Pneumoencephalography
Computerised axial tomography in patients with severe migraine: a preliminary report. (1/64)
Patients suffering from severe migraine, usually for many years, have been examined by the EMI scanner between attacks. Judged by criteria validated originally by comparison with pneumoencephalography, about half of the patients showed evidence of cerebral atrophy. Perhaps of more significance than generalised atrophy was the frequency of areas of focal atrophy and of evidence of infarction. (+info)The empty sella syndrome. (2/64)
The empty sella syndrome (ESS) presents a varied clinical and radiographic picture. It may remain asymptomatic or may stimulate an intrasellar growth thereby causing diagnostic and therapeutic problems. An air encephalogram (AEG) is required for diagnosis. The purpose of this paper is to review the clinical and radiological features of the ESS and to discuss the pathogenetic mechanisms involved. (+info)A retrospective analysis of spontaneous sphenoid sinus fistula: MR and CT findings. (3/64)
BACKGROUND AND PURPOSE: The sphenoid sinus is rarely implicated as a site of spontaneous CSF fistula. We undertook this study to evaluate the potential etiopathogenesis of spontaneous CSF fistula involving the sphenoid sinus and to review the imaging findings. METHODS: We retrospectively reviewed the imaging findings of 145 cases of CSF fistula from our departmental archives (August 1995 through August 1998). Fifteen (10%) patients had CSF fistulas involving the sphenoid sinus. Eleven (7%) patients had spontaneous CSF fistulas, whereas in four patients, the CSF fistulas in the sphenoid sinus were related to trauma. Of the 11 patients, nine underwent only plain high-resolution CT and MR cisternography. One patient additionally underwent contrast-enhanced CT cisternography, and one other patient underwent MR cisternography only. For each patient, the CSF fistula site was surgically confirmed. The MR imaging technique included T1-weighted and fast spin-echo T2-weighted 3-mm-thick coronal sequences obtained with the patient in the supine position. The plain high-resolution CT study included 3-mm-thick, and sometimes 1- to 1.5-mm-thick, coronal sections obtained with the patient in the prone position. Similar sections were obtained after injecting nonionic contrast material intrathecally via lumbar puncture for the CT cisternographic study. We evaluated each of the 11 patients for the exact site of CSF leak in the sphenoid sinus. We also determined the presence of pneumatization of lateral recess of the sphenoid sinus, orientation of the lateral wall of the sphenoid sinus, presence of arachnoid pits, presence of brain tissue herniation, and presence of empty sella in each of these patients. RESULTS: The exact sites of the CSF fistulas were documented for all 11 patients by using plain high-resolution CT, MR cisternography, or CT cisternography. In nine (82%) patients, the sites of the CSF fistulas were at the junction of the anterior portion of the lateral wall of the sphenoid sinus and the floor of the middle cranial fossa. In the remaining two (18%) patients, the sites of the CSF fistulas were along the midportion of the lateral wall of the sphenoid sinus. Of these 11 patients, one had bilateral sites of the CSF fistula at the junction of the anterior portion of the lateral wall of the sphenoid sinus with the floor of the middle cranial fossa. In nine (82%) patients, the presence of brain tissue herniation was revealed, and this finding was best shown by MR cisternography. Ten (91%) patients had extensive pneumatization of the lateral recess of the sphenoid sinus, with an equal number having outward concave orientation of the inferior portion of the lateral wall of the sphenoid sinus. In seven (63%) patients, the presence of arachnoid pits, predominantly along the anteromedial aspect of the middle cranial fossa, was shown. In seven (63%) patients, empty sella was shown. For comparison, we reviewed the CT studies of the paranasal sinuses in 100 age-matched control subjects from a normal population. Twenty-three had extensive lateral pneumatization of the sphenoid sinus along with outward concavity of the inferior portion of the lateral wall. None of these 23 patients had arachnoid pits. CONCLUSION: The sphenoid sinus, when implicated as a site of spontaneous CSF leak, yields a multitude of imaging findings. These are extensive pneumatization of the lateral recess of the sphenoid sinus, outward concave orientation of the inferior portion of the lateral wall of the sphenoid sinus, arachnoid pits, and empty sella. Considering the normative data, we speculate that this constellation of findings could play a role in the etiopathogenesis of spontaneous sphenoid sinus fistulas. Our findings also show the efficacy of noninvasive imaging techniques, such as plain high-resolution CT and MR cisternography, in the evaluation of sphenoid sinus CSF leak. Our data also suggest that spontaneous sphenoid sinus CSF leak is not an uncommon occurrenc (+info)Radiological abnormalities in temporal lobe epilepsy with clinicopathological correlations. (4/64)
In 73 patients with drug-resistant temporal lobe epilepsy submitted to an unilateral anterior temporal lobectomy the radiographs were studied to see if there were any correlation with the pathology subsequently found and with the outcome of the operation. A small middle cranial fossa, focal calcification, and temporal horn displacement are often better indices of the underlying pathology than temporal horn dilatation alone. In a small number of cases, however, radiological changes were seen on the side opposite to an unilateral EEG focus, thus suggesting bilateral disease. (+info)Supratentorial extracerebral cysts in infants and children. (5/64)
Twelve cases of supratentorial extracerebral cysts in infants and children are reported. Eight were located in the Sylvian fissure, two in the interhemispheric fissue, and two over the convexity of the cerebral hemispheres. Irrespective of their precise location these cysts, in their common, uncomplicated form, give rise to a clinical syndrome different from that recorded in older patients, with a symmetrical macrocrania of a severe degree unassociated with any neurological signs or abnormalities in psychomotor development. Extensive unilateral transillumination of the skull is common (six cases). These features, in association with specific angiographic and pneumoencephalographic findings, make a preoperative diagnosis possible. Extracerebral cysts (either arachnoidal or histologically more complex) should be distinguished from intracerebral cavities which may closely mimic them, even at surgery. The natural history of infatile cysts is studied and serial head-measurements (pre-and postoperative) are presented in five cases. Insufficient knowledge of the spontaneous course and incidence of complications prevents definite statements on the necessity and type of therapy. (+info)Electroencephalographic findings in a case of globoid cell leukodystrophy. (6/64)
An increased slow wave pattern of the EEG basic waves without epileptogenic discharges was observed in an early stage of a case of Krabbe's disease. In the later stage of the illness, spikes and sharp waves were mixed with. The peculiar runs of fast activity which were described by Kliemann et al. (1969) were not observed during the course of our patient. (+info)MR cisternography of the cerebellopontine angle: comparison of three-dimensional fast asymmetrical spin-echo and three-dimensional constructive interference in the steady-state sequences. (7/64)
BACKGROUND AND PURPOSE: MR cisternography has been used as the noninvasive screening tool of the cerebellopontine angle. The purpose of this study was to directly compare two currently dominant types of sequences for heavily T2-weighted MR cisternography. METHODS: Three-dimensional fast asymmetric spin-echo (3D-FASE) sequences, which are 3D half-Fourier rapid acquisition with relaxation enhancement and 3D constructive interference in the steady-state (3D-CISS) sequences, were compared on a clinical 1.5-T MR unit using the same scan times. In five healthy volunteers, the contrast-to-noise ratio (C/N) between CSF and the cerebellum was measured at three locations. Then, for qualitative analysis, the quality of the labyrinth was scored on the original source multiplanar reformatted images, the virtual endoscopic images, and the maximum intensity projection (MIP) images. In 20 consecutive patients with suspected cerebellopontine angle tumors, visualization of the tumors was evaluated using 3D contrast-enhanced spoiled gradient-echo imaging as the standard of reference. RESULTS: Both sequences showed comparable mean C/N values; however, in qualitative analysis, the scores for 3D-CISS on the source, virtual endoscopic, and MIP images were significantly lower than those on the images obtained with 3D-FASE, owing to more prominent flow and magnetic susceptibility artifacts on the 3D-CISS sequences. In all subjects, discontinuity of the semicircular canals was seen on the virtual endoscopic and MIP images obtained with 3D-CISS, owing to susceptibility artifacts, but not on those obtained with 3D-FASE. All 12 tumors were detected by both sequences, but 3D-CISS gave one false-positive result. CONCLUSION: 3D-FASE is considered the method of choice because artifacts are reduced and specificity is increased. (+info)Acute hemiplegia of childhood. (8/64)
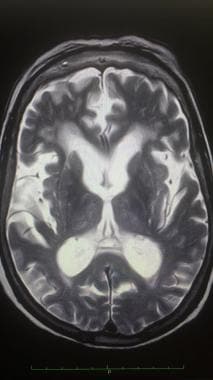
Acute hemiplegia of obscure cause occurred in 28 children: 13 had had prolonged seizures and a high temperature (considered to have been the direct cause of the brain damage); 5 had had brief seizures, a lower temperature and a depressed level of consciousness; and 10 had a nonfebrile onset of hemiplegia and were found to have vascular abnormalities. Most of the first group were retarded and epileptic at long-term follow-up, as were about half of the second group, whereas children in the third group were of normal intelligence and epilepsy was uncommon among them. Hemiplegia persisted at follow-up in most of the children in each group, the proportion being at least in the third group; if cerebral angiography had demonstrated carotid stenosis or occlusion there was usually poor recovery from the hemiplegia. Bilateral changes on plain skull films or pneumoencephalograms were associated with mental retardation. Failure to control prolonged seizures accompanied by a high temperature predisposes to brain damage; therefore, early and vigorous management is essential. (+info)Pneumoencephalography is a diagnostic procedure that is rarely used today, due to the development of less invasive techniques. It involves the introduction of air or another gas into the ventricular system or subarachnoid space of the brain, followed by X-ray imaging to visualize the structures and any abnormalities within the intracranial cavity.
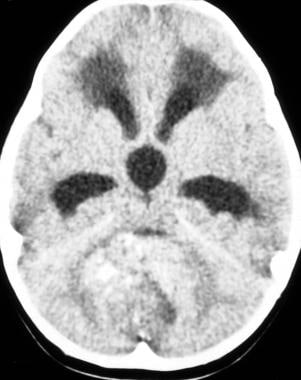
The primary purpose of this procedure was to diagnose conditions affecting the brain's ventricles, such as hydrocephalus, tumors, or inflammation. The introduction of air into the cranium allowed for better visualization of these structures and any potential abnormalities. However, due to its invasive nature, risks associated with the procedure, and the availability of non-invasive imaging techniques like CT and MRI scans, pneumoencephalography has fallen out of favor in modern medicine.
Cerebral ventriculography is a medical imaging technique that involves the injection of a contrast material into the cerebral ventricles, which are fluid-filled spaces within the brain. The purpose of this procedure is to produce detailed images of the ventricular system and the surrounding structures in order to diagnose and evaluate various neurological conditions, such as hydrocephalus (excessive accumulation of cerebrospinal fluid in the ventricles), tumors, or other abnormalities that may be causing obstruction or compression of the ventricular system.
The procedure typically involves inserting a thin, flexible tube called a catheter into the lateral ventricle of the brain through a small hole drilled in the skull. The contrast material is then injected through the catheter and X-ray images are taken as the contrast material flows through the ventricular system. These images can help to identify any abnormalities or blockages that may be present.
Cerebral ventriculography has largely been replaced by non-invasive imaging techniques, such as computed tomography (CT) and magnetic resonance imaging (MRI), which provide similar information without the need for invasive procedures. However, cerebral ventriculography may still be used in certain cases where these other methods are not sufficient to make a definitive diagnosis.
 Pneumoencephalography
Pneumoencephalography
History of neuroimaging
Neuroimaging
Walter Dandy
Kurt Amplatz
Encephalography
History of computed tomography
Septum pellucidum
Lars Leksell
Jean-Athanase Sicard
Cerebellar vermis
Charles Bradley (medical doctor)
William H. Oldendorf
Timeline of tuberous sclerosis
Hypopituitarism
Radiocontrast agent
Harvey Cushing
Henrietta Lacks
Amygdalotomy
Psychosis
Peg
Central Institute of Psychiatry Ranchi
Brain tumor
List of MeSH codes (E01)
Pneumoencephalography - Wikipedia
Intraocular haemorrhage as a complication of pneumoencephalography. | Journal of Neurology, Neurosurgery & Psychiatry
Intraocular haemorrhage as a complication of pneumoencephalography. | Journal of Neurology, Neurosurgery & Psychiatry
 Intellectual development in shunted hydrocephalic children
Intellectual development in shunted hydrocephalic children Normal Pressure Hydrocephalus Imaging: Practice Essentials, Computed Tomography, Magnetic Resonance Imaging
Normal Pressure Hydrocephalus Imaging: Practice Essentials, Computed Tomography, Magnetic Resonance Imaging
Download The European Convention On Human Rights : A Commentary
 9 Great Neurosurgery Accomplishments and Achievements of the Last Century - The Frisky
9 Great Neurosurgery Accomplishments and Achievements of the Last Century - The Frisky
Plus it
PEDIATRIC NEURORADIOLOGY | American Journal of Neuroradiology
 Surgical Neurology International
Surgical Neurology International
 Empty sella | Radiology Reference Article | Radiopaedia.org
Empty sella | Radiology Reference Article | Radiopaedia.org
Magnetoencephalography - Wikipedia
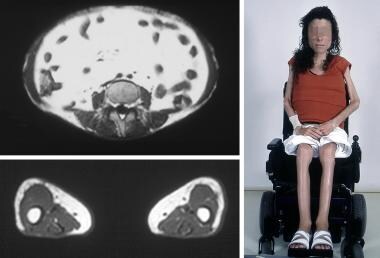
 WIDI - N7) Weakness and parasthesias in an immunosuppressed patient
WIDI - N7) Weakness and parasthesias in an immunosuppressed patient
Pneumoradiography | Profiles RNS
pneumogastric | Encyclopedia.com
Frederick H Sklar - Research output - University of Texas Southwestern Medical Center
 Крок 2 Медицина - 2020 1 день
Крок 2 Медицина - 2020 1 день
 HANGMAN SOLVER - English 19 letter words - Containing letters ng - page 1
HANGMAN SOLVER - English 19 letter words - Containing letters ng - page 1TRICARE Manuals - Display Chap 199.4 (Change 3, Dec 11, 2018)
 Communicating hydrocephalus
Communicating hydrocephalus
 Brain Changes Occur in Mentally Ill Who Have Never Been Medicated : Mental Illness Policy Org
Brain Changes Occur in Mentally Ill Who Have Never Been Medicated : Mental Illness Policy Org
SECOND WORLD WAR | NZETC
Download Edv Systeme Im Finanz
Shop Real World Windows 8 App Development With Javascript: Create Great Windows Store Apps 2013
 Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS
Wilhelm Roentgen | Radiology Reference Article | Radiopaedia.org
 Empty sella prevalence: step by step | Russian Open Medical Journal
Empty sella prevalence: step by step | Russian Open Medical Journal
From the archives: Crownsville State Hospital
Density of Lumbar Cerebrospinal Fluid in Pregnant and Nonpregnant Humans | Anesthesiology | American Society of...
Angiography3
- I was surprised to find, when undertaking this assignment, that the first 5 years of pediatric neuroimaging in the AJNR were not defined by conventional angiography, pneumoencephalography, or ventriculography, as we might expect, but rather by sonography and CT. (ajnr.org)
- Before the development of cross-sectional and multiplanar imaging, angiography and pneumoencephalography were used to localize brain masses and characterize tumor vascularity. (medscape.com)
- There has been a decline in the use of cerebral angiography and pneumoencephalography, especially the latter, in the diagnostic workup of these patients since the introduction of CT scanning. (jamanetwork.com)
Ventriculography1
- When it comes to important accomplishments, these include the design of air ventriculography and pneumoencephalography, the illustration of brain endoscopy and the circulation of cerebrospinal fluid in the brain, medical treatment of hydrocephalus , as well as the launching of the first intensive care unit in 1923. (thefrisky.com)
Obsolete2
- Modern imaging techniques such as MRI and CT have rendered pneumoencephalography obsolete. (wikipedia.org)
- Since more modern, less aggressive neuroimaging techniques have been employed during recent years, pneumoencephalography is considered to be obsolete and is seldom used anymore. (largest.org)
Hydrocephalus1
- Pneumoencephalography was used to demonstrate nonobstructive hydrocephalus. (medscape.com)
Brain3
- Though pneumoencephalography was the single most important way of localizing brain lesions of its time, it was nevertheless extremely painful and generally not well tolerated by conscious patients. (wikipedia.org)
- Despite its overall usefulness, there were major portions of the brain and other structures of the head that pneumoencephalography was unable to image. (wikipedia.org)
- Pneumoencephalography is also sometimes called an "air study" and involves removing the vast majority of the cerebrospinal fluid from around the brain. (largest.org)
Development1
- Following the development of pneumoencephalography in the 1920s, Jacobi and Winkler (1927) used this technique on 19 patients with schizophrenia and reported that 18 of them had enlarged cerebral ventricles. (mentalillnesspolicy.org)
Plain2
- Pneumoencephalography makes use of plain X-ray images. (wikipedia.org)
- It should be noted that the term was originally described in the context of an enlarged fossa seen on plain radiography (or pneumoencephalography , etc.), without a mass being found at surgery. (radiopaedia.org)
Painful2
- Though pneumoencephalography was the single most important way of localizing brain lesions of its time, it was nevertheless extremely painful and generally not well tolerated by conscious patients. (wikipedia.org)
- Pneumoencephalography was a painful procedure that required a lumbar puncture and an injection into the cerebrospinal fluid space, followed by radiography. (medscape.com)
Structures3
- The aim of pneumoencephalography is to outline these shadow-forming air-filled structures so that their shape and anatomical location can be examined. (wikipedia.org)
- Despite its overall usefulness, there were major portions of the brain and other structures of the head that pneumoencephalography was unable to image. (wikipedia.org)
- However, at that time, only primitive methods for visualizing intracranial structures were available, such as pneumoventriculography and pneumoencephalography. (medscape.com)
Risk1
- Another drawback of pneumoencephalography was that the risk and discomfort it carried meant that repeat studies were generally avoided, thus making it difficult to assess disease progression over time. (wikipedia.org)