Mandibular Nerve
Lingual Nerve
Pterygoid Muscles
Sciatic Nerve
Clinically safe dosage of felypressin for patients with essential hypertension. (1/166)
Hemodynamic changes were evaluated in patients with essential hypertension when felypressin of various concentrations was administered. The parameters studied were systolic pressure, diastolic pressure, heart rate, left ventricular systolic phase, and endocardial viability ratio. Results showed that blood pressure tended to increase, and the value of 1/pre-ejection period2 (PEP2) tended to decrease, upon administration of 3 ml of 2% propitocaine containing 0.06 international units/ml (IU/ml) of felypressin. Significant increase of blood pressure and decrease in 1/PEP2 was noted upon administration of 3 ml of anesthetic solution containing 0.13 IU/ml of felypressin. No ischemic change of the myocardium was detected even with the highest felypressin concentration (3 ml of 2% propitocaine containing 0.25 IU/ml of felypressin). These results suggest that the clinically safe dosage of felypressin for patients with essential hypertension is approximately 0.18 IU. This amount is equivalent to 6 ml of 3% propitocaine with 0.03 IU/ml of felypressin, which is a commercially available local anesthetic for dental use. It seems that the decrease in 1/PEP2 that occurred during blood pressure increase was due to the increase in afterload caused by contraction of the arterioles. Although in the present study no ischemic change was noted, special care should be taken to prevent myocardial ischemia in patients with severe hypertension. (+info)Prolonged diplopia following a mandibular block injection. (2/166)
A case is presented in which a 14-yr-old girl developed diplopia after injection of the local anesthetic Xylotox E 80 A (2% lidocaine with 1:80,000 epinephrine). Since the complication had a relatively slow onset and lasted for 24 hr, the commonly suggested explanations based on vascular, lymphatic, and neural route theories do not adequately fit the observations. No treatment, other than reassurance, was necessary, and the patient recovered fully. (+info)Efficacy of mandibular topical anesthesia varies with the site of administration. (3/166)
This study compared the threshold of pain sensitivity in the anterior mandibular mucobuccal fold with the posterior. This was followed by a comparison of the reduction of needle insertion pain in the anterior mucobuccal fold and the pterygo-temporal depression by either topical anesthesia or nitrous oxide inhalation. The pain threshold was determined by an analgometer, a pain-measuring device that depends on pressure readings; additionally, pain caused by a needle inserted by a normal technique was assessed using a visual analog scale (VAS). The threshold of pain was significantly lower in the incisor and canine regions than in the premolar and the molar regions (P < 0.001). Compared to a placebo, topical anesthesia significantly reduced the pain from needle insertion in the mucobuccal fold adjacent to the mandibular canine (P < 0.001), but did not significantly reduce pain in the pterygotemporal depression. The addition of 30% nitrous oxide did not significantly alter pain reduction compared to a control of 100% oxygen. These results suggest that topical anesthesia application may be effective in reducing the pain of needle insertion in the anterior mandibular mucobuccal fold, but may not be as effective for a standard inferior alveolar nerve block. The addition of 30% nitrous oxide did not lead to a significant improvement. (+info)Neural modulation of inflammatory reactions in dental tissues incident to orthodontic tooth movement. A review of the literature. (4/166)
This article reviews the current knowledge of the biological aspects of dental tissue changes incident to orthodontic tooth movement. The inflammatory nature of these tissue changes was first recognized in the early 1970s, and since then a number of morphological and quantitative investigations have been published in support of this view. The studies dealing with vascular and cellular dental tissue changes, as well as those concerned with inflammatory mediators present at sites of orthodontic tooth movement are systematized and presented accordingly. Special emphasis is placed upon the role of the sensory nerve fibres and their neuropeptides in the control, and development of an inflammatory process, i.e. their role in tooth movement. (+info)Anesthetic efficacy of a repeated intraosseous injection given 30 min following an inferior alveolar nerve block/intraosseous injection. (5/166)
To determine whether a repeated intraosseous (IO) injection would increase or prolong pulpal anesthesia, we measured the degree of anesthesia obtained by a repeated IO injection given 30 min following a combination inferior alveolar nerve block/intraosseous injection (IAN/IO) in mandibular second premolars and in first and second molars. Using a repeated-measures design, we randomly assigned 38 subjects to receive two combinations of injections at two separate appointments. The combinations were an IAN/IO injection followed approximately 30 min later by another IO injection of 0.9 ml of 2% lidocaine with 1:100,000 epinephrine and a combination IAN/IO injection followed approximately 30 min later by a mock IO injection. The second premolar, first molar, and second molar were blindly tested with an Analytic Technology pulp tester at 2-min cycles for 120 min postinjection. Anesthesia was considered successful when two consecutive readings of 80 were obtained. One hundred percent of the subjects had lip numbness with IAN/IO and with IAN/IO plus repeated IO techniques. Rates of anesthetic success for the IAN/IO and for the IAN/IO plus repeated IO injection, respectively, were 100% and 97% for the second premolar, 95% and 95% for the first molar, and 87% and 87% for the second molar. The repeated IO injection increased pulpal anesthesia for approximately 14 min in the second premolar and for 6 min in the first molar, but no statistically significant differences (P > 0.05) were shown. In conclusion, the repeated IO injection of 0.9 ml of 2% lidocaine with 1:100,000 epinephrine given 30 min following a combination IAN/IO injection did not significantly increase pulpal anesthesia in mandibular second premolars or in first and second molars. (+info)Course and composition of the nerves that supply the mandibular teeth of the rat. (6/166)
The rodent dentition has become an important model for investigations of interactions between dental tissues and peripheral neurons. Although experimental nerve injury has been widely used for such studies, there is uncertainty about the courses of nerve fibers supplying the mandibular teeth. In order to clarify this, we used a mixture of monoclonal antibodies against neurofilament proteins to enhance demonstration of nerve fibers so that small nerves could be readily traced in serial frozen sections of mandibles of Sprague Dawley rats ranging in age from embryonic day (E) 18 to postnatal day (P) 90. The 1st molar and anterior portion of the 2nd molar were innervated by small nerves that emerged as distinct branches of the IAN trunk at or near the mandibular foramen. In contrast, the nerve supply to the 3rd molar and posterior part of the 2nd molar was a branch of the lingual nerve that bypassed the mandibular canal altogether. The IAN trunk split into the mental nerve and a large branch to the incisor about 2 mm anterior to the mandibular foramen. Thick branches of the incisor nerve descended into the incisor socket to form a dense plexus of nerve fiber bundles extending along the length of the incisor periodontium. The sparse pulpal innervation of the incisor was provided by a few thin fascicles that emerged from the caudal portion of the periodontal plexus to enter the incisor apex. The dental branches of the IAN and lingual nerve seen in the adult were well established and readily identifiable at age E18 even though their targets were limited to the follicles of the developing teeth. These studies show that the trigeminal branches that supply the mandibular teeth can be identified at a wide range of ages as distinct nerves at a considerable distance proximal to their targets. This detailed information on the courses taken by the dental nerves can provide an anatomical basis for increased precision in characterization and perturbation of neural pathways from the molars and incisor. (+info)Primary afferent synaptic responses recorded from trigeminal caudal neurons in a mandibular nerve-brainstem preparation of neonatal rats. (7/166)
1. Whole-cell patch-clamp recordings were made from the neurons in the superficial trigeminal caudal nucleus (substantia gelatinosa) visually identified in a parasagittal brainstem slice of neonatal rat with the mandibular nerve attached. 2. Stimulation of the mandibular nerve at 0.03 Hz evoked compound excitatory postsynaptic potentials (EPSPs) or currents (EPSCs) in trigeminal caudal neurons. When stimulated at higher frequency (> 0.5 Hz), compound synaptic responses were largely attenuated and a small component remained. This component had a monosynaptic nature, following high-frequency stimulation (33-50 Hz) with a stable synaptic latency. 3. The N-methyl-D-aspartate (NMDA) receptor antagonist D(-)-2-amino-5-phosphonopentanoic acid (D-AP5, 50 microM) largely attenuated the slow polysynaptic EPSCs. The AMPA/kainate receptor antagonist 6-cyano-7-nitroquinoxaline-2,3-dione (CNQX, 10 microM) largely attenuated monosynaptic EPSCs, but only weakly attenuated slow polysynaptic EPSCs. Simultaneous application of CNQX and D-AP5 completely abolished EPSCs. The monosynaptic EPSCs isolated by repetitive stimulation had both NMDA and non-NMDA components. 4. Monosynaptic EPSCs having high threshold had a relatively long latency. During repetitive stimulation (0.5-5.0 Hz), EPSCs having high threshold and long latency underwent a stepwise potentiation in an activity-dependent manner. The conduction velocity estimated for these EPSCs fell into the range of C-fibres. The activity-dependent potentiation was observed for both non-NMDA and NMDA EPSCs and was accompanied by a significant decrease in the coefficient of variation of EPSC amplitude. 5. We suggest that the activity-dependent potentiation of EPSCs is induced presynaptically and that it may underlie the wind-up phenomenon, an activity-dependent hyperexcitability of the primary afferent C-fibres. (+info)Effects of different types of injury to the inferior alveolar nerve on the behavior of Schwann cells during the regeneration of periodontal nerve fibers of rat incisor. (8/166)
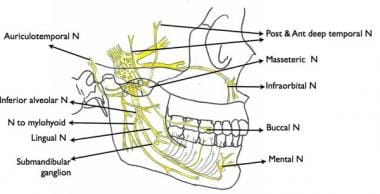
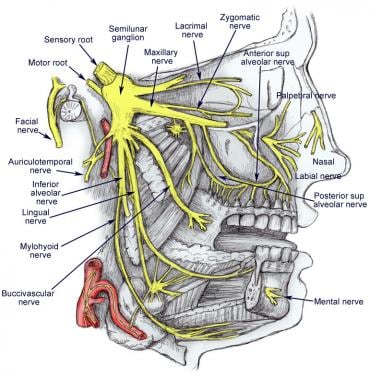
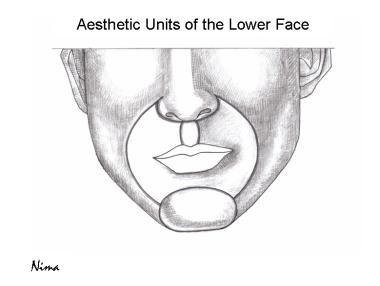
The present study reports on different regeneration patterns of axons and Schwann cells in the periodontal ligament of the rat incisor using immunohistochemistry of protein gene product 9.5 (PGP 9.5) and S-100 protein. Three kinds of injury (transection, crush and segmental resection) were applied to the inferior alveolar nerve. In normal animals, PGP 9.5- and S-100-immunoreactivities were detected in the axons and Schwann cell elements of periodontal Ruffini endings, respectively. They were restricted to the alveolus-related part, occurring only rarely in the tooth-related part and in the shear zone (the border between the alveolus-related and tooth-related parts). Both transection and segmental resection caused the complete disappearance of PGP 9.5-immunoreactive nerve fibers in the periodontal ligament, while a small number of them could be found following the crush injury. Regenerating PGP 9.5-reactive nerve fibers appeared at 5 days and 21 days following the transection and segmental resection, respectively. The regeneration of periodontal nerve fibers completed in a period of 21-28 days and 14-21 days following the transection and crush, respectively, but was not completed even at 56 days following the segmental resection. The behavior of Schwann cells during regeneration was similar after the different nerve injuries; spindle-shaped S-100-immunoreactive cells, presumably Schwann cells, appeared in the shear zone and the tooth-related part. These cells disappeared 5-7 days prior to the completion of the regeneration of axonal elements of the periodontal ligament following the transection and crush. Following the segmental resection, in contrast, spindle-shaped S-100-positive cells disappeared from the tooth-related part at 42 days, although the axonal regeneration of periodontal Ruffini endings proceeded even until 56 days. We thus conclude that the duration of the migration of Schwann cells depends on the state of the regeneration of axons. (+info)The mandibular nerve is a branch of the trigeminal nerve (the fifth cranial nerve), which is responsible for sensations in the face and motor functions such as biting and chewing. The mandibular nerve provides both sensory and motor innervation to the lower third of the face, below the eye and nose down to the chin.
More specifically, it carries sensory information from the lower teeth, lower lip, and parts of the oral cavity, as well as the skin over the jaw and chin. It also provides motor innervation to the muscles of mastication (chewing), which include the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles.
Damage to the mandibular nerve can result in numbness or loss of sensation in the lower face and mouth, as well as weakness or difficulty with chewing and biting.
The lingual nerve is a branch of the mandibular division of the trigeminal nerve (cranial nerve V). It provides general sensory innervation to the anterior two-thirds of the tongue, including taste sensation from the same region. It also supplies sensory innervation to the floor of the mouth and the lingual gingiva (gum tissue). The lingual nerve is closely associated with the submandibular and sublingual salivary glands and their ducts.
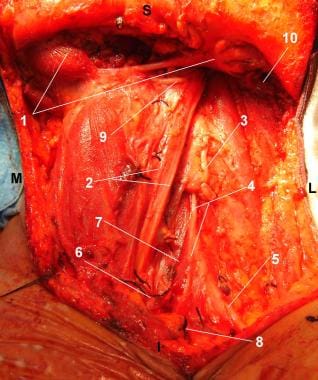
The pterygoid muscles are a pair of muscles located in the deep part of the lateral aspect of the nasopharynx, in the human head. They are part of the group of muscles known as the muscles of mastication, which are involved in the chewing process.
There are two sets of pterygoid muscles: the medial and lateral pterygoids. The medial pterygoids are located deep within the jaw, near the temporomandibular joint (TMJ). They originate from the medial surface of the lateral pterygoid plate of the sphenoid bone and insert onto the inner aspect of the angle of the mandible (lower jawbone). The main function of the medial pterygoids is to assist in closing the jaw and moving it forward during chewing.
The lateral pterygoids, on the other hand, are located more superficially than the medial pterygoids and are situated near the TMJ. They have two heads: the upper head originates from the greater wing of the sphenoid bone, while the lower head arises from the lateral surface of the lateral pterygoid plate. The lateral pterygoids insert onto the front part of the neck of the mandible and the disc of the TMJ. Their main function is to assist in opening the jaw and moving it sideways during chewing.
Together, the pterygoid muscles play a crucial role in the movement and function of the jaw, allowing us to chew food effectively and speak clearly.
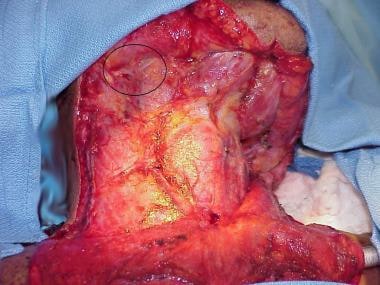
Glossectomy is a surgical procedure that involves the partial or total removal of the tongue. This type of surgery may be performed for various reasons, such as treating certain types of cancer (like oral or tongue cancer) that have not responded to other forms of treatment, or removing a portion of the tongue that's severely damaged or injured due to trauma.
The extent of the glossectomy depends on the size and location of the tumor or lesion. A partial glossectomy refers to the removal of a part of the tongue, while a total glossectomy involves the complete excision of the tongue. In some cases, reconstructive surgery may be performed to help restore speech and swallowing functions after the procedure.
It is essential to note that a glossectomy can significantly impact a patient's quality of life, as the tongue plays crucial roles in speaking, swallowing, and taste sensation. Therefore, multidisciplinary care involving speech therapists, dietitians, and other healthcare professionals is often necessary to help patients adapt to their new conditions and optimize their recovery process.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
 Mandibular nerve
Mandibular nerve
Meningeal branch of the mandibular nerve
Marginal mandibular branch of the facial nerve
Mandibular canal
Medial pterygoid nerve
Mandibular prominence
Mental foramen
Masseter muscle
Inferior alveolar nerve
Muscles of mastication
Lingual nerve
Orthognathic surgery
Pharyngeal pouch (embryology)
Masseteric nerve
Tensor veli palatini muscle
Medial pterygoid muscle
Inferior alveolar artery
Pterygopalatine nerves
Foramen ovale (skull)
Mandibular foramen
Submandibular gland
Hyoglossus
Lateral pterygoid muscle
Brasilodon
Middle meningeal artery
Chorda tympani
Mentalis
Depressor anguli oris muscle
Dental extraction
Depressor labii inferioris muscle
Ophthalmic2
- In neuroanatomy, the mandibular nerve (V3) is the largest of the three divisions of the trigeminal nerve, the fifth cranial nerve (CN V). Unlike the other divisions of the trigeminal nerve (ophthalmic nerve, maxillary nerve) which contain only afferent fibers, the mandibular nerve contains both afferent and efferent fibers. (wikipedia.org)
- ganglion, ophthalmic, mandibular and maxillary nerves. (canstockphoto.ca)
Mandible5
- The purpose of this study is to assess the incidence of marginal mandibular nerve palsy, or damage to the nerve that controls the muscles of the lower lip and chin, following mandible distraction osteogenesis (MDO) in infants with Pierre Robin Sequence. (chp.edu)
- As a result, any pain sensations originating from irritated nerves in the lower teeth and roots may be felt more intensely and transmitted more readily through the dense mandible bone. (cdhp.org)
- This nerve runs on the inside of the upper part of the mandible, or lower jawbone, and turns over the jawbone's uppermost tip after giving off parotid branches. (healthline.com)
- Class III BMCs were observed uni- the mandible from the mandibular fora- in 4200 panoramic radiographs of Syr- laterally in eight cases (19.5%), five on men to the mental foramen, involving ian subjects (1899 women and 2301 the right side and three on the left side. (who.int)
- Involvement of the mandibular division of the trigeminal nerve may manifest as hypesthesia along the mandible or wasting of the temporalis or masseter muscles. (medscape.com)
Inferior alveolar8
- We hypothesize that the removal of mandibular third molars (M3) 6 months prior to a bilateral sagittal split osteotomy (BSSO) could allow the displacement of the inferior alveolar nerve (IAN) in a favorable lingual position. (em-consulte.com)
- This study confirms the absence of influence of mandibular third molar removal on the inferior alveolar nerve route prior to BSSO. (em-consulte.com)
- Objectives The aim of this study was to compare the onset, success rate, injection pain, and post-injection pain of mental/incisive nerve block (MINB) with that of inferior alveolar nerve block (IANB) using 4% articaine in mandibular premolars with symptomatic irreversible pulpitis. (drnekoofar.com)
- Comparison of panoramic radiograph and cone beam computed tomography findings for impacted mandibular third molar root and inferior alveolar nerve canal relation. (revistamedical.com)
- The main nerves supplying and interacting with the lower teeth are the left and right inferior alveolar nerves. (cdhp.org)
- I was wondering about this recently as my dentist raised a huge syringe and moved it toward my mandibular nerve, hoping for a complete blockage of pain sensations that would travel up from the inferior alveolar nerve in my lower jaw. (wallstreetpit.com)
- the inferior alveolar nerve, artery and men), ranging in age from 18 to 55 Five cases were males while three were vein. (who.int)
- the inferior alveolar dental nerve block is the method most commonly used by endodontists to achieve local anesthesia during treatments. (bvsalud.org)
Molars5
- In this situation, it may be associated with the injection of a local anesthetic, prolonged surgical procedure for the removal of mandibular molars and infections of dental origin. (bvsalud.org)
- Accuracy of panoramic radiographic predictor signs in the assessment of proximity of impacted third molars with the mandibular canal. (revistamedical.com)
- Tofangchiha M, Koushaei S, Mortazavi M, Souri Z, Alizadeh A, Patini R. Positive Predictive Value of Panoramic Radiography for Assessment of the Relationship of Impacted Mandibular Third Molars with the Mandibular Canal Based on Cone-Beam Computed Tomography: A Cross-Sectional Study. (revistamedical.com)
- The presentation of a bifid mandibular canal poses difficulties when carrying out dental procedures, including administration of mandibular block anaesthesia, oral surgical procedures of the lower third molars, orthognathic surgery and implant placement. (edu.au)
- Martínez-Martínez A, Freyle-Granados E, Senior-Carmona N. Efficacy of 2% lidocaine and 4% articaine in mandibular molars with different pulp diagnoses in the mandibular technique. (bvsalud.org)
Marginal mandibular nerve2
- To calculate the incidence of marginal mandibular nerve palsy, researchers from the Cleft-Craniofacial Center of UPMC Children's Hospital of Pittsburgh will collect photographs and/or video of participants smiling and making other facial expressions. (chp.edu)
- While MDO is effective, complications are not uncommon, including facial nerve dysfunction (FND), particularly involving the marginal mandibular nerve (MMN). (nesps.org)
Bifid mandibular canals4
- Bilateral bifid mandibular canals: special relevance to a general dental practitioner. (edu.au)
- Dental practitioners may encounter bifid mandibular canals upon radiographic assessment, and may not understand the true extent of this presentation. (edu.au)
- The purpose of the communication is to draw dental practitioner's attention to the variations of bifid mandibular canals and ensure practitioners interpret radiograph correctly to make an informed diagnosis and eliminate the risk of damage and discomfort in the event of surgical treatment being carried out. (edu.au)
- ABSTRACT The objective of this study was to classify the different routes of the bifid mandibular canals (BMCs) on 2400 panoramic radiographs in a Syrian population. (who.int)
Canal9
- Its sensory branch enters the mandibular canal and is sensory to the lower teeth and gums. (medscape.com)
- The motor branch to the mylohyoid is given off before the nerve enters the mandibular canal and serves as motor supply to the mylohyoid muscle. (medscape.com)
- The CBCT images of 30 randomly selected patients (mean age 15.5 years, 19 females and 11 males) were segmented regarding the mandibular bone and the IAN canal. (em-consulte.com)
- It has been described as a persistent neuropathic pain that may be initiated after the deafferentiation of trigeminal nerve fibers following a root canal treatment, an apicoectomy, or a tooth extraction, or it may be of idiopathic origin [ 1 ]. (hindawi.com)
- This nerve supplies the external acoustic meatus (ear canal), auricle (what people usually call the ear), external part of the tympanic membrane (eardrum), and the temporal skin, which is on the sides of the head. (healthline.com)
- The chorda tympani is a nerve that branches from the facial nerve (cranial nerve VII) inside the facial canal , just before the facial nerve exits the skull via the stylomastoid foramen . (wikidoc.org)
- leads into mandibular canal 7. (slideshare.net)
- Class IV BMCs were identified of the mandibular canal. (who.int)
- five were in fid mandibular canal (BMC). (who.int)
Anesthesia4
- Budenz AW, Osterman SR. A review of mandibular anesthesia nerve block techniques. (medscape.com)
- The "ART" mandibular nerve block: a new approach to accomplishing regional anesthesia. (medscape.com)
- We report a case of complete facial nerve palsy during a mandibular nerve block anesthesia in a 63-year-old woman. (bvsalud.org)
- In a study of 12 C57/BL strain mice under inhalation anesthesia, we collected images of the mandibular condyle at 6 weeks after birth and then every 5 weeks from 10 to 25 weeks after birth. (go.jp)
Branches10
- After giving off 2 branches, the mandibular nerve bifurcates into anterior and posterior divisions (see the image below). (medscape.com)
- It divides into 2 branches, which are the nerves to the tensor tympani and the tensor veli palatini. (medscape.com)
- Furthermore, major nerves in the head and neck region like the trigeminal nerve have additional nerve branches that connect to and provide sensation to the lower teeth. (cdhp.org)
- The nervus spinosus divides off the mandibular division just below the foramen ovale and just before it branches into anterior and posterior divisions . (radiopaedia.org)
- However, appropriate techniques for anesthetizing branches of the mandibular and maxillary nerves have not been described for. (awionline.org)
- Several articular branches are also carried with the nerve, which supply blood to the temporomandibular joints (TMJ). (healthline.com)
- The auriculotemporal nerve is the primary nerve to supply the TMJ, together with the masseteric nerve branches and the deep temporal. (healthline.com)
- The ilioinguinal nerve branches off the first lumbar nerve, which is near the lower back. (healthline.com)
- In the upper arm and near the shoulder, the median nerve branches off of the brachial plexus. (healthline.com)
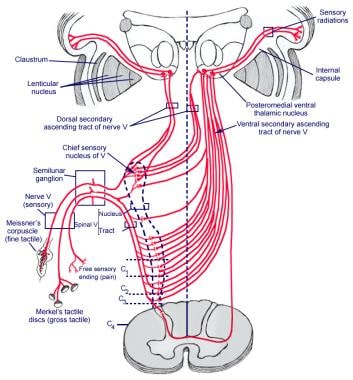
- The fibers of the mandibular division of the trigeminal nerve include sensory branches that transmit impulses from the skin of the jaw, the lower teeth, the lower gum, and the lower lip. (innerbody.com)
Anterior9
- The nerve then divides into a small anterior division and a large posterior division. (wikipedia.org)
- Sensory nerves from the anterior division include the buccal nerve, which is sensory to the mucosa of the mouth and gums and the skin on the cheek. (medscape.com)
- The mandibular region lies anterior to the masseter and inferior to the lower lip . (medscape.com)
- The anterior half is supplied by the middle meningeal nerve from the maxillary division of the trigeminal nerve. (radiopaedia.org)
- Rather than leave the skull with the facial nerve, the chorda tympani travels through the middle ear , where it runs from posterior to anterior across the tympanic membrane . (wikidoc.org)
- Special sensory (taste) fibers also extend from the chorda tympani to the anterior 2/3rds of the tongue via the lingual nerve. (wikidoc.org)
- Lingula: projection anterior to mandibular foramen 8. (slideshare.net)
- Learn to identify anterior loops of the mental foramen/nerve. (resnikimplantinstitute.com)
- A nerve block of the mental nerve anesthetizes the ipsilateral lower lip and skin of the chin, as well as the lateral (buccal) gingiva and mucosa anterior to the mental foramen up to the midline. (msdmanuals.com)
Canals2
- Some of the AI features of this software integration include 3D X-ray landmark detection, tooth-centric workflows, correction of patient positioning, and annotation of mandibular nerve canals. (ktsm.com)
- eral bifid canals that extend to the servers and the classification proposed mandibular third molar area or the by Langlias et al. (who.int)
Tensor veli pal1
- better source needed] The mandibular nerve immediately passes between tensor veli palatini, which is medial, and lateral pterygoid, which is lateral, and gives off a meningeal branch (nervus spinosus) and the nerve to medial pterygoid from its medial side. (wikipedia.org)
Nervus spinosus1
- The nervus spinosus (plural: nervi spinosi), also known as the meningeal branch of the mandibular nerve , is a branch of the mandibular division of the trigeminal nerve which innervates the dura of the middle cranial fossa . (radiopaedia.org)
Cervical1
- Many of the children developed severe infections with clinical diagnoses such as cervical lymphadenitis and mandibular or maxillary osteomyelitis, and required hospitalization, treatments such as intravenous antibiotics, and surgical procedures. (cdc.gov)
Divides1
- Additionally, the facial nerve divides into smaller nerves that reach into the face, neck, salivary glands and the outer ear. (innerbody.com)
Trigeminal ganglion3
- The large sensory root of mandibular nerve emerges from the lateral part of the trigeminal ganglion and exits the cranial cavity through the foramen ovale. (wikipedia.org)
- The motor root (Latin: radix motoria s. portio minor), the small motor root of the trigeminal nerve, passes under the trigeminal ganglion and through the foramen ovale to unite with the sensory root just outside the skull. (wikipedia.org)
- The mandibular nerve is the largest division of the trigeminal nerve, with sensory roots from the trigeminal ganglion and motor roots from the pons and the medulla. (medscape.com)
Branch4
- The nerve to the medial pterygoid is a motor branch that innervates the medial pterygoid muscle. (medscape.com)
- Chorda tympani is a branch of the facial nerve (the seventh cranial nerve) that serves the taste buds in the front of the tongue , runs through the middle ear , and carries taste messages to the brain. (wikidoc.org)
- It soon combines with the larger lingual nerve , a branch of the mandibular nerve (cranial nerve V 3 ). (wikidoc.org)
- Pterygoid branch of Trigeminal nerve. (intelligentdental.com)
Sensory3
- It then exits via the mental foramen as the mental and incisive nerves, which are sensory to the chin and the lower teeth. (medscape.com)
- These sensory modifications were located intraoral on the site of the treated tooth, suggesting a disturbance of the central processing or craniofacial information carried by the trigeminal nerve [ 9 ]. (hindawi.com)
- The sensory nerves of the mouth descend from both the trigeminal nerve and more prominently from the facial nerve. (innerbody.com)
Facial nerve6
- Facial nerve palsy has many etiologies, such as viruses, facial trauma, iatrogenesis, tumors, idiopathic conditions, cerebral infarction and pseudobulbar palsy, as a result of which it is rarely observed during dental treatment. (bvsalud.org)
- We monitored facial nerve conduction in infants with RS undergoing MDO from 2019 to 2022 in our tertiary care institution, using electroneuronography (ENoG). (nesps.org)
- This technique involves electrical stimulation of the facial nerve (FN) near the stylomastoid foramen and subsequent measurement of the motoric response, recorded at the orbicularis oculi and mentalis muscles. (nesps.org)
- Real-time facial nerve intraoperative monitoring may be a useful tool that protects the MMN. (nesps.org)
- The course and connections of the facial nerve in the temporal bone. (wikidoc.org)
- Complications from their infections included permanent tooth loss, hearing loss, facial nerve palsy, and incision fibrosis. (cdc.gov)
Bone4
- There is less dense bone, nerve tissue, and other biological material protecting the bottom tooth roots compared to the upper tooth roots. (cdhp.org)
- The nerve continues to course between the squamous and petrous parts of the temporal bone , entering and supplying the mastoid antrum and the mastoid air cells . (radiopaedia.org)
- When the mandibular bone disappears, the mandibular nerve moves closer to the jawbone. (achance2talk.com)
- 8 Cranial and facial Bones Mandibular bone 1. (slideshare.net)
Local anesthetic1
- A nerve block is used instead of local anesthetic infiltration when accurate approximation of wound edges is important (eg, skin or lip repair), because a nerve block does not distort the tissue as does local infiltration. (msdmanuals.com)
Chin1
- These nerve fibers innervate structures of the lower jaw and face, such as the tongue, lower lip, and chin. (wikipedia.org)
Innervates1
- The mandibular nerve also innervates the muscles of mastication. (wikipedia.org)
Fibers2
- The chorda tympani appears to exert a particularly strong inhibitory influence on other taste nerves, as well as on pain fibers in the tongue. (wikidoc.org)
- The fibers of the chorda tympani travel with the lingual nerve to the submandibular ganglion . (wikidoc.org)
Anatomical1
- A nerve block is interpreted as the anaesthetising of a substantial segment of the body innervated by a large nerve or an area supplied by a smaller nerve where the technique demands expert anatomical knowledge and a high degree of precision. (health.gov.au)
Articaine2
- Conclusions MINB and IANB with 4% articaine had similar efficacy in anesthetizing mandibular premolars with irreversible pulpitis. (drnekoofar.com)
- Clinical relevance MINB and IANB with 4% articaine can be used interchangeably to anesthetize mandibular premolars with irreversible pulpitis. (drnekoofar.com)
Meningeal1
- The two roots of this nerve surround the medial meningeal artery , and finally combine into a single nerve. (healthline.com)
Block9
- Mandibular nerve block is a safe procedure. (medscape.com)
- The mandibular nerve area is generally blocked by using more specific nerve blocks rather than by performing a complete nerve block. (medscape.com)
- The mandibular nerve block has a success rate of 95%-98%, whereas the IAN block is successful in only 65%-85% of cases. (medscape.com)
- An oral nerve block is a simple and effective way to manage orofacial pain without distorting the anatomy of a wound and without the use of narcotics. (medscape.com)
- Where anaesthesia combines a regional nerve block with general anaesthesia for an operative procedure, benefit will be paid only under the relevant anaesthesia item as set out in Group T10. (health.gov.au)
- Where a regional or field nerve block is administered by a medical practitioner other than the practitioner carrying out the operation, the block attracts benefits under the Group T10 anaesthesia item and not the block item in Group T7. (health.gov.au)
- If not stipulated in the item descriptor, when a regional nerve block or field nerve block covered by an item in Group T7 of the Schedule is administered by a medical practitioner in the course of a surgical procedure undertaken by the same medical practitioner, then such a block will attract benefit under the appropriate item in Group T7. (health.gov.au)
- If stipulated in the item descriptor, when a regional nerve block or field nerve block covered by an item in Group T7 of the Schedule is administered by a medical practitioner in the course of a surgical procedure the block will not attract benefit under the relevant item in Group T7 unless the block has been performed using a targeted percutaneous approach. (health.gov.au)
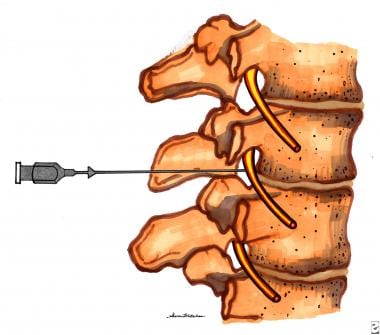
- Paravertebral nerve block item 18276 covers the provision of regional anaesthesia for surgical and related procedures for the management acute pain or of chronic pain related to radiculopathy. (health.gov.au)
Foramen ovale1
- The 2 roots exit the cranium via the foramen ovale and unite just outside the cranium to form the mandibular nerve. (medscape.com)
Vagus nerve2
- What is the Vagus Nerve? (healthline.com)
- The vagus nerve is the longest of the 12 cranial nerves. (healthline.com)
Injuries1
- Mandibular division trigeminal nerve injuries following primary endodontic treatment. (bvsalud.org)
Clinical1
- We aim to evaluate changes in nerve conduction during MDO procedures and analyze if these changes are associated with clinical findings of FND. (nesps.org)
Cranial nerve1
- The accessory nerve is a cranial nerve that controls the movement of certain neck muscles. (healthline.com)
Sphenopalatine1
- Palatal hypesthesia indicates trigeminal nerve involvement in the sphenopalatine foramen or pterygopalatine fossa extension. (medscape.com)
Emerges1
- The nerve continues through the petrotympanic fissure , after which it emerges from the skull into the infratemporal fossa . (wikidoc.org)
Glossopharyngeal1
- Gunbey HP, Kutlar G, Aslan K, Sayit AT, Incesu L. Magnetic Resonance Imaging Evidence of Varicella Zoster Virus Polyneuropathy: Involvement of the Glossopharyngeal and Vagus Nerves Associated With Ramsay Hunt Syndrome. (medscape.com)
Medial pterygoid1
- Mandibular nerve through the medial pterygoid. (intelligentdental.com)
Molar3
- Hasani A, Ahmadi Moshtaghin F, Roohi P, Rakhshan V. Diagnostic value of cone beam computed tomography and panoramic radiography in predicting mandibular nerve exposure during third molar surgery. (revistamedical.com)
- Baqain ZH, AlHadidi A, AbuKaraky A, Khader Y. Does the Use of Cone-Beam Computed Tomography Before Mandibular Third Molar Surgery Impact Treatment Planning? (revistamedical.com)
- Første molar i mandibelen er den tann hvor en oftest opplever anestesiproblem, etterfulgt av andre molar og første premolar. (tannlegetidende.no)
Dental1
- no se encontraron diferencias estadísticamente significativas en la eficacia anestésica entre la lidocaína al pulpa dental, 2% y la articaína al 4% en molares inferiores con pulpa vital. (bvsalud.org)
Phenol1
- Item 18292 may not be claimed for the injection of botulinum toxin, but may be claimed where a neurolytic agent (such as phenol) is used to treat the obturator nerve in patients receiving botulinum toxin injections under item 18354 for a dynamic foot deformity. (health.gov.au)
Artery1
- The auriculotemporal nerve originates from the back part of the mandibular nerve, which travels alongside the superficial temporal vein and artery. (healthline.com)
Lingual1
- The IAN descends into the pterygomandibular space along with the lingual nerve. (medscape.com)