Cerebellar Neoplasms
Neuroma, Acoustic
Facial Nerve Diseases
Epidermal Cyst
Cranial Nerve Neoplasms
Meningioma
Trigeminal Neuralgia
Ear Neoplasms
Vestibulocochlear Nerve Diseases
Hemifacial Spasm
Petrous Bone
Cerebellar Diseases
Meningeal Neoplasms
Choroid Plexus Neoplasms
Neurilemmoma
Vestibulocochlear Nerve
Cranial Fossa, Posterior
Cochlear Aqueduct
Tinnitus
Facial Muscles
Spasm
Ganglioglioma
Facial Nerve
Magnetic Resonance Imaging
Endolymphatic Sac
Trigeminal Nerve
Nerve Compression Syndromes
Papilloma, Choroid Plexus
Facial Paralysis
Lipoma
Neurothekeoma
Ear, Inner
Tomography, X-Ray Computed
Temporal Bone
Sarcoma, Myeloid
Radiosurgery
Treatment Outcome
Contralateral deafness following unilateral suboccipital brain tumor surgery in a patient with large vestibular aqueduct--case report. (1/142)
A 68-year-old female developed contralateral deafness following extirpation of a left cerebellopontine angle epidermoid cyst. Computed tomography showed that large vestibular aqueduct was present. This unusual complication may have been caused by an abrupt pressure change after cerebrospinal fluid release, which was transmitted through the large vestibular aqueduct and resulted in cochlear damage. (+info)Clinical features and outcomes in patients with non-acoustic cerebellopontine angle tumours. (2/142)
OBJECTIVES: Non-acoustic tumours of the cerebellopontine angle differ from vestibular schwannomas in their prevalence, clinical features, operative management, and surgical outcome. These features were studied in patients presenting to the regional neuro-otological unit. METHODS: A retrospective analysis of clinical notes identified 42 patients with non-acoustic tumours of the cerebellopontine angle. Data were extracted regarding presenting clinical features, histopathological data after surgical resection, surgical morbidity and mortality, and clinical outcome (mean 32 months follow up). RESULTS: The study group comprised 25 meningiomas (60%), 12 epidermoid cysts/cholesteatomata (28%), and five other tumours. In patients with meningiomas, symptoms differed considerably from patients presenting with vestibular schwannomas. Cerebellar signs were present in 52% and hearing loss in only 68%. Twenty per cent of patients had hydrocephalus at the time of diagnosis. After surgical resection, normal facial nerve function was preserved in 75% of cases. In the epidermoid group, fifth, seventh, and eighth nerve deficits were present in 42%, 33%, and 66% respectively. There were no new postoperative facial palsies. There were two recurrences (17%) requiring reoperation. Overall, there were two perioperative deaths from pneumonia and meningitis. CONCLUSIONS: Patients with non-acoustic lesions of the cerebellopontine angle often present with different symptoms and signs from those found in patients with schwannomas. Hearing loss is less prevalent and cerebellar signs and facial paresis are more common as presenting features. Hydrocephalus is often present in patients presenting with cerebellopontine angle meningiomas. Non-acoustic tumours can usually be resected with facial nerve preservation. (+info)Choroid plexus papilloma of cerebellopontine angle with extension to foramen magnum. (3/142)
A case of choroid plexus papilloma resembling meningioma of cerebellopontine (CP) angle with its extension to foramen magnum is presented. Occurrence of this tumour in CP angle is very rare. Its extension towards foramen magnum is further rare. It was a real diagnostic enigma preoperatively as the tumour was resembling meningioma upto some extent on radiological study. Retromastoid craniectomy with microsurgical excision of tumour and its extension was achieved in toto. Tumour was attached to few rootlets of lower cranial nerves which were preserved. Attachment of the tumour with lower cranial nerves again caused diagnostic confusion with neurofibroma intraoperatively. (+info)High-resolution MR cisternography of the cerebellopontine angle: 2D versus 3D fast spin-echo sequences. (4/142)
BACKGROUND AND PURPOSE: The clinical usefulness of MR cisternography of the cerebellopontine angle, applying 2D or 3D fast spin-echo sequences, has been reported recently. Our purpose was to investigate the cause of signal loss in CSF in the prepontine or cerebellopontine angle cistern on 2D FSE MR images and to compare the cisternographic effects of 2D and 3D FSE sequences. METHODS: Preliminary experiments were performed in four volunteers to assess the causes of signal loss. Initially, using a 2D cardiac-gated cine phase-contrast method with a velocity encoding value of 6 cm/s, we measured the velocity and flow pattern of CSF. Comparisons were made to assess the effects of intravoxel dephasing, amplitude of the section-selecting gradient, echo time (TE), and section thickness. Four healthy subjects and 13 patients with ear symptoms were examined, and multisection 3-mm-thick 2D images and 30-mm-slab, 1-mm-section 3D images were compared qualitatively and quantitatively. Then, 3D MR cisternography was performed in 400 patients with ear symptoms, and qualitative evaluation was performed. RESULTS: In volunteers, the average peak velocity of CSF was 1.2 cm/s. With TE = 250, CSF may move an average of 3 mm, and can be washed out of a 3-mm-thick 2D section volume. The CSF signal relative to that of a water phantom decreased gradually as TE increased on single-section 3-mm-thick 2D images. The CSF signal relative to that of the water phantom increased gradually as section thickness increased. No significant differences were noted in intravoxel dephasing and amplitude of the section-selecting gradient. The contrast-to-noise ratio (CNR) between CSF and the cerebellar peduncle, and the visibility of the cranial nerves and vertebrobasilar artery were significantly improved on 3D images in 17 subjects. In images from 400 patients, no significant signal loss in the cistern was observed using 3D FSE. CONCLUSION: CSF signal loss in thin-section 2D MR cisternography is mainly attributable to the wash-out phenomenon. 3D acquisition can reduce this phenomenon and provide thinner sections. The scan time for 3D acquisition is not excessive when a long echo train length and half-Fourier imaging are used. MR cisternography should be performed using a 3D acquisition. (+info)High-resolution MR cisternography of the cerebellopontine angle, obtained with a three-dimensional fast asymmetric spin-echo sequence in a 0.35-T open MR imaging unit. (5/142)
High-resolution MR cisternography performed with 3D fast asymmetric spin-echo imaging (3D fast spin-echo with an ultra-long echo train length and asymmetric Fourier imaging) was optimized in a 0.35-T open MR imaging unit. The 0.35- and 1.5-T images of the two volunteers and three patients with acoustic schwannomas were then compared. The optimal parameters for images obtained by 3D fast asymmetric spin-echo imaging at 0.35 T were as follows: field of view, 15 cm; matrix, 256 x 256 x 40; section thickness, 1 mm; echo train length, 76; and imaging time, 10 minutes 44 seconds. Scans obtained from both normal volunteers showed the facial, cochlear, and superior and inferior vestibular nerves separately in the internal auditory canal on both 0.35- and 1.5-T images. All three acoustic schwannomas were depicted on both 0.35- and 1.5-T images. Screening for disease at the cerebellopontine angle and in the internal auditory canal, without the administration of contrast material on a low-field open MR imaging unit and within a clinically acceptable imaging time, may be possible. Further controlled prospective studies are required, however, before implementation on a wide basis. If proved effective, this may be of particular value for reducing healthcare costs and for imaging claustrophobic and pediatric patients in an open system. (+info)Posterior fossa surgery in the sitting position in a pregnant patient with cerebellopontine angle meningioma. (6/142)
Primary brain tumours and pregnancy rarely occur together; meningioma and pregnancy is rarer still. We describe a 30-yr-old woman in the 25th week of pregnancy who underwent surgery in the sitting position for a large cerebellopontine angle meningioma that was compressing and displacing the pons and medulla. The surgical procedure and postoperative period were uneventful. This case demonstrates that when absolutely necessary, anaesthesia and neurosurgery for posterior fossa lesions can be successful during the second trimester of pregnancy. Furthermore, if indicated and if the operating team is experienced, the operation can be performed safely with the patient in the classical sitting position. It is emphasized that continuous and attentive monitoring of the mother and fetus are essential. (+info)Magnetic resonance imaging artifact following acoustic neurofibroma surgery--case report. (7/142)
Metallic artifacts in magnetic resonance (MR) imaging occur mostly in patients who have received an implant at surgery. Similar artifacts are now increasingly recognized in patients in whom high-speed drills have been used. A 15-year-old male with neurofibromatosis 2 had undergone excision of acoustic neurofibroma on the left 1.5 years prior to the present admission. MR imaging to evaluate the acoustic neurofibroma on the right showed a metallic artifact at the site of the previous surgery. Computed tomography did not show any evidence of metal debris. The artifact was probably caused by metallic dust or debris from a high-speed drill during the first surgery. We suggest that care should be taken to prevent deposition of such debris in the operative field to prevent this complication. (+info)Malignant spread of haemangioblastoma: report on two cases. (8/142)
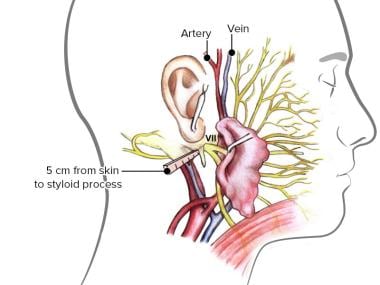
Two cases are described in which, after successful removal of a cerebellar haemangioblastoma followed by several years of freedom from symptoms, there developed a progressive spinal cord compression, leading to death. At necropsy the spinal cords in both cases and the brainstem in one case, were irregularly plastered with haemangioblastoma. Although there was no doubt that malignant spread had occurred from one or more primary tumours, the histology of the tumour tissue was in no way different from that of conventional haemangioblastoma. (+info)The cerebellopontine angle (CPA) is a narrow space located at the junction of the brainstem and the cerebellum, where the pons and cerebellum meet. This region is filled with several important nerves, blood vessels, and membranous coverings called meninges. The CPA is a common site for various neurological disorders because it contains critical structures such as:
1. Cerebellum: A part of the brain responsible for coordinating muscle movements, maintaining balance, and fine-tuning motor skills.
2. Pons: A portion of the brainstem that plays a role in several vital functions, including facial movements, taste sensation, sleep regulation, and respiration.
3. Cranial nerves: The CPA is home to the following cranial nerves:
* Vestibulocochlear nerve (CN VIII): This nerve has two components - cochlear and vestibular. The cochlear part is responsible for hearing, while the vestibular part contributes to balance and eye movement.
* Facial nerve (CN VII): This nerve controls facial expressions, taste sensation in the anterior two-thirds of the tongue, salivary gland function, and lacrimation (tear production).
4. Blood vessels: The CPA contains critical blood vessels like the anterior inferior cerebellar artery (AICA), which supplies blood to various parts of the brainstem, cerebellum, and cranial nerves.
5. Meninges: These are protective membranes surrounding the brain and spinal cord. In the CPA, the meninges include the dura mater, arachnoid mater, and pia mater.
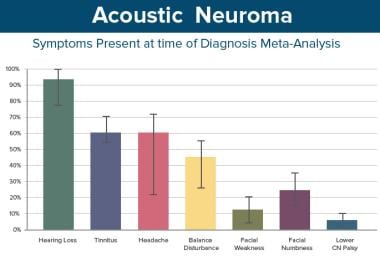
Disorders that can affect the structures in the cerebellopontine angle include acoustic neuromas (vestibular schwannomas), meningiomas, epidermoids, and arteriovenous malformations. These conditions may cause symptoms such as hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), facial weakness or numbness, difficulty swallowing, and imbalance.
Cerebellar neoplasms refer to abnormal growths or tumors that develop in the cerebellum, which is the part of the brain responsible for coordinating muscle movements and maintaining balance. These tumors can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells within the cerebellum.
The most common type of cerebellar neoplasm is a medulloblastoma, which arises from primitive nerve cells in the cerebellum. Other types of cerebellar neoplasms include astrocytomas, ependymomas, and brain stem gliomas. Symptoms of cerebellar neoplasms may include headaches, vomiting, unsteady gait, coordination problems, and visual disturbances. Treatment options depend on the type, size, and location of the tumor, as well as the patient's overall health and age. Treatment may involve surgery, radiation therapy, chemotherapy, or a combination of these approaches.
An acoustic neuroma, also known as vestibular schwannoma, is not actually a neuroma but rather a benign (noncancerous) tumor that develops on the vestibular nerve. This nerve is one of the two nerves that transmit sound and balance information from the inner ear to the brain. The tumor arises from an overproduction of Schwann cells, which normally provide a protective covering for the nerve fibers. As the tumor grows, it can press against the hearing and balance nerves, causing symptoms such as hearing loss, ringing in the ear (tinnitus), unsteadiness, and disequilibrium. In some cases, acoustic neuromas can become quite large and cause additional symptoms by pressing on nearby cranial nerves. Treatment options include observation, radiation therapy, or surgical removal of the tumor.
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
An epidermal cyst is a common benign skin condition characterized by the growth of a sac-like structure filled with keratin, a protein found in the outermost layer of the skin (epidermis). These cysts typically appear as round, firm bumps just under the surface of the skin, often on the face, neck, trunk, or scalp. They can vary in size from a few millimeters to several centimeters in diameter.
Epidermal cysts usually develop as a result of the accumulation of dead skin cells that become trapped within a hair follicle or a pilosebaceous unit (a structure that contains a hair follicle and an oil gland). The keratin produced by the skin cells then collects inside the sac, causing it to expand gradually.
These cysts are generally slow-growing, painless, and rarely cause any symptoms. However, they may become infected or inflamed, leading to redness, tenderness, pain, or pus formation. In such cases, medical attention might be necessary to drain the cyst or administer antibiotics to treat the infection.
Epidermal cysts can be removed surgically if they cause cosmetic concerns or become frequently infected. The procedure typically involves making an incision in the skin and removing the entire sac along with its contents to prevent recurrence.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
A meningioma is a type of slow-growing tumor that forms on the membranes (meninges) surrounding the brain and spinal cord. It's usually benign, meaning it doesn't spread to other parts of the body, but it can still cause serious problems if it grows and presses on nearby tissues.
Meningiomas most commonly occur in adults, and are more common in women than men. They can cause various symptoms depending on their location and size, including headaches, seizures, vision or hearing problems, memory loss, and changes in personality or behavior. In some cases, they may not cause any symptoms at all and are discovered only during imaging tests for other conditions.
Treatment options for meningiomas include monitoring with regular imaging scans, surgery to remove the tumor, and radiation therapy to shrink or kill the tumor cells. The best treatment approach depends on factors such as the size and location of the tumor, the patient's age and overall health, and their personal preferences.
Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which is one of the largest nerves in the head. It carries sensations from the face to the brain.
Medically, trigeminal neuralgia is defined as a neuropathic disorder characterized by episodes of intense, stabbing, electric shock-like pain in the areas of the face supplied by the trigeminal nerve (the ophthalmic, maxillary, and mandibular divisions). The pain can be triggered by simple activities such as talking, eating, brushing teeth, or even touching the face lightly.
The condition is more common in women over 50, but it can occur at any age and in either gender. While the exact cause of trigeminal neuralgia is not always known, it can sometimes be related to pressure on the trigeminal nerve from a nearby blood vessel or other causes such as multiple sclerosis. Treatment typically involves medications, surgery, or a combination of both.
Ear neoplasms refer to abnormal growths or tumors that occur in the ear. These growths can be benign (non-cancerous) or malignant (cancerous) and can affect any part of the ear, including the outer ear, middle ear, inner ear, and the ear canal.
Benign ear neoplasms are typically slow-growing and do not spread to other parts of the body. Examples include exostoses, osteomas, and ceruminous adenomas. These types of growths are usually removed surgically for cosmetic reasons or if they cause discomfort or hearing problems.
Malignant ear neoplasms, on the other hand, can be aggressive and may spread to other parts of the body. Examples include squamous cell carcinoma, basal cell carcinoma, and adenoid cystic carcinoma. These types of tumors often require more extensive treatment, such as surgery, radiation therapy, and chemotherapy.
It is important to note that any new growth or change in the ear should be evaluated by a healthcare professional to determine the nature of the growth and develop an appropriate treatment plan.
The vestibulocochlear nerve, also known as the 8th cranial nerve, is responsible for transmitting sound and balance information from the inner ear to the brain. Vestibulocochlear nerve diseases refer to conditions that affect this nerve and can result in hearing loss, vertigo, and balance problems.
These diseases can be caused by various factors, including genetics, infection, trauma, tumors, or degeneration. Some examples of vestibulocochlear nerve diseases include:
1. Vestibular neuritis: an inner ear infection that causes severe vertigo, nausea, and balance problems.
2. Labyrinthitis: an inner ear infection that affects both the vestibular and cochlear nerves, causing vertigo, hearing loss, and tinnitus.
3. Acoustic neuroma: a benign tumor that grows on the vestibulocochlear nerve, causing hearing loss, tinnitus, and balance problems.
4. Meniere's disease: a inner ear disorder that causes vertigo, hearing loss, tinnitus, and a feeling of fullness in the ear.
5. Ototoxicity: damage to the inner ear caused by certain medications or chemicals that can result in hearing loss and balance problems.
6. Vestibular migraine: a type of migraine that is associated with vertigo, dizziness, and balance problems.
Treatment for vestibulocochlear nerve diseases varies depending on the specific condition and its severity. It may include medication, physical therapy, surgery, or a combination of these approaches.
Hemifacial spasm is a neuromuscular disorder characterized by involuntary, irregular contractions or twitching of the muscles on one side of the face. These spasms typically begin around the eye and may progress to involve the muscles of the lower face, including those around the mouth.
The primary cause of hemifacial spasm is pressure on or irritation of the facial nerve (cranial nerve VII) as it exits the brainstem, often due to a blood vessel or tumor. This pressure can lead to abnormal electrical signals in the facial nerve, resulting in uncontrolled muscle contractions.
In some cases, hemifacial spasm may be associated with other conditions such as multiple sclerosis or Bell's palsy. Treatment options for hemifacial spasm include medications to help relax the muscles, botulinum toxin (Botox) injections to paralyze the affected muscles temporarily, and, in rare cases, surgical intervention to relieve pressure on the facial nerve.
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
Cerebellar diseases refer to a group of medical conditions that affect the cerebellum, which is the part of the brain located at the back of the head, below the occipital lobe and above the brainstem. The cerebellum plays a crucial role in motor control, coordination, balance, and some cognitive functions.
Cerebellar diseases can be caused by various factors, including genetics, infections, tumors, stroke, trauma, or degenerative processes. These conditions can result in a wide range of symptoms, such as:
1. Ataxia: Loss of coordination and unsteady gait
2. Dysmetria: Inability to judge distance and force while performing movements
3. Intention tremors: Shaking or trembling that worsens during purposeful movements
4. Nystagmus: Rapid, involuntary eye movement
5. Dysarthria: Speech difficulty due to muscle weakness or incoordination
6. Hypotonia: Decreased muscle tone
7. Titubation: Rhythmic, involuntary oscillations of the head and neck
8. Cognitive impairment: Problems with memory, attention, and executive functions
Some examples of cerebellar diseases include:
1. Ataxia-telangiectasia
2. Friedrich's ataxia
3. Multiple system atrophy (MSA)
4. Spinocerebellar ataxias (SCAs)
5. Cerebellar tumors, such as medulloblastomas or astrocytomas
6. Infarctions or hemorrhages in the cerebellum due to stroke or trauma
7. Infections, such as viral encephalitis or bacterial meningitis
8. Autoimmune disorders, like multiple sclerosis (MS) or paraneoplastic syndromes
9. Metabolic disorders, such as Wilson's disease or phenylketonuria (PKU)
10. Chronic alcoholism and withdrawal
Treatment for cerebellar diseases depends on the underlying cause and may involve medications, physical therapy, surgery, or supportive care to manage symptoms and improve quality of life.
Meningeal neoplasms, also known as malignant meningitis or leptomeningeal carcinomatosis, refer to cancerous tumors that originate in the meninges, which are the membranes covering the brain and spinal cord. These tumors can arise primarily from the meningeal cells themselves, although they more commonly result from the spread (metastasis) of cancer cells from other parts of the body, such as breast, lung, or melanoma.
Meningeal neoplasms can cause a variety of symptoms, including headaches, nausea and vomiting, mental status changes, seizures, and focal neurological deficits. Diagnosis typically involves imaging studies (such as MRI) and analysis of cerebrospinal fluid obtained through a spinal tap. Treatment options may include radiation therapy, chemotherapy, or surgery, depending on the type and extent of the tumor. The prognosis for patients with meningeal neoplasms is generally poor, with a median survival time of several months to a year.
Choroid plexus neoplasms are rare types of brain tumors that arise from the choroid plexus, which are clusters of blood vessels in the ventricles (fluid-filled spaces) of the brain. These tumors can be benign (choroid plexus papilloma) or malignant (choroid plexus carcinoma). Choroid plexus neoplasms most commonly occur in children under the age of 2, but they can also affect adults. Symptoms may include increased head circumference, hydrocephalus (fluid buildup in the brain), vomiting, and developmental delays. Treatment typically involves surgical removal of the tumor, followed by radiation therapy or chemotherapy for malignant tumors.
A neurilemmoma, also known as schwannoma or peripheral nerve sheath tumor, is a benign, slow-growing tumor that arises from the Schwann cells, which produce the myelin sheath that surrounds and insulates peripheral nerves. These tumors can occur anywhere along the course of a peripheral nerve, but they most commonly affect the acoustic nerve (vestibulocochlear nerve), leading to a type of tumor called vestibular schwannoma or acoustic neuroma. Neurilemmomas are typically encapsulated and do not invade the surrounding tissue, although larger ones may cause pressure-related symptoms due to compression of nearby structures. Rarely, these tumors can undergo malignant transformation, leading to a condition called malignant peripheral nerve sheath tumor or neurofibrosarcoma.
I'm sorry for any confusion, but "Financial Audit" is not a medical term. It belongs to the field of accounting and finance. A financial audit is an independent examination of an organization's financial records, statements, and accounting practices to ensure that they are accurate, complete, and in accordance with applicable laws and regulations. This process is conducted by professional auditors who are unbiased and independent from the organization being audited.
The vestibulocochlear nerve, also known as the auditory-vestibular nerve or cranial nerve VIII, is a paired peripheral nerve that transmits sensory information from the inner ear to the brain. It has two distinct parts: the cochlear part and the vestibular part.
The cochlear part is responsible for hearing and transmits sound signals from the cochlea to the brain. The vestibular part, on the other hand, is responsible for maintaining balance and spatial orientation by transmitting information about head movement and position from the vestibular apparatus (utricle, saccule, and semicircular canals) in the inner ear to the brain.
Together, these two parts of the vestibulocochlear nerve play a crucial role in our ability to hear and maintain balance. Damage to this nerve can result in hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), or balance problems.
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
The cochlear aqueduct is a small canal that runs from the inner ear to the brain. It contains a fluid called perilymph, which helps to protect and cushion the structures of the inner ear. The cochlear aqueduct also serves as a passageway for the endolymphatic duct and sac, which are involved in the regulation of the inner ear's fluid balance.
Anomalies or abnormalities of the cochlear aqueduct can lead to hearing problems, balance disorders, and other symptoms. For example, a large or dilated cochlear aqueduct may be associated with an increased risk of meningitis, a serious infection of the membranes surrounding the brain and spinal cord. In some cases, surgical closure of the cochlear aqueduct may be necessary to prevent recurrent meningitis or other complications.
Tinnitus is the perception of ringing or other sounds in the ears or head when no external sound is present. It can be described as a sensation of hearing sound even when no actual noise is present. The sounds perceived can vary widely, from a whistling, buzzing, hissing, swooshing, to a pulsating sound, and can be soft or loud.
Tinnitus is not a disease itself but a symptom that can result from a wide range of underlying causes, such as hearing loss, exposure to loud noises, ear infections, earwax blockage, head or neck injuries, circulatory system disorders, certain medications, and age-related hearing loss.
Tinnitus can be temporary or chronic, and it may affect one or both ears. While tinnitus is not usually a sign of a serious medical condition, it can significantly impact quality of life and interfere with daily activities, sleep, and concentration.
Facial muscles, also known as facial nerves or cranial nerve VII, are a group of muscles responsible for various expressions and movements of the face. These muscles include:
1. Orbicularis oculi: muscle that closes the eyelid and raises the upper eyelid
2. Corrugator supercilii: muscle that pulls the eyebrows down and inward, forming wrinkles on the forehead
3. Frontalis: muscle that raises the eyebrows and forms horizontal wrinkles on the forehead
4. Procerus: muscle that pulls the medial ends of the eyebrows downward, forming vertical wrinkles between the eyebrows
5. Nasalis: muscle that compresses or dilates the nostrils
6. Depressor septi: muscle that pulls down the tip of the nose
7. Levator labii superioris alaeque nasi: muscle that raises the upper lip and flares the nostrils
8. Levator labii superioris: muscle that raises the upper lip
9. Zygomaticus major: muscle that raises the corner of the mouth, producing a smile
10. Zygomaticus minor: muscle that raises the nasolabial fold and corner of the mouth
11. Risorius: muscle that pulls the angle of the mouth laterally, producing a smile
12. Depressor anguli oris: muscle that pulls down the angle of the mouth
13. Mentalis: muscle that raises the lower lip and forms wrinkles on the chin
14. Buccinator: muscle that retracts the cheek and helps with chewing
15. Platysma: muscle that depresses the corner of the mouth and wrinkles the skin of the neck.
These muscles are innervated by the facial nerve, which arises from the brainstem and exits the skull through the stylomastoid foramen. Damage to the facial nerve can result in facial paralysis or weakness on one or both sides of the face.
A spasm is a sudden, involuntary contraction or tightening of a muscle, group of muscles, or a hollow organ such as the ureter or bronchi. Spasms can occur as a result of various factors including muscle fatigue, injury, irritation, or abnormal nerve activity. They can cause pain and discomfort, and in some cases, interfere with normal bodily functions. For example, a spasm in the bronchi can cause difficulty breathing, while a spasm in the ureter can cause severe pain and may lead to a kidney stone blockage. The treatment for spasms depends on the underlying cause and may include medication, physical therapy, or lifestyle changes.
Ganglioglioma is a rare, typically slow-growing tumor that occurs in the brain or spinal cord. It is composed of both neuronal (ganglion cell) and glial elements. These tumors most commonly occur in the temporal lobe of the brain and are usually found in children and young adults.
Gangliogliomas can be benign or malignant, with the majority being low-grade (benign). Symptoms vary depending on the location of the tumor but may include seizures, headaches, changes in behavior or cognition, and motor weakness or paralysis. Treatment typically involves surgical removal of the tumor, and in some cases, radiation therapy or chemotherapy may be recommended.
It's important to note that while I strive to provide accurate information, my responses should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider for any medical concerns.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
The endolymphatic sac is a small, fluid-filled structure that is part of the inner ear. It is located near the vestibular aqueduct and is responsible for maintaining the balance of fluids in the inner ear. The endolymphatic sac also plays a role in the resorption of endolymph, which is the fluid that fills the membranous labyrinth of the inner ear. Disorders of the endolymphatic sac can lead to conditions such as Meniere's disease, which is characterized by vertigo, hearing loss, and tinnitus.
The trigeminal nerve, also known as the fifth cranial nerve or CNV, is a paired nerve that carries both sensory and motor information. It has three major branches: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic branch provides sensation to the forehead, eyes, and upper portion of the nose; the maxillary branch supplies sensation to the lower eyelid, cheek, nasal cavity, and upper lip; and the mandibular branch is responsible for sensation in the lower lip, chin, and parts of the oral cavity, as well as motor function to the muscles involved in chewing. The trigeminal nerve plays a crucial role in sensations of touch, pain, temperature, and pressure in the face and mouth, and it also contributes to biting, chewing, and swallowing functions.
Nerve compression syndromes refer to a group of conditions characterized by the pressure or irritation of a peripheral nerve, causing various symptoms such as pain, numbness, tingling, and weakness in the affected area. This compression can occur due to several reasons, including injury, repetitive motion, bone spurs, tumors, or swelling. Common examples of nerve compression syndromes include carpal tunnel syndrome, cubital tunnel syndrome, radial nerve compression, and ulnar nerve entrapment at the wrist or elbow. Treatment options may include physical therapy, splinting, medications, injections, or surgery, depending on the severity and underlying cause of the condition.
A choroid plexus papilloma is a rare, benign (non-cancerous) tumor that develops in the choroid plexus, which are clusters of blood vessels and specialized cells in the ventricles of the brain. These tumors can occur at any age but are more common in children under the age of 10.
Choroid plexus papillomas arise from the ependymal cells that line the ventricular system and produce cerebrospinal fluid (CSF). The tumor grows slowly and tends to block the flow of CSF, leading to increased intracranial pressure and symptoms such as headaches, vomiting, irritability, and developmental delays in children.
The medical definition of choroid plexus papilloma is: "A benign, slow-growing tumor that arises from the ependymal cells of the choroid plexus in the ventricles of the brain. The tumor can obstruct the flow of cerebrospinal fluid and cause increased intracranial pressure."
It is important to note that while choroid plexus papillomas are generally benign, they can still cause significant symptoms due to their location in the brain and the obstruction of CSF flow. Treatment typically involves surgical removal of the tumor, followed by radiation therapy or chemotherapy if necessary.
Facial paralysis is a loss of facial movement due to damage or dysfunction of the facial nerve (cranial nerve VII). This nerve controls the muscles involved in facial expressions, such as smiling, frowning, and closing the eyes. Damage to one side of the facial nerve can cause weakness or paralysis on that side of the face.
Facial paralysis can result from various conditions, including:
1. Bell's palsy - an idiopathic (unknown cause) inflammation of the facial nerve
2. Trauma - skull fractures, facial injuries, or surgical trauma to the facial nerve
3. Infections - Lyme disease, herpes zoster (shingles), HIV/AIDS, or bacterial infections like meningitis
4. Tumors - benign or malignant growths that compress or invade the facial nerve
5. Stroke - damage to the brainstem where the facial nerve originates
6. Congenital conditions - some people are born with facial paralysis due to genetic factors or birth trauma
Symptoms of facial paralysis may include:
* Inability to move one or more parts of the face, such as the eyebrows, eyelids, mouth, or cheeks
* Drooping of the affected side of the face
* Difficulty closing the eye on the affected side
* Changes in saliva and tear production
* Altered sense of taste
* Pain around the ear or jaw
* Speech difficulties due to weakened facial muscles
Treatment for facial paralysis depends on the underlying cause. In some cases, such as Bell's palsy, spontaneous recovery may occur within a few weeks to months. However, physical therapy, medications, and surgical interventions might be necessary in other situations to improve function and minimize complications.
A lipoma is a common, benign (non-cancerous) soft tissue growth. It is composed of adipose or fatty tissue and typically found just beneath the skin, but they can also occur deeper within the body. Lipomas are usually round, moveable, and painless, although they may cause discomfort if they grow large enough to put pressure on nearby nerves or if they're located in a sensitive area. They generally grow slowly over time. Surgical removal is an option if the lipoma becomes bothersome or grows significantly in size. It's important to note that while lipomas are typically harmless, any new lumps or bumps should be evaluated by a healthcare professional to confirm the diagnosis and rule out other more serious conditions.
A "reflex, acoustic" is not a standard medical term. However, it seems like you might be looking for a definition of the "acoustic reflex." The acoustic reflex is an involuntary muscle contraction that occurs in the middle ear in response to loud sounds. This reflex helps protect the inner ear from damage caused by high-intensity sounds.
When a loud sound reaches the ear, it stimulates the stapedius muscle in the middle ear, which then contracts and causes the stapes bone (one of the three bones in the middle ear) to become stiffer. This stiffening reduces the amount of sound that is transmitted to the inner ear, thus protecting it from potential harm.
The acoustic reflex can be measured using a device called an impedance audiometer, which measures changes in the pressure within the ear canal caused by muscle contraction during the reflex. This measurement provides valuable information for diagnosing and monitoring various hearing and balance disorders.
Neurothekeoma is a rare, benign cutaneous neoplasm (tumor) that originates from the nerve sheath. It typically presents as a solitary, slow-growing, well-circumscribed nodule or mass in the skin. Neurothekeomas are more commonly found in young adults and children, with a slight female predominance.
Histologically (under the microscope), neurothekeomas are characterized by the presence of epithelioid cells arranged in lobules or nests, separated by fibrous septa. The tumor cells may contain eosinophilic (pink) cytoplasm and may show nuclear atypia, but mitotic figures are usually absent or rare. Immunohistochemical staining may reveal positivity for S-100 protein, neuron-specific enolase, and/or smooth muscle actin.
Neurothekeomas have been classified into two types: classic neurothekeoma and cellular neurothekeoma. Classic neurothekeomas are more common and typically show a biphasic pattern with both epithelioid and spindle cells, while cellular neurothekeomas are less common and composed predominantly of epithelioid cells.
The treatment of choice for neurothekeoma is surgical excision with clear margins. Recurrence is uncommon but may occur if the tumor is not completely removed. Malignant transformation is extremely rare, but possible.
The inner ear is the innermost part of the ear that contains the sensory organs for hearing and balance. It consists of a complex system of fluid-filled tubes and sacs called the vestibular system, which is responsible for maintaining balance and spatial orientation, and the cochlea, a spiral-shaped organ that converts sound vibrations into electrical signals that are sent to the brain.
The inner ear is located deep within the temporal bone of the skull and is protected by a bony labyrinth. The vestibular system includes the semicircular canals, which detect rotational movements of the head, and the otolith organs (the saccule and utricle), which detect linear acceleration and gravity.
Damage to the inner ear can result in hearing loss, tinnitus (ringing in the ears), vertigo (a spinning sensation), and balance problems.
A craniotomy is a surgical procedure where a bone flap is temporarily removed from the skull to access the brain. This procedure is typically performed to treat various neurological conditions, such as brain tumors, aneurysms, arteriovenous malformations, or traumatic brain injuries. After the underlying brain condition is addressed, the bone flap is usually replaced and secured back in place with plates and screws. The purpose of a craniotomy is to provide access to the brain for diagnostic or therapeutic interventions while minimizing potential damage to surrounding tissues.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Neurosurgical procedures are operations that are performed on the brain, spinal cord, and peripheral nerves. These procedures are typically carried out by neurosurgeons, who are medical doctors with specialized training in the diagnosis and treatment of disorders of the nervous system. Neurosurgical procedures can be used to treat a wide range of conditions, including traumatic injuries, tumors, aneurysms, vascular malformations, infections, degenerative diseases, and congenital abnormalities.
Some common types of neurosurgical procedures include:
* Craniotomy: A procedure in which a bone flap is temporarily removed from the skull to gain access to the brain. This type of procedure may be performed to remove a tumor, repair a blood vessel, or relieve pressure on the brain.
* Spinal fusion: A procedure in which two or more vertebrae in the spine are fused together using bone grafts and metal hardware. This is often done to stabilize the spine and alleviate pain caused by degenerative conditions or spinal deformities.
* Microvascular decompression: A procedure in which a blood vessel that is causing pressure on a nerve is repositioned or removed. This type of procedure is often used to treat trigeminal neuralgia, a condition that causes severe facial pain.
* Deep brain stimulation: A procedure in which electrodes are implanted in specific areas of the brain and connected to a battery-operated device called a neurostimulator. The neurostimulator sends electrical impulses to the brain to help alleviate symptoms of movement disorders such as Parkinson's disease or dystonia.
* Stereotactic radiosurgery: A non-invasive procedure that uses focused beams of radiation to treat tumors, vascular malformations, and other abnormalities in the brain or spine. This type of procedure is often used for patients who are not good candidates for traditional surgery due to age, health status, or location of the lesion.
Neurosurgical procedures can be complex and require a high degree of skill and expertise. Patients considering neurosurgical treatment should consult with a qualified neurosurgeon to discuss their options and determine the best course of action for their individual situation.
The temporal bone is a paired bone that is located on each side of the skull, forming part of the lateral and inferior walls of the cranial cavity. It is one of the most complex bones in the human body and has several important structures associated with it. The main functions of the temporal bone include protecting the middle and inner ear, providing attachment for various muscles of the head and neck, and forming part of the base of the skull.
The temporal bone is divided into several parts, including the squamous part, the petrous part, the tympanic part, and the styloid process. The squamous part forms the lateral portion of the temporal bone and articulates with the parietal bone. The petrous part is the most medial and superior portion of the temporal bone and contains the inner ear and the semicircular canals. The tympanic part forms the lower and anterior portions of the temporal bone and includes the external auditory meatus or ear canal. The styloid process is a long, slender projection that extends downward from the inferior aspect of the temporal bone and serves as an attachment site for various muscles and ligaments.
The temporal bone plays a crucial role in hearing and balance, as it contains the structures of the middle and inner ear, including the oval window, round window, cochlea, vestibule, and semicircular canals. The stapes bone, one of the three bones in the middle ear, is entirely encased within the petrous portion of the temporal bone. Additionally, the temporal bone contains important structures for facial expression and sensation, including the facial nerve, which exits the skull through the stylomastoid foramen, a small opening in the temporal bone.
A myeloid sarcoma is a rare type of cancer that can develop in various parts of the body. It is also known as a granulocytic sarcoma or chloroma.
Myeloid sarcomas occur when immature white blood cells, called myeloblasts, accumulate and form a tumor in an extramedullary site, which means outside of the bone marrow. These tumors can develop in various organs and tissues, such as the skin, soft tissue, bones, lymph nodes, or gastrointestinal tract.
Myeloid sarcomas are often associated with acute myeloid leukemia (AML), a type of blood cancer that affects the bone marrow's ability to produce healthy blood cells. However, they can also occur in individuals who have previously been treated for AML or other myeloid disorders, or rarely, in those without a known history of these conditions.
The diagnosis of myeloid sarcoma typically involves a biopsy of the affected tissue, followed by microscopic examination and immunohistochemical staining to confirm the presence of myeloblasts and other specific markers. Treatment options for myeloid sarcoma depend on several factors, including the patient's overall health, the extent and location of the disease, and whether it is associated with AML or another myeloid disorder. Treatment may include chemotherapy, radiation therapy, targeted therapy, or stem cell transplantation.
Radiosurgery is a non-invasive surgical procedure that uses precisely focused beams of radiation to treat various medical conditions, primarily in the field of neurosurgery and oncology. It allows for the destruction of targeted tissue while minimizing damage to surrounding healthy structures. Unlike traditional surgery, radiosurgery does not require any incisions, as it delivers radiation through the skin to reach the intended target.
The term "stereotactic" is often associated with radiosurgery, which refers to the use of a three-dimensional coordinate system to precisely locate and target the affected area. This technique enables high doses of radiation to be delivered accurately and efficiently, maximizing therapeutic effectiveness while minimizing side effects.
Radiosurgery can be used to treat various conditions such as brain tumors (both malignant and benign), arteriovenous malformations (AVMs), trigeminal neuralgia, acoustic neuromas, pituitary adenomas, and spinal cord tumors. Common radiosurgery platforms include the Gamma Knife, CyberKnife, and linear accelerator-based systems like Novalis Tx or TrueBeam.
It is essential to note that although it is called "surgery," radiosurgery does not involve any physical incisions or removal of tissue. Instead, it relies on the destructive effects of high-dose radiation to ablate or damage targeted cells over time, leading to their eventual death and resolution of symptoms or tumor control.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
The Sella Turcica, also known as the Turkish saddle, is a depression or fossa in the sphenoid bone located at the base of the skull. It forms a housing for the pituitary gland, which is a small endocrine gland often referred to as the "master gland" because it controls other glands and makes several essential hormones. The Sella Turcica has a saddle-like shape, with its anterior and posterior clinoids forming the front and back of the saddle, respectively. This region is of significant interest in neuroimaging and clinical settings, as various conditions such as pituitary tumors or other abnormalities may affect the size, shape, and integrity of the Sella Turcica.
 Cerebellopontine angle
Cerebellopontine angle
Cerebellopontine angle syndrome
Translabyrinthine approach
Cerebellopontine cistern
Arachnoid cyst
Choroid plexus papilloma
Neurosurgery
Intracranial epidermoid cyst
Robert F. Spetzler
Granulomatous meningoencephalitis
Anatomy of the cerebellum
Trigeminal neuralgia
Bruns nystagmus
Pons
Lipoma
Subarachnoid cisterns
Craniofacial regeneration
Melanocytoma
Dextroscope
Hemifacial spasm
Vestibular schwannoma
Vestibulocochlear nerve
Ludvig Puusepp
Central nervous system cyst
Atypical teratoid rhabdoid tumor
Choroid plexus tumor
Sensorineural hearing loss
Ectopic salivary gland tissue
Index of anatomy articles
Cerebrospinal fluid
Cerebellopontine angle - Wikipedia
Proceedings: Lateral extradural approach to schwannomas of the cerebellopontine angle. | Journal of Neurology, Neurosurgery &...
 Approaches to the Cerebellopontine Angle
Approaches to the Cerebellopontine Angle
 Subjects: Cerebellopontine Angle - Digital Collections - National Library of Medicine Search Results
Subjects: Cerebellopontine Angle - Digital Collections - National Library of Medicine Search Results
 Skull Base Tumor and Other CPA Tumors: Practice Essentials, History of the Procedure, Problem
Skull Base Tumor and Other CPA Tumors: Practice Essentials, History of the Procedure, Problem
 Cerebellopontine angle meningioma (Radiopaedia 48434-53348 Axial DWI) - NC Commons
Cerebellopontine angle meningioma (Radiopaedia 48434-53348 Axial DWI) - NC Commons
Magnified View of the Right Cerebellopontine angle | Neuroanatomy | The Neurosurgical Atlas
MR Imaging of the Temporal Bone: Overview, Basics of Magnetic Resonance Imaging, Cerebellopontine Angle Tumors
Leksell Top 25 - Meningioma Journals
 Acoustic neuroma: MedlinePlus Medical Encyclopedia
Acoustic neuroma: MedlinePlus Medical Encyclopedia
 Radiosurgery for bilateral neurinomas associated with neurofibromatosis type 2
Radiosurgery for bilateral neurinomas associated with neurofibromatosis type 2
Subependymoma of the cerebellopontine angle and prepontine cistern in a 15-year-old adolescent boy<...
 Acute vestibular neuritis: A rare complication after the adenoviral vector-based COVID-19 vaccine | Journal of NeuroVirology
Acute vestibular neuritis: A rare complication after the adenoviral vector-based COVID-19 vaccine | Journal of NeuroVirology
 Meningiomas - Classifications, Risk Factors, Diagnosis and Treatment
Meningiomas - Classifications, Risk Factors, Diagnosis and Treatment
Plus it
Browse | jns Journals
 Myles L. Pensak, MD,FACS
Myles L. Pensak, MD,FACS
 Hemifacial Spasm (12.10.2012)
Hemifacial Spasm (12.10.2012)
 Paul O. Dutcher, M.D. | UR Medicine
Paul O. Dutcher, M.D. | UR Medicine
 Vestibular (Balance and Dizziness) Service - St George's University Hospitals NHS Foundation Trust
Vestibular (Balance and Dizziness) Service - St George's University Hospitals NHS Foundation Trust
 Thieme E-Books & E-Journals - Radiologie up2date / Neuroradiologie
Thieme E-Books & E-Journals - Radiologie up2date / Neuroradiologie
 Baby’s Pregnancy Calendar
Baby’s Pregnancy Calendar
Neurosurgery - Wikipedia
Meningioma: Practice Essentials, Background, Pathophysiology
 Frontiers | Pediatric Central Nervous System Tumors: State-of-the-Art and Debated Aspects
Frontiers | Pediatric Central Nervous System Tumors: State-of-the-Art and Debated Aspects
 Hearing loss and Alzheimer?s disease: A Review
Hearing loss and Alzheimer?s disease: A Review
 Pathology Outlines - Atypical teratoid / rhabdoid tumor
Pathology Outlines - Atypical teratoid / rhabdoid tumor
 Clinical Electrocochleography: Overview of Theories, Techniques and Applications
Clinical Electrocochleography: Overview of Theories, Techniques and ApplicationsTumors2
- Cerebellopontine angle (CPA) tumors are the most common neoplasms in the posterior fossa, accounting for 5-10% of intracranial tumors. (medscape.com)
- Gadolinium-DTPA-enhanced magnetic resonance scanning in cerebellopontine angle tumors. (rochester.edu)
Meningioma1
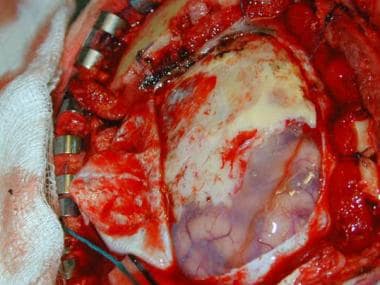
- The dura is opened, and the meningioma can be seen extending en plaque over the surface of the brain. (medscape.com)
Cistern5
- The cerebellopontine angle is the site of the cerebellopontine angle cistern. (wikipedia.org)
- The angle formed in turn creates a subarachnoid cistern, the cerebellopontine angle cistern. (wikipedia.org)
- The pia mater follows the outline of the fissure and the arachnoid mater continues across the divide so that the subarachnoid space is dilated at this area, forming the cerebellopontine angle cistern. (wikipedia.org)
- The coexistence of hyper-inflow aneurysms and cerebellopontine angle cistern (CPAc) arterial venous malformations (AVMs) have been rarely reported and most commonly associated with high risk of bleeding. (surgicalneurologyint.com)
- 27 , 29 ] Cerebellopontine angle cistern (CPAc) AVMs are even rarer,[ 32 ] especially when associated with aneurysms originating from the same parent artery (2.8-9.3% of all AVMs). (surgicalneurologyint.com)
Lesions2
- Surgery of Cerebellopontine Lesions. (wikipedia.org)
- Otherwise, options for management of lesions in the cerebellopontine angle (CPA) include observation with serial imaging, radiation therapy, or surgery. (medscape.com)
Surgery2
- Diluted intracisternal papaverine for microvascular protection of cranial nerves during vestibular schwannoma and cerebello-pontine angle surgery. (nih.gov)
- 2cm in size within the CP angle taking into account age, presence of other health co-morbidities and whether hearing is serviceable (and associated with favorable prognostic findings for hearing preservation surgery). (anac.ca)
Retrosigmoid Approach1
- A retrosigmoid approach has historically been used to approach the Cerebellopontine Angle (CPA). (heraldopenaccess.us)
Cerebellum2
- The cerebellopontine angle (CPA) (Latin: angulus cerebellopontinus) is located between the cerebellum and the pons. (wikipedia.org)
- This fissure is made when the cerebellum folds over to the pons, creating a sharply defined angle between them. (wikipedia.org)
Cerebello-pontine angle1
- cerebello-pontine angle [3,8]. (who.int)
Cavernous1
- 1. Oldenburg MS et al: Cavernous hemangiomas of the internal auditory canal and cerebellopontine angle. (meduniver.com)
Tumor1
- Increasing tumor volume (odds ratio [OR] 1.06, 95% CI 1.01-1.10, p = 0.009) and clival, petrous, or cerebellopontine angle location as compared with petroclival, tentorial, and foramen magnum location (OR 1.95, 95% CI 1.05-3.65, p = 0.036) were predictive of neurological decline after radiosurgery. (thejns.org)
Tumours1
- citation needed] Tumours can arise in the cerebellopontine angle. (wikipedia.org)
Pons1
- The cerebellopontine angle (CPA) is formed by the petrosal cerebellar surface, middle cerebellar peduncle, lateral pons, petrosal surface of the petrous bone, and clival portion of the occipital bone. (duke.edu)
ARTERY2
- citation needed] The anterior inferior cerebellar artery (AICA) is the principal vessel of the cerebellopontine angle. (wikipedia.org)
- The acute origin angle of the vessel from the basilar artery made both malformations unsuitable for endovascular treatment. (surgicalneurologyint.com)
Intracranial1
- Seaman B, Brem S, Fromm A, Staller A, McCardle T, Jain S. Intracranial spread of Merkel cell carcinoma to the cerebellopontine angle. (moffitt.org)
Approach2
- Proceedings: Lateral extradural approach to schwannomas of the cerebellopontine angle. (bmj.com)
- Experiences with a translabyrinthine-transtentorial approach to the cerebellopontine angle. (bvsalud.org)
Case1
- Motor cortex stimulation in a three-year-old child with trigeminal neuropathic pain caused by a malignant glioma in the cerebellopontine angle: case report. (saintluc.be)
Site1
- The cerebellopontine angle is also the site of a set of neurological disorders known as the cerebellopontine angle syndrome. (wikipedia.org)
Auditory canal1
- Imaging revealed a 2.8-cm hemorrhagic left cerebellopontine angle lesion extending into the left internal auditory canal, consistent with hemorrhagic vestibular schwannoma. (thejns.org)
Posterior3
- 6,8 Epidermoids are classically extra-axial, most frequently in the posterior fossa, and most commonly at the cerebellopontine angle. (appliedradiology.com)
- Glossopharyngeal neuralgia is characterized by recurrent attacks of severe pain in the 9th and 10th cranial nerve distribution (posterior pharynx, tonsils, back of the tongue, middle ear, under the angle of the jaw). (merckmanuals.com)
- Dural venous sinus thrombosis is a potentially significant complication that may occur following intracranial operations, especially posterior fossa surgery for cerebellopontine angle tumour resection through either a retrosigmoid or translabyrinthine approach, due to its proximity to the transverse and sigmoid sinus. (web.app)
Arachnoid1
- 5. Arachnoid cyst of the cerebellopontine angle associated with gliosis of the eighth cranial nerve. (nih.gov)
Skull Base1
- For pathologic conditions affecting the skull base and cerebellopontine angle, imaging techniques have advanced to assess for residual disease, disease progression, and postoperative complications. (radiologykey.com)
Anatomy1
- This guide covers the following topics related to Facial Nerve Anatomy: Embryology of the Facial Nerve, Central Connections, Cerebellopontine Angle and the Internal Acoustic Meatus, Intratemporal Course of the Facial Nerve, Extratemporal Facial Nerve, Facial Nerve Paralysis and Vascular Supply of the Facial Nerve. (freebookcentre.net)
Acoustic2
- 8. Trigeminal neuralgia due to an acoustic neuroma in the cerebellopontine angle. (nih.gov)
- It travels with the motor root of the facial nerve through the cerebellopontine angle towards the internal acoustic meatus where it enters the anterior superior quadrant to travel through the petrous temporal bone . (radiopaedia.org)
Syndrome1
- The cerebellopontine angle is also the site of a set of neurological disorders known as the cerebellopontine angle syndrome. (wikipedia.org)
Axial2
Anterior1
- citation needed] The anterior inferior cerebellar artery (AICA) is the principal vessel of the cerebellopontine angle. (wikipedia.org)
Rare1
- We present a rare and interesting case of a cerebellopontine angle cyst containing ectopic choroid plexus tissue in a 26 year-old female. (bris.ac.uk)
Left2
- A left retrosigmoid craniotomy reveals the cerebellopontine angle and the associated cerebrovascular and neurologic landmarks. (neurosurgicalatlas.com)
- An MRI showed a 4.4 x 2.5 x 3.4 centimeters (CC by AP by transverse) avidly enhancing heterogeneous T1 hypointense and T2 hyperintense mass with cystic components centered in the left cerebellopontine angle and widening extending through the left jugular foramen into the left carotid space. (upmc.edu)