Inappropriate ADH Syndrome
Water Intoxication
Myelinolysis, Central Pontine
Receptors, Vasopressin
Sodium
Demeclocycline
Saline Solution, Hypertonic
Vasopressins
Water-Electrolyte Balance
Confusion
Adrenal Insufficiency
Deamino Arginine Vasopressin
Hypovolemia
Empty Sella Syndrome
Arginine Vasopressin
Myxedema
Antidiuretic Agents
Hypopituitarism
Azotemia
Osmolar Concentration
Hyperkalemia
Fluid Therapy
Demyelinating Diseases
Polydipsia, Psychogenic
Kluver-Bucy Syndrome
Renal Agents
Neurophysins
Chlorpropamide
Acute and chronic dose-response relationships for angiotensin, aldosterone, and arterial pressure at varying levels of sodium intake. (1/614)
We examined the acute and chronic dose-response relationships between intravenously infused angiotensin II (A II) and the resulting changes in arterial pressure and plasma aldosterone concentration at varying levels of sodium intake. Sequential analysis of plasma aldosterone at each A II infusion rate resulted in an acute dose-related increase in plasma aldosterone which was markedly attenuated after the first 24 hours of infusion, the final level being directly related to the dose of A II and inversely related to sodium intake. A II infused at 5,15, and 23 ng/kg per min was associated with an initial increase (2nd to 8th hour) in plasma aldosterone to 2,6, and 9 times control values, respectively, in dogs receiving 40 mEq Na+/day. But, after the 1st day, aldosterone averaged only 1, 1.7, and 3 times control values for the next 2 weeks at the same rates of A II infusion. Dogs receiving 120 mEq Na+/day during A II infusion exhibited only a transient increase in plasma aldosterone during the 1st day. Sustained hypertension developed over a period of a week at all doses of A II at normal and high sodium intake, but did not occur at any dose of A II in sodium-depleted dogs. Increasing sodium intake from 40 to 120 mEq/day resulted in higher levels of hypertension, 125% compared to 140% of ocntrol values for dogs infused with A II, 5.0 ng/kg per min. We conclude that primary angiotensin-induced hypertension need not be associated with increased levels of plasma aldosterone, which appears to remain elevated only with amounts of A II greater than those required to sustain a significant degree of hypertension. (+info)Central peptidergic neurons are hyperactive during collateral sprouting and inhibition of activity suppresses sprouting. (2/614)
Little is known regarding the effect of chronic changes in neuronal activity on the extent of collateral sprouting by identified CNS neurons. We have investigated the relationship between activity and sprouting in oxytocin (OT) and vasopressin (VP) neurons of the hypothalamic magnocellular neurosecretory system (MNS). Uninjured MNS neurons undergo a robust collateral-sprouting response that restores the axon population of the neural lobe (NL) after a lesion of the contralateral MNS (). Simultaneously, lesioned rats develop chronic urinary hyperosmolality indicative of heightened neurosecretory activity. We therefore tested the hypothesis that sprouting MNS neurons are hyperactive by measuring changes in cell and nuclear diameters, OT and VP mRNA pools, and axonal cytochrome oxidase activity (COX). Each of these measures was significantly elevated during the period of most rapid axonal growth between 1 and 4 weeks after the lesion, confirming that both OT and VP neurons are hyperactive while undergoing collateral sprouting. In a second study the hypothesis that chronic inhibition of neuronal activity would interfere with the sprouting response was tested. Chronic hyponatremia (CH) was induced 3 d before the hypothalamic lesion and sustained for 4 weeks to suppress neurosecretory activity. CH abolished the lesion-induced increases in OT and VP mRNA pools and virtually eliminated measurable COX activity in MNS terminals. Counts of the total number of axon profiles in the NL revealed that CH also prevented axonal sprouting from occurring. These results are consistent with the hypothesis that increased neuronal activity is required for denervation-induced collateral sprouting to occur in the MNS. (+info)Drug-induced hyponatraemia in psychogenic polydipsia. (3/614)
Two patients with psychogenic polydipsia developed hyponatraemia, one in association with administration of hydrochlorothiazide and the other with that of tolbutamide. It is suggested that the increased fluid intake in such patients may make them more susceptible to the development of hyponatraemia from thiazide or sulphonylurea compounds. (+info)Incidence and risk factors for hyponatraemia following treatment with fluoxetine or paroxetine in elderly people. (4/614)
AIMS: To establish the incidence, time course and risk factors of hyponatraemia complicating treatment with fluoxetine or paroxetine in an elderly population. METHODS: Retrospective descriptive and case control study in an inpatient/outpatient assessment and rehabilitation service for people aged 65 years and over. Fourteen elderly patients with hyponatraemia complicating treatment with fluoxetine or paroxetine, matched with 56 controls drawn from 845 patients treated with fluoxetine or paroxetine over 3.5 years. No other SSRI antidepressants were used over the study period. RESULTS: The incidence of hyponatraemia was 4.7/1000 people treated/year (6.3/1000 for fluoxetine and 3.5/1000 for paroxetine). Hyponatraemia was detected at a median 13.5 (mean 18.6, range 4-64) days after commencing the drug. Mean (95% confidence intervals) body weights were lower in cases at 53.0 (95% CI 46.5-59.5) kg compared with controls at 64.5 (95% CI 60.1-68.4) kg (P<0.01). 71% of cases were women compared with 45% of controls (P=0.07) but the effect of gender was confounded by body weight. There were trends for cases to be older (odds ratio 1.10: 95% CI 0.99, 1.23) and lighter (odds ratio 0.92, 95% CI 0.86, 0.99). CONCLUSIONS: Approximately 1 in 200 elderly people treated per year with fluoxetine or paroxetine developed complicating hyponatraemia. Low body weight was a particular risk factor. Most cases occurred within 3 weeks of treatment. (+info)Hyponatremic-hypertensive syndrome with renal ischemia: an underrecognized disorder. (5/614)
Renal artery stenosis or occlusion causing the hyponatremic-hypertensive syndrome has been rarely reported. Our impression, however, was that the disorder is not uncommon. Case records from patients in one city (population 350 000) presenting between 1980 and 1997 with hypertension, hyponatremia, and evidence of renal ischemia were scrutinized. Thirty-two patients fulfilling inclusion criteria were identified. Admission supine arterial pressures were high (mean 228/124 mm Hg), but there was a vigorous fall in pressure on standing (26/12.7 mm Hg recorded in 27 patients). Mean plasma concentrations of sodium (129.7 mmol/L) and potassium (2.7 mmol/L) were low, and 24-hour urine protein excretion was elevated in 19 of 26 patients. Twenty-two of the 32 patients were female, the majority were asthenic, and all but 5 were smokers. Symptoms precipitating hospitalization were headache, clouding of consciousness, confusion, weakness, weight loss, thirst, and polyuria. Plasma renin levels, measured in 20 patients, were elevated in most cases and correlated inversely (r=-0.63, P<0.01) with the plasma sodium concentration. The hyponatremic-hypertensive syndrome in patients with renal ischemia is not rare: Rather, it is underreported. It tends to affect elderly asthenic women who smoke heavily. Stimulation of renin release from the ischemic kidney is probably central to the pathophysiology. The syndrome deserves better recognition to ensure appropriate investigations and management. (+info)Hyponatraemia: biochemical and clinical perspectives. (6/614)
Hyponatraemia is a common bio-chemical abnormality, occurring in about 15% of hospital inpatients. It is often associated with severe illness and relatively poor outcome. Pathophysiologically, hyponatraemia may be spurious, dilutional, depletional or redistributional. Particularly difficult causes and concepts of hyponatraemia are the syndrome of inappropriate antidiuresis and the sick cell syndrome, which are discussed here in detail. Therapy should always be targeted at the underlying disease process. 'Hyponatraemic symptoms' are of doubtful importance, and may be more related to water overload and/or the causative disease, than to hyponatraemia per se. Artificial elevation of plasma sodium by saline infusion carries the risk of induction of osmotic demyelination (central pontine myelinolysis). (+info)Effect of liver disease and transplantation on urea synthesis in humans: relationship to acid-base status. (7/614)
It has been suggested that hepatic urea synthesis, which consumes HCO-3, plays an important role in acid-base homeostasis. This study measured urea synthesis rate (Ra urea) directly to assess its role in determining the acid-base status in patients with end-stage cirrhosis and after orthotopic liver transplantation (OLT). Cirrhotic patients were studied before surgery (n = 7) and on the second postoperative day (n = 11), using a 5-h primed-constant infusion of [15N2]urea. Six healthy volunteers served as controls. Ra urea was 5.05 +/- 0.40 (SE) and 3.11 +/- 0.51 micromol. kg-1. min-1, respectively, in controls and patients with cirrhosis (P < 0. 05). Arterial base excess was 0.6 +/- 0.3 meq/l in controls and -1.1 +/- 1.3 meq/l in cirrhotic patients (not different). After OLT, Ra urea was 15.05 +/- 1.73 micromol. kg-1. min-1, which accompanied an arterial base excess of 7.0 +/- 0.3 meq/l (P < 0.001). We conclude that impaired Ra urea in cirrhotic patients does not produce metabolic alkalosis. Concurrent postoperative metabolic alkalosis and increased Ra urea indicate that the alkalosis is not caused by impaired Ra urea. It is consistent with, but does not prove, the concept that the graft liver responds to metabolic alkalosis by augmenting Ra urea, thus increasing HCO-3 consumption and moderating the severity of metabolic alkalosis produced elsewhere. (+info)Syndrome of inappropriate secretion of antidiuretic hormone associated with idiopathic normal pressure hydrocephalus. (8/614)
A 79-year-old woman suffering from urinary incontinence and unsteady gait was diagnosed as having idiopathic normal pressure hydrocephalus (NPH) with hyponatremia due to the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). The concentration of antidiuretic hormone was high while the plasma osmolality was low in the presence of concentrated urine during the episodes of hyponatremia. Magnetic resonance imaging (MRI) of the head showed enlargement of the third and lateral ventricles. After ventriculoperitoneal shunt surgery, the symptoms of NPH and hyponatremia improved. It may be possibly explained that mechanical pressure on the hypothalamus from the third ventricle is responsible for hyponatremia. (+info)Hyponatremia is a condition characterized by abnormally low sodium levels in the blood, specifically levels less than 135 mEq/L. Sodium is an essential electrolyte that helps regulate water balance in and around your cells and plays a crucial role in nerve and muscle function. Hyponatremia can occur due to various reasons, including certain medical conditions, medications, or excessive water intake leading to dilution of sodium in the body. Symptoms may range from mild, such as nausea, confusion, and headache, to severe, like seizures, coma, or even death in extreme cases. It's essential to seek medical attention if you suspect hyponatremia, as prompt diagnosis and treatment are vital for a favorable outcome.
Inappropriate Antidiuretic Hormone (ADH) Syndrome, also known as the Syndrome of Inappropriate Antidiuresis (SIAD), is a condition characterized by the excessive release or action of antidiuretic hormone (ADH) leading to an imbalance of water and electrolytes in the body.
ADH is a hormone produced by the pituitary gland that helps regulate water balance in the body by controlling the amount of urine produced by the kidneys. In normal conditions, ADH levels increase in response to dehydration or decreased blood volume, causing the kidneys to retain water and decrease urine output.
However, in Inappropriate ADH Syndrome, there is an overproduction or inappropriate release of ADH, even when the body does not need it. This can lead to a condition called hyponatremia, which is low sodium levels in the blood. Hyponatremia can cause symptoms such as headache, confusion, seizures, and in severe cases, coma or death.
Inappropriate ADH Syndrome can be caused by various factors, including certain medications, brain tumors, lung diseases, and other medical conditions that affect the production or release of ADH. It is important to diagnose and treat Inappropriate ADH Syndrome promptly to prevent serious complications from hyponatremia. Treatment typically involves addressing the underlying cause and adjusting fluid intake and electrolyte levels as needed.
Medical Definition of Water Intoxication:
Water intoxication, also known as hyponatremia, is a condition that occurs when an individual consumes water in such large quantities that the body's electrolyte balance is disrupted. This results in an abnormally low sodium level in the blood (hyponatremia), which can cause symptoms ranging from mild to severe, including nausea, headache, confusion, seizures, coma, and even death in extreme cases. It's important to note that water intoxication is rare and typically only occurs in situations where large amounts of water are consumed in a short period of time, such as during endurance sports or when someone is trying to intentionally harm themselves.
Central pontine myelinolysis (CPM) is a neurological disorder that results from the damage to the myelin sheath in the central pons region of the brainstem. Myelin is the fatty substance that insulates and protects nerve fibers, allowing for the efficient transmission of electrical signals.
In CPM, the myelin sheath in the center of the pons area becomes damaged or destroyed due to various factors, most commonly rapid correction of hyponatremia (low sodium levels in the blood). This rapid correction can lead to an osmotic shift of water from inside the cells to outside, causing swelling and damage to the myelin sheath.
CPM is characterized by the development of symmetrical lesions in the central pons region, which can result in a range of neurological symptoms, including weakness or paralysis of muscles, difficulty swallowing, speech impairment, and altered levels of consciousness. In severe cases, CPM can lead to coma, respiratory failure, and even death.
It's important to note that the management of CPM involves preventing further damage to the myelin sheath by avoiding rapid correction of hyponatremia and providing supportive care for the neurological symptoms. Currently, there is no specific treatment for CPM, and recovery can be slow and incomplete.
Hypernatremia is a medical condition characterized by an abnormally high concentration of sodium (na+) in the blood, specifically a serum sodium level greater than 145 mEq/L. Sodium is an essential electrolyte that helps regulate water balance in and around your cells. It's crucial for many body functions, including the maintenance of blood pressure, regulation of nerve and muscle function, and regulation of fluid balance.
Hypernatremia typically results from a deficit of total body water relative to solute, which can be caused by decreased water intake, increased water loss, or a combination of both. Common causes include dehydration due to severe vomiting or diarrhea, excessive sweating, burns, kidney diseases, and the use of certain medications such as diuretics.
Symptoms of hypernatremia can range from mild to severe and may include thirst, muscle weakness, lethargy, irritability, confusion, seizures, and in extreme cases, coma or even death. Treatment typically involves correcting the underlying cause and gradually rehydrating the individual with intravenous fluids to restore normal sodium levels.
Vasopressin receptors are a type of G protein-coupled receptor that bind to and are activated by the hormone vasopressin (also known as antidiuretic hormone or ADH). There are two main types of vasopressin receptors, V1 and V2.
V1 receptors are found in various tissues throughout the body, including vascular smooth muscle, heart, liver, and kidney. Activation of V1 receptors leads to vasoconstriction (constriction of blood vessels), increased heart rate and force of heart contractions, and release of glycogen from the liver.
V2 receptors are primarily found in the kidney's collecting ducts. When activated, they increase water permeability in the collecting ducts, allowing for the reabsorption of water into the bloodstream and reducing urine production. This helps to regulate fluid balance and maintain normal blood pressure.
Abnormalities in vasopressin receptor function can contribute to various medical conditions, including hypertension, heart failure, and kidney disease.
Sodium is an essential mineral and electrolyte that is necessary for human health. In a medical context, sodium is often discussed in terms of its concentration in the blood, as measured by serum sodium levels. The normal range for serum sodium is typically between 135 and 145 milliequivalents per liter (mEq/L).
Sodium plays a number of important roles in the body, including:
* Regulating fluid balance: Sodium helps to regulate the amount of water in and around your cells, which is important for maintaining normal blood pressure and preventing dehydration.
* Facilitating nerve impulse transmission: Sodium is involved in the generation and transmission of electrical signals in the nervous system, which is necessary for proper muscle function and coordination.
* Assisting with muscle contraction: Sodium helps to regulate muscle contractions by interacting with other minerals such as calcium and potassium.
Low sodium levels (hyponatremia) can cause symptoms such as confusion, seizures, and coma, while high sodium levels (hypernatremia) can lead to symptoms such as weakness, muscle cramps, and seizures. Both conditions require medical treatment to correct.
Demeclocycline is a type of antibiotic known as a tetracycline. It is used to treat various types of bacterial infections, such as respiratory infections, urinary tract infections, and skin infections. Demeclocycline works by inhibiting the growth of bacteria, specifically by binding to the 30S ribosomal subunit and preventing the addition of amino acids to the growing peptide chain. This leads to the disruption of protein synthesis and ultimately results in bacterial death.
Demeclocycline is available as a tablet for oral administration, and it is typically prescribed to be taken two to four times daily. The dosage may vary depending on the type and severity of the infection being treated. Common side effects of demeclocycline include stomach upset, diarrhea, and skin rash. It is important to note that demeclocycline can cause photosensitivity, so it is recommended to avoid excessive sun exposure while taking this medication.
Demeclocycline is not typically a first-line antibiotic due to its potential for serious side effects and the availability of other antibiotics with similar efficacy and fewer side effects. It should be used with caution in patients with impaired kidney or liver function, as well as in pregnant women and children under the age of 8. Additionally, demeclocycline can interact with certain medications, such as antacids, iron supplements, and calcium-containing products, so it is important to inform your healthcare provider of all medications you are taking before starting treatment with demeclocycline.
Water-electrolyte imbalance refers to a disturbance in the balance of water and electrolytes (such as sodium, potassium, chloride, and bicarbonate) in the body. This imbalance can occur when there is an excess or deficiency of water or electrolytes in the body, leading to altered concentrations in the blood and other bodily fluids.
Such imbalances can result from various medical conditions, including kidney disease, heart failure, liver cirrhosis, severe dehydration, burns, excessive sweating, vomiting, diarrhea, and certain medications. Symptoms of water-electrolyte imbalance may include weakness, fatigue, muscle cramps, seizures, confusion, and in severe cases, coma or even death. Treatment typically involves addressing the underlying cause and correcting the electrolyte and fluid levels through appropriate medical interventions.
A hypertonic saline solution is a type of medical fluid that contains a higher concentration of salt (sodium chloride) than is found in the average person's blood. This solution is used to treat various medical conditions, such as dehydration, brain swelling, and increased intracranial pressure.
The osmolarity of a hypertonic saline solution typically ranges from 1500 to 23,400 mOsm/L, with the most commonly used solutions having an osmolarity of around 3000 mOsm/L. The high sodium concentration in these solutions creates an osmotic gradient that draws water out of cells and into the bloodstream, helping to reduce swelling and increase fluid volume in the body.
It is important to note that hypertonic saline solutions should be administered with caution, as they can cause serious side effects such as electrolyte imbalances, heart rhythm abnormalities, and kidney damage if not used properly. Healthcare professionals must carefully monitor patients receiving these solutions to ensure safe and effective treatment.
Vasopressin, also known as antidiuretic hormone (ADH), is a hormone that helps regulate water balance in the body. It is produced by the hypothalamus and stored in the posterior pituitary gland. When the body is dehydrated or experiencing low blood pressure, vasopressin is released into the bloodstream, where it causes the kidneys to decrease the amount of urine they produce and helps to constrict blood vessels, thereby increasing blood pressure. This helps to maintain adequate fluid volume in the body and ensure that vital organs receive an adequate supply of oxygen-rich blood. In addition to its role in water balance and blood pressure regulation, vasopressin also plays a role in social behaviors such as pair bonding and trust.
Benzazepines are a class of heterocyclic compounds that contain a benzene fused to a diazepine ring. In the context of pharmaceuticals, benzazepines refer to a group of drugs with various therapeutic uses, such as antipsychotics and antidepressants. Some examples of benzazepine-derived drugs include clozapine, olanzapine, and loxoprofen. These drugs have complex mechanisms of action, often involving multiple receptor systems in the brain.
Water-electrolyte balance refers to the regulation of water and electrolytes (sodium, potassium, chloride, bicarbonate) in the body to maintain homeostasis. This is crucial for various bodily functions such as nerve impulse transmission, muscle contraction, fluid balance, and pH regulation. The body maintains this balance through mechanisms that control water intake, excretion, and electrolyte concentration in various body fluids like blood and extracellular fluid. Disruptions in water-electrolyte balance can lead to dehydration or overhydration, and imbalances in electrolytes can cause conditions such as hyponatremia (low sodium levels) or hyperkalemia (high potassium levels).
Confusion is a state of bewilderment or disorientation in which a person has difficulty processing information, understanding their surroundings, and making clear decisions. It can be caused by various medical conditions such as infections, brain injury, stroke, dementia, alcohol or drug intoxication or withdrawal, and certain medications. Confusion can also occur in older adults due to age-related changes in the brain.
In medical terms, confusion is often referred to as "acute confusional state" or "delirium." It is characterized by symptoms such as difficulty paying attention, memory loss, disorientation, hallucinations, and delusions. Confusion can be a serious medical condition that requires immediate evaluation and treatment by a healthcare professional.
Adrenal insufficiency is a condition in which the adrenal glands do not produce adequate amounts of certain hormones, primarily cortisol and aldosterone. Cortisol helps regulate metabolism, respond to stress, and suppress inflammation, while aldosterone helps regulate sodium and potassium levels in the body to maintain blood pressure.
Primary adrenal insufficiency, also known as Addison's disease, occurs when there is damage to the adrenal glands themselves, often due to autoimmune disorders, infections, or certain medications. Secondary adrenal insufficiency occurs when the pituitary gland fails to produce enough adrenocorticotropic hormone (ACTH), which stimulates the adrenal glands to produce cortisol.
Symptoms of adrenal insufficiency may include fatigue, weakness, weight loss, decreased appetite, nausea, vomiting, diarrhea, abdominal pain, low blood pressure, dizziness, and darkening of the skin. Treatment typically involves replacing the missing hormones with medications taken orally or by injection.
Desmopressin, also known as 1-deamino-8-D-arginine vasopressin (dDAVP), is a synthetic analogue of the natural hormone arginine vasopressin. It is commonly used in medical practice for the treatment of diabetes insipidus, a condition characterized by excessive thirst and urination due to lack of antidiuretic hormone (ADH).
Desmopressin works by binding to V2 receptors in the kidney, which leads to increased water reabsorption and reduced urine production. It also has some effect on V1 receptors, leading to vasoconstriction and increased blood pressure. However, its primary use is for its antidiuretic effects.
In addition to its use in diabetes insipidus, desmopressin may also be used to treat bleeding disorders such as hemophilia and von Willebrand disease, as it can help to promote platelet aggregation and reduce bleeding times. It is available in various forms, including nasal sprays, injectable solutions, and oral tablets or dissolvable films.
Hypovolemia is a medical condition characterized by a decreased volume of circulating blood in the body, leading to inadequate tissue perfusion and oxygenation. This can occur due to various reasons such as bleeding, dehydration, vomiting, diarrhea, or excessive sweating, which result in a reduced amount of fluid in the intravascular space.
The severity of hypovolemia depends on the extent of fluid loss and can range from mild to severe. Symptoms may include thirst, dry mouth, weakness, dizziness, lightheadedness, confusion, rapid heartbeat, low blood pressure, and decreased urine output. Severe hypovolemia can lead to shock, organ failure, and even death if not treated promptly and effectively.
Empty Sella Syndrome is a condition characterized by the absence or near-absence of the pituitary gland in the sella turcica, a bony structure at the base of the skull that houses the pituitary gland. This can occur due to the herniation of the arachnoid membrane, which surrounds the brain and spinal cord, into the sella turcica, compressing or replacing the pituitary gland.
In some cases, Empty Sella Syndrome may be asymptomatic and discovered incidentally on imaging studies. However, in other cases, it can lead to hormonal imbalances due to the disruption of the pituitary gland's function. Symptoms may include headaches, vision changes, menstrual irregularities, fatigue, and decreased libido. Treatment typically involves addressing any underlying hormonal deficiencies with medication or hormone replacement therapy.
Arginine vasopressin (AVP), also known as antidiuretic hormone (ADH), is a hormone produced in the hypothalamus and stored in the posterior pituitary gland. It plays a crucial role in regulating water balance and blood pressure in the body.
AVP acts on the kidneys to promote water reabsorption, which helps maintain adequate fluid volume and osmotic balance in the body. It also constricts blood vessels, increasing peripheral vascular resistance and thereby helping to maintain blood pressure. Additionally, AVP has been shown to have effects on cognitive function, mood regulation, and pain perception.
Deficiencies or excesses of AVP can lead to a range of medical conditions, including diabetes insipidus (characterized by excessive thirst and urination), hyponatremia (low sodium levels in the blood), and syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Myxedema is not a term used in modern medicine to describe a specific medical condition. However, historically, it was used to refer to the severe form of hypothyroidism, a condition characterized by an underactive thyroid gland that doesn't produce enough thyroid hormones. In hypothyroidism, various body functions slow down, which can lead to symptoms such as fatigue, weight gain, cold intolerance, constipation, and dry skin.
Myxedema specifically refers to the physical signs of severe hypothyroidism, including swelling (edema) and thickening of the skin, particularly around the face, hands, and feet, as well as a puffy appearance of the face. The term myxedema coma was used to describe a rare but life-threatening complication of long-standing, untreated hypothyroidism, characterized by altered mental status, hypothermia, and other systemic manifestations.
Nowadays, healthcare professionals use more precise medical terminology to describe these conditions, such as hypothyroidism or myxedematous edema, rather than the outdated term myxedema.
Antidiuretic agents are medications or substances that reduce the amount of urine produced by the body. They do this by increasing the reabsorption of water in the kidneys, which leads to a decrease in the excretion of water and solutes in the urine. This can help to prevent dehydration and maintain fluid balance in the body.
The most commonly used antidiuretic agent is desmopressin, which works by mimicking the action of a natural hormone called vasopressin (also known as antidiuretic hormone or ADH). Vasopressin is produced by the pituitary gland and helps to regulate water balance in the body. When the body's fluid levels are low, vasopressin is released into the bloodstream, where it causes the kidneys to reabsorb more water and produce less urine.
Antidiuretic agents may be used to treat a variety of medical conditions, including diabetes insipidus (a rare disorder that causes excessive thirst and urination), bedwetting in children, and certain types of headaches. They may also be used to manage fluid balance in patients with kidney disease or heart failure.
It is important to use antidiuretic agents only under the supervision of a healthcare provider, as they can have side effects and may interact with other medications. Overuse or misuse of these drugs can lead to water retention, hyponatremia (low sodium levels in the blood), and other serious complications.
Hypopituitarism is a medical condition characterized by deficient secretion of one or more hormones produced by the pituitary gland, a small endocrine gland located at the base of the brain. The pituitary gland controls several other endocrine glands in the body, including the thyroid, adrenals, and sex glands (ovaries and testes).
Hypopituitarism can result from damage to the pituitary gland due to various causes such as tumors, surgery, radiation therapy, trauma, or inflammation. In some cases, hypopituitarism may also be caused by a dysfunction of the hypothalamus, a region in the brain that regulates the pituitary gland's function.
The symptoms and signs of hypopituitarism depend on which hormones are deficient and can include fatigue, weakness, decreased appetite, weight loss, low blood pressure, decreased sex drive, infertility, irregular menstrual periods, intolerance to cold, constipation, thinning hair, dry skin, and depression.
Treatment of hypopituitarism typically involves hormone replacement therapy to restore the deficient hormones' normal levels. The type and dosage of hormones used will depend on which hormones are deficient and may require regular monitoring and adjustments over time.
Azotemia is a medical term that refers to an elevated level of urea and other nitrogenous waste products in the blood. This condition is typically caused by impaired kidney function, which can lead to the accumulation of these substances in the body.
Normally, the kidneys filter waste products from the blood and excrete them in the urine. However, when the kidneys are not functioning properly, they may be unable to remove these waste products efficiently, leading to their buildup in the bloodstream. This can cause a range of symptoms, including nausea, vomiting, fatigue, and confusion.
Azotemia is often classified based on the level of urea in the blood, with mild azotemia defined as a blood urea nitrogen (BUN) level between 20 and 39 mg/dL, moderate azotemia defined as a BUN level between 40 and 89 mg/dL, and severe azotemia defined as a BUN level of 90 mg/dL or higher.
Treatment for azotemia typically involves addressing the underlying cause of the condition, which may involve medications to control high blood pressure or diabetes, dietary changes, or dialysis in severe cases.
Osmolar concentration is a measure of the total number of solute particles (such as ions or molecules) dissolved in a solution per liter of solvent (usually water), which affects the osmotic pressure. It is expressed in units of osmoles per liter (osmol/L). Osmolarity and osmolality are related concepts, with osmolarity referring to the number of osmoles per unit volume of solution, typically measured in liters, while osmolality refers to the number of osmoles per kilogram of solvent. In clinical contexts, osmolar concentration is often used to describe the solute concentration of bodily fluids such as blood or urine.
Fludrocortisone is a synthetic corticosteroid hormone, specifically a mineralocorticoid. It is often used to treat conditions associated with low levels of corticosteroids, such as Addison's disease. It works by helping the body retain sodium and lose potassium, which helps to maintain fluid balance and blood pressure.
In medical terms, fludrocortisone is defined as a synthetic mineralocorticoid with glucocorticoid activity used in the treatment of adrenogenital syndrome and Addison's disease, and as an adjunct in the treatment of rheumatoid arthritis. It is also used to treat orthostatic hypotension by helping the body retain sodium and water, thereby increasing blood volume and blood pressure.
It is important to note that fludrocortisone can have significant side effects, particularly if used in high doses or for long periods of time. These can include fluid retention, high blood pressure, increased risk of infection, and slowed growth in children. As with any medication, it should be used under the close supervision of a healthcare provider.
The term "drinking" is commonly used to refer to the consumption of beverages, but in a medical context, it usually refers to the consumption of alcoholic drinks. According to the Merriam-Webster Medical Dictionary, "drinking" is defined as:
1. The act or habit of swallowing liquid (such as water, juice, or alcohol)
2. The ingestion of alcoholic beverages
It's important to note that while moderate drinking may not pose significant health risks for some individuals, excessive or binge drinking can lead to a range of negative health consequences, including addiction, liver disease, heart disease, and increased risk of injury or violence.
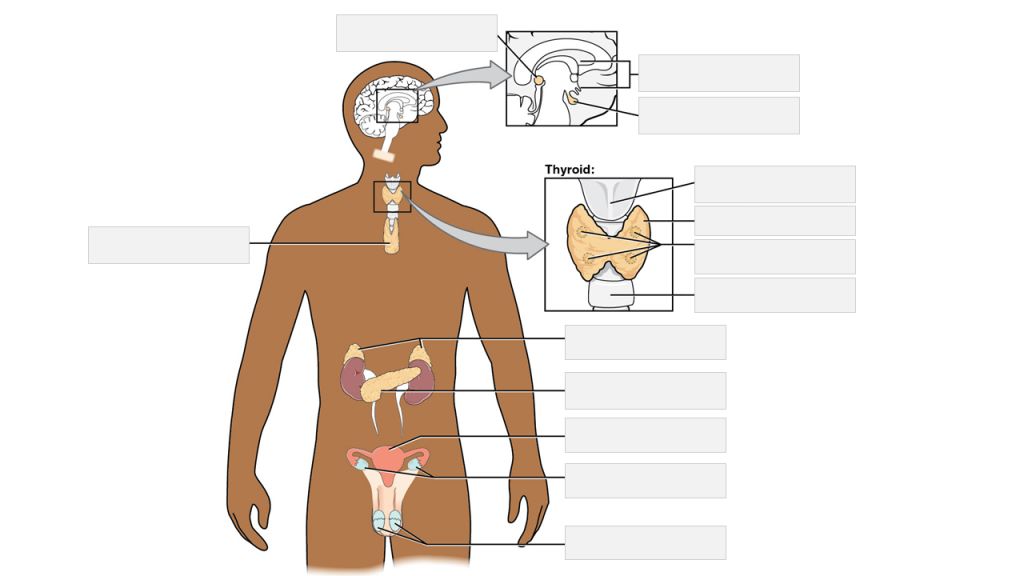
Endocrine surgical procedures refer to the surgical removal or manipulation of endocrine glands or related structures. Endocrine glands are specialized organs that produce, store, and secrete hormones directly into the bloodstream. These hormones regulate various physiological processes in the body, including metabolism, growth, development, and reproduction.
Some common endocrine surgical procedures include:
1. Thyroidectomy: Surgical removal of all or part of the thyroid gland, which is located in the neck and produces hormones regulating metabolism. Indications for thyroidectomy may include thyroid cancer, benign thyroid nodules, hyperthyroidism, and Graves' disease.
2. Parathyroidectomy: Surgical removal of one or more parathyroid glands, which are located near the thyroid gland and regulate calcium levels in the blood. Indications for parathyroidectomy may include hyperparathyroidism, parathyroid tumors, and kidney stones caused by high calcium levels.
3. Adrenalectomy: Surgical removal of one or both adrenal glands, which are located on top of the kidneys and produce hormones regulating stress response, metabolism, and blood pressure. Indications for adrenalectomy may include adrenal cancer, pheochromocytoma, Cushing's syndrome, and Conn's syndrome.
4. Pancreatectomy: Surgical removal of all or part of the pancreas, which is a gland located behind the stomach and produces hormones regulating blood sugar levels (insulin and glucagon) and enzymes for digestion. Indications for pancreatectomy may include pancreatic cancer, chronic pancreatitis, and insulinoma.
5. Neuroendocrine tumor resection: Surgical removal of neuroendocrine tumors, which are rare tumors that arise from hormone-producing cells in various organs, including the pancreas, lung, and gastrointestinal tract. Indications for neuroendocrine tumor resection may include symptoms caused by hormone excess or risk of metastasis.
These surgical procedures are complex and require specialized training and expertise. Patients should consult with a qualified surgeon to discuss the risks and benefits of each procedure and determine the best course of treatment.
Hyperkalemia is a medical condition characterized by an elevated level of potassium (K+) in the blood serum, specifically when the concentration exceeds 5.0-5.5 mEq/L (milliequivalents per liter). Potassium is a crucial intracellular ion that plays a significant role in various physiological processes, including nerve impulse transmission, muscle contraction, and heart rhythm regulation.
Mild to moderate hyperkalemia might not cause noticeable symptoms but can still have harmful effects on the body, particularly on the cardiovascular system. Severe cases of hyperkalemia (potassium levels > 6.5 mEq/L) can lead to potentially life-threatening arrhythmias and heart failure.
Hyperkalemia may result from various factors, such as kidney dysfunction, hormonal imbalances, medication side effects, trauma, or excessive potassium intake. Prompt identification and management of hyperkalemia are essential to prevent severe complications and ensure proper treatment.
Fluid therapy, in a medical context, refers to the administration of fluids into a patient's circulatory system for various therapeutic purposes. This can be done intravenously (through a vein), intraosseously (through a bone), or subcutaneously (under the skin). The goal of fluid therapy is to correct or prevent imbalances in the body's fluids and electrolytes, maintain or restore blood volume, and support organ function.
The types of fluids used in fluid therapy can include crystalloids (which contain electrolytes and water) and colloids (which contain larger molecules like proteins). The choice of fluid depends on the patient's specific needs and condition. Fluid therapy is commonly used in the treatment of dehydration, shock, sepsis, trauma, surgery, and other medical conditions that can affect the body's fluid balance.
Proper administration of fluid therapy requires careful monitoring of the patient's vital signs, urine output, electrolyte levels, and overall clinical status to ensure that the therapy is effective and safe.
Demyelinating diseases are a group of disorders that are characterized by damage to the myelin sheath, which is the protective covering surrounding nerve fibers in the brain, optic nerves, and spinal cord. Myelin is essential for the rapid transmission of nerve impulses, and its damage results in disrupted communication between the brain and other parts of the body.
The most common demyelinating disease is multiple sclerosis (MS), where the immune system mistakenly attacks the myelin sheath. Other demyelinating diseases include:
1. Acute Disseminated Encephalomyelitis (ADEM): An autoimmune disorder that typically follows a viral infection or vaccination, causing widespread inflammation and demyelination in the brain and spinal cord.
2. Neuromyelitis Optica (NMO) or Devic's Disease: A rare autoimmune disorder that primarily affects the optic nerves and spinal cord, leading to severe vision loss and motor disability.
3. Transverse Myelitis: Inflammation of the spinal cord causing damage to both sides of one level (segment) of the spinal cord, resulting in various neurological symptoms such as muscle weakness, numbness, or pain, depending on which part of the spinal cord is affected.
4. Guillain-Barré Syndrome: An autoimmune disorder that causes rapid-onset muscle weakness, often beginning in the legs and spreading to the upper body, including the face and breathing muscles. It occurs when the immune system attacks the peripheral nerves' myelin sheath.
5. Central Pontine Myelinolysis (CPM): A rare neurological disorder caused by rapid shifts in sodium levels in the blood, leading to damage to the myelin sheath in a specific area of the brainstem called the pons.
These diseases can result in various symptoms, such as muscle weakness, numbness, vision loss, difficulty with balance and coordination, and cognitive impairment, depending on the location and extent of the demyelination. Treatment typically focuses on managing symptoms, modifying the immune system's response, and promoting nerve regeneration and remyelination when possible.
Body water refers to the total amount of water present in the human body. It is an essential component of life and makes up about 60-70% of an adult's body weight. Body water is distributed throughout various fluid compartments within the body, including intracellular fluid (water inside cells), extracellular fluid (water outside cells), and transcellular fluid (water found in specific bodily spaces such as the digestive tract, eyes, and joints). Maintaining proper hydration and balance of body water is crucial for various physiological processes, including temperature regulation, nutrient transportation, waste elimination, and overall health.
Psychogenic polydipsia is a condition characterized by excessive fluid intake (polydipsia) due to psychological factors rather than physical causes. It is often seen in individuals with mental health disorders such as schizophrenia, affective disorders, or dementia. In these cases, the individual may have a fixed belief that they are thirsty and need to drink large amounts of water or other fluids, even when their body does not require it. This can lead to dilution of the sodium levels in the blood (hyponatremia), which can cause serious health complications if left untreated. It is important to note that psychogenic polydipsia should be distinguished from physical causes of polydipsia, such as diabetes insipidus or diabetes mellitus, which require different treatment approaches.
Kluver-Bucy Syndrome is a rare and complex neurobehavioral disorder, typically caused by damage to the temporal lobes and surrounding structures in the brain, particularly the amygdala and hippocampus. The syndrome is characterized by a range of symptoms that may include:
1. Hyperorality (excessive exploration of objects with the mouth)
2. Visual agnosia (inability to recognize familiar objects despite intact vision)
3. Hypermetamorphosis (compulsively looking at and exploring new objects)
4. Dietary changes, such as increased appetite and food preference changes
5. Emotional changes, including decreased emotional responsiveness and loss of fear or anxiety
6. Memory impairment
7. Increased sexual behavior
8. Hyperactivity and decreased initiative
9. Altered sleep-wake cycle
10. Inability to recognize faces (prosopagnosia)
It's important to note that the presence and severity of these symptoms can vary widely between individuals with Kluver-Bucy Syndrome, depending on the extent and location of brain damage. The syndrome is often associated with conditions such as herpes encephalitis, traumatic brain injury, or neurodegenerative diseases like Alzheimer's disease.
"Renal agents" is not a standardized medical term with a single, widely accepted definition. However, in a general sense, renal agents could refer to medications or substances that have an effect on the kidneys or renal function. This can include drugs that are primarily used to treat kidney diseases or disorders (such as certain types of diuretics, ACE inhibitors, or ARBs), as well as chemicals or toxins that can negatively impact renal function if they are not properly eliminated from the body.
It's worth noting that the term "renal agent" is not commonly used in medical literature or clinical practice, and its meaning may vary depending on the context in which it is used. If you have any specific questions about a particular medication or substance and its effect on renal function, I would recommend consulting with a healthcare professional for more accurate information.
Neurophysins are small protein molecules that are derived from the larger precursor protein, pro-neurophysin. They are synthesized in the hypothalamus of the brain and are stored in and released from neurosecretory granules, along with neurohypophysial hormones such as oxytocin and vasopressin.
Neurophysins serve as carrier proteins for these hormones, helping to stabilize them and facilitate their transport and release into the bloodstream. There are two main types of neurophysins, neurophysin I and neurophysin II, which are associated with oxytocin and vasopressin, respectively.
Neurophysins have been studied for their potential role in various physiological processes, including water balance, social behavior, and reproductive functions. However, their precise mechanisms of action and functional significance are still not fully understood.
Chlorpropamide is a type of oral anti-diabetic drug known as a sulfonylurea, which is used to lower blood glucose levels in people with type 2 diabetes. It works by stimulating the release of insulin from the pancreas and increasing the sensitivity of peripheral tissues to insulin.
Here's the medical definition:
Chlorpropamide: A first-generation sulfonylurea medication used in the management of type 2 diabetes mellitus. It acts by stimulating the release of insulin from the pancreatic beta cells and increasing peripheral tissue sensitivity to insulin. Chlorpropamide has a longer duration of action than other sulfonylureas, with a peak effect at around 6-12 hours after administration. Common side effects include hypoglycemia, weight gain, and gastrointestinal symptoms such as nausea and diarrhea. It is important to monitor blood glucose levels regularly while taking chlorpropamide to avoid hypoglycemia.
Diuretics are a type of medication that increase the production of urine and help the body eliminate excess fluid and salt. They work by interfering with the reabsorption of sodium in the kidney tubules, which in turn causes more water to be excreted from the body. Diuretics are commonly used to treat conditions such as high blood pressure, heart failure, liver cirrhosis, and kidney disease. There are several types of diuretics, including loop diuretics, thiazide diuretics, potassium-sparing diuretics, and osmotic diuretics, each with its own mechanism of action and potential side effects. It is important to use diuretics under the guidance of a healthcare professional, as they can interact with other medications and have an impact on electrolyte balance in the body.
Metabolic brain diseases refer to a group of conditions that are caused by disruptions in the body's metabolic processes, which affect the brain. These disorders can be inherited or acquired and can result from problems with the way the body produces, breaks down, or uses energy and nutrients.
Examples of metabolic brain diseases include:
1. Mitochondrial encephalomyopathies: These are a group of genetic disorders that affect the mitochondria, which are the energy-producing structures in cells. When the mitochondria don't function properly, it can lead to muscle weakness, neurological problems, and developmental delays.
2. Leukodystrophies: These are a group of genetic disorders that affect the white matter of the brain, which is made up of nerve fibers covered in myelin, a fatty substance that insulates the fibers and helps them transmit signals. When the myelin breaks down or is not produced properly, it can lead to cognitive decline, motor problems, and other neurological symptoms.
3. Lysosomal storage disorders: These are genetic disorders that affect the lysosomes, which are structures in cells that break down waste products and recycle cellular materials. When the lysosomes don't function properly, it can lead to the accumulation of waste products in cells, including brain cells, causing damage and neurological symptoms.
4. Maple syrup urine disease: This is a genetic disorder that affects the way the body breaks down certain amino acids, leading to a buildup of toxic levels of these substances in the blood and urine. If left untreated, it can cause brain damage, developmental delays, and other neurological problems.
5. Homocystinuria: This is a genetic disorder that affects the way the body processes an amino acid called methionine, leading to a buildup of homocysteine in the blood. High levels of homocysteine can cause damage to the blood vessels and lead to neurological problems, including seizures, developmental delays, and cognitive decline.
Treatment for metabolic brain diseases may involve dietary changes, supplements, medications, or other therapies aimed at managing symptoms and preventing further damage to the brain. In some cases, a stem cell transplant may be recommended as a treatment option.
 Hyponatremia
Hyponatremia Synonyms of hyponatremia | FactMonster
Synonyms of hyponatremia | FactMonster Hyponatremia: Practice Essentials, Pathophysiology, Epidemiology
Hyponatremia: Practice Essentials, Pathophysiology, Epidemiology A case of recurrent hyponatremia induced by venlafaxine
A case of recurrent hyponatremia induced by venlafaxine Hyponatremia vs. Hyperglycemia: Knowing the Difference
Hyponatremia vs. Hyperglycemia: Knowing the Difference Hyperosmolar Hyponatremia
Hyperosmolar Hyponatremia Hyponatremia: Causes, Symptoms, Diagnosis & Treatment
Hyponatremia: Causes, Symptoms, Diagnosis & Treatment Hyponatremia Discussion and Explanation
Hyponatremia Discussion and Explanation How Athletes Can Spot and Prevent Exercise-associated Hyponatremia (EAH)
How Athletes Can Spot and Prevent Exercise-associated Hyponatremia (EAH) Exertional Hyponatremia, Active Component, U.S. Armed Forces, 2006-2021 | Health.mil
Exertional Hyponatremia, Active Component, U.S. Armed Forces, 2006-2021 | Health.mil Hyponatremia Prevention, Causes and Symptoms for Exercising Athletes
Hyponatremia Prevention, Causes and Symptoms for Exercising Athletes Hyponatremia: What is it? | Straight to the Bar
Hyponatremia: What is it? | Straight to the Bar Low Sodium in Blood (Hyponatremia): Causes, Symptoms, & Treatment
Low Sodium in Blood (Hyponatremia): Causes, Symptoms, & Treatment Erowid.org: Erowid Reference 153 : Hyponatraemia, seizures and stupor associated with ecstasy ingestion in a female : Magee C,...
Erowid.org: Erowid Reference 153 : Hyponatraemia, seizures and stupor associated with ecstasy ingestion in a female : Magee C,... Using Osmolality to Diagnose and Treat Hyponatremia in COVID-19 Patients - Advanced instruments
Using Osmolality to Diagnose and Treat Hyponatremia in COVID-19 Patients - Advanced instruments Diagnosis and treatment of hyponatremia: a systematic review of clinical practice guidelines and consensus statements | BMC...
Diagnosis and treatment of hyponatremia: a systematic review of clinical practice guidelines and consensus statements | BMC... 3% NaCl Infusions Via Peripheral Line to Treat Hyponatremia | UPMC Physician Resources
3% NaCl Infusions Via Peripheral Line to Treat Hyponatremia | UPMC Physician Resources Hyponatremia - Endocrine and Metabolic Disorders - MSD Manual Professional Edition
Hyponatremia - Endocrine and Metabolic Disorders - MSD Manual Professional Edition MANAGEMENT OF ENDOCRINE DISEASE: Hypothyroidism-associated hyponatremia: mechanisms, implications and treatment. | Read by QxMD
MANAGEMENT OF ENDOCRINE DISEASE: Hypothyroidism-associated hyponatremia: mechanisms, implications and treatment. | Read by QxMD About Hyponatremia
About Hyponatremia