Cranial Nerves
Cranial Nerve Diseases
Cranial Nerve Injuries
Cranial Nerve Neoplasms
Abducens Nerve Diseases
Facial Nerve
Oculomotor Nerve Diseases
Sciatic Nerve
Glossopharyngeal Nerve
Oculomotor Nerve
Peripheral Nerves
Trigeminal Nerve
Abducens Nerve
Vestibulocochlear Nerve
Optic Nerve
Nerve Fibers
Mobius Syndrome
Nerve Compression Syndromes
Accessory Nerve
Ophthalmoplegia
Facial Paralysis
Trigeminal Nerve Diseases
Vestibulocochlear Nerve Diseases
Trochlear Nerve
Trigeminal Neuralgia
Paralysis
Facial Nerve Diseases
Skull Base Neoplasms
Facial Nerve Injuries
Hypoglossal Nerve
Glomus Jugulare Tumor
Nerve Block
Nerve Endings
Petrous Bone
Sural Nerve
Cavernous Sinus
Median Nerve
Tibial Nerve
Skull Base
Ulnar Nerve
Diplopia
Glossopharyngeal Nerve Diseases
Cranial Fossa, Posterior
Femoral Nerve
Magnetic Resonance Imaging
Spinal Nerves
Cochlear Nerve
Neurilemmoma
Nerve Growth Factor
Nerve Growth Factors
Facial Muscles
Neuroma, Acoustic
Vagus Nerve Injuries
Carotid Body Tumor
Phrenic Nerve
Duane Retraction Syndrome
Radial Nerve
Recurrent Laryngeal Nerve
Brain Stem
Spinal Nerve Roots
Meningeal Carcinomatosis
Hypoglossal Nerve Diseases
Olfactory Nerve
Ophthalmic Nerve
Neural Conduction
Temporal Bone
Meningitis, Aseptic
Nerve Tissue
Mandibular Nerve
Recurrent Laryngeal Nerve Injuries
Hemifacial Spasm
Oculomotor Muscles
Abducens Nerve Injury
Meningioma
Sphenoid Sinus
Rhombencephalon
Spasm
Splanchnic Nerves
Tongue
Vertigo
Meningeal Neoplasms
Neurologic Examination
Optic Nerve Injuries
Polyradiculoneuropathy
Horner Syndrome
Optic Nerve Diseases
Carotid Artery, Internal
Meninges
Herpes Zoster Oticus
Thoracic Nerves
Nerve Fibers, Myelinated
Neurofibromatosis 2
Brain Stem Neoplasms
Laryngeal Nerves
Endarterectomy, Carotid
Nerve Tissue Proteins
Infratentorial Neoplasms
Sympathetic Nervous System
Subarachnoid Space
Papilledema
Tomography, X-Ray Computed
Guillain-Barre Syndrome
Sphenoid Bone
Diabetic Neuropathies
Dura Mater
Branchial Region
Lingual Nerve
Pons
Neurologic Manifestations
Reflex, Abnormal
Bulbar Palsy, Progressive
Intracranial Aneurysm
Tuberculosis, Meningeal
Retrospective Studies
Fatal Outcome
Polyvinyls
Nerve Degeneration
Platybasia
Sagittal Sinus Thrombosis
Spinal Cord
Otitis Externa
Tinnitus
Embolization, Therapeutic
Ear
Botulism
Vocal Cord Paralysis
Vagus Nerve
Chemoreceptor Cells
Radiosurgery
Cerebellar Diseases
Miller Fisher Syndrome
Cats
Medulla Oblongata
Treatment Outcome
Maxillary Nerve
Neural Crest
Ganglia
Dysarthria
Nerve Sheath Neoplasms
Peripheral Nervous System Diseases
Receptors, Nerve Growth Factor
Bell Palsy
Brain Diseases
Decompression, Surgical
Meningitis
Taste Buds
Carotid Artery, External
Brain Stem Infarctions
Central Nervous System Diseases
Brain
Sciatic Neuropathy
Pituitary Apoplexy
Evoked Potentials, Auditory, Brain Stem
Epidermal Cyst
Cranial Sinuses
Nervous System
Chorda Tympani Nerve
Strabismus
Carotid Artery Diseases
Sarcoidosis
Gills
Follow-Up Studies
Vestibular Nerve
Skull Fractures
Immunohistochemistry
Nerve Fibers, Unmyelinated
Electromyography
Postoperative Complications
Reticular Formation
Central Nervous System
Carotid Stenosis
Differential distribution of retinoic acid synthesis in the chicken embryo as determined by immunolocalization of the retinoic acid synthetic enzyme, RALDH-2. (1/248)
Retinaldehyde dehydrogenase type 2 (RALDH-2) is a major retinoic acid generating enzyme in the early embryo. Here we report the immunolocalization of this enzyme (RALDH-2-IR) in stage 6-29 chicken embryos; we also show that tissues that exhibit strong RALDH-2-IR in the embryo contain RALDH-2 and synthesize retinoic acid. RALDH-2-IR indicates dynamic and discrete patterns of retinoic acid synthesis in the embryo, particularly within the somitic mesoderm, lateral mesoderm, kidney, heart, and spinal motor neurons. Prior to somitogenesis, RALDH-2-IR is present in the paraxial mesoderm with a rostral boundary at the level of the presumptive first somite; as the somites form, they exhibit strong RALDH-2-IR. Cervical presomitic mesoderm exhibits RALDH-2-IR but thoracic presomitic mesoderm does not. Neural crest cells do not express detectable levels of RALDH-2, but migrating crest cells are associated with RALDH-2 expressing mesoderm. The developing limb mesoderm expresses little RALDH-2-IR; however, RALDH-2-IR is strongly expressed in tissues adjacent to the limb. The most lateral, earliest-projecting motor neurons at all levels of the spinal cord exhibit RALDH-2-IR. Subsequently, many additional motor neurons in the brachial and lumbar cord regions express RALDH-2-IR. Motor neuronal expression of RALDH-2-IR is present in the growing axons as they extend to the periphery, indicating a potential role of retinoic acid in nerve influences on peripheral differentiation. With the exception of a transient expression in the facial/vestibulocochlear nucleus, cranial motor neurons do not express detectable levels of RALDH-2-IR. (+info)Chronic inflammatory demyelinating polyneuropathy with multiple hypertrophic nerves in intracranial, and intra- and extra-spinal segments. (2/248)
Hypertrophic nerves have occasionally been seen in chronic inflammatory demyelinating polyneuropathy (CIDP), but most are in the cauda equina. We report a case with CIDP in whom magnetic resonance imaging (MRI) with gadolinium diethylene triamine penta-acetic acid (Gd-DTPA) enhancement demonstrated hypertrophy of various peripheral nerves including multiple cranial nerves. Interestingly, none showed neurological signs corresponding to the lesions, except for clinical signs consistent with CIDP. MRI can be useful for the detection of silent, but abnormal nerve involvement in CIDP. (+info)Key roles of retinoic acid receptors alpha and beta in the patterning of the caudal hindbrain, pharyngeal arches and otocyst in the mouse. (3/248)
Mouse fetuses carrying targeted inactivations of both the RAR(&agr;) and the RARbeta genes display a variety of malformations in structures known to be partially derived from the mesenchymal neural crest originating from post-otic rhombomeres (e.g. thymus and great cephalic arteries) (Ghyselinck, N., Dupe, V., Dierich, A., Messaddeq, N., Garnier, J.M., Rochette-Egly, C., Chambon, P. and Mark M. (1997). Int. J. Dev. Biol. 41, 425-447). In a search for neural crest defects, we have analysed the rhombomeres, cranial nerves and pharyngeal arches of these double null mutants at early embryonic stages. The mutant post-otic cranial nerves are disorganized, indicating that RARs are involved in the patterning of structures derived from neurogenic neural crest, even though the lack of RARalpha and RARbeta has no detectable effect on the number and migration path of neural crest cells. Interestingly, the double null mutation impairs early developmental processes known to be independent of the neural crest e.g., the initial formation of the 3rd and 4th branchial pouches and of the 3rd, 4th and 6th arch arteries. The double mutation also results in an enlargement of rhombomere 5, which is likely to be responsible for the induction of supernumerary otic vesicles, in a disappearance of the rhombomere 5/6 boundary, and in profound alterations of rhombomere identities. In the mutant hindbrain, the expression domain of kreisler is twice its normal size and the caudal stripe of Krox-20 extends into the presumptive rhombomeres 6 and 7 region. In this region, Hoxb-1 is ectopically expressed, Hoxb-3 is ectopically up-regulated and Hoxd-4 expression is abolished. These data, which indicate that retinoic acid signaling through RARalpha and/or RARbeta is essential for the specification of rhombomere identities and for the control of caudal hindbrain segmentation by restricting the expression domains of kreisler and of Krox-20, also strongly suggest that this signaling plays a crucial role in the posteriorization of the hindbrain neurectoderm. (+info)Hepatocyte growth factor/scatter factor is a neurotrophic survival factor for lumbar but not for other somatic motoneurons in the chick embryo. (4/248)
Hepatocyte growth factor/scatter factor (HGF/SF) is expressed in the developing limb muscles of the chick embryo during the period of spinal motoneuron (MN) programmed cell death, and its receptor c-met is expressed in lumbar MNs during this same period. Although cultured motoneurons from brachial, thoracic, and lumbar segments are all rescued from cell death by chick embryo muscle extract (CMX) as well as by other specific trophic agents, HGF/SF only promotes the survival of lumbar MNs. Similarly, treatment of embryos in ovo with exogenous HGF/SF rescues lumbar but not other somatic MNs from cell death. Blocking antibodies to HGF/SF (anti-HGF) reduce the effects of CMX on MN survival in vitro and decrease the number of lumbar MNs in vivo. The expression of c-met on MNs in vivo is regulated by a limb-derived trophic signal distinct from HGF/SF. HGF/SF is a potent, select, and physiologically relevant survival factor for a subpopulation of developing spinal MNs in the lumbar segments of the chick embryo. (+info)Neuropilin-2 regulates the development of selective cranial and sensory nerves and hippocampal mossy fiber projections. (5/248)
Neuropilin-1 and neuropilin-2 bind differentially to different class 3 semaphorins and are thought to provide the ligand-binding moieties in receptor complexes mediating repulsive responses to these semaphorins. Here, we have studied the function of neuropilin-2 through analysis of a neuropilin-2 mutant mouse, which is viable and fertile. Repulsive responses of sympathetic and hippocampal neurons to Sema3F but not to Sema3A are abolished in the mutant. Marked defects are observed in the development of several cranial nerves, in the initial central projections of spinal sensory axons, and in the anterior commissure, habenulo-interpeduncular tract, and the projections of hippocampal mossyfiber axons in the infrapyramidal bundle. Our results show that neuropilin-2 is an essential component of the Sema3F receptor and identify key roles for neuropilin-2 in axon guidance in the PNS and CNS. (+info)Vitamin A deficiency results in the dose-dependent acquisition of anterior character and shortening of the caudal hindbrain of the rat embryo. (6/248)
The developing nervous system is particularly vulnerable to vitamin A deficiency. Retinoid has been proposed to be a posteriorizing factor during hindbrain development, although direct evidence in the mammalian embryo is lacking. In the present study, pregnant vitamin A-deficient (VAD) rats were fed purified diets containing varying levels of all-trans-retinoic acid (atRA; 0, 0.5, 1.5, 6, 12, 25, 50, 125, or 250 microg/g diet) or were supplemented with retinol. Hindbrain development was studied from embryonic day 10 to 12.5 ( approximately 6 to 40 somites). Normal morphogenesis was observed in all embryos from groups fed 250 microg atRA/g diet or retinol. The most caudal region of the hindbrain was the most sensitive to retinoid insufficiency, as evidenced by a loss of the hypoglossal nerve (cranial nerve XII) in embryos from the 125 microg atRA/g diet group. Further reduction of atRA to 50 microg/g diet led to the loss of cranial nerves IX, X, XI, and XII and associated sensory ganglia IX and X in all embryos as well as the loss of hindbrain segmentation caudal to the rhombomere (r) 3/4 border in a subset of embryos. Dysmorphic orthotopic otic vesicles or immature otic-like vesicles in both orthotopic and caudally ectopic locations were also observed. As the level of atRA was reduced, a loss of caudal hindbrain segmentation was observed in all embryos and the incidence of otic vesicle abnormalities increased. Perturbations in hindbrain segmentation, cranial nerve formation, and otic vesicle development were associated with abnormal patterning of the posterior hindbrain. Embryos from VAD dams fed between 0.5 and 50 microg atRA/g diet exhibited Hoxb-1 protein expression along the entire neural tube caudal to the r3/r4 border at a time when it should be restricted to r4. Krox-20 protein expression was expanded in r3 but absent or reduced in presumptive r5. Hoxd-4 mRNA expression was absent in the posterior hindbrain, and the rostral limit of Hoxb-5 protein expression in the neural tube was anteriorized, suggesting that the most posterior hindbrain region (r7/r8) had been deleted and/or improperly patterned. Thus, when limiting amounts of atRA are provided to VAD dams, the caudal portion of the hindbrain is shortened and possesses r4/r5-like characteristics, with this region finally exhibiting r4-like gene expression when retinoid is restricted even more severely. Thus, regions of the anterior hindbrain (i.e., r3 and r4) appear to be greatly expanded, whereas the posterior hindbrain (r5-r8) is reduced or absent. This work shows that retinoid plays a critical role in patterning, segmentation, and neurogenesis of the caudal hindbrain and serves as an essential posteriorizing signal for this region of the central nervous system in the mammal. (+info)Development of the cavernous sinus in the fetal period: a morphological study. (7/248)
The development and morphological structure of the lateral sellar compartment (LSC), an interdural space containing the cavernous sinus (CS), cranial nerves, and internal carotid artery (ICA), was investigated by histological examination of sections of the LSC and cerebral venograms from human fetal specimens. Twenty-eight LSC coronal sections were obtained from 14 fetuses of 13-32 weeks' gestation. Venograms of 11 other fetuses of 13-32 weeks' gestation were studied to observe changes in venous drainage. The CS appeared as a collection of small venous canals with an endothelial layer. These venous canals gradually became much larger through expansion and unification. The CS and basilar venous plexus were demonstrated as a faint cluster of small vessels on venograms obtained after 13 weeks' gestation. The dura mater increased in thickness and collagen fiber networks developed around all the components in the LSC after 23 weeks' gestation. The LSC lateral wall could not be histologically differentiated as separate multiple layers. Branching and joining of the cranial nerve fascicles were completed with the envelopment of collagen fibers after 23 weeks' gestation. The ICA at 13-15 weeks' gestation ran straight within the LSC, becoming tortuous before birth. CS formation occurs through the development of venous canals without smooth muscle layers, followed by web-formation by collagen fibers in the mesenchymal interstices. LSC formation, including the dense dura mater and an internal structure like that seen in the adult, is largely completed before birth. (+info)Facial palsy in cerebral venous thrombosis : transcranial stimulation and pathophysiological considerations. (8/248)
BACKGROUND: Cranial nerve palsy in cerebral sinovenous thrombosis (CVT) is rare, its pathophysiology remains unclear, and data from electrophysiological examinations in such patients are missing. CASE DESCRIPTION: We report the case of a 17-year-old woman with familial protein S deficiency who was admitted with extensive multiple CVT. Two weeks after onset of symptoms, she developed isolated right peripheral facial palsy, and MR venography showed segmental occlusion of the ipsilateral transverse sinus. Complete recovery of facial palsy occurred concomitant with recanalization of the transverse sinus. Facial neurography, including transcranial magnetic stimulation of the facial nerve and related motor cortex, ruled out a coincidental idiopathic palsy and revealed conduction block proximal to the facial canal. CONCLUSIONS: Facial palsy in our patient was caused by transient neurapraxia in the intracranial segment of the nerve. We suggest that elevated venous transmural pressure in the nerve's satellite vein, which belongs to the affected drainage territory of the transverse sinus, might have caused venous blood-brain barrier dysfunction in the intrinsic vascular system of the nerve, with leakage of fluids and ions into the endoneurial space and thus an increase in interstitial resistance. (+info)Cranial nerves are a set of twelve pairs of nerves that originate from the brainstem and skull, rather than the spinal cord. These nerves are responsible for transmitting sensory information (such as sight, smell, hearing, and taste) to the brain, as well as controlling various muscles in the head and neck (including those involved in chewing, swallowing, and eye movement). Each cranial nerve has a specific function and is named accordingly. For example, the optic nerve (cranial nerve II) transmits visual information from the eyes to the brain, while the vagus nerve (cranial nerve X) controls parasympathetic functions in the body such as heart rate and digestion.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
Cranial nerve injuries refer to damages or trauma to one or more of the twelve cranial nerves (CN I through CN XII). These nerves originate from the brainstem and are responsible for transmitting sensory information (such as vision, hearing, smell, taste, and balance) and controlling various motor functions (like eye movement, facial expressions, swallowing, and speaking).
Cranial nerve injuries can result from various causes, including head trauma, tumors, infections, or neurological conditions. The severity of the injury may range from mild dysfunction to complete loss of function, depending on the extent of damage to the nerve. Treatment options vary based on the type and location of the injury but often involve a combination of medical management, physical therapy, surgical intervention, or rehabilitation.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
The abducens nerve, also known as the sixth cranial nerve, is responsible for controlling the lateral rectus muscle of the eye, which enables the eye to move outward. Abducens nerve diseases refer to conditions that affect this nerve and can result in various symptoms, primarily affecting eye movement.
Here are some medical definitions related to abducens nerve diseases:
1. Abducens Nerve Palsy: A condition characterized by weakness or paralysis of the abducens nerve, causing difficulty in moving the affected eye outward. This results in double vision (diplopia), especially when gazing towards the side of the weakened nerve. Abducens nerve palsy can be congenital, acquired, or caused by various factors such as trauma, tumors, aneurysms, infections, or diseases like diabetes and multiple sclerosis.
2. Sixth Nerve Palsy: Another term for abducens nerve palsy, referring to the weakness or paralysis of the sixth cranial nerve.
3. Internuclear Ophthalmoplegia (INO): A neurological condition affecting eye movement, often caused by a lesion in the medial longitudinal fasciculus (MLF), a bundle of nerve fibers that connects the abducens nucleus with the oculomotor nucleus. INO results in impaired adduction (inward movement) of the eye on the side of the lesion and nystagmus (involuntary eye movements) of the abducting eye on the opposite side when attempting to look towards the side of the lesion.
4. One-and-a-Half Syndrome: A rare neurological condition characterized by a combination of INO and internuclear ophthalmoplegia with horizontal gaze palsy on the same side, caused by damage to both the abducens nerve and the paramedian pontine reticular formation (PPRF). This results in limited or no ability to move the eyes towards the side of the lesion and impaired adduction of the eye on the opposite side.
5. Brainstem Encephalitis: Inflammation of the brainstem, which can affect the abducens nerve and other cranial nerves, leading to various neurological symptoms such as diplopia (double vision), ataxia (loss of balance and coordination), and facial weakness. Brainstem encephalitis can be caused by infectious agents, autoimmune disorders, or paraneoplastic syndromes.
6. Multiple Sclerosis (MS): An autoimmune disorder characterized by inflammation and demyelination of the central nervous system, including the brainstem and optic nerves. MS can cause various neurological symptoms, such as diplopia, nystagmus, and INO, due to damage to the abducens nerve and other cranial nerves.
7. Wernicke's Encephalopathy: A neurological disorder caused by thiamine (vitamin B1) deficiency, often seen in alcoholics or individuals with malnutrition. Wernicke's encephalopathy can affect the brainstem and cause various symptoms such as diplopia, ataxia, confusion, and oculomotor abnormalities.
8. Pontine Glioma: A rare type of brain tumor that arises from the glial cells in the pons (a part of the brainstem). Pontine gliomas can cause various neurological symptoms such as diplopia, facial weakness, and difficulty swallowing due to their location in the brainstem.
9. Brainstem Cavernous Malformation: A benign vascular lesion that arises from the small blood vessels in the brainstem. Brainstem cavernous malformations can cause various neurological symptoms such as diplopia, ataxia, and facial weakness due to their location in the brainstem.
10. Pituitary Adenoma: A benign tumor that arises from the pituitary gland, located at the base of the brain. Large pituitary adenomas can compress the optic nerves and cause various visual symptoms such as diplopia, visual field defects, and decreased vision.
11. Craniopharyngioma: A benign tumor that arises from the remnants of the Rathke's pouch, a structure that gives rise to the anterior pituitary gland. Craniopharyngiomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the optic nerves and pituitary gland.
12. Meningioma: A benign tumor that arises from the meninges, the protective covering of the brain and spinal cord. Meningiomas can cause various neurological symptoms such as diplopia, headaches, and seizures depending on their location in the brain or spinal cord.
13. Chordoma: A rare type of malignant tumor that arises from the remnants of the notochord, a structure that gives rise to the spine during embryonic development. Chordomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the brainstem and spinal cord.
14. Metastatic Brain Tumors: Malignant tumors that spread from other parts of the body to the brain. Metastatic brain tumors can cause various neurological symptoms such as diplopia, headaches, seizures, and cognitive impairment depending on their location in the brain.
15. Other Rare Brain Tumors: There are many other rare types of brain tumors that can cause diplopia or other neurological symptoms, including gliomas, ependymomas, pineal region tumors, and others. These tumors require specialized diagnosis and treatment by neuro-oncologists and neurosurgeons with expertise in these rare conditions.
In summary, diplopia can be caused by various brain tumors, including pituitary adenomas, meningiomas, chordomas, metastatic brain tumors, and other rare types of tumors. It is important to seek medical attention promptly if you experience diplopia or other neurological symptoms, as early diagnosis and treatment can improve outcomes and quality of life.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
The oculomotor nerve, also known as the third cranial nerve (CN III), is responsible for controlling several important eye movements and functions. Oculomotor nerve diseases refer to conditions that affect this nerve and can lead to various symptoms related to eye movement and function. Here's a medical definition of oculomotor nerve diseases:
Oculomotor nerve diseases are a group of medical disorders characterized by the dysfunction or damage to the oculomotor nerve (CN III), resulting in impaired eye movements, abnormalities in pupillary response, and potential effects on eyelid position. These conditions can be congenital, acquired, or traumatic in nature and may lead to partial or complete paralysis of the nerve. Common oculomotor nerve diseases include oculomotor nerve palsy, third nerve ganglionopathies, and compressive oculomotor neuropathies caused by various pathologies such as aneurysms, tumors, or infections.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
The glossopharyngeal nerve, also known as the ninth cranial nerve (IX), is a mixed nerve that carries both sensory and motor fibers. It originates from the medulla oblongata in the brainstem and has several functions:
1. Sensory function: The glossopharyngeal nerve provides general sensation to the posterior third of the tongue, the tonsils, the back of the throat (pharynx), and the middle ear. It also carries taste sensations from the back one-third of the tongue.
2. Special visceral afferent function: The nerve transmits information about the stretch of the carotid artery and blood pressure to the brainstem.
3. Motor function: The glossopharyngeal nerve innervates the stylopharyngeus muscle, which helps elevate the pharynx during swallowing. It also provides parasympathetic fibers to the parotid gland, stimulating saliva production.
4. Visceral afferent function: The glossopharyngeal nerve carries information about the condition of the internal organs in the thorax and abdomen to the brainstem.
Overall, the glossopharyngeal nerve plays a crucial role in swallowing, taste, saliva production, and monitoring blood pressure and heart rate.
The oculomotor nerve, also known as the third cranial nerve (CN III), is a motor nerve that originates from the midbrain. It controls the majority of the eye muscles, including the levator palpebrae superioris muscle that raises the upper eyelid, and the extraocular muscles that enable various movements of the eye such as looking upward, downward, inward, and outward. Additionally, it carries parasympathetic fibers responsible for pupillary constriction and accommodation (focusing on near objects). Damage to this nerve can result in various ocular motor disorders, including strabismus, ptosis, and pupillary abnormalities.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
Hypoglossal nerve injuries refer to damages or impairments to the twelfth cranial nerve, also known as the hypoglossal nerve. This nerve is primarily responsible for controlling the movements of the tongue.
An injury to this nerve can result in various symptoms, depending on the severity and location of the damage. These may include:
1. Deviation of the tongue to one side when protruded (usually away from the side of the lesion)
2. Weakness or paralysis of the tongue muscles
3. Difficulty with speaking, swallowing, and articulation
4. Changes in taste and sensation on the back of the tongue (in some cases)
Hypoglossal nerve injuries can occur due to various reasons, such as trauma, surgical complications, tumors, or neurological disorders like stroke or multiple sclerosis. Treatment for hypoglossal nerve injuries typically focuses on managing symptoms and may involve speech and language therapy, exercises to strengthen the tongue muscles, and, in some cases, surgical intervention.
The trigeminal nerve, also known as the fifth cranial nerve or CNV, is a paired nerve that carries both sensory and motor information. It has three major branches: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic branch provides sensation to the forehead, eyes, and upper portion of the nose; the maxillary branch supplies sensation to the lower eyelid, cheek, nasal cavity, and upper lip; and the mandibular branch is responsible for sensation in the lower lip, chin, and parts of the oral cavity, as well as motor function to the muscles involved in chewing. The trigeminal nerve plays a crucial role in sensations of touch, pain, temperature, and pressure in the face and mouth, and it also contributes to biting, chewing, and swallowing functions.
The abducens nerve, also known as the sixth cranial nerve (CN VI), is a motor nerve that controls the lateral rectus muscle of the eye. This muscle is responsible for moving the eye away from the midline (towards the temple) and enables the eyes to look towards the side while keeping them aligned. Any damage or dysfunction of the abducens nerve can result in strabismus, where the eyes are misaligned and point in different directions, specifically an adduction deficit, also known as abducens palsy or sixth nerve palsy.
The vestibulocochlear nerve, also known as the auditory-vestibular nerve or cranial nerve VIII, is a paired peripheral nerve that transmits sensory information from the inner ear to the brain. It has two distinct parts: the cochlear part and the vestibular part.
The cochlear part is responsible for hearing and transmits sound signals from the cochlea to the brain. The vestibular part, on the other hand, is responsible for maintaining balance and spatial orientation by transmitting information about head movement and position from the vestibular apparatus (utricle, saccule, and semicircular canals) in the inner ear to the brain.
Together, these two parts of the vestibulocochlear nerve play a crucial role in our ability to hear and maintain balance. Damage to this nerve can result in hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), or balance problems.
The optic nerve, also known as the second cranial nerve, is the nerve that transmits visual information from the retina to the brain. It is composed of approximately one million nerve fibers that carry signals related to vision, such as light intensity and color, from the eye's photoreceptor cells (rods and cones) to the visual cortex in the brain. The optic nerve is responsible for carrying this visual information so that it can be processed and interpreted by the brain, allowing us to see and perceive our surroundings. Damage to the optic nerve can result in vision loss or impairment.
Nerve fibers are specialized structures that constitute the long, slender processes (axons) of neurons (nerve cells). They are responsible for conducting electrical impulses, known as action potentials, away from the cell body and transmitting them to other neurons or effector organs such as muscles and glands. Nerve fibers are often surrounded by supportive cells called glial cells and are grouped together to form nerve bundles or nerves. These fibers can be myelinated (covered with a fatty insulating sheath called myelin) or unmyelinated, which influences the speed of impulse transmission.
Möbius syndrome is a rare neurological disorder characterized by congenital facial palsy and abducens palsy, which are paralyses of the muscles that control lateral movement of the eye and facial expression. The condition is present at birth and is thought to be caused by underdevelopment of the cranial nerves (VI and VII) during embryonic development.
Individuals with Möbius syndrome may have a variety of symptoms, including:
* Inability to move the eyes from side to side
* Absent or weak facial expressions
* Difficulty with sucking, swallowing, and speaking
* Dental abnormalities
* Hearing loss
* Limb abnormalities
Möbius syndrome is typically diagnosed based on physical examination and medical history. There is no cure for the condition, but treatment may include physical therapy, speech therapy, and surgical interventions to improve function and appearance. The exact cause of Möbius syndrome is not known, but it is believed to be related to genetic or environmental factors during fetal development.
Nerve compression syndromes refer to a group of conditions characterized by the pressure or irritation of a peripheral nerve, causing various symptoms such as pain, numbness, tingling, and weakness in the affected area. This compression can occur due to several reasons, including injury, repetitive motion, bone spurs, tumors, or swelling. Common examples of nerve compression syndromes include carpal tunnel syndrome, cubital tunnel syndrome, radial nerve compression, and ulnar nerve entrapment at the wrist or elbow. Treatment options may include physical therapy, splinting, medications, injections, or surgery, depending on the severity and underlying cause of the condition.
The accessory nerve, also known as the eleventh cranial nerve (XI), has both a cranial and spinal component. It primarily controls the function of certain muscles in the back of the neck and shoulder.
The cranial part arises from nuclei in the brainstem and innervates some of the muscles that help with head rotation, including the sternocleidomastoid muscle. The spinal root originates from nerve roots in the upper spinal cord (C1-C5), exits the spine, and joins the cranial part to form a single trunk. This trunk then innervates the trapezius muscle, which helps with shoulder movement and stability.
Damage to the accessory nerve can result in weakness or paralysis of the affected muscles, causing symptoms such as difficulty turning the head, weak shoulder shrugging, or winged scapula (a condition where the shoulder blade protrudes from the back).
Laryngeal nerve injuries refer to damages or injuries to the recurrent laryngeal nerve (RLN) and/or the superior laryngeal nerve (SLN), which are the primary nerves that supply the larynx, or voice box. These nerves play crucial roles in controlling the vocal cord movements and protecting the airway during swallowing.
The recurrent laryngeal nerve provides motor function to all intrinsic muscles of the larynx, except for the cricothyroid muscle, which is innervated by the superior laryngeal nerve. The RLN also carries sensory fibers from a small area of the mucous membrane below the vocal folds.
Injuries to these nerves can result in voice changes, breathing difficulties, and swallowing problems. Depending on the severity and location of the injury, patients may experience hoarseness, weak voice, breathy voice, coughing while swallowing, or even complete airway obstruction in severe cases. Laryngeal nerve injuries can occur due to various reasons, such as surgical complications (e.g., thyroid, esophageal, and cardiovascular surgeries), neck trauma, tumors, infections, or iatrogenic causes.
Ophthalmoplegia is a medical term that refers to the paralysis or weakness of the eye muscles, which can result in double vision (diplopia) or difficulty moving the eyes. It can be caused by various conditions, including nerve damage, muscle disorders, or neurological diseases such as myasthenia gravis or multiple sclerosis. Ophthalmoplegia can affect one or more eye muscles and can be partial or complete. Depending on the underlying cause, ophthalmoplegia may be treatable with medications, surgery, or other interventions.
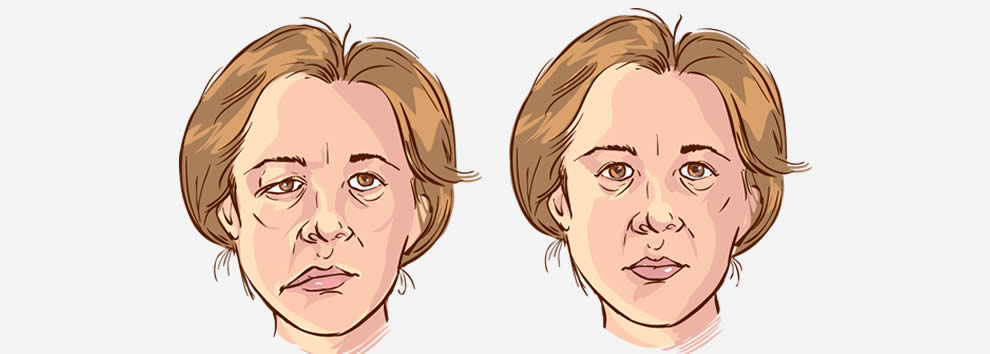
Facial paralysis is a loss of facial movement due to damage or dysfunction of the facial nerve (cranial nerve VII). This nerve controls the muscles involved in facial expressions, such as smiling, frowning, and closing the eyes. Damage to one side of the facial nerve can cause weakness or paralysis on that side of the face.
Facial paralysis can result from various conditions, including:
1. Bell's palsy - an idiopathic (unknown cause) inflammation of the facial nerve
2. Trauma - skull fractures, facial injuries, or surgical trauma to the facial nerve
3. Infections - Lyme disease, herpes zoster (shingles), HIV/AIDS, or bacterial infections like meningitis
4. Tumors - benign or malignant growths that compress or invade the facial nerve
5. Stroke - damage to the brainstem where the facial nerve originates
6. Congenital conditions - some people are born with facial paralysis due to genetic factors or birth trauma
Symptoms of facial paralysis may include:
* Inability to move one or more parts of the face, such as the eyebrows, eyelids, mouth, or cheeks
* Drooping of the affected side of the face
* Difficulty closing the eye on the affected side
* Changes in saliva and tear production
* Altered sense of taste
* Pain around the ear or jaw
* Speech difficulties due to weakened facial muscles
Treatment for facial paralysis depends on the underlying cause. In some cases, such as Bell's palsy, spontaneous recovery may occur within a few weeks to months. However, physical therapy, medications, and surgical interventions might be necessary in other situations to improve function and minimize complications.
Trigeminal nerve diseases refer to conditions that affect the trigeminal nerve, which is one of the cranial nerves responsible for sensations in the face and motor functions such as biting and chewing. The trigeminal nerve has three branches: ophthalmic, maxillary, and mandibular, which innervate different parts of the face and head.
Trigeminal nerve diseases can cause various symptoms, including facial pain, numbness, tingling, or weakness. Some common trigeminal nerve diseases include:
1. Trigeminal neuralgia: A chronic pain condition that affects the trigeminal nerve, causing intense, stabbing, or electric shock-like pain in the face.
2. Hemifacial spasm: A neuromuscular disorder that causes involuntary muscle spasms on one side of the face, often affecting the muscles around the eye and mouth.
3. Trigeminal neuropathy: Damage or injury to the trigeminal nerve, which can result in numbness, tingling, or weakness in the face.
4. Herpes zoster oticus (Ramsay Hunt syndrome): A viral infection that affects the facial nerve and geniculate ganglion of the trigeminal nerve, causing facial paralysis, ear pain, and a rash around the ear.
5. Microvascular compression: Compression of the trigeminal nerve by a blood vessel, which can cause symptoms similar to trigeminal neuralgia.
Treatment for trigeminal nerve diseases depends on the specific condition and its severity. Treatment options may include medication, surgery, or radiation therapy.
The vestibulocochlear nerve, also known as the 8th cranial nerve, is responsible for transmitting sound and balance information from the inner ear to the brain. Vestibulocochlear nerve diseases refer to conditions that affect this nerve and can result in hearing loss, vertigo, and balance problems.
These diseases can be caused by various factors, including genetics, infection, trauma, tumors, or degeneration. Some examples of vestibulocochlear nerve diseases include:
1. Vestibular neuritis: an inner ear infection that causes severe vertigo, nausea, and balance problems.
2. Labyrinthitis: an inner ear infection that affects both the vestibular and cochlear nerves, causing vertigo, hearing loss, and tinnitus.
3. Acoustic neuroma: a benign tumor that grows on the vestibulocochlear nerve, causing hearing loss, tinnitus, and balance problems.
4. Meniere's disease: a inner ear disorder that causes vertigo, hearing loss, tinnitus, and a feeling of fullness in the ear.
5. Ototoxicity: damage to the inner ear caused by certain medications or chemicals that can result in hearing loss and balance problems.
6. Vestibular migraine: a type of migraine that is associated with vertigo, dizziness, and balance problems.
Treatment for vestibulocochlear nerve diseases varies depending on the specific condition and its severity. It may include medication, physical therapy, surgery, or a combination of these approaches.
Nerve regeneration is the process of regrowth and restoration of functional nerve connections following damage or injury to the nervous system. This complex process involves various cellular and molecular events, such as the activation of support cells called glia, the sprouting of surviving nerve fibers (axons), and the reformation of neural circuits. The goal of nerve regeneration is to enable the restoration of normal sensory, motor, and autonomic functions impaired due to nerve damage or injury.
The trochlear nerve, also known as the fourth cranial nerve (CN IV), is a nerve that originates in the midbrain and innervates the superior oblique muscle of the eye. This muscle helps with the downward and outward movement of the eye, playing a crucial role in controlling eye movements and maintaining binocular vision. The trochlear nerve's main function is to provide motor (efferent) innervation to the superior oblique muscle, enabling fine-tuning of eye movements during activities such as reading, writing, or driving. Damage to this nerve can result in vertical diplopia (double vision), strabismus (eye misalignment), and other visual impairments.
Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which is one of the largest nerves in the head. It carries sensations from the face to the brain.
Medically, trigeminal neuralgia is defined as a neuropathic disorder characterized by episodes of intense, stabbing, electric shock-like pain in the areas of the face supplied by the trigeminal nerve (the ophthalmic, maxillary, and mandibular divisions). The pain can be triggered by simple activities such as talking, eating, brushing teeth, or even touching the face lightly.
The condition is more common in women over 50, but it can occur at any age and in either gender. While the exact cause of trigeminal neuralgia is not always known, it can sometimes be related to pressure on the trigeminal nerve from a nearby blood vessel or other causes such as multiple sclerosis. Treatment typically involves medications, surgery, or a combination of both.
Paralysis is a loss of muscle function in part or all of your body. It can be localized, affecting only one specific area, or generalized, impacting multiple areas or even the entire body. Paralysis often occurs when something goes wrong with the way messages pass between your brain and muscles. In most cases, paralysis is caused by damage to the nervous system, especially the spinal cord. Other causes include stroke, trauma, infections, and various neurological disorders.
It's important to note that paralysis doesn't always mean a total loss of movement or feeling. Sometimes, it may just cause weakness or numbness in the affected area. The severity and extent of paralysis depend on the underlying cause and the location of the damage in the nervous system.
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
The cerebellopontine angle (CPA) is a narrow space located at the junction of the brainstem and the cerebellum, where the pons and cerebellum meet. This region is filled with several important nerves, blood vessels, and membranous coverings called meninges. The CPA is a common site for various neurological disorders because it contains critical structures such as:
1. Cerebellum: A part of the brain responsible for coordinating muscle movements, maintaining balance, and fine-tuning motor skills.
2. Pons: A portion of the brainstem that plays a role in several vital functions, including facial movements, taste sensation, sleep regulation, and respiration.
3. Cranial nerves: The CPA is home to the following cranial nerves:
* Vestibulocochlear nerve (CN VIII): This nerve has two components - cochlear and vestibular. The cochlear part is responsible for hearing, while the vestibular part contributes to balance and eye movement.
* Facial nerve (CN VII): This nerve controls facial expressions, taste sensation in the anterior two-thirds of the tongue, salivary gland function, and lacrimation (tear production).
4. Blood vessels: The CPA contains critical blood vessels like the anterior inferior cerebellar artery (AICA), which supplies blood to various parts of the brainstem, cerebellum, and cranial nerves.
5. Meninges: These are protective membranes surrounding the brain and spinal cord. In the CPA, the meninges include the dura mater, arachnoid mater, and pia mater.
Disorders that can affect the structures in the cerebellopontine angle include acoustic neuromas (vestibular schwannomas), meningiomas, epidermoids, and arteriovenous malformations. These conditions may cause symptoms such as hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), facial weakness or numbness, difficulty swallowing, and imbalance.
Skull base neoplasms refer to abnormal growths or tumors located in the skull base, which is the region where the skull meets the spine and where the brain connects with the blood vessels and nerves that supply the head and neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells in this area, including bone, nerve, glandular, and vascular tissue.
Skull base neoplasms can cause a range of symptoms depending on their size, location, and growth rate. Some common symptoms include headaches, vision changes, hearing loss, facial numbness or weakness, difficulty swallowing, and balance problems. Treatment options for skull base neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. The specific treatment plan will depend on the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history.
Facial nerve injuries refer to damages or trauma inflicted on the facial nerve, also known as the seventh cranial nerve (CN VII). This nerve is responsible for controlling the muscles involved in facial expressions, eyelid movement, and taste sensation in the front two-thirds of the tongue.
There are two main types of facial nerve injuries:
1. Peripheral facial nerve injury: This type of injury occurs when damage affects the facial nerve outside the skull base, usually due to trauma from cuts, blunt force, or surgical procedures in the parotid gland or neck region. The injury may result in weakness or paralysis on one side of the face, known as Bell's palsy, and may also impact taste sensation and salivary function.
2. Central facial nerve injury: This type of injury occurs when damage affects the facial nerve within the skull base, often due to stroke, brain tumors, or traumatic brain injuries. Central facial nerve injuries typically result in weakness or paralysis only on the lower half of the face, as the upper motor neurons responsible for controlling the upper face receive innervation from both sides of the brain.
Treatment for facial nerve injuries depends on the severity and location of the damage. For mild to moderate injuries, physical therapy, protective eyewear, and medications like corticosteroids and antivirals may be prescribed. Severe cases might require surgical intervention, such as nerve grafts or muscle transfers, to restore function. In some instances, facial nerve injuries may heal on their own over time, particularly when the injury is mild and there is no ongoing compression or tension on the nerve.
A Trochlear nerve injury, also known as Fourth cranial nerve palsy, refers to damage or dysfunction of the fourth cranial nerve (trochlear nerve). This nerve is responsible for controlling the movement of the eye's superior oblique muscle, which helps in downward and outward movement of the eye.
Trochlear nerve injuries can result in vertical diplopia (double vision), where images appear double when looking downwards or to the side. The diplopia may be worse when looking down and out, such as when walking down stairs or reading.
The injury can be caused by various factors including head trauma, increased intracranial pressure, tumors, aneurysms, or other neurological conditions. Treatment options depend on the severity and cause of the injury and may include eye patches, prism lenses, or surgical intervention in some cases.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for innervating the muscles of the tongue, allowing for its movement and function. These muscles include the intrinsic muscles that alter the shape of the tongue and the extrinsic muscles that position it in the oral cavity. The hypoglossal nerve also has some minor contributions to the innervation of two muscles in the neck: the sternocleidomastoid and the trapezius. These functions are related to head turning and maintaining head position. Any damage to this nerve can lead to weakness or paralysis of the tongue, causing difficulty with speech, swallowing, and tongue movements.
A Glomus Jugulare Tumor is a rare, usually benign, slow-growing tumor that develops from the glomus body, a small collection of modified blood vessels involved in temperature regulation, located near the jugular bulb in the skull. This type of tumor can cause symptoms such as hearing loss, pulsatile tinnitus (a rhythmic sound in the ear), and cranial nerve palsies due to its proximity to critical structures in the head and neck. Treatment typically involves surgical removal or radiation therapy.
A nerve block is a medical procedure in which an anesthetic or neurolytic agent is injected near a specific nerve or bundle of nerves to block the transmission of pain signals from that area to the brain. This technique can be used for both diagnostic and therapeutic purposes, such as identifying the source of pain, providing temporary or prolonged relief, or facilitating surgical procedures in the affected region.
The injection typically contains a local anesthetic like lidocaine or bupivacaine, which numbs the nerve, preventing it from transmitting pain signals. In some cases, steroids may also be added to reduce inflammation and provide longer-lasting relief. Depending on the type of nerve block and its intended use, the injection might be administered close to the spine (neuraxial blocks), at peripheral nerves (peripheral nerve blocks), or around the sympathetic nervous system (sympathetic nerve blocks).
While nerve blocks are generally safe, they can have side effects such as infection, bleeding, nerve damage, or in rare cases, systemic toxicity from the anesthetic agent. It is essential to consult with a qualified medical professional before undergoing this procedure to ensure proper evaluation, technique, and post-procedure care.
Nerve endings, also known as terminal branches or sensory receptors, are the specialized structures present at the termination point of nerve fibers (axons) that transmit electrical signals to and from the central nervous system (CNS). They primarily function in detecting changes in the external environment or internal body conditions and converting them into electrical impulses.
There are several types of nerve endings, including:
1. Free Nerve Endings: These are unencapsulated nerve endings that respond to various stimuli like temperature, pain, and touch. They are widely distributed throughout the body, especially in the skin, mucous membranes, and visceral organs.
2. Encapsulated Nerve Endings: These are wrapped by specialized connective tissue sheaths, which can modify their sensitivity to specific stimuli. Examples include Pacinian corpuscles (responsible for detecting deep pressure and vibration), Meissner's corpuscles (for light touch), Ruffini endings (for stretch and pressure), and Merkel cells (for sustained touch).
3. Specialised Nerve Endings: These are nerve endings that respond to specific stimuli, such as auditory, visual, olfactory, gustatory, and vestibular information. They include hair cells in the inner ear, photoreceptors in the retina, taste buds in the tongue, and olfactory receptors in the nasal cavity.
Nerve endings play a crucial role in relaying sensory information to the CNS for processing and initiating appropriate responses, such as reflex actions or conscious perception of the environment.
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
The sural nerve is a purely sensory peripheral nerve in the lower leg and foot. It provides sensation to the outer ( lateral) aspect of the little toe and the adjacent side of the fourth toe, as well as a small portion of the skin on the back of the leg between the ankle and knee joints.
The sural nerve is formed by the union of branches from the tibial and common fibular nerves (branches of the sciatic nerve) in the lower leg. It runs down the calf, behind the lateral malleolus (the bony prominence on the outside of the ankle), and into the foot.
The sural nerve is often used as a donor nerve during nerve grafting procedures due to its consistent anatomy and relatively low risk for morbidity at the donor site.
The cavernous sinus is a venous structure located in the middle cranial fossa, which is a depression in the skull that houses several important nerves and blood vessels. The cavernous sinus is situated on either side of the sphenoid bone, near the base of the skull, and it contains several important structures:
* The internal carotid artery, which supplies oxygenated blood to the brain
* The abducens nerve (cranial nerve VI), which controls lateral movement of the eye
* The oculomotor nerve (cranial nerve III), which controls most of the muscles that move the eye
* The trochlear nerve (cranial nerve IV), which controls one of the muscles that moves the eye
* The ophthalmic and maxillary divisions of the trigeminal nerve (cranial nerve V), which transmit sensory information from the face and head
The cavernous sinus is an important structure because it serves as a conduit for several critical nerves and blood vessels. However, it is also vulnerable to various pathological conditions such as thrombosis (blood clots), infection, tumors, or aneurysms, which can lead to serious neurological deficits or even death.
The median nerve is one of the major nerves in the human body, providing sensation and motor function to parts of the arm and hand. It originates from the brachial plexus, a network of nerves that arise from the spinal cord in the neck. The median nerve travels down the arm, passing through the cubital tunnel at the elbow, and continues into the forearm and hand.
In the hand, the median nerve supplies sensation to the palm side of the thumb, index finger, middle finger, and half of the ring finger. It also provides motor function to some of the muscles that control finger movements, allowing for flexion of the fingers and opposition of the thumb.
Damage to the median nerve can result in a condition called carpal tunnel syndrome, which is characterized by numbness, tingling, and weakness in the hand and fingers.
A nerve crush injury is a type of peripheral nerve injury that occurs when there is excessive pressure or compression applied to a nerve, causing it to become damaged or dysfunctional. This can happen due to various reasons such as trauma from accidents, surgical errors, or prolonged pressure on the nerve from tight casts, clothing, or positions.
The compression disrupts the normal functioning of the nerve, leading to symptoms such as numbness, tingling, weakness, or pain in the affected area. In severe cases, a nerve crush injury can cause permanent damage to the nerve, leading to long-term disability or loss of function. Treatment for nerve crush injuries typically involves relieving the pressure on the nerve, providing supportive care, and in some cases, surgical intervention may be necessary to repair the damaged nerve.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
The Tibial nerve is a major branch of the sciatic nerve that originates in the lower back and runs through the buttock and leg. It provides motor (nerve impulses that control muscle movement) and sensory (nerve impulses that convey information about touch, temperature, and pain) innervation to several muscles and skin regions in the lower limb.
More specifically, the Tibial nerve supplies the following structures:
1. Motor Innervation: The Tibial nerve provides motor innervation to the muscles in the back of the leg (posterior compartment), including the calf muscles (gastrocnemius and soleus) and the small muscles in the foot (intrinsic muscles). These muscles are responsible for plantarflexion (pointing the foot downward) and inversion (turning the foot inward) of the foot.
2. Sensory Innervation: The Tibial nerve provides sensory innervation to the skin on the sole of the foot, as well as the heel and some parts of the lower leg.
The Tibial nerve travels down the leg, passing behind the knee and through the calf, where it eventually joins with the common fibular (peroneal) nerve to form the tibial-fibular trunk. This trunk then divides into several smaller nerves that innervate the foot's intrinsic muscles and skin.
Damage or injury to the Tibial nerve can result in various symptoms, such as weakness or paralysis of the calf and foot muscles, numbness or tingling sensations in the sole of the foot, and difficulty walking or standing on tiptoes.
The skull base is the lower part of the skull that forms the floor of the cranial cavity and the roof of the facial skeleton. It is a complex anatomical region composed of several bones, including the frontal, sphenoid, temporal, occipital, and ethmoid bones. The skull base supports the brain and contains openings for blood vessels and nerves that travel between the brain and the face or neck. The skull base can be divided into three regions: the anterior cranial fossa, middle cranial fossa, and posterior cranial fossa, which house different parts of the brain.
The Ulnar nerve is one of the major nerves in the forearm and hand, which provides motor function to the majority of the intrinsic muscles of the hand (except for those innervated by the median nerve) and sensory innervation to the little finger and half of the ring finger. It originates from the brachial plexus, passes through the cubital tunnel at the elbow, and continues down the forearm, where it runs close to the ulna bone. The ulnar nerve then passes through the Guyon's canal in the wrist before branching out to innervate the hand muscles and provide sensation to the skin on the little finger and half of the ring finger.
Diplopia is a medical term that refers to the condition where a person sees two images of a single object. It is commonly known as double vision. This can occur due to various reasons, such as nerve damage or misalignment of the eyes. Diplopia can be temporary or chronic and can affect one or both eyes. If you're experiencing diplopia, it's essential to consult an eye care professional for proper evaluation and treatment.
The glossopharyngeal nerve, also known as the ninth cranial nerve (CN IX), is primarily responsible for providing motor innervation to the stylopharyngeus muscle and sensory innervation to parts of the pharynx, middle ear, and posterior tongue. It also plays a role in the reflexive control of heart rate via the baroreceptors located in the carotid sinus.
Glossopharyngeal nerve diseases refer to conditions that affect the function of this nerve, leading to various symptoms. These diseases can be classified into two main categories: peripheral and central. Peripheral disorders are caused by damage or injury to the nerve itself, while central disorders result from problems in the brainstem where the glossopharyngeal nerve originates.
Some examples of glossopharyngeal nerve diseases include:
1. Glossopharyngeal neuralgia: A rare condition characterized by severe, stabbing pain in the throat, ear, or tongue, often triggered by swallowing or talking. This disorder may be caused by compression of the nerve by blood vessels or other structures.
2. Infections: Bacterial and viral infections can cause inflammation and damage to the glossopharyngeal nerve, leading to dysfunction. Examples include Lyme disease, herpes zoster (shingles), and meningitis.
3. Tumors: Benign or malignant growths in the head and neck region can compress and injure the glossopharyngeal nerve, resulting in symptoms related to its dysfunction.
4. Trauma: Direct trauma to the neck or skull base can damage the glossopharyngeal nerve, causing various deficits depending on the severity of the injury.
5. Neurological disorders: Conditions such as multiple sclerosis and stroke can affect the central connections of the glossopharyngeal nerve in the brainstem, leading to dysfunction.
6. Genetic conditions: Rare genetic disorders like Moersch-Woltman syndrome (also known as stiff person syndrome) can involve the glossopharyngeal nerve and cause symptoms related to its dysfunction.
Symptoms of glossopharyngeal nerve dysfunction may include difficulty swallowing, hoarseness, loss of taste on the back of the tongue, decreased sensation in the throat or ear, and pain in the neck, throat, or ear. Treatment for these conditions depends on the underlying cause and may involve medications, surgery, or other interventions to address the specific problem.
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
The femoral nerve is a major nerve in the thigh region of the human body. It originates from the lumbar plexus, specifically from the ventral rami (anterior divisions) of the second, third, and fourth lumbar nerves (L2-L4). The femoral nerve provides motor and sensory innervation to various muscles and areas in the lower limb.
Motor Innervation:
The femoral nerve is responsible for providing motor innervation to several muscles in the anterior compartment of the thigh, including:
1. Iliacus muscle
2. Psoas major muscle
3. Quadriceps femoris muscle (consisting of four heads: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius)
These muscles are involved in hip flexion, knee extension, and stabilization of the hip joint.
Sensory Innervation:
The sensory distribution of the femoral nerve includes:
1. Anterior and medial aspects of the thigh
2. Skin over the anterior aspect of the knee and lower leg (via the saphenous nerve, a branch of the femoral nerve)
The saphenous nerve provides sensation to the skin on the inner side of the leg and foot, as well as the medial malleolus (the bony bump on the inside of the ankle).
In summary, the femoral nerve is a crucial component of the lumbar plexus that controls motor functions in the anterior thigh muscles and provides sensory innervation to the anterior and medial aspects of the thigh and lower leg.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Spinal nerves are the bundles of nerve fibers that transmit signals between the spinal cord and the rest of the body. There are 31 pairs of spinal nerves in the human body, which can be divided into five regions: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve carries both sensory information (such as touch, temperature, and pain) from the periphery to the spinal cord, and motor information (such as muscle control) from the spinal cord to the muscles and other structures in the body. Spinal nerves also contain autonomic fibers that regulate involuntary functions such as heart rate, digestion, and blood pressure.
The cochlear nerve, also known as the auditory nerve, is the sensory nerve that transmits sound signals from the inner ear to the brain. It consists of two parts: the outer spiral ganglion and the inner vestibular portion. The spiral ganglion contains the cell bodies of the bipolar neurons that receive input from hair cells in the cochlea, which is the snail-shaped organ in the inner ear responsible for hearing. These neurons then send their axons to form the cochlear nerve, which travels through the internal auditory meatus and synapses with neurons in the cochlear nuclei located in the brainstem.
Damage to the cochlear nerve can result in hearing loss or deafness, depending on the severity of the injury. Common causes of cochlear nerve damage include acoustic trauma, such as exposure to loud noises, viral infections, meningitis, and tumors affecting the nerve or surrounding structures. In some cases, cochlear nerve damage may be treated with hearing aids, cochlear implants, or other assistive devices to help restore or improve hearing function.
A neurilemmoma, also known as schwannoma or peripheral nerve sheath tumor, is a benign, slow-growing tumor that arises from the Schwann cells, which produce the myelin sheath that surrounds and insulates peripheral nerves. These tumors can occur anywhere along the course of a peripheral nerve, but they most commonly affect the acoustic nerve (vestibulocochlear nerve), leading to a type of tumor called vestibular schwannoma or acoustic neuroma. Neurilemmomas are typically encapsulated and do not invade the surrounding tissue, although larger ones may cause pressure-related symptoms due to compression of nearby structures. Rarely, these tumors can undergo malignant transformation, leading to a condition called malignant peripheral nerve sheath tumor or neurofibrosarcoma.
The glossopharyngeal nerve (cranial nerve IX) is a mixed nerve that provides both sensory and motor functions to the posterior third of the tongue, the pharynx, the middle ear, and parts of the palate and neck. Glossopharyngeal nerve injuries refer to damages or trauma to this nerve, which can result in various symptoms:
1. Ipsilateral loss of taste sensation on the posterior one-third of the tongue.
2. Difficulty swallowing (dysphagia) and speaking due to paralysis of the associated muscles.
3. Reduced sensitivity to touch, pressure, and temperature in the affected areas.
4. Impaired or absent gag reflex on the side of the injury.
5. Pain in the ear (otalgia), throat, or neck.
6. Hoarseness or weak voice due to vocal cord paralysis.
Glossopharyngeal nerve injuries can occur due to various reasons, such as trauma, tumors, surgical complications, or neurological disorders like multiple sclerosis and stroke. Proper diagnosis and management of these injuries require a thorough examination by a healthcare professional, often involving a detailed clinical evaluation and imaging studies.
Neuroradiography is a subspecialty of radiology that focuses on the diagnosis and treatment of medical conditions related to the nervous system, including the brain, spine, and peripheral nerves, using various imaging techniques. These techniques may include X-rays, computed tomography (CT) scans, magnetic resonance imaging (MRI), positron emission tomography (PET) scans, and angiography. Neuroradiographers use these tools to identify and diagnose a wide range of conditions, such as tumors, strokes, aneurysms, spinal cord injuries, and degenerative diseases. They work closely with other medical specialists, such as neurologists and neurosurgeons, to provide comprehensive care for patients with neurological disorders.
Nerve Growth Factor (NGF) is a small secreted protein that is involved in the growth, maintenance, and survival of certain neurons (nerve cells). It was the first neurotrophin to be discovered and is essential for the development and function of the nervous system. NGF binds to specific receptors on the surface of nerve cells and helps to promote their differentiation, axonal growth, and synaptic plasticity. Additionally, NGF has been implicated in various physiological processes such as inflammation, immune response, and wound healing. Deficiencies or excesses of NGF have been linked to several neurological disorders, including Alzheimer's disease, Parkinson's disease, and pain conditions.
Nerve Growth Factors (NGFs) are a family of proteins that play an essential role in the growth, maintenance, and survival of certain neurons (nerve cells). They were first discovered by Rita Levi-Montalcini and Stanley Cohen in 1956. NGF is particularly crucial for the development and function of the peripheral nervous system, which connects the central nervous system to various organs and tissues throughout the body.
NGF supports the differentiation and survival of sympathetic and sensory neurons during embryonic development. In adults, NGF continues to regulate the maintenance and repair of these neurons, contributing to neuroplasticity – the brain's ability to adapt and change over time. Additionally, NGF has been implicated in pain transmission and modulation, as well as inflammatory responses.
Abnormal levels or dysfunctional NGF signaling have been associated with various medical conditions, including neurodegenerative diseases (e.g., Alzheimer's and Parkinson's), chronic pain disorders, and certain cancers (e.g., small cell lung cancer). Therefore, understanding the role of NGF in physiological and pathological processes may provide valuable insights into developing novel therapeutic strategies for these conditions.
Facial muscles, also known as facial nerves or cranial nerve VII, are a group of muscles responsible for various expressions and movements of the face. These muscles include:
1. Orbicularis oculi: muscle that closes the eyelid and raises the upper eyelid
2. Corrugator supercilii: muscle that pulls the eyebrows down and inward, forming wrinkles on the forehead
3. Frontalis: muscle that raises the eyebrows and forms horizontal wrinkles on the forehead
4. Procerus: muscle that pulls the medial ends of the eyebrows downward, forming vertical wrinkles between the eyebrows
5. Nasalis: muscle that compresses or dilates the nostrils
6. Depressor septi: muscle that pulls down the tip of the nose
7. Levator labii superioris alaeque nasi: muscle that raises the upper lip and flares the nostrils
8. Levator labii superioris: muscle that raises the upper lip
9. Zygomaticus major: muscle that raises the corner of the mouth, producing a smile
10. Zygomaticus minor: muscle that raises the nasolabial fold and corner of the mouth
11. Risorius: muscle that pulls the angle of the mouth laterally, producing a smile
12. Depressor anguli oris: muscle that pulls down the angle of the mouth
13. Mentalis: muscle that raises the lower lip and forms wrinkles on the chin
14. Buccinator: muscle that retracts the cheek and helps with chewing
15. Platysma: muscle that depresses the corner of the mouth and wrinkles the skin of the neck.
These muscles are innervated by the facial nerve, which arises from the brainstem and exits the skull through the stylomastoid foramen. Damage to the facial nerve can result in facial paralysis or weakness on one or both sides of the face.
An acoustic neuroma, also known as vestibular schwannoma, is not actually a neuroma but rather a benign (noncancerous) tumor that develops on the vestibular nerve. This nerve is one of the two nerves that transmit sound and balance information from the inner ear to the brain. The tumor arises from an overproduction of Schwann cells, which normally provide a protective covering for the nerve fibers. As the tumor grows, it can press against the hearing and balance nerves, causing symptoms such as hearing loss, ringing in the ear (tinnitus), unsteadiness, and disequilibrium. In some cases, acoustic neuromas can become quite large and cause additional symptoms by pressing on nearby cranial nerves. Treatment options include observation, radiation therapy, or surgical removal of the tumor.
Vagus nerve injuries refer to damages or traumas affecting the vagus nerve, which is the tenth cranial nerve (CN X) in the human body. This nerve plays a crucial role in the autonomic nervous system, regulating essential functions such as heart rate, respiratory rate, and digestion.
Vagus nerve injuries can occur due to various reasons, including trauma during surgical procedures, neck or head injuries, inflammation, compression, or tumors affecting the nerve. Symptoms of vagus nerve injuries may include:
1. Hoarseness or voice changes
2. Difficulty swallowing (dysphagia)
3. Pain in the throat or ear
4. Changes in heart rate and blood pressure
5. Nausea, vomiting, or abdominal pain
6. Shortness of breath or difficulty breathing
The severity and nature of symptoms can vary depending on the location and extent of the injury to the vagus nerve. Treatment for vagus nerve injuries typically involves addressing the underlying cause, such as surgical intervention, physical therapy, or medication to manage pain and inflammation. In some cases, recovery may be incomplete, leading to long-term complications or disabilities.
A carotid body tumor is a rare, usually noncancerous (benign) growth that develops in the carotid body, a small structure located near the bifurcation (fork) of the common carotid artery in the neck. The carotid body is part of the chemoreceptor system that helps regulate breathing and blood pressure by responding to changes in oxygen, carbon dioxide, and pH levels in the blood.
Carotid body tumors are also known as carotid body paragangliomas or chemodectomas. They typically grow slowly and may not cause any symptoms for many years. However, as they enlarge, they can cause a visible or palpable mass in the neck, along with symptoms such as difficulty swallowing, hoarseness, or voice changes. In some cases, carotid body tumors can compress nearby nerves or blood vessels, leading to more serious complications like stroke or nerve damage.
Treatment for carotid body tumors typically involves surgical removal of the growth, which may be performed using traditional open surgery or minimally invasive techniques such as endovascular surgery or robotic-assisted surgery. Radiation therapy and chemotherapy are generally not effective in treating these tumors. Regular follow-up care is important to monitor for recurrence or development of new tumors.
The phrenic nerve is a motor nerve that originates from the cervical spine (C3-C5) and descends through the neck to reach the diaphragm, which is the primary muscle used for breathing. The main function of the phrenic nerve is to innervate the diaphragm and control its contraction and relaxation, thereby enabling respiration.
Damage or injury to the phrenic nerve can result in paralysis of the diaphragm, leading to difficulty breathing and potentially causing respiratory failure. Certain medical conditions, such as neuromuscular disorders, spinal cord injuries, and tumors, can affect the phrenic nerve and impair its function.
Duane Retraction Syndrome (DRS) is a congenital eye movement disorder, characterized by limited abduction (lateral movement away from the nose) of the affected eye, and on attempted adduction (movement towards the nose), the eye retracts into the orbit and the lid narrows. It is often accompanied by other eye alignment or vision anomalies. The exact cause is not known, but it is believed to be a result of abnormal development of the cranial nerves that control eye movement during fetal development. DRS is usually idiopathic, but it can also be associated with other congenital anomalies. It is typically diagnosed in early childhood and managed with a combination of observation, prism glasses, and/or surgery, depending on the severity and impact on vision.
The Radial nerve is a major peripheral nerve in the human body that originates from the brachial plexus, which is a network of nerves formed by the union of the ventral rami (anterior divisions) of spinal nerves C5-T1. The radial nerve provides motor function to extensor muscles of the upper limb and sensation to parts of the skin on the back of the arm, forearm, and hand.
More specifically, the radial nerve supplies motor innervation to:
* Extensor muscles of the shoulder (e.g., teres minor, infraspinatus)
* Rotator cuff muscles
* Elbow joint stabilizers (e.g., lateral head of the triceps)
* Extensors of the wrist, fingers, and thumb
The radial nerve also provides sensory innervation to:
* Posterior aspect of the upper arm (from the lower third of the humerus to the elbow)
* Lateral forearm (from the lateral epicondyle of the humerus to the wrist)
* Dorsum of the hand (skin over the radial side of the dorsum, including the first web space)
Damage or injury to the radial nerve may result in various symptoms, such as weakness or paralysis of the extensor muscles, numbness or tingling sensations in the affected areas, and difficulty with extension movements of the wrist, fingers, and thumb. Common causes of radial nerve injuries include fractures of the humerus bone, compression during sleep or prolonged pressure on the nerve (e.g., from crutches), and entrapment syndromes like radial tunnel syndrome.
The Recurrent Laryngeal Nerve (RLN) is a branch of the vagus nerve (cranial nerve X), which is a mixed sensory, motor, and autonomic nerve. The RLN has important functions in providing motor innervation to the intrinsic muscles of the larynx, except for the cricothyroid muscle, which is supplied by the external branch of the superior laryngeal nerve.
The recurrent laryngeal nerve supplies all the muscles that are responsible for adduction (bringing together) of the vocal cords, including the vocalis muscle, lateral cricoarytenoid, thyroarytenoid, and interarytenoid muscles. These muscles play a crucial role in voice production, coughing, and swallowing.
The right recurrent laryngeal nerve has a longer course than the left one. It loops around the subclavian artery in the chest before ascending to the larynx, while the left RLN hooks around the arch of the aorta. This anatomical course makes them vulnerable to injury during various surgical procedures, such as thyroidectomy and neck dissection, leading to potential voice impairment or vocal cord paralysis.
The brainstem is the lower part of the brain that connects to the spinal cord. It consists of the midbrain, pons, and medulla oblongata. The brainstem controls many vital functions such as heart rate, breathing, and blood pressure. It also serves as a relay center for sensory and motor information between the cerebral cortex and the rest of the body. Additionally, several cranial nerves originate from the brainstem, including those that control eye movements, facial movements, and hearing.
Spinal nerve roots are the initial parts of spinal nerves that emerge from the spinal cord through the intervertebral foramen, which are small openings between each vertebra in the spine. These nerve roots carry motor, sensory, and autonomic fibers to and from specific regions of the body. There are 31 pairs of spinal nerve roots in total, with 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal pair. Each root has a dorsal (posterior) and ventral (anterior) ramus that branch off to form the peripheral nervous system. Irritation or compression of these nerve roots can result in pain, numbness, weakness, or loss of reflexes in the affected area.
Meningeal carcinomatosis, also known as leptomeningeal metastasis or neoplastic meningitis, is a medical condition characterized by the spread of cancer cells to the meninges, which are the thin layers of tissue that cover and protect the brain and spinal cord.
In this condition, cancer cells from a primary tumor or metastatic cancer elsewhere in the body invade the cerebrospinal fluid (CSF) and spread throughout the meningeal spaces, causing inflammation and damage to the surrounding tissues. This can result in various neurological symptoms such as headache, nausea, vomiting, seizures, confusion, weakness, or paralysis, depending on the location of the cancer cells in the meninges.
Meningeal carcinomatosis is a serious and often life-threatening complication of advanced cancer, with a poor prognosis and limited treatment options. It can occur in various types of cancer, including lung, breast, melanoma, and hematological malignancies such as leukemia and lymphoma. Early diagnosis and prompt treatment are crucial to improve the quality of life and prolong survival in affected patients.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for controlling tongue movements. Hypoglossal nerve diseases refer to conditions that affect this nerve and result in various tongue-related symptoms. These disorders can be congenital or acquired, and they may stem from different causes such as trauma, tumors, infections, inflammation, or degenerative processes.
Hypoglossal nerve diseases can present with the following symptoms:
1. Weakness or paralysis of the tongue muscles on one or both sides.
2. Deviation of the tongue towards the affected side when protruded.
3. Fasciculations (involuntary muscle twitches) or atrophy (wasting) of the tongue muscles.
4. Difficulty with speaking, swallowing, and chewing due to tongue weakness.
5. Changes in taste and sensation on the back of the tongue and throat.
Some specific hypoglossal nerve diseases include:
1. Hypoglossal nerve palsy: A condition characterized by unilateral or bilateral weakness or paralysis of the tongue due to damage to the hypoglossal nerve. Causes can include trauma, tumors, stroke, multiple sclerosis, or other neurological disorders.
2. Hypoglossal neuritis: Inflammation of the hypoglossal nerve, often caused by viral infections or autoimmune processes, leading to tongue weakness and atrophy.
3. Congenital hypoglossal nerve anomalies: Abnormal development of the hypoglossal nerve during fetal growth can result in various tongue-related symptoms and difficulties with speech and swallowing.
4. Tumors affecting the hypoglossal nerve: Both benign and malignant tumors, such as schwannomas or neurofibromas, can compress or infiltrate the hypoglossal nerve, causing weakness or paralysis.
5. Hypoglossal-facial anastomosis: A surgical procedure that connects the hypoglossal nerve to the facial nerve to restore facial movement in cases of facial nerve palsy. This connection can lead to tongue weakness as a side effect.
Hyperostosis is a medical term that refers to an excessive growth or abnormal thickening of bone tissue. It can occur as a result of various conditions, such as inflammation, injury, or genetic disorders. The extra bone growth can cause pain, stiffness, and limited mobility in the affected area. In some cases, hyperostosis can also lead to deformities and other complications.
There are several types of hyperostosis, including:
1. Diffuse idiopathic skeletal hyperostosis (DISH): This is a condition that affects the spine, causing calcification and stiffening of the ligaments and bone spurs to form along the edges of the vertebrae. It is often asymptomatic but can cause pain and stiffness in some cases.
2. Flat bone hyperostosis: This type of hyperostosis affects the flat bones of the body, such as the skull, ribs, and pelvis. It can be caused by various conditions, including Paget's disease, fibrous dysplasia, and certain types of cancer.
3. Focal hyperostosis: This refers to localized areas of bone overgrowth that can occur in response to injury, infection, or inflammation. Examples include heterotopic ossification (the formation of bone in soft tissues) and Freiberg's infarction (a condition that affects the joint surface of the metatarsal bones in the foot).
4. Hyperostosis frontalis interna: This is a benign condition that causes thickening of the inner table of the frontal bone in the skull. It is more common in women and often asymptomatic but can cause headaches and other symptoms in some cases.
Treatment for hyperostosis depends on the underlying cause and severity of the condition. In some cases, no treatment may be necessary. However, if the condition causes pain or limits mobility, various treatments may be recommended, such as medication, physical therapy, or surgery.
The olfactory nerve, also known as the first cranial nerve (I), is a specialized sensory nerve that is responsible for the sense of smell. It consists of thin, delicate fibers called olfactory neurons that are located in the upper part of the nasal cavity. These neurons have hair-like structures called cilia that detect and transmit information about odors to the brain.
The olfactory nerve has two main parts: the peripheral process and the central process. The peripheral process extends from the olfactory neuron to the nasal cavity, where it picks up odor molecules. These molecules bind to receptors on the cilia, which triggers an electrical signal that travels along the nerve fiber to the brain.
The central process of the olfactory nerve extends from the olfactory bulb, a structure at the base of the brain, to several areas in the brain involved in smell and memory, including the amygdala, hippocampus, and thalamus. Damage to the olfactory nerve can result in a loss of smell (anosmia) or distorted smells (parosmia).
The ophthalmic nerve, also known as the first cranial nerve or CN I, is a sensory nerve that primarily transmits information about vision, including light intensity and color, and sensation in the eye and surrounding areas. It is responsible for the sensory innervation of the upper eyelid, conjunctiva, cornea, iris, ciliary body, and nasal cavity. The ophthalmic nerve has three major branches: the lacrimal nerve, frontal nerve, and nasociliary nerve. Damage to this nerve can result in various visual disturbances and loss of sensation in the affected areas.
Neural conduction is the process by which electrical signals, known as action potentials, are transmitted along the axon of a neuron (nerve cell) to transmit information between different parts of the nervous system. This electrical impulse is generated by the movement of ions across the neuronal membrane, and it propagates down the length of the axon until it reaches the synapse, where it can then stimulate the release of neurotransmitters to communicate with other neurons or target cells. The speed of neural conduction can vary depending on factors such as the diameter of the axon, the presence of myelin sheaths (which act as insulation and allow for faster conduction), and the temperature of the environment.
The temporal bone is a paired bone that is located on each side of the skull, forming part of the lateral and inferior walls of the cranial cavity. It is one of the most complex bones in the human body and has several important structures associated with it. The main functions of the temporal bone include protecting the middle and inner ear, providing attachment for various muscles of the head and neck, and forming part of the base of the skull.
The temporal bone is divided into several parts, including the squamous part, the petrous part, the tympanic part, and the styloid process. The squamous part forms the lateral portion of the temporal bone and articulates with the parietal bone. The petrous part is the most medial and superior portion of the temporal bone and contains the inner ear and the semicircular canals. The tympanic part forms the lower and anterior portions of the temporal bone and includes the external auditory meatus or ear canal. The styloid process is a long, slender projection that extends downward from the inferior aspect of the temporal bone and serves as an attachment site for various muscles and ligaments.
The temporal bone plays a crucial role in hearing and balance, as it contains the structures of the middle and inner ear, including the oval window, round window, cochlea, vestibule, and semicircular canals. The stapes bone, one of the three bones in the middle ear, is entirely encased within the petrous portion of the temporal bone. Additionally, the temporal bone contains important structures for facial expression and sensation, including the facial nerve, which exits the skull through the stylomastoid foramen, a small opening in the temporal bone.
Aseptic meningitis is a type of meningitis (inflammation of the membranes covering the brain and spinal cord) that is not caused by bacterial infection. Instead, it can be due to viral infections, fungal infections, or non-infectious causes such as certain medications, chemical irritants, or underlying medical conditions. In aseptic meningitis, the cerebrospinal fluid (CSF) analysis may show increased white blood cells, typically lymphocytes, but no bacterial growth on culture. Common viral causes include enteroviruses, herpes simplex virus, and varicella-zoster virus. Treatment depends on the underlying cause and may include supportive care, antiviral medications, or immunosuppressive therapy in some cases.
Nerve tissue, also known as neural tissue, is a type of specialized tissue that is responsible for the transmission of electrical signals and the processing of information in the body. It is a key component of the nervous system, which includes the brain, spinal cord, and peripheral nerves. Nerve tissue is composed of two main types of cells: neurons and glial cells.
Neurons are the primary functional units of nerve tissue. They are specialized cells that are capable of generating and transmitting electrical signals, known as action potentials. Neurons have a unique structure, with a cell body (also called the soma) that contains the nucleus and other organelles, and processes (dendrites and axons) that extend from the cell body and are used to receive and transmit signals.
Glial cells, also known as neuroglia or glia, are non-neuronal cells that provide support and protection for neurons. There are several different types of glial cells, including astrocytes, oligodendrocytes, microglia, and Schwann cells. These cells play a variety of roles in the nervous system, such as providing structural support, maintaining the proper environment for neurons, and helping to repair and regenerate nerve tissue after injury.
Nerve tissue is found throughout the body, but it is most highly concentrated in the brain and spinal cord, which make up the central nervous system (CNS). The peripheral nerves, which are the nerves that extend from the CNS to the rest of the body, also contain nerve tissue. Nerve tissue is responsible for transmitting sensory information from the body to the brain, controlling muscle movements, and regulating various bodily functions such as heart rate, digestion, and respiration.
The mandibular nerve is a branch of the trigeminal nerve (the fifth cranial nerve), which is responsible for sensations in the face and motor functions such as biting and chewing. The mandibular nerve provides both sensory and motor innervation to the lower third of the face, below the eye and nose down to the chin.
More specifically, it carries sensory information from the lower teeth, lower lip, and parts of the oral cavity, as well as the skin over the jaw and chin. It also provides motor innervation to the muscles of mastication (chewing), which include the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles.
Damage to the mandibular nerve can result in numbness or loss of sensation in the lower face and mouth, as well as weakness or difficulty with chewing and biting.
Recurrent laryngeal nerve injuries refer to damages or trauma inflicted on the recurrent laryngeal nerve, which is a branch of the vagus nerve that supplies motor function to the intrinsic muscles of the larynx, except for the cricothyroid muscle. This nerve plays a crucial role in controlling vocal fold movement and swallowing.
Injuries to this nerve can result in voice changes, hoarseness, or even complete loss of voice, depending on the severity and location of the injury. Additionally, it may also lead to breathing difficulties, coughing, and choking while swallowing due to impaired laryngeal function.
Recurrent laryngeal nerve injuries can occur due to various reasons, such as surgical complications (particularly during thyroid or neck surgeries), tumors, infections, inflammation, or direct trauma to the neck region. In some cases, these injuries may be temporary and resolve on their own or through appropriate treatment; however, severe or prolonged injuries might require medical intervention, including possible surgical repair.
Hemifacial spasm is a neuromuscular disorder characterized by involuntary, irregular contractions or twitching of the muscles on one side of the face. These spasms typically begin around the eye and may progress to involve the muscles of the lower face, including those around the mouth.
The primary cause of hemifacial spasm is pressure on or irritation of the facial nerve (cranial nerve VII) as it exits the brainstem, often due to a blood vessel or tumor. This pressure can lead to abnormal electrical signals in the facial nerve, resulting in uncontrolled muscle contractions.
In some cases, hemifacial spasm may be associated with other conditions such as multiple sclerosis or Bell's palsy. Treatment options for hemifacial spasm include medications to help relax the muscles, botulinum toxin (Botox) injections to paralyze the affected muscles temporarily, and, in rare cases, surgical intervention to relieve pressure on the facial nerve.
I'm sorry for any confusion, but "Racquet Sports" is not a term that has a specific medical definition. It generally refers to sports that involve using a racquet to hit a ball or other object back and forth, such as tennis, badminton, squash, and racquetball. However, in a medical context, these sports might be discussed in terms of the types of injuries or health benefits associated with playing them (for example, overuse injuries in the elbow from repetitive motions). If you have any specific questions about the medical aspects of participating in racquet sports, I'd be happy to try to help answer them!
Skull neoplasms refer to abnormal growths or tumors that develop within the skull. These growths can be benign (non-cancerous) or malignant (cancerous). They can originate from various types of cells, such as bone cells, nerve cells, or soft tissues. Skull neoplasms can cause various symptoms depending on their size and location, including headaches, seizures, vision problems, hearing loss, and neurological deficits. Treatment options include surgery, radiation therapy, and chemotherapy. It is important to note that a neoplasm in the skull can also refer to metastatic cancer, which has spread from another part of the body to the skull.
An axon is a long, slender extension of a neuron (a type of nerve cell) that conducts electrical impulses (nerve impulses) away from the cell body to target cells, such as other neurons or muscle cells. Axons can vary in length from a few micrometers to over a meter long and are typically surrounded by a myelin sheath, which helps to insulate and protect the axon and allows for faster transmission of nerve impulses.
Axons play a critical role in the functioning of the nervous system, as they provide the means by which neurons communicate with one another and with other cells in the body. Damage to axons can result in serious neurological problems, such as those seen in spinal cord injuries or neurodegenerative diseases like multiple sclerosis.
The oculomotor muscles are a group of extraocular muscles that control the movements of the eye. They include:
1. Superior rectus: This muscle is responsible for elevating the eye and helping with inward rotation (intorsion) when looking downwards.
2. Inferior rectus: It depresses the eye and helps with outward rotation (extorsion) when looking upwards.
3. Medial rectus: This muscle adducts, or moves, the eye towards the midline of the face.
4. Inferior oblique: The inferior oblique muscle intorts and elevates the eye.
5. Superior oblique: It extorts and depresses the eye.
These muscles work together to allow for smooth and precise movements of the eyes, enabling tasks such as tracking moving objects, reading, and maintaining visual fixation on a single point in space.
The abducens nerve, also known as the sixth cranial nerve, is responsible for controlling the lateral rectus muscle of the eye, which allows for horizontal movement of the eye outwards. An injury to the abducens nerve can result in various symptoms related to eye movement and alignment.
Medical definition:
Abducens nerve injury refers to damage or trauma to the sixth cranial nerve, resulting in dysfunction of the lateral rectus muscle and subsequent impairment of horizontal gaze. The affected individual may experience difficulty in moving the eye outwards, double vision (diplopia), or a condition known as strabismus, where the eyes are misaligned and point in different directions. Abducens nerve injury can occur due to various reasons, such as head trauma, tumors, increased intracranial pressure, or neurological disorders like multiple sclerosis. Treatment typically involves addressing the underlying cause and may include surgical intervention, eye patching, or prism lenses to manage symptoms and improve visual function.
A meningioma is a type of slow-growing tumor that forms on the membranes (meninges) surrounding the brain and spinal cord. It's usually benign, meaning it doesn't spread to other parts of the body, but it can still cause serious problems if it grows and presses on nearby tissues.
Meningiomas most commonly occur in adults, and are more common in women than men. They can cause various symptoms depending on their location and size, including headaches, seizures, vision or hearing problems, memory loss, and changes in personality or behavior. In some cases, they may not cause any symptoms at all and are discovered only during imaging tests for other conditions.
Treatment options for meningiomas include monitoring with regular imaging scans, surgery to remove the tumor, and radiation therapy to shrink or kill the tumor cells. The best treatment approach depends on factors such as the size and location of the tumor, the patient's age and overall health, and their personal preferences.
The foramen magnum is the largest opening in the human skull, located at the base of the skull, through which the spinal cord connects to the brain. It is a crucial structure for the transmission of nerve impulses between the brain and the rest of the body. The foramen magnum also provides passage for blood vessels that supply the brainstem and upper spinal cord.
The occipital bone is the single, posterior cranial bone that forms the base of the skull and encloses the brain. It articulates with the parietal bones anteriorly and the temporal bones laterally. The occipital bone also contains several important structures such as the foramen magnum, through which the spinal cord connects to the brain, and the external and internal occipital protuberances, which serve as attachment points for neck muscles.
The sphenoid sinuses are air-filled spaces located within the sphenoid bone, which is one of the bones that make up the skull base. These sinuses are located deep inside the skull, behind the eyes and nasal cavity. They are paired and separated by a thin bony septum, and each one opens into the corresponding nasal cavity through a small opening called the sphenoethmoidal recess. The sphenoid sinuses vary greatly in size and shape between individuals. They develop during childhood and continue to grow until early adulthood. The function of the sphenoid sinuses, like other paranasal sinuses, is not entirely clear, but they may contribute to reducing the weight of the skull, resonating voice during speech, and insulating the brain from trauma.
The rhombencephalon is a term used in the field of neuroanatomy, which refers to the most posterior region of the developing brain during embryonic development. It is also known as the hindbrain and it gives rise to several important structures in the adult brain.
More specifically, the rhombencephalon can be further divided into two main parts: the metencephalon and the myelencephalon. The metencephalon eventually develops into the pons and cerebellum, while the myelencephalon becomes the medulla oblongata.
The rhombencephalon plays a crucial role in several critical functions of the nervous system, including regulating heart rate and respiration, maintaining balance and posture, and coordinating motor movements. Defects or abnormalities in the development of the rhombencephalon can lead to various neurological disorders, such as cerebellar hypoplasia, Chiari malformation, and certain forms of brainstem tumors.
A spasm is a sudden, involuntary contraction or tightening of a muscle, group of muscles, or a hollow organ such as the ureter or bronchi. Spasms can occur as a result of various factors including muscle fatigue, injury, irritation, or abnormal nerve activity. They can cause pain and discomfort, and in some cases, interfere with normal bodily functions. For example, a spasm in the bronchi can cause difficulty breathing, while a spasm in the ureter can cause severe pain and may lead to a kidney stone blockage. The treatment for spasms depends on the underlying cause and may include medication, physical therapy, or lifestyle changes.
The splanchnic nerves are a set of nerve fibers that originate from the thoracic and lumbar regions of the spinal cord and innervate various internal organs. They are responsible for carrying both sensory information, such as pain and temperature, from the organs to the brain, and motor signals, which control the function of the organs, from the brain to the organs.
There are several splanchnic nerves, including the greater, lesser, and least splanchnic nerves, as well as the lumbar splanchnic nerves. These nerves primarily innervate the autonomic nervous system, which controls the involuntary functions of the body, such as heart rate, digestion, and respiration.
The greater splanchnic nerve arises from the fifth to the ninth thoracic ganglia and passes through the diaphragm to reach the abdomen. It innervates the stomach, esophagus, liver, pancreas, and adrenal glands.
The lesser splanchnic nerve arises from the tenth and eleventh thoracic ganglia and innervates the upper part of the small intestine, the pancreas, and the adrenal glands.
The least splanchnic nerve arises from the twelfth thoracic ganglion and innervates the lower part of the small intestine and the colon.
The lumbar splanchnic nerves arise from the first three or four lumbar ganglia and innervate the lower parts of the colon, the rectum, and the reproductive organs.
In medical terms, the tongue is a muscular organ in the oral cavity that plays a crucial role in various functions such as taste, swallowing, and speech. It's covered with a mucous membrane and contains papillae, which are tiny projections that contain taste buds to help us perceive different tastes - sweet, salty, sour, and bitter. The tongue also assists in the initial process of digestion by moving food around in the mouth for chewing and mixing with saliva. Additionally, it helps in forming words and speaking clearly by shaping the sounds produced in the mouth.
Vertigo is a specific type of dizziness characterized by the sensation that you or your surroundings are spinning or moving, even when you're perfectly still. It's often caused by issues with the inner ear or the balance-sensing systems of the body. Vertigo can be brought on by various conditions, such as benign paroxysmal positional vertigo (BPPV), labyrinthitis, vestibular neuritis, Meniere's disease, and migraines. In some cases, vertigo may also result from head or neck injuries, brain disorders like stroke or tumors, or certain medications. Treatment for vertigo depends on the underlying cause and can include specific exercises, medication, or surgery in severe cases.
Meningeal neoplasms, also known as malignant meningitis or leptomeningeal carcinomatosis, refer to cancerous tumors that originate in the meninges, which are the membranes covering the brain and spinal cord. These tumors can arise primarily from the meningeal cells themselves, although they more commonly result from the spread (metastasis) of cancer cells from other parts of the body, such as breast, lung, or melanoma.
Meningeal neoplasms can cause a variety of symptoms, including headaches, nausea and vomiting, mental status changes, seizures, and focal neurological deficits. Diagnosis typically involves imaging studies (such as MRI) and analysis of cerebrospinal fluid obtained through a spinal tap. Treatment options may include radiation therapy, chemotherapy, or surgery, depending on the type and extent of the tumor. The prognosis for patients with meningeal neoplasms is generally poor, with a median survival time of several months to a year.
A neurological examination is a series of tests used to evaluate the functioning of the nervous system, including both the central nervous system (the brain and spinal cord) and peripheral nervous system (the nerves that extend from the brain and spinal cord to the rest of the body). It is typically performed by a healthcare professional such as a neurologist or a primary care physician with specialized training in neurology.
During a neurological examination, the healthcare provider will assess various aspects of neurological function, including:
1. Mental status: This involves evaluating a person's level of consciousness, orientation, memory, and cognitive abilities.
2. Cranial nerves: There are 12 cranial nerves that control functions such as vision, hearing, smell, taste, and movement of the face and neck. The healthcare provider will test each of these nerves to ensure they are functioning properly.
3. Motor function: This involves assessing muscle strength, tone, coordination, and reflexes. The healthcare provider may ask the person to perform certain movements or tasks to evaluate these functions.
4. Sensory function: The healthcare provider will test a person's ability to feel different types of sensations, such as touch, pain, temperature, vibration, and proprioception (the sense of where your body is in space).
5. Coordination and balance: The healthcare provider may assess a person's ability to perform coordinated movements, such as touching their finger to their nose or walking heel-to-toe.
6. Reflexes: The healthcare provider will test various reflexes throughout the body using a reflex hammer.
The results of a neurological examination can help healthcare providers diagnose and monitor conditions that affect the nervous system, such as stroke, multiple sclerosis, Parkinson's disease, or peripheral neuropathy.
Microsurgery is a surgical technique that requires the use of an operating microscope and fine instruments to perform precise surgical manipulations. It is commonly used in various fields such as ophthalmology, neurosurgery, orthopedic surgery, and plastic and reconstructive surgery. The magnification provided by the microscope allows surgeons to work on small structures like nerves, blood vessels, and tiny bones. Some of the most common procedures that fall under microsurgery include nerve repair, replantation of amputated parts, and various types of reconstructions such as free tissue transfer for cancer reconstruction or coverage of large wounds.
Optic nerve injuries refer to damages or trauma inflicted on the optic nerve, which is a crucial component of the visual system. The optic nerve transmits visual information from the retina to the brain, enabling us to see. Injuries to the optic nerve can result in various visual impairments, including partial or complete vision loss, decreased visual acuity, changes in color perception, and reduced field of view.
These injuries may occur due to several reasons, such as:
1. Direct trauma to the eye or head
2. Increased pressure inside the eye (glaucoma)
3. Optic neuritis, an inflammation of the optic nerve
4. Ischemia, or insufficient blood supply to the optic nerve
5. Compression from tumors or other space-occupying lesions
6. Intrinsic degenerative conditions affecting the optic nerve
7. Toxic exposure to certain chemicals or medications
Optic nerve injuries are diagnosed through a comprehensive eye examination, including visual acuity testing, slit-lamp examination, dilated fundus exam, and additional diagnostic tests like optical coherence tomography (OCT) and visual field testing. Treatment options vary depending on the cause and severity of the injury but may include medications, surgery, or vision rehabilitation.
Polyradiculoneuropathy is a medical term that refers to a condition affecting multiple nerve roots and peripheral nerves. It's a type of neuropathy, which is damage or disease affecting the peripheral nerves, and it involves damage to the nerve roots as they exit the spinal cord.
The term "poly" means many, "radiculo" refers to the nerve root, and "neuropathy" indicates a disorder of the nerves. Therefore, polyradiculoneuropathy implies that multiple nerve roots and peripheral nerves are affected.
This condition can result from various causes, such as infections (like Guillain-Barre syndrome), autoimmune disorders (such as lupus or rheumatoid arthritis), diabetes, cancer, or exposure to toxins. Symptoms may include weakness, numbness, tingling, or pain in the limbs, which can progress and become severe over time. Proper diagnosis and management are crucial for improving outcomes and preventing further nerve damage.
Horner syndrome, also known as Horner's syndrome or oculosympathetic palsy, is a neurological disorder characterized by the interruption of sympathetic nerve pathways that innervate the head and neck, leading to a constellation of signs affecting the eye and face on one side of the body.
The classic triad of symptoms includes:
1. Ptosis (drooping) of the upper eyelid: This is due to the weakness or paralysis of the levator palpebrae superioris muscle, which is responsible for elevating the eyelid.
2. Miosis (pupillary constriction): The affected pupil becomes smaller in size compared to the other side, and it may not react as robustly to light.
3. Anhydrosis (decreased sweating): There is reduced or absent sweating on the ipsilateral (same side) of the face, particularly around the forehead and upper eyelid.
Horner syndrome can be caused by various underlying conditions, such as brainstem stroke, tumors, trauma, or certain medical disorders affecting the sympathetic nervous system. The diagnosis typically involves a thorough clinical examination, pharmacological testing, and sometimes imaging studies to identify the underlying cause. Treatment is directed towards managing the underlying condition responsible for Horner syndrome.
Optic nerve diseases refer to a group of conditions that affect the optic nerve, which transmits visual information from the eye to the brain. These diseases can cause various symptoms such as vision loss, decreased visual acuity, changes in color vision, and visual field defects. Examples of optic nerve diseases include optic neuritis (inflammation of the optic nerve), glaucoma (damage to the optic nerve due to high eye pressure), optic nerve damage from trauma or injury, ischemic optic neuropathy (lack of blood flow to the optic nerve), and optic nerve tumors. Treatment for optic nerve diseases varies depending on the specific condition and may include medications, surgery, or lifestyle changes.
A craniotomy is a surgical procedure where a bone flap is temporarily removed from the skull to access the brain. This procedure is typically performed to treat various neurological conditions, such as brain tumors, aneurysms, arteriovenous malformations, or traumatic brain injuries. After the underlying brain condition is addressed, the bone flap is usually replaced and secured back in place with plates and screws. The purpose of a craniotomy is to provide access to the brain for diagnostic or therapeutic interventions while minimizing potential damage to surrounding tissues.
The internal carotid artery is a major blood vessel that supplies oxygenated blood to the brain. It originates from the common carotid artery and passes through the neck, entering the skull via the carotid canal in the temporal bone. Once inside the skull, it branches into several smaller vessels that supply different parts of the brain with blood.
The internal carotid artery is divided into several segments: cervical, petrous, cavernous, clinoid, and supraclinoid. Each segment has distinct clinical significance in terms of potential injury or disease. The most common conditions affecting the internal carotid artery include atherosclerosis, which can lead to stroke or transient ischemic attack (TIA), and dissection, which can cause severe headache, neck pain, and neurological symptoms.
It's important to note that any blockage or damage to the internal carotid artery can have serious consequences, as it can significantly reduce blood flow to the brain and lead to permanent neurological damage or even death. Therefore, regular check-ups and screening tests are recommended for individuals at high risk of developing vascular diseases.
The meninges are the protective membranes that cover the brain and spinal cord. They consist of three layers: the dura mater (the outermost, toughest layer), the arachnoid mater (middle layer), and the pia mater (the innermost, delicate layer). These membranes provide protection and support to the central nervous system, and contain blood vessels that supply nutrients and remove waste products. Inflammation or infection of the meninges is called meningitis, which can be a serious medical condition requiring prompt treatment.
Herpes zoster oticus, also known as Ramsay Hunt syndrome type 2, is a viral infection that affects the facial nerve (cranial nerve VII). It is caused by the reactivation of the varicella-zoster virus, which is the same virus responsible for chickenpox. After an initial chickenpox infection, the virus can remain dormant in the body and later reactivate, causing herpes zoster oticus.
In this condition, the virus affects the geniculate ganglion of the facial nerve, leading to inflammation and damage to the nerve fibers. This results in various symptoms, including:
1. Painful rash around the ear, on the face, or in the mouth
2. Facial weakness or paralysis on one side of the face
3. Hearing loss, tinnitus (ringing in the ears), or vertigo (dizziness)
4. Loss of taste sensation on the anterior two-thirds of the tongue
5. Difficulty closing one eye, leading to dryness and irritation
Immediate medical attention is necessary for proper diagnosis and treatment, which typically involves antiviral medications and corticosteroids to reduce inflammation and speed up recovery. Early treatment can help minimize the risk of complications, such as permanent facial nerve damage or hearing loss.
Thoracic nerves are the 12 paired nerves that originate from the thoracic segment (T1-T12) of the spinal cord. These nerves provide motor and sensory innervation to the trunk and abdomen, specifically to the muscles of the chest wall, the skin over the back and chest, and some parts of the abdomen. They also contribute to the formation of the sympathetic trunk, which is a part of the autonomic nervous system that regulates unconscious bodily functions such as heart rate and digestion. Each thoracic nerve emerges from the intervertebral foramen, a small opening between each vertebra, and splits into anterior and posterior branches to innervate the corresponding dermatomes and myotomes.
Myelinated nerve fibers are neuronal processes that are surrounded by a myelin sheath, a fatty insulating substance that is produced by Schwann cells in the peripheral nervous system and oligodendrocytes in the central nervous system. This myelin sheath helps to increase the speed of electrical impulse transmission, also known as action potentials, along the nerve fiber. The myelin sheath has gaps called nodes of Ranvier where the electrical impulses can jump from one node to the next, which also contributes to the rapid conduction of signals. Myelinated nerve fibers are typically found in the peripheral nerves and the optic nerve, but not in the central nervous system (CNS) tracts that are located within the brain and spinal cord.
Neurofibromatosis 2 (NF2) is a genetic disorder characterized by the development of non-cancerous tumors in the nervous system, particularly on the nerves related to hearing and balance. It's also known as central neurofibromatosis or bilateral acoustic neuroma syndrome.
The primary feature of NF2 is the growth of schwannomas, which are tumors that develop from the cells surrounding nerve fibers. These typically grow on the vestibular nerve, leading to hearing loss, ringing in the ears (tinnitus), and balance problems. Bilateral acoustic neuromas (schwannomas affecting both vestibular nerves) are a hallmark of this condition.
Other common features include:
1. Meningiomas: These are tumors that grow in the meninges, the protective layers surrounding the brain and spinal cord.
2. Ependymomas: These are tumors that develop from the ependymal cells lining the ventricles (fluid-filled spaces) in the brain or the spinal cord canal.
3. Neurofibromas: Unlike in Neurofibromatosis type 1, these are less common and typically don't become cancerous.
4. Skin changes: While not as prevalent as in NF1, some people with NF2 may have skin freckles, café-au-lait spots, or skin tumors.
5. Eye problems: Some individuals may experience cataracts, retinal abnormalities, or optic nerve tumors (optic gliomas).
6. Other potential symptoms: Headaches, facial weakness or numbness, and difficulty swallowing or speaking.
NF2 is an autosomal dominant disorder, meaning that a person has a 50% chance of inheriting the condition if one of their parents has it. However, about half of all NF2 cases result from spontaneous genetic mutations with no family history of the disorder.
Motor neurons are specialized nerve cells in the brain and spinal cord that play a crucial role in controlling voluntary muscle movements. They transmit electrical signals from the brain to the muscles, enabling us to perform actions such as walking, talking, and swallowing. There are two types of motor neurons: upper motor neurons, which originate in the brain's motor cortex and travel down to the brainstem and spinal cord; and lower motor neurons, which extend from the brainstem and spinal cord to the muscles. Damage or degeneration of these motor neurons can lead to various neurological disorders, such as amyotrophic lateral sclerosis (ALS) and spinal muscular atrophy (SMA).
Neurosurgical procedures are operations that are performed on the brain, spinal cord, and peripheral nerves. These procedures are typically carried out by neurosurgeons, who are medical doctors with specialized training in the diagnosis and treatment of disorders of the nervous system. Neurosurgical procedures can be used to treat a wide range of conditions, including traumatic injuries, tumors, aneurysms, vascular malformations, infections, degenerative diseases, and congenital abnormalities.
Some common types of neurosurgical procedures include:
* Craniotomy: A procedure in which a bone flap is temporarily removed from the skull to gain access to the brain. This type of procedure may be performed to remove a tumor, repair a blood vessel, or relieve pressure on the brain.
* Spinal fusion: A procedure in which two or more vertebrae in the spine are fused together using bone grafts and metal hardware. This is often done to stabilize the spine and alleviate pain caused by degenerative conditions or spinal deformities.
* Microvascular decompression: A procedure in which a blood vessel that is causing pressure on a nerve is repositioned or removed. This type of procedure is often used to treat trigeminal neuralgia, a condition that causes severe facial pain.
* Deep brain stimulation: A procedure in which electrodes are implanted in specific areas of the brain and connected to a battery-operated device called a neurostimulator. The neurostimulator sends electrical impulses to the brain to help alleviate symptoms of movement disorders such as Parkinson's disease or dystonia.
* Stereotactic radiosurgery: A non-invasive procedure that uses focused beams of radiation to treat tumors, vascular malformations, and other abnormalities in the brain or spine. This type of procedure is often used for patients who are not good candidates for traditional surgery due to age, health status, or location of the lesion.
Neurosurgical procedures can be complex and require a high degree of skill and expertise. Patients considering neurosurgical treatment should consult with a qualified neurosurgeon to discuss their options and determine the best course of action for their individual situation.
Brain stem neoplasms refer to tumors that originate in the brainstem, which is the lower part of the brain that connects to the spinal cord. These tumors can be benign or malignant and can arise from various types of cells within the brainstem, such as nerve cells, glial cells (which support and protect nerve cells), or cells that make up blood vessels.
Brain stem neoplasms are relatively rare, accounting for about 2% of all primary brain tumors. They can cause a variety of symptoms depending on their size and location, including headache, vomiting, double vision, difficulty swallowing, facial weakness, and problems with balance and coordination. Treatment options may include surgery, radiation therapy, and chemotherapy, depending on the type, location, and extent of the tumor.
The laryngeal nerves are a pair of nerves that originate from the vagus nerve (cranial nerve X) and provide motor and sensory innervation to the larynx. There are two branches of the laryngeal nerves: the superior laryngeal nerve and the recurrent laryngeal nerve.
The superior laryngeal nerve has two branches: the external branch, which provides motor innervation to the cricothyroid muscle and sensation to the mucous membrane of the laryngeal vestibule; and the internal branch, which provides sensory innervation to the mucous membrane of the laryngeal vestibule.
The recurrent laryngeal nerve provides motor innervation to all the intrinsic muscles of the larynx, except for the cricothyroid muscle, and sensation to the mucous membrane below the vocal folds. The right recurrent laryngeal nerve has a longer course than the left one, as it hooks around the subclavian artery before ascending to the larynx.
Damage to the laryngeal nerves can result in voice changes, difficulty swallowing, and respiratory distress.
Carotid endarterectomy is a surgical procedure to remove plaque buildup (atherosclerosis) from the carotid arteries, which are the major blood vessels that supply oxygen-rich blood to the brain. The surgery involves making an incision in the neck, opening the carotid artery, and removing the plaque from the inside of the artery wall. The goal of the procedure is to restore normal blood flow to the brain and reduce the risk of stroke caused by the narrowing or blockage of the carotid arteries.
Nerve tissue proteins are specialized proteins found in the nervous system that provide structural and functional support to nerve cells, also known as neurons. These proteins include:
1. Neurofilaments: These are type IV intermediate filaments that provide structural support to neurons and help maintain their shape and size. They are composed of three subunits - NFL (light), NFM (medium), and NFH (heavy).
2. Neuronal Cytoskeletal Proteins: These include tubulins, actins, and spectrins that provide structural support to the neuronal cytoskeleton and help maintain its integrity.
3. Neurotransmitter Receptors: These are specialized proteins located on the postsynaptic membrane of neurons that bind neurotransmitters released by presynaptic neurons, triggering a response in the target cell.
4. Ion Channels: These are transmembrane proteins that regulate the flow of ions across the neuronal membrane and play a crucial role in generating and transmitting electrical signals in neurons.
5. Signaling Proteins: These include enzymes, receptors, and adaptor proteins that mediate intracellular signaling pathways involved in neuronal development, differentiation, survival, and death.
6. Adhesion Proteins: These are cell surface proteins that mediate cell-cell and cell-matrix interactions, playing a crucial role in the formation and maintenance of neural circuits.
7. Extracellular Matrix Proteins: These include proteoglycans, laminins, and collagens that provide structural support to nerve tissue and regulate neuronal migration, differentiation, and survival.
Infratentorial neoplasms refer to tumors that originate in the region of the brain called the posterior fossa, which is located below the tentorium cerebelli (a membranous structure that separates the cerebrum from the cerebellum). This area contains several important structures such as the cerebellum, pons, medulla oblongata, and fourth ventricle. Infratentorial neoplasms can be benign or malignant and can arise from various cell types including nerve cells, glial cells, or supportive tissues. They can cause a variety of symptoms depending on their location and size, such as headache, vomiting, unsteady gait, weakness, numbness, vision changes, hearing loss, and difficulty swallowing or speaking. Treatment options may include surgery, radiation therapy, and chemotherapy.
The sympathetic nervous system (SNS) is a part of the autonomic nervous system that operates largely below the level of consciousness, and it functions to produce appropriate physiological responses to perceived danger. It's often associated with the "fight or flight" response. The SNS uses nerve impulses to stimulate target organs, causing them to speed up (e.g., increased heart rate), prepare for action, or otherwise respond to stressful situations.
The sympathetic nervous system is activated due to stressful emotional or physical situations and it prepares the body for immediate actions. It dilates the pupils, increases heart rate and blood pressure, accelerates breathing, and slows down digestion. The primary neurotransmitter involved in this system is norepinephrine (also known as noradrenaline).
The subarachnoid space is the area between the arachnoid mater and pia mater, which are two of the three membranes covering the brain and spinal cord (the third one being the dura mater). This space is filled with cerebrospinal fluid (CSF), which provides protection and cushioning to the central nervous system. The subarachnoid space also contains blood vessels that supply the brain and spinal cord with oxygen and nutrients. It's important to note that subarachnoid hemorrhage, a type of stroke, can occur when there is bleeding into this space.
Papilledema is a medical term that refers to swelling of the optic nerve head, also known as the disc, which is the point where the optic nerve enters the back of the eye (the retina). This swelling can be caused by increased pressure within the skull, such as from brain tumors, meningitis, or idiopathic intracranial hypertension. Papilledema is usually detected through a routine eye examination and may be accompanied by symptoms such as headaches, visual disturbances, and nausea. If left untreated, papilledema can lead to permanent vision loss.
Afferent neurons, also known as sensory neurons, are a type of nerve cell that conducts impulses or signals from peripheral receptors towards the central nervous system (CNS), which includes the brain and spinal cord. These neurons are responsible for transmitting sensory information such as touch, temperature, pain, sound, and light to the CNS for processing and interpretation. Afferent neurons have specialized receptor endings that detect changes in the environment and convert them into electrical signals, which are then transmitted to the CNS via synapses with other neurons. Once the signals reach the CNS, they are processed and integrated with other information to produce a response or reaction to the stimulus.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Guillain-Barré syndrome (GBS) is a rare autoimmune disorder in which the body's immune system mistakenly attacks the peripheral nervous system, leading to muscle weakness, tingling sensations, and sometimes paralysis. The peripheral nervous system includes the nerves that control our movements and transmit signals from our skin, muscles, and joints to our brain.
The onset of GBS usually occurs after a viral or bacterial infection, such as respiratory or gastrointestinal infections, or following surgery, vaccinations, or other immune system triggers. The exact cause of the immune response that leads to GBS is not fully understood.
GBS typically progresses rapidly over days or weeks, with symptoms reaching their peak within 2-4 weeks after onset. Most people with GBS experience muscle weakness that starts in the lower limbs and spreads upward to the upper body, arms, and face. In severe cases, the diaphragm and chest muscles may become weakened, leading to difficulty breathing and requiring mechanical ventilation.
The diagnosis of GBS is based on clinical symptoms, nerve conduction studies, and sometimes cerebrospinal fluid analysis. Treatment typically involves supportive care, such as pain management, physical therapy, and respiratory support if necessary. In addition, plasma exchange (plasmapheresis) or intravenous immunoglobulin (IVIG) may be used to reduce the severity of symptoms and speed up recovery.
While most people with GBS recover completely or with minimal residual symptoms, some may experience long-term disability or require ongoing medical care. The prognosis for GBS varies depending on the severity of the illness and the individual's age and overall health.
The sphenoid bone is a complex, irregularly shaped bone located in the middle cranial fossa and forms part of the base of the skull. It articulates with several other bones, including the frontal, parietal, temporal, ethmoid, palatine, and zygomatic bones. The sphenoid bone has two main parts: the body and the wings.
The body of the sphenoid bone is roughly cuboid in shape and contains several important structures, such as the sella turcica, which houses the pituitary gland, and the sphenoid sinuses, which are air-filled cavities within the bone. The greater wings of the sphenoid bone extend laterally from the body and form part of the skull's lateral walls. They contain the superior orbital fissure, through which important nerves and blood vessels pass between the cranial cavity and the orbit of the eye.
The lesser wings of the sphenoid bone are thin, blade-like structures that extend anteriorly from the body and form part of the floor of the anterior cranial fossa. They contain the optic canal, which transmits the optic nerve and ophthalmic artery between the brain and the orbit of the eye.
Overall, the sphenoid bone plays a crucial role in protecting several important structures within the skull, including the pituitary gland, optic nerves, and ophthalmic arteries.
Diabetic neuropathies refer to a group of nerve disorders that are caused by diabetes. High blood sugar levels can injure nerves throughout the body, but diabetic neuropathies most commonly affect the nerves in the legs and feet.
There are four main types of diabetic neuropathies:
1. Peripheral neuropathy: This is the most common type of diabetic neuropathy. It affects the nerves in the legs and feet, causing symptoms such as numbness, tingling, burning, or shooting pain.
2. Autonomic neuropathy: This type of neuropathy affects the autonomic nerves, which control involuntary functions such as heart rate, blood pressure, digestion, and bladder function. Symptoms may include dizziness, fainting, digestive problems, sexual dysfunction, and difficulty regulating body temperature.
3. Proximal neuropathy: Also known as diabetic amyotrophy, this type of neuropathy affects the nerves in the hips, thighs, or buttocks, causing weakness, pain, and difficulty walking.
4. Focal neuropathy: This type of neuropathy affects a single nerve or group of nerves, causing symptoms such as weakness, numbness, or pain in the affected area. Focal neuropathies can occur anywhere in the body, but they are most common in the head, torso, and legs.
The risk of developing diabetic neuropathies increases with the duration of diabetes and poor blood sugar control. Other factors that may contribute to the development of diabetic neuropathies include genetics, age, smoking, and alcohol consumption.
Dura Mater is the thickest and outermost of the three membranes (meninges) that cover the brain and spinal cord. It provides protection and support to these delicate structures. The other two layers are called the Arachnoid Mater and the Pia Mater, which are thinner and more delicate than the Dura Mater. Together, these three layers form a protective barrier around the central nervous system.
Electric stimulation, also known as electrical nerve stimulation or neuromuscular electrical stimulation, is a therapeutic treatment that uses low-voltage electrical currents to stimulate nerves and muscles. It is often used to help manage pain, promote healing, and improve muscle strength and mobility. The electrical impulses can be delivered through electrodes placed on the skin or directly implanted into the body.
In a medical context, electric stimulation may be used for various purposes such as:
1. Pain management: Electric stimulation can help to block pain signals from reaching the brain and promote the release of endorphins, which are natural painkillers produced by the body.
2. Muscle rehabilitation: Electric stimulation can help to strengthen muscles that have become weak due to injury, illness, or surgery. It can also help to prevent muscle atrophy and improve range of motion.
3. Wound healing: Electric stimulation can promote tissue growth and help to speed up the healing process in wounds, ulcers, and other types of injuries.
4. Urinary incontinence: Electric stimulation can be used to strengthen the muscles that control urination and reduce symptoms of urinary incontinence.
5. Migraine prevention: Electric stimulation can be used as a preventive treatment for migraines by applying electrical impulses to specific nerves in the head and neck.
It is important to note that electric stimulation should only be administered under the guidance of a qualified healthcare professional, as improper use can cause harm or discomfort.
The branchial region, also known as the pharyngeal region or viscerocranium, is a term used in human anatomy to refer to the area of the developing embryo that gives rise to structures derived from the branchial (or pharyngeal) arches. The branchial arches are a series of paired, rod-like structures that appear early in embryonic development and give rise to various head and neck structures, including the bones and muscles of the face, jaws, and neck, as well as the associated nerves, blood vessels, and connective tissues.
The branchial region is divided into several subregions, each corresponding to a specific branchial arch. The first branchial arch gives rise to structures such as the mandible (lower jaw), maxilla (upper jaw), and muscles of mastication (chewing). The second branchial arch forms the stapes and styloid process in the ear, as well as some neck muscles. The third and fourth branchial arches contribute to the formation of the larynx, thyroid cartilage, and other structures in the neck.
Abnormalities in the development of the branchial region can lead to a variety of congenital defects, such as cleft palate, micrognathia (small jaw), and branchial cysts or sinuses. These conditions may require surgical intervention to correct.
The lingual nerve is a branch of the mandibular division of the trigeminal nerve (cranial nerve V). It provides general sensory innervation to the anterior two-thirds of the tongue, including taste sensation from the same region. It also supplies sensory innervation to the floor of the mouth and the lingual gingiva (gum tissue). The lingual nerve is closely associated with the submandibular and sublingual salivary glands and their ducts.
The mastoid is a term used in anatomy and refers to the bony prominence located at the base of the skull, posterior to the ear. More specifically, it's part of the temporal bone, one of the bones that forms the side and base of the skull. The mastoid process provides attachment for various muscles involved in chewing and moving the head.
In a medical context, "mastoid" can also refer to conditions or procedures related to this area. For example, mastoiditis is an infection of the mastoid process, while a mastoidectomy is a surgical procedure that involves removing part or all of the mastoid process.
The pons is a part of the brainstem that lies between the medulla oblongata and the midbrain. Its name comes from the Latin word "ponte" which means "bridge," as it serves to connect these two regions of the brainstem. The pons contains several important structures, including nerve fibers that carry signals between the cerebellum (the part of the brain responsible for coordinating muscle movements) and the rest of the nervous system. It also contains nuclei (clusters of neurons) that help regulate various functions such as respiration, sleep, and facial movements.
Neurologic manifestations refer to the signs and symptoms that occur due to a disturbance or disease of the nervous system, which includes the brain, spinal cord, nerves, and muscles. These manifestations can vary widely depending on the specific location and nature of the underlying problem. They may include motor (movement-related) symptoms such as weakness, paralysis, tremors, or difficulty with coordination; sensory symptoms such as numbness, tingling, or pain; cognitive or behavioral changes; seizures; and autonomic symptoms such as changes in blood pressure, heart rate, or sweating. Neurologic manifestations can be caused by a wide range of conditions, including infections, injuries, degenerative diseases, strokes, tumors, and autoimmune disorders.
An abnormal reflex in a medical context refers to an involuntary and exaggerated response or lack of response to a stimulus that is not expected in the normal physiological range. These responses can be indicative of underlying neurological disorders or damage to the nervous system. Examples include hyperreflexia (overactive reflexes) and hyporeflexia (underactive reflexes). The assessment of reflexes is an important part of a physical examination, as it can provide valuable information about the functioning of the nervous system.
Progressive bulbar palsy (PBP) is a form of motor neuron disease (MND), also known as Amyotrophic Lateral Sclerosis (ALS). It is characterized by the progressive degeneration of the motor neurons in the brainstem, which control vital functions such as swallowing, speaking, chewing, and breathing.
In PBP, these symptoms gradually worsen over time, often resulting in severe disability and ultimately death due to respiratory failure. The progression of the disease can vary from person to person, but it typically advances more slowly than other forms of ALS. There is currently no cure for PBP or any other form of MND, and treatment is focused on managing symptoms and maintaining quality of life.
An intracranial aneurysm is a localized, blood-filled dilation or bulging in the wall of a cerebral artery within the skull (intracranial). These aneurysms typically occur at weak points in the arterial walls, often at branching points where the vessel divides into smaller branches. Over time, the repeated pressure from blood flow can cause the vessel wall to weaken and balloon out, forming a sac-like structure. Intracranial aneurysms can vary in size, ranging from a few millimeters to several centimeters in diameter.
There are three main types of intracranial aneurysms:
1. Saccular (berry) aneurysm: This is the most common type, characterized by a round or oval shape with a narrow neck and a bulging sac. They usually develop at branching points in the arteries due to congenital weaknesses in the vessel wall.
2. Fusiform aneurysm: These aneurysms have a dilated segment along the length of the artery, forming a cigar-shaped or spindle-like structure. They are often caused by atherosclerosis and can affect any part of the cerebral arteries.
3. Dissecting aneurysm: This type occurs when there is a tear in the inner lining (intima) of the artery, allowing blood to flow between the layers of the vessel wall. It can lead to narrowing or complete blockage of the affected artery and may cause subarachnoid hemorrhage if it ruptures.
Intracranial aneurysms can be asymptomatic and discovered incidentally during imaging studies for other conditions. However, when they grow larger or rupture, they can lead to severe complications such as subarachnoid hemorrhage, stroke, or even death. Treatment options include surgical clipping, endovascular coiling, or flow diversion techniques to prevent further growth and potential rupture of the aneurysm.
Meningeal tuberculosis, also known as Tuberculous meningitis, is a severe form of tuberculosis (TB) that affects the meninges, which are the membranes covering the brain and spinal cord. It is caused by the Mycobacterium tuberculosis bacterium, which can spread through the bloodstream from a primary infection site in the lungs or elsewhere in the body.
In meningeal tuberculosis, the bacteria cause inflammation and thickening of the meninges, leading to increased intracranial pressure, cerebral edema, and vasculitis. These conditions can result in various neurological symptoms such as headache, fever, stiff neck, altered mental status, seizures, and focal neurologic deficits. If left untreated, meningeal tuberculosis can lead to severe complications, including brain damage, hydrocephalus, and even death.
Diagnosis of meningeal tuberculosis typically involves a combination of clinical symptoms, cerebrospinal fluid (CSF) analysis, imaging studies, and sometimes molecular or culture-based tests to detect the presence of Mycobacterium tuberculosis in the CSF. Treatment usually involves a prolonged course of antibiotics specifically designed to target TB, such as isoniazid, rifampin, ethambutol, and pyrazinamide, often administered for six to nine months or longer. In some cases, corticosteroids may also be used to reduce inflammation and prevent complications.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Botulinum antitoxin refers to a medication made from the antibodies that are generated in response to the botulinum toxin, which is produced by the bacterium Clostridium botulinum. Botulinum toxin is a potent neurotoxin that can cause paralysis and other serious medical complications in humans and animals.
The antitoxin works by neutralizing the effects of the toxin in the body, preventing further damage to the nervous system. It is typically used in emergency situations to treat individuals who have been exposed to large amounts of botulinum toxin, such as in a bioterrorism attack or accidental exposure in a laboratory setting.
Botulinum antitoxin is not the same as botulinum toxin type A (Botox), which is a purified form of the toxin that is used for cosmetic and therapeutic purposes. Botox works by temporarily paralyzing muscles, whereas the antitoxin works by neutralizing the toxin in the body.
A fatal outcome is a term used in medical context to describe a situation where a disease, injury, or illness results in the death of an individual. It is the most severe and unfortunate possible outcome of any medical condition, and is often used as a measure of the severity and prognosis of various diseases and injuries. In clinical trials and research, fatal outcome may be used as an endpoint to evaluate the effectiveness and safety of different treatments or interventions.
I'm sorry for any confusion, but "Polyvinyls" is not a medical term. It is a chemical term that refers to polymers made from vinyl chloride, which is used in the production of various plastics and resins. If you have any questions about medical terms or concepts, I'd be happy to help with those!
Nerve degeneration, also known as neurodegeneration, is the progressive loss of structure and function of neurons, which can lead to cognitive decline, motor impairment, and various other symptoms. This process occurs due to a variety of factors, including genetics, environmental influences, and aging. It is a key feature in several neurological disorders such as Alzheimer's disease, Parkinson's disease, Huntington's disease, and multiple sclerosis. The degeneration can affect any part of the nervous system, leading to different symptoms depending on the location and extent of the damage.
Platybasia is a medical term that refers to a condition where the base of the skull is flattened or broadened, resulting in an abnormal increase in the angle between the clivus (a part of the sphenoid bone) and the posterior aspect of the upper surface of the palatine bone. This condition can be congenital or acquired and is often associated with other skeletal abnormalities. In some cases, platybasia may lead to neurological symptoms such as headaches, neck pain, or even brainstem compression.
Sagittal sinus thrombosis is a medical condition that refers to the formation of a blood clot (thrombus) in the sagittal sinus, which is a venous structure located in the brain. The sagittal sinus runs along the midline of the brain and receives blood from the superficial veins of the brain.
Sagittal sinus thrombosis can occur as a result of various conditions, such as head trauma, infection, cancer, or certain medical disorders that cause hypercoagulability (an increased tendency to form blood clots). The formation of a blood clot in the sagittal sinus can obstruct the flow of blood from the brain, leading to symptoms such as headache, seizures, altered consciousness, and focal neurological deficits.
Diagnosis of sagittal sinus thrombosis typically involves imaging studies such as computed tomography (CT) or magnetic resonance imaging (MRI) scans, which can show the presence of a blood clot in the sagittal sinus. Treatment may involve administering anticoagulant medications to prevent further growth of the blood clot and reduce the risk of complications such as pulmonary embolism or cerebral infarction. In some cases, surgical intervention may be necessary to remove the blood clot or alleviate pressure on the brain.
The spinal cord is a major part of the nervous system, extending from the brainstem and continuing down to the lower back. It is a slender, tubular bundle of nerve fibers (axons) and support cells (glial cells) that carries signals between the brain and the rest of the body. The spinal cord primarily serves as a conduit for motor information, which travels from the brain to the muscles, and sensory information, which travels from the body to the brain. It also contains neurons that can independently process and respond to information within the spinal cord without direct input from the brain.
The spinal cord is protected by the bony vertebral column (spine) and is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each segment corresponds to a specific region of the body and gives rise to pairs of spinal nerves that exit through the intervertebral foramina at each level.
The spinal cord is responsible for several vital functions, including:
1. Reflexes: Simple reflex actions, such as the withdrawal reflex when touching a hot surface, are mediated by the spinal cord without involving the brain.
2. Muscle control: The spinal cord carries motor signals from the brain to the muscles, enabling voluntary movement and muscle tone regulation.
3. Sensory perception: The spinal cord transmits sensory information, such as touch, temperature, pain, and vibration, from the body to the brain for processing and awareness.
4. Autonomic functions: The sympathetic and parasympathetic divisions of the autonomic nervous system originate in the thoracolumbar and sacral regions of the spinal cord, respectively, controlling involuntary physiological responses like heart rate, blood pressure, digestion, and respiration.
Damage to the spinal cord can result in various degrees of paralysis or loss of sensation below the level of injury, depending on the severity and location of the damage.
Otitis externa, also known as swimmer's ear, is a medical condition characterized by inflammation or infection of the external auditory canal (the outermost part of the ear canal leading to the eardrum). It often occurs when water stays in the ear after swimming, creating a moist environment that promotes bacterial growth.
The symptoms of otitis externa may include:
- Redness and swelling of the ear canal
- Pain or discomfort in the ear, especially when moving the jaw or chewing
- Itching in the ear
- Discharge from the ear (pus or clear fluid)
- Hearing loss or difficulty hearing
Otitis externa is typically treated with antibiotic eardrops and sometimes oral antibiotics. Keeping the ear dry during treatment is important to prevent further irritation and promote healing. In severe cases, a healthcare provider may need to clean the ear canal before administering medication.
Tinnitus is the perception of ringing or other sounds in the ears or head when no external sound is present. It can be described as a sensation of hearing sound even when no actual noise is present. The sounds perceived can vary widely, from a whistling, buzzing, hissing, swooshing, to a pulsating sound, and can be soft or loud.
Tinnitus is not a disease itself but a symptom that can result from a wide range of underlying causes, such as hearing loss, exposure to loud noises, ear infections, earwax blockage, head or neck injuries, circulatory system disorders, certain medications, and age-related hearing loss.
Tinnitus can be temporary or chronic, and it may affect one or both ears. While tinnitus is not usually a sign of a serious medical condition, it can significantly impact quality of life and interfere with daily activities, sleep, and concentration.
Therapeutic embolization is a medical procedure that involves intentionally blocking or obstructing blood vessels to stop excessive bleeding or block the flow of blood to a tumor or abnormal tissue. This is typically accomplished by injecting small particles, such as microspheres or coils, into the targeted blood vessel through a catheter, which is inserted into a larger blood vessel and guided to the desired location using imaging techniques like X-ray or CT scanning. The goal of therapeutic embolization is to reduce the size of a tumor, control bleeding, or block off abnormal blood vessels that are causing problems.
The ear is the sensory organ responsible for hearing and maintaining balance. It can be divided into three parts: the outer ear, middle ear, and inner ear. The outer ear consists of the pinna (the visible part of the ear) and the external auditory canal, which directs sound waves toward the eardrum. The middle ear contains three small bones called ossicles that transmit sound vibrations from the eardrum to the inner ear. The inner ear contains the cochlea, a spiral-shaped organ responsible for converting sound vibrations into electrical signals that are sent to the brain, and the vestibular system, which is responsible for maintaining balance.
Botulism is a rare but serious condition caused by the toxin produced by the bacterium Clostridium botulinum. The neurotoxin causes muscle paralysis, which can lead to respiratory failure and death if not treated promptly. Botulism can occur in three main forms: foodborne, wound, and infant.
Foodborne botulism is caused by consuming contaminated food, usually home-canned or fermented foods with low acid content. Wound botulism occurs when the bacterium infects a wound and produces toxin in the body. Infant botulism affects babies under one year of age who have ingested spores of the bacterium, which then colonize the intestines and produce toxin.
Symptoms of botulism include double vision, drooping eyelids, slurred speech, difficulty swallowing, dry mouth, muscle weakness, and paralysis that progresses downward from the head to the limbs. Treatment typically involves supportive care such as mechanical ventilation, intensive care unit monitoring, and antitoxin therapy. Prevention measures include proper food handling and canning techniques, prompt wound care, and avoiding consumption of known sources of contaminated food.
Vocal cord paralysis is a medical condition characterized by the inability of one or both vocal cords to move or function properly due to nerve damage or disruption. The vocal cords are two bands of muscle located in the larynx (voice box) that vibrate to produce sound during speech, singing, and breathing. When the nerves that control the vocal cord movements are damaged or not functioning correctly, the vocal cords may become paralyzed or weakened, leading to voice changes, breathing difficulties, and other symptoms.
The causes of vocal cord paralysis can vary, including neurological disorders, trauma, tumors, surgery, or infections. The diagnosis typically involves a physical examination, including a laryngoscopy, to assess the movement and function of the vocal cords. Treatment options may include voice therapy, surgical procedures, or other interventions to improve voice quality and breathing functions.
The vagus nerve, also known as the 10th cranial nerve (CN X), is the longest of the cranial nerves and extends from the brainstem to the abdomen. It has both sensory and motor functions and plays a crucial role in regulating various bodily functions such as heart rate, digestion, respiratory rate, speech, and sweating, among others.
The vagus nerve is responsible for carrying sensory information from the internal organs to the brain, and it also sends motor signals from the brain to the muscles of the throat and voice box, as well as to the heart, lungs, and digestive tract. The vagus nerve helps regulate the body's involuntary responses, such as controlling heart rate and blood pressure, promoting relaxation, and reducing inflammation.
Dysfunction in the vagus nerve can lead to various medical conditions, including gastroparesis, chronic pain, and autonomic nervous system disorders. Vagus nerve stimulation (VNS) is a therapeutic intervention that involves delivering electrical impulses to the vagus nerve to treat conditions such as epilepsy, depression, and migraine headaches.
Chemoreceptor cells are specialized sensory neurons that detect and respond to chemical changes in the internal or external environment. They play a crucial role in maintaining homeostasis within the body by converting chemical signals into electrical impulses, which are then transmitted to the central nervous system for further processing and response.
There are two main types of chemoreceptor cells:
1. Oxygen Chemoreceptors: These cells are located in the carotid bodies near the bifurcation of the common carotid artery and in the aortic bodies close to the aortic arch. They monitor the levels of oxygen, carbon dioxide, and pH in the blood and respond to decreases in oxygen concentration or increases in carbon dioxide and hydrogen ions (indicating acidity) by increasing their firing rate. This signals the brain to increase respiratory rate and depth, thereby restoring normal oxygen levels.
2. Taste Cells: These chemoreceptor cells are found within the taste buds of the tongue and other areas of the oral cavity. They detect specific tastes (salty, sour, sweet, bitter, and umami) by interacting with molecules from food. When a tastant binds to receptors on the surface of a taste cell, it triggers a series of intracellular signaling events that ultimately lead to the generation of an action potential. This information is then relayed to the brain, where it is interpreted as taste sensation.
In summary, chemoreceptor cells are essential for maintaining physiological balance by detecting and responding to chemical stimuli in the body. They play a critical role in regulating vital functions such as respiration and digestion.
Radiosurgery is a non-invasive surgical procedure that uses precisely focused beams of radiation to treat various medical conditions, primarily in the field of neurosurgery and oncology. It allows for the destruction of targeted tissue while minimizing damage to surrounding healthy structures. Unlike traditional surgery, radiosurgery does not require any incisions, as it delivers radiation through the skin to reach the intended target.
The term "stereotactic" is often associated with radiosurgery, which refers to the use of a three-dimensional coordinate system to precisely locate and target the affected area. This technique enables high doses of radiation to be delivered accurately and efficiently, maximizing therapeutic effectiveness while minimizing side effects.
Radiosurgery can be used to treat various conditions such as brain tumors (both malignant and benign), arteriovenous malformations (AVMs), trigeminal neuralgia, acoustic neuromas, pituitary adenomas, and spinal cord tumors. Common radiosurgery platforms include the Gamma Knife, CyberKnife, and linear accelerator-based systems like Novalis Tx or TrueBeam.
It is essential to note that although it is called "surgery," radiosurgery does not involve any physical incisions or removal of tissue. Instead, it relies on the destructive effects of high-dose radiation to ablate or damage targeted cells over time, leading to their eventual death and resolution of symptoms or tumor control.
Cerebellar diseases refer to a group of medical conditions that affect the cerebellum, which is the part of the brain located at the back of the head, below the occipital lobe and above the brainstem. The cerebellum plays a crucial role in motor control, coordination, balance, and some cognitive functions.
Cerebellar diseases can be caused by various factors, including genetics, infections, tumors, stroke, trauma, or degenerative processes. These conditions can result in a wide range of symptoms, such as:
1. Ataxia: Loss of coordination and unsteady gait
2. Dysmetria: Inability to judge distance and force while performing movements
3. Intention tremors: Shaking or trembling that worsens during purposeful movements
4. Nystagmus: Rapid, involuntary eye movement
5. Dysarthria: Speech difficulty due to muscle weakness or incoordination
6. Hypotonia: Decreased muscle tone
7. Titubation: Rhythmic, involuntary oscillations of the head and neck
8. Cognitive impairment: Problems with memory, attention, and executive functions
Some examples of cerebellar diseases include:
1. Ataxia-telangiectasia
2. Friedrich's ataxia
3. Multiple system atrophy (MSA)
4. Spinocerebellar ataxias (SCAs)
5. Cerebellar tumors, such as medulloblastomas or astrocytomas
6. Infarctions or hemorrhages in the cerebellum due to stroke or trauma
7. Infections, such as viral encephalitis or bacterial meningitis
8. Autoimmune disorders, like multiple sclerosis (MS) or paraneoplastic syndromes
9. Metabolic disorders, such as Wilson's disease or phenylketonuria (PKU)
10. Chronic alcoholism and withdrawal
Treatment for cerebellar diseases depends on the underlying cause and may involve medications, physical therapy, surgery, or supportive care to manage symptoms and improve quality of life.
In medical terms, the orbit refers to the bony cavity or socket in the skull that contains and protects the eye (eyeball) and its associated structures, including muscles, nerves, blood vessels, fat, and the lacrimal gland. The orbit is made up of several bones: the frontal bone, sphenoid bone, zygomatic bone, maxilla bone, and palatine bone. These bones form a pyramid-like shape that provides protection for the eye while also allowing for a range of movements.
Miller Fisher Syndrome (MFS) is a rare neurological disorder that is considered a variant of Guillain-Barré syndrome. It is characterized by the triad of symptoms including ophthalmoplegia (paralysis of the eye muscles), ataxia (loss of coordination and balance), and areflexia (absence of reflexes). Some patients may also experience weakness or paralysis in the limbs, and some cases may involve bulbar symptoms such as dysphagia (difficulty swallowing) and dysarthria (slurred speech). The syndrome is caused by an immune response that damages the nerves, and it often follows a viral infection. Treatment typically includes supportive care, plasma exchange, or intravenous immunoglobulin therapy to help reduce the severity of the symptoms.
"Cat" is a common name that refers to various species of small carnivorous mammals that belong to the family Felidae. The domestic cat, also known as Felis catus or Felis silvestris catus, is a popular pet and companion animal. It is a subspecies of the wildcat, which is found in Europe, Africa, and Asia.
Domestic cats are often kept as pets because of their companionship, playful behavior, and ability to hunt vermin. They are also valued for their ability to provide emotional support and therapy to people. Cats are obligate carnivores, which means that they require a diet that consists mainly of meat to meet their nutritional needs.
Cats are known for their agility, sharp senses, and predatory instincts. They have retractable claws, which they use for hunting and self-defense. Cats also have a keen sense of smell, hearing, and vision, which allow them to detect prey and navigate their environment.
In medical terms, cats can be hosts to various parasites and diseases that can affect humans and other animals. Some common feline diseases include rabies, feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), and toxoplasmosis. It is important for cat owners to keep their pets healthy and up-to-date on vaccinations and preventative treatments to protect both the cats and their human companions.
The medulla oblongata is a part of the brainstem that is located in the posterior portion of the brainstem and continues with the spinal cord. It plays a vital role in controlling several critical bodily functions, such as breathing, heart rate, and blood pressure. The medulla oblongata also contains nerve pathways that transmit sensory information from the body to the brain and motor commands from the brain to the muscles. Additionally, it is responsible for reflexes such as vomiting, swallowing, coughing, and sneezing.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
The maxillary nerve, also known as the second division of the trigeminal nerve (cranial nerve V2), is a primary sensory nerve that provides innervation to the skin of the lower eyelid, side of the nose, part of the cheek, upper lip, and roof of the mouth. It also supplies sensory fibers to the mucous membranes of the nasal cavity, maxillary sinus, palate, and upper teeth. Furthermore, it contributes motor innervation to the muscles involved in chewing (muscles of mastication), specifically the tensor veli palatini and tensor tympani. The maxillary nerve originates from the trigeminal ganglion and passes through the foramen rotundum in the skull before reaching its target areas.
The neural crest is a transient, multipotent embryonic cell population that originates from the ectoderm (outermost layer) of the developing neural tube (precursor to the central nervous system). These cells undergo an epithelial-to-mesenchymal transition and migrate throughout the embryo, giving rise to a diverse array of cell types and structures.
Neural crest cells differentiate into various tissues, including:
1. Peripheral nervous system (PNS) components: sensory neurons, sympathetic and parasympathetic ganglia, and glial cells (e.g., Schwann cells).
2. Facial bones and cartilage, as well as connective tissue of the skull.
3. Melanocytes, which are pigment-producing cells in the skin.
4. Smooth muscle cells in major blood vessels, heart, gastrointestinal tract, and other organs.
5. Secretory cells in endocrine glands (e.g., chromaffin cells of the adrenal medulla).
6. Parts of the eye, such as the cornea and iris stroma.
7. Dental tissues, including dentin, cementum, and dental pulp.
Due to their wide-ranging contributions to various tissues and organs, neural crest cells play a crucial role in embryonic development and organogenesis. Abnormalities in neural crest cell migration or differentiation can lead to several congenital disorders, such as neurocristopathies.
A ganglion is a cluster of neuron cell bodies in the peripheral nervous system. Ganglia are typically associated with nerves and serve as sites for sensory processing, integration, and relay of information between the periphery and the central nervous system (CNS). The two main types of ganglia are sensory ganglia, which contain pseudounipolar neurons that transmit sensory information to the CNS, and autonomic ganglia, which contain multipolar neurons that control involuntary physiological functions.
Examples of sensory ganglia include dorsal root ganglia (DRG), which are associated with spinal nerves, and cranial nerve ganglia, such as the trigeminal ganglion. Autonomic ganglia can be further divided into sympathetic and parasympathetic ganglia, which regulate different aspects of the autonomic nervous system.
It's worth noting that in anatomy, "ganglion" refers to a group of nerve cell bodies, while in clinical contexts, "ganglion" is often used to describe a specific type of cystic structure that forms near joints or tendons, typically in the wrist or foot. These ganglia are not related to the peripheral nervous system's ganglia but rather are fluid-filled sacs that may cause discomfort or pain due to their size or location.
The skull is the bony structure that encloses and protects the brain, the eyes, and the ears. It is composed of two main parts: the cranium, which contains the brain, and the facial bones. The cranium is made up of several fused flat bones, while the facial bones include the upper jaw (maxilla), lower jaw (mandible), cheekbones, nose bones, and eye sockets (orbits).
The skull also provides attachment points for various muscles that control chewing, moving the head, and facial expressions. Additionally, it contains openings for blood vessels, nerves, and the spinal cord to pass through. The skull's primary function is to protect the delicate and vital structures within it from injury and trauma.
Dysarthria is a motor speech disorder that results from damage to the nervous system, particularly the brainstem or cerebellum. It affects the muscles used for speaking, causing slurred, slow, or difficult speech. The specific symptoms can vary depending on the underlying cause and the extent of nerve damage. Treatment typically involves speech therapy to improve communication abilities.
Nerve sheath neoplasms are a group of tumors that arise from the cells surrounding and supporting the nerves. These tumors can be benign or malignant and include schwannomas, neurofibromas, and malignant peripheral nerve sheath tumors (MPNSTs). Schwannomas develop from the Schwann cells that produce the myelin sheath of the nerve, while neurofibromas arise from the nerve's supporting cells called fibroblasts. MPNSTs are cancerous tumors that can grow rapidly and invade surrounding tissues. Nerve sheath neoplasms can cause various symptoms depending on their location and size, including pain, numbness, weakness, or paralysis in the affected area.
Peripheral Nervous System (PNS) diseases, also known as Peripheral Neuropathies, refer to conditions that affect the functioning of the peripheral nervous system, which includes all the nerves outside the brain and spinal cord. These nerves transmit signals between the central nervous system (CNS) and the rest of the body, controlling sensations, movements, and automatic functions such as heart rate and digestion.
PNS diseases can be caused by various factors, including genetics, infections, toxins, metabolic disorders, trauma, or autoimmune conditions. The symptoms of PNS diseases depend on the type and extent of nerve damage but often include:
1. Numbness, tingling, or pain in the hands and feet
2. Muscle weakness or cramps
3. Loss of reflexes
4. Decreased sensation to touch, temperature, or vibration
5. Coordination problems and difficulty with balance
6. Sexual dysfunction
7. Digestive issues, such as constipation or diarrhea
8. Dizziness or fainting due to changes in blood pressure
Examples of PNS diseases include Guillain-Barre syndrome, Charcot-Marie-Tooth disease, diabetic neuropathy, and peripheral nerve injuries. Treatment for these conditions varies depending on the underlying cause but may involve medications, physical therapy, lifestyle changes, or surgery.
Nerve Growth Factor (NGF) receptors are a type of protein molecule found on the surface of certain cells, specifically those associated with the nervous system. They play a crucial role in the development, maintenance, and survival of neurons (nerve cells). There are two main types of NGF receptors:
1. Tyrosine Kinase Receptor A (TrkA): This is a high-affinity receptor for NGF and is primarily found on sensory neurons and sympathetic neurons. TrkA activation by NGF leads to the initiation of various intracellular signaling pathways that promote neuronal survival, differentiation, and growth.
2. P75 Neurotrophin Receptor (p75NTR): This is a low-affinity receptor for NGF and other neurotrophins. It can function as a coreceptor with Trk receptors to modulate their signals or act independently to mediate cell death under certain conditions.
Together, these two types of NGF receptors help regulate the complex interactions between neurons and their targets during development and throughout adult life.
Bell palsy is a peripheral facial nerve palsy, which means that it is a weakness or paralysis of the facial nerves (cranial nerve VII) that causes sudden asymmetric weakness on one side of the face. The symptoms can vary from mild to severe and may include:
* Sudden weakness or paralysis on one side of the face
* Drooping of the mouth, causing difficulty with smiling, eating, drinking, or speaking
* Inability to close one eye
* Dryness of the eye and mouth
* Changes in taste sensation
* Discomfort around the jaw and behind the ear
* Headache
* Increased sensitivity to sound
The exact cause of Bell palsy is not known, but it is believed to be related to inflammation or swelling of the facial nerve. It may also be associated with viral infections such as herpes simplex virus or HIV. In most cases, Bell palsy resolves on its own within a few weeks to months, although some people may experience residual symptoms such as facial weakness or asymmetry. Treatment typically involves corticosteroids and antiviral medications, which can help reduce inflammation and speed up recovery.
Brain diseases, also known as neurological disorders, refer to a wide range of conditions that affect the brain and nervous system. These diseases can be caused by various factors such as genetics, infections, injuries, degeneration, or structural abnormalities. They can affect different parts of the brain, leading to a variety of symptoms and complications.
Some examples of brain diseases include:
1. Alzheimer's disease - a progressive degenerative disorder that affects memory and cognitive function.
2. Parkinson's disease - a movement disorder characterized by tremors, stiffness, and difficulty with coordination and balance.
3. Multiple sclerosis - a chronic autoimmune disease that affects the nervous system and can cause a range of symptoms such as vision loss, muscle weakness, and cognitive impairment.
4. Epilepsy - a neurological disorder characterized by recurrent seizures.
5. Brain tumors - abnormal growths in the brain that can be benign or malignant.
6. Stroke - a sudden interruption of blood flow to the brain, which can cause paralysis, speech difficulties, and other neurological symptoms.
7. Meningitis - an infection of the membranes surrounding the brain and spinal cord.
8. Encephalitis - an inflammation of the brain that can be caused by viruses, bacteria, or autoimmune disorders.
9. Huntington's disease - a genetic disorder that affects muscle coordination, cognitive function, and mental health.
10. Migraine - a neurological condition characterized by severe headaches, often accompanied by nausea, vomiting, and sensitivity to light and sound.
Brain diseases can range from mild to severe and may be treatable or incurable. They can affect people of all ages and backgrounds, and early diagnosis and treatment are essential for improving outcomes and quality of life.
Surgical decompression is a medical procedure that involves relieving pressure on a nerve or tissue by creating additional space. This is typically accomplished through the removal of a portion of bone or other tissue that is causing the compression. The goal of surgical decompression is to alleviate symptoms such as pain, numbness, tingling, or weakness caused by the compression.
In the context of spinal disorders, surgical decompression is often used to treat conditions such as herniated discs, spinal stenosis, or bone spurs that are compressing nerves in the spine. The specific procedure used may vary depending on the location and severity of the compression, but common techniques include laminectomy, discectomy, and foraminotomy.
It's important to note that surgical decompression is a significant medical intervention that carries risks such as infection, bleeding, and injury to surrounding tissues. As with any surgery, it should be considered as a last resort after other conservative treatments have been tried and found to be ineffective. A thorough evaluation by a qualified medical professional is necessary to determine whether surgical decompression is appropriate in a given case.
Meningitis is a medical condition characterized by the inflammation of the meninges, which are the membranes that cover the brain and spinal cord. This inflammation can be caused by various infectious agents, such as bacteria, viruses, fungi, or parasites, or by non-infectious causes like autoimmune diseases, cancer, or certain medications.
The symptoms of meningitis may include fever, headache, stiff neck, nausea, vomiting, confusion, and sensitivity to light. In severe cases, it can lead to seizures, coma, or even death if not treated promptly and effectively. Bacterial meningitis is usually more severe and requires immediate medical attention, while viral meningitis is often less severe and may resolve on its own without specific treatment.
It's important to note that meningitis can be a serious and life-threatening condition, so if you suspect that you or someone else has symptoms of meningitis, you should seek medical attention immediately.
A taste bud is a cluster of specialized sensory cells found primarily on the tongue, soft palate, and cheek that are responsible for the sense of taste. They contain receptor cells which detect specific tastes: sweet, salty, sour, bitter, and umami (savory). Each taste bud contains supporting cells and 50-100 taste receptor cells. These cells have hair-like projections called microvilli that come into contact with food or drink, transmitting signals to the brain to interpret the taste.
The external carotid artery is a major blood vessel in the neck that supplies oxygenated blood to the structures of the head and neck, excluding the brain. It originates from the common carotid artery at the level of the upper border of the thyroid cartilage, then divides into several branches that supply various regions of the head and neck, including the face, scalp, ears, and neck muscles.
The external carotid artery has eight branches:
1. Superior thyroid artery: Supplies blood to the thyroid gland, larynx, and surrounding muscles.
2. Ascending pharyngeal artery: Supplies blood to the pharynx, palate, and meninges of the brain.
3. Lingual artery: Supplies blood to the tongue and floor of the mouth.
4. Facial artery: Supplies blood to the face, nose, lips, and palate.
5. Occipital artery: Supplies blood to the scalp and muscles of the neck.
6. Posterior auricular artery: Supplies blood to the ear and surrounding muscles.
7. Maxillary artery: Supplies blood to the lower face, nasal cavity, palate, and meninges of the brain.
8. Superficial temporal artery: Supplies blood to the scalp, face, and temporomandibular joint.
The external carotid artery is an essential structure for maintaining adequate blood flow to the head and neck, and any damage or blockage can lead to serious medical conditions such as stroke or tissue necrosis.
Brainstem infarctions refer to the damage or death of brain tissue in the brainstem due to lack of blood supply, resulting in a localized injury known as an infarction. The brainstem is a critical region that controls essential functions such as breathing, heart rate, and consciousness. Infarctions in this area can result in various symptoms depending on the location and extent of damage, which may include:
1. Hemiparesis or paralysis on one side of the body
2. Cranial nerve dysfunction, leading to double vision, slurred speech, or facial weakness
3. Difficulty swallowing or speaking
4. Unstable blood pressure and heart rate
5. Altered level of consciousness, ranging from confusion to coma
6. Abnormal muscle tone and reflexes
7. Respiratory disturbances, such as irregular breathing patterns or apnea (cessation of breathing)
Brainstem infarctions can be caused by various conditions, including atherosclerosis, embolism, vasospasm, or small vessel disease. Prompt diagnosis and treatment are crucial to minimize the risk of long-term disability or death.
Central nervous system (CNS) diseases refer to medical conditions that primarily affect the brain and spinal cord. The CNS is responsible for controlling various functions in the body, including movement, sensation, cognition, and behavior. Therefore, diseases of the CNS can have significant impacts on a person's quality of life and overall health.
There are many different types of CNS diseases, including:
1. Infectious diseases: These are caused by viruses, bacteria, fungi, or parasites that infect the brain or spinal cord. Examples include meningitis, encephalitis, and polio.
2. Neurodegenerative diseases: These are characterized by progressive loss of nerve cells in the brain or spinal cord. Examples include Alzheimer's disease, Parkinson's disease, and Huntington's disease.
3. Structural diseases: These involve damage to the physical structure of the brain or spinal cord, such as from trauma, tumors, or stroke.
4. Functional diseases: These affect the function of the nervous system without obvious structural damage, such as multiple sclerosis and epilepsy.
5. Genetic disorders: Some CNS diseases are caused by genetic mutations, such as spinal muscular atrophy and Friedreich's ataxia.
Symptoms of CNS diseases can vary widely depending on the specific condition and the area of the brain or spinal cord that is affected. They may include muscle weakness, paralysis, seizures, loss of sensation, difficulty with coordination and balance, confusion, memory loss, changes in behavior or mood, and pain. Treatment for CNS diseases depends on the specific condition and may involve medications, surgery, rehabilitation therapy, or a combination of these approaches.
The brain is the central organ of the nervous system, responsible for receiving and processing sensory information, regulating vital functions, and controlling behavior, movement, and cognition. It is divided into several distinct regions, each with specific functions:
1. Cerebrum: The largest part of the brain, responsible for higher cognitive functions such as thinking, learning, memory, language, and perception. It is divided into two hemispheres, each controlling the opposite side of the body.
2. Cerebellum: Located at the back of the brain, it is responsible for coordinating muscle movements, maintaining balance, and fine-tuning motor skills.
3. Brainstem: Connects the cerebrum and cerebellum to the spinal cord, controlling vital functions such as breathing, heart rate, and blood pressure. It also serves as a relay center for sensory information and motor commands between the brain and the rest of the body.
4. Diencephalon: A region that includes the thalamus (a major sensory relay station) and hypothalamus (regulates hormones, temperature, hunger, thirst, and sleep).
5. Limbic system: A group of structures involved in emotional processing, memory formation, and motivation, including the hippocampus, amygdala, and cingulate gyrus.
The brain is composed of billions of interconnected neurons that communicate through electrical and chemical signals. It is protected by the skull and surrounded by three layers of membranes called meninges, as well as cerebrospinal fluid that provides cushioning and nutrients.
Eyelids are the thin folds of skin that cover and protect the front surface (cornea) of the eye when closed. They are composed of several layers, including the skin, muscle, connective tissue, and a mucous membrane called the conjunctiva. The upper and lower eyelids meet at the outer corner of the eye (lateral canthus) and the inner corner of the eye (medial canthus).
The main function of the eyelids is to protect the eye from foreign particles, light, and trauma. They also help to distribute tears evenly over the surface of the eye through blinking, which helps to keep the eye moist and healthy. Additionally, the eyelids play a role in facial expressions and non-verbal communication.
Denervation is a medical term that refers to the loss or removal of nerve supply to an organ or body part. This can occur as a result of surgical intervention, injury, or disease processes that damage the nerves leading to the affected area. The consequences of denervation depend on the specific organ or tissue involved, but generally, it can lead to changes in function, sensation, and muscle tone. For example, denervation of a skeletal muscle can cause weakness, atrophy, and altered reflexes. Similarly, denervation of an organ such as the heart can lead to abnormalities in heart rate and rhythm. In some cases, denervation may be intentional, such as during surgical procedures aimed at treating chronic pain or spasticity.
Sciatic neuropathy is a condition that results from damage or injury to the sciatic nerve, which is the largest nerve in the human body. The sciatic nerve originates from the lower spine (lumbar and sacral regions) and travels down through the buttocks, hips, and legs to the feet.
Sciatic neuropathy can cause various symptoms, including pain, numbness, tingling, weakness, or difficulty moving the affected leg or foot. The pain associated with sciatic neuropathy is often described as sharp, shooting, or burning and may worsen with movement, coughing, or sneezing.
The causes of sciatic neuropathy include compression or irritation of the nerve due to conditions such as herniated discs, spinal stenosis, bone spurs, tumors, or piriformis syndrome. Trauma or injury to the lower back, hip, or buttocks can also cause sciatic neuropathy.
Diagnosing sciatic neuropathy typically involves a physical examination and medical history, as well as imaging tests such as X-rays, MRI, or CT scans to visualize the spine and surrounding structures. Treatment options may include pain management, physical therapy, steroid injections, or surgery, depending on the severity and underlying cause of the condition.
Pituitary apoplexy is a medical emergency that involves bleeding into the pituitary gland (a small gland at the base of the brain) and/or sudden swelling of the pituitary gland. This can lead to compression of nearby structures, such as the optic nerves and the hypothalamus, causing symptoms like severe headache, visual disturbances, hormonal imbalances, and altered mental status. It is often associated with a pre-existing pituitary tumor (such as a pituitary adenoma), but can also occur in individuals without any known pituitary abnormalities. Immediate medical attention is required to manage this condition, which may include surgical intervention, hormone replacement therapy, and supportive care.
Eye diseases are a range of conditions that affect the eye or visual system, causing damage to vision and, in some cases, leading to blindness. These diseases can be categorized into various types, including:
1. Refractive errors: These include myopia (nearsightedness), hyperopia (farsightedness), astigmatism, and presbyopia, which affect the way light is focused on the retina and can usually be corrected with glasses or contact lenses.
2. Cataracts: A clouding of the lens inside the eye that leads to blurry vision, glare, and decreased contrast sensitivity. Cataract surgery is the most common treatment for this condition.
3. Glaucoma: A group of diseases characterized by increased pressure in the eye, leading to damage to the optic nerve and potential blindness if left untreated. Treatment includes medications, laser therapy, or surgery.
4. Age-related macular degeneration (AMD): A progressive condition that affects the central part of the retina called the macula, causing blurry vision and, in advanced stages, loss of central vision. Treatment may include anti-VEGF injections, laser therapy, or nutritional supplements.
5. Diabetic retinopathy: A complication of diabetes that affects the blood vessels in the retina, leading to bleeding, leakage, and potential blindness if left untreated. Treatment includes laser therapy, anti-VEGF injections, or surgery.
6. Retinal detachment: A separation of the retina from its underlying tissue, which can lead to vision loss if not treated promptly with surgery.
7. Amblyopia (lazy eye): A condition where one eye does not develop normal vision, often due to a misalignment or refractive error in childhood. Treatment includes correcting the underlying problem and encouraging the use of the weaker eye through patching or other methods.
8. Strabismus (crossed eyes): A misalignment of the eyes that can lead to amblyopia if not treated promptly with surgery, glasses, or other methods.
9. Corneal diseases: Conditions that affect the transparent outer layer of the eye, such as keratoconus, Fuchs' dystrophy, and infectious keratitis, which can lead to vision loss if not treated promptly.
10. Uveitis: Inflammation of the middle layer of the eye, which can cause vision loss if not treated promptly with anti-inflammatory medications or surgery.
Auditory brainstem evoked potentials (ABEPs or BAEPs) are medical tests that measure the electrical activity in the auditory pathway of the brain in response to sound stimulation. The test involves placing electrodes on the scalp and recording the tiny electrical signals generated by the nerve cells in the brainstem as they respond to clicks or tone bursts presented through earphones.
The resulting waveform is analyzed for latency (the time it takes for the signal to travel from the ear to the brain) and amplitude (the strength of the signal). Abnormalities in the waveform can indicate damage to the auditory nerve or brainstem, and are often used in the diagnosis of various neurological conditions such as multiple sclerosis, acoustic neuroma, and brainstem tumors.
The test is non-invasive, painless, and takes only a few minutes to perform. It provides valuable information about the functioning of the auditory pathway and can help guide treatment decisions for patients with hearing or balance disorders.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
An epidermal cyst is a common benign skin condition characterized by the growth of a sac-like structure filled with keratin, a protein found in the outermost layer of the skin (epidermis). These cysts typically appear as round, firm bumps just under the surface of the skin, often on the face, neck, trunk, or scalp. They can vary in size from a few millimeters to several centimeters in diameter.
Epidermal cysts usually develop as a result of the accumulation of dead skin cells that become trapped within a hair follicle or a pilosebaceous unit (a structure that contains a hair follicle and an oil gland). The keratin produced by the skin cells then collects inside the sac, causing it to expand gradually.
These cysts are generally slow-growing, painless, and rarely cause any symptoms. However, they may become infected or inflamed, leading to redness, tenderness, pain, or pus formation. In such cases, medical attention might be necessary to drain the cyst or administer antibiotics to treat the infection.
Epidermal cysts can be removed surgically if they cause cosmetic concerns or become frequently infected. The procedure typically involves making an incision in the skin and removing the entire sac along with its contents to prevent recurrence.
Cranial sinuses are a part of the venous system in the human head. They are air-filled spaces located within the skull and are named according to their location. The cranial sinuses include:
1. Superior sagittal sinus: It runs along the top of the brain, inside the skull, and drains blood from the scalp and the veins of the brain.
2. Inferior sagittal sinus: It runs along the bottom of the brain and drains into the straight sinus.
3. Straight sinus: It is located at the back of the brain and receives blood from the inferior sagittal sinus and great cerebral vein.
4. Occipital sinuses: They are located at the back of the head and drain blood from the scalp and skull.
5. Cavernous sinuses: They are located on each side of the brain, near the temple, and receive blood from the eye and surrounding areas.
6. Sphenoparietal sinus: It is a small sinus that drains blood from the front part of the brain into the cavernous sinus.
7. Petrosquamosal sinuses: They are located near the ear and drain blood from the scalp and skull.
The cranial sinuses play an essential role in draining blood from the brain and protecting it from injury.
The nervous system is a complex, highly organized network of specialized cells called neurons and glial cells that communicate with each other via electrical and chemical signals to coordinate various functions and activities in the body. It consists of two main parts: the central nervous system (CNS), including the brain and spinal cord, and the peripheral nervous system (PNS), which includes all the nerves and ganglia outside the CNS.
The primary function of the nervous system is to receive, process, and integrate information from both internal and external environments and then respond by generating appropriate motor outputs or behaviors. This involves sensing various stimuli through specialized receptors, transmitting this information through afferent neurons to the CNS for processing, integrating this information with other inputs and memories, making decisions based on this processed information, and finally executing responses through efferent neurons that control effector organs such as muscles and glands.
The nervous system can be further divided into subsystems based on their functions, including the somatic nervous system, which controls voluntary movements and reflexes; the autonomic nervous system, which regulates involuntary physiological processes like heart rate, digestion, and respiration; and the enteric nervous system, which is a specialized subset of the autonomic nervous system that controls gut functions. Overall, the nervous system plays a critical role in maintaining homeostasis, regulating behavior, and enabling cognition and consciousness.
The chorda tympani nerve is a branch of the facial nerve (cranial nerve VII) that has both sensory and taste functions. It carries taste sensations from the anterior two-thirds of the tongue and sensory information from the oral cavity, including touch, temperature, and pain.
Anatomically, the chorda tympani nerve originates from the facial nerve's intermediate nerve, which is located in the temporal bone of the skull. It then travels through the middle ear, passing near the tympanic membrane (eardrum) before leaving the skull via the petrotympanic fissure. From there, it joins the lingual nerve, a branch of the mandibular division of the trigeminal nerve (cranial nerve V), which carries the taste and sensory information to the brainstem for processing.
Clinically, damage to the chorda tympani nerve can result in loss of taste sensation on the anterior two-thirds of the tongue and altered sensations in the oral cavity. This type of injury can occur during middle ear surgery or as a result of various medical conditions that affect the facial nerve or its branches.
Strabismus is a condition of the ocular muscles where the eyes are not aligned properly and point in different directions. One eye may turn inward, outward, upward, or downward while the other one remains fixed and aligns normally. This misalignment can occur occasionally or constantly. Strabismus is also commonly referred to as crossed eyes or walleye. The condition can lead to visual impairments such as amblyopia (lazy eye) and depth perception problems if not treated promptly and effectively, usually through surgery, glasses, or vision therapy.
Carotid artery diseases refer to conditions that affect the carotid arteries, which are the major blood vessels that supply oxygen-rich blood to the head and neck. The most common type of carotid artery disease is atherosclerosis, which occurs when fatty deposits called plaques build up in the inner lining of the arteries.
These plaques can cause the arteries to narrow or become blocked, reducing blood flow to the brain and increasing the risk of stroke. Other carotid artery diseases include carotid artery dissection, which occurs when there is a tear in the inner lining of the artery, and fibromuscular dysplasia, which is a condition that affects the muscle and tissue in the walls of the artery.
Symptoms of carotid artery disease may include neck pain or pulsations, transient ischemic attacks (TIAs) or "mini-strokes," and strokes. Treatment options for carotid artery disease depend on the severity and type of the condition but may include lifestyle changes, medications, endarterectomy (a surgical procedure to remove plaque from the artery), or angioplasty and stenting (procedures to open blocked arteries using a balloon and stent).
Sarcoidosis is a multi-system disorder characterized by the formation of granulomas (small clumps of inflammatory cells) in various organs, most commonly the lungs and lymphatic system. These granulomas can impair the function of the affected organ(s), leading to a variety of symptoms. The exact cause of sarcoidosis is unknown, but it's thought to be an overactive immune response to an unknown antigen, possibly triggered by an infection, chemical exposure, or another environmental factor.
The diagnosis of sarcoidosis typically involves a combination of clinical evaluation, imaging studies (such as chest X-rays and CT scans), and laboratory tests (including blood tests and biopsies). While there is no cure for sarcoidosis, treatment may be necessary to manage symptoms and prevent complications. Corticosteroids are often used to suppress the immune system and reduce inflammation, while other medications may be prescribed to treat specific organ involvement or symptoms. In some cases, sarcoidosis may resolve on its own without any treatment.
Gills are specialized respiratory organs found in many aquatic organisms such as fish, crustaceans, and some mollusks. They are typically thin, feathery structures that increase the surface area for gas exchange between the water and the animal's bloodstream. Gills extract oxygen from water while simultaneously expelling carbon dioxide.
In fish, gills are located in the gill chamber, which is covered by opercula or protective bony flaps. Water enters through the mouth, flows over the gills, and exits through the opercular openings. The movement of water over the gills allows for the diffusion of oxygen and carbon dioxide across the gill filaments and lamellae, which are the thin plates where gas exchange occurs.
Gills contain a rich supply of blood vessels, allowing for efficient transport of oxygen to the body's tissues and removal of carbon dioxide. The counter-current flow of water and blood in the gills ensures that the concentration gradient between the water and the blood is maximized, enhancing the efficiency of gas exchange.
Follow-up studies are a type of longitudinal research that involve repeated observations or measurements of the same variables over a period of time, in order to understand their long-term effects or outcomes. In medical context, follow-up studies are often used to evaluate the safety and efficacy of medical treatments, interventions, or procedures.
In a typical follow-up study, a group of individuals (called a cohort) who have received a particular treatment or intervention are identified and then followed over time through periodic assessments or data collection. The data collected may include information on clinical outcomes, adverse events, changes in symptoms or functional status, and other relevant measures.
The results of follow-up studies can provide important insights into the long-term benefits and risks of medical interventions, as well as help to identify factors that may influence treatment effectiveness or patient outcomes. However, it is important to note that follow-up studies can be subject to various biases and limitations, such as loss to follow-up, recall bias, and changes in clinical practice over time, which must be carefully considered when interpreting the results.
The vestibular nerve, also known as the vestibulocochlear nerve or cranial nerve VIII, is a pair of nerves that transmit sensory information from the balance-sensing structures in the inner ear (the utricle, saccule, and semicircular canals) to the brain. This information helps the brain maintain balance and orientation of the head in space. The vestibular nerve also plays a role in hearing by transmitting sound signals from the cochlea to the brain.
A skull fracture is a break in one or more of the bones that form the skull. It can occur from a direct blow to the head, penetrating injuries like gunshot wounds, or from strong rotational forces during an accident. There are several types of skull fractures, including:
1. Linear Skull Fracture: This is the most common type, where there's a simple break in the bone without any splintering, depression, or displacement. It often doesn't require treatment unless it's near a sensitive area like an eye or ear.
2. Depressed Skull Fracture: In this type, a piece of the skull is pushed inward toward the brain. Surgery may be needed to relieve pressure on the brain and repair the fracture.
3. Diastatic Skull Fracture: This occurs along the suture lines (the fibrous joints between the skull bones) that haven't fused yet, often seen in infants and young children.
4. Basilar Skull Fracture: This involves fractures at the base of the skull. It can be serious due to potential injury to the cranial nerves and blood vessels located in this area.
5. Comminuted Skull Fracture: In this severe type, the bone is shattered into many pieces. These fractures usually require extensive surgical repair.
Symptoms of a skull fracture can include pain, swelling, bruising, bleeding (if there's an open wound), and in some cases, clear fluid draining from the ears or nose (cerebrospinal fluid leak). Severe fractures may cause brain injury, leading to symptoms like confusion, loss of consciousness, seizures, or neurological deficits. Immediate medical attention is necessary for any suspected skull fracture.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
Unmyelinated nerve fibers, also known as unmyelinated axons or non-myelinated fibers, are nerve cells that lack a myelin sheath. Myelin is a fatty, insulating substance that surrounds the axon of many nerve cells and helps to increase the speed of electrical impulses traveling along the nerve fiber.
In unmyelinated nerve fibers, the axons are surrounded by a thin layer of Schwann cell processes called the endoneurium, but there is no continuous myelin sheath. Instead, the axons are packed closely together in bundles, with several axons lying within the same Schwann cell.
Unmyelinated nerve fibers tend to be smaller in diameter than myelinated fibers and conduct electrical impulses more slowly. They are commonly found in the autonomic nervous system, which controls involuntary functions such as heart rate, blood pressure, and digestion, as well as in sensory nerves that transmit pain and temperature signals.
Electromyography (EMG) is a medical diagnostic procedure that measures the electrical activity of skeletal muscles during contraction and at rest. It involves inserting a thin needle electrode into the muscle to record the electrical signals generated by the muscle fibers. These signals are then displayed on an oscilloscope and may be heard through a speaker.
EMG can help diagnose various neuromuscular disorders, such as muscle weakness, numbness, or pain, and can distinguish between muscle and nerve disorders. It is often used in conjunction with other diagnostic tests, such as nerve conduction studies, to provide a comprehensive evaluation of the nervous system.
EMG is typically performed by a neurologist or a physiatrist, and the procedure may cause some discomfort or pain, although this is usually minimal. The results of an EMG can help guide treatment decisions and monitor the progression of neuromuscular conditions over time.
Postoperative complications refer to any unfavorable condition or event that occurs during the recovery period after a surgical procedure. These complications can vary in severity and may include, but are not limited to:
1. Infection: This can occur at the site of the incision or inside the body, such as pneumonia or urinary tract infection.
2. Bleeding: Excessive bleeding (hemorrhage) can lead to a drop in blood pressure and may require further surgical intervention.
3. Blood clots: These can form in the deep veins of the legs (deep vein thrombosis) and can potentially travel to the lungs (pulmonary embolism).
4. Wound dehiscence: This is when the surgical wound opens up, which can lead to infection and further complications.
5. Pulmonary issues: These include atelectasis (collapsed lung), pneumonia, or respiratory failure.
6. Cardiovascular problems: These include abnormal heart rhythms (arrhythmias), heart attack, or stroke.
7. Renal failure: This can occur due to various reasons such as dehydration, blood loss, or the use of certain medications.
8. Pain management issues: Inadequate pain control can lead to increased stress, anxiety, and decreased mobility.
9. Nausea and vomiting: These can be caused by anesthesia, opioid pain medication, or other factors.
10. Delirium: This is a state of confusion and disorientation that can occur in the elderly or those with certain medical conditions.
Prompt identification and management of these complications are crucial to ensure the best possible outcome for the patient.
In medical terms, the "neck" is defined as the portion of the body that extends from the skull/head to the thorax or chest region. It contains 7 cervical vertebrae, muscles, nerves, blood vessels, lymphatic vessels, and glands (such as the thyroid gland). The neck is responsible for supporting the head, allowing its movement in various directions, and housing vital structures that enable functions like respiration and circulation.
The reticular formation is not a single structure but rather a complex network of interconnected neurons located in the brainstem, extending from the medulla oblongata through the pons and mesencephalon (midbrain) up to the diencephalon (thalamus and hypothalamus). It forms part of the reticular activating system, which is involved in regulating arousal, awareness, and sleep-wake cycles.
The reticular formation plays a crucial role in various functions such as:
1. Modulation of sensory input: The neurons in the reticular formation receive inputs from all senses (visual, auditory, tactile, etc.) and help filter and prioritize this information before it reaches higher cognitive areas.
2. Control of motor function: The reticular formation contributes to the regulation of muscle tone, posture, and locomotion by modulating the activity of motor neurons in the spinal cord.
3. Regulation of autonomic functions: The reticular formation is involved in controlling heart rate, blood pressure, respiration, and other visceral functions through its connections with the autonomic nervous system.
4. Consciousness and arousal: The ascending reticular activating system (ARAS) originates from the reticular formation and projects to the thalamus and cerebral cortex, where it helps maintain wakefulness and arousal. Damage to the ARAS can lead to coma or other states of altered consciousness.
5. Sleep-wake cycle regulation: The reticular formation contains cells that release neurotransmitters like histamine, serotonin, and orexin/hypocretin, which are essential for sleep-wake regulation. Dysfunction in these circuits has been implicated in various sleep disorders, such as narcolepsy and insomnia.
Nasopharyngeal neoplasms refer to abnormal growths or tumors in the nasopharynx, which is the upper part of the pharynx (throat) behind the nose. These growths can be benign (non-cancerous) or malignant (cancerous).
Malignant nasopharyngeal neoplasms are often referred to as nasopharyngeal carcinoma or cancer. There are different types of nasopharyngeal carcinomas, including keratinizing squamous cell carcinoma, non-keratinizing carcinoma, and basaloid squamous cell carcinoma.
The risk factors for developing nasopharyngeal neoplasms include exposure to the Epstein-Barr virus (EBV), consumption of certain foods, smoking, and genetic factors. Symptoms may include a lump in the neck, nosebleeds, hearing loss, ringing in the ears, and difficulty swallowing or speaking. Treatment options depend on the type, size, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
The Central Nervous System (CNS) is the part of the nervous system that consists of the brain and spinal cord. It is called the "central" system because it receives information from, and sends information to, the rest of the body through peripheral nerves, which make up the Peripheral Nervous System (PNS).
The CNS is responsible for processing sensory information, controlling motor functions, and regulating various autonomic processes like heart rate, respiration, and digestion. The brain, as the command center of the CNS, interprets sensory stimuli, formulates thoughts, and initiates actions. The spinal cord serves as a conduit for nerve impulses traveling to and from the brain and the rest of the body.
The CNS is protected by several structures, including the skull (which houses the brain) and the vertebral column (which surrounds and protects the spinal cord). Despite these protective measures, the CNS remains vulnerable to injury and disease, which can have severe consequences due to its crucial role in controlling essential bodily functions.
Carotid stenosis is a medical condition that refers to the narrowing or constriction of the lumen (inner space) of the carotid artery. The carotid arteries are major blood vessels that supply oxygenated blood to the head and neck. Carotid stenosis usually results from the buildup of plaque, made up of fat, cholesterol, calcium, and other substances, on the inner walls of the artery. This process is called atherosclerosis.
As the plaque accumulates, it causes the artery to narrow, reducing blood flow to the brain. Severe carotid stenosis can increase the risk of stroke, as a clot or debris from the plaque can break off and travel to the brain, blocking a smaller blood vessel and causing tissue damage or death.
Carotid stenosis is typically diagnosed through imaging tests such as ultrasound, CT angiography, or MRI angiography. Treatment options may include lifestyle modifications (such as quitting smoking, controlling blood pressure, and managing cholesterol levels), medications to reduce the risk of clots, or surgical procedures like endarterectomy or stenting to remove or bypass the blockage.
In medical terms, dissection refers to the separation of the layers of a biological tissue or structure by cutting or splitting. It is often used to describe the process of surgically cutting through tissues, such as during an operation to separate organs or examine their internal structures.
However, "dissection" can also refer to a pathological condition in which there is a separation of the layers of a blood vessel wall by blood, creating a false lumen or aneurysm. This type of dissection is most commonly seen in the aorta and can be life-threatening if not promptly diagnosed and treated.
In summary, "dissection" has both surgical and pathological meanings related to the separation of tissue layers, and it's essential to consider the context in which the term is used.
Sensorineural hearing loss (SNHL) is a type of hearing impairment that occurs due to damage to the inner ear (cochlea) or to the nerve pathways from the inner ear to the brain. It can be caused by various factors such as aging, exposure to loud noises, genetics, certain medical conditions (like diabetes and heart disease), and ototoxic medications.
SNHL affects the ability of the hair cells in the cochlea to convert sound waves into electrical signals that are sent to the brain via the auditory nerve. As a result, sounds may be perceived as muffled, faint, or distorted, making it difficult to understand speech, especially in noisy environments.
SNHL is typically permanent and cannot be corrected with medication or surgery, but hearing aids or cochlear implants can help improve communication and quality of life for those affected.
Histochemistry is the branch of pathology that deals with the microscopic localization of cellular or tissue components using specific chemical reactions. It involves the application of chemical techniques to identify and locate specific biomolecules within tissues, cells, and subcellular structures. This is achieved through the use of various staining methods that react with specific antigens or enzymes in the sample, allowing for their visualization under a microscope. Histochemistry is widely used in diagnostic pathology to identify different types of tissues, cells, and structures, as well as in research to study cellular and molecular processes in health and disease.
Ocular motility disorders refer to a group of conditions that affect the movement of the eyes. These disorders can result from nerve damage, muscle dysfunction, or brain injuries. They can cause abnormal eye alignment, limited range of motion, and difficulty coordinating eye movements. Common symptoms include double vision, blurry vision, strabismus (crossed eyes), nystagmus (involuntary eye movement), and difficulty tracking moving objects. Ocular motility disorders can be congenital or acquired and may require medical intervention to correct or manage the condition.
 Cranial nerves
Cranial nerves Cranial Nerve V - Trigeminal Maxillary Nerve
Cranial Nerve V - Trigeminal Maxillary Nerve Cranial Nerves Flashcards
Cranial Nerves Flashcards Abducens Nerve Palsy (Sixth Cranial Nerve Palsy): Background, Pathophysiology, Epidemiology
Abducens Nerve Palsy (Sixth Cranial Nerve Palsy): Background, Pathophysiology, Epidemiology Cranial Nerve Treatment and Surgery Options | UPMC
Cranial Nerve Treatment and Surgery Options | UPMC Cranial Nerves: Anatomy, Function and Clinical Significance - Nova Science Publishers
Cranial Nerves: Anatomy, Function and Clinical Significance - Nova Science Publishers Diagnose This: Aberrant regeneration of 3rd cranial nerve - American Academy of Ophthalmology
Diagnose This: Aberrant regeneration of 3rd cranial nerve - American Academy of Ophthalmology Lyme Disease Presenting with Multiple Cranial Nerve Deficits: Report of a Case
Lyme Disease Presenting with Multiple Cranial Nerve Deficits: Report of a Case Image: Functions of the 12 Cranial Nerves - Merck Veterinary Manual
Image: Functions of the 12 Cranial Nerves - Merck Veterinary Manual Head and Neck Anatomy: Part III - Cranial Nerves | Continuing Education Course | dentalcare.com
Head and Neck Anatomy: Part III - Cranial Nerves | Continuing Education Course | dentalcare.com Cranial nerve nuclei | Radiology Reference Article | Radiopaedia.org
Cranial nerve nuclei | Radiology Reference Article | Radiopaedia.org Implanted Sacral Nerve Stimulator,Implanted Cranial Nerve Stimulator Suppliers & Manufacturers
Implanted Sacral Nerve Stimulator,Implanted Cranial Nerve Stimulator Suppliers & Manufacturers TIFFANY AND TANYA - CRANIAL NERVE SONG JINGLE BELL ROCK CHORDS by Misc Originals @ Ultimate-Guitar.Com
TIFFANY AND TANYA - CRANIAL NERVE SONG JINGLE BELL ROCK CHORDS by Misc Originals @ Ultimate-Guitar.Com Cranial Nerves - Nerves - Anatomy - Picmonic for Nursing RN
Cranial Nerves - Nerves - Anatomy - Picmonic for Nursing RN Cranial Nerves
Cranial Nerves cranial nerves introduction
cranial nerves introduction Metaphysical Energy Therapy in the Treatment of Cranial Nerve Palsies with Special Reference to Bell's Palsy
Metaphysical Energy Therapy in the Treatment of Cranial Nerve Palsies with Special Reference to Bell's Palsy Testing Cranial Nerves - VetSci
Testing Cranial Nerves - VetSci The Lower Cranial Nerves
The Lower Cranial Nerves Cranial Nerves - Word Search Labs
Cranial Nerves - Word Search Labs