Paraganglia, Nonchromaffin
Paraganglia, Chromaffin
Glomus Jugulare
Aortic Bodies
Paraganglioma
Paraganglioma, Extra-Adrenal
Pheochromocytoma
Unusual eustachian tube mass: glomus tympanicum. (1/22)
SUMMARY: A case of recurrent glomus tympanicum presenting with epistaxis is described. CT and MR imaging revealed a homogeneously enhancing mass extending along the entire course of the eustachian tube, with a portion protruding into the nasopharynx. Glomus tumors tend to spread along the path of least resistance and may extend into the eustachian tube. The unique imaging appearance should place a glomus tumor high on the list of differential diagnoses. (+info)The distribution of presumptive thoracic paraganglionic tissue in the common marmoset (Callithrix jacchus). (2/22)
The aortic-pulmonary regions (APR) of seven adult marmosets (Callithrix jacchus) and the region of the right subclavian artery of a further three marmosets were diffusion-fixed with 10% buffered formol-saline solution. In both regions serial 5 microm sections were cut and stained by the Martius yellow, brilliant crystal scarlet and soluble blue method. Presumptive thoracic paraganglionic (PTP) tissue was only observed in the APR. PTP tissue was composed of small groups of cells that varied in size and number. The distribution of the groups of cells was extremely variable, so much so that it would be misleading to attempt to classify their position; they were not circumscribed by a connective tissue capsule, but were always related to the thoracic branches of the left vagus nerve. The cells lay in loose areolar tissue characteristic of this part of the mediastinum and received their blood supply from small adjacent connective tissue arterioles. Unlike the paraganglionic tissue found in the carotid body the cells in the thorax did not appear to have a profuse capillary blood supply. There was, however, a close cellular-neural relationship. The cells, 10-15 microm in diameter, were oval or rounded in appearance and possessed a central nucleus and clear cytoplasm. No evidence was found that these cells possessed a 'companion' cell reminiscent of the arrangement of type 1 and type 2 cells in the carotid body. In conclusion, we found evidence of presumed paraganglionic tissue in the APR of the marmoset which, however, did not show the characteristic histological features of the aortic body chemoreceptors that have been described in some non-primate mammals. A survey of the mediastina of other non-human primates is required to establish whether this finding is atypical for these animals. (+info)Hereditary paraganglioma targets diverse paraganglia. (3/22)
Paragangliomas are highly vascularised and often heritable tumours derived from paraganglia, a diffuse neuroendocrine system dispersed from skull base to the pelvic floor. The carotid body, a small oxygen sensing organ located at the bifurcation of the carotid artery in the head and neck and the adrenal medulla in the abdomen, are the most common tumour sites. It now appears that mutations in SDHB, SDHC, and SDHD, which encode subunits of mitochondrial complex II (succinate dehydrogenase; succinate-ubiquinone oxidoreductase), are responsible for the majority of familial paragangliomas and also for a significant fraction of non-familial tumours. Germline mutations in complex II genes are associated with the development of paragangliomas in diverse anatomical locations, including phaeochromocytomas, a finding that has important implications for the clinical management of patients and genetic counselling of families. Consequently, patients with a paraganglioma tumour, including phaeochromocytoma, and a complex II germline mutation should be diagnosed with hereditary paraganglioma, regardless of family history, anatomical location, or multiplicity of tumours. This short review attempts to bring together relevant genetic data on paragangliomas with a particular emphasis on head and neck paragangliomas and phaeochromocytomas. (+info)Paraganglial cells of urinary bladder and prostate: potential diagnostic problem. (4/22)
A transurethral prostatic resection for prostatism in a 73 year old man showed a cluster of richly capillarised clear cells originally thought to be indicative of invasive carcinoma. Immunohistochemical studies were carried out on this tissue specimen and three similar cases using a variety of antibodies--Neuron specific enolase, PGP 9.5, chromogranin, synaptophysin, serotonin, somatostatin, substance P, calcitonin, calcitonin gene related peptide, met-enkephalin, VIP, neurofilament, CAM 5.2, S100 protein, prostatic specific antigen and prostatic acid phosphatase. The cellular foci were shown to be composed of paraganglionic cells. The cell clusters were well defined and predominantly comprised clear cells with scanty, fine eosinophilic cytoplasmic granules in three cases. The cell nuclei were round to oval, moderately pleomorphic, with evenly dispersed dense chromatin. It is concluded that the presence of minute foci of paraganglial cells in the bladder wall and prostate gland may be misinterpreted as malignant because of their close association with nerves and their relative rarity. Immunohistochemical staining with neuroendocrine markers should dispel any doubt about their identity. (+info)Mechanisms of low-glucose sensitivity in carotid body glomus cells. (5/22)
OBJECTIVE: Glucose sensing is essential for the adaptive counterregulatory responses to hypoglycemia. We investigated the mechanisms underlying carotid body (CB) glomus cells activation by low glucose. RESEARCH DESIGN/METHODS AND RESULTS: Removal of extracellular glucose elicited a cell secretory response, abolished by blockade of plasma membrane Ca(2+) channels, and a reversible increase in cytosolic Ca(2+) concentration. These data indicated that glucopenia induces transmembrane Ca(2+) influx and transmitter secretion. In patch-clamped glomus cells, exposure to low glucose resulted in inhibition of macroscopic outward K(+) currents and in the generation of a depolarizing receptor potential (DRP). The DRP was abolished upon removal of extracellular Na(+). The membrane-permeable 1-oleoyl-2-acetyl-sn-glycerol induced inward currents of similar characteristics as the current triggered by glucose deficiency. The functional and pharmacological analyses suggest that low glucose activates background cationic Na(+)-permeant channels, possibly of the transient receptor potential C subtype. Rotenone, a drug that occludes glomus cell sensitivity to hypoxia, did not abolish responsiveness to low glucose. The association of Glut2 and glucokinase, characteristic of some high glucose-sensing cells, did not seem to be needed for low glucose detection. CONCLUSIONS: Altogether, these data support the view that the CB is a multimodal chemoreceptor with a physiological role in glucose homeostasis. (+info)Chronic carotid glomitis and the glomus pulmonale. (6/22)
A histological study was made of the carotid bodies and glomus pulmonale in 50 consecutive subjects over the age of 50 years who came to necropsy to determine if chronic glomitis is confined to the carotid bodies or whether it also occurs in other glomera. Lymphoid aggregates and plasma cell activity were found in the glomus pulmonale just as they were in the carotid bodies. Chronic pulmonary glomitis sometimes occurred in association with chronic carotid glomitis and sometimes independently of this. The mean age of the affected subjects was 76 years in isolated pulmonary glomitis and 79 years in chronic carotid glomitis. Chronic carotid glomitis affected seven (14%) subjects and predominated in women (six to one). In the seven cases of isolated pulmonary glomitis women predominated five to two. Chronic glomitis seems to be a disease process which may affect at least two members of the non-chromaffin paraganglionic system, but it is not clear why focal chronic inflammation affects the glomus pulmonale of one person but not of another. (+info)Ultrastructural morphometric observations on the extramural aortico-pulmonary bodies of the domestic fowl. (7/22)
The extramural aortico-pulmonary bodies of the domestic fowl were analysed in electron micrographs by point-counting morphometry. The Type I cell constituted about 34% of the total volume of the parenchyma, whereas the supporting cells (Type II cells, pericytes and Schwann cells) constituted about 26%. The blood capillaries occupied the lowest volume density of about 5%. The mitochondria and the dense-cored vesicles occupied about the same volume (8%) of the Type I cell cytoplasm. The results obtained in the present study are compared with other similar studies on the aortic and carotid bodies of mammals. (+info)Aortico-pulmonary bodies in the domestic fowl: ultrastructure, innervation and secretion. (8/22)
In adult and immature domestic fowl, aggregations of large pale-staining cells were found in the wall of the aorta, and of the pulmonary trunk and arteries, in modified regions typified by interruption or loss of elastic laminae and smooth muscle cells. Encapsulated extramural aggregations of similar cells were identified either on the actual surface or well outside the arterial wall of the aorta, and pulmonary trunk and arteries. The electron microscope revealed that the pale cells in these intramural and extramural structures were granular cells characterised by dense-cored vesicles typically about 60-140 nm in diameter. Supporting cells partly invested the granular cells. These intramural and extramural structures are interpreted as aortico-pulmonary bodies. The extramural and to a lesser extent the intramural cells were associated with many axonal endings and fenestrated blood capillaries. The axonal endings formed presumptive afferent, efferent and reciprocal synapses with the granular cells. Both intra- and extramural granular cells displayed evidence of exocytosis and were also shown by autoradiography to handle amines. It is concluded that the ultrastructural features of these aortico-pulmonary bodies resemble those of the carotid body. It is therefore suggested that the aortico-pulmonary bodies of the domestic fowl have a chemoreceptor function similar to that of the carotid body. It is also suggested that they may have a general secretory function. (+info)Paraganglia, nonchromaffin are neuroendocrine tissues that originate from the neural crest and are widely distributed throughout the body. They are similar to chromaffin paraganglia (which contain catecholamines) but do not contain catecholamines or only contain them in trace amounts. Instead, they produce and secrete various neuropeptides and hormones, such as serotonin, somatostatin, and calcitonin gene-related peptide (CGRP).
Nonchromaffin paraganglia are divided into two main groups: the head and neck (HNP) and the thoracoabdominal (TAP) paraganglia. The HNP include the carotid body, jugular body, vagal body, and laryngeal paraganglia, while the TAP include the aorticopulmonary, organ of Zuckerkandl, and other abdominal and pelvic paraganglia.
Nonchromaffin paragangliomas are rare tumors that arise from these tissues. They can be functional or nonfunctional, depending on whether they produce and secrete hormones or not. Functional tumors can cause a variety of symptoms due to the excessive release of hormones, while nonfunctional tumors usually present as masses that may compress surrounding structures.
Paraganglia, chromaffin are neuroendocrine tissues that are derived from the neural crest and are located outside the adrenal gland. They are capable of producing catecholamines, including epinephrine (adrenaline) and norepinephrine (noradrenaline), in response to various stimuli such as stress or changes in blood pressure.
Chromaffin paraganglia are named for their ability to undergo a chemical reaction that results in brown coloration when exposed to chromium salts, a characteristic known as "chromaffinity." These tissues are found throughout the body, but the majority of them are clustered around the sympathetic and parasympathetic ganglia of the autonomic nervous system.
Examples of chromaffin paraganglia include the adrenal medulla (the inner part of the adrenal gland), the sympathetic paraganglia (such as the organ of Zuckerkandl, which is located near the aorta and is particularly prominent in fetuses and young children), and the parasympathetic paraganglia (such as the carotid body, which is located near the bifurcation of the common carotid artery).
Abnormal growths or tumors of chromaffin paraganglia are called pheochromocytomas if they arise from the adrenal medulla and paragangliomas if they arise from extra-adrenal locations. These tumors can cause excessive production of catecholamines, leading to hypertension, tachycardia, sweating, and other symptoms associated with the "fight or flight" response.
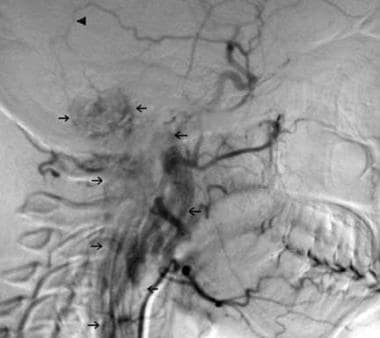
Glomus jugulare is a small, highly vascular tumor that originates from the glomus body, which is a type of nerve ending involved in temperature regulation, located near the jugular bulb in the skull. These tumors are typically benign but can cause serious symptoms due to their location and effects on surrounding structures. Symptoms may include hearing loss, pulsatile tinnitus (a rhythmic buzzing or whooshing sound in the ear), dizziness, and difficulty swallowing. Treatment options include surgical removal and radiation therapy.
Aortic bodies, also known as aortic arch chemoreceptors or simply as carotid and aortic bodies, are small clusters of nerve cells located near the bifurcation of the common carotid artery (carotid body) and in the wall of the aortic arch (aortic body). They are part of the peripheral chemoreceptor system that responds to changes in chemical composition of the blood, particularly to decreases in oxygen levels, increases in carbon dioxide levels, and changes in pH. These receptors send signals to the brainstem, which in turn regulates breathing rate and depth to maintain adequate gas exchange and acid-base balance in the body.
Paraganglioma is a rare type of tumor that develops in the nervous system, specifically in the paraganglia. Paraganglia are clusters of specialized nerve cells throughout the body that release hormones in response to stress or physical activity. Most paragangliomas are benign (noncancerous), but some can be malignant (cancerous) and may spread to other parts of the body.
Paragangliomas can occur in various locations, including the head and neck region (called "head and neck paragangliomas") or near the spine, abdomen, or chest (called "extra-adrenal paragangliomas"). When they develop in the adrenal glands, which are located on top of each kidney, they are called pheochromocytomas.
Paragangliomas can produce and release hormones such as epinephrine (adrenaline) and norepinephrine, leading to symptoms like high blood pressure, rapid heart rate, sweating, anxiety, and headaches. Treatment typically involves surgical removal of the tumor, along with medications to manage symptoms and control hormone levels before and after surgery.
Paraganglioma, extra-adrenal, is a type of rare tumor that develops in the nervous system's paraganglia, which are groups of specialized cells that are responsible for regulating blood pressure and other bodily functions. Unlike adrenal paragangliomas, which form in the adrenal glands located on top of the kidneys, extra-adrenal paragangliomas develop outside of the adrenal glands, in various locations along the sympathetic and parasympathetic nervous systems. These tumors can be functional or nonfunctional, meaning they may or may not produce hormones such as catecholamines (epinephrine, norepinephrine, and dopamine). Functional extra-adrenal paragangliomas can cause symptoms related to excessive hormone production, including hypertension, sweating, headaches, and rapid heartbeat. Treatment typically involves surgical removal of the tumor, along with preoperative preparation to manage potential hormonal imbalances.
Pheochromocytoma is a rare type of tumor that develops in the adrenal glands, which are triangular-shaped glands located on top of each kidney. These tumors produce excessive amounts of hormones called catecholamines, including adrenaline and noradrenaline. This can lead to a variety of symptoms such as high blood pressure, sweating, headaches, rapid heartbeat, and anxiety.
Pheochromocytomas are typically slow-growing and can be benign or malignant (cancerous). While the exact cause of these tumors is not always known, some genetic factors have been identified that may increase a person's risk. Treatment usually involves surgical removal of the tumor, along with medications to manage symptoms and control blood pressure before and after surgery.
Adrenal gland neoplasms refer to abnormal growths or tumors in the adrenal glands. These glands are located on top of each kidney and are responsible for producing hormones that regulate various bodily functions such as metabolism, blood pressure, and stress response. Adrenal gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign adrenal tumors are called adenomas and are usually small and asymptomatic. However, some adenomas may produce excessive amounts of hormones, leading to symptoms such as high blood pressure, weight gain, and mood changes.
Malignant adrenal tumors are called adrenocortical carcinomas and are rare but aggressive cancers that can spread to other parts of the body. Symptoms of adrenocortical carcinoma may include abdominal pain, weight loss, and hormonal imbalances.
It is important to diagnose and treat adrenal gland neoplasms early to prevent complications and improve outcomes. Diagnostic tests may include imaging studies such as CT scans or MRIs, as well as hormone level testing and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
 Paraganglion
Paraganglion
Glomus cell
List of MeSH codes (A08)
Peripheral chemoreceptors
Chromaffin cell
Paraganglion - Wikipedia
English-Armenian Medical - Terms starting with 'P' - MEDINDEX.AM
 Glomus Jugulare Tumors: Practice Essentials, Relevant Anatomy, Pathophysiology
Glomus Jugulare Tumors: Practice Essentials, Relevant Anatomy, Pathophysiology
 Búsqueda | BVS Bolivia
Búsqueda | BVS Bolivia
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
 MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
 Potential Biomarkers of Metastasizing Paragangliomas and Pheochromocytomas | Encyclopedia MDPI
Potential Biomarkers of Metastasizing Paragangliomas and Pheochromocytomas | Encyclopedia MDPI
An Alu-mediated partial SDHC deletion causes familial and sporadic paraganglioma | Journal of Medical Genetics
 A Not-So-Simple Thyroid Nodule | Endocrinology | JN Learning | AMA Ed Hub
A Not-So-Simple Thyroid Nodule | Endocrinology | JN Learning | AMA Ed Hub
 Lack of an adrenal cortex in Sf1 mutant mice is compatible with the generation and differentiation of chromaffin cells |...
Lack of an adrenal cortex in Sf1 mutant mice is compatible with the generation and differentiation of chromaffin cells |...
Extra-Adrenal and Adrenal Pheochromocytomas Associated With SDHC Mutation
 TREE NUMBER DESCRIPTOR
TREE NUMBER DESCRIPTOR
![HRP Anti-SDHB antibody [EPR10880] (ab198329) | Abcam](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAABm0lEQVQ4jaWTv0tbURTHP/cl75lqTIiNRFyEJIiUxNB2qf+D6NIuDg7WwcXFxU2yOznYte2klFIqpXVqoXQqgTYZKhURUURTlajJy++Xdx1eeJrmTc/vcuHc8/3cc869V8ileBZkClcSOcW9GUCmFPdmS16n4PfjKp/2KxQbJsmwxnwywOs/RUoNCcB0rI+xAbUb0DQls9tnbO7qHcC3OyWOigbn1RYA0aDXGbD8o8Dmro6qCOYS/Tx6qPHztMbGXx3Zzll5FuJppKe7hULNZD17jQA+TA0xGe21Nh4HmRj2sfjtAoDno36iQdUG2EPM5Gs0WpJ4SL01t7UwHqBPdZ63HTVMaxWOaWBK6Ri3AU8iPSgC9i6bfDmodCS9yhWpGs4AT3piIA3Qrykc6y1+ndV5v1cmX25xWGqy9vua1cyVbRh84GEk4CXk81gVy6WYja4YkpnP/9jaL3eckghrnOgGhZrV57vJCC9G/cB/19jrFXycHuLrUZXtgwpXdZPUoMbLZIA3dx5SMnx7jR0VuNG9/4ICIufaLWT2BlLHjkWr+SchAAAAAElFTkSuQmCC) HRP Anti-SDHB antibody [EPR10880] (ab198329) | Abcam
HRP Anti-SDHB antibody [EPR10880] (ab198329) | Abcam
MESH TREE NUMBER CHANGES - 2015 MeSH
 MeSH Browser
MeSH Browser
MeSH Browser
DeCS
MeSH Browser
 Genetic and epigenetic differences of benign and malignant pheochromocytomas and paragangliomas (PPGLs) - PubMed
Genetic and epigenetic differences of benign and malignant pheochromocytomas and paragangliomas (PPGLs) - PubMed
Sarcoma
Descriptors in 2013 MeSH. Preferred term only. December 14, 2012
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
MESH TREE NUMBER CHANGES - 2015 MeSH
 C C177536 GDC Property Terminology C129439 Medulloblastoma, Molecularly Defined A term that refers to the classification of...
C C177536 GDC Property Terminology C129439 Medulloblastoma, Molecularly Defined A term that refers to the classification of...
 Molecular Mechanisms of Acute Oxygen Sensing by Arterial Chemoreceptor Cells. Role of Hif2α
Molecular Mechanisms of Acute Oxygen Sensing by Arterial Chemoreceptor Cells. Role of Hif2α
Chemoreceptor Cells | Profiles RNS
MeSH Browser
 Hereditary Paraganglioma-Pheochromocytoma Syndromes - GeneReviews® - NCBI Bookshelf
Hereditary Paraganglioma-Pheochromocytoma Syndromes - GeneReviews® - NCBI Bookshelf
Lack of an adrenal cortex in Sf1 mutant mice is compatible with the generation and differentiation of chromaffin cells |...
Parasympathetic paraganglia3
- They are essentially of two types: (1) chromaffin or sympathetic paraganglia made of chromaffin cells and (2) nonchromaffin or parasympathetic paraganglia made of glomus cells. (wikipedia.org)
- Sympathetic paraganglia consist of chromaffin cells and are involved in the secretion of catecholamines (norepinephrine, epinephrine, and dopamine), while parasympathetic paraganglia consist of glomus (nonchromaffin) cells and act as chemoreceptors [ 1 ] . (encyclopedia.pub)
- Parasympathetic paraganglia include supracardiac paraganglia, paraganglia of the carotid body, middle ear, and larynx, as well as paraganglia distributed along the vagus nerve and several other smaller paraganglia [ 2 ] . (encyclopedia.pub)
Glomus1
- [ 3 ] Glomus tumors are also referred to as chemodectomas or nonchromaffin paragangliomas. (medscape.com)
Paragangliomas3
- Tumors of the paraganglionic tissues are known as paragangliomas, though this term tends to imply the nonchromaffin type, and can occur at a number of sites throughout the body. (wikipedia.org)
- Nonchromaffin paragangliomas are usually benign. (wikipedia.org)
- Tumors developing from paraganglia outside the adrenal gland are termed paragangliomas (PGLs). (encyclopedia.pub)
Ganglia of the sympathetic trunk1
- Chromaffin paraganglia (also called chromaffin bodies) are connected with the ganglia of the sympathetic trunk and the ganglia of the celiac, renal, adrenal, aortic and hypogastric plexuses. (wikipedia.org)
Carotid2
- Nonchromaffin paraganglia include carotid bodies and aortic bodies, some are distributed in the ear, along the vagus nerve, in the larynx and at various other places. (wikipedia.org)
- 1 Common tumour sites include the carotid body in the head and neck and adrenal and extra-adrenal paraganglia in the abdomen. (bmj.com)
Adrenal1
- The tumors that arise from the largest sympathetic paraganglia forming the adrenal medulla are called pheochromocytomas (PHEOs). (encyclopedia.pub)
Found1
- These paraganglia are common throughout the body, but most are found in the head and neck area [ 3 ] . (encyclopedia.pub)
Chromaffin1
- Chromaffin paraganglia (also called chromaffin bodies) are connected with the ganglia of the sympathetic trunk and the ganglia of the celiac, renal, adrenal, aortic and hypogastric plexuses. (wikipedia.org)
Cells1
- A paraganglion (pl. paraganglia) is a group of non-neuronal cells derived of the neural crest. (wikipedia.org)