Nephrotic Syndrome
Nephrosis, Lipoid
Glomerulonephritis, Membranous
Glomerulosclerosis, Focal Segmental
Puromycin Aminonucleoside
Kidney Glomerulus
Prednisolone
Podocytes
Glomerulonephritis
Steroids
Glomerulonephritis, Membranoproliferative
Nephrosis
Kidney
Immunosuppressive Agents
Edema
Biopsy
Down Syndrome
Cyclosporine
Metabolic Syndrome X
Amyloidosis
Drug Resistance
Adrenal Cortex Hormones
Serum Albumin
Glucocorticoids
Prednisone
Remission, Spontaneous
Remission Induction
Treatment Outcome
Paraneoplastic Syndromes
Sjogren's Syndrome
Abnormalities, Multiple
Chlorambucil
Membrane Proteins
Albumins
Glomerulonephritis, IGA
Levamisole
Glomerular Basement Membrane
Retrospective Studies
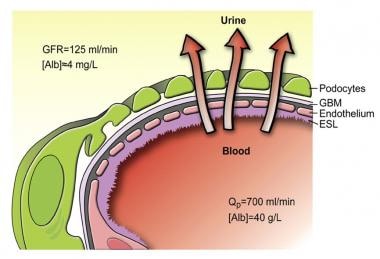
Glomerular Filtration Barrier
Kidney Function Tests
Plasmapheresis
Frasier Syndrome
Drug Therapy, Combination
Turner Syndrome
Intracellular Signaling Peptides and Proteins
Fitzgerald factor (high molecular weight kininogen) clotting activity in human plasma in health and disease in various animal plasmas. (1/1128)
Fitzgerald factor (high molecular weight kininogen) is an agent in normal human plasma that corrects the impaired in vitro surface-mediated plasma reactions of blood coagulation, fibrinolysis, and kinin generation observed in Fitzgerald trait plasma. To assess the possible pathophysiologic role of Fitzgerald factor, its titer was measured by a functional clot-promoting assay. Mean +/- SD in 42 normal adults was 0.99+/-0.25 units/ml, one unit being the activity in 1 ml of normal pooled plasma. No difference in titer was noted between normal men and women, during pregnancy, or after physical exercise. Fitzgerald factor activity was significantly reduced in the plasmas of eight patients with advanced hepatic cirrhosis (0.40+/-0.09 units/ml) and of ten patients with disseminated intravascular coagulation (0.60+/-0.30 units/ml), but was normal in plasmas of patients with other congenital clotting factor deficiencies, nephrotic syndrome, rheumatoid arthritis, systemic lupus erythematosus, or sarcoidosis, or under treatment with warfarin. The plasmas of 21 mammalian species tested appeared to contain Fitzgerald factor activity, but those of two avian, two repitilian, and one amphibian species did not correct the coagulant defect in Fitzgerald trait plasmas. (+info)Hypoalbuminemia increases lysophosphatidylcholine in low-density lipoprotein of normocholesterolemic subjects. (2/1128)
BACKGROUND: A phospholipid, lysophosphatidylcholine (LPC), is the major determinant of the atherosclerotic properties of oxidized low-density lipoprotein (LDL). Under normal circumstances most LPC is bound to albumin. We hypothesized that lipoprotein LPC concentrations are increased in hypoalbuminemic patients with the nephrotic syndrome, irrespective of their lipid levels. To test this hypothesis, we selected nephrotic and control subjects with matched LDL cholesterol levels. METHODS: Lipoproteins and the albumin-rich lipoprotein-deficient fractions were separated by ultracentrifugation and their phospholipid composition was analyzed by thin-layer chromatography. RESULTS: Nephrotic subjects (albumin 23 +/- 2 g/liter and LDL cholesterol 3.1 +/- 0.2 mmol/liter) had a LDL LPC concentration that was increased (P < 0.05) to 66 +/- 7 vs. 35 +/- 6 micromol/liter in matched controls (albumin 42 +/- 5 g/liter and LDL cholesterol 3.1 +/- 0.2 mmol/liter). LPC in very low-density lipoprotein plus intermediate-density lipoprotein (VLDL + IDL) in these subjects was also increased to 33 +/- 7 vs. 9 +/- 2 micromol/liter in controls (P < 0.05). Conversely, LPC was decreased to 19 +/- 4 micromol/liter in the albumin-containing fraction of these hypoalbuminemic patients, as compared to 46 +/- 10 micromol/liter in the controls (P < 0.05). LPC was also low (14 +/- 4 micromol/liter) in the albumin-containing fraction of hypoalbuminemic, hypocholesterolemic patients with nonrenal diseases. In hyperlipidemic nephrotic subjects (albumin 21 +/- 2 g/liter and LDL cholesterol 5.7 +/- 0.5 mmol/liter) the LPC levels in LDL and VLDL + IDL were further increased, to 95 +/- 20 and 56 +/- 23 micromol/liter, respectively (P < 0.05). CONCLUSION: These findings suggest that in the presence of hypoalbuminemia in combination with proteinuria, LPC shifts from albumin to VLDL, IDL and LDL. This effect is independent of hyperlipidemia. Increased LPC in lipoproteins may be an important factor in the disproportionate increase in cardiovascular disease in nephrotic patients with hypoalbuminemia. (+info)Circulating vascular endothelial growth factor is not increased during relapses of steroid-sensitive nephrotic syndrome. (3/1128)
BACKGROUND: An uncharacterized circulating factor that increases vascular permeability has previously been described in childhood steroid-sensitive nephrotic syndrome (SSNS). The aim of this study was to determine whether this factor is vascular endothelial growth factor (VEGF), the recently described endothelial cell mitogen and enhancer of vascular permeability. METHODS: Plasma and urine VEGF levels were measured in children with SSNS in both relapse and remission and in normal age- and sex-matched controls. Semiquantitative reverse transcriptase-polymerase chain reaction studies investigating VEGF mRNA expression were performed on peripheral blood mononuclear cells isolated from children with SSNS in relapse and controls. In two experimental models (one-hour and three-day follow-up postinfusion), Sprague-Dawley rats were intravenously administered 50 microg rVEGF to determine whether this induced either proteinuria or glomerular histologic change. RESULTS: Plasma VEGF levels and urine VEGF/creatinine ratios were not elevated in SSNS relapse compared with remission and control samples. Peripheral blood mononuclear cell VEGF mRNA expression was no different in SSNS patients compared with controls. The administration of VEGF to rats induced an acute reversible fall in systemic blood pressure but did not result in the development of either proteinuria or glomerular histologic change. CONCLUSION: Increased circulating VEGF levels are not responsible for the proteinuria observed during relapses of SSNS. Further studies are warranted to investigate intrarenal VEGF expression. (+info)Nephrotic syndrome as a clinical manifestation of graft-versus-host disease (GVHD) in a marrow transplant recipient after cyclosporine withdrawal. (4/1128)
GVHD is one of the most frequent complications of BMT and recently nephrotic syndrome (NS) has been described as a manifestation of chronic GVHD. Here, we present an AA patient who developed NS 1 year after BMT when cyclosporine was stopped. Renal biopsy showed focal sclerosis associated with membranous deposits. He also had other clinical manifestations of chronic GVHD: sicca-like syndrome and colestasis. After 15 days of CsA therapy, he experienced a remarkable improvement in the NS and GVHD as a whole. We comment on immunological mechanisms that could be involved in the pathogenesis of this manifestation. (+info)Acute haemodynamic and proteinuric effects of prednisolone in patients with a nephrotic syndrome. (5/1128)
BACKGROUND: Administration of prednisolone causes an abrupt rise in proteinuria in patients with a nephrotic syndrome. METHODS: To clarify the mechanisms responsible for this increase in proteinuria we have performed a placebo controlled study in 26 patients with a nephrotic syndrome. Systemic and renal haemodynamics and urinary protein excretion were measured after prednisolone and after placebo. RESULTS: After i.v. administration of 125-150 mg prednisolone total proteinuria increased from 6.66+/-4.42 to 9.37+/-6.07 mg/min (P<0.001). By analysing the excretion of proteins with different charge and weight (albumin, transferrin, IgG, IgG4 and beta2-microglobulin) it became apparent that the increase of proteinuria was the result of a change in size selectivity rather than a change in glomerular charge selectivity or tubular protein reabsorption. Glomerular filtration rate rose from 83+/-34 ml to 95+/-43 ml/min (P<0.001) after 5 h, whereas effective renal plasma flow and endogenous creatinine clearance remained unchanged. As a result filtration fraction was increased, compatible with an increased glomerular pressure, which probably contributes to the size selectivity changes. Since corticosteroids affect both the renin-angiotensin system and renal prostaglandins, we have evaluated the effects of prednisolone on proteinuria after pretreatment with 3 months of the angiotensin-converting enzyme inhibitor lisinopril or after 2 weeks of the prostaglandin synthesis inhibitor indomethacin. Neither drug had any effect on prednisolone-induced increases of proteinuria. CONCLUSIONS: Prednisolone increases proteinuria by changing the size selective barrier of the glomerular capillary. Neither the renin-angiotensin axis nor prostaglandins seem to be involved in these effects of prednisolone on proteinuria. (+info)Altered gene expression and functions of mitochondria in human nephrotic syndrome. (6/1128)
The molecular basis of glomerular permselectivity remains largely unknown. The congenital nephrotic syndrome of the Finnish type (CNF) characterized by massive proteinuria already present but without extrarenal symptoms is a unique human disease model of pure proteinuria. In search of genes and pathophysiologic mechanisms associated with proteinuria, we used differential display-PCR to identify differences in gene expression between glomeruli from CNF and control kidneys. A distinctly underexpressed PCR product of the CNF kidneys showed over 98% identity with a mitochondrially encoded cytochrome c oxidase (COX I). Using a full-length COX I cDNA probe, we verified down-regulation of COX I mRNA to 1/4 of normal kidney values on Northern blots. In addition, transcripts of other mitochondrially encoded respiratory chain complexes showed a similar down-regulation whereas the respective nuclearly encoded complexes were expressed at comparable levels. Additional studies using histochemical, immunohistochemical, in situ hybridization, RT-PCR, and biochemical and electron microscopic methods all showed a mitochondrial involvement in the diseased kidneys but not in extrarenal blood vessels. As a secondary sign of mitochondrial dysfunction, excess lipid peroxidation products were found in glomerular structures in CNF samples. Our data suggest that mitochondrial dysfunction occurs in the kidneys of patients with CNF, with subsequent lipid peroxidation at the glomerular basement membrane. Our additional studies have revealed similar down-regulation of mitochondrial functions in experimental models of proteinuria. Thus, mitochondrial dysfunction may be a crucial pathophysiologic factor in this symptom. (+info)Th1 and Th2 cytokine mRNA profiles in childhood nephrotic syndrome: evidence for increased IL-13 mRNA expression in relapse. (7/1128)
Idiopathic nephrotic syndrome of childhood is thought to be associated with T lymphocyte dysfunction often triggered by viral infections, with the production of circulating factor(s) resulting in proteinuria. In view of the conflicting evidence of T cell activation and Th1 or Th2 pattern of cytokine synthesis in this disease, this study examined the mRNA expression of interleukin-2 (IL-2), interferon-gamma, IL-4, and IL-13 from CD4+ and CD8+ T cells in steroid-responsive nephrotic patients in relapse and remission. Fifty-five children with steroid-responsive nephrotic syndrome were included in this study, together with 34 normal controls and 24 patient controls with viral infections. RNA was isolated from purified CD4+ or CD8+ cells from peripheral blood and subjected to reverse transcription-PCR. Cytokine mRNA expression was measured semiquantitatively, and a cytokine index was derived from densitometric readings, with cyclophilin as the housekeeping gene. Both cross-sectional and paired data showed an increased CD4+ and CD8+ IL-13 mRNA expression in patients with nephrotic relapse as compared to remission, normal, and patient controls (P < 0.008). This was also associated with increased cytoplasmic IL-13 expression in phorbol myristate acetate/ionomycin-activated CD3+ cells (6.66+/-3.39%) from patients with nephrotic relapse compared to remission (2.59+/-1.35%) (P < 0.0001). However, there was no significant difference in CD4+ or CD8+ IL-2, interferon-gamma and IL-4 mRNA expression. IL-13 is an important T cell cytokine with anti-inflammatory and immunomodulatory functions on B cells and monocytes. It is conceivable that IL-13 may act on monocytes to produce vascular permeability factor(s) involved in the pathogenesis of proteinuria in patients with relapse nephrotic syndrome. (+info)Possible induction of renal dysfunction in patients with lecithin:cholesterol acyltransferase deficiency by oxidized phosphatidylcholine in glomeruli. (8/1128)
To clarify the causes of renal dysfunction in familial lecithin:cholesterol acyltransferase (LCAT) deficiency, kidney samples from 4 patients with LCAT deficiency (3 homozygotes and 1 heterozygote) were examined immunohistochemically. All of the patients exhibited corneal opacities, anemia, renal dysfunction, deficiencies in plasma high density lipoprotein and LCAT activity and mass, and an increase in the ratio of plasma unesterified cholesterol to esterified cholesterol. Renal lesions began with the deposition of lipidlike structures in the glomerular basement membrane, and these structures accumulated in the mesangium and capillary subendothelium. By electron microscopy, 2 types of distinctive structure were found in glomerular lesions: vacuole structures and cross-striated, membranelike structures. The plasma oxidized phosphatidylcholine (oxPC) -modified low density lipoprotein (LDL) levels in LCAT-deficient subjects were significantly (P<0.01) higher than those in controls (1.30+/-0.82 versus 0.42+/-0.32 ng/5 microg LDL, respectively), and a significant (P<0.01) difference was observed even after adjustment for confounding factors by an analysis of covariance. The patient with the highest plasma oxPC-modified LDL had the most membranelike structures in the glomeruli and showed the greatest renal deterioration from a young age. In glomerular lesions, although there was an abundance of apoB and apoE, oil red O-positive lipids, macrophages, apoA1, and malondialdehyde were scarce. OxPC was found extracellularly in glomerular lesions, and although its distribution differed from that of apolipoproteins, it was quite similar to that of phospholipids. In conclusion, these results indicate that oxPC in plasma and glomeruli is distinctive for patients with LCAT deficiency. Therefore, oxPC may be a factor in the deterioration of kidneys in patients with familial LCAT deficiency. (+info)Nephrotic syndrome is a group of symptoms that indicate kidney damage, specifically damage to the glomeruli—the tiny blood vessel clusters in the kidneys that filter waste and excess fluids from the blood. The main features of nephrotic syndrome are:
1. Proteinuria (excess protein in urine): Large amounts of a protein called albumin leak into the urine due to damaged glomeruli, which can't properly filter proteins. This leads to low levels of albumin in the blood, causing fluid buildup and swelling.
2. Hypoalbuminemia (low blood albumin levels): As albumin leaks into the urine, the concentration of albumin in the blood decreases, leading to hypoalbuminemia. This can cause edema (swelling), particularly in the legs, ankles, and feet.
3. Edema (fluid retention and swelling): With low levels of albumin in the blood, fluids move into the surrounding tissues, causing swelling or puffiness. The swelling is most noticeable around the eyes, face, hands, feet, and abdomen.
4. Hyperlipidemia (high lipid/cholesterol levels): The kidneys play a role in regulating lipid metabolism. Damage to the glomeruli can lead to increased lipid production and high cholesterol levels in the blood.
Nephrotic syndrome can result from various underlying kidney diseases, such as minimal change disease, membranous nephropathy, or focal segmental glomerulosclerosis. Treatment depends on the underlying cause and may include medications to control inflammation, manage high blood pressure, and reduce proteinuria. In some cases, dietary modifications and lifestyle changes are also recommended.
Lipoid nephrosis is a historical term for a kidney disorder now more commonly referred to as minimal change disease (MCD). It is a type of glomerulonephritis which is characterized by the loss of proteins in the urine (proteinuria) due to damage to the glomeruli, the tiny filtering units within the kidneys.
The term "lipoid" refers to the presence of lipids or fats in the glomeruli, which can be observed under a microscope. However, it's worth noting that not all cases of MCD involve lipid accumulation in the glomeruli.
MCD is typically idiopathic, meaning its cause is unknown, but it can also occur as a secondary condition related to other medical disorders such as allergies, infections, or medications. It primarily affects children, but can also occur in adults. Treatment usually involves corticosteroids and other immunosuppressive therapies to control proteinuria and prevent kidney damage.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Membranous glomerulonephritis (MGN) is a kidney disorder that leads to the inflammation and damage of the glomeruli, which are the tiny blood vessels in the kidneys responsible for filtering waste and excess fluids from the blood. In MGN, the membrane that surrounds the glomerular capillaries becomes thickened and damaged due to the deposit of immune complexes, primarily composed of antibodies and antigens.
The onset of membranous glomerulonephritis can be either primary (idiopathic) or secondary to various underlying conditions such as autoimmune diseases (like systemic lupus erythematosus), infections (hepatitis B or C, syphilis, endocarditis), medications, or malignancies.
The symptoms of membranous glomerulonephritis may include:
1. Proteinuria - the presence of excess protein, specifically albumin, in the urine. This can lead to nephrotic syndrome, characterized by heavy protein loss in urine, edema (swelling), hypoalbuminemia (low blood albumin levels), and hyperlipidemia (high blood lipid levels).
2. Hematuria - the presence of red blood cells in the urine, which can be visible or microscopic.
3. Hypertension - high blood pressure.
4. Edema - swelling in various body parts due to fluid retention.
5. Nephrotic range proteinuria (protein loss greater than 3.5 grams per day) and/or nephritic syndrome (a combination of hematuria, proteinuria, hypertension, and kidney dysfunction) can be observed in some cases.
The diagnosis of membranous glomerulonephritis typically involves a thorough medical history, physical examination, urinalysis, blood tests, and imaging studies. A definitive diagnosis often requires a kidney biopsy to assess the glomerular structure and the nature of the immune complex deposits. Treatment depends on the underlying cause and severity of the disease and may include corticosteroids, immunosuppressants, blood pressure management, and supportive care for symptoms like edema and proteinuria.
Focal segmental glomerulosclerosis (FSGS) is a pattern of kidney injury that involves scarring or sclerosis in some (segmental) areas of some (focal) glomeruli. Glomeruli are the tiny blood vessel clusters within the kidneys that filter waste and excess fluids from the blood.
In FSGS, the scarring occurs due to damage to the glomerular basement membrane, which can be caused by various factors such as genetic mutations, viral infections, or immune system disorders. The damage leads to the accumulation of extracellular matrix proteins and the formation of scar tissue, impairing the kidney's ability to filter blood effectively.
FSGS is characterized by proteinuria (protein in the urine), hematuria (blood in the urine), hypertension (high blood pressure), and declining kidney function, which can lead to end-stage renal disease if left untreated. The focal and segmental nature of the scarring means that not all glomeruli are affected, and only some areas of each affected glomerulus are damaged, making FSGS a highly variable condition with different clinical presentations and outcomes.
Proteinuria is a medical term that refers to the presence of excess proteins, particularly albumin, in the urine. Under normal circumstances, only small amounts of proteins should be found in the urine because the majority of proteins are too large to pass through the glomeruli, which are the filtering units of the kidneys.
However, when the glomeruli become damaged or diseased, they may allow larger molecules such as proteins to leak into the urine. Persistent proteinuria is often a sign of kidney disease and can indicate damage to the glomeruli. It is usually detected through a routine urinalysis and may be confirmed with further testing.
The severity of proteinuria can vary, and it can be a symptom of various underlying conditions such as diabetes, hypertension, glomerulonephritis, and other kidney diseases. Treatment for proteinuria depends on the underlying cause and may include medications to control blood pressure, manage diabetes, or reduce protein loss in the urine.
Puromycin aminonucleoside is not a medical condition, but rather a laboratory reagent used in research. It is a synthetic antibiotic and analogue of the amino acid tyrosine, which specifically inhibits protein synthesis in eukaryotic cells by interacting with the peptidyl transferase center of the 60S ribosomal subunit. This compound has been widely used as a tool to study various cellular processes, including programmed cell death (apoptosis), autophagy, and lysosome biogenesis. Prolonged exposure to puromycin aminonucleoside can induce cytopathic effects, such as vacuolization and detachment of cells, which are often used as markers for its effectiveness in inhibiting protein synthesis.
A kidney glomerulus is a functional unit in the nephron of the kidney. It is a tuft of capillaries enclosed within a structure called Bowman's capsule, which filters waste and excess fluids from the blood. The glomerulus receives blood from an afferent arteriole and drains into an efferent arteriole.
The process of filtration in the glomerulus is called ultrafiltration, where the pressure within the glomerular capillaries drives plasma fluid and small molecules (such as ions, glucose, amino acids, and waste products) through the filtration membrane into the Bowman's space. Larger molecules, like proteins and blood cells, are retained in the blood due to their larger size. The filtrate then continues down the nephron for further processing, eventually forming urine.
Prednisolone is a synthetic glucocorticoid drug, which is a class of steroid hormones. It is commonly used in the treatment of various inflammatory and autoimmune conditions due to its potent anti-inflammatory and immunosuppressive effects. Prednisolone works by binding to specific receptors in cells, leading to changes in gene expression that reduce the production of substances involved in inflammation, such as cytokines and prostaglandins.
Prednisolone is available in various forms, including tablets, syrups, and injectable solutions. It can be used to treat a wide range of medical conditions, including asthma, rheumatoid arthritis, inflammatory bowel disease, allergies, skin conditions, and certain types of cancer.
Like other steroid medications, prednisolone can have significant side effects if used in high doses or for long periods of time. These may include weight gain, mood changes, increased risk of infections, osteoporosis, diabetes, and adrenal suppression. As a result, the use of prednisolone should be closely monitored by a healthcare professional to ensure that its benefits outweigh its risks.
Podocytes are specialized cells that make up the visceral epithelial layer of the glomerular basement membrane in the kidney. They have long, interdigitating foot processes that wrap around the capillaries of the glomerulus and play a crucial role in maintaining the filtration barrier of the kidney. The slit diaphragms between the foot processes allow for the passage of small molecules while retaining larger proteins in the bloodstream. Podocytes also contribute to the maintenance and regulation of the glomerular filtration rate, making them essential for normal renal function. Damage or loss of podocytes can lead to proteinuria and kidney disease.
Glomerulonephritis is a medical condition that involves inflammation of the glomeruli, which are the tiny blood vessel clusters in the kidneys that filter waste and excess fluids from the blood. This inflammation can impair the kidney's ability to filter blood properly, leading to symptoms such as proteinuria (protein in the urine), hematuria (blood in the urine), edema (swelling), hypertension (high blood pressure), and eventually kidney failure.
Glomerulonephritis can be acute or chronic, and it may occur as a primary kidney disease or secondary to other medical conditions such as infections, autoimmune disorders, or vasculitis. The diagnosis of glomerulonephritis typically involves a combination of medical history, physical examination, urinalysis, blood tests, and imaging studies, with confirmation often requiring a kidney biopsy. Treatment depends on the underlying cause and severity of the disease but may include medications to suppress inflammation, control blood pressure, and manage symptoms.
Steroids, also known as corticosteroids, are a type of hormone that the adrenal gland produces in your body. They have many functions, such as controlling the balance of salt and water in your body and helping to reduce inflammation. Steroids can also be synthetically produced and used as medications to treat a variety of conditions, including allergies, asthma, skin conditions, and autoimmune disorders.
Steroid medications are available in various forms, such as oral pills, injections, creams, and inhalers. They work by mimicking the effects of natural hormones produced by your body, reducing inflammation and suppressing the immune system's response to prevent or reduce symptoms. However, long-term use of steroids can have significant side effects, including weight gain, high blood pressure, osteoporosis, and increased risk of infections.
It is important to note that anabolic steroids are a different class of drugs that are sometimes abused for their muscle-building properties. These steroids are synthetic versions of the male hormone testosterone and can have serious health consequences when taken in large doses or without medical supervision.
Membranoproliferative Glomerulonephritis (MPGN) is a type of glomerulonephritis, which is a group of kidney disorders characterized by inflammation and damage to the glomeruli, the tiny blood vessels in the kidneys responsible for filtering waste and excess fluids from the blood.
MPGN is specifically characterized by thickening of the glomerular basement membrane and proliferation (increased number) of cells in the mesangium, a region within the glomerulus. This condition can be primary or secondary to other diseases such as infections, autoimmune disorders, or monoclonal gammopathies.
MPGN is typically classified into three types based on the pattern of injury seen on electron microscopy: Type I, Type II (Dense Deposit Disease), and Type III. Each type has distinct clinical features, laboratory findings, and treatment approaches. Symptoms of MPGN may include hematuria (blood in urine), proteinuria (protein in urine), hypertension (high blood pressure), edema (swelling), and eventually progress to chronic kidney disease or end-stage renal disease if left untreated.
Nephrosis is an older term that was used to describe a group of kidney diseases, primarily characterized by the damage and loss of function in the glomeruli - the tiny filtering units within the kidneys. This results in the leakage of large amounts of protein (primarily albumin) into the urine, a condition known as proteinuria.
The term "nephrosis" was often used interchangeably with "minimal change nephropathy," which is a specific type of kidney disorder that demonstrates little to no changes in the glomeruli under a microscope, despite significant protein leakage. However, current medical terminology and classifications prefer the use of more precise terms to describe various kidney diseases, such as minimal change disease, focal segmental glomerulosclerosis, or membranous nephropathy, among others.
It is important to consult with a healthcare professional or refer to updated medical resources for accurate and current information regarding kidney diseases and their specific diagnoses.
A kidney, in medical terms, is one of two bean-shaped organs located in the lower back region of the body. They are essential for maintaining homeostasis within the body by performing several crucial functions such as:
1. Regulation of water and electrolyte balance: Kidneys help regulate the amount of water and various electrolytes like sodium, potassium, and calcium in the bloodstream to maintain a stable internal environment.
2. Excretion of waste products: They filter waste products from the blood, including urea (a byproduct of protein metabolism), creatinine (a breakdown product of muscle tissue), and other harmful substances that result from normal cellular functions or external sources like medications and toxins.
3. Endocrine function: Kidneys produce several hormones with important roles in the body, such as erythropoietin (stimulates red blood cell production), renin (regulates blood pressure), and calcitriol (activated form of vitamin D that helps regulate calcium homeostasis).
4. pH balance regulation: Kidneys maintain the proper acid-base balance in the body by excreting either hydrogen ions or bicarbonate ions, depending on whether the blood is too acidic or too alkaline.
5. Blood pressure control: The kidneys play a significant role in regulating blood pressure through the renin-angiotensin-aldosterone system (RAAS), which constricts blood vessels and promotes sodium and water retention to increase blood volume and, consequently, blood pressure.
Anatomically, each kidney is approximately 10-12 cm long, 5-7 cm wide, and 3 cm thick, with a weight of about 120-170 grams. They are surrounded by a protective layer of fat and connected to the urinary system through the renal pelvis, ureters, bladder, and urethra.
Immunosuppressive agents are medications that decrease the activity of the immune system. They are often used to prevent the rejection of transplanted organs and to treat autoimmune diseases, where the immune system mistakenly attacks the body's own tissues. These drugs work by interfering with the immune system's normal responses, which helps to reduce inflammation and damage to tissues. However, because they suppress the immune system, people who take immunosuppressive agents are at increased risk for infections and other complications. Examples of immunosuppressive agents include corticosteroids, azathioprine, cyclophosphamide, mycophenolate mofetil, tacrolimus, and sirolimus.
Edema is the medical term for swelling caused by excess fluid accumulation in the body tissues. It can affect any part of the body, but it's most commonly noticed in the hands, feet, ankles, and legs. Edema can be a symptom of various underlying medical conditions, such as heart failure, kidney disease, liver disease, or venous insufficiency.
The swelling occurs when the capillaries leak fluid into the surrounding tissues, causing them to become swollen and puffy. The excess fluid can also collect in the cavities of the body, leading to conditions such as pleural effusion (fluid around the lungs) or ascites (fluid in the abdominal cavity).
The severity of edema can vary from mild to severe, and it may be accompanied by other symptoms such as skin discoloration, stiffness, and pain. Treatment for edema depends on the underlying cause and may include medications, lifestyle changes, or medical procedures.
A biopsy is a medical procedure in which a small sample of tissue is taken from the body to be examined under a microscope for the presence of disease. This can help doctors diagnose and monitor various medical conditions, such as cancer, infections, or autoimmune disorders. The type of biopsy performed will depend on the location and nature of the suspected condition. Some common types of biopsies include:
1. Incisional biopsy: In this procedure, a surgeon removes a piece of tissue from an abnormal area using a scalpel or other surgical instrument. This type of biopsy is often used when the lesion is too large to be removed entirely during the initial biopsy.
2. Excisional biopsy: An excisional biopsy involves removing the entire abnormal area, along with a margin of healthy tissue surrounding it. This technique is typically employed for smaller lesions or when cancer is suspected.
3. Needle biopsy: A needle biopsy uses a thin, hollow needle to extract cells or fluid from the body. There are two main types of needle biopsies: fine-needle aspiration (FNA) and core needle biopsy. FNA extracts loose cells, while a core needle biopsy removes a small piece of tissue.
4. Punch biopsy: In a punch biopsy, a round, sharp tool is used to remove a small cylindrical sample of skin tissue. This type of biopsy is often used for evaluating rashes or other skin abnormalities.
5. Shave biopsy: During a shave biopsy, a thin slice of tissue is removed from the surface of the skin using a sharp razor-like instrument. This technique is typically used for superficial lesions or growths on the skin.
After the biopsy sample has been collected, it is sent to a laboratory where a pathologist will examine the tissue under a microscope and provide a diagnosis based on their findings. The results of the biopsy can help guide further treatment decisions and determine the best course of action for managing the patient's condition.
Down syndrome is a genetic disorder caused by the presence of all or part of a third copy of chromosome 21. It is characterized by intellectual and developmental disabilities, distinctive facial features, and sometimes physical growth delays and health problems. The condition affects approximately one in every 700 babies born in the United States.
Individuals with Down syndrome have varying degrees of cognitive impairment, ranging from mild to moderate or severe. They may also have delayed development, including late walking and talking, and may require additional support and education services throughout their lives.
People with Down syndrome are at increased risk for certain health conditions, such as congenital heart defects, respiratory infections, hearing loss, vision problems, gastrointestinal issues, and thyroid disorders. However, many individuals with Down syndrome live healthy and fulfilling lives with appropriate medical care and support.
The condition is named after John Langdon Down, an English physician who first described the syndrome in 1866.
Cyclosporine is a medication that belongs to a class of drugs called immunosuppressants. It is primarily used to prevent the rejection of transplanted organs, such as kidneys, livers, and hearts. Cyclosporine works by suppressing the activity of the immune system, which helps to reduce the risk of the body attacking the transplanted organ.
In addition to its use in organ transplantation, cyclosporine may also be used to treat certain autoimmune diseases, such as rheumatoid arthritis and psoriasis. It does this by suppressing the overactive immune response that contributes to these conditions.
Cyclosporine is available in capsule, oral solution, and injectable forms. Common side effects of the medication include kidney problems, high blood pressure, tremors, headache, and nausea. Long-term use of cyclosporine can also increase the risk of certain types of cancer and infections.
It is important to note that cyclosporine should only be used under the close supervision of a healthcare provider, as it requires regular monitoring of blood levels and kidney function.
Metabolic syndrome, also known as Syndrome X, is a cluster of conditions that increase the risk of heart disease, stroke, and diabetes. It is not a single disease but a group of risk factors that often co-occur. According to the American Heart Association and the National Heart, Lung, and Blood Institute, a person has metabolic syndrome if they have any three of the following five conditions:
1. Abdominal obesity (waist circumference of 40 inches or more in men, and 35 inches or more in women)
2. Triglyceride level of 150 milligrams per deciliter of blood (mg/dL) or greater
3. HDL cholesterol level of less than 40 mg/dL in men or less than 50 mg/dL in women
4. Systolic blood pressure of 130 millimeters of mercury (mmHg) or greater, or diastolic blood pressure of 85 mmHg or greater
5. Fasting glucose level of 100 mg/dL or greater
Metabolic syndrome is thought to be caused by a combination of genetic and lifestyle factors, such as physical inactivity and a diet high in refined carbohydrates and unhealthy fats. Treatment typically involves making lifestyle changes, such as eating a healthy diet, getting regular exercise, and losing weight if necessary. In some cases, medication may also be needed to manage individual components of the syndrome, such as high blood pressure or high cholesterol.
Amyloidosis is a medical condition characterized by the abnormal accumulation of insoluble proteins called amyloid in various tissues and organs throughout the body. These misfolded protein deposits can disrupt the normal function of affected organs, leading to a range of symptoms depending on the location and extent of the amyloid deposition.
There are different types of amyloidosis, classified based on the specific proteins involved:
1. Primary (AL) Amyloidosis: This is the most common form, accounting for around 80% of cases. It results from the overproduction and misfolding of immunoglobulin light chains, typically by clonal plasma cells in the bone marrow. The amyloid deposits can affect various organs, including the heart, kidneys, liver, and nervous system.
2. Secondary (AA) Amyloidosis: This form is associated with chronic inflammatory diseases, such as rheumatoid arthritis, tuberculosis, or familial Mediterranean fever. The amyloid fibrils are composed of serum amyloid A protein (SAA), an acute-phase reactant produced during the inflammatory response. The kidneys are commonly affected in this type of amyloidosis.
3. Hereditary or Familial Amyloidosis: These forms are caused by genetic mutations that result in the production of abnormal proteins prone to misfolding and amyloid formation. Examples include transthyretin (TTR) amyloidosis, fibrinogen amyloidosis, and apolipoprotein AI amyloidosis. These forms can affect various organs, including the heart, nerves, and kidneys.
4. Dialysis-Related Amyloidosis: This form is seen in patients undergoing long-term dialysis for chronic kidney disease. The amyloid fibrils are composed of beta-2 microglobulin, a protein that accumulates due to impaired clearance during dialysis. The joints and bones are commonly affected in this type of amyloidosis.
The diagnosis of amyloidosis typically involves a combination of clinical evaluation, imaging studies, and tissue biopsy with the demonstration of amyloid deposition using special stains (e.g., Congo red). Treatment depends on the specific type and extent of organ involvement and may include supportive care, medications to target the underlying cause (e.g., chemotherapy, immunomodulatory agents), and organ transplantation in some cases.
Drug resistance, also known as antimicrobial resistance, is the ability of a microorganism (such as bacteria, viruses, fungi, or parasites) to withstand the effects of a drug that was originally designed to inhibit or kill it. This occurs when the microorganism undergoes genetic changes that allow it to survive in the presence of the drug. As a result, the drug becomes less effective or even completely ineffective at treating infections caused by these resistant organisms.
Drug resistance can develop through various mechanisms, including mutations in the genes responsible for producing the target protein of the drug, alteration of the drug's target site, modification or destruction of the drug by enzymes produced by the microorganism, and active efflux of the drug from the cell.
The emergence and spread of drug-resistant microorganisms pose significant challenges in medical treatment, as they can lead to increased morbidity, mortality, and healthcare costs. The overuse and misuse of antimicrobial agents, as well as poor infection control practices, contribute to the development and dissemination of drug-resistant strains. To address this issue, it is crucial to promote prudent use of antimicrobials, enhance surveillance and monitoring of resistance patterns, invest in research and development of new antimicrobial agents, and strengthen infection prevention and control measures.
Recurrence, in a medical context, refers to the return of symptoms or signs of a disease after a period of improvement or remission. It indicates that the condition has not been fully eradicated and may require further treatment. Recurrence is often used to describe situations where a disease such as cancer comes back after initial treatment, but it can also apply to other medical conditions. The likelihood of recurrence varies depending on the type of disease and individual patient factors.
The adrenal cortex hormones are a group of steroid hormones produced and released by the outer portion (cortex) of the adrenal glands, which are located on top of each kidney. These hormones play crucial roles in regulating various physiological processes, including:
1. Glucose metabolism: Cortisol helps control blood sugar levels by increasing glucose production in the liver and reducing its uptake in peripheral tissues.
2. Protein and fat metabolism: Cortisol promotes protein breakdown and fatty acid mobilization, providing essential building blocks for energy production during stressful situations.
3. Immune response regulation: Cortisol suppresses immune function to prevent overactivation and potential damage to the body during stress.
4. Cardiovascular function: Aldosterone regulates electrolyte balance and blood pressure by promoting sodium reabsorption and potassium excretion in the kidneys.
5. Sex hormone production: The adrenal cortex produces small amounts of sex hormones, such as androgens and estrogens, which contribute to sexual development and function.
6. Growth and development: Cortisol plays a role in normal growth and development by influencing the activity of growth-promoting hormones like insulin-like growth factor 1 (IGF-1).
The main adrenal cortex hormones include:
1. Glucocorticoids: Cortisol is the primary glucocorticoid, responsible for regulating metabolism and stress response.
2. Mineralocorticoids: Aldosterone is the primary mineralocorticoid, involved in electrolyte balance and blood pressure regulation.
3. Androgens: Dehydroepiandrosterone (DHEA) and its sulfate derivative (DHEAS) are the most abundant adrenal androgens, contributing to sexual development and function.
4. Estrogens: Small amounts of estrogens are produced by the adrenal cortex, mainly in women.
Disorders related to impaired adrenal cortex hormone production or regulation can lead to various clinical manifestations, such as Addison's disease (adrenal insufficiency), Cushing's syndrome (hypercortisolism), and congenital adrenal hyperplasia (CAH).
Serum albumin is the most abundant protein in human blood plasma, synthesized by the liver. It plays a crucial role in maintaining the oncotic pressure or colloid osmotic pressure of blood, which helps to regulate the fluid balance between the intravascular and extravascular spaces.
Serum albumin has a molecular weight of around 66 kDa and is composed of a single polypeptide chain. It contains several binding sites for various endogenous and exogenous substances, such as bilirubin, fatty acids, hormones, and drugs, facilitating their transport throughout the body. Additionally, albumin possesses antioxidant properties, protecting against oxidative damage.
Albumin levels in the blood are often used as a clinical indicator of liver function, nutritional status, and overall health. Low serum albumin levels may suggest liver disease, malnutrition, inflammation, or kidney dysfunction.
Glucocorticoids are a class of steroid hormones that are naturally produced in the adrenal gland, or can be synthetically manufactured. They play an essential role in the metabolism of carbohydrates, proteins, and fats, and have significant anti-inflammatory effects. Glucocorticoids suppress immune responses and inflammation by inhibiting the release of inflammatory mediators from various cells, such as mast cells, eosinophils, and lymphocytes. They are frequently used in medical treatment for a wide range of conditions, including allergies, asthma, rheumatoid arthritis, dermatological disorders, and certain cancers. Prolonged use or high doses of glucocorticoids can lead to several side effects, such as weight gain, mood changes, osteoporosis, and increased susceptibility to infections.
Prednisone is a synthetic glucocorticoid, which is a type of corticosteroid hormone. It is primarily used to reduce inflammation in various conditions such as asthma, allergies, arthritis, and autoimmune disorders. Prednisone works by mimicking the effects of natural hormones produced by the adrenal glands, suppressing the immune system's response and reducing the release of substances that cause inflammation.
It is available in oral tablet form and is typically prescribed to be taken at specific times during the day, depending on the condition being treated. Common side effects of prednisone include increased appetite, weight gain, mood changes, insomnia, and easy bruising. Long-term use or high doses can lead to more serious side effects such as osteoporosis, diabetes, cataracts, and increased susceptibility to infections.
Healthcare providers closely monitor patients taking prednisone for extended periods to minimize the risk of adverse effects. It is essential to follow the prescribed dosage regimen and not discontinue the medication abruptly without medical supervision, as this can lead to withdrawal symptoms or a rebound of the underlying condition.
Spontaneous remission in a medical context refers to the disappearance or significant improvement of symptoms of a disease or condition without any specific treatment being administered. In other words, it's a situation where the disease resolves on its own, without any apparent cause. While spontaneous remission can occur in various conditions, it is relatively rare and not well understood. It's important to note that just because a remission occurs without treatment doesn't mean that medical care should be avoided, as many conditions can worsen or lead to complications if left untreated.
Remission induction is a treatment approach in medicine, particularly in the field of oncology and hematology. It refers to the initial phase of therapy aimed at reducing or eliminating the signs and symptoms of active disease, such as cancer or autoimmune disorders. The primary goal of remission induction is to achieve a complete response (disappearance of all detectable signs of the disease) or a partial response (a decrease in the measurable extent of the disease). This phase of treatment is often intensive and may involve the use of multiple drugs or therapies, including chemotherapy, immunotherapy, or targeted therapy. After remission induction, patients may receive additional treatments to maintain the remission and prevent relapse, known as consolidation or maintenance therapy.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Paraneoplastic syndromes refer to a group of rare disorders that are caused by an abnormal immune system response to a cancerous (malignant) tumor. These syndromes are characterized by symptoms or signs that do not result directly from the growth of the tumor itself, but rather from substances produced by the tumor or the body's immune system in response to the tumor.
Paraneoplastic syndromes can affect various organs and systems in the body, including the nervous system, endocrine system, skin, and joints. Examples of paraneoplastic syndromes include Lambert-Eaton myasthenic syndrome (LEMS), which affects nerve function and causes muscle weakness; cerebellar degeneration, which can cause difficulty with coordination and balance; and dermatomyositis, which is an inflammatory condition that affects the skin and muscles.
Paraneoplastic syndromes can occur in association with a variety of different types of cancer, including lung cancer, breast cancer, ovarian cancer, and lymphoma. Treatment typically involves addressing the underlying cancer, as well as managing the symptoms of the paraneoplastic syndrome.
Kidney disease, also known as nephropathy or renal disease, refers to any functional or structural damage to the kidneys that impairs their ability to filter blood, regulate electrolytes, produce hormones, and maintain fluid balance. This damage can result from a wide range of causes, including diabetes, hypertension, glomerulonephritis, polycystic kidney disease, lupus, infections, drugs, toxins, and congenital or inherited disorders.
Depending on the severity and progression of the kidney damage, kidney diseases can be classified into two main categories: acute kidney injury (AKI) and chronic kidney disease (CKD). AKI is a sudden and often reversible loss of kidney function that occurs over hours to days, while CKD is a progressive and irreversible decline in kidney function that develops over months or years.
Symptoms of kidney diseases may include edema, proteinuria, hematuria, hypertension, electrolyte imbalances, metabolic acidosis, anemia, and decreased urine output. Treatment options depend on the underlying cause and severity of the disease and may include medications, dietary modifications, dialysis, or kidney transplantation.
Sjögren's syndrome is a chronic autoimmune disorder in which the body's immune system mistakenly attacks its own moisture-producing glands, particularly the tear and salivary glands. This can lead to symptoms such as dry eyes, dry mouth, and dryness in other areas of the body. In some cases, it may also affect other organs, leading to a variety of complications.
There are two types of Sjögren's syndrome: primary and secondary. Primary Sjögren's syndrome occurs when the condition develops on its own, while secondary Sjögren's syndrome occurs when it develops in conjunction with another autoimmune disease, such as rheumatoid arthritis or lupus.
The exact cause of Sjögren's syndrome is not fully understood, but it is believed to involve a combination of genetic and environmental factors. Treatment typically focuses on relieving symptoms and may include artificial tears, saliva substitutes, medications to stimulate saliva production, and immunosuppressive drugs in more severe cases.
Pulse therapy, in the context of drug treatment, refers to a therapeutic regimen where a medication is administered in large doses for a short period of time, followed by a break or "drug-free" interval before the next dose. This cycle is then repeated at regular intervals. The goal of pulse therapy is to achieve high concentrations of the drug in the body to maximize its therapeutic effect while minimizing overall exposure and potential side effects.
This approach is often used for drugs that have a long half-life or slow clearance, as it allows for periodic "washing out" of the drug from the body. Pulse therapy can also help reduce the risk of developing drug resistance in certain conditions like rheumatoid arthritis and tuberculosis. Common examples include pulse methotrexate for rheumatoid arthritis and intermittent preventive treatment with anti-malarial drugs.
It is important to note that the use of pulse therapy should be based on a thorough understanding of the drug's pharmacokinetics, therapeutic index, and potential adverse effects. Close monitoring of patients undergoing pulse therapy is essential to ensure safety and efficacy.
'Abnormalities, Multiple' is a broad term that refers to the presence of two or more structural or functional anomalies in an individual. These abnormalities can be present at birth (congenital) or can develop later in life (acquired). They can affect various organs and systems of the body and can vary greatly in severity and impact on a person's health and well-being.
Multiple abnormalities can occur due to genetic factors, environmental influences, or a combination of both. Chromosomal abnormalities, gene mutations, exposure to teratogens (substances that cause birth defects), and maternal infections during pregnancy are some of the common causes of multiple congenital abnormalities.
Examples of multiple congenital abnormalities include Down syndrome, Turner syndrome, and VATER/VACTERL association. Acquired multiple abnormalities can result from conditions such as trauma, infection, degenerative diseases, or cancer.
The medical evaluation and management of individuals with multiple abnormalities depend on the specific abnormalities present and their impact on the individual's health and functioning. A multidisciplinary team of healthcare professionals is often involved in the care of these individuals to address their complex needs.
Chlorambucil is a medication that belongs to a class of drugs called alkylating agents. It is an antineoplastic drug, which means it is used to treat cancer. Chlorambucil works by interfering with the DNA in cells, which prevents them from dividing and growing. This makes it useful for treating certain types of cancer, such as chronic lymphocytic leukemia (CLL) and Hodgkin's lymphoma.
Chlorambucil is available in tablet form and is typically taken once a day. It is important to take chlorambucil exactly as directed by your healthcare provider, as the dosage and schedule will depend on your individual medical condition and response to treatment.
Like all medications, chlorambucil can cause side effects. Common side effects of chlorambucil include nausea, vomiting, diarrhea, and loss of appetite. It can also cause more serious side effects, such as a decrease in the number of white blood cells (which can increase the risk of infection), anemia (low red blood cell count), and thrombocytopenia (low platelet count). Chlorambucil may also increase the risk of certain types of cancer, such as acute myeloid leukemia (AML) and solid tumors.
It is important to discuss the potential risks and benefits of chlorambucil with your healthcare provider before starting treatment. They can help you understand the potential side effects and how to manage them, as well as any other precautions you should take while taking this medication.
Membrane proteins are a type of protein that are embedded in the lipid bilayer of biological membranes, such as the plasma membrane of cells or the inner membrane of mitochondria. These proteins play crucial roles in various cellular processes, including:
1. Cell-cell recognition and signaling
2. Transport of molecules across the membrane (selective permeability)
3. Enzymatic reactions at the membrane surface
4. Energy transduction and conversion
5. Mechanosensation and signal transduction
Membrane proteins can be classified into two main categories: integral membrane proteins, which are permanently associated with the lipid bilayer, and peripheral membrane proteins, which are temporarily or loosely attached to the membrane surface. Integral membrane proteins can further be divided into three subcategories based on their topology:
1. Transmembrane proteins, which span the entire width of the lipid bilayer with one or more alpha-helices or beta-barrels.
2. Lipid-anchored proteins, which are covalently attached to lipids in the membrane via a glycosylphosphatidylinositol (GPI) anchor or other lipid modifications.
3. Monotopic proteins, which are partially embedded in the membrane and have one or more domains exposed to either side of the bilayer.
Membrane proteins are essential for maintaining cellular homeostasis and are targets for various therapeutic interventions, including drug development and gene therapy. However, their structural complexity and hydrophobicity make them challenging to study using traditional biochemical methods, requiring specialized techniques such as X-ray crystallography, nuclear magnetic resonance (NMR) spectroscopy, and single-particle cryo-electron microscopy (cryo-EM).
Albumins are a type of protein found in various biological fluids, including blood plasma. The most well-known albumin is serum albumin, which is produced by the liver and is the most abundant protein in blood plasma. Serum albumin plays several important roles in the body, such as maintaining oncotic pressure (which helps to regulate fluid balance in the body), transporting various substances (such as hormones, fatty acids, and drugs), and acting as an antioxidant.
Albumins are soluble in water and have a molecular weight ranging from 65,000 to 69,000 daltons. They are composed of a single polypeptide chain that contains approximately 585 amino acid residues. The structure of albumin is characterized by a high proportion of alpha-helices and beta-sheets, which give it a stable, folded conformation.
In addition to their role in human physiology, albumins are also used as diagnostic markers in medicine. For example, low serum albumin levels may indicate liver disease, malnutrition, or inflammation, while high levels may be seen in dehydration or certain types of kidney disease. Albumins may also be used as a replacement therapy in patients with severe protein loss, such as those with nephrotic syndrome or burn injuries.
IGA glomerulonephritis (also known as Berger's disease) is a type of glomerulonephritis, which is a condition characterized by inflammation of the glomeruli, the tiny filtering units in the kidneys. In IgA glomerulonephritis, the immune system produces an abnormal amount of IgA antibodies, which deposit in the glomeruli and cause inflammation. This can lead to symptoms such as blood in the urine, protein in the urine, and swelling in the legs and feet. In some cases, it can also lead to kidney failure. The exact cause of IgA glomerulonephritis is not known, but it is often associated with other conditions such as infections, autoimmune diseases, and certain medications.
The renal veins are a pair of large veins that carry oxygen-depleted blood and waste products from the kidneys to the inferior vena cava, which is the largest vein in the body that returns blood to the heart. The renal veins are formed by the union of several smaller veins that drain blood from different parts of the kidney.
In humans, the right renal vein is shorter and passes directly into the inferior vena cava, while the left renal vein is longer and passes in front of the aorta before entering the inferior vena cava. The left renal vein also receives blood from the gonadal (testicular or ovarian) veins, suprarenal (adrenal) veins, and the lumbar veins.
It is important to note that the renal veins are vulnerable to compression by surrounding structures, such as the overlying artery or a tumor, which can lead to renal vein thrombosis, a serious condition that requires prompt medical attention.
Levamisole is an anthelmintic medication used to treat parasitic worm infections. It works by paralyzing the worms, allowing the body to remove them from the system. In addition, levamisole has been used in veterinary medicine as an immunomodulator, a substance that affects the immune system.
In human medicine, levamisole was previously used in the treatment of colon cancer and autoimmune disorders such as rheumatoid arthritis. However, its use in these areas has largely been discontinued due to side effects and the availability of more effective treatments.
It is important to note that levamisole has also been identified as a common adulterant in cocaine, which can lead to various health issues, including agranulocytosis (a severe decrease in white blood cells), skin lesions, and neurological symptoms.
The Glomerular Basement Membrane (GBM) is a part of the filtration barrier in the nephron of the kidney. It is a thin, porous sheet of extracellular matrix that lies between the glomerular endothelial cells and the visceral epithelial cells (podocytes). The GBM plays a crucial role in the process of ultrafiltration, allowing the passage of water and small molecules while preventing the loss of larger proteins into the urine. It is composed mainly of type IV collagen, laminin, nidogen, and heparan sulfate proteoglycans. Certain kidney diseases, such as Goodpasture's disease and some forms of glomerulonephritis, can involve damage to the GBM.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
The Glomerular Filtration Barrier is a complex structure in the kidney that is responsible for the initial filtration of blood in the nephron. It is made up of three layers: the fenestrated endothelial cells, the glomerular basement membrane (GBM), and the epithelial cells (podocytes) with their interdigitating foot processes. This barrier allows for the filtration of small molecules, such as water and solutes, while preventing the passage of larger molecules, like proteins, into the urinary space. The proper functioning of this barrier is crucial for maintaining normal kidney function and overall health.
Kidney function tests (KFTs) are a group of diagnostic tests that evaluate how well your kidneys are functioning by measuring the levels of various substances in the blood and urine. The tests typically assess the glomerular filtration rate (GFR), which is an indicator of how efficiently the kidneys filter waste from the blood, as well as the levels of electrolytes, waste products, and proteins in the body.
Some common KFTs include:
1. Serum creatinine: A waste product that's produced by normal muscle breakdown and is excreted by the kidneys. Elevated levels may indicate reduced kidney function.
2. Blood urea nitrogen (BUN): Another waste product that's produced when protein is broken down and excreted by the kidneys. Increased BUN levels can suggest impaired kidney function.
3. Estimated glomerular filtration rate (eGFR): A calculation based on serum creatinine, age, sex, and race that estimates the GFR and provides a more precise assessment of kidney function than creatinine alone.
4. Urinalysis: An examination of a urine sample to detect abnormalities such as protein, blood, or bacteria that may indicate kidney disease.
5. Electrolyte levels: Measurement of sodium, potassium, chloride, and bicarbonate in the blood to ensure they're properly balanced, which is essential for normal kidney function.
KFTs are often ordered as part of a routine check-up or when kidney disease is suspected based on symptoms or other diagnostic tests. Regular monitoring of kidney function can help detect and manage kidney disease early, potentially preventing or slowing down its progression.
Plasmapheresis is a medical procedure where the liquid portion of the blood (plasma) is separated from the blood cells. The plasma, which may contain harmful substances such as antibodies or toxins, is then removed and replaced with fresh plasma or a plasma substitute. The remaining blood cells are mixed with the new plasma and returned to the body. This process is also known as therapeutic plasma exchange (TPE). It's used to treat various medical conditions including certain autoimmune diseases, poisonings, and neurological disorders.
I'm sorry for any confusion, but "Frasier Syndrome" is not a recognized medical condition or syndrome in the standard medical literature. It seems like it might be a term that is specific to a certain context or fictional work. In popular culture, "Frasier" is a television show about a character named Frasier Crane, and it's possible that "Frasier Syndrome" could refer to something within the realm of that fiction. However, without more specific information about where you encountered this term, I cannot provide an accurate definition.
Combination drug therapy is a treatment approach that involves the use of multiple medications with different mechanisms of action to achieve better therapeutic outcomes. This approach is often used in the management of complex medical conditions such as cancer, HIV/AIDS, and cardiovascular diseases. The goal of combination drug therapy is to improve efficacy, reduce the risk of drug resistance, decrease the likelihood of adverse effects, and enhance the overall quality of life for patients.
In combining drugs, healthcare providers aim to target various pathways involved in the disease process, which may help to:
1. Increase the effectiveness of treatment by attacking the disease from multiple angles.
2. Decrease the dosage of individual medications, reducing the risk and severity of side effects.
3. Slow down or prevent the development of drug resistance, a common problem in chronic diseases like HIV/AIDS and cancer.
4. Improve patient compliance by simplifying dosing schedules and reducing pill burden.
Examples of combination drug therapy include:
1. Antiretroviral therapy (ART) for HIV treatment, which typically involves three or more drugs from different classes to suppress viral replication and prevent the development of drug resistance.
2. Chemotherapy regimens for cancer treatment, where multiple cytotoxic agents are used to target various stages of the cell cycle and reduce the likelihood of tumor cells developing resistance.
3. Cardiovascular disease management, which may involve combining medications such as angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, diuretics, and statins to control blood pressure, heart rate, fluid balance, and cholesterol levels.
4. Treatment of tuberculosis, which often involves a combination of several antibiotics to target different aspects of the bacterial life cycle and prevent the development of drug-resistant strains.
When prescribing combination drug therapy, healthcare providers must carefully consider factors such as potential drug interactions, dosing schedules, adverse effects, and contraindications to ensure safe and effective treatment. Regular monitoring of patients is essential to assess treatment response, manage side effects, and adjust the treatment plan as needed.
Turner Syndrome is a genetic disorder that affects females, caused by complete or partial absence of one X chromosome. The typical karyotype is 45,X0 instead of the normal 46,XX in women. This condition leads to distinctive physical features and medical issues in growth, development, and fertility. Characteristic features include short stature, webbed neck, low-set ears, and swelling of the hands and feet. Other potential symptoms can include heart defects, hearing and vision problems, skeletal abnormalities, kidney issues, and learning disabilities. Not all individuals with Turner Syndrome will have every symptom, but most will require medical interventions and monitoring throughout their lives to address various health concerns associated with the condition.
Intracellular signaling peptides and proteins are molecules that play a crucial role in transmitting signals within cells, which ultimately lead to changes in cell behavior or function. These signals can originate from outside the cell (extracellular) or within the cell itself. Intracellular signaling molecules include various types of peptides and proteins, such as:
1. G-protein coupled receptors (GPCRs): These are seven-transmembrane domain receptors that bind to extracellular signaling molecules like hormones, neurotransmitters, or chemokines. Upon activation, they initiate a cascade of intracellular signals through G proteins and secondary messengers.
2. Receptor tyrosine kinases (RTKs): These are transmembrane receptors that bind to growth factors, cytokines, or hormones. Activation of RTKs leads to autophosphorylation of specific tyrosine residues, creating binding sites for intracellular signaling proteins such as adapter proteins, phosphatases, and enzymes like Ras, PI3K, and Src family kinases.
3. Second messenger systems: Intracellular second messengers are small molecules that amplify and propagate signals within the cell. Examples include cyclic adenosine monophosphate (cAMP), cyclic guanosine monophosphate (cGMP), diacylglycerol (DAG), inositol triphosphate (IP3), calcium ions (Ca2+), and nitric oxide (NO). These second messengers activate or inhibit various downstream effectors, leading to changes in cellular responses.
4. Signal transduction cascades: Intracellular signaling proteins often form complex networks of interacting molecules that relay signals from the plasma membrane to the nucleus. These cascades involve kinases (protein kinases A, B, C, etc.), phosphatases, and adapter proteins, which ultimately regulate gene expression, cell cycle progression, metabolism, and other cellular processes.
5. Ubiquitination and proteasome degradation: Intracellular signaling pathways can also control protein stability by modulating ubiquitin-proteasome degradation. E3 ubiquitin ligases recognize specific substrates and conjugate them with ubiquitin molecules, targeting them for proteasomal degradation. This process regulates the abundance of key signaling proteins and contributes to signal termination or amplification.
In summary, intracellular signaling pathways involve a complex network of interacting proteins that relay signals from the plasma membrane to various cellular compartments, ultimately regulating gene expression, metabolism, and other cellular processes. Dysregulation of these pathways can contribute to disease development and progression, making them attractive targets for therapeutic intervention.
A mutation is a permanent change in the DNA sequence of an organism's genome. Mutations can occur spontaneously or be caused by environmental factors such as exposure to radiation, chemicals, or viruses. They may have various effects on the organism, ranging from benign to harmful, depending on where they occur and whether they alter the function of essential proteins. In some cases, mutations can increase an individual's susceptibility to certain diseases or disorders, while in others, they may confer a survival advantage. Mutations are the driving force behind evolution, as they introduce new genetic variability into populations, which can then be acted upon by natural selection.
 Nephrotic syndrome
Nephrotic syndrome Nephrotic syndrome: MedlinePlus Medical Encyclopedia
Nephrotic syndrome: MedlinePlus Medical Encyclopedia Nephrotic syndrome Definition & Meaning - Merriam-Webster
Nephrotic syndrome Definition & Meaning - Merriam-Webster Nephrotic Syndrome: Practice Essentials, Pathophysiology, Etiology
Nephrotic Syndrome: Practice Essentials, Pathophysiology, Etiology![Pathogenetic aspectics of nephrotic syndrome]](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Pathogenetic aspectics of nephrotic syndrome]
Pathogenetic aspectics of nephrotic syndrome] A to Z: Nephrotic Syndrome (for Parents) - Primary Children's Hospital
A to Z: Nephrotic Syndrome (for Parents) - Primary Children's Hospital Nephrotic Syndrome (Kidney Disease) | Boston Children's Hospital
Nephrotic Syndrome (Kidney Disease) | Boston Children's Hospital Pathology Outlines - Congenital nephrotic syndrome
Pathology Outlines - Congenital nephrotic syndrome Dr. Kumud Mehta | Nephrotic Syndrome - Videos
Dr. Kumud Mehta | Nephrotic Syndrome - Videos Information for "Nephrotic syndrome primary prevention" - wikidoc
Information for "Nephrotic syndrome primary prevention" - wikidoc Have I had a nephrotic syndrome relapse?
Have I had a nephrotic syndrome relapse? The Influence Of Butea Monosperma On Doxorubicin-induced Nephrotic Syndrome In Rats | 4749
The Influence Of Butea Monosperma On Doxorubicin-induced Nephrotic Syndrome In Rats | 4749 Diet Chart For Nephrotic Syndrome - Food to Take / Food to Avoid
Diet Chart For Nephrotic Syndrome - Food to Take / Food to Avoid Interferon beta: risk of thrombotic microangiopathy and nephrotic syndrome | MIMS online
Interferon beta: risk of thrombotic microangiopathy and nephrotic syndrome | MIMS online Steroid-sensitive nephrotic syndrome and vascular endothelial growth factor gene polymorphisms<...
Steroid-sensitive nephrotic syndrome and vascular endothelial growth factor gene polymorphisms<... Pulsenotes | Nephrotic syndrome
Pulsenotes | Nephrotic syndrome An adolescent with nephrotic syndrome and multiple leg nodules - Fingerprint
- Experts@Minnesota
An adolescent with nephrotic syndrome and multiple leg nodules - Fingerprint
- Experts@Minnesota Genetic Identification of Two Novel Loci Associated with Steroid-Sensitive Nephrotic Syndrome<...
Genetic Identification of Two Novel Loci Associated with Steroid-Sensitive Nephrotic Syndrome<... Nephrotic syndrome - The Curbsiders
Nephrotic syndrome - The Curbsiders Nephrotic Syndrome - Armando Hasudungan
Nephrotic Syndrome - Armando Hasudungan Nephrotic Syndrome | Signs, Symptoms, Support
Nephrotic Syndrome | Signs, Symptoms, Support Chlormethine Hydrochloride is Not Inferior to Tacrolimus in Treating Steroid-Resistant Nephrotic Syndrome. - AMiner
Chlormethine Hydrochloride is Not Inferior to Tacrolimus in Treating Steroid-Resistant Nephrotic Syndrome. - AMiner Liver, Kidney, & Urinary System | Condition Categories | UR Medicine
Liver, Kidney, & Urinary System | Condition Categories | UR Medicine