Porphobilinogen Synthase
Porphobilinogen
Hydroxymethylbilane Synthase
Ammonia-Lyases
Zinc
Porphyria, Acute Intermittent
Protein Structure, Quaternary
Porphyrias
Aminolevulinic Acid
Porphyrins
Uroporphyrinogens
Porphyrias, Hepatic
Uroporphyrins
Fluids and Secretions
Holy Roman Empire
Cooking and Eating Utensils
Food Preservatives
Roman World
Encyclopedias as Topic
Pharmacology, Clinical
Sleep Deprivation
Seizures
Tablets
Electroencephalography
Epilepsy, Absence
Pamphlets
Relationships between lead absorption and peripheral nerve conduction velocities in lead workers. (1/277)
The motor sensory, and mixed nerve conduction velocities of median and posterior tibial nerves were measured in 39 lead workers whose blood lead (PbB) concentrations ranged from 2 to 73 mug/100 g with anaverage of 29 mug/100 g. The PbB concentrations significantly correlated with the maximal motor nerve conduction velocities (MCV) and mixed nerve conduction velocities (MNCV) of the median nerve in the forearm and with the MCV of the posterior tibial nerve. Erythrocyte delta-aminolevulinic acid dehydratase (ALAD) activity correlated similarly with the MCV and MNCV of the median nerve in the forearm, and the 24-hour urinary lead excretion following the intravenous administration of CaEDTA (20 mg/kg) (lead mobilization test) correlated with the MNCV. But no parameter correlated with the sensory nerve conduction velocities. By multiple regression analysis, a combination of the three parameters of lead absorption was found to correlate significantly with the MCV and MNCV of the median nerve in the forearm. The MCVs of the median and posterior tibial nerves in lead workers were significantly delayed in the PbB range of 29-73 mug/100 g (mean 45), in the lead mobilization test range from 173 to 3,540 mug/day (mean 973), and the ALAD activity range from 4.4 to 19.4 u. (mean 14.0), respectively. (+info)The Schiff base complex of yeast 5-aminolaevulinic acid dehydratase with laevulinic acid. (2/277)
The X-ray structure of the complex formed between yeast 5-aminolaevulinic acid dehydratase (ALAD) and the inhibitor laevulinic acid has been determined at 2.15 A resolution. The inhibitor binds by forming a Schiff base link with one of the two invariant lysines at the catalytic center: Lys263. It is known that this lysine forms a Schiff base link with substrate bound at the enzyme's so-called P-site. The carboxyl group of laevulinic acid makes hydrogen bonds with the side-chain-OH groups of Tyr329 and Ser290, as well as with the main-chain >NH group of Ser290. The aliphatic moiety of the inhibitor makes hydrophobic interactions with surrounding aromatic residues in the protein including Phe219, which resides in the flap covering the active site. Our analysis strongly suggests that the same interactions will be made by P-side substrate and also indicates that the substrate that binds at the enzyme's A-site will interact with the enzyme's zinc ion bound by three cysteines (133, 135, and 143). Inhibitor binding caused a substantial ordering of the active site flap (residues 217-235), which was largely invisible in the native electron density map and indicates that this highly conserved yet flexible region has a specific role in substrate binding during catalysis. (+info)Tissue variant effects of heme inhibitors on the mouse cytochrome c oxidase gene expression and catalytic activity of the enzyme complex. (3/277)
The in vivo effects of heme biosynthesis inhibitors, succinylacetone and CoCl2 on the cytochrome c oxidase (COX) gene expression and enzyme activity in different mouse tissues were investigated. Succinylacetone and CoCl2 showed tissue-specific differences in their ability to modulate heme aa3 content. A single dose of succinylacetone treatment for 8 h reduced the heme aa3 content of kidney mitochondria with no effect on the liver. CoCl2 treatment for 8 h, however, selectively affected the heme aa3 level in the liver. Reduced mitochondrial heme aa3 with both treatments was accompanied by approximately 50% reduced, mitochondrial genome-encoded COX I and II mRNAs and nuclear genome-encoded COX Vb mRNAs, but no change in COX IV mRNA level. Use of isolated mouse liver and brain mitochondrial systems showed a 50-80% reduction in mitochondrial transcription and translation rates in heme-depleted tissues. Blue native gel electrophoresis followed by immunoblot analysis showed that the complex from heme-depleted tissues contained a 30-50% reduction in levels of subunits I, IV, Vb and near normal levels of subunit VIc, indicating altered subunit content. Treatment of submitochondrial particles with protein kinase A and ATP resulted in partial dissociation of COX, suggesting a mechanistic basis for the reduced subunit content of the complex from heme-depleted tissues. Surprisingly, the enzyme from heme-depleted tissues showed twofold to fourfold higher turnover rates for cytochrome c oxidation, suggesting alterations in the kinetic characteristics of the enzyme following heme reduction. This is probably the first evidence that the tissue heme level regulates not only the mammalian COX gene expression, but also the catalytic activity of the enzyme, probably by affecting its stability. (+info)Biosynthesis of delta-aminolevulinic acid from the intact carbon skeleton of glutamic acid in greening barley. (4/277)
The customary route in animals and bacteria for delta-aminolevulinic acid biosynthesis is from glycine and succinyl CoA, catalyzed by the enzyme delta-aminolevulinic acid synthetase [succinyl-CoA:glycine C-succinyltransferase (decarboxylating), EC 2.3.1.37]. Attempts to demonstrate this route in plants have been unsuccessful. Evidence is given for a new enzymic route of synthesis of delta-aminolevulinic acid in plants. This route involves the incorporation of the intact five-carbon skeleton of glutamic acid into delta-aminolevulinic acid. Demonstration of the new pathway in plants has been made by feeding specifically labeled [14C]glutamic acid to etiolated barley shoots greening in the light. In the presence of levulinate, a competitive inhibitor of delta-aminolevulinic acid dehydrastase [porphobilinogen synthase; delta-aminolevulinate hydro-lyase (adding delta-aminolevulinate and cyclizing); EC 4.2.1.24], delta-aminolevulinate accumulates. The delta-aminolevulinate formed was chemically degraded by periodate to formaldehyde and succinic acid. The C5 (formaldehyde) fragment was separated, as the 5,5-dimethyl-1,3-cyclohexanedione (dimedone) derivative, from the C1-C4 (succinic acid) fragment. The C5 atom contained radioactivity predominantly derived from C1 of glutamic acid. Conversely, the labeled C3 and C4 atoms of glutamic acid were found primarily in the succinic acid (C1-C4) fragment of delta-aminolevulinate. This labeling pattern for delta-aminolevulinic acid is consistent with a biosynthetic route utilizing the intact five-carbon skeleton of alpha-ketoglutarate, glutamate, or glutamine, and is inconsistent with the delta-aminolevulinic acid synthetase pathway utilizing glycine and succinyl CoA as precursors. (+info)An artificial gene for human porphobilinogen synthase allows comparison of an allelic variation implicated in susceptibility to lead poisoning. (5/277)
Porphobilinogen synthase (PBGS) is an ancient enzyme essential to tetrapyrrole biosynthesis (e.g. heme, chlorophyll, and vitamin B(12)). Two common alleles encoding human PBGS, K59 and N59, have been correlated with differential susceptibility of humans to lead poisoning. However, a model for human PBGS based on homologous crystal structures shows the location of the allelic variation to be distant from the active site with its two Zn(II). Previous microbial expression systems for human PBGS have resulted in a poor yield. Here, an artificial gene encoding human PBGS was constructed by recursive polymerase chain reaction from synthetic oligonucleotides to rectify this problem. The artificial gene was made to resemble the highly expressed homologous Escherichia coli hemB gene and to remove rare codons that can confound heterologous protein expression in E. coli. We have expressed and purified recombinant human PBGS variants K59 and N59 in 100-mg quantities. Both human PBGS proteins purified with eight Zn(II)/octamer; Zn(II) binding was shown to be pH-dependent; and Pb(II) could displace some of the Zn(II). However, there was no differential displacement of Zn(II) by Pb(II) between K59 and N59, and simple Pb(II) inhibition studies revealed no allelic difference. (+info)Genetic susceptibility to lead poisoning. (6/277)
Major strides have been taken in the regulation of lead intoxication in the general population, but studies using genetic markers of susceptibility to environmental toxicants raise the question of whether genes can make certain individuals more vulnerable to environmental toxins such as lead. At least three polymorphic genes have been identified that potentially can influence the bioaccumulation and toxicokinetics of lead in humans. The first gene to be discussed in this review is the gene coding for delta-aminolevulinic acid dehydratase (ALAD), an enzyme of heme biosynthesis, that exists in two polymorphic forms. The resulting isozymes have been shown to affect the blood and bone lead levels in human populations. The effects of ALAD in lead intoxication have also been studied in laboratory mice that differ in the genetic dose for this enzyme. The second gene reviewed here is the vitamin D receptor (VDR) gene. The VDR is involved in calcium absorption through the gut and into calcium-rich tissues such as bone. Recent findings suggest that VDR polymorphism may influence the accumulation of lead in bone. Finally, the third gene to be discussed here that may influence the absorption of lead is the hemochromatosis gene coding for the HFE protein. The presence of mutations in the HFE gene leads to hemochromatosis in homozygotic individuals. Because of the associations between iron and lead transport, it is possible that polymorphisms in the HFE gene may also influence the absorption of lead, but this has not yet been studied. More studies will be needed to define the role of these genes in lead intoxication. (+info)Inhibition of Escherichia coli porphobilinogen synthase using analogs of postulated intermediates. (7/277)
BACKGROUND: Porphobilinogen synthase is the second enzyme involved in the biosynthesis of natural tetrapyrrolic compounds, and condenses two molecules of 5-aminolevulinic acid (ALA) through a nonsymmetrical pathway to form porphobilinogen. Each substrate is recognized individually at two different active site positions to be regioselectively introduced into the product. According to pulse-labeling experiments, the substrate forming the propionic acid sidechain of porphobilinogen is recognized first. Two different mechanisms for the first bond-forming step between the two substrates have been proposed. The first involves carbon-carbon bond formation (an aldol-type reaction) and the second carbon-nitrogen bond formation, leading to an iminium ion. RESULTS: With the help of kinetic studies, we determined the Michaelis constants for each substrate recognition site. These results explain the Michaelis-Menten behavior of substrate analog inhibitors - they act as competitive inhibitors. Under standard conditions, however, another set of inhibitors demonstrates uncompetitive, mixed, pure irreversible, slow-binding or even quasi-irreversible inhibition behavior. CONCLUSIONS: Analysis of the different classes of inhibition behavior allowed us to make a correlation between the type of inhibition and a specific site of interaction. Analyzing the inhibition behavior of analogs of postulated intermediates strongly suggests that carbon-nitrogen bond formation occurs first. (+info)Alcohol and porphyrin metabolism. (8/277)
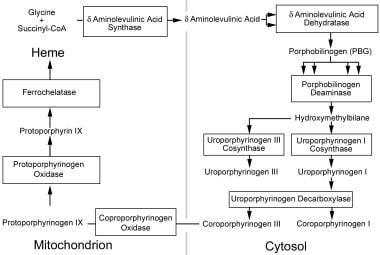
Alcohol is a porphyrinogenic agent which may cause disturbances in porphyrin metabolism in healthy persons as well as biochemical and clinical manifestations of acute and chronic hepatic porphyrias. After excessive consumption of alcohol, a temporary, clinically asymptomatic secondary hepatic coproporphyrinuria is observable, which can become persistent in cases of alcohol-induced liver damage. Nowadays, the alcohol-liver-porphyrinuria syndrome is the first to be mentioned in secondary hepatic disturbances of porphyrin metabolism. Acute hepatic porphyrias (acute intermittent porphyria, variegate porphyria and hereditary coproporphyria) are considered to be molecular regulatory diseases, in contrast to non-acute, chronic hepatic porphyria, clinically appearing as porphyria cutanea tarda (PCT). Porphyrins do not accumulate in the liver in acute porphyrias, whereas in chronic hepatic porphyrias they do. Thus, chronic hepatic porphyria is a porphyrin-accumulation disease, whereas acute hepatic porphyrias are haem-pathway-dysregulation diseases, characterized in general by induction of delta-aminolevulinic acid synthase in the liver and excessive stimulation of the pathway without storage of porphyrins in the liver. The clinical expression of acute hepatic porphyrias can be triggered by alcohol, because alcohol augments the inducibility of delta-aminolevulinic acid synthase. In chronic hepatic porphyrias, however, which are already associated with liver damage, alcohol potentiates the disturbance of the decarboxylation of uro- and heptacarboxyporphyrinogen, which is followed by a hepatic accumulation of uro- and heptacarboxyporphyrin and their sometimes extreme urinary excretion. Especially in persons with a genetic deficiency of uroporphyrinogen decarboxylase, but also in patients with the so-called sporadic variety of PCT, alcohol is able to transform an asymptomatic coproporphyrinuria into PCT. Alcohol has many biochemical and clinical effects on porphyrin and haem synthesis both in humans and laboratory animals. Ethanol suppresses the activity of porphobilinogen synthase (synonym: delta-aminolevulinic acid dehydratase), uroporphyrinogen decarboxylase, coproporphyrinogen oxidase and ferrochelatase, whereas it induces the first and rate-limiting enzyme in the pathway, delta-aminolevulinic acid synthase and also porphobilinogen deaminase. Therefore, teetotalism is a therapeutically and prophylactically important measure in all types of hepatic porphyrias. (+info)Porphobilinogen Synthase (also known as PBGD or hydroxymethylbilane synthase) is an enzyme that catalyzes the second step in the heme biosynthesis pathway. This enzyme is responsible for converting two molecules of porphobilinogen into a linear tetrapyrrole called hydroxymethylbilane, which is then converted into uroporphyrinogen III by uroporphyrinogen III synthase.
Deficiency in Porphobilinogen Synthase can lead to a rare genetic disorder known as acute intermittent porphyria (AIP), which is characterized by the accumulation of porphobilinogen and other precursors in the heme biosynthesis pathway, resulting in neurovisceral symptoms such as abdominal pain, vomiting, neuropathy, and psychiatric disturbances.
Porphobilinogen (PBG) is a bioactive compound that plays a crucial role in the biosynthesis pathway of heme, which is an essential component of hemoglobin and other hemoproteins. It is a porphyrin precursor and is synthesized from aminolevulinic acid (ALA) by the enzyme ALA dehydratase in the second step of heme biosynthesis.
In medical terms, abnormal accumulation or increased levels of PBG in the body can indicate an underlying disorder in heme biosynthesis, such as acute intermittent porphyria (AIP), variegate porphyria (VP), or hereditary coproporphyria (HCP). These disorders are known as porphyrias and are characterized by the buildup of porphyrin precursors in various tissues, leading to neurological and gastrointestinal symptoms.
Therefore, measuring PBG levels in urine or blood can help diagnose and monitor these conditions.
Hydroxymethylbilane Synthase (HMBS) is an enzyme that plays a crucial role in the metabolic pathway known as heme biosynthesis. Heme is an essential component of various proteins, including hemoglobin, which is responsible for oxygen transport in the blood.
The HMBS enzyme catalyzes the conversion of aminolevulinic acid (ALA) and glycine into a linear tetrapyrrole intermediate called hydroxymethylbilane. This reaction is the third step in the heme biosynthesis pathway, and it takes place in the mitochondria of cells.
Deficiencies in HMBS can lead to a rare genetic disorder called acute intermittent porphyria (AIP), which is characterized by neurovisceral attacks and neurological symptoms such as abdominal pain, vomiting, hypertension, tachycardia, and mental disturbances.
Heptanoates are chemical compounds that contain the functional group of heptanoic acid. Heptanoic acid, also known as n-caproic acid, is a type of carboxylic acid with a 7-carbon chain and the molecular formula C7H15COOH.
Heptanoates are commonly used in the production of various chemicals, including flavors, fragrances, and pharmaceuticals. In medicine, heptanoates may be used as esters in the formulation of drugs to improve their solubility, absorption, and stability. For example, some injectable forms of medications may use heptanoate salts or esters to enhance their delivery into the body.
It's important to note that specific medical definitions for "heptanoates" may vary depending on the context and application.
Levulinic acid is not specifically a medical term, but it is a chemical compound with the formula C5H8O2. It is a white crystalline solid that is used in the production of various chemicals and materials. However, I can provide you with some general information about levulinic acid:
Levulinic acid is a saturated carboxylic acid, which means it contains a carboxyl group (-COOH) and is fully saturated with hydrogen atoms. It is an alpha-beta unsaturated carboxylic acid due to the presence of a carbon-carbon double bond (C=C) between the second and third carbon atoms in its structure.
Levulinic acid can be found naturally in small amounts in various fruits, such as apples and grapes, and is also present in some fermented foods like beer and wine. It can be produced industrially from biomass sources, such as cellulose or lignocellulosic materials, through a process called acid hydrolysis.
In the medical field, levulinic acid may have potential applications as an antimicrobial agent due to its ability to inhibit the growth of certain bacteria and fungi. It is also used in the synthesis of pharmaceuticals and other chemical products. However, it is not a substance that is typically directly associated with medical treatment or diagnosis.
Ammonia-lyases are a class of enzymes that catalyze the removal of an amino group from a substrate, releasing ammonia in the process. These enzymes play important roles in various biological pathways, including the biosynthesis and degradation of various metabolites such as amino acids, carbohydrates, and aromatic compounds.
The reaction catalyzed by ammonia-lyases typically involves the conversion of an alkyl or aryl group to a carbon-carbon double bond through the elimination of an amine group. This reaction is often reversible, allowing the enzyme to also catalyze the addition of an amino group to a double bond.
Ammonia-lyases are classified based on the type of substrate they act upon and the mechanism of the reaction they catalyze. Some examples of ammonia-lyases include aspartate ammonia-lyase, which catalyzes the conversion of aspartate to fumarate, and tyrosine ammonia-lyase, which converts tyrosine to p-coumaric acid.
These enzymes are important in both plant and animal metabolism and have potential applications in biotechnology and industrial processes.
Zinc is an essential mineral that is vital for the functioning of over 300 enzymes and involved in various biological processes in the human body, including protein synthesis, DNA synthesis, immune function, wound healing, and cell division. It is a component of many proteins and participates in the maintenance of structural integrity and functionality of proteins. Zinc also plays a crucial role in maintaining the sense of taste and smell.
The recommended daily intake of zinc varies depending on age, sex, and life stage. Good dietary sources of zinc include red meat, poultry, seafood, beans, nuts, dairy products, and fortified cereals. Zinc deficiency can lead to various health problems, including impaired immune function, growth retardation, and developmental delays in children. On the other hand, excessive intake of zinc can also have adverse effects on health, such as nausea, vomiting, and impaired immune function.
Acute Intermittent Porphyria (AIP) is a rare inherited metabolic disorder that affects the production of heme, a component in hemoglobin. This condition is part of a group of disorders known as the porphyrias, which are caused by genetic mutations that result in enzyme deficiencies needed to produce heme.
In AIP, specifically, there is a deficiency in the enzyme porphobilinogen deaminase (PBGD). This leads to the buildup of porphyrin precursors, particularly porphobilinogen and delta-aminolevulinic acid (ALA), in the body. These substances are toxic and can cause acute attacks when they accumulate in high concentrations.
Acute attacks are characterized by severe abdominal pain, nausea, vomiting, constipation or diarrhea, muscle weakness, seizures, and mental changes such as confusion, hallucinations, or anxiety. These symptoms can be triggered by certain factors like drugs, alcohol, hormonal changes, infections, or stress.
It is essential to differentiate AIP from other medical conditions that may present with similar symptoms, as the treatment strategies differ significantly. Diagnosis typically involves measuring porphyrin precursors in urine, especially during an acute attack, and can be confirmed by genetic testing for the PBGD gene mutation.
Treatment of AIP primarily focuses on managing acute attacks with intravenous heme preparations, which help to reduce the production of toxic porphyrin precursors. In addition, providing supportive care such as hydration, pain management, and addressing any triggers or complications is crucial. Long-term management includes avoiding identified triggers, monitoring for early signs of acute attacks, and implementing a low-purine diet in some cases.
Quaternary protein structure refers to the arrangement and interaction of multiple folded protein molecules in a multi-subunit complex. These subunits can be identical or different forms of the same protein or distinctly different proteins that associate to form a functional complex. The quaternary structure is held together by non-covalent interactions, such as hydrogen bonds, ionic bonds, and van der Waals forces. Understanding quaternary structure is crucial for comprehending the function, regulation, and assembly of many protein complexes involved in various cellular processes.
Porphyrias are a group of rare genetic disorders that affect the production of heme, a component in hemoglobin that carries oxygen in the blood. The diseases are caused by mutations in the genes involved in the production of heme, leading to the buildup of porphyrins or their precursors in the body. These substances can be toxic and can cause various symptoms depending on the specific type of porphyria. Symptoms may include abdominal pain, neurological problems, and skin issues. Porphyrias are typically divided into two categories: acute porphyrias, which affect the nervous system, and cutaneous porphyrias, which primarily affect the skin.
In the context of medicine and pharmacology, "kinetics" refers to the study of how a drug moves throughout the body, including its absorption, distribution, metabolism, and excretion (often abbreviated as ADME). This field is called "pharmacokinetics."
1. Absorption: This is the process of a drug moving from its site of administration into the bloodstream. Factors such as the route of administration (e.g., oral, intravenous, etc.), formulation, and individual physiological differences can affect absorption.
2. Distribution: Once a drug is in the bloodstream, it gets distributed throughout the body to various tissues and organs. This process is influenced by factors like blood flow, protein binding, and lipid solubility of the drug.
3. Metabolism: Drugs are often chemically modified in the body, typically in the liver, through processes known as metabolism. These changes can lead to the formation of active or inactive metabolites, which may then be further distributed, excreted, or undergo additional metabolic transformations.
4. Excretion: This is the process by which drugs and their metabolites are eliminated from the body, primarily through the kidneys (urine) and the liver (bile).
Understanding the kinetics of a drug is crucial for determining its optimal dosing regimen, potential interactions with other medications or foods, and any necessary adjustments for special populations like pediatric or geriatric patients, or those with impaired renal or hepatic function.
Aminolevulinic acid (ALA) is a naturally occurring compound in the human body and is a key precursor in the biosynthesis of heme, which is a component of hemoglobin in red blood cells. It is also used as a photosensitizer in dermatology for the treatment of certain types of skin conditions such as actinic keratosis and basal cell carcinoma.
In medical terms, ALA is classified as an α-keto acid and a porphyrin precursor. It is synthesized in the mitochondria from glycine and succinyl-CoA in a reaction catalyzed by the enzyme aminolevulinic acid synthase. After its synthesis, ALA is transported to the cytosol where it undergoes further metabolism to form porphyrins, which are then used for heme biosynthesis in the mitochondria.
In dermatology, topical application of ALA followed by exposure to a specific wavelength of light can lead to the production of reactive oxygen species that destroy abnormal cells in the skin while leaving healthy cells unharmed. This makes it an effective treatment for precancerous and cancerous lesions on the skin.
It is important to note that ALA can cause photosensitivity, which means that patients who have undergone ALA-based treatments should avoid exposure to sunlight or other sources of bright light for a period of time after the treatment to prevent adverse reactions.
Porphyrins are complex organic compounds that contain four pyrrole rings joined together by methine bridges (=CH-). They play a crucial role in the biochemistry of many organisms, as they form the core structure of various heme proteins and other metalloproteins. Some examples of these proteins include hemoglobin, myoglobin, cytochromes, and catalases, which are involved in essential processes such as oxygen transport, electron transfer, and oxidative metabolism.
In the human body, porphyrins are synthesized through a series of enzymatic reactions known as the heme biosynthesis pathway. Disruptions in this pathway can lead to an accumulation of porphyrins or their precursors, resulting in various medical conditions called porphyrias. These disorders can manifest as neurological symptoms, skin lesions, and gastrointestinal issues, depending on the specific type of porphyria and the site of enzyme deficiency.
It is important to note that while porphyrins are essential for life, their accumulation in excessive amounts or at inappropriate locations can result in pathological conditions. Therefore, understanding the regulation and function of porphyrin metabolism is crucial for diagnosing and managing porphyrias and other related disorders.
Uroporphyrinogens are organic compounds that are intermediate products in the synthesis of heme, which is a crucial component of hemoglobin and other important molecules in the body. Specifically, uroporphyrinogens are tetrapyrroles, which means they contain four pyrrole rings linked together. They have eight carboxylic acid side chains and two propionic acid side chains.
There are two types of uroporphyrinogens: Type I and Type III. Uroporphyrinogen III is the precursor to heme, while uroporphyrinogen I is a dead-end metabolite that is not used in heme synthesis. Defects in the enzymes involved in heme biosynthesis can lead to various porphyrias, which are genetic disorders characterized by the accumulation of porphyrins and their precursors in the body.
Hepatic porphyrias are a group of rare genetic disorders that affect the production of heme in the liver. Heme is a crucial component of hemoglobin, the protein in red blood cells that carries oxygen throughout the body. In hepatic porphyrias, there is a buildup of porphyrins or porphyrin precursors, which are toxic and can cause a variety of symptoms.
The four types of hepatic porphyrias are:
1. Acute Intermittent Porphyria (AIP): This is the most common type of hepatic porphyria. It is characterized by attacks of abdominal pain, nausea, vomiting, constipation, and neurological symptoms such as muscle weakness, seizures, and mental changes.
2. Variegate Porphyria (VP): This type of porphyria is more common in South Africa but can occur worldwide. It is characterized by skin symptoms such as blistering and scarring after exposure to sunlight, as well as acute attacks similar to those seen in AIP.
3. Hereditary Coproporphyria (HCP): This type of porphyria is similar to VP, but the symptoms are usually less severe. It can cause both skin symptoms and acute attacks.
4. ALA Dehydratase Deficiency Porphyria (ADDP): This is the rarest type of hepatic porphyria. It is characterized by severe neurological symptoms and is often diagnosed in infancy or early childhood.
The diagnosis of hepatic porphyrias typically involves measuring the levels of porphyrins and their precursors in the urine, blood, or stool during an attack or between attacks. Treatment may include avoiding trigger factors such as certain medications, alcohol, and smoking, as well as providing supportive care during acute attacks. In some cases, medication to reduce porphyrin production or prevent attacks may be necessary.
Uroporphyrins are porphyrin derivatives that contain four carboxylic acid groups. They are intermediates in the biosynthesis of heme, which is a component of hemoglobin and other hemoproteins. Uroporphyrinogen I and III are precursors to uroporphyrin I and III, respectively, through the action of uroporphyrinogen decarboxylase.
Uroporphyrin I and III differ in the position of acetate and propionate side chains on the porphyrin ring. Uroporphyrins are usually elevated in the urine of patients with certain inherited metabolic disorders, such as acute intermittent porphyria, variegate porphyria, and hereditary coproporphyria, due to enzyme deficiencies in the heme biosynthetic pathway.
The measurement of uroporphyrins in urine or other body fluids can be helpful in diagnosing and monitoring these disorders.
Fluids and secretions in a medical context refer to the various liquids produced by different tissues, organs, and systems in the body. These fluids have specific compositions and functions that are essential for maintaining homeostasis and supporting physiological processes. Here are brief definitions of some key fluids and secretions:
1. Intracellular fluid (ICF): The fluid inside cells, accounting for about 65% of total body water. It contains various ions, nutrients, waste products, and organelles necessary for cell function.
2. Extracellular fluid (ECF): The fluid outside cells, making up around 35% of total body water. ECF is further divided into interstitial fluid, blood plasma, and transcellular fluid.
* Interstitial fluid: The fluid that surrounds the cells in the body, acting as a medium for exchanging nutrients, waste products, and gases between cells and blood vessels.
* Blood plasma: The liquid component of blood, containing water, ions, nutrients, waste products, hormones, gases, and proteins that help regulate fluid balance, immunity, and other vital functions.
* Transcellular fluid: Specialized fluids found in specific locations, such as cerebrospinal fluid (CSF) surrounding the brain and spinal cord, synovial fluid lubricating joints, pleural fluid surrounding lungs, pericardial fluid around the heart, and aqueous humor within the eyes.
3. Secretions: Fluids produced by glands or specialized cells, which can be classified into exocrine and endocrine secretions.
* Exocrine secretions: Fluids released through ducts to specific locations on the body's surface or into cavities. Examples include saliva from salivary glands, digestive enzymes from the pancreas, bile from the liver and gallbladder, sweat from sweat glands, and mucus from respiratory and reproductive tracts.
* Endocrine secretions: Hormones released directly into the bloodstream by endocrine glands or cells, such as insulin from the pancreas, thyroid hormones from the thyroid gland, adrenal hormones from the adrenal gland, and steroid hormones from the ovaries and testes.
4. Excretions: Waste products eliminated from the body, including urine (containing urea and other metabolic waste), feces (containing undigested food particles, bacteria, and bile pigments), sweat (containing water, salts, and small amounts of waste products), and carbon dioxide exhaled through the lungs.
5. Diapedesis: The process by which white blood cells (leukocytes) move from blood vessels into surrounding tissues to combat infection or inflammation. This occurs through gaps between endothelial cells lining blood vessel walls, allowing leukocytes to migrate towards sites of injury or infection.
6. Transudate: A clear, straw-colored fluid that forms when there is increased hydrostatic pressure or decreased oncotic (protein) pressure in the capillaries, causing leakage into surrounding tissues. This can occur due to heart failure, liver cirrhosis, or kidney disease.
7. Exudate: A cloudy, yellowish-green or brown fluid that forms when there is inflammation or infection in the body, leading to increased vascular permeability and leakage of proteins, white blood cells, and other cellular debris into surrounding tissues. This can be seen in conditions such as pneumonia, abscesses, or burns.
8. Plasma: The liquid component of blood, which carries cells (red blood cells, white blood cells, and platelets) and various substances (nutrients, hormones, waste products, gases) throughout the body. Plasma is about 90% water and 10% dissolved solutes, including proteins, electrolytes, glucose, lipids, vitamins, and gases.
9. Serum: The clear, straw-colored fluid that remains after blood clots and the clotting factors are removed. Serum contains all the dissolved substances found in plasma except for fibrinogen and other clotting factors. It is commonly used for diagnostic tests to measure various components, such as electrolytes, enzymes, hormones, antibodies, and drugs.
10. Hematocrit: The percentage of red blood cells in whole blood, measured by centrifuging a sample of blood to separate the cellular components from the plasma. A high hematocrit indicates increased numbers of red blood cells, which may be due to dehydration, living at high altitudes, or certain medical conditions like polycythemia vera. A low hematocrit suggests anemia or blood loss.
11. Hemoglobin: The iron-containing protein in red blood cells responsible for carrying oxygen from the lungs to tissues and carbon dioxide from tissues to the lungs. Each hemoglobin molecule can bind four oxygen molecules, making it highly efficient at transporting oxygen throughout the body.
12. Mean corpuscular volume (MCV): The average size of red blood cells, measured in femtoliters (fL). MCV is calculated by dividing the hematocrit by the red blood cell count. Normal values range from 80-100 fL. High MCV suggests macrocytic anemia, while low MCV indicates microcytic anemia.
13. Mean corpuscular hemoglobin (MCH): The average amount of hemoglobin in a red blood cell, measured in picograms (pg). MCH is calculated by dividing the total amount of hemoglobin by the red blood cell count. Normal values range from 27-31 pg. High MCH suggests macrocytic anemia, while low MCH indicates microcytic anemia.
14. Mean corpuscular hemoglobin concentration (MCHC): The average concentration of hemoglobin in a red blood cell, measured as a percentage. MCHC is calculated by dividing the total amount of hemoglobin by the hematocrit. Normal values range from 32-36%. High MCHC suggests hemoglobinopathies or dehydration, while low MCHC indicates iron deficiency anemia.
15. Red cell distribution width (RDW): A measure of the variation in red blood cell size, expressed as a coefficient of variation (CV). RDW is calculated by dividing the standard deviation of red blood cell volume by the MCV and multiplying by 100. Normal values range from 11-14.5%. High RDW suggests anisocytosis, which can be seen in various types of anemia, including iron deficiency anemia, megaloblastic anemia, and hemolytic anemia.
16. Platelet count: The number of platelets (thrombocytes) present in a sample of blood, expressed as cells per liter (cells/L). Normal values range from 150-450 x 10^9/L. Low platelet counts can be seen in various conditions, including vitamin B12 or folate deficiency, disseminated intravascular coagulation (DIC), and certain medications. High platelet counts can be seen in inflammatory conditions, malignancies, and certain medications.
17. Mean platelet volume (MPV): The average size of platelets in a sample of blood, expressed as femtoliters (fL). Normal values range from 7-12 fL. High MPV suggests increased platelet production or activation, which can be seen in various conditions, including inflammatory disorders, malignancies, and certain medications. Low MPV suggests decreased platelet production or increased destruction, which can be seen in various conditions, including vitamin B12 or folate deficiency, DIC, and certain medications.
18. Platelet distribution width (PDW): A measure of the variability in size of platelets in a sample of blood, expressed as a percentage. Normal values range from 10-20%. High PDW suggests increased platelet production or activation, which can be seen in various conditions, including inflammatory disorders, malignancies, and certain medications. Low PDW suggests decreased platelet production or increased destruction, which can be seen in various conditions, including vitamin B12 or folate deficiency, DIC, and certain medications.
19. Reticulocyte count: The number of reticulocytes (immature red blood cells) present in a sample of blood, expressed as a percentage of the total red blood cell count. Normal values range from 0.5-2%. High reticulocyte counts can be seen in various conditions that cause increased red blood cell production, such as hemolytic anemia or blood loss. Low reticulocyte counts can be seen in various conditions that cause decreased
I'm sorry for any confusion, but the term "Holy Roman Empire" is not a medical concept or term. It refers to a political entity that existed in Western and Central Europe from 962 to 1806. At its height, it was one of the most powerful states in Europe, encompassing modern-day Germany, Austria, the Czech Republic, Switzerland, and other territories. The Holy Roman Empire was not a nation-state in the modern sense but rather a complex collection of principalities, duchies, free cities, and bishoprics, each with its own ruler and degree of autonomy.
If you have any medical questions or concerns, I would be happy to help answer them!
Cooking and eating utensils are devices or tools used in the preparation, cooking, and serving of food. Here is a brief medical definition for some common types:
1. Cooking utensils: These include various tools and equipment used to prepare and cook food, such as knives, cutting boards, pots, pans, whisks, spatulas, colanders, and measuring cups/spoons. They help to chop, dice, mix, blend, stir, sauté, boil, fry, bake, or grill ingredients.
2. Eating utensils: These are devices used to consume food and include items like forks, spoons, knives, chopsticks, and straws. They aid in bringing food from the plate or bowl to the mouth and cutting or separating food into manageable pieces.
Proper cleaning and maintenance of cooking and eating utensils are essential to prevent cross-contamination of bacteria, viruses, or other microorganisms that can cause foodborne illnesses. Using clean utensils and following safe food handling practices can help minimize the risk of infection and promote overall health.
Food preservatives are substances added to foods to prevent or slow down spoilage caused by microorganisms such as bacteria, yeasts, and molds, or to retard quality deterioration due to oxidation or other chemical reactions. They work by inhibiting the growth of microorganisms, preventing enzymatic reactions that cause spoilage, or scavenging oxygen that can lead to food degradation. Examples of commonly used food preservatives include sodium benzoate, potassium sorbate, sulfites, and nitrites. It is important to note that while food preservatives play a crucial role in maintaining the safety and quality of our food supply, excessive consumption of certain preservatives may have adverse health effects.
I'm sorry for any confusion, but "Roman World" is not a medical term. It may refer to the geographical area, culture, or time period associated with the ancient Roman Empire. If you have any questions about medical terminology or concepts, I would be happy to help answer those!
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
Clinical pharmacology is a branch of medicine that deals with the study of drugs and their interactions with living organisms. It involves understanding how drugs are absorbed, distributed, metabolized, and excreted by the body, as well as their therapeutic effects, side effects, and toxicity. Clinical pharmacology also encompasses the design and conduct of clinical trials to evaluate the safety and efficacy of new drugs in human subjects. The ultimate goal of clinical pharmacology is to optimize drug therapy for individual patients by considering factors such as age, sex, genetics, lifestyle, and comorbidities. In summary, clinical pharmacology is the application of pharmacological principles to the practice of medicine for the benefit of patients.
Sorbic acid is a chemical compound that is commonly used as a preservative in various food and cosmetic products. Medically, it's not typically used as a treatment for any specific condition. However, its preservative properties help prevent the growth of bacteria, yeast, and mold, which can improve the safety and shelf life of certain medical supplies such as ointments and eye drops.
The chemical structure of sorbic acid is that of a carboxylic acid with two double bonds, making it a unsaturated fatty acid. It's naturally found in some fruits like rowanberries and serviceberries, but most commercial sorbic acid is synthetically produced.
Food-grade sorbic acid is generally recognized as safe (GRAS) by the U.S. Food and Drug Administration (FDA), and it has a wide range of applications in food preservation, including baked goods, cheeses, wines, and fruit juices. In cosmetics, it's often used to prevent microbial growth in products like creams, lotions, and makeup.
It is important to note that some people may have allergic reactions to sorbic acid or its salts (sorbates), so caution should be exercised when introducing new products containing these substances into personal care routines or diets.
Sleep deprivation is a condition that occurs when an individual fails to get sufficient quality sleep or the recommended amount of sleep, typically 7-9 hours for adults. This can lead to various physical and mental health issues. It can be acute, lasting for one night or a few days, or chronic, persisting over a longer period.
The consequences of sleep deprivation include:
1. Fatigue and lack of energy
2. Difficulty concentrating or remembering things
3. Mood changes, such as irritability or depression
4. Weakened immune system
5. Increased appetite and potential weight gain
6. Higher risk of accidents due to decreased reaction time
7. Health problems like high blood pressure, diabetes, and heart disease over time
Sleep deprivation can be caused by various factors, including stress, shift work, sleep disorders like insomnia or sleep apnea, poor sleep hygiene, and certain medications. It's essential to address the underlying causes of sleep deprivation to ensure proper rest and overall well-being.
A seizure is an uncontrolled, abnormal firing of neurons (brain cells) that can cause various symptoms such as convulsions, loss of consciousness, altered awareness, or changes in behavior. Seizures can be caused by a variety of factors including epilepsy, brain injury, infection, toxic substances, or genetic disorders. They can also occur without any identifiable cause, known as idiopathic seizures. Seizures are a medical emergency and require immediate attention.
In the context of medical terminology, tablets refer to pharmaceutical dosage forms that contain various active ingredients. They are often manufactured in a solid, compressed form and can be administered orally. Tablets may come in different shapes, sizes, colors, and flavors, depending on their intended use and the manufacturer's specifications.
Some tablets are designed to disintegrate or dissolve quickly in the mouth, making them easier to swallow, while others are formulated to release their active ingredients slowly over time, allowing for extended drug delivery. These types of tablets are known as sustained-release or controlled-release tablets.
Tablets may contain a single active ingredient or a combination of several ingredients, depending on the intended therapeutic effect. They are typically manufactured using a variety of excipients, such as binders, fillers, and disintegrants, which help to hold the tablet together and ensure that it breaks down properly when ingested.
Overall, tablets are a convenient and widely used dosage form for administering medications, offering patients an easy-to-use and often palatable option for receiving their prescribed treatments.
Electroencephalography (EEG) is a medical procedure that records electrical activity in the brain. It uses small, metal discs called electrodes, which are attached to the scalp with paste or a specialized cap. These electrodes detect tiny electrical charges that result from the activity of brain cells, and the EEG machine then amplifies and records these signals.
EEG is used to diagnose various conditions related to the brain, such as seizures, sleep disorders, head injuries, infections, and degenerative diseases like Alzheimer's or Parkinson's. It can also be used during surgery to monitor brain activity and ensure that surgical procedures do not interfere with vital functions.
EEG is a safe and non-invasive procedure that typically takes about 30 minutes to an hour to complete, although longer recordings may be necessary in some cases. Patients are usually asked to relax and remain still during the test, as movement can affect the quality of the recording.
Absence epilepsy is a type of epilepsy characterized by recurrent brief episodes of "absences," or staring spells, that can last from a few seconds to several minutes. These episodes are often accompanied by subtle body movements such as lip smacking or eyelid flutters. Absence epilepsy is most commonly diagnosed in children and adolescents, and it is more common in girls than boys.
The seizures in absence epilepsy are caused by abnormal electrical activity in the brain, specifically in a part of the brain called the cortex. These abnormal electrical discharges occur in a pattern that involves both sides of the brain simultaneously. This differs from other types of epilepsy, which may involve only one side of the brain or specific areas within a single hemisphere.
Absence seizures are typically brief and do not cause confusion or disorientation after they end. However, if they occur frequently, they can interfere with learning and social development. In some cases, absence epilepsy may be associated with other types of seizures, such as generalized tonic-clonic (grand mal) seizures or myoclonic jerks.
The diagnosis of absence epilepsy is usually made based on the characteristic symptoms and the results of an electroencephalogram (EEG), which can detect the abnormal electrical activity in the brain during a seizure. Treatment typically involves medication to control the seizures, such as ethosuximide or valproic acid. In some cases, a ketogenic diet may also be recommended as an alternative treatment option.
I'm sorry for any confusion, but "pamphlets" is not a medical term. It refers to a small paper booklet or leaflet that can be used to provide information on various topics, including non-medical subjects. If you have any questions about medical terminology or concepts, I'd be happy to help with those!
Neurology is a branch of medicine that deals with the study and treatment of diseases and disorders of the nervous system, which includes the brain, spinal cord, peripheral nerves, muscles, and autonomic nervous system. Neurologists are medical doctors who specialize in this field, diagnosing and treating conditions such as stroke, Alzheimer's disease, epilepsy, Parkinson's disease, multiple sclerosis, and various types of headaches and pain disorders. They use a variety of diagnostic tests, including imaging studies like MRI and CT scans, electrophysiological tests like EEG and EMG, and laboratory tests to evaluate nerve function and identify any underlying conditions or abnormalities. Treatment options may include medication, surgery, rehabilitation, or lifestyle modifications.