Drug Dosage Calculations
Pharmaceutical Preparations
Drug Monitoring
Dose-Response Relationship, Drug
Relapse following discontinuation of imatinib mesylate therapy for FIP1L1/PDGFRA-positive chronic eosinophilic leukemia: implications for optimal dosing. (1/205)
Although imatinib is clearly the treatment of choice for FIP1L1/PDGFRA-positive chronic eosinophilic leukemia (CEL), little is known about optimal dosing, duration of treatment, and the possibility of cure in this disorder. To address these questions, 5 patients with FIP1L1/PDGFRA-positive CEL with documented clinical, hematologic, and molecular remission on imatinib (400 mg daily) and without evidence of cardiac involvement were enrolled in a dose de-escalation trial. The imatinib dose was tapered slowly with close follow-up for evidence of clinical, hematologic, and molecular relapse. Two patients with endomyocardial fibrosis were maintained on imatinib 300 to 400 mg daily and served as controls. All 5 patients who underwent dose de-escalation, but neither of the control patients, experienced molecular relapse (P < .05). None developed recurrent symptoms, and eosinophil counts, serum B12, and tryptase levels remained suppressed. Reinitiation of therapy at the prior effective dose led to molecular remission in all 5 patients, although 2 patients subsequently required increased dosing to maintain remission. These data are consistent with suppression rather than elimination of the clonal population in FIP1L1/PDGFRA-positive CEL and suggest that molecular monitoring may be the most useful method in determining optimal dosing without the risk of disease exacerbation. This trial was registered at http://www.clinicaltrials.gov as no. NCT00044304. (+info)Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. (2/205)
BACKGROUND: Pharmacogenetic-guided dosing of warfarin is a promising application of "personalized medicine" but has not been adequately tested in randomized trials. METHODS AND RESULTS: Consenting patients (n=206) being initiated on warfarin were randomized to pharmacogenetic-guided or standard dosing. Buccal swab DNA was genotyped for CYP2C9 *2 and CYP2C9 *3 and VKORC1C1173T with a rapid assay. Standard dosing followed an empirical protocol, whereas pharmacogenetic-guided dosing followed a regression equation including the 3 genetic variants and age, sex, and weight. Prothrombin time international normalized ratio (INR) was measured routinely on days 0, 3, 5, 8, 21, 60, and 90. A research pharmacist unblinded to treatment strategy managed dose adjustments. Patients were followed up for up to 3 months. Pharmacogenetic-guided predicted doses more accurately approximated stable doses (P<0.001), resulting in smaller (P=0.002) and fewer (P=0.03) dosing changes and INRs (P=0.06). However, percent out-of-range INRs (pharmacogenetic = 30.7%, standard = 33.1%), the primary end point, did not differ significantly between arms. Despite this, when restricted to wild-type patients (who required larger doses; P=0.001) and multiple variant carriers (who required smaller doses; P<0.001) in exploratory analyses, results (pharmacogenetic = 29%, standard = 39%) achieved nominal significance (P=0.03). Multiple variant allele carriers were at increased risk of an INR of > or = 4 (P=0.03). CONCLUSIONS: An algorithm guided by pharmacogenetic and clinical factors improved the accuracy and efficiency of warfarin dose initiation. Despite this, the primary end point of a reduction in out-of-range INRs was not achieved. In subset analyses, pharmacogenetic guidance showed promise for wild-type and multiple variant genotypes. (+info)Pharmaceutical calculations instruction and assessment in US colleges and schools of pharmacy. (3/205)
OBJECTIVE: To characterize the current strategies used in the instruction and assessment of pharmaceutical calculations content through the administration of a nationwide survey. METHODS: Instructors of pharmaceutical calculations were invited to complete a 34-item questionnaire designed to gather information on course logistics, content delivery, covered topics, homework, examinations, and retention measures. RESULTS: Seventy-two colleges and schools responded to the survey. Exactly half of the respondents indicated that they had a standalone pharmaceutical calculations course, while the other half indicated this material was integrated into other coursework. An average of 24.8 hours was devoted to calculations topics. A minimum passing examination score of 70% was reported by 53% of programs. Knowledge retention was formally measured in 16% of programs, while 27% responded that they did not measure retention. CONCLUSION: This survey provided the first assessment of the strategies used to teach and assess pharmaceutical calculations content. Further work is needed to determine the optimal teaching and assessment strategies for pharmaceutical calculations, as well as optimal methods of evaluating and promoting retention of this material. (+info)Control of IGF-I levels with titrated dosing of lanreotide Autogel over 48 weeks in patients with acromegaly. (4/205)
(+info)Thiotepa/cyclophosphamide/TBI as a conditioning regimen for allogeneic hematopoietic stem cell transplantation in patients aged 50 years and over. (5/205)
OBJECTIVE: To reduce the relapse rate for hematological malignancies after allogeneic hematopoietic stem cell transplantation, we employed a myeloablative regimen comprising thiotepa 400 mg/m(2), cyclophosphamide 3,600 mg/m(2) and total body irradiation 10 Gy. MATERIALS AND METHODS: Subjects comprised 17 patients (median age, 53 years; range, 50-56 years) with hematological malignancies who received allogeneic hematopoietic stem cell transplantation from HLA-identical related (n=6), HLA-mismatched family (n=2) or unrelated donors (n=9). Prophylaxis of acute graft-versus-host disease (GVHD) consisted of short-term methotrexate and cyclosporine (n=4) or short-term methotrexate and tacrolimus (n=13). RESULTS: No grade IV regimen-related toxicities as determined by Bearman's criteria were encountered. Acute grade II-IV GVHD developed in 7 patients, with chronic GVHD in 11 patients. With a median follow-up of 39 months, 3 years survival rate after transplantation was 59%. Two patients died due to infection by 100 days after transplantation. Only 1 patient with Philadelphia-positive acute lymphoblastic leukemia experienced relapse. Eight patients died of non-leukemic causes (sepsis, n=2; liver dysfunction, n=2; idiopathic interstitial pneumonia, n=1; bacterial pneumonia, n=1; bronchiolitis obliterans resulting from chronic GVHD, n=1; and disseminated infection with varicella zoster virus, n=1). CONCLUSIONS: This regimen was tolerable, but a large trial is warranted to confirm the efficacy of this conditioning. (+info)Daily insulin requirement of children and adolescents with type 1 diabetes: effect of age, gender, body mass index and mode of therapy. (6/205)
(+info)Individual fluorouracil dose adjustment based on pharmacokinetic follow-up compared with conventional dosage: results of a multicenter randomized trial of patients with metastatic colorectal cancer. (7/205)
(+info)Intravenous postoperative fluid prescriptions for children: a survey of practice. (8/205)
(+info)Drug dosage calculations refer to the process of determining the appropriate amount of a medication that should be administered to a patient, based on various factors such as the patient's weight, age, kidney and liver function, and the route of administration. The calculation is crucial to ensure that the patient receives a safe and effective dose, neither too much nor too little.
The formula used to calculate drug dosages may vary depending on the medication and the route of administration. For instance, the dosage for intravenous (IV) medications may be calculated based on the patient's body surface area, while oral medications may be dosed based on weight or age.
Accurate drug dosage calculations require a solid understanding of mathematical principles, as well as knowledge of the medication being administered and the patient's individual health status. Healthcare professionals, such as nurses, pharmacists, and physicians, are trained to perform these calculations and must adhere to strict protocols to minimize errors and ensure patient safety.
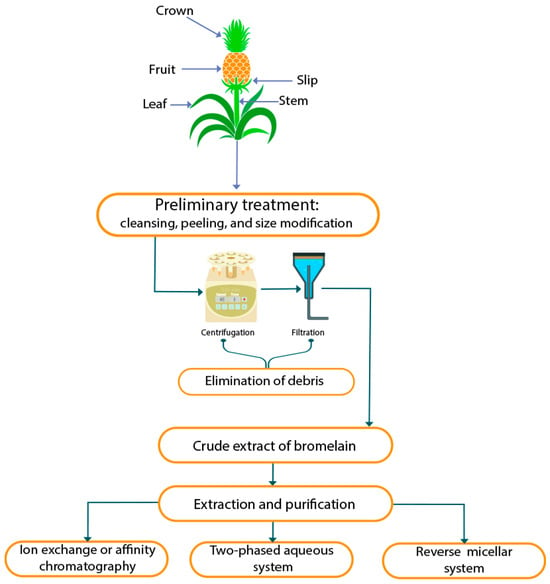
Pharmaceutical preparations refer to the various forms of medicines that are produced by pharmaceutical companies, which are intended for therapeutic or prophylactic use. These preparations consist of an active ingredient (the drug) combined with excipients (inactive ingredients) in a specific formulation and dosage form.
The active ingredient is the substance that has a therapeutic effect on the body, while the excipients are added to improve the stability, palatability, bioavailability, or administration of the drug. Examples of pharmaceutical preparations include tablets, capsules, solutions, suspensions, emulsions, ointments, creams, and injections.
The production of pharmaceutical preparations involves a series of steps that ensure the quality, safety, and efficacy of the final product. These steps include the selection and testing of raw materials, formulation development, manufacturing, packaging, labeling, and storage. Each step is governed by strict regulations and guidelines to ensure that the final product meets the required standards for use in medical practice.
Drug monitoring, also known as therapeutic drug monitoring (TDM), is a medical practice that involves testing blood or other bodily fluids to determine the concentration of a particular medication. This information is used to ensure that the patient is receiving an appropriate dosage and to help guide adjustments in medication therapy. It can be especially important for medications with a narrow therapeutic index, meaning that there is a small range between the effective dose and a toxic dose.
The goal of drug monitoring is to optimize medication effectiveness while minimizing potential side effects. This may involve measuring the concentration of a drug at various times after dosing to determine how quickly it is being metabolized or eliminated from the body, as well as to assess compliance with the prescribed treatment regimen.
Drug monitoring can be performed using a variety of methods, including immunoassays, chromatography, and mass spectrometry. The specific method used will depend on the drug being monitored and the level of sensitivity required. Results from drug monitoring tests are typically interpreted in conjunction with other clinical information, such as the patient's age, weight, renal function, liver function, and overall health status.
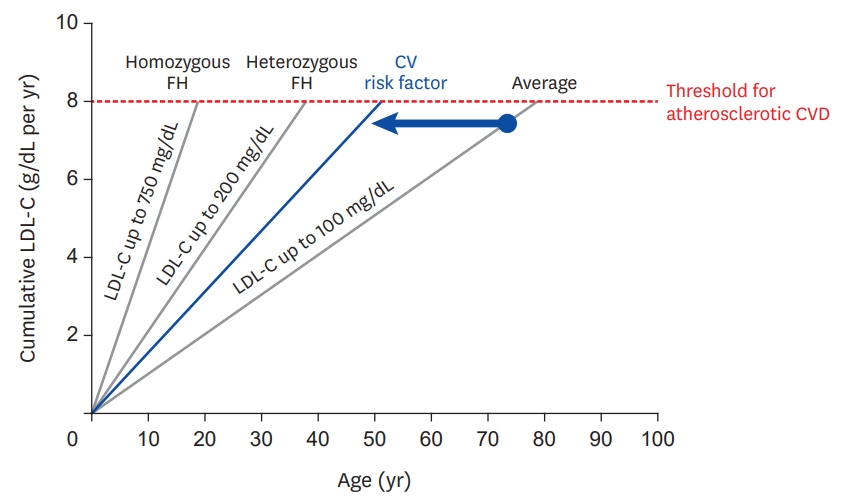
A dose-response relationship in the context of drugs refers to the changes in the effects or symptoms that occur as the dose of a drug is increased or decreased. Generally, as the dose of a drug is increased, the severity or intensity of its effects also increases. Conversely, as the dose is decreased, the effects of the drug become less severe or may disappear altogether.
The dose-response relationship is an important concept in pharmacology and toxicology because it helps to establish the safe and effective dosage range for a drug. By understanding how changes in the dose of a drug affect its therapeutic and adverse effects, healthcare providers can optimize treatment plans for their patients while minimizing the risk of harm.
The dose-response relationship is typically depicted as a curve that shows the relationship between the dose of a drug and its effect. The shape of the curve may vary depending on the drug and the specific effect being measured. Some drugs may have a steep dose-response curve, meaning that small changes in the dose can result in large differences in the effect. Other drugs may have a more gradual dose-response curve, where larger changes in the dose are needed to produce significant effects.
In addition to helping establish safe and effective dosages, the dose-response relationship is also used to evaluate the potential therapeutic benefits and risks of new drugs during clinical trials. By systematically testing different doses of a drug in controlled studies, researchers can identify the optimal dosage range for the drug and assess its safety and efficacy.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
 Imperial units
Imperial units 9780323310697 - Calculation of Drug Dosages: A Work Text by Sheila J. Ogden | eCampus.com
9780323310697 - Calculation of Drug Dosages: A Work Text by Sheila J. Ogden | eCampus.com Book-Organized: Ogden Calculation of Drug Dosages - Sherpath for Drug Calculations, 11th Edition - 9780323826051
Book-Organized: Ogden Calculation of Drug Dosages - Sherpath for Drug Calculations, 11th Edition - 9780323826051 Nursing Drug Dosage Calculation Test Questions and Answers
Nursing Drug Dosage Calculation Test Questions and Answers Dosage Calculations | Mathematical Association of America
Dosage Calculations | Mathematical Association of America Pediatric Dosage Calculations | Davis's Drug Guide
Pediatric Dosage Calculations | Davis's Drug Guide Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health
Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health Health Informatics BS | Minnesota State University, Mankato
Health Informatics BS | Minnesota State University, Mankato Pharmacy Technician - Belmont College
Pharmacy Technician - Belmont College Electronic Health Records (for Parents) - Helen DeVos
Electronic Health Records (for Parents) - Helen DeVos COURSE DESCRIPTIONS
COURSE DESCRIPTIONS Schedule of Classes
Schedule of Classes Nursing: Practical
- Sauk Valley Community College
Nursing: Practical
- Sauk Valley Community College TECH310-0121: Don't Sweat It, Just Calculate It: Building Confidence with Veterinary Calculations | Continual Education | VSPN
TECH310-0121: Don't Sweat It, Just Calculate It: Building Confidence with Veterinary Calculations | Continual Education | VSPN 4 chemical kinetics and stability | PPT
4 chemical kinetics and stability | PPT Vetcalculators on the App Store
Vetcalculators on the App Store Full-Time Pharmacy Technician - Waco, Texas - RPh on the Go
Full-Time Pharmacy Technician - Waco, Texas - RPh on the Go Medical Assistant - A.A.S. Degree - Dakota County Technical College | DCTC - a 2-Year Minnesota School Offering Associate...
Medical Assistant - A.A.S. Degree - Dakota County Technical College | DCTC - a 2-Year Minnesota School Offering Associate... MatthewsBooks.com - 9781719633505 (1719633509) : Upper Cape Cod/Full-Time Fall 2022 Package : Davis : : Books
MatthewsBooks.com - 9781719633505 (1719633509) : Upper Cape Cod/Full-Time Fall 2022 Package : Davis : : Books Brookhaven: 2018-2019 Catalog - Course Descriptions for HITT 2371
Brookhaven: 2018-2019 Catalog - Course Descriptions for HITT 2371 Mohammed Dalwai | Ashoka | Everyone a Changemaker
Mohammed Dalwai | Ashoka | Everyone a Changemaker Chapter 25 The Changing Paradigm in Preclinical Toxicology: in vitro and in silico Methods in Liver Toxicity Evaluations in:...
Chapter 25 The Changing Paradigm in Preclinical Toxicology: in vitro and in silico Methods in Liver Toxicity Evaluations in:... Improvements to Prescription Drug Monitoring Programs Can Inform Prescribing | The Pew Charitable Trusts
Improvements to Prescription Drug Monitoring Programs Can Inform Prescribing | The Pew Charitable Trusts