Parathyroid Hormone
Parathyroid Glands
Parathyroid Diseases
Parathyroid Hormone-Related Protein
Receptor, Parathyroid Hormone, Type 1
Receptors, Parathyroid Hormone
Hyperparathyroidism
Mechanism of parathyroid tumourigenesis in uraemia. (1/562)
Clonal analysis has shown that in renal hyperparathyroidism (2-HPT), parathyroid glands initially grow diffusely and polyclonally after which the foci of nodular hyperplasia are transformed to monoclonal neoplasia. There is a great deal of information about genetic abnormalities contributing to the tumourigenesis of parathyroid neoplasia in primary hyperparathyroidism. It is speculated that allelic loss of the MEN1 suppressor gene and overexpression of cyclin D1 induced by rearrangement of the parathyroid hormone gene may be the major genetic abnormality in sporadic parathyroid adenoma but not in 2-HPT. The pathogenesis of 2-HPT, abnormality of the Ca2+-sensing receptor (CaR) gene and the vitamin D receptor gene may possibly contribute to parathyroid tumourigenesis in 2-HPT. However, this is not yet clear and heterogeneous and multiple genetic abnormalities may be responsible for the progression of secondary parathyroid hyperplasia. (+info)The elevated serum alkaline phosphatase--the chase that led to two endocrinopathies and one possible unifying diagnosis. (2/562)
A 39-year-old Chinese man with hypertension being evaluated for elevated serum alkaline phosphatase (SAP) levels was found to have an incidental right adrenal mass. The radiological features were characteristic of a large adrenal myelolipoma. This mass was resected and the diagnosis confirmed pathologically. His blood pressure normalised after removal of the myelolipoma, suggesting that the frequently observed association between myelolipomas and hypertension may not be entirely coincidental. Persistent elevation of the SAP levels and the discovery of hypercalcaemia after surgery led to further investigations which confirmed primary hyperparathyroidism due to a parathyroid adenoma. The patient's serum biochemistry normalised after removal of the adenoma. The association of adrenal myelolipoma with primary hyperparathyroidism has been reported in the literature only once previously. Although unconfirmed by genetic studies this association may possibly represent an unusual variation of the multiple endocrine neoplasia type 1 syndrome. (+info)A large intrathoracic parathyroid adenoma. (3/562)
A case is described in which an unusually large parathyroid adenoma was visible on the plain chest radiograph taken during the investigation of hypercalcaemia. This was diagnosed preoperatively and a scheme is suggested whereby such a disgnosis can now readily be made. The differential diagnosis is discussed ant the literature is reviewed. (+info)Expression of PRAD1/cyclin D1, retinoblastoma gene products, and Ki67 in parathyroid hyperplasia caused by chronic renal failure versus primary adenoma. (4/562)
BACKGROUND: In primary hyperparathyroidism, certain genetic abnormalities responsible for parathyroid tumorigenesis are proposed, and it has been reported that the overexpression of PRAD1/cyclin D1 induced by a DNA rearrangement of the parathyroid hormone (PTH) gene is one of the genetic disorders in a number of primary parathyroid adenomas. However, in secondary hyperparathyroidism caused by uremia, the mechanism of monoclonal proliferation in nodular parathyroid hyperplasia is not well understood. To elucidate the mechanism, we examined the expression of PRAD1/cyclin D1, retinoblastoma gene products, and Ki67 in primary adenoma and secondary hyperplasia. METHODS: In adenomas (N = 15) and associated glands (N = 7) with normal histology obtained from patients with primary hyperparathyroidism and in diffuse (N = 14), multinodular (N = 58), and single nodular (N = 28) glands from patients who underwent parathyroidectomy for renal hyperparathyroidism, the expression of these cell cycle regulators was evaluated by immunohistochemical technique. A labeling index was used to define the proportion of cells with positive nuclear staining by each antibody. RESULTS: In 6 out of 15 (40%) primary adenomas, PRAD1/cyclin D1 was overexpressed (a labeling index of more than 500), possibly because of the PTH gene rearrangement, but not in secondary hyperplasia, including single nodular glands. Compared with diffuse hyperplasia, nodular hyperplasia showed a significantly higher expression of PRAD1/cyclin D1 (P < 0.05), retinoblastoma gene products (P < 0.05), and Ki67 (P < 0.05). However, no statistically significant correlation between the expression of PRAD1/cyclin D1 and that of Ki67 was observed in both primary adenoma and secondary hyperplasia. CONCLUSIONS: These results suggest that in secondary hyperplasia caused by uremia, at least remarkable overexpression of PRAD1/cyclin D1 induced by PTH gene rearrangement may be not the major genetic abnormality responsible for tumorigenesis. Heterogenous genetic changes seem to contribute to monoclonal proliferation of parathyroid cells induced by the expression of PRAD1/cyclin D1 or by some other mechanism independent of the amplification of the proto-oncogene. (+info)Bilateral hemothorax revealing mediastinal parathyroid adenoma. (5/562)
We report the case of a 63-year-old woman admitted to hospital because of bilateral hemothorax associated with acute respiratory failure and laterotracheal neoformation. A right thoracoscopy biopsy revealed a paratracheal parathyroid adenoma which was responsible for bilateral hemothorax and primary hyperparathyroidism. A curative resection was successfully performed by cervicotomy. (+info)Ultrasound-guided unilateral neck exploration for sporadic primary hyperparathyroidism: is it worthwhile? (6/562)
The role of preoperative localisation tests before initial neck exploration for primary hyperparathyroidism (PHP) remains controversial, as does the optimal surgical approach. We report our experience with preoperative ultrasound (US) and the operative management of sporadic PHP between 1990 and 1995. Preoperative US was carried out by an experienced radiologist. Three surgeons adopted a policy of 'selective' US-guided unilateral neck exploration (UNE); the fourth surgeon performed routine bilateral neck exploration (BNE). There were 72 patients: 26 men and 46 women, with a mean age of 57.4 +/- 12.5 years (range 21-80 years). All patients underwent initial neck exploration for 'sporadic' PHP, of whom 63 had preoperative US. This was positive in 52 patients; 27 of whom underwent a UNE, 23 had a BNE, and two patients had a UNE converted to a BNE. Patients with 'negative' US (n = 11), and those receiving no preoperative localisation test (n = 90) underwent a BNE. The sensitivity, specificity and accuracy of US were 80% (52/65), 100% (61/61), and 90% (113/126), respectively. Comparable success rates were achieved (BNE: 97% (33/34) vs UNE: 93% (27/29), P < 0.05), with very low morbidity. Failures with the scan-guided UNE were caused by missed contralateral adenomas. An experienced radiologist and a low incidence of multiglandular disease (MGD) are essential prerequisites for the scan-guided unilateral approach. An experienced surgeon, on the other hand, is the only prerequisite for the 'gold standard' bilateral approach. (+info)Identification of a novel activated form of the keratinocyte growth factor receptor by expression cloning from parathyroid adenoma tissue. (7/562)
Parathyroid adenomas are benign tumors in the parathyroid glands, whose pathogenesis is largely unknown. We utilized an expression cDNA cloning strategy to identify oncogenes activated in parathyroid adenomas. An expression cDNA library was prepared directly from a clinical sample of parathyroid adenoma tissue, transfected into NIH3T3 cells, and foci of morphologically transformed cells were isolated. Following plasmid rescue, we identified cDNAs for the keratinocyte growth factor receptor at a high frequency. Interestingly, approximately half of the clones encoded a variant receptor containing an altered C-terminus. Analysis of the transforming activity of the variant receptor revealed that the altered C-terminus up-regulated the transforming activity in a ligand-independent manner. The higher transforming activity was not accompanied by increase of dimerization or overall autophosphorylation of the receptor. However, tyrosine phosphorylation of downstream receptor substrates, including Shc isoforms and possibly FRS2, are increased in the transfectants expressing the parathyroid tumor-derived receptor. Genomic analysis showed that a previously unidentified exon was used to form the novel isoform. This alternative splicing appears to occur preferentially in parathyroid adenomas. (+info)Hyperfunctional parathyroid glands with 99mTc-MIBI scan: semiquantitative analysis correlated with histologic findings. (8/562)
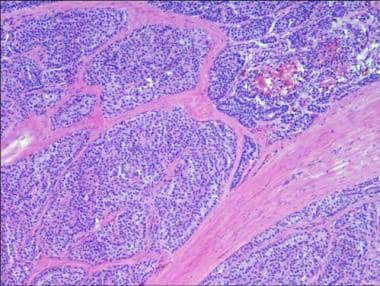
The purpose of this study was to correlate the semiquantitative analysis of 99mTc-methoxyisobutyl isonitrile (MIBI) scan with histologic findings of hyperfunctional parathyroid glands. METHODS: Early and delayed cervical images of MIBI scans were reviewed in 31 patients who eventually underwent parathyroidectomies because of biochemically suspected hyperparathyroidism ([HPT], primary, n = 13; secondary, n = 18). The sensitivity of a scan for localizing the diseased glands was determined by comparing scan findings with pathologic findings, which were considered the gold standard. The average ratio of parathyroid-to-thyroid (P/T) count was compared between glands with large and small areas of whole gland, chief cell, oxyphil cell or cellular components. The mean areas of whole gland, chief cells and oxyphil cells were also compared between glands detected by MIBI scan and those that the scan missed. RESULTS: There were 99 resected lesions, including 9 parathyroid adenomas and 61 hyperplastic parathyroids. The sensitivity for localizing the diseased glands in patients with primary HPT (91%) was higher than that in patients with secondary HPT (83%). Significantly greater average P/T counts ratio on both early and delayed images was observed in the diseased glands with greater areas of whole gland, chief cells, oxyphil cells or cellular components. Fifty-nine MIBI-positive glands had significantly greater average areas of whole gland (P < 0.001) and chief cell (P = 0.002) than did 11 MIBI-negative glands. CONCLUSION: The uptake of MIBI in hyperfunctional parathyroid is dependent on gland size and the amount of cellular components, chief cells and oxyphil cells. However, the amount of oxyphil cells does not clearly affect the results of MIBI parathyroid scintigraphy, because it is small in most hyperfunctional glands. (+info)Parathyroid neoplasms refer to abnormal growths in the parathyroid glands, which are small endocrine glands located in the neck, near or within the thyroid gland. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parathyroid neoplasms are typically called parathyroid adenomas and are the most common type of parathyroid disorder. They result in overproduction of parathyroid hormone (PTH), leading to a condition known as primary hyperparathyroidism. Symptoms may include kidney stones, osteoporosis, fatigue, depression, and abdominal pain.
Malignant parathyroid neoplasms are called parathyroid carcinomas. They are rare but more aggressive than adenomas, with a higher risk of recurrence and metastasis. Symptoms are similar to those of benign neoplasms but may also include hoarseness, difficulty swallowing, and enlarged lymph nodes in the neck.
It is important to note that parathyroid neoplasms can only be definitively diagnosed through biopsy or surgical removal and subsequent histopathological examination.
Parathyroid hormone (PTH) is a polypeptide hormone that plays a crucial role in the regulation of calcium and phosphate levels in the body. It is produced and secreted by the parathyroid glands, which are four small endocrine glands located on the back surface of the thyroid gland.
The primary function of PTH is to maintain normal calcium levels in the blood by increasing calcium absorption from the gut, mobilizing calcium from bones, and decreasing calcium excretion by the kidneys. PTH also increases phosphate excretion by the kidneys, which helps to lower serum phosphate levels.
In addition to its role in calcium and phosphate homeostasis, PTH has been shown to have anabolic effects on bone tissue, stimulating bone formation and preventing bone loss. However, chronic elevations in PTH levels can lead to excessive bone resorption and osteoporosis.
Overall, Parathyroid Hormone is a critical hormone that helps maintain mineral homeostasis and supports healthy bone metabolism.
The parathyroid glands are four small endocrine glands located in the neck, usually near or behind the thyroid gland. They secrete parathyroid hormone (PTH), which plays a critical role in regulating calcium and phosphate levels in the blood and bones. PTH helps maintain the balance of these minerals by increasing the absorption of calcium from food in the intestines, promoting reabsorption of calcium in the kidneys, and stimulating the release of calcium from bones when needed. Additionally, PTH decreases the excretion of calcium through urine and reduces phosphate reabsorption in the kidneys, leading to increased phosphate excretion. Disorders of the parathyroid glands can result in conditions such as hyperparathyroidism (overactive glands) or hypoparathyroidism (underactive glands), which can have significant impacts on calcium and phosphate homeostasis and overall health.
Parathyroid diseases refer to conditions that affect the parathyroid glands, which are small endocrine glands located in the neck, near or attached to the back surface of the thyroid gland. The primary function of the parathyroid glands is to produce and secrete parathyroid hormone (PTH), a crucial hormone that helps regulate calcium and phosphorus levels in the blood and bones.
There are four parathyroid glands, and they can develop various diseases, including:
1. Hyperparathyroidism: A condition where one or more parathyroid glands produce excessive amounts of PTH. This can lead to an imbalance in calcium and phosphorus levels, resulting in symptoms such as fatigue, weakness, bone pain, kidney stones, and increased risk of osteoporosis. Hyperparathyroidism can be primary (caused by a benign or malignant tumor in the parathyroid gland), secondary (due to chronic kidney disease or vitamin D deficiency), or tertiary (when secondary hyperparathyroidism becomes autonomous and continues even after correcting the underlying cause).
2. Hypoparathyroidism: A condition where the parathyroid glands do not produce enough PTH, leading to low calcium levels in the blood (hypocalcemia) and high phosphorus levels (hyperphosphatemia). Symptoms of hypoparathyroidism may include muscle spasms, tingling sensations in the fingers, toes, or lips, anxiety, cataracts, and seizures. Hypoparathyroidism can be caused by surgical removal of the parathyroid glands, autoimmune disorders, radiation therapy, or genetic conditions.
3. Parathyroid tumors: Abnormal growths in the parathyroid glands can lead to hyperparathyroidism. Benign tumors (adenomas) are the most common cause of primary hyperparathyroidism. Malignant tumors (carcinomas) are rare but can also occur, leading to more severe symptoms and a worse prognosis.
4. Parathyroid dysfunction in genetic disorders: Some genetic syndromes, such as multiple endocrine neoplasia type 1 (MEN1), multiple endocrine neoplasia type 2A (MEN2A), and hyperparathyroidism-jaw tumor syndrome (HPT-JT), can involve parathyroid gland abnormalities, leading to hyperparathyroidism or other related conditions.
Proper diagnosis and management of parathyroid disorders are crucial for maintaining optimal calcium homeostasis and preventing complications associated with hypocalcemia or hypercalcemia. Treatment options may include surgery, medication, dietary modifications, and monitoring hormone levels.
Parathyroid Hormone-Related Protein (PTHrP) is a protein that is encoded by the PTHLH gene in humans. It is structurally similar to parathyroid hormone (PTH) and was initially identified due to its role in humoral hypercalcemia of malignancy, a condition characterized by high levels of calcium in the blood caused by certain types of cancer.
PTHrP has a variety of functions in the body, including regulation of calcium and phosphate homeostasis, cell growth and differentiation, and bone metabolism. It acts through a specific G protein-coupled receptor called the PTH/PTHrP receptor, which is found in many tissues throughout the body, including bone, kidney, and cartilage.
In contrast to PTH, which is primarily produced by the parathyroid glands and regulates calcium levels in the blood, PTHrP is produced by many different types of cells throughout the body. Its expression is regulated in a tissue-specific manner, and its functions can vary depending on the context in which it is produced.
Overall, PTHrP plays important roles in normal physiology as well as in various disease states, including cancer, bone disorders, and developmental abnormalities.
Parathyroid Hormone Receptor Type 1 (PTH1R) is a type of G protein-coupled receptor that binds to parathyroid hormone (PTH) and parathyroid hormone-related peptide (PTHrP). It is primarily found in bone and kidney cells.
The activation of PTH1R by PTH or PTHrP leads to a series of intracellular signaling events that regulate calcium homeostasis, bone metabolism, and renal function. In the bone, PTH1R stimulates the release of calcium from bone matrix into the bloodstream, while in the kidney, it increases the reabsorption of calcium in the distal tubule and inhibits phosphate reabsorption.
Mutations in the gene encoding PTH1R can lead to several genetic disorders, such as Blomstrand chondrodysplasia, Jansen metaphyseal chondrodysplasia, and hypoparathyroidism type 1B. These conditions are characterized by abnormalities in bone development, growth, and mineralization.
Parathyroid hormone (PTH) receptors are a type of cell surface receptor that bind to and respond to parathyroid hormone, a hormone secreted by the parathyroid glands. These receptors are found in various tissues throughout the body, including bone, kidney, and intestine.
The PTH receptor is a member of the G protein-coupled receptor (GPCR) family, which consists of seven transmembrane domains. When PTH binds to the receptor, it activates a signaling pathway that leads to increased calcium levels in the blood. In bone, activation of PTH receptors stimulates the release of calcium from bone matrix, while in the kidney, it increases the reabsorption of calcium from the urine and decreases the excretion of phosphate.
In the intestine, PTH receptors play a role in the regulation of vitamin D metabolism, which is important for calcium absorption. Overall, the activation of PTH receptors helps to maintain normal calcium levels in the blood and regulate bone metabolism.
Hyperparathyroidism is a condition in which the parathyroid glands produce excessive amounts of parathyroid hormone (PTH). There are four small parathyroid glands located in the neck, near or within the thyroid gland. They release PTH into the bloodstream to help regulate the levels of calcium and phosphorus in the body.
In hyperparathyroidism, overproduction of PTH can lead to an imbalance in these minerals, causing high blood calcium levels (hypercalcemia) and low phosphate levels (hypophosphatemia). This can result in various symptoms such as fatigue, weakness, bone pain, kidney stones, and cognitive issues.
There are two types of hyperparathyroidism: primary and secondary. Primary hyperparathyroidism occurs when there is a problem with one or more of the parathyroid glands, causing them to become overactive and produce too much PTH. Secondary hyperparathyroidism develops as a response to low calcium levels in the body due to conditions like vitamin D deficiency, chronic kidney disease, or malabsorption syndromes.
Treatment for hyperparathyroidism depends on the underlying cause and severity of symptoms. In primary hyperparathyroidism, surgery to remove the overactive parathyroid gland(s) is often recommended. For secondary hyperparathyroidism, treating the underlying condition and managing calcium levels with medications or dietary changes may be sufficient.
Parathyroidectomy is a surgical procedure for the removal of one or more of the parathyroid glands. These glands are located in the neck and are responsible for producing parathyroid hormone (PTH), which helps regulate the levels of calcium and phosphorus in the body.
Parathyroidectomy is typically performed to treat conditions such as hyperparathyroidism, where one or more of the parathyroid glands become overactive and produce too much PTH. This can lead to high levels of calcium in the blood, which can cause symptoms such as weakness, fatigue, bone pain, kidney stones, and mental confusion.
There are different types of parathyroidectomy procedures, including:
* Partial parathyroidectomy: removal of one or more, but not all, of the parathyroid glands.
* Total parathyroidectomy: removal of all four parathyroid glands.
* Subtotal parathyroidectomy: removal of three and a half of the four parathyroid glands, leaving a small portion of one gland to prevent hypoparathyroidism (a condition where the body produces too little PTH).
The choice of procedure depends on the underlying condition and its severity. After the surgery, patients may need to have their calcium levels monitored and may require calcium and vitamin D supplements to maintain normal calcium levels in the blood.
Hypercalcemia is a medical condition characterized by an excess of calcium ( Ca2+ ) in the blood. While the normal range for serum calcium levels is typically between 8.5 to 10.2 mg/dL (milligrams per deciliter) or 2.14 to 2.55 mmol/L (millimoles per liter), hypercalcemia is generally defined as a serum calcium level greater than 10.5 mg/dL or 2.6 mmol/L.
Hypercalcemia can result from various underlying medical disorders, including primary hyperparathyroidism, malignancy (cancer), certain medications, granulomatous diseases, and excessive vitamin D intake or production. Symptoms of hypercalcemia may include fatigue, weakness, confusion, memory loss, depression, constipation, nausea, vomiting, increased thirst, frequent urination, bone pain, and kidney stones. Severe or prolonged hypercalcemia can lead to serious complications such as kidney failure, cardiac arrhythmias, and calcification of soft tissues. Treatment depends on the underlying cause and severity of the condition.
 Parathyroid neoplasm
Parathyroid neoplasm Videos • parathyroid neoplasms
Videos • parathyroid neoplasms What are parathyroid neoplasms? | Nicklaus Children's Hospital
What are parathyroid neoplasms? | Nicklaus Children's Hospital Parathyroid cancer: MedlinePlus Genetics
Parathyroid cancer: MedlinePlus Genetics Does intraoperative quick parathyroid hormone assay improve the results of parathyroidectomy?
Does intraoperative quick parathyroid hormone assay improve the results of parathyroidectomy? Parathyroid Carcinoma: Practice Essentials, Background, Pathophysiology
Parathyroid Carcinoma: Practice Essentials, Background, Pathophysiology Pathological Anatomy (LZ-H) 2023/2024 - University of Bologna
Pathological Anatomy (LZ-H) 2023/2024 - University of Bologna Endocrine Unit Research Lab
Endocrine Unit Research Lab Pancreatic Neuroendocrine Neoplasms (pNENs) - Symptoms, Causes, Treatment | NORD
Pancreatic Neuroendocrine Neoplasms (pNENs) - Symptoms, Causes, Treatment | NORD Elizabeth Gardner Grubbs | MD Anderson Cancer Center
Elizabeth Gardner Grubbs | MD Anderson Cancer Center 2015 Oncology Meetings - The ASCO Post
2015 Oncology Meetings - The ASCO Post Dr. Virginia Madey, MD, General Surgery Specialist - Springfield, VA | Sharecare
Dr. Virginia Madey, MD, General Surgery Specialist - Springfield, VA | Sharecare Thyroid | Centro Médico Teknon
Thyroid | Centro Médico Teknon Case 196 --Neuropathology Case
Case 196 --Neuropathology Case Authors
Authors Faculty Of Life & Health Sciences - Research output
- Ulster University
Faculty Of Life & Health Sciences - Research output
- Ulster University Parathyroid MEN1 gene mutations in relation to clinical characteristics of nonfamilial primary hyperparathyroidism | Lund...
Parathyroid MEN1 gene mutations in relation to clinical characteristics of nonfamilial primary hyperparathyroidism | Lund... RILUTEK® (riluzole) Tablets
RILUTEK® (riluzole) Tablets Clinical Biochemistry - Clinical Pathology and Procedures - Merck Veterinary Manual
Clinical Biochemistry - Clinical Pathology and Procedures - Merck Veterinary Manual Book - Essentials of Pediatric Surgery
| Bentham Science
Book - Essentials of Pediatric Surgery
| Bentham Science