Tracheoesophageal Fistula
Esophageal Atresia
Larynx, Artificial
Speech, Esophageal
Esophagus
Speech, Alaryngeal
Abnormalities, Multiple
Fistula
Esophageal atresia and tracheoesophageal fistula. (1/109)
Esophageal atresia, with or without tracheoesophageal fistula, is a fairly common congenital disorder that family physicians should consider in the differential diagnosis of a neonate who develops feeding difficulties and respiratory distress in the first few days of life. Esophageal atresia is often associated with other congenital anomalies, most commonly cardiac abnormalities such as ventricular septal defect, patent ductus arteriosus or tetralogy of Fallot. Prompt recognition, appropriate clinical management to prevent aspiration, and swift referral to an appropriate tertiary care center have resulted in a significant improvement in the rates of morbidity and mortality in these infants over the past 50 years. (+info)Respiratory function in childhood following repair of oesophageal atresia and tracheoesophageal fistula. (2/109)
AIM: To determine the relation between respiratory function in infancy and at school age in children who have undergone oesophageal atresia and tracheoesophageal fistula repair, and assess the value of infant respiratory function testing; and to examine the effect of bronchodilators. METHOD: Fourteen children (6 girls, and 8 boys) who had undergone respiratory function testing in infancy were retested at school age (7-12 years). Measurements included lung volume, airways resistance, peak flow, and spirometry. Clinical problems were investigated by questionnaire. Twelve children had repeat measurements after taking salbutamol. RESULTS: Predominant complaints were non-productive cough and dysphagia, but even those children with major problems in infancy reported few restrictions at school or in sport or social activities. Respiratory function and clinical findings at school age appeared unrelated to status in infancy, such that even the patients with severe tracheomalacia requiring aortopexy did not have lung function testing suggestive of malacia at school age. Most patients showed a restrictive pattern of lung volume which would appear to result from reduced lung growth after surgery rather than being a concomitant feature of the primary congenital abnormality. Although six children reported wheeze and four had a diagnosis of asthma, only one responded to salbutamol. This suggests that a tendency to attribute all lower respiratory symptoms to asthma may have led to an overdiagnosis of this condition in this patient group. CONCLUSION: Respiratory function testing in infancy is of limited value in medium term prognosis, but may aid management of contemporary clinical signs. In children respiratory function testing is valuable in assessing suspected asthma and effects of bronchodilators. (+info)Increased fetal nuchal translucency: possible association with esophageal atresia. (3/109)
We describe a case in which in-utero diagnosis of an esophageal atresia with a tracheo-esophageal fistula in the third trimester followed the finding of an increased nuchal translucency in the first trimester and suggest a mechanism by which these two findings might be associated. (+info)Oesophageal atresia in the South West of England. (4/109)
A retrospective anatomical and family study was made of 345 patients with oesophageal atresia who were born in the South West of England between 1942 and 1973. There were 186 males and 159 females. Twenty-one cases were stillborn. Eighty-five percent of the patients had a combination of oesophageal atresia with a tracheo-oesophageal fistula to the distal oesophageal segment, and 9 percent had atresia without a fistula. Fifty-five per cent of the patients had other congenital malformations and these tended to be multiple rather than single. Thirty-six per cent of singletons had unequivocal fetal growth retardation, and there is some evidence that nearly all cases have poor fetal growth. There appeared to be a maternal age effect, with an excess of mothers under 20 and over 35, and there was an unexplained excess of fathers employed in the Armed Forces. Ten per cent of the cases were illegitimate. There were 21 twins which is nearly three times the expected number; there were two pairs of twins concordant for oesophageal atresia, one being monozygotic and the other dizygotic. In one case there were two sibs with oesophageal atresia. Five out of 365 sibs had anencephaly. The blood group distributions of the patients and their mothers did not significantly differ from the expected distribution. Oesophageal atresia is aetiologically heterogenous. In this series there were at least five, and probably 10 cases of trisomy 18 and four cases of trisomy 21. Five mothers had overt diabetes, and there is some suggestion from other work that maternal diabetes or its treatment may be aetiologically important. Oesophageal atresia was part of a possibly recessively inherited malformation syndrome in two cases. A sibship with a case of rectal atresia, a case of Hirschprung's disease and a case of oesophageal atresia may represent the action of another recessive gene. It seems likely that oesophageal atresia is a rather non-specific consequence of several teratological processes. (+info)Separation between the digestive and the respiratory lumina during the human embryonic period: morphometric study along the tracheo-oesophageal septum. (5/109)
An isolated tracheo-oesophageal fistula could be caused by close proximity of the epithelia of both organs (O'Rahilly & Muller, 1984; Kluth et al. 1987) at certain embryonic stages, the most frequent location being the tracheal bifurcation. Thus the relative position and degree of separation between the digestive and the respiratory tubes throughout their development may be relevant to the origin of this anomaly. The aim of this study was to analyse along the different segments of the tracheo-oesophageal septum (TES) where the closest relationship between both lumina occurred and what degree of separation was present at each segment. Computer imaging techniques were applied on cross sections of a graded series of normal human embryos (Carnegie stages (CS) 13-23). In addition, the differentiation of the primitive TES was also studied (from CS 12) by light microscopy. Between CS 13 and 16 both tubes tended to separate (phase of separation), principally at the proximal segments of the laryngopharyngeal and the tracheo-oesophageal portions of the TES. During this phase the separation between the trachea and oesophagus was wider than between the larynx and pharynx. From CS 17 to CS 23 the digestive and respiratory lumina reached their widest separation at different levels of the laryngopharyngeal portion. Below these levels they tended to come closer together, principally at the proximal segment of the tracheo-oesophageal portion, but also at the distal part of the laryngopharyngeal portion. During this phase of approximation they reached their closest relationship at the proximal (CS 17) and the distal (from CS 18) segments of the tracheo-oesophageal portion. When finally the distal segment of the trachea (which includes the bifurcation) comes closest to the oesophagus, the coats of both organs have already undergone an appreciable differentiation. According to these observations, the origin of the most frequent isolated tracheo-oesophageal fistula at the bifurcation region could not be explained from the normal development of the TES. (+info)Evidence of a common pathogenesis for foregut duplications and esophageal atresia with tracheo-esophageal fistula. (6/109)
The pathogenesis of the alimentary tract duplications, including foregut duplications (FgD) remains speculative. The accidental finding of FgD in fetal rats with esophageal atresia and tracheoesophageal fistula (EA-TEF) induced by Adriamycin provided an animal model to investigate a possible relationship between these two entities. Timed-pregnant rats were intraperitoneally injected with Adriamycin (1.75 mg/kg) on gestational Days 6 to 9. Their embryos were harvested by Caesarean section from gestational Days 14 to 21. Forty-six of embryos were processed and serially sectioned in the transverse or sagittal planes. EA-TEF occurred in 43/46 (93%) embryos of which 11 (24%) were found to have an associated FgD located at the level where the esophagus was absent. Six FgDs communicated with the foregut or the trachea. Five noncommunicating FgDs were located between the foregut and the vertebral column. In the control embryo, the notochord was located in the centre of the vertebral column from Day 11 of the gestation. In Day 14, 15 and 16, however, embryos exposed to Adriamycin, an abnormal notochord or branch frequently was located within the mesenchyme of the maldeveloped foregut or attached to the duplication cyst. In some, it appeared that the notochord was drawing the cyst-like structure away from the foregut. The present study confirms that duplications adjacent to the esophagus arise from the foregut and that failure of the foregut to detach from the notochord at the normal time may contribute to the development of foregut duplications. (+info)Unilateral bronchiectasis and esophageal dysmotility in congenital adult tracheoesophageal fistula. (7/109)
Tracheoesophageal fistulas (TEF) in adults are most commonly neoplastic, and very rarely congenital in nature. We report a 45-year-old Hispanic male with TEF and initial presentation of minimal hemoptysis. The patient had radiographic evidence of unilateral upper lobe (RUL) bronchiectasis, massive esophageal dilatation, and dysmotility. However, there was no evidence of esophageal malignancy, achalasia, or Chagas' disease. Bronchoscopy revealed a large TEF in the posterior wall of trachea, which was not visualized on esophagram or esophagoscopy. Bronchoalveolar lavage (BAL) cultures grew Mycobacterium avium complex (MAC). Our report illustrates that idiopathic, or congenital, TEF can be associated with esophageal dysmotility, adulthood bronchiectasis, and atypical mycobacterial superinfection. (+info)Button battery ingestion: an analysis of 25 cases. (8/109)
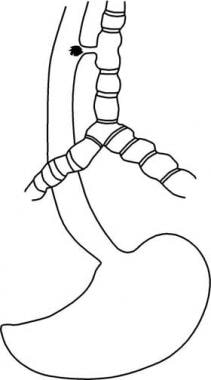
BACKGROUND: Button batteries represent a distinct type of foreign body. Serious complications can be resulted, particularly when the battery is impacted in the esophagus. The potentially detrimental effects of button battery ingestion have often been overlooked in Taiwan. We surveyed patients following button battery ingestion to define the characteristics and outcomes of this population. METHODS: The records of 25 patients with button battery ingestion that had been reported to the Taipei Veterans General Hospital Poison Control Center from July 1988 through January 1998 were retrospectively reviewed. RESULTS: Button battery ingestion occurred most commonly in male children (N=20; 80%) and children under 3 years of age (N= 19; 76%). Most children were asymptomatic (N=22; 88%). Two children suffered abdominal pain, and one suffered dyspnea and stridor. Reported complications included black stools (N=3) and tracheoesophageal fistula formation (N= 1). Two children underwent endoscopic battery removal, and batteries passed the entire gastrointestinal tract in all other subjects. The interval between battery ingestion and passage when documented (N= 16) was never more than 5 days. CONCLUSION: Most ingested batteries passed through the gastrointestinal tract without any adverse effects. An initial roentgenogram should be obtained promptly to determine battery location and diameter, and the battery's chemical composition should be determined when possible. Esophageal impaction of the batteries requires emergency endoscopic or surgical removal. For patients without esophageal impaction, conservative intervention is recommended in the absence of symptoms and signs of injury. (+info)A tracheoesophageal fistula (TEF) is an abnormal connection between the trachea (windpipe) and the esophagus (tube that carries food from the mouth to the stomach). This congenital anomaly is usually present at birth and can vary in size and location. It can cause complications such as respiratory distress, feeding difficulties, and recurrent lung infections. TEF is often treated surgically to separate the trachea and esophagus and restore their normal functions.
Esophageal atresia is a congenital condition in which the esophagus, the tube that connects the throat to the stomach, does not develop properly. In most cases, the upper esophagus ends in a pouch instead of connecting to the lower esophagus and stomach. This condition prevents food and liquids from reaching the stomach, leading to difficulty swallowing and feeding problems in newborn infants. Esophageal atresia often occurs together with a congenital defect called tracheoesophageal fistula, in which there is an abnormal connection between the esophagus and the windpipe (trachea).
The medical definition of 'Esophageal Atresia' is:
A congenital anomaly characterized by the absence of a normal connection between the upper esophagus and the stomach, resulting in the separation of the proximal and distal esophageal segments. The proximal segment usually ends in a blind pouch, while the distal segment may communicate with the trachea through a tracheoesophageal fistula. Esophageal atresia is often associated with other congenital anomalies and can cause serious complications if not diagnosed and treated promptly after birth.
An artificial larynx, also known as a voice prosthesis or speech aid, is a device used to help individuals who have undergone a laryngectomy (surgical removal of the larynx) or have other conditions that prevent them from speaking normally. The device generates sound mechanically, which can then be shaped into speech by the user.
There are two main types of artificial larynx devices:
1. External: This type of device consists of a small electronic unit that produces sound when the user presses a button or activates it with a breath. The sound is then directed through a tube or hose into a face mask or a mouthpiece, where the user can shape it into speech.
2. Internal: An internal artificial larynx, also known as a voice prosthesis, is implanted in the body during surgery. It works by allowing air to flow from the trachea into the esophagus and then through the voice prosthesis, which creates sound that can be used for speech.
Both types of artificial larynx devices require practice and training to use effectively, but they can significantly improve communication and quality of life for individuals who have lost their natural voice due to laryngeal cancer or other conditions.
Esophageal speech is not a type of "speech" in the traditional sense, but rather a method of producing sounds or words using the esophagus after a laryngectomy (surgical removal of the voice box). Here's a medical definition:
Esophageal Speech: A form of alaryngeal speech produced by swallowing air into the esophagus and releasing it through the upper esophageal sphincter, creating vibrations that are shaped into sounds and words. This method is used by individuals who have undergone a laryngectomy, where the vocal cords are removed, making traditional speech impossible. Mastering esophageal speech requires extensive practice and rehabilitation.
Esophageal stenosis is a medical condition characterized by the narrowing or constriction of the esophagus, which is the muscular tube that connects the throat to the stomach. This narrowing can make it difficult to swallow food and liquids, leading to symptoms such as dysphagia (difficulty swallowing), pain or discomfort while swallowing, regurgitation, and weight loss.
Esophageal stenosis can be caused by a variety of factors, including:
1. Scarring or fibrosis due to prolonged acid reflux or gastroesophageal reflux disease (GERD)
2. Radiation therapy for cancer treatment
3. Ingestion of corrosive substances
4. Eosinophilic esophagitis, an allergic condition that affects the esophagus
5. Esophageal tumors or cancers
6. Surgical complications
Depending on the underlying cause and severity of the stenosis, treatment options may include medications to manage symptoms, dilation procedures to widen the narrowed area, or surgery to remove the affected portion of the esophagus. It is important to seek medical attention if you experience any difficulty swallowing or other symptoms related to esophageal stenosis.
The esophagus is the muscular tube that connects the throat (pharynx) to the stomach. It is located in the midline of the neck and chest, passing through the diaphragm to enter the abdomen and join the stomach. The main function of the esophagus is to transport food and liquids from the mouth to the stomach for digestion.
The esophagus has a few distinct parts: the upper esophageal sphincter (a ring of muscle that separates the esophagus from the throat), the middle esophagus, and the lower esophageal sphincter (another ring of muscle that separates the esophagus from the stomach). The lower esophageal sphincter relaxes to allow food and liquids to enter the stomach and then contracts to prevent stomach contents from flowing back into the esophagus.
The walls of the esophagus are made up of several layers, including mucosa (a moist tissue that lines the inside of the tube), submucosa (a layer of connective tissue), muscle (both voluntary and involuntary types), and adventitia (an outer layer of connective tissue).
Common conditions affecting the esophagus include gastroesophageal reflux disease (GERD), Barrett's esophagus, esophageal cancer, esophageal strictures, and eosinophilic esophagitis.
Alaryngeal speech refers to the various methods of communicating without the use of the vocal folds (cords) in the larynx, which are typically used for producing sounds during normal speech. This type of communication is necessary for individuals who have lost their larynx or have a non-functioning larynx due to conditions such as cancer, trauma, or surgery.
There are several types of alaryngeal speech, including:
1. Esophageal speech: In this method, air is swallowed into the esophagus and then released in short bursts to produce sounds. This technique requires significant practice and training to master.
2. Tracheoesophageal puncture (TEP) speech: A small opening is created between the trachea and the esophagus, allowing air from the lungs to pass directly into the esophagus. A one-way valve is placed in the opening to prevent food and liquids from entering the trachea. The air passing through the esophagus produces sound, which can be modified with articulation and resonance to produce speech.
3. Electrolarynx: This is a small electronic device that is held against the neck or jaw and produces vibrations that are used to create sound for speech. The user then shapes these sounds into words using their articulatory muscles (lips, tongue, teeth, etc.).
Alaryngeal speech can be challenging to learn and may require extensive therapy and practice to achieve proficiency. However, with proper training and support, many individuals are able to communicate effectively using these methods.
A laryngectomy is a surgical procedure that involves the removal of the larynx, also known as the voice box. This is typically performed in cases of advanced laryngeal cancer or other severe diseases of the larynx. After the surgery, the patient will have a permanent stoma (opening) in the neck to allow for breathing. The ability to speak after a total laryngectomy can be restored through various methods such as esophageal speech, tracheoesophageal puncture with a voice prosthesis, or electronic devices.
'Abnormalities, Multiple' is a broad term that refers to the presence of two or more structural or functional anomalies in an individual. These abnormalities can be present at birth (congenital) or can develop later in life (acquired). They can affect various organs and systems of the body and can vary greatly in severity and impact on a person's health and well-being.
Multiple abnormalities can occur due to genetic factors, environmental influences, or a combination of both. Chromosomal abnormalities, gene mutations, exposure to teratogens (substances that cause birth defects), and maternal infections during pregnancy are some of the common causes of multiple congenital abnormalities.
Examples of multiple congenital abnormalities include Down syndrome, Turner syndrome, and VATER/VACTERL association. Acquired multiple abnormalities can result from conditions such as trauma, infection, degenerative diseases, or cancer.
The medical evaluation and management of individuals with multiple abnormalities depend on the specific abnormalities present and their impact on the individual's health and functioning. A multidisciplinary team of healthcare professionals is often involved in the care of these individuals to address their complex needs.
A fistula is an abnormal connection or passage between two organs, vessels, or body parts that usually do not connect. It can form as a result of injury, infection, surgery, or disease. A fistula can occur anywhere in the body but commonly forms in the digestive system, genital area, or urinary system. The symptoms and treatment options for a fistula depend on its location and underlying cause.
Voice quality, in the context of medicine and particularly in otolaryngology (ear, nose, and throat medicine), refers to the characteristic sound of an individual's voice that can be influenced by various factors. These factors include the vocal fold vibration, respiratory support, articulation, and any underlying medical conditions.
A change in voice quality might indicate a problem with the vocal folds or surrounding structures, neurological issues affecting the nerves that control vocal fold movement, or other medical conditions. Examples of terms used to describe voice quality include breathy, hoarse, rough, strained, or tense. A detailed analysis of voice quality is often part of a speech-language pathologist's assessment and can help in diagnosing and managing various voice disorders.
 Tracheoesophageal fistula
Tracheoesophageal fistula
Esophageal atresia
Tracheoesophageal septum
VACTERL association
Herpes esophagitis
Alexander Marmureanu
Double aortic arch
Tracheal agenesis
Weekend effect
Mandibulofacial dysostosis-microcephaly syndrome
Self-expandable metallic stent
NK2 homeobox 1
Esophagus
Tracheotomy
Lung bud
TBX2
Sonic hedgehog protein
Orvar Swenson
Trachea
Esophageal food bolus obstruction
Gollop-Wolfgang complex
C. Everett Koop
Pulmonary agenesis
Arthrogryposis
Fistula
Laryngeal cleft
Upper gastrointestinal series
TOF
Congenital heart defect
List of diseases (T)
Tracheoesophageal fistula - Wikipedia
 Esophageal atresia/tracheoesophageal fistula: MedlinePlus Genetics
Esophageal atresia/tracheoesophageal fistula: MedlinePlus Genetics
 Tracheoesophageal Fistula: Background, Pathophysiology, Etiology
Tracheoesophageal Fistula: Background, Pathophysiology, Etiology
 Oesophageal Atresia-Tracheoesophageal Fistula | Frontiers Research Topic
Oesophageal Atresia-Tracheoesophageal Fistula | Frontiers Research Topic
 Tracheoesophageal Fistula & Esophageal Atresia | University of Utah Health
Tracheoesophageal Fistula & Esophageal Atresia | University of Utah Health
 V013 Laparoscopic Collis-nissen Fundoplication In A Patient With Tracheoesophageal Fistula Repair from the SAGES Video Library
V013 Laparoscopic Collis-nissen Fundoplication In A Patient With Tracheoesophageal Fistula Repair from the SAGES Video Library
 Rendezvous technique using bronchoscopy and gastroscopy to close a tracheoesophageal fistula by placement of an over-the-scope...
Rendezvous technique using bronchoscopy and gastroscopy to close a tracheoesophageal fistula by placement of an over-the-scope...
 Tracheoesophageal Fistula | Pearson's General Thoracic
Tracheoesophageal Fistula | Pearson's General Thoracic
 Philippines FACEBOOK Group - Atresia / tracheoesophageal Fistula / VACTERL
Philippines FACEBOOK Group - Atresia / tracheoesophageal Fistula / VACTERL
 Tracheoesophageal Fistula and Esophageal Atresia | 5-Minute Pediatric Consult
Tracheoesophageal Fistula and Esophageal Atresia | 5-Minute Pediatric Consult
 CliniDo | Book best doctor present Tracheoesophageal Fistula surgeries in Egypt
CliniDo | Book best doctor present Tracheoesophageal Fistula surgeries in Egypt
 Quick Facts: Esophageal Atresia and Tracheoesophageal Fistula - MSD Manual Consumer Version
Quick Facts: Esophageal Atresia and Tracheoesophageal Fistula - MSD Manual Consumer Version
Esophageal Atresia With or Without Tracheoesophageal Fistula: Background, History of the Procedure, Problem
 A Case of Agenesis of the Right Lung with H-type Tracheoesophageal Fistula
A Case of Agenesis of the Right Lung with H-type Tracheoesophageal Fistula
 ERNICA has launched its website ! - The Federation of Esophageal Atresia and Tracheo-Esophageal Fistula
ERNICA has launched its website ! - The Federation of Esophageal Atresia and Tracheo-Esophageal Fistula
 February 1973 - Volume 51 - Issue 2 : Plastic and Reconstructive Surgery
February 1973 - Volume 51 - Issue 2 : Plastic and Reconstructive Surgery
 Welcome to Esophageal Atresia Care | Columbia Surgery
Welcome to Esophageal Atresia Care | Columbia Surgery
 Surgical technique and results of tracheal and carinal replacement with aortic allografts for salivary gland-type carcinoma
Surgical technique and results of tracheal and carinal replacement with aortic allografts for salivary gland-type carcinoma
 Congenital Anomalies of the Digestive System | NCBDDD | CDC
Congenital Anomalies of the Digestive System | NCBDDD | CDC
A novel approach of management by Amplatz vascular plug for recurrent tracheoesophageal fistula underlying acquired...
 Spontaneous Ventilation and Epidural Anesthesia in a Patient with a Large Tracheoesophageal Fistula and Esophageal Cancer...
Spontaneous Ventilation and Epidural Anesthesia in a Patient with a Large Tracheoesophageal Fistula and Esophageal Cancer...
Complex Airway Program | BIDMC of Boston
Cline R[au] - Search Results - PubMed
GERD and Swallowing Services | Swedish
 Videofluoroscopic Swallow Study (VFSS)
Videofluoroscopic Swallow Study (VFSS)
 Recurrent croup | Children's Hospital of Philadelphia
Recurrent croup | Children's Hospital of Philadelphia
 Sudish Murthy, MD, PhD | Cleveland Clinic
Sudish Murthy, MD, PhD | Cleveland Clinic
 NY Otolaryngology Group - Laryngology Glossary
NY Otolaryngology Group - Laryngology GlossaryEsophagus and the trachea3
- see spelling differences) is an abnormal connection (fistula) between the esophagus and the trachea. (wikipedia.org)
- A tracheoesophageal fistula is an abnormal connection between the esophagus and the trachea (which leads to the lungs). (msdmanuals.com)
- One or more fistulae may be present between the malformed esophagus and the trachea. (medscape.com)
Esophageal atresia and tracheoesophageal fistula2
- How can doctors tell if my baby has esophageal atresia and tracheoesophageal fistula? (msdmanuals.com)
- How do doctors treat esophageal atresia and tracheoesophageal fistula? (msdmanuals.com)
Distal tracheoesophageal fistula1
- In 1696, Gibson provided the first description of esophageal atresia with a distal tracheoesophageal fistula (TEF). (medscape.com)
Atresia11
- Esophageal atresia/tracheoesophageal fistula (EA/TEF) is a condition resulting from abnormal development before birth of the tube that carries food from the mouth to the stomach (the esophagus ). (medlineplus.gov)
- The third most common anomaly is the H-type fistula, which consists of a TEF without esophageal atresia. (medscape.com)
- Oesophageal Atresia-Tracheoesophageal Fistula (OA-TOF) is one of the most common digestive malformations occurring in 1 in 2,400 to 4,500 births worldwide. (frontiersin.org)
- Esophageal atresia with tracheoesophageal fistula (EA-TEF) is a congenital condition of incomplete formation of the esophagus. (unboundmedicine.com)
- In a 1987 report, Kluth eschews the concept that tracheoesophageal septation has a key role in the development of esophageal atresia. (medscape.com)
- He also suggests that esophageal vascular events, ischemic events, or both may be causes in cases of esophageal atresia without fistula. (medscape.com)
- Esophageal atresia/tracheoesophageal fistula (EA/TEF) is a rare birth defect occurring in 1 in 2,500-4,000 babies where the esophagus fails to properly connect the mouth to the stomach. (columbiasurgery.org)
- Esophageal atresia (EA) and tracheoesophageal fistula (TEF) is one of the most common congenital malformations of the esophagus, with an incidence of 1/2,500-1/4,500 ( 1 ). (frontiersin.org)
- El tipo de fÃ-stula más frecuente fue el del tipo C de Gross (atresia esofágica más fÃ-stula traqueoesofágica distal) en el 88.89 por ciento. (who.int)
- Jason was born with Esophageal Atresia & Tracheoesophageal Fistula which is the imperfect formation of the esophagus & Trachea. (gofundme.com)
- Esophageal atresia with or without tracheoesophageal fistula (EA/TEF) is the most common congenital malformation of the upper digestive tract. (lu.se)
Abnormal5
- A fistula, from the Latin meaning 'a pipe', is an abnormal connection running either between two tubes or between a tube and a surface. (wikipedia.org)
- A tracheoesophageal fistula is an abnormal connection (fistula) between the windpipes (trachea) and the esophagus (the passageway that extends from your throat to your stomach). (bidmc.org)
- This work involves molecular developmental pathophysiology of abnormal tracheoesophageal development. (cincinnatichildrens.org)
- A bronchoesophageal fistula (BEF) is an abnormal connection that forms between the esophagus and the bronchus, most commonly within the right bronchial tree. (appliedradiology.com)
- 1,3 Surgical treatment, which consists of excision of the fistula with closure of the abnormal openings, has a high rate of success. (appliedradiology.com)
Tracheomalacia2
- The primary complications during the postoperative period are leak and stenosis of the anastomosis, gastroesophageal reflux, esophageal dysmotility, fistula recurrence, respiratory disorders including tracheomalacia and "cyanotic spells" and deformities of the thoracic wall. (frontiersin.org)
- Acquired tracheomalacia could develop to Trachoeoesophageal Fistula (TEF) by the damage of tracheal and oesophageal wall secondary to the long term endotracheal or tracheostomy tubes. (biomedres.info)
Trachea and esophagus3
- citation needed] Fistulae between the trachea and esophagus in the newborn can be of diverse morphology and anatomical location. (wikipedia.org)
- A tracheoesophageal fistula (TEF) is a congenital or acquired communication between the trachea and esophagus. (medscape.com)
- Some babies have a hole or connection between the trachea and esophagus, called a trachehoesophageal fistula, or TEF. (columbiasurgery.org)
Diverticulum1
- Type 1 BEFs consist of an esophageal diverticulum forming the fistula, type 2 consist of an extension of the esophagus into a lobar or segmental bronchus (most common), type 3 result from an extending bronchogenic cyst, and type 4 results from a pulmonary sequestration. (appliedradiology.com)
Anomalies2
- Approximately 17-70% of children with tracheoesophageal fistulas (TEFs) have associated developmental anomalies. (medscape.com)
- H-type tracheoesophageal fistula in approximately 4% of exophageal anomalies. (e-cep.org)
Recurrent2
- Surgical repair can sometimes result in complications, including:[citation needed] Stricture, due to gastric acid erosion of the shortened esophagus Leak of contents at the point of anastomosis Recurrence of fistula Gastro-esophageal reflux disease Dysphagia Asthma-like symptoms, such as persistent coughing/wheezing Recurrent chest infections Tracheomalacia Neonates with TEF or esophageal atresia are unable to feed properly. (wikipedia.org)
- Recurrent tracheoesophageal fistula. (nih.gov)
Gastrointestinal1
- History of abdominal or tracheoesophageal fistula or gastrointestinal perforation within 6 months prior to inclusion. (who.int)
Resection3
- It is surgically corrected, with resection of any fistula and anastomosis of any discontinuous segments. (wikipedia.org)
- Primary repair without tracheal resection may be possible for small fistulas. (sts.org)
- Lower fistulas, or fistulas involving the esophagus and a major bronchus, are approached through the right chest, and tracheal resection may not be required. (sts.org)
Agenesis2
- citation needed] Not all types include both esophageal agenesis and tracheoesophageal fistula, but the most common types do. (wikipedia.org)
- We experienced a case of agenesis of the right lung with H-type tracheoesophageal fistula in a 1day-old male patient. (e-cep.org)
Strictures1
- Cook Medical has received FDA approval for company's Evolution esophageal stent, designed for people with malignant esophageal strictures and tracheoesophageal fistulas. (medgadget.com)
Airway1
- My research areas include developmental biology, esophageal arresia, tracheoesophageal fistula and airway malacia. (cincinnatichildrens.org)
Windpipe3
- Saliva, liquids fed to the infant, or digestive fluids may enter the windpipe through the tracheoesophageal fistula, leading to coughing, respiratory distress, and a bluish appearance of the skin or lips (cyanosis). (medlineplus.gov)
- Tracheoesophageal fistula is an opening between the esophagus and windpipe (trachea), so when the baby swallows, food goes into the baby's windpipe and lungs. (msdmanuals.com)
- For tracheoesophageal fistula, they'll close the connection between the esophagus and windpipe. (msdmanuals.com)
Salivation1
- Tracheoesophageal fistula is suggested in a newborn by copious salivation associated with choking, coughing, vomiting, and cyanosis coincident with the onset of feeding. (wikipedia.org)
Separation2
- The posterior deviation of the tracheoesophageal septum causes incomplete separation of the esophagus from the laryngotracheal tube and results in a TEF. (medscape.com)
- In 1984, O'Rahilly proposed that a fixed cephalad point of tracheoesophageal separation is present, with the tracheobronchial and esophageal elements elongating in a caudal direction from this point. (medscape.com)
Commonly3
- Tracheoesophageal fistula (TEF) is commonly associated with EA. (utah.edu)
- Diagnosis is commonly delayed or potentially misdiagnosed, whereas tracheoesophageal fistulas, which have a higher incidence and greater association with endotracheal intubation, are typically diagnosed much more quickly. (appliedradiology.com)
- Congenital abnormality characterized by the lack of full development of the ESOPHAGUS that commonly occurs with TRACHEOESOPHAGEAL FISTULA. (bvsalud.org)
Patient1
- Patient has a fistula (e.g., tracheoesophageal fistula). (asha.org)
Tracheal2
Morbidity2
- Three of the first 4 patients experienced major morbidity, mainly fistulas between the esophagus and graft. (nih.gov)
- Bronchoesophageal fistulas are associated with a high morbidity and mortality, and the underlying cause should be investigated. (appliedradiology.com)
Occurs1
- Pure TEF without EA occurs in 3-4% ("H type fistula", Gross type E). (unboundmedicine.com)
Patients3
- In patients with an H-type fistula, diagnosis may be delayed. (unboundmedicine.com)
- All grafts were wrapped with bulky and well-vascularized flaps (pectoral muscle flap all patients, with an additional "thymopericardial fat flap" in the last 2) to promote revascularization and to prevent erosion of adjacent large vessels or fistulas. (nih.gov)
- Patients with tracheoesophageal fistula. (mayo.edu)
VATER2
- His medical history included VATER syndrome [1] with corrective surgery for the tracheoesophageal fistula (TEF). (lancs.ac.uk)
- 4) Other associations noted are Simpson-Golabi-Behmel syndrome (5), tracheoesophageal fistula (6), ventricular septal defect (7), and VATER (8). (pediatriconcall.com)
Placement1
- however, in cases where the fistula is small and covered by a mucosal flap, as described here, a combined procedure can facilitate identification of the opening and direction of the fistula to aid accurate clip placement. (lancs.ac.uk)
Mucosal1
- 5 Congenital BEFs may present with normal mucosal lining within the fistula, unlike the acquired etiologies, which show absence of the normal mucosal lining. (appliedradiology.com)
Diagnosis1
- Acquired tracheoesophageal fistula (TEF) Is uncommon and requires a high index of suspicion for accurate and early diagnosis. (sts.org)
Surgical1
- 1,8 Alternative treatments include either surgical stapling or applying acetic acid and sodium hydroxide to both ends of the fistula. (appliedradiology.com)
Repair1
- This course is designed for pediatric surgeons seeking advanced minimally invasiveskills for thoracoscopic lobectomy and tracheoesophageal fistula repair. (ipeg.org)
Injury1
- The child seemed comfortable and asymptomatic but suffered significant injury resulting in esophageal pleural fistula within 4 days of ingestion. (ispub.com)
Closure2
- Successful closure of the fistula was confirmed by the complete absence of air drainage from the Ryle's tube, improvement in the ventilatory mechanics, and by a Gastrografin swallow. (lancs.ac.uk)
- OTSCs are widely used for closure of perforations and fistulas [2] [3]. (lancs.ac.uk)
Common2
- 1 Bronchoesophageal fistulas may be congenital or acquired, with acquired causes being more common. (appliedradiology.com)
- Acquired BEFs are less common than tracheoesophageal fistulas. (appliedradiology.com)
Type2
- H-type of tracheoesophageal fistula. (medscape.com)
- Sometimes people are born with this type of fistula. (bidmc.org)
Cases1
- In most cases, the atretic (blind-ending) esophagus has an aberrant fistula to the trachea (TEF). (unboundmedicine.com)
Rare1
- Bronchoesophageal fistulas are rare, with very few reported in the medical literature. (appliedradiology.com)
Development1
- Congenital TEF can arise due to failed fusion of the tracheoesophageal ridges after the fourth week of embryological development. (wikipedia.org)