Facial Muscles
Facial Paralysis
Facial Nerve
Zygoma
Nerve Transfer
Masticatory Muscles
Skull Base Neoplasms
Electromyography
Muscle Proteins
Muscle, Smooth
Muscle, Skeletal
Muscle Fibers, Skeletal
Facial Nerve Diseases
Facial Bones
Muscle Development
Electrical stimulation as a therapeutic option to improve eyelid function in chronic facial nerve disorders. (1/322)
PURPOSE: To establish whether it is possible to improve orbicularis oculi muscle function in the eyelids of patients with a chronic seventh cranial nerve palsy by using transcutaneous electrical stimulation to the point at which electrical stimulation induces a functional blink. METHODS: Ten subjects (one woman, nine men) aged 36 to 76 with chronic, moderate to severe facial nerve palsy were recruited into the study. Voluntary and spontaneous eyelid movements were assessed, using an optical measuring system, before, during, and after a 3-month treatment period. Voluntary and spontaneous lid velocities were also measured and compared with eyelid kinematic data in normal subjects (12 women, 18 men; age range, 22-56 years). RESULTS: Therapeutic electrical stimulation applied over 3 months produced improvement in eyelid movement (>2 mm) in 8 of 10 patients during voluntary eyelid closure. However, there was no significant improvement recorded in spontaneous blink amplitudes or peak downward-phase velocity of the upper eyelid. This regimen of stimulation failed to recover function well enough that a functional blink could be induced in the paretic eyelid by electrical stimulation. CONCLUSIONS: Electrical stimulation using transcutaneous electrical nerve stimulators units can improve voluntary eye closure, apparently because of a reduction in stiffness of eyelid mechanics, rather than an improvement of muscle function. Investigation of alternative stimulation regimens is warranted. (+info)Anticonvulsant-induced dyskinesias: a comparison with dyskinesias induced by neuroleptics. (2/322)
Anticonvulsants cause dyskinesias more commonly than has been appreciated. Diphenylhydantoin (DPH), carbamazepine, primidone, and phenobarbitone may cause asterixis. DPH, but not other anticonvulsants, may cause orofacial dyskinesias, limb chorea, and dystonia in intoxicated patients. These dyskinesias are similar to those caused by neuroleptic drugs and may be related to dopamine antagonistic properties possessed by DPH. (+info)MR imaging of Dejerine-Sottas disease. (3/322)
We report the MR findings in two patients with clinically and histologically proved Dejerine-Sottas disease. One patient had spinal involvement with multiple thickened and clumped nerve roots of the cauda equina; the second had multiple enlarged and enhancing cranial nerves. Although these findings are not specific for Dejerine-Sottas disease, they are suggestive of the diagnosis, which is further corroborated with history and confirmed with sural nerve biopsy and laboratory studies. (+info)MR appearance of rhinoscleroma. (4/322)
BACKGROUND AND PURPOSE: We describe the MR imaging appearance of rhinoscleroma, an endemic, chronic, granulomatous disease whose causative agent is Klebsiella rhinoscleromatis. METHODS: The study included 15 patients (nine males and six females; mean age, 25 years; range, 13-36 years) with rhinoscleroma. MR imaging was performed in all patients. The signal intensity of the nasal masses was compared with that of fat, muscle, and CSF on both T1- and T2-weighted images. All cases were proved by histopathologic examination. RESULTS: The nasal masses were bilateral and symmetrical (n = 6), asymmetrical (n = 4), or unilateral (n = 5). They extended through the anterior nares (n = 9) or posterior choana into the nasopharynx (n = 3). They obstructed the ostiomeatal units with retained secretions in the related sinuses (n = 10). On T1-weighted images, rhinoscleroma showed striking (n = 9) or mild (n = 6) high signal intensity relative to muscle and CSF, but less hyperintensity than fat. On T2-weighted images, the nasal masses showed homogeneous high signal intensity (n = 10) or heterogeneous high signal intensity associated with hypointense foci (n = 5). They were hyperintense relative to fat and muscle, but less hyperintense than CSF. CONCLUSION: The hypertrophic stage of rhinoscleroma has characteristic mild to marked high signal intensity on both T1- and T2-weighted MR images. (+info)The neuromuscular control of birdsong. (5/322)
Birdsong requires complex learned motor skills involving the coordination of respiratory, vocal organ and craniomandibular muscle groups. Recent studies have added to our understanding of how these vocal subsystems function and interact during song production. The respiratory rhythm determines the temporal pattern of song. Sound is produced during expiration and each syllable is typically followed by a small inspiration, except at the highest syllable repetition rates when a pattern of pulsatile expiration is used. Both expiration and inspiration are active processes. The oscine vocal organ, the syrinx, contains two separate sound sources at the cranial end of each bronchus, each with independent motor control. Dorsal syringeal muscles regulate the timing of phonation by adducting the sound-generating labia into the air stream. Ventral syringeal muscles have an important role in determining the fundamental frequency of the sound. Different species use the two sides of their vocal organ in different ways to achieve the particular acoustic properties of their song. Reversible paralysis of the vocal organ during song learning in young birds reveals that motor practice is particularly important in late plastic song around the time of song crystallization in order for normal adult song to develop. Even in adult crystallized song, expiratory muscles use sensory feedback to make compensatory adjustments to perturbations of respiratory pressure. The stereotyped beak movements that accompany song appear to have a role in suppressing harmonics, particularly at low frequencies. (+info)Features of cortically evoked swallowing in the awake primate (Macaca fascicularis). (6/322)
Although the cerebral cortex has been implicated in the control of swallowing, the output organization of the cortical swallowing representation, and features of cortically evoked swallowing, remain unclear. The present study defined the output features of the primate "cortical swallowing representation" with intracortical microstimulation (ICMS) applied within the lateral sensorimotor cortex. In four hemispheres of two awake monkeys, microelectrode penetrations were made at 5 mm deep to the cortical surface corresponding to both the white matter underlying the CMA and the frontal operculum; EMG patterns of swallows elicited from these four cortical regions showed some statistically significant differences. Whereas swallowing ONLY was evoked at some sites, particularly within the deep cortical area, swallowing was more frequently evoked together with other orofacial responses including rhythmic jaw movements. Increasing ICMS intensity increased the magnitude, and decreased the latency, of the swallow-related EMG burst in the genioglossus muscle at some sites. These findings suggest that a number of distinct cortical foci may participate in the initiation and modulation of the swallowing synergy as well as in integrating the swallow within the masticatory sequence. (+info)Direct injection of liposome-encapsulated doxorubicin optimizes chemomyectomy in rabbit eyelid. (7/322)
PURPOSE: Doxorubicin chemomyectomy presently represents the only permanent, nonsurgical treatment for blepharospasm and hemifacial spasm. The major deterrent to an otherwise extremely effective treatment protocol is the development in patients of localized inflammation, discomfort, and skin injury over the injection site. As a potential alternative therapy, Doxil (Sequus, Menlo Park, CA), a liposome-encapsulated form of doxorubicin that displays tissue-selective therapeutic effects compared with free doxorubicin, was examined. These effects have been related to its increased retention in tissues and its sustained release over time. For the skin, Doxil is classified as an irritant rather than a vesicant. METHODS: Rabbits received direct injections of 1, 2, or 3 mg Doxil alone or in sequence with other agents directly into the lower eyelids. The treated eyelids were examined daily for signs of skin injury. One month after the last injection, the rabbits were euthanatized, and their eyelids were examined histologically for the effect of Doxil on the orbicularis oculi muscle and the skin. RESULTS: At equivalent milligram doses of free doxorubicin, Doxil spared the skin from injury. Doxil was only approximately 60% as effective in killing muscles as the same milligram dose of free doxorubicin. However, either two injections of Doxil spaced 2 months apart or preinjury of the lid with bupivacaine before a single dose of Doxil treatment resulted in increased muscle loss compared with a single dose of Doxil alone and was as effective as free doxorubicin. Higher doses of Doxil did not increase the desired myotoxic effect; apparently, the dose effect levels off at a maximum. Signs of skin injury were minimal; there were small or no adverse skin changes at the maximum effective myotoxic doses. CONCLUSIONS: Injection of Doxil resulted in significant reduction of skin injury compared with doxorubicin alone. Although single injections of Doxil were myotoxic, multiple exposure of the eyelid to the liposome-encapsulated form substantially improved myotoxicity while sparing the skin. Repeated doses of the liposome-encapsulated form of doxorubicin may be as clinically effective as free doxorubicin injections and may produce fewer unwanted side effects. (+info)Differentiation of avian craniofacial muscles: I. Patterns of early regulatory gene expression and myosin heavy chain synthesis. (8/322)
Myogenic populations of the avian head arise within both epithelial (somitic) and mesenchymal (unsegmented) mesodermal populations. The former, which gives rise to neck, tongue, laryngeal, and diaphragmatic muscles, show many similarities to trunk axial, body wall, and appendicular muscles. However, muscle progenitors originating within unsegmented head mesoderm exhibit several distinct features, including multiple ancestries, the absence of several somite lineage-determining regulatory gene products, diverse locations relative to neuraxial and pharyngeal tissues, and a prolonged and necessary interaction with neural crest cells. The object of this study has been to characterize the spatial and temporal patterns of early muscle regulatory gene expression and subsequent myosin heavy chain isoform appearance in avian mesenchyme-derived extraocular and branchial muscles, and compare these with expression patterns in myotome-derived neck and tongue muscles. Myf5 and myoD transcripts are detected in the dorsomedial (epaxial) region of the occipital somites before stage 12, but are not evident in the ventrolateral domain until stage 14. Within unsegmented head mesoderm, myf5 expression begins at stage 13.5 in the second branchial arch, followed within a few hours in the lateral rectus and first branchial arch myoblasts, then other eye and branchial arch muscles. Expression of myoD is detected initially in the first branchial arch beginning at stage 14.5, followed quickly by its appearance in other arches and eye muscles. Multiple foci of myoblasts expressing these transcripts are evident during the early stages of myogenesis in the first and third branchial arches and the lateral rectus-pyramidalis/quadratus complex, suggesting an early patterned segregation of muscle precursors within head mesoderm. Myf5-positive myoblasts forming the hypoglossal cord emerge from the lateral borders of somites 4 and 5 by stage 15 and move ventrally as a cohort. Myosin heavy chain (MyHC) is first immunologically detectable in several eye and branchial arch myofibers between stages 21 and 22, although many tongue and laryngeal muscles do not initiate myosin production until stage 24 or later. Detectable synthesis of the MyHC-S3 isoform, which characterizes myofibers as having "slow" contraction properties, occurs within 1-2 stages of the onset of MyHC synthesis in most head muscles, with tongue and laryngeal muscles being substantially delayed. Such a prolonged, 2- to 3-day period of regulatory gene expression preceding the onset of myosin production contrasts with the interval seen in muscles developing in axial (approximately 18 hr) and wing (approximately 1-1.5 days) locations, and is unique to head muscles. This finding suggests that ongoing interactions between head myoblasts and their surroundings, most likely neural crest cells, delay myoblast withdrawal from the mitotic pool. These descriptions define a spatiotemporal pattern of muscle regulatory gene and myosin heavy chain expression unique to head muscles. This pattern is independent of origin (somitic vs. unsegmented paraxial vs. prechordal mesoderm), position (extraocular vs. branchial vs. subpharyngeal), and fiber type (fast vs. slow) and is shared among all muscles whose precursors interact with cephalic neural crest populations. Dev Dyn 1999;216:96-112. (+info)Facial muscles, also known as facial nerves or cranial nerve VII, are a group of muscles responsible for various expressions and movements of the face. These muscles include:
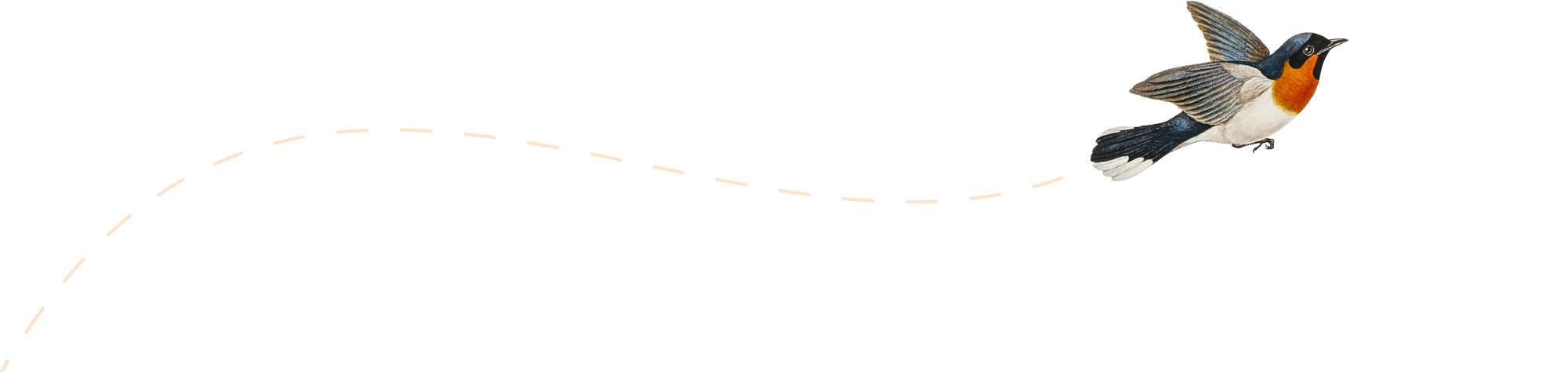
1. Orbicularis oculi: muscle that closes the eyelid and raises the upper eyelid
2. Corrugator supercilii: muscle that pulls the eyebrows down and inward, forming wrinkles on the forehead
3. Frontalis: muscle that raises the eyebrows and forms horizontal wrinkles on the forehead
4. Procerus: muscle that pulls the medial ends of the eyebrows downward, forming vertical wrinkles between the eyebrows
5. Nasalis: muscle that compresses or dilates the nostrils
6. Depressor septi: muscle that pulls down the tip of the nose
7. Levator labii superioris alaeque nasi: muscle that raises the upper lip and flares the nostrils
8. Levator labii superioris: muscle that raises the upper lip
9. Zygomaticus major: muscle that raises the corner of the mouth, producing a smile
10. Zygomaticus minor: muscle that raises the nasolabial fold and corner of the mouth
11. Risorius: muscle that pulls the angle of the mouth laterally, producing a smile
12. Depressor anguli oris: muscle that pulls down the angle of the mouth
13. Mentalis: muscle that raises the lower lip and forms wrinkles on the chin
14. Buccinator: muscle that retracts the cheek and helps with chewing
15. Platysma: muscle that depresses the corner of the mouth and wrinkles the skin of the neck.
These muscles are innervated by the facial nerve, which arises from the brainstem and exits the skull through the stylomastoid foramen. Damage to the facial nerve can result in facial paralysis or weakness on one or both sides of the face.
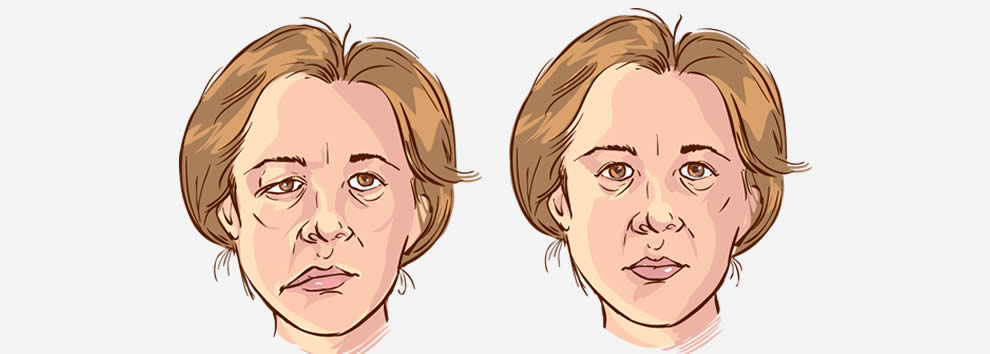
Facial paralysis is a loss of facial movement due to damage or dysfunction of the facial nerve (cranial nerve VII). This nerve controls the muscles involved in facial expressions, such as smiling, frowning, and closing the eyes. Damage to one side of the facial nerve can cause weakness or paralysis on that side of the face.
Facial paralysis can result from various conditions, including:
1. Bell's palsy - an idiopathic (unknown cause) inflammation of the facial nerve
2. Trauma - skull fractures, facial injuries, or surgical trauma to the facial nerve
3. Infections - Lyme disease, herpes zoster (shingles), HIV/AIDS, or bacterial infections like meningitis
4. Tumors - benign or malignant growths that compress or invade the facial nerve
5. Stroke - damage to the brainstem where the facial nerve originates
6. Congenital conditions - some people are born with facial paralysis due to genetic factors or birth trauma
Symptoms of facial paralysis may include:
* Inability to move one or more parts of the face, such as the eyebrows, eyelids, mouth, or cheeks
* Drooping of the affected side of the face
* Difficulty closing the eye on the affected side
* Changes in saliva and tear production
* Altered sense of taste
* Pain around the ear or jaw
* Speech difficulties due to weakened facial muscles
Treatment for facial paralysis depends on the underlying cause. In some cases, such as Bell's palsy, spontaneous recovery may occur within a few weeks to months. However, physical therapy, medications, and surgical interventions might be necessary in other situations to improve function and minimize complications.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
I'm sorry for any confusion, but "smiling" is not typically considered a medical term. It's a part of normal human behavior and facial expression. A smile usually refers to the action of turning up the corners of the mouth to signal pleasure, affection, amusement, or approval. However, in a medical context, a person may be unable to smile due to various conditions, such as facial paralysis caused by Bell's palsy or a stroke. In such cases, the ability to smile can be an important part of rehabilitation and recovery.
A facial expression is a result of the contraction or relaxation of muscles in the face that change the physical appearance of an individual's face to convey various emotions, intentions, or physical sensations. Facial expressions can be voluntary or involuntary and are a form of non-verbal communication that plays a crucial role in social interaction and conveying a person's state of mind.
The seven basic facial expressions of emotion, as proposed by Paul Ekman, include happiness, sadness, fear, disgust, surprise, anger, and contempt. These facial expressions are universally recognized across cultures and can be detected through the interpretation of specific muscle movements in the face, known as action units, which are measured and analyzed in fields such as psychology, neurology, and computer vision.
The zygoma is the scientific name for the cheekbone. It is a part of the facial skeleton that forms the prominence of the cheek and houses the maxillary sinus, one of the pairs of paranasal sinuses. The zygomatic bone, also known as the malar bone, contributes to the formation of the zygoma.
A nerve transfer is a surgical procedure where a functioning nerve is connected to an injured nerve to restore movement, sensation or function. The functioning nerve, called the donor nerve, usually comes from another less critical location in the body and has spare nerve fibers that can be used to reinnervate the injured nerve, called the recipient nerve.
During the procedure, a small section of the donor nerve is carefully dissected and prepared for transfer. The recipient nerve is also prepared by removing any damaged or non-functioning portions. The two ends are then connected using microsurgical techniques under a microscope. Over time, the nerve fibers from the donor nerve grow along the recipient nerve and reinnervate the muscles or sensory structures that were previously innervated by the injured nerve.
Nerve transfers can be used to treat various types of nerve injuries, including brachial plexus injuries, facial nerve palsy, and peripheral nerve injuries. The goal of the procedure is to restore function as quickly and efficiently as possible, allowing for a faster recovery and improved quality of life for the patient.
Facial asymmetry refers to a condition in which the facial features are not identical or proportionate on both sides of a vertical line drawn down the middle of the face. This can include differences in the size, shape, or positioning of facial features such as the eyes, ears, nose, cheeks, and jaw. Facial asymmetry can be mild and barely noticeable, or it can be more severe and affect a person's appearance and/or functionality of the mouth and jaw.
Facial asymmetry can be present at birth (congenital) or can develop later in life due to various factors such as injury, surgery, growth disorders, nerve damage, or tumors. In some cases, facial asymmetry may not cause any medical problems and may only be of cosmetic concern. However, in other cases, it may indicate an underlying medical condition that requires treatment.
Depending on the severity and cause of the facial asymmetry, treatment options may include cosmetic procedures such as fillers or surgery, orthodontic treatment, physical therapy, or medication to address any underlying conditions.
Masticatory muscles are a group of skeletal muscles responsible for the mastication (chewing) process in humans and other animals. They include:
1. Masseter muscle: This is the primary muscle for chewing and is located on the sides of the face, running from the lower jawbone (mandible) to the cheekbone (zygomatic arch). It helps close the mouth and elevate the mandible during chewing.
2. Temporalis muscle: This muscle is situated in the temporal region of the skull, covering the temple area. It assists in closing the jaw, retracting the mandible, and moving it sideways during chewing.
3. Medial pterygoid muscle: Located deep within the cheek, near the angle of the lower jaw, this muscle helps move the mandible forward and grind food during chewing. It also contributes to closing the mouth.
4. Lateral pterygoid muscle: Found inside the ramus (the vertical part) of the mandible, this muscle has two heads - superior and inferior. The superior head helps open the mouth by pulling the temporomandibular joint (TMJ) downwards, while the inferior head assists in moving the mandible sideways during chewing.
These muscles work together to enable efficient chewing and food breakdown, preparing it for swallowing and digestion.
Skull base neoplasms refer to abnormal growths or tumors located in the skull base, which is the region where the skull meets the spine and where the brain connects with the blood vessels and nerves that supply the head and neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells in this area, including bone, nerve, glandular, and vascular tissue.
Skull base neoplasms can cause a range of symptoms depending on their size, location, and growth rate. Some common symptoms include headaches, vision changes, hearing loss, facial numbness or weakness, difficulty swallowing, and balance problems. Treatment options for skull base neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. The specific treatment plan will depend on the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history.
A muscle is a soft tissue in our body that contracts to produce force and motion. It is composed mainly of specialized cells called muscle fibers, which are bound together by connective tissue. There are three types of muscles: skeletal (voluntary), smooth (involuntary), and cardiac. Skeletal muscles attach to bones and help in movement, while smooth muscles are found within the walls of organs and blood vessels, helping with functions like digestion and circulation. Cardiac muscle is the specific type that makes up the heart, allowing it to pump blood throughout the body.
Electromyography (EMG) is a medical diagnostic procedure that measures the electrical activity of skeletal muscles during contraction and at rest. It involves inserting a thin needle electrode into the muscle to record the electrical signals generated by the muscle fibers. These signals are then displayed on an oscilloscope and may be heard through a speaker.
EMG can help diagnose various neuromuscular disorders, such as muscle weakness, numbness, or pain, and can distinguish between muscle and nerve disorders. It is often used in conjunction with other diagnostic tests, such as nerve conduction studies, to provide a comprehensive evaluation of the nervous system.
EMG is typically performed by a neurologist or a physiatrist, and the procedure may cause some discomfort or pain, although this is usually minimal. The results of an EMG can help guide treatment decisions and monitor the progression of neuromuscular conditions over time.
Parotid neoplasms refer to abnormal growths or tumors in the parotid gland, which is the largest of the salivary glands and is located in front of the ear and extends down the neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parotid neoplasms are typically slow-growing, painless masses that may cause facial asymmetry or difficulty in chewing or swallowing if they become large enough to compress surrounding structures. The most common type of benign parotid tumor is a pleomorphic adenoma.
Malignant parotid neoplasms, on the other hand, are more aggressive and can invade nearby tissues and spread to other parts of the body. They may present as rapidly growing masses that are firm or fixed to surrounding structures. Common types of malignant parotid tumors include mucoepidermoid carcinoma, adenoid cystic carcinoma, and squamous cell carcinoma.
The diagnosis of parotid neoplasms typically involves a thorough clinical evaluation, imaging studies such as CT or MRI scans, and fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Treatment options depend on the type, size, and location of the neoplasm but may include surgical excision, radiation therapy, and chemotherapy.
Muscle proteins are a type of protein that are found in muscle tissue and are responsible for providing structure, strength, and functionality to muscles. The two major types of muscle proteins are:
1. Contractile proteins: These include actin and myosin, which are responsible for the contraction and relaxation of muscles. They work together to cause muscle movement by sliding along each other and shortening the muscle fibers.
2. Structural proteins: These include titin, nebulin, and desmin, which provide structural support and stability to muscle fibers. Titin is the largest protein in the human body and acts as a molecular spring that helps maintain the integrity of the sarcomere (the basic unit of muscle contraction). Nebulin helps regulate the length of the sarcomere, while desmin forms a network of filaments that connects adjacent muscle fibers together.
Overall, muscle proteins play a critical role in maintaining muscle health and function, and their dysregulation can lead to various muscle-related disorders such as muscular dystrophy, myopathies, and sarcopenia.
Smooth muscle, also known as involuntary muscle, is a type of muscle that is controlled by the autonomic nervous system and functions without conscious effort. These muscles are found in the walls of hollow organs such as the stomach, intestines, bladder, and blood vessels, as well as in the eyes, skin, and other areas of the body.
Smooth muscle fibers are shorter and narrower than skeletal muscle fibers and do not have striations or sarcomeres, which give skeletal muscle its striped appearance. Smooth muscle is controlled by the autonomic nervous system through the release of neurotransmitters such as acetylcholine and norepinephrine, which bind to receptors on the smooth muscle cells and cause them to contract or relax.
Smooth muscle plays an important role in many physiological processes, including digestion, circulation, respiration, and elimination. It can also contribute to various medical conditions, such as hypertension, gastrointestinal disorders, and genitourinary dysfunction, when it becomes overactive or underactive.
Skeletal muscle, also known as striated or voluntary muscle, is a type of muscle that is attached to bones by tendons or aponeuroses and functions to produce movements and support the posture of the body. It is composed of long, multinucleated fibers that are arranged in parallel bundles and are characterized by alternating light and dark bands, giving them a striped appearance under a microscope. Skeletal muscle is under voluntary control, meaning that it is consciously activated through signals from the nervous system. It is responsible for activities such as walking, running, jumping, and lifting objects.
Skeletal muscle fibers, also known as striated muscle fibers, are the type of muscle cells that make up skeletal muscles, which are responsible for voluntary movements of the body. These muscle fibers are long, cylindrical, and multinucleated, meaning they contain multiple nuclei. They are surrounded by a connective tissue layer called the endomysium, and many fibers are bundled together into fascicles, which are then surrounded by another layer of connective tissue called the perimysium.
Skeletal muscle fibers are composed of myofibrils, which are long, thread-like structures that run the length of the fiber. Myofibrils contain repeating units called sarcomeres, which are responsible for the striated appearance of skeletal muscle fibers. Sarcomeres are composed of thick and thin filaments, which slide past each other during muscle contraction to shorten the sarcomere and generate force.
Skeletal muscle fibers can be further classified into two main types based on their contractile properties: slow-twitch (type I) and fast-twitch (type II). Slow-twitch fibers have a high endurance capacity and are used for sustained, low-intensity activities such as maintaining posture. Fast-twitch fibers, on the other hand, have a higher contractile speed and force generation capacity but fatigue more quickly and are used for powerful, explosive movements.
A smooth muscle within the vascular system refers to the involuntary, innervated muscle that is found in the walls of blood vessels. These muscles are responsible for controlling the diameter of the blood vessels, which in turn regulates blood flow and blood pressure. They are called "smooth" muscles because their individual muscle cells do not have the striations, or cross-striped patterns, that are observed in skeletal and cardiac muscle cells. Smooth muscle in the vascular system is controlled by the autonomic nervous system and by hormones, and can contract or relax slowly over a period of time.
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
The facial bones, also known as the facial skeleton, are a series of bones that make up the framework of the face. They include:
1. Frontal bone: This bone forms the forehead and the upper part of the eye sockets.
2. Nasal bones: These two thin bones form the bridge of the nose.
3. Maxilla bones: These are the largest bones in the facial skeleton, forming the upper jaw, the bottom of the eye sockets, and the sides of the nose. They also contain the upper teeth.
4. Zygomatic bones (cheekbones): These bones form the cheekbones and the outer part of the eye sockets.
5. Palatine bones: These bones form the back part of the roof of the mouth, the side walls of the nasal cavity, and contribute to the formation of the eye socket.
6. Inferior nasal conchae: These are thin, curved bones that form the lateral walls of the nasal cavity and help to filter and humidify air as it passes through the nose.
7. Lacrimal bones: These are the smallest bones in the skull, located at the inner corner of the eye socket, and help to form the tear duct.
8. Mandible (lower jaw): This is the only bone in the facial skeleton that can move. It holds the lower teeth and forms the chin.
These bones work together to protect vital structures such as the eyes, brain, and nasal passages, while also providing attachment points for muscles that control chewing, expression, and other facial movements.
Muscle development, also known as muscle hypertrophy, refers to the increase in size and mass of the muscles through a process called myofiber growth. This is primarily achieved through resistance or strength training exercises that cause micro-tears in the muscle fibers, leading to an inflammatory response and the release of hormones that promote muscle growth. As the muscles repair themselves, they become larger and stronger than before. Proper nutrition, including adequate protein intake, and rest are also essential components of muscle development.
It is important to note that while muscle development can lead to an increase in strength and muscular endurance, it does not necessarily result in improved athletic performance or overall fitness. A well-rounded exercise program that includes cardiovascular activity, flexibility training, and resistance exercises is recommended for optimal health and fitness outcomes.
Facial injuries refer to any damage or trauma caused to the face, which may include the bones of the skull that form the face, teeth, salivary glands, muscles, nerves, and skin. Facial injuries can range from minor cuts and bruises to severe fractures and disfigurement. They can be caused by a variety of factors such as accidents, falls, sports-related injuries, physical assaults, or animal attacks.
Facial injuries can affect one or more areas of the face, including the forehead, eyes, nose, cheeks, ears, mouth, and jaw. Common types of facial injuries include lacerations (cuts), contusions (bruises), abrasions (scrapes), fractures (broken bones), and burns.
Facial injuries can have significant psychological and emotional impacts on individuals, in addition to physical effects. Treatment for facial injuries may involve simple first aid, suturing of wounds, splinting or wiring of broken bones, reconstructive surgery, or other medical interventions. It is essential to seek prompt medical attention for any facial injury to ensure proper healing and minimize the risk of complications.
Muscle contraction is the physiological process in which muscle fibers shorten and generate force, leading to movement or stability of a body part. This process involves the sliding filament theory where thick and thin filaments within the sarcomeres (the functional units of muscles) slide past each other, facilitated by the interaction between myosin heads and actin filaments. The energy required for this action is provided by the hydrolysis of adenosine triphosphate (ATP). Muscle contractions can be voluntary or involuntary, and they play a crucial role in various bodily functions such as locomotion, circulation, respiration, and posture maintenance.
 Facial muscles - Wikipedia
Facial muscles - Wikipedia Learning From The Dead: What Facial Muscles Can Tell Us About Emotion | ScienceDaily
Learning From The Dead: What Facial Muscles Can Tell Us About Emotion | ScienceDaily Facial Anatomy in Cutaneous Surgery: Skin Tension Lines, Cosmetic Units and Subunits, Muscles of Facial Expression
Facial Anatomy in Cutaneous Surgery: Skin Tension Lines, Cosmetic Units and Subunits, Muscles of Facial Expression Archaeological facial reconstruction muscle-by-muscle with Blender - BlenderNation
Archaeological facial reconstruction muscle-by-muscle with Blender - BlenderNation Repêchage Facial Massage & Muscles (2022 version) - Repêchage®
Repêchage Facial Massage & Muscles (2022 version) - Repêchage® Medical arithmetic: a 'popped' muscle, skin thickening and facial telangiectasia - Pulse Today
Medical arithmetic: a 'popped' muscle, skin thickening and facial telangiectasia - Pulse Today 3 Ways To Relax Your Facial Muscles + Ease Expression Wrinkles | mindbodygreen
3 Ways To Relax Your Facial Muscles + Ease Expression Wrinkles | mindbodygreen Facial Muscles - Bellezza
Facial Muscles - Bellezza Facial Mimetic Muscles - Poster - Archidemia
Facial Mimetic Muscles - Poster - Archidemia Facial muscles - Symptoms - Parkinson's UK Forum
Facial muscles - Symptoms - Parkinson's UK Forum Harvard Psychiatrist Gives 7 Skills to Help You Get Along With Others
Harvard Psychiatrist Gives 7 Skills to Help You Get Along With Others Facial Muscle Exercises | NEODERMA
Facial Muscle Exercises | NEODERMA Facial Muscle Health | westfernspa.com
Facial Muscle Health | westfernspa.com Muscle homo anal invasion And Facial
Muscle homo anal invasion And Facial Facials: Muscle Hunks Unload - TwinksVids.com
Facials: Muscle Hunks Unload - TwinksVids.com Biting Tongue in Sleep: Symptoms, Causes, and Treatment
Biting Tongue in Sleep: Symptoms, Causes, and Treatment absent facial muscle - Ontology Browser - Rat Genome Database
absent facial muscle - Ontology Browser - Rat Genome Database Best Seller Facial Muscle Fitness - New Zealand Trends
Best Seller Facial Muscle Fitness - New Zealand Trends 3D ultrasonography for evaluation of muscles following facial palsy | ENT & Audiology News
3D ultrasonography for evaluation of muscles following facial palsy | ENT & Audiology News Facial Ice Muscle Instrument Handheld Face Cooling Tool - EFFOREST
Facial Ice Muscle Instrument Handheld Face Cooling Tool - EFFOREST Is it safe to exercise facial and neck muscles with FacExer after havi
Is it safe to exercise facial and neck muscles with FacExer after havi Best ems facial device face electronic muscle stimulator | IDEAL BEAUTY
Best ems facial device face electronic muscle stimulator | IDEAL BEAUTY Risorius | Facial muscles | Head and Neck | Anatomy.app | Learn anatomy | 3D models, articles, and quizzes
Risorius | Facial muscles | Head and Neck | Anatomy.app | Learn anatomy | 3D models, articles, and quizzes