Hypogonadism
Kallmann Syndrome
Puberty, Delayed
Testosterone
Hormone Replacement Therapy
Klinefelter Syndrome
Andropause
Gonadotropins
Gonadotropin-Releasing Hormone
Gynecomastia
Eunuchism
Endocrine System Diseases
DAX-1 Orphan Nuclear Receptor
Receptors, LHRH
Erectile Dysfunction
Luteinizing Hormone, beta Subunit
Follicle Stimulating Hormone
Leuprolide
CHARGE Syndrome
Olfaction Disorders
Luteinizing Hormone
Hypopituitarism
Libido
Sex Hormone-Binding Globulin
Hypothalamic Diseases
Puberty
Gonadotropins, Pituitary
Kisspeptins
Infertility, Male
Androgens
Testis
Receptor, Fibroblast Growth Factor, Type 1
Adrenal Insufficiency
Prader-Willi Syndrome
Gonadal Dysgenesis, 46,XX
Pedigree
Hyperprolactinemia
Sex Chromosome Aberrations
Sustained anabolic effects of long-term androgen administration in men with AIDS wasting. (1/683)
Fifty-one human immunodeficiency virus-positive men with hypogonadism and wasting were randomized to receive testosterone enanthate, 300 mg i.m. every 3 weeks, or placebo for 6 months, followed by open-label testosterone administration for 6 months. Subjects initially randomized to placebo gained lean body mass (LBM) only after crossover to testosterone administration (mean change +/- standard error of the mean, -0.6 +/- 0.7 kg [months 0-6] vs. 1.9 +/- 0.7 kg [months 6-12]; P = .03). In contrast, subjects initially randomized to testosterone continued to gain LBM during open-label administration (2.0 +/- 0.7 kg [months 0-6] vs. 1.6 +/- 0.6 kg [months 6-12]; P = .62) and had gained more LBM at 1 year than did subjects receiving testosterone for only the final 6 months of the study (3.7 +/- 0.8 kg vs. 1.0 +/- 1.0 kg; P = .05). Testosterone administration results in sustained increases in LBM during 1 year of therapy in hypogonadal men with AIDS wasting. (+info)Intramuscular injection of testosterone undecanoate for the treatment of male hypogonadism: phase I studies. (2/683)
OBJECTIVE: In the search for long-acting testosterone preparations suited for substitution therapy of hypogonadal men, testosterone undecanoate (TU) dissolved in either tea seed oil or castor oil was investigated. DESIGN: In study I, 1000 mg TU in tea seed oil (125 mg/ml) were injected in equal parts into the gluteal muscles of seven hypogonadal men. In study II, 1000 mg TU in castor oil (250 mg/ml) were injected into one gluteal muscle of 14 patients. RESULTS: In comparison with published data on testosterone enanthate, most widely used for i.m. injections, the kinetic profiles of both TU preparations showed extended half-lives and serum levels not exceeding the upper limit of normal. The castor oil preparation had a longer half-life than TU in tea seed oil (33.9+/-4.9 vs 20.9+/-6.0 days (mean pm S.E.M.)). CONCLUSION: The longer half-life and the smaller injection volume make TU in castor oil a strong candidate for further applications in substitution therapy and in trials for male contraception. (+info)A female case of Kallmann's syndrome. (3/683)
A case of 20-year-old woman with hypogonadotropic hypogonadism and anosmia is reported, since very few female cases of Kallmann's syndrome have been reported so far in Japan. Three uncles on the father's side had no children. Height was 168 cm, and arm span 165 cm. The olfactory test revealed complete anosmia. Bone age was 13 year. Chromosome was 46 XX and normal karyotype. Basal levels of serum FSH, LH and estrogens (E1, E2 and E3) were low. Serum FSH and LH levels rose slightly only after LH-RH administration, and did not increase in clomiphene test. Plasma estrogens did not increase after daily injection of 150 IU of HMG for 3 successive days. The response of serum GH to arginine infusion was normal, while that to insulin-induced hypoglycemia was poor. (+info)Anti-nuclear antibodies in patients with premature ovarian failure. (4/683)
We examined the prevalence of anti-nuclear antibodies (ANA) in 32 consecutive patients with premature ovarian failure with and without chromosomal abnormalities. Blood samples were taken for karyotype determination as well as detection of autoantibodies, X-terminal microdeletions and spontaneous follicular growth. The correlation between ANA positivity and the age at onset of amenorrhoea, as well as the presence of karyotype abnormalities, X-terminal microdeletions and follicular growth was determined. Ten of the 24 patients with normal karyotype and none of the 8 patients with karyotype abnormalities were ANA positive. ANA were found more frequently in patients with premature ovarian failure with normal karyotypes than in control amenorrhoeic patients (42 versus 6, P < 0.01). ANA were found in 77% (10/13) of premature ovarian failure patients with normal karyotypes who developed amenorrhoea at or under the age of 30 years, but not in the patients who developed amenorrhoea later in life. Follicular growth was evident in 50% (5/10) of karyotypically normal patients with ANA, 71% (10/14) of karyotypically normal patients without ANA and 38% (3/8) of patients with karyotype abnormalities. X-terminal microdeletions were not found in any of the patients studied. These results suggest that patients with premature ovarian failure and ANA are an aetiologically and clinically distinct group. (+info)Imprinting by neonatal sex steroids on the structure and function of the mature mouse prostate. (5/683)
Perinatal sex-steroid exposure may result in permanent modifications in the structure and function of the prostate gland. The mechanism of such long-range alterations in hormonal sensitivity is not known. This study aimed to define the molecular requirements for neonatal sex-steroid imprinting and to investigate whether combined administration of neonatal androgens and estrogens had synergistic effects upon the mature mouse prostate. Since the interaction between endogenous and exogenous sex steroids in normal mice makes it difficult to dissociate direct from indirect effects, we used the hypogonadal (hpg) mouse, characterized by congenital androgen deficiency yet still fully responsive to exogenous androgens. Newborn mice (Days 1-2) were administered a single s.c. injection of androgens alone or in combination with an estrogen followed by testosterone-induced maximal prostate growth at maturity. The final effects were determined in 7-wk-old mice through study of ductal architecture in microdissected ventral prostates (VP) and quantitation of volume densities and diameters of prostate tissue components. A single neonatal dose of androgens, but not of estrogen, increased branching morphogenesis and VP weights at adulthood. These effects did not differ significantly between various androgens; in addition, combined androgen and estrogen treatment failed to demonstrate any synergistic effects on the prostate. We conclude that neonatal androgens induce long-range effects upon the mature VP structure as well as its secretory function and that this imprinting occurs via the androgen receptor without requiring aromatization of androgens. However, these conclusions, based on a specific treatment protocol, are confined only to the distal segment of VP, and effects of neonatal sex-steroid exposure in other regions or lobes of VP may differ. (+info)A concomitant decrease in cortical and trabecular bone mass in isolated hypogonadotropic hypogonadism and gonadal dysgenesis. (6/683)
To assess the impact of hypogonadism on bone mineral density, we performed a cross-sectional study of 70 amenorrheic women, comprising 22 cases of gonadal dysgenesis and 48 cases of isolated hypogonadotropic hypogonadism (IHH). Bone mineral density was measured by DEXA at four sites: the femur neck, Ward's triangle, trochanter, and lumbar spine (L2-4). The results were compared to those of a control group consisting of 60 age-matched, normal-cycling women. Bone mineral densities around age 20 were already significantly lower at all four sites in patients with IHH and gonadal dysgenesis when compared with controls, suggesting that these patients failed to achieve peak bone mass during pubertal development. In patients with IHH, the initial BMD around age 18-20 were significantly lower at all four sites and the decrease in bone density continued rapidly during the early twenties up to age 25, and then it slowed markedly thereafter. Bone biochemical marker, ICTP and osteocalcin were significantly negatively correlated with age and remained increased until age 40, which was reminiscent of menopausal bone loss pattern such as high bone turn-over in the early twenties, followed by slow bone loss in the late twenties. In patients with gonadal dysgenesis, bone biochemical marker, ICTP and osteocalcin were also significantly negative correlated with age and remained increased until age 40, but no significant changes in BMD were noted as a function of age, which may be attributed to the small sample size and slow bone loss. These findings suggest that the initiation of prompt and timely therapeutic intervention as early as possible in the menarchal period and throughout the remainder of life, particularly during the period associated with rapid bone loss. (+info)Osteopenia in young hypogonadal women with systemic lupus erythematosus receiving chronic steroid therapy: a randomized controlled trial comparing calcitriol and hormonal replacement therapy. (7/683)
OBJECTIVE: To evaluate the efficacy of calcitriol and hormonal replacement therapy (HRT) in the treatment of steroid-induced osteoporosis in hypogonadal women. METHODS: We studied 28 young patients (aged 37 +/- 6 yr) with systemic lupus erythematosus (SLE) on chronic steroid therapy for 130 +/- 22 months and requiring more than 10 mg/day prednisone. They were amenorrhoeic for more than 2 yr with proven ovarian failure. All had osteopenia with a T score at L2-4 of less than -1. They were randomized to receive HRT (conjugated oestrogen 0.625 mg daily from day 1 to day 21 plus medroxyprogesterone acetate 5 mg daily days 10-21) or calcitriol 0.5 microg daily. All received calcium carbonate 1 g/day. RESULTS: There were no differences in the baseline demographic, bone mineral density (BMD) and biochemical data between the two groups. Lumbar spine BMD increased by 2.0 +/- 0.4% after 2 yr with HRT (P<0.05), but reduced by 1.74 +/- 0.4% (P<0.05) with calcitriol treatment. No change was seen at the distal one-third radius with HRT treatment but significant bone loss (2.3 +/- 1.4%, P<0.02) was observed with calcitriol therapy. BMD at the hip did not change in both groups. Comparing both treatment groups, significant differences in the BMD at the spine (P<0.03) and radius (P<0.05) were seen at the end of 2 yr. The changes in urinary n-telopeptide excretion but not serum osteocalcin at 6 months and 12 months were inversely correlated with the changes in lumbar spine BMD at 24 months. HRT did not cause an adverse effect on SLE disease activity. CONCLUSION: HRT but not calcitriol could prevent bone loss in young hypogonadal women on chronic steroid therapy. (+info)A novel mutation of the KAL1 gene in Kallmann syndrome. (8/683)
Kallmann syndrome is defined by the association of hypogonadotropic hypogonadism and anosmia, for which three modes of transmission have been described: X-linked, autosomal recessive and autosomal dominant. The KAL1 gene, responsible for the X-linked form of the disease, has been isolated and its intron-exon organization determined. We report sequence analysis using PCR-direct sequencing method of the entire coding region and splice site junctions of the KAL1 gene in three males with Kallmann syndrome. We found a novel mutation in one case and no mutation in the other two cases. The mutation consisted of a C to T substitution in exon 1 converting codon 66 (CAG) encoding glutamine into a termination codon (TAG)/(Q66X). As a consequence of this mutation, the function of the KAL1 protein consisting of 680 amino acids was severely truncated so as to be consistent with Kallmann syndrome. As only this patient had unilateral renal hypoplasia among the three cases, this would suggest the existence of KAL1 gene mutation in this abnormality. (+info)Hypogonadism is a medical condition characterized by the inability of the gonads (testes in males and ovaries in females) to produce sufficient amounts of sex hormones, such as testosterone and estrogen. This can lead to various symptoms including decreased libido, erectile dysfunction in men, irregular menstrual periods in women, and reduced fertility in both sexes. Hypogonadism may be caused by genetic factors, aging, injury to the gonads, or certain medical conditions such as pituitary disorders. It can be treated with hormone replacement therapy.
Kallmann Syndrome is a genetic condition that is characterized by hypogonadotropic hypogonadism (reduced or absent function of the gonads (ovaries or testes) due to deficient secretion of pituitary gonadotropins) and anosmia or hyposmia (reduced or absent sense of smell). It is caused by abnormal migration of neurons that produce gonadotropin-releasing hormone (GnRH) during fetal development, which results in decreased production of sex hormones and delayed or absent puberty.
Kallmann Syndrome can also be associated with other symptoms such as color vision deficiency, hearing loss, renal agenesis, and neurological defects. It is typically inherited in an autosomal dominant or X-linked recessive pattern, and diagnosis usually involves a combination of clinical evaluation, hormonal testing, and genetic analysis. Treatment may include hormone replacement therapy to induce puberty and maintain sexual function, as well as management of associated symptoms.
Delayed puberty is a condition where the typical physical changes of puberty, such as the development of secondary sexual characteristics, growth spurt, and fertility, do not begin to occur during the expected age range. In medical terms, delayed puberty is defined as the absence of signs of puberty by age 13 in girls (such as breast development or menstruation) and by age 14 in boys (such as testicular enlargement or growth of facial hair).
There are various factors that can contribute to delayed puberty, including genetic conditions, chronic illnesses, hormonal imbalances, eating disorders, and excessive exercise. In some cases, the cause may be unknown. Delayed puberty can have significant emotional and social consequences for affected individuals, so it is important to seek medical evaluation and treatment if there are concerns about delayed puberty. Treatment options may include hormone replacement therapy or other interventions to support normal pubertal development.
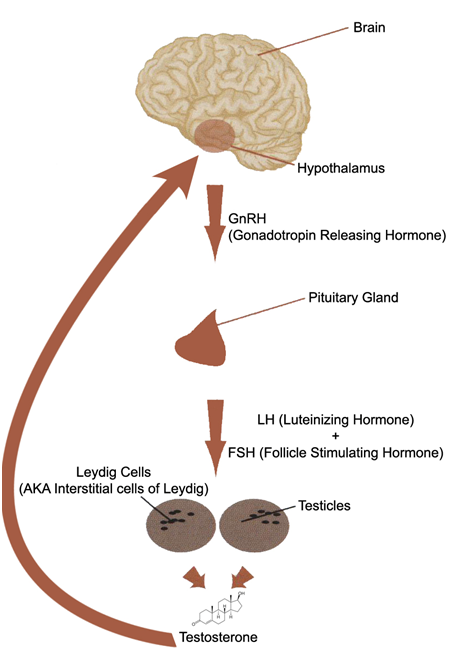
Testosterone is a steroid hormone that belongs to androsten class of hormones. It is primarily secreted by the Leydig cells in the testes of males and, to a lesser extent, by the ovaries and adrenal glands in females. Testosterone is the main male sex hormone and anabolic steroid. It plays a key role in the development of masculine characteristics, such as body hair and muscle mass, and contributes to bone density, fat distribution, red cell production, and sex drive. In females, testosterone contributes to sexual desire and bone health. Testosterone is synthesized from cholesterol and its production is regulated by luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Hormone Replacement Therapy (HRT) is a medical treatment that involves the use of hormones to replace or supplement those that the body is no longer producing or no longer producing in sufficient quantities. It is most commonly used to help manage symptoms associated with menopause and conditions related to hormonal imbalances.
In women, HRT typically involves the use of estrogen and/or progesterone to alleviate hot flashes, night sweats, vaginal dryness, and mood changes that can occur during menopause. In some cases, testosterone may also be prescribed to help improve energy levels, sex drive, and overall sense of well-being.
In men, HRT is often used to treat low testosterone levels (hypogonadism) and related symptoms such as fatigue, decreased muscle mass, and reduced sex drive.
It's important to note that while HRT can be effective in managing certain symptoms, it also carries potential risks, including an increased risk of blood clots, stroke, breast cancer (in women), and cardiovascular disease. Therefore, the decision to undergo HRT should be made carefully and discussed thoroughly with a healthcare provider.
Klinefelter Syndrome: A genetic disorder in males, caused by the presence of one or more extra X chromosomes, typically resulting in XXY karyotype. It is characterized by small testes, infertility, gynecomastia (breast enlargement), tall stature, and often mild to moderate intellectual disability. The symptoms can vary greatly among individuals with Klinefelter Syndrome. Some men may not experience any significant health problems and may never be diagnosed, while others may have serious medical or developmental issues that require treatment. It is one of the most common chromosomal disorders, affecting about 1 in every 500-1,000 newborn males.
Andropause is a term that is sometimes used to describe the gradual decrease in hormone production that occurs in middle-aged men. The term is not widely accepted or used in the medical community, and it is not officially recognized as a medical condition.
The more commonly used medical term for this phenomenon is "testosterone deficiency" or "hypogonadism," which refers to a decrease in the production of the hormone testosterone by the testes. This can lead to various symptoms such as decreased sex drive, fatigue, mood changes, and difficulty with concentration and memory.
It's important to note that while some men may experience these symptoms as they age, not all men will develop a testosterone deficiency. Additionally, other factors such as chronic medical conditions or medications can also contribute to these symptoms. A healthcare provider can evaluate symptoms and perform tests to determine if a testosterone deficiency is present and recommend appropriate treatment options.
Gonadotropins are hormones that stimulate the gonads (sex glands) to produce sex steroids and gametes (sex cells). In humans, there are two main types of gonadotropins: follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which are produced and released by the anterior pituitary gland.
FSH plays a crucial role in the development and maturation of ovarian follicles in females and sperm production in males. LH triggers ovulation in females, causing the release of a mature egg from the ovary, and stimulates testosterone production in males.
Gonadotropins are often used in medical treatments to stimulate the gonads, such as in infertility therapies where FSH and LH are administered to induce ovulation or increase sperm production.
Gonadotropin-Releasing Hormone (GnRH), also known as Luteinizing Hormone-Releasing Hormone (LHRH), is a hormonal peptide consisting of 10 amino acids. It is produced and released by the hypothalamus, an area in the brain that links the nervous system to the endocrine system via the pituitary gland.
GnRH plays a crucial role in regulating reproduction and sexual development through its control of two gonadotropins: follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These gonadotropins, in turn, stimulate the gonads (ovaries or testes) to produce sex steroids and eggs or sperm.
GnRH acts on the anterior pituitary gland by binding to its specific receptors, leading to the release of FSH and LH. The hypothalamic-pituitary-gonadal axis is under negative feedback control, meaning that when sex steroid levels are high, they inhibit the release of GnRH, which subsequently decreases FSH and LH secretion.
GnRH agonists and antagonists have clinical applications in various medical conditions, such as infertility treatments, precocious puberty, endometriosis, uterine fibroids, prostate cancer, and hormone-responsive breast cancer.
Gynecomastia is a medical term that refers to the benign enlargement of the glandular tissue in male breasts, usually caused by an imbalance of the hormones estrogen and testosterone. It's important to note that gynecomastia is not the same as having excess fat in the breast area, which is called pseudogynecomastia.
Gynecomastia can occur during infancy, puberty, or old age due to natural hormonal changes. Certain medications, medical conditions, and recreational drugs can also cause gynecomastia by affecting hormone levels in the body. In some cases, the exact cause of gynecomastia may remain unknown.
Mild cases of gynecomastia may not require treatment, but severe or persistent cases may be treated with medication or surgery to remove excess breast tissue. It's essential to consult a healthcare professional for an accurate diagnosis and appropriate treatment options if you suspect you have gynecomastia.
Eunuchism is a state of being a eunuch, which is a person who has had their gonads (testicles or ovaries) removed or damaged, typically as a castrated male. Historically, eunuchs were often employed in royal households and religious institutions due to their perceived lack of sexual desire and potential for loyalty. In modern medical terms, eunuchism may also refer to a condition where a person is born with underdeveloped or absent gonads, which can result in reduced sex hormone production and infertility.
The endocrine system is a complex network of glands and organs that produce, store, and secrete hormones. It plays a crucial role in regulating various functions in the body, including metabolism, growth and development, tissue function, sexual function, reproduction, sleep, and mood.
Endocrine system diseases or disorders occur when there is a problem with the production or regulation of hormones. This can result from:
1. Overproduction or underproduction of hormones by the endocrine glands.
2. Impaired response of target cells to hormones.
3. Disruption in the feedback mechanisms that regulate hormone production.
Examples of endocrine system diseases include:
1. Diabetes Mellitus - a group of metabolic disorders characterized by high blood sugar levels due to insulin deficiency or resistance.
2. Hypothyroidism - underactive thyroid gland leading to slow metabolism, weight gain, fatigue, and depression.
3. Hyperthyroidism - overactive thyroid gland causing rapid heartbeat, anxiety, weight loss, and heat intolerance.
4. Cushing's Syndrome - excess cortisol production resulting in obesity, high blood pressure, and weak muscles.
5. Addison's Disease - insufficient adrenal hormone production leading to weakness, fatigue, and low blood pressure.
6. Acromegaly - overproduction of growth hormone after puberty causing enlargement of bones, organs, and soft tissues.
7. Gigantism - similar to acromegaly but occurs before puberty resulting in excessive height and body size.
8. Hypopituitarism - underactive pituitary gland leading to deficiencies in various hormones.
9. Hyperparathyroidism - overactivity of the parathyroid glands causing calcium imbalances and kidney stones.
10. Precocious Puberty - early onset of puberty due to premature activation of the pituitary gland.
Treatment for endocrine system diseases varies depending on the specific disorder and may involve medication, surgery, lifestyle changes, or a combination of these approaches.
DAX-1 (Dosage-sensitive sex reversal, adrenal hypoplasia critical region, on chromosome X, gene 1) is a nuclear receptor protein that functions as a transcriptional regulator. It is also known as NR0B1 (Nuclear Receptor Subfamily 0, Group B, Member 1).
DAX-1 plays crucial roles in various developmental processes, including sexual differentiation and adrenal gland development. Mutations in the DAX-1 gene have been associated with X-linked adrenal hypoplasia congenita (AHC), a condition characterized by defective adrenal gland development and primary adrenal insufficiency.
The term "Orphan Nuclear Receptor" refers to a class of nuclear receptors for which no natural ligand has been identified yet. DAX-1 is one such orphan nuclear receptor, as its specific endogenous ligand remains unknown. However, recent studies suggest that steroids and other small molecules might interact with DAX-1 and modulate its activity.
LHRH (Luteinizing Hormone-Releasing Hormone) receptors are a type of G protein-coupled receptor found on the surface of certain cells in the body, most notably in the anterior pituitary gland. These receptors bind to LHRH, a hormone that is produced and released by the hypothalamus in the brain.
When LHRH binds to its receptor, it triggers a series of intracellular signaling events that ultimately lead to the release of two other hormones from the anterior pituitary gland: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). These hormones play critical roles in regulating reproductive function, including the development and maturation of sex cells (sperm and eggs), the production of sex steroid hormones (such as testosterone and estrogen), and the regulation of the menstrual cycle in females.
Disorders of the LHRH receptor or its signaling pathway can lead to a variety of reproductive disorders, including precocious puberty, delayed puberty, and infertility.
Erectile dysfunction (ED) is the inability to achieve or maintain an erection sufficient for satisfactory sexual performance. It can have physical and psychological causes, such as underlying health conditions like diabetes, heart disease, obesity, and mental health issues like stress, anxiety, and depression. ED can also be a side effect of certain medications. Treatment options include lifestyle changes, medication, counseling, and in some cases, surgery.
Amenorrhea is a medical condition characterized by the absence or cessation of menstrual periods in women of reproductive age. It can be categorized as primary amenorrhea, when a woman who has not yet had her first period at the expected age (usually around 16 years old), or secondary amenorrhea, when a woman who has previously had regular periods stops getting them for six months or more.
There are various causes of amenorrhea, including hormonal imbalances, pregnancy, breastfeeding, menopause, extreme weight loss or gain, eating disorders, intense exercise, stress, chronic illness, tumors, and certain medications or medical treatments. In some cases, amenorrhea may indicate an underlying medical condition that requires further evaluation and treatment.
Amenorrhea can have significant impacts on a woman's health and quality of life, including infertility, bone loss, and emotional distress. Therefore, it is essential to consult with a healthcare provider if you experience amenorrhea or missed periods to determine the underlying cause and develop an appropriate treatment plan.
Luteinizing Hormone (LH) is a glycoprotein hormone secreted by the anterior pituitary gland. It plays a crucial role in regulating the reproductive system. The beta subunit of LH is one of the two non-identical polypeptide chains that make up the LH molecule (the other being the alpha subunit, which is common to several hormones).
The beta subunit of LH is unique to LH and is often used in assays to measure and determine the concentration of LH in blood or urine. It's responsible for the biological specificity and activity of the LH hormone. Any changes in the structure of this subunit can affect the function of LH, which in turn can have implications for reproductive processes such as ovulation and testosterone production.
Follicle-Stimulating Hormone (FSH) is a glycoprotein hormone secreted and released by the anterior pituitary gland. In females, it promotes the growth and development of ovarian follicles in the ovary, which ultimately leads to the maturation and release of an egg (ovulation). In males, FSH stimulates the testes to produce sperm. It works in conjunction with luteinizing hormone (LH) to regulate reproductive processes. The secretion of FSH is controlled by the hypothalamic-pituitary-gonadal axis and its release is influenced by the levels of gonadotropin-releasing hormone (GnRH), estrogen, inhibin, and androgens.
Leuprolide is a synthetic hormonal analog of gonadotropin-releasing hormone (GnRH or LHRH). It acts as a potent agonist of GnRH receptors, leading to the suppression of pituitary gland's secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). This, in turn, results in decreased levels of sex hormones such as testosterone and estrogen.
Leuprolide is used clinically for the treatment of various conditions related to hormonal imbalances, including:
- Prostate cancer: Leuprolide can help slow down the growth of prostate cancer cells by reducing testosterone levels in the body.
- Endometriosis: By lowering estrogen levels, leuprolide can alleviate symptoms associated with endometriosis such as pelvic pain and menstrual irregularities.
- Central precocious puberty: Leuprolide is used to delay the onset of puberty in children who experience it prematurely by inhibiting the release of gonadotropins.
- Uterine fibroids: Lowering estrogen levels with leuprolide can help shrink uterine fibroids and reduce symptoms like heavy menstrual bleeding and pelvic pain.
Leuprolide is available in various formulations, such as injectable depots or implants, for long-term hormonal suppression. Common side effects include hot flashes, mood changes, and potential loss of bone density due to prolonged hormone suppression.
CHARGE syndrome is a genetic disorder that is associated with a variety of birth defects and medical issues. The name CHARGE is an acronym that stands for:
* Coloboma of the eye, which is a hole in the structure of the eye that is present at birth.
* Heart defects, which can range from mild to severe.
* Atresia of the choanae, which is the absence or closure of the nasal passages.
* Retardation of growth and/or development.
* Genital and/or urinary abnormalities.
* Ear abnormalities and deafness.
CHARGE syndrome is caused by mutations in the CHD7 gene, which is located on chromosome 8. This gene provides instructions for making a protein that is involved in the development of the eyes, ears, and other parts of the body. Mutations in the CHD7 gene can lead to the characteristic features of CHARGE syndrome.
CHARGE syndrome is typically diagnosed based on the presence of certain physical characteristics and medical issues. A genetic test can be done to confirm the diagnosis and identify the specific mutation that is causing the disorder.
Treatment for CHARGE syndrome depends on the severity of the symptoms and may include surgery, therapy, and other medical interventions. With appropriate care, many people with CHARGE syndrome are able to lead fulfilling lives.
Olfaction disorders, also known as smell disorders, refer to conditions that affect the ability to detect or interpret odors. These disorders can be categorized into two main types:
1. Anosmia: This is a complete loss of the sense of smell. It can be caused by various factors such as nasal polyps, sinus infections, head injuries, and degenerative diseases like Alzheimer's and Parkinson's.
2. Hyposmia: This is a reduced ability to detect odors. Like anosmia, it can also be caused by similar factors including aging and exposure to certain chemicals.
Other olfaction disorders include parosmia, which is a distortion of smell where individuals may perceive a smell as being different from its original scent, and phantosmia, which is the perception of a smell that isn't actually present.
Luteinizing Hormone (LH) is a glycoprotein hormone, which is primarily produced and released by the anterior pituitary gland. In women, a surge of LH triggers ovulation, the release of an egg from the ovaries during the menstrual cycle. During pregnancy, LH stimulates the corpus luteum to produce progesterone. In men, LH stimulates the testes to produce testosterone. It plays a crucial role in sexual development, reproduction, and maintaining the reproductive system.
Hypopituitarism is a medical condition characterized by deficient secretion of one or more hormones produced by the pituitary gland, a small endocrine gland located at the base of the brain. The pituitary gland controls several other endocrine glands in the body, including the thyroid, adrenals, and sex glands (ovaries and testes).
Hypopituitarism can result from damage to the pituitary gland due to various causes such as tumors, surgery, radiation therapy, trauma, or inflammation. In some cases, hypopituitarism may also be caused by a dysfunction of the hypothalamus, a region in the brain that regulates the pituitary gland's function.
The symptoms and signs of hypopituitarism depend on which hormones are deficient and can include fatigue, weakness, decreased appetite, weight loss, low blood pressure, decreased sex drive, infertility, irregular menstrual periods, intolerance to cold, constipation, thinning hair, dry skin, and depression.
Treatment of hypopituitarism typically involves hormone replacement therapy to restore the deficient hormones' normal levels. The type and dosage of hormones used will depend on which hormones are deficient and may require regular monitoring and adjustments over time.
Libido, in medical and psychological terms, refers to a person's overall sexual drive or desire for sexual activity. This term was first introduced by Sigmund Freud in his psychoanalytic theory, where he described it as one of the three components of human personality. Libido is influenced by biological, psychological, and social factors, and can vary significantly among individuals. It's important to note that a low or absent libido does not necessarily indicate an underlying medical issue, but could be a result of various factors such as stress, fatigue, relationship issues, mental health disorders, or hormonal imbalances. If you have concerns about your libido, it is recommended to consult with a healthcare professional for a proper evaluation and guidance.
Sex Hormone-Binding Globulin (SHBG) is a protein produced mainly in the liver that plays a crucial role in regulating the active forms of the sex hormones, testosterone and estradiol, in the body. SHBG binds to these hormones in the bloodstream, creating a reservoir of bound hormones. Only the unbound (or "free") fraction of testosterone and estradiol is considered biologically active and can easily enter cells to exert its effects.
By binding to sex hormones, SHBG helps control their availability and transport in the body. Factors such as age, sex, infection with certain viruses (like hepatitis or HIV), liver disease, obesity, and various medications can influence SHBG levels and, consequently, impact the amount of free testosterone and estradiol in circulation.
SHBG is an essential factor in maintaining hormonal balance and has implications for several physiological processes, including sexual development, reproduction, bone health, muscle mass, and overall well-being. Abnormal SHBG levels can contribute to various medical conditions, such as hypogonadism (low testosterone levels), polycystic ovary syndrome (PCOS), and certain types of cancer.
Hypothalamic diseases refer to conditions that affect the hypothalamus, a small but crucial region of the brain responsible for regulating many vital functions in the body. The hypothalamus helps control:
1. Body temperature
2. Hunger and thirst
3. Sleep cycles
4. Emotions and behavior
5. Release of hormones from the pituitary gland
Hypothalamic diseases can be caused by genetic factors, infections, tumors, trauma, or other conditions that damage the hypothalamus. Some examples of hypothalamic diseases include:
1. Hypothalamic dysfunction syndrome: A condition characterized by various symptoms such as obesity, sleep disturbances, and hormonal imbalances due to hypothalamic damage.
2. Kallmann syndrome: A genetic disorder that affects the development of the hypothalamus and results in a lack of sexual maturation and a decreased sense of smell.
3. Prader-Willi syndrome: A genetic disorder that causes obesity, developmental delays, and hormonal imbalances due to hypothalamic dysfunction.
4. Craniopharyngiomas: Tumors that develop near the pituitary gland and hypothalamus, often causing visual impairment, hormonal imbalances, and growth problems.
5. Infiltrative diseases: Conditions such as sarcoidosis or histiocytosis can infiltrate the hypothalamus, leading to various symptoms related to hormonal imbalances and neurological dysfunction.
6. Traumatic brain injury: Damage to the hypothalamus due to head trauma can result in various hormonal and neurological issues.
7. Infections: Bacterial or viral infections that affect the hypothalamus, such as encephalitis or meningitis, can cause damage and lead to hypothalamic dysfunction.
Treatment for hypothalamic diseases depends on the underlying cause and may involve medications, surgery, hormone replacement therapy, or other interventions to manage symptoms and improve quality of life.
Puberty is the period of sexual maturation, generally occurring between the ages of 10 and 16 in females and between 12 and 18 in males. It is characterized by a series of events including rapid growth, development of secondary sexual characteristics, and the acquisition of reproductive capabilities. Puberty is initiated by the activation of the hypothalamic-pituitary-gonadal axis, leading to the secretion of hormones such as estrogen and testosterone that drive the physical changes associated with this stage of development.
In females, puberty typically begins with the onset of breast development (thelarche) and the appearance of pubic hair (pubarche), followed by the start of menstruation (menarche). In males, puberty usually starts with an increase in testicular size and the growth of pubic hair, followed by the deepening of the voice, growth of facial hair, and the development of muscle mass.
It's important to note that the onset and progression of puberty can vary widely among individuals, and may be influenced by genetic, environmental, and lifestyle factors.
Gonadotropins are hormones produced and released by the anterior pituitary gland, a small endocrine gland located at the base of the brain. These hormones play crucial roles in regulating reproduction and sexual development. There are two main types of gonadotropins:
1. Follicle-Stimulating Hormone (FSH): FSH is essential for the growth and development of follicles in the ovaries (in females) or sperm production in the testes (in males). In females, FSH stimulates the maturation of eggs within the follicles.
2. Luteinizing Hormone (LH): LH triggers ovulation in females, causing the release of a mature egg from the dominant follicle. In males, LH stimulates the production and secretion of testosterone in the testes.
Together, FSH and LH work synergistically to regulate various aspects of reproductive function and sexual development. Their secretion is controlled by the hypothalamus, which releases gonadotropin-releasing hormone (GnRH) to stimulate the production and release of FSH and LH from the anterior pituitary gland.
Abnormal levels of gonadotropins can lead to various reproductive disorders, such as infertility or menstrual irregularities in females and issues related to sexual development or function in both sexes. In some cases, synthetic forms of gonadotropins may be used clinically to treat these conditions or for assisted reproductive technologies (ART).
Kisspeptins are a family of peptides that are derived from the preproprotein kisspeptin. The most well-known member of this family is kisspeptin-54, which is also known as metastin. Kisspeptins play important roles in several physiological processes, including the regulation of growth, inflammation, and energy homeostasis. However, they are perhaps best known for their role in the reproductive system.
In the reproductive system, kisspeptins act as key regulators of the hypothalamic-pituitary-gonadal (HPG) axis, which is responsible for controlling reproductive function. Kisspeptins are produced by neurons in the hypothalamus and bind to receptors on other neurons that release gonadotropin-releasing hormone (GnRH). GnRH then stimulates the pituitary gland to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which act on the gonads to promote the production of sex steroids and eggs or sperm.
Dysregulation of the HPG axis, including abnormal kisspeptin signaling, has been implicated in a number of reproductive disorders, such as precocious puberty, delayed puberty, and infertility. As such, there is significant interest in understanding the role of kisspeptins in reproductive function and developing therapies that target this pathway.
Male infertility is a condition characterized by the inability to cause pregnancy in a fertile female. It is typically defined as the failure to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse.
The causes of male infertility can be varied and include issues with sperm production, such as low sperm count or poor sperm quality, problems with sperm delivery, such as obstructions in the reproductive tract, or hormonal imbalances that affect sperm production. Other factors that may contribute to male infertility include genetic disorders, environmental exposures, lifestyle choices, and certain medical conditions or treatments.
It is important to note that male infertility can often be treated or managed with medical interventions, such as medication, surgery, or assisted reproductive technologies (ART). A healthcare provider can help diagnose the underlying cause of male infertility and recommend appropriate treatment options.
Androgens are a class of hormones that are primarily responsible for the development and maintenance of male sexual characteristics and reproductive function. Testosterone is the most well-known androgen, but other androgens include dehydroepiandrosterone (DHEA), androstenedione, and dihydrotestosterone (DHT).
Androgens are produced primarily by the testes in men and the ovaries in women, although small amounts are also produced by the adrenal glands in both sexes. They play a critical role in the development of male secondary sexual characteristics during puberty, such as the growth of facial hair, deepening of the voice, and increased muscle mass.
In addition to their role in sexual development and function, androgens also have important effects on bone density, mood, and cognitive function. Abnormal levels of androgens can contribute to a variety of medical conditions, including infertility, erectile dysfunction, acne, hirsutism (excessive hair growth), and prostate cancer.
The testis, also known as the testicle, is a male reproductive organ that is part of the endocrine system. It is located in the scrotum, outside of the abdominal cavity. The main function of the testis is to produce sperm and testosterone, the primary male sex hormone.
The testis is composed of many tiny tubules called seminiferous tubules, where sperm are produced. These tubules are surrounded by a network of blood vessels, nerves, and supportive tissues. The sperm then travel through a series of ducts to the epididymis, where they mature and become capable of fertilization.
Testosterone is produced in the Leydig cells, which are located in the interstitial tissue between the seminiferous tubules. Testosterone plays a crucial role in the development and maintenance of male secondary sexual characteristics, such as facial hair, deep voice, and muscle mass. It also supports sperm production and sexual function.
Abnormalities in testicular function can lead to infertility, hormonal imbalances, and other health problems. Regular self-examinations and medical check-ups are recommended for early detection and treatment of any potential issues.
Fibroblast Growth Factor Receptor 1 (FGFR1) is a type of receptor tyrosine kinase that plays a crucial role in various biological processes such as cell survival, proliferation, differentiation, and migration. It is a transmembrane protein that binds to fibroblast growth factors (FGFs), leading to the activation of intracellular signaling pathways.
FGFR1 is specifically involved in the regulation of embryonic development, tissue repair, and angiogenesis. Mutations in the FGFR1 gene have been associated with several human diseases, including various types of cancer, skeletal dysplasias, and developmental disorders.
In summary, Fibroblast Growth Factor Receptor 1 (FGFR1) is a cell surface receptor that binds to fibroblast growth factors (FGFs) and activates intracellular signaling pathways involved in various biological processes, including cell survival, proliferation, differentiation, and migration.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Gonadal disorders refer to conditions that affect the function or structure of the gonads, which are the primary reproductive organs. In females, the gonads are the ovaries, and in males, they are the testes. These disorders can result in issues related to sexual development, reproduction, and hormone production.
Examples of gonadal disorders include:
1. Ovarian dysfunction: This includes conditions such as polycystic ovary syndrome (PCOS), premature ovarian failure, and ovarian insufficiency, which can affect menstruation, fertility, and hormone levels.
2. Testicular disorders: These include conditions such as undescended testes, Klinefelter syndrome, and varicocele, which can impact sperm production, male secondary sexual characteristics, and hormone levels.
3. Gonadal dysgenesis: This is a condition where the gonads do not develop properly during fetal development, leading to ambiguous genitalia or sex chromosome abnormalities.
4. Cancer of the gonads: Both ovarian and testicular cancers can affect gonadal function and require prompt medical attention.
5. Gonadal injury or trauma: Injuries to the gonads can impact their function, leading to fertility issues or hormonal imbalances.
Treatment for gonadal disorders depends on the specific condition and its severity. It may involve medications, surgery, hormone replacement therapy, or assisted reproductive technologies.
Adrenal insufficiency is a condition in which the adrenal glands do not produce adequate amounts of certain hormones, primarily cortisol and aldosterone. Cortisol helps regulate metabolism, respond to stress, and suppress inflammation, while aldosterone helps regulate sodium and potassium levels in the body to maintain blood pressure.
Primary adrenal insufficiency, also known as Addison's disease, occurs when there is damage to the adrenal glands themselves, often due to autoimmune disorders, infections, or certain medications. Secondary adrenal insufficiency occurs when the pituitary gland fails to produce enough adrenocorticotropic hormone (ACTH), which stimulates the adrenal glands to produce cortisol.
Symptoms of adrenal insufficiency may include fatigue, weakness, weight loss, decreased appetite, nausea, vomiting, diarrhea, abdominal pain, low blood pressure, dizziness, and darkening of the skin. Treatment typically involves replacing the missing hormones with medications taken orally or by injection.
Prader-Willi Syndrome (PWS) is a genetic disorder that affects several parts of the body and is characterized by a range of symptoms including:
1. Developmental delays and intellectual disability.
2. Hypotonia (low muscle tone) at birth, which can lead to feeding difficulties in infancy.
3. Excessive appetite and obesity, typically beginning around age 2, due to a persistent hunger drive and decreased satiety.
4. Behavioral problems such as temper tantrums, stubbornness, and compulsive behaviors.
5. Hormonal imbalances leading to short stature, small hands and feet, incomplete sexual development, and decreased bone density.
6. Distinctive facial features including a thin upper lip, almond-shaped eyes, and a narrowed forehead.
7. Sleep disturbances such as sleep apnea or excessive daytime sleepiness.
PWS is caused by the absence of certain genetic material on chromosome 15, which results in abnormal gene function. It affects both males and females equally and has an estimated incidence of 1 in 10,000 to 30,000 live births. Early diagnosis and management can help improve outcomes for individuals with PWS.
Gonadal dysgenesis, 46,XX is a medical condition where an individual with a 46,XX karyotype has underdeveloped or absent gonads (ovaries). Normally, individuals with a 46,XX karyotype have ovaries that produce female sex hormones and develop into reproductive organs. However, in cases of gonadal dysgenesis, the gonads do not develop properly and may appear as streak gonads, which lack germ cells and are incapable of producing sex hormones or gametes (eggs).
Individuals with 46,XX gonadal dysgenesis often have female external genitalia but may have primary amenorrhea (absence of menstruation) due to the underdeveloped or absent ovaries. They may also have other features such as short stature, webbed neck, and intellectual disability, depending on the underlying cause of the condition.
The underlying causes of 46,XX gonadal dysgenesis can vary, including genetic mutations, chromosomal abnormalities, or exposure to environmental factors during fetal development. Some individuals with this condition may have an increased risk of developing gonadal tumors, so regular monitoring and follow-up care are essential.
I must clarify that the term "pedigree" is not typically used in medical definitions. Instead, it is often employed in genetics and breeding, where it refers to the recorded ancestry of an individual or a family, tracing the inheritance of specific traits or diseases. In human genetics, a pedigree can help illustrate the pattern of genetic inheritance in families over multiple generations. However, it is not a medical term with a specific clinical definition.
Hyperprolactinemia is a medical condition characterized by abnormally high levels of prolactin, a hormone produced by the pituitary gland. In women, this can lead to menstrual irregularities, milk production outside of pregnancy (galactorrhea), and infertility. In men, it can cause decreased libido, erectile dysfunction, breast enlargement (gynecomastia), and infertility. The condition can be caused by various factors, including pituitary tumors, certain medications, and hypothyroidism. Treatment typically involves addressing the underlying cause and may include medication to lower prolactin levels.
Sex chromosome aberrations refer to structural and numerical abnormalities in the sex chromosomes, which are typically represented as X and Y chromosomes in humans. These aberrations can result in variations in the number of sex chromosomes, such as Klinefelter syndrome (47,XXY), Turner syndrome (45,X), and Jacobs/XYY syndrome (47,XYY). They can also include structural changes, such as deletions, duplications, or translocations of sex chromosome material.
Sex chromosome aberrations may lead to a range of phenotypic effects, including differences in physical characteristics, cognitive development, fertility, and susceptibility to certain health conditions. The manifestation and severity of these impacts can vary widely depending on the specific type and extent of the aberration, as well as individual genetic factors and environmental influences.
It is important to note that while sex chromosome aberrations may pose challenges and require medical management, they do not inherently define or limit a person's potential, identity, or worth. Comprehensive care, support, and education can help individuals with sex chromosome aberrations lead fulfilling lives and reach their full potential.
The pituitary gland is a small, endocrine gland located at the base of the brain, in the sella turcica of the sphenoid bone. It is often called the "master gland" because it controls other glands and makes the hormones that trigger many body functions. The pituitary gland measures about 0.5 cm in height and 1 cm in width, and it weighs approximately 0.5 grams.
The pituitary gland is divided into two main parts: the anterior lobe (adenohypophysis) and the posterior lobe (neurohypophysis). The anterior lobe is further divided into three zones: the pars distalis, pars intermedia, and pars tuberalis. Each part of the pituitary gland has distinct functions and produces different hormones.
The anterior pituitary gland produces and releases several important hormones, including:
* Growth hormone (GH), which regulates growth and development in children and helps maintain muscle mass and bone strength in adults.
* Thyroid-stimulating hormone (TSH), which controls the production of thyroid hormones by the thyroid gland.
* Adrenocorticotropic hormone (ACTH), which stimulates the adrenal glands to produce cortisol and other steroid hormones.
* Follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which regulate reproductive function in both males and females.
* Prolactin, which stimulates milk production in pregnant and lactating women.
The posterior pituitary gland stores and releases two hormones that are produced by the hypothalamus:
* Antidiuretic hormone (ADH), which helps regulate water balance in the body by controlling urine production.
* Oxytocin, which stimulates uterine contractions during childbirth and milk release during breastfeeding.
Overall, the pituitary gland plays a critical role in maintaining homeostasis and regulating various bodily functions, including growth, development, metabolism, and reproductive function.
 Hypogonadism
Hypogonadism Hypogonadism | Medscape
Hypogonadism | Medscape Hypogonadism: MedlinePlus Medical Encyclopedia
Hypogonadism: MedlinePlus Medical Encyclopedia Hypogonadism Clinical Research Trials | CenterWatch
Hypogonadism Clinical Research Trials | CenterWatch Is male hypogonadism a risk factor for hospitalization for COVID-19?
Is male hypogonadism a risk factor for hospitalization for COVID-19? Clomid dosage male hypogonadism
Clomid dosage male hypogonadism Hypogonadism | Condition | UAMS Health
Hypogonadism | Condition | UAMS Health Frontiers | The relationship between exposure to phthalate metabolites and adult-onset hypogonadism
Frontiers | The relationship between exposure to phthalate metabolites and adult-onset hypogonadism New and Consolidated Therapeutic Options for Pubertal Induction in Hypogonadism: In-depth Review of the Literature
New and Consolidated Therapeutic Options for Pubertal Induction in Hypogonadism: In-depth Review of the Literature Understanding Hypogonadism (Low Testosterone) - Cleveland Clinic
Understanding Hypogonadism (Low Testosterone) - Cleveland Clinic FDA approves oral testosterone replacement therapy for hypogonadism
FDA approves oral testosterone replacement therapy for hypogonadism Hypogonadism in young men treated for cancer.<...
Hypogonadism in young men treated for cancer.<... Hypogonadism | Ask or chat with U.S. doctors on HealthTap
Hypogonadism | Ask or chat with U.S. doctors on HealthTap Identification of Late-Onset Hypogonadism in Middle-Aged and Elderly Men | Lund University Publications
Identification of Late-Onset Hypogonadism in Middle-Aged and Elderly Men | Lund University Publications Global Male Hypogonadism Market: Growth Demand & Forecast | Persistence Market Research (PMR)
Global Male Hypogonadism Market: Growth Demand & Forecast | Persistence Market Research (PMR) Information for Hypogonadism male
Information for Hypogonadism male JCI Insight -
Defective jagged-1 signaling affects GnRH development and contributes to congenital hypogonadotropic hypogonadism
JCI Insight -
Defective jagged-1 signaling affects GnRH development and contributes to congenital hypogonadotropic hypogonadism Hypogonadism in Prader‑Willi Syndrome
Hypogonadism in Prader‑Willi Syndrome Unilaterally Disrupted Structural and Functional Connectivity of The Fronto-Iimbic System In Idiopathic Hypogonadotropic...
Unilaterally Disrupted Structural and Functional Connectivity of The Fronto-Iimbic System In Idiopathic Hypogonadotropic... VisualAbstract: Testosterone-replacement therapy for middle-aged and older men with hypogonadism does not increase risk of...
VisualAbstract: Testosterone-replacement therapy for middle-aged and older men with hypogonadism does not increase risk of... Hypogonadism; What is it, symptoms and treatment
Hypogonadism; What is it, symptoms and treatment Aveed (testosterone undecanoate) for the Treatment of Men with Hypogonadism - Clinical Trials Arena
Aveed (testosterone undecanoate) for the Treatment of Men with Hypogonadism - Clinical Trials Arena "Low T? Late Onset Hypogonadism" by Cheng-Wei Huang
"Low T? Late Onset Hypogonadism" by Cheng-Wei Huang Male Hypogonadism Market - Request for covid19 Impact Analysis
Male Hypogonadism Market - Request for covid19 Impact Analysis