Skull Base Neoplasms
Skull Base
Chordoma
Skull Fractures
Cerebrospinal Fluid Rhinorrhea
Surgical Equipment
Meningioma
Sphenoid Sinus
Base Pairing
Sphenoid Bone
Base Sequence
Meningeal Neoplasms
Cranial Fossa, Posterior
Ethmoid Bone
Cranial Nerve Diseases
Endoscopy
Tomography, X-Ray Computed
Petrous Bone
Neuronavigation
Otorhinolaryngologic Surgical Procedures
Cranial Nerve Neoplasms
Temporal Bone
Nasal Cavity
Paranasal Sinuses
Paraganglioma in the frontal skull base--case report. (1/187)
A 56-year-old female presented with a paraganglioma in the left anterior cranial fossa who manifesting as persistent headache. Computed tomography and magnetic resonance imaging showed a solid, enhanced tumor with a cystic component located medially. The tumor was attached to the left frontal base and the sphenoid ridge. Angiography demonstrated a hypervascular tumor fed mainly by the left middle meningeal artery at the left sphenoid ridge. The preoperative diagnosis was meningioma of the left frontal base. The tumor was totally resected via a left frontotemporal craniotomy. Histological examination revealed the characteristic cellular arrangement of paraganglioma generally designated as the "Zellbaren pattern" on light microscopy. Only 10 patients with supratentorial paraganglioma have been reported, seven located in the parasellar area. The origin of the present tumor may have been the paraganglionic cells which strayed along the middle meningeal artery at differentiation. (+info)Primary osteogenic sarcoma involving sella-sphenoid sinus--case report. (2/187)
A 38-year-old male presented with an extremely rare primary osteogenic sarcoma, unassociated with Paget's disease or late effects of radiation, involving the sella and sphenoid sinus region. Complete excision of the tumor was achieved through an extended frontobasal approach. Postoperatively, six cycles of combination chemotherapy (adriamycin, ifosphamide, and cisplatin) followed by a total of 55 Gy local radiotherapy in 33 fractions was given. Primary osteogenic sarcoma should be considered in the differential diagnosis of the central skull base tumors. Osteogenic sarcoma, in general, has a bad prognosis, and should be managed aggressively with multimodality treatment including gross total surgical resection, combination chemotherapy, and radiotherapy. (+info)Cranionavigator combining a high-speed drill and a navigation system for skull base surgery--technical note. (3/187)
Drilling of the skull base bone without damaging the important inside structures and with the correct orientation is very difficult even with the help of the anatomical landmarks. Monitoring of the location and direction of the drill tip and indications of the removed part of the bone during the drilling procedure enhances safety and achieves less invasive neurosurgery. We have developed a novel cranionavigator by combining a high-speed drill with a neurosurgical navigation system. To reduce the positional error to less than 1.5 mm, the position sensor (magnetic field sensor) must be attached 5 cm from the metallic fan portion of the drill and the sensor kept at least 10 cm away from the operating microscope. Simulation studies with the cranionavigator using two dried skulls and three cadaver heads were performed before clinical application. Clinically, this surgical instrument was used in four patients with the skull base tumor. The cranionavigator helped to safely drill the skull base bone in a shorter time by dynamic and real-time display of the precise operating site and extent of bone drilling on the preoperative computed tomography scans or magnetic resonance images. The cranionavigator is a very helpful instrument for skull base surgery in the hands of neurosurgeons with extensive expertise and anatomical knowledge. (+info)Pure extradural approach for skull base lesions. (4/187)
Lesions in the parasellar and paracavernous regions can be removed by various skull base approaches involving basal osteotomies. A major complication of intradural skull base approaches is CSF leak and associated meningitis. We have managed 5 patients with skull base lesions with a pure extradural approach using wide basal osteotomies. The operative techniques are described. (+info)Infratemporal fossa approaches to the lateral skull base. (5/187)
The infra-temporal fossa approach is one of the lateral approaches to the skull base. It is indicated for the treatment of tumors such as glomus tumor, petrous apex cholesteatoma, chondroma, lower cranial nerve neuroma and nasopharyngeal cancer. In the present paper, we described the surgical anatomy of the lateral skull base and the indications for the infra-temporal fossa approach with its variants. We showed the hints and pitfalls in the procedures. Five illustrative cases are also presented. (+info)Recurrence of clival chordoma along the surgical pathway. (6/187)
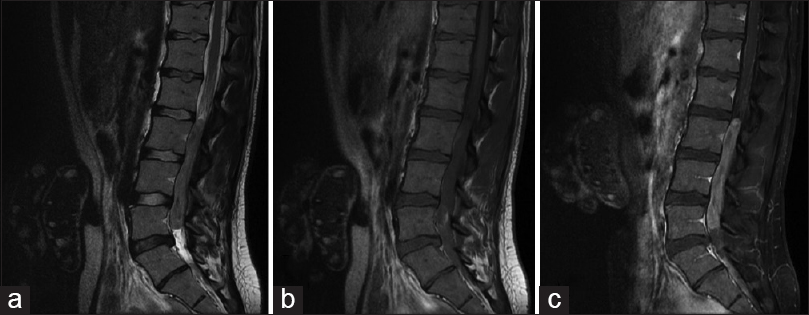
Chordomas are locally aggressive malignant tumors of notochordal origin whose metastatic potential is increasingly recognized. Surgical pathway recurrence has been noted only rarely in the literature. We present three patients with clival chordomas whose sole or initial recurrence was along the pathway of prior surgical access. A characteristic mass found along the pathway of prior surgical access for resection of a chordoma should suggest recurrent chordoma. (+info)Imaging findings in schwannomas of the jugular foramen. (7/187)
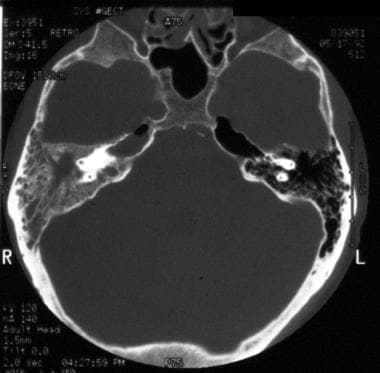
BACKGROUND AND PURPOSE: Tumors of the cranial nerve sheath constitute 5% to 10% of all intracranial neoplasms, yet few articles have described their CT and MR characteristics. We report the imaging findings in a relatively large series of schwannomas of the jugular foramen, contrasting them with other disease entities, especially vestibular schwannomas and tumors of the glomus jugulare. METHODS: CT and/or MR studies of eight patients who underwent surgery for histologically proved schwannomas were reviewed retrospectively. One additional patient with an assumed schwannoma of the jugular foramen, who did not have surgery, was also included. RESULTS: Surgical findings showed schwannomas of the glossopharyngeal nerve in seven patients and tumor involvement of both the glossopharyngeal and vagal nerves in one patient. All tumors were partially located within the jugular foramen. Growth extending within the temporal bone was typical. Tumor extended into the posterior cranial fossa in all nine patients and produced mass effect on the brain stem and/or cerebellum in seven patients; in five patients, tumor extended below the skull base. On unenhanced CT scans, tumors were isodense with brain in six patients and hypodense in two. In seven patients, CT scans with bone algorithm showed an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. On MR images, T1 signal from tumor was low and T2 signal was high relative to white matter in all patients. Contrast enhancement on CT and/or MR studies was strong in eight patients and moderate in one. CONCLUSION: Schwannoma of the jugular foramen is characteristically a sharply demarcated, contrast-enhancing tumor, typically centered on or based in an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. Intraosseous extension may be marked. (+info)Low-stage medulloblastoma: final analysis of trial comparing standard-dose with reduced-dose neuraxis irradiation. (8/187)
PURPOSE: To evaluate prospectively the effects on survival, relapse-free survival, and patterns of relapse of reduced-dose (23.4 Gy in 13 fractions) compared with standard-dose (36 Gy in 20 fractions) neuraxis irradiation in patients 3 to 21 years of age with low-stage medulloblastoma, minimal postoperative residual disease, and no evidence of neuraxis disease. PATIENTS AND METHODS: The Pediatric Oncology Group and Children's Cancer Group randomized 126 patients to the study. All patients received posterior fossa irradiation to a total dose of 54 Gy in addition to the neuraxis treatment. Patients were staged postoperatively with contrast-enhanced cranial computed tomography, myelography, and CSF cytology. Of the registered patients, 38 were ineligible. RESULTS: The planned interim analysis that resulted in closure of the protocol showed that patients randomized to the reduced neuraxis treatment had increased frequency of relapse. In the final analysis, eligible patients receiving standard-dose neuraxis irradiation had 67% event-free survival (EFS) at 5 years (SE = 7.4%), whereas eligible patients receiving reduced-dose neuraxis irradiation had 52% event-free survival at 5 years (SE = 7.7%) (P =.080). At 8 years, the respective EFS proportions were also 67% (SE = 8.8%) and 52% (SE = 11%) (P =.141). These data confirm the original one-sided conclusions but suggest that differences are less marked with time. CONCLUSION: Reduced-dose neuraxis irradiation (23.4 Gy) is associated with increased risk of early relapse, early isolated neuraxis relapse, and lower 5-year EFS and overall survival than standard irradiation (36 Gy). The 5-year EFS for patients receiving standard-dose irradiation is suboptimal, and improved techniques and/or therapies are needed to improve ultimate outcome. Chemotherapy may contribute to this improvement. (+info)Skull base neoplasms refer to abnormal growths or tumors located in the skull base, which is the region where the skull meets the spine and where the brain connects with the blood vessels and nerves that supply the head and neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells in this area, including bone, nerve, glandular, and vascular tissue.
Skull base neoplasms can cause a range of symptoms depending on their size, location, and growth rate. Some common symptoms include headaches, vision changes, hearing loss, facial numbness or weakness, difficulty swallowing, and balance problems. Treatment options for skull base neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. The specific treatment plan will depend on the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history.
The skull base is the lower part of the skull that forms the floor of the cranial cavity and the roof of the facial skeleton. It is a complex anatomical region composed of several bones, including the frontal, sphenoid, temporal, occipital, and ethmoid bones. The skull base supports the brain and contains openings for blood vessels and nerves that travel between the brain and the face or neck. The skull base can be divided into three regions: the anterior cranial fossa, middle cranial fossa, and posterior cranial fossa, which house different parts of the brain.
The skull is the bony structure that encloses and protects the brain, the eyes, and the ears. It is composed of two main parts: the cranium, which contains the brain, and the facial bones. The cranium is made up of several fused flat bones, while the facial bones include the upper jaw (maxilla), lower jaw (mandible), cheekbones, nose bones, and eye sockets (orbits).
The skull also provides attachment points for various muscles that control chewing, moving the head, and facial expressions. Additionally, it contains openings for blood vessels, nerves, and the spinal cord to pass through. The skull's primary function is to protect the delicate and vital structures within it from injury and trauma.
Skull neoplasms refer to abnormal growths or tumors that develop within the skull. These growths can be benign (non-cancerous) or malignant (cancerous). They can originate from various types of cells, such as bone cells, nerve cells, or soft tissues. Skull neoplasms can cause various symptoms depending on their size and location, including headaches, seizures, vision problems, hearing loss, and neurological deficits. Treatment options include surgery, radiation therapy, and chemotherapy. It is important to note that a neoplasm in the skull can also refer to metastatic cancer, which has spread from another part of the body to the skull.
A chordoma is a rare, slow-growing tumor that typically develops in the bones of the spine or skull. These tumors originate from remnants of the notochord, a structure that forms during embryonic development and eventually becomes part of the spinal cord. Chordomas are usually low-grade malignancies but can be aggressive and locally invasive, potentially causing pain, neurological symptoms, or structural damage to the spine or skull. Treatment typically involves surgical resection, often combined with radiation therapy.
A skull fracture is a break in one or more of the bones that form the skull. It can occur from a direct blow to the head, penetrating injuries like gunshot wounds, or from strong rotational forces during an accident. There are several types of skull fractures, including:
1. Linear Skull Fracture: This is the most common type, where there's a simple break in the bone without any splintering, depression, or displacement. It often doesn't require treatment unless it's near a sensitive area like an eye or ear.
2. Depressed Skull Fracture: In this type, a piece of the skull is pushed inward toward the brain. Surgery may be needed to relieve pressure on the brain and repair the fracture.
3. Diastatic Skull Fracture: This occurs along the suture lines (the fibrous joints between the skull bones) that haven't fused yet, often seen in infants and young children.
4. Basilar Skull Fracture: This involves fractures at the base of the skull. It can be serious due to potential injury to the cranial nerves and blood vessels located in this area.
5. Comminuted Skull Fracture: In this severe type, the bone is shattered into many pieces. These fractures usually require extensive surgical repair.
Symptoms of a skull fracture can include pain, swelling, bruising, bleeding (if there's an open wound), and in some cases, clear fluid draining from the ears or nose (cerebrospinal fluid leak). Severe fractures may cause brain injury, leading to symptoms like confusion, loss of consciousness, seizures, or neurological deficits. Immediate medical attention is necessary for any suspected skull fracture.
Cerebrospinal fluid (CSF) rhinorrhea is a condition where the cerebrospinal fluid, which surrounds and protects the brain and spinal cord, leaks through the nasal cavity. This occurs due to a defect or opening in the skull base or the thin bone that separates the brain from the nasal cavity, known as the cribriform plate.
CSF rhinorrhea can result from trauma, surgery, or spontaneously due to increased pressure in the brain. It is important to diagnose and treat this condition promptly because it increases the risk of meningitis, an infection of the membranes covering the brain and spinal cord. Treatment options include bed rest, hydration, stool softeners, and sometimes surgical repair of the defect.
Surgical equipment refers to the specialized tools and instruments used by medical professionals during surgical procedures. These devices are designed to assist in various aspects of surgery, such as cutting, grasping, retraction, clamping, and suturing. Surgical equipment can be categorized into several types based on their function and use:
1. Cutting instruments: These include scalpels, scissors, and surgical blades designed to cut through tissues with precision and minimal trauma.
2. Grasping forceps: Forceps are used to hold, manipulate, or retrieve tissue, organs, or other surgical tools. Examples include Babcock forceps, Kelly forceps, and Allis tissue forceps.
3. Retractors: These devices help to expose deeper structures by holding open body cavities or tissues during surgery. Common retractors include Weitlaner retractors, Army-Navy retractors, and self-retaining retractors like the Bookwalter system.
4. Clamps: Used for occluding blood vessels, controlling bleeding, or approximating tissue edges before suturing. Examples of clamps are hemostats, bulldog clips, and Satinsky clamps.
5. Suction devices: These tools help remove fluids, debris, and smoke from the surgical site, improving visibility for the surgeon. Examples include Yankauer suctions and Frazier tip suctions.
6. Needle holders: Specialized forceps designed to hold suture needles securely during the process of suturing or approximating tissue edges.
7. Surgical staplers: Devices that place linear staple lines in tissues, used for quick and efficient closure of surgical incisions or anastomoses (joining two structures together).
8. Cautery devices: Electrosurgical units that use heat generated by electrical current to cut tissue and coagulate bleeding vessels.
9. Implants and prosthetics: Devices used to replace or reinforce damaged body parts, such as artificial joints, heart valves, or orthopedic implants.
10. Monitoring and navigation equipment: Advanced tools that provide real-time feedback on patient physiology, surgical site anatomy, or instrument positioning during minimally invasive procedures.
These are just a few examples of the diverse range of instruments and devices used in modern surgery. The choice of tools depends on various factors, including the type of procedure, patient characteristics, and surgeon preference.
A meningioma is a type of slow-growing tumor that forms on the membranes (meninges) surrounding the brain and spinal cord. It's usually benign, meaning it doesn't spread to other parts of the body, but it can still cause serious problems if it grows and presses on nearby tissues.
Meningiomas most commonly occur in adults, and are more common in women than men. They can cause various symptoms depending on their location and size, including headaches, seizures, vision or hearing problems, memory loss, and changes in personality or behavior. In some cases, they may not cause any symptoms at all and are discovered only during imaging tests for other conditions.
Treatment options for meningiomas include monitoring with regular imaging scans, surgery to remove the tumor, and radiation therapy to shrink or kill the tumor cells. The best treatment approach depends on factors such as the size and location of the tumor, the patient's age and overall health, and their personal preferences.
The sphenoid sinuses are air-filled spaces located within the sphenoid bone, which is one of the bones that make up the skull base. These sinuses are located deep inside the skull, behind the eyes and nasal cavity. They are paired and separated by a thin bony septum, and each one opens into the corresponding nasal cavity through a small opening called the sphenoethmoidal recess. The sphenoid sinuses vary greatly in size and shape between individuals. They develop during childhood and continue to grow until early adulthood. The function of the sphenoid sinuses, like other paranasal sinuses, is not entirely clear, but they may contribute to reducing the weight of the skull, resonating voice during speech, and insulating the brain from trauma.
A craniotomy is a surgical procedure where a bone flap is temporarily removed from the skull to access the brain. This procedure is typically performed to treat various neurological conditions, such as brain tumors, aneurysms, arteriovenous malformations, or traumatic brain injuries. After the underlying brain condition is addressed, the bone flap is usually replaced and secured back in place with plates and screws. The purpose of a craniotomy is to provide access to the brain for diagnostic or therapeutic interventions while minimizing potential damage to surrounding tissues.
Base pairing is a specific type of chemical bonding that occurs between complementary base pairs in the nucleic acid molecules DNA and RNA. In DNA, these bases are adenine (A), thymine (T), guanine (G), and cytosine (C). Adenine always pairs with thymine via two hydrogen bonds, while guanine always pairs with cytosine via three hydrogen bonds. This precise base pairing is crucial for the stability of the double helix structure of DNA and for the accurate replication and transcription of genetic information. In RNA, uracil (U) takes the place of thymine and pairs with adenine.
The sphenoid bone is a complex, irregularly shaped bone located in the middle cranial fossa and forms part of the base of the skull. It articulates with several other bones, including the frontal, parietal, temporal, ethmoid, palatine, and zygomatic bones. The sphenoid bone has two main parts: the body and the wings.
The body of the sphenoid bone is roughly cuboid in shape and contains several important structures, such as the sella turcica, which houses the pituitary gland, and the sphenoid sinuses, which are air-filled cavities within the bone. The greater wings of the sphenoid bone extend laterally from the body and form part of the skull's lateral walls. They contain the superior orbital fissure, through which important nerves and blood vessels pass between the cranial cavity and the orbit of the eye.
The lesser wings of the sphenoid bone are thin, blade-like structures that extend anteriorly from the body and form part of the floor of the anterior cranial fossa. They contain the optic canal, which transmits the optic nerve and ophthalmic artery between the brain and the orbit of the eye.
Overall, the sphenoid bone plays a crucial role in protecting several important structures within the skull, including the pituitary gland, optic nerves, and ophthalmic arteries.
A base sequence in the context of molecular biology refers to the specific order of nucleotides in a DNA or RNA molecule. In DNA, these nucleotides are adenine (A), guanine (G), cytosine (C), and thymine (T). In RNA, uracil (U) takes the place of thymine. The base sequence contains genetic information that is transcribed into RNA and ultimately translated into proteins. It is the exact order of these bases that determines the genetic code and thus the function of the DNA or RNA molecule.
Meningeal neoplasms, also known as malignant meningitis or leptomeningeal carcinomatosis, refer to cancerous tumors that originate in the meninges, which are the membranes covering the brain and spinal cord. These tumors can arise primarily from the meningeal cells themselves, although they more commonly result from the spread (metastasis) of cancer cells from other parts of the body, such as breast, lung, or melanoma.
Meningeal neoplasms can cause a variety of symptoms, including headaches, nausea and vomiting, mental status changes, seizures, and focal neurological deficits. Diagnosis typically involves imaging studies (such as MRI) and analysis of cerebrospinal fluid obtained through a spinal tap. Treatment options may include radiation therapy, chemotherapy, or surgery, depending on the type and extent of the tumor. The prognosis for patients with meningeal neoplasms is generally poor, with a median survival time of several months to a year.
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
The ethmoid bone is a paired, thin, and lightweight bone that forms part of the skull's anterior cranial fossa and contributes to the formation of the orbit and nasal cavity. It is located between the frontal bone above and the maxilla and palatine bones below. The ethmoid bone has several important features:
1. Cribriform plate: This is the horizontal, sieve-like portion that forms part of the anterior cranial fossa and serves as the roof of the nasal cavity. It contains small openings (foramina) through which olfactory nerves pass.
2. Perpendicular plate: The perpendicular plate is a vertical structure that projects downward from the cribriform plate, forming part of the nasal septum and separating the left and right nasal cavities.
3. Superior and middle nasal conchae: These are curved bony projections within the lateral walls of the nasal cavity that help to warm, humidify, and filter incoming air.
4. Lacrimal bone: The ethmoid bone articulates with the lacrimal bone, forming part of the medial wall of the orbit.
5. Frontal process: This is a thin, vertical plate that articulates with the frontal bone above the orbit.
6. Sphenoidal process: The sphenoidal process connects the ethmoid bone to the sphenoid bone posteriorly.
The ethmoid bone plays a crucial role in protecting the brain and providing structural support for the eyes, as well as facilitating respiration by warming, humidifying, and filtering incoming air.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
Endoscopy is a medical procedure that involves the use of an endoscope, which is a flexible tube with a light and camera at the end, to examine the interior of a body cavity or organ. The endoscope is inserted through a natural opening in the body, such as the mouth or anus, or through a small incision. The images captured by the camera are transmitted to a monitor, allowing the physician to visualize the internal structures and detect any abnormalities, such as inflammation, ulcers, or tumors. Endoscopy can also be used for diagnostic purposes, such as taking tissue samples for biopsy, or for therapeutic purposes, such as removing polyps or performing minimally invasive surgeries.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
Neuronavigation is a surgical technique that uses imaging technology, such as MRI or CT scans, to create a 3D map of the patient's brain in real-time during surgery. This allows surgeons to accurately locate and navigate to specific areas of the brain with greater precision and less invasiveness, improving surgical outcomes and reducing the risk of complications.
The neuronavigation system typically consists of a computer workstation, tracking systems, and instruments that are equipped with sensors. The system is able to track the position and orientation of these instruments relative to the patient's brain, allowing the surgeon to visualize the location of the instruments on the 3D map in real-time.
Neuronavigation has become an essential tool in many neurosurgical procedures, including tumor resection, functional neurosurgery, and deep brain stimulation. It enables surgeons to perform more complex surgeries with increased safety and efficacy, ultimately improving the quality of care for patients undergoing these procedures.
Paranasal sinus neoplasms refer to abnormal growths or tumors that develop within the paranasal sinuses, which are air-filled cavities located inside the skull near the nasal cavity. These tumors can be benign (noncancerous) or malignant (cancerous), and they can arise from various types of tissue within the sinuses, such as the lining of the sinuses (mucosa), bone, or other soft tissues.
Paranasal sinus neoplasms can cause a variety of symptoms, including nasal congestion, nosebleeds, facial pain or numbness, and visual disturbances. The diagnosis of these tumors typically involves a combination of imaging studies (such as CT or MRI scans) and biopsy to determine the type and extent of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches, depending on the specific type and stage of the neoplasm.
Otorhinolaryngologic surgical procedures are surgeries that are performed on the head and neck region, specifically involving the ear, nose, and throat (ENT) regions. This field is also known as otolaryngology-head and neck surgery. The procedures can range from relatively minor ones, such as removing a small nasal polyp or inserting ear tubes, to more complex surgeries like cochlear implantation, endoscopic sinus surgery, or removal of tumors in the head and neck region. These surgical procedures are typically performed by specialized physicians called otorhinolaryngologists (also known as ENT surgeons) who have completed extensive training in this area.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
The temporal bone is a paired bone that is located on each side of the skull, forming part of the lateral and inferior walls of the cranial cavity. It is one of the most complex bones in the human body and has several important structures associated with it. The main functions of the temporal bone include protecting the middle and inner ear, providing attachment for various muscles of the head and neck, and forming part of the base of the skull.
The temporal bone is divided into several parts, including the squamous part, the petrous part, the tympanic part, and the styloid process. The squamous part forms the lateral portion of the temporal bone and articulates with the parietal bone. The petrous part is the most medial and superior portion of the temporal bone and contains the inner ear and the semicircular canals. The tympanic part forms the lower and anterior portions of the temporal bone and includes the external auditory meatus or ear canal. The styloid process is a long, slender projection that extends downward from the inferior aspect of the temporal bone and serves as an attachment site for various muscles and ligaments.
The temporal bone plays a crucial role in hearing and balance, as it contains the structures of the middle and inner ear, including the oval window, round window, cochlea, vestibule, and semicircular canals. The stapes bone, one of the three bones in the middle ear, is entirely encased within the petrous portion of the temporal bone. Additionally, the temporal bone contains important structures for facial expression and sensation, including the facial nerve, which exits the skull through the stylomastoid foramen, a small opening in the temporal bone.
The nasal cavity is the air-filled space located behind the nose, which is divided into two halves by the nasal septum. It is lined with mucous membrane and is responsible for several functions including respiration, filtration, humidification, and olfaction (smell). The nasal cavity serves as an important part of the upper respiratory tract, extending from the nares (nostrils) to the choanae (posterior openings of the nasal cavity that lead into the pharynx). It contains specialized structures such as turbinate bones, which help to warm, humidify and filter incoming air.
Paranasal sinuses are air-filled cavities in the skull that surround the nasal cavity. There are four pairs of paranasal sinuses, including the maxillary, frontal, ethmoid, and sphenoid sinuses. These sinuses help to warm, humidify, and filter the air we breathe. They also contribute to our voice resonance and provide a slight cushioning effect for the skull. The openings of the paranasal sinuses lead directly into the nasal cavity, allowing mucus produced in the sinuses to drain into the nose. Infections or inflammation of the paranasal sinuses can result in conditions such as sinusitis.
 Rathke's pouch
Rathke's pouch Researchers interested in Skull Base Neoplasms | Yale School of Medicine
Researchers interested in Skull Base Neoplasms | Yale School of Medicine Benign Tumors of the Skull Base: Practice Essentials, Epidemiology, Etiology
Benign Tumors of the Skull Base: Practice Essentials, Epidemiology, Etiology ESTRO ACROP guideline for target volume delineation of skull base tumors
ESTRO ACROP guideline for target volume delineation of skull base tumors Publications | Plural Publishing
Publications | Plural Publishing Nikolas Blevins, MD's Profile | Stanford Profiles
Nikolas Blevins, MD's Profile | Stanford Profiles Portal Regional da BVS
Portal Regional da BVS The Radiology Assistant : Trigeminal neuralgia
The Radiology Assistant : Trigeminal neuralgia Mariana Bradshaw, Ph.D. - Neuro-Oncology Faculty | MD Anderson Cancer Center
Mariana Bradshaw, Ph.D. - Neuro-Oncology Faculty | MD Anderson Cancer Center Serous fluid: Metastatic sarcomas, melanoma, and other non-epithelial neoplasms - CytoJournal
Serous fluid: Metastatic sarcomas, melanoma, and other non-epithelial neoplasms - CytoJournal Dr. Charles Suntra M.D., Doctor in Modesto, CA | Sutter Health
Dr. Charles Suntra M.D., Doctor in Modesto, CA | Sutter Health Brain Tumors in Dogs and Cats: Diagnosis and Therapy - WSAVA 2003 Congress - VIN
Brain Tumors in Dogs and Cats: Diagnosis and Therapy - WSAVA 2003 Congress - VIN Neurofibromatosis 1 and intracranial neoplasms of childhood | MedLink Neurology
Neurofibromatosis 1 and intracranial neoplasms of childhood | MedLink Neurology Namespace
Namespace Lateral Temporal Bone Resection | Iowa Head and Neck Protocols
Lateral Temporal Bone Resection | Iowa Head and Neck Protocols Benign neoplasm of pituitary gland (Concept Id: C0496901)
- MedGen - NCBI
Benign neoplasm of pituitary gland (Concept Id: C0496901)
- MedGen - NCBI "OncoLog Volume 51, Number 11, November 2006" by Sunni Hosemann and Reginald F. Munden MD
"OncoLog Volume 51, Number 11, November 2006" by Sunni Hosemann and Reginald F. Munden MD Etiologies and Treatment Options for Sudden Sensorineural Hearing Loss | The Hearing Review
Etiologies and Treatment Options for Sudden Sensorineural Hearing Loss | The Hearing Review transcranial magnetic stimulation
transcranial magnetic stimulation