Post-Dural Puncture Headache
Blood Patch, Epidural
Spinal Puncture
Headache
Dura Mater
Analgesia, Epidural
Anesthesia, Obstetrical
Punctures
Analgesia, Obstetrical
Headache Disorders
Encyclopedias as Topic
Vertigo
Scalp
Access to Information
Journal Impact Factor
Peer Review, Research
Publishing
Diagnostic lumbar puncture. Comparative study between 22-gauge pencil point and sharp bevel needle. (1/32)
Post-lumbar puncture headache is a frequent clinical problem. Needle design is expected to reduce post-puncture headache. In this study, we compared two different lumbar puncture needle designs in diagnostic lumbar puncture and analysed post-dural puncture headache (PDPH) and social and economical harm associated with the diagnostic lumbar puncture procedure. This prospective, controlled study consisted of 80 consecutive adult patients requiring elective diagnostic lumbar puncture due to various neurological symptoms. Lumbar puncture was completed either with Spinocan 22 G sharp bevel needle or Whitacre 22G pencil point needle. Patients were asked about previous headache symptoms and pain provoked by puncture. One week after the lumbar puncture all patients were interviewed by telephone and occurrence and type of headache, headache intensity, medication and frequency of impairment in activities of daily living were asked. Need for epidural blood patch was also recorded. Thirty-three of 78 (42%) patients experienced headache after diagnostic lumbar puncture and in 26 (33%) the headache could be classified as PDPH. There were no statistically significant differences between needle types in the frequency of common headache, PDPH, puncture pain intensity, need for epidural blood patch or sick leave. Also, there were no other complications except local back pain or headache. In this study, the needle design did not affect the frequency of PDPH. Also, PDPH was common, occurring in 33% cases and caused a considerable amount of disturbance in daily activities. Seeking help for this condition was insufficient and only part of these PDPH patients were treated with epidural blood patch. (+info)Gender and post-dural puncture headache. (2/32)
Gender is believed to be an independent risk factor for the development of post-dural puncture headache, but there are some of the inconsistencies in the available data. This systematic review examined a total of 18 trials (2,163 males, 1,917 females). The odds of developing a post-dural puncture headache were significantly lower for male than nonpregnant female subjects (odds ratio = 0.55; 95% confidence interval, 0.44-0.67). Although the authors found that nonpregnant female subjects seem to have a higher incidence of post-dural puncture headache than males, the etiology behind these findings is not clear from the current meta-analysis. (+info)Post lumbar puncture headache: diagnosis and management. (3/32)
Lumbar puncture is a frequently performed procedure in medical emergencies and anaesthesia. Headache after lumbar puncture is a common occurrence (32%) and carries a considerable morbidity, with symptoms lasting for several days, at times severe enough to immobilize the patient. If untreated, it can result in serious complications such as subdural haematoma and seizures, which could be fatal. Certain factors contribute to the development of headache after lumbar puncture. If these factors are taken into consideration, the incidence of headache could be markedly reduced. It is therefore important that the doctors are aware of the methods available for reducing the incidence of headaches after lumbar puncture. On the other hand, there are several misconceptions that are thought to decrease the incidence of headaches with no scientific basis. This article reviews the scientific literature and highlights the practical issues involved in the diagnosis and management of headaches after lumbar puncture, including the epidural blood patch treatment. (+info)Non-surgical management of intracranial subdural hematoma complicating spinal anesthesia. (4/32)
We report the case of a 29 year-old woman who presented a symptomatic intracranial subdural hematoma developing shortly after spinal anesthesia. The patient was fully conscious at clinical onset, and thus we treated her conservatively with an epidural autologous blood patch and close neurological observation. Given the clinical improvement the possibility of surgery was discauded in agreement with the neurosurgical team. Most cases of subdural hematoma appearing after spinal anesthesia are treated with surgery. In the present case the subdural hemorrhage was detected at our hospital 20 days after the anesthetic procedure, and given the excellent state of consciousness, we choosed a conservative management. (+info)Acute spinal pain during an attempted lumbar epidural blood patch in congenital lumbar spinal stenosis and epidural lipomatosis. (5/32)
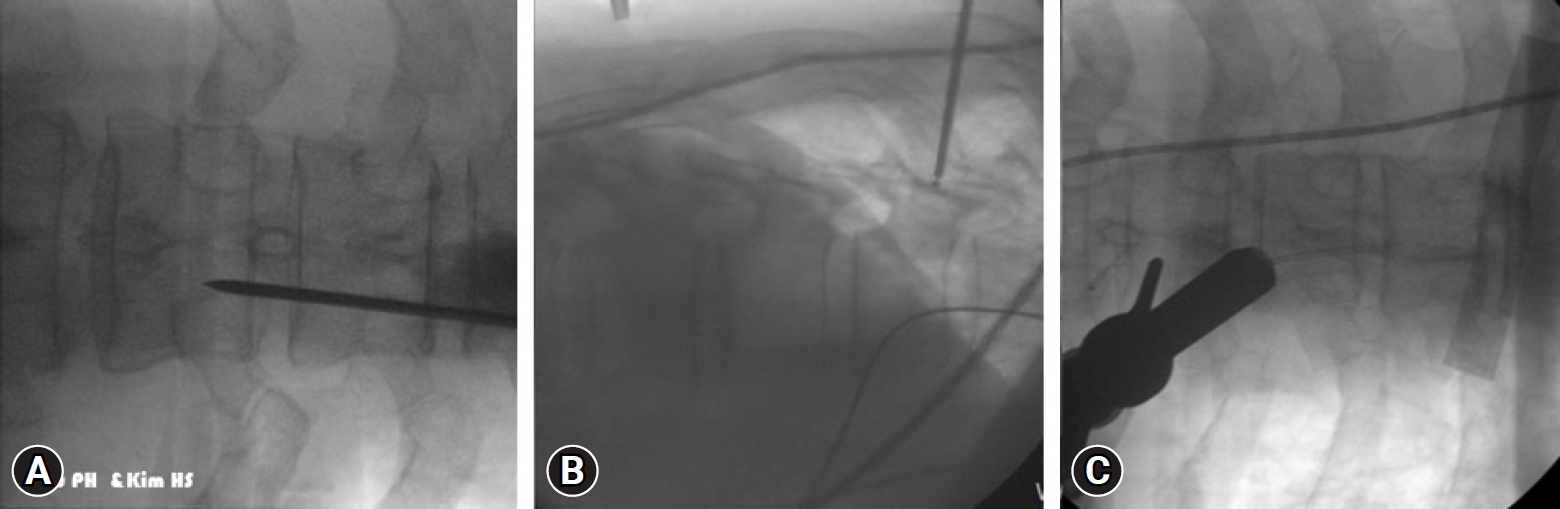
Congenital lumbar spinal stenosis is an uncommon condition that is often asymptomatic in young adults. Herein, we document the first reported occurrence of acute radicular back pain and associated congenital lumbar spinal stenosis in a healthy 24-year-old woman undergoing an epidural blood patch for treatment of a post-dural puncture headache related to an accidental dural puncture sustained during placement of a labor epidural catheter. The acute pain symptoms were elicited twice with injection of less than 1 mL of fluid into the epidural space during the fluoroscopically assisted epidural blood patch. Subsequent magnetic resonance imaging of the lumbar spine demonstrated shortened pedicle length consistent with severe congenital lumbar spinal stenosis and prominent epidural fat. We speculate that the transient increase in pressure within the epidural compartment following injection of a small amount of fluid could have compressed neural structures resulting in severe radicular pain. The prominent epidural fat could have prevented rapid disbursement of the injected fluid which could have further served to propagate the pressure increase throughout the epidural compartment. The unique radiographic features of congenital spinal stenosis could predispose some patients with this unrecognized condition to develop acute pain upon injection of a small amount of fluid into the epidural compartment. Unrecognized congenital lumbar spinal stenosis is an important addition to the differential diagnosis of acute radicular pain elicited during an epidural blood patch in previously asymptomatic patients. (+info)Subdural hematoma following spinal cord stimulator implant. (6/32)
Headache following interventional procedures is a diagnostic challenge due to the multitude of possible etiologies involved. Presentation can be simple (PDPH alone) or complex (exacerbation of pre-existing chronic headache along with PDPH) or headache associated with a new onset intracranial process. Subdural hematoma is a rare complication of cranio-spinal trauma. Cranial subdural hematoma may present in an acute, sub-acute, or chronic fashion. Diagnosis of a subdural hematoma in the wake of a PDPH is difficult, requiring a high level of suspicion. Delayed diagnosis of subdural hematoma is usually related to failure to consider it in the differential diagnosis. Thorough history, assessment of the evolution of symptoms, and imaging studies may identify the possible cause and help direct treatment. Change in the character of initial presenting symptoms may be a sign of resolution of the headache or the onset of a secondary process. We report a case of acute intracranial subdural hematoma secondary to unintentional dural puncture during placement of a permanent spinal cord stimulator lead for refractory angina. There is need for careful follow-up of patients with a known post-dural tear. Failure to identify uncommon adverse events in patients with complicated spinal cord stimulator implantation may lead to permanent injury. (+info)Unusually early onset of post-dural puncture headache after spinal anaesthesia using a 27G Whittacre needle. (7/32)
(+info)Post-epidural headache: how late can it occur? (8/32)
(+info)Post-dural puncture headache (PDPH) is a type of headache that can occur following a procedure where the dura mater, the outer layer of the meninges that surrounds the brain and spinal cord, is punctured. This most commonly occurs during lumbar punctures (spinal taps), epidural anesthesia or central line placements.
The headache is typically described as a positional headache, meaning it worsens with sitting upright or standing and improves with lying down. The exact cause of PDPH is not fully understood, but it's thought to be due to the loss of cerebrospinal fluid (CSF) that cushions the brain and spinal cord. This leads to traction on pain-sensitive structures in the head and neck.
PDPH usually begins within 48 hours of the procedure, but can sometimes occur up to five days later. In addition to positional headache, symptoms may include nausea, vomiting, neck stiffness, photophobia (light sensitivity), tinnitus (ringing in the ears), and hearing loss. The headache usually resolves on its own within a few days or weeks, but in some cases, it can last for months or even become chronic. Treatment options include hydration, caffeine, analgesics, and in some refractory cases, an epidural blood patch.
A blood patch, epidural is a medical procedure used to treat a post-dural puncture headache (PDPH), which can occur after a lumbar puncture or spinal anesthesia. During the procedure, a small amount of the patient's own blood is withdrawn and injected into the epidural space, forming a clot that seals the dural tear and alleviates the headache.
The blood patch procedure involves several steps:
1. The patient is typically placed in a lateral decubitus position (lying on their side) to widen the intervertebral space.
2. The area is cleaned and prepared for the injection, similar to other sterile procedures.
3. Using a local anesthetic, the skin and underlying tissues are numbed to minimize discomfort during the procedure.
4. A thin needle is inserted into the epidural space, usually at the same level as the original dural puncture.
5. Once the needle is in the correct position, a small amount of blood (usually around 10-20 mL) is drawn from a vein in the patient's arm.
6. The withdrawn blood is then slowly injected into the epidural space through the needle.
7. After the injection, the needle is removed, and the patient is monitored for any adverse reactions or complications.
The clot formed by the injected blood helps to seal the dural tear, preventing cerebrospinal fluid (CSF) from leaking into the epidural space and causing a headache. The blood patch procedure typically provides rapid relief from PDPH, with most patients experiencing significant improvement within 30 minutes to an hour after the injection. However, in some cases, multiple blood patches may be required to achieve complete resolution of the headache.
A spinal puncture, also known as a lumbar puncture or a spinal tap, is a medical procedure in which a thin, hollow needle is inserted between two vertebrae in the lower back to extract cerebrospinal fluid (CSF) from the subarachnoid space. This procedure is typically performed to diagnose conditions affecting the central nervous system, such as meningitis, encephalitis, or subarachnoid hemorrhage, by analyzing the CSF for cells, chemicals, bacteria, or viruses. Additionally, spinal punctures can be used to administer medications or anesthetics directly into the CSF space, such as in the case of epidural anesthesia during childbirth.
The medical definition of a spinal puncture is: "A diagnostic and therapeutic procedure that involves introducing a thin needle into the subarachnoid space, typically at the lumbar level, to collect cerebrospinal fluid or administer medications."
A headache is defined as pain or discomfort in the head, scalp, or neck. It can be a symptom of various underlying conditions such as stress, sinus congestion, migraine, or more serious issues like meningitis or concussion. Headaches can vary in intensity, ranging from mild to severe, and may be accompanied by other symptoms such as nausea, vomiting, or sensitivity to light and sound. There are over 150 different types of headaches, including tension headaches, cluster headaches, and sinus headaches, each with their own specific characteristics and causes.
Dura Mater is the thickest and outermost of the three membranes (meninges) that cover the brain and spinal cord. It provides protection and support to these delicate structures. The other two layers are called the Arachnoid Mater and the Pia Mater, which are thinner and more delicate than the Dura Mater. Together, these three layers form a protective barrier around the central nervous system.
In the context of medicine, "needles" are thin, sharp, and typically hollow instruments used in various medical procedures to introduce or remove fluids from the body, administer medications, or perform diagnostic tests. They consist of a small-gauge metal tube with a sharp point on one end and a hub on the other, where a syringe is attached.
There are different types of needles, including:
1. Hypodermic needles: These are used for injections, such as intramuscular (IM), subcutaneous (SC), or intravenous (IV) injections, to deliver medications directly into the body. They come in various sizes and lengths depending on the type of injection and the patient's age and weight.
2. Blood collection needles: These are used for drawing blood samples for diagnostic tests. They have a special vacuum-assisted design that allows them to easily penetrate veins and collect the required amount of blood.
3. Surgical needles: These are used in surgeries for suturing (stitching) wounds or tissues together. They are typically curved and made from stainless steel, with a triangular or reverse cutting point to facilitate easy penetration through tissues.
4. Acupuncture needles: These are thin, solid needles used in traditional Chinese medicine for acupuncture therapy. They are inserted into specific points on the body to stimulate energy flow and promote healing.
It is essential to follow proper infection control procedures when handling and disposing of needles to prevent the spread of bloodborne pathogens and infectious diseases.
Spinal anesthesia is a type of regional anesthesia that involves injecting local anesthetic medication into the cerebrospinal fluid in the subarachnoid space, which is the space surrounding the spinal cord. This procedure is typically performed by introducing a needle into the lower back, between the vertebrae, to reach the subarachnoid space.
Once the local anesthetic is introduced into this space, it spreads to block nerve impulses from the corresponding levels of the spine, resulting in numbness and loss of sensation in specific areas of the body below the injection site. The extent and level of anesthesia depend on the amount and type of medication used, as well as the patient's individual response.
Spinal anesthesia is often used for surgeries involving the lower abdomen, pelvis, or lower extremities, such as cesarean sections, hernia repairs, hip replacements, and knee arthroscopies. It can also be utilized for procedures like epidural steroid injections to manage chronic pain conditions affecting the spine and lower limbs.
While spinal anesthesia provides effective pain relief during and after surgery, it may cause side effects such as low blood pressure, headache, or difficulty urinating. These potential complications should be discussed with the healthcare provider before deciding on this type of anesthesia.
Epidural analgesia is a type of regional anesthesia used to manage pain, most commonly during childbirth and after surgery. The term "epidural" refers to the location of the injection, which is in the epidural space of the spinal column.
In this procedure, a small amount of local anesthetic or narcotic medication is injected into the epidural space using a thin catheter. This medication blocks nerve impulses from the lower body, reducing or eliminating pain sensations without causing complete loss of feeling or muscle movement.
Epidural analgesia can be used for both short-term and long-term pain management. It is often preferred in situations where patients require prolonged pain relief, such as during labor and delivery or after major surgery. The medication can be administered continuously or intermittently, depending on the patient's needs and the type of procedure being performed.
While epidural analgesia is generally safe and effective, it can have side effects, including low blood pressure, headache, and difficulty urinating. In rare cases, it may also cause nerve damage or infection. Patients should discuss the risks and benefits of this procedure with their healthcare provider before deciding whether to undergo epidural analgesia.
Epidural anesthesia is a type of regional anesthesia that involves the injection of local anesthetic medication into the epidural space in the spine, which is the space surrounding the dura mater, a membrane that covers the spinal cord. The injection is typically administered through a catheter placed in the lower back using a needle.
The local anesthetic drug blocks nerve impulses from the affected area, numbing it and relieving pain. Epidural anesthesia can be used for various surgical procedures, such as cesarean sections, knee or hip replacements, and hernia repairs. It is also commonly used during childbirth to provide pain relief during labor and delivery.
The effects of epidural anesthesia can vary depending on the dose and type of medication used, as well as the individual's response to the drug. The anesthetic may take several minutes to start working, and its duration of action can range from a few hours to a day or more. Epidural anesthesia is generally considered safe when administered by trained medical professionals, but like any medical procedure, it carries some risks, including infection, bleeding, nerve damage, and respiratory depression.
Obstetrical anesthesia refers to the use of anesthetic techniques and medications during childbirth or obstetrical procedures. The goal is to provide pain relief and comfort to the birthing person while ensuring the safety of both the mother and the baby. There are different types of obstetrical anesthesia, including:
1. Local anesthesia: Injection of a local anesthetic agent to numb a specific area, such as the perineum (the area between the vagina and the anus) during childbirth.
2. Regional anesthesia: Numbing a larger region of the body using techniques like spinal or epidural anesthesia. These methods involve injecting local anesthetic agents near the spinal cord to block nerve impulses, providing pain relief in the lower half of the body.
3. General anesthesia: Using inhaled gases or intravenous medications to render the birthing person unconscious during cesarean sections (C-sections) or other surgical procedures related to childbirth.
The choice of anesthetic technique depends on various factors, including the type of delivery, the mother's medical history, and the preferences of both the mother and the healthcare team. Obstetrical anesthesia requires specialized training and expertise to ensure safe and effective pain management during labor and delivery.
A puncture, in medical terms, refers to a small hole or wound that is caused by a sharp object penetrating the skin or other body tissues. This can result in damage to underlying structures such as blood vessels, nerves, or organs, and may lead to complications such as bleeding, infection, or inflammation.
Punctures can occur accidentally, such as from stepping on a nail or getting pricked by a needle, or they can be inflicted intentionally, such as during medical procedures like injections or blood draws. In some cases, puncture wounds may require medical attention to clean and close the wound, prevent infection, and promote healing.
Obstetrical analgesia refers to the use of medications or techniques to relieve pain during childbirth. The goal of obstetrical analgesia is to provide comfort and relaxation for the mother during labor and delivery while minimizing risks to both the mother and the baby. There are several methods of obstetrical analgesia, including:
1. Systemic opioids: These medications, such as morphine or fentanyl, can be given intravenously to help reduce the pain of contractions. However, they can cause side effects such as drowsiness, nausea, and respiratory depression in the mother and may also affect the baby's breathing and alertness at birth.
2. Regional anesthesia: This involves numbing a specific area of the body using local anesthetics. The two most common types of regional anesthesia used during childbirth are epidural and spinal anesthesia.
a. Epidural anesthesia: A catheter is inserted into the lower back, near the spinal cord, to deliver a continuous infusion of local anesthetic and sometimes opioids. This numbs the lower half of the body, reducing the pain of contractions and allowing for a more comfortable delivery. Epidural anesthesia can also be used for cesarean sections.
b. Spinal anesthesia: A single injection of local anesthetic is given into the spinal fluid, numbing the lower half of the body. This type of anesthesia is often used for cesarean sections and can also be used for vaginal deliveries in some cases.
3. Nitrous oxide: Also known as laughing gas, this colorless, odorless gas can be inhaled through a mask to help reduce anxiety and provide some pain relief during labor. It is not commonly used in the United States but is more popular in other countries.
When choosing an obstetrical analgesia method, it's essential to consider the potential benefits and risks for both the mother and the baby. Factors such as the mother's health, the progression of labor, and personal preferences should all be taken into account when making this decision. It is crucial to discuss these options with a healthcare provider to determine the most appropriate choice for each individual situation.
Headache disorders refer to a group of conditions characterized by recurrent headaches that cause significant distress and impairment in daily functioning. The most common types of headache disorders are tension-type headaches, migraines, and cluster headaches.
Tension-type headaches are typically described as a dull, aching sensation around the head and neck, often accompanied by tightness or pressure. Migraines, on the other hand, are usually characterized by moderate to severe throbbing pain on one or both sides of the head, often accompanied by nausea, vomiting, sensitivity to light and sound, and visual disturbances.
Cluster headaches are relatively rare but extremely painful, with attacks lasting from 15 minutes to three hours and occurring several times a day for weeks or months. They typically affect one side of the head and are often accompanied by symptoms such as redness and tearing of the eye, nasal congestion, and sweating on the affected side of the face.
Headache disorders can have a significant impact on quality of life, and effective treatment often requires a multidisciplinary approach that may include medication, lifestyle changes, and behavioral therapies.
The epidural space is the potential space located outside the dura mater, which is the outermost of the three membranes covering the brain and spinal cord (the meninges). This space runs the entire length of the spinal canal and contains fatty tissue, blood vessels, and nerve roots. It is often used as a route for administering anesthesia during childbirth or surgery, as well as for pain management in certain medical conditions. The injection of medications into this space is called an epidural block.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
Vertigo is a specific type of dizziness characterized by the sensation that you or your surroundings are spinning or moving, even when you're perfectly still. It's often caused by issues with the inner ear or the balance-sensing systems of the body. Vertigo can be brought on by various conditions, such as benign paroxysmal positional vertigo (BPPV), labyrinthitis, vestibular neuritis, Meniere's disease, and migraines. In some cases, vertigo may also result from head or neck injuries, brain disorders like stroke or tumors, or certain medications. Treatment for vertigo depends on the underlying cause and can include specific exercises, medication, or surgery in severe cases.
The scalp is the anatomical region located at the upper part of the human head, covering the skull except for the face and the ears. It is made up of several layers: the skin, the connective tissue, the galea aponeurotica (a strong, flat, tendinous sheet), loose areolar tissue, and the periosteum (the highly vascularized innermost layer that attaches directly to the skull bones). The scalp has a rich blood supply and is home to numerous sensory receptors, including those for touch, pain, and temperature. It also contains hair follicles, sebaceous glands, and sweat glands.
"Access to information," in a medical context, refers to the ability of individuals, patients, healthcare providers, and researchers to obtain, request, and disseminate health-related data, records, research findings, and other important information. This includes access to personal medical records, clinical trial results, evidence-based practices, and public health statistics.
Promoting access to information is crucial for informed decision-making, ensuring transparency, advancing medical research, improving patient care, and enhancing overall healthcare system performance. Various laws, regulations, and policies at the local, national, and international levels aim to protect and facilitate access to information while balancing privacy concerns, data security, and intellectual property rights.
The Journal Impact Factor (JIF) is a measure of the frequency with which the "average article" in a journal has been cited in a particular year. It is calculated by dividing the number of current year citations to the source items published in that journal during the previous two years. For example, if a journal has an Impact Factor of 3 in 2020, that means articles published in 2018 and 2019 were cited 3 times on average in 2020. It is used to gauge the importance or rank of a journal by comparing the times it's articles are cited relative to other journals in the field. However, it has been criticized for various limitations such as being manipulated by editors and not reflecting the quality of individual articles.
A "periodical" in the context of medicine typically refers to a type of publication that is issued regularly, such as on a monthly or quarterly basis. These publications include peer-reviewed journals, magazines, and newsletters that focus on medical research, education, and practice. They may contain original research articles, review articles, case reports, editorials, letters to the editor, and other types of content related to medical science and clinical practice.
As a "Topic," periodicals in medicine encompass various aspects such as their role in disseminating new knowledge, their impact on clinical decision-making, their quality control measures, and their ethical considerations. Medical periodicals serve as a crucial resource for healthcare professionals, researchers, students, and other stakeholders to stay updated on the latest developments in their field and to share their findings with others.
Peer review in the context of research refers to the evaluation of scientific, academic, or professional work by others working in the same field. The purpose of peer review is to ensure that the research is rigorous, valid, and relevant to the field. In a peer-review process, experts in the relevant field assess the research article, report, or other type of scholarly work for its accuracy, quality, and significance before it is published or presented at a conference.
The peer-review process typically involves several stages:
1. Submission: The author(s) submit their manuscript to a journal, conference, or other publication venue.
2. Assignment: The editor of the publication assigns the manuscript to one or more reviewers who are experts in the field.
3. Review: The reviewers evaluate the manuscript based on criteria such as originality, methodology, data analysis, interpretation of results, and contribution to the field. They provide feedback and recommendations to the editor.
4. Decision: Based on the feedback from the reviewers, the editor makes a decision about whether to accept, reject, or request revisions to the manuscript.
5. Revision: If the manuscript is rejected or requires revisions, the author(s) may have an opportunity to revise and resubmit the manuscript for further consideration.
Peer review is a critical component of the scientific process, as it helps ensure that research is held to high standards of quality and integrity. It also provides a mechanism for identifying and correcting errors or weaknesses in research before it is published or disseminated widely.
I'm sorry for any confusion, but "publishing" is not a term that has a medical definition. Publishing typically refers to the process of preparing and disseminating information, such as books, journals, or articles, to the public or a specific audience. It could involve both print and digital media. If you have any questions related to medicine or healthcare, I'd be happy to try to help answer those!
Anesthesiology is a medical specialty concerned with providing anesthesia, which is the loss of sensation or awareness, to patients undergoing surgical, diagnostic, or therapeutic procedures. Anesthesiologists are responsible for administering various types of anesthetics, monitoring the patient's vital signs during the procedure, and managing any complications that may arise. They also play a critical role in pain management before, during, and after surgery, as well as in the treatment of chronic pain conditions.
Anesthesiologists work closely with other medical professionals, including surgeons, anesthetists, nurses, and respiratory therapists, to ensure that patients receive the best possible care. They must have a thorough understanding of human physiology, pharmacology, and anatomy, as well as excellent communication skills and the ability to make quick decisions under high pressure.
The primary goal of anesthesiology is to provide safe and effective anesthesia that minimizes pain and discomfort while maximizing patient safety and comfort. This requires a deep understanding of the risks and benefits associated with different types of anesthetics, as well as the ability to tailor the anesthetic plan to each individual patient's needs and medical history.
In summary, anesthesiology is a critical medical specialty focused on providing safe and effective anesthesia and pain management for patients undergoing surgical or other medical procedures.
Isoflurane is a volatile halogenated ether used for induction and maintenance of general anesthesia. It is a colorless liquid with a pungent, sweet odor. Isoflurane is an agonist at the gamma-aminobutyric acid type A (GABAA) receptor and inhibits excitatory neurotransmission in the brain, leading to unconsciousness and immobility. It has a rapid onset and offset of action due to its low blood solubility, allowing for quick adjustments in anesthetic depth during surgery. Isoflurane is also known for its bronchodilator effects, making it useful in patients with reactive airway disease. However, it can cause dose-dependent decreases in heart rate and blood pressure, so careful hemodynamic monitoring is required during its use.
 Post-dural-puncture headache
Post-dural-puncture headache
Theophylline
Epidural blood patch
Causes of cancer pain
Cerebrospinal fluid
Pterygopalatine ganglion
Epidural administration
Sumatriptan
Cerebrospinal fluid leak
Combined spinal and epidural anaesthesia
Caesarean section
Cancer pain
Spinal anaesthesia
Lumbar puncture
Nusinersen
Spinal cord stimulator
NIH classification of headaches
List of MeSH codes (C10)
Orthostatic headache
International Classification of Headache Disorders
Intracranial hemorrhage
Cerebral angiography
Postpartum psychosis
Dura mater
Meningitis
Post-dural-puncture headache - Wikipedia
 Neostigmine and atropine as a treatment for Postdural Puncture Headache after spinal anesthesia in cesarean section: A Case...
Neostigmine and atropine as a treatment for Postdural Puncture Headache after spinal anesthesia in cesarean section: A Case...
Postdural puncture headache<...
 Management of post dural puncture headache Screening | Belfast Health & Social Care Trust website
Management of post dural puncture headache Screening | Belfast Health & Social Care Trust website
 Trans-nasal sphenopalatine ganglion block for post-dural puncture headache management: a meta-analysis of randomized trials |...
Trans-nasal sphenopalatine ganglion block for post-dural puncture headache management: a meta-analysis of randomized trials |...
 Treatment of post-dural puncture headache using epidural injection of fibrin sealant as an alternative to autologous epidural...
Treatment of post-dural puncture headache using epidural injection of fibrin sealant as an alternative to autologous epidural...
 Factors Predisposing to Postdural Puncture Headache after Spinal Anaesthesia among Elective Caesarean Section Patients at Thika...
Factors Predisposing to Postdural Puncture Headache after Spinal Anaesthesia among Elective Caesarean Section Patients at Thika...
 Obstetrics - ProProfs Quiz
Obstetrics - ProProfs Quiz
 Caffeine Uptake into the Vitreous after Peroral Coffee Consumption | Ophthalmic Research | Karger Publishers
Caffeine Uptake into the Vitreous after Peroral Coffee Consumption | Ophthalmic Research | Karger Publishers
 5th ESRA Residents & Trainees Workshop - ESRA
5th ESRA Residents & Trainees Workshop - ESRA
 Randomised controlled trial of atraumatic versus standard needles for diagnostic lumbar puncture | The BMJ
Randomised controlled trial of atraumatic versus standard needles for diagnostic lumbar puncture | The BMJ
 Claes Möller - Institutionen för hälsovetenskaper - Örebro universitet
Claes Möller - Institutionen för hälsovetenskaper - Örebro universitet
Internet Scientific Publications
Drug Summary
 Magiran | جستجوی کلیدواژه «Orthopedics»
Magiran | جستجوی کلیدواژه «Orthopedics»
 LAVENDER: Overview, Uses, Side Effects, Precautions, Interactions, Dosing and Reviews
LAVENDER: Overview, Uses, Side Effects, Precautions, Interactions, Dosing and Reviews
![がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAAC0klEQVQ4jcWTzWscZQDGf+/7zuzMZPY72W6baEIlmGD8KkSKVK1FUfxCEKkHMZeCUBAvgr0pFUFPimChqAcpFIuKIHjxJkEvCmporajZbtpkTbr5aJLdnZ2dmfd9PRRs7x58/oAfv4eHB/7vCAC7MQ+N96H+FMQtKEwD+ERXXmZo/+dEjTV+OgGP/yiwqRUjh/4FOPZToPkReHtA+XfgFGeQwTy9xVkGa69hTR2neI77T99HvPQNjte2+g+EmrpuYK29brJ85hmyzpNEzZcQqonuj2D6dXLlayjRxyldoHrwBOVHF9AXrHDuAkByVEDryzKD9QNEjRfRnQCzM0PO1CkWoKgqVMMqo8MrFNrHMT/UEN0bFfjgq8Ok6w8jdo/hk8ctgOehXUWiLD2hGfJCHbjyXiF4AzG+ib16E0D4P5Mftih/HLF9EDfndLk21ehusBWlQJ7by5Nnfa/4ZhwX1wL/d6B6EyDsdAj3r2B7p1ATpwY6mWtuL41cjcOyNsJ6Koy2k8rfteyhrcBZzZFNJCjvxoxrSYOaWEXSA+dueWm3caux3pFuuv5qX+8ERXfP2Xxu9Ot99q8DCl1M4osf9itHcUUesEhho0A6h+SfAwukxtjB5cnS7JkhN/9K4OTPV/zRb8fy078txpeeWx6sDBaRuITerr5C32wiLsffP5aY6Alp3Y83k6WLY94scRbRzdYLFvN23qm9lZro6Yzuu54sPe/mTGCtOVJ0xt8zNi05EvlLZuOTme48W1B7Twaq/JkQIhHSxL1sc0tK7W9HG3dmxGaiMLY30qvvONJ1d/XytECeV3OvH44CVU5SE88Zmz2obTbf6v+6vBovmErulgcMSSvL5EKgStHAdqa6WfsRhA6VVEoK9xNZz81QdW/7IifDc8amtZ2kdTqUtWP3hHM5KUXbke6+kj+cIvR4O2oe7+ktT5M1AznyQtWZ/O4/v/EfNE86A/msCDkAAAAASUVORK5CYII=) がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain
がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain
Articles online first - Minerva Medica - Journals
 Meredith Barad, MD | Stanford Medicine
Meredith Barad, MD | Stanford Medicine
 Nate Mercaldo's Publications - MGH Institute for Technology Assessment
Nate Mercaldo's Publications - MGH Institute for Technology Assessment
 A-Z fact sheets | The Royal Women's Hospital
A-Z fact sheets | The Royal Women's Hospital
 Milestone Scientific Reports Ninth Published Study Reinforcing Efficacy of CompuFlo(R) Epidural Instrument as an Objective Tool...
Milestone Scientific Reports Ninth Published Study Reinforcing Efficacy of CompuFlo(R) Epidural Instrument as an Objective Tool...
Atraumatic lumbar puncture needles are associated with fewer complications than conventional needles | ADC Education & Practice...
 E-CONGRES ESRA
- Détails de l'Evenement
E-CONGRES ESRA
- Détails de l'Evenement
UMEM Educational Pearls - University of Maryland School of Medicine, Department of Emergency Medicine
E-CONGRES ESRA
- Détails de l'Evenement
During your anaesthetic - ASA
 Biologics
Biologics
 Journal of Anesthesia and Patient Care | Open Access Journal | Annex Publishers
Journal of Anesthesia and Patient Care | Open Access Journal | Annex Publishers
PDPH14
- Post-dural-puncture headache (PDPH) is a complication of puncture of the dura mater (one of the membranes around the brain and spinal cord). (wikipedia.org)
- PDPH is a common side effect of lumbar puncture and spinal anesthesia. (wikipedia.org)
- PDPH is estimated to occur in between 0.1% and 36% people following dural puncture. (wikipedia.org)
- PDPH typically occurs hours to days after puncture and presents with symptoms such as headache (which is mostly bi-frontal or occipital) and nausea that typically worsen when the patient assumes an upright posture. (wikipedia.org)
- However, the evidence that atraumatic needles reduce the risk of post-dural puncture headache (PDPH) without increasing adverse events such as paraesthesia or backache is moderate-quality and further research should be done. (wikipedia.org)
- PDPH is roughly twice as common in lumbar puncture than spinal anaesthesia, almost certainly due to the atraumatic needles used in spinal anaesthesia. (wikipedia.org)
- Background Post dural puncture headache (PDPH) is an iatrogenic cause of patient morbidity in pain management after spinal or epidural anaesthesia, as well as after diagnostic lumbar puncture. (utoledo.edu)
- To evaluate the efficacy and safety of trans-nasal Sphenopalatine Ganglion (SPG) block over other treatments for Post-Dural Puncture Headache (PDPH) management. (bvsalud.org)
- Postdural puncture headache (PDPH) is a common complication following spinal anaesthesia for Caesarean section (CS). (journalajmah.com)
- The study aimed to investigate the incidence and factors predisposing patients to PDPH after a dural puncture during a planned Caesarean section under spinal anaesthesia at Thika Level 5 Hospital, Kenya. (journalajmah.com)
- Patient factors (age, BMI, bed rest, and previous history of PDPH), healthcare provider factors (qualification, experience, and the number of dural punctures), and equipment factors (size, design, and spinal needle orientation) were evaluated to determine predisposing factors for PDPH. (journalajmah.com)
- Kassa A, Beyen T, Zenu Z. Post dural puncture headache (PDPH) and associated factors after spinal anaesthesia among patients in the university of Gondar referral and teaching hospital, Gondar, North West Ethiopia. (journalajmah.com)
- Although placing an epidural catheter can be technically challenging in obese patients, the incidence of PDPH following dural puncture is decreased. (proprofs.com)
- Post-dural puncture headache (PDPH) is one of the most frequent complications of neuraxial anesthesia and analgesia. (annexpublishers.co)
Incidence12
- Incidence and risk factors of postdural puncture headache: Prospective cohort study design. (journalajmah.com)
- To compare the ease of use of atraumatic needles with standard needles for diagnostic lumbar puncture and the incidence of headache after their use. (bmj.com)
- The primary end point was intention to treat analysis of incidence of moderate to severe headache, assessed at one week by telephone interview. (bmj.com)
- Secondary end points were incidence of headache at one week analysed by needle type, ease of use by operator according to a visual analogue scale, incidence of backache, and failure rate of puncture. (bmj.com)
- Higher body mass index was associated with an increased failure rate with atraumatic needles, but the reduced incidence of headache was maintained. (bmj.com)
- Atraumatic needles significantly reduced the incidence of moderate to severe headache and the need for medical interventions after diagnostic lumbar punctures, but they were associated with a higher failure rate than standard needles. (bmj.com)
- 4 5 Atraumatic ("blunt") needles have been in clinical use since the 1950s, principally in anaesthetic practice, where there is substantial evidence of a reduced incidence of headache and other neurological complications after their use. (bmj.com)
- The incidence of headache after spinal anaesthesia is typically half that after diagnostic lumbar puncture. (bmj.com)
- We aimed to compare the incidence of headache with atraumatic and standard needles and to evaluate technical difficulties. (bmj.com)
- Data suggest an inverse linear relation between needle gauge and headache incidence, and some authors recommend using a 22-gauge needle regardless of what size needle is supplied with the kit. (medscape.com)
- Postdural-puncture headache incidence dropped significantly from 11.0% in the conventional needle group to 4.2% in the atraumatic group. (medscape.com)
- Lumbar puncture success on the first attempt, failure rate, average number of attempts, and incidence of traumatic tap and backache were similar with the two needle types. (medscape.com)
Accidental dural puncture3
- it has not been studied for accidental dural puncture with a large bore needle. (uky.edu)
- Easier identification of the epidural space is essential to reducing the number of epidural attempts and risk of accidental dural puncture. (milestonescientific.com)
- As reported in the article, accidental dural puncture is particularly troublesome in the obstetric population as more than half of all patients who experience accidental dural puncture with epidural needles may eventually develop a post-dural puncture headache 1 . (milestonescientific.com)
Obstetric patients2
- Mohammed AD, Ayyuba R, Salisu I, Nagoma AU, Owolabi LF, Ibrahim A. An analysis of post-dural puncture headache in obstetric patients: A study from Kano, Nigeria. (journalajmah.com)
- Which of the following obstetric patients has the lowest risk for post-dural puncture headache? (proprofs.com)
Lumbar punctures2
- Headache due to a reduced volume of cerebrospinal fluid and reduced pressure complicates a substantial proportion of lumbar punctures. (bmj.com)
- The answer to the question, 'Are atraumatic needles better for lumbar punctures? (medscape.com)
Needles7
- Standardised protocol for lumbar puncture with 20 gauge atraumatic or standard needles. (bmj.com)
- Spinal anaesthesia and myelography differ from diagnostic lumbar puncture because smaller gauge needles are used, smaller volumes of cerebrospinal fluid are removed, and other fluids can be introduced. (bmj.com)
- 2 6 Despite evidence that relevant physical characteristics of atraumatic needles, such as flow rates, are comparable to those of standard needles, 6 there are limited data on their benefit in diagnostic lumbar puncture. (bmj.com)
- 7-9 The Cochrane Collaboration has identified only two methodologically adequate studies of atraumatic needles for diagnostic lumbar puncture (C Sudlow, personal communication). (bmj.com)
- NEW YORK (Reuters Health) - Atraumatic lumbar puncture needles are safe and effective, and they cause fewer postdural-puncture headaches and returns to the hospital for additional treatment, according to a systematic review and meta-analysis. (medscape.com)
- As they report in The Lancet, online December 6, Dr. Almenawer and colleagues conducted a systematic review and meta-analysis to compare patient outcomes after lumbar puncture with atraumatic needles versus conventional needles. (medscape.com)
- The researchers searched 13 databases with no language restrictions from inception to Aug 15, 2017, for randomized controlled trials comparing the use of atraumatic needles and conventional needles for any lumbar puncture indication. (medscape.com)
Complication3
- PURPOSE OF REVIEW: Postdural puncture headache remains the most frequent complication of neuraxial anesthesia. (uky.edu)
- Especially the frequency of post-lumbar puncture headache will decrease, and the number of hospital readmissions or epidural blood patches for this complication will be strongly reduced," added Dr. Brouwer, who co-wrote an editorial about the study. (medscape.com)
- Iatrogenic meningitis is a well-documented complication of lumbar puncture and carries an estimated mortality of ~35% extrapolated from a US data review ( 8 ). (cdc.gov)
Complications3
- 1-3 In the 1920s Greene hypothesised that complications could be reduced by using a smaller, tapered needle with a blunt tip, which would separate rather than cut dural fibres and thus reduce fluid leakage. (bmj.com)
- This should change clinical practice and result in fewer patients with lumbar puncture complications. (medscape.com)
- the patient showed no signs of complications immediately post-procedure and was discharged after 4 hours of observation. (cdc.gov)
Anesthesia1
- It can occur following uncomplicated spinal anesthesia as well as unintended dural puncture during epidural anesthesia. (uky.edu)
Current Pain and Headache Reports1
- Current Pain and Headache Reports. (psu.edu)
Cerebrospinal fluid4
- The most promising is an intrathecal catheter as it avoids further dural puncture and seals the hole during the time it is in place, decreasing cerebrospinal fluid loss. (uky.edu)
- We excluded patients with a history of chronic headache requiring analgesics and those with known or suspected idiopathic intracranial hypertension or other causes of an increased cerebrospinal fluid pressure. (bmj.com)
- Lumbar puncture is a procedure that is often performed in the emergency department to obtain information about the cerebrospinal fluid (CSF). (medscape.com)
- Isolated disk edema (eg, caused by optic neuritis or ischemic optic neuropathy) without the retinal findings indicative of elevated cerebrospinal fluid pressure is not considered papilledema (unless the intracranial pressure is elevated on concurrent lumbar puncture). (msdmanuals.com)
Diagnostic4
- 116 patients requiring elective diagnostic lumbar puncture. (bmj.com)
- Previous studies of diagnostic lumbar puncture have potentially been confounded by comparing different needle gauges, failing to define the operators' previous experience or the length of follow up, and not addressing technical difficulties. (bmj.com)
- We considered as eligible for our study all patients attending the investigation ward of a regional neurology unit for elective diagnostic lumbar puncture between September 1998 and February 1999. (bmj.com)
- Most cases occur after catheter insertion or injection into the intrathecal space, but infection related to diagnostic lumbar puncture is less common. (cdc.gov)
Neurologic2
- Lumbar puncture should be performed only after a neurologic examination but should never delay potentially life-saving interventions, such as the administration of antibiotics and steroids to patients with suspected bacterial meningitis. (medscape.com)
- Neuroimaging is not necessary in patients with a history of recurrent migraine headaches and a normal neurologic examination. (medscape.com)
Severe headache1
- The patient came to the emergency department within 18 hours of the procedure after onset of confusion, severe headache, neck pain, nausea, vomiting, and fever. (cdc.gov)
Procedure1
- Lumbar puncture is an extremely common procedure, and the strong results from this study call for switching the type of needle. (medscape.com)
Patients2
- Patients may have symptoms of increased intracranial pressure, such as headache or nausea and vomiting. (msdmanuals.com)
- Don't perform neuroimaging studies in patients with stable headaches that meet criteria for migraine. (medscape.com)
Intravenous1
- Subgroup analyses of postdural-puncture headache showed no interactions between needle type and patient sex, age, position, bed rest after puncture, needle gauge, indication for lumbar puncture, use of intravenous fluid, or clinician specialty. (medscape.com)
Risk3
- Conclusion We successfully treated the post dural puncture headache and avoided the risk of viral seeding of the meninges by using a fibrin sealant. (utoledo.edu)
- Risk factors of post-dural puncture headache receiving a blood-patch in the obstetric patient. (annexpublishers.co)
- The smaller the needle used for the lumbar puncture, the lower the risk that the patient will experience a post-lumbar puncture headache. (medscape.com)
Intracranial1
- citation needed] Although in very rare cases the headache may present immediately after a puncture, this is almost always due to another cause such as increased intracranial pressure and requires immediate attention. (wikipedia.org)
Posture1
- Posture and fluids for preventing post‐ dural puncture headache. (journalajmah.com)
Migraine4
- p class=\'abstract\'>Migraine headaches are among the most prevalent and disabling pain conditions worldwide. (stanford.edu)
- Migraine is a complex disorder characterized by recurrent episodes of headache, most often unilateral and in some cases associated with visual or sensory symptoms-collectively known as an aura-that arise most often before the head pain but that may occur during or afterward (see the image below). (medscape.com)
- Selection of laboratory and/or imaging studies to rule out conditions other than migraine headache is determined by the individual presentation (eg, erythrocyte sedimentation rate and C-reactive protein levels may be appropriate to exclude temporal/giant cell arteritis). (medscape.com)
- The American Headache Society released a list of 5 commonly performed tests or procedures that are not always necessary in the treatment of migraine and headache, as part of the American Board of Internal Medicine (ABIM) Foundation's Choosing Wisely campaign. (medscape.com)
Trials1
- They excluded randomized trials in which no dural puncture was performed (epidural injections) and those without a conventional needle control group. (medscape.com)
Occur1
- The headache usually occurs 24-48 hours after puncture but may occur as many as 12 days after. (wikipedia.org)
Patient1
- This patient reported that these visual auras preceded her headache by 20-30 minutes. (medscape.com)
Subsequent2
- Compliance with the provisions in this LCD may be monitored and addressed through post payment data analysis and subsequent medical review audits. (cms.gov)
- Diagnosis is by ophthalmoscopy with further tests, usually brain imaging and sometimes subsequent lumbar puncture, to determine cause. (msdmanuals.com)
Treatment1
- My current research interests involve novel treatment paradigms for challenging pain problems such as orofacial pain, trigeminal neuralgia and low pressure headaches. (stanford.edu)
Body mass1
- Serbulent GB, Tolga E, Aykut S, Fath S, Ali MU, Ali E, Burcu D. The interrelation between body mass index and post-dural puncture headache in parturient women. (journalajmah.com)
Emergency1
- Don't perform computed tomography imaging for headache when magnetic resonance imaging is available, except in emergency settings. (medscape.com)
Pain2
- Dr. Barad is a board-certified Neurologist, Headache and Pain physician. (stanford.edu)
- She has collaborated in creating a cross-disciplinary headache center and is the co-director of the Stanford Orofacial Pain Program. (stanford.edu)