Radiology Department, Hospital
Radiology Information Systems
Radiology
Teleradiology
Analog-Digital Conversion
Work Simplification
Personnel Staffing and Scheduling Information Systems
Waste Management
Computer Systems
Radiographic Image Enhancement
Radiology, Interventional
Diagnostic Imaging
Tomography, X-Ray Computed
User-Computer Interface
Emergency Service, Hospital
Hospitals, Teaching
Hospitals, University
Hospitals, General
Hospital Costs
Retrospective Studies
Radiography
Mammography: influence of departmental practice and women's characteristics on patient satisfaction: comparison of six departments in Norway. (1/200)
OBJECTIVE: To investigate how departmental practice and women's characteristics are related to low patient satisfaction with mammography. DESIGN: Survey of patients by means of self administered questionnaires before and after mammography. PATIENTS: 488 women (89% of those invited), aged 23-86 years, at six departments. MAIN OUTCOME MEASURES: Low level of satisfaction measured on psychometric scales of physical pain, psychological distress, staff punctuality and technical skills, information provided, and physical surroundings. RESULTS: Satisfaction varied by department on the scales for pain, punctuality, information, and surroundings. After adjustment for women's characteristics an attributable risk of negative outcome by department was identified on the scales for pain, distress, punctuality, information, and surroundings. Adjusted odds ratio (ORs) ranged from 0.3 (95% confidence interval (95% CI) 1.2 to 6.0) on the pain scale, to 6.0 (2.9 to 12.3) on the punctuality scale. After adjustment for confounding variables, higher risk of dissatisfaction was associated with age < 50, nervousness about mammography, expected pain, lack of knowledge about mammography, and distrust in mammography (adjusted OR (95% CI) ranged from 1.6 (1.0 to 2.7) to 3.7 (2.0 to 7.3)). CONCLUSION: Departmental practices differed for breast compression, information, punctuality, and facilities and were associated with a low level of satisfaction irrespective of patient characteristics. Women's lack of knowledge about mammography and distrust in the procedure were confirmed as risk factors for dissatisfaction. All these factors might be helped by training the staff, improving facilities, and informing the women. (+info)Challenges associated with the incorporation of digital radiography into a picture archival and communication system. (2/200)
Digital radiography (DR) has recently emerged as an attractive alternative to computed radiography (CR) for the acquisition of general radiographic studies in a digital environment. It offers the possibility of improved spatial and contrast resolution, decreased radiation dose due to improved efficiency of detection of x-ray photons, and perhaps most importantly, holds out the promise of increased technologist productivity. To achieve maximum efficiency, DR must be completely integrated into existing information systems, including the hospital and radiology information systems (HIS/RIS) and, when present, the picture archival and communication system (PACS). The early experience with the integration of DR at the Baltimore Veterans Affairs Medical Center (VAMC) has identified several challenges that exist to the successful integration of DR. DR has only recently been defined as a separate Digital Imaging and Communications in Medicine (DICOM) modality and images obtained will, at first, be listed under the category of CR. Matrix sizes with some DR products on the market exceed the current size limitations of some PACS. The patient throughput may be substantially greater with DR than with CR, and this in combination with the larger size of image files may result in greater demands for network and computer performance in the process of communication with the HIS/RIS and PACS. Additionally, in a hybrid department using both CR and DR, new rules must be defined for prefetching and display of general radiographic studies to permit these examinations to be retrieved and compared together. Advanced features that are planned for DR systems, such as dual-energy subtraction, tomosynthesis, and temporal subtraction, will likely require additional workstation tools beyond those currently available for CR. (+info)Process reengineering: the role of a planning methodology and picture archiving and communications system team building. (3/200)
The acquisition of a picture archiving and communications system (PACS) is an opportunity to reengineer business practices and should optimally consider the entire process from image acquisition to communication of results. The purpose of this presentation is to describe the PACS planning methodology used by the Department of Defense (DOD) Joint Imaging Technology Project Office (JITPO), outline the critical procedures for each phase, and review the military experience using this model. The methodology is segmented into four phases: strategic planning, clinical scenario planning, installation planning, and implementation planning. Each is further subdivided based on the specific tasks that need to be accomplished within that phase. By using this method, an institution will have clearly defined program goals, objectives, and PACS requirements before vendors are contacted. The development of an institution-specific PACS requirement should direct the process of proposal comparisons to be based on functionality and exclude unnecessary equipment. This PACS planning methodology is being used at more than eight DOD medical treatment facilities. When properly executed, this methodology facilitates a seamless transition to the electronic environment and contributes to the successful integration of the healthcare enterprise. A crucial component of this methodology is the development of a local PACS planning team to manage all aspects of the process. A plan formulated by the local team is based on input from each department that will be integrating with the PACS. Involving all users in the planning process is paramount for successful implementation. (+info)Electronic imaging and clinical implementation: work group approach at Mayo Clinic, Rochester. (4/200)
Electronic imaging clinical implementation strategies and principles need to be developed as we move toward replacement of film-based radiology practices. During an 8-month period (1998 to 1999), an Electronic Imaging Clinical Implementation Work Group (EICIWG) was formed from sections of our department: Informatics Lab, Finance Committee, Management Section, Regional Practice Group, as well as several organ and image modality sections of the Department of Diagnostic Radiology. This group was formed to study and implement policies and strategies regarding implementation of electronic imaging into our practice. The following clinical practice issues were identified as key focus areas: (1) optimal electronic worklist organization; (2) how and when to link images with reports; (3) how to redistribute technical and professional relative value units (RVU); (4) how to facilitate future practice changes within our department regarding physical location and work redistribution; and (5) how to integrate off-campus imaging into on-campus workflow. The EICIWG divided their efforts into two phases. Phase I consisted of Fact finding and review of current practice patterns and current economic models, as well as radiology consulting needs. Phase II involved the development of recommendations, policies, and strategies for reengineering the radiology department to maintain current practice goals and use electronic imaging to improve practice patterns. The EICIWG concluded that electronic images should only be released with a formal report, except in emergent situations. Electronic worklists should support and maintain the physical presence of radiologists in critical areas and direct imaging to targeted subspecialists when possible. Case tools should be developed and used in radiology and hospital information systems (RIS/HIS) to monitor a number of parameters, including professional and technical RVU data. As communication standards improve, proper staffing models must be developed to facilitate electronic on-campus and off-campus consultation. (+info)The importance of a picture archiving and communications system (PACS) manager for large-scale PACS installations. (5/200)
Installing a picture archiving and communication system (PACS) is a massive undertaking for any radiology department. Facilities making a successful transition to digital systems are finding that a PACS manager helps guide the way and offers a heightened return on the investment. The PACS manager fills a pivotal role in a multiyear, phased PACS installation. PACS managers navigate a facility through the complex sea of issues surrounding a PACS installation by coordinating the efforts of the vendor, radiology staff, hospital administration, and the information technology group. They are involved in the process from the purchase decision through the design and implementation phases. They can help administrators justify a PACS, purchase and shape the request for proposal (RFP) process before a vendor is even chosen. Once a supplier has been selected, the PACS manager works closely with the vendor and facility staff to determine the best equipment configuration for his or her facility, and makes certain that all deadlines are met during the planning and installation phase. The PACS manager also ensures that the infrastructure and backbone of the facility are ready for installation of the equipment. PACS managers also help the radiology staff gain acceptance of the technology by serving as teachers, troubleshooters, and the primary point-of-contact for all PACS issues. This session will demonstrate the value of a PACS manager, as well as point out ways to determine the manager's responsibilities. By the end of the session, participants will be able to describe the role of a PACS manager as it relates to departmental operation and in partnership with equipment vendors, justify a full-time position for a PACS manager, and identify the qualifications of candidates for the position of PACS manager. (+info)Care and feeding of a staff for filmless radiology. (6/200)
Texas Children's Hospital, a definitive care pediatric hospital located in the Texas Medical Center, has been constructing a large-scale picture archival and communications system (PACS) including ultrasound (US), computed tomography (CT), magnetic resonance (MR), and computed radiography (CR). Developing staffing adequate to meet the demands of filmless radiology operations has been a continuous challenge. Overall guidance for the PACS effort is provided by a hospital-level PACS Committee, a department-level PACS Steering Committee, and an Operations Committee. Operational Subcommittees have been formed to address service-specific implementation, such as the Emergency Center Operations Subcommittee. These committees include membership by those affected by the change, as well as those effecting the change. Initially, personnel resources for PACS were provided through additional duties of existing imaging service personnel. As the PACS effort became more complex, full-time positions were created, including a PACS Coordinator, a PACS Analyst, and a Digital Imaging Assistant. Each position requires a job description, qualifications, and personnel development plans that are difficult to anticipate in an evolving PACS implementation. These positions have been augmented by temporary full-time assignments, position reclassifications, and cross-training of other imaging personnel. Imaging personnel are assisted by other hospital personnel from Biomedical Engineering and Information Services. Ultimately, the PACS staff grows to include all those who must operate the PACS equipment in the normal course of their duties. The effectiveness of the PACS staff is limited by their level of their expertise. This report discusses our methods to obtain training from outside our institution and to develop, conduct, and document standardized in-house training. We describe some of the products of this work, including policies and procedures, clinical competency criteria, PACS inservice topics, and an informal PACS newsletter. As the PACS system software and hardware changes, and as our implementation grows, these products must to be revised and training must be repeated. (+info)The process of converting to a near filmless operation at the University of Utah, Department of Radiology. (7/200)
The Department of Radiology at the University of Utah Health Sciences Center has made the transition from a traditional film-based department to a near filmless operation. The University of Utah is a large teaching hospital and the transition from film in an educational facility will be discussed. This transition has had its difficulties and its success is dependent on the support of departmental leadership and hospital administration. We have had more than 100 years of experience with film, and current procedures were efficient given the limitations of the medium. While motivated by the traditional reasons for moving to a picture archival and communications system (PACS), such as film savings, unavailable films, and faster reports, we found the intangibles to be the larger issue, as well as a source for the largest benefits. This report will discuss the implementation process and the affect it had on all areas of the hospital, including its impact on hospital physicians, radiologists, file room personnel, and technologists. Procedure changes to the flow of patients, film, and electronic images will also be described. This process cannot be viewed as a one-time change, but must be viewed as a continuous process as areas of improvement are identified and new and improved technologies are developed. (+info)Maintaining continuity of clinical operations while implementing large-scale filmless operations. (8/200)
Texas Children's Hospital is a pediatric tertiary care facility in the Texas Medical Center with a large-scale, Digital Imaging and Communications in Medicine (DICOM)-compliant picture archival and communications system (PACS) installation. As our PACS has grown from an ultrasound niche PACS into a full-scale, multimodality operation, assuring continuity of clinical operations has become the number one task of the PACS staff. As new equipment is acquired and incorporated into the PACS, workflow processes, responsibilities, and job descriptions must be revised to accommodate filmless operations. Round-the-clock clinical operations must be supported with round-the-clock service, including three shifts, weekends, and holidays. To avoid unnecessary interruptions in clinical service, this requirement includes properly trained operators and users, as well as service personnel. Redundancy is a cornerstone in assuring continuity of clinical operations. This includes all PACS components such as acquisition, network interfaces, gateways, archive, and display. Where redundancy is not feasible, spare parts must be readily available. The need for redundancy also includes trained personnel. Procedures for contingency operations in the event of equipment failures must be devised, documented, and rehearsed. Contingency operations might be required in the event of scheduled as well as unscheduled service events, power outages, network outages, or interruption of the radiology information system (RIS) interface. Methods must be developed and implemented for reporting and documenting problems. We have a Trouble Call service that records a voice message and automatically pages the PACS Console Operator on duty. We also have developed a Maintenance Module on our RIS system where service calls are recorded by technologists and service actions are recorded and monitored by PACS support personnel. In a filmless environment, responsibility for the delivery of images to the radiologist and referring physician must be accepted by each imaging supervisor. Thus, each supervisor must initiate processes to verify correct patient and examination identification and the correct count and routing of images with each examination. (+info)A Radiology Department in a hospital is a specialized unit where diagnostic and therapeutic imaging examinations are performed using various forms of radiant energy, including X-rays, magnetic fields, ultrasound, and radio waves. The department is staffed by radiologists (physicians who specialize in the interpretation of medical images) and radiologic technologists who operate the imaging equipment.
The Radiology Department provides a range of services, such as:
1. Diagnostic Radiology: Uses various imaging techniques to diagnose and monitor diseases and injuries, including X-ray, computed tomography (CT), magnetic resonance imaging (MRI), ultrasound, and mammography.
2. Interventional Radiology: Utilizes image guidance to perform minimally invasive procedures, such as biopsies, tumor ablations, and angioplasty.
3. Nuclear Medicine: Uses small amounts of radioactive materials to diagnose and treat diseases, including bone scans, thyroid studies, and positron emission tomography (PET) scans.
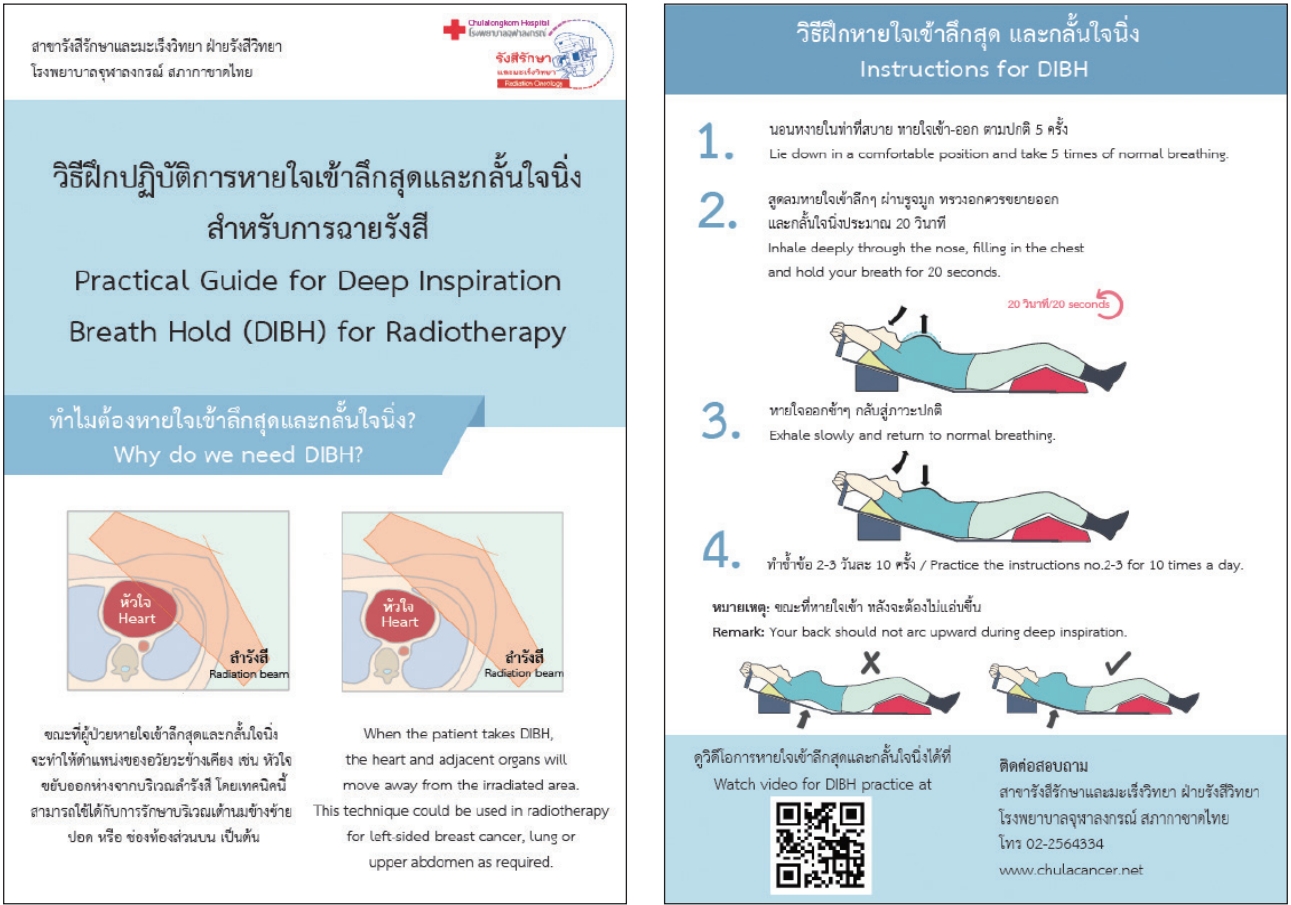
4. Radiation Therapy: Treats cancer using high-energy radiation beams targeted at tumors to destroy cancer cells while minimizing damage to surrounding healthy tissue.
The primary goal of the Radiology Department is to provide accurate and timely diagnostic information, support clinical decision-making, and contribute to improved patient outcomes through effective imaging services.
A Radiology Information System (RIS) is a type of healthcare software specifically designed to manage medical imaging data and related patient information. It serves as a centralized database and communication platform for radiology departments, allowing the integration, storage, retrieval, and sharing of patient records, orders, reports, images, and other relevant documents.
The primary functions of a RIS typically include:
1. Scheduling and tracking: Managing appointments, scheduling resources, and monitoring workflow within the radiology department.
2. Order management: Tracking and processing requests for imaging exams from referring physicians or other healthcare providers.
3. Image tracking: Monitoring the movement of images throughout the entire imaging process, from acquisition to reporting and storage.
4. Report generation: Assisting radiologists in creating structured, standardized reports based on the interpreted imaging studies.
5. Results communication: Sending finalized reports back to the referring physicians or other healthcare providers, often through integration with electronic health records (EHRs) or hospital information systems (HIS).
6. Data analytics: Providing tools for analyzing and reporting departmental performance metrics, such as turnaround times, equipment utilization, and patient satisfaction.
7. Compliance and security: Ensuring adherence to regulatory requirements related to data privacy, protection, and storage, while maintaining secure access controls for authorized users.
By streamlining these processes, a RIS helps improve efficiency, reduce errors, enhance communication, and support better patient care within radiology departments.
Radiology is a medical specialty that uses imaging technologies to diagnose and treat diseases. These imaging technologies include X-rays, computed tomography (CT) scans, magnetic resonance imaging (MRI) scans, positron emission tomography (PET) scans, ultrasound, and mammography. Radiologists are medical doctors who have completed specialized training in interpreting these images to diagnose medical conditions and guide treatment plans. They also perform image-guided procedures such as biopsies and tumor ablations. The goal of radiology is to provide accurate and timely information to help physicians make informed decisions about patient care.
Teleradiology is a subspecialty of radiology that involves the transmission of medical images from one location to another for the purpose of interpretation and diagnosis by a radiologist. This technology allows radiologists to review and report on imaging studies, such as X-rays, CT scans, and MRI scans, remotely using secure electronic communication systems.
Teleradiology has become increasingly important in modern healthcare, particularly in emergency situations where immediate interpretation of medical images is necessary. It also enables radiologists to provide specialized expertise for complex cases, regardless of their geographic location. The use of teleradiology must comply with all relevant regulations and laws regarding patient privacy and data security.
Analog-digital conversion, also known as analog-to-digital conversion (ADC) or digitization, is the process of converting a continuous physical quantity or analog signal into a discrete numerical representation or digital signal. This process typically involves sampling the analog signal at regular intervals and then quantizing each sample by assigning it to a specific numerical value within a range. The resulting digital signal can be processed, stored, and transmitted more easily than an analog signal. In medical settings, this type of conversion is often used in devices such as electrocardiograms (ECGs) and blood pressure monitors to convert physiological signals into digital data that can be analyzed and interpreted by healthcare professionals.
I'm sorry for any confusion, but "work simplification" is not a medical term. It is a general term used in various fields such as industrial engineering, ergonomics, and management to refer to the process of redesigning or modifying work methods, processes, or environments to make them more efficient, less strenuous, and easier to perform.
Work simplification can involve various techniques, including task analysis, process mapping, eliminating unnecessary steps, standardizing work procedures, and using appropriate tools and equipment. While not a medical term, work simplification may have applications in occupational therapy, rehabilitation, and disability management to help individuals with injuries or disabilities perform their job tasks more easily and safely.
I could not find a specific medical definition for "Personnel Staffing and Scheduling Information Systems" as it is more related to healthcare management and human resources. However, I can provide you with a general definition and explain its relevance to the medical field:
Personnel Staffing and Scheduling Information Systems refer to automated or computerized systems designed to manage and optimize staffing and scheduling processes within an organization. These systems help streamline workforce management by tracking employee availability, qualifications, and schedules while ensuring adequate coverage for various shifts, departments, or positions.
In the medical field, these systems are particularly important for managing healthcare personnel, such as nurses, doctors, and allied health professionals. Proper staffing and scheduling are crucial for maintaining high-quality patient care, ensuring compliance with regulatory requirements, and optimizing resource allocation. Personnel Staffing and Scheduling Information Systems in healthcare can help:
1. Match staff skills and qualifications to patient needs and unit requirements.
2. Ensure adequate coverage during peak demand periods or emergencies.
3. Minimize overstaffing and reduce labor costs.
4. Prevent scheduling conflicts, fatigue, and burnout by tracking employee work hours and mandatory rest periods.
5. Facilitate communication between staff members, managers, and human resources departments.
6. Monitor compliance with labor laws, union rules, and organizational policies related to staffing and scheduling.
7. Provide data for workforce planning, performance evaluation, and continuous improvement initiatives.
An X-ray film, also known as radiograph, is a medical imaging tool that uses X-rays to create images of the body's internal structures. The film itself is a light-sensitive material that reacts to the X-rays passing through the body and records the resulting shadows and patterns on its surface.
The process involves exposing the patient to a controlled amount of X-ray radiation, which passes through the body and is absorbed differently by various tissues and structures. Denser materials such as bone absorb more X-rays and appear white or light gray on the film, while less dense materials such as soft tissues absorb fewer X-rays and appear darker.
Once the X-ray exposure is complete, the film is developed using a chemical process that produces a visible image of the internal structures. This image can then be analyzed by medical professionals to diagnose injuries, diseases, or other conditions affecting the body's internal structures.
It's worth noting that in modern medical imaging, digital X-ray sensors have largely replaced traditional X-ray film, offering several advantages such as reduced radiation exposure, faster image processing, and easier storage and retrieval of images.
I'm happy to help, but I must clarify that I can't provide a "medical definition" of waste management since it is not a medical term per se. Waste management is a broader environmental and public health issue. However, I can offer a definition related to healthcare facilities:
Waste management in the context of healthcare facilities refers to the practices, processes, and systems used to collect, transport, treat, dispose, recycle, or reuse waste materials generated from healthcare activities. This includes various types of waste such as hazardous (e.g., infectious, chemical, pharmaceutical), non-hazardous, and radioactive waste. Proper management is crucial to prevent infection, protect the environment, conserve resources, and ensure occupational safety for healthcare workers and the public.
A computer system is a collection of hardware and software components that work together to perform specific tasks. This includes the physical components such as the central processing unit (CPU), memory, storage devices, and input/output devices, as well as the operating system and application software that run on the hardware. Computer systems can range from small, embedded systems found in appliances and devices, to large, complex networks of interconnected computers used for enterprise-level operations.
In a medical context, computer systems are often used for tasks such as storing and retrieving electronic health records (EHRs), managing patient scheduling and billing, performing diagnostic imaging and analysis, and delivering telemedicine services. These systems must adhere to strict regulatory standards, such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States, to ensure the privacy and security of sensitive medical information.
Radiographic image enhancement refers to the process of improving the quality and clarity of radiographic images, such as X-rays, CT scans, or MRI images, through various digital techniques. These techniques may include adjusting contrast, brightness, and sharpness, as well as removing noise and artifacts that can interfere with image interpretation.
The goal of radiographic image enhancement is to provide medical professionals with clearer and more detailed images, which can help in the diagnosis and treatment of medical conditions. This process may be performed using specialized software or hardware tools, and it requires a strong understanding of imaging techniques and the specific needs of medical professionals.
Interventional radiology (IR) is a subspecialty of radiology that uses minimally invasive image-guided procedures to diagnose and treat various medical conditions. The main goal of interventional radiology is to offer patients less invasive options for treatment, which can result in smaller incisions, reduced recovery time, and fewer complications compared to traditional open surgeries.
Interventional radiologists use a variety of imaging techniques, such as X-rays, fluoroscopy, computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound, to guide catheters, wires, needles, and other small instruments through the body to target specific areas. These targeted interventions can be used for both diagnostic and therapeutic purposes, including:
1. Biopsies: Obtaining tissue samples from organs or tumors to determine a diagnosis.
2. Drainage procedures: Removing fluid from abscesses, cysts, or blocked areas to alleviate symptoms and promote healing.
3. Stent placements: Opening narrowed or obstructed blood vessels, bile ducts, or airways using small mesh tubes called stents.
4. Embolization: Blocking abnormal blood vessels or reducing blood flow to tumors, aneurysms, or other problematic areas.
5. Tumor ablation: Destroying tumors using heat (radiofrequency ablation, microwave ablation), cold (cryoablation), or other energy sources.
6. Pain management: Treating chronic pain by targeting specific nerves and blocking their transmission of pain signals.
7. Vascular access: Creating secure pathways to blood vessels for dialysis, chemotherapy, or other long-term treatments.
8. Aneurysm repair: Reinforcing weakened or bulging blood vessel walls using coils, stents, or flow diverters.
9. Vertebroplasty and kyphoplasty: Stabilizing fractured vertebrae in the spine to alleviate pain and improve mobility.
10. Uterine fibroid embolization: Reducing the size and symptoms of uterine fibroids by blocking their blood supply.
These are just a few examples of interventional radiology procedures. The field is constantly evolving, with new techniques and technologies being developed to improve patient care and outcomes. Interventional radiologists work closely with other medical specialists to provide minimally invasive treatment options for a wide range of conditions.
Diagnostic imaging is a medical specialty that uses various technologies to produce visual representations of the internal structures and functioning of the body. These images are used to diagnose injury, disease, or other abnormalities and to monitor the effectiveness of treatment. Common modalities of diagnostic imaging include:
1. Radiography (X-ray): Uses ionizing radiation to produce detailed images of bones, teeth, and some organs.
2. Computed Tomography (CT) Scan: Combines X-ray technology with computer processing to create cross-sectional images of the body.
3. Magnetic Resonance Imaging (MRI): Uses a strong magnetic field and radio waves to generate detailed images of soft tissues, organs, and bones.
4. Ultrasound: Employs high-frequency sound waves to produce real-time images of internal structures, often used for obstetrics and gynecology.
5. Nuclear Medicine: Involves the administration of radioactive tracers to assess organ function or detect abnormalities within the body.
6. Positron Emission Tomography (PET) Scan: Uses a small amount of radioactive material to produce detailed images of metabolic activity in the body, often used for cancer detection and monitoring treatment response.
7. Fluoroscopy: Utilizes continuous X-ray imaging to observe moving structures or processes within the body, such as swallowing studies or angiography.
Diagnostic imaging plays a crucial role in modern medicine, allowing healthcare providers to make informed decisions about patient care and treatment plans.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
A User-Computer Interface (also known as Human-Computer Interaction) refers to the point at which a person (user) interacts with a computer system. This can include both hardware and software components, such as keyboards, mice, touchscreens, and graphical user interfaces (GUIs). The design of the user-computer interface is crucial in determining the usability and accessibility of a computer system for the user. A well-designed interface should be intuitive, efficient, and easy to use, minimizing the cognitive load on the user and allowing them to effectively accomplish their tasks.
An emergency service in a hospital is a department that provides immediate medical or surgical care for individuals who are experiencing an acute illness, injury, or severe symptoms that require immediate attention. The goal of an emergency service is to quickly assess, stabilize, and treat patients who require urgent medical intervention, with the aim of preventing further harm or death.
Emergency services in hospitals typically operate 24 hours a day, 7 days a week, and are staffed by teams of healthcare professionals including physicians, nurses, physician assistants, nurse practitioners, and other allied health professionals. These teams are trained to provide rapid evaluation and treatment for a wide range of medical conditions, from minor injuries to life-threatening emergencies such as heart attacks, strokes, and severe infections.
In addition to providing emergency care, hospital emergency services also serve as a key point of entry for patients who require further hospitalization or specialized care. They work closely with other departments within the hospital, such as radiology, laboratory, and critical care units, to ensure that patients receive timely and appropriate treatment. Overall, the emergency service in a hospital plays a crucial role in ensuring that patients receive prompt and effective medical care during times of crisis.
A "Teaching Hospital" is a healthcare institution that provides medical education and training to future healthcare professionals, such as medical students, residents, and fellows. These hospitals are often affiliated with medical schools or universities and have a strong focus on research and innovation in addition to patient care. They typically have a larger staff of specialized doctors and medical professionals who can provide comprehensive care for complex and rare medical conditions. Teaching hospitals also serve as important resources for their communities, providing access to advanced medical treatments and contributing to the development of new healthcare technologies and practices.
There seems to be a misunderstanding in your question. "Hospital Departments" is not a medical term or diagnosis, but rather an organizational structure used by hospitals to divide their services and facilities into different units based on medical specialties or patient populations. Examples of hospital departments include internal medicine, surgery, pediatrics, emergency medicine, radiology, and pathology. Each department typically has its own staff, equipment, and facilities to provide specialized care for specific types of patients or medical conditions.
A "University Hospital" is a type of hospital that is often affiliated with a medical school or university. These hospitals serve as major teaching institutions where medical students, residents, and fellows receive their training and education. They are equipped with advanced medical technology and resources to provide specialized and tertiary care services. University hospitals also conduct research and clinical trials to advance medical knowledge and practices. Additionally, they often treat complex and rare cases and provide a wide range of medical services to the community.
A "General Hospital" is a type of hospital that provides a broad range of medical and surgical services to a diverse patient population. It typically offers general medical care, emergency services, intensive care, diagnostic services (such as laboratory testing and imaging), and inpatient and outpatient surgical services. General hospitals may also have specialized departments or units for specific medical conditions or populations, such as pediatrics, obstetrics and gynecology, geriatrics, oncology, and mental health. They are usually staffed by a variety of healthcare professionals, including physicians, nurses, pharmacists, therapists, and support personnel. General hospitals can be found in both urban and rural areas and may be operated by governmental, non-profit, or for-profit organizations.
Hospital costs are the total amount of money that is expended by a hospital to provide medical and healthcare services to patients. These costs can include expenses related to:
* Hospital staff salaries and benefits
* Supplies, such as medications, medical devices, and surgical equipment
* Utilities, such as electricity, water, and heating
* Facility maintenance and renovation
* Equipment maintenance and purchase
* Administrative costs, such as billing and insurance processing
Hospital costs can also be classified into fixed and variable costs. Fixed costs are those that do not change with the volume of services provided, such as rent or depreciation of equipment. Variable costs are those that change with the volume of services provided, such as supplies and medications.
It's important to note that hospital costs can vary widely depending on factors such as the complexity of care provided, the geographic location of the hospital, and the patient population served. Additionally, hospital costs may not always align with charges or payments for healthcare services, which can be influenced by factors such as negotiated rates with insurance companies and government reimbursement policies.
"Urban hospitals" is not a medical term per se, but rather a term that describes the location and setting of healthcare facilities. In this context, "urban" refers to densely populated cities or built-up areas, as opposed to rural or suburban regions. Therefore, urban hospitals are medical institutions located in or near urban centers, serving large populations and typically providing a wide range of specialized services.
These hospitals often have more resources, advanced technology, and subspecialties compared to their rural counterparts due to the higher patient volume and financial support they receive. They also tend to be teaching hospitals affiliated with medical schools and research institutions, contributing significantly to medical education, innovation, and clinical trials.
However, it is important to note that urban hospitals may face unique challenges in providing care, such as serving diverse populations with varying socioeconomic backgrounds, addressing health disparities, managing high patient volumes, and dealing with issues related to overcrowding and resource allocation.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
A pediatric hospital is a specialized medical facility that provides comprehensive healthcare services for infants, children, adolescents, and young adults up to the age of 21. These hospitals employ medical professionals with expertise in treating various childhood illnesses, injuries, and developmental disorders. The facilities are designed to cater to the unique needs of children, including child-friendly environments, specialized equipment, and age-appropriate care.
Pediatric hospitals offer a wide range of services such as inpatient and outpatient care, emergency services, surgical procedures, diagnostic testing, rehabilitation, and mental health services. They also focus on preventive healthcare, family-centered care, and education to support the overall well-being of their young patients. Some pediatric hospitals may specialize further, focusing on specific areas such as cancer treatment, cardiology, neurology, or orthopedics.
Radiography is a diagnostic technique that uses X-rays, gamma rays, or similar types of radiation to produce images of the internal structures of the body. It is a non-invasive procedure that can help healthcare professionals diagnose and monitor a wide range of medical conditions, including bone fractures, tumors, infections, and foreign objects lodged in the body.
During a radiography exam, a patient is positioned between an X-ray machine and a special film or digital detector. The machine emits a beam of radiation that passes through the body and strikes the film or detector, creating a shadow image of the internal structures. Denser tissues, such as bones, block more of the radiation and appear white on the image, while less dense tissues, such as muscles and organs, allow more of the radiation to pass through and appear darker.
Radiography is a valuable tool in modern medicine, but it does involve exposure to ionizing radiation, which can carry some risks. Healthcare professionals take steps to minimize these risks by using the lowest possible dose of radiation necessary to produce a diagnostic image, and by shielding sensitive areas of the body with lead aprons or other protective devices.
'Hospital Nursing Staff' refers to the group of healthcare professionals who are licensed and trained to provide nursing care to patients in a hospital setting. They work under the direction of a nurse manager or director and collaborate with an interdisciplinary team of healthcare providers, including physicians, therapists, social workers, and other support staff.
Hospital nursing staff can include registered nurses (RNs), licensed practical nurses (LPNs) or vocational nurses (LVNs), and unlicensed assistive personnel (UAPs) such as nursing assistants, orderlies, and patient care technicians. Their responsibilities may vary depending on their role and the needs of the patients, but they typically include:
* Administering medications and treatments prescribed by physicians
* Monitoring patients' vital signs and overall condition
* Providing emotional support and education to patients and their families
* Assisting with activities of daily living such as bathing, dressing, and grooming
* Documenting patient care and progress in medical records
* Collaborating with other healthcare professionals to develop and implement individualized care plans.
Hospital nursing staff play a critical role in ensuring the safety, comfort, and well-being of hospitalized patients, and they are essential members of the healthcare team.