Myelitis
Neuromyelitis Optica
Myelitis, Transverse
Colon, Transverse
Neuroschistosomiasis
Aquaporin 4
Magnetic Resonance Imaging
Spinal Cord
Transverse Sinuses
Paraplegia
Muscle Hypotonia
Central Nervous System Helminthiasis
Tabes Dorsalis
Meningitis, Aseptic
Demyelinating Autoimmune Diseases, CNS
Rapid onset transverse myelitis in adolescence: implications for pathogenesis and prognosis. (1/114)
Five adolescents with transverse myelitis were reviewed. All presented with a rapid onset paralysis of the lower limbs and impairment of bladder control. The maximum disability developed between 10 minutes and six hours. There was no history of trauma, asthma, or prodromal illness. Investigations failed to demonstrate a vascular cause. Extensive spinal cord abnormalities were observed on magnetic resonance imaging. Electrophysiological investigations, performed in four cases, were all consistent with anterior horn cell damage. In all five adolescents there was poor recovery. The underlying pathogenesis of this rapid onset condition remains a subject of debate. Similarities with both transverse myelitis and fibrocartilaginous emboli are evident, widening the spectrum of conditions within the transverse myelitis umbrella. These observations suggest that in rapid onset "transverse myelitis" the combination of extensive hyperintensity on spinal cord neuroimaging with electrophysiological evidence of anterior horn cell involvement might have adverse prognostic significance. (+info)Somatosensory evoked potentials by paraspinal stimulation in acute transverse myelitis. (2/114)
Somatosensory evoked potentials by paraspinal stimulation were studied in 6 patients with acute transverse myelitis. In one patient in whom posterior tibial somatosensory evoked potentials were not recordable, a poorly formed response was seen with paraspinal stimulation. Slowing of conduction across the involved segment was seen in the remaining 5 patients and fairly correlated with the clinical localization. (+info)Decrease in multiple sclerosis with acute transverse myelitis in Japan. (3/114)
Acute transverse myelitis (ATM) may be a manifestation of multiple sclerosis (MS) and was reported to be more common among Japanese MS patients than in Caucasian MS patients. Recently there are arguments whether clinical manifestations of MS may have changed. Therefore, we studied the frequency of ATM in MS and the clinical subtypes of MS in 86 clinically definite MS patients whose onsets were in 1970-1979, 1980-1989, and 1990-1998 in Sendai City, Japan. Fifty-six of the patients were women and 30 were men. Forty-four patients had the conventional form of MS (C-MS) commonly seen in Western countries, and 42 had optic-spinal or spinal forms of MS (OSS-MS). Twenty MS patients had ATM, and all of them were belong to optic-spinal form of MS. ATM was not seen in any cases of C-MS. The mean onset age (years) of the clinical subtypes was 25.5 in C-MS, 34.1 in OSS-MS without ATM, and 30.9 in OSS-MS with ATM. Among the patients whose onset of the disease was in 1970-1979, 60.0% of them were cases of OSS-MS with ATM, but such cases were markedly decreased to 5.3% in 1990-1998. In contrast, the frequency of C-MS increased to 63.2% in 1990-1998 compared with 20.0% in 1970-1979. Analysis of the data by the year of birth of the patients showed similar results. Our data suggest that the frequency of ATM in MS markedly decreased, and that of C-MS increased during the last 30 years in Sendai, Japan. Since the genetic background of Japanese has not changed, some exogenous factors, such as food, infectious microorganisms, and chemicals in our environment, may be responsible for the change. (+info)Acute transverse myelitis: MR characteristics. (4/114)
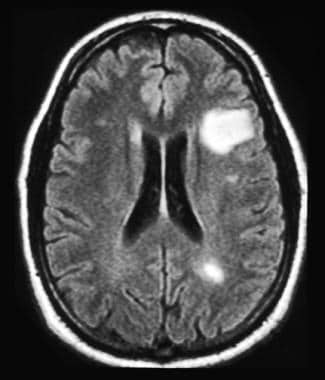
Magnetic resonance imaging findings in 13 patients with acute transverse myelitis are reviewed. In 12 cases centrally located high intensity signal extending over few spinal segments was noted. The lesion occupied more than two thirds of the cord's cross-sectional area in 8 patients. Central dot sign was noted in 7 patients. Variable cord enlargement was seen in 5 patients. Contrast study in one patient showed peripheral enhancement. The MR characteristics that help in differentiating transverse myelitis from spinal form of multiple sclerosis are discussed. (+info)Non-compressive myelopathy: clinical and radiological study. (5/114)
Fifty seven patients (42 males and 15 females) with non-compressive myelopathy were studied from 1997 to 1999. Acute transverse myelitis (ATM) was the commonest (31) followed by Vit B12 deficiency myelopathy (8), primary progressive multiple sclerosis (5), hereditary spastic paraplegia (3), tropical spastic paraplegia (2), subacute necrotising myelitis (1), radiation myelitis (1), syphilitic myelitis (1) and herpes zoster myelitis (1). 4 cases remained unclassified. In the ATM group, mean age was 30.35 years, antecedent event was observed in 41.9% case, 25 cases had symmetrical involvement and most of the cases had severe deficit at onset. CSF study carried out in 23 patients of ATM revealed rise in proteins (mean 147.95mg%, range 20-1200 mg/dL) and pleocytosis (mean 20.78/cumm, range 0-200 mm3). Oligoclonal band (OCB) was present in 28% of cases of ATM. The most common abnormality detected was a multisegment hyperintense lesion on T2W images, that occupied the central area on cross section. In 6 patients hyperintense signal was eccentric in location. MRI was normal in 4 cases of ATM. Thus ATM is the leading cause of non-compressive myelopathy. Clinical features combined with MRI findings are helpful in defining the cause of ATM. (+info)Successful treatment of Epstein-Barr virus-induced transverse myelitis with ganciclovir and cytomegalovirus hyperimmune globulin following unrelated bone marrow transplantation. (6/114)
We report a patient who developed Epstein-Barr virus (EBV)-induced transverse myelitis 19 months after unrelated bone marrow transplantation (BMT). The disease was diagnosed by physical examination, serologic determinations, EBV-specific polymerase chain reaction in peripheral blood lymphocytes and cerebrospinal fluid, and characteristic magnetic resonance imaging scan of the spine. The patient was treated with ganciclovir and cytomegalovirus (CMV) hyperimmune globulin. He gradually improved and recovered completely within 4 weeks. This case suggests that ganciclovir and CMV hyperimmune globulin appear to be effective for the treatment of EBV-induced transverse myelitis in immunocompromised patients following BMT. (+info)Transverse myelopathy in systemic lupus erythematosus: an analysis of 14 cases and review of the literature. (7/114)
OBJECTIVE: To give a comprehensive review of transverse myelopathy (TM), a rare but serious condition reported in 1-2% of patients with systemic lupus erythematosus (SLE). METHODS: 14 patients with SLE and TM were evaluated and 91 additional cases published in the English and German literature reviewed. RESULTS: TM presented either as the initial manifestation or within five years of the diagnosis of SLE. Most patients presented with a detectable sensory deficit at the thoracic level. In our 14 patients, 22% of the patients showed complete neurological recovery, whereas in the total patient population of 105 (our cases plus those reviewed in the literature), complete recovery was observed in 50%, partial recovery in 29% and no improvement or deterioration in 21%. Treatment with intravenous methylprednisolone followed by cyclophosphamide seemed to be most effective. Seventy per cent of the total patient population had abnormal magnetic resonance imaging findings. In our group of 14 patients, those with higher disease activity (measured by the SLAM) at onset of TM were treated more aggressively (for example, with plasmapheresis and intravenous pulse cyclophosphamide). TM in our patients was associated with antiphospholipid antibodies in 43% of the cases as compared with 64% of the total patient population. Optic neuritis occurred in 48% of the total patient population with SLE and TM, suggesting an association. CONCLUSIONS: TM in SLE is a poorly understood entity. Outcome might be more favourable than previously suggested. There is an association of TM with antiphospholipid antibodies in SLE patients. Treatment including intravenous cyclophosphamide may improve the final outcome. This report emphasises the need for multicentre trials to establish guidelines for optimal treatment. (+info)Sjogren's syndrome with primary biliary cirrhosis, complicated by transverse myelitis and malignant lymphoma. (8/114)
A 53-year-old woman with Sjogren's syndrome (SS) and primary biliary cirrhosis (PBC) complicated by transverse myelitis (TM) and malignant lymphoma (ML) is reported. TM has been described only in seven cases of primary SS, including three with PBC and four without PBC. The features of SS associated with PBC and complicated by TM were less typical compared with those seen in SS without PBC complicated by TM. This case is the first report of a case with SS, PBC, TM and ML. SS in association with PBC is, in general, overlooked, but such cases must be investigated with great caution for extraglandular complications. (+info)Myelitis is a medical term that refers to inflammation of the spinal cord. This inflammation can cause damage to the myelin sheath, which is the protective covering of nerve fibers in the spinal cord. As a result, the transmission of nerve impulses along the spinal cord may be disrupted, leading to various neurological symptoms.
Myelitis can affect any part of the spinal cord and can have many different causes, including infections (such as viral or bacterial infections), autoimmune disorders (such as multiple sclerosis), and other conditions (such as spinal cord injuries or tumors). The specific symptoms of myelitis depend on the location and severity of the inflammation. They may include muscle weakness, numbness or tingling sensations, pain, bladder or bowel dysfunction, and difficulty with coordination and balance.
Myelitis can be a serious condition that requires prompt medical attention and treatment. Treatment typically focuses on addressing the underlying cause of the inflammation, as well as managing symptoms and supporting recovery.
Neuromyelitis optica (NMO), also known as Devic's disease, is an autoimmune disorder that affects the central nervous system (CNS). It primarily causes inflammation and damage to the optic nerves (which transmit visual signals from the eye to the brain) and the spinal cord. This results in optic neuritis (inflammation of the optic nerve, causing vision loss) and myelitis (inflammation of the spinal cord, leading to motor, sensory, and autonomic dysfunction).
A key feature of NMO is the presence of autoantibodies against aquaporin-4 (AQP4-IgG), a water channel protein found in astrocytes (a type of glial cell) in the CNS. These antibodies play a crucial role in the development of the disease, as they target and damage the AQP4 proteins, leading to inflammation, demyelination (loss of the protective myelin sheath around nerve fibers), and subsequent neurological dysfunction.
NMO is distinct from multiple sclerosis (MS), another autoimmune disorder affecting the CNS, as it has different clinical features, radiological findings, and treatment responses. However, NMO can sometimes be misdiagnosed as MS due to overlapping symptoms in some cases. Accurate diagnosis of NMO is essential for appropriate management and treatment, which often includes immunosuppressive therapies to control the autoimmune response and prevent further damage to the nervous system.
Transverse Myelitis is a neurological disorder that involves inflammation of the spinal cord, leading to damage in both sides of the cord. This results in varying degrees of motor, sensory, and autonomic dysfunction, typically defined by the level of the spine that's affected. Symptoms may include a sudden onset of lower back pain, muscle weakness, paraesthesia or loss of sensation, and bowel/bladder dysfunction. The exact cause is often unknown but can be associated with infections, autoimmune disorders, or other underlying conditions.
The transverse colon is the section of the large intestine that runs horizontally across the abdomen, located between the ascending colon and the descending colon. It receives digested food material from the left side of the cecum via the transverse mesocolon, a double-layered fold of peritoneum that attaches it to the posterior abdominal wall.
The transverse colon is responsible for absorbing water, electrolytes, and vitamins from the digested food material before it moves into the distal sections of the large intestine. It also contains a large number of bacteria that help in the breakdown of complex carbohydrates and the production of certain vitamins, such as vitamin K and biotin.
The transverse colon is highly mobile and can change its position within the abdomen depending on factors such as respiration, digestion, and posture. It is also prone to various pathological conditions, including inflammation (colitis), diverticulosis, and cancer.
Neuroschistosomiasis is a form of schistosomiasis, which is a parasitic infection caused by Schistosoma species. It is characterized by the invasion and inflammation of the central nervous system (CNS) by the parasite's eggs or larvae. This can lead to various neurological symptoms such as seizures, headaches, visual disturbances, and motor or sensory deficits. Neuroschistosomiasis is a serious and potentially life-threatening condition that requires prompt diagnosis and treatment.
The two Schistosoma species most commonly associated with neuroschistosomiasis are S. japonicum and S. mansoni. The parasites typically enter the human body through skin contact with contaminated water, where they mature into adult worms in the bloodstream. Female worms then lay eggs, some of which may be carried to the CNS by the circulatory system.
Neuroschistosomiasis can occur in both acute and chronic forms. Acute neuroschistosomiasis is characterized by an inflammatory response to the parasite's eggs or larvae, which can cause eosinophilic meningitis or encephalitis. Chronic neuroschistosomiasis may result in the formation of granulomas around the eggs, leading to various neurological symptoms depending on the location and extent of the damage.
Diagnosis of neuroschistosomiasis typically involves a combination of clinical evaluation, imaging studies (such as MRI or CT scans), and laboratory tests (such as serology or CSF analysis). Treatment usually consists of anti-parasitic drugs such as praziquantel, combined with corticosteroids to manage the inflammatory response. In severe cases, surgical intervention may be necessary to alleviate symptoms or prevent further damage.
Aquaporin 4 (AQP4) is a water channel protein that is primarily found in the membranes of astrocytes, which are a type of glial cell in the central nervous system. AQP4 plays a crucial role in the regulation of water homeostasis and the clearance of excess fluid from the brain and spinal cord. It also facilitates the rapid movement of water across the blood-brain barrier and between astrocytes, which is important for maintaining proper neuronal function and protecting the brain from edema or swelling.
Mutations in the AQP4 gene can lead to various neurological disorders, such as neurodegenerative diseases and neuromyelitis optica spectrum disorder (NMOSD), a severe autoimmune condition that affects the optic nerves and spinal cord. In NMOSD, the immune system mistakenly attacks AQP4 proteins, causing inflammation, demyelination, and damage to the nervous tissue.
Methylprednisolone is a synthetic glucocorticoid drug, which is a class of hormones that naturally occur in the body and are produced by the adrenal gland. It is often used to treat various medical conditions such as inflammation, allergies, and autoimmune disorders. Methylprednisolone works by reducing the activity of the immune system, which helps to reduce symptoms such as swelling, pain, and redness.
Methylprednisolone is available in several forms, including tablets, oral suspension, and injectable solutions. It may be used for short-term or long-term treatment, depending on the condition being treated. Common side effects of methylprednisolone include increased appetite, weight gain, insomnia, mood changes, and increased susceptibility to infections. Long-term use of methylprednisolone can lead to more serious side effects such as osteoporosis, cataracts, and adrenal suppression.
It is important to note that methylprednisolone should be used under the close supervision of a healthcare provider, as it can cause serious side effects if not used properly. The dosage and duration of treatment will depend on various factors such as the patient's age, weight, medical history, and the condition being treated.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
The spinal cord is a major part of the nervous system, extending from the brainstem and continuing down to the lower back. It is a slender, tubular bundle of nerve fibers (axons) and support cells (glial cells) that carries signals between the brain and the rest of the body. The spinal cord primarily serves as a conduit for motor information, which travels from the brain to the muscles, and sensory information, which travels from the body to the brain. It also contains neurons that can independently process and respond to information within the spinal cord without direct input from the brain.
The spinal cord is protected by the bony vertebral column (spine) and is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each segment corresponds to a specific region of the body and gives rise to pairs of spinal nerves that exit through the intervertebral foramina at each level.
The spinal cord is responsible for several vital functions, including:
1. Reflexes: Simple reflex actions, such as the withdrawal reflex when touching a hot surface, are mediated by the spinal cord without involving the brain.
2. Muscle control: The spinal cord carries motor signals from the brain to the muscles, enabling voluntary movement and muscle tone regulation.
3. Sensory perception: The spinal cord transmits sensory information, such as touch, temperature, pain, and vibration, from the body to the brain for processing and awareness.
4. Autonomic functions: The sympathetic and parasympathetic divisions of the autonomic nervous system originate in the thoracolumbar and sacral regions of the spinal cord, respectively, controlling involuntary physiological responses like heart rate, blood pressure, digestion, and respiration.
Damage to the spinal cord can result in various degrees of paralysis or loss of sensation below the level of injury, depending on the severity and location of the damage.
The transverse sinuses are a pair of venous channels located within the skull. They are part of the intracranial venous system and are responsible for draining blood from the brain. The transverse sinuses run horizontally along the upper portion of the inner skull, starting at the occipital bone (at the back of the head) and extending to the temporal bones (on the sides of the head).
These sinuses receive blood from the superior sagittal sinus, straight sinus, and the occipital sinus. After passing through the transverse sinuses, the blood is then drained into the sigmoid sinuses, which in turn drain into the internal jugular veins. The transverse sinuses are an essential component of the cerebral venous system, ensuring proper blood flow and drainage from the brain.
Paraplegia is a medical condition characterized by partial or complete loss of motor function and sensation in the lower extremities, typically affecting both legs. This results from damage to the spinal cord, often due to trauma such as accidents, falls, or gunshot wounds, or from diseases like spina bifida, polio, or tumors. The specific area and extent of the injury on the spinal cord determine the severity and location of paralysis. Individuals with paraplegia may require assistive devices for mobility, such as wheelchairs, and may face various health challenges, including pressure sores, urinary tract infections, and chronic pain.
Muscle hypotonia, also known as decreased muscle tone, refers to a condition where the muscles appear to be flaccid or lacking in tension and stiffness. This results in reduced resistance to passive movements, making the limbs feel "floppy" or "like a rag doll." It can affect any muscle group in the body and can be caused by various medical conditions, including neurological disorders, genetic diseases, and injuries to the nervous system. Hypotonia should not be confused with muscle weakness, which refers to the inability to generate normal muscle strength.
Central nervous system helminthiasis is a medical condition that refers to the invasion and infection of the central nervous system (CNS), specifically the brain and spinal cord, by parasitic worms, also known as helminths. This rare but serious condition can occur when helminth larvae or eggs accidentally migrate from their usual location in the body to the CNS through the bloodstream or cerebrospinal fluid.
The most common types of helminths that can cause CNS helminthiasis include:
1. Neurocysticercosis: This is caused by the larval stage of the tapeworm Taenia solium, which typically infects the muscles and brain. However, when the larvae invade the CNS, they can form cysts that cause inflammation, swelling, and damage to brain tissue.
2. Echinococcosis: This is caused by the larval stage of the tapeworm Echinococcus granulosus or Echinococcus multilocularis. The larvae can form hydatid cysts in various organs, including the brain, leading to neurological symptoms.
3. Gnathostomiasis: This is caused by the larval stage of the nematode Gnathostoma spinigerum or Gnathostoma hispidum. The larvae can migrate to various organs, including the CNS, causing inflammation and damage to brain tissue.
4. Angiostrongyliasis: This is caused by the nematode Angiostrongylus cantonensis, which typically infects rats but can accidentally infect humans through contaminated food or water. The larvae can migrate to the CNS and cause eosinophilic meningitis, an inflammation of the membranes surrounding the brain and spinal cord.
Symptoms of CNS helminthiasis depend on the type of parasite involved, the location and extent of the infection, and the host's immune response. They can range from mild to severe and may include headache, seizures, weakness, numbness, vision changes, confusion, and cognitive impairment. Diagnosis is usually based on clinical presentation, imaging studies, and laboratory tests, such as serology or CSF analysis. Treatment depends on the type of parasite involved and may include antiparasitic drugs, corticosteroids, and supportive care. Prevention measures include avoiding contaminated food and water, practicing good hygiene, and using insect repellents to prevent mosquito-borne infections.
Tabes dorsalis is a late-stage complication of untreated neurosyphilis, a sexually transmitted infection caused by the bacterium Treponema pallidum. It is characterized by degeneration of the posterior columns and dorsal roots of the spinal cord, leading to various neurological symptoms.
The medical definition of Tabes Dorsalis is:
A chronic progressive degenerative disease of the spinal cord, specifically affecting the dorsal root ganglia and posterior columns, caused by the tertiary stage of syphilis. The condition is characterized by a combination of motor, sensory, and autonomic disturbances, including ataxia, Romberg's sign, lightning pains, hypo- or areflexia, impaired proprioception, dissociated sensations, and Argyll Robertson pupils. If left untreated, Tabes Dorsalis can lead to significant disability and even death.
Aseptic meningitis is a type of meningitis (inflammation of the membranes covering the brain and spinal cord) that is not caused by bacterial infection. Instead, it can be due to viral infections, fungal infections, or non-infectious causes such as certain medications, chemical irritants, or underlying medical conditions. In aseptic meningitis, the cerebrospinal fluid (CSF) analysis may show increased white blood cells, typically lymphocytes, but no bacterial growth on culture. Common viral causes include enteroviruses, herpes simplex virus, and varicella-zoster virus. Treatment depends on the underlying cause and may include supportive care, antiviral medications, or immunosuppressive therapy in some cases.
Demyelinating autoimmune diseases of the central nervous system (CNS) are a group of disorders characterized by inflammation and damage to the myelin sheath, which is the protective covering that surrounds nerve fibers in the brain and spinal cord. This damage can result in various neurological symptoms, including muscle weakness, sensory loss, vision problems, and cognitive impairment.
The most common demyelinating autoimmune disease of the CNS is multiple sclerosis (MS), which affects approximately 2.3 million people worldwide. Other examples include neuromyelitis optica spectrum disorder (NMOSD), acute disseminated encephalomyelitis (ADEM), and transverse myelitis.
These conditions are thought to arise when the immune system mistakenly attacks the myelin sheath, leading to inflammation, damage, and scarring (sclerosis) in the CNS. The exact cause of this autoimmune response is not fully understood, but it is believed to involve a complex interplay between genetic, environmental, and immunological factors.
Treatment for demyelinating autoimmune diseases of the CNS typically involves a combination of medications to manage symptoms, reduce inflammation, and modify the course of the disease. These may include corticosteroids, immunosuppressive drugs, and disease-modifying therapies (DMTs) that target specific components of the immune system.
 Transverse myelitis
Transverse myelitis Transverse Myelitis and MS | National MS Society
Transverse Myelitis and MS | National MS Society Transverse myelitis
Transverse myelitis transverse myelitis | Virology Blog
transverse myelitis | Virology Blog Acute transverse myelitis of the cervical spine secondary to psoas abscess | BMC Infectious Diseases | Full Text
Acute transverse myelitis of the cervical spine secondary to psoas abscess | BMC Infectious Diseases | Full Text Acute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional Edition
Acute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional Edition Probable Spinal Neuroschistosomiasis Manifesting as Transverse Myelitis. - MORU Tropical Health Network
Probable Spinal Neuroschistosomiasis Manifesting as Transverse Myelitis. - MORU Tropical Health Network Transverse Myelitis
Transverse Myelitis transverse myelitis
transverse myelitis transverse myelitis - The Curbsiders
transverse myelitis - The Curbsiders What is Transverse Myelitis?
What is Transverse Myelitis? Transverse Myelitis | Northwestern Medicine
Transverse Myelitis | Northwestern Medicine Diagnosing Transverse Myelitis | PainScale
Diagnosing Transverse Myelitis | PainScale Acute transverse myelitis - Radiology Cases
Acute transverse myelitis - Radiology Cases Transverse myelitis, acute - CCMDB Wiki
Transverse myelitis, acute - CCMDB Wiki "Getting Transverse Myelitis" by Robert A. Slayton
"Getting Transverse Myelitis" by Robert A. Slayton Scott's Story - Transverse Myelitis & MOG Antibody Disease
Scott's Story - Transverse Myelitis & MOG Antibody Disease Transverse myelitis - Causes, Symptoms, Treatment, Prognosis and Complications
Transverse myelitis - Causes, Symptoms, Treatment, Prognosis and Complications Guillain-Barré syndrome, transverse myelitis and infectious diseases
Guillain-Barré syndrome, transverse myelitis and infectious diseases Acute Transverse Myelitis - REBEL EM - Emergency Medicine Blog
Acute Transverse Myelitis - REBEL EM - Emergency Medicine Blog Transverse Myelitis - Symptoms, Causes and Treatment - Apollo Hospital
Transverse Myelitis - Symptoms, Causes and Treatment - Apollo Hospital NFL Players Raise Awareness for Transverse Myelitis Patients - Global Genes
NFL Players Raise Awareness for Transverse Myelitis Patients - Global Genes