Oliguria
Anuria
Acute Kidney Injury
Kidney Tubular Necrosis, Acute
Risk factors for death and changing patterns in leptospirosis acute renal failure. (1/78)
The risk factors for death and changes in clinical patterns in leptospirosis (Weil's disease) have not been well studied. We retrospectively studied 110 patients with Weil's disease hospitalized in Brazil between 1985 and 1996. Univariate statistical analysis showed that nonsurvivors were older than survivors, and had higher frequency of oliguria, cardiac arrhythmia, dyspnea, and pulmonary rales. Logistic regression showed that the only independent factor associated with death was oliguria (odds ratio [OR] = 8.98). The presence of arthralgia (OR = 4.71), dehydration (OR = 6.26), dyspnea (OR = 17.7), and pulmonary rales (OR = 9.91) increased after 1994. These data suggest that in Weil's disease the clinical patterns have changed and the presence of oliguria is a risk factor for death. (+info)Nutritional aspects of high-altitude exposure in women. (2/78)
The nutrient intake and urinary excretion characteristics of eight young university women were studied over a 4-day period at low altitude (140 m) and subsequently over a 7-day sojourn on Pikes Peak (4,300 m). High-altitude exposure was associated with a transient decrease in the consumption of protein, carbohydrate, fat, sodium, calcium, phosphorus, vitamin A, riboflavin, thiamin, and niacin and a more sustained decrease in the consumption of potassium and ascorbic acid. In most instances minimal values were observed during the first 3 days of exposure. The carbohydrate fraction of energy intake was increased at the expense of fat during this time period. Individual hypophagic responses appeared to be related to severity of acute mountain sickness. Altitude had no effect on water consumption but did lead to an average body weight loss of 1 kg. Urinary measurements revealed a marked oliguria during the entire sojourn. These measurements also showed the first 3 days to be associated with a net loss of body nitrogen and sodium. During this time period body potassium and phosphorus were conserved, and probably increased. The urea fraction of body potassium and phosphorus were conserved, and probably increased. The urea fraction of total urinary nitrogen was not affected by altitude exposure, nor was the daily excretion of uric acid and creatinine. Ammonia excretion, however, was reduced to 50% of the low-altitude value and remained at this level throughout the sojourn. With a few exceptions, the qualitative characteristics of altitude hypophagia in women were similar to those reported for men. Quantitatively, however, the responses were much more transient in women. (+info)Treatment-related acute renal failure in the elderly: a hospital-based prospective study. (3/78)
BACKGROUND: Elderly individuals need a host of diagnostic procedures and therapeutic interventions to take care of ailments. This prospective study was carried out to determine the magnitude of treatment-related acute renal failure (ARF) in the elderly in a hospital setting, to know about pathogenetic factors and to study the factors that could predict an adverse outcome. METHODS: All elderly patients (>60 years) admitted over a 12-month period were screened prospectively throughout their hospital stay for the development of ARF. RESULTS: Of 31860 patients admitted, 4176 (13%) were elderly. Of these 59 (1.4%) developed ARF in the hospital. Nephrotoxic drugs contributed towards development of ARF in 39 (66%), sepsis and hypoperfusion in 27 (45.7%) each, contrast medium in 10 (16.9%) and postoperative ARF occurred in 15 (25.4%) patients. These pathogenetic factors were responsible for ARF in different combinations. Amongst these combination of pathogenetic factors, radiocontrast administration (partial chi(2) 28.1, P<0.0001), surgery (partial chi(2) 14.89, P=0.001), and drugs (partial chi(2) 6. 22, P=0.0126) predicted ARF on their own. Nine patients (15.23%) needed dialytic support. Of 59 patients, 15 (25.4%) died, of those who survived, 38 (86.3%) recovered renal function completely and six (13.6%) partially. Mortality in the elderly with ARF was significantly higher than in those without ARF (25.4 vs 12.5%; chi(2) 8.3, P=0.03). Sepsis (odds ratio 43), oliguria (odds ratio 64), and hypotension (odds ratio 15) were independent predictors of poor patient outcome on logistic regression analysis. CONCLUSION: Incidence of treatment-related ARF in the elderly was 1.4%, with more than one pathogenetic factor playing a role in the development of ARF in the majority. Sepsis, hypotension, and oliguria were the independent predictors of poor patient outcome. (+info)The mechanism of acute renal failure after uranyl nitrate. (4/78)
Administration of 25 mg/kg uranyl nitrate (UN) to rats leads to a brief period of polyuria followed by progressive oliguria with death at 5 days. Factors that determine glomerular filtration rate (GFR) were examined in control Munich-Wistar rats (n equals 16) and 2 h after either 15 mg/kg (n equals 8) or 25 mg/kg (n equals 7) of UN (i.v.) utilizing direct measurements of hydrostatic and oncotic pressures and plasma flow. Total kidney GFR was reduced to 47% of control in the low dose group and to 21% in the high dose group. The simultaneous nephron filtration rate (sngfr) was 28.6 plus or minus 0.8 nl/min/g kidney wt in control, 29.1 plus or minus 1.0 in the low dose group, and 18.1 plus or minus 1.2 (P less than 0.001) in the higher dose group. This disparity in UN effect upon GFR and sngfr was due to tubular back-diffusion of solute through damaged epithelia beyond the early proximal tubule as demonstrated by microinjection of inulin and mannitol in the proximal tubule. Inulin "leak" persisted at 6 h after UN when tubular pressure had returned to normal. Comparison of sngfr measured in early vs. late proximal tubule revealed no difference after high dose UN, suggesting no significant leak of inulin from the early proximal tubule, and that the decreased sngfr was due to primary reductions in ultrafiltration. Nephron plasma flow was equal to control at both doses of UN. Also directly measured hydrostatic pressure gradient across the glomerular capillary was not changed. The effective filtration pressure achieved equilibrium in control of animals but became significantly positive at the efferent end of the capillary at both doses of UN and increased. Total glomerular permeability (LpA) was progressively reduced from control (0.089 plus or minus 0.005 nl/s/g kidney wt/mm Hg) at low dose UN (0.047 plus or minus 0.013) and high dose 0.024 plus or minus 0.003 nl/s/g kidney wt/mm Hg). Therefore UN decreases GFR by two mechanisms: (1) tubular damage leading to back-diffusion of solutes and (b) a primary reduction in sngfr due to reduced LpA. (+info)Use of radionuclide imaging in the early diagnosis and treatment of renal allograft rejection. (5/78)
Data are presented on the clinical application of radionuclide imaging to evaluate changes in cadaver transplant function in the immediate postoperative period. The method uses orthoiodohippuric acid (hippuran) administered IV, with scintillation imaging, and curve analysis by a digital computer. An initial study is always obtained 24 hours after transplantation. Serial studies are then obtained, as needed, to interpret the clinical course. Selected cases are presented which illustrate the use of this protocol in various clinical settings. In the oliguric patient serial studies have been of particular value. They have identified ATN so that over-enthusiastic treatment for rejection could be avoided. They have also identified acute rejection complicating ATN so that high dose steroid therapy could be administered appropriately. In the non-oliguric patient they have frequently contributed to the early diagnosis of acute rejection, and they have been useful in monitoring the effect and duration of treatment for severe rejection crisis. It is concluded that radionuclide imaging studies, when carefully applied and interpreted, are a valuable adjunct to the management of patients in this complex clinical setting. (+info)A comparison of ibuprofen and indomethacin for closure of patent ductus arteriosus. (6/78)
BACKGROUND: Indomethacin is the conventional treatment for hemodynamically important patent ductus arteriosus in preterm infants. However, its use is associated with various side effects. In a prospective study, we compared ibuprofen and indomethacin with regard to efficacy and safety for the early treatment of patent ductus arteriosus in preterm infants. METHODS: We studied 148 infants (gestational age, 24 to 32 weeks) who had the respiratory distress syndrome and an echocardiographically confirmed, hemodynamically important patent ductus arteriosus. The infants were randomly assigned at five neonatal intensive care centers to receive three intravenous doses of either indomethacin (0.2 mg per kilogram of body weight, given at 12-hour intervals) or ibuprofen (a first dose of 10 mg per kilogram, followed at 24-hour intervals by two doses of 5 mq per kilogram each), starting on the third day of life. The rate of ductal closure, the need for additional treatment, side effects, complications, and the infants' clinical course were recorded. RESULTS: The rate of ductal closure was similar with the two treatments: ductal closure occurred in 49 of 74 infants given indomethacin (66 percent), and in 52 of 74 given ibuprofen (70 percent) (relative risk, 0.94; 95 percent confidence interval, 0.76 to 1.17; P=0.41). The numbers of infants who needed a second pharmacologic treatment or surgical ductal ligation did not differ significantly between the two groups. Oliguria occurred in 5 infants treated with ibuprofen and in 14 treated with indomethacin (P=0.03). There were no significant differences with respect to other side effects or complications. CONCLUSIONS: Ibuprofen therapy on the third day of life is as efficacious as indomethacin for the treatment of patent ductus arteriosus in preterm infants with the respiratory distress syndrome and is significantly less likely to induce oliguria. (+info)Effect of the selective adenosine A1-receptor antagonist KW-3902 on lipopolysaccharide-induced reductions in urine volume and renal blood flow in anesthetized dogs. (7/78)
We investigated the effects of KW-3902 (8-noradamantan-3-yl-1,3-dipropylxanthine), a potent and selective adenosine A1-receptor antagonist, on lipopolysaccharide (LPS)-induced reduction of urine volume (UV) in anesthetized dogs, in comparison with those of furosemide. LPS was intravenously administered at a dose of 0.5 mg/kg; and the heart rate (HR), systemic blood pressure (BP), renal blood flow (RBF) and UV were measured every 15 min for 4 h. Administration of LPS continuously decreased HR, BP, RBF and UV. KW-3902, furosemide or their corresponding vehicle was given as a bolus injection 5 min after the LPS injection. Treatment with KW-3902 (1 mg/kg, i.v.) ameliorated the LPS-induced decline of UV and RBF. Furosemide (3.2 mg/kg, i.v.) tended to ameliorate the LPS-induced decline of UV but not RBF, the duration of the effect being shorter than that of KW-3902. These results suggest that KW-3902 can ameliorate the oliguria and the decrease in RBF during the early phase of LPS-induced shock. Endogenous adenosine may be involved in the endotoxin-induced oliguria via the adenosine A1-receptor. (+info)Daily hemodialysis and the outcome of acute renal failure. (8/78)
BACKGROUND: Intermittent hemodialysis is widely used as renal-replacement therapy in patients with acute renal failure, but an adequate dose has not been defined. We performed a prospective study to determine the effect of daily intermittent hemodialysis, as compared with conventional (alternate-day) intermittent hemodialysis, on survival among patients with acute renal failure. METHODS: A total of 160 patients with acute renal failure were assigned to receive daily or conventional intermittent hemodialysis. Survival was the primary end point of the study. The duration of acute renal failure and the frequency of therapy-related complications were secondary end points. RESULTS: The two study groups were similar with respect to age, sex, cause and severity of acute renal failure, medical or surgical intensive care setting, and the score on the Acute Physiology, Age, and Chronic Health Evaluation. Daily hemodialysis resulted in better control of uremia, fewer hypotensive episodes during hemodialysis, and more rapid resolution of acute renal failure (mean [+/-SD], 9+/-2 vs. 16+/-6 days; P=0.001) than did conventional hemodialysis. The mortality rate, according to the intention-to-treat analysis, was 28 percent for daily dialysis and 46 percent for alternate-day dialysis (P=0.01). In a multiple regression analysis, less frequent hemodialysis (on alternate days, as opposed to daily) was an independent risk factor for death. CONCLUSIONS: The high mortality rate among critically ill patients with acute renal failure who require renal-replacement therapy is related to both coexisting conditions and uremic damage to other organ systems. Intensive hemodialysis reduces mortality without increasing hemodynamically induced morbidity. (+info)Oliguria is a medical term that refers to a condition where the urine output is significantly reduced, typically defined as less than 400 milliliters (or about 13 ounces) in 24 hours for an adult. This condition can be a sign of underlying kidney dysfunction or other medical conditions that affect urine production, such as dehydration, shock, or obstruction of the urinary tract. It is important to note that oliguria can be a serious symptom and requires prompt medical attention to determine the cause and initiate appropriate treatment.
Anuria is a medical condition characterized by the absence or near-absence of urine output, typically defined as less than 100 milliliters in 24 hours. This occurs when the kidneys are unable to produce urine due to a complete or nearly complete failure of both kidneys' function. Anuria can be caused by various underlying medical conditions such as severe dehydration, kidney damage, obstruction in the urinary tract, or certain medications that affect kidney function. It is considered a serious medical emergency and requires immediate evaluation and treatment to prevent further complications, including potential permanent kidney damage or even death.
Acute kidney injury (AKI), also known as acute renal failure, is a rapid loss of kidney function that occurs over a few hours or days. It is defined as an increase in the serum creatinine level by 0.3 mg/dL within 48 hours or an increase in the creatinine level to more than 1.5 times baseline, which is known or presumed to have occurred within the prior 7 days, or a urine volume of less than 0.5 mL/kg per hour for six hours.
AKI can be caused by a variety of conditions, including decreased blood flow to the kidneys, obstruction of the urinary tract, exposure to toxic substances, and certain medications. Symptoms of AKI may include decreased urine output, fluid retention, electrolyte imbalances, and metabolic acidosis. Treatment typically involves addressing the underlying cause of the injury and providing supportive care, such as dialysis, to help maintain kidney function until the injury resolves.
Acute Kidney Tubular Necrosis (ATN) is a medical condition characterized by the death of tubular epithelial cells that make up the renal tubules of the kidneys. This damage can occur as a result of various insults, including ischemia (lack of blood flow), toxins, or medications.
In ATN, the necrosis of the tubular cells leads to a decrease in the kidney's ability to concentrate urine, regulate electrolytes and remove waste products from the body. This can result in symptoms such as decreased urine output, fluid and electrolyte imbalances, and the accumulation of waste products in the blood (azotemia).
Acute Kidney Tubular Necrosis is usually diagnosed based on clinical findings, laboratory tests, and imaging studies. Treatment typically involves supportive care, such as administering intravenous fluids to maintain hydration and electrolyte balance, managing any underlying conditions that may have contributed to the development of ATN, and providing dialysis if necessary to support kidney function until the tubular cells can recover.
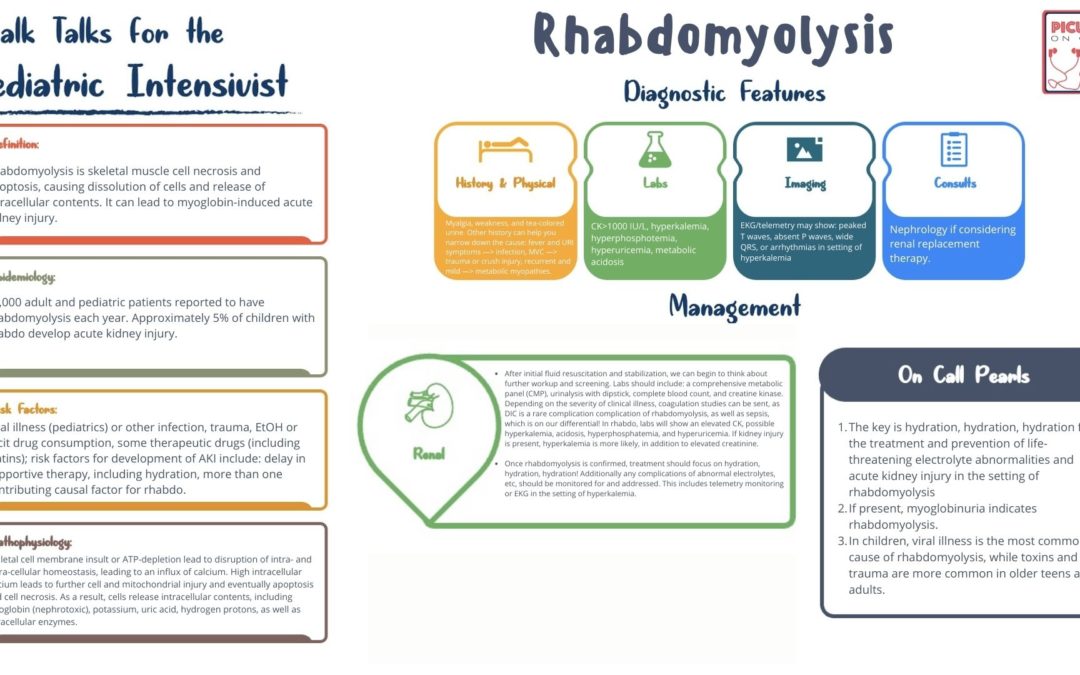
Rhabdomyolysis is a medical condition characterized by the breakdown and degeneration of skeletal muscle fibers, leading to the release of their intracellular contents into the bloodstream. This can result in various complications, including electrolyte imbalances, kidney injury or failure, and potentially life-threatening conditions if not promptly diagnosed and treated.
The process of rhabdomyolysis typically involves three key components:
1. Muscle injury: Direct trauma, excessive exertion, prolonged immobilization, infections, metabolic disorders, toxins, or medications can cause muscle damage, leading to the release of intracellular components into the bloodstream.
2. Release of muscle contents: When muscle fibers break down, they release various substances, such as myoglobin, creatine kinase (CK), lactate dehydrogenase (LDH), aldolase, and potassium ions. Myoglobin is a protein that can cause kidney damage when present in high concentrations in the bloodstream, particularly when it is filtered through the kidneys and deposits in the renal tubules.
3. Systemic effects: The release of muscle contents into the bloodstream can lead to various systemic complications, such as electrolyte imbalances (particularly hyperkalemia), acidosis, hypocalcemia, and kidney injury or failure due to myoglobin-induced tubular damage.
Symptoms of rhabdomyolysis can vary widely depending on the severity and extent of muscle damage but may include muscle pain, weakness, swelling, stiffness, dark urine, and tea-colored or cola-colored urine due to myoglobinuria. In severe cases, patients may experience symptoms related to kidney failure, such as nausea, vomiting, fatigue, and decreased urine output.
Diagnosis of rhabdomyolysis typically involves measuring blood levels of muscle enzymes (such as CK and LDH) and evaluating renal function through blood tests and urinalysis. Treatment generally focuses on addressing the underlying cause of muscle damage, maintaining fluid balance, correcting electrolyte imbalances, and preventing or managing kidney injury.
Dysuria is a medical term that describes painful or difficult urination. This symptom can be caused by various conditions, including urinary tract infections (UTIs), bladder infections, kidney stones, enlarged prostate, and certain sexually transmitted infections (STIs). Dysuria can also occur as a side effect of certain medications or medical procedures.
The pain or discomfort associated with dysuria can range from a burning sensation to a sharp stabbing pain, and it may occur during urination, immediately after urination, or throughout the day. Other symptoms that may accompany dysuria include frequent urination, urgency to urinate, cloudy or strong-smelling urine, blood in the urine, and lower abdominal or back pain.
If you are experiencing dysuria, it is important to seek medical attention promptly to determine the underlying cause and receive appropriate treatment. In many cases, dysuria can be treated effectively with antibiotics, medications, or other interventions.
A critical illness is a serious condition that has the potential to cause long-term or permanent disability, or even death. It often requires intensive care and life support from medical professionals. Critical illnesses can include conditions such as:
1. Heart attack
2. Stroke
3. Organ failure (such as kidney, liver, or lung)
4. Severe infections (such as sepsis)
5. Coma or brain injury
6. Major trauma
7. Cancer that has spread to other parts of the body
These conditions can cause significant physical and emotional stress on patients and their families, and often require extensive medical treatment, rehabilitation, and long-term care. Critical illness insurance is a type of insurance policy that provides financial benefits to help cover the costs associated with treating these serious medical conditions.
 Oliguria
Oliguria
Kidney failure
Nephritis
Polyuria
Lung (Chinese medicine)
Ovarian hyperstimulation syndrome
Rapidly progressive glomerulonephritis
Grape toxicity in dogs
Urine
Urinary system
Scurvy
Nephrotic syndrome
Liquidambar formosana
Salmonellosis
Ischemic hepatitis
Salmonella
Hypovolemia
Echis carinatus
List of dangerous snakes
Dolichandra unguis-cati
Acute proliferative glomerulonephritis
Ricin
Anuria
Sepsis
Malarial nephropathy
ACE inhibitor
Hypovolemic shock
McKittrick-Wheelock syndrome
Liver support system
Killip class
Oliguria - Wikipedia
 Oliguria: Practice Essentials, Background, Etiology
Oliguria: Practice Essentials, Background, Etiology
oliguria Mammalian Phenotype Term (MP:0003620)
Abdominal Pain, Anemia, and Oliguria in a Distressed Woman
 Oliguria - Critical Care Medicine - MSD Manual Professional Edition
Oliguria - Critical Care Medicine - MSD Manual Professional Edition
Oliguria: Background, Etiology, Epidemiology
 Management of oliguria - OSCEstop
Management of oliguria - OSCEstop
Oliguria other imaging findings - wikidoc
Oliguria and Anuria definition and causes
 Oliguria and Urinary Electrolytes - Crashing Patient
Oliguria and Urinary Electrolytes - Crashing Patient
 Common oliguria puckering, occurring: antipsychotic case.
Common oliguria puckering, occurring: antipsychotic case.
 oliguria | BELLEZZA - COSMETICI- CURA DEL CORPO - CONSULENZA
oliguria | BELLEZZA - COSMETICI- CURA DEL CORPO - CONSULENZA
 Association between urinary TIMP-2 and IGFBP7 as early biomarkers of AKI and oliguria during liver surgery: a prospective pilot...
Association between urinary TIMP-2 and IGFBP7 as early biomarkers of AKI and oliguria during liver surgery: a prospective pilot...
Preeclampsia: Practice Essentials, Overview, Pathophysiology
Table 1 - Leptospirosis-associated Severe Pulmonary Hemorrhagic Syndrome, Salvador, Brazil - Volume 14, Number 3-March 2008 -...
 Arsenic Toxicity: Clinical Assessment | Environmental Medicine | ATSDR
Arsenic Toxicity: Clinical Assessment | Environmental Medicine | ATSDR
Ricin: Biotoxin | NIOSH | CDC
Acute Glomerulonephritis Clinical Presentation: History, Physical Examination, Complications
 Mannitol
Mannitol
 Chelation Therapy - Medical Clinical Policy Bulletins | Aetna
Chelation Therapy - Medical Clinical Policy Bulletins | Aetna
 DailyMed - DEXMEDETOMIDINE HCL injection
DailyMed - DEXMEDETOMIDINE HCL injection
DailyMed - ARSENIC TRIOXIDE injection, solution
 Intensive Care Medicine 1/2023 | springermedizin.de
Intensive Care Medicine 1/2023 | springermedizin.de
 Corlopam (Fenoldopam Mesylate Injection): Uses, Dosage, Side Effects, Interactions, Warning
Corlopam (Fenoldopam Mesylate Injection): Uses, Dosage, Side Effects, Interactions, Warning
 Approach to shock - EMCrit Project
Approach to shock - EMCrit Project
 Acute Kidney Injury
Acute Kidney Injury
 SIRS to Septic Shock
SIRS to Septic Shock
 Lunesta: Insomnia Medication Treatment (Full Prescribing Information) | HealthyPlace
Lunesta: Insomnia Medication Treatment (Full Prescribing Information) | HealthyPlace
 SciELO - MedicalExpress, Volume: 3, Issue: 3, Published: 2016
SciELO - MedicalExpress, Volume: 3, Issue: 3, Published: 2016Anuria3
- Beyond oliguria is anuria, which represents an absence of urine, clinically classified as below 80 or 100 ml/day. (wikipedia.org)
- In some patients the syndrome is distinguished by oliguria or anuria, but today this classical feature of ARF is less predictable. (vin.com)
- Oliguria and less frequently anuria were at one time considered signatures of ARF and discriminators for chronic renal failure. (vin.com)
Urine output4
- Oliguria is defined as a urine output that is less than 1 mL/kg/h in infants, less than 0.5 mL/kg/h in children, and less than 400 mL or 500 mL per 24h in adults - this equals 17 or 21 mL/hour. (wikipedia.org)
- A standardized definition of AKI has been proposed by the Kidney Disease: Improving Global Outcomes (KDIGO) AKI working group, which identifies and stages AKI based on changes in serum creatinine from baseline or a decrease in urine output (oliguria) as shown below. (medscape.com)
- However, over the past week, the patient's urine output began to decrease markedly (oliguria). (weber.edu)
- Oliguria can be defined as urine output of less than or equal to 0.5 or 1 ml/kg/hr depending on the age. (bvsalud.org)
Transient oliguria2
Acute tubular1
- Persistent oliguria from acute tubular necrosis can result in acute renal failure. (aafp.org)
Renal failure2
- In most clinical situations, acute oliguria is reversible and does not result in intrinsic renal failure. (medscape.com)
- Oliguria and renal failure often occur 1 to 3 days after exposure (1-3). (cdc.gov)
Abdominal Pain1
- Cite this: Abdominal Pain, Anemia, and Oliguria in a Distressed Woman - Medscape - Apr 30, 2021. (medscape.com)
Perfusion1
- Rapid reversibility of oliguria following timely reestablishment of renal perfusion is an important characteristic and is the usual scenario in prerenal insufficiency. (medscape.com)
Edema1
- During June 1-4, he became progressively hypoxemic and developed pulmonary alveolar edema and oliguria. (cdc.gov)
Prerenal1
- Oliguria may result from prerenal, intrinsic renal, or postrenal processes. (medscape.com)
Output1
- Oliguria or hypouresis is the low output of urine specifically more than 80 ml/day but less than 400ml/day. (wikipedia.org)
Creatinine1
- In addition, oliguria that lasted more than 12 hours (KDIGO stage 2 or 3) was associated with higher 90-day mortality, regardless of changes in serum creatinine levels. (medscape.com)
Kidney2
- Not all cases of acute kidney injury are characterized by oliguria. (medscape.com)
- This pilot study demonstrated the association between [TIMP-2]*[IGFBP7] increase and oliguria and may therefore indicate kidney damage during liver surgery. (biomedcentral.com)
Patient1
- Six hours after initial complaint of oliguria, patient started to complain of difficulty in breathing and pain in epigastric area. (hindawi.com)
Patients1
- Cette étude a permis de déterminer la fréquence et l'étiologie de l'insuffisance rénale aiguë chez des patients hospitalisés en Arabie saoudite sur une période de 2 ans. (who.int)
Frequently1
- At onset, oliguria is frequently acute. (medscape.com)
Common2
- Common oliguria puckering, occurring: antipsychotic case. (studiokregoslupa.pl)
- Reply To: Common oliguria puckering, occurring: antipsychotic case. (studiokregoslupa.pl)
Urine output of less1
- Oliguria can be defined as urine output of less than or equal to 0.5 or 1 ml/kg/hr depending on the age. (bvsalud.org)
Acute kidney1
- Not all cases of acute kidney injury are characterized by oliguria. (medscape.com)
Hypotension1
- Infants with histories of in utero exposure to an angiotensin II receptor antagonist should be closely observed for hypotension, oliguria, and hyperkalemia. (druglib.com)
Anemia1
- Cite this: Abdominal Pain, Anemia, and Oliguria in a Distressed Woman - Medscape - Apr 30, 2021. (medscape.com)
Baseline1
- A standardized definition of AKI has been proposed by the Kidney Disease: Improving Global Outcomes (KDIGO) AKI working group, which identifies and stages AKI based on changes in serum creatinine from baseline or a decrease in urine output (oliguria) as shown below. (medscape.com)
Blood1
- If oliguria occurs, attention should be directed toward support of blood pressure and renal perfusion. (druglib.com)
Code1
- oliguria) Are we supposed to code it as T86.12 (failure) or T86.19 (other comps of renal tra. (aapc.com)