Gait Disorders, Neurologic
Gait Ataxia
Gait Apraxia
Walking
Biomechanical Phenomena
Postural Balance
Orthotic Devices
Ankle Joint
Locomotion
Foot
Amputees
Paresis
Hemiplegia
Range of Motion, Articular
Cerebral Palsy
Parkinson Disease
Robotics
Shoes
Hip Joint
Weight-Bearing
Foot Orthoses
Physical Therapy Modalities
Exercise Therapy
Electromyography
Movement Disorders
Visual control of locomotion in Parkinson's disease. (1/2687)
The effect of placing parallel lines on the walking surface on parkinsonian gait was evaluated. To identify the kind of visual cues (static or dynamic) required for the control of locomotion, we tested two visual conditions: normal lighting and stroboscopic illumination (three flashes/s), the latter acting to suppress dynamic visual cues completely. Sixteen subjects with idiopathic Parkinson's disease (nine males, seven females; mean age 68.8 years) and the same number of age-matched controls (seven males; nine females, mean age 67.5 years) were studied. During the baseline phase, Parkinson's disease patients walked with a short-stepped, slow velocity pattern. The double limb support duration was increased and the step cadence was reduced relative to normal. Under normal lighting, visual cues from the lines on the walking surface induced a significant improvement in gait velocity and stride length in Parkinson's disease patients. With stroboscopic illumination and without lines, both groups reduced their stride length and velocity but the changes were significant only in the Parkinson's disease group, indicating greater dependence on dynamic visual information. When stroboscopic light was used with stripes on the floor, the improvement in gait due to the stripes was suppressed in parkinsonian patients. These results demonstrate that the perceived motion of stripes, induced by the patient's walking, is essential to improve the gait parameters and thus favour the hypothesis of a specific visual-motor pathway which is particularly responsive to rapidly moving targets. Previous studies have proposed a cerebellar circuit, allowing the visual stimuli to by-pass the damaged basal ganglia. (+info)Development of a 12-min treadmill walk test at a self-selected pace for the evaluation of cardiorespiratory fitness in adult men. (2/2687)
The direct measurement of true maximal oxygen uptake (VO2max) and oxygen uptake corresponding to anaerobic threshold (VO2AT) is not always practical, especially in middle age and older populations. Therefore, the purpose of this study was to develop a simple test that could accurately estimate cardiorespiratory fitness using a submaximal treadmill walking protocol for middle age, older, sedentary individuals and patients with chronic disease. Subjects for this study were 42 men (44.9 +/- 15.7 years), which included 17 patients with coronary heart disease (57.0 +/- 9.6 years). VO2peak and VO2AT were measured using a treadmill protocol (VO2peak; 38.4 +/- 11.6 ml/kg/min, VO2AT; 22.9 +/- 7.4 ml/kg/min). This simple test assessed the total distance covered in 12 minutes on the treadmill at an intensity corresponding to either 1) 11 on the Borg scale of ratings of perceived exertion (RPE11), 2) 13 on the Borg scale of ratings of perceived exertion (RPE13), or 3) "Optimal" by subjective judgment. The correlation coefficients between VO2peak or VO2AT and total distance at the three intensities (RPE11; 950 +/- 100 m, RPE13; 1080 +/- 140 m Optimal; 1050 +/- 110 m) were statistically significant, ranging from 0.72 to 0.85. The test-retest reliability coefficient on 12 subjects was 0.98. The oxygen uptake (VO2) was measured during the three walk tests on 15 subjects. There were no significant changes in submaximal VO2 values from min 4 to min 12 (RPE11; 19.8 +/- 4.7 ml/kg/min, RPE13; 24.1 +/- 4.9 ml/kg/min, Optimal; 23.1 +/- 4.8 ml/kg/min) in any of the three tests. Similarly, the three submaximal VO2 values did not differ from the VO2AT value (21.2 +/- 8.3 ml/kg/min) obtained in the initial maximal test. These results suggest that the 12-min submaximal treadmill walk test (STWT) is a valid method for the assessment of VO2peak and VO2AT. Therefore, the STWT could be a useful performance test for evaluating cardiorespiratory fitness in middle age, older, sedentary individuals and patients with chronic disease. (+info)Maturation of gait dynamics: stride-to-stride variability and its temporal organization in children. (3/2687)
In very young children, immature control of posture and gait results in unsteady locomotion. In children of approximately 3 yr of age, gait appears relatively mature; however, it is unknown whether the dynamics of walking change beyond this age. Because stride dynamics depend on neural control, we hypothesized that motor control would continue to develop beyond age 3. To test this hypothesis, we measured the gait cycle duration on a stride-by-stride basis in 50 healthy 3- to 14-yr-old children (25 girls). Measurements of stride-to-stride variability were significantly larger both in the 3- and 4-yr-old children, compared with the 6- and 7-yr-old children, and in the 6- and 7-yr-old children, compared with the 11- to 14-yr-old children. Measurements of the temporal organization of gait also revealed significant age-dependent changes. The effects of age persisted even after adjusting for height. These findings indicate that mature stride dynamics may not be completely developed even in healthy 7-yr-old children and that different aspects of stride dynamics mature at different ages. (+info)A clinical guide to assess the role of lower limb extensor overactivity in hemiplegic gait disorders. (4/2687)
BACKGROUND AND PURPOSE: The aim of this study was to assess the role of knee and ankle extensor overactivity in the hemiplegic gait observed in stroke victims and to propose a clinical guide for selecting patients before treatment of a supposed disabling spasticity. METHODS: A standardized physical examination procedure was performed in 135 consecutive stroke patients. All patients were able to walk without human assistance. The period after stroke ranged from 3 to 24 months (mean, 11.5+/-7.25 months). Spasticity was evaluated with the stroke victim in sitting position and during walking. Overactivity of the quadriceps was considered disabling when inducing inability to flex the knee during the swing phase despite adequate control of knee flexion in sitting and standing positions; overactivity of the triceps surae was considered to be disabling when heel strike was not possible despite good control of the ankle flexion in sitting position; triceps retraction was also considered. RESULTS: Disabling overactivity was observed in 56 (41.5%) patients: 11 times for the quadriceps femoris, 21 times for the triceps surae, and 21 times for both muscles. It was considered to be the main disorder impairing gait among only 16 (12%) patients: 9 for the quadriceps alone, 3 for the triceps alone, and 4 for both. Sitting spasticity of the lower limb was not predictive of disabling overactivity during walking. CONCLUSIONS: Extensor muscle overactivity is one of the components of gait disorders in stroke patients. The difficulty in assessing spasticity and its real causal effect in gait disturbances are discussed. A clinical guide is proposed. (+info)Standard osteopathic manipulative treatment acutely improves gait performance in patients with Parkinson's disease. (5/2687)
Patients with Parkinson's disease exhibit a variety of motor deficits which can ultimately result in complete disability. The primary objective of this study was to quantitatively evaluate the effect of osteopathic manipulative treatment (OMT) on the gait of patients with Parkinson's disease. Ten patients with idiopathic Parkinson's disease and a group of eight age-matched normal control subjects were subjected to an analysis of gait before and after a single session of an OMT protocol. A separate group of 10 patients with Parkinson's disease was given a sham-control procedure and tested in the same manner. In the treated group of patients with Parkinson's disease, statistically significant increases were observed in stride length, cadence, and the maximum velocities of upper and lower extremities after treatment. There were no significant differences observed in the control groups. The data demonstrate that a single session of an OMT protocol has an immediate impact on Parkinsonian gait. Osteopathic manipulation may be an effective physical treatment method in the management of movement deficits in patients with Parkinson's disease. (+info)Relationship of lesion location to clinical outcome following microelectrode-guided pallidotomy for Parkinson's disease. (6/2687)
The purpose of this study was to examine the relationship between lesion location and clinical outcome following globus pallidus internus (GPi) pallidotomy for advanced Parkinson's disease. Thirty-three patients were prospectively studied with extensive neurological examinations before and at 6 and 12 months following microelectrode-guided pallidotomy. Lesion location was characterized using volumetric MRI. The position of lesions within the posteroventral region of the GPi was measured, from anteromedial to posterolateral along an axis parallel to the internal capsule. To relate lesion position to clinical outcome, hierarchical multiple regression analysis was used. The variance in outcome measures that was related to preoperative scores and lesion volume was first calculated, and then the remaining variance attributable to lesion location was determined. Lesion location along the anteromedial-to-posterolateral axis within the GPi influenced the variance in total score on the Unified Parkinson's Disease Rating Scale in the postoperative 'off' period, and in 'on' period dyskinesia scores. Within the posteroventral GPi, anteromedial lesions were associated with greater improvement in 'off' period contralateral rigidity and 'on' period dyskinesia, whereas more centrally located lesions correlated with better postoperative scores of contralateral akinesia and postural instability/gait disturbance. Improvement in contralateral tremor was weakly related to lesion location, being greater with posterolateral lesions. We conclude that improvement in specific motor signs in Parkinson's disease following pallidotomy is related to lesion position within the posteroventral GPi. These findings are consistent with the known segregated but parallel organization of specific motor circuits in the basal ganglia, and may explain the variability in clinical outcome after pallidotomy and therefore have important therapeutic implications. (+info)Reassessment of unilateral pallidotomy in Parkinson's disease. A 2-year follow-up study. (7/2687)
Unilateral pallidotomy has gained popularity in treating the motor symptoms of Parkinson's disease. We present the results of a 2-year post-pallidotomy follow-up study. Using the Unified Parkinson's Disease Rating Scale (UPDRS), the Goetz dyskinesia scale and the Purdue Pegboard Test (PPBT), we evaluated 20 patients at regular intervals both off and on medications for 2 years post-pallidotomy. There were no significant changes in the dosages of antiparkinsonian medications from 3 months pre-pallidotomy to 2 years post-pallidotomy. On the side contralateral to the operation, the improvements were preserved in 'on'-state dyskinesia (83% reduction from pre-pallidotomy to 2 years post-pallidotomy, P < 0.001) and 'off'-state tremor (90% reduction from pre-pallidotomy to 2 years post-pallidotomy, P = 0.005). There were no statistically significant differences between pre-pallidotomy scores and those at 2 years post-pallidotomy in ipsilateral dyskinesia, axial dyskinesia, 'off'- or 'on'-state PPBT, 'off'-state Activities of Daily Living (ADL) and 'off'-state gait and postural stability. After 2 years, the 'on'-state ADL scores worsened by 75%, compared with pre-pallidotomy (P = 0.005). We conclude that 2 years after pallidotomy, the improvements in dyskinesia and tremor on the side contralateral to pallidotomy are preserved, while the initial improvements in most other deficits disappear, either because of progression of pathology or loss of the early efficacy achieved by surgery. (+info)Impaired modulation of quadriceps tendon jerk reflex during spastic gait: differences between spinal and cerebral lesions. (8/2687)
In healthy subjects, functionally appropriate modulation of short latency leg muscle reflexes occurs during gait. This modulation has been ascribed, in part, to changes in presynaptic inhibition of Ia afferents. The changes in modulation of quadriceps tendon jerk reflexes during gait of healthy subjects were compared with those of hemi- or paraparetic spastic patients. The spasticity was due to unilateral cerebral infarction or traumatic spinal cord injury, respectively. The modulation of the quadriceps femoris tendon jerk reflex at 16 phases of the step cycle was studied. The reflex responses obtained during treadmill walking were compared with control values obtained during gait-mimicking standing postures with corresponding levels of voluntary muscle contraction and knee angles. In healthy subjects the size of the reflexes was profoundly modulated and was generally depressed throughout the step cycle. In patients with spinal lesion the reflex depression during gait was almost removed and was associated with weak or no modulation during the step cycle. In patients with cerebral lesion there was less depression of the reflex size associated with a reduced reflex modulation on the affected side compared with healthy subjects. On the 'unaffected' side of these patients reflex modulation was similar to that of healthy subjects, but the reflex size during gait was not significantly different from standing control values. These observations suggest that the mechanisms responsible for the depression of reflex size and the modulation normally seen during gait in healthy subjects are impaired to different extents in spasticity of spinal or cerebral origin, possibly due to the unilateral preservation of fibre tracts in hemiparesis. (+info)Gait is a medical term used to describe the pattern of movement of the limbs during walking or running. It includes the manner or style of walking, including factors such as rhythm, speed, and step length. A person's gait can provide important clues about their physical health and neurological function, and abnormalities in gait may indicate the presence of underlying medical conditions, such as neuromuscular disorders, orthopedic problems, or injuries.
A typical human gait cycle involves two main phases: the stance phase, during which the foot is in contact with the ground, and the swing phase, during which the foot is lifted and moved forward in preparation for the next step. The gait cycle can be further broken down into several sub-phases, including heel strike, foot flat, midstance, heel off, and toe off.
Gait analysis is a specialized field of study that involves observing and measuring a person's gait pattern using various techniques, such as video recordings, force plates, and motion capture systems. This information can be used to diagnose and treat gait abnormalities, improve mobility and function, and prevent injuries.
A gait disorder is a disturbance in the ability to walk that can't be attributed to physical disabilities such as weakness or paralysis. Neurologic gait disorders are those specifically caused by underlying neurological conditions. These disorders can result from damage to the brain, spinal cord, or peripheral nerves that disrupts communication between the muscles and the brain.
Neurologic gait disorders can present in various ways, including:
1. **Spastic Gait:** This is a stiff, foot-dragging walk caused by increased muscle tone (hypertonia) and stiffness (spasticity). It's often seen in conditions like cerebral palsy or multiple sclerosis.
2. **Ataxic Gait:** This is a broad-based, unsteady, and irregular walk caused by damage to the cerebellum, which affects balance and coordination. Conditions such as cerebellar atrophy or stroke can cause this type of gait disorder.
3. **Parkinsonian Gait:** This is a shuffling walk with small steps, flexed knees, and difficulty turning. It's often seen in Parkinson's disease.
4. **Neuropathic Gait:** This is a high-stepping walk caused by foot drop (difficulty lifting the front part of the foot), which results from damage to the peripheral nerves. Conditions such as diabetic neuropathy or Guillain-Barre syndrome can cause this type of gait disorder.
5. **Choreic Gait:** This is an irregular, dance-like walk caused by involuntary movements (chorea) seen in conditions like Huntington's disease.
6. **Mixed Gait:** Sometimes, a person may exhibit elements of more than one type of gait disorder.
The specific type of gait disorder can provide important clues about the underlying neurological condition and help guide diagnosis and treatment.
Gait ataxia is a type of ataxia, which refers to a lack of coordination or stability, specifically involving walking or gait. It is characterized by an unsteady, uncoordinated, and typically wide-based gait pattern. This occurs due to dysfunction in the cerebellum or its connecting pathways, responsible for maintaining balance and coordinating muscle movements.
In gait ataxia, individuals often have difficulty with controlling the rhythm and pace of their steps, tend to veer or stagger off course, and may display a reeling or stumbling motion while walking. They might also have trouble performing rapid alternating movements like quickly tapping their foot or heel. These symptoms are usually worse when the person is tired or attempting to walk in the dark.
Gait ataxia can be caused by various underlying conditions, including degenerative neurological disorders (e.g., cerebellar atrophy, multiple sclerosis), stroke, brain injury, infection (e.g., alcoholism, HIV), or exposure to certain toxins. Proper diagnosis and identification of the underlying cause are essential for effective treatment and management of gait ataxia.
Gait apraxia is a neurological disorder that affects an individual's ability to perform coordinated and complex movements required for walking, despite having the physical capability to do so. It is not caused by weakness or sensory loss, but rather by damage to the brain areas responsible for motor planning and execution, particularly in the frontal lobes.
Gait apraxia is characterized by a wide-based, hesitant, and unsteady gait pattern. Individuals with this condition may have difficulty initiating walking, changing direction, or adjusting their stride length and speed. They may also exhibit symptoms such as freezing of gait, where they are unable to move their feet forward despite intending to walk.
This disorder is often associated with various neurological conditions, including cerebrovascular accidents (strokes), degenerative diseases such as Parkinson's disease and multiple sclerosis, traumatic brain injuries, and infections of the central nervous system. Treatment typically involves physical therapy, gait training, and the use of assistive devices to improve mobility and safety.
Medical science often defines and describes "walking" as a form of locomotion or mobility where an individual repeatedly lifts and sets down each foot to move forward, usually bearing weight on both legs. It is a complex motor activity that requires the integration and coordination of various systems in the human body, including the musculoskeletal, neurological, and cardiovascular systems.
Walking involves several components such as balance, coordination, strength, and endurance. The ability to walk independently is often used as a measure of functional mobility and overall health status. However, it's important to note that the specific definition of walking may vary depending on the context and the medical or scientific field in question.
Biomechanics is the application of mechanical laws to living structures and systems, particularly in the field of medicine and healthcare. A biomechanical phenomenon refers to a observable event or occurrence that involves the interaction of biological tissues or systems with mechanical forces. These phenomena can be studied at various levels, from the molecular and cellular level to the tissue, organ, and whole-body level.
Examples of biomechanical phenomena include:
1. The way that bones and muscles work together to produce movement (known as joint kinematics).
2. The mechanical behavior of biological tissues such as bone, cartilage, tendons, and ligaments under various loads and stresses.
3. The response of cells and tissues to mechanical stimuli, such as the way that bone tissue adapts to changes in loading conditions (known as Wolff's law).
4. The biomechanics of injury and disease processes, such as the mechanisms of joint injury or the development of osteoarthritis.
5. The use of mechanical devices and interventions to treat medical conditions, such as orthopedic implants or assistive devices for mobility impairments.
Understanding biomechanical phenomena is essential for developing effective treatments and prevention strategies for a wide range of medical conditions, from musculoskeletal injuries to neurological disorders.
Postural balance is the ability to maintain, achieve, or restore a state of equilibrium during any posture or activity. It involves the integration of sensory information (visual, vestibular, and proprioceptive) to control and adjust body position in space, thereby maintaining the center of gravity within the base of support. This is crucial for performing daily activities and preventing falls, especially in older adults and individuals with neurological or orthopedic conditions.
Orthotic devices are custom-made or prefabricated appliances designed to align, support, prevent deformity, or improve the function of movable body parts. They are frequently used in the treatment of various musculoskeletal disorders, such as foot and ankle conditions, knee problems, spinal alignment issues, and hand or wrist ailments. These devices can be adjustable or non-adjustable and are typically made from materials like plastic, metal, leather, or fabric. They work by redistributing forces across joints, correcting alignment, preventing unwanted movements, or accommodating existing deformities. Examples of orthotic devices include ankle-foot orthoses, knee braces, back braces, wrist splints, and custom-made foot insoles.
The ankle joint, also known as the talocrural joint, is the articulation between the bones of the lower leg (tibia and fibula) and the talus bone in the foot. It is a synovial hinge joint that allows for dorsiflexion and plantarflexion movements, which are essential for walking, running, and jumping. The ankle joint is reinforced by strong ligaments on both sides to provide stability during these movements.
Locomotion, in a medical context, refers to the ability to move independently and change location. It involves the coordinated movement of the muscles, bones, and nervous system that enables an individual to move from one place to another. This can include walking, running, jumping, or using assistive devices such as wheelchairs or crutches. Locomotion is a fundamental aspect of human mobility and is often assessed in medical evaluations to determine overall health and functioning.
"Walker" is not a medical term per se, but it is often used in the medical field to refer to a mobility aid that helps individuals who have difficulty walking independently. Walkers are typically made of lightweight metal and have four legs that provide stability and support. Some walkers come with wheels or glides on the front legs to make it easier for users to move around. They may also include brakes, seats, and baskets for added functionality.
Walkers can be beneficial for people who have mobility limitations due to various medical conditions such as arthritis, stroke, fractures, neurological disorders, or aging-related issues. Using a walker can help reduce the risk of falls, improve balance, increase independence, and enhance overall quality of life.
It is essential to consult with a healthcare professional before using a walker to ensure proper fit, adjustment, and usage techniques for maximum safety and effectiveness.
In medical terms, the foot is the part of the lower limb that is distal to the leg and below the ankle, extending from the tarsus to the toes. It is primarily responsible for supporting body weight and facilitating movement through push-off during walking or running. The foot is a complex structure made up of 26 bones, 33 joints, and numerous muscles, tendons, ligaments, and nerves that work together to provide stability, balance, and flexibility. It can be divided into three main parts: the hindfoot, which contains the talus and calcaneus (heel) bones; the midfoot, which includes the navicular, cuboid, and cuneiform bones; and the forefoot, which consists of the metatarsals and phalanges that form the toes.
An accidental fall is an unplanned, unexpected event in which a person suddenly and involuntarily comes to rest on the ground or other lower level, excluding intentional changes in position (e.g., jumping to catch a ball) and landings that are part of a planned activity (e.g., diving into a pool). Accidental falls can occur for various reasons, such as environmental hazards, muscle weakness, balance problems, visual impairment, or certain medical conditions. They are a significant health concern, particularly among older adults, as they can lead to serious injuries, loss of independence, reduced quality of life, and increased mortality.
An amputee is a person who has had a limb or extremity removed by trauma, medical illness, or surgical intervention. Amputation may affect any part of the body, including fingers, toes, hands, feet, arms, and legs. The level of amputation can vary from partial loss to complete removal of the affected limb.
There are several reasons why a person might become an amputee:
- Trauma: Accidents, injuries, or violence can result in amputations due to severe tissue damage or irreparable vascular injury.
- Medical illness: Certain medical conditions such as diabetes, peripheral arterial disease, and cancer may require amputation if the affected limb cannot be saved through other treatments.
- Infection: Severe infections that do not respond to antibiotics or other treatments may necessitate amputation to prevent the spread of infection.
- Congenital defects: Some individuals are born with missing or malformed limbs, making them congenital amputees.
Amputees face various challenges, including physical limitations, emotional distress, and social adjustment. However, advancements in prosthetics and rehabilitation have significantly improved the quality of life for many amputees, enabling them to lead active and fulfilling lives.
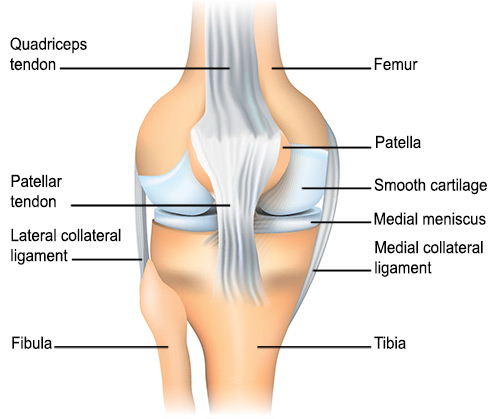
The knee joint, also known as the tibiofemoral joint, is the largest and one of the most complex joints in the human body. It is a synovial joint that connects the thighbone (femur) to the shinbone (tibia). The patella (kneecap), which is a sesamoid bone, is located in front of the knee joint and helps in the extension of the leg.
The knee joint is made up of three articulations: the femorotibial joint between the femur and tibia, the femoropatellar joint between the femur and patella, and the tibiofibular joint between the tibia and fibula. These articulations are surrounded by a fibrous capsule that encloses the synovial membrane, which secretes synovial fluid to lubricate the joint.
The knee joint is stabilized by several ligaments, including the medial and lateral collateral ligaments, which provide stability to the sides of the joint, and the anterior and posterior cruciate ligaments, which prevent excessive forward and backward movement of the tibia relative to the femur. The menisci, which are C-shaped fibrocartilaginous structures located between the femoral condyles and tibial plateaus, also help to stabilize the joint by absorbing shock and distributing weight evenly across the articular surfaces.
The knee joint allows for flexion, extension, and a small amount of rotation, making it essential for activities such as walking, running, jumping, and sitting.
Paresis is a medical term that refers to a partial loss of voluntary muscle function. It is often described as muscle weakness, and it can affect one or several parts of the body. Paresis can be caused by various conditions, including nerve damage, stroke, spinal cord injuries, multiple sclerosis, and infections like polio or botulism. The severity of paresis can range from mild to severe, depending on the underlying cause and the specific muscles involved. Treatment for paresis typically focuses on addressing the underlying condition causing it.
Hemiplegia is a medical term that refers to paralysis affecting one side of the body. It is typically caused by damage to the motor center of the brain, such as from a stroke, head injury, or brain tumor. The symptoms can vary in severity but often include muscle weakness, stiffness, and difficulty with coordination and balance on the affected side. In severe cases, the individual may be unable to move or feel anything on that side of the body. Hemiplegia can also affect speech, vision, and other functions controlled by the damaged area of the brain. Rehabilitation therapy is often recommended to help individuals with hemiplegia regain as much function as possible.
Lameness in animals refers to an alteration in the animal's normal gait or movement, which is often caused by pain, injury, or disease affecting the locomotor system. This can include structures such as bones, joints, muscles, tendons, and ligaments. The severity of lameness can vary from subtle to non-weight bearing, and it can affect one or more limbs.
Lameness can have various causes, including trauma, infection, degenerative diseases, congenital defects, and neurological disorders. In order to diagnose and treat lameness in animals, a veterinarian will typically perform a physical examination, observe the animal's gait and movement, and may use diagnostic imaging techniques such as X-rays or ultrasound to identify the underlying cause. Treatment for lameness can include medication, rest, physical therapy, surgery, or a combination of these approaches.
In the context of medicine and physiology, acceleration refers to the process of increasing or quickening a function or process. For example, heart rate acceleration is an increase in the speed at which the heart beats. It can also refer to the rate at which something increases, such as the acceleration of muscle strength during rehabilitation. In physics terms, acceleration refers to the rate at which an object changes its velocity, but this definition is not typically used in a medical context.
Articular Range of Motion (AROM) is a term used in physiotherapy and orthopedics to describe the amount of movement available in a joint, measured in degrees of a circle. It refers to the range through which synovial joints can actively move without causing pain or injury. AROM is assessed by measuring the degree of motion achieved by active muscle contraction, as opposed to passive range of motion (PROM), where the movement is generated by an external force.
Assessment of AROM is important in evaluating a patient's functional ability and progress, planning treatment interventions, and determining return to normal activities or sports participation. It is also used to identify any restrictions in joint mobility that may be due to injury, disease, or surgery, and to monitor the effectiveness of rehabilitation programs.
Crutches are medical devices that provide support and assistance for mobility, typically used by individuals who have difficulty walking or standing due to injury, illness, or disability. They help to reduce weight-bearing stress on the affected limb, improve balance, and increase stability during ambulation. Crutches can be either manually operated or designed with special features such as springs or shock absorbers to enhance comfort and functionality. Proper fit, adjustment, and usage of crutches are crucial for ensuring safety, preventing further injury, and promoting rehabilitation.
Artificial limbs, also known as prosthetics, are artificial substitutes that replace a part or all of an absent extremity or limb. They are designed to restore the function, mobility, and appearance of the lost limb as much as possible. Artificial limbs can be made from various materials such as wood, plastic, metal, or carbon fiber, and they can be custom-made to fit the individual's specific needs and measurements.
Prosthetic limbs can be categorized into two main types: cosmetic and functional. Cosmetic prosthetics are designed to look like natural limbs and are primarily used to improve the appearance of the person. Functional prosthetics, on the other hand, are designed to help the individual perform specific tasks and activities. They may include features such as hooks, hands, or specialized feet that can be used for different purposes.
Advances in technology have led to the development of more sophisticated artificial limbs, including those that can be controlled by the user's nervous system, known as bionic prosthetics. These advanced prosthetic devices can provide a greater degree of mobility and control for the user, allowing them to perform complex movements and tasks with ease.
Cerebral palsy (CP) is a group of disorders that affect a person's ability to move and maintain balance and posture. According to the Mayo Clinic, CP is caused by abnormal brain development or damage to the developing brain that affects a child's ability to control movement.
The symptoms of cerebral palsy can vary in severity and may include:
* Spasticity (stiff or tight muscles)
* Rigidity (resistance to passive movement)
* Poor coordination and balance
* Weakness or paralysis
* Tremors or involuntary movements
* Abnormal gait or difficulty walking
* Difficulty with fine motor skills, such as writing or using utensils
* Speech and language difficulties
* Vision, hearing, or swallowing problems
It's important to note that cerebral palsy is not a progressive condition, meaning that it does not worsen over time. However, the symptoms may change over time, and some individuals with CP may experience additional medical conditions as they age.
Cerebral palsy is usually caused by brain damage that occurs before or during birth, but it can also be caused by brain injuries that occur in the first few years of life. Some possible causes of cerebral palsy include:
* Infections during pregnancy
* Lack of oxygen to the brain during delivery
* Traumatic head injury during birth
* Brain bleeding or stroke in the newborn period
* Genetic disorders
* Maternal illness or infection during pregnancy
There is no cure for cerebral palsy, but early intervention and treatment can help improve outcomes and quality of life. Treatment may include physical therapy, occupational therapy, speech therapy, medications to manage symptoms, surgery, and assistive devices such as braces or wheelchairs.
Parkinson's disease is a progressive neurodegenerative disorder that affects movement. It is characterized by the death of dopamine-producing cells in the brain, specifically in an area called the substantia nigra. The loss of these cells leads to a decrease in dopamine levels, which results in the motor symptoms associated with Parkinson's disease. These symptoms can include tremors at rest, stiffness or rigidity of the limbs and trunk, bradykinesia (slowness of movement), and postural instability (impaired balance and coordination). In addition to these motor symptoms, non-motor symptoms such as cognitive impairment, depression, anxiety, and sleep disturbances are also common in people with Parkinson's disease. The exact cause of Parkinson's disease is unknown, but it is thought to be a combination of genetic and environmental factors. There is currently no cure for Parkinson's disease, but medications and therapies can help manage the symptoms and improve quality of life.
Robotics, in the medical context, refers to the branch of technology that deals with the design, construction, operation, and application of robots in medical fields. These machines are capable of performing a variety of tasks that can aid or replicate human actions, often with high precision and accuracy. They can be used for various medical applications such as surgery, rehabilitation, prosthetics, patient care, and diagnostics. Surgical robotics, for example, allows surgeons to perform complex procedures with increased dexterity, control, and reduced fatigue, while minimizing invasiveness and improving patient outcomes.
I'm sorry for any confusion, but "shoes" are not a medical term. Shoes are items of footwear intended to protect and comfort the feet. They typically have a durable sole that provides protection from sharp objects, hot surfaces, and the effects of moisture. The upper part of a shoe can be made from various materials such as leather, plastic, or textiles, and is designed to provide coverage and support for the foot.
If you have any questions related to medical terminology or health-related topics, I'd be happy to help!
The hip joint, also known as the coxal joint, is a ball-and-socket type synovial joint that connects the femur (thigh bone) to the pelvis. The "ball" is the head of the femur, while the "socket" is the acetabulum, a concave surface on the pelvic bone.
The hip joint is surrounded by a strong fibrous capsule and is reinforced by several ligaments, including the iliofemoral, ischiofemoral, and pubofemoral ligaments. The joint allows for flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction movements, making it one of the most mobile joints in the body.
The hip joint is also supported by various muscles, including the gluteus maximus, gluteus medius, gluteus minimus, iliopsoas, and other hip flexors and extensors. These muscles provide stability and strength to the joint, allowing for weight-bearing activities such as walking, running, and jumping.
"Weight-bearing" is a term used in the medical field to describe the ability of a body part or limb to support the weight or pressure exerted upon it, typically while standing, walking, or performing other physical activities. In a clinical setting, healthcare professionals often use the term "weight-bearing exercise" to refer to physical activities that involve supporting one's own body weight, such as walking, jogging, or climbing stairs. These exercises can help improve bone density, muscle strength, and overall physical function, particularly in individuals with conditions affecting the bones, joints, or muscles.
In addition, "weight-bearing" is also used to describe the positioning of a body part during medical imaging studies, such as X-rays or MRIs. For example, a weight-bearing X-ray of the foot or ankle involves taking an image while the patient stands on the affected limb, allowing healthcare providers to assess any alignment or stability issues that may not be apparent in a non-weight-bearing position.
In medical terms, the leg refers to the lower portion of the human body that extends from the knee down to the foot. It includes the thigh (femur), lower leg (tibia and fibula), foot, and ankle. The leg is primarily responsible for supporting the body's weight and enabling movements such as standing, walking, running, and jumping.
The leg contains several important structures, including bones, muscles, tendons, ligaments, blood vessels, nerves, and joints. These structures work together to provide stability, support, and mobility to the lower extremity. Common medical conditions that can affect the leg include fractures, sprains, strains, infections, peripheral artery disease, and neurological disorders.
Foot orthoses, also known as orthotic devices or simply orthotics, are custom-made or prefabricated shoe inserts that are designed to support, align, correct, or accommodate various foot and ankle deformities or biomechanical issues. They can be made of different materials such as plastic, rubber, leather, or foam and are inserted into the shoes to provide extra cushioning, arch support, or realignment of the foot structure.
Custom-made foot orthoses are created based on a mold or a digital scan of the individual's foot, taking into account their specific needs and medical condition. These devices are typically prescribed by healthcare professionals such as podiatrists, orthopedic surgeons, or physical therapists to treat various conditions such as plantar fasciitis, flat feet, high arches, bunions, diabetic foot ulcers, or arthritis.
Foot orthoses can help improve foot function, reduce pain and discomfort, prevent further deformities, and enhance overall mobility and quality of life.
The term "canes" is a common name for walking sticks that are used as a mobility aid. They are typically made of materials such as wood, metal, or fiberglass and have a handle at the top and a single foot at the bottom to provide support and stability while walking.
However, in medical terminology, "canes" does not have a specific definition. It is simply another name for walking sticks or walking canes. If you are looking for a medical definition related to a specific medical condition or treatment, could you please provide more context?
Mobility limitation refers to the partial or complete inability to move or perform functional mobility tasks independently and safely. This condition can affect any part of the body, such as limited joint range of motion, muscle weakness, or neurological impairments, making it difficult for a person to perform activities like walking, standing, transferring, balancing, and reaching. Mobility limitations can be temporary or permanent and vary in severity, significantly impacting a person's quality of life, independence, and overall health.
In medical terms, the knee is referred to as the largest and one of the most complex joints in the human body. It is a hinge joint that connects the thigh bone (femur) to the shin bones (tibia and fibula), enabling movements like flexion, extension, and a small amount of rotation. The knee also contains several other components such as menisci, ligaments, tendons, and bursae, which provide stability, cushioning, and protection during movement.
Physical therapy modalities refer to the various forms of treatment that physical therapists use to help reduce pain, promote healing, and restore function to the body. These modalities can include:
1. Heat therapy: This includes the use of hot packs, paraffin baths, and infrared heat to increase blood flow, relax muscles, and relieve pain.
2. Cold therapy: Also known as cryotherapy, this involves the use of ice packs, cold compresses, or cooling gels to reduce inflammation, numb the area, and relieve pain.
3. Electrical stimulation: This uses electrical currents to stimulate nerves and muscles, which can help to reduce pain, promote healing, and improve muscle strength and function.
4. Ultrasound: This uses high-frequency sound waves to penetrate deep into tissues, increasing blood flow, reducing inflammation, and promoting healing.
5. Manual therapy: This includes techniques such as massage, joint mobilization, and stretching, which are used to improve range of motion, reduce pain, and promote relaxation.
6. Traction: This is a technique that uses gentle pulling on the spine or other joints to help relieve pressure and improve alignment.
7. Light therapy: Also known as phototherapy, this involves the use of low-level lasers or light-emitting diodes (LEDs) to promote healing and reduce pain and inflammation.
8. Therapeutic exercise: This includes a range of exercises that are designed to improve strength, flexibility, balance, and coordination, and help patients recover from injury or illness.
Physical therapy modalities are often used in combination with other treatments, such as manual therapy and therapeutic exercise, to provide a comprehensive approach to rehabilitation and pain management.
Exercise therapy is a type of medical treatment that uses physical movement and exercise to improve a patient's physical functioning, mobility, and overall health. It is often used as a component of rehabilitation programs for individuals who have experienced injuries, illnesses, or surgeries that have impaired their ability to move and function normally.
Exercise therapy may involve a range of activities, including stretching, strengthening, balance training, aerobic exercise, and functional training. The specific exercises used will depend on the individual's needs, goals, and medical condition.
The benefits of exercise therapy include:
* Improved strength and flexibility
* Increased endurance and stamina
* Enhanced balance and coordination
* Reduced pain and inflammation
* Improved cardiovascular health
* Increased range of motion and joint mobility
* Better overall physical functioning and quality of life.
Exercise therapy is typically prescribed and supervised by a healthcare professional, such as a physical therapist or exercise physiologist, who has experience working with individuals with similar medical conditions. The healthcare professional will create an individualized exercise program based on the patient's needs and goals, and will provide guidance and support to ensure that the exercises are performed safely and effectively.
Electromyography (EMG) is a medical diagnostic procedure that measures the electrical activity of skeletal muscles during contraction and at rest. It involves inserting a thin needle electrode into the muscle to record the electrical signals generated by the muscle fibers. These signals are then displayed on an oscilloscope and may be heard through a speaker.
EMG can help diagnose various neuromuscular disorders, such as muscle weakness, numbness, or pain, and can distinguish between muscle and nerve disorders. It is often used in conjunction with other diagnostic tests, such as nerve conduction studies, to provide a comprehensive evaluation of the nervous system.
EMG is typically performed by a neurologist or a physiatrist, and the procedure may cause some discomfort or pain, although this is usually minimal. The results of an EMG can help guide treatment decisions and monitor the progression of neuromuscular conditions over time.
Movement disorders are a group of neurological conditions that affect the control and coordination of voluntary movements. These disorders can result from damage to or dysfunction of the cerebellum, basal ganglia, or other parts of the brain that regulate movement. Symptoms may include tremors, rigidity, bradykinesia (slowness of movement), akathisia (restlessness and inability to remain still), dystonia (sustained muscle contractions leading to abnormal postures), chorea (rapid, unpredictable movements), tics, and gait disturbances. Examples of movement disorders include Parkinson's disease, Huntington's disease, Tourette syndrome, and dystonic disorders.
The term "lower extremity" is used in the medical field to refer to the portion of the human body that includes the structures below the hip joint. This includes the thigh, lower leg, ankle, and foot. The lower extremities are responsible for weight-bearing and locomotion, allowing individuals to stand, walk, run, and jump. They contain many important structures such as bones, muscles, tendons, ligaments, nerves, and blood vessels.
 Gait
Gait Abnormal Gait | Walking Problems | MedlinePlus
Abnormal Gait | Walking Problems | MedlinePlus Gait Definition & Meaning | YourDictionary
Gait Definition & Meaning | YourDictionary GAIT Therapeutic Riding Center
GAIT Therapeutic Riding Center OTC Gait Transfer Belt (2466-48) | Staples
OTC Gait Transfer Belt (2466-48) | Staples![dict.cc | [gait] | English Dictionary](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAABx0lEQVQ4jZWSzUtUURjGf+fcO2emGM2mD5iGArOvhdkq0jAKgkBwnf/AuGnXtj/BVkHSIsE2QnuhRYtaBG1HGUJBAzEo08IauH7cud3XxXvs3qmwejfnvF/PeZ73PUaennO44iTCRf7P5mjv3g9xpQninfrBtQZ+7EIaqxseBmNvUHAbISLX/vpWsg1nbkPvHQVrTsHmMoRuODywUVJ/JnBpDM6OqD//ZL/AWpA/0I2hHYGxCmILULmg6fUGtD5AUFA1nf0GkgiO9MLlOlSvgghsLkG55gHmVZLr8gB5hGQLjvXDyDMoV7P48f7svj4HxngFgkUk0xseglsPtTnZgjcPYGYQVl5qTdqGr+9UkrdsiMk29I3CiQH1m9PQeAyFMpSOaqy1qvr3AX5jUM1tdPUVBCXoOg0V/8c2mhC3dLjespuxUKp07IO4BSevgOv2+hvZavXV3BAlhehTlrs5AQPjULuexb40wYb5/pyEoAiLz1UnQE8fnBriZz5ag2/vwbpfGXgKQRG+r8DsXagNQ5rAx7dK33Xr/4gjsEFeZBoivAaGQBQkWoOFGcB4/7PKM96ng8ALIyIwdX4MuKdd/2Qx8Ij60uwe8S+fCLB5Xh8AAAAASUVORK5CYII=) dict.cc | [gait] | English Dictionary
dict.cc | [gait] | English Dictionary Dual Decline in Gait, Cognition Linked to Increased Dementia Risk
Dual Decline in Gait, Cognition Linked to Increased Dementia Risk Wearable gait sensor provides in-home physical therapy - Springwise
Wearable gait sensor provides in-home physical therapy - Springwise gait biometrics
gait biometrics make, take, and gait | Bloglovin'
make, take, and gait | Bloglovin' Gait - MedFriendly.com
Gait - MedFriendly.com Stanley E Fulton Gait Research & Movement Analysis Lab
Stanley E Fulton Gait Research & Movement Analysis Lab
 Power Boothe | Gait | Whitney Museum of American Art
Power Boothe | Gait | Whitney Museum of American Art GALOP - Gait Ataxia Late Onset Polyneuropathy
GALOP - Gait Ataxia Late Onset Polyneuropathy DLR - Institute of Robotics and Mechatronics - Gait generation and walking stabilization
DLR - Institute of Robotics and Mechatronics - Gait generation and walking stabilization Gait Biomechanics
Gait Biomechanics Gait blog posts | Noldus
Gait blog posts | Noldus Frontiers | BeatWalk: Personalized Music-Based Gait Rehabilitation in Parkinson's Disease
Frontiers | BeatWalk: Personalized Music-Based Gait Rehabilitation in Parkinson's Disease Motion & Gait Analysis Labs | University of Dundee, UK
Motion & Gait Analysis Labs | University of Dundee, UK American Gaited Horses for Sale
American Gaited Horses for Sale Using electrical energy to unfreeze gait - Parkinson Canada
Using electrical energy to unfreeze gait - Parkinson Canada Evaluation of Gait Performance of a Hemipelvectomy Amputation Walking with a Canadian Prosthesis
Evaluation of Gait Performance of a Hemipelvectomy Amputation Walking with a Canadian Prosthesis Data Logging | Gait Analysis | Research | BIOPAC
Data Logging | Gait Analysis | Research | BIOPAC Gait Definitions - Physiopedia
Gait Definitions - Physiopedia Wearable sensors objectively measure gait parameters in Parkinson's disease | PLOS ONE
Wearable sensors objectively measure gait parameters in Parkinson's disease | PLOS ONE

.jpg)