Trench Fever
Bartonella quintana
Pediculus
Typhus, Epidemic Louse-Borne
Phthiraptera
Rickettsiaceae
Bartonella
Bartonella Infections
Immersion Foot
Q Fever
Water Pollutants, Radioactive
Yellow Fever
Typhoid Fever
Lice Infestations
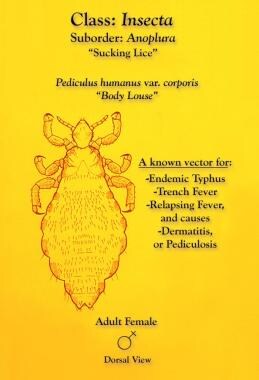
Anoplura
Culture of Bartonella quintana and Bartonella henselae from human samples: a 5-year experience (1993 to 1998). (1/63)
Bartonella quintana and Bartonella henselae are fastidious gram-negative bacteria responsible for bacillary angiomatosis, trench fever, cat scratch disease, and endocarditis. During a 5-year period, we received 2,043 samples for culture of Bartonella sp. We found Bartonella sp. to be the etiologic agent in 38 cases of endocarditis, 78 cases of cat scratch disease, 16 cases of bacteremia in homeless people, and 7 cases of bacillary angiomatosis. We correlated the results of positive cultures with the clinical form of the disease, type of sample, culture procedure, PCR-based genomic detection, and antibody determination. Seventy-two isolates of B. quintana and nine isolates of B. henselae from 43 patients were obtained. Sixty-three of the B. quintana isolates and two of the B. henselae isolates, obtained from patients with no prior antibiotic therapy, were stably subcultured. The sensitivity of culture was low when compared with that of PCR-based detection methods in valves of patients with endocarditis (44 and 81%, respectively), skin biopsy samples of patients with bacillary angiomatosis (43 and 100%, respectively), and lymph nodes of cat scratch disease (13 and 30%, respectively). Serological diagnosis was also more sensitive in cases of endocarditis (97%) and cat scratch disease (90%). Among endocarditis patients, the sensitivity of the shell vial culture assay was 28% when inoculated with blood samples and 44% when inoculated with valvular biopsy samples, and the sensitivity of both was significantly higher than that of culture on agar (5% for blood [P = 0.045] and 4% for valve biopsy samples [P < 0.0005]). The most efficient culture procedure was the subculture of blood culture broth into shell vials (sensitivity, 71%). For patients with endocarditis, previous antibiotic therapy significantly affected results of blood culture; no patient who had been administered antibiotics yielded a positive blood culture, whereas 80% of patients with no previous antibiotic therapy yielded positive blood cultures (P = 0.0006). Previous antibiotic therapy did not, however, prevent isolation of Bartonella sp. from cardiac valves but did prevent the establishment of strains, as none of the 15 isolates from treated patients could be successfully subcultured. For the diagnosis of B. quintana bacteremia in homeless people, the efficiency of systematic subculture of blood culture broth onto agar was higher than that of direct blood plating (respective sensitivities, 98 and 10% [P < 10(-7)]). Nevertheless, both procedures are complementary, since when used together their sensitivity reached 100%. All homeless people with positive blood cultures had negative serology. The isolation rate of B. henselae from PCR-positive lymph nodes, in patients with cat scratch disease, was significantly lower than that from valves of endocarditis patients and skin biopsy samples from bacillary angiomatosis patients (13 and 33%, respectively [P = 0.084]). In cases of bacillary angiomatosis for which an agent was identified to species level, the isolation rate of B. henselae was lower than the isolation rate of B. quintana (28 and 64%, respectively [P = 0.003]). If culture is to be considered an efficient tool for the diagnosis of several Bartonella-related diseases, methodologies need to be improved, notably for the recovery of B. henselae from lymph nodes of patients with cat scratch disease. (+info)Survey of three bacterial louse-associated diseases among rural Andean communities in Peru: prevalence of epidemic typhus, trench fever, and relapsing fever. (2/63)
Typhus and other louse-transmitted bacterial infections in Peruvian sierra communities are known to occur but have not recently been assessed. In this study, 194 of 1,280 inhabitants of four villages in Calca Province in the Urubamba Valley were included. Thirty-nine (20%) of the 194 volunteers had antibodies to Rickettsia prowazekii, whereas 24 (12%) had antibodies to Bartonella quintana and 2 against Borrelia recurrentis. There was a significant correlation between the presence of infesting ectoparasites and antibodies to R. prowazekii, as well as between antibodies to R. prowazekii and ectoparasite infestation and fever in the previous 6 months. The proportion of inhabitants infested with ectoparasites was significantly higher in the highest-altitude village than in the other three villages. Two volunteers' antibody levels suggested a recent typhus infection, but only B. quintana DNA was amplified from lice. Epidemic typhus remains extant in the area, and B. quintana infections were encountered and documented for the first time in South America. (+info)The body louse as a vector of reemerging human diseases. (3/63)
The body louse, Pediculus humanus humanus, is a strict human parasite, living and multiplying in clothing. Louse infestation is associated with cold weather and a lack of hygiene. Three pathogenic bacteria are transmitted by the body louse. Borrelia recurrentis is a spirochete, the agent of relapsing fever, recently cultured on axenic medium. Historically, massive outbreaks have occurred in Eurasia and Africa, but currently the disease is found only in Ethiopia and neighboring countries. Bartonella quintana is now recognized as an agent of bacillary angiomatosis bacteremia, trench fever, endocarditis, and chronic lymphadenopathy among the homeless. Rickettsia prowazekii is the agent of epidemic typhus. The most recent outbreak (and the largest since World War II) was observed in Burundi. A small outbreak was also reported in Russia in 1997. Louse infestation appears to become more prevalent worldwide, associated with a decline in social and hygienic conditions provoked by civil unrest and economic instability. (+info)Bartonella quintana and urban trench fever. (4/63)
Contemporary Bartonella quintana infections have emerged in diverse regions of the world, predominantly involving socially disadvantaged persons. Available data suggest that the human body louse Pediculus humanus is the vector for transmission of B. quintana. Descriptions of the clinical manifestations associated with contemporary B. quintana infections have varied considerably and include asymptomatic infection, a relapsing febrile illness, headache, leg pain, "culture-negative" endocarditis, and, in human immunodeficiency virus-infected persons, bacillary angiomatosis. Laboratory diagnosis is most convincing when B. quintana is isolated in blood culture, but growth often takes 20-40 days; problems exist with both sensitivity and specificity of serological assays. On the basis of available information, use of doxycycline, erythromycin, or azithromycin to treat B. quintana infections is recommended. Treatment of uncomplicated B. quintana bacteremia for 4-6 weeks and treatment of B. quintana endocarditis (in a person who does not undergo valve surgery) for 4-6 months are recommended, with the addition of a bactericidal agent (such as a third-generation cephalosporin or an aminoglycoside) during the initial 2-3 weeks of therapy for endocarditis. (+info)Detection and culture of Bartonella quintana, Serratia marcescens, and Acinetobacter spp. from decontaminated human body lice. (5/63)
As part of a survey for trench fever among homeless people in Marseilles, France, we attempted isolation of Bartonella quintana from body lice. A decontamination protocol of immersion in 70% ethanol with 0.2% iodine was devised and was tested with a laboratory colony of body lice. Lice which had been experimentally contaminated with either Escherichia coli, Staphylococcus epidermidis, or Acinetobacter spp. were successfully decontaminated, and this process did not prevent the culture of B. quintana from these lice. One hundred sixty-one lice obtained from homeless patients were studied by the protocol. B. quintana was isolated on axenic medium from 15 of 161 body lice and was detected in 41 of 161 lice by PCR. Acinetobacter spp. and Serratia marcescens were also isolated from body lice. The sensitivities of PCR and culture of B. quintana were 98 and 36%, respectively. These procedures may be useful for epidemiologic studies of trench fever and for the recovery of strains for characterization and comparison. (+info)Prosthetic valve endocarditis caused by Bartonella quintana. (6/63)
We describe the first case of Bartonella quintana endocarditis affecting a prosthetic valve in a person with no known risk factors for this infection. Bartonella should be considered as a cause of endocarditis in any clinical setting. (+info)Bartonella quintana Bacteremia among Homeless People. (7/63)
Bartonella quintana infections have recently reemerged, predominantly among the homeless populations in cities in both Europe and the United States. B. quintana can cause trench fever, endocarditis, and chronic bacteremia; the human body louse is the only known vector. Homeless people who presented to the emergency departments of University Hospital in Marseilles, France, were studied, as were those who had been admitted to other medical facilities in the city since 1 January 1997. Samples of blood and body lice were collected for culture for B. quintana and for serological testing. Bartonella bacteremia was associated with sweats, evidence of louse infestation, serological tests that were positive for B. quintana, and high titers of B. quintana antibody. Bacteremia was also associated with being homeless for <3 years. Asymptomatic, prolonged bacteremia (duration, up to 78 weeks) and intermittent bacteremia were found to occur. Data obtained regarding antibiotic regimens showed that treatment with gentamicin and doxycycline was effective in preventing relapses of bacteremia. (+info)Comparison of in-house and commercial slides for detection by immunofluorescence of immunoglobulins G and M against Bartonella henselae and Bartonella quintana. (8/63)
We compared the sensitivities and specificities of indirect fluorescent antibody tests developed in our laboratory and commercially available from Focus Technologies (FT; formerly MRL Diagnostic) for detection of serum antibodies to Bartonella spp. Serum samples tested were from patients with culture- or PCR-confirmed Bartonella quintana or B. henselae infections causing cat scratch disease (CSD), chronic bacteremia, or endocarditis. At a cutoff titer of 64, the FT test had higher sensitivity than our in-house test in detecting anti-B. henselae immunoglobulin G (IgG) antibodies in CSD patients (91.2 versus 52.9%; P < 0.001). The specificity in serum samples from 85 control patients was, however, lower with the FT test (87%) than with the in-house test (98.8%) (P = 0.002). A cutoff titer of 128 improves the specificity for the FT test but lowers the sensitivity to 85%. For patients infected with B. henselae, our in-house test, but not the FT test, enabled endocarditis to be detected more reliably. With the in-house test, titers of IgG against B. henselae of >/=1,024 were found only in endocarditis patients and not in CSD patients. With the FT test, 19.1% of CSD patients had titers of IgG against B. henselae of >/=1,024 (P < 0.001). Our in-house technique also improved detection of anti-B. quintana antibodies in homeless patients with endocarditis. IgG titers of >/=1,024 were present in 75% of serum samples, but only in 16.7% of serum samples with the FT test (P = 0.004). Since each test has advantages over the other, the serological diagnosis of Bartonella infections would benefit if both tests were used concurrently. (+info)Trench fever is a historical medical condition that primarily affected soldiers during World War I. It is caused by Bartonella quintana, a type of bacterium that is transmitted through the feces of body lice. The name "trench fever" comes from the fact that it was common among soldiers living in trenches, where poor hygiene and crowded conditions facilitated the spread of the disease.
Symptoms of trench fever include sudden onset of fever, severe headache, muscle pain, and a rash. The fever typically lasts for about five days and then recurs every four to six days, which is why it was also known as "five-day fever" or "recrudescence fever." Other symptoms can include fatigue, anemia, and swelling of the spleen and liver.
Trench fever is treated with antibiotics such as doxycycline or azithromycin. Prevention measures include good personal hygiene, such as regular bathing and changing clothes, as well as environmental controls to reduce louse populations, such as delousing stations and insecticides.
While trench fever is no longer a major public health concern, it remains an important historical medical condition that highlights the importance of hygiene and infection control in military settings.
Bartonella quintana is a gram-negative, aerobic bacillus that is the causative agent of trench fever, a disease first described during World War I. The bacterium is primarily transmitted to humans through the feces of body lice, and it can also cause endocarditis and other systemic infections.
The name "quintana" refers to the characteristic fever pattern of the disease, which features recurring episodes every fifth day. Other symptoms of trench fever include headache, muscle pain, and a rash. The disease is typically treated with antibiotics, such as doxycycline or azithromycin.
Bartonella quintana is also known to cause cat scratch disease in immunocompromised individuals. It can be transmitted through the scratches or bites of cats infected with the bacterium. The symptoms of cat scratch disease include fever, swollen lymph nodes, and fatigue.
Overall, Bartonella quintana is a significant public health concern, particularly in populations with poor hygiene and crowded living conditions, such as homeless individuals and refugees.
"Pediculus" is the medical term for a type of small, wingless parasitic insect that can be found in human hair and on the body. There are two main species that affect humans:
1. Pediculus humanus capitis - also known as the head louse, it primarily lives on the scalp and is responsible for causing head lice infestations.
2. Pediculus humanus corporis - also known as the body louse, it typically lives in clothing and on the body, particularly in seams and folds of clothing, and can cause body lice infestations.
Both species of Pediculus feed on human blood and can cause itching and skin irritation. They are primarily spread through close personal contact and sharing of items such as hats, combs, and clothing.
Epidemic Typhus, also known as Louse-Born Typhus, is a severe, infectious disease caused by the bacterium Rickettsia prowazekii. The disease is primarily transmitted to humans through the infected body lice (Pediculus humanus corporis) or their feces.
The typical symptoms of Epidemic Typhus include sudden onset of fever, severe headache, muscle pain, and a rash that usually appears around day 5 of illness. The rash starts on the trunk and then spreads to the arms and legs, but it does not typically affect the face, palms, or soles. Other possible symptoms are cough, nausea, vomiting, abdominal pain, and diarrhea. Complications can be severe and include delirium, seizures, pneumonia, and inflammation of the heart, lungs, or brain.
Epidemic Typhus is a serious disease that requires prompt medical attention and treatment with antibiotics, such as doxycycline or tetracycline. If left untreated, Epidemic Typhus can be fatal in up to 30% of cases. It is more common in areas of poor hygiene, overcrowding, and where there is a lack of access to medical care. Outbreaks of Epidemic Typhus have occurred during wars, natural disasters, and other situations that lead to large-scale population displacement.
Phthiraptera is an order of small parasitic insects, also known as lice. They are characterized by having a specialized body structure adapted for living in close association with birds and mammals. There are three main subgroups: Anoplura (sucking lice), Ischnocera (chewing lice), and Rhynchophthirina (large-biting lice). Lice can cause itching, discomfort, and spread diseases to their hosts.
Rickettsiaceae is a family of Gram-negative, obligate intracellular bacteria that are primarily parasitic in arthropods and mammals. They are the causative agents of several important human diseases, including typhus fever, Rocky Mountain spotted fever, and rickettsialpox. These bacteria are typically transmitted to humans through the bites of infected arthropods such as ticks, fleas, or lice.
The bacteria in Rickettsiaceae are small, non-motile, and have a unique bipolar appearance with tapered ends. They can only replicate inside host cells, where they manipulate the host cell's machinery to create a protective niche for themselves. This makes them difficult to culture and study outside of their hosts.
Rickettsiaceae bacteria are divided into several genera based on their genetic and antigenic characteristics, including Rickettsia, Orientia, and Coxiella. Each genus contains several species that can cause different diseases in humans. For example, Rickettsia rickettsii is the causative agent of Rocky Mountain spotted fever, while Rickettsia prowazekii causes epidemic typhus.
Overall, Rickettsiaceae bacteria are important pathogens that can cause serious and sometimes fatal diseases in humans. Prompt diagnosis and treatment with appropriate antibiotics is essential for a successful outcome.
"Bartonella" is a genus of gram-negative bacteria that are facultative intracellular pathogens, meaning they can live and multiply inside host cells. They are the cause of several emerging infectious diseases in humans and animals. Some species of Bartonella are associated with clinical syndromes such as cat scratch disease, trench fever, and Carrion's disease. The bacteria are transmitted to humans through the bites or feces of insect vectors (such as fleas, lice, and sandflies) or through contact with infected animals. Once inside the host, Bartonella can evade the immune system and cause chronic infection, which can lead to a variety of clinical manifestations, including fever, fatigue, lymphadenopathy, endocarditis, and neurological symptoms.
The medical definition of 'Bartonella' is: A genus of fastidious, gram-negative bacteria that are facultative intracellular pathogens. Bartonella species are the cause of several emerging infectious diseases in humans and animals. The bacteria are transmitted to humans through the bites or feces of insect vectors (such as fleas, lice, and sandflies) or through contact with infected animals. Bartonella species can evade the immune system and cause chronic infection, leading to a variety of clinical manifestations, including fever, fatigue, lymphadenopathy, endocarditis, and neurological symptoms.
Bartonella infections are a group of diseases caused by bacteria belonging to the Bartonella genus. These gram-negative bacteria can infect humans and animals, causing various symptoms depending on the specific Bartonella species involved. Some common Bartonella infections include:
1. Cat scratch disease (Bartonella henselae): This is the most common Bartonella infection, usually transmitted through contact with a cat's scratch or saliva. The primary symptom is a tender, swollen lymph node near the site of the scratch. Other symptoms may include fever, fatigue, and headache.
2. Trench fever (Bartonella quintana): This infection was first identified during World War I among soldiers living in trenches, hence its name. It is primarily transmitted through the feces of body lice. Symptoms include fever, severe headaches, muscle pain, and a rash.
3. Carrion's disease (Bartonella bacilliformis): This infection is endemic to South America, particularly in the Andean regions of Peru, Ecuador, and Colombia. It is transmitted through the bite of sandflies. The acute phase of the disease, known as Oroya fever, is characterized by high fever, severe anemia, and potentially life-threatening complications. The chronic phase, known as verruga peruana, presents with skin lesions resembling warts or boils.
Diagnosis of Bartonella infections typically involves blood tests to detect antibodies against the bacteria or direct detection of the bacterial DNA using PCR techniques. Treatment usually consists of antibiotics such as azithromycin, doxycycline, or rifampin, depending on the specific infection and severity of symptoms.
Immersion foot, also known as trench foot, is a medical condition that occurs when the feet are exposed to cold and wet conditions for prolonged periods. It is not necessarily caused by immersion in water, but rather by the persistent dampness and chilling of the feet.
The symptoms can include numbness, pain, swelling, redness, and blistering. In severe cases, it can lead to tissue damage and even gangrene, which may require amputation. It's important to note that this condition can occur at temperatures above freezing, and it's often associated with poor hygiene and lack of proper foot care. Early treatment is crucial to prevent serious complications.
Fever, also known as pyrexia or febrile response, is a common medical sign characterized by an elevation in core body temperature above the normal range of 36.5-37.5°C (97.7-99.5°F) due to a dysregulation of the body's thermoregulatory system. It is often a response to an infection, inflammation, or other underlying medical conditions, and it serves as a part of the immune system's effort to combat the invading pathogens or to repair damaged tissues.
Fevers can be classified based on their magnitude:
* Low-grade fever: 37.5-38°C (99.5-100.4°F)
* Moderate fever: 38-39°C (100.4-102.2°F)
* High-grade or severe fever: above 39°C (102.2°F)
It is important to note that a single elevated temperature reading does not necessarily indicate the presence of a fever, as body temperature can fluctuate throughout the day and can be influenced by various factors such as physical activity, environmental conditions, and the menstrual cycle in females. The diagnosis of fever typically requires the confirmation of an elevated core body temperature on at least two occasions or a consistently high temperature over a period of time.
While fevers are generally considered beneficial in fighting off infections and promoting recovery, extremely high temperatures or prolonged febrile states may necessitate medical intervention to prevent potential complications such as dehydration, seizures, or damage to vital organs.
There is no single, universally accepted medical definition of "homeless persons." However, in the public health and healthcare contexts, homeless individuals are often defined as those who lack a fixed, regular, and adequate nighttime residence. This can include people who are living on the streets, in shelters, vehicles, or other temporary or emergency housing situations. The McKinney-Vento Homeless Assistance Act, a major federal law in the United States that provides funding for homeless services programs, defines homeless individuals as those who lack a fixed, regular, and adequate nighttime residence, and includes people who are living in shelters, transitional housing, or doubled up with family or friends due to loss of housing, economic hardship, or similar reasons.
Q fever is a zoonotic disease caused by the bacterium Coxiella burnetii. It is characterized by acute or chronic flu-like symptoms, pneumonia, and hepatitis. The bacteria are primarily transmitted to humans through inhalation of contaminated dust or aerosols from infected animals such as cattle, sheep, and goats. Q fever can also be transmitted through consumption of unpasteurized milk or direct contact with infected animals. It is often asymptomatic or mildly symptomatic in animals but can cause severe disease in humans.
The acute form of Q fever typically presents with sudden onset of high fever, severe headache, fatigue, muscle pain, and cough. Some patients may also develop pneumonia or hepatitis. The chronic form of the disease is less common but more serious, often affecting people with compromised immune systems. Chronic Q fever can lead to endocarditis, an infection of the inner lining of the heart, which can be life-threatening if left untreated.
Diagnosis of Q fever typically involves a combination of clinical evaluation, serological testing, and PCR (polymerase chain reaction) assays. Treatment usually involves antibiotics such as doxycycline or fluoroquinolones for several weeks to months, depending on the severity and duration of the illness. Prevention measures include avoiding contact with infected animals, wearing protective clothing and masks when handling animal products, and pasteurizing milk before consumption.
Radioactive water pollutants refer to contaminants in water sources that contain radioactive materials. These materials can include substances such as radium, uranium, and cesium, which emit ionizing radiation. This type of pollution can occur through various means, including the disposal of radioactive waste from nuclear power plants, hospitals, and research facilities; oil and gas drilling operations; and mining activities.
Exposure to radioactive water pollutants can have serious health consequences, as ionizing radiation has been linked to an increased risk of cancer, genetic mutations, and other harmful effects. Therefore, it is essential to regulate and monitor radioactive water pollution to protect public health and the environment.
Yellow fever is an acute viral hemorrhagic disease that's transmitted to humans through the bite of infected mosquitoes. The "yellow" in the name refers to the jaundice that can occur in some patients, resulting from liver damage caused by the virus. The disease is endemic in tropical regions of Africa and Central and South America.
The yellow fever virus is a single-stranded RNA virus that belongs to the Flaviviridae family, genus Flavivirus. It's closely related to other mosquito-borne viruses like dengue and Zika. The virus has three distinct geographical variants (West African, East African, and South American), each with different epidemiological patterns and clinical features.
The incubation period for yellow fever is typically 3 to 6 days after infection. The initial symptoms include fever, chills, headache, back pain, myalgia, and fatigue. Most patients recover after this initial phase, but around 15% of those infected enter a more severe phase characterized by high fever, jaundice, abdominal pain, vomiting, bleeding, and often rapid death within 7 to 10 days.
There is no specific treatment for yellow fever, and management is focused on supportive care, including fluid replacement, blood transfusions, and addressing any complications that arise. Prevention relies on vaccination and mosquito control measures. The yellow fever vaccine is safe and highly effective, providing immunity in 95% of those who receive it. A single dose offers lifelong protection in most individuals. Mosquito control efforts, such as reducing breeding sites and using insecticide-treated materials, can help prevent the spread of the virus in affected areas.
Typhoid fever is an acute illness caused by the bacterium Salmonella enterica serovar Typhi. It is characterized by sustained fever, headache, constipation or diarrhea, rose-colored rash (in some cases), abdominal pain, and weakness. The bacteria are spread through contaminated food, water, or direct contact with an infected person's feces. If left untreated, typhoid fever can lead to severe complications and even be fatal. It is diagnosed through blood, stool, or urine tests and treated with antibiotics. Vaccination is available for prevention.
A lice infestation, also known as pediculosis, is a condition characterized by the presence and multiplication of parasitic insects called lice on a person's body. The three main types of lice that can infest humans are:
1. Head lice (Pediculus humanus capitis): These lice primarily live on the scalp, neck, and behind the ears, feeding on human blood. They lay their eggs (nits) on hair shafts close to the scalp. Head lice infestations are most common in children aged 3-12 years old.
2. Body lice (Pediculus humanus corporis): These lice typically live and lay eggs on clothing, particularly seams and collars, near the body's warmest areas. They move to the skin to feed on blood, usually at night. Body lice infestations are more common in people who experience homelessness or overcrowded living conditions with limited access to clean clothing and hygiene facilities.
3. Pubic lice (Pthirus pubis): Also known as crab lice, these lice primarily live in coarse body hair, such as the pubic area, armpits, eyelashes, eyebrows, beard, or mustache. They feed on human blood and lay eggs on hair shafts close to the skin. Pubic lice infestations are typically sexually transmitted but can also occur through close personal contact with an infected individual or sharing contaminated items like bedding or clothing.
Symptoms of a lice infestation may include intense itching, tickling sensations, and visible red bumps or sores on the skin caused by lice bites. In some cases, secondary bacterial infections can occur due to scratching. Diagnosis is usually made through visual identification of lice or nits on the body or clothing. Treatment typically involves topical medications, such as shampoos, creams, or lotions, and thorough cleaning of bedding, clothing, and personal items to prevent reinfestation.
Anoplura is an order of insects that are external parasites, specifically known as sucking lice. They are ectoparasites that live on the skin and hair of mammals, including humans, and feed on their blood. Anoplura species have a specialized mouthpart called a fascicle, which consists of several parts working together to pierce the host's skin and suck blood.
The most common and medically significant example of Anoplura is Pediculus humanus, which includes two subspecies: P. h. capitis (head louse) and P. h. corporis (body louse). These species are obligate parasites that can only survive on human hosts. Infestations with these lice can cause skin irritation, itching, and the transmission of diseases such as typhus and trench fever.
It is important to note that Anoplura species are not to be confused with other types of lice, such as chewing lice (Mallophaga), which primarily feed on dead skin scales and hair rather than blood.
Scalp dermatoses refer to various skin conditions that affect the scalp. These can include inflammatory conditions such as seborrheic dermatitis (dandruff, cradle cap), psoriasis, atopic dermatitis (eczema), and lichen planus; infectious processes like bacterial folliculitis, tinea capitis (ringworm of the scalp), and viral infections; as well as autoimmune conditions such as alopecia areata. Symptoms can range from mild scaling and itching to severe redness, pain, and hair loss. The specific diagnosis and treatment of scalp dermatoses depend on the underlying cause.
 Trench fever
Trench fever Trench Fever: Practice Essentials, Background, Pathophysiology
Trench Fever: Practice Essentials, Background, Pathophysiology What is Trench Fever|Causes|Symptoms|Treatment|Risk Factors|Prevention
What is Trench Fever|Causes|Symptoms|Treatment|Risk Factors|Prevention Trench Fever - Infectious Diseases - MSD Manual Professional Edition
Trench Fever - Infectious Diseases - MSD Manual Professional Edition Trench mouth: MedlinePlus Medical Encyclopedia
Trench mouth: MedlinePlus Medical Encyclopedia Ancient Diseases Plague Canada's Homeless Communities - Invisible People
Ancient Diseases Plague Canada's Homeless Communities - Invisible People Today's Homeless Are Getting 'Trench Fever,' Infamous from WW I | San Juan Regional Medical Center
Today's Homeless Are Getting 'Trench Fever,' Infamous from WW I | San Juan Regional Medical Center help with editing music
help with editing music Lymphocytosis: Definition, symptoms, and causes
Lymphocytosis: Definition, symptoms, and causes Academic Subject: Poetry-Collections of Poems
Academic Subject: Poetry-Collections of Poems Rogers, Travers Guy (Oral history) | Imperial War Museums
Rogers, Travers Guy (Oral history) | Imperial War Museums Historical Review: Rickettsial Diseases and Their Impact on U.S. Military Forces | Health.mil
Historical Review: Rickettsial Diseases and Their Impact on U.S. Military Forces | Health.mil Advanced Search Results - Public Health Image Library(PHIL)
Advanced Search Results - Public Health Image Library(PHIL) Coming Soon: Horseshoes And Horsepower - WIBC 93.1 FM
Coming Soon: Horseshoes And Horsepower - WIBC 93.1 FM Gibert-Knowlton-Lytle Family Papers - Library
Gibert-Knowlton-Lytle Family Papers - Library Graphic Guide to Infectious Disease Elsevier eBook on VitalSource (Retail Access Card), 1st Edition - 9780323442169
Graphic Guide to Infectious Disease Elsevier eBook on VitalSource (Retail Access Card), 1st Edition - 9780323442169 EENY-103/IN260: Crab Louse, Pthirus pubis (Linnaeus) (Insecta: Phthiraptera (Anoplura): Pediculidae)
EENY-103/IN260: Crab Louse, Pthirus pubis (Linnaeus) (Insecta: Phthiraptera (Anoplura): Pediculidae) Life and Times of J.R.R. Tolkien Essay - Free Essay Example | Artscolumbia
Life and Times of J.R.R. Tolkien Essay - Free Essay Example | Artscolumbia Recommendations of the ITFDE
Recommendations of the ITFDE The Hobbit at 80: What were JRR Tolkien's inspirations behind his first fantasy tale of Middle Earth? | The Independent | The...
The Hobbit at 80: What were JRR Tolkien's inspirations behind his first fantasy tale of Middle Earth? | The Independent | The... In memory of the fallen of the University: 1914-1918 | Bangor University
In memory of the fallen of the University: 1914-1918 | Bangor University Jenny Turner · Reasons for Liking Tolkien: The Hobbit Habit
Jenny Turner · Reasons for Liking Tolkien: The Hobbit Habit Head and body lice splice their identical genes differently | New Scientist
Head and body lice splice their identical genes differently | New Scientist Inglis, William Keith - Faculty of Medicine Online Museum and Archive
Inglis, William Keith - Faculty of Medicine Online Museum and Archive Students showcase summer research projects at SURF Symposium - Montana Tech - Montana's Premier STEM University
Students showcase summer research projects at SURF Symposium - Montana Tech - Montana's Premier STEM University