Fracture Fixation, Internal
Osseointegration
Bone and Bones
Fracture Healing
Bone Remodeling
Bone Density
Spinal Fusion
Internal Fixators
Bone Marrow
Bone Plates
Bone Development
Bone Marrow Cells
Thoracic Vertebrae
Bone Regeneration
Bone Nails
Lumbar Vertebrae
Axis
Scoliosis
Cervical Vertebrae
Spinal Diseases
Bone Matrix
Surgery, Computer-Assisted
Bone Marrow Transplantation
Orthopedic Procedures
Bone Substitutes
Orthopedic Fixation Devices
Sacrum
Bone Cements
Biomechanical Phenomena
Neuronavigation
Fracture Fixation, Intramedullary
Bone Diseases, Metabolic
Modified Bankart procedure for recurrent anterior dislocation and subluxation of the shoulder in athletes. (1/1294)
Thirty-four athletes (34 shoulders) with recurrent anterior glenohumeral instability were treated with a modified Bankart procedure, using a T-shaped capsular incision in the anterior capsule. The inferior flap was advanced medially and/or superiorly and rigidly fixed at the point of the Bankart lesion by a small cancellous screw and a spike-washer. The superior flap was advanced inferiority and sutured over the inferior flap. Twenty-five athletes (median age: 22) were evaluated over a mean period of follow-up of 65 months. The clinical results were graded, according to Rowe, as 22 (88%) excellent, 3 (12%) good, and none as fair or poor. The mean postoperative range of movement was 92 degrees of external rotation in 90 degrees of abduction. Elevation and internal rotation was symmetrical with the opposite side. Twenty-four patients returned to active sport, 22 at their previous level. This modified Bankart procedure is an effective treatment for athletes with recurrent anterior glenohumeral instability. (+info)Results of the Bosworth method for unstable fractures of the distal clavicle. (2/1294)
Eleven consecutive Neer's type II unstable fractures of the distal third of the clavicle were treated by open reduction and internal fixation, using a temporary Bosworth-type screw. In all cases, fracture healing occurred within 10 weeks. Shoulder function was restored to the pre-injury level. A Bosworth-type screw fixation is a relatively easy and safe technique of open reduction and internal fixation of type II fractures of the distal third of the clavicle. (+info)In vivo and in vitro CT analysis of the occiput. (3/1294)
Arguments concerning the best procedure for occipito-cervical fusion have rarely been based upon occipital bone thickness or only based on in vitro studies. To close this gap and to offer an outlook on preoperative evaluation of the patient, 28 patients were analysed in vivo by means of spiral CT. Ten macerated human skulls were measured by means of CT and directly. Measurements were taken according to a matrix of 66 points following a grid with 1 cm spacing based upon McRae's line. Maximum thickness in the patient group was met 4 cm above the reference plane in the median slice (11.87 mm; SD 3.41 mm) and 5 cm above it in the skull group (15.85 mm; SD 1.81 mm). Correlation between CT and direct measurements was good (91.79%). Intra-individual discrepancies from one side to the respective point on the other side are common (difference > 1 mm in 60%). Judging areas suitable for operative fixation using the 10% percentile value (6.68 mm for the maximum value of 11.87 mm) led to the conclusion that screws should only be inserted along the occipital crest in an area extending from 1.5 cm above the posterior margin of the foramen magnum to the external occipital protuberance (EOP). At the level of the EOP screws may also be inserted up to 1 cm lateral of the midline. A reduction of screw length to 7 mm (9 mm for the EOP) is proposed. Preoperative evaluation of the patient should be carried out by spiral CT with 1 mm slicing and sagittal reconstructions. (+info)Lumbar intradiscal pressure after posterolateral fusion and pedicle screw fixation. (4/1294)
In vitro biomechanical testing was performed in single-functional spinal units of fresh calf lumbar spines, using pressure needle transducers to investigate the effect of posterolateral fusion (PLF) and pedicle screw constructs (PS) on intradiscal pressure (IDP), in order to elucidate the mechanical factors concerned with residual low back pain after PLF. IDP of 6 calf lumbar spines consisting of L4 and L5 vertebrae and an intervening disc was measured under axial compression, flexion-extension and lateral bending in the intact spine, PS, PLF and the destabilized spine. Relative to the intact spines, the destabilized spines showed increased IDP in all of lordings and moments. IDP under PS and PLF were significantly decreased in axial compression, extension and lateral bending loads (p<0.05). In flexion, IDP under PS and PLF increased linearly proportional to the magnitude of flexion moment and reached as high as IDP of the intact spines. These results demonstrated that despite an increase in the stiffness of motion segments after PLF and PS, significant high disc pressure is still generated in flexion. Flexibility of PS and PLF may cause increased axial load sharing of the disc in flexion and increased IDP. This high IDP may explain patients' persisting pain following PS and PLF. (+info)MR imaging for early complications of transpedicular screw fixation. (5/1294)
This series comprises ten patients treated with transpedicular screw fixation, who suffered early postoperative problems such as radicular pain or motor weakness. Besides plain radiographs, all patients were also evaluated with MR imaging. Three patients were reoperated for either repositioning or removal of the screws. MR images, especially T1-weighted ones, were very helpful for visualizing the problem and verifying the positions of the screws. In cases of wide areas of signal void around the screws, the neighboring axial MR images at either side, which have fewer artifacts, gave more information about the screws and the vertebrae. (+info)Unusual presentation of spinal cord compression related to misplaced pedicle screws in thoracic scoliosis. (6/1294)
Utilization of thoracic pedicle screws is controversial, especially in the treatment of scoliosis. We present a case of a 15-year-old girl seen 6 months after her initial surgery for scoliosis done elsewhere. She complained of persistent epigastric pain, tremor of the right foot at rest, and abnormal feelings in her legs. Clinical examination revealed mild weakness in the right lower extremity, a loss of thermoalgic discrimination, and a forward imbalance. A CT scan revealed at T8 and T10 that the right pedicle screws were misplaced by 4 mm in the spinal canal. At the time of the revision surgery the somatosensory evoked potentials (SSEP) returned to normal after screw removal. The clinical symptoms resolved 1 month after the revision. The authors conclude that after pedicle instrumentation at the thoracic level a spinal cord compression should be looked for in case of subtle neurologic findings such as persistent abdominal pain, mild lower extremity weakness, tremor at rest, thermoalgic discrimination loss, or unexplained imbalance. (+info)Spinal instrumentation for unstable C1-2 injury. (7/1294)
Seventeen patients with unstable C1-2 injuries were treated between 1990 and 1997. Various methods of instrumentation surgery were performed in 16 patients, excluding a case of atlantoaxial rotatory fixation. Posterior stabilization was carried out in 14 cases using Halifax interlaminar clamp, Sof'wire or Danek cable, or more recently, transarticular screws. Transodontoid anterior screw fixation was performed in four cases of odontoid process fractures, with posterior instrumentation in two cases because of malunion. Rigid internal fixation by instrumentation surgery for the unstable C1-2 injury avoids long-term application of a Halo brace and facilitates early rehabilitation. However, the procedure is technically demanding with the risk of neural and vascular injuries, particularly with posterior screw fixation. Sagittal reconstruction of thin-sliced computed tomography scans at the C1-2 region, neuronavigator, and intraoperative fluoroscopy are essential to allow preoperative surgical planning and intraoperative guidance. (+info)The 'MW' sacropelvic construct: an enhanced fixation of the lumbosacral junction in neuromuscular pelvic obliquity. (8/1294)
Fixation to the lumbosacral spine to correct pelvic obliquity in neuromuscular scoliosis has always remained a surgical challenge. The strongest fixation of the lumbosacral junction has been achieved with either a Galveston technique with rods or screws or with iliosacral screws. We have devised a new fixation system, in which iliosacral screws are combined with iliac screws. This is made possible by using the AO Universal Spine System with side opening hooks above and below the iliosacral screws and iliac screws below it. The whole sacropelvis is thus encompassed by a maximum width (MW) fixation, which gives an 'M' appearance on the pelvic radiographs and a 'W' appearance in the axial plane. We report on our surgical technique and the early results where such a technique was used. We feel that this new means of fixation (by combining the strongest fixation systems) is extremely solid and should be included in the wide armamentarium of sacropelvic fixation. (+info)Bone screws are medical devices used in orthopedic and trauma surgery to affix bone fracture fragments or to attach bones to other bones or to metal implants such as plates, rods, or artificial joints. They are typically made of stainless steel or titanium alloys and have a threaded shaft that allows for purchase in the bone when tightened. The head of the screw may have a hexagonal or star-shaped design to allow for precise tightening with a screwdriver. Bone screws come in various shapes, sizes, and designs, including fully threaded, partially threaded, cannulated (hollow), and headless types, depending on their intended use and location in the body.
Fracture fixation, internal, is a surgical procedure where a fractured bone is fixed using metal devices such as plates, screws, or rods that are implanted inside the body. This technique helps to maintain the alignment and stability of the broken bone while it heals. The implants may be temporarily or permanently left inside the body, depending on the nature and severity of the fracture. Internal fixation allows for early mobilization and rehabilitation, which can result in a faster recovery and improved functional outcome.
Osseointegration is a direct structural and functional connection between living bone and the surface of an implant. It's a process where the bone grows in and around the implant, which is typically made of titanium or another biocompatible material. This process provides a solid foundation for dental prosthetics, such as crowns, bridges, or dentures, or for orthopedic devices like artificial limbs. The success of osseointegration depends on various factors, including the patient's overall health, the quality and quantity of available bone, and the surgical technique used for implant placement.
"Bone" is the hard, dense connective tissue that makes up the skeleton of vertebrate animals. It provides support and protection for the body's internal organs, and serves as a attachment site for muscles, tendons, and ligaments. Bone is composed of cells called osteoblasts and osteoclasts, which are responsible for bone formation and resorption, respectively, and an extracellular matrix made up of collagen fibers and mineral crystals.
Bones can be classified into two main types: compact bone and spongy bone. Compact bone is dense and hard, and makes up the outer layer of all bones and the shafts of long bones. Spongy bone is less dense and contains large spaces, and makes up the ends of long bones and the interior of flat and irregular bones.
The human body has 206 bones in total. They can be further classified into five categories based on their shape: long bones, short bones, flat bones, irregular bones, and sesamoid bones.
Fracture healing is the natural process by which a broken bone repairs itself. When a fracture occurs, the body responds by initiating a series of biological and cellular events aimed at restoring the structural integrity of the bone. This process involves the formation of a hematoma (a collection of blood) around the fracture site, followed by the activation of inflammatory cells that help to clean up debris and prepare the area for repair.
Over time, specialized cells called osteoblasts begin to lay down new bone matrix, or osteoid, along the edges of the broken bone ends. This osteoid eventually hardens into new bone tissue, forming a bridge between the fracture fragments. As this process continues, the callus (a mass of newly formed bone and connective tissue) gradually becomes stronger and more compact, eventually remodeling itself into a solid, unbroken bone.
The entire process of fracture healing can take several weeks to several months, depending on factors such as the severity of the injury, the patient's age and overall health, and the location of the fracture. In some cases, medical intervention may be necessary to help promote healing or ensure proper alignment of the bone fragments. This may include the use of casts, braces, or surgical implants such as plates, screws, or rods.
X-ray microtomography, often referred to as micro-CT, is a non-destructive imaging technique used to visualize and analyze the internal structure of objects with high spatial resolution. It is based on the principles of computed tomography (CT), where multiple X-ray images are acquired at different angles and then reconstructed into cross-sectional slices using specialized software. These slices can be further processed to create 3D visualizations, allowing researchers and clinicians to examine the internal structure and composition of samples in great detail. Micro-CT is widely used in materials science, biology, medicine, and engineering for various applications such as material characterization, bone analysis, and defect inspection.
Bone remodeling is the normal and continuous process by which bone tissue is removed from the skeleton (a process called resorption) and new bone tissue is formed (a process called formation). This ongoing cycle allows bones to repair microdamage, adjust their size and shape in response to mechanical stress, and maintain mineral homeostasis. The cells responsible for bone resorption are osteoclasts, while the cells responsible for bone formation are osteoblasts. These two cell types work together to maintain the structural integrity and health of bones throughout an individual's life.
During bone remodeling, the process can be divided into several stages:
1. Activation: The initiation of bone remodeling is triggered by various factors such as microdamage, hormonal changes, or mechanical stress. This leads to the recruitment and activation of osteoclast precursor cells.
2. Resorption: Osteoclasts attach to the bone surface and create a sealed compartment called a resorption lacuna. They then secrete acid and enzymes that dissolve and digest the mineralized matrix, creating pits or cavities on the bone surface. This process helps remove old or damaged bone tissue and releases calcium and phosphate ions into the bloodstream.
3. Reversal: After resorption is complete, the osteoclasts undergo apoptosis (programmed cell death), and mononuclear cells called reversal cells appear on the resorbed surface. These cells prepare the bone surface for the next stage by cleaning up debris and releasing signals that attract osteoblast precursors.
4. Formation: Osteoblasts, derived from mesenchymal stem cells, migrate to the resorbed surface and begin producing a new organic matrix called osteoid. As the osteoid mineralizes, it forms a hard, calcified structure that gradually replaces the resorbed bone tissue. The osteoblasts may become embedded within this newly formed bone as they differentiate into osteocytes, which are mature bone cells responsible for maintaining bone homeostasis and responding to mechanical stress.
5. Mineralization: Over time, the newly formed bone continues to mineralize, becoming stronger and more dense. This process helps maintain the structural integrity of the skeleton and ensures adequate calcium storage.
Throughout this continuous cycle of bone remodeling, hormones, growth factors, and mechanical stress play crucial roles in regulating the balance between resorption and formation. Disruptions to this delicate equilibrium can lead to various bone diseases, such as osteoporosis, where excessive resorption results in weakened bones and increased fracture risk.
Bone density refers to the amount of bone mineral content (usually measured in grams) in a given volume of bone (usually measured in cubic centimeters). It is often used as an indicator of bone strength and fracture risk. Bone density is typically measured using dual-energy X-ray absorptiometry (DXA) scans, which provide a T-score that compares the patient's bone density to that of a young adult reference population. A T-score of -1 or above is considered normal, while a T-score between -1 and -2.5 indicates osteopenia (low bone mass), and a T-score below -2.5 indicates osteoporosis (porous bones). Regular exercise, adequate calcium and vitamin D intake, and medication (if necessary) can help maintain or improve bone density and prevent fractures.
Spinal fusion is a surgical procedure where two or more vertebrae in the spine are fused together to create a solid bone. The purpose of this procedure is to restrict movement between the fused vertebrae, which can help reduce pain and stabilize the spine. This is typically done using bone grafts or bone graft substitutes, along with hardware such as rods, screws, or cages to hold the vertebrae in place while they heal together. The procedure may be recommended for various spinal conditions, including degenerative disc disease, spinal stenosis, spondylolisthesis, scoliosis, or fractures.
Internal fixators are medical devices that are implanted into the body through surgery to stabilize and hold broken or fractured bones in the correct position while they heal. These devices can be made from various materials, such as metal (stainless steel or titanium) or bioabsorbable materials. Internal fixators can take many forms, including plates, screws, rods, nails, wires, or cages, depending on the type and location of the fracture.
The main goal of using internal fixators is to promote bone healing by maintaining accurate reduction and alignment of the fractured bones, allowing for early mobilization and rehabilitation. This can help reduce the risk of complications such as malunion, nonunion, or deformity. Internal fixators are typically removed once the bone has healed, although some bioabsorbable devices may not require a second surgery for removal.
It is important to note that while internal fixators provide stability and support for fractured bones, they do not replace the need for proper immobilization, protection, or rehabilitation during the healing process. Close follow-up with an orthopedic surgeon is essential to ensure appropriate healing and address any potential complications.
Bone resorption is the process by which bone tissue is broken down and absorbed into the body. It is a normal part of bone remodeling, in which old or damaged bone tissue is removed and new tissue is formed. However, excessive bone resorption can lead to conditions such as osteoporosis, in which bones become weak and fragile due to a loss of density. This process is carried out by cells called osteoclasts, which break down the bone tissue and release minerals such as calcium into the bloodstream.
Bone marrow is the spongy tissue found inside certain bones in the body, such as the hips, thighs, and vertebrae. It is responsible for producing blood-forming cells, including red blood cells, white blood cells, and platelets. There are two types of bone marrow: red marrow, which is involved in blood cell production, and yellow marrow, which contains fatty tissue.
Red bone marrow contains hematopoietic stem cells, which can differentiate into various types of blood cells. These stem cells continuously divide and mature to produce new blood cells that are released into the circulation. Red blood cells carry oxygen throughout the body, white blood cells help fight infections, and platelets play a crucial role in blood clotting.
Bone marrow also serves as a site for immune cell development and maturation. It contains various types of immune cells, such as lymphocytes, macrophages, and dendritic cells, which help protect the body against infections and diseases.
Abnormalities in bone marrow function can lead to several medical conditions, including anemia, leukopenia, thrombocytopenia, and various types of cancer, such as leukemia and multiple myeloma. Bone marrow aspiration and biopsy are common diagnostic procedures used to evaluate bone marrow health and function.
Bone plates are medical devices used in orthopedic surgery to stabilize and hold together fractured or broken bones during the healing process. They are typically made of surgical-grade stainless steel, titanium, or other biocompatible materials. The plate is shaped to fit the contour of the bone and is held in place with screws that are inserted through the plate and into the bone on either side of the fracture. This provides stability and alignment to the broken bones, allowing them to heal properly. Bone plates can be used to treat a variety of fractures, including those that are complex or unstable. After healing is complete, the bone plate may be left in place or removed, depending on the individual's needs and the surgeon's recommendation.
Bone neoplasms are abnormal growths or tumors that develop in the bone. They can be benign (non-cancerous) or malignant (cancerous). Benign bone neoplasms do not spread to other parts of the body and are rarely a threat to life, although they may cause problems if they grow large enough to press on surrounding tissues or cause fractures. Malignant bone neoplasms, on the other hand, can invade and destroy nearby tissue and may spread (metastasize) to other parts of the body.
There are many different types of bone neoplasms, including:
1. Osteochondroma - a benign tumor that develops from cartilage and bone
2. Enchondroma - a benign tumor that forms in the cartilage that lines the inside of the bones
3. Chondrosarcoma - a malignant tumor that develops from cartilage
4. Osteosarcoma - a malignant tumor that develops from bone cells
5. Ewing sarcoma - a malignant tumor that develops in the bones or soft tissues around the bones
6. Giant cell tumor of bone - a benign or occasionally malignant tumor that develops from bone tissue
7. Fibrosarcoma - a malignant tumor that develops from fibrous tissue in the bone
The symptoms of bone neoplasms vary depending on the type, size, and location of the tumor. They may include pain, swelling, stiffness, fractures, or limited mobility. Treatment options depend on the type and stage of the tumor but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
Bone development, also known as ossification, is the process by which bone tissue is formed and grows. This complex process involves several different types of cells, including osteoblasts, which produce new bone matrix, and osteoclasts, which break down and resorb existing bone tissue.
There are two main types of bone development: intramembranous and endochondral ossification. Intramembranous ossification occurs when bone tissue forms directly from connective tissue, while endochondral ossification involves the formation of a cartilage model that is later replaced by bone.
During fetal development, most bones develop through endochondral ossification, starting as a cartilage template that is gradually replaced by bone tissue. However, some bones, such as those in the skull and clavicles, develop through intramembranous ossification.
Bone development continues after birth, with new bone tissue being laid down and existing tissue being remodeled throughout life. This ongoing process helps to maintain the strength and integrity of the skeleton, allowing it to adapt to changing mechanical forces and repair any damage that may occur.
Bone marrow cells are the types of cells found within the bone marrow, which is the spongy tissue inside certain bones in the body. The main function of bone marrow is to produce blood cells. There are two types of bone marrow: red and yellow. Red bone marrow is where most blood cell production takes place, while yellow bone marrow serves as a fat storage site.
The three main types of bone marrow cells are:
1. Hematopoietic stem cells (HSCs): These are immature cells that can differentiate into any type of blood cell, including red blood cells, white blood cells, and platelets. They have the ability to self-renew, meaning they can divide and create more hematopoietic stem cells.
2. Red blood cell progenitors: These are immature cells that will develop into mature red blood cells, also known as erythrocytes. Red blood cells carry oxygen from the lungs to the body's tissues and carbon dioxide back to the lungs.
3. Myeloid and lymphoid white blood cell progenitors: These are immature cells that will develop into various types of white blood cells, which play a crucial role in the body's immune system by fighting infections and diseases. Myeloid progenitors give rise to granulocytes (neutrophils, eosinophils, and basophils), monocytes, and megakaryocytes (which eventually become platelets). Lymphoid progenitors differentiate into B cells, T cells, and natural killer (NK) cells.
Bone marrow cells are essential for maintaining a healthy blood cell count and immune system function. Abnormalities in bone marrow cells can lead to various medical conditions, such as anemia, leukopenia, leukocytosis, thrombocytopenia, or thrombocytosis, depending on the specific type of blood cell affected. Additionally, bone marrow cells are often used in transplantation procedures to treat patients with certain types of cancer, such as leukemia and lymphoma, or other hematologic disorders.
Bone diseases is a broad term that refers to various medical conditions that affect the bones. These conditions can be categorized into several groups, including:
1. Developmental and congenital bone diseases: These are conditions that affect bone growth and development before or at birth. Examples include osteogenesis imperfecta (brittle bone disease), achondroplasia (dwarfism), and cleidocranial dysostosis.
2. Metabolic bone diseases: These are conditions that affect the body's ability to maintain healthy bones. They are often caused by hormonal imbalances, vitamin deficiencies, or problems with mineral metabolism. Examples include osteoporosis, osteomalacia, and Paget's disease of bone.
3. Inflammatory bone diseases: These are conditions that cause inflammation in the bones. They can be caused by infections, autoimmune disorders, or other medical conditions. Examples include osteomyelitis, rheumatoid arthritis, and ankylosing spondylitis.
4. Degenerative bone diseases: These are conditions that cause the bones to break down over time. They can be caused by aging, injury, or disease. Examples include osteoarthritis, avascular necrosis, and diffuse idiopathic skeletal hyperostosis (DISH).
5. Tumors and cancers of the bone: These are conditions that involve abnormal growths in the bones. They can be benign or malignant. Examples include osteosarcoma, chondrosarcoma, and Ewing sarcoma.
6. Fractures and injuries: While not strictly a "disease," fractures and injuries are common conditions that affect the bones. They can result from trauma, overuse, or weakened bones. Examples include stress fractures, compound fractures, and dislocations.
Overall, bone diseases can cause a wide range of symptoms, including pain, stiffness, deformity, and decreased mobility. Treatment for these conditions varies depending on the specific diagnosis but may include medication, surgery, physical therapy, or lifestyle changes.
Bone transplantation, also known as bone grafting, is a surgical procedure in which bone or bone-like material is transferred from one part of the body to another or from one person to another. The graft may be composed of cortical (hard outer portion) bone, cancellous (spongy inner portion) bone, or a combination of both. It can be taken from different sites in the same individual (autograft), from another individual of the same species (allograft), or from an animal source (xenograft). The purpose of bone transplantation is to replace missing bone, provide structural support, and stimulate new bone growth. This procedure is commonly used in orthopedic, dental, and maxillofacial surgeries to repair bone defects caused by trauma, tumors, or congenital conditions.
The thoracic vertebrae are the 12 vertebrae in the thoracic region of the spine, which is the portion between the cervical and lumbar regions. These vertebrae are numbered T1 to T12, with T1 being closest to the skull and T12 connecting to the lumbar region.
The main function of the thoracic vertebrae is to provide stability and support for the chest region, including protection for the vital organs within, such as the heart and lungs. Each thoracic vertebra has costal facets on its sides, which articulate with the heads of the ribs, forming the costovertebral joints. This connection between the spine and the ribcage allows for a range of movements while maintaining stability.
The thoracic vertebrae have a unique structure compared to other regions of the spine. They are characterized by having long, narrow bodies, small bony processes, and prominent spinous processes that point downwards. This particular shape and orientation of the thoracic vertebrae contribute to their role in limiting excessive spinal movement and providing overall trunk stability.
A bone fracture is a medical condition in which there is a partial or complete break in the continuity of a bone due to external or internal forces. Fractures can occur in any bone in the body and can vary in severity from a small crack to a shattered bone. The symptoms of a bone fracture typically include pain, swelling, bruising, deformity, and difficulty moving the affected limb. Treatment for a bone fracture may involve immobilization with a cast or splint, surgery to realign and stabilize the bone, or medication to manage pain and prevent infection. The specific treatment approach will depend on the location, type, and severity of the fracture.
Bone regeneration is the biological process of new bone formation that occurs after an injury or removal of a portion of bone. This complex process involves several stages, including inflammation, migration and proliferation of cells, matrix deposition, and mineralization, leading to the restoration of the bone's structure and function.
The main cells involved in bone regeneration are osteoblasts, which produce new bone matrix, and osteoclasts, which resorb damaged or old bone tissue. The process is tightly regulated by various growth factors, hormones, and signaling molecules that promote the recruitment, differentiation, and activity of these cells.
Bone regeneration can occur naturally in response to injury or surgical intervention, such as fracture repair or dental implant placement. However, in some cases, bone regeneration may be impaired due to factors such as age, disease, or trauma, leading to delayed healing or non-union of the bone. In these situations, various strategies and techniques, including the use of bone grafts, scaffolds, and growth factors, can be employed to enhance and support the bone regeneration process.
I believe you are referring to "bone pins" or "bone nails" rather than "bone nails." These terms are used in the medical field to describe surgical implants made of metal or biocompatible materials that are used to stabilize and hold together fractured bones during the healing process. They can also be used in spinal fusion surgery to provide stability and promote bone growth between vertebrae.
Bone pins or nails typically have a threaded or smooth shaft, with a small diameter that allows them to be inserted into the medullary canal of long bones such as the femur or tibia. They may also have a head or eyelet on one end that allows for attachment to external fixation devices or other surgical instruments.
The use of bone pins and nails has revolutionized orthopedic surgery, allowing for faster healing times, improved stability, and better functional outcomes for patients with fractures or spinal deformities.
The lumbar vertebrae are the five largest and strongest vertebrae in the human spine, located in the lower back region. They are responsible for bearing most of the body's weight and providing stability during movement. The lumbar vertebrae have a characteristic shape, with a large body in the front, which serves as the main weight-bearing structure, and a bony ring in the back, formed by the pedicles, laminae, and processes. This ring encloses and protects the spinal cord and nerves. The lumbar vertebrae are numbered L1 to L5, starting from the uppermost one. They allow for flexion, extension, lateral bending, and rotation movements of the trunk.
In medical terms, "axis" is used to describe a line or lines along which a structure or body part can move or around which it is oriented. It is often used in anatomical context to refer to specific axes of movement or alignment for various parts of the body. For example:
* The axial skeleton, also known as the upright skeleton, includes the skull, vertebral column, and chest cage.
* In neurology, the term "axis" is used to describe the second cervical vertebra (C2), which is also called the axis because it serves as a pivot point for head movement.
* The term "longitudinal axis" is used to describe an imaginary line that runs from the head to the foot, passing through the center of the body.
* In imaging studies such as X-rays or MRIs, the term "axis" may be used to describe a specific orientation or alignment for the image.
Overall, the term "axis" is used in medicine to describe lines or planes that serve as reference points for movement, alignment, or orientation of various body structures and parts.
Scoliosis is a medical condition characterized by an abnormal lateral curvature of the spine, which most often occurs in the thoracic or lumbar regions. The curvature can be "C" or "S" shaped and may also include rotation of the vertebrae. Mild scoliosis doesn't typically cause problems, but severe cases can interfere with breathing and other bodily functions.
The exact cause of most scoliosis is unknown, but it may be related to genetic factors. It often develops in the pre-teen or teenage years, particularly in girls, and is more commonly found in individuals with certain neuromuscular disorders such as cerebral palsy and muscular dystrophy.
Treatment for scoliosis depends on the severity of the curve, its location, and the age and expected growth of the individual. Mild cases may only require regular monitoring to ensure the curve doesn't worsen. More severe cases may require bracing or surgery to correct the curvature and prevent it from getting worse.
The cervical vertebrae are the seven vertebrae that make up the upper part of the spine, also known as the neck region. They are labeled C1 to C7, with C1 being closest to the skull and C7 connecting to the thoracic vertebrae in the chest region. The cervical vertebrae have unique structures to allow for a wide range of motion in the neck while also protecting the spinal cord and providing attachment points for muscles and ligaments.
Fluoroscopy is a type of medical imaging that uses X-rays to obtain real-time moving images of the internal structures of the body. A continuous X-ray beam is passed through the body part being examined, and the resulting fluoroscopic images are transmitted to a monitor, allowing the medical professional to view the structure and movement of the internal organs and bones in real time.
Fluoroscopy is often used to guide minimally invasive procedures such as catheterization, stent placement, or joint injections. It can also be used to diagnose and monitor a variety of medical conditions, including gastrointestinal disorders, musculoskeletal injuries, and cardiovascular diseases.
It is important to note that fluoroscopy involves exposure to ionizing radiation, and the risks associated with this exposure should be carefully weighed against the benefits of the procedure. Medical professionals are trained to use the lowest possible dose of radiation necessary to obtain the desired diagnostic information.
Spinal diseases refer to a range of medical conditions that affect the spinal column, which is made up of vertebrae (bones), intervertebral discs, facet joints, nerves, ligaments, and muscles. These diseases can cause pain, discomfort, stiffness, numbness, weakness, or even paralysis, depending on the severity and location of the condition. Here are some examples of spinal diseases:
1. Degenerative disc disease: This is a condition where the intervertebral discs lose their elasticity and height, leading to stiffness, pain, and decreased mobility.
2. Herniated disc: This occurs when the inner material of the intervertebral disc bulges or herniates out through a tear in the outer layer, causing pressure on the spinal nerves and resulting in pain, numbness, tingling, or weakness in the affected area.
3. Spinal stenosis: This is a narrowing of the spinal canal or the neural foramen (the openings where the spinal nerves exit the spinal column), which can cause pressure on the spinal cord or nerves and result in pain, numbness, tingling, or weakness.
4. Scoliosis: This is a curvature of the spine that can occur in children or adults, leading to an abnormal posture, back pain, and decreased lung function.
5. Osteoarthritis: This is a degenerative joint disease that affects the facet joints in the spine, causing pain, stiffness, and decreased mobility.
6. Ankylosing spondylitis: This is a chronic inflammatory disease that affects the spine and sacroiliac joints, leading to pain, stiffness, and fusion of the vertebrae.
7. Spinal tumors: These are abnormal growths that can occur in the spinal column, which can be benign or malignant, causing pain, neurological symptoms, or even paralysis.
8. Infections: Bacterial or viral infections can affect the spine, leading to pain, fever, and other systemic symptoms.
9. Trauma: Fractures, dislocations, or sprains of the spine can occur due to accidents, falls, or sports injuries, causing pain, neurological deficits, or even paralysis.
Bone matrix refers to the non-cellular component of bone that provides structural support and functions as a reservoir for minerals, such as calcium and phosphate. It is made up of organic and inorganic components. The organic component consists mainly of type I collagen fibers, which provide flexibility and tensile strength to the bone. The inorganic component is primarily composed of hydroxyapatite crystals, which give bone its hardness and compressive strength. Bone matrix also contains other proteins, growth factors, and signaling molecules that regulate bone formation, remodeling, and repair.
Computer-assisted surgery (CAS) refers to the use of computer systems and technologies to assist and enhance surgical procedures. These systems can include a variety of tools such as imaging software, robotic systems, and navigation devices that help surgeons plan, guide, and perform surgeries with greater precision and accuracy.
In CAS, preoperative images such as CT scans or MRI images are used to create a three-dimensional model of the surgical site. This model can be used to plan the surgery, identify potential challenges, and determine the optimal approach. During the surgery, the surgeon can use the computer system to navigate and guide instruments with real-time feedback, allowing for more precise movements and reduced risk of complications.
Robotic systems can also be used in CAS to perform minimally invasive procedures with smaller incisions and faster recovery times. The surgeon controls the robotic arms from a console, allowing for greater range of motion and accuracy than traditional hand-held instruments.
Overall, computer-assisted surgery provides a number of benefits over traditional surgical techniques, including improved precision, reduced risk of complications, and faster recovery times for patients.
Bone marrow transplantation (BMT) is a medical procedure in which damaged or destroyed bone marrow is replaced with healthy bone marrow from a donor. Bone marrow is the spongy tissue inside bones that produces blood cells. The main types of BMT are autologous, allogeneic, and umbilical cord blood transplantation.
In autologous BMT, the patient's own bone marrow is used for the transplant. This type of BMT is often used in patients with lymphoma or multiple myeloma who have undergone high-dose chemotherapy or radiation therapy to destroy their cancerous bone marrow.
In allogeneic BMT, bone marrow from a genetically matched donor is used for the transplant. This type of BMT is often used in patients with leukemia, lymphoma, or other blood disorders who have failed other treatments.
Umbilical cord blood transplantation involves using stem cells from umbilical cord blood as a source of healthy bone marrow. This type of BMT is often used in children and adults who do not have a matched donor for allogeneic BMT.
The process of BMT typically involves several steps, including harvesting the bone marrow or stem cells from the donor, conditioning the patient's body to receive the new bone marrow or stem cells, transplanting the new bone marrow or stem cells into the patient's body, and monitoring the patient for signs of engraftment and complications.
BMT is a complex and potentially risky procedure that requires careful planning, preparation, and follow-up care. However, it can be a life-saving treatment for many patients with blood disorders or cancer.
Orthopedic procedures are surgical or nonsurgical methods used to treat musculoskeletal conditions, including injuries, deformities, or diseases of the bones, joints, muscles, ligaments, and tendons. These procedures can range from simple splinting or casting to complex surgeries such as joint replacements, spinal fusions, or osteotomies (cutting and repositioning bones). The primary goal of orthopedic procedures is to restore function, reduce pain, and improve the quality of life for patients.
Bone substitutes are materials that are used to replace missing or damaged bone in the body. They can be made from a variety of materials, including natural bone from other parts of the body or from animals, synthetic materials, or a combination of both. The goal of using bone substitutes is to provide structural support and promote the growth of new bone tissue.
Bone substitutes are often used in dental, orthopedic, and craniofacial surgery to help repair defects caused by trauma, tumors, or congenital abnormalities. They can also be used to augment bone volume in procedures such as spinal fusion or joint replacement.
There are several types of bone substitutes available, including:
1. Autografts: Bone taken from another part of the patient's body, such as the hip or pelvis.
2. Allografts: Bone taken from a deceased donor and processed to remove any cells and infectious materials.
3. Xenografts: Bone from an animal source, typically bovine or porcine, that has been processed to remove any cells and infectious materials.
4. Synthetic bone substitutes: Materials such as calcium phosphate ceramics, bioactive glass, and polymer-based materials that are designed to mimic the properties of natural bone.
The choice of bone substitute material depends on several factors, including the size and location of the defect, the patient's medical history, and the surgeon's preference. It is important to note that while bone substitutes can provide structural support and promote new bone growth, they may not have the same strength or durability as natural bone. Therefore, they may not be suitable for all applications, particularly those that require high load-bearing capacity.
A cadaver is a deceased body that is used for medical research or education. In the field of medicine, cadavers are often used in anatomy lessons, surgical training, and other forms of medical research. The use of cadavers allows medical professionals to gain a deeper understanding of the human body and its various systems without causing harm to living subjects. Cadavers may be donated to medical schools or obtained through other means, such as through consent of the deceased or their next of kin. It is important to handle and treat cadavers with respect and dignity, as they were once living individuals who deserve to be treated with care even in death.
Orthopedic fixation devices are medical implants used in orthopedic surgery to provide stability and promote the healing of fractured or broken bones, as well as joints or spinal segments. These devices can be internal or external and include a variety of products such as:
1. Intramedullary nails: Long rods that are inserted into the center of a bone to stabilize fractures in long bones like the femur or tibia.
2. Plates and screws: Metal plates are attached to the surface of a bone with screws to hold the fragments together while they heal.
3. Screws: Used alone or in combination with other devices, they can be used to stabilize small fractures or to fix implants like total joint replacements.
4. Wires: Used to hold bone fragments together, often in conjunction with other devices.
5. External fixators: A external frame attached to the bones using pins or wires that is placed outside the skin to provide stability and alignment of fractured bones.
6. Spinal fixation devices: These include pedicle screws, rods, hooks, and plates used to stabilize spinal fractures or deformities.
7. Orthopedic staples: Small metal staples used to stabilize small bone fragments or for joint fusion.
The choice of orthopedic fixation device depends on the location and severity of the injury or condition being treated. The primary goal of these devices is to provide stability, promote healing, and restore function.
The sacrum is a triangular-shaped bone in the lower portion of the human vertebral column, located between the lumbar spine and the coccyx (tailbone). It forms through the fusion of several vertebrae during fetal development. The sacrum's base articulates with the fifth lumbar vertebra, while its apex connects with the coccyx.
The sacrum plays an essential role in supporting the spine and transmitting weight from the upper body to the pelvis and lower limbs. It also serves as an attachment site for various muscles and ligaments. The sacral region is often a focus in medical and chiropractic treatments due to its importance in spinal stability, posture, and overall health.
The Cervical Atlas, also known as C1 or the atlas vertebra, is the uppermost and most superior of the seven cervical vertebrae in the human spine. It plays a crucial role in supporting and facilitating the movement of the head, as it articulates with both the occipital bone (forming the joint called the atlanto-occipital joint) and the axis (or C2) vertebra (forming the atlantoaxial joint). The unique structure of the cervical atlas lacks a body, instead having an anterior and posterior arch with two lateral masses that form the facet joints for articulation with the axis. This arrangement allows for a wide range of motion in the neck, including flexion, extension, lateral bending, and rotation.
Bone cements are medical-grade materials used in orthopedic and trauma surgery to fill gaps between bone surfaces and implants, such as artificial joints or screws. They serve to mechanically stabilize the implant and provide a smooth, load-bearing surface. The two most common types of bone cement are:
1. Polymethylmethacrylate (PMMA) cement: This is a two-component system consisting of powdered PMMA and liquid methyl methacrylate monomer. When mixed together, they form a dough-like consistency that hardens upon exposure to air. PMMA cement has been widely used for decades in joint replacement surgeries, such as hip or knee replacements.
2. Calcium phosphate (CP) cement: This is a two-component system consisting of a powdered CP compound and an aqueous solution. When mixed together, they form a paste that hardens through a chemical reaction at body temperature. CP cement has lower mechanical strength compared to PMMA but demonstrates better biocompatibility, bioactivity, and the ability to resorb over time.
Both types of bone cements have advantages and disadvantages, and their use depends on the specific surgical indication and patient factors.
A spinal fracture, also known as a vertebral compression fracture, is a break in one or more bones (vertebrae) of the spine. This type of fracture often occurs due to weakened bones caused by osteoporosis, but it can also result from trauma such as a car accident or a fall.
In a spinal fracture, the front part of the vertebra collapses, causing the height of the vertebra to decrease, while the back part of the vertebra remains intact. This results in a wedge-shaped deformity of the vertebra. Multiple fractures can lead to a hunched forward posture known as kyphosis or dowager's hump.
Spinal fractures can cause pain, numbness, tingling, or weakness in the back, legs, or arms, depending on the location and severity of the fracture. In some cases, spinal cord compression may occur, leading to more severe symptoms such as paralysis or loss of bladder and bowel control.
The atlanto-axial joint is the joint between the first and second cervical vertebrae, also known as C1 (atlas) and C2 (axis). It consists of two separate joints: the median atlanto-axial joint, which is a pivot joint that allows for rotation of the head, and the paired lateral atlanto-axial joints, which are plane joints that allow for limited gliding movements.
The atlanto-axial joint is surrounded by several ligaments that provide stability and limit excessive movement. The transverse ligament, located on the anterior aspect of the joint, is particularly important as it prevents excessive movement of the atlas on the axis and helps to protect the spinal cord.
Abnormalities or injuries to the atlanto-axial joint can result in instability and potentially serious neurological complications.
Biomechanics is the application of mechanical laws to living structures and systems, particularly in the field of medicine and healthcare. A biomechanical phenomenon refers to a observable event or occurrence that involves the interaction of biological tissues or systems with mechanical forces. These phenomena can be studied at various levels, from the molecular and cellular level to the tissue, organ, and whole-body level.
Examples of biomechanical phenomena include:
1. The way that bones and muscles work together to produce movement (known as joint kinematics).
2. The mechanical behavior of biological tissues such as bone, cartilage, tendons, and ligaments under various loads and stresses.
3. The response of cells and tissues to mechanical stimuli, such as the way that bone tissue adapts to changes in loading conditions (known as Wolff's law).
4. The biomechanics of injury and disease processes, such as the mechanisms of joint injury or the development of osteoarthritis.
5. The use of mechanical devices and interventions to treat medical conditions, such as orthopedic implants or assistive devices for mobility impairments.
Understanding biomechanical phenomena is essential for developing effective treatments and prevention strategies for a wide range of medical conditions, from musculoskeletal injuries to neurological disorders.
Neuronavigation is a surgical technique that uses imaging technology, such as MRI or CT scans, to create a 3D map of the patient's brain in real-time during surgery. This allows surgeons to accurately locate and navigate to specific areas of the brain with greater precision and less invasiveness, improving surgical outcomes and reducing the risk of complications.
The neuronavigation system typically consists of a computer workstation, tracking systems, and instruments that are equipped with sensors. The system is able to track the position and orientation of these instruments relative to the patient's brain, allowing the surgeon to visualize the location of the instruments on the 3D map in real-time.
Neuronavigation has become an essential tool in many neurosurgical procedures, including tumor resection, functional neurosurgery, and deep brain stimulation. It enables surgeons to perform more complex surgeries with increased safety and efficacy, ultimately improving the quality of care for patients undergoing these procedures.
Intramedullary fracture fixation is a surgical technique used to stabilize and align bone fractures. In this procedure, a metal rod or nail is inserted into the marrow cavity (intramedullary canal) of the affected bone, spanning the length of the fracture. The rod is then secured to the bone using screws or other fixation devices on either side of the fracture. This provides stability and helps maintain proper alignment during the healing process.
The benefits of intramedullary fixation include:
1. Load sharing: The intramedullary rod shares some of the load bearing capacity with the bone, which can help reduce stress on the healing bone.
2. Minimal soft tissue dissection: Since the implant is inserted through the medullary canal, there is less disruption to the surrounding muscles, tendons, and ligaments compared to other fixation methods.
3. Biomechanical stability: Intramedullary fixation provides rotational and bending stiffness, which helps maintain proper alignment of the fracture fragments during healing.
4. Early mobilization: Patients with intramedullary fixation can often begin weight bearing and rehabilitation exercises earlier than those with other types of fixation, leading to faster recovery times.
Common indications for intramedullary fracture fixation include long bone fractures in the femur, tibia, humerus, and fibula, as well as certain pelvic and spinal fractures. However, the choice of fixation method depends on various factors such as patient age, fracture pattern, location, and associated injuries.
The spine, also known as the vertebral column, is a complex structure in the human body that is part of the axial skeleton. It is composed of 33 individual vertebrae (except in some people where there are fewer due to fusion of certain vertebrae), intervertebral discs, facet joints, ligaments, muscles, and nerves.
The spine has several important functions:
1. Protection: The spine protects the spinal cord, which is a major component of the nervous system, by enclosing it within a bony canal.
2. Support: The spine supports the head and upper body, allowing us to maintain an upright posture and facilitating movement of the trunk and head.
3. Movement: The spine enables various movements such as flexion (bending forward), extension (bending backward), lateral flexion (bending sideways), and rotation (twisting).
4. Weight-bearing: The spine helps distribute weight and pressure evenly across the body, reducing stress on individual vertebrae and other structures.
5. Blood vessel and nerve protection: The spine protects vital blood vessels and nerves that pass through it, including the aorta, vena cava, and spinal nerves.
The spine is divided into five regions: cervical (7 vertebrae), thoracic (12 vertebrae), lumbar (5 vertebrae), sacrum (5 fused vertebrae), and coccyx (4 fused vertebrae, also known as the tailbone). Each region has unique characteristics that allow for specific functions and adaptations to the body's needs.
The femur is the medical term for the thigh bone, which is the longest and strongest bone in the human body. It connects the hip bone to the knee joint and plays a crucial role in supporting the weight of the body and allowing movement during activities such as walking, running, and jumping. The femur is composed of a rounded head, a long shaft, and two condyles at the lower end that articulate with the tibia and patella to form the knee joint.
Metabolic bone diseases are a group of conditions that affect the bones and are caused by disorders in the body's metabolism. These disorders can result in changes to the bone structure, density, and strength, leading to an increased risk of fractures and other complications. Some common examples of metabolic bone diseases include:
1. Osteoporosis: a condition characterized by weak and brittle bones that are more likely to break, often as a result of age-related bone loss or hormonal changes.
2. Paget's disease of bone: a chronic disorder that causes abnormal bone growth and deformities, leading to fragile and enlarged bones.
3. Osteomalacia: a condition caused by a lack of vitamin D or problems with the body's ability to absorb it, resulting in weak and soft bones.
4. Hyperparathyroidism: a hormonal disorder that causes too much parathyroid hormone to be produced, leading to bone loss and other complications.
5. Hypoparathyroidism: a hormonal disorder that results in low levels of parathyroid hormone, causing weak and brittle bones.
6. Renal osteodystrophy: a group of bone disorders that occur as a result of chronic kidney disease, including osteomalacia, osteoporosis, and high turnover bone disease.
Treatment for metabolic bone diseases may include medications to improve bone density and strength, dietary changes, exercise, and lifestyle modifications. In some cases, surgery may be necessary to correct bone deformities or fractures.
 Herbert screw
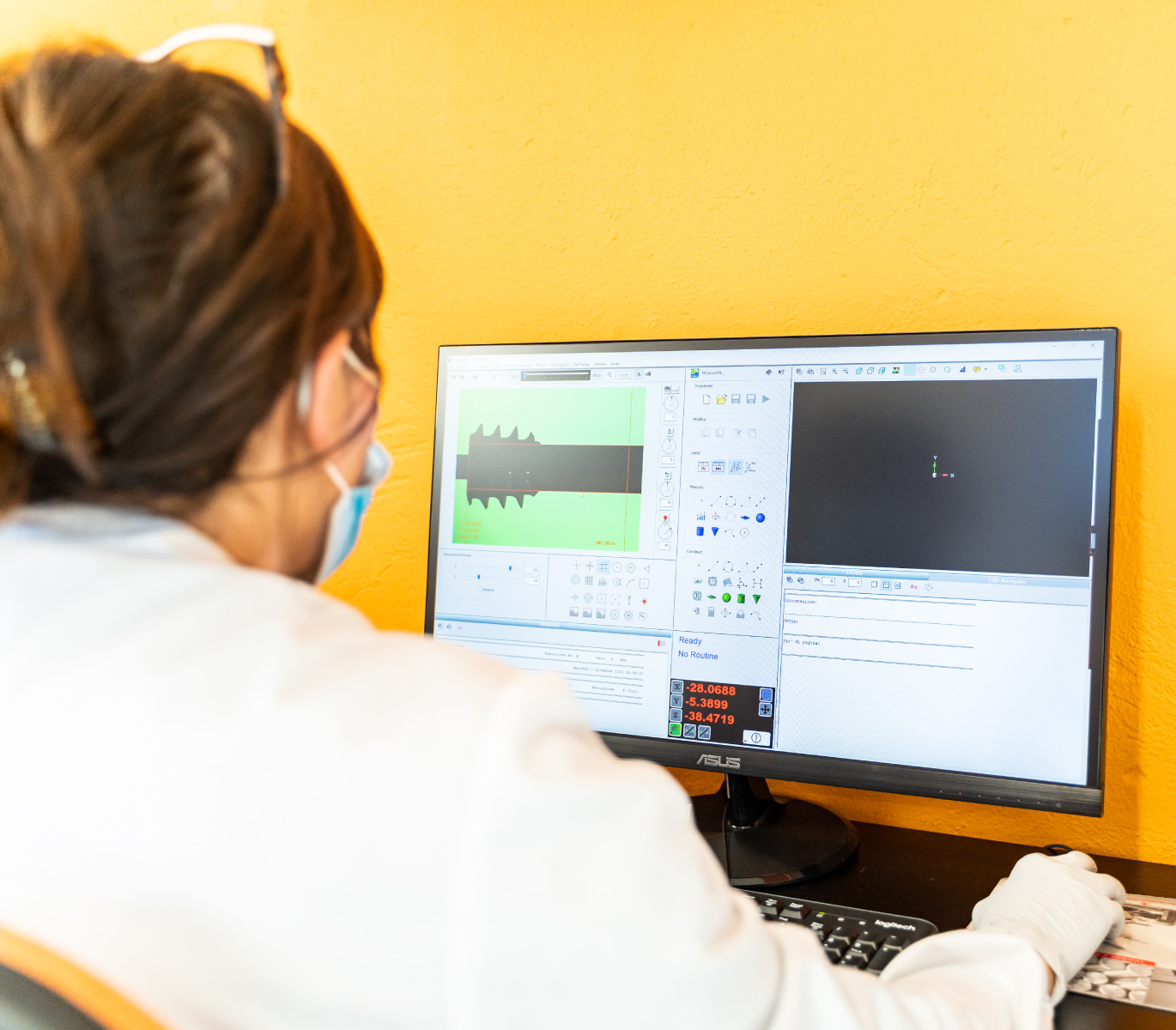
Herbert screw Technical paper Measurement of bone plates and screws
Technical paper Measurement of bone plates and screws Nose Rings Nose Screws Nose bones & studs
Nose Rings Nose Screws Nose bones & studs Fenestrated pedicle screws for cement-augmented purchase in patients with bone softening: a review of 21 cases
Fenestrated pedicle screws for cement-augmented purchase in patients with bone softening: a review of 21 cases Cortical threaded pedicle screw improves fatigue strength in decreased bone quality | European Spine Journal
Cortical threaded pedicle screw improves fatigue strength in decreased bone quality | European Spine Journal what type of screws may be used + best natural bone graft substitutes
what type of screws may be used + best natural bone graft substitutes Augmented screwdrivers reduce bone stripping rates and optimize tightness when inserting non-locking screws (TightRight)
Augmented screwdrivers reduce bone stripping rates and optimize tightness when inserting non-locking screws (TightRight) 01024BO Overflow Plate Screw - Brass - 2.25' - Bone
- Eagle Mountain
01024BO Overflow Plate Screw - Brass - 2.25' - Bone
- Eagle Mountain xSPECT Bone Used to Delineate Cervical Vertebral Screw Loosening
xSPECT Bone Used to Delineate Cervical Vertebral Screw Loosening bone screws | IRD Glass
bone screws | IRD Glass Bone Screw | Pain Solutions Medical
Bone Screw | Pain Solutions Medical Hybrid pedicle screw and modified cortical bone trajectory technique in transforaminal lumbar interbody fusion at L4-L5 segment...
Hybrid pedicle screw and modified cortical bone trajectory technique in transforaminal lumbar interbody fusion at L4-L5 segment... Titanium Screws and Driver Guided Bone Regenerative Dental Tool Kit
Titanium Screws and Driver Guided Bone Regenerative Dental Tool Kit Small 1.7mm Herbert Bone Cannulated Screws For Hand Finger
Small 1.7mm Herbert Bone Cannulated Screws For Hand Finger Bone Screw | Veterinary Cortex Screws | Veterinary Cortical Screws | Cancellous Screws Manufacturer
Bone Screw | Veterinary Cortex Screws | Veterinary Cortical Screws | Cancellous Screws Manufacturer Archimedes Screw Fossil (021021e) - The Stones & Bones Collection
Archimedes Screw Fossil (021021e) - The Stones & Bones Collection Is there a place for thermocautery of the soft palate? | IVIS
Is there a place for thermocautery of the soft palate? | IVIS Dental Bone Screws Kit bone fixation screw kit tools instruments totalimplant.com
Dental Bone Screws Kit bone fixation screw kit tools instruments totalimplant.com EFR Remover Screw Normal Straumann Bone Level |
Kompodent verkkokauppa
EFR Remover Screw Normal Straumann Bone Level |
Kompodent verkkokauppa Three-Year Analysis of Tapered Screw Vent Implants Placed Into Maxillary Sinuses Grafted With Mineralized Bone Allograft |...
Three-Year Analysis of Tapered Screw Vent Implants Placed Into Maxillary Sinuses Grafted With Mineralized Bone Allograft |...