Trochlear Nerve
Trochlear Nerve Diseases
Abducens Nerve
Ophthalmic Nerve
Diplopia
Cranial Sinuses
Tolosa-Hunt Syndrome
Cisterna Magna
Ophthalmoplegia
Oculomotor Muscles
Cranial Nerve Diseases
Cavernous Sinus
Oculomotor Nerve
Patellofemoral Joint
Neuroimaging
Mesencephalon
Sciatic Nerve
Posterior fossa epithelial cyst: case report and review of the literature. (1/42)
A 49-year old woman with progressive cranial nerve signs and hemiparesis was found at MR imaging and at surgery to have a cyst at the foramen magnum. Immunohistochemistry and electron microscopy showed an epithelial cyst of endodermal origin. MR findings were of an extraaxial mass, with short T1 and T2 times. Unless immunohistochemistry and electron microscopy are used in the final diagnosis of such cysts, all posterior fossa cysts lined by a single layer of epithelium should be described simply as epithelial cysts. (+info)Neuropilin-2 is required in vivo for selective axon guidance responses to secreted semaphorins. (2/42)
Neuropilins are receptors for class 3 secreted semaphorins, most of which can function as potent repulsive axon guidance cues. We have generated mice with a targeted deletion in the neuropilin-2 (Npn-2) locus. Many Npn-2 mutant mice are viable into adulthood, allowing us to assess the role of Npn-2 in axon guidance events throughout neural development. Npn-2 is required for the organization and fasciculation of several cranial nerves and spinal nerves. In addition, several major fiber tracts in the brains of adult mutant mice are either severely disorganized or missing. Our results show that Npn-2 is a selective receptor for class 3 semaphorins in vivo and that Npn-1 and Npn-2 are required for development of an overlapping but distinct set of CNS and PNS projections. (+info)Nerve fiber composition of the intracranial portion of the oculomotor, trochlear, and abducens nerves in the sheep. (3/42)
In the present investigation, the fiber content and the diameter spectra of the intracranial portion of the three oculomotor nerves (oculomotor, trochlear, and abducens nerves) were analysed in sheep by light and electron microscopy. It was determined that up to 14.98% of fibers in the oculomotor nerve, 17.01% in the trochlear nerve, and 11.87% in the abducens nerve were unmyelinated. The myelinated fibers showed a bimodal distribution in their size spectrum in all three nerves, with a majority of large myelinated axons, but a considerable proportion of small myelinated fibers, as well. The sensory function of the unmyelinated fibers present in the three oculomotor nerves is discussed also on the basis of our previous morphofunctional investigations. (+info)Intracranial distribution of the sympathetic system in mice: DiI tracing and immunocytochemical labeling. (4/42)
The intracranial distribution of the cephalic branches of the superior cervical ganglion (scg) was studied in mice using indocarbocyanine dye (DiI) anterograde tracing. Two main branches were traced from the scg. The first branch joined the nerve of the pterygoid canal (the vidian nerve), npc, from which several intracranial sympathetic branches passed to the branches of the trigeminal nerve (tgn), abducent nerve (abn), trochlear nerve (trn), and oculomotor nerve (ocn). Most of the second branch joined the abn, from which sympathetic fibers dispersed in the distal region of the trigeminal ganglion (tgg) to form a plexus close to the ganglion's branches. Branches from this plexus joined the branches of the tgn, trn, and ocn. Several minor branches arising from the second branch of the scg were also observed. One formed a sympathetic plexus around the internal carotid artery (ica); a second formed a sympathetic plexus in the proximal region of tgg, close to its root; and a third branch coursed laterally to reach the ear by passing along the greater petrosal nerve (gpn). All of the intracranial trajectories traced from scg were found to be catecholaminergic, and likely sympathetic, using tyrosine hydroxylase (TH) immunocytochemistry. (+info)Vestibuloocular reflex of the adult flatfish. III. A species-specific reciprocal pattern of excitation and inhibition. (5/42)
In juvenile flatfish the vestibuloocular reflex (VOR) circuitry that underlies compensatory eye movements adapts to a 90 degrees relative displacement of vestibular and oculomotor reference frames during metamorphosis. VOR pathways are rearranged to allow horizontal canal-activated second-order vestibular neurons in adult flatfish to control extraocular motoneurons innervating vertical eye muscles. This study describes the anatomy and physiology of identified flatfish-specific excitatory and inhibitory vestibular pathways. In antidromically identified oculomotor and trochlear motoneurons, excitatory postsynaptic potentials (EPSPs) were elicited after electrical stimulation of the horizontal canal nerve expected to provide excitatory input. Electrotonic depolarizations (0.8-0.9 ms) preceded small amplitude (<0.5 mV) chemical EPSPs at 1.2-1.6 ms with much larger EPSPs (>1 mV) recorded around 2.5 ms. Stimulation of the opposite horizontal canal nerve produced inhibitory postsynaptic potentials (IPSPs) at a disynaptic latency of 1.6-1.8 ms that were depolarizing at membrane resting potentials around -60 mV. Injection of chloride ions increased IPSP amplitude, and current-clamp analysis showed the IPSP equilibrium potential to be near the membrane resting potential. Repeated electrical stimulation of either the excitatory or inhibitory horizontal canal vestibular nerve greatly increased the amplitude of the respective synaptic responses. These observations suggest that the large terminal arborizations of each VOR neuron imposes an electrotonic load requiring multiple action potentials to maximize synaptic efficacy. GABA antibodies labeled axons in the medial longitudinal fasciculus (MLF) some of which were hypothesized to originate from horizontal canal-activated inhibitory vestibular neurons. GABAergic terminal arborizations were distributed largely on the somata and proximal dendrites of oculomotor and trochlear motoneurons. These findings suggest that the species-specific horizontal canal inhibitory pathway exhibits similar electrophysiological and synaptic transmitter profiles as the anterior and posterior canal inhibitory projections to oculomotor and trochlear motoneurons. Electron microscopy showed axosomatic and axodendritic synaptic endings containing spheroidal synaptic vesicles to establish chemical excitatory synaptic contacts characterized by asymmetrical pre/postsynaptic membrane specializations as well as gap junctional contacts consistent with electrotonic coupling. Another type of axosomatic synaptic ending contained pleiomorphic synaptic vesicles forming chemical, presumed inhibitory, synaptic contacts on motoneurons that never included gap junctions. Altogether these data provide electrophysiological, immunohistochemical, and ultrastructural evidence for reciprocal excitatory/inhibitory organization of the novel vestibulooculomotor projections in adult flatfish. The appearance of unique second-order vestibular neurons linking the horizontal canal to vertical oculomotor neurons suggests that reciprocal excitation and inhibition are a fundamental, developmentally linked trait of compensatory eye movement circuits in vertebrates. (+info)Establishing the trochlear motor axon trajectory: role of the isthmic organiser and Fgf8. (6/42)
Formation of the trochlear nerve within the anterior hindbrain provides a model system to study a simple axonal projection within the vertebrate central nervous system. We show that trochlear motor neurons are born within the isthmic organiser and also immediately posterior to it in anterior rhombomere 1. Axons of the most anterior cells follow a dorsal projection, which circumnavigates the isthmus, while those of more posterior trochlear neurons project anterodorsally to enter the isthmus. Once within the isthmus, axons form large fascicles that extend to a dorsal exit point. We investigated the possibility that the projection of trochlear axons towards the isthmus and their subsequent growth within that tissue might depend upon chemoattraction. We demonstrate that both isthmic tissue and Fgf8 protein are attractants for trochlear axons in vitro, while ectopic Fgf8 causes turning of these axons away from their normal routes in vivo. Both inhibition of FGF receptor activation and inhibition of Fgf8 function in vitro affect formation of the trochlear projection within explants in a manner consistent with a guidance function of Fgf8 during trochlear axon navigation. (+info)The contractile properties of slow muscle fibres in sheep extraocular muscle. (7/42)
1. The diameters of nerve fibres in the sheep trochlear nerve were measured and they fell into two distinct groups. 2. Selective stimulation of the small diameter group of nerve fibres gave rise to a slow contraction of the superior oblique muscle which was attributed to multiply innervated muscle fibres. 3. The slow fibre contraction following a single stimulus to the small diameter nerves had a rise time of 20-50 msec and was 150-980 mg in size. On repetitive stimulation, a maximum slow fibre contraction was developed at 120-140 Hz, and maximum velocity of tension development at 170-200 Hz. 4. The maximum slow fibre tetanic tension was 7-0-12-3 g, which amounted to 5-3% of the whole muscle tetanic tension, while the maximum contracture following an injection of suxamethonium was 7% of the whole muscle tetanic tension. 5. The slow fibres were very resistant to fatigue and their contraction increased the resistance of the muscle to stretching. 6. Discrepancies from earlier work and the possible significance of the slow fibres are discussed. (+info)Neurotization of oculomotor, trochlear and abducent nerves in skull base surgery. (8/42)
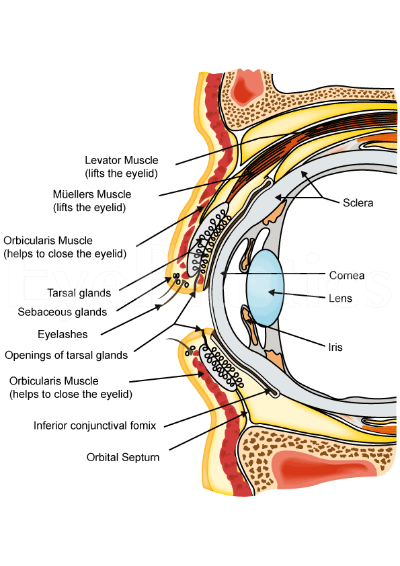
OBJECTIVE: To anatomically reconstruct the oculomotor nerve, trochlear nerve, and abducent nerve by skull base surgery. METHODS: Seventeen cranial nerves (three oculomotor nerves, eight trochlear nerves and six abducent nerves) were injured and anatomically reconstructed in thirteen skull base operations during a period from 1994 to 2000. Repair techniques included end-to-end neurosuture or fibrin glue adhesion, graft neurosuture or fibrin glue adhesion. The relationships between repair techniques and functional recovery and the related factors were analyzed. RESULTS: Functional recovery began from 3 to 8 months after surgery. During a follow-up period of 4 months to 6 years, complete recovery of function was observed in 6 trochlear nerves (75%) and 4 abducent nerves (67%), while partial functional recovery was observed in the other cranial nerves including 2 trochlear nerves, 2 abducent nerves, and 3 oculomotor nerves. CONCLUSIONS: Complete or partial functional recovery could be expected after anatomical neurotization of an injured oculomotor, trochlear or abducent nerve. Our study demonstrated that, in terms of functional recovery, trochlear and abducent nerves are more responsive than oculomotor nerves, and that end-to-end reconstruction is more efficient than graft reconstruction. These results encourage us to perform reconstruction for a separated cranial nerve as often as possible during skull base surgery. (+info)The trochlear nerve, also known as the fourth cranial nerve (CN IV), is a nerve that originates in the midbrain and innervates the superior oblique muscle of the eye. This muscle helps with the downward and outward movement of the eye, playing a crucial role in controlling eye movements and maintaining binocular vision. The trochlear nerve's main function is to provide motor (efferent) innervation to the superior oblique muscle, enabling fine-tuning of eye movements during activities such as reading, writing, or driving. Damage to this nerve can result in vertical diplopia (double vision), strabismus (eye misalignment), and other visual impairments.
The trochlear nerve, also known as the fourth cranial nerve (CN IV), is responsible for controlling the movement of the eye. It innervates the superior oblique muscle, which helps in depressing and rotating the eye downwards and outwards. Trochlear nerve diseases refer to conditions that affect this nerve and impair its function, leading to symptoms such as double vision (diplopia), vertical misalignment of the eyes, and difficulty with depth perception.
Trochlear nerve diseases can be caused by various factors, including trauma, compression, inflammation, infection, or tumors. Some common conditions that affect the trochlear nerve include:
1. Trochlear nerve palsy: This is a weakness or paralysis of the trochlear nerve, which can cause vertical and torsional diplopia, especially when looking downwards or to the side. It can be congenital or acquired due to trauma, compression, or other causes.
2. Aneurysm: Aneurysms in the vicinity of the trochlear nerve can compress or damage it, leading to palsy and diplopia.
3. Meningitis: Inflammation of the meninges (the membranes surrounding the brain and spinal cord) due to infection or other causes can affect the trochlear nerve and cause palsy.
4. Multiple sclerosis (MS): This is a chronic autoimmune disease that affects the central nervous system, including the cranial nerves. MS can cause demyelination of the trochlear nerve, leading to palsy and diplopia.
5. Diabetes: People with diabetes are at risk of developing diabetic neuropathy, which can affect any peripheral nerve, including the trochlear nerve.
6. Tumors: Space-occupying lesions in the brain or skull base, such as meningiomas, schwannomas, or pituitary adenomas, can compress the trochlear nerve and cause palsy.
The diagnosis of trochlear nerve diseases involves a thorough neurological examination, including assessment of eye movements and alignment. Imaging studies such as MRI or CT scans may be ordered to identify any structural lesions causing compression or damage to the nerve. Treatment depends on the underlying cause and may involve surgical intervention, medication, or observation.
A Trochlear nerve injury, also known as Fourth cranial nerve palsy, refers to damage or dysfunction of the fourth cranial nerve (trochlear nerve). This nerve is responsible for controlling the movement of the eye's superior oblique muscle, which helps in downward and outward movement of the eye.
Trochlear nerve injuries can result in vertical diplopia (double vision), where images appear double when looking downwards or to the side. The diplopia may be worse when looking down and out, such as when walking down stairs or reading.
The injury can be caused by various factors including head trauma, increased intracranial pressure, tumors, aneurysms, or other neurological conditions. Treatment options depend on the severity and cause of the injury and may include eye patches, prism lenses, or surgical intervention in some cases.
The abducens nerve, also known as the sixth cranial nerve (CN VI), is a motor nerve that controls the lateral rectus muscle of the eye. This muscle is responsible for moving the eye away from the midline (towards the temple) and enables the eyes to look towards the side while keeping them aligned. Any damage or dysfunction of the abducens nerve can result in strabismus, where the eyes are misaligned and point in different directions, specifically an adduction deficit, also known as abducens palsy or sixth nerve palsy.
The ophthalmic nerve, also known as the first cranial nerve or CN I, is a sensory nerve that primarily transmits information about vision, including light intensity and color, and sensation in the eye and surrounding areas. It is responsible for the sensory innervation of the upper eyelid, conjunctiva, cornea, iris, ciliary body, and nasal cavity. The ophthalmic nerve has three major branches: the lacrimal nerve, frontal nerve, and nasociliary nerve. Damage to this nerve can result in various visual disturbances and loss of sensation in the affected areas.
Diplopia is a medical term that refers to the condition where a person sees two images of a single object. It is commonly known as double vision. This can occur due to various reasons, such as nerve damage or misalignment of the eyes. Diplopia can be temporary or chronic and can affect one or both eyes. If you're experiencing diplopia, it's essential to consult an eye care professional for proper evaluation and treatment.
Cranial sinuses are a part of the venous system in the human head. They are air-filled spaces located within the skull and are named according to their location. The cranial sinuses include:
1. Superior sagittal sinus: It runs along the top of the brain, inside the skull, and drains blood from the scalp and the veins of the brain.
2. Inferior sagittal sinus: It runs along the bottom of the brain and drains into the straight sinus.
3. Straight sinus: It is located at the back of the brain and receives blood from the inferior sagittal sinus and great cerebral vein.
4. Occipital sinuses: They are located at the back of the head and drain blood from the scalp and skull.
5. Cavernous sinuses: They are located on each side of the brain, near the temple, and receive blood from the eye and surrounding areas.
6. Sphenoparietal sinus: It is a small sinus that drains blood from the front part of the brain into the cavernous sinus.
7. Petrosquamosal sinuses: They are located near the ear and drain blood from the scalp and skull.
The cranial sinuses play an essential role in draining blood from the brain and protecting it from injury.
Tolosa-Hunt syndrome is a rare disorder characterized by the inflammation of the nerve structures (including the fifth and sixth cranial nerves) within the cavernous sinus, a venous space near the base of the skull. This inflammation can lead to various symptoms such as:
1. Unilateral or bilateral orbital pain, which may be severe and deep, often radiating around the eye and temple.
2. Ophthalmoplegia (paralysis of the eye muscles), causing double vision (diplopia) and limited eye movement in specific directions.
3. Ptosis (drooping of the eyelid).
4. Other possible symptoms include decreased sensation around the forehead, cheek, or upper jaw, and loss of taste on the anterior part of the tongue.
The exact cause of Tolosa-Hunt syndrome is unknown, but it's believed to be related to an autoimmune response or a non-specific inflammatory process. It can also occur in conjunction with other medical conditions like neoplasms (tumors) or infections. The diagnosis typically involves imaging studies such as MRI and CT scans, along with blood tests and a thorough neurological examination.
Treatment usually includes corticosteroids to reduce inflammation and alleviate symptoms. In some cases, immunosuppressive medications or radiation therapy may be necessary. If left untreated, Tolosa-Hunt syndrome can lead to permanent visual impairment or other neurological deficits.
The term "cisterna magna" is derived from Latin, where "cisterna" means "reservoir" or "receptacle," and "magna" means "large." In medical anatomy, the cisterna magna refers to a large, sac-like space located near the lower part of the brainstem. It is a subarachnoid cistern, which means it is a space that contains cerebrospinal fluid (CSF) between the arachnoid and pia mater membranes covering the brain and spinal cord.
More specifically, the cisterna magna is situated between the cerebellum (the lower part of the brain responsible for coordinating muscle movements and maintaining balance) and the occipital bone (the bone at the back of the skull). This space contains a significant amount of CSF, which serves as a protective cushion for the brain and spinal cord, helps regulate intracranial pressure, and facilitates the circulation of nutrients and waste products.
The cisterna magna is an essential structure in neurosurgical procedures and diagnostic imaging techniques like lumbar puncture (spinal tap) or myelograms, where contrast agents are introduced into the CSF to visualize the spinal cord and surrounding structures. Additionally, it serves as a crucial landmark for various surgical approaches to the posterior fossa (the lower part of the skull that houses the cerebellum and brainstem).
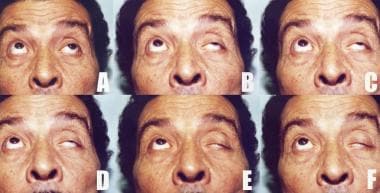
Ophthalmoplegia is a medical term that refers to the paralysis or weakness of the eye muscles, which can result in double vision (diplopia) or difficulty moving the eyes. It can be caused by various conditions, including nerve damage, muscle disorders, or neurological diseases such as myasthenia gravis or multiple sclerosis. Ophthalmoplegia can affect one or more eye muscles and can be partial or complete. Depending on the underlying cause, ophthalmoplegia may be treatable with medications, surgery, or other interventions.
The oculomotor muscles are a group of extraocular muscles that control the movements of the eye. They include:
1. Superior rectus: This muscle is responsible for elevating the eye and helping with inward rotation (intorsion) when looking downwards.
2. Inferior rectus: It depresses the eye and helps with outward rotation (extorsion) when looking upwards.
3. Medial rectus: This muscle adducts, or moves, the eye towards the midline of the face.
4. Inferior oblique: The inferior oblique muscle intorts and elevates the eye.
5. Superior oblique: It extorts and depresses the eye.
These muscles work together to allow for smooth and precise movements of the eyes, enabling tasks such as tracking moving objects, reading, and maintaining visual fixation on a single point in space.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
The cavernous sinus is a venous structure located in the middle cranial fossa, which is a depression in the skull that houses several important nerves and blood vessels. The cavernous sinus is situated on either side of the sphenoid bone, near the base of the skull, and it contains several important structures:
* The internal carotid artery, which supplies oxygenated blood to the brain
* The abducens nerve (cranial nerve VI), which controls lateral movement of the eye
* The oculomotor nerve (cranial nerve III), which controls most of the muscles that move the eye
* The trochlear nerve (cranial nerve IV), which controls one of the muscles that moves the eye
* The ophthalmic and maxillary divisions of the trigeminal nerve (cranial nerve V), which transmit sensory information from the face and head
The cavernous sinus is an important structure because it serves as a conduit for several critical nerves and blood vessels. However, it is also vulnerable to various pathological conditions such as thrombosis (blood clots), infection, tumors, or aneurysms, which can lead to serious neurological deficits or even death.
The oculomotor nerve, also known as the third cranial nerve (CN III), is a motor nerve that originates from the midbrain. It controls the majority of the eye muscles, including the levator palpebrae superioris muscle that raises the upper eyelid, and the extraocular muscles that enable various movements of the eye such as looking upward, downward, inward, and outward. Additionally, it carries parasympathetic fibers responsible for pupillary constriction and accommodation (focusing on near objects). Damage to this nerve can result in various ocular motor disorders, including strabismus, ptosis, and pupillary abnormalities.
The patellofemoral joint is the articulation between the patella (kneecap) and the femur (thigh bone). It is a synovial joint, which means it is surrounded by a joint capsule containing synovial fluid to lubricate the joint. This joint is responsible for providing stability to the knee extensor mechanism and allows for smooth movement of the patella during activities like walking, running, and jumping. Pain or dysfunction in this joint can result in various conditions such as patellofemoral pain syndrome, chondromalacia patella, or patellar dislocation.
Neuroimaging is a medical term that refers to the use of various techniques to either directly or indirectly image the structure, function, or pharmacology of the nervous system. It includes techniques such as computed tomography (CT), magnetic resonance imaging (MRI), functional MRI (fMRI), positron emission tomography (PET), single-photon emission computed tomography (SPECT), and diffusion tensor imaging (DTI). These techniques are used to diagnose and monitor various neurological and psychiatric conditions, as well as to understand the underlying mechanisms of brain function in health and disease.
The mesencephalon, also known as the midbrain, is the middle portion of the brainstem that connects the hindbrain (rhombencephalon) and the forebrain (prosencephalon). It plays a crucial role in several important functions including motor control, vision, hearing, and the regulation of consciousness and sleep-wake cycles. The mesencephalon contains several important structures such as the cerebral aqueduct, tectum, tegmentum, cerebral peduncles, and several cranial nerve nuclei (III and IV).
Patellar dislocation is a medical condition characterized by the displacement of the patella (kneecap) from its normal position in the femoral groove, which is a part of the femur (thighbone). This displacement usually occurs laterally, meaning that the patella moves toward the outer side of the knee.
Patellar dislocation can happen as a result of direct trauma or due to various factors that increase the laxity of the medial patellofemoral ligament and tightness of the lateral structures, leading to abnormal tracking of the patella. These factors include anatomical variations, muscle imbalances, genetic predisposition, or degenerative changes in the knee joint.
Dislocation of the patella can cause pain, swelling, and difficulty in moving the knee. In some cases, it might be associated with other injuries such as fractures or damage to the articular cartilage and surrounding soft tissues. Immediate medical attention is required for proper diagnosis and treatment, which may involve reduction, immobilization, physical therapy, bracing, or even surgery in severe cases.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
The patella, also known as the kneecap, is a sesamoid bone located at the front of the knee joint. It is embedded in the tendon of the quadriceps muscle and serves to protect the knee joint and increase the leverage of the extensor mechanism, allowing for greater extension force of the lower leg. The patella moves within a groove on the femur called the trochlea during flexion and extension of the knee.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
 Trochlear nerve
Trochlear nerve
Congenital fourth nerve palsy
Supratrochlear artery
Parks-Bielschowsky three-step test
Torticollis
Recurrent painful ophthalmoplegic neuropathy
Motor neuron
Chiasm (anatomy)
Superior cerebellar artery
Brain herniation
Superior oblique muscle
Cranial nerves
Superior oblique myokymia
Vergence
Medial longitudinal fasciculus
Orbital blowout fracture
Axial twist theory
Cavernous nerve plexus
Sense of balance
Ophthalmoparesis
Brainstem
Cranial nerve nucleus
Trochlear nucleus
Ambient cistern
Alfred Bielschowsky
Roundabout family
Fourth nerve palsy
Gaze (physiology)
Superior orbital fissure
SO4
Trochlear nerve - Wikipedia
 Trochlear Nerve Palsy (Fourth Nerve Palsy): Background, History of the Procedure, Problem
Trochlear Nerve Palsy (Fourth Nerve Palsy): Background, History of the Procedure, Problem
 Fourth Cranial Nerve (Trochlear Nerve) Palsy - Brain, Spinal Cord, and Nerve Disorders - Merck Manuals Consumer Version
Fourth Cranial Nerve (Trochlear Nerve) Palsy - Brain, Spinal Cord, and Nerve Disorders - Merck Manuals Consumer Version
 Anatomy Dissected: CNIV (trochlear nerve) | Complete Anatomy
Anatomy Dissected: CNIV (trochlear nerve) | Complete Anatomy
 Familial congenital palsy of trochlear nerve | Rare Diseases | RareGuru
Familial congenital palsy of trochlear nerve | Rare Diseases | RareGuru
 View of Maxillary Sinus Carcinoma Presenting as Trochlear Nerve Palsy
View of Maxillary Sinus Carcinoma Presenting as Trochlear Nerve Palsy
Fourth Cranial (Trochlear) Nerve Palsy - Neurologic Disorders - MSD Manual Professional Edition
Trochlear nerve schwannoma with intratumoral hemorrhage: case report. - Fingerprint - Keio University
 ICD-10-CM Diagnosis Code S04.21XA - Injury of trochlear nerve, right side, initial encounter
ICD-10-CM Diagnosis Code S04.21XA - Injury of trochlear nerve, right side, initial encounter
The Neurologic Examination of Animals - Nervous System - Merck Veterinary Manual
![Hironaka K[au] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Hironaka K[au] - Search Results - PubMed
Hironaka K[au] - Search Results - PubMed
 BRAINMAPS.ORG - BRAIN ATLAS, BRAIN MAPS, BRAIN STRUCTURE,
NEUROINFORMATICS, BRAIN, STEREOTAXIC ATLAS, NEUROSCIENCE
BRAINMAPS.ORG - BRAIN ATLAS, BRAIN MAPS, BRAIN STRUCTURE,
NEUROINFORMATICS, BRAIN, STEREOTAXIC ATLAS, NEUROSCIENCE
 Cranial Nerves Flashcards
Cranial Nerves Flashcards
 Electronystagmography: MedlinePlus Medical Encyclopedia
Electronystagmography: MedlinePlus Medical Encyclopedia
 Bassett Collection - Lane Medical Library - Stanford University School of Medicine
Bassett Collection - Lane Medical Library - Stanford University School of Medicine
2011 ICD-9-CM Diagnosis Code 995.1 : Angioneurotic edema not elsewhere classified
Bassett Collection - Lane Medical Library - Stanford University School of Medicine
The supracerebellar-transtentorial approach to posteromedial temporal lesions in children with refractory epilepsy in: Journal...
 Powtoon - Sistem saraf by ain
Powtoon - Sistem saraf by ain
 Cavernous sinus contents (mnemonic) | Radiology Reference Article | Radiopaedia.org
Cavernous sinus contents (mnemonic) | Radiology Reference Article | Radiopaedia.org
 Interactive Prenatal Development Timeline - Advanced
Interactive Prenatal Development Timeline - Advanced
Ophthalmologic Manifestations of Myasthenia Gravis: Overview, Patient History, Physical Examination
 Clinical Services Offered
Clinical Services Offered
 Brainstem Anatomy Quiz Questions And Answers - ProProfs Quiz
Brainstem Anatomy Quiz Questions And Answers - ProProfs Quiz
 Strabismus - StatPearls - NCBI Bookshelf
Strabismus - StatPearls - NCBI Bookshelf
 The Function Of Your Midbrain - Database Football
The Function Of Your Midbrain - Database Football
 How I Do It: Gasserian Ganglion Block for Trigeminal Neuralgia
How I Do It: Gasserian Ganglion Block for Trigeminal Neuralgia
 Frontiers | Sensory Evolution and Ecology of Early Turtles Revealed by Digital Endocranial Reconstructions
Frontiers | Sensory Evolution and Ecology of Early Turtles Revealed by Digital Endocranial Reconstructions
Migraine Variants: Overview, Pathophysiology, Epidemiology
Trigeminal nerve10
- Stay tuned for next week, where we'll be covering CNV (the trigeminal nerve) in detail. (3d4medical.com)
- Cranial nerve V, also known as the trigeminal nerve, originates from the pons, which is a part of the brainstem. (proprofs.com)
- The trigeminal nerve is responsible for transmitting sensory information from the face and controlling the muscles involved in chewing. (proprofs.com)
- TN is characterized by recurrent short episodes of sharp, electrical shock like pain, typically abrupt in onset and termination, along the distribution of one or more divisions of the trigeminal nerve. (asra.com)
- The trigeminal nerve supplies the sensory innervation to the face as well as the sensory and motor innervation to the mastication muscles. (asra.com)
- Third division of trigeminal nerve innervates masseter and temporalis, so you should check for contraction of both muscles! (usc.edu)
- The trigeminal nerve provides sensory supply to the face and mouth. (usc.edu)
- The corneal reflex has two parts: the sensory, or afferent, part of the reflex is mediated by the ophthalmic branch of the trigeminal nerve, and the motor, or efferent, part of the reflex is mediated by the facial nerve. (usc.edu)
- The syndrome is characterised by retro-orbital paralysis of extraocular muscles impairment of the branches of the 1st division of the trigeminal nerve and frequently extension to involve the optic nerve. (medicosnotes.com)
- The trigeminal nerve has two roots, motor and sensory. (bookdome.com)
Palsy44
- An injury to the trochlear nucleus in the brainstem will result in an contralateral superior oblique muscle palsy, whereas an injury to the trochlear nerve (after it has emerged from the brainstem) results in an ipsilateral superior oblique muscle palsy. (wikipedia.org)
- Trochlear nerve palsy also affects torsion (rotation of the eyeball in the plane of the face). (wikipedia.org)
- The most common cause of acute fourth nerve palsy is head trauma. (wikipedia.org)
- Trochlear nerve palsy is mentioned in ophthalmology texts dating to the mid nineteenth century. (medscape.com)
- In 1935, Bielschowsky correctly noted that trochlear nerve palsy was the most common cause of vertical diplopia and introduced his classic head-tilt test. (medscape.com)
- A fourth nerve palsy is a common cause of binocular vertical oblique diplopia in isolation. (medscape.com)
- An isolated fourth cranial nerve palsy usually can be diagnosed using the 3-step test. (medscape.com)
- Most cases of isolated fourth nerve palsy are believed to be congenital. (medscape.com)
- [ 5 ] However, estimating the true frequency of congenital fourth nerve palsy is difficult. (medscape.com)
- Some of the best information regarding the incidence of acquired fourth nerve palsy can be found in the Mayo Clinic series. (medscape.com)
- Trochlear nerve palsy was less common than abducens or oculomotor palsies. (medscape.com)
- Of 4,373 acquired cases of extraocular muscle palsy in adults, there were only 657 cases of isolated fourth nerve disease. (medscape.com)
- [ 6 ] Fourth nerve palsy also was the least frequent in a pediatric population. (medscape.com)
- In a similar Mayo Clinic study of 160 children, 19 of them had isolated fourth nerve palsy. (medscape.com)
- One must consider the possibility of underlying structural abnormalities (eg, skull based tumor) if fourth nerve palsy results after only minor trauma. (medscape.com)
- Microvasculopathy secondary to diabetes, atherosclerosis, or hypertension also may cause isolated fourth nerve palsy. (medscape.com)
- There are rare reports of thyroid ophthalmopathy and myasthenia gravis mimicking an isolated fourth nerve palsy. (medscape.com)
- Tumor, aneurysm, multiple sclerosis , or iatrogenic injury may present with isolated fourth nerve palsy that may evolve over time to include other cranial nerve palsies or neurologic symptoms. (medscape.com)
- Fourth nerve palsy may become manifest after cataract surgery. (medscape.com)
- Patients with underlying, well-controlled, and asymptomatic fourth nerve palsy may decompensate gradually as they lose binocular function resulting from cataract. (medscape.com)
- This syndrome was present in 73% of congenital trochlear nerve palsy cases and is characterized by absence of the trochlear nerve and secondary atrophy of the superior oblique muscle. (medscape.com)
- A palsy of the 4th cranial nerve affects vertical eye movements. (merckmanuals.com)
- Doctors suspect palsy of the 4th cranial nerve based on the symptoms, but computed tomography or magnetic resonance imaging may be done. (merckmanuals.com)
- Often, the cause of 4th cranial nerve palsy cannot be identified. (merckmanuals.com)
- causes this palsy by damaging small blood vessels that carry blood to the nerve. (merckmanuals.com)
- Usually, 4th cranial nerve palsy is suspected if a person has characteristic limited eye movement. (merckmanuals.com)
- The disorder causing 4th cranial nerve palsy, if identified, is treated. (merckmanuals.com)
- Connect with other caregivers and patients with Familial congenital palsy of trochlear nerve and get the support you need. (rareguru.com)
- Familial congenital palsy of trochlear nerve is a rare, genetic, neuro- ophthalmological disease characterized by congenital fourth cranial nerve palsy, manifesting with hypertropia in side gaze, unexplained head tilt, acquired vertical diplopia, and progressive increase in vertical fusional vergence amplitudes with prolonged occlusion. (rareguru.com)
- Fourth cranial nerve palsy impairs the superior oblique muscle, causing paresis of vertical gaze, mainly in adduction. (msdmanuals.com)
- Fourth cranial nerve palsy may affect one or both eyes. (msdmanuals.com)
- Isolated trochlear nerve palsy with perimesencephalic subarachnoid haemorrhage. (nih.gov)
- I crashed my bike in February, getting knocked out, breaking some bones and being saddled with Trochlear Nerve Palsy . (shardcore.org)
- Fourth nerve palsy, also known as superior oblique palsy or trochlear nerve palsy, occurs when the fourth cranial nerve becomes diseased or damaged. (optometrists.org)
- Idiopathic fourth nerve palsy occurs when there is no known cause for the nerve paralysis. (optometrists.org)
- What are the symptoms of fourth nerve palsy? (optometrists.org)
- Fourth nerve palsy generally affects only one eye, but it can affect both eyes as well. (optometrists.org)
- How is fourth nerve palsy diagnosed? (optometrists.org)
- To diagnose fourth nerve palsy, your eye doctor will first conduct a full medical history. (optometrists.org)
- How is fourth nerve palsy treated? (optometrists.org)
- The treatment options for fourth nerve palsy depend on the underlying cause of the condition. (optometrists.org)
- When fourth nerve palsy is idiopathic or caused by an injury to the nerve, it may improve on its own after several months. (optometrists.org)
- Vision therapy is an effective treatment option for some patients with fourth nerve palsy, as it can help to improve eye movements and binocular vision. (optometrists.org)
- The sooner fourth nerve palsy is diagnosed, the greater your chances of optimal treatment results. (optometrists.org)
Oculomotor nerve7
- Cranial nerves IV (trochlear nerve) and III (oculomotor nerve) originate from the midbrain. (proprofs.com)
- The trochlear nerve controls the superior oblique muscle, which helps with eye movement, while the oculomotor nerve controls several eye muscles responsible for eye movement, pupil constriction, and focusing. (proprofs.com)
- Among the options given, the only cranial nerve that exits from this location is the third cranial nerve, also known as the oculomotor nerve. (proprofs.com)
- The oculomotor nerve runs the ventral width of the tegmentum, emerging out of the nucleus. (databasefootball.com)
- and (2) a superior part, subjacent to the superior colliculi which is traversed by the emerging bundles of the oculomotor nerve. (co.ma)
- in the superior part, the nucleus of the oculomotor nerve is situated. (co.ma)
- The PTA offers a wide surgical corridor that can only be afforded by exposing the lateral wall of the cavernous sinus, drilling the anterior clinoid process extradurally, dividing the distal dural ring, and fully mobilizing the oculomotor nerve, including often drilling the posterior clinoid process. (surgicalneurologyint.com)
Inferior9
- The trochlear nerve decussates within the brainstem before emerging on the contralateral side of the brainstem (at the level of the inferior colliculus). (wikipedia.org)
- From their respective nuclei, the two trochlear nerves then travel dorsal-ward through the substance of the midbrain surrounded by the periaqueductal gray, crossing over (decussating) within the midbrain before emerging from the dorsal midbrain just inferior to the inferior colliculus. (wikipedia.org)
- Near the superior colliculi are the inferior colliculi, which are responsible for the processing of auditory information and are found just above the trochlear nerve. (databasefootball.com)
- In contrast, the trochlear nuclei are found at the level of the inferior colliculus and they help refine vision, focusing the eyes on proximal objects. (databasefootball.com)
- There are several important structures that reside in the vicinity of the ganglion: the cavernous sinus, the optic and trochlear nerves medially, the inferior surface of the temporal lobe of the brain superiorly, and the brain stem posteriorly. (asra.com)
- The mandibular division exits through the foramen ovale (FO) and divides into the buccal, lingual, inferior alveolar, and auriculotemporal nerves. (asra.com)
- The infraorbital foramen, for the nerve and artery of the same name, is less than 1 cm inferior to the inferior margin. (dartmouth.edu)
- The inferior orbital fissure communicates with the infratemporal and pterygopalatine fossae and transmits the zygomatic nerve. (dartmouth.edu)
- the inferior maxillary division is a mixed nerve, as it is joined by the motor root. (bookdome.com)
Glossopharyngeal1
- Cranial nerve 9, also known as the Glossopharyngeal nerve, controls functions like taste and swallowing. (proprofs.com)
Muscles2
- The orbits (figs. 45-1 and 45-2 ) are two bony cavities occupied by the eyes and associated muscles, nerves, blood vessels, fat, and much of the lacrimal apparatus. (dartmouth.edu)
- The facial motor nerve supplies motor branches to the muscles of facial expression. (usc.edu)
Innervates3
- pulley-like nerve) also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye (which operates through the pulley-like trochlea). (wikipedia.org)
- The superior oblique muscle which the trochlear nerve innervates ends in a tendon that passes through a fibrous loop, the trochlea, located anteriorly on the medial aspect of the orbit. (wikipedia.org)
- The fourth cranial nerve innervates the superior oblique muscle, which intorts, depresses, and abducts the globe. (medscape.com)
Nuclei2
- The cerebral aqueduct contains the nuclei of two pairs of cranial nerves , the oculomotor nuclei and the trochlear nuclei. (databasefootball.com)
- The lateral lemniscus, to a large extent, comes from the nuclei of termination of the cochlear nerve of the opposite side. (co.ma)
Congenital1
- A series of high-definition magnetic resonance imaging (MRI) studies by Yang et al have identified 2 etiologies of congenital trochlear nerve palsies, with the most common being congenital cranial dysinnervation syndrome. (medscape.com)
Olfactory nerves1
- You can see this projection along the base of the brain, so this is called the olfactory bulb, and the olfactory nerves, synapse on to this olfactory bulb. (anatomyzone.com)
Nasociliary nerves2
- It divides into the supraorbital, supratrochlear, and nasociliary nerves to supply the forehead and nose. (asra.com)
- It divides near the superior orbital fissure into the lacrimal, frontal, and nasociliary nerves. (dartmouth.edu)
Sensory6
- You've got somatic and visceral components, they've got motor components and there's some nerves which have special sensory components, so components to do with the special senses, like smell, vision, hearing, balance and taste. (anatomyzone.com)
- These ganglia are the cell bodies of neurons with axons that are sensory endings in the periphery, such as in the skin, and that extend into the CNS through the dorsal nerve root. (lumenlearning.com)
- Another type of sensory ganglion is a cranial nerve ganglion . (lumenlearning.com)
- The ophthalmic nerve, the first division of the trigeminal (fifth cranial) nerve, is a wholly afferent nerve that supplies the globe and conjunctiva, lacrimal gland and sac, nasal mucosa and frontal sinus, external nose, upper eyelid, forehead, and scalp, It arises from the trigeminal ganglion which contains the cell bodies of its sensory nerve fibers. (dartmouth.edu)
- The olfactory is a sensory nerve, and damage in the nasal epithelium or the basal gangliamight impair the ability to discriminate different smells. (usc.edu)
- The corneal reflex should also be examined as the sensory supply to the cornea is from this nerve. (usc.edu)
Supraorbital1
- The superior margin, formed by the frontal bone, presents near its medial end either a supraorbital notch or a supraorbital foramen, which transmits the nerve and vessels of the same name. (dartmouth.edu)
Midbrain3
- citation needed] Each trochlear nerve originates from a trochlear nucleus in the medial midbrain. (wikipedia.org)
- The human trochlear nerve is derived from the basal plate of the embryonic midbrain. (wikipedia.org)
- Which Cranial nerve(s) come from the midbrain? (proprofs.com)
Cranial nerve palsies1
- Several studies reported the incidence and etiology of acquired cranial nerve palsies in adult and pediatric patients. (medscape.com)
Dorsal3
- It is the only cranial nerve that exits from the dorsal (rear) aspect of the brainstem. (wikipedia.org)
- Also, the fibrous region is composed of the axons of these neurons that are passing through the ganglion to be part of the dorsal nerve root (tissue source: canine). (lumenlearning.com)
- This is analogous to the dorsal root ganglion, except that it is associated with a cranial nerve instead of a spinal nerve . (lumenlearning.com)
Fibres4
- Nerve-fibres reach the superior colliculus through-(1) the lemnisci and (2) the superior brachium. (co.ma)
- After their origins from the olfactory cells of the olfactory region on the upper part of the nasal septum and the corresponding part of the lateral wall of the nasal cavity, the nerve fibres form fine plexuses from which the terminal filaments pass through the cribriform plates of the ethmoid on their way to the olfactory bulb. (co.ma)
- The second or optic nerve consists of nerve fibres which spring from the ganglion cells of the retina, and converge to the optic papilla, where they are grouped together to form the optic nerve. (co.ma)
- these fibres arise from the nerve cells of the Gasserian (semilunar) ganglion. (bookdome.com)
Arteries2
- At the junction of the medial wall with the roof, the anterior and posterior ethmoidal foramina transmit the nerves and arteries of the same name. (dartmouth.edu)
- Associated with the orbit are foramina and fissures (see Table 1, below), which are important in transmitting nerves, arteries, and veins. (medscape.com)
Originates1
- The nerve originates from the midlateral surface of pons. (asra.com)
Optic nerves1
- Multiple Sclerosis (MS) In multiple sclerosis, patches of myelin (the substance that covers most nerve fibers) and underlying nerve fibers in the brain, optic nerves, and spinal cord are damaged or destroyed. (merckmanuals.com)
Injury4
- citation needed] Injury to the trochlear nerve cause weakness of downward eye movement with consequent vertical diplopia (double vision). (wikipedia.org)
- Any disease or injury that damages the acoustic nerve can cause vertigo. (medlineplus.gov)
- Concussions and whiplash are the most common causes of injury to the fourth cranial nerve. (optometrists.org)
- Poor blood flow related to diabetes is another common cause of nerve injury or disease. (optometrists.org)
Fourth8
- the fourth nerve is thus also named after this structure. (wikipedia.org)
- The characteristic appearance of patients with fourth nerve palsies (head tilted to one side, chin tucked in) suggests the diagnosis, but other causes must be ruled out. (wikipedia.org)
- Even relatively minor trauma can transiently stretch the fourth nerve (by transiently displacing the brainstem relative to the posterior clinoid process). (wikipedia.org)
- Patients with minor damage to the fourth nerve will complain of "blurry" vision. (wikipedia.org)
- With greater clinical interest, the number of identified fourth nerve palsies has increased. (medscape.com)
- The fourth cranial nerve exits dorsally and has the longest intracranial course. (medscape.com)
- Welcome to the fourth in our Anatomy Dissected series on the cranial nerves. (3d4medical.com)
- The fourth cranial nerve controls the actions of the superior oblique eye muscle. (optometrists.org)
Fibers3
- They also help control certain eye movements and interact with fibers of the optic nerve. (databasefootball.com)
- Under microscopic inspection, it can be seen to include the cell bodies of the neurons, as well as bundles of fibers that are the posterior nerve root (Figure 1). (lumenlearning.com)
- Throughout the years, in the absence of ancillary or diagnostic tools, many descriptive phrases, clichés, or analogies have been used to describe the eye, such as "the eye is the window to the soul," the "eye works like a camera," and "the eye is the only structure that allows us to physically see blood vessels and nerve fibers. (medscape.com)
Sixth1
- The cranial nerves that come from the pontomedullary junction are the sixth (VI) and seventh (VII) cranial nerves. (proprofs.com)
Paresis1
- Extraocular Paresis of cranial nerves III, IV, and VI causing ophthalmoplegia. (medicosnotes.com)
Pons2
- Each trochlear nerve thus comes to course on the contralateral side, first passing laterally (to the side) and then anteriorly around the pons, then running forward toward the eye in the subarachnoid space. (wikipedia.org)
- For example, the trigeminal ganglion is superficial to the temporal bone whereas its associated nerve is attached to the mid-pons region of the brain stem. (lumenlearning.com)
Ganglion1
- The ganglion is an enlargement of the nerve root. (lumenlearning.com)
Palsies2
- This accounts for the "dejected" appearance of patients with "pathetic nerve" palsies. (wikipedia.org)
- To compensate for this, patients with trochlear nerve palsies tilt their heads to the opposite side, in order to fuse the two images into a single visual field. (wikipedia.org)
Blood vessels1
- Blood vessel complications in diabetes People with diabetes mellitus have many serious long-term complications that affect many areas of the body, particularly the blood vessels, nerves, eyes, and kidneys. (merckmanuals.com)
Exits1
- The statement suggests that one of these cranial nerves exits from the intermedullary fossa. (proprofs.com)
Pairs4
- Overview of the Cranial Nerves Twelve pairs of nerves-the cranial nerves-lead directly from the brain to various parts of the head, neck, and trunk. (merckmanuals.com)
- Cranial nerves are nerves that emerge directly from the brain, and you've got 12 pairs of cranial nerves, and they're a part of the peripheral nervous system. (anatomyzone.com)
- All 12 pairs are a part of the peripheral nervous system, except cranial nerve number 2, which actually emerges from, which is kind of like an extension of the brain, so it's not technically a peripheral nerve. (anatomyzone.com)
- The cranial nerves arise directly from the brain (including the brainstem), they emerge from the central nervous system above the level of the first vertebrae of the vertebral column, They are 12 pairs of. (online-sciences.com)
Nucleus1
- A peripheral lesion is damage to the bundle of nerves, in contrast to a central lesion, which is damage to the trochlear nucleus. (wikipedia.org)
Cerebral1
- The deep connexions of the cerebral nerves are dealt with in the section which treats of the Brain (pp. 592 to 607). (co.ma)
Peripheral1
- The common abnormalities include disease of the muscle itself (myopathy), and motor nerve damage in peripheral/spinal cord/brain from cancer or trauma. (usc.edu)
Neurologic1
- When the patient cannot track motion this means neurologic damage involving cranial nerves III, IV, or VI. (usc.edu)
Disorders1
- thus, they can be considered cranial nerve disorders, neuro-ophthalmologic. (msdmanuals.com)
Sciatic nerve1
- The pudendal nerve, derived from S2, S3 and S4, leaves the pelvis m edial to the sciatic nerve via the higher sciatic foram en. (dnahelix.com)
Superior oblique3
- The remaining 27% had a normal trochlear nerve and superior oblique muscle size, but an abnormal superior oblique tendon, which may explain the variations in superior oblique tendon laxity encountered surgically. (medscape.com)
- This week, Dr. Chukwudi Ekomaru uses Complete Anatomy to explore Cranial Nerve IV (the trochlear nerve), which is responsible for innervating the superior oblique muscle of the eye. (3d4medical.com)
- The roof (frontal and sphenoid bones) presents the fossa for the lacrimal gland anterolaterally and the trochlear pit for the cartilaginous or bony pulley of the superior oblique muscle anteromedially. (dartmouth.edu)
Roots2
- The roots of cranial nerves are within the cranium, whereas the ganglia are outside the skull. (lumenlearning.com)
- In the development of the sympathetic it is at least highly probable that a mesoblastic rudiment or precursor forms the basis of the sympathetic system, which is secondarily joined by nervefibres from the roots of the spinal nerves. (co.ma)
Efferent2
- Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve (somatic efferent nerve). (wikipedia.org)
- the trochlear nerve thus carries axons of general somatic efferent type. (wikipedia.org)