38°C (100.4°F) for adults and above 37.5-38°C (99.5-101.3°F) for children, depending on the source.
Therefore, when a medical professional talks about "hot temperature," they may be referring to a body temperature that is higher than normal due to fever or other causes. It's important to note that a high environmental temperature can also contribute to an elevated body temperature, so it's essential to consider both the body temperature and the environmental temperature when assessing a patient's condition.
"Cat" is a common name that refers to various species of small carnivorous mammals that belong to the family Felidae. The domestic cat, also known as Felis catus or Felis silvestris catus, is a popular pet and companion animal. It is a subspecies of the wildcat, which is found in Europe, Africa, and Asia.
Domestic cats are often kept as pets because of their companionship, playful behavior, and ability to hunt vermin. They are also valued for their ability to provide emotional support and therapy to people. Cats are obligate carnivores, which means that they require a diet that consists mainly of meat to meet their nutritional needs.
Cats are known for their agility, sharp senses, and predatory instincts. They have retractable claws, which they use for hunting and self-defense. Cats also have a keen sense of smell, hearing, and vision, which allow them to detect prey and navigate their environment.
In medical terms, cats can be hosts to various parasites and diseases that can affect humans and other animals. Some common feline diseases include rabies, feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), and toxoplasmosis. It is important for cat owners to keep their pets healthy and up-to-date on vaccinations and preventative treatments to protect both the cats and their human companions.
The accessory nerve, also known as the eleventh cranial nerve (XI), has both a cranial and spinal component. It primarily controls the function of certain muscles in the back of the neck and shoulder.
The cranial part arises from nuclei in the brainstem and innervates some of the muscles that help with head rotation, including the sternocleidomastoid muscle. The spinal root originates from nerve roots in the upper spinal cord (C1-C5), exits the spine, and joins the cranial part to form a single trunk. This trunk then innervates the trapezius muscle, which helps with shoulder movement and stability.
Damage to the accessory nerve can result in weakness or paralysis of the affected muscles, causing symptoms such as difficulty turning the head, weak shoulder shrugging, or winged scapula (a condition where the shoulder blade protrudes from the back).
A reflex is an automatic, involuntary and rapid response to a stimulus that occurs without conscious intention. In the context of physiology and neurology, it's a basic mechanism that involves the transmission of nerve impulses between neurons, resulting in a muscle contraction or glandular secretion.
Reflexes are important for maintaining homeostasis, protecting the body from harm, and coordinating movements. They can be tested clinically to assess the integrity of the nervous system, such as the knee-j jerk reflex, which tests the function of the L3-L4 spinal nerve roots and the sensitivity of the stretch reflex arc.
Naloxone is a medication used to reverse the effects of opioids, both illicit and prescription. It works by blocking the action of opioids on the brain and restoring breathing in cases where opioids have caused depressed respirations. Common brand names for naloxone include Narcan and Evzio.
Naloxone is an opioid antagonist, meaning that it binds to opioid receptors in the body without activating them, effectively blocking the effects of opioids already present at these sites. It has no effect in people who have not taken opioids and does not reverse the effects of other sedatives or substances.
Naloxone can be administered via intranasal, intramuscular, intravenous, or subcutaneous routes. The onset of action varies depending on the route of administration but generally ranges from 1 to 5 minutes when given intravenously and up to 10-15 minutes with other methods.
The duration of naloxone's effects is usually shorter than that of most opioids, so multiple doses or a continuous infusion may be necessary in severe cases to maintain reversal of opioid toxicity. Naloxone has been used successfully in emergency situations to treat opioid overdoses and has saved many lives.
It is important to note that naloxone does not reverse the effects of other substances or address the underlying causes of addiction, so it should be used as part of a comprehensive treatment plan for individuals struggling with opioid use disorders.
The abducens nerve, also known as the sixth cranial nerve (CN VI), is a motor nerve that controls the lateral rectus muscle of the eye. This muscle is responsible for moving the eye away from the midline (towards the temple) and enables the eyes to look towards the side while keeping them aligned. Any damage or dysfunction of the abducens nerve can result in strabismus, where the eyes are misaligned and point in different directions, specifically an adduction deficit, also known as abducens palsy or sixth nerve palsy.
The oculomotor nerve, also known as the third cranial nerve (CN III), is a motor nerve that originates from the midbrain. It controls the majority of the eye muscles, including the levator palpebrae superioris muscle that raises the upper eyelid, and the extraocular muscles that enable various movements of the eye such as looking upward, downward, inward, and outward. Additionally, it carries parasympathetic fibers responsible for pupillary constriction and accommodation (focusing on near objects). Damage to this nerve can result in various ocular motor disorders, including strabismus, ptosis, and pupillary abnormalities.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
Facial nerve injuries refer to damages or trauma inflicted on the facial nerve, also known as the seventh cranial nerve (CN VII). This nerve is responsible for controlling the muscles involved in facial expressions, eyelid movement, and taste sensation in the front two-thirds of the tongue.
There are two main types of facial nerve injuries:
1. Peripheral facial nerve injury: This type of injury occurs when damage affects the facial nerve outside the skull base, usually due to trauma from cuts, blunt force, or surgical procedures in the parotid gland or neck region. The injury may result in weakness or paralysis on one side of the face, known as Bell's palsy, and may also impact taste sensation and salivary function.
2. Central facial nerve injury: This type of injury occurs when damage affects the facial nerve within the skull base, often due to stroke, brain tumors, or traumatic brain injuries. Central facial nerve injuries typically result in weakness or paralysis only on the lower half of the face, as the upper motor neurons responsible for controlling the upper face receive innervation from both sides of the brain.
Treatment for facial nerve injuries depends on the severity and location of the damage. For mild to moderate injuries, physical therapy, protective eyewear, and medications like corticosteroids and antivirals may be prescribed. Severe cases might require surgical intervention, such as nerve grafts or muscle transfers, to restore function. In some instances, facial nerve injuries may heal on their own over time, particularly when the injury is mild and there is no ongoing compression or tension on the nerve.
Spinal muscular atrophies (SMAs) of childhood are a group of inherited neuromuscular disorders characterized by degeneration and loss of lower motor neurons in the spinal cord, leading to progressive muscle weakness and atrophy. The severity and age of onset can vary significantly, with some forms presenting in infancy and others in later childhood or even adulthood.
The most common form of SMA is 5q autosomal recessive SMA, also known as survival motor neuron (SMN) disease, which results from mutations in the SMN1 gene. The severity of this form can range from severe (type I or Werdnig-Hoffmann disease), intermediate (type II or chronic infantile neurodegenerative disorder), to mild (type III or Kugelberg-Welander disease).
Type I SMA is the most severe form, with onset before 6 months of age and rapid progression leading to death within the first two years of life if left untreated. Type II SMA has an onset between 6 and 18 months of age, with affected children never achieving the ability to walk independently. Type III SMA has a later onset, typically after 18 months of age, and is characterized by a slower progression, allowing for the ability to walk unaided, although mobility may be lost over time.
Other forms of childhood-onset SMA include autosomal dominant distal SMA, X-linked SMA, and spinal bulbar muscular atrophy (SBMA or Kennedy's disease). These forms have distinct genetic causes and clinical presentations.
In general, SMAs are characterized by muscle weakness, hypotonia, fasciculations, tongue atrophy, and depressed or absent deep tendon reflexes. Respiratory and nutritional support is often required in more severe cases. Recent advances in gene therapy have led to the development of disease-modifying treatments for some forms of SMA.
The olfactory nerve, also known as the first cranial nerve (I), is a specialized sensory nerve that is responsible for the sense of smell. It consists of thin, delicate fibers called olfactory neurons that are located in the upper part of the nasal cavity. These neurons have hair-like structures called cilia that detect and transmit information about odors to the brain.
The olfactory nerve has two main parts: the peripheral process and the central process. The peripheral process extends from the olfactory neuron to the nasal cavity, where it picks up odor molecules. These molecules bind to receptors on the cilia, which triggers an electrical signal that travels along the nerve fiber to the brain.
The central process of the olfactory nerve extends from the olfactory bulb, a structure at the base of the brain, to several areas in the brain involved in smell and memory, including the amygdala, hippocampus, and thalamus. Damage to the olfactory nerve can result in a loss of smell (anosmia) or distorted smells (parosmia).
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
The Recurrent Laryngeal Nerve (RLN) is a branch of the vagus nerve (cranial nerve X), which is a mixed sensory, motor, and autonomic nerve. The RLN has important functions in providing motor innervation to the intrinsic muscles of the larynx, except for the cricothyroid muscle, which is supplied by the external branch of the superior laryngeal nerve.
The recurrent laryngeal nerve supplies all the muscles that are responsible for adduction (bringing together) of the vocal cords, including the vocalis muscle, lateral cricoarytenoid, thyroarytenoid, and interarytenoid muscles. These muscles play a crucial role in voice production, coughing, and swallowing.
The right recurrent laryngeal nerve has a longer course than the left one. It loops around the subclavian artery in the chest before ascending to the larynx, while the left RLN hooks around the arch of the aorta. This anatomical course makes them vulnerable to injury during various surgical procedures, such as thyroidectomy and neck dissection, leading to potential voice impairment or vocal cord paralysis.
A muscle is a soft tissue in our body that contracts to produce force and motion. It is composed mainly of specialized cells called muscle fibers, which are bound together by connective tissue. There are three types of muscles: skeletal (voluntary), smooth (involuntary), and cardiac. Skeletal muscles attach to bones and help in movement, while smooth muscles are found within the walls of organs and blood vessels, helping with functions like digestion and circulation. Cardiac muscle is the specific type that makes up the heart, allowing it to pump blood throughout the body.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for innervating the muscles of the tongue, allowing for its movement and function. These muscles include the intrinsic muscles that alter the shape of the tongue and the extrinsic muscles that position it in the oral cavity. The hypoglossal nerve also has some minor contributions to the innervation of two muscles in the neck: the sternocleidomastoid and the trapezius. These functions are related to head turning and maintaining head position. Any damage to this nerve can lead to weakness or paralysis of the tongue, causing difficulty with speech, swallowing, and tongue movements.
The lingual nerve is a branch of the mandibular division of the trigeminal nerve (cranial nerve V). It provides general sensory innervation to the anterior two-thirds of the tongue, including taste sensation from the same region. It also supplies sensory innervation to the floor of the mouth and the lingual gingiva (gum tissue). The lingual nerve is closely associated with the submandibular and sublingual salivary glands and their ducts.
A spinal fracture, also known as a vertebral compression fracture, is a break in one or more bones (vertebrae) of the spine. This type of fracture often occurs due to weakened bones caused by osteoporosis, but it can also result from trauma such as a car accident or a fall.
In a spinal fracture, the front part of the vertebra collapses, causing the height of the vertebra to decrease, while the back part of the vertebra remains intact. This results in a wedge-shaped deformity of the vertebra. Multiple fractures can lead to a hunched forward posture known as kyphosis or dowager's hump.
Spinal fractures can cause pain, numbness, tingling, or weakness in the back, legs, or arms, depending on the location and severity of the fracture. In some cases, spinal cord compression may occur, leading to more severe symptoms such as paralysis or loss of bladder and bowel control.
In medical terms, the skin is the largest organ of the human body. It consists of two main layers: the epidermis (outer layer) and dermis (inner layer), as well as accessory structures like hair follicles, sweat glands, and oil glands. The skin plays a crucial role in protecting us from external factors such as bacteria, viruses, and environmental hazards, while also regulating body temperature and enabling the sense of touch.
Spinal cord regeneration is the process of regrowth or repair of damaged or severed nerves and neural connections within the spinal cord. This complex process involves various biological mechanisms, including the activation of stem cells, the promotion of axonal growth, and the remodeling of neural circuits. The ultimate goal of spinal cord regeneration research is to develop effective therapies for individuals with spinal cord injuries, enabling them to regain sensory and motor functions and improve their quality of life.
Electromyography (EMG) is a medical diagnostic procedure that measures the electrical activity of skeletal muscles during contraction and at rest. It involves inserting a thin needle electrode into the muscle to record the electrical signals generated by the muscle fibers. These signals are then displayed on an oscilloscope and may be heard through a speaker.
EMG can help diagnose various neuromuscular disorders, such as muscle weakness, numbness, or pain, and can distinguish between muscle and nerve disorders. It is often used in conjunction with other diagnostic tests, such as nerve conduction studies, to provide a comprehensive evaluation of the nervous system.
EMG is typically performed by a neurologist or a physiatrist, and the procedure may cause some discomfort or pain, although this is usually minimal. The results of an EMG can help guide treatment decisions and monitor the progression of neuromuscular conditions over time.
The spinal trigeminal nucleus is a component of the trigeminal nerve sensory nuclear complex located in the brainstem. It is responsible for receiving and processing pain, temperature, and tactile discrimination sensations from the face and head, particularly from the areas of the face that are more sensitive to pain and temperature (the forehead, eyes, nose, and mouth). The spinal trigeminal nucleus is divided into three subnuclei: pars oralis, pars interpolaris, and pars caudalis. These subnuclei extend from the pons to the upper part of the medulla oblongata.
 Spinal nerve
Spinal nerve
Spinal nerve root
Cervical spinal nerve 2
Thoracic spinal nerve 12
Sacral spinal nerve 4
Thoracic spinal nerve 3
Sacral spinal nerve 2
Cervical spinal nerve 3
Thoracic spinal nerve 9
Root of spinal nerve
Thoracic spinal nerve 2
Thoracic spinal nerve 6
Thoracic spinal nerve 8
Cervical spinal nerve 4
Cervical spinal nerve 1
Sacral spinal nerve 3
Cervical spinal nerve 5
Sacral spinal nerve 1
Cervical spinal nerve 7
Thoracic spinal nerve 11
Thoracic spinal nerve 5
Thoracic spinal nerve 7
Cervical spinal nerve 6
Cervical spinal nerve 8
Thoracic spinal nerve 10
Ramus of spinal nerve
Thoracic spinal nerve 4
Thoracic spinal nerve 1
Sacral spinal nerve 5
Ventral ramus of spinal nerve
Spine19
- Everywhere else in the spine, the nerve emerges below the vertebra with the same name. (wikipedia.org)
- Unlike PNS, however, spinal nerve root stimulators are located along the relatively stable and immobile spine. (medscape.com)
- It's hard to understand the wide-ranging effects compressed nerves can have on the body, much less how your spine is contributing to these nerve impediments. (idealspine.com)
- Considering the direct path of most nerve bundles is through the spine, it makes sense to conclude a problem here. (idealspine.com)
- Through palpitation of the spine and diagnostic imaging, chiropractors are able to track down exactly where nerve impediments are occurring. (idealspine.com)
- The lower thoracic spine and upper lumbar spine are common areas of interest, since a majority of abdominal organ nerves branch out from these segments. (idealspine.com)
- Your spinal cord is the thick bundle of nerves that runs from your brain down the inside of your spine. (msdmanuals.com)
- Spinal Cord The spinal cord is a long, fragile tubelike structure that begins at the end of the brain stem and continues down almost to the bottom of the spine. (msdmanuals.com)
- Because many of these nerves run throughout your spine, sometimes your back structures are the cause of the entrapped nerve. (sinicropispine.com)
- Since an entrapped nerve can lead to symptoms in other areas of your body, the true source of pain may actually be housed in a different area of your spine. (sinicropispine.com)
- Your spine specialist can help pinpoint exactly where the trapped nerve is located so that treatment is focused on the correct location. (sinicropispine.com)
- It depicts the cervical, thoracic, lumbar, and sacral sections of the spine, indicates the exit points of the nerve roots and how they combine into spinal nerves, and labels the sensory distribution of each nerve to the arms, torso, and legs. (typecalendar.com)
- It illustrates the cervical, thoracic, lumbar, and sacral regions of the spine and the associated spinal nerves. (typecalendar.com)
- If you've tried everything for your excruciating chronic spine or nerve pain and you don't think there is anything that can help, a nerve stimulator might be right for you. (keyclinics.com)
- A spinal cord stimulator consists of electrodes that are placed along the affected area of the spine. (keyclinics.com)
- Depending on the area of the spine involved, he makes an incision through which he places the electrodes that run along the spinal cord. (keyclinics.com)
- Maldonado, AA & Spinner, RJ 2017, ' Lateral pectoral nerve transfer for spinal accessory nerve injury ', Journal of Neurosurgery: Spine , vol. 26, no. 1, pp. 112-115. (elsevierpure.com)
- Intraoperative neuromonitoring (IONM) is a technique that has become an essential tool in spine and peripheral nerve surgeries. (genesispub.org)
- Spina bifida is a neural tube defect - a type of birth defect of the brain, spine, or spinal cord. (nih.gov)
Injuries20
- The researchers are the first to use decorin to suppress inflammation and scar formation in spinal cord injuries. (scienceblog.com)
- Infusion of decorin into spinal cord injuries prevents the formation of proteoglycan rich scar tissue by suppressing inflammation. (scienceblog.com)
- Misaligned scar tissue that forms at spinal cord injuries physically blocks nerve regeneration and contains molecules called chondroitin sulfate proteoglycans that inhibit nerve fiber growth. (scienceblog.com)
- Decorin inhibits the action of pro - inflammatory molecules released in spinal cord injuries, called transforming growth factors, which are thought to promote the formation of scar tissue. (scienceblog.com)
- Using a high-powered laser scanning microscope and protein chemistry to analyze tissue samples, Davies and co-workers were able to show that decorin infusion reduced inflammation, scar formation and the levels of some proteoglycans by 80-95 percent allowing nerve fibers (called axons) to grow across spinal cord injuries in just four days. (scienceblog.com)
- Such injuries can damage a few, many, or almost all of the nearby axons-the extensions of nerve cells that carry signals up and down the spinal cord between the brain and the rest of the body. (nih.gov)
- People who survive severe spinal cord injuries often experience life-long disability. (nih.gov)
- Peripheral nerve injuries frequently occur secondary to myopathy in recumbent adult cattle. (nih.gov)
- Nerves and Nerve Injuries. (radiopaedia.org)
- Spinal cord injuries often cause severe and lifelong health problems for the sufferer, and as a result, they (and their loved ones) endure financial significant financial stress. (eglaw.com)
- On the job injuries for those that perform physical labor and operate heavy machinery like construction workers also see a higher level of spinal cord injuries, but these cases are handled through workers' compensation . (eglaw.com)
- Spinal cord injuries can have lasting and devastating effects on mobility and cognitive function due to permanent nerve cell damage or death. (spinalcordinjuryzone.com)
- Spinal cord injury is a serious disease of the central nervous system involving irreversible nerve injury and various organ system injuries . (bvsalud.org)
- Learning the spinal nerves and their corresponding vertebral levels provides a foundation for diagnosing and treating spinal disorders and injuries. (typecalendar.com)
- The authors present 2 patients who presented late (8 and 10 months) after their SAN injuries, in whom a lateral pectoral nerve transfer to the SAN was performed successfully using a supraclavicular approach. (elsevierpure.com)
- Spinal nerve blocks are indicated to relieve pain, weakness, numbness and tingling sensations in your neck, back, and extremities due to nerve injuries such as a pinched nerve or narrowing of the spinal column (stenosis). (bluewaterpain.com)
- Complex sciatic nerve gap injuries in rats were repaired with cell-free and cell-laden nerve scaffolds for 12 weeks (scaffold and NCSC groups, respectively). (biomedcentral.com)
- It provides real-time information about the function of the spinal cord and peripheral nerves, allowing surgeons to detect potential injuries and take immediate corrective action. (genesispub.org)
- Spinal injuries can be like downed power lines - even if everything on either side of the injury is perfectly functional, the break can effectively shut down the whole system. (newatlas.com)
- There's a perception that people with spinal cord injuries will only be happy if they can walk again. (newatlas.com)
Posterior17
- The dorsal ramus contains nerves that serve the posterior portions of the trunk carrying visceral motor, somatic motor, and somatic sensory information to and from the skin and muscles of the back (epaxial muscles). (wikipedia.org)
- The posterior distribution includes the suboccipital nerve (C1), the greater occipital nerve (C2) and the third occipital nerve (C3). (wikipedia.org)
- The medial branches of the posterior divisions of the lumbar nerves run close to the articular processes of the vertebrae and end in the multifidus muscle. (wikipedia.org)
- The afferent fibers (somatic sensory, sympathetic, and taste) have their cells of origin in the jugular ganglion and in the nodosal ganglion (ganglion of the trunk) and on entering the medulla divide into ascending and descending branches as do the sensory fibers of the posterior roots of the spinal nerves after they enter the spinal cord. (bartleby.com)
- 1) The somatic sensory fibers are few in number, convey impulses from a limited area of the skin on the back of the ear and posterior part of the external auditory meatus, and probably join the spinal tract of the trigeminal nerve to terminate in its nucleus. (bartleby.com)
- The commonest cause of injury to the spinal accessory nerve is iatrogenic, occurring as it does during surgical excision biopsy of cervical lymph nodes in the posterior triangle of the neck. (stateclaims.ie)
- The nerve is extremely vulnerable because it is covered only by the skin and subcutaneous fascia in the posterior triangle of the neck. (stateclaims.ie)
- If open lymph node biopsy is necessary, the procedure, even though considered minor and routine, should be performed by an experienced surgeon who is aware of the potential for injury to surrounding structures, such as the spinal accessory nerve in the case of posterior triangle node biopsy. (stateclaims.ie)
- Cranial nerve XI, the spinal accessory nerve (SAN), is vulnerable to injury, owing to its long and superficial course in the posterior cervical neck. (medscape.com)
- Course of the spinal accessory nerve (SAN) in the posterior cervical triangle. (medscape.com)
- Each nerve then divides into anterior and posterior nerve fibres. (teachmeanatomy.info)
- These nerves all enter the skin at the middle of the posterior border of the sternocleidomastoid. (teachmeanatomy.info)
- The nerve also communicates with the auricular branch of the vagus nerve and the posterior auricular branch of the facial nerve (which innervates some small muscles around the ear). (teachmeanatomy.info)
- The posterior (or dorsal) branches (or divisions) of the spinal nerves are as a rule smaller than the anterior divisions. (wikidoc.org)
- Additionally, we will look at the specialized posterior, anterior, and lateral spinal nerve roots that carry information between the cord and periphery. (typecalendar.com)
- Right side: The nerve passes posterior to the IJV, crosses the first part of subclavian artery, and then enters the thorax. (medscape.com)
- Left side: The nerve passes between the left common carotid artery and the subclavian artery and posterior to the left brachiocephalic vein to enter thorax. (medscape.com)
Disorders4
- A team led by Drs. Zu-Hang Sheng from NIH's National Institute of Neurological Disorders and Stroke (NINDS) and Xiao-Ming Xu from Indiana University have proposed that a lack of energy in injured nerve cells might contribute to impaired repair and regeneration. (nih.gov)
- Disorders of the spinal cord and cauda equina. (nih.gov)
- Understanding the fundamental anatomy and organization of this intricate structure lays the groundwork for medical professionals to diagnose and treat spinal disorders. (typecalendar.com)
- Additionally, our findings extend beyond nerve injury to other disorders, such as neurodegenerative diseases, where neuroinflammation also occurs," added Dr. Le Pichon. (nih.gov)
Ventral8
- Each spinal nerve is a mixed nerve, formed from the combination of nerve root fibers from its dorsal and ventral roots. (wikipedia.org)
- The ventral ramus contains nerves that serve the remaining anterior parts of the trunk and the upper and lower limbs (hypaxial muscles) carrying visceral motor, somatic motor, and sensory information to and from the ventrolateral body surface, structures in the body wall, and the limbs. (wikipedia.org)
- The spinal nucleus lies ventral to the vestibular and cochlear nuclei and medial to the inferior cerebellar peduncles . (radiopaedia.org)
- The formation of the spinal nerve from the dorsal and ventral roots. (wikidoc.org)
- It labels the dorsal and ventral rami of each spinal nerve and shows how they innervate specific areas of the body. (typecalendar.com)
- Each spinal nerve also has a mix of nerve fibers from the dorsal and ventral roots of the spinal cord. (pediaa.com)
- The cranial nerves are 12 pairs of nerves that can be seen on the ventral (bottom) surface of the brain. (washington.edu)
- Note: the olfactory "nerve" is composed of the rootlets of olfactory hair cells in the nasal mucosa and is not visible on the ventral surface of the brain. (washington.edu)
Showing the spinal cord1
- Lateral view of the spinal column with brain silhouetted showing the spinal cord origin of the spinal nerves. (smartdraw.com)
Anatomy9
- In this review we discuss the anatomy, techniques, advantages and disadvantages, and clinical studies available for each of these types of spinal nerve root stimulation. (medscape.com)
- The classic and much-used Gray's Anatomy assigned cervical nerves to a proprioceptive sensory role, with only the SAN providing motor innervation to the trapezius. (medscape.com)
- Understanding spinal anatomy and the network of nerves that transmit signals throughout the body is key for medical students and healthcare professionals. (typecalendar.com)
- Let's dive in to decoding the anatomy of spinal nerves . (typecalendar.com)
- The clear and detailed illustrations with accompanying explanatory text outline the basic anatomy of the spinal cord, spinal nerves, nerve plexuses, and dermatomes. (typecalendar.com)
- In this article, we will provide an overview of basic spinal cord anatomy, exploring key components like vertebrae, nerve roots, spinal segments, gray matter, white matter, and the integrating network of neuronal pathways. (typecalendar.com)
- Gaining familiarity with core spinal cord anatomy and terminology provides the basis for appreciating its physiology and pathology. (typecalendar.com)
- On this chart, the detailed anatomy of the brain is shown along with a section of the spinal cord. (3bscientific.com)
- The two lower images show the anatomy of the nerves themselves and cross section reveals the minute bundles contain within each nerve fiber. (doereport.com)
Brain35
- The findings, published today online in the journal Brain , show that when the cell receptor was blocked, nerve cells were preserved, protecting against loss of motor function. (newswise.com)
- Every organ in our bodies functions by way of sending and receiving electrical impulses, transmitted via nerves to and from the brain. (idealspine.com)
- If a nerve is too taut or slack the wave amplitude will be smaller and slower, resulting in incomplete information transmitted from the point of stimulus to the brain. (spinalresearch.com.au)
- The serotonin system has widespread influences across many brain and body functions, and a reduced action of serotonin on the motor nerve cells would make them harder to activate and keep firing. (meresearch.org.uk)
- That is, stronger signals from the brain to the spinal nerve cells would be required for the same muscle contractions, and this would be perceived as more effort. (meresearch.org.uk)
- Viral meningitis is inflammation of the layers of tissue that cover the brain and spinal cord (meninges) and of the fluid-filled space between the meninges (subarachnoid space) when it is caused by viruses. (merckmanuals.com)
- Introduction to Meningitis Meningitis is inflammation of the layers of tissue that cover the brain and spinal cord (meninges) and of the fluid-filled space between the meninges (subarachnoid space). (merckmanuals.com)
- The brain and spinal cord are covered by three layers of tissue called meninges. (merckmanuals.com)
- The subarachnoid space is located between the middle layer and the inner layer of the meninges, which cover the brain and spinal cord. (merckmanuals.com)
- It contains the cerebrospinal fluid, which flows through the meninges, fills the spaces within the brain, and helps cushion the brain and spinal cord. (merckmanuals.com)
- Your muscles move when your brain sends a signal to them through your nerves. (msdmanuals.com)
- The spinal cord is like an electric cable that carries signals back and forth between your brain and body. (msdmanuals.com)
- Spinal fluid is a liquid that surrounds your brain and spinal cord. (msdmanuals.com)
- Spinal fluid helps cushion your brain if you hit your head or fall. (msdmanuals.com)
- Spinal fluid moves freely around your brain and spinal cord. (msdmanuals.com)
- The peripheral nervous system consists of more than 100 billion nerve cells (neurons) that run throughout the body like strings, making connections with the brain, other parts of the body, and often with each other. (msdmanuals.com)
- Overview of the Peripheral Nervous System The peripheral nervous system refers to the parts of the nervous system that are outside the central nervous system, that is, those outside the brain and spinal cord. (msdmanuals.com)
- Brain The brain's functions are both mysterious and remarkable, relying on billions of nerve cells and the internal communication between them. (msdmanuals.com)
- Each large axon is surrounded by oligodendrocytes in the brain and spinal cord and by Schwann cells in the peripheral nervous system. (msdmanuals.com)
- Nerves that directly connect the brain and the brain stem with the eyes, ears, nose, and throat and with various parts of the head, neck, and trunk are called cranial nerves. (msdmanuals.com)
- The spinal cord is a vital part of the central nervous system, relaying messages from the brain to the rest of the body including muscles and organs. (eglaw.com)
- Sensory nerves send information such as touch, temperature, and pain to the brain and spinal cord. (github.io)
- Motor nerves send signals from the brain back into the muscles, causing them to contract either voluntarily or reflexively. (github.io)
- The spinal cord is a fundamental part of the central nervous system, transmitting neural signals between the brain and the rest of the body. (typecalendar.com)
- The spinal nerves, which branch out from the spinal cord, transmit sensory information and movement instructions between the brain and the rest of the body. (advancedosm.com)
- Spinal levels of extracellular signal-regulated kinase (ERK), NF-κB P65, brain-derived neurotrophic factor (BDNF), growth-associated protein (GAP)-43, calcitonin gene-related peptide (CGRP), and inflammation factors were calculated by western blot analysis. (biomedcentral.com)
- Peripheral nerves are nerves that reside outside the brain and spinal cord. (pediaa.com)
- Peripheral nerves send messages from the brain and spinal cord to the other parts of the body. (pediaa.com)
- A nerve injury impairs the ability of the brain to communicate with the other parts, muscles, and organs. (pediaa.com)
- Peripheral nerves are nerves that reside outside the brain and spinal cord, whereas spinal nerves are mixed nerves that directly interact with the spinal cord to modulate motor and sensory information from the body's periphery. (pediaa.com)
- The olfactory tract contains nerve fibers projecting out of the olfactory bulb to the brain. (washington.edu)
- The poster details the entire human nervous system including the human brain and spinal cord. (3bscientific.com)
- Motor nerves carry messages from the brain to muscles and organs, telling them how to respond. (amnh.org)
- This signal travels along your nerves to the part of your brain that processes the message as pain. (amnh.org)
- That's because nerves on each side of the body connect to the opposite side of the brain. (amnh.org)
Network of interc1
- Some anterior rami merge with adjacent anterior rami to form a nerve plexus, a network of interconnecting nerves. (wikipedia.org)
Hypoglossal Nerve2
- The Hypoglossal Nerve ( XII cranial ) consists of somatic motor fibers only and supplies the muscles of the tongue. (bartleby.com)
- These nerves travel with the hypoglossal nerve to reach their respective muscles. (teachmeanatomy.info)
Lumbar9
- There are eight pairs of cervical nerves, twelve pairs of thoracic nerves, five pairs of lumbar nerves, five pairs of sacral nerves, and one pair of coccygeal nerves. (wikipedia.org)
- The thoracic, lumbar, and sacral nerves are then numbered by the vertebra above. (wikipedia.org)
- The lumbar nerves are the five spinal nerves emerging from the lumbar vertebrae. (wikipedia.org)
- Doctors suspect viral meningitis based on symptoms and do a spinal tap (lumbar puncture) to confirm the diagnosis. (merckmanuals.com)
- Under anesthesia, the lumbar (L) L5 and L6 spinal nerves are ligated while L4 is left untouched, inducing long-lasting mechanical and cold allodynia while minimizing motor impairments. (nih.gov)
- More specifically, there are eight cervical nerve pairs (C1-C8), twelve thoracic nerve pairs (T1-T12), five lumbar nerve pairs (L1-L5), 5 sacral (S1-S5), and a single coccygeal nerve pair. (github.io)
- We will examine how the delicate spinal cord is protected within the vertebral column and its sectional organization into cervical, thoracic, lumbar, and sacral regions based on vertebral level. (typecalendar.com)
- The spinal cord is a cylindrical structure of nervous tissue that extends from the medulla oblongata in the brainstem down to the lumbar region of the vertebral column. (typecalendar.com)
- Generally, they consist of eight cervical spinal nerve pairs, twelve thoracic pairs, five lumbar pairs, five sacral pairs, and one coccygeal pair. (pediaa.com)
Vertebral column5
- In the human body there are 31 pairs of spinal nerves, one on each side of the vertebral column. (wikipedia.org)
- Outside the vertebral column, the nerve divides into branches. (wikipedia.org)
- The spinal cord and its peripheral nerves are protected by the vertebral column, a stack of bones which surround and provide support. (medlineplus.gov)
- At each vertebral level, paired spinal nerves leave the spinal cord via the intervertebral foramina of the vertebral column. (teachmeanatomy.info)
- A spinal nerve chart is a diagram that maps the spinal nerves branching from the vertebral column to the parts of the body they innervate. (typecalendar.com)
Innervation5
- Nerve conduction studies, one year later, showed minimal partial re-innervation and no further return of muscle function could be expected. (stateclaims.ie)
- Anatomic study of the SAN has long maintained a debate as to the exact contributions of this nerve and other cervical motor nerves to the innervation of the trapezius muscle. (medscape.com)
- Subsequent anatomic study reported a possible plexus composed of both cervical nerves and contributions from the SAN that collectively provided trapezial motor innervation. (medscape.com)
- The cervical plexus is a network of nerve fibres that supplies innervation to some of the structures in the neck and trunk. (teachmeanatomy.info)
- In this article, we'll explore how to read and utilize a spinal nerve chart to map innervation patterns. (typecalendar.com)
Peripheral nerve injury6
- In small ruminants, peripheral nerve injury seems less common, most likely due to their smaller size,but may occur from predator wounds or iatrogenically following intramuscular drug administration. (nih.gov)
- Spinal or peripheral nerve injury. (caa.co.uk)
- Severe peripheral nerve injury significantly affects patients' quality of life and induces neuropathic pain. (biomedcentral.com)
- Neural crest stem cells (NCSCs) exhibit several attractive characteristics for cell-based therapies following peripheral nerve injury. (biomedcentral.com)
- Treatment of peripheral nerve injury (PNI) remains a worldwide clinical challenge. (biomedcentral.com)
- AFAIU, the silicone scaffold is intended to mimic the function of the myelin sheaths that guide nerve regrowth in the case of peripheral nerve injury. (newatlas.com)
Vagus Nerve4
- They are said to join the vagus nerve. (bartleby.com)
- The Vagus Nerve ( X cranial ) contains somatic sensory, sympathetic afferent, somatic motor, sympathetic efferent and (taste fibers? (bartleby.com)
- The vagus nerve exits the skull through the jugular foramen. (medscape.com)
- As it emerges from the jugular foramen, the vagus nerve bears the superior and inferior ganglionic swellings that are the sensory ganglia of the nerve. (medscape.com)
Fibers in the spinal1
- The descending fibers in the spinal tract of the trigeminal terminating in the nucleus of the tract probably establish relations through connecting neurons with motor nuclei in the anterior column of the spinal cord and with motor nuclei of the medulla. (bartleby.com)
Bundles of nerve fibers2
- Peripheral nerves consist of bundles of nerve fibers. (msdmanuals.com)
- They are bundles of nerve fibers that connect to the spinal cord and carry information to and away from the spinal nerves. (pediaa.com)
Signals8
- A spinal nerve is a mixed nerve, which carries motor, sensory, and autonomic signals between the spinal cord and the body. (wikipedia.org)
- For the gut especially, getting nerve signals in their full capacity is crucial. (idealspine.com)
- Faulty nerve signals most often meet their impediment between their point of origin and their destination. (idealspine.com)
- You can't feel blocked nerve signals, but your gut definitely can. (idealspine.com)
- Signals of muscle activity can be recorded using a grid of electrodes placed on the skin which, when decoded using computer algorithms, can give information about the activity of the motor nerve cells. (meresearch.org.uk)
- A spinal nerve chart provides a visual reference to help memorize the vertebral levels, sensory pathways, and motor functions of the network of nerves that transmit signals between the central nervous system and periphery. (typecalendar.com)
- Both peripheral nerves and spinal nerves are responsible for transmitting signals throughout the body. (pediaa.com)
- Nerves carry signals in one direction. (amnh.org)
Impulses8
- Unlike spinal cord stimulation, in which electrical impulses are directed at the dorsal columns, spinal nerve root stimulation guides electrical current directly to one or more nerve roots. (medscape.com)
- The spinal nucleus receives afferent impulses from the ipsilateral face which convey information about pain, temperature and crude touch. (radiopaedia.org)
- These layers form the myelin sheath, which speeds the conduction of nerve impulses along the nerve fiber. (msdmanuals.com)
- Nerves conduct impulses at different speeds depending on their diameter and on the amount of myelin around them. (msdmanuals.com)
- A nerve cell (neuron) consists of a large cell body and nerve fibers-one elongated extension (axon) for sending impulses and usually many branches (dendrites) for receiving impulses. (msdmanuals.com)
- The impulses from the axon cross a synapse (the junction between two nerve cells) to the dendrite of another cell. (msdmanuals.com)
- Nerve impulses travel much faster in nerves with a myelin sheath than in those without one. (msdmanuals.com)
- Additionally, peripheral nerves carry either efferent (motor) or afferent (sensory) electrical impulses. (pediaa.com)
Muscles4
- The cervical nerves innervate the sternohyoid, sternothyroid and omohyoid muscles. (wikipedia.org)
- Reduced muscle strength may be due to problems with the nerves that drive these muscles, specifically those nerves in the spinal cord that supply the muscle fibres and control our movements. (meresearch.org.uk)
- The behaviour of motor nerve cells during contractions of the ankle muscles will be compared between people with ME/CFS and healthy control subjects. (meresearch.org.uk)
- The cranial part sends it fibers through the vagus to the laryngeal nerves to supply the muscles of the larynx. (bartleby.com)
Recovery after spinal cord i2
- We have found a promising new approach to control inflammation and scar formation, which will be an important part of future strategies to encourage axon regeneration and recovery after spinal cord injury," Davies said. (scienceblog.com)
- Restoring Cellular Energetics Promotes Axonal Regeneration and Functional Recovery after Spinal Cord Injury. (nih.gov)
Axons9
- Mitochondria, illustrated here, provide the energy that nerve cells need to regenerate their axons after injury. (nih.gov)
- In nerve cell axons, mitochondria are anchored to their spots by a protein called syntaphilin. (nih.gov)
- As expected, damaged axons didn't regrow in normal mice after a moderate spinal cord injury. (nih.gov)
- Each year thousands of patients confront this reality, facing life-long losses in sensation and motor function from spinal cord injury and related conditions in which axons are badly damaged or severed. (nih.gov)
- Temple University researchers have found that Lin28, a molecule involved in the self-renewal of stem cells, can lead to the long-distance regeneration of axons in mice with spinal cord or optic nerve damage. (spinalcordinjuryzone.com)
- In mice that sustained injury to the spinal cord or optic nerve tracts, which connect to the retina in the eye, upregulation of Lin28 led to significant long-distance regeneration of both axons and the optic nerve in adult mice. (spinalcordinjuryzone.com)
- It was found that treating mice (normal, non-transgenic) post-spinal cord or optic nerve injury stimulated significant regeneration of spinal tract and optic nerve axons after incurred injury. (spinalcordinjuryzone.com)
- According to the study, "In mice with spinal cord injury, Lin28 injection resulted in the growth of axons to more than three millimeters beyond the area of axon damage, while in animals with optic nerve injury, axons regrew the entire length of the optic nerve tract. (spinalcordinjuryzone.com)
- Peripheral nerves have both myelinated and unmyelinated axons . (pediaa.com)
Vertebrae10
- The spinal nerve emerges from the spinal column through an opening (intervertebral foramen) between adjacent vertebrae. (wikipedia.org)
- The meningeal branches (recurrent meningeal or sinuvertebral nerves) branch from the spinal nerve and re-enter the intervertebral foramen to serve the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum of the vertebrae. (wikipedia.org)
- The cervical nerves are the spinal nerves from the cervical vertebrae in the cervical segment of the spinal cord. (wikipedia.org)
- Although there are seven cervical vertebrae (C1-C7), there are eight cervical nerves C1-C8. (wikipedia.org)
- The thoracic nerves are the twelve spinal nerves emerging from the thoracic vertebrae. (wikipedia.org)
- A downloadable spinal nerve chart PDF is included, listing each nerve, its origin vertebrae, and the region it enervates. (typecalendar.com)
- Use the chart to memorize the arrangements and relationships between vertebrae, nerves, and extremities or as a practical guide for pathology analysis. (typecalendar.com)
- It presents the spinal nerves in sequential order, beginning with C1 exiting between the skull and C1 vertebra and descending to S5 between the L5 and S1 vertebrae. (typecalendar.com)
- This is a procedure in which a small portion of the arch of the vertebrae is removed to relieve pressure on the pinched nerve. (drrobertblok.com)
- The spinal nerves exit the spinal cord through small openings between vertebrae (foramina). (advancedosm.com)
Mice with spinal cord i1
- In a study published online in the journal Molecular Therapy , the Temple researchers describe the ability of Lin28 - when expressed above its usual levels - to fuel axon regrowth in mice with spinal cord injury or optic nerve injury, enabling repair of the body's communication grid. (nih.gov)
Vertebra5
- This is true for all spinal nerves except for the first spinal nerve pair (C1), which emerges between the occipital bone and the atlas (the first vertebra). (wikipedia.org)
- Thus the cervical nerves are numbered by the vertebra below, except spinal nerve C8, which exists below vertebra C7 and above vertebra T1. (wikipedia.org)
- In the case of a lumbarized S1 vertebra (also known as L6) or a sacralized L5 vertebra, the nerves are typically still counted to L5 and the next nerve is S1. (wikipedia.org)
- Each thoracic nerve T1-T12 originates from below each corresponding thoracic vertebra. (wikipedia.org)
- The chart depicts the intervertebral foramina between each vertebra where the spinal nerves exit. (typecalendar.com)
Anatomical5
- The spinal nerve chart pdf is an anatomical diagram showing the nerves that exit from the spinal cord. (typecalendar.com)
- Overall, the spinal nerve chart pdf is an essential anatomical study aid. (typecalendar.com)
- For example, we recently utilized 3D printing to fabricate anatomical nerve guidance conduits with gradients of growth factors (nerve growth factor and glial cell derived neurotrophic factor) that contained physical (topographical) and biochemical cues to promote the regeneration of a sciatic nerve tibial bifurcation injury model [ 6 ]. (biomedcentral.com)
- This colorful anatomical poster focuses on the spinal nerves of the human nervous system. (3bscientific.com)
- Owing to this close anatomical relationship, the nerve is at risk of injury during thyroid surgeries. (medscape.com)
Neck11
- Furthermore, peripheral nerve stimulators are often needed in regions of the body such as the neck or extremities that are highly mobile, placing high levels of stress along the course of the electrode systems. (medscape.com)
- Nerve conduction studies confirmed complete motor conduction block at the level of the surgical scar in her neck. (stateclaims.ie)
- This area is known as the nerve point of the neck (Erb's point), and is utilised when performing a cervical plexus nerve block. (teachmeanatomy.info)
- The nerve then pierces the deep cervical fascia and then gives branches that pass superiorly and inferiorly to supply the anterolateral skin of the neck and upper sternum. (teachmeanatomy.info)
- A herniated disc commonly causes a sharp or shock-like pain in the neck and/or arm by inflaming or compressing a nearby nerve root. (spine-health.com)
- This pain can radiate from a pinched nerve in the neck down through the shoulder, arm, hand, and/or fingers. (spine-health.com)
- A pinched nerve can occur in multiple places in your body, but is very common in the neck and back. (triadspine.com)
- Many people correctly associate pinched spinal nerves with neck and back pain. (advancedosm.com)
- In addition to localized neck or back pain, pinched spinal nerves can produce a number of other uncomfortable symptoms. (advancedosm.com)
- Spinal nervous supply is present all over the body except in the head and neck regions. (pediaa.com)
- Dr. Devin and his partners use gentle chiropractic methods including NUCCA upper cervical chiropractic, ArthroStim (similar to ProAdjuster) and FDA cleared low level laser therapy to help with painful and chronic conditions including headaches and migraines, neck pain, back pain, shoulder pain, knee pain, disc problems, pinched nerves, sciatica, carpal tunnel syndrome and other persistent conditions. (thechronicpainchronicle.com)
Origin of the spinal1
- The nucleus of origin of the spinal part undoubtedly receives either directly or indirectly terminals and collaterals controlling voluntary movements from the pyramidal tracts. (bartleby.com)
Damage16
- One of the contributing factors to CSM is cell death, which ultimately leads to nerve damage and lost motor function. (newswise.com)
- Adult nerve cells in the spinal cord don't regrow after damage. (nih.gov)
- This not only means more severe symptoms, but the prospect of permanent nerve damage. (idealspine.com)
- Spinal cord damage can certainly occur through infections, but most happen through physical trauma. (eglaw.com)
- Damage to the spinal accessory nerve has life-long implications for the patient and can be associated with significant litigation costs. (stateclaims.ie)
- In rare cases, an operation is needed to fix the problem or prevent further damage to the nerve. (sinicropispine.com)
- As with any procedure, a spinal nerve block may be associated with certain risks and complications such as pain (temporary), bruising, infection at the site of the injection and nerve damage. (bluewaterpain.com)
- I am losing the use of my legs due to 'scar tissue' nerve/muscle damage from radiation. (cancer.org)
- The radiation did severe damage to the tissue, on top of that he has a nerve-damage. (cancer.org)
- SSEPs are particularly useful in surgeries involving the spinal cord, where damage to the sensory pathways can lead to loss of sensation or even paralysis. (genesispub.org)
- We call damage to a peripheral nerve peripheral neuropathy. (pediaa.com)
- This can damage the nerves and spinal cord. (nih.gov)
- This often results in damage to the spinal cord and nerves. (cdc.gov)
- There is usually little or no nerve damage. (cdc.gov)
- After an injury, neurons undergo genetic changes that are initiated by DLK and lead to pain and nerve damage. (nih.gov)
- Damage to the spinal cord can develop hours to days after nerve injury. (nih.gov)
Nervous system8
- The spinal nerves are part of the peripheral nervous system. (wikipedia.org)
- With this chart , you'll have a handy visual aid to quickly reference the segments, roots, and branches of the elaborate spinal cord nervous system. (typecalendar.com)
- The main difference between peripheral nerve and spinal nerve is that peripheral nerves reside outside the central nervous system , whereas spinal nerves reside within the central nervous system. (pediaa.com)
- Nerves are glistening white chord-like bundles of fibers surrounded by a sheet that connects the nervous system with the other parts of the body. (pediaa.com)
- These nerves belong to the peripheral nervous system. (pediaa.com)
- Peripheral nerves are outside the central nervous system, whereas spinal nerves are within the central nervous system. (pediaa.com)
- The nervous system is made of different kinds of nerves. (amnh.org)
- The spinal cord is the main highway of the nervous system. (amnh.org)
Thoracic nerves1
- The intercostal nerves come from thoracic nerves T1-T11, and run between the ribs. (wikipedia.org)
Suffer a spinal cord i2
Plexus8
- Nerves emerging from a plexus contain fibers from various spinal nerves, which are now carried together to some target location. (wikipedia.org)
- A loop of nerves called ansa cervicalis is part of the cervical plexus. (wikipedia.org)
- The plexus is formed by the anterior rami (divisions) of cervical spinal nerves C1-C4. (teachmeanatomy.info)
- The spinal nerves C1 - C4 form the basis of the cervical plexus. (teachmeanatomy.info)
- The cervical plexus begins as the anterior fibres of the spinal nerves C1, C2, C3 and C4. (teachmeanatomy.info)
- After arising from the cervical plexus, the nerve travels down the surface of the anterior scalene muscle and enters the thorax. (teachmeanatomy.info)
- An orientation of the cervical nerves ( brachial plexus) is included. (doereport.com)
- The pharyngeal plexus innervates the palate and pharynx and is formed by branches from the external laryngeal nerve, pharyngeal nerves, branches from the cranial nerve IX, and the sympathetic trunk. (medscape.com)
Lateral4
- The spinal part arises from lateral cell groups in the anterior column near its dorso-lateral margin in the upper five or six segments of the cord, its roots pass through the lateral funiculus to the lateral surface of the cord. (bartleby.com)
- The cranial part arises from the nucleus ambiguus, the continuation in the medulla oblongata of the lateral cell groups of the anterior column of the spinal cord from which the spinal part has origin. (bartleby.com)
- The root fibers of the cranial part of the accessory nerve pass anterior to the spinal tract of the trigeminal while those of the vagus pass through or dorsal to the trigeminal root, and emerge in the line of the postero-lateral sulcus. (bartleby.com)
- Spinner, Robert J. / Lateral pectoral nerve transfer for spinal accessory nerve injury . (elsevierpure.com)
Symptoms4
- They will also assess whether any abnormalities are consistent with reduced actions of serotonin, and determine whether changes in nerve cell behaviour are associated with symptoms of ME/CFS. (meresearch.org.uk)
- The signs and symptoms caused by a cervical herniated disc can vary depending on which nerve root is compressed. (spine-health.com)
- Any of these structures can potentially press on a nerve, pinching it and producing symptoms. (advancedosm.com)
- What are the symptoms of a pinched spinal nerve? (advancedosm.com)
Injury to the spinal1
- In this article, Professor Patrick Broe, retired Consultant Surgeon and Clinical Director at the RCSI Hospital Group, highlights the causes of surgical injury to the spinal accessory nerve, which is frequently not recognised, and discusses the risks with performing surgical cervical lymph node biopsy. (stateclaims.ie)
Inflammation4
- In severe cases, nerves experiencing inflammation may require more complex treatment as defined by an ongoing Chiropractic BioPhysics (CBP) treatment plan. (idealspine.com)
- A pinched nerve or nerve root inflammation may also cause numbness and/or weakness to radiate down into the shoulder, arm, hand, and/or fingers. (spine-health.com)
- Long-term pain and inflammation that occurs after nerve injury is triggered by a specific protein, according to a study in mice led by NIH's Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and the National Center for Complementary and Integrative Health (NCCIH). (nih.gov)
- They found that mice missing DLK did not develop long-term pain after injury, nor did their spinal cords develop a hallmark of nerve inflammation called microgliosis. (nih.gov)
Axon3
- In their study - published online in the journal Molecular Therapy - the Temple University researchers found that the overexpression of Lin28 in mice with spinal cord or optic nerve injury led to stimulation of axon regrowth, allowing the repair of neuronal communication networks in the body. (spinalcordinjuryzone.com)
- In explaining the findings, Dr. Li said, "We observed a lot of axon regrowth, which could be very significant clinically, since there currently are no regenerative treatments for spinal cord injury or optic nerve injury. (spinalcordinjuryzone.com)
- It protects the axon against the stretching forces on the nerve. (pediaa.com)
Glossopharyngeal1
- The upper part of the nucleus ambiguus gives motor fibers to the vagus and glossopharyngeal nerves. (bartleby.com)
Surgical5
- Of course, PNS has its limitations, including the need for surgical access to the target nerve and restriction of pain relief to the distribution of the target nerve. (medscape.com)
- What is the Non-surgical Method of Spinal Decompression? (drrobertblok.com)
- What is the Surgical Method of Spinal Decompression? (drrobertblok.com)
- At Advanced Orthopaedics & Sports Medicine of Houston, TX, we offer a comprehensive range of treatment options - both conservative and surgical - for pinched spinal nerves. (advancedosm.com)
- IONM helps preserve nerve function, reduces surgical complications and improves patient outcomes. (genesispub.org)
Abstract1
- abstract = "Spinal accessory nerve (SAN) injury results in loss of motor function of the trapezius muscle and leads to severe shoulder problems. (elsevierpure.com)
Accessory nerve injury3
- The State Claims Agency received five claims in the last six years relating to spinal accessory nerve injury, two of which were finalised resulting in paid damages of €261,308. (stateclaims.ie)
- The neurologist made a diagnosis of left spinal accessory nerve injury, due to the previous lymph node biopsy. (stateclaims.ie)
- High-resolution ultrasonography (HRUS) allows visualization of the normal SAN, as well as changes after accessory nerve injury. (medscape.com)
Damaged spinal cords1
- Infusing a naturally occurring anti-scarring agent called decorin into the damaged spinal cords of rats suppresses key molecules that block nerve regeneration after spinal cord injury, say researchers in the European Journal of Neuroscience. (scienceblog.com)
Afferent1
- It has been demonstrated that PNI changes both primary afferent and second-order spinal cord neurons, leading to sensitization and abnormal responses to peripheral stimuli [ 8 ]. (biomedcentral.com)
Anterior1
- The phrenic nerve arises from the anterior rami of C3-C5. (teachmeanatomy.info)
Regrowth1
- Mice engineered to lack a protein that anchors mitochondria in injured nerve cells showed regrowth of those cells after a spinal cord injury. (nih.gov)
Larynx2
- The C1 spinal nerve gives rise to nerves to the geniohyoid (moves the hyoid bone anteriorly and upwards, expanding the airway) and the thyrohyoid (which depresses the hyoid bone and elevates the larynx). (teachmeanatomy.info)
- Several nerves in the larynx control these tasks. (medscape.com)
Sensory nerves2
- It is also connected indirectly with the spinal somatic sensory nerves by association fibers of the proper fasciculi. (bartleby.com)
- Sensory nerves carry messages such as pressure, pain, and temperature. (amnh.org)
Ansa cervicalis1
- The ansa cervicalis is a loop of nerves, formed by nerve roots C1-C3. (teachmeanatomy.info)
Trigeminal5
- The spinal nucleus of the trigeminal nerve is one of three major nuclei that make up the trigeminal sensory nerve nuclear complex along with the main sensory nucleus and the mesencephalic nucleus 1-2 . (radiopaedia.org)
- The spinal nucleus of the trigeminal nerve is a paired structure and is an inferior continuation of the main sensory nucleus of the trigeminal nerve. (radiopaedia.org)
- The trigeminal nerve has both sensory and motor functions. (washington.edu)
- To test the sensory part of the trigeminal nerve, lightly touch various parts of your partner's face with piece of cotton or a blunt object. (washington.edu)
- Although much of the mouth and teeth are innervated by the trigeminal nerve, don't put anything into your subject's mouth. (washington.edu)
Types of nerves1
- There are basically two major types of nerves: sensory and motor. (github.io)
Pairs3
- In total, there are 31 pairs of spinal nerves grouped regionally by spinal region. (github.io)
- The pdf provides a visual reference for the 31 bilateral pairs of spinal nerves and their origins along the spinal cord. (typecalendar.com)
- In fact, humans have 31 pairs of spinal nerves. (pediaa.com)
Sciatic5
- Kadekaro, Massako, Alison M. Crane, Louis Sokoloff, and National Institute of Mental Health (U.S.). 'Differential Effects of Electrical Stimulation of Sciatic Nerve on Metabolic Activity in Spinal Cord and Dorsal Root Ganglion in the Rat. (nih.gov)
- One common type of radiculopathy is sciatica, which affects the lower body and occurs when the large sciatic nerve becomes compressed. (advancedosm.com)
- Here, we investigate the therapeutic effect of NCSC therapy and associated changes in the spinal cord in a sciatic nerve transection (SNT) model. (biomedcentral.com)
- NCSC-laden nerve scaffolds mitigated SNT-induced neuropathic pain and improved motor function recovery after sciatic nerve repair. (biomedcentral.com)
- The mechanical principle that disc narrowing can reduce the pressure on a nerve root produced by a disc protrusion may be an explanation of how chemonycleolysis relieves sciatic pain. (cdc.gov)