Inguinal Canal
Spermatic Cord
Cryptorchidism
Hernia, Inguinal
Round Ligament
Semicircular Canals
Testis
Ear Canal
Root Canal Preparation
Root Canal Irrigants
Dental Pulp Cavity
Root Canal Filling Materials
Anal Canal
Penetrating sledding injuries to the lower torso--2 case reports. (1/173)
Sledding accidents are frequent and vary in severity. Penetrating sledding injuries are uncommon but may be devastating. Snow-racers--sleds with both steering and braking devices--may be associated with an increased rate of injury. The authors present 2 cases of lower-torso penetrating trauma associated with the use of snow-racers. Both cases involved penetration--of the perineum in one case and the inguinal area in the other--by wooden sticks. Both patients recovered fully after prompt surgical intervention. The authors suggest that the absence of a protective panel at the front of the snow-racer may result in the sledder's lower torso being more exposed to objects encountered while sledding. The injuries reported raise concerns about the safety of modern sleds and the possibility that design changes are needed. (+info)Superficial femoral eversion endarterectomy combined with a vein segment as a composite artery-vein bypass graft for infrainguinal arterial reconstruction. (2/173)
OBJECTIVE: The purpose of this study was to determine the results of composite artery-vein bypass grafting for infrainguinal arterial reconstruction. METHODS: This study was designed as a retrospective case series in two tertiary referral centers. Forty-eight of 51 patients underwent the procedure of interest for the treatment of ischemic skin lesions (n = 42), rest pain (n = 3), disabling claudication (n = 1), and infected prosthesis (n = 2). The intervention used was infrainguinal composite artery-vein bypass grafting to popliteal (n = 18) and infrapopliteal (n = 30) arteries, with an occluded segment of the superficial femoral artery prepared with eversion endarterectomy and an autogenous vein conduit harvested from greater saphenous veins (n = 43), arm veins (n = 3), and lesser saphenous veins (n = 2). The main outcome measures, primary graft patency rates, foot salvage rates, and patient survival rates, were described by means of the life-table method for a mean follow-up time of 15.5 months. RESULTS: The cumulative loss during the follow-up period was 6% and 24% at 6 and 12 months, respectively. The primary graft patency rates, the foot salvage rates, and the patient survival rates for patients with popliteal grafts were 60.0% +/- 9.07%, 75.7% +/- 9.18%, and 93.5% +/- 6.03%, respectively, at 1 month; 53.7% +/- 11.85%, 68.9% +/- 12.47%, and 85. 0% +/- 9.92% at 1 year; and 46.7% +/- 18.19%, 68.9% +/- 20.54%, and 53.1% +/- 17.15% at 5 years. For infrapopliteal grafts, the corresponding estimates were 72.4% +/- 7.06%, 72.9% +/- 6.99%, and 92.7% +/- 4.79% at 1 month; 55.6% +/- 10.70%, 55.4% +/- 10.07%, and 77.9% +/- 9.02% at 1 year; and 33.6% +/- 22.36%, 55.4% +/- 30.20%, and 20.8% +/- 9.89% at 5 years. CONCLUSION: The composite artery-vein bypass graft is a useful autogenous alternative for infrainguinal arterial reconstruction when a vein of the required quality is not available or when the procedure needs to be confined to the affected limb. (+info)Access to occluded infrainguinal bypass grafts with a loopsnare. (3/173)
Thrombolysis for the treatment of occluded bypass grafts is used in selected clinical circumstances. Unfortunately, a minority of these procedures are technical failures because of the inability to access the occluded graft. We describe a technique that greatly increases the chances of technical success. (+info)Experimental study of lymph node auto-transplantation in rats. (4/173)
OBJECTIVE: To observe the restoration of structure and function of auto-transplanted lymph nodes. METHODS: Inguinal lymph nodes in Spregue-Dawley (SD) rats were auto-transplanted by free implantation, or with an intact vascular pedicle, or by free transplantation with microvascular anastomosis, to the popliteal fossa where lymph nodes were removed. The observation methods included emission computerized tomographic (ECT) scanning, staining of China ink and methylthionine chloride to observe the histological changes. RESULTS: After four weeks, these vascularized nodes showed normal histological appearances and spontaneously reestablished afferent and efferent lymphatic reconnection with the surrounding lymphatic vessels. ECT lymphoscintigraphy with 99mTc-Dx showed that vascularized lymph nodes had restored their normal function. CONCLUSION: Vascularized lymph node transplantation is a useful method for draining extremity lymph edema. (+info)The myth of the in situ graft: superiority in infrainguinal bypass surgery? (5/173)
OBJECTIVES: to compare the clinical outcome of in situ and reversed bypass grafting. DESIGN: multicentre, prospective, non-randomised study. PATIENTS AND METHODS: five-hundred patients with an in situ graft and 955 patients with a reversed graft were compared regarding graft occlusion, the need for graft revision, and limb salvage. RESULTS: two-year assisted primary patency of femoropopliteal bypass procedures was 82% for in situ and 82% for reversed grafts. The corresponding hazard ratio (HR) for occlusion was 1.27 (95% CI 0. 91-1.77). The 2-year assisted primary patency of femorocrural bypass procedures was 69% for in situ vs. 70% for reversed grafts. The corresponding HR was 1.13 (95% CI 0.73-1.75). Adjustment for relevant baseline variables did not change the results. More reinterventions were needed to maintain integrity and patency of the in situ graft especially in crural bypasses. No differences in limb salvage rates were seen. CONCLUSIONS: reversed and in situ vein grafts have similar patency and limb salvage rates for both femoropopliteal and femorocrural bypass procedures. The in situ graft needs more secondary interventions. (+info)A new method of intraoperative hydraulic impedance measurement provides valuable prognostic information about infrainguinal graft patency. (6/173)
PURPOSE: Prognostic information about graft outcome, obtained by using a new method for intraoperative measurement of vascular impedance, was evaluated. METHODS: Hydraulic impedance was measured in 136 infrainguinal bypass grafts that were entered into a multicenter trial. Seventy femoropopliteal and 66 femorocrural polytetrafluoroethylene (PTFE) grafts were used. The arterial impedance measurement involved a silicon bypass graft temporarily inserted between the proximal and distal anastomoses sites. A flowmeter probe and a pressure transducer were incorporated into the tube. The digitally stored waveforms were subjected to a fast Fourier transformation and both input (Z(x)) and characteristic (Z(0)) impedances, as well as phase relations, were computed and related to graft outcome after 3 years. RESULTS: Significant prognostic information for both popliteal and crural grafts was provided by means of the phase angle of the first harmonic. Primary and secondary patency rates for popliteal bypasses were 45% +/- 1% and 65% +/- 2% for phase angles greater than -40 degrees (n = 57) and 37% +/- 1% and 40% +/- 1% for phase angles less than -40 degrees (n = 13, p(prim ) = not significant, p(sec) < 0.01). For crural grafts, the secondary patency rates were 49% +/- 1% and 61% +/- 2% for phase angles greater than -40 degrees (n = 53) and 15% +/- 1% and 0% for phase angles less than -40 degrees (n = 13, P <.01). All crural bypass grafts with phase angles less than -40 degrees occluded within 16 months. Steady flow resistance, as well as Z(x) and Z(0), failed to indicate a significant relation to graft prognosis. CONCLUSION: This method provides reliable prognostic information regarding graft patency and opens hydraulic impedance measurement to clinical surgery. The phase lag between flow and pressure curves, as expressed by the phase angle of the first harmonic, provides significant prognostic information. (+info)Impact of race on the treatment for peripheral arterial occlusive disease. (7/173)
PURPOSE: The purpose of this study was to determine the impact of race on the treatment of peripheral artery occlusive disease (PAOD) and to examine the role of access to care and disease distribution on the observed racial disparity. METHODS: The study was performed as a retrospective analysis of hospital discharge abstracts from 1992 to 1995 in 202 non-federal, acute-care hospitals in the state of Florida. The subjects were patients older than 44 years of age who underwent major lower extremity amputation or revascularization (bypass grafting or angioplasty) for PAOD. The main outcome measures were incidence of intervention, incidence per demographic group, multivariate predictors of amputation versus revascularization, multivariate predictors of amputation versus revascularization among those patients with access to sophisticated care (hospital with arteriographic capabilities), and multivariate predictors of surgical bypass graft type (aortoiliac vs infrainguinal). RESULTS: A total of 51,819 procedures (9.1 per 10,000 population) were performed for PAOD during the study period and included 15,579 major lower extremity amputations (30.1%) and 36,240 revascularizations (69.9%). Although the incidence of a procedure for PAOD was comparable between African Americans and whites (9.0 vs 9.6 per 10, 000 demographic group), the incidence of amputation (5.0 vs 2.5 per 10,000 demographic group) was higher and the incidence of revascularization (4.0 vs 7.1 per 10,000 demographic group) was lower among African Americans. Furthermore, multivariate analysis results showed that African Americans (odds ratio, 3.79; 95% confidence interval [CI], 3.34 to 4.30) were significantly more likely than whites to undergo amputation as opposed to revascularization. The secondary multivariate analyses results revealed that African Americans (odds ratio, 2.29; 95% CI, 1.58 to 3. 33) were more likely to undergo amputation among those patients (n = 9193) who underwent arteriography during the procedural admission and to undergo infrainguinal bypass grafting (odds ratio, 2.00; 95% CI, 1.48 to 2.71) among those patients (n = 27,796) who underwent surgical bypass grafting. CONCLUSION: There is a marked racial disparity in the treatment of patients with PAOD that may be caused in part by differences in the severity of disease or disease distribution. (+info)Potential predictors of outcome in patients with tissue loss who undergo infrainguinal vein bypass grafting. (8/173)
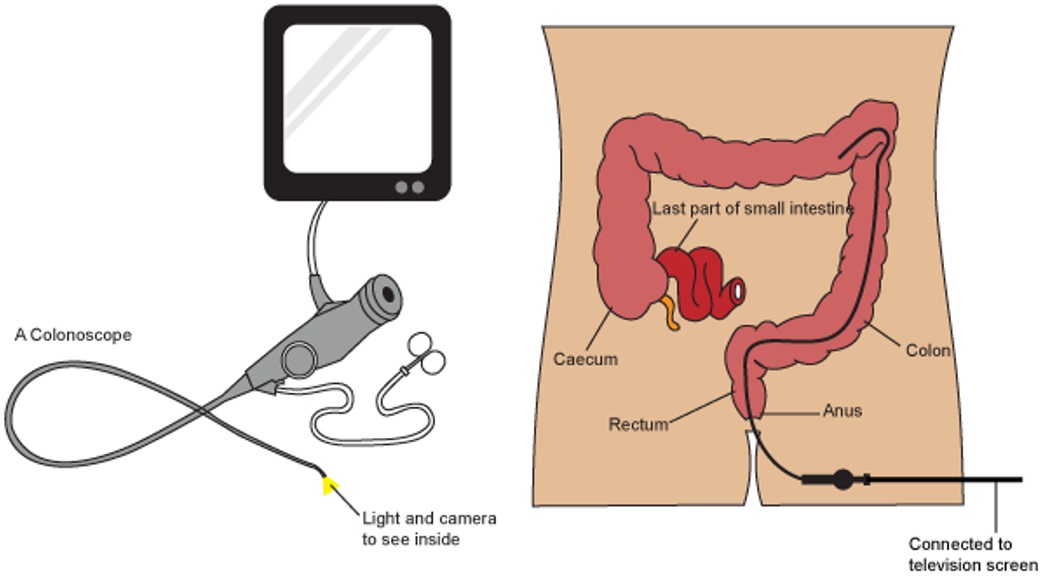
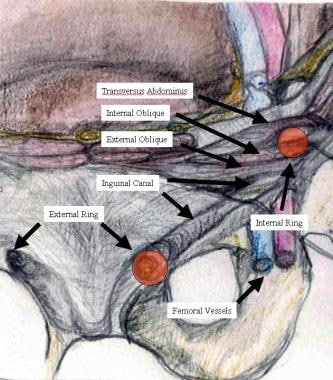
PURPOSE: Aggressive attempts at limb salvage in patients with ischemic tissue loss are justified by favorable initial results in most patients. The identification of patients whose conditions will not benefit from attempted revascularization remains difficult. METHODS: This study was designed as a retrospective review of prospectively collected clinical data. The subjects were 210 consecutive patients who underwent infrainguinal vein bypass grafting for ischemic tissue loss in the setting of an academic medical center. Bypass grafting was to the popliteal artery in 56 patients, to the infrapopliteal arteries in 131 patients, and to the pedal arteries in 23 patients. The follow-up examination was complete in 209 of 210 patients. One hundred twenty-five patients underwent blinded review of duplex scan venous mapping and arteriography to determine simplified vein and run-off scores. The outcome measures were the influence of risk factors, venous conduit, and runoff on mortality, limb loss, and graft failure at the 6-month follow-up examination. RESULTS: One hundred seventy patients (81%) were alive and had limb salvage. Nineteen patients (9.1%) died, with need for a simultaneous inflow procedure and end-stage renal disease being most commonly associated with mortality. Thirty-three patients (15.8%) had undergone amputation: 18 after graft failure, and 15 for progressive tissue loss despite a patent graft. Amputation was significantly more common in patients with diabetes (P =.05) and with poor runoff scores (poor runoff, 44.4% vs good runoff, 7.4%; P <.01). Amputation despite a patent graft also correlated with runoff (poor runoff, 41.7% vs good runoff, 4.3%; P <.01). Twenty-five patients had graft failure without amputation, so that only 145 patients (69.4%) were alive, had limb salvage, and had a patent graft. Run-off score was the strongest predictor of outcome, with 70% of patients with poor run-off scores having death, amputation, or graft failure. CONCLUSION: Aggressive use of infrainguinal vein bypass grafting in patients with ischemic tissue loss results in a high rate of initial limb salvage but significant morbidity and mortality. Arteriographically determined runoff scores appear to potentially identify patients at high risk for a poor initial outcome and may provide a method of selecting patients for primary amputation. (+info)The inguinal canal is a narrow passage in the lower abdominal wall. In males, it allows for the spermatic cord and blood vessels to travel from the abdomen to the scrotum. In females, it provides a pathway for the round ligament of the uterus to pass through. The inguinal canal is located in the groin region, and an inguinal hernia occurs when a portion of the intestine protrudes through this canal.
The spermatic cord is a fibrous structure that contains the vas deferens, blood vessels, nerves, and lymphatics, which provide passage for these structures between the abdomen and the scrotum in males. It is covered by several layers of protective sheaths, including the internal spermatic fascia, cremasteric fascia, and external spermatic fascia. The spermatic cord allows the testicles to be located outside the body, which helps maintain a cooler temperature for optimal sperm production.
Cryptorchidism is a medical condition in which one or both of a male infant's testicles fail to descend from the abdomen into the scrotum before birth or within the first year of life. Normally, the testicles descend from the abdomen into the scrotum during fetal development in the second trimester. If the testicles do not descend on their own, medical intervention may be necessary to correct the condition.
Cryptorchidism is a common birth defect, affecting about 3-5% of full-term and 30% of preterm male infants. In most cases, the testicle will descend on its own within the first six months of life. If it does not, treatment may be necessary to prevent complications such as infertility, testicular cancer, and inguinal hernia.
Treatment for cryptorchidism typically involves surgery to bring the testicle down into the scrotum. This procedure is called orchiopexy and is usually performed before the age of 2. In some cases, hormonal therapy may be used as an alternative to surgery. However, this approach has limited success and is generally only recommended in certain situations.
Overall, cryptorchidism is a treatable condition that can help prevent future health problems if addressed early on. Regular check-ups with a pediatrician or healthcare provider can help ensure timely diagnosis and treatment of this condition.
Inguinal hernia, also known as an inguinal rupture or groin hernia, is a protrusion of abdominal-cavity contents through the inguinal canal. The inguinal canal is a passage in the lower abdominal wall that carries the spermatic cord in males and a round ligament in females. Inguinal hernias are more common in men than women.
There are two types of inguinal hernias: direct and indirect. Direct inguinal hernias occur when the abdominal lining and/or fat push through a weakened area in the lower abdominal wall, while indirect inguinal hernias result from a congenital condition where the abdominal lining and/or fat protrude through the internal inguinal ring, a normal opening in the abdominal wall.
Inguinal hernias can cause discomfort or pain, especially during physical activities, coughing, sneezing, or straining. In some cases, incarceration or strangulation of the hernia may occur, leading to serious complications such as bowel obstruction or tissue necrosis, which require immediate medical attention.
Surgical repair is the standard treatment for inguinal hernias, and it can be performed through open or laparoscopic techniques. The goal of surgery is to return the protruding tissues to their proper position and strengthen the weakened abdominal wall with sutures or mesh reinforcement.
Papillary cystadenoma is a type of benign (non-cancerous) tumor that arises from the glandular cells in various organs. It is characterized by the growth of finger-like projections (papillae) inside the cysts. These tumors can occur in different parts of the body, including the ovaries, pancreas, and the lining of the abdominal cavity (peritoneum).
In general, papillary cystadenomas are slow-growing and do not typically spread to other organs. However, they can cause symptoms such as pain or discomfort if they become large enough to press on surrounding tissues. Treatment usually involves surgical removal of the tumor. It is important to note that while papillary cystadenomas are generally benign, there is a small risk that they may undergo malignant transformation and develop into cancerous tumors over time. Regular follow-up with a healthcare provider is recommended to monitor for any changes in the tumor or the development of new symptoms.
The round ligament is a cord-like structure in the female pelvis that extends from the uterus to the labia majora. It is one of the major ligaments that support the uterus and helps to maintain its position within the pelvis. The round ligament is composed of fibrous tissue and smooth muscle, and it plays a role in maintaining the tone and shape of the uterus.
During pregnancy, the round ligament can become stretched and thickened as the uterus grows and expands. This can sometimes cause discomfort or pain, particularly on one side of the pelvis. In some cases, the round ligament may also contribute to the development of certain gynecological conditions, such as uterine prolapse or urinary incontinence.
It is important for healthcare providers to consider the round ligament when evaluating and treating female reproductive health issues, as it can have a significant impact on the function and positioning of the uterus and other pelvic organs.
The semicircular canals are part of the vestibular system in the inner ear that contributes to the sense of balance and spatial orientation. They are composed of three fluid-filled tubes, each located in a different plane (anterior, posterior, and horizontal) and arranged at approximately right angles to each other. The semicircular canals detect rotational movements of the head, enabling us to maintain our equilibrium during movement.
When the head moves, the fluid within the semicircular canals moves in response to that motion. At the end of each canal is a structure called the ampulla, which contains hair cells with hair-like projections (stereocilia) embedded in a gelatinous substance. As the fluid moves, it bends the stereocilia, stimulating the hair cells and sending signals to the brain via the vestibular nerve. The brain then interprets these signals to determine the direction and speed of head movement, allowing us to maintain our balance and orientation in space.
The testis, also known as the testicle, is a male reproductive organ that is part of the endocrine system. It is located in the scrotum, outside of the abdominal cavity. The main function of the testis is to produce sperm and testosterone, the primary male sex hormone.
The testis is composed of many tiny tubules called seminiferous tubules, where sperm are produced. These tubules are surrounded by a network of blood vessels, nerves, and supportive tissues. The sperm then travel through a series of ducts to the epididymis, where they mature and become capable of fertilization.
Testosterone is produced in the Leydig cells, which are located in the interstitial tissue between the seminiferous tubules. Testosterone plays a crucial role in the development and maintenance of male secondary sexual characteristics, such as facial hair, deep voice, and muscle mass. It also supports sperm production and sexual function.
Abnormalities in testicular function can lead to infertility, hormonal imbalances, and other health problems. Regular self-examinations and medical check-ups are recommended for early detection and treatment of any potential issues.
The ear canal, also known as the external auditory canal, is the tubular passage that extends from the outer ear (pinna) to the eardrum (tympanic membrane). It is lined with skin and tiny hairs, and is responsible for conducting sound waves from the outside environment to the middle and inner ear. The ear canal is typically about 2.5 cm long in adults and has a self-cleaning mechanism that helps to keep it free of debris and wax.
The spinal canal is the bony, protective channel within the vertebral column that contains and houses the spinal cord. It extends from the foramen magnum at the base of the skull to the sacrum, where the spinal cord ends and forms the cauda equina. The spinal canal is formed by a series of vertebral bodies stacked on top of each other, intervertebral discs in between them, and the laminae and spinous processes that form the posterior elements of the vertebrae. The spinal canal provides protection to the spinal cord from external trauma and contains cerebrospinal fluid (CSF) that circulates around the cord, providing nutrients and cushioning. Any narrowing or compression of the spinal canal, known as spinal stenosis, can cause various neurological symptoms due to pressure on the spinal cord or nerve roots.
Root canal preparation is a procedure in endodontics, which is the branch of dentistry dealing with the dental pulp and tissues surrounding the root of a tooth. The goal of root canal preparation is to thoroughly clean, shape, and disinfect the root canal system of an infected or damaged tooth, in order to prepare it for a filling material that will seal and protect the tooth from further infection or damage.
The procedure involves the use of specialized dental instruments, such as files and reamers, to remove the infected or necrotic pulp tissue and debris from within the root canal. The root canal is then shaped using progressively larger files to create a tapering preparation that facilitates the placement of the filling material. Irrigation solutions are used to help flush out any remaining debris and disinfect the canal.
The success of root canal preparation depends on several factors, including the thoroughness of cleaning and shaping, the effectiveness of disinfection, and the sealing ability of the filling material. Properly performed, root canal preparation can alleviate pain, save a tooth from extraction, and restore function and aesthetics to the mouth.
Root canal irrigants are substances used during root canal treatment to clean, disinfect and rinse the root canal system. The main goal is to remove tissue remnants, dentinal debris, and microorganisms from the root canal space, thus reducing the risk of reinfection and promoting healing. Commonly used irrigants include sodium hypochlorite (NaOCl), which is a potent antimicrobial agent, and ethylenediaminetetraacetic acid (EDTA), which is used to remove the smear layer and improve the penetration of other irrigants and root canal sealers. The choice of irrigant, concentration, and application technique may vary depending on the specific case and clinician's preference.
The dental pulp cavity, also known as the pulp chamber, is the innermost part of a tooth that contains the dental pulp. It is located in the crown portion of the tooth and is shaped like an upside-down pyramid with the narrow end point towards the root of the tooth.
The dental pulp is a soft tissue that contains nerves, blood vessels, and connective tissue. It plays an important role in the development and maintenance of the tooth, including providing nutrients to the dentin and producing reparative dentin.
The dental pulp cavity can become infected or inflamed due to tooth decay, trauma, or other factors, leading to symptoms such as pain, sensitivity, and swelling. In such cases, treatment options may include root canal therapy, which involves removing the infected or inflamed pulp tissue from the dental pulp cavity and sealing the space to prevent further infection.
Root canal filling materials are substances used to fill and seal the root canal system inside a tooth following root canal treatment. The main goal of using these materials is to prevent reinfection, provide structural support to the weakened tooth, and restore its functionality.
Commonly used root canal filling materials include:
1. Gutta-percha: A rubber-like material derived from the sap of the Palaquium gutta tree. It is widely used as the primary filling material due to its biocompatibility, malleability, and ability to be compacted into the root canal space. Gutta-percha points or cones are typically used in conjunction with a sealer for optimal adaptation and seal.
2. Sealers: These are adhesive materials that help bond gutta-percha to dentin walls and improve the seal between the filling material and root canal walls. Some commonly used sealers include zinc oxide eugenol, calcium hydroxide-based sealers, and resin-based sealers.
3. Silver points: These are silver cones with a sharp tip that can be inserted into the root canal space as an alternative to gutta-percha. However, their use has declined due to concerns about corrosion and potential tooth discoloration.
4. Mineral trioxide aggregate (MTA): A biocompatible cement composed primarily of Portland cement, bismuth oxide, and other additives. MTA is used for various applications in endodontics, including root-end filling, perforation repair, and apexification. It has excellent sealing ability, antibacterial properties, and promotes hard tissue formation.
5. Bioceramics: These are advanced materials with similar properties to MTA but with improved handling characteristics and setting times. They include materials like Bioaggregate, EndoSequence BC Sealer, and iRoot SP.
6. Thermoplasticized gutta-percha: This technique involves heating and softening gutta-percha using a specialized device called a thermomechanical compactor or an oven. The softened gutta-percha is then injected into the root canal space, providing better adaptation to the root canal walls and creating a more uniform seal.
The choice of materials depends on various factors, including the clinical situation, patient's needs, and practitioner's preference.
The anal canal is the terminal portion of the digestive tract, located between the rectum and the anus. It is a short tube-like structure that is about 1 to 1.5 inches long in adults. The main function of the anal canal is to provide a seal for the elimination of feces from the body while also preventing the leakage of intestinal contents.
The inner lining of the anal canal is called the mucosa, which is kept moist by the production of mucus. The walls of the anal canal contain specialized muscles that help control the passage of stool during bowel movements. These muscles include the internal and external sphincters, which work together to maintain continence and allow for the voluntary release of feces.
The anal canal is an important part of the digestive system and plays a critical role in maintaining bowel function and overall health.
The tooth apex is the tip or the narrowed end of the root of a tooth. It is the portion that is located deepest within the jawbone and it contains dental pulp tissue, which includes nerves and blood vessels. The apex plays an essential role in the development and maintenance of a tooth, as well as in the process of root canal treatment, where instruments and materials are introduced through it to clean and fill the root canals. It is also a crucial landmark in endodontic surgery and dental imaging.
 Inguinal canal
Inguinal canal Inguinal Canal (definition)
Inguinal Canal (definition) Flashcards - Inguinal Canal, Scrotum, & Testis
Flashcards - Inguinal Canal, Scrotum, & Testis American Sign Language ASL Video Dictionary - inguinal canal
American Sign Language ASL Video Dictionary - inguinal canal Testicular Masses | AAFP
Testicular Masses | AAFP Inguinal Region Anatomy: Overview, Gross Anatomy, Pathophysiological Variants
Inguinal Region Anatomy: Overview, Gross Anatomy, Pathophysiological Variants Inguinal ligament
Inguinal ligament Groin hernia (or inguinal hernia)</span><i class="icon" aria-hidden=...
Groin hernia (or inguinal hernia)</span><i class="icon" aria-hidden=... Make the Diagnosis: Why Did This Toddler Stop Walking? - Medpage Today
Make the Diagnosis: Why Did This Toddler Stop Walking? - Medpage Today Digestive tract with an inset showing an indirect inguinal hernia in a male, with labels - Media Asset - NIDDK
Digestive tract with an inset showing an indirect inguinal hernia in a male, with labels - Media Asset - NIDDK Inguinal Hernias (for Parents) - CareSource
Inguinal Hernias (for Parents) - CareSource Giedrius Salkus - Fingerprint
- Aalborg University's Research Portal
Giedrius Salkus - Fingerprint
- Aalborg University's Research Portal female reproductive system - Ontology Report - Rat Genome Database
female reproductive system - Ontology Report - Rat Genome Database Advanced Search Results - Public Health Image Library(PHIL)
Advanced Search Results - Public Health Image Library(PHIL) Undescended Testis | Symptoms, Diagnosis & Treatment
Undescended Testis | Symptoms, Diagnosis & Treatment The inguinal release procedure for groin pain: initial experience in 73 sportsmen/women | British Journal of Sports Medicine
The inguinal release procedure for groin pain: initial experience in 73 sportsmen/women | British Journal of Sports Medicine 2019 Salon Winners
2019 Salon Winners Hydrocele Formation
Hydrocele Formation Cryptorchidism (Undescended Testicles) in Horses - American College of Veterinary Surgeons
Cryptorchidism (Undescended Testicles) in Horses - American College of Veterinary Surgeons The Girl's Guide to Tucking Your Dick
The Girl's Guide to Tucking Your Dick Healthcare | Free Full-Text | Physiotherapy Screening for Referral of a Patient with Peripheral Arterial Disease Masquerading...
Healthcare | Free Full-Text | Physiotherapy Screening for Referral of a Patient with Peripheral Arterial Disease Masquerading...