Insurance, Health, Reimbursement
Reimbursement, Incentive
Diagnosis-Related Groups
Medicare
Medicaid
United States
Cost Control
Cost Allocation
Insurance, Hospitalization
Costs and Cost Analysis
Capitation Fee
Health Care Costs
Prospective Payment System
Drug Costs
Group Purchasing
Centers for Medicare and Medicaid Services (U.S.)
Current Procedural Terminology
Fee-for-Service Plans
Cost-Benefit Analysis
Insurance, Pharmaceutical Services
Hospital Costs
Health Expenditures
Practice Management, Medical
Fee Schedules
Cost Savings
Economics, Pharmaceutical
Skilled Nursing Facilities
Financial Management, Hospital
Medicare Part B
Fees, Pharmaceutical
Medicare Part A
Physician's Practice Patterns
Managed Care Programs
Health Policy
Uncompensated Care
Nursing Homes
Medical Laboratory Science
Orphan Drug Production
Formularies as Topic
State Health Plans
Inventions
Private Practice
Practice patterns, case mix, Medicare payment policy, and dialysis facility costs. (1/500)
OBJECTIVE: To evaluate the effects of case mix, practice patterns, features of the payment system, and facility characteristics on the cost of dialysis. DATA SOURCES/STUDY SETTING: The nationally representative sample of dialysis units in the 1991 U.S. Renal Data System's Case Mix Adequacy (CMA) Study. The CMA data were merged with data from Medicare Cost Reports, HCFA facility surveys, and HCFA's end-stage renal disease patient registry. STUDY DESIGN: We estimated a statistical cost function to examine the determinants of costs at the dialysis unit level. PRINCIPAL FINDINGS: The relationship between case mix and costs was generally weak. However, dialysis practices (type of dialysis membrane, membrane reuse policy, and treatment duration) did have a significant effect on costs. Further, facilities whose payment was constrained by HCFA's ceiling on the adjustment for area wage rates incurred higher costs than unconstrained facilities. The costs of hospital-based units were considerably higher than those of freestanding units. Among chain units, only members of one of the largest national chains exhibited significant cost savings relative to independent facilities. CONCLUSIONS: Little evidence showed that adjusting dialysis payment to account for differences in case mix across facilities would be necessary to ensure access to care for high-cost patients or to reimburse facilities equitably for their costs. However, current efforts to increase dose of dialysis may require higher payments. Longer treatments appear to be the most economical method of increasing the dose of dialysis. Switching to more expensive types of dialysis membranes was a more costly means of increasing dose and hence must be justified by benefits beyond those of higher dose. Reusing membranes saved money, but the savings were insufficient to offset the costs associated with using more expensive membranes. Most, but not all, of the higher costs observed in hospital-based units appear to reflect overhead cost allocation rather than a difference in real resources devoted to treatment. The economies experienced by the largest chains may provide an explanation for their recent growth in market share. The heterogeneity of results by chain size implies that characterizing units using a simple chain status indicator variable is inadequate. Cost differences by facility type and the effects of the ongoing growth of large chains are worthy of continued monitoring to inform both payment policy and antitrust enforcement. (+info)Can restrictions on reimbursement for anti-ulcer drugs decrease Medicaid pharmacy costs without increasing hospitalizations? (2/500)
OBJECTIVE: To examine the impact of a policy restricting reimbursement for Medicaid anti-ulcer drugs on anti-ulcer drug use and peptic-related hospitalizations. DATA SOURCES/STUDY SETTING: In addition to U.S. Census Bureau data, all of the following from Florida: Medicaid anti-ulcer drug claims data, 1989-1993; Medicaid eligibility data, 1989-1993; and acute care nonfederal hospital discharge abstract data (Medicaid and non-Medicaid), 1989-1993. STUDY DESIGN: In this observational study, a Poisson multiple regression model was used to compare changes, after policy implementation, in Medicaid reimbursement for prescription anti-ulcer drugs as well as hospitalization rates between pre- and post-implementation periods in Medicaid versus non-Medicaid patients hospitalized with peptic ulcer disease. PRINCIPAL FINDINGS: Following policy implementation, the rate of Medicaid reimbursement for anti-ulcer drugs decreased 33 percent (p < .001). No associated increase occurred in the rate of Medicaid peptic-related hospitalizations. CONCLUSIONS: Florida's policy restricting Medicaid reimbursement for anti-ulcer drugs was associated with a substantial reduction in outpatient anti-ulcer drug utilization without any significant increase in the rate of hospitalization for peptic-related conditions. (+info)Financial incentives and drug spending in managed care. (3/500)
This study estimates the impact of patient financial incentives on the use and cost of prescription drugs in the context of differing physician payment mechanisms. A large data set was developed that covers persons in managed care who pay varying levels of cost sharing and whose physicians are compensated under two different models: independent practice association (IPA)-model and network-model health maintenance organizations (HMOs). Our results indicate that higher patient copayments for prescription drugs are associated with lower drug spending in IPA models (in which physicians are not at risk for drug costs) but have little effect in network models (in which physicians bear financial risk for all prescribing behavior). (+info)Health insurance in developing countries: lessons from experience. (4/500)
Many developing countries are currently considering the possibility of introducing compulsory health insurance schemes. One reason is to attract more resources to the health sector. If those who, together with their employers, can pay for their health services and are made to do so by insurance, the limited tax funds can be concentrated on providing services for fewer people and thus improve coverage and raise standards. A second reason is dissatisfaction with existing services in which staff motivation is poor, resources are not used to best advantage and patients are not treated with sufficient courtesy and respect. This article describes the historical experience of the developed countries in introducing and steadily expanding the coverage of health insurance, sets out the consensus which has developed about health insurance (at least in Western European countries) and describes the different forms which health insurance can take. The aim is to bring out the advantages and disadvantages of different approaches from this experience, to set out the options for developing countries and to give warnings about the dangers of some approaches. (+info)Prepaid capitation versus fee-for-service reimbursement in a Medicaid population. (5/500)
Utilization of health resources by 37,444 Medicaid recipients enrolled in a capitated health maintenance organization was compared with that of 227,242 Medicaid recipients enrolled in a traditional fee-for-service system over a 1-year period (1983-1984) in the state of Kentucky. Primary care providers in the capitated program had financial incentives to reduce downstream costs like specialist referral, emergency room use, and hospitalizations. The average number of physician visits was similar for both groups (4.47/year in the capitated program; 5.09/year in the fee-for-service system). However, the average number of prescriptions (1.9 versus 4.9 per year), average number of hospital admissions per recipient (0.11 versus 0.22 per year), and average number of hospital days per 1,000 recipients (461 versus 909 per year) were 5% to 60% lower in the capitated group than in the fee-for-service group. The Citicare capitated program resulted in a dramatic reduction in healthcare resource utilization compared with the concurrent fee-for-service system for statewide Medicaid recipients. (+info)Regulating the financial incentives facing physicians in managed care plans. (6/500)
Recent accounts of enrolees in managed care plans being denied access to potentially lifesaving services have heightened public anxiety about the impact of managed care on the accessibility and appropriateness of care, and this anxiety has been translated into legislative action. The present review focuses on an area of managed care operations that has received considerable attention in state legistlatures and in Congress during the past 2 years: the financial relationship between managed care health plans and physicians. Twelve states now mandate that managed care plans disclose information about their financial relationship with physicians, and 11 states regulate the method used by managed care health plans to compensate physicians. Most laws that regulate methods of compensation prohibit health plans from providing physicians an inducement to reduce or limit the delivery of "medically necessary" services. Moreover, in 1996 the Health Care Financing Administration finalized its regulations governing the financial incentives facing physicians in plans that treat Medicaid or Medicare patients, and these regulations went into effect on January 1, 1997. These regulations also are examined in this study. (+info)Behavioral health services: carved out and managed. (7/500)
This article highlights the financial pressures that led to an examination of how mental healthcare was provided and paid for, and discusses the rise, characteristics, and functioning of carved-out behavioral healthcare. The typical characteristics of managed behavioral health carve outs (MBHCOs), including contracts, payment arrangements, provider networks, and data collection are discussed and illustrated using the example of United Behavioral Health. The article details the function of the MBHCO on cost and utilization, access, quality, and the relationship of behavioral health services to general medical care and other human services, but cautions that further research is needed to evaluate the qualitative aspects of care. (+info)Inborn errors of metabolism: medical and administrative "orphans". (8/500)
CONTEXT: Inborn errors of metabolism are genetic conditions that affect the normal biochemical functions of the body in any organ and at any age. More than 500 metabolic diseases are known; almost all are classified as orphan diseases under the US Food and Drug Administration guidelines (incidence < 200,000 persons) and each has its own requirements for diagnosis and treatment. Management of these complex, lifelong, multisystem disorders often requires a coordinated, multidisciplinary approach involving several subspecialists and which may include complex laboratory evaluations, genetic counseling, nutritional therapy, and unusual therapeutic approaches that have been used in only a small number of cases. RESULTS: Not infrequently, inborn errors of metabolism fall outside current standard diagnostic and treatment guidelines of managed care plans. This results in delays in diagnosis and appropriate management, with increased costs to patients and to society. CONCLUSIONS: Patients with inborn errors of metabolism should not be discriminated against and all health plans should specify that access to specialists and metabolic centers are a covered benefit of the plan. The acceptance of treatment guidelines, the development of international disease classification codes for the disorders, and the performance of cost-benefit analyses would all greatly facilitate this process. However, without recognition that these disorders require such services, and steps to provide them by the insurance industry, the care of children with metabolic disorders and other chronic diseases will continue to be a source of frustration and anger among the caregivers and the families they serve. (+info)Reimbursement mechanisms in a medical context refer to the various systems and methods used by health insurance companies, government agencies, or other payers to refund or recompense healthcare providers, institutions, or patients for the costs associated with medical services, treatments, or products. These mechanisms ensure that covered individuals receive necessary medical care while protecting payers from unnecessary expenses.
There are several types of reimbursement mechanisms, including:
1. Fee-for-service (FFS): In this model, healthcare providers are paid for each service or procedure they perform, with the payment typically based on a predetermined fee schedule. This can lead to overutilization and increased costs if providers perform unnecessary services to increase their reimbursement.
2. Capitation: Under capitation, healthcare providers receive a set amount of money per patient enrolled in their care for a specified period, regardless of the number or type of services provided. This encourages providers to manage resources efficiently and focus on preventive care to maintain patients' health and reduce overall costs.
3. Bundled payments: Also known as episode-based payment, this model involves paying a single price for all the services related to a specific medical event, treatment, or condition over a defined period. This encourages coordination among healthcare providers and can help eliminate unnecessary procedures and costs.
4. Resource-Based Relative Value Scale (RBRVS): RBRVS is a payment system that assigns relative value units (RVUs) to various medical services based on factors such as time, skill, and intensity required for the procedure. The RVUs are then converted into a monetary amount using a conversion factor. This system aims to create more equitable and consistent payments across different medical specialties and procedures.
5. Prospective payment systems (PPS): In PPS, healthcare providers receive predetermined fixed payments for specific services or conditions based on established diagnosis-related groups (DRGs) or other criteria. This system encourages efficiency in care delivery and can help control costs by setting limits on reimbursement amounts.
6. Pay-for-performance (P4P): P4P models tie a portion of healthcare providers' reimbursements to their performance on specific quality measures, such as patient satisfaction scores or adherence to evidence-based guidelines. This system aims to incentivize high-quality care and improve overall healthcare outcomes.
7. Shared savings/risk arrangements: In these models, healthcare providers form accountable care organizations (ACOs) or other collaborative entities that assume responsibility for managing the total cost of care for a defined population. If they can deliver care at lower costs while maintaining quality standards, they share in the savings with payers. However, if costs exceed targets, they may be required to absorb some of the financial risk.
These various reimbursement models aim to balance the need for high-quality care with cost control and efficiency in healthcare delivery. By aligning incentives and promoting coordination among providers, these systems can help improve patient outcomes while reducing unnecessary costs and waste in the healthcare system.
Health Insurance Reimbursement refers to the process of receiving payment from a health insurance company for medical expenses that you have already paid out of pocket. Here is a brief medical definition of each term:
1. Insurance: A contract, represented by a policy, in which an individual or entity receives financial protection or reimbursement against losses from an insurance company. The company pools clients' risks to make payments more affordable for the insured.
2. Health: Refers to the state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.
3. Reimbursement: The act of refunding or compensating a person for expenses incurred, especially those that have been previously paid by the individual and are now being paid back by an insurance company.
In the context of health insurance, reimbursement typically occurs when you receive medical care, pay the provider, and then submit a claim to your insurance company for reimbursement. The insurance company will review the claim, determine whether the services are covered under your policy, and calculate the amount they will reimburse you based on your plan's benefits and any applicable co-pays, deductibles, or coinsurance amounts. Once this process is complete, the insurance company will issue a payment to you to cover a portion or all of the costs you incurred for the medical services.
"Reimbursement, Incentive" is not a standard medical term, but I can provide an explanation based on the individual terms:
1. Reimbursement: This refers to the act of paying back or giving compensation for expenses that have already been incurred. In a medical context, this often relates to insurance companies reimbursing patients or healthcare providers for the costs of medical services or supplies after they have been paid.
2. Incentive: An incentive is a motivating factor that encourages someone to do something. In healthcare, incentives can be used to encourage patients to make healthier choices or to participate in certain programs. They can also be used to motivate healthcare providers to follow best practices or to improve the quality of care they provide.
Therefore, "Reimbursement, Incentive" could refer to a payment made after the fact to compensate for expenses incurred, with the added intention of encouraging certain behaviors or actions. For example, an insurance company might offer to reimburse patients for the cost of gym memberships as an incentive to encourage them to exercise regularly.
Diagnosis-Related Groups (DRGs) are a system of classifying hospital patients based on their severity of illness, resource utilization, and other factors. DRGs were developed by the US federal government to determine the relative cost of providing inpatient care for various types of diagnoses and procedures.
The DRG system categorizes patients into one of several hundred groups based on their diagnosis, treatment, and other clinical characteristics. Each DRG has a corresponding payment weight that reflects the average resource utilization and costs associated with caring for patients in that group. Hospitals are then reimbursed for inpatient services based on the DRG payment weights, providing an incentive to provide more efficient and cost-effective care.
DRGs have been widely adopted as a tool for managing healthcare costs and improving quality of care. They are used by Medicare, Medicaid, and many private insurers to determine payments for inpatient hospital services. DRGs can also be used to compare the performance of hospitals and healthcare providers, identify best practices, and support quality improvement initiatives.
Medicare is a social insurance program in the United States, administered by the Centers for Medicare & Medicaid Services (CMS), that provides health insurance coverage to people who are aged 65 and over; or who have certain disabilities; or who have End-Stage Renal Disease (permanent kidney failure requiring dialysis or a transplant).
The program consists of four parts:
1. Hospital Insurance (Part A), which helps pay for inpatient care in hospitals, skilled nursing facilities, hospices, and home health care.
2. Medical Insurance (Part B), which helps pay for doctors' services, outpatient care, medical supplies, and preventive services.
3. Medicare Advantage Plans (Part C), which are private insurance plans that provide all of your Part A and Part B benefits, and may include additional benefits like dental, vision, and hearing coverage.
4. Prescription Drug Coverage (Part D), which helps pay for medications doctors prescribe for treatment.
Medicare is funded by payroll taxes, premiums paid by beneficiaries, and general revenue. Beneficiaries typically pay a monthly premium for Part B and Part D coverage, while Part A is generally free for those who have worked and paid Medicare taxes for at least 40 quarters.
Medicaid is a joint federal-state program that provides health coverage for low-income individuals, including children, pregnant women, elderly adults, and people with disabilities. Eligibility, benefits, and administration vary by state, but the program is designed to ensure that low-income individuals have access to necessary medical services. Medicaid is funded jointly by the federal government and the states, and is administered by the states under broad federal guidelines.
Medicaid programs must cover certain mandatory benefits, such as inpatient and outpatient hospital services, laboratory and X-ray services, and physician services. States also have the option to provide additional benefits, such as dental care, vision services, and prescription drugs. In addition, many states have expanded their Medicaid programs to cover more low-income adults under the Affordable Care Act (ACA).
Medicaid is an important source of health coverage for millions of Americans, providing access to necessary medical care and helping to reduce financial burden for low-income individuals.
I'm sorry for any confusion, but "United States" is a geopolitical entity, specifically the name of the country consisting of 50 states, and it is not a medical term or concept. Therefore, I can't provide a medical definition for it. If you have any questions related to health, medicine, or biology, I would be happy to try to help answer those!
Cost control in a medical context refers to the strategies and practices employed by healthcare organizations to manage and reduce the costs associated with providing patient care while maintaining quality and safety. The goal is to optimize resource allocation, increase efficiency, and contain expenses without compromising the standard of care. This may involve measures such as:
1. Utilization management: Reviewing and monitoring the use of medical services, tests, and treatments to ensure they are necessary, appropriate, and evidence-based.
2. Case management: Coordinating patient care across various healthcare providers and settings to improve outcomes, reduce unnecessary duplication of services, and control costs.
3. Negotiating contracts with suppliers and vendors to secure favorable pricing for medical equipment, supplies, and pharmaceuticals.
4. Implementing evidence-based clinical guidelines and pathways to standardize care processes and reduce unwarranted variations in practice that can drive up costs.
5. Using technology such as electronic health records (EHRs) and telemedicine to streamline operations, improve communication, and reduce errors.
6. Investing in preventive care and wellness programs to keep patients healthy and reduce the need for costly interventions and hospitalizations.
7. Continuously monitoring and analyzing cost data to identify trends, opportunities for improvement, and areas of potential waste or inefficiency.
Cost allocation is the process of distributing or assigning costs to different departments, projects, products, or services within an organization. The goal of cost allocation is to more accurately determine the true cost of producing a product or providing a service, taking into account all related expenses. This can help organizations make better decisions about pricing, resource allocation, and profitability analysis.
There are various methods for allocating costs, including activity-based costing (ABC), which assigns costs based on the activities required to produce a product or provide a service; traditional costing, which uses broad categories such as direct labor, direct materials, and overhead; and causal allocation, which assigns costs based on a specific cause-and-effect relationship.
In healthcare, cost allocation is particularly important for determining the true cost of patient care, including both direct and indirect costs. This can help hospitals and other healthcare organizations make informed decisions about resource allocation, pricing, and reimbursement strategies.
Hospitalization Insurance is a type of health insurance that provides coverage for the expenses incurred during a hospital stay, including surgery, diagnostic tests, doctor's visits, and other related services. This type of insurance may also cover the cost of hospital room and board, intensive care unit (ICU) stays, and nursing services. Some policies may also provide coverage for ambulance transportation, home health care, and rehabilitation services following a hospital stay. The specific benefits and coverage limits will vary depending on the policy and insurance provider.
Costs refer to the total amount of resources, such as money, time, and labor, that are expended in the provision of a medical service or treatment. Costs can be categorized into direct costs, which include expenses directly related to patient care, such as medication, supplies, and personnel; and indirect costs, which include overhead expenses, such as rent, utilities, and administrative salaries.
Cost analysis is the process of estimating and evaluating the total cost of a medical service or treatment. This involves identifying and quantifying all direct and indirect costs associated with the provision of care, and analyzing how these costs may vary based on factors such as patient volume, resource utilization, and reimbursement rates.
Cost analysis is an important tool for healthcare organizations to understand the financial implications of their operations and make informed decisions about resource allocation, pricing strategies, and quality improvement initiatives. It can also help policymakers and payers evaluate the cost-effectiveness of different treatment options and develop evidence-based guidelines for clinical practice.
A capitation fee is a payment model in healthcare systems where physicians or other healthcare providers receive a set amount of money per patient assigned to their care, per period of time, whether or not that patient seeks care. This fee is intended to cover all the necessary medical services for that patient during that time frame. It is a type of risk-based payment model that encourages providers to manage resources efficiently and provide appropriate care to keep patients healthy and avoid unnecessary procedures or hospitalizations. The amount of the capitation fee can vary based on factors such as the patient's age, health status, and any specific healthcare needs they may have.
Hospital economics refers to the study and application of economic principles and concepts in the management and operation of hospitals and healthcare organizations. This field examines issues such as cost containment, resource allocation, financial management, reimbursement systems, and strategic planning. The goal of hospital economics is to improve the efficiency and effectiveness of hospital operations while maintaining high-quality patient care. It involves understanding and analyzing various economic factors that affect hospitals, including government regulations, market forces, technological advancements, and societal values. Hospital economists may work in a variety of settings, including hospitals, consulting firms, academic institutions, and government agencies.
Health care costs refer to the expenses incurred for medical services, treatments, procedures, and products that are used to maintain or restore an individual's health. These costs can be categorized into several types:
1. Direct costs: These include payments made for doctor visits, hospital stays, medications, diagnostic tests, surgeries, and other medical treatments and services. Direct costs can be further divided into two subcategories:
* Out-of-pocket costs: Expenses paid directly by patients, such as co-payments, deductibles, coinsurance, and any uncovered medical services or products.
* Third-party payer costs: Expenses covered by insurance companies, government programs (like Medicare, Medicaid), or other entities that pay for health care services on behalf of patients.
2. Indirect costs: These are the expenses incurred as a result of illness or injury that indirectly impact an individual's ability to work and earn a living. Examples include lost productivity, absenteeism, reduced earning capacity, and disability benefits.
3. Non-medical costs: These are expenses related to caregiving, transportation, home modifications, assistive devices, and other non-medical services required for managing health conditions or disabilities.
Health care costs can vary significantly depending on factors such as the type of medical service, geographic location, insurance coverage, and individual health status. Understanding these costs is essential for patients, healthcare providers, policymakers, and researchers to make informed decisions about treatment options, resource allocation, and health system design.
A Prospective Payment System (PPS) is a method of reimbursement in which the payment for a specific service is determined before the service is provided. It is commonly used in healthcare systems, including hospitals and post-acute care facilities, to control costs and promote efficiency. Under this system, providers are paid a predetermined amount based on the patient's diagnosis or the type of procedure being performed, rather than being reimbursed for each individual service provided. This encourages providers to deliver care in the most cost-effective manner possible while still meeting quality standards. The Centers for Medicare and Medicaid Services (CMS) uses PPS for many of its payment models, including the Inpatient Prospective Payment System (IPPS) and the Outpatient Prospective Payment System (OPPS).
"Drug costs" refer to the amount of money that must be paid to acquire and use a particular medication. These costs can include the following:
1. The actual purchase price of the drug, which may vary depending on factors such as the dosage form, strength, and quantity of the medication, as well as whether it is obtained through a retail pharmacy, mail-order service, or other distribution channel.
2. Any additional fees or charges associated with obtaining the drug, such as shipping and handling costs, insurance copayments or coinsurance amounts, and deductibles.
3. The cost of any necessary medical services or supplies that are required to administer the drug, such as syringes, needles, or alcohol swabs for injectable medications, or nebulizers for inhaled drugs.
4. The cost of monitoring and managing any potential side effects or complications associated with the use of the drug, which may include additional medical appointments, laboratory tests, or other diagnostic procedures.
It is important to note that drug costs can vary widely depending on a variety of factors, including the patient's insurance coverage, the pharmacy where the drug is obtained, and any discounts or rebates that may be available. Patients are encouraged to shop around for the best prices and to explore all available options for reducing their out-of-pocket costs, such as using generic medications or participating in manufacturer savings programs.
Group purchasing in a healthcare context refers to the practice where multiple healthcare organizations, such as hospitals or clinics, join together to negotiate and purchase medical supplies, pharmaceuticals, and other goods or services from vendors at a reduced price. By pooling their resources and purchasing power, these organizations can secure better pricing, terms, and contractual agreements than they might be able to obtain individually. This collaborative approach can help healthcare organizations reduce costs, improve operational efficiency, and ensure access to high-quality products and services.
Medical fees are the charges for services provided by medical professionals and healthcare facilities. These fees can vary widely depending on the type of service, the provider, and the geographic location. They may include charges for office visits, procedures, surgeries, hospital stays, diagnostic tests, and prescribed medications. In some cases, medical fees may be covered in part or in full by health insurance, but in other cases patients may be responsible for paying these fees out of pocket. It is important for patients to understand the fees associated with their medical care and to ask questions about any charges that they do not understand.
Current Procedural Terminology (CPT) is a system of medical codes, developed and maintained by the American Medical Association (AMA), that are used to describe medical, surgical, and diagnostic services provided by healthcare professionals. The codes are used for administrative purposes, such as billing and insurance claims processing, and consist of a five-digit alphanumeric code that identifies the specific service or procedure performed.
The CPT code set is organized into three categories: Category I codes describe common medical, surgical, and diagnostic services; Category II codes are used for performance measurement and tracking of quality improvement initiatives; and Category III codes are used for emerging technologies, experimental procedures, and services that do not have a defined CPT code.
Healthcare professionals and facilities rely on the accuracy and specificity of CPT codes to ensure appropriate reimbursement for their services. The AMA regularly updates the CPT code set to reflect changes in medical practice and technology, and provides guidance and resources to help healthcare professionals navigate the complexities of coding and billing.
Fee-for-service (FFS) plans are a type of medical reimbursement model in which healthcare providers are paid for each specific service or procedure they perform. In this system, the patient or their insurance company is charged separately for each appointment, test, or treatment, and the provider receives payment based on the number and type of services delivered.
FFS plans can be either traditional fee-for-service or modified fee-for-service. Traditional FFS plans offer providers more autonomy in setting their fees but may lead to higher healthcare costs due to potential overutilization of services. Modified FFS plans, on the other hand, involve pre-negotiated rates between insurance companies and healthcare providers, aiming to control costs while still allowing providers to be compensated for each service they deliver.
It is important to note that FFS plans can sometimes create financial incentives for healthcare providers to perform more tests or procedures than necessary, potentially leading to increased healthcare costs and potential overtreatment. As a result, alternative payment models like capitation, bundled payments, and value-based care have emerged as alternatives to address these concerns.
"Rate setting and review" is not a commonly used medical term with a specific definition in the field. However, I can provide you with information about what these terms might refer to in a broader healthcare context:
Rate setting generally refers to the process of determining the payment rates for healthcare services, programs, or products. This could involve setting reimbursement rates for medical procedures, medications, or durable medical equipment under government-funded health insurance programs like Medicare and Medicaid, or in the private insurance sector. Rate setting can be influenced by various factors, including the cost of providing care, resource utilization, quality metrics, and market competition.
Review, in this context, typically refers to the process of evaluating and assessing healthcare services, programs, or products to ensure their quality, effectiveness, and efficiency. This could involve reviewing medical records, clinical outcomes, and financial data to determine if the care provided is consistent with evidence-based guidelines, industry best practices, and regulatory requirements. Regular reviews are essential for maintaining high standards of care, identifying areas for improvement, and ensuring that resources are allocated efficiently.
Together, "rate setting and review" may refer to a comprehensive approach to managing healthcare costs and quality by establishing appropriate payment rates while continuously monitoring and improving the effectiveness and efficiency of healthcare services.
Cost-benefit analysis (CBA) is a systematic process used to compare the costs and benefits of different options to determine which one provides the greatest net benefit. In a medical context, CBA can be used to evaluate the value of medical interventions, treatments, or policies by estimating and monetizing all the relevant costs and benefits associated with each option.
The costs included in a CBA may include direct costs such as the cost of the intervention or treatment itself, as well as indirect costs such as lost productivity or time away from work. Benefits may include improved health outcomes, reduced morbidity or mortality, and increased quality of life.
Once all the relevant costs and benefits have been identified and quantified, they are typically expressed in monetary terms to allow for a direct comparison. The option with the highest net benefit (i.e., the difference between total benefits and total costs) is considered the most cost-effective.
It's important to note that CBA has some limitations and can be subject to various biases and assumptions, so it should be used in conjunction with other evaluation methods to ensure a comprehensive understanding of the value of medical interventions or policies.
In the context of medical billing and healthcare, remuneration refers to the payment or compensation received by healthcare professionals or facilities for the medical services or treatments provided to patients. This can include fees for office visits, procedures, surgeries, hospital stays, and other healthcare-related services. Remuneration can come from various sources such as insurance companies, government programs like Medicare and Medicaid, and out-of-pocket payments from patients. It is important to note that the rules and regulations regarding remuneration in healthcare are subject to strict compliance requirements to prevent fraud, abuse, and conflicts of interest.
Pharmaceutical services insurance refers to a type of coverage that helps individuals and families pay for their prescription medications. This type of insurance is often offered as part of a larger health insurance plan, but can also be purchased as a standalone policy.
The specifics of pharmaceutical services insurance coverage can vary widely depending on the policy. Some plans may cover only generic medications, while others may cover both brand-name and generic drugs. Additionally, some policies may require individuals to pay a portion of the cost of their prescriptions in the form of copays or coinsurance, while others may cover the full cost of medications.
Pharmaceutical services insurance can be especially important for individuals who have chronic medical conditions that require ongoing treatment with expensive prescription medications. By helping to offset the cost of these medications, pharmaceutical services insurance can make it easier for people to afford the care they need to manage their health and improve their quality of life.
Hospital costs are the total amount of money that is expended by a hospital to provide medical and healthcare services to patients. These costs can include expenses related to:
* Hospital staff salaries and benefits
* Supplies, such as medications, medical devices, and surgical equipment
* Utilities, such as electricity, water, and heating
* Facility maintenance and renovation
* Equipment maintenance and purchase
* Administrative costs, such as billing and insurance processing
Hospital costs can also be classified into fixed and variable costs. Fixed costs are those that do not change with the volume of services provided, such as rent or depreciation of equipment. Variable costs are those that change with the volume of services provided, such as supplies and medications.
It's important to note that hospital costs can vary widely depending on factors such as the complexity of care provided, the geographic location of the hospital, and the patient population served. Additionally, hospital costs may not always align with charges or payments for healthcare services, which can be influenced by factors such as negotiated rates with insurance companies and government reimbursement policies.
Health expenditures refer to the total amount of money spent on health services, goods, and resources in a given period. This can include expenses for preventive care, medical treatments, medications, long-term care, and administrative costs. Health expenditures can be made by individuals, corporations, insurance companies, or governments, and they can be measured at the national, regional, or household level.
Health expenditures are often used as an indicator of a country's investment in its healthcare system and can reflect the overall health status of a population. High levels of health expenditures may indicate a strong commitment to healthcare, but they can also place a significant burden on individuals, businesses, and governments. Understanding patterns and trends in health expenditures is important for policymakers, healthcare providers, and researchers who are working to improve the efficiency, effectiveness, and accessibility of healthcare services.
Medical practice management refers to the administrative and operational aspects of running a healthcare organization or medical practice. It involves overseeing and coordinating various business functions such as finance, human resources, marketing, patient scheduling, billing and coding, compliance with regulations, and information technology systems. The goal of medical practice management is to ensure that the practice runs efficiently, effectively, and profitably while delivering high-quality care to patients.
Medical practice managers may be responsible for developing policies and procedures, hiring and training staff, managing patient flow, ensuring regulatory compliance, implementing quality improvement initiatives, and overseeing financial performance. They must have a strong understanding of medical billing and coding practices, healthcare regulations, and electronic health record (EHR) systems. Effective communication skills, leadership abilities, and attention to detail are also important qualities for successful medical practice managers.
A fee schedule in a medical context refers to a list of fees that healthcare providers charge for various procedures, services, or treatments. It is essentially a price list that outlines the cost of each service offered by the healthcare provider. Fee schedules can be established by individual practitioners, hospitals, clinics, or insurance networks and may vary based on factors such as location, specialty, and complexity of the procedure.
In some cases, fee schedules are negotiated between healthcare providers and insurance companies to determine the allowed amount for reimbursement. This helps ensure that patients receive consistent and predictable pricing for medical services while also allowing healthcare providers to maintain a sustainable practice. Additionally, fee schedules can help patients understand their financial responsibilities before undergoing medical procedures or treatments.
Fees and charges in a medical context refer to the costs that patients are required to pay for healthcare services, treatments, or procedures. These may include:
1. Professional fees: The amount charged by healthcare professionals such as doctors, nurses, or therapists for their time, expertise, and services provided during consultations, examinations, or treatments.
2. Hospital charges: The costs associated with a patient's hospital stay, including room and board, nursing care, medications, and diagnostic tests.
3. Facility fees: Additional charges levied by hospitals, clinics, or ambulatory surgery centers to cover the overhead expenses of maintaining the facility and its equipment.
4. Procedure or treatment-specific fees: Costs directly related to specific medical procedures, surgeries, or treatments, such as anesthesia, radiology services, laboratory tests, or surgical supplies.
5. Ancillary fees: Additional costs for items like crutches, slings, or durable medical equipment that patients may need during their recovery process.
6. Insurance copayments, coinsurance, and deductibles: The portion of healthcare expenses that patients are responsible for paying based on their insurance policy terms.
It is essential for patients to understand the fees and charges associated with their medical care to make informed decisions about their treatment options and manage their healthcare costs effectively.
Cost savings in a medical context generally refers to the reduction in expenses or resources expended in the delivery of healthcare services, treatments, or procedures. This can be achieved through various means such as implementing more efficient processes, utilizing less expensive treatment options when appropriate, preventing complications or readmissions, and negotiating better prices for drugs or supplies.
Cost savings can also result from comparative effectiveness research, which compares the relative benefits and harms of different medical interventions to help doctors and patients make informed decisions about which treatment is most appropriate and cost-effective for a given condition.
Ultimately, cost savings in healthcare aim to improve the overall value of care delivered by reducing unnecessary expenses while maintaining or improving quality outcomes for patients.
Pharmaceutical economics is a branch of economics that focuses on the production and distribution of pharmaceutical products and services. It involves the analysis of various factors that influence the development, pricing, and accessibility of medications, including issues related to healthcare policy, regulation, reimbursement, and market competition.
Pharmaceutical economists study topics such as:
1. The research and development (R&D) process for new drugs, including the costs, risks, and uncertainties associated with bringing a new drug to market.
2. The pricing of pharmaceuticals, taking into account factors such as production costs, R&D expenses, market competition, and the value that medications provide to patients and society.
3. The impact of government regulations and policies on the pharmaceutical industry, including issues related to intellectual property protection, drug safety, and efficacy testing.
4. The role of health insurance and other third-party payers in shaping the demand for and access to pharmaceuticals.
5. The evaluation of pharmaceutical interventions' cost-effectiveness and their impact on healthcare outcomes and patient well-being.
6. The analysis of market structures, competitive dynamics, and strategic decision-making within the pharmaceutical industry.
7. The assessment of globalization, international trade, and cross-border collaboration in the pharmaceutical sector.
Pharmaceutical economics plays a crucial role in informing healthcare policy decisions, improving patient access to essential medications, and promoting sustainable and innovative practices within the pharmaceutical industry.
Skilled Nursing Facilities (SNFs) are healthcare facilities that provide round-the-clock skilled nursing care and medical supervision to individuals who require rehabilitation or long-term care. These facilities are designed for patients who need more medical attention and assistance with activities of daily living than can be provided at home or in an assisted living facility.
SNFs offer a wide range of services, including:
1. Skilled nursing care: Registered nurses (RNs) and licensed practical nurses (LPNs) provide 24-hour medical care and monitoring for patients with complex medical needs.
2. Rehabilitation services: Physical, occupational, and speech therapists work with patients to help them regain strength, mobility, and communication skills after an illness, injury, or surgery.
3. Medical management: SNFs have a team of healthcare professionals, such as physicians, nurse practitioners, and pharmacists, who collaborate to manage each patient's medical needs and develop individualized care plans.
4. Nutritional support: Registered dietitians assess patients' nutritional needs and provide specialized diets and feeding assistance when necessary.
5. Social services: Case managers and social workers help patients and their families navigate the healthcare system, coordinate discharge planning, and connect them with community resources.
6. Personal care: Certified nursing assistants (CNAs) provide assistance with activities of daily living, such as bathing, dressing, grooming, and using the bathroom.
7. Therapeutic recreation: Recreational therapists offer activities designed to improve patients' physical, cognitive, and emotional well-being.
SNFs may be standalone facilities or part of a larger healthcare system, such as a hospital or continuing care retirement community (CCRC). To qualify for Medicare coverage in an SNF, individuals must have a qualifying hospital stay of at least three days and need skilled nursing or rehabilitation services. Medicaid and private insurance may also cover the cost of care in Skilled Nursing Facilities.
Financial management in a hospital setting refers to the planning, organizing, directing, and controlling of financial resources in order to achieve the hospital's mission, vision, and strategic objectives. This includes developing financial strategies, preparing budget plans, managing revenue cycles, controlling costs, ensuring compliance with financial regulations, and making informed decisions about resource allocation. Effective financial management is critical for the sustainability and growth of hospitals, as it enables them to provide high-quality patient care while maintaining fiscal responsibility.
Medicare Part B is the component of Medicare, a federal health insurance program in the United States, that covers medically necessary outpatient services and preventive services. These services include doctor visits, laboratory tests, diagnostic imaging, durable medical equipment, mental health services, ambulance services, and some home health care services.
Medicare Part B also covers certain preventive services such as cancer screenings, vaccinations, and wellness visits to help maintain an individual's health and prevent illnesses or diseases from getting worse. It is financed through a combination of monthly premiums paid by enrollees and funds from the federal government's general revenue. Enrollment in Medicare Part B is voluntary, but there are penalties for not enrolling when first eligible, unless an individual has creditable coverage from another source.
Pharmaceutical fees are charges that healthcare professionals or institutions may impose on patients for various services related to the prescribing and dispensing of medications. These fees can include costs associated with medication therapy management, drug monitoring, medication reconciliation, and other clinical services provided by pharmacists or other healthcare providers.
It's important to note that these fees are separate from the cost of the medication itself and may not be covered by insurance. Patients should always ask about any potential fees before receiving pharmaceutical services and clarify whether they will be responsible for paying them out-of-pocket.
Medicare Part A is the hospital insurance component of Medicare, which is a federal health insurance program in the United States. Specifically, Part A helps cover the costs associated with inpatient care in hospitals, skilled nursing facilities, and some types of home health care. This can include things like semi-private rooms, meals, nursing services, and any other necessary hospital services and supplies.
Part A coverage also extends to hospice care for individuals who are terminally ill and have a life expectancy of six months or less. In this case, Part A helps cover the costs associated with hospice care, including pain management, symptom control, and emotional and spiritual support for both the patient and their family.
It's important to note that Medicare Part A is not completely free, as most people do not pay a monthly premium for this coverage. However, there are deductibles and coinsurance costs associated with using Part A services, which can vary depending on the specific service being provided.
Physician's practice patterns refer to the individual habits and preferences of healthcare providers when it comes to making clinical decisions and managing patient care. These patterns can encompass various aspects, such as:
1. Diagnostic testing: The types and frequency of diagnostic tests ordered for patients with similar conditions.
2. Treatment modalities: The choice of treatment options, including medications, procedures, or referrals to specialists.
3. Patient communication: The way physicians communicate with their patients, including the amount and type of information shared, as well as the level of patient involvement in decision-making.
4. Follow-up care: The frequency and duration of follow-up appointments, as well as the monitoring of treatment effectiveness and potential side effects.
5. Resource utilization: The use of healthcare resources, such as hospitalizations, imaging studies, or specialist consultations, and the associated costs.
Physician practice patterns can be influenced by various factors, including medical training, clinical experience, personal beliefs, guidelines, and local availability of resources. Understanding these patterns is essential for evaluating the quality of care, identifying potential variations in care, and implementing strategies to improve patient outcomes and reduce healthcare costs.
Managed care programs are a type of health insurance plan that aims to control healthcare costs and improve the quality of care by managing the utilization of healthcare services. They do this by using a network of healthcare providers who have agreed to provide services at reduced rates, and by implementing various strategies such as utilization review, case management, and preventive care.
In managed care programs, there is usually a primary care physician (PCP) who acts as the patient's main doctor and coordinates their care within the network of providers. Patients may need a referral from their PCP to see specialists or access certain services. Managed care programs can take various forms, including Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), Point-of-Service (POS) plans, and Exclusive Provider Organizations (EPOs).
The goal of managed care programs is to provide cost-effective healthcare services while maintaining or improving the quality of care. They can help patients save money on healthcare costs by providing coverage for a range of services at lower rates than traditional fee-for-service plans, but they may also limit patient choice and require prior authorization for certain procedures or treatments.
Health policy refers to a set of decisions, plans, and actions that are undertaken to achieve specific healthcare goals within a population. It is formulated by governmental and non-governmental organizations with the objective of providing guidance and direction for the management and delivery of healthcare services. Health policies address various aspects of healthcare, including access, financing, quality, and equity. They can be designed to promote health, prevent disease, and provide treatment and rehabilitation services to individuals who are sick or injured. Effective health policies require careful consideration of scientific evidence, ethical principles, and societal values to ensure that they meet the needs of the population while being fiscally responsible.
Uncompensated care refers to healthcare services provided by hospitals or other healthcare providers that are not paid for by the patient or by third-party payers such as insurance companies. This can include both charity care, where services are provided for free or at reduced costs to patients who cannot afford to pay, and bad debt, where services are provided but remain unpaid because the patient is unable or unwilling to pay their bills. Uncompensated care is a significant issue for many hospitals, particularly those that serve large numbers of low-income or uninsured patients, as it can result in significant financial losses for the institution.
A nursing home, also known as a skilled nursing facility, is a type of residential healthcare facility that provides round-the-clock care and assistance to individuals who require a high level of medical care and support with activities of daily living. Nursing homes are designed for people who cannot be cared for at home or in an assisted living facility due to their complex medical needs, mobility limitations, or cognitive impairments.
Nursing homes provide a range of services, including:
1. Skilled nursing care: Registered nurses and licensed practical nurses provide 24-hour medical care and monitoring for residents with chronic illnesses, disabilities, or those recovering from surgery or illness.
2. Rehabilitation services: Physical, occupational, and speech therapists help residents regain strength, mobility, and communication skills after an injury, illness, or surgery.
3. Personal care: Certified nursing assistants (CNAs) help residents with activities of daily living, such as bathing, dressing, grooming, and using the bathroom.
4. Meals and nutrition: Nursing homes provide three meals a day, plus snacks, and accommodate special dietary needs.
5. Social activities: Recreational programs and social events are organized to help residents stay active and engaged with their peers.
6. Hospice care: Some nursing homes offer end-of-life care for residents who require palliative or comfort measures.
7. Secure environments: For residents with memory impairments, specialized units called memory care or Alzheimer's units provide a secure and structured environment to help maintain their safety and well-being.
When selecting a nursing home, it is essential to consider factors such as the quality of care, staff-to-resident ratio, cleanliness, and overall atmosphere to ensure the best possible experience for the resident.
Medical Laboratory Science, also known as Clinical Laboratory Science, is a healthcare profession that involves the performance and interpretation of laboratory tests to detect, diagnose, monitor, and treat diseases. Medical Laboratory Scientists (MLS) work in various settings such as hospitals, clinics, research institutions, and diagnostic laboratories. They analyze body fluids, tissues, and cells using sophisticated instruments and techniques to provide accurate and timely results that aid in the clinical decision-making process.
MLS professionals perform a range of laboratory tests including hematology, clinical chemistry, microbiology, immunology, molecular biology, urinalysis, and blood banking. They follow standardized procedures and quality control measures to ensure the accuracy and reliability of test results. MLS professionals also evaluate complex data, correlate test findings with clinical symptoms, and communicate their findings to healthcare providers.
MLS education typically requires a bachelor's degree in Medical Laboratory Science or a related field, followed by a clinical internship or residency program. Many MLS professionals are certified or licensed by professional organizations such as the American Society for Clinical Pathology (ASCP) and the National Accrediting Agency for Clinical Laboratory Sciences (NAACLS).
An "Orphan Drug" is a pharmaceutical agent that is developed to treat a rare medical condition, disorder, or disease that affects a small number of people in comparison to other conditions. In the United States, this is defined as a condition or disease that affects fewer than 200,000 people nationwide. Due to the limited market for these drugs, pharmaceutical companies are often reluctant to invest in their development and production.
"Orphan Drug Production," therefore, refers to the manufacturing process of these rare disease treatments. To encourage the development and production of orphan drugs, governments and regulatory agencies offer incentives such as tax credits, grants, and exclusive marketing rights for a certain period of time. These measures help offset the higher costs and lower profit margins associated with developing and producing orphan drugs, ultimately benefiting patients with rare diseases who often have few or no treatment options available to them.
A formulary is a list of prescription drugs, both generic and brand-name, that are approved for use in a specific health plan or healthcare system. The formulary includes information on the preferred drugs within each therapeutic class, along with any restrictions or limitations on their use. Formularies are developed and maintained by a committee of healthcare professionals, including pharmacists and physicians, who evaluate the safety, efficacy, and cost-effectiveness of different medications.
The purpose of a formulary is to promote the appropriate use of medications, improve patient outcomes, and manage healthcare costs. By establishing a preferred list of drugs, health plans and healthcare systems can negotiate better prices with pharmaceutical manufacturers and ensure that patients receive high-quality, evidence-based care.
Formularies may include various types of medications, such as oral solid dosage forms, injectables, inhalants, topicals, and others. They are typically organized by therapeutic class, and each drug is assigned a tier based on its cost and clinical value. Tier 1 drugs are usually preferred generics or lower-cost brand-name medications, while Tier 2 drugs may be higher-cost brand-name medications that have no generic equivalent. Tier 3 drugs are typically specialty medications that are used to treat complex or rare conditions and are often associated with high costs.
Healthcare providers are encouraged to prescribe drugs that are listed on the formulary, as these medications have been thoroughly reviewed and deemed safe and effective for use in their patient population. However, there may be situations where a non-formulary medication is necessary to treat a particular patient's condition. In such cases, healthcare providers can request an exception or prior authorization to prescribe the non-formulary drug.
Formularies are regularly updated to reflect new drugs that come on the market, changes in clinical guidelines, and shifts in the therapeutic landscape. Health plans and healthcare systems may also modify their formularies in response to feedback from patients and providers or to address concerns about safety, efficacy, or cost.
In summary, a formulary is a comprehensive list of prescription drugs that are approved for use in a specific health plan or healthcare system. Formularies promote the appropriate use of medications, improve patient outcomes, and manage costs by encouraging the prescribing of safe and effective drugs that have been thoroughly reviewed and deemed appropriate for their patient population.
"State Health Plans" is a general term that refers to the healthcare coverage programs offered or managed by individual states in the United States. These plans can be divided into two main categories: Medicaid and state-based marketplaces.
1. **Medicaid**: This is a joint federal-state program that provides healthcare coverage to low-income individuals, families, and qualifying groups, such as pregnant women, children, elderly people, and people with disabilities. Each state administers its own Medicaid program within broad federal guidelines, and therefore, the benefits, eligibility criteria, and enrollment processes can vary from state to state.
2. **State-based Marketplaces (SBMs)**: These are online platforms where individuals and small businesses can compare and purchase health insurance plans that meet the standards set by the Affordable Care Act (ACA). SBMs operate in accordance with federal regulations, but individual states have the flexibility to design their own marketplace structure, manage their own enrollment process, and determine which insurers can participate.
It is important to note that state health plans are subject to change based on federal and state laws, regulations, and funding allocations. Therefore, it is always recommended to check the most recent and specific information from the relevant state agency or department.
I'm sorry for any confusion, but "inventions" is not a term that has a medical definition. An invention is a unique or novel device, method, composition, or process that is created by someone, typically through significant creativity and innovation. It may be a product or a procedure that is newly designed or constructed, or it may be a new use for an existing product or process.
If you have any questions related to healthcare, medicine, or biology, I would be happy to try to help answer them!
In medical terms, "private practice" refers to the provision of healthcare services by a licensed and trained medical professional (such as a doctor, nurse practitioner, or dentist) who operates independently and is not employed by a hospital, clinic, or other health care institution. In private practice, these professionals offer their medical expertise and treatments directly to patients on a fee-for-service basis or through insurance billing. They are responsible for managing their own schedules, appointments, staff, and finances while maintaining compliance with relevant laws, regulations, and professional standards.
Private practices can vary in size and structure, ranging from solo practitioners working alone to larger group practices with multiple healthcare providers sharing resources and expertise. The primary advantage of private practice is the autonomy it provides for medical professionals to make decisions regarding patient care, treatment options, and business management without interference from external entities.
Physician services insurance refers to a type of health insurance coverage that helps pay for medically necessary services provided by licensed physicians. This can include office visits, hospital care, diagnostic tests, and treatments for injuries and illnesses. The specific services covered and the amount reimbursed will depend on the terms of the individual's insurance policy. Some policies may also have restrictions on which providers are considered in-network and covered under the plan. It is important to understand the details of one's coverage to know what is included and what out-of-pocket costs may be required.
 Healthcare payment
Healthcare payment
Special education in the United States
Federal political financing in Canada
Acquisition and Cross-Servicing Agreement
Health insurance coverage in the United States
Healthcare in the United States
Medicine in China
Rural health clinic
Mahiben Maruthappu
2020 in the Philippines
CARES Act
List of MeSH codes (N03)
Social franchising
Center for Medicare and Medicaid Innovation
Polish Film Institute
Asoke Kumar Mukerji
Tim Pawlenty
Massification
Impact attenuator
Kobi Peleg
Frederick Holbrook
Menno Snel
List of countries with universal health care
Piwniczna-Zdrój
Trans-Pacific Partnership
United States Congressional Joint Select Committee on Deficit Reduction
Market access
Ahmed Laaouej
Bus transport in the United Kingdom
Lift chair
 Reimbursement & financial mechanisms in digital health. What do the probable futures look like? | ECHAlliance
Reimbursement & financial mechanisms in digital health. What do the probable futures look like? | ECHAlliance
 Subjects: Reimbursement Mechanisms -- economics - Digital Collections - National Library of Medicine Search Results
Subjects: Reimbursement Mechanisms -- economics - Digital Collections - National Library of Medicine Search Results
 Reimbursement & financial mechanisms in digital health. What do the probable futures look like?
Reimbursement & financial mechanisms in digital health. What do the probable futures look like?
 Perceived, actual, and desired knowledge regarding Medicare billing and reimbursement. A national needs assessment survey of...
Perceived, actual, and desired knowledge regarding Medicare billing and reimbursement. A national needs assessment survey of...
Effective financing of maternal health services: a review of the literature
 Estimating Contraceptive Needs and Increasing Access to Contraception in Response to the Zika Virus Disease Outbreak - Puerto...
Estimating Contraceptive Needs and Increasing Access to Contraception in Response to the Zika Virus Disease Outbreak - Puerto...
 Telepractice
Telepractice
 Incentivizing Innovation to Tackle Antimicrobial Resistance | BCG
Incentivizing Innovation to Tackle Antimicrobial Resistance | BCG
A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States:...
 Tax Reimbursement Clauses: What They Are And Why You Need To Know
Tax Reimbursement Clauses: What They Are And Why You Need To Know
 Payment by results suspended | News | Health Service Journal
Payment by results suspended | News | Health Service Journal
 Author Page for Robert Zeithammer :: SSRN
Author Page for Robert Zeithammer :: SSRN
Progress in Public Health Genomics Depends on Measuring Population Level Outcomes | Blogs | CDC
 2017 News
2017 News
 Analysis of Bundled Payment | RAND
Analysis of Bundled Payment | RAND
 FDA Issues New Rules and Clarifies Its Policies on Charging for Investigational Drugs | Insights | Ropes & Gray LLP
FDA Issues New Rules and Clarifies Its Policies on Charging for Investigational Drugs | Insights | Ropes & Gray LLP
Chronic disease excellence: "Service line 2.0" for health systems? | McKinsey
 Cardiovascular Information System Market to Witness Vigorous Expansion by 2024 | Key Players: Philips Healthcare, GE Healthcare...
Cardiovascular Information System Market to Witness Vigorous Expansion by 2024 | Key Players: Philips Healthcare, GE Healthcare...
Healthcare payment - Wikipedia
 Wide variation in payments for Medicare beneficiary oncology services suggests room for practice-level improvement.
Wide variation in payments for Medicare beneficiary oncology services suggests room for practice-level improvement.
 Opportunities and Challenges in China's Reimbursement Landscape | Simon-Kucher
Opportunities and Challenges in China's Reimbursement Landscape | Simon-Kucher
 EULAR evidence-based recommendations for the management of fibromyalgia syndrome | Annals of the Rheumatic Diseases
EULAR evidence-based recommendations for the management of fibromyalgia syndrome | Annals of the Rheumatic Diseases
 Frontiers | Editorial: Digital health adoption: Looking beyond the role of technology
Frontiers | Editorial: Digital health adoption: Looking beyond the role of technology
 School-Based Medicaid Program (SBMP) | Mass.gov
School-Based Medicaid Program (SBMP) | Mass.gov
 Charter Statement - Bill C-76: An Act to amend the Canada Elections Act and other Acts and to make certain consequential...
Charter Statement - Bill C-76: An Act to amend the Canada Elections Act and other Acts and to make certain consequential...
 Medicines Pricing and Reimbursement: Demonstrating Value and Sharing Risk in the EU and United States - Events
Medicines Pricing and Reimbursement: Demonstrating Value and Sharing Risk in the EU and United States - Events
Improving Language Equity in Hospitalized Children of Families With LEP: Challenges and Solutions | Hospital Pediatrics |...
Seek reimbursement3
- Local Education Agencies (LEAs), such as municipal (cities and towns) school districts, regional school districts, regional vocational/technical schools, or public charter schools, may seek reimbursement for Medicaid-covered services and associated administrative expenses. (mass.gov)
- This resource, and other supporting materials, outlines how employers can implement billing and reimbursement practices for ATs who deliver physical medicine and rehabilitation services and desire to seek reimbursement from an insurer for selected services, said Joe Greene, MS, ATC, who facilitates third party reimbursement advocacy efforts on behalf of NATA. (nata.org)
- In addition, a written request for services from a physician may be required if the audiologist or speech-language pathologist intends to seek reimbursement for clinical services from third-party payers such as Medicare, Medicaid, or private insurance companies. (asha.org)
Medicare12
- Perceived, actual, and desired knowledge regarding Medicare billing and reimbursement. (nih.gov)
- To determine perceived, desired, and actual knowledge of Medicare billing and reimbursement among residents compared with community-based General Internists. (nih.gov)
- The residents also strongly agree that they do not receive enough education about Medicare reimbursement, and believe it should be a requirement in residency training. (nih.gov)
- Payment reform driven by the Affordable Care Act (ACA) and the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) continues to be a catalyst for change as the volume-based reimbursement system shifts to a value-based reimbursement system. (contingencies.org)
- Between Congress, the Medicare Payment Advisory Commission (MedPAC) and the Center for Medicare & Medicaid Innovation (CMMI), there have been a number of policy proposals of late that would change reimbursement for medicines covered by Medicare Part B, some of which may harm patient access to important treatments. (phrma.org)
- A rural health clinic (RHC) is a clinic located in a rural, medically under-served area in the United States that has a separate reimbursement structure from the standard medical office under the Medicare and Medicaid programs. (wikipedia.org)
- The RHC program increases access to health care in rural areas by creating special reimbursement mechanisms that allow clinicians to practice in rural, under-served areas increasing utilization of physician assistants (PA) and nurse practitioners (NP) As of 2018, there were approximately 4,300 RHCs across 44 states in the U.S. RHCs facilitate 35.7 million visits per year and provide services for millions of people, including 8 million Medicare beneficiaries. (wikipedia.org)
- To encourage the development of RHCs serving rural, under-served communities, Medicare reimburses RHCs using cost-based reimbursement. (wikipedia.org)
- Prior to 2001, State Medicaid Programs were required to pay RHCs via a cost-based reimbursement model similar to that of Medicare. (wikipedia.org)
- However, the passage of the Medicare, Medicaid and SCHIP Benefits Improvement and Protection Act of 2000 (BIPA 2000) replaced cost-based reimbursement with a state-specific prospective payment system (PPS). (wikipedia.org)
- Under the interim final rule for PBDs, CMS is establishing "a billing mechanism for hospitals to report and receive payment under the MPFS" for items and services rendered to Medicare beneficiaries at PBDs. (healthleadersmedia.com)
- Health maintenance organizations (HMOs), Medicare, Medicaid, private insurance companies, and Individualized Education Programs (IEPs) developed for students with disabilities under the Individuals with Disabilities Education Act (IDEA) may prescribe services, protocols, and procedures which they then authorize and/or approve for reimbursement. (asha.org)
Capitation1
- It has been portrayed as a middle ground between fee-for-service reimbursement and capitation (in which providers are paid a "lump sum" per patient regardless of how many services the patient receives), given that risk is shared between payer and provider. (wikipedia.org)
Healthcare4
- With reducing reimbursements, healthcare providers are striving to have a cost curbing solutions such as CVIS. (prnewswire.com)
- Although the mechanisms differ, these demands stem from the same driver-the perceived need to control healthcare product budgets. (morganlewis.com)
- This paper sheds some light on these questions in the context of rural China, by analyzing the relationship between incomes and healthcare expenditure reimbursements. (biomedcentral.com)
- Likewise, some government healthcare programs have overhauled their reimbursement mechanisms to dramatic effect. (pharmexec.com)
Medicines4
- In both the European Union and United States, commissioners, regulators, and payers are making increasing evidential demands to show value in relation to the pricing and reimbursement of innovative medicines. (morganlewis.com)
- As prices in the market are constantly changing, there is an agreed mechanism in place to increase and decrease the reimbursement prices for medicines. (nhsbsa.nhs.uk)
- Part B uses a unique payment mechanism known as average sales price (ASP) to calculate the price of most of the wide range of medicines it covers. (phrma.org)
- Longer-term mechanisms are needed to ensure financial protection, especially among the poorest, beyond three months when most free services and medicines have ended. (who.int)
Barriers2
- Lack of transparency and unclear reimbursement model for the innovative treatments or digital health therapies, lack of funding for early stage startups, policies, regulations… All this was recognised as some of the barriers in the area of reimbursement and financial mechanisms by the participants of the futures workshops organised by the ECHAlliance in early December 2022. (echalliance.com)
- To promote vaccination in all settings, health-care providers should implement standing orders to identify adults recommended for hepatitis B vaccination and administer vaccination as part of routine clinical services, not require acknowledgment of an HBV infection risk factor for adults to receive vaccine, and use available reimbursement mechanisms to remove financial barriers to hepatitis B vaccination. (cdc.gov)
Workers compensation3
- These intrastate agreements allow jurisdictions to help one another while having provisions in place to address reimbursement, liability and workers compensation issues. (ehstoday.com)
- Although reform has progressed more slowly in the workers compensation arena- where generous reimbursement policies are the norm-several states have implemented measures to better control costs and utilization. (pharmexec.com)
- For example, significant progress in managing workers compensation medical spend was achieved in Oklahoma, Texas, and Washington State, which adopted closed drug formularies, and in Ohio and Mississippi, which imposed reimbursement caps on compounded products. (pharmexec.com)
Expenditures1
- The existing local and national mechanisms for health financing were promising and should be strengthened to reduce out-of-pocket expenses and protect people from catastrophic expenditures. (who.int)
Payers3
- Since National Reimbursement Drug List (NRDL) negotiations were first introduced in 2015 by China's State Council and National Health and Family Planning Commission (NHFPC), national drug price negotiation for high-cost drugs has become a critical cost containment tool for Chinese payers, and a key opportunity for manufacturers to increase their sales in the Chinese market. (simon-kucher.com)
- The combined growth in compounding costs and utilization has negatively impacted many commercial and government payers, particularly those that base reimbursement on the prices of bulk ingredients. (pharmexec.com)
- Pricing, Reimbursement, Funding & Market Access Issues, 2013 Edition, a new publication from Justpharmareports, finds that if there is discrimination by payers towards orphan drugs as a group it is still in a positive way. (prnewswire.com)
Economics1
- Economics and reimbursement have become a daily part of practicing physicians' lives. (nih.gov)
Differ1
- The home philosophies of care, nursing mean length of time on EOL care was approximately 5 months and did not differ homes' reimbursement mechanisms and by whether the care started on or prior to admission or after admission to the regulation, and resident characteristics nursing home. (cdc.gov)
Liability1
- Consideration of legal issues related to worker compensation, liability, credentialing and reimbursement. (cdc.gov)
Expenses1
- Decree no. 2008-1501 of 30/12/2008 relating to the reimbursement of transport expenses of private employees/Decree no. 2010-676 of 21/06/2010 relating to the reimbursement of transport expenses for public sector agents. (filbleu.fr)
Hospital4
- Consolidating hospital systems often acquire physician groups to foster clinically integrated networks in an attempt to raise reimbursement rates and increase patient volume. (contingencies.org)
- If an RHC is owned by a hospital with fewer than fifty beds, there is no cap for the cost-based reimbursement. (wikipedia.org)
- If, however, the RHC is owned by a hospital with more than fifty beds the cost-based reimbursement is capped at $83.45 per visit. (wikipedia.org)
- 8-10 PhilHealth also allowed delivery of hospital reimbursements in advance of claims to enable rebuilding and rehabilitating health facilities (PhilHealth Circular Nos. (who.int)
Generous1
- Germany pairs generous levels of supply of providers with reimbursement systems that set incentives on high volumes and low waiting times, and low prices compared to other OECD countries. (who.int)
Trusts2
- Tax reimbursement clauses are a common clause in many trusts. (forbes.com)
- It adds that all trusts will move to a system of block contracts next month, with mechanisms for reimbursement if costs exceed the agreed amount. (hsj.co.uk)
Volumes1
- Over the same time, overall commercial group volumes and reimbursement levels are projected to remain unchanged. (mckinsey.com)
Establishment1
- NATA is working to establish strategy that not only enhances near term reimbursement success, but will also lead to the long-term establishment of reimbursement as a standard for those ATs and employers who wish to use ATs in a billable capacity. (nata.org)
Payment3
- system, reimbursement is directly related to the volume of services provided and there is little incentive to reduce unnecessary care, the use of bundled payment mechanisms promotes a more efficient use of services. (rand.org)
- Bundled payment is the reimbursement of health care providers on the basis of expected costs for episodes of care. (wikipedia.org)
- There are PBD items and services that will be exempt from the new payment mechanism, including payment for separately payable drugs, which will not be subject to the lower payment rate. (healthleadersmedia.com)
Policy2
- When this happens fully, it is our belief that Insurance companies will still maintain their established policy toward reimbursement for physical medicine and rehabilitation services delivered by ATs regardless of the shift into telehealth. (nata.org)
- Notably, on May 1, 2015, TRICARE, the government health plan covering civilian health benefits for military personnel, revised its reimbursement policy to screen for all ingredients in compounded prescriptions and reject coverage for any non-FDA approved ingredients. (pharmexec.com)
Challenges1
- Join our Washington, DC, and London lawyers and pricing and reimbursement experts for a one-hour webinar to discuss the issues and challenges arising from the growing need in both countries for producers to demonstrate value and share risk. (morganlewis.com)
Decrease1
- Over the years, the current agreement has had a neutral effect on pharmacy contractors' reimbursement given that prices decrease as well as increase from time to time. (nhsbsa.nhs.uk)
Incentives1
- To mitigate these effects, we need a systems based incentives approach via a new paradigm for insurance reimbursement concentrated on prevention and health promotion. (cdc.gov)
Prescriptions2
- A price change after the 8th of the month will be applied for reimbursement purposes to prescriptions dispensed one month later. (nhsbsa.nhs.uk)
- For example, if the manufacturer's list price for a proprietary product changed on 6 February, the new reimbursement price would apply to prescriptions dispensed in March. (nhsbsa.nhs.uk)
Providers1
- The country reimburses inpatient providers almost exclusively on the basis of DRGs, outpatient specialists largely on the basis of fee-for-service (FFS), outpatient general practitioners by a combination of FFS, budgets and other modes of reimbursement, and nursing homes on a per-diem basis. (who.int)
Receive1
- Most items and services rendered at PBDs will receive reimbursement at 50% of the OPPS rate, according to CMS. (healthleadersmedia.com)
Price4
- In the Japanese health care system, FFS is mixed with a nationwide price setting mechanism (all-payer rate setting) to control costs. (wikipedia.org)
- Community Pharmacy England (CPE) keeps the proprietary and non-proprietary price change mechanisms under close review. (nhsbsa.nhs.uk)
- For non-proprietary or generic products (excluding products in Part VIIIA, Category M) the reimbursement price change takes place one month earlier than proprietary products. (nhsbsa.nhs.uk)
- Availability, price and reimbursement status for all 64 EU-designated orphan drugs as of June 2013 with centralised marketing authorisations granted prior to end-2012. (prnewswire.com)
Mutual aid2
- Thirty-six states also have a regional mutual aid mechanism in place. (ehstoday.com)
- Ratified by Congress and signed into law in 1996, the Emergency Management Assistance Compact (EMAC) external icon is an interstate mutual aid agreement that provides a mechanism for sharing personnel, equipment and resources among states during emergencies and disasters. (cdc.gov)
System3
- It is a patient driven informatics obtained from ECG and EKG, Haemodynamic system and echo machines coupled with inventory, business analytics, and billing mechanisms. (prnewswire.com)
- Cooperative Research and Development Agreement (CRADA) - Probably the most commonly used technology transfer mechanism, CRADAs are instruments that may be used in all aspects of a product and/or system lifecycle where research, development, test and evaluation (RDT&E) activities occur. (dhs.gov)
- ASP is a market-based reimbursement system created by Congress in 2003 that has helped manage medication spending, control costs for seniors and provide patients access to the medications they need. (phrma.org)
Regulatory2
Costs5
- A reimbursement mechanism to offset local education agency costs for providing certain health care services and administrative activities in a school setting. (mass.gov)
- Of the 35 facilities that completed the reimbursement section, 29 (83%) reported they had received reimbursement from the federal government and 3 (9%) from the state government for costs in establishing or maintaining their unit. (cdc.gov)
- Help Americans with out-of-pocket costs through expansion of Health Savings Accounts and Health Reimbursement Arrangements. (theglobalipcenter.com)
- The BIPA PPS model requires states to reimburse RHCs at least 100 percent of the average of the costs of the clinic in fiscal years (FY) 1999 and 2000 trended forward for inflation, creating a "floor" for Medicaid reimbursement. (wikipedia.org)
- This descriptive study used a survey and document review to report direct and indirect health-care costs and existing financial protection mechanisms used by households in two municipalities in the Philippines at one week and at seven months post-Haiyan. (who.int)
Model1
- The subscription model is not perfect, and the eventual solution will likely require a mix of different instruments, including both push and pull mechanisms. (bcg.com)
Coverage4
- These diseases may not be considered a priority in universal health coverage packages and may thus be left out of public procurement and reimbursement. (who.int)
- Expand coverage options through mechanisms like Association Health Plans. (theglobalipcenter.com)
- Commercial insurers have been quick to question the value and efficacy of many compounded products while implementing reimbursement caps and coverage restrictions. (pharmexec.com)
- At the moment, there are no specific participation mechanisms during the technology evaluation process or coverage decision-making for potentially interested or affected parties (citizens, patients and caregivers, health professionals, organizations, professional associations, industry). (bvsalud.org)
Third party1
- The NATA Third Party Reimbursement Initiative created the Guidance on Billing and Reimbursement for Athletic Trainers document in 2018 to shed light on reimbursement best practices. (nata.org)
Issues1
- Research and Markets ( http://www.researchandmarkets.com/research/t2f5mf/orphan_drugs_in ) has announced the addition of a new report "Orphan Drugs in Europe: Pricing, Reimbursement, Funding & Market Access Issues" to their offering. (prnewswire.com)
Services2
- The federal parties may provide personnel, services, facilities, equipment, intellectual property or other resources with or without reimbursement (but not funds to the non-federal parties). (dhs.gov)
- Traditionally, many athletic trainers do not understand how reimbursement could potentially affect them because they are contracted and employed by a given entity to deliver AT services that are not billed," Greene said. (nata.org)
Levels2
- Explained variables include obtainment, levels and rates of NCMS reimbursement. (biomedcentral.com)
- Prior to 2009 reforms, higher income in our sample was statistically significantly related to higher probability of obtaining reimbursement, as well as higher levels and rates of reimbursement. (biomedcentral.com)
Program2
- As we debate these proposals, it's important to levelset on how reimbursement works in the program today. (phrma.org)
- The RHC program was criticized in the 1990s for allowing enhanced reimbursement to remain for RHCs, even if that clinic is no longer in a rural or under-served community. (wikipedia.org)
Commonly1
- Pediatric patients with surgical ventricular scars, such as those with postoperative ventricular tachycardia (VT) after repair of tetralogy of Fallot , are commonly cited examples of this mechanism. (medscape.com)
Financial2
- Reimbursement & financial mechanisms in digital health. (echalliance.com)
- Back to this particular futures workshop, which was organised to crowdsource the visions for the futures around financial mechanisms and digital health in 2030. (echalliance.com)
Long-term1
- The planning, budgeting and reimbursement of the inpatient and outpatient sectors and long-term care are strictly separated. (who.int)
Section1
- See the Reimbursement section below for further details. (asha.org)
Pricing1
- Thus, in the topsy-turvy world of drug pricing and reimbursement, compounding is viewed as both a cause for escalating drug prices as well as a potential catalyst for reform. (pharmexec.com)
Resource2
- In addition to the lack of transparency and fragmentation of the reimbursement models, the resource wasting does not support efficiency and has an effect on equity and quality of care. (echalliance.com)
- Any AT is able to benefit from the NATA Billing and Reimbursement Guidance resource as it outlines how health systems and independent settings can implement reimbursements for ATs into their company. (nata.org)
Details1
- Ask your company for more details about the reimbursement mechanism. (filbleu.fr)
Independent1
- Reimbursement for independent RHCs is capped at the same rate as provider-based RHCs with more than fifty beds. (wikipedia.org)
Funds1
- The purpose of a tax reimbursement clause is to provide funds to the grantor to pay the income tax on the income earned in the grantor trust (because, of course, the income of a grantor trust is attributed to the grantor who must report that income and pay the income tax on it. (forbes.com)
Public1
- The participants of the workshop created an intense discussion around the ideas and scenarios for 2030, including reimbursement models, impact based investing, the share of the roles between the public and private sectors, and support for early-stage startups. (echalliance.com)
Works1
- To understand the use of a tax reimbursement clause you need to first understand what a grantor trust is and how it works. (forbes.com)
Systems1
- How reimbursement systems treat orphan drugs. (prnewswire.com)
Products1
- On a more positive note, September 2013 saw the start of the first pilot pan-EU assessment under the Mechanism of Co-ordinated Access to Orphan Medicinal Products (MoCA-OMP) initiative. (prnewswire.com)
Prevent5
- They establish reasonable administrative mechanisms to facilitate the right to vote and to prevent practices - including deceptive practices - that undermine the integrity of the vote. (gc.ca)
- Two newly discovered mechanisms of heart cells may result in a better understanding of cardiovascular disease and lead to new treatment options that prevent damage. (pharmacytimes.com)
- The authors of a study published by Cell Reports discovered that these biological mechanisms may prevent damage to the network of mitochondrial circuits that provide energy to the cells. (pharmacytimes.com)
- Manufacturers of treatments for Fabry and Pompe diseases are currently negotiating discounts in the Netherlands to prevent delisting after results from a four-year conditional reimbursement PMS period disappointed. (prnewswire.com)
- To prevent this, the EU needs to set up a European energy solidarity mechanism. (epc.eu)


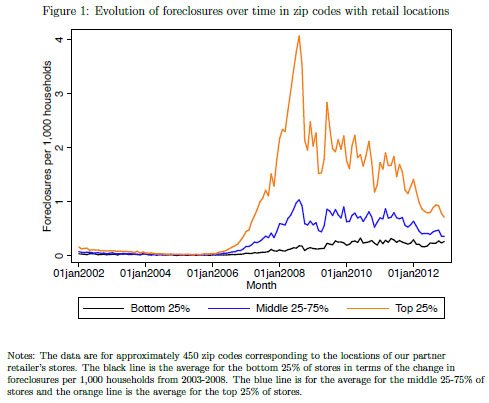





.jpg)


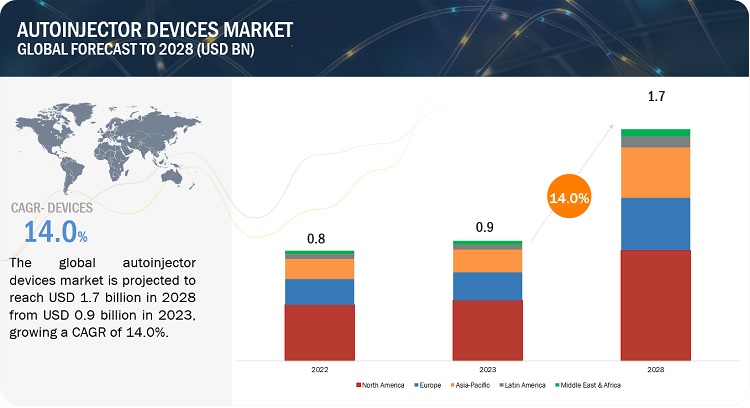




/https://cdn.rollick.io/images/crs/400x200/2021_KYMCO_AK_550.jpg)
/https://cdn.dealerspike.com/imglib/v1/1024x1024/imglib/Assets/Inventory/82/BC/82BCC912-8CF1-4747-95E5-EA1B9FC15B5E.jpg)