Osteotomy, Le Fort
Jaw Fixation Techniques
Dentofacial Deformities
Maxillary Osteotomy
Maxilla
Dimensional Measurement Accuracy
Malocclusion, Angle Class III
Orthognathic Surgical Procedures
Oral Surgical Procedures
Mandible
Joint Deformities, Acquired
Hip Dislocation, Congenital
Fractures, Malunited
Hallux Valgus
Tibia
Osteotomy, Sagittal Split Ramus
History of Medicine
Metatarsal Bones
Acetabulum
Pelvic Bones
Legg-Calve-Perthes Disease
Hip Joint
Bone Plates
Range of Motion, Articular
Bone Lengthening
Bone Malalignment
Bone Diseases, Developmental
Isatis
Mandibular Osteotomy
Kyphosis
Femur Head
Fracture Healing
Treatment Outcome
Femur Head Necrosis
Leg Length Inequality
Osteogenesis, Distraction
An evaluation of the changes in maxillary pulpal blood flow associated with orthognathic surgery. (1/46)
The objective of this study was to evaluate the use of the Laser Doppler Flowmeter (LDF) in the measurement of pulpal blood flow following orthognathic surgery and to conduct an initial study of the effects of a Le Fort I osteotomy on the pulpal blood flow of the maxillary central incisors. The design consisted of a preliminary prospective controlled consecutive clinical trial undertaken at the Orthodontic Clinic, University Dental Hospital NHS Trust, Wales, 1994. The study group consisted of 15 consecutive patients who were to receive a standard advancement Le Fort I osteotomy. Seven patients who were to undergo a mandibular advancement only acted as a control. A further 20 separate patients participated in a study for the assessment of measurement error. The blood flow in relative perfusion unit v. time, was measured using a Laser Doppler Flowmeter. Measurement error for flowmeter recordings with hand-held application and custom-made splint support showed no consistent difference or significant random variation between the two methods for holding the probe against the teeth (pooled S.D. of reproducibility 1/1 = 1.91/1.39 for custom splint location as opposed to 0.96/1.07 for hand-held/fixed bracket location). For the surgical patients under investigation no significant differences for maxillary pulpal blood flow were found in the control group (mandibular osteotomy) over time. However, in the maxillary osteotomy patients there was a tendency for an initial rise in the maxillary perfusion post-surgery as measured at the central incisor pulps, followed by an overall reduction at 6 months. As an example, the mean value for the upper right central showed a significant increase in blood flow during the immediate post-operative period (P < 0.05), but at 6 months after surgery demonstrated a statistically significant overall reduction in comparison with the presurgical reading (P < 0.001). The laser Doppler flowmeter is not an easy instrument to use in the clinical assessment of pulpal blood flow. However, it would appear from these longitudinal series of readings, taken over a 6-month period on 15 patients, that the maxillary perfusion recorded at the central incisor pulps may be permanently affected in many Le Fort I osteotomy patients. For patients that already have a prejudiced blood supply this could lead to devitalization and discoloration of incisors. It is not known if this affect on the perfusion of the pulp continues beyond 6 months post-surgery. (+info)Intra-operative blood loss and operating time in orthognathic surgery using induced hypotensive general anaesthesia: prospective study. (2/46)
We investigated the average operating time and extent of intra-operative blood loss in orthognathic surgeries performed using induced hypotensive general anaesthesia, with the intention of devising a practical guideline for blood unit preparation for these procedures. We prospectively studied 32 Chinese patients undergoing surgery to correct dentofacial deformities at a public hospital in Hong Kong from 1 December 1997 to 1 December 1998. Most patients (72. 4%) needed double-jaw surgery. The mean estimated blood loss was approximately 617.6 mL. The blood loss during simple Le Fort I osteotomies was about half that of multiple segmentalised osteotomies. For mandibular ramus osteotomies, the mean blood loss and operating time for were approximately 280 mL and 2 hours, respectively; for anterior mandibular osteotomies, the corresponding values were 171.3 mL and 1 hour 13 minutes. The average drop in the haematocrit value was 15.4%, and the crossmatch to transfusion ratio was 29. A bivariate correlation test between the blood loss and operating time gave a strong correlation (P<0.01), as did blood loss with a drop in haematocrit value (P<0.01). Orthognathic surgeries are thus safe and predictable in terms of intra-operative blood loss and operating time, and a 'type, screen, and save' policy for blood unit preparation is more appropriate than a 'crossmatch' policy. (+info)Temporomandibular dysfunction in patients treated with orthodontics in combination with orthognathic surgery. (3/46)
Fifty-two patients with malocclusions underwent orthodontic treatment in combination with orthognathic surgery involving a Le Fort I and/or sagittal split osteotomy. Approximately 5 years after surgery, the patients were examined for signs and symptoms of temporomandibular disorders (TMD). The frequencies were found to be low in comparison with epidemiological studies in this field. The aesthetic outcome and chewing ability were improved in most patients (about 80 per cent). Some of the patients had reported recurrent and daily headaches before treatment. At examination, only two patients had reported having a headache once or twice a week, while all the others suffered from headaches less often or had no headache at all. Eighty-three per cent of the patients reported that they would be prepared to undergo the orthodontic/surgical treatment again with their present knowledge of the procedure. This study shows that orthodontic/surgical treatment of malocclusions not only has a beneficial effect on the aesthetic appearance and chewing ability, but also results in an improvement in signs and symptoms of TMD, including headaches. (+info)Open bite: stability after bimaxillary surgery--2-year treatment outcomes in 58 patients. (4/46)
Stability after bimaxillary surgery to correct open bite malocclusion and mandibular retrognathism was evaluated on lateral cephalograms before surgery, 8 weeks post-operatively, and after 2 years. The 58 consecutive patients were treated to a normal occlusion and good facial aesthetics. Treatment included the orthodontic alignment of teeth by maxillary and mandibular fixed appliances, Le Fort I osteotomy, and bilateral sagittal split ramus osteotomy. Twenty-six patients also had a genioplasty. Intra-osseous wires or bicortical screws were used for fixation. Twenty-three patients had maxillo-mandibular fixation (MMF) for 8 weeks or more, six for 4-7 weeks, 14 for 1-3 weeks, and 15 had no fixation. At follow-up 2 years later, the maxilla remained unchanged and the mandible had rotated on average 1.4 degrees posteriorly. Seventeen patients had an open bite. Among them, eight patients had undergone segmental osteotomies. The relapse was mainly due to incisor proclination. The most stabile overbite was found in the group with no MMF after surgery. (+info)A validation of two orthognathic model surgery techniques. (5/46)
In order to create an evidence-based orthognathic surgery planning protocol, an investigation of two popular model surgery techniques, the Lockwood keyspacer and the Eastman anatomically-orientated system was carried. This determined (a) the accuracy of positioning of the maxillary cast according to the prescribed treatment plan and (b) the relocation of the maxilla after a simulated Le Fort I down fracture osteotomy using the intermediate wafer as a guide. Fifteen patients-five Class II division 1, five Class II division 2, and five Class III-were included in the study. All the measurements were taken with Erickson's vertically mounted electronic caliper and variations from the treatment plan were analysed. The mean model surgery positioning errors +/- SD (mm) were: (i) vertical plane-Lockwood -0*8 +/- 1*6 and Eastman 0*00 +/- 1*0 (P = 0*0001); (ii) anteroposterior plane-Lockwood 1*2 +/- 1*8 and Eastman -0*1 +/- 1*4 (P = 0*05); and (iii) transverse plane-Lockwood 0*9 +/- 0*9 and Eastman 1*0 +/- 0*9 (P = 0*34). After the simulated osteotomy, the mean errors +/- SD were: (i) vertical plane-Lockwood -0*5 +/- 1*5 and Eastman 0*3 +/- 1*1 (P = 0*001); (ii) in anteroposterior plane-Lockwood 0*8 +/- 2*0 and Eastman 0*7 +/- 1*0 (P = 0*89); and (iii) transverse plane-Lockwood 0*8 +/- 0*6 and Eastman 0*7 +/- 0*5 (P = 0*83). The Eastman technique was relatively better especially in the vertical plane. The variations from the treatment plan were on the whole anatomically small, but in some cases could be clinically significant. (+info)Skeletal and dento-alveolar stability after surgical-orthodontic treatment of anterior open bite: a retrospective study. (6/46)
The aim of this investigation was to assess skeletal and dento-alveolar stability after surgical-orthodontic correction of skeletal anterior open bite treated by maxillary intrusion (group A) versus extrusion (group B). The cephalometric records of 49 adult anterior open bite patients (group A: n = 38, group B: n = 11), treated by the same maxillofacial surgeon, were examined at different timepoints, i.e. at the start of the orthodontic treatment (T1), before surgery (T2), immediately after surgery (T3), early post-operatively (+/- 20 weeks, T4) and one year post-operatively (T5). A bimaxillary operation was performed in 31 of the patients in group A and in six in group B. Rigid internal fixation was standard. If maxillary expansion was necessary, surgically assisted rapid palatal expansion (SRPE) was performed at least 9 months before the Le Fort I osteotomy. Forty-five patients received combined surgical and orthodontic treatment. The surgical open bite reduction (A, mean 3.9 mm; B, mean 7.7 mm) and the increase of overbite (A, mean 2.4 mm; B, mean 2.7 mm), remained stable one year post-operatively. SNA (T2-T3), showed a high tendency for relapse. The clockwise rotation of the palatal plane (1.7 degrees; T2-T3), relapsed completely within the first post-operative year. Anterior facial height reduction (A, mean -5.5 mm; B, mean -0.8 mm) occurred at the time of surgery. It can be concluded that open bite patients, treated by posterior Le Fort I impaction as well as with anterior extrusion, with or without an additional bilateral sagittal split osteotomy (BSSO), one year post-surgery, exhibit relatively good clinical dental and skeletal stability. (+info)Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery. (7/46)
In this study, the post-operative change of the maxilla in six non-cleft patients who underwent combination (Le Fort I and horseshoe) osteotomy for superior repositioning of the maxilla was investigated. In all patients, the maxilla was first osteotomized and fixed with four Luhr plates. No iliac bone graft was applied to the maxilla. A bilateral sagittal split ramus osteotomy of the mandible (BSSRO) was then carried out and titanium screw fixation was performed. No maxillo-mandibular fixation (MMF) with stainless steel wire was used post-operatively in any patient. Lateral cephalograms were obtained pre-operatively, 5 days post-operatively, and 3, 6, and 12 months after surgery. The changes in anterior nasal spine (ANS), point A, upper incisor (U1), and point of maxillary tuberosity (PMT) were examined. The maxillae in the six subjects were repositioned nearly in their planned positions during surgery and no significant post-operative changes in the examined points of the maxilla were found. These results suggest that a combination of a Le Fort I and horseshoe osteotomy is a useful technique for reliable superior repositioning of the maxilla. The post-operative change in the maxilla using this combination osteotomy is comparatively stable. (+info)Dental tipping and rotation immediately after surgically assisted rapid palatal expansion. (8/46)
The purpose of this investigation was to evaluate the effects of dental tipping and rotation immediately after surgically assisted rapid palatal expansion (SARPE). Fourteen patients (10 females, four males; mean age 25.6 years) who required a SARPE procedure were available for this study. A palatal expander appliance was cemented on four abutment teeth (first premolars and first molars) of each patient 1 week prior to surgery. Maxillary study models were taken before surgery and 2-3 weeks after full expansion (7 mm). Each model was trimmed to have the base parallel to its occlusal plane. From an occlusal view, measurements were made to determine if the abutment teeth underwent rotation from SARPE. From a postero-anterior view, the abutment teeth were examined for any tipping effect due to SARPE. The results showed that from pre- to post-expansion, the two first premolars displayed 2.32 +/- 8.29 degrees of mesiobuccal rotation (P > 0.05) and the two first molars displayed 3.09 +/- 5.89 degrees of mesiobuccal rotation (P > 0.05). Each first premolar showed 6.48 +/- 2.29 degrees of buccal tipping (P < 0.05) and each first molar 7.04 +/- 4.58 degrees of buccal tipping (P < 0.05). SARPE induced a slight mesiobuccal rotation (P > 0.05) and significant buccal tipping of the first premolars and the first molars (P < 0.05). Some overexpansion is suggested to counteract the relapse effect of buccal tipping of the posterior teeth that takes place during SARPE. (+info)An "osteotomy" refers to a surgical procedure in which a bone is cut. A "Le Fort osteotomy" is a specific type of osteotomy that involves cutting and repositioning the middle (midface) portion of the facial bones. There are three types of Le Fort osteotomies, named after the French surgeon René Le Fort who first described them:
1. Le Fort I osteotomy: This procedure involves making a horizontal cut through the lower part of the maxilla (upper jaw) and separating it from the rest of the facial bones. It is often used to treat conditions such as severe jaw deformities or obstructive sleep apnea.
2. Le Fort II osteotomy: In this procedure, an upward curved cut is made through the lower part of the maxilla and the middle portion of the nasal bones. This allows for the repositioning of the midface and nose. It may be used to treat conditions such as severe facial fractures or congenital deformities.
3. Le Fort III osteotomy: A Le Fort III osteotomy involves making a cut through the upper part of the maxilla, the orbital bones (bones surrounding the eyes), and the zygomatic bones (cheekbones). This procedure allows for significant repositioning of the midface and is often used to treat severe facial fractures or congenital deformities.
It's important to note that Le Fort osteotomies are complex surgical procedures that should only be performed by experienced oral and maxillofacial surgeons or craniofacial surgeons.
Osteotomy is a surgical procedure in which a bone is cut to shorten, lengthen, or change its alignment. It is often performed to correct deformities or to realign bones that have been damaged by trauma or disease. The bone may be cut straight across (transverse osteotomy) or at an angle (oblique osteotomy). After the bone is cut, it can be realigned and held in place with pins, plates, or screws until it heals. This procedure is commonly performed on bones in the leg, such as the femur or tibia, but can also be done on other bones in the body.
Jaw fixation techniques, also known as maxillomandibular fixation (MMF), are procedures used in dental and oral surgery to hold the jaw in a specific position. This is typically done by wiring the upper and lower teeth together or using elastic bands and other devices to keep the jaws aligned. The technique is often used after surgical procedures on the jaw, such as corrective jaw surgery (orthognathic surgery) or fracture repair, to help promote proper healing and alignment of the bones. It may also be used in the management of temporomandibular joint disorders or other conditions affecting the jaw. The duration of jaw fixation can vary depending on the specific procedure and individual patient needs, but it typically lasts several weeks.
Dentofacial deformities refer to abnormalities in the growth and development of the teeth and facial bones. These deformities can affect the alignment, shape, and function of the teeth and jaws, leading to problems with chewing, speaking, and breathing. Dentofacial deformities can be caused by genetic factors, environmental influences, or a combination of both.
There are various types of dentofacial deformities, including:
1. Overbite: Also known as buck teeth, an overbite occurs when the upper front teeth overlap the lower front teeth excessively.
2. Underbite: An underbite occurs when the lower front teeth protrude beyond the upper front teeth.
3. Crossbite: A crossbite occurs when the upper and lower teeth do not meet properly, causing the jaw to shift to one side.
4. Open bite: An open bite occurs when there is a space between the upper and lower front teeth when the back teeth are biting together.
5. Protrusion: Protrusion refers to the abnormal forward placement of the upper or lower teeth.
6. Asymmetry: Facial asymmetry occurs when the left and right sides of the face are not symmetrical, leading to a crooked smile or jaw.
7. Jaw deformities: Jaw deformities can include a small or recessed chin (retrogenia), a prominent chin (prognathism), or a narrow or wide jaw.
Treatment for dentofacial deformities may involve orthodontic treatment, such as braces or aligners, to correct tooth alignment. In more severe cases, surgery may be required to reshape or reposition the facial bones. Early intervention and treatment can help prevent long-term complications and improve overall oral health and function.
A maxillary osteotomy is a surgical procedure that involves making cuts in the bone of the upper jaw (maxilla). This type of surgery may be performed for various reasons, such as to correct jaw deformities, realign the jaws, or treat sleep apnea. In some cases, it may also be done in conjunction with other procedures, such as a genioplasty (chin surgery) or rhinoplasty (nose surgery).
During a maxillary osteotomy, an incision is made inside the mouth, and the surgeon carefully cuts through the bone of the upper jaw. The maxilla is then repositioned as needed and held in place with small plates and screws. In some cases, bone grafts may also be used to help support the new position of the jaw. After the surgery, the incision is closed with stitches.
It's important to note that a maxillary osteotomy is a complex surgical procedure that requires careful planning and execution. It should only be performed by an experienced oral and maxillofacial surgeon or craniofacial surgeon. As with any surgery, there are risks involved, including infection, bleeding, and reactions to anesthesia. It's important to discuss these risks with your surgeon and to follow all post-operative instructions carefully to help ensure a successful recovery.
The maxilla is a paired bone that forms the upper jaw in vertebrates. In humans, it is a major bone in the face and plays several important roles in the craniofacial complex. Each maxilla consists of a body and four processes: frontal process, zygomatic process, alveolar process, and palatine process.
The maxillae contribute to the formation of the eye sockets (orbits), nasal cavity, and the hard palate of the mouth. They also contain the upper teeth sockets (alveoli) and help form the lower part of the orbit and the cheekbones (zygomatic arches).
Here's a quick rundown of its key functions:
1. Supports the upper teeth and forms the upper jaw.
2. Contributes to the formation of the eye sockets, nasal cavity, and hard palate.
3. Helps shape the lower part of the orbit and cheekbones.
4. Partakes in the creation of important sinuses, such as the maxillary sinus, which is located within the body of the maxilla.
Dimensional measurement accuracy refers to the degree of closeness with which the measured dimension of a object or feature corresponds to its true value. It is usually expressed as a tolerance, which indicates the maximum allowable deviation from the true value. This measurement accuracy can be affected by various factors such as the precision and calibration of the measuring instrument, the skill and experience of the person taking the measurement, and environmental conditions such as temperature and humidity. High dimensional measurement accuracy is essential in many fields, including manufacturing, engineering, and scientific research, to ensure that parts and products meet specified dimensions and function properly.
Malocclusion, Angle Class III is a type of orthodontic problem characterized by a misalignment of the teeth and jaws. This classification was first described by Edward Angle, an American dentist who is considered the father of modern orthodontics. In Class III malocclusion, the lower jaw (mandible) protrudes forward beyond the upper jaw (maxilla), resulting in a misaligned bite.
In this condition, the lower front teeth are positioned in front of the upper front teeth when the jaws are closed. This can lead to various dental and skeletal problems, such as abnormal tooth wear, difficulty in chewing and speaking, and aesthetic concerns. Class III malocclusion can be mild, moderate, or severe and may require orthodontic treatment, including braces, appliances, or even surgery, to correct the problem.
Orthognathic surgical procedures are a type of surgery used to correct jaw misalignments and improve the bite and function of the jaws. The term "orthognathic" comes from the Greek words "orthos," meaning straight or correct, and "gnathos," meaning jaw. These surgeries are typically performed by oral and maxillofacial surgeons in conjunction with orthodontic treatment to achieve proper alignment of the teeth and jaws.
Orthognathic surgical procedures may be recommended for patients who have significant discrepancies between the size and position of their upper and lower jaws, which can result in problems with chewing, speaking, breathing, and sleeping. These procedures can also improve facial aesthetics by correcting jaw deformities and imbalances.
The specific surgical procedure used will depend on the nature and extent of the jaw misalignment. Common orthognathic surgical procedures include:
1. Maxillary osteotomy: This procedure involves making cuts in the upper jawbone (maxilla) and moving it forward or backward to correct a misalignment.
2. Mandibular osteotomy: This procedure involves making cuts in the lower jawbone (mandible) and moving it forward or backward to correct a misalignment.
3. Genioplasty: This procedure involves reshaping or repositioning the chin bone (mentum) to improve facial aesthetics and jaw function.
4. Orthognathic surgery for sleep apnea: This procedure involves repositioning the upper and/or lower jaws to open up the airway and improve breathing during sleep.
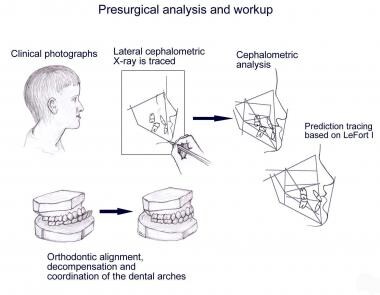
Orthognathic surgical procedures require careful planning and coordination between the surgeon, orthodontist, and patient. The process typically involves taking detailed measurements and images of the jaw and teeth, creating a surgical plan, and undergoing orthodontic treatment to align the teeth prior to surgery. After surgery, patients may need to wear braces or other appliances to maintain the alignment of their teeth and jaws during healing.
Maxillary fractures, also known as Le Fort fractures, are complex fractures that involve the upper jaw or maxilla. Named after the French surgeon René Le Fort who first described them in 1901, these fractures are categorized into three types (Le Fort I, II, III) based on the pattern and level of bone involvement.
1. Le Fort I fracture: This type of maxillary fracture involves a horizontal separation through the lower part of the maxilla, just above the teeth's roots. It often results from direct blows to the lower face or chin.
2. Le Fort II fracture: A Le Fort II fracture is characterized by a pyramidal-shaped fracture pattern that extends from the nasal bridge through the inferior orbital rim and maxilla, ending at the pterygoid plates. This type of fracture usually results from forceful impacts to the midface or nose.
3. Le Fort III fracture: A Le Fort III fracture is a severe craniofacial injury that involves both the upper and lower parts of the face. It is also known as a "craniofacial dysjunction" because it separates the facial bones from the skull base. The fracture line extends through the nasal bridge, orbital rims, zygomatic arches, and maxilla, ending at the pterygoid plates. Le Fort III fractures typically result from high-impact trauma to the face, such as car accidents or assaults.
These fractures often require surgical intervention for proper alignment and stabilization of the facial bones.
Prognathism is a dental and maxillofacial term that refers to a condition where the jaw, particularly the lower jaw (mandible), protrudes or sticks out beyond the normal range, resulting in the forward positioning of the chin and teeth. It can be classified as horizontal or vertical, depending on whether the protrusion is side-to-side or up-and-down.
This condition can be mild or severe and may affect one's appearance and dental health. In some cases, it can also cause issues with speaking, chewing, and breathing. Prognathism can be a result of genetic factors or certain medical conditions, such as acromegaly or gigantism. Treatment options for prognathism include orthodontic treatment, surgery, or a combination of both.
Oral surgical procedures refer to various types of surgeries performed in the oral cavity and maxillofacial region, which includes the mouth, jaws, face, and skull. These procedures are typically performed by oral and maxillofacial surgeons, who are dental specialists with extensive training in surgical procedures involving the mouth, jaws, and face.
Some common examples of oral surgical procedures include:
1. Tooth extractions: This involves removing a tooth that is damaged beyond repair or causing problems for the surrounding teeth. Wisdom tooth removal is a common type of tooth extraction.
2. Dental implant placement: This procedure involves placing a small titanium post in the jawbone to serve as a replacement root for a missing tooth. A dental crown is then attached to the implant, creating a natural-looking and functional replacement tooth.
3. Jaw surgery: Also known as orthognathic surgery, this procedure involves repositioning the jaws to correct bite problems or facial asymmetry.
4. Biopsy: This procedure involves removing a small sample of tissue from the oral cavity for laboratory analysis, often to diagnose suspicious lesions or growths.
5. Lesion removal: This procedure involves removing benign or malignant growths from the oral cavity, such as tumors or cysts.
6. Temporomandibular joint (TMJ) surgery: This procedure involves treating disorders of the TMJ, which connects the jawbone to the skull and allows for movement when eating, speaking, and yawning.
7. Facial reconstruction: This procedure involves rebuilding or reshaping the facial bones after trauma, cancer surgery, or other conditions that affect the face.
Overall, oral surgical procedures are an important part of dental and medical care, helping to diagnose and treat a wide range of conditions affecting the mouth, jaws, and face.
The mandible, also known as the lower jaw, is the largest and strongest bone in the human face. It forms the lower portion of the oral cavity and plays a crucial role in various functions such as mastication (chewing), speaking, and swallowing. The mandible is a U-shaped bone that consists of a horizontal part called the body and two vertical parts called rami.
The mandible articulates with the skull at the temporomandibular joints (TMJs) located in front of each ear, allowing for movements like opening and closing the mouth, protrusion, retraction, and side-to-side movement. The mandible contains the lower teeth sockets called alveolar processes, which hold the lower teeth in place.
In medical terminology, the term "mandible" refers specifically to this bone and its associated structures.
Acquired joint deformities refer to structural changes in the alignment and shape of a joint that develop after birth, due to various causes such as injury, disease, or wear and tear. These deformities can affect the function and mobility of the joint, causing pain, stiffness, and limited range of motion. Examples of conditions that can lead to acquired joint deformities include arthritis, infection, trauma, and nerve damage. Treatment may involve medication, physical therapy, or surgery to correct the deformity and alleviate symptoms.
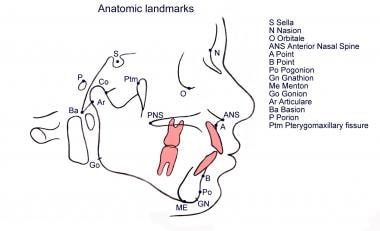
Cephalometry is a medical term that refers to the measurement and analysis of the skull, particularly the head face relations. It is commonly used in orthodontics and maxillofacial surgery to assess and plan treatment for abnormalities related to the teeth, jaws, and facial structures. The process typically involves taking X-ray images called cephalograms, which provide a lateral view of the head, and then using various landmarks and reference lines to make measurements and evaluate skeletal and dental relationships. This information can help clinicians diagnose problems, plan treatment, and assess treatment outcomes.
Congenital hip dislocation, also known as developmental dysplasia of the hip (DDH), is a condition where the hip joint fails to develop normally in utero or during early infancy. In a healthy hip, the head of the femur (thigh bone) fits snugly into the acetabulum (hip socket). However, in congenital hip dislocation, the femoral head is not held firmly in place within the acetabulum due to abnormal development or laxity of the ligaments that support the joint.
There are two types of congenital hip dislocations:
1. Teratologic dislocation: This type is present at birth and occurs due to abnormalities in the development of the hip joint during fetal growth. The femoral head may be completely outside the acetabulum or partially dislocated.
2. Developmental dysplasia: This type develops after birth, often within the first few months of life, as a result of ligamentous laxity and shallow acetabulum. In some cases, it can progress to a complete hip dislocation if left untreated.
Risk factors for congenital hip dislocation include family history, breech presentation during delivery, and female gender. Early diagnosis and treatment are crucial to prevent long-term complications such as pain, limited mobility, and osteoarthritis. Treatment options may include bracing, closed reduction, or surgical intervention, depending on the severity and age of the child at diagnosis.
Malunited fractures refer to a type of fracture where the bones do not heal in their proper alignment or position. This can occur due to various reasons such as inadequate reduction of the fracture fragments during initial treatment, improper casting or immobilization, or failure of the patient to follow proper immobilization instructions. Malunited fractures can result in deformity, limited range of motion, and decreased functionality of the affected limb. Additional treatments such as surgery may be required to correct the malunion and restore normal function.
Hallux Valgus is a medical condition that affects the foot, specifically the big toe joint. It is characterized by the deviation of the big toe (hallux) towards the second toe, resulting in a prominent bump on the inner side of the foot at the base of the big toe. This bump is actually the metatarsal head of the first bone in the foot that becomes exposed due to the angulation.
The deformity can lead to pain, stiffness, and difficulty wearing shoes. In severe cases, it can also cause secondary arthritis in the joint. Hallux Valgus is more common in women than men and can be caused by genetic factors, foot shape, or ill-fitting shoes that put pressure on the big toe joint.
The tibia, also known as the shin bone, is the larger of the two bones in the lower leg and part of the knee joint. It supports most of the body's weight and is a major insertion point for muscles that flex the foot and bend the leg. The tibia articulates with the femur at the knee joint and with the fibula and talus bone at the ankle joint. Injuries to the tibia, such as fractures, are common in sports and other activities that put stress on the lower leg.
Sagittal split ramus osteotomy (SSRO) is a specific type of orthognathic surgery, which is performed on the ramus of the mandible (lower jaw). The procedure involves making a surgical cut in the ramus bone in a sagittal direction (splitting it from front to back), and then splitting the bone further into two segments. These segments are then repositioned to correct dentofacial deformities, such as jaw misalignment or asymmetry. The procedure is often used to treat severe cases of malocclusion (bad bite) and jaw joint disorders. After the bones are repositioned, they are stabilized with plates and screws until they heal together in their new position.
The "History of Medicine" refers to the evolution and development of medical knowledge, practices, and institutions over time. It includes the study of key figures, discoveries, theories, treatments, and societal attitudes that have shaped the way medicine is practiced and understood in different cultures and historical periods. This can encompass various fields such as clinical medicine, public health, medical ethics, and healthcare systems. The history of medicine provides valuable insights into the advances and setbacks in medical knowledge and offers lessons for addressing current and future medical challenges.
The femur is the medical term for the thigh bone, which is the longest and strongest bone in the human body. It connects the hip bone to the knee joint and plays a crucial role in supporting the weight of the body and allowing movement during activities such as walking, running, and jumping. The femur is composed of a rounded head, a long shaft, and two condyles at the lower end that articulate with the tibia and patella to form the knee joint.
The metatarsal bones are a group of five long bones in the foot that connect the tarsal bones in the hindfoot to the phalanges in the forefoot. They are located between the tarsal and phalangeal bones and are responsible for forming the arch of the foot and transmitting weight-bearing forces during walking and running. The metatarsal bones are numbered 1 to 5, with the first metatarsal being the shortest and thickest, and the fifth metatarsal being the longest and thinnest. Each metatarsal bone has a base, shaft, and head, and they articulate with each other and with the surrounding bones through joints. Any injury or disorder affecting the metatarsal bones can cause pain and difficulty in walking or standing.
The acetabulum is the cup-shaped cavity in the pelvic bone (specifically, the os coxa) where the head of the femur bone articulates to form the hip joint. It provides a stable and flexible connection between the lower limb and the trunk, allowing for a wide range of movements such as flexion, extension, abduction, adduction, rotation, and circumduction. The acetabulum is lined with articular cartilage, which facilitates smooth and frictionless movement of the hip joint. Its stability is further enhanced by various ligaments, muscles, and the labrum, a fibrocartilaginous rim that deepens the socket and increases its contact area with the femoral head.
The pelvic bones, also known as the hip bones, are a set of three irregularly shaped bones that connect to form the pelvic girdle in the lower part of the human body. They play a crucial role in supporting the spine and protecting the abdominal and pelvic organs.
The pelvic bones consist of three bones:
1. The ilium: This is the largest and uppermost bone, forming the majority of the hip bone and the broad, flaring part of the pelvis known as the wing of the ilium or the iliac crest, which can be felt on the side of the body.
2. The ischium: This is the lower and back portion of the pelvic bone that forms part of the sitting surface or the "sit bones."
3. The pubis: This is the front part of the pelvic bone, which connects to the other side at the pubic symphysis in the midline of the body.
The pelvic bones are joined together at the acetabulum, a cup-shaped socket that forms the hip joint and articulates with the head of the femur (thigh bone). The pelvic bones also have several openings for the passage of blood vessels, nerves, and reproductive and excretory organs.
The shape and size of the pelvic bones differ between males and females due to their different roles in childbirth and locomotion. Females typically have a wider and shallower pelvis than males to accommodate childbirth, while males usually have a narrower and deeper pelvis that is better suited for weight-bearing and movement.
Legg-Calve-Perthes disease is a childhood hip disorder that occurs when the blood supply to the ball part of the thigh bone (femoral head) is disrupted. This causes the bone tissue to die, leading to its collapse and deformity. The femoral head then regenerates itself, but often not as round and smooth as it should be, which can lead to hip problems in later life.
The disease is named after three doctors who independently described it: Arthur Legg, Jacques Calve, and Georg Perthes. It typically affects children between the ages of 4 and 10, more commonly boys than girls. Symptoms may include limping, pain in the hip or knee, reduced range of motion in the hip, and muscle wasting. Treatment often involves rest, physical therapy, and sometimes surgery to realign or reshape the femoral head.
The hip joint, also known as the coxal joint, is a ball-and-socket type synovial joint that connects the femur (thigh bone) to the pelvis. The "ball" is the head of the femur, while the "socket" is the acetabulum, a concave surface on the pelvic bone.
The hip joint is surrounded by a strong fibrous capsule and is reinforced by several ligaments, including the iliofemoral, ischiofemoral, and pubofemoral ligaments. The joint allows for flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction movements, making it one of the most mobile joints in the body.
The hip joint is also supported by various muscles, including the gluteus maximus, gluteus medius, gluteus minimus, iliopsoas, and other hip flexors and extensors. These muscles provide stability and strength to the joint, allowing for weight-bearing activities such as walking, running, and jumping.
Bone plates are medical devices used in orthopedic surgery to stabilize and hold together fractured or broken bones during the healing process. They are typically made of surgical-grade stainless steel, titanium, or other biocompatible materials. The plate is shaped to fit the contour of the bone and is held in place with screws that are inserted through the plate and into the bone on either side of the fracture. This provides stability and alignment to the broken bones, allowing them to heal properly. Bone plates can be used to treat a variety of fractures, including those that are complex or unstable. After healing is complete, the bone plate may be left in place or removed, depending on the individual's needs and the surgeon's recommendation.
Articular Range of Motion (AROM) is a term used in physiotherapy and orthopedics to describe the amount of movement available in a joint, measured in degrees of a circle. It refers to the range through which synovial joints can actively move without causing pain or injury. AROM is assessed by measuring the degree of motion achieved by active muscle contraction, as opposed to passive range of motion (PROM), where the movement is generated by an external force.
Assessment of AROM is important in evaluating a patient's functional ability and progress, planning treatment interventions, and determining return to normal activities or sports participation. It is also used to identify any restrictions in joint mobility that may be due to injury, disease, or surgery, and to monitor the effectiveness of rehabilitation programs.
A hip dislocation is a medical emergency that occurs when the head of the femur (thighbone) slips out of its socket in the pelvis. This can happen due to high-energy trauma, such as a car accident or a severe fall. Hip dislocations can also occur in people with certain health conditions that make their hips more prone to displacement, such as developmental dysplasia of the hip.
There are two main types of hip dislocations: posterior and anterior. In a posterior dislocation, the femur head moves out of the back of the socket, which is the most common type. In an anterior dislocation, the femur head moves out of the front of the socket. Both types of hip dislocations can cause severe pain, swelling, and difficulty moving the affected leg.
Immediate medical attention is necessary for a hip dislocation to realign the bones and prevent further damage. Treatment typically involves sedation or anesthesia to relax the muscles around the joint, followed by a closed reduction procedure to gently guide the femur head back into the socket. In some cases, surgery may be required to repair any associated injuries, such as fractures or damaged ligaments. After treatment, physical therapy and rehabilitation are usually necessary to restore strength, mobility, and function to the affected hip joint.
Bone lengthening is a surgical procedure that involves cutting and then gradually stretching the bone apart, allowing new bone to grow in its place. This process is also known as distraction osteogenesis. The goal of bone lengthening is to increase the length of a bone, either to improve function or to correct a deformity.
The procedure typically involves making an incision in the skin over the bone and using specialized tools to cut through the bone. Once the bone is cut, a device called an external fixator is attached to the bone on either side of the cut. The external fixator is then gradually adjusted over time to slowly stretch the bone apart, creating a gap between the two ends of the bone. As the bone is stretched, new bone tissue begins to grow in the space between the two ends, eventually filling in the gap and lengthening the bone.
Bone lengthening can be used to treat a variety of conditions, including limb length discrepancies, congenital deformities, and injuries that result in bone loss. It is typically performed by an orthopedic surgeon and may require several months of follow-up care to ensure proper healing and growth of the new bone tissue.
I apologize for any confusion, but "Military Personnel" is not a medical term. It refers to individuals who serve in the military forces of a country, including the Army, Navy, Air Force, Marine Corps, and Coast Guard. Medical terms typically refer to specific conditions, diagnoses, treatments, or anatomical features related to healthcare. If you have any questions about medical terminology or concepts, I would be happy to help clarify!
Bone malalignment is a term used to describe the abnormal alignment or positioning of bones in relation to each other. This condition can occur as a result of injury, deformity, surgery, or disease processes that affect the bones and joints. Bone malalignment can cause pain, stiffness, limited mobility, and an increased risk of further injury. In some cases, bone malalignment may require treatment such as bracing, physical therapy, or surgery to correct the alignment and improve function.
Developmental bone diseases are a group of medical conditions that affect the growth and development of bones. These diseases are present at birth or develop during childhood and adolescence, when bones are growing rapidly. They can result from genetic mutations, hormonal imbalances, or environmental factors such as poor nutrition.
Some examples of developmental bone diseases include:
1. Osteogenesis imperfecta (OI): Also known as brittle bone disease, OI is a genetic disorder that affects the body's production of collagen, a protein necessary for healthy bones. People with OI have fragile bones that break easily and may also experience other symptoms such as blue sclerae (whites of the eyes), hearing loss, and joint laxity.
2. Achondroplasia: This is the most common form of dwarfism, caused by a genetic mutation that affects bone growth. People with achondroplasia have short limbs and a large head relative to their body size.
3. Rickets: A condition caused by vitamin D deficiency or an inability to absorb or use vitamin D properly. This leads to weak, soft bones that can bow or bend easily, particularly in children.
4. Fibrous dysplasia: A rare bone disorder where normal bone is replaced with fibrous tissue, leading to weakened bones and deformities.
5. Scoliosis: An abnormal curvature of the spine that can develop during childhood or adolescence. While not strictly a developmental bone disease, scoliosis can be caused by various underlying conditions such as cerebral palsy, muscular dystrophy, or spina bifida.
Treatment for developmental bone diseases varies depending on the specific condition and its severity. Treatment may include medication, physical therapy, bracing, or surgery to correct deformities and improve function. Regular follow-up with a healthcare provider is essential to monitor growth, manage symptoms, and prevent complications.
The metatarsus is the region in the foot between the tarsal bones (which form the hindfoot and midfoot) and the phalanges (toes). It consists of five long bones called the metatarsals, which articulate with the tarsal bones proximally and the phalanges distally. The metatarsus plays a crucial role in weight-bearing, support, and propulsion during walking and running. Any abnormalities or injuries to this region may result in various foot conditions, such as metatarsalgia, Morton's neuroma, or hammertoes.
I am not aware of a medical definition for the term "Isatis." It is a genus of flowering plants in the family Brassicaceae, also known as woad. Woad has been used traditionally for medicinal purposes, including as an anti-inflammatory and to treat skin conditions. However, it is not commonly used in modern medicine and does not have a specific medical definition associated with it. If you are referring to a different "Isatis," please provide more context so I can give a more accurate response.
A mandibular osteotomy is a surgical procedure that involves making a cut in the mandible (lower jawbone). This procedure is often performed to correct various dental and maxillofacial conditions such as jaw misalignment, sleep apnea, or jaw tumors. The specific type of osteotomy performed depends on the individual patient's needs and may involve making cuts at different locations along the mandible.
During the procedure, the surgeon makes an incision in the gum tissue to expose the mandible and then uses specialized instruments to make a precise cut in the bone. The surgeon can then move the jawbone into the desired position and secure it with plates, screws, or wires. In some cases, bone grafting may also be necessary to provide additional support.
After the procedure, patients may experience swelling, bruising, and discomfort, which can be managed with pain medication and cold compresses. Patients are usually advised to follow a soft diet for several weeks while the jaw heals. The recovery period can vary depending on the individual patient's healing process, but most patients can return to their normal activities within a few weeks.
Kyphosis is a medical term used to describe an excessive curvature of the spine in the sagittal plane, leading to a rounded or humped back appearance. This condition often affects the thoracic region of the spine and can result from various factors such as age-related degenerative changes, congenital disorders, Scheuermann's disease, osteoporosis, or traumatic injuries. Mild kyphosis may not cause any significant symptoms; however, severe cases can lead to pain, respiratory difficulties, and decreased quality of life. Treatment options typically include physical therapy, bracing, and, in some cases, surgical intervention.
The ulna is one of the two long bones in the forearm, the other being the radius. It runs from the elbow to the wrist and is located on the medial side of the forearm, next to the bone called the humerus in the upper arm. The ulna plays a crucial role in the movement of the forearm and also serves as an attachment site for various muscles.
Arthroplasty is a surgical procedure to restore the integrity and function of a joint. The term is derived from two Greek words: "arthro" meaning joint, and "plasty" meaning to mold or form. There are several types of arthroplasty, but most involve resurfacing the damaged joint cartilage with artificial materials such as metal, plastic, or ceramic.
The goal of arthroplasty is to relieve pain, improve mobility, and restore function in a joint that has been damaged by arthritis, injury, or other conditions. The most common types of arthroplasty are total joint replacement (TJR) and partial joint replacement (PJR).
In TJR, the surgeon removes the damaged ends of the bones in the joint and replaces them with artificial components called prostheses. These prostheses can be made of metal, plastic, or ceramic materials, and are designed to mimic the natural movement and function of the joint.
In PJR, only one side of the joint is resurfaced, typically because the damage is less extensive. This procedure is less invasive than TJR and may be recommended for younger patients who are still active or have a higher risk of complications from a full joint replacement.
Other types of arthroplasty include osteotomy, in which the surgeon cuts and reshapes the bone to realign the joint; arthrodesis, in which the surgeon fuses two bones together to create a stable joint; and resurfacing, in which the damaged cartilage is removed and replaced with a smooth, artificial surface.
Arthroplasty is typically recommended for patients who have tried other treatments, such as physical therapy, medication, or injections, but have not found relief from their symptoms. While arthroplasty can be highly effective in relieving pain and improving mobility, it is not without risks, including infection, blood clots, and implant failure. Patients should discuss the benefits and risks of arthroplasty with their healthcare provider to determine if it is the right treatment option for them.
The femoral head is the rounded, ball-like top portion of the femur (thigh bone) that fits into the hip socket (acetabulum) to form the hip joint. It has a smooth, articular cartilage surface that allows for smooth and stable articulation with the pelvis. The femoral head is connected to the femoral neck, which is a narrower section of bone that angles downward and leads into the shaft of the femur. Together, the femoral head and neck provide stability and range of motion to the hip joint.
Fracture healing is the natural process by which a broken bone repairs itself. When a fracture occurs, the body responds by initiating a series of biological and cellular events aimed at restoring the structural integrity of the bone. This process involves the formation of a hematoma (a collection of blood) around the fracture site, followed by the activation of inflammatory cells that help to clean up debris and prepare the area for repair.
Over time, specialized cells called osteoblasts begin to lay down new bone matrix, or osteoid, along the edges of the broken bone ends. This osteoid eventually hardens into new bone tissue, forming a bridge between the fracture fragments. As this process continues, the callus (a mass of newly formed bone and connective tissue) gradually becomes stronger and more compact, eventually remodeling itself into a solid, unbroken bone.
The entire process of fracture healing can take several weeks to several months, depending on factors such as the severity of the injury, the patient's age and overall health, and the location of the fracture. In some cases, medical intervention may be necessary to help promote healing or ensure proper alignment of the bone fragments. This may include the use of casts, braces, or surgical implants such as plates, screws, or rods.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Femoral head necrosis, also known as avascular necrosis of the femoral head, is a medical condition that results from the interruption of blood flow to the femoral head, which is the rounded end of the thigh bone that fits into the hip joint. This lack of blood supply can cause the bone tissue to die, leading to the collapse of the femoral head and eventually resulting in hip joint damage or arthritis.
The condition can be caused by a variety of factors, including trauma, alcohol abuse, corticosteroid use, radiation therapy, and certain medical conditions such as sickle cell disease and lupus. Symptoms may include pain in the hip or groin, limited range of motion, and difficulty walking. Treatment options depend on the severity and progression of the necrosis and may include medication, physical therapy, or surgical intervention.
'Leg length inequality' (LLIS) is a condition where there is a discrepancy in the lengths of an individual's lower extremities, specifically the bones of the thigh (femur) and/or the leg (tibia/fibula). This discrepancy can be congenital or acquired due to various causes such as fractures, infections, or surgical procedures. The inequality can lead to functional scoliosis, lower back pain, and other musculoskeletal issues. It is typically diagnosed through physical examination and imaging studies like X-rays, and may be treated with various methods including orthotics, shoe lifts, or in some cases, surgical intervention.
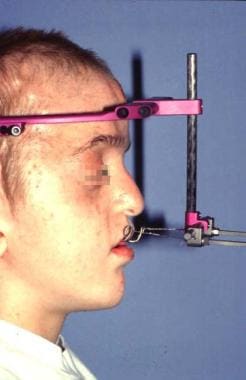
Osteogenesis, distraction refers to a surgical procedure and controlled rehabilitation process used in orthopedic surgery, oral and maxillofacial surgery, and neurosurgery to lengthen bones or correct bone deformities. The term "osteogenesis" means bone formation, while "distraction" refers to the gradual separation of bone segments.
In this procedure, a surgeon first cuts the bone (osteotomy) and then applies an external or internal distraction device that slowly moves apart the cut ends of the bone. Over time, new bone forms in the gap between the separated bone segments through a process called distraction osteogenesis. This results in increased bone length or correction of deformities.
Distraction osteogenesis is often used to treat various conditions such as limb length discrepancies, craniofacial deformities, and spinal deformities. The procedure requires careful planning, precise surgical technique, and close postoperative management to ensure optimal outcomes.
A forehead, in medical terms, refers to the portion of the human skull that lies immediately above the eyes and serves as an attachment site for the frontal bone. It is a common area for the examination of various clinical signs, such as assessing the level of consciousness (by checking if the patient's eyebrows or eyelids twitch in response to a light touch) or looking for signs of increased intracranial pressure (such as bulging fontanelles in infants). Additionally, the forehead is often used as a site for non-invasive procedures like Botox injections.
Bone screws are medical devices used in orthopedic and trauma surgery to affix bone fracture fragments or to attach bones to other bones or to metal implants such as plates, rods, or artificial joints. They are typically made of stainless steel or titanium alloys and have a threaded shaft that allows for purchase in the bone when tightened. The head of the screw may have a hexagonal or star-shaped design to allow for precise tightening with a screwdriver. Bone screws come in various shapes, sizes, and designs, including fully threaded, partially threaded, cannulated (hollow), and headless types, depending on their intended use and location in the body.
A "cheek" is the fleshy, muscular area of the face that forms the side of the face below the eye and above the jaw. It contains the buccinator muscle, which helps with chewing by moving food to the back teeth for grinding and also assists in speaking and forming facial expressions. The cheek also contains several sensory receptors that allow us to perceive touch, temperature, and pain in this area of the face. Additionally, there is a mucous membrane lining inside the mouth cavity called the buccal mucosa which covers the inner surface of the cheek.
 Le Fort osteotomy
Le Fort osteotomy
Le Fort III osteotomy
Le Fort fracture of skull
Open bite malocclusion
Surgically assisted rapid palatal expansion
Hugo Obwegeser
Arrhinia
William Harrison Bell
Le Fort III
Le Fort
List of MeSH codes (E04)
List of MeSH codes (E06)
List of orthopaedic eponyms
Index of trauma and orthopaedics articles
Jaw abnormality
Craniofacial cleft
Mandibular setback surgery
Bone fracture
Shan K. Bagby
Le Fort osteotomy - Wikipedia
 Osteotomy, Le Fort | Harvard Catalyst Profiles | Harvard Catalyst
Osteotomy, Le Fort | Harvard Catalyst Profiles | Harvard Catalyst
 Le Fort I osteotomy
Le Fort I osteotomy
 Halo-Distraction Le Fort III Osteotomy | Orange County Surgeons
Halo-Distraction Le Fort III Osteotomy | Orange County Surgeons
 Le fort i osteotomy: interest aspects in juvenile nasoangiobibroma management
Le fort i osteotomy: interest aspects in juvenile nasoangiobibroma management
 Mandibular Sagittal Split Osteotomy in Singapore - Compare Prices
Mandibular Sagittal Split Osteotomy in Singapore - Compare Prices
Acellular dermal matrix as an adjunct material in cleft le Fort i osteotomies<...
 Cephalometric Analysis of Hard and Soft Tissue Changes Following Anterior Maxillary Osteotomy Distraction in Cleft Maxillary...
Cephalometric Analysis of Hard and Soft Tissue Changes Following Anterior Maxillary Osteotomy Distraction in Cleft Maxillary...
Prognostic factors for maxillary sinus mucosal thickening following Le Fort I osteotomy: a retrospective analysis |...
 Le Fort I and Bilateral Sagittal Split Osteotomy for Correction of Mandibular Retrognathia, Vertical Maxillary Excess, and...
Le Fort I and Bilateral Sagittal Split Osteotomy for Correction of Mandibular Retrognathia, Vertical Maxillary Excess, and...
 Airway changes following Le Fort III distraction osteogenesis for syndromic craniosynostosis: a clinical and cephalometric study
Airway changes following Le Fort III distraction osteogenesis for syndromic craniosynostosis: a clinical and cephalometric study
 LeFort I Horizontal Osteotomy: Defining the Feasibility of the 'High Osteotomy'. | Cleft Palate Craniofac J;:...
LeFort I Horizontal Osteotomy: Defining the Feasibility of the 'High Osteotomy'. | Cleft Palate Craniofac J;:...
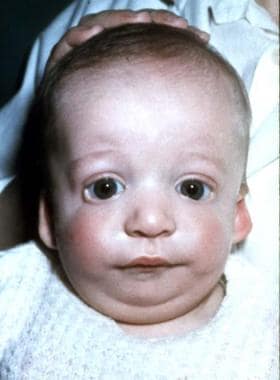
 Manifestations of Craniofacial Syndromes: Overview, Classification, Apert Syndrome
Manifestations of Craniofacial Syndromes: Overview, Classification, Apert Syndrome
 Atlas of Oral and Maxillofacial Surgery - Elsevier E-Book on VitalSource, 2nd Edition - 9780323789653
Atlas of Oral and Maxillofacial Surgery - Elsevier E-Book on VitalSource, 2nd Edition - 9780323789653
 Contemporary Surgical Planning For Jaw Deformities: A Free Online Resource by Houston Methodist Professional Publications -...
Contemporary Surgical Planning For Jaw Deformities: A Free Online Resource by Houston Methodist Professional Publications -...
 Distraction osteogenesis in the m... | Archive ouverte UNIGE
Distraction osteogenesis in the m... | Archive ouverte UNIGE
 Maxillary distraction osteogenesis versus orthognathic surgery for cleft patients | Cochrane
Maxillary distraction osteogenesis versus orthognathic surgery for cleft patients | Cochrane
Orthognathic Surgery: Background, History of the Procedure, Problem
 Platelet-rich fibrin in combination with mandibular or maxillary non-vascularized bone graft: a systematic review
Platelet-rich fibrin in combination with mandibular or maxillary non-vascularized bone graft: a systematic review
 What does the inside of the check look and feel like after a biopsy of the inside of a cheek?
What does the inside of the check look and feel like after a biopsy of the inside of a cheek?
 Apert Syndrome in an Infant
Apert Syndrome in an Infant
 Huddersfield Repository - University of Huddersfield
Huddersfield Repository - University of Huddersfield
 Orthognathic Surgery | Boston Children's Hospital
Orthognathic Surgery | Boston Children's Hospital
Suresh Pillai - نتاج البحث
 HKU Scholars Hub: Browsing DSpace
HKU Scholars Hub: Browsing DSpace
 Scientific database - Osstell®
Scientific database - Osstell®
 Acta Scientific | International Open Library | Open Access Journals Publishing Group
Acta Scientific | International Open Library | Open Access Journals Publishing Group
JOMR | Journal of Oral & Maxillofacial Research
Sagittal split ramus2
- sagittal split ramus osteotomy. (ejomr.org)
- This paper looked at 63 sagittal split ramus osteotomy sites. (entandaudiologynews.com)
Distraction12
- Retroposition of the Globe After Le Fort III Midfacial Distraction. (harvard.edu)
- During halo-distraction Le Fort III osteotomy, the nose, upper jaw, and cheek bones are moved together (and sometimes forward) in order to align with the forehead and chin. (orangecountysurgeons.org)
- Halo-distraction Le Fort III osteotomy is utilized in cases of Pfeiffer syndrome and congenital facial abnormality. (orangecountysurgeons.org)
- Halo-distraction Le Fort III osteotomy is performed under general anesthesia, which means that the patient is asleep and completely unaware during the procedure. (orangecountysurgeons.org)
- Possible risks following halo-distraction Le Fort III osteotomy include soreness, swelling, bruising, infection, bleeding, nerve damage and a negative reaction to the anesthesia. (orangecountysurgeons.org)
- The prognosis for a positive end result following halo-distraction Le Fort III osteotomy is very good. (orangecountysurgeons.org)
- Cheung LK, Chua HD (2006) A meta-analysis of cleft maxillary osteotomy and distraction osteogenesis. (springer.com)
- Markose E, Paulose J, Paul ET (2013) Soft tissue changes in cleft lip and palate patients: anterior maxillary distraction versus conventional Le-Fort I osteotomy. (springer.com)
- Le Fort III distraction osteogenesis improves midface form and dental relationships in patients with syndromic craniosynostosis, but its effect on the upper airway is not well documented. (nih.gov)
- A retrospective review was conducted of patients with syndromic craniosynostosis undergoing Le Fort III distraction osteogenesis from 2000 to 2006 (n = 20). (nih.gov)
- Le Fort III distraction osteogenesis significantly increases nasopharyngeal and velopharyngeal airspaces in patients with syndromic craniosynostosis. (nih.gov)
- Upper jaw was more stable in the distraction osteogenesis group than the conventional osteotomy group five years after surgery. (cochrane.org)
Orthognathic surgery4
- A type of surgery called orthognathic surgery, which involves surgical cutting of bone to realign the upper jaw (osteotomy), is usually performed in this situation. (cochrane.org)
- Conventional orthognathic surgery, such as Le Fort I osteotomy, is often performed for the correction of maxillary hypoplasia. (cochrane.org)
- Common procedures performed as part of our Orthognathic Surgery Program include Le Fort I osteotomy, bilateral sagittal split osteotomy, malar implants, and genioplasty. (childrenshospital.org)
- Six months after disjunction, bimaxillary orthognathic surgery was performed, with Le Fort I type osteotomy in the maxilla and bilateral sagittal osteotomy of the mandible. (actascientific.com)
Cleft2
- Does the Nostril Shape Change After Le Fort I Advancement in Patients With Unilateral Complete Cleft Lip? (harvard.edu)
- One (2.9%) osteotomy cut was above the level of the cleft superior alar crease, and no cuts were above the level of the non-cleft superior ala. (bvsalud.org)
Genioplasty1
- 4) Sliding osteotomy genioplasty, single piece. (essaywritemypaper.com)
Bilateral sagittal1
- Correct Your Lower Jaw MisalignmentInsurance ClaimableImmediate and Permanent ResultsNo Visible IncisionsA Bilateral Sagittal Split Osteotomy (BSSO) is performed to correct mal-alignment of jaws and teeth. (whatclinic.com)
Mandible1
- 6) Osteotomy of mandible, segmental. (essaywritemypaper.com)
Fracture3
- The LeFort I osteotomy is named after the fracture pattern originally described by Rene LeFort in 1901 that extends from the nasal septum, along the tooth apices, and through the pterygomaxillary junction. (wikipedia.org)
- Le Fort III osteotomy for the treatment of maxillary fractures with fracture of one or more facial bones. (harvard.edu)
- Fort described the classic lines of maxillary form of motivation and includes longtstandt fracture. (who.int)
Monobloc2
- Le Fort IV" has been used to describe a monobloc frontofacial osteotomy in 2000s French literature, but the use is heavily disputed. (wikipedia.org)
- In 2014, the same term was used by a Japanese group to describe a "monobloc minus Le Fort I" osteotomy. (wikipedia.org)
Advancement5
- Single jaw one-piece Le Fort I advancement surgery . (bvsalud.org)
- I recently had le fort I upper jaw advancement and feel like it isn't right. (bracesinfo.com)
- Do I require lefort 1 advancement? (bracesinfo.com)
- My surgeon says I wouldn't need lefort 1 advancement unless my ortho tilts my bottom front teeth out. (bracesinfo.com)
- This paper from Turkey divided 28 patients into three groups: those having a maxillary advancement osteotomy, those with a maxillary advancement and impaction, and those that underwent advancement with a yaw rotation. (entandaudiologynews.com)
Surgery5
- Mansour S, Burstone C, Legan H (1983) An evaluation of soft-tissue changes resulting from Le Fort I maxillary surgery. (springer.com)
- A year ago I had jaw surgery, maxillary osteotomy. (bracesinfo.com)
- Le Fort I osteotomy was popularized by Considering the psychological aspects, Obwegeser in the midt20th century as a neuroticism may have a negative effect standard procedure in maxillofacial surgery on the early postoperative phase but not to correct dentofacial deformities [ 4,5 ]. (who.int)
- VR Surgery is the first multi-sensory, holistic surgical training experience demonstrating Le Fort I osteotomy, a type of maxillofacial surgery, using Oculus Rift and Leap Motion devices. (hud.ac.uk)
- Experimental group participants learnt about the Le Fort I procedure using VR Surgery on an Oculus Rift. (hud.ac.uk)
20201
- 34 skeletally mature, nonsyndromic patients with unilateral CLP who underwent Le Fort I osteotomy between 2013 and 2020. (bvsalud.org)
Malocclusion2
- The Le Fort I osteotomy advances the jaw in case of malocclusion and maxillomandibular deformities. (wikipedia.org)
- Variables associated with stability after Le Fort I osteotomy for skeletal class III malocclusion. (harvard.edu)
Retrospective1
- Methods: This was a retrospective cohort study of patients with residual/recurrent oronasal fistulae who underwent Le Fort I osteotomy. (johnshopkins.edu)
Underwent1
- 3) Patient underwent osteotomy and discectomy of a single cervical spine vertebral segmet. (essaywritemypaper.com)
Anterior2
- AMOD is an extension of anterior maxillary osteotomy where the resulting segment anterior to the chosen site of vertical corticotomy cut is distracted with the help of hyrax screw through a tooth-borne appliance. (springer.com)
- 5) Reconstruction midface, Lefort II with anterior intrusion. (essaywritemypaper.com)
Patients3
- Au stade préopératoire, les raisons esthétiques constituaient le motif principal de la demande d'intervention pour95% des patients. (who.int)
- En postopératoire, 85% des patients se déclaraient satisfaits durésultatdel'interventionetquantàsoneffetsurleurqualitédevie.L'améliorationpostopératoirede l'esthétiquefacialedespatientsestapparueassociéeàuneaméliorationdelaqualitédeviepourtous lesaspectsconsidérés. (who.int)
- The surgical strategy was differently tailored in the two patients, respectively, using a Le Fort I/transclival and a Kawase approach. (surgicalneurologyint.com)
Abnormalities2
- The Le Fort III osteotomy treats midfacial abnormalities and deficiencies. (wikipedia.org)
- Le Fort III is often used also to correct craniofacial dysostosis and related facial abnormalities. (harvard.edu)
Clinics1
- We have all the information you need about public and private dental clinics that provide mandibular sagittal split osteotomy in Singapore. (whatclinic.com)
Deficiencies1
- Wassmund, in 1927, was the first ing inner feelings about deficiencies in surgeon to use an osteotomy line on Le Fort one's appearance. (who.int)
Deficiency2
- Purpose: To evaluate the use of acellular dermal matrix in the management of nasal lining deficiency at the time of Le Fort I osteotomy. (johnshopkins.edu)
- Conclusion: Acellular dermal matrix is a useful adjunct for managing nasal lining deficiency at the time of Le Fort I osteotomy. (johnshopkins.edu)
Procedure1
- To define "high osteotomy " and determine the feasibility of performing this procedure . (bvsalud.org)
Implants1
- Simultaneous Le Fort I osteotomy and zygomatic implants placement with delayed prosthetic rehabilitation. (osstell.com)
Split1
- Compare all the dentists and contact the mandibular sagittal split osteotomy clinic in Singapore that's right for you. (whatclinic.com)
Surgeon2
- They are based on the analogous bone fractures described by the French surgeon and physician René Le Fort. (wikipedia.org)
- My orthodontist said I should ask my surgeon if I should do lefort 1. (bracesinfo.com)
Bone1
- Residual alveolar clefts and oronasal fistulae can be successfully managed at the time of Le Fort I osteotomy using allograft bone and acellular dermal matrix. (johnshopkins.edu)
Include1
- The surgical approaches used for resection of these tumors include the approach transmaxillary (le fort I), transnasal, transpalatal, combined endoscopic and others. (bvsalud.org)
Types1
- A Le Fort osteotomy is the name for three types of osteotomies of the jaw and face. (wikipedia.org)
Year1
- This graph shows the total number of publications written about "Osteotomy, Le Fort" by people in Harvard Catalyst Profiles by year, and whether "Osteotomy, Le Fort" was a major or minor topic of these publication. (harvard.edu)