Aromatase Inhibitors
Triazoles
Nitriles
Fadrozole
Aromatase
Androstatrienes
Antineoplastic Agents, Hormonal
Tamoxifen
Androstenedione
Postmenopause
Neoplasms, Hormone-Dependent
Estrogens
Estrogen Antagonists
Androstadienes
Estradiol
Receptors, Estrogen
Estrogen Receptor Modulators
Testolactone
Chemotherapy, Adjuvant
Selective Estrogen Receptor Modulators
Testosterone
Estrone
Gynecomastia
Enzyme Inhibitors
Receptors, Progesterone
Megestrol Acetate
Estrogen Receptor alpha
Ovary
Clinical Trials as Topic
Androgens
Drug Resistance, Neoplasm
Puberty, Precocious
Papio anubis
Hot Flashes
Dihydrotestosterone
Endometriosis
Sex Differentiation
Follicle Stimulating Hormone
Clomiphene
Bone Density Conservation Agents
Treatment Outcome
Neoadjuvant Therapy
Estrogen Receptor beta
Gonadotropins
Luteinizing Hormone
Receptor, erbB-2
Randomized Controlled Trials as Topic
Mammary Neoplasms, Experimental
Ovulation Induction
Placenta
Puberty, Delayed
Fibrous Dysplasia, Polyostotic
Steroids
Diphosphonates
Double-Blind Method
Drug Administration Schedule
Bone Density
The aromatase inactivator 4-hydroxyandrostenedione (4-OH-A) inhibits tamoxifen metabolism by rat hepatic cytochrome P-450 3A: potential for drug-drug interaction of tamoxifen and 4-OH-A in combined anti-breast cancer therapy. (1/981)
Tamoxifen (tam), an anti-breast cancer agent, is metabolized into tam-N-oxide by the hepatic flavin-containing monooxygenase and into N-desmethyl- and 4-hydroxy-tam by cytochrome P-450s (CYPs). Additionally, tam is metabolically activated by hepatic CYP3A, forming a reactive intermediate that binds covalently to proteins. Tam and 4-hydroxyandrostenedione (4-OH-A) are currently used to treat breast cancer, and it has been contemplated that 4-OH-A be given concurrently with tam to contravene potential tumor resistance to tam. Because alterations in tam metabolism may influence its therapeutic efficacy, the effect of 4-OH-A on tam metabolism was examined. Incubation of tam with liver microsomes from phenobarbital-treated rats, in the presence of 4-OH-A (10-100 microM), resulted in marked inhibition of tam-N-demethylation and tam covalent binding and in decreased tam-N-oxide accumulation; however, there was no inhibition of the formation of 4-hydroxy-tam and of 3,4-dihydroxytamoxifen. These findings indicate that 4-OH-A inhibits CYP3A, but not P-450(s) that catalyze tam 4-hydroxylation. The diminished tam-N-oxide accumulation could be due to decreased N-oxide formation and/or due to increased N-oxide reduction. Incubation of tam-N-oxide with liver microsomes containing heat-inactivated flavin-containing monooxygenase demonstrated that 4-OH-A increases the accumulation of tam, possibly by diminishing its P-450-mediated metabolism. Kinetic studies indicate that 4-OH-A is a competitive inhibitor of CYP3A, but not a time-dependent inactivator. Consequently, the concurrent treatment of tam and 4-OH-A may result in increased tam half-life and thus could potentiate the therapeutic efficacy of tam and diminish the potential side effects of tam by inhibiting its covalent binding to proteins and possibly to DNA. (+info)Inhibitory effects of nitric oxide on the expression and activity of aromatase in human granulosa cells. (2/981)
The aim of the present study was to explore the mechanisms by which nitric oxide (NO) may inhibit aromatase activity of human granulosa cells. Ovarian granulosa-luteal cells, obtained from patients undergoing in-vitro fertilization (IVF) were cultured in the presence of NO-related substances. After 24 h of culture, aromatase activity of the cells was significantly inhibited by treatment with the NO donors, SNAP or NOC12 at > or =10(-4) M in a dose-dependent manner. Treatment with NO catabolites or a peroxynitrite-releasing compound, SIN1, had no significant influence. Treatment with SNAP at 10(-3) M decreased relative aromatase mRNA values by 72% (P<0.05) and intracellular cyclic AMP concentrations by 53% (P<0.01). However, treatment with H89, an inhibitor of protein kinase A, did not inhibit aromatase activity. Since there were no significant effects of NO catabolites or peroxinitrite, the inhibitory action of NO donors on aromatase must be related to NO release. The action of NO is, in part, attributable to the down-regulation of aromatase gene transcription. Although NO decreased intracellular cAMP values, down-regulation of aromatase gene transcription may not be mediated by protein kinase A-dependent mechanisms. (+info)Evidence of sex reversal in the gonads of chicken embryos after oestrogen treatment as detected by expression of lutropin receptor. (3/981)
In chicken embryos, there is a difference between the sexes in the onset of lutropin receptor mRNA expression in the gonads. The effects of oestrogen on lutropin receptor expression were studied to investigate the mechanism controlling this difference. Lutropin receptor mRNA expression was detected in the ovaries of sesame oil-treated control female embryos on day 12 of incubation, while no expression was found in the testes of the male controls. Oestradiol administration to genetically male embryos before sexual differentiation resulted in gonadal sex reversal which was characterized histologically by the proliferation of cortical cords and the presence of lacunae. Lutropin receptor expression was detected in the feminizing testis on day 12 of incubation. Administration of aromatase inhibitor (CGS 16949 A) to genetically female embryos before sexual differentiation inhibited the formation of cortical cords, although a relatively weak expression of lutropin receptor was detected. These results indicate that early expression of the lutropin receptor is regulated by oestrogen. (+info)Presence of an aromatase inhibitor, possibly heat shock protein 90, in dominant follicles of cattle. (4/981)
In cattle, it has been suggested that follicular fluid has direct modulatory effects on follicular growth and maturation. In the first part of this study, an in vitro test using aromatase activity of follicular wall fragments as an end point was validated for cattle follicles and was used to test whether follicular fluid (from dominant or non-dominant follicles) modulates aromatase activity. Fluid from dominant follicles at a concentration of 24 or 12% (obtained during the luteal and follicular phases, respectively) significantly inhibited aromatase activity. Inhibitory activity was low or absent in fluid from non-dominant follicles. FSH-stimulated aromatase activity was also reduced by fluid from dominant follicles, but not to a greater extent than in basal conditions. Finally, charcoal-treated fluid from dominant follicles retained its inhibitory activity. In contrast, ovarian venous serum draining a dominant follicle had no activity at the three concentrations tested (6, 12 and 24%). In the second part of the study, identification of the compounds involved in this modulatory activity was attempted using SDS-PAGE. Comparison of the fluorographs from de novo synthesized proteins stored in follicular fluid (inhibitory medium) with those secreted in incubation medium (inactive medium) demonstrated that one protein (90 kDa, pI 5.8) was significantly (P < 0.05) more abundant in fluid from dominant follicles (2.0 +/- 0.09%) than in the culture medium (1.3 +/- 0.1% of the total proteins). This protein had characteristics similar to those of heat shock protein 90 (hsp 90). Therefore, in the final part of the study, the presence of hsp 90 in ovarian cells and follicular fluid was investigated using immunohistochemistry and western blot analysis. After immunohistochemistry, a positive signal was detected mainly in the granulosa cells of larger follicles and to a smaller extent in thecal cells and oocytes. Western blot analysis also demonstrated the presence of hsp 90 in follicular wall fragments and fluid. When blotting was achieved on a sample of follicular fluid resolved by two-dimensional PAGE, the spot detected had a similar location to that at 90 kDa and pI 5.8. Addition of purified hsp 90 to bovine follicles in vitro depressed aromatase activity by altering the K(m) value (and possibly the Vmax value) of the enzyme. It is proposed that hsp 90 is a functional regulator of follicular maturation through its action on aromatase. (+info)The third-generation non-steroidal aromatase inhibitors: a review of their clinical benefits in the second-line hormonal treatment of advanced breast cancer. (5/981)
Three new aromatase inhibitors have recently completed phase III evaluation as treatment of metastatic breast cancer in post-menopausal women whose disease has progressed despite tamoxifen therapy: anastrozole (ARIMIDEX, Zeneca), letrozole (FEMARA, Novartis) and vorozole (RIVIZOR, Janssen). All belong to the third generation of non-steroidal aromatase inhibitors, and each is superior to previous generations in terms of potency and selectivity. The trials that have been performed compare each agent to megestrol acetate, and letrozole and vorozole to aminoglutethimide. Although the studies are not directly comparable due to differing study designs and patient populations, it has been demonstrated each of these drugs provides single agent, once-daily, oral palliation of hormone-responsive, post-menopausal metastatic breast cancer. Letrozole is clearly more effective than megestrol acetate, and anastrozole and vorozole are possibly so. All three are better tolerated than the progestin, particularly in terms of weight gain. Both letrozole and vorozole are significantly more effective, and better tolerated than aminoglutethimide. Overall, this most recent generation of aromatase inhibitors is a clear improvement on our current standard second-line therapies. In 1999, tamoxifen remains the first choice in the hormonal therapy of breast cancer. Following tamoxifen failure, the optimal second-line hormonal therapy remains undefined, but aminoglutethimide and megestrol acetate are no longer optimal therapy in this setting. The third-generation non-steroidal aromatase inhibitors must now be compared to each other, to the steroidal aromatase inhibitors, to the pure anti-oestrogens, and to tamoxifen. (+info)Estrogen-inducible, sex-specific expression of brain-derived neurotrophic factor mRNA in a forebrain song control nucleus of the juvenile zebra finch. (6/981)
The expression of brain-derived neurotrophic factor (BDNF) mRNA is increased significantly within the high vocal center (HVc) of male but not female zebra finches from posthatching day 30-35 on. The population of HVc cells expressing BDNF mRNA included 35% of the neurons projecting to the nucleus robustus of the archistriatum (RA). In the RA and in RA-projecting neurons of the lateral portion of the magnocellular nucleus of the anterior neostriatum, BDNF mRNA was expressed at very low levels in both sexes. The BDNF-receptor trkB mRNA was expressed in the RA, in RA-projecting neurons of lateral portion of the magnocellular nucleus of the anterior neostriatum, and in the HVc, except in most of its RA-projecting neurons. Premature stimulation and an inhibitory effect on the normal increase of the BDNF mRNA expression in juvenile males occurred after treatments with 17beta-estradiol and the aromatase inhibitor fadrozole, respectively. The up-regulation of the BDNF expression in the HVc could be a mechanism by which estrogen triggers the differentiation of cells within and connected to the HVc of male zebra finches. (+info)Mitogenic and antioxidant mechanisms of estradiol action in preovulatory ovine follicles: relevance to luteal function. (7/981)
The objectives of this investigation were to determine the intrafollicular mechanisms and physiological consequences of estradiol actions in preovulatory ovine follicles. Acute suppression of estradiol production in proestrous ewes by an aromatase inhibitor (Arimidex) was associated with follicular lipid peroxidation, testosterone accumulation, and a granulosa cell deficiency (decreased proliferation/increased apoptosis). Estradiol-17beta stimulated granulosa proliferating cell nuclear antigen (PCNA) and protected cells from oxidative (H(2)O(2)) stress-induced apoptosis in vitro; the PCNA, but not the antiapoptotic response, was negated by the transcriptional inhibitor actinomycin D. Thus, it appears that genomic/mitotic and cytoprotective (oxygen-scavenging) modes of estradiol action operate in preovulatory follicles. Luteal (large steroidogenic cell) function was diminished following ovulation induction of estradiol-deficient follicles. It is suggested that inadequate exposure of the preovulatory follicle to estradiol caused the granulosa lutein insufficiency. (+info)Gonadal stage-dependent effects of gonadal steroids on gonadotropin II secretion in the Atlantic croaker (Micropogonias undulatus). (8/981)
Involvement of gonadal steroids in the control of gonadotropin II (GTH II) (homologous to LH) secretion was investigated in the Atlantic croaker (Micropogonias undulatus) using gonadectomy (Gx) and steroid replacement paradigms. Gonadectomy in males and females during the late gonadal recrudescence phase elicited significant increases in the gonadotropin response to stimulation by an LHRH analog (LHRHa), without altering basal GTH II secretion. Slow-release silicone elastomer implants of testosterone or estradiol significantly inhibited LHRHa-induced GTH II secretion in gonad-intact and Gx males, and in Gx females, whereas 5alpha-dihydrotestosterone, a nonaromatizable androgen, was ineffective. Pretreatment of fish with an aromatase inhibitor, 1,4, 6-androstatrien-3,17-dione, 2 days before the administration of testosterone implants, completely blocked the negative effect of testosterone on LHRHa-induced GTH II secretion in males, but only partially restored it in females. This suggests that the negative feedback of testosterone in males is primarily mediated by its conversion to estradiol at the level of the hypothalamus and/or pituitary gland, while in females the androgen may also exert a direct inhibitory effect on GTH II secretion, probably mediated via an androgen receptor. In addition, estradiol and testosterone exerted positive effects on basal and LHRHa-induced GTH II secretion during the early-recrudescence phase of the gonadal cycle. The steroids switched to a negative effect on LHRHa-induced GTH II secretion once the fish had fully developed gonads, possibly as a mechanism that prevents a precocious surge in GTH II secretion and final gamete maturation until gametogenesis is complete and the environmental conditions are appropriate for spawning. (+info)Aromatase inhibitors (AIs) are a class of drugs that are primarily used in the treatment of hormone-sensitive breast cancer in postmenopausal women. They work by inhibiting the enzyme aromatase, which is responsible for converting androgens into estrogens. By blocking this conversion, AIs decrease the amount of estrogen in the body, thereby depriving hormone-sensitive breast cancer cells of the estrogen they need to grow and multiply.
There are three main types of aromatase inhibitors:
1. Letrozole (Femara) - a non-steroidal AI that is taken orally once a day.
2. Anastrozole (Arimidex) - another non-steroidal AI that is also taken orally once a day.
3. Exemestane (Aromasin) - a steroidal AI that is taken orally once a day.
In addition to their use in breast cancer treatment, AIs are also sometimes used off-label for the treatment of estrogen-dependent conditions such as endometriosis and uterine fibroids. However, it's important to note that the use of aromatase inhibitors can have significant side effects, including hot flashes, joint pain, and bone loss, so they should only be used under the close supervision of a healthcare provider.
Triazoles are a class of antifungal medications that have broad-spectrum activity against various fungi, including yeasts, molds, and dermatophytes. They work by inhibiting the synthesis of ergosterol, an essential component of fungal cell membranes, leading to increased permeability and disruption of fungal growth. Triazoles are commonly used in both systemic and topical formulations for the treatment of various fungal infections, such as candidiasis, aspergillosis, cryptococcosis, and dermatophytoses. Some examples of triazole antifungals include fluconazole, itraconazole, voriconazole, and posaconazole.
Nitriles, in a medical context, refer to a class of organic compounds that contain a cyano group (-CN) bonded to a carbon atom. They are widely used in the chemical industry and can be found in various materials, including certain plastics and rubber products.
In some cases, nitriles can pose health risks if ingested, inhaled, or come into contact with the skin. Short-term exposure to high levels of nitriles can cause irritation to the eyes, nose, throat, and respiratory tract. Prolonged or repeated exposure may lead to more severe health effects, such as damage to the nervous system, liver, and kidneys.
However, it's worth noting that the medical use of nitriles is not very common. Some nitrile gloves are used in healthcare settings due to their resistance to many chemicals and because they can provide a better barrier against infectious materials compared to latex or vinyl gloves. But beyond this application, nitriles themselves are not typically used as medications or therapeutic agents.
Fadrozole is a non-steroidal aromatase inhibitor drug that is used in the treatment of breast cancer. Aromatase inhibitors work by blocking the production of estrogen, which some types of breast cancer cells need to grow. By reducing the amount of estrogen in the body, fadrozole can help slow or stop the growth of these cancer cells.
Fadrozole is typically used as a treatment for postmenopausal women with hormone receptor-positive breast cancer. It may be used as a first-line therapy or after other treatments have failed. The drug is administered orally, and the typical dosage is 1-2 mg per day.
Like all medications, fadrozole can cause side effects, including hot flashes, nausea, vomiting, and joint pain. In some cases, it may also cause more serious side effects such as liver damage or an increased risk of bone fractures. Patients taking fadrozole should be monitored closely by their healthcare provider to ensure that the drug is working effectively and to manage any side effects that may occur.
Aromatase is a enzyme that belongs to the cytochrome P450 superfamily, and it is responsible for converting androgens into estrogens through a process called aromatization. This enzyme plays a crucial role in the steroid hormone biosynthesis pathway, particularly in females where it is primarily expressed in adipose tissue, ovaries, brain, and breast tissue.
Aromatase inhibitors are used as a treatment for estrogen receptor-positive breast cancer in postmenopausal women, as they work by blocking the activity of aromatase and reducing the levels of circulating estrogens in the body.
Androstatrienes are a class of steroidal compounds that contain a 1,2-dehydrogenated A-ring in their chemical structure. They are named after androstane, which is the reduced form of testosterone, by replacing two hydrogen atoms with a double bond between the first and second carbon atoms in the A-ring.
Androstatrienes do not have any significant medical relevance on their own, but some compounds that contain an androstadiene structure may have biological activity. For example, certain androstadienedione derivatives have been investigated for their potential as progestins or as inhibitors of 5α-reductase, an enzyme involved in the conversion of testosterone to dihydrotestosterone.
It is worth noting that some androstadiene compounds may be produced endogenously in the human body, while others may be synthesized in the laboratory for research or therapeutic purposes. However, it is important to note that some androstadienes are also found in certain anabolic-androgenic steroids (AAS) and can be used as markers of AAS use in drug testing.
Antineoplastic agents, hormonal, are a class of drugs used to treat cancers that are sensitive to hormones. These agents work by interfering with the production or action of hormones in the body. They can be used to slow down or stop the growth of cancer cells and may also help to relieve symptoms caused by the spread of cancer.
Hormonal therapies can work in one of two ways: they can either block the production of hormones or prevent their action on cancer cells. For example, some hormonal therapies work by blocking the action of estrogen or testosterone, which are hormones that can stimulate the growth of certain types of cancer cells.
Examples of hormonal agents used to treat cancer include:
* Aromatase inhibitors (such as letrozole, anastrozole, and exemestane), which block the production of estrogen in postmenopausal women
* Selective estrogen receptor modulators (such as tamoxifen and raloxifene), which block the action of estrogen on cancer cells
* Luteinizing hormone-releasing hormone agonists (such as leuprolide, goserelin, and triptorelin), which block the production of testosterone in men
* Antiandrogens (such as bicalutamide, flutamide, and enzalutamide), which block the action of testosterone on cancer cells
Hormonal therapies are often used in combination with other treatments, such as surgery or radiation therapy. They may be used to shrink tumors before surgery, to kill any remaining cancer cells after surgery, or to help control the spread of cancer that cannot be removed by surgery. Hormonal therapies can also be used to relieve symptoms and improve quality of life in people with advanced cancer.
It's important to note that hormonal therapies are not effective for all types of cancer. They are most commonly used to treat breast, prostate, and endometrial cancers, which are known to be sensitive to hormones. Hormonal therapies may also be used to treat other types of cancer in certain situations.
Like all medications, hormonal therapies can have side effects. These can vary depending on the specific drug and the individual person. Common side effects of hormonal therapies include hot flashes, fatigue, mood changes, and sexual dysfunction. Some hormonal therapies can also cause more serious side effects, such as an increased risk of osteoporosis or blood clots. It's important to discuss the potential risks and benefits of hormonal therapy with a healthcare provider before starting treatment.
Tamoxifen is a selective estrogen receptor modulator (SERM) medication that is primarily used in the treatment and prevention of breast cancer. It works by blocking the action of estrogen in the body, particularly in breast tissue. This can help to stop or slow the growth of hormone-sensitive tumors.
Tamoxifen has been approved by the U.S. Food and Drug Administration (FDA) for use in both men and women. It is often used as a part of adjuvant therapy, which is treatment given after surgery to reduce the risk of cancer recurrence. Tamoxifen may also be used to treat metastatic breast cancer that has spread to other parts of the body.
Common side effects of tamoxifen include hot flashes, vaginal discharge, and changes in mood or vision. Less commonly, tamoxifen can increase the risk of blood clots, stroke, and endometrial cancer (cancer of the lining of the uterus). However, for many women with breast cancer, the benefits of taking tamoxifen outweigh the risks.
It's important to note that while tamoxifen can be an effective treatment option for some types of breast cancer, it is not appropriate for all patients. A healthcare professional will consider a variety of factors when determining whether tamoxifen is the right choice for an individual patient.
Breast neoplasms refer to abnormal growths in the breast tissue that can be benign or malignant. Benign breast neoplasms are non-cancerous tumors or growths, while malignant breast neoplasms are cancerous tumors that can invade surrounding tissues and spread to other parts of the body.
Breast neoplasms can arise from different types of cells in the breast, including milk ducts, milk sacs (lobules), or connective tissue. The most common type of breast cancer is ductal carcinoma, which starts in the milk ducts and can spread to other parts of the breast and nearby structures.
Breast neoplasms are usually detected through screening methods such as mammography, ultrasound, or MRI, or through self-examination or clinical examination. Treatment options for breast neoplasms depend on several factors, including the type and stage of the tumor, the patient's age and overall health, and personal preferences. Treatment may include surgery, radiation therapy, chemotherapy, hormone therapy, or targeted therapy.
Androstenedione is a steroid hormone produced by the adrenal glands, ovaries, and testes. It is a precursor to both male and female sex hormones, including testosterone and estrogen. In the adrenal glands, it is produced from cholesterol through a series of biochemical reactions involving several enzymes. Androstenedione can also be converted into other steroid hormones, such as dehydroepiandrosterone (DHEA) and estrone.
In the body, androstenedione plays an important role in the development and maintenance of secondary sexual characteristics, such as facial hair and a deep voice in men, and breast development and menstrual cycles in women. It also contributes to bone density, muscle mass, and overall physical strength.
Androstenedione is available as a dietary supplement and has been marketed as a way to boost athletic performance and increase muscle mass. However, its effectiveness for these purposes is not supported by scientific evidence, and it may have harmful side effects when taken in high doses or for extended periods of time. Additionally, the use of androstenedione as a dietary supplement is banned by many sports organizations, including the International Olympic Committee and the National Collegiate Athletic Association.
Aminoglutethimide is a medication that is primarily used to treat hormone-sensitive cancers such as breast cancer and prostate cancer. It works by blocking the production of certain hormones in the body, including estrogen and cortisol. Aminoglutethimide is an inhibitor of steroid synthesis, specifically targeting the enzymes involved in the conversion of cholesterol to steroid hormones.
The medication is available in oral form and is typically taken 2-3 times a day. Common side effects include drowsiness, dizziness, dry mouth, skin rash, and changes in appetite or weight. More serious side effects may include liver damage, severe allergic reactions, and changes in heart rhythm.
It's important to note that aminoglutethimide can interact with other medications, so it's crucial to inform your healthcare provider about all the drugs you are currently taking before starting this medication. Additionally, regular monitoring of liver function and hormone levels may be necessary during treatment with aminoglutethimide.
Postmenopause is a stage in a woman's life that follows 12 months after her last menstrual period (menopause) has occurred. During this stage, the ovaries no longer release eggs and produce lower levels of estrogen and progesterone hormones. The reduced levels of these hormones can lead to various physical changes and symptoms, such as hot flashes, vaginal dryness, and mood changes. Postmenopause is also associated with an increased risk of certain health conditions, including osteoporosis and heart disease. It's important for women in postmenopause to maintain a healthy lifestyle, including regular exercise, a balanced diet, and routine medical check-ups to monitor their overall health and manage any potential risks.
Hormone-dependent neoplasms are a type of tumor that requires the presence of specific hormones to grow and multiply. These neoplasms have receptors on their cell surfaces that bind to the hormones, leading to the activation of signaling pathways that promote cell division and growth.
Examples of hormone-dependent neoplasms include breast cancer, prostate cancer, and endometrial cancer. In breast cancer, for instance, estrogen and/or progesterone can bind to their respective receptors on the surface of cancer cells, leading to the activation of signaling pathways that promote tumor growth. Similarly, in prostate cancer, androgens such as testosterone can bind to androgen receptors on the surface of cancer cells, promoting cell division and tumor growth.
Hormone-dependent neoplasms are often treated with hormonal therapies that aim to reduce or block the production of the relevant hormones or interfere with their ability to bind to their respective receptors. This can help slow down or stop the growth of the tumor and improve outcomes for patients.
Estrogens are a group of steroid hormones that are primarily responsible for the development and regulation of female sexual characteristics and reproductive functions. They are also present in lower levels in males. The main estrogen hormone is estradiol, which plays a key role in promoting the growth and development of the female reproductive system, including the uterus, fallopian tubes, and breasts. Estrogens also help regulate the menstrual cycle, maintain bone density, and have important effects on the cardiovascular system, skin, hair, and cognitive function.
Estrogens are produced primarily by the ovaries in women, but they can also be produced in smaller amounts by the adrenal glands and fat cells. In men, estrogens are produced from the conversion of testosterone, the primary male sex hormone, through a process called aromatization.
Estrogen levels vary throughout a woman's life, with higher levels during reproductive years and lower levels after menopause. Estrogen therapy is sometimes used to treat symptoms of menopause, such as hot flashes and vaginal dryness, or to prevent osteoporosis in postmenopausal women. However, estrogen therapy also carries risks, including an increased risk of certain cancers, blood clots, and stroke, so it is typically recommended only for women who have a high risk of these conditions.
Estrogen antagonists, also known as antiestrogens, are a class of drugs that block the effects of estrogen in the body. They work by binding to estrogen receptors and preventing the natural estrogen from attaching to them. This results in the inhibition of estrogen-mediated activities in various tissues, including breast and uterine tissue.
There are two main types of estrogen antagonists: selective estrogen receptor modulators (SERMs) and pure estrogen receptor downregulators (PERDS), also known as estrogen receptor downregulators (ERDs). SERMs, such as tamoxifen and raloxifene, can act as estrogen agonists or antagonists depending on the tissue type. For example, they may block the effects of estrogen in breast tissue while acting as an estrogen agonist in bone tissue, helping to prevent osteoporosis.
PERDS, such as fulvestrant, are pure estrogen receptor antagonists and do not have any estrogen-like activity. They are used primarily for the treatment of hormone receptor-positive breast cancer in postmenopausal women.
Overall, estrogen antagonists play an important role in the management of hormone receptor-positive breast cancer and other conditions where inhibiting estrogen activity is beneficial.
Androstadienes are a class of steroid hormones that are derived from androstenedione, which is a weak male sex hormone. Androstadienes include various compounds such as androstadiene-3,17-dione and androstanedione, which are intermediate products in the biosynthesis of more potent androgens like testosterone and dihydrotestosterone.
Androstadienes are present in both males and females but are found in higher concentrations in men. They can be detected in various bodily fluids, including blood, urine, sweat, and semen. In addition to their role in steroid hormone synthesis, androstadienes have been studied for their potential use as biomarkers of physiological processes and disease states.
It's worth noting that androstadienes are sometimes referred to as "androstenes" in the literature, although this term can also refer to other related compounds.
Estradiol is a type of estrogen, which is a female sex hormone. It is the most potent and dominant form of estrogen in humans. Estradiol plays a crucial role in the development and maintenance of secondary sexual characteristics in women, such as breast development and regulation of the menstrual cycle. It also helps maintain bone density, protect the lining of the uterus, and is involved in cognition and mood regulation.
Estradiol is produced primarily by the ovaries, but it can also be synthesized in smaller amounts by the adrenal glands and fat cells. In men, estradiol is produced from testosterone through a process called aromatization. Abnormal levels of estradiol can contribute to various health issues, such as hormonal imbalances, infertility, osteoporosis, and certain types of cancer.
Estrogen receptors (ERs) are a type of nuclear receptor protein that are expressed in various tissues and cells throughout the body. They play a critical role in the regulation of gene expression and cellular responses to the hormone estrogen. There are two main subtypes of ERs, ERα and ERβ, which have distinct molecular structures, expression patterns, and functions.
ERs function as transcription factors that bind to specific DNA sequences called estrogen response elements (EREs) in the promoter regions of target genes. When estrogen binds to the ER, it causes a conformational change in the receptor that allows it to recruit co-activator proteins and initiate transcription of the target gene. This process can lead to a variety of cellular responses, including changes in cell growth, differentiation, and metabolism.
Estrogen receptors are involved in a wide range of physiological processes, including the development and maintenance of female reproductive tissues, bone homeostasis, cardiovascular function, and cognitive function. They have also been implicated in various pathological conditions, such as breast cancer, endometrial cancer, and osteoporosis. As a result, ERs are an important target for therapeutic interventions in these diseases.
Estrogen receptor modulators (ERMs) are a class of medications that act on the estrogen receptors in the body. They can have mixed estrogenic and anti-estrogenic effects, depending on the target tissue. In some tissues, ERMs behave as estrogen agonists, activating the estrogen receptor and mimicking the effects of estrogen. In other tissues, they act as estrogen antagonists, blocking the effects of estrogen.
ERMs are often used in hormone replacement therapy and to treat certain types of breast cancer. Tamoxifen is a well-known example of an ERM that is commonly used to treat estrogen receptor-positive (ER+) breast cancer. It works by blocking the effects of estrogen on cancer cells, thereby slowing or stopping the growth of the tumor. Other examples of ERMs include raloxifene and toremifene.
While ERMs can be effective in treating certain conditions, they can also have side effects, including an increased risk of blood clots, hot flashes, and mood changes. It is important for individuals taking ERMs to be monitored by a healthcare provider to manage any potential side effects and ensure that the medication is working effectively.
Testolactone is a medication that is primarily used in the treatment of breast cancer. It is an oral steroidal aromatase inhibitor, which means it works by blocking the enzyme aromatase, thereby preventing the conversion of androgens into estrogens. This helps to reduce the amount of estrogen in the body, which can slow or stop the growth of certain types of breast cancer cells that need estrogen to grow.
Testolactone is not as commonly used as other aromatase inhibitors such as letrozole, anastrozole, and exemestane, but it may be prescribed in certain cases where these medications are not suitable or have not been effective. It is important to note that testolactone can have side effects, including nausea, vomiting, diarrhea, skin rash, and changes in liver function tests. As with any medication, it should only be taken under the supervision of a healthcare provider.
Adjuvant chemotherapy is a medical treatment that is given in addition to the primary therapy, such as surgery or radiation, to increase the chances of a cure or to reduce the risk of recurrence in patients with cancer. It involves the use of chemicals (chemotherapeutic agents) to destroy any remaining cancer cells that may not have been removed by the primary treatment. This type of chemotherapy is typically given after the main treatment has been completed, and its goal is to kill any residual cancer cells that may be present in the body and reduce the risk of the cancer coming back. The specific drugs used and the duration of treatment will depend on the type and stage of cancer being treated.
Selective estrogen receptor modulators (SERMs) are a class of medications that act as either agonists or antagonists on the estrogen receptors in different tissues of the body. They selectively bind to estrogen receptors and can have opposite effects depending on the target tissue. In some tissues, such as bone and liver, SERMs behave like estrogens and stimulate estrogen receptors, promoting bone formation and reducing cholesterol levels. In contrast, in other tissues, such as breast and uterus, SERMs block the effects of estrogen, acting as estrogen antagonists and preventing the growth of hormone-sensitive tumors.
Examples of SERMs include:
* Tamoxifen: used for the prevention and treatment of breast cancer in both pre- and postmenopausal women.
* Raloxifene: used for the prevention and treatment of osteoporosis in postmenopausal women, as well as for reducing the risk of invasive breast cancer in high-risk postmenopausal women.
* Toremifene: used for the treatment of metastatic breast cancer in postmenopausal women with estrogen receptor-positive tumors.
* Lasofoxifene: used for the prevention and treatment of osteoporosis in postmenopausal women, as well as reducing the risk of invasive breast cancer in high-risk postmenopausal women.
It is important to note that SERMs can have side effects, including hot flashes, vaginal dryness, and an increased risk of blood clots. The choice of a specific SERM depends on the individual patient's needs, medical history, and potential risks.
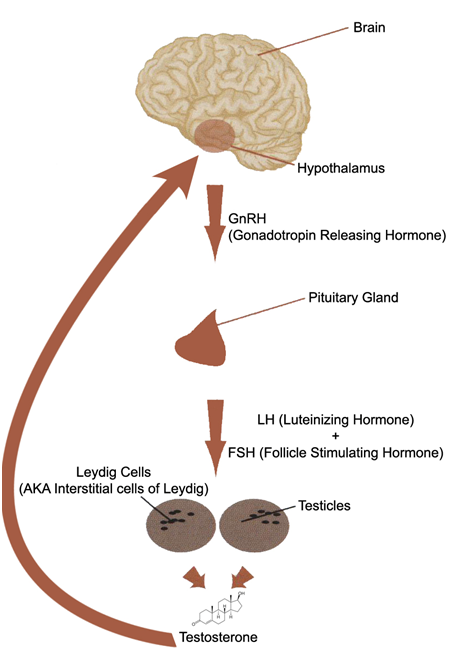
Testosterone is a steroid hormone that belongs to androsten class of hormones. It is primarily secreted by the Leydig cells in the testes of males and, to a lesser extent, by the ovaries and adrenal glands in females. Testosterone is the main male sex hormone and anabolic steroid. It plays a key role in the development of masculine characteristics, such as body hair and muscle mass, and contributes to bone density, fat distribution, red cell production, and sex drive. In females, testosterone contributes to sexual desire and bone health. Testosterone is synthesized from cholesterol and its production is regulated by luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Estrone is a type of estrogen, which is a female sex hormone. It's one of the three major naturally occurring estrogens in women, along with estradiol and estriol. Estrone is weaker than estradiol but has a longer half-life, meaning it remains active in the body for a longer period of time.
Estrone is produced primarily in the ovaries, adrenal glands, and fat tissue. In postmenopausal women, when the ovaries stop producing estradiol, estrone becomes the dominant form of estrogen. It plays a role in maintaining bone density, regulating the menstrual cycle, and supporting the development and maintenance of female sexual characteristics.
Like other forms of estrogen, estrone can also have effects on various tissues throughout the body, including the brain, heart, and breast tissue. Abnormal levels of estrone, either too high or too low, can contribute to a variety of health issues, such as osteoporosis, menstrual irregularities, and increased risk of certain types of cancer.
Gynecomastia is a medical term that refers to the benign enlargement of the glandular tissue in male breasts, usually caused by an imbalance of the hormones estrogen and testosterone. It's important to note that gynecomastia is not the same as having excess fat in the breast area, which is called pseudogynecomastia.
Gynecomastia can occur during infancy, puberty, or old age due to natural hormonal changes. Certain medications, medical conditions, and recreational drugs can also cause gynecomastia by affecting hormone levels in the body. In some cases, the exact cause of gynecomastia may remain unknown.
Mild cases of gynecomastia may not require treatment, but severe or persistent cases may be treated with medication or surgery to remove excess breast tissue. It's essential to consult a healthcare professional for an accurate diagnosis and appropriate treatment options if you suspect you have gynecomastia.
Enzyme inhibitors are substances that bind to an enzyme and decrease its activity, preventing it from catalyzing a chemical reaction in the body. They can work by several mechanisms, including blocking the active site where the substrate binds, or binding to another site on the enzyme to change its shape and prevent substrate binding. Enzyme inhibitors are often used as drugs to treat various medical conditions, such as high blood pressure, abnormal heart rhythms, and bacterial infections. They can also be found naturally in some foods and plants, and can be used in research to understand enzyme function and regulation.
Antineoplastic agents are a class of drugs used to treat malignant neoplasms or cancer. These agents work by inhibiting the growth and proliferation of cancer cells, either by killing them or preventing their division and replication. Antineoplastic agents can be classified based on their mechanism of action, such as alkylating agents, antimetabolites, topoisomerase inhibitors, mitotic inhibitors, and targeted therapy agents.
Alkylating agents work by adding alkyl groups to DNA, which can cause cross-linking of DNA strands and ultimately lead to cell death. Antimetabolites interfere with the metabolic processes necessary for DNA synthesis and replication, while topoisomerase inhibitors prevent the relaxation of supercoiled DNA during replication. Mitotic inhibitors disrupt the normal functioning of the mitotic spindle, which is essential for cell division. Targeted therapy agents are designed to target specific molecular abnormalities in cancer cells, such as mutated oncogenes or dysregulated signaling pathways.
It's important to note that antineoplastic agents can also affect normal cells and tissues, leading to various side effects such as nausea, vomiting, hair loss, and myelosuppression (suppression of bone marrow function). Therefore, the use of these drugs requires careful monitoring and management of their potential adverse effects.
Progesterone receptors (PRs) are a type of nuclear receptor proteins that are expressed in the nucleus of certain cells and play a crucial role in the regulation of various physiological processes, including the menstrual cycle, embryo implantation, and maintenance of pregnancy. These receptors bind to the steroid hormone progesterone, which is produced primarily in the ovaries during the second half of the menstrual cycle and during pregnancy.
Once progesterone binds to the PRs, it triggers a series of molecular events that lead to changes in gene expression, ultimately resulting in the modulation of various cellular functions. Progesterone receptors exist in two main isoforms, PR-A and PR-B, which differ in their size, structure, and transcriptional activity. Both isoforms are expressed in a variety of tissues, including the female reproductive tract, breast, brain, and bone.
Abnormalities in progesterone receptor expression or function have been implicated in several pathological conditions, such as uterine fibroids, endometriosis, breast cancer, and osteoporosis. Therefore, understanding the molecular mechanisms underlying PR signaling is essential for developing novel therapeutic strategies to treat these disorders.
Megestrol acetate is a synthetic progestin, which is a hormone that acts like progesterone in the body. It is used to treat various conditions such as endometrial cancer, breast cancer, and anorexia associated with AIDS. It works by blocking the action of certain hormones in the body, which can slow or stop the growth of some types of cancer cells. In addition, megestrol acetate can help increase appetite and weight gain in people with HIV/AIDS.
The medication is available in various forms, including tablets and oral suspension, and its use should be under the supervision of a healthcare professional who will determine the appropriate dosage based on the patient's medical condition and response to treatment. Common side effects of megestrol acetate include nausea, vomiting, diarrhea, gas, headache, dizziness, and changes in mood or sex drive.
Estrogen Receptor alpha (ERα) is a type of nuclear receptor protein that is activated by the hormone estrogen. It is encoded by the gene ESR1 and is primarily expressed in the cells of the reproductive system, breast, bone, liver, heart, and brain tissue.
When estrogen binds to ERα, it causes a conformational change in the receptor, which allows it to dimerize and translocate to the nucleus. Once in the nucleus, ERα functions as a transcription factor, binding to specific DNA sequences called estrogen response elements (EREs) and regulating the expression of target genes.
ERα plays important roles in various physiological processes, including the development and maintenance of female reproductive organs, bone homeostasis, and lipid metabolism. It is also a critical factor in the growth and progression of certain types of breast cancer, making ERα status an important consideration in the diagnosis and treatment of this disease.
An ovary is a part of the female reproductive system in which ova or eggs are produced through the process of oogenesis. They are a pair of solid, almond-shaped structures located one on each side of the uterus within the pelvic cavity. Each ovary measures about 3 to 5 centimeters in length and weighs around 14 grams.
The ovaries have two main functions: endocrine (hormonal) function and reproductive function. They produce and release eggs (ovulation) responsible for potential fertilization and development of an embryo/fetus during pregnancy. Additionally, they are essential in the production of female sex hormones, primarily estrogen and progesterone, which regulate menstrual cycles, sexual development, and reproduction.
During each menstrual cycle, a mature egg is released from one of the ovaries into the fallopian tube, where it may be fertilized by sperm. If not fertilized, the egg, along with the uterine lining, will be shed, leading to menstruation.
Clinical trials are research studies that involve human participants and are designed to evaluate the safety and efficacy of new medical treatments, drugs, devices, or behavioral interventions. The purpose of clinical trials is to determine whether a new intervention is safe, effective, and beneficial for patients, as well as to compare it with currently available treatments. Clinical trials follow a series of phases, each with specific goals and criteria, before a new intervention can be approved by regulatory authorities for widespread use.
Clinical trials are conducted according to a protocol, which is a detailed plan that outlines the study's objectives, design, methodology, statistical analysis, and ethical considerations. The protocol is developed and reviewed by a team of medical experts, statisticians, and ethicists, and it must be approved by an institutional review board (IRB) before the trial can begin.
Participation in clinical trials is voluntary, and participants must provide informed consent before enrolling in the study. Informed consent involves providing potential participants with detailed information about the study's purpose, procedures, risks, benefits, and alternatives, as well as their rights as research subjects. Participants can withdraw from the study at any time without penalty or loss of benefits to which they are entitled.
Clinical trials are essential for advancing medical knowledge and improving patient care. They help researchers identify new treatments, diagnostic tools, and prevention strategies that can benefit patients and improve public health. However, clinical trials also pose potential risks to participants, including adverse effects from experimental interventions, time commitment, and inconvenience. Therefore, it is important for researchers to carefully design and conduct clinical trials to minimize risks and ensure that the benefits outweigh the risks.
Androgens are a class of hormones that are primarily responsible for the development and maintenance of male sexual characteristics and reproductive function. Testosterone is the most well-known androgen, but other androgens include dehydroepiandrosterone (DHEA), androstenedione, and dihydrotestosterone (DHT).
Androgens are produced primarily by the testes in men and the ovaries in women, although small amounts are also produced by the adrenal glands in both sexes. They play a critical role in the development of male secondary sexual characteristics during puberty, such as the growth of facial hair, deepening of the voice, and increased muscle mass.
In addition to their role in sexual development and function, androgens also have important effects on bone density, mood, and cognitive function. Abnormal levels of androgens can contribute to a variety of medical conditions, including infertility, erectile dysfunction, acne, hirsutism (excessive hair growth), and prostate cancer.
Pargyline is an antihypertensive drug and a irreversible monoamine oxidase inhibitor (MAOI) of type B. It works by blocking the breakdown of certain chemicals in the brain, such as neurotransmitters, which can help improve mood and behavior in people with depression.
Pargyline is not commonly used as a first-line treatment for depression due to its potential for serious side effects, including interactions with certain foods and medications that can lead to dangerously high blood pressure. It is also associated with a risk of serotonin syndrome when taken with selective serotonin reuptake inhibitors (SSRIs) or other drugs that increase serotonin levels in the brain.
Pargyline is available only through a prescription and should be used under the close supervision of a healthcare provider.
Drug resistance in neoplasms (also known as cancer drug resistance) refers to the ability of cancer cells to withstand the effects of chemotherapeutic agents or medications designed to kill or inhibit the growth of cancer cells. This can occur due to various mechanisms, including changes in the cancer cell's genetic makeup, alterations in drug targets, increased activity of drug efflux pumps, and activation of survival pathways.
Drug resistance can be intrinsic (present at the beginning of treatment) or acquired (developed during the course of treatment). It is a significant challenge in cancer therapy as it often leads to reduced treatment effectiveness, disease progression, and poor patient outcomes. Strategies to overcome drug resistance include the use of combination therapies, development of new drugs that target different mechanisms, and personalized medicine approaches that consider individual patient and tumor characteristics.
Precocious puberty is a medical condition where the onset of sexual maturation occurs at an unusually early age, typically before the age of 8 in girls and before the age of 9 in boys. It is characterized by the development of secondary sexual characteristics such as breast development or growth of facial hair, as well as the start of menstruation in girls. This condition can be caused by various factors including central nervous system abnormalities, genetic disorders, or exposure to certain hormones. Early diagnosis and treatment are important to prevent potential negative effects on growth, bone health, and psychosocial development.
"Papio anubis" is the scientific name for the Olive Baboon, which is a species of Old World monkey found in savannas, open woodlands, and hills in East Africa. The term "Papio" refers to the genus of baboons, while "anubis" is the specific name for this particular species.
The Olive Baboon is named for its distinctive olive-gray fur, which can vary in color depending on the subspecies. They have a distinct dog-like face with a pink or red area around their mouths and noses. Adult males typically have a large, rough cheek pad on either side of their faces, which they use to display dominance during social interactions.
Olive Baboons are highly social animals that live in large troops consisting of several adult males, females, and their offspring. They have a complex social hierarchy based on age, size, and rank, and engage in various behaviors such as grooming, playing, and communication to maintain social bonds.
While "Papio anubis" is a medical or scientific term, it is not typically used in clinical settings. However, understanding the behavior and ecology of primates like Olive Baboons can provide valuable insights into human evolution, behavior, and disease transmission.
A hot flash is a sudden, intense feeling of heat, particularly in the face, neck and chest regions, which is often accompanied by perspiration, reddening of the skin (flush or blush), and rapid heartbeat. It is a common symptom experienced by individuals, especially women during menopause or perimenopause, although it can also occur in other medical conditions or as a side effect of certain medications. The exact cause of hot flashes is not fully understood, but they are thought to be related to changes in hormone levels and the body's regulation of temperature.
Arthralgia is a medical term that refers to pain in the joints. It does not involve inflammation, which would be referred to as arthritis. The pain can range from mild to severe and may occur in one or multiple joints. Arthralgia can have various causes, including injuries, infections, degenerative conditions, or systemic diseases. In some cases, the underlying cause of arthralgia remains unknown. Treatment typically focuses on managing the pain and addressing the underlying condition if it can be identified.
Dihydrotestosterone (DHT) is a sex hormone and androgen that plays a critical role in the development and maintenance of male characteristics, such as facial hair, deep voice, and muscle mass. It is synthesized from testosterone through the action of the enzyme 5-alpha reductase. DHT is essential for the normal development of the male genitalia during fetal development and for the maturation of the sexual organs at puberty.
In addition to its role in sexual development, DHT also contributes to the growth of hair follicles, the health of the prostate gland, and the maintenance of bone density. However, an excess of DHT has been linked to certain medical conditions, such as benign prostatic hyperplasia (BPH) and androgenetic alopecia (male pattern baldness).
DHT exerts its effects by binding to androgen receptors in various tissues throughout the body. Once bound, DHT triggers a series of cellular responses that regulate gene expression and influence the growth and differentiation of cells. In some cases, these responses can lead to unwanted side effects, such as hair loss or prostate enlargement.
Medications that block the action of 5-alpha reductase, such as finasteride and dutasteride, are sometimes used to treat conditions associated with excess DHT production. These drugs work by reducing the amount of DHT available to bind to androgen receptors, thereby alleviating symptoms and slowing disease progression.
In summary, dihydrotestosterone is a potent sex hormone that plays a critical role in male sexual development and function. While it is essential for normal growth and development, an excess of DHT has been linked to certain medical conditions, such as BPH and androgenetic alopecia. Medications that block the action of 5-alpha reductase are sometimes used to treat these conditions by reducing the amount of DHT available to bind to androgen receptors.
Endometriosis is a medical condition in which tissue similar to the lining of the uterus (endometrium) grows outside the uterine cavity, most commonly on the ovaries, fallopian tubes, and the pelvic peritoneum. This misplaced endometrial tissue continues to act as it would inside the uterus, thickening, breaking down, and bleeding with each menstrual cycle. However, because it is outside the uterus, this blood and tissue have no way to exit the body and can lead to inflammation, scarring, and the formation of adhesions (tissue bands that bind organs together).
The symptoms of endometriosis may include pelvic pain, heavy menstrual periods, painful intercourse, and infertility. The exact cause of endometriosis is not known, but several theories have been proposed, including retrograde menstruation (the backflow of menstrual blood through the fallopian tubes into the pelvic cavity), genetic factors, and immune system dysfunction.
Endometriosis can be diagnosed through a combination of methods, such as medical history, physical examination, imaging tests like ultrasound or MRI, and laparoscopic surgery with tissue biopsy. Treatment options for endometriosis include pain management, hormonal therapies, and surgical intervention to remove the misplaced endometrial tissue. In severe cases, a hysterectomy (removal of the uterus) may be recommended, but this is typically considered a last resort due to its impact on fertility and quality of life.
Musculoskeletal pain is discomfort or pain that affects the muscles, bones, ligaments, tendons, and nerves. It can be caused by injury, overuse, or disease and can affect any part of the body, including the neck, back, shoulders, hips, and extremities. The pain can range from mild to severe and may be accompanied by stiffness, swelling, and decreased range of motion. Common causes of musculoskeletal pain include arthritis, fibromyalgia, tendinitis, bursitis, and muscle or ligament strain. Treatment for musculoskeletal pain depends on the underlying cause and may include physical therapy, medication, and in some cases, surgery.
"Sex differentiation" is a term used in the field of medicine, specifically in reproductive endocrinology and genetics. It refers to the biological development of sexual characteristics that distinguish males from females. This process is regulated by hormones and genetic factors.
There are two main stages of sex differentiation: genetic sex determination and gonadal sex differentiation. Genetic sex determination occurs at fertilization, where the combination of X and Y chromosomes determines the sex of the individual (typically, XX = female and XY = male). Gonadal sex differentiation then takes place during fetal development, where the genetic sex signals the development of either ovaries or testes.
Once the gonads are formed, they produce hormones that drive further sexual differentiation, leading to the development of internal reproductive structures (such as the uterus and fallopian tubes in females, and the vas deferens and seminal vesicles in males) and external genitalia.
It's important to note that while sex differentiation is typically categorized as male or female, there are individuals who may have variations in their sexual development, leading to intersex conditions. These variations can occur at any stage of the sex differentiation process and can result in a range of physical characteristics that do not fit neatly into male or female categories.
Follicle-Stimulating Hormone (FSH) is a glycoprotein hormone secreted and released by the anterior pituitary gland. In females, it promotes the growth and development of ovarian follicles in the ovary, which ultimately leads to the maturation and release of an egg (ovulation). In males, FSH stimulates the testes to produce sperm. It works in conjunction with luteinizing hormone (LH) to regulate reproductive processes. The secretion of FSH is controlled by the hypothalamic-pituitary-gonadal axis and its release is influenced by the levels of gonadotropin-releasing hormone (GnRH), estrogen, inhibin, and androgens.
Ovariectomy is a surgical procedure in which one or both ovaries are removed. It is also known as "ovary removal" or "oophorectomy." This procedure is often performed as a treatment for various medical conditions, including ovarian cancer, endometriosis, uterine fibroids, and pelvic pain. Ovariectomy can also be part of a larger surgical procedure called an hysterectomy, in which the uterus is also removed.
In some cases, an ovariectomy may be performed as a preventative measure for individuals at high risk of developing ovarian cancer. This is known as a prophylactic ovariectomy. After an ovariectomy, a person will no longer have menstrual periods and will be unable to become pregnant naturally. Hormone replacement therapy may be recommended in some cases to help manage symptoms associated with the loss of hormones produced by the ovaries.
Clomiphene is a medication that is primarily used to treat infertility in women. It is an ovulatory stimulant, which means that it works by stimulating the development and release of mature eggs from the ovaries (a process known as ovulation). Clomiphene is a selective estrogen receptor modulator (SERM), which means that it binds to estrogen receptors in the body and blocks the effects of estrogen in certain tissues, while enhancing the effects of estrogen in others.
In the ovary, clomiphene works by blocking the negative feedback effect of estrogen on the hypothalamus and pituitary gland, which results in an increase in the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These hormones stimulate the growth and development of ovarian follicles, which contain eggs. As the follicles grow and mature, they produce increasing amounts of estrogen, which eventually triggers a surge in LH that leads to ovulation.
Clomiphene is typically taken orally for 5 days, starting on the 3rd, 4th, or 5th day of the menstrual cycle. The dosage may be adjusted based on the patient's response to treatment. Common side effects of clomiphene include hot flashes, mood changes, breast tenderness, and ovarian hyperstimulation syndrome (OHSS), which is a potentially serious complication characterized by the enlargement of the ovaries and the accumulation of fluid in the abdomen.
It's important to note that clomiphene may not be suitable for everyone, and its use should be carefully monitored by a healthcare provider. Women with certain medical conditions, such as liver disease, thyroid disorders, or uterine fibroids, may not be able to take clomiphene. Additionally, women who become pregnant while taking clomiphene have an increased risk of multiple pregnancies (e.g., twins or triplets), which can pose additional risks to both the mother and the fetuses.
Bone density conservation agents, also known as anti-resorptive agents or bone-sparing drugs, are a class of medications that help to prevent the loss of bone mass and reduce the risk of fractures. They work by inhibiting the activity of osteoclasts, the cells responsible for breaking down and reabsorbing bone tissue during the natural remodeling process.
Examples of bone density conservation agents include:
1. Bisphosphonates (e.g., alendronate, risedronate, ibandronate, zoledronic acid) - These are the most commonly prescribed class of bone density conservation agents. They bind to hydroxyapatite crystals in bone tissue and inhibit osteoclast activity, thereby reducing bone resorption.
2. Denosumab (Prolia) - This is a monoclonal antibody that targets RANKL (Receptor Activator of Nuclear Factor-κB Ligand), a key signaling molecule involved in osteoclast differentiation and activation. By inhibiting RANKL, denosumab reduces osteoclast activity and bone resorption.
3. Selective estrogen receptor modulators (SERMs) (e.g., raloxifene) - These medications act as estrogen agonists or antagonists in different tissues. In bone tissue, SERMs mimic the bone-preserving effects of estrogen by inhibiting osteoclast activity and reducing bone resorption.
4. Hormone replacement therapy (HRT) - Estrogen hormone replacement therapy has been shown to preserve bone density in postmenopausal women; however, its use is limited due to increased risks of breast cancer, cardiovascular disease, and thromboembolic events.
5. Calcitonin - This hormone, secreted by the thyroid gland, inhibits osteoclast activity and reduces bone resorption. However, it has largely been replaced by other more effective bone density conservation agents.
These medications are often prescribed for individuals at high risk of fractures due to conditions such as osteoporosis or metabolic disorders that affect bone health. It is essential to follow the recommended dosage and administration guidelines to maximize their benefits while minimizing potential side effects. Regular monitoring of bone density, blood calcium levels, and other relevant parameters is also necessary during treatment with these medications.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Neoadjuvant therapy is a treatment regimen that is administered to patients before they undergo definitive or curative surgery for their cancer. The main goal of neoadjuvant therapy is to reduce the size and extent of the tumor, making it easier to remove surgically and increasing the likelihood of complete resection. This type of therapy often involves the use of chemotherapy, radiation therapy, or targeted therapy, and it can help improve treatment outcomes by reducing the risk of recurrence and improving overall survival rates. Neoadjuvant therapy is commonly used in the treatment of various types of cancer, including breast, lung, esophageal, rectal, and bladder cancer.
Gonads are the reproductive organs that produce gametes (sex cells) and sex hormones. In males, the gonads are the testes, which produce sperm and testosterone. In females, the gonads are the ovaries, which produce eggs and estrogen and progesterone. The development, function, and regulation of the gonads are crucial for reproductive health and fertility.
Estrogen Receptor beta (ER-β) is a protein that is encoded by the gene ESR2 in humans. It belongs to the family of nuclear receptors, which are transcription factors that regulate gene expression in response to hormonal signals. ER-β is one of two main estrogen receptors, the other being Estrogen Receptor alpha (ER-α), and it plays an important role in mediating the effects of estrogens in various tissues, including the breast, uterus, bone, brain, and cardiovascular system.
Estrogens are steroid hormones that play a critical role in the development and maintenance of female reproductive and sexual function. They also have important functions in other tissues, such as maintaining bone density and promoting cognitive function. ER-β is widely expressed in many tissues, including those outside of the reproductive system, suggesting that it may have diverse physiological roles beyond estrogen-mediated reproduction.
ER-β has been shown to have both overlapping and distinct functions from ER-α, and its expression patterns differ between tissues. For example, in the breast, ER-β is expressed at higher levels in normal tissue compared to cancerous tissue, suggesting that it may play a protective role against breast cancer development. In contrast, in the uterus, ER-β has been shown to have anti-proliferative effects and may protect against endometrial cancer.
Overall, ER-β is an important mediator of estrogen signaling and has diverse physiological roles in various tissues. Understanding its functions and regulation may provide insights into the development of novel therapies for a range of diseases, including cancer, osteoporosis, and cardiovascular disease.
Gonadotropins are hormones that stimulate the gonads (sex glands) to produce sex steroids and gametes (sex cells). In humans, there are two main types of gonadotropins: follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which are produced and released by the anterior pituitary gland.
FSH plays a crucial role in the development and maturation of ovarian follicles in females and sperm production in males. LH triggers ovulation in females, causing the release of a mature egg from the ovary, and stimulates testosterone production in males.
Gonadotropins are often used in medical treatments to stimulate the gonads, such as in infertility therapies where FSH and LH are administered to induce ovulation or increase sperm production.
Luteinizing Hormone (LH) is a glycoprotein hormone, which is primarily produced and released by the anterior pituitary gland. In women, a surge of LH triggers ovulation, the release of an egg from the ovaries during the menstrual cycle. During pregnancy, LH stimulates the corpus luteum to produce progesterone. In men, LH stimulates the testes to produce testosterone. It plays a crucial role in sexual development, reproduction, and maintaining the reproductive system.
"ErbB-2" is also known as "HER2" or "human epidermal growth factor receptor 2." It is a type of receptor tyrosine kinase (RTK) found on the surface of some cells. ErbB-2 does not bind to any known ligands, but it can form heterodimers with other ErbB family members, such as ErbB-3 and ErbB-4, which do have identified ligands. When a ligand binds to one of these receptors, it causes a conformational change that allows the ErbB-2 receptor to become activated through transphosphorylation. This activation triggers a signaling cascade that regulates cell growth, differentiation, and survival.
Overexpression or amplification of the ERBB2 gene, which encodes the ErbB-2 protein, is observed in approximately 20-30% of breast cancers and is associated with a more aggressive disease phenotype and poorer prognosis. Therefore, ErbB-2 has become an important target for cancer therapy, and several drugs that target this receptor have been developed, including trastuzumab (Herceptin), lapatinib (Tykerb), and pertuzumab (Perjeta).
A randomized controlled trial (RCT) is a type of clinical study in which participants are randomly assigned to receive either the experimental intervention or the control condition, which may be a standard of care, placebo, or no treatment. The goal of an RCT is to minimize bias and ensure that the results are due to the intervention being tested rather than other factors. This design allows for a comparison between the two groups to determine if there is a significant difference in outcomes. RCTs are often considered the gold standard for evaluating the safety and efficacy of medical interventions, as they provide a high level of evidence for causal relationships between the intervention and health outcomes.
'Mammary neoplasms, experimental' is not a recognized medical term. However, I can provide definitions for the individual terms:
1. Mammary: Pertaining to the breast or mammary glands in females, which are responsible for milk production.
2. Neoplasms: Abnormal growths of tissue, also known as tumors or masses, that can be benign (non-cancerous) or malignant (cancerous).
3. Experimental: Relating to a scientific experiment or study, typically conducted in a controlled setting to test hypotheses and gather data.
In the context of medical research, 'experimental mammary neoplasms' may refer to artificially induced breast tumors in laboratory animals (such as rats or mice) for the purpose of studying the development, progression, treatment, and prevention of breast cancer. These studies can help researchers better understand the biology of breast cancer and develop new therapies and strategies for its diagnosis and management.
Ovulation induction is a medical procedure that involves the stimulation of ovulation (the release of an egg from the ovaries) in women who have difficulties conceiving due to ovulatory disorders. This is typically achieved through the use of medications such as clomiphene citrate or gonadotropins, which promote the development and maturation of follicles in the ovaries containing eggs. The process is closely monitored through regular ultrasounds and hormone tests to ensure appropriate response and minimize the risk of complications like multiple pregnancies. Ovulation induction may be used as a standalone treatment or in conjunction with other assisted reproductive technologies (ART), such as intrauterine insemination (IUI) or in vitro fertilization (IVF).
The placenta is an organ that develops in the uterus during pregnancy and provides oxygen and nutrients to the growing baby through the umbilical cord. It also removes waste products from the baby's blood. The placenta attaches to the wall of the uterus, and the baby's side of the placenta contains many tiny blood vessels that connect to the baby's circulatory system. This allows for the exchange of oxygen, nutrients, and waste between the mother's and baby's blood. After the baby is born, the placenta is usually expelled from the uterus in a process called afterbirth.
Delayed puberty is a condition where the typical physical changes of puberty, such as the development of secondary sexual characteristics, growth spurt, and fertility, do not begin to occur during the expected age range. In medical terms, delayed puberty is defined as the absence of signs of puberty by age 13 in girls (such as breast development or menstruation) and by age 14 in boys (such as testicular enlargement or growth of facial hair).
There are various factors that can contribute to delayed puberty, including genetic conditions, chronic illnesses, hormonal imbalances, eating disorders, and excessive exercise. In some cases, the cause may be unknown. Delayed puberty can have significant emotional and social consequences for affected individuals, so it is important to seek medical evaluation and treatment if there are concerns about delayed puberty. Treatment options may include hormone replacement therapy or other interventions to support normal pubertal development.
Fibrous Dysplasia, Polyostotic is a rare genetic disorder that affects the bone tissue. It is characterized by the replacement of normal bone tissue with fibrous (scar-like) tissue, leading to weak and fragile bones that are prone to fractures and deformities. The term "polyostotic" refers to the involvement of multiple bones in the body.
In this condition, there is an abnormal development of the bone during fetal growth or early childhood due to a mutation in the GNAS gene. This results in the formation of fibrous tissue instead of normal bone tissue, leading to the characteristic features of Fibrous Dysplasia, Polyostotic.
The symptoms of this condition can vary widely depending on the severity and location of the affected bones. Common symptoms include:
* Bone pain and tenderness
* Bone deformities (such as bowing of the legs)
* Increased risk of fractures
* Skin pigmentation changes (cafe-au-lait spots)
* Hearing loss or other hearing problems (if the skull is affected)
Fibrous Dysplasia, Polyostotic can also be associated with endocrine disorders such as precocious puberty and hyperthyroidism. Treatment typically involves a combination of medications to manage pain and prevent fractures, as well as surgical intervention to correct bone deformities or stabilize fractures.
Uterine diseases refer to a range of medical conditions that affect the uterus, which is the reproductive organ in females where fetal development occurs. These diseases can be categorized into structural abnormalities, infectious diseases, and functional disorders. Here are some examples:
1. Structural abnormalities: These include congenital malformations such as septate uterus or bicornuate uterus, as well as acquired conditions like endometrial polyps, fibroids (benign tumors of the muscular wall), and adenomyosis (where the endometrial tissue grows into the muscular wall).
2. Infectious diseases: The uterus can be affected by various infections, including bacterial, viral, fungal, or parasitic agents. Examples include pelvic inflammatory disease (PID), tuberculosis, and candidiasis.
3. Functional disorders: These are conditions that affect the normal functioning of the uterus without any apparent structural abnormalities or infections. Examples include dysmenorrhea (painful periods), menorrhagia (heavy periods), and endometriosis (where the endometrial tissue grows outside the uterus).
4. Malignant diseases: Uterine cancer, including endometrial cancer and cervical cancer, are significant health concerns for women.
5. Other conditions: Miscarriage, ectopic pregnancy, and infertility can also be considered as uterine diseases since they involve the abnormal functioning or structural issues of the uterus.
Steroids, also known as corticosteroids, are a type of hormone that the adrenal gland produces in your body. They have many functions, such as controlling the balance of salt and water in your body and helping to reduce inflammation. Steroids can also be synthetically produced and used as medications to treat a variety of conditions, including allergies, asthma, skin conditions, and autoimmune disorders.
Steroid medications are available in various forms, such as oral pills, injections, creams, and inhalers. They work by mimicking the effects of natural hormones produced by your body, reducing inflammation and suppressing the immune system's response to prevent or reduce symptoms. However, long-term use of steroids can have significant side effects, including weight gain, high blood pressure, osteoporosis, and increased risk of infections.
It is important to note that anabolic steroids are a different class of drugs that are sometimes abused for their muscle-building properties. These steroids are synthetic versions of the male hormone testosterone and can have serious health consequences when taken in large doses or without medical supervision.
Diphosphonates are a class of medications that are used to treat bone diseases, such as osteoporosis and Paget's disease. They work by binding to the surface of bones and inhibiting the activity of bone-resorbing cells called osteoclasts. This helps to slow down the breakdown and loss of bone tissue, which can help to reduce the risk of fractures.
Diphosphonates are typically taken orally in the form of tablets, but some forms may be given by injection. Commonly prescribed diphosphonates include alendronate (Fosamax), risedronate (Actonel), and ibandronate (Boniva). Side effects of diphosphonates can include gastrointestinal symptoms such as nausea, heartburn, and abdominal pain. In rare cases, they may also cause esophageal ulcers or osteonecrosis of the jaw.
It is important to follow the instructions for taking diphosphonates carefully, as they must be taken on an empty stomach with a full glass of water and the patient must remain upright for at least 30 minutes after taking the medication to reduce the risk of esophageal irritation. Regular monitoring of bone density and kidney function is also recommended while taking these medications.
The double-blind method is a study design commonly used in research, including clinical trials, to minimize bias and ensure the objectivity of results. In this approach, both the participants and the researchers are unaware of which group the participants are assigned to, whether it be the experimental group or the control group. This means that neither the participants nor the researchers know who is receiving a particular treatment or placebo, thus reducing the potential for bias in the evaluation of outcomes. The assignment of participants to groups is typically done by a third party not involved in the study, and the codes are only revealed after all data have been collected and analyzed.
A "Drug Administration Schedule" refers to the plan for when and how a medication should be given to a patient. It includes details such as the dose, frequency (how often it should be taken), route (how it should be administered, such as orally, intravenously, etc.), and duration (how long it should be taken) of the medication. This schedule is often created and prescribed by healthcare professionals, such as doctors or pharmacists, to ensure that the medication is taken safely and effectively. It may also include instructions for missed doses or changes in the dosage.
Bone density refers to the amount of bone mineral content (usually measured in grams) in a given volume of bone (usually measured in cubic centimeters). It is often used as an indicator of bone strength and fracture risk. Bone density is typically measured using dual-energy X-ray absorptiometry (DXA) scans, which provide a T-score that compares the patient's bone density to that of a young adult reference population. A T-score of -1 or above is considered normal, while a T-score between -1 and -2.5 indicates osteopenia (low bone mass), and a T-score below -2.5 indicates osteoporosis (porous bones). Regular exercise, adequate calcium and vitamin D intake, and medication (if necessary) can help maintain or improve bone density and prevent fractures.
Cyprinidae is a family of fish that includes carps, minnows, and barbs. It is the largest family of freshwater fish, with over 2,400 species found worldwide, particularly in Asia and Europe. These fish are characterized by their lack of teeth on the roof of their mouths and have a single dorsal fin. Some members of this family are economically important as food fish or for aquarium trade.
 Non steroidal aromatase inhibitors
Non steroidal aromatase inhibitors
Aromatase inhibitor
Steroidal aromatase inhibitor
Aromatase
Aminoglutethimide
Aromatization
Angela Hartley Brodie
Gynecomastia
Gilles-Éric Séralini
Chalconoid
Endometriosis
Minamestane
Exemestane
Rogletimide
Antiestrogen
Comparison of bicalutamide with other antiandrogens
Bicalutamide
Medical uses of bicalutamide
Hypoestrogenism
Testolactone
Finrozole
Breast cancer
Letrozole
Selective estrogen receptor degrader
Brassaiopsis glomerulata
Ketoconazole
Amenorrhea
Leiomyosarcoma
Kathleen I. Pritchard
Bifonazole
Non steroidal aromatase inhibitors - Wikipedia
 Aromatase Inhibitors: Benefits, Side Effects, and More
Aromatase Inhibitors: Benefits, Side Effects, and More
 Aromatase inhibitors for short stature in male children and adolescents
Aromatase inhibitors for short stature in male children and adolescents
 Aromatase Inhibitors
Aromatase Inhibitors
 FORCE | Acupressure to Self-Manage Aromatase Inhibitor Musculoskeletal Symptoms in Breast Cancer Survivors
FORCE | Acupressure to Self-Manage Aromatase Inhibitor Musculoskeletal Symptoms in Breast Cancer Survivors
 aromatase inhibitor - Naturopathic Doctor News and Review
aromatase inhibitor - Naturopathic Doctor News and Review
 Aromatase inhibitors increased risk of heart disease in postmenopausal women with breast cancer | health.am
Aromatase inhibitors increased risk of heart disease in postmenopausal women with breast cancer | health.am
 Coping with Aromatase Inhibitors and Tamoxifen Support Group - New York | SHARE Cancer Support
Coping with Aromatase Inhibitors and Tamoxifen Support Group - New York | SHARE Cancer Support
 Patricia A. Ganz, MD: Aromatase Inhibitors Data Review - The ASCO Post
Patricia A. Ganz, MD: Aromatase Inhibitors Data Review - The ASCO Post
 Anyone stop Aromatase Inhibitor - Stage 4 HER2+/E+ - Breastcancer.org
Anyone stop Aromatase Inhibitor - Stage 4 HER2+/E+ - Breastcancer.org
 Aromatase inhibitors help women react better to strength training - IronMag Bodybuilding & Fitness Blog
Aromatase inhibitors help women react better to strength training - IronMag Bodybuilding & Fitness Blog
 RACGP - Bone loss associated with aromatase inhibitor therapy for breast cancer and androgen deprivation therapy for prostate...
RACGP - Bone loss associated with aromatase inhibitor therapy for breast cancer and androgen deprivation therapy for prostate...
 Surviving & Thriving on Aromatase Inhibitors | Breast Cancer Coalition of Rochester
Surviving & Thriving on Aromatase Inhibitors | Breast Cancer Coalition of Rochester
New structure-activity relationships of A-and D-ring modified steroidal aromatase inhibitors: Design, synthesis, and...
Cognitive complaints during breast cancer endocrine therapy: aromatase inhibitors versus tamoxifen | BMJ Supportive &...
 Femara / Letrozole / Dragon Pharma Aromatase Inhibitor
Femara / Letrozole / Dragon Pharma Aromatase Inhibitor
 Aromatase Inhibitor I - CAS 331684-05-0 - Calbiochem | 182540
Aromatase Inhibitor I - CAS 331684-05-0 - Calbiochem | 182540
 Studies on the effects of aromatase inhibitors in model systems for breast cancer
Studies on the effects of aromatase inhibitors in model systems for breast cancer
 Aromatase Inhibitor - Lifeology
Aromatase Inhibitor - Lifeology
 aromatase inhibitor Archives » MENELITE
aromatase inhibitor Archives » MENELITE
 Breast Cancer Pharmacogenomics of Aromatase Inhibitors | 50120
Breast Cancer Pharmacogenomics of Aromatase Inhibitors | 50120
Vaginal Estrogen Not Recommended With Aromatase Inhibitors - Zonamedica
 FEMAMED 2.5 Aromatase Inhibitor | Deus Medical
FEMAMED 2.5 Aromatase Inhibitor | Deus Medical
Anastrox / Anastrozole / Zerox Pharmaceuticals Aromatase Inhibitor
 Hormone Therapy - Chemocare
Hormone Therapy - Chemocare
Lymphangioleiomyomatosis Medication: Immunosuppressant agents, Antimalarials, Aminoquinoline, Antineoplastics, Aromatase...
 Survival Outcomes Following Palbociclib Plus Aromatase Inhibitor Therapy in HR+/HER2− Metastatic Breast Cancer | PracticeUpdate
Survival Outcomes Following Palbociclib Plus Aromatase Inhibitor Therapy in HR+/HER2− Metastatic Breast Cancer | PracticeUpdate
 Aromatase inhibitors (anastrozole, exemestane and letrozole) | Breast Cancer Now
Aromatase inhibitors (anastrozole, exemestane and letrozole) | Breast Cancer Now
 7Lab Pharm PCT Products for Sale: Aromatase Inhibitors, SERMs
7Lab Pharm PCT Products for Sale: Aromatase Inhibitors, SERMs
 aromatase inhibitors - Weekly Wilson - Blog of Author Connie C. Wilson
aromatase inhibitors - Weekly Wilson - Blog of Author Connie C. Wilson
Tamoxifen13
- Among postmenopausal women with hormone receptor-positive breast cancer, aromatase inhibitors (alone or after tamoxifen) offer the same or slightly greater benefit compared to tamoxifen alone [ 88,105-108 ]. (komen.org)
- When an aromatase inhibitor is taken after tamoxifen, the drugs are taken for a combined total of 5-10 years. (komen.org)
- Tamoxifen blocks the effect of estrogen in breast tissue, whereas aromatase inhibitors prevent the production of estrogen. (health.am)
- The researchers examined data from seven large randomized clinical trials that compared tamoxifen with aromatase inhibitors in postmenopausal women with early-stage breast cancer. (health.am)
- As a secondary analysis, they determined if switching from treatment with tamoxifen to aromatase inhibitors had any effect on mortality or adverse effects. (health.am)
- Results showed that the risk for serious adverse effects were similar when aromatase inhibitors were used as an initial treatment compared with switching to aromatase inhibitors after treatment with tamoxifen. (health.am)
- This support group is for women who are currently taking aromatase inhibitors or tamoxifen, as well as for those trying to decide whether or not to take them. (sharecancersupport.org)
- Objective Previous data hypothesise that women receiving aromatase inhibitors (AIs) exhibit worse cognitive functioning than patients on tamoxifen (TAM) since their oestrogen levels are lower. (bmj.com)
- Men with breast cancer may be given an aromatase inhibitor, although another drug called tamoxifen is more commonly used. (breastcancernow.org)
- Women who have completed a full 5-year course of tamoxifen may also benefit from aromatase inhibitor treatment as indicated by the MA 17 trial, which investigated letrozole as extended adjuvant therapy. (openrepository.com)
- Fulvestrant is effective in tamoxifen-resistant disease, and phase II trial data suggest that fulvestrant may also be effective following aromatase inhibitor failure. (openrepository.com)
- We compared the antitumor activity of Z-endoxifen with tamoxifen and letrozole in the letrozole-sensitive MCF7 aromatase expressing model (MCF7AC1), as well as with tamoxifen, fulvestrant, exemestane, and exemestane plus everolimus in a letrozole-resistant MCF7 model (MCF7LR). (biomedcentral.com)
- In endocrine-sensitive and letrozole-resistant breast tumors, Z-endoxifen results in robust antitumor and antiestrogenic activity compared to tamoxifen and aromatase inhibitor monotherapy. (biomedcentral.com)
Anastrozole6
- On the other hand, in December 2008, the Food and Drug Administration added a warning label to anastrozole, an aromatase inhibitor, which indicated potential increased risk for heart disease. (health.am)
- Ultimately, I had to discontinue taking Anastrozole or any other aromatase inhibitor. (weeklywilson.com)
- Exemestane and anastrozole are aromatase inhibitor drugs. (komen.org)
- Learn about aromatase inhibitors (including exemestane and anastrozole) and breast cancer treatment . (komen.org)
- We assessed the efficacy and safety of the aromatase inhibitor anastrozole for prevention of breast cancer in postmenopausal women who are at high risk of the disease. (nih.gov)
- A triazole and benzonitrile derivative that is a selective non-steroidal aromatase inhibitor, similar to ANASTROZOLE. (bvsalud.org)
Letrozole3
- Letrozole stops the activity of Aromatase, which consequently prevents estrogen formation, leading to a slowing down or reversal of breast cancer growth. (deusmedical.com)
- Letrozole is an aromatase inhibitor with antiestrogenic effects that is being tested in LAM. (medscape.com)
- The aromatase inhibitor drug letrozole (Femara) is under study to see whether it lowers breast cancer risk in postmenopausal women at high risk. (komen.org)
Enzyme17
- NSAIs binding is a reversible process where NSAIs binds to the aromatase enzyme through non-covalent interactions. (wikipedia.org)
- When aromatase inhibitors (AIs) are used to treat breast cancer the main target is the aromatase enzyme which is responsible for the high estrogen level. (wikipedia.org)
- AIs inhibit the enzyme aromatase that converts testosterone to estrogen and that is used clinically in treatments of breast cancer in postmenopausal women. (wikipedia.org)
- Aromatase is an enzyme that belongs to the cytochrome P450 family located on chromosome 15. (wikipedia.org)
- The active binding site of the aromatase enzyme is a subunit with a heme moiety (Fe2+). (wikipedia.org)
- The binding of the NSAIs depends on the binding site of the aromatase as it has to fit into the substrate-binding site of the aromatase enzyme. (wikipedia.org)
- Aromatase inhibitors lower estrogen levels in the body by blocking aromatase, an enzyme that converts other hormones into estrogen. (komen.org)
- In JEG-3 cells which express aromatase, these inhibitors showed different effects on the enzyme. (umaryland.edu)
- Although all inhibited aromatase activity competitively, pretreatment with 4-OHA induced profound and sustained inhibition (inactivation of the enzyme) via an irreversible interaction at the active site. (umaryland.edu)
- Aromatase inhibitors block the enzyme aromatase (found in the body's muscle, skin, breast and fat), which is used to convert androgens (hormones produced by the adrenal glands) into estrogen. (chemocare.com)
- Aromatase is an enzyme that helps in the production of estrogen. (deusmedical.com)
- It is a nonsteroidal competitive inhibitor of the aromatase enzyme system. (medscape.com)
- This process involves an enzyme (a type of protein) called aromatase. (breastcancernow.org)
- Aromatase inhibitors stop this enzyme from working. (breastcancernow.org)
- It uses a naturally occurring enzyme called aromatase to convert testosterone into estrogen. (elitehealthonline.com)
- The best way to stop your body from turning testosterone to estrogen is to block the aromatase enzyme. (elitehealthonline.com)
- Another family of drugs which act to reduce hormone levels are the medicines known as aromatase inhibitors (these drugs work by blocking the aromatase enzyme reducing the amount of oestrogen in the body). (healthtalk.org)
Combination with an aromatase inhibitor1
- Biocon Biologics Ltd), BT-ON014 - in combination with docetaxel for the treatment of those patients who have not received chemotherapy for their metastatic disease - in combination with an aromatase inhibitor for the treatment of postmenopausal patients with hormone-receptor positive MBC, not previously treated with trastuzumab. (who.int)
Antiestrogen2
- While antiestrogen therapy has become an accepted practice, clinical utilization of selective aromatase (estrogen synthetase) inhibitor only began in the last few years. (umaryland.edu)
- Tumors developed from the cells and their growth was dependent on estrogen synthesized by intratumoral aromatization of supplemented {dollar}\Delta\sp4{dollar}A. Both aromatase inhibitors and antiestrogen inhibited tumor growth. (umaryland.edu)
Take aromatase inhibitors2
Steroidal aromatase inhibitors2
- Non-Steroidal Aromatase Inhibitors (NSAIs) are one of two categories of aromatase inhibitors (AIs). (wikipedia.org)
- AIs are divided into two categories, steroidal aromatase inhibitors (SAIs, type 1 inhibitors) and non-steroidal aromatase inhibitors (type 2 inhibitors) that is based on their mechanism of action and structure. (wikipedia.org)
Musculoskeletal3
- Aromatase inhibitor musculoskeletal symptoms have a negative effect on a woman's physical function and quality of life. (facingourrisk.org)
- Patricia A. Ganz, MD , of the UCLA Jonsson Comprehensive Cancer Center, summarizes two studies on using duloxetine for aromatase inhibitor-associated musculoskeletal symptoms, and aromatase inhibitors' effect on endothelial function and heart disease (Abstracts S5-06 and S5-07). (ascopost.com)
- Musculoskeletal adverse events (MSAEs) and vasomotor symptoms (VMSs) are known side-effects of aromatase inhibitors, and may be related to genetic variations of the aromatase gene (CYP19A1). (eur.nl)
Potent aromatase2
- With the exception of acute phase reactant fibrinogen, this study did not identify an increase in parameters associated with cardiovascular disease in women treated with fadrozole, a potent aromatase inhibitor. (psu.edu)
- We conclude that the recently developed potent aromatase inhibitors are candidate drugs in the treatment of endometriosis that is resistant to standard regimens. (elsevierpure.com)
Adjuvant2
- SUMMARY: The introduction of the third-generation aromatase inhibitors has caused a paradigm shift in adjuvant endocrine treatment. (openrepository.com)
- Benefit with aromatase inhibitors in the adjuvant setting for postmenopausal women with breast cancer. (openrepository.com)
Endocrine2
- Aromatase inhibitors are a hormone therapy (also called endocrine therapy). (komen.org)
- This review was prompted by a wealth of new data on several newer endocrine agents, including selective oestrogen receptor modulators, aromatase inhibitors and a new oestrogen receptor antagonist, fulvestrant, which unlike the selective oestrogen receptor modulators has no oestrogen agonist effects. (openrepository.com)
Selective3
- Hormonal therapies including SERMs (selective estrogen receptor modulators) as well as aromatase inhibitors (AIs) are the two major classes of drugs that are widely used to treat ER+ disease. (interesjournals.org)
- Selective oestrogen receptor modulators, aromatase inhibitors and the female breast. (openrepository.com)
- Where do selective estrogen receptor modulators (SERMs) and aromatase inhibitors (AIs) now fit into breast cancer treatment algorithms? (openrepository.com)
Metastatic breast cancer1
- Learn about aromatase inhibitors and other hormone therapies for metastatic breast cancer . (komen.org)
Estrogen receptor-positive breast cancer1
- Aromatase inhibitors are hormone therapy drugs used to treat estrogen receptor-positive breast cancer in postmenopausal women. (komen.org)
Amount of oestrogen1
- Aromatase inhibitors help reduce the amount of oestrogen made in the body. (breastcancernow.org)
Postmenopausal breast cancer2
- Aminoglutethimide is an NSAIs and therefore inhibits aromatase among other biosynthesis and is for example used to treat absence seizures, Cushing's syndrome, postmenopausal breast cancer and prostate cancer The first aromatase inhibitor that was discovered was aminoglutethimide, classified as first-generation AIs. (wikipedia.org)
- Arora A., Potter J.(2004) Aromatase Inhibitors: Current indications and future prospects for treatment of postmenopausal breast cancer. (bvsalud.org)
Adverse1
- They inhibit aromatase specifically but not other biosynthesis like the first-generation, therefore many adverse effects are avoided. (wikipedia.org)
Inhibition4
- When estrogen production is blocked by inhibition of the aromatase, it releases the hypothalamic-pituitary axis from the estrogenic negative feedback. (wikipedia.org)
- CGS 16949A was also found to cause irreversible inhibition of aromatase but by a different mechanism from that of 4-OHA. (umaryland.edu)
- dollar}90% inhibition of aromatase activity. (umaryland.edu)
- There have been a few limited clinical trials done on aromatase inhibition in males. (elitehealthonline.com)
Nonsteroidal1
- Fadrozole hydrochloride (CGS 16949A) is a highly potent, nonsteroidal aromatase inhibitor that significantly lowers estrogen levels in postmenopausal women and can he effective therapy for patients with advanced hormone-dependent breast carcinoma. (psu.edu)
Premenopausal women1
- However, some premenopausal women may take an aromatase inhibitor when combined with ovarian suppression . (komen.org)
Women12
- Aromatase inhibitors are used to treat breast cancer in women. (komen.org)
- Randomized clinical trials have compared outcomes for women who used aromatase inhibitors for 10 years versus 5 years [ 109,312 ]. (komen.org)
- Women who take an aromatase inhibitor for more than 5 years continue to have side effects from the drug, including a higher number of bone fractures and a higher rate of osteoporosis [ 109-112 ]. (komen.org)
- These data, presented at the 33rd Annual CTRC-AACR San Antonio Breast Cancer Symposium, indicate that women presenting with breast cancer treatment who have risk factors for cardiovascular disease should be considered for a shorter duration of use of aromatase inhibitors. (health.am)
- Women who have survived breast cancer and use aromatase inhibitors react surprisingly well to strength training. (ironmagazine.com)
- Then they noticed that women who used aromatase inhibitors and trained with weights did build up significantly more bone-free lean mass. (ironmagazine.com)
- Find out about aromatase inhibitors, a type of hormone therapy normally used to treat breast cancer in women who have gone through the menopause, including side effects and how they work. (breastcancernow.org)
- Aromatase inhibitors are used in post-menopausal women. (healthtalk.org)
- Aromatase inhibitors effectively prevent breast cancer recurrence and development of new contralateral tumours in postmenopausal women. (nih.gov)
- Prolia was later approved to treat men with osteoporosis, glucocorticoid induced osteoporosis, bone loss in men receiving androgen deprivation therapy for prostate cancer and in women receiving aromatase inhibitor therapy for breast cancer. (medlineplus.gov)
- E2 measurements are reported to be inaccurate and highly variable, especially at the low concentrations observed in men, postmenopausal women, and women on aromatase inhibitor therapy. (cdc.gov)
- For example, it has been suggested that in postmenopausal women on aromatase inhibitor therapy, inaccurate measurements can lead to incorrect assessments of treatment efficacy. (cdc.gov)
Recurrence1
- I was wondering if anyone who is HER2+/estrogen+ has successfully gotten off of an aromatase inhibitor but stayed on Herceptin without recurrence issues? (breastcancer.org)
Side Effects7
- Learn more about the side effects of aromatase inhibitors . (komen.org)
- Severe joint pain and muscle stiffness are common side effects of taking Aromatase Inhibitors. (facingourrisk.org)
- It appears that aromatase inhibitors have a significant increase in cardiotoxic side effects, such as heart attack, angina and heart failure," said Eitan Amir, M.D., a senior fellow in the division of medical oncology and hematology at the Princess Margaret Hospital, Toronto, Canada. (health.am)
- 3. Which aromatase inhibitor causes fewer side effects? (breastcancernow.org)
- Like all drugs, aromatase inhibitors can cause side effects. (breastcancernow.org)
- If you're finding it hard to cope with side effects from one aromatase inhibitor, your specialist may recommend changing to a different aromatase inhibitor or another hormone therapy drug. (breastcancernow.org)
- The use and benefits of aromatase inhibitors to decrease estrogen levels are pretty straightforward, but the side effects of aromatase inhibitors are not. (elitehealthonline.com)
Post Cycle T1
- Aromatase Inhibitor for Post Cycle Therapy. (bodypharm.biz)
Free testosterone2
- Recently, aromatase inhibitors use has been shown to increase free testosterone and lean mass in breast cancer survivors without concomitant changes in body fat. (ironmagazine.com)
- Arimigen™ acts as an anti-aromatase agent and is thus a powerful elevator of total testosterone and maximum liberator of free testosterone. (hitechpharma.com)
Cardiovascular disease1
- Data from the analysis confirmed that any duration of use of an aromatase inhibitor was associated with a 20 percent higher probability of developing cardiovascular disease. (health.am)
Androgen2
- In MCF-7 human breast cancer cells transfected with aromatase gene (MCF-7Ca), growth was stimulated by aromatizable androgen, androstenedione ({dollar}\Delta\sp4{dollar}A) in cell culture. (umaryland.edu)
- Lower aromatase activity will leaves more testosterone to bind with androgen receptors to exert its anabolic effect, as well as to be converted to DHT via 5-AR (5 alpha reductase). (men-elite.com)
Gene1
- MCF7 human breast cancer cells stably transfected with the human aromatase gene (MCF7AC1) [ 12 ] (a kind gift from Angela H. Brodie, University of Maryland, Baltimore, MD), were cultured in phenol-red-free IMEM medium supplemented with 10% fetal bovine serum (FBS) and 600 μg/ml geneticin (G418). (biomedcentral.com)
Breast cancer survivors3
- This study will look at and test auricular (ear) point acupressure to manage aromatase-inhibitor-caused joint pain and muscle stiffness in breast cancer survivors. (facingourrisk.org)
- A possible synergistic effect of aromatase inhibitors and resistance training on lean mass in breast cancer survivors is an intriguing finding that is worth further study. (ironmagazine.com)
- 15. Breast cancer survivors who have had chemotherapy within the last 5 years or are on aromatase inhibitors. (who.int)
Researchers3
- Researchers at Oregon Health and Science University discovered that the use of aromatase inhibitors can speed up the formation of new muscle mass in cancer survivors. (ironmagazine.com)
- But this picture changed when the researchers also looked at the use of aromatase inhibitors and put together the figure shown above. (ironmagazine.com)
- In our study, we found greater between group differences in lean body mass over 1 year among aromatase inhibitor users that suggest a potentiating influence of aromatase inhibitors on training-induced hypertrophy", the researchers write. (ironmagazine.com)
Drugs2
- All 3 aromatase inhibitor drugs have similar effects and no one drug is better than another. (breastcancernow.org)
- As SNPs impact the efficacy or toxicity of drugs , evaluating them with mutated conformations would help in identifying potential inhibitors. (bvsalud.org)
Pretreatment2
- In contrast, the inhibitory effect of AG was completely reversible and caused an increase in aromatase activity when AG was removed after pretreatment. (umaryland.edu)
- Markedly high pretreatment levels of aromatase P450 messenger RNA in the endometriotic tissue became undetectable in a specimen obtained from a repeated biopsy after 6 months of treatment. (elsevierpure.com)
Treatment3
- Have you been diagnosed with breast cancer and prescribed an aromatase inhibitor as part of your treatment? (bccr.org)
- Conclusion(s): This is the first description of the use of an aromatase inhibitor in the treatment of endometriosis. (elsevierpure.com)
- Aromatase inhibitors are used in the treatment of breast cancer as they are effective in decreasing the concentration of estrogen . (bvsalud.org)
Pills1
- Aromatase inhibitors are pills. (komen.org)
Outcomes2
- As a result of the essential role of oestrogens in epiphyseal closure, aromatase inhibitors have been trialled as an intervention to improve height outcomes in male children and adolescents by inhibiting the conversion of testosterone to oestradiol. (nih.gov)
- Available evidence suggested that aromatase inhibitors improved short-term growth outcomes. (nih.gov)