Myocardial Ischemia
Ischemia
Brain Ischemia
Myocardial Reperfusion Injury
Myocardium
Coronary Disease
Electrocardiography
Reperfusion Injury
Exercise Test
Myocardial Infarction
Myocardial Reperfusion
Angina Pectoris
Cardiotonic Agents
Ischemic Preconditioning, Myocardial
Hemodynamics
Dogs
Electrocardiography, Ambulatory
Disease Models, Animal
Coronary Angiography
Tomography, Emission-Computed, Single-Photon
Arrhythmias, Cardiac
Reperfusion
Rats, Sprague-Dawley
Myocardial Perfusion Imaging
Ventricular Function, Left
Creatine Kinase
Ischemic Preconditioning
Ischemic Attack, Transient
Rats, Wistar
Warm Ischemia
Dipyridamole
Myocardial Stunning
Thallium Radioisotopes
Adenosine
Coronary Artery Disease
Collateral Circulation
Dobutamine
Myocytes, Cardiac
Swine
Intraoperative Complications
Echocardiography
Cold Ischemia
Echocardiography, Stress
Troponin I
Rabbits
Heart Ventricles
Ischemic Postconditioning
Gerbillinae
Spinal Cord Ischemia
Ventricular Fibrillation
Troponin T
Nitroglycerin
Anesthesia
Lactic Acid
Cardiovascular Agents
Prospective Studies
Swine, Miniature
Predictive Value of Tests
Random Allocation
Necrosis
Angina Pectoris, Variant
Coronary Vessel Anomalies
Neuroprotective Agents
L-Lactate Dehydrogenase
Biological Markers
Ventricular Dysfunction, Left
Infarction, Middle Cerebral Artery
Mice, Inbred C57BL
Peroxidase
Adenosine Triphosphate
Adrenergic beta-Antagonists
Coronary Artery Bypass
Apoptosis
Microvascular Angina
Oxygen Consumption
Ergonovine
Diltiazem
Risk Factors
Phosphocreatine
Technetium Tc 99m Sestamibi
Angioplasty, Balloon, Coronary
Sensitivity and Specificity
Nitric Oxide
Neovascularization, Physiologic
Pericardium
Cats
Organotechnetium Compounds
Oxygen
Arterial Occlusive Diseases
Ventricular Pressure
Iodobenzenes
Anti-Arrhythmia Agents
Heart Conduction System
Blood Flow Velocity
Cerebral Infarction
Acetanilides
Brain
Dose-Response Relationship, Drug
Hindlimb
Double-Blind Method
Cardiac Pacing, Artificial
Analysis of Variance
Isosorbide Dinitrate
Oxidative Stress
Prognosis
Radiopharmaceuticals
Follow-Up Studies
Acidosis
Stroke Volume
Severity of Illness Index
Endothelium, Vascular
Mice, Knockout
Chronic Disease
Cardiac Catheterization
Cell Death
Enzyme Inhibitors
Models, Animal
Signal Transduction
Cardiac-Gated Single-Photon Emission Computer-Assisted Tomography
Myocardial Revascularization
Vectorcardiography
Monitoring, Physiologic
Sympathetic Nervous System
Energy Metabolism
Coronary Occlusion
Cardioplegic Solutions
Microspheres
Risk Assessment
Receptors, Histamine H3
Postoperative Complications
Rats, Inbred Strains
Potassium Channels
Norepinephrine
Mesenteric Vascular Occlusion
Models, Cardiovascular
Immunohistochemistry
Sus scrofa
Myocardial Bridging
In Situ Nick-End Labeling
Monitoring, Intraoperative
Tachycardia
Neurons
Mucocutaneous Lymph Node Syndrome
Neutrophils
Atenolol
Cytoprotection
Bradykinin
Isoflurane
Premedication
Calcium
Reproducibility of Results
Fractional Flow Reserve, Myocardial
Brain Edema
Blotting, Western
Cells, Cultured
Troponin
Antioxidants
Reactive Oxygen Species
Nitric Oxide Synthase
Vasodilation
AMP-activated protein kinase phosphorylation of endothelial NO synthase. (1/6685)
The AMP-activated protein kinase (AMPK) in rat skeletal and cardiac muscle is activated by vigorous exercise and ischaemic stress. Under these conditions AMPK phosphorylates and inhibits acetyl-coenzyme A carboxylase causing increased oxidation of fatty acids. Here we show that AMPK co-immunoprecipitates with cardiac endothelial NO synthase (eNOS) and phosphorylates Ser-1177 in the presence of Ca2+-calmodulin (CaM) to activate eNOS both in vitro and during ischaemia in rat hearts. In the absence of Ca2+-calmodulin, AMPK also phosphorylates eNOS at Thr-495 in the CaM-binding sequence, resulting in inhibition of eNOS activity but Thr-495 phosphorylation is unchanged during ischaemia. Phosphorylation of eNOS by the AMPK in endothelial cells and myocytes provides a further regulatory link between metabolic stress and cardiovascular function. (+info)Differential regulation of Bcl-2, AP-1 and NF-kappaB on cardiomyocyte apoptosis during myocardial ischemic stress adaptation. (2/6685)
Acute ischemia followed by prolonged reperfusion has been shown to induce cardiomyocyte apoptosis. In this report, we demonstrate that myocardial adaptation to ischemia induced by repeated cyclic episodes of short-term ischemia each followed by another short duration of reperfusion reduced cardiomyocyte apoptosis and DNA fragmentation. This was associated with the induction of the expression of Bcl-2 mRNA and translocation and activation of NF-kappaB. Another transcription factor, AP-1, remained unaffected by repeated ischemia and reperfusion, but exhibited significant upregulation by a single episode of 30 min ischemia followed by 2 h of reperfusion. This activation of AP-1 was inhibited by a scavenger of oxygen free radicals, DMTU. Thirty minutes ischemia and 120 min reperfusion downregulated the induction of the expression of Bcl-2 mRNA, but moderately activated NF-kappaB binding activity. This was associated with an increased number of apoptotic cells and DNA fragmentation in cardiomyocytes which were attenuated by DMTU. The results of this study indicate that Bcl-2, AP-1 and NF-kappaB differentially regulate cardiomyocyte apoptosis mediated by acute ischemia and prolonged reperfusion. (+info)Chlamydia pneumoniae antibodies are associated with an atherogenic lipid profile. (3/6685)
OBJECTIVE: To determine, within a representative population group of men and women, whether alteration of the lipid profile might underlie the reported association between Chlamydia pneumoniae and ischaemic heart disease. DESIGN AND SETTING: Cross sectional survey in an area with a high incidence of ischaemic heart disease. SUBJECTS: 400 randomly selected participants in the World Health Organisation MONICA project's third population survey in Northern Ireland. MAIN OUTCOME MEASURES: Stored sera were examined by microimmunofluorescence for IgG antibodies to C pneumoniae at a dilution of 1 in 64. Mean total and high density lipoprotein (HDL) cholesterol were compared between seropositive and seronegative individuals with adjustment for age, measures of socioeconomic status, smoking habit, alcohol consumption, body mass index, and the season during which blood had been taken. RESULTS: In seropositive men, adjusted mean serum total cholesterol and HDL cholesterol were 0.5 mmol/l (9.2%) higher and 0.11 mmol/l (9.3%) lower, respectively, than in seronegative men. Differences in women did not achieve statistical significance, but both total cholesterol and HDL cholesterol were higher (3.6% and 5.8%, respectively) in seropositive than in seronegative individuals. CONCLUSIONS: There is serological evidence that C pneumoniae infection is associated with an atherogenic lipid profile in men. Altered lipid levels may underlie the association between C pneumoniae and ischaemic heart disease. (+info)Cytomegalovirus seropositivity and incident ischaemic heart disease in the Caerphilly prospective heart disease study. (4/6685)
OBJECTIVE: To assess the role of cytomegalovirus (CMV) infection in primary ischaemic heart disease. METHODS: Plasma specimens collected during 1979-83 from men in Caerphilly, south Wales, were analysed for IgG antibodies to CMV by enzyme linked immunosorbent assay and latex tests. Incident ischaemic heart disease events were ascertained after five and 10 years from death certificates, hospital records, and ECG changes; 195 incident ischaemic heart disease cases were compared with 216 controls of a similar age drawn from the rest of the cohort. RESULTS: 164 cases (84%) and 180 controls (83%) were seropositive for CMV. Optical density, an indicator of CMV antibody titre, was similar for cases and controls. Among controls, seropositivity was not associated with age, socioeconomic status currently or in childhood, smoking, height, body mass index, blood pressure, total cholesterol, fibrinogen, plasma viscosity, or leucocyte count. The unadjusted odds ratio relating CMV seropositivity to incident ischaemic heart disease was 1.06 (95% confidence interval 0.63 to 1.79) and was little changed (1.11, 0.63 to 1.97) after adjustment for age, smoking, body mass index, systolic blood pressure, total cholesterol, and socioeconomic status currently and in childhood. CONCLUSIONS: CMV infection is unlikely to be a strong risk factor for development of myocardial infarction in middle aged men. (+info)Reactive oxygen species play an important role in the activation of heat shock factor 1 in ischemic-reperfused heart. (5/6685)
BACKGROUND: The myocardial protective role of heat shock protein (HSP) has been demonstrated. Recently, we reported that ischemia/reperfusion induced a significant activation of heat shock factor (HSF) 1 and an accumulation of mRNA for HSP70 and HSP90. We examined the role of reactive oxygen species (ROSs) in the induction of stress response in the ischemic-reperfused heart. METHODS AND RESULTS: Rat hearts were isolated and perfused with Krebs-Henseleit buffer by the Langendorff method. Whole-cell extracts were prepared for gel mobility shift assay using oligonucleotides containing the heat shock element. Induction of mRNA for HSP70 and HSP90 was examined by Northern blot analysis. Repetitive ischemia/reperfusion, which causes recurrent bursts of free radical generation, resulted in burst activation of HSF1, and this burst activation was significantly reduced with either allopurinol 1 mmol/L (an inhibitor of xanthine oxidase) or catalase 2x10(5) U/L (a scavenger of H2O2). Significant activation of HSF1 was observed on perfusion with buffer containing H2O2 150 micromol/L or xanthine 1 mmol/L plus xanthine oxidase 5 U/L. The accumulation of mRNA for HSP70 or HSP90 after repetitive ischemia/reperfusion was reduced with either allopurinol or catalase. CONCLUSIONS: Our findings demonstrate that ROSs play an important role in the activation of HSF1 and the accumulation of mRNA for HSP70 and HSP90 in the ischemic-reperfused heart. (+info)Bradykinin promotes ischemic norepinephrine release in guinea pig and human hearts. (6/6685)
We previously reported that bradykinin (BK; 1-1000 nM) facilitates norepinephrine (NE) release from cardiac sympathetic nerves. Because BK production increases in myocardial ischemia, endogenous BK could foster NE release and associated arrhythmias. We tested this hypothesis in guinea pig and human myocardial ischemia models. BK administration (100 nM) markedly enhanced exocytotic and carrier-mediated NE overflow from guinea pig hearts subjected to 10- and 20-min ischemia/reperfusion, respectively. Ventricular fibrillation invariably occurred after 20-min global ischemia; BK prolonged its duration 3-fold. The BK B2 receptor antagonist HOE140 (30 nM) blocked the effects of BK, whereas the B1 receptor antagonist des-Arg9-Leu8-BK (1 microM; i.e., 2.5 x pA2) did not. When serine proteinase inhibitors (500 KIU/ml aprotinin and 100 microg/ml soybean trypsin inhibitor) were used to prevent the formation of endogenous BK, NE overflow and reperfusion arrhythmias were diminished. In contrast, when kininase I and II inhibitors (DL-2-mercaptomethyl-3-guanidinoethylthiopropanoic acid and enalaprilat, each 1 microM) were used to prevent the degradation of endogenous BK, NE overflow and reperfusion arrhythmias were enhanced. B2 receptor blockade abolished these effects but was ineffective if kininases were not inhibited. B2 receptor stimulation, by either exogenous or endogenous BK, also markedly enhanced carrier-mediated NE release in the human myocardial ischemia model; conversely, inhibition of BK biosynthesis diminished ischemic NE release. Because atherosclerotic heart disease impairs endothelial BK production, in myocardial ischemia BK could accumulate at sympathetic nerve endings, thus augmenting exocytotic and carrier-mediated NE release and favoring coronary vasoconstriction and arrhythmias. (+info)Labeling of the internal pool of GP IIb-IIIa in platelets by c7E3 Fab fragments (abciximab): flow and endocytic mechanisms contribute to the transport. (7/6685)
Abciximab is a new antiplatelet therapeutic in ischemic cardiovascular disease. The drug, chimeric Fab fragments of a murine monoclonal antibody (MoAb) (c7E3), blocks GP IIb-IIIa function. However, its capacity to reach all receptor pools in platelets is unknown. Electron microscopy and immunogold labeling were used to localize abciximab in platelets of patients receiving the drug for up to 24 hours. Studies on frozen-thin sections showed that c7E3 Fab, in addition to the surface pool, also labeled the surface-connected canalicular system (SCCS) and alpha-granules. Analysis of gold particle distribution showed that intraplatelet labeling was not accumulative and in equilibrium with the surface pool. After short-term incubations of platelets with c7E3 Fab in vitro, gold particles were often seen in lines within thin elements of the SCCS, some of which appeared in contact with alpha-granules. Little labeling was associated with Glanzmann's thrombasthenia platelets, confirming that the channels contained bound and not free c7E3 Fab. Endocytosis of abciximab in clathrin-containing vesicles was visualized by double staining and constitutes an alternative mechanism of transport. The remaining free pool of GP IIb-IIIa was evaluated with the MoAb AP-2; flow cytometry showed it to be about 9% on the surface of nonstimulated platelets but 33% on thrombin-activated platelets. The ability of drugs to block all pools of GP IIb-IIIa and then to be associated with secretion-dependent residual aggregation must be considered when evaluating their efficiency in a clinical context. (+info)An inhibitor of p38 mitogen-activated protein kinase protects neonatal cardiac myocytes from ischemia. (8/6685)
Cellular ischemia results in activation of a number of kinases, including p38 mitogen-activated protein kinase (MAPK); however, it is not yet clear whether p38 MAPK activation plays a role in cellular damage or is part of a protective response against ischemia. We have developed a model to study ischemia in cultured neonatal rat cardiac myocytes. In this model, two distinct phases of p38 MAPK activation were observed during ischemia. The first phase began within 10 min and lasted less than 1 h, and the second began after 2 h and lasted throughout the ischemic period. Similar to previous studies using in vivo models, the nonspecific activator of p38 MAPK and c-Jun NH2-terminal kinase, anisomycin, protected cardiac myocytes from ischemic injury, decreasing the release of cytosolic lactate dehydrogenase by approximately 25%. We demonstrated, however, that a selective inhibitor of p38 MAPK, SB 203580, also protected cardiac myocytes against extended ischemia in a dose-dependent manner. The protective effect was seen even when the inhibitor was present during only the second, sustained phase of p38 MAPK activation. We found that ischemia induced apoptosis in neonatal rat cardiac myocytes and that SB 203580 reduced activation of caspase-3, a key event in apoptosis. These results suggest that p38 MAPK induces apoptosis during ischemia in cardiac myocytes and that selective inhibition of p38 MAPK could be developed as a potential therapy for ischemic heart disease. (+info)Myocardial ischemia is a condition in which the blood supply to the heart muscle (myocardium) is reduced or blocked, leading to insufficient oxygen delivery and potential damage to the heart tissue. This reduction in blood flow typically results from the buildup of fatty deposits, called plaques, in the coronary arteries that supply the heart with oxygen-rich blood. The plaques can rupture or become unstable, causing the formation of blood clots that obstruct the artery and limit blood flow.
Myocardial ischemia may manifest as chest pain (angina pectoris), shortness of breath, fatigue, or irregular heartbeats (arrhythmias). In severe cases, it can lead to myocardial infarction (heart attack) if the oxygen supply is significantly reduced or cut off completely, causing permanent damage or death of the heart muscle. Early diagnosis and treatment of myocardial ischemia are crucial for preventing further complications and improving patient outcomes.
Ischemia is the medical term used to describe a lack of blood flow to a part of the body, often due to blocked or narrowed blood vessels. This can lead to a shortage of oxygen and nutrients in the tissues, which can cause them to become damaged or die. Ischemia can affect many different parts of the body, including the heart, brain, legs, and intestines. Symptoms of ischemia depend on the location and severity of the blockage, but they may include pain, cramping, numbness, weakness, or coldness in the affected area. In severe cases, ischemia can lead to tissue death (gangrene) or organ failure. Treatment for ischemia typically involves addressing the underlying cause of the blocked blood flow, such as through medication, surgery, or lifestyle changes.
Brain ischemia is the medical term used to describe a reduction or interruption of blood flow to the brain, leading to a lack of oxygen and glucose delivery to brain tissue. This can result in brain damage or death of brain cells, known as infarction. Brain ischemia can be caused by various conditions such as thrombosis (blood clot formation), embolism (obstruction of a blood vessel by a foreign material), or hypoperfusion (reduced blood flow). The severity and duration of the ischemia determine the extent of brain damage. Symptoms can range from mild, such as transient ischemic attacks (TIAs or "mini-strokes"), to severe, including paralysis, speech difficulties, loss of consciousness, and even death. Immediate medical attention is required for proper diagnosis and treatment to prevent further damage and potential long-term complications.
Myocardial reperfusion injury is a pathological process that occurs when blood flow is restored to the heart muscle (myocardium) after a period of ischemia or reduced oxygen supply, such as during a myocardial infarction (heart attack). The restoration of blood flow, although necessary to salvage the dying tissue, can itself cause further damage to the heart muscle. This paradoxical phenomenon is known as myocardial reperfusion injury.
The mechanisms behind myocardial reperfusion injury are complex and involve several processes, including:
1. Oxidative stress: The sudden influx of oxygen into the previously ischemic tissue leads to an overproduction of reactive oxygen species (ROS), which can damage cellular structures, such as proteins, lipids, and DNA.
2. Calcium overload: During reperfusion, there is an increase in calcium influx into the cardiomyocytes (heart muscle cells). This elevated intracellular calcium level can disrupt normal cellular functions, leading to further damage.
3. Inflammation: Reperfusion triggers an immune response, with the recruitment of inflammatory cells, such as neutrophils and monocytes, to the site of injury. These cells release cytokines and other mediators that can exacerbate tissue damage.
4. Mitochondrial dysfunction: The restoration of blood flow can cause mitochondria, the powerhouses of the cell, to malfunction, leading to the release of pro-apoptotic factors and contributing to cell death.
5. Vasoconstriction and microvascular obstruction: During reperfusion, there may be vasoconstriction of the small blood vessels (microvasculature) in the heart, which can further limit blood flow and contribute to tissue damage.
Myocardial reperfusion injury is a significant concern because it can negate some of the benefits of early reperfusion therapy, such as thrombolysis or primary percutaneous coronary intervention (PCI), used to treat acute myocardial infarction. Strategies to minimize myocardial reperfusion injury are an area of active research and include pharmacological interventions, ischemic preconditioning, and remote ischemic conditioning.
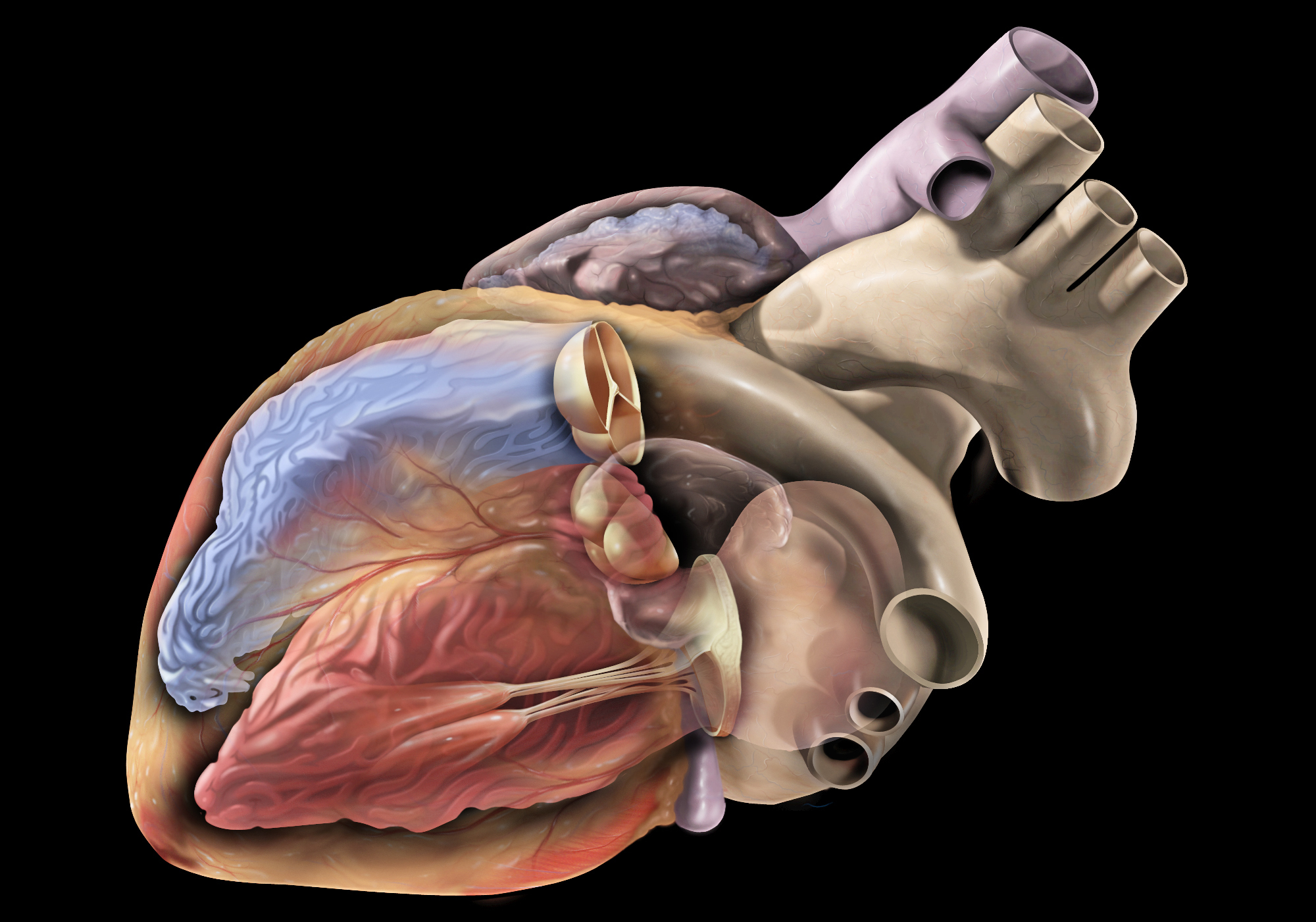
The myocardium is the middle layer of the heart wall, composed of specialized cardiac muscle cells that are responsible for pumping blood throughout the body. It forms the thickest part of the heart wall and is divided into two sections: the left ventricle, which pumps oxygenated blood to the rest of the body, and the right ventricle, which pumps deoxygenated blood to the lungs.
The myocardium contains several types of cells, including cardiac muscle fibers, connective tissue, nerves, and blood vessels. The muscle fibers are arranged in a highly organized pattern that allows them to contract in a coordinated manner, generating the force necessary to pump blood through the heart and circulatory system.
Damage to the myocardium can occur due to various factors such as ischemia (reduced blood flow), infection, inflammation, or genetic disorders. This damage can lead to several cardiac conditions, including heart failure, arrhythmias, and cardiomyopathy.
Coronary circulation refers to the circulation of blood in the coronary vessels, which supply oxygenated blood to the heart muscle (myocardium) and drain deoxygenated blood from it. The coronary circulation system includes two main coronary arteries - the left main coronary artery and the right coronary artery - that branch off from the aorta just above the aortic valve. These arteries further divide into smaller branches, which supply blood to different regions of the heart muscle.
The left main coronary artery divides into two branches: the left anterior descending (LAD) artery and the left circumflex (LCx) artery. The LAD supplies blood to the front and sides of the heart, while the LCx supplies blood to the back and sides of the heart. The right coronary artery supplies blood to the lower part of the heart, including the right ventricle and the bottom portion of the left ventricle.
The veins that drain the heart muscle include the great cardiac vein, the middle cardiac vein, and the small cardiac vein, which merge to form the coronary sinus. The coronary sinus empties into the right atrium, allowing deoxygenated blood to enter the right side of the heart and be pumped to the lungs for oxygenation.
Coronary circulation is essential for maintaining the health and function of the heart muscle, as it provides the necessary oxygen and nutrients required for proper contraction and relaxation of the myocardium. Any disruption or blockage in the coronary circulation system can lead to serious consequences, such as angina, heart attack, or even death.
Coronary artery disease, often simply referred to as coronary disease, is a condition in which the blood vessels that supply oxygen-rich blood to the heart become narrowed or blocked due to the buildup of fatty deposits called plaques. This can lead to chest pain (angina), shortness of breath, or in severe cases, a heart attack.
The medical definition of coronary artery disease is:
A condition characterized by the accumulation of atheromatous plaques in the walls of the coronary arteries, leading to decreased blood flow and oxygen supply to the myocardium (heart muscle). This can result in symptoms such as angina pectoris, shortness of breath, or arrhythmias, and may ultimately lead to myocardial infarction (heart attack) or heart failure.
Risk factors for coronary artery disease include age, smoking, high blood pressure, high cholesterol, diabetes, obesity, physical inactivity, and a family history of the condition. Lifestyle changes such as quitting smoking, exercising regularly, eating a healthy diet, and managing stress can help reduce the risk of developing coronary artery disease. Medical treatments may include medications to control blood pressure, cholesterol levels, or irregular heart rhythms, as well as procedures such as angioplasty or bypass surgery to improve blood flow to the heart.
Electrocardiography (ECG or EKG) is a medical procedure that records the electrical activity of the heart. It provides a graphic representation of the electrical changes that occur during each heartbeat. The resulting tracing, called an electrocardiogram, can reveal information about the heart's rate and rhythm, as well as any damage to its cells or abnormalities in its conduction system.
During an ECG, small electrodes are placed on the skin of the chest, arms, and legs. These electrodes detect the electrical signals produced by the heart and transmit them to a machine that amplifies and records them. The procedure is non-invasive, painless, and quick, usually taking only a few minutes.
ECGs are commonly used to diagnose and monitor various heart conditions, including arrhythmias, coronary artery disease, heart attacks, and electrolyte imbalances. They can also be used to evaluate the effectiveness of certain medications or treatments.
Reperfusion injury is a complex pathophysiological process that occurs when blood flow is restored to previously ischemic tissues, leading to further tissue damage. This phenomenon can occur in various clinical settings such as myocardial infarction (heart attack), stroke, or peripheral artery disease after an intervention aimed at restoring perfusion.
The restoration of blood flow leads to the generation of reactive oxygen species (ROS) and inflammatory mediators, which can cause oxidative stress, cellular damage, and activation of the immune system. This results in a cascade of events that may lead to microvascular dysfunction, capillary leakage, and tissue edema, further exacerbating the injury.
Reperfusion injury is an important consideration in the management of ischemic events, as interventions aimed at restoring blood flow must be carefully balanced with potential harm from reperfusion injury. Strategies to mitigate reperfusion injury include ischemic preconditioning (exposing the tissue to short periods of ischemia before a prolonged ischemic event), ischemic postconditioning (applying brief periods of ischemia and reperfusion after restoring blood flow), remote ischemic preconditioning (ischemia applied to a distant organ or tissue to protect the target organ), and pharmacological interventions that scavenge ROS, reduce inflammation, or improve microvascular function.
An exercise test, also known as a stress test or an exercise stress test, is a medical procedure used to evaluate the heart's function and response to physical exertion. It typically involves walking on a treadmill or pedaling a stationary bike while being monitored for changes in heart rate, blood pressure, electrocardiogram (ECG), and sometimes other variables such as oxygen consumption or gas exchange.
During the test, the patient's symptoms, such as chest pain or shortness of breath, are also closely monitored. The exercise test can help diagnose coronary artery disease, assess the severity of heart-related symptoms, and evaluate the effectiveness of treatments for heart conditions. It may also be used to determine a person's safe level of physical activity and fitness.
There are different types of exercise tests, including treadmill stress testing, stationary bike stress testing, nuclear stress testing, and stress echocardiography. The specific type of test used depends on the patient's medical history, symptoms, and overall health status.
Myocardial infarction (MI), also known as a heart attack, is a medical condition characterized by the death of a segment of heart muscle (myocardium) due to the interruption of its blood supply. This interruption is most commonly caused by the blockage of a coronary artery by a blood clot formed on the top of an atherosclerotic plaque, which is a buildup of cholesterol and other substances in the inner lining of the artery.
The lack of oxygen and nutrients supply to the heart muscle tissue results in damage or death of the cardiac cells, causing the affected area to become necrotic. The extent and severity of the MI depend on the size of the affected area, the duration of the occlusion, and the presence of collateral circulation.
Symptoms of a myocardial infarction may include chest pain or discomfort, shortness of breath, nausea, lightheadedness, and sweating. Immediate medical attention is necessary to restore blood flow to the affected area and prevent further damage to the heart muscle. Treatment options for MI include medications, such as thrombolytics, antiplatelet agents, and pain relievers, as well as procedures such as percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG).
Myocardial reperfusion is the restoration of blood flow to the heart muscle (myocardium), usually after a period of ischemia or reduced oxygen supply, such as during a myocardial infarction (heart attack). This can be achieved through various medical interventions, including thrombolytic therapy, percutaneous coronary intervention (PCI), or coronary artery bypass surgery (CABG). The goal of myocardial reperfusion is to salvage the jeopardized myocardium, preserve cardiac function, and reduce the risk of complications like heart failure or arrhythmias. However, it's important to note that while reperfusion is crucial for treating ischemic heart disease, it can also lead to additional injury to the heart muscle, known as reperfusion injury.
In medical terms, the heart is a muscular organ located in the thoracic cavity that functions as a pump to circulate blood throughout the body. It's responsible for delivering oxygen and nutrients to the tissues and removing carbon dioxide and other wastes. The human heart is divided into four chambers: two atria on the top and two ventricles on the bottom. The right side of the heart receives deoxygenated blood from the body and pumps it to the lungs, while the left side receives oxygenated blood from the lungs and pumps it out to the rest of the body. The heart's rhythmic contractions and relaxations are regulated by a complex electrical conduction system.
Angina pectoris is a medical term that describes chest pain or discomfort caused by an inadequate supply of oxygen-rich blood to the heart muscle. This condition often occurs due to coronary artery disease, where the coronary arteries become narrowed or blocked by the buildup of cholesterol, fatty deposits, and other substances, known as plaques. These blockages can reduce blood flow to the heart, causing ischemia (lack of oxygen) and leading to angina symptoms.
There are two primary types of angina: stable and unstable. Stable angina is predictable and usually occurs during physical exertion or emotional stress when the heart needs more oxygen-rich blood. The pain typically subsides with rest or after taking prescribed nitroglycerin medication, which helps widen the blood vessels and improve blood flow to the heart.
Unstable angina, on the other hand, is more severe and unpredictable. It can occur at rest, during sleep, or with minimal physical activity and may not be relieved by rest or nitroglycerin. Unstable angina is considered a medical emergency, as it could indicate an imminent heart attack.
Symptoms of angina pectoris include chest pain, pressure, tightness, or heaviness that typically radiates to the left arm, neck, jaw, or back. Shortness of breath, nausea, sweating, and fatigue may also accompany angina symptoms. Immediate medical attention is necessary if you experience chest pain or discomfort, especially if it's new, severe, or persistent, as it could be a sign of a more serious condition like a heart attack.
Cardiotonic agents are a type of medication that have a positive inotropic effect on the heart, meaning they help to improve the contractility and strength of heart muscle contractions. These medications are often used to treat heart failure, as they can help to improve the efficiency of the heart's pumping ability and increase cardiac output.
Cardiotonic agents work by increasing the levels of calcium ions inside heart muscle cells during each heartbeat, which in turn enhances the force of contraction. Some common examples of cardiotonic agents include digitalis glycosides (such as digoxin), which are derived from the foxglove plant, and synthetic medications such as dobutamine and milrinone.
While cardiotonic agents can be effective in improving heart function, they can also have potentially serious side effects, including arrhythmias, electrolyte imbalances, and digestive symptoms. As a result, they are typically used under close medical supervision and their dosages may need to be carefully monitored to minimize the risk of adverse effects.
Ischemic preconditioning, myocardial is a phenomenon in cardiac physiology where the heart muscle (myocardium) is made more resistant to the damaging effects of a prolonged period of reduced blood flow (ischemia) or oxygen deprivation (hypoxia), followed by reperfusion (restoration of blood flow). This resistance is developed through a series of brief, controlled episodes of ischemia and reperfusion, which act as "preconditioning" stimuli, protecting the myocardium from subsequent more severe ischemic events. The adaptive responses triggered during preconditioning include the activation of various protective signaling pathways, release of protective factors, and modulation of cellular metabolism, ultimately leading to reduced infarct size, improved contractile function, and attenuated reperfusion injury in the myocardium.
Hemodynamics is the study of how blood flows through the cardiovascular system, including the heart and the vascular network. It examines various factors that affect blood flow, such as blood volume, viscosity, vessel length and diameter, and pressure differences between different parts of the circulatory system. Hemodynamics also considers the impact of various physiological and pathological conditions on these variables, and how they in turn influence the function of vital organs and systems in the body. It is a critical area of study in fields such as cardiology, anesthesiology, and critical care medicine.
I believe there might be a misunderstanding in your question. "Dogs" is not a medical term or condition. It is the common name for a domesticated carnivore of the family Canidae, specifically the genus Canis, which includes wolves, foxes, and other extant and extinct species of mammals. Dogs are often kept as pets and companions, and they have been bred in a wide variety of forms and sizes for different purposes, such as hunting, herding, guarding, assisting police and military forces, and providing companionship and emotional support.
If you meant to ask about a specific medical condition or term related to dogs, please provide more context so I can give you an accurate answer.
Ambulatory electrocardiography, also known as ambulatory ECG or Holter monitoring, is a non-invasive method of recording the electrical activity of the heart over an extended period of time (typically 24 hours or more) while the patient goes about their daily activities. The device used to record the ECG is called a Holter monitor, which consists of a small, portable recorder that is attached to the patient's chest with electrodes.
The recorded data provides information on any abnormalities in the heart's rhythm or electrical activity during different stages of activity and rest, allowing healthcare providers to diagnose and evaluate various cardiac conditions such as arrhythmias, ischemia, and infarction. The ability to monitor the heart's activity over an extended period while the patient performs their normal activities provides valuable information that may not be captured during a standard ECG, which only records the heart's electrical activity for a few seconds.
In summary, ambulatory electrocardiography is a diagnostic tool used to evaluate the electrical activity of the heart over an extended period, allowing healthcare providers to diagnose and manage various cardiac conditions.
Coronary vessels refer to the network of blood vessels that supply oxygenated blood and nutrients to the heart muscle, also known as the myocardium. The two main coronary arteries are the left main coronary artery and the right coronary artery.
The left main coronary artery branches off into the left anterior descending artery (LAD) and the left circumflex artery (LCx). The LAD supplies blood to the front of the heart, while the LCx supplies blood to the side and back of the heart.
The right coronary artery supplies blood to the right lower part of the heart, including the right atrium and ventricle, as well as the back of the heart.
Coronary vessel disease (CVD) occurs when these vessels become narrowed or blocked due to the buildup of plaque, leading to reduced blood flow to the heart muscle. This can result in chest pain, shortness of breath, or a heart attack.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
Animal disease models are specialized animals, typically rodents such as mice or rats, that have been genetically engineered or exposed to certain conditions to develop symptoms and physiological changes similar to those seen in human diseases. These models are used in medical research to study the pathophysiology of diseases, identify potential therapeutic targets, test drug efficacy and safety, and understand disease mechanisms.
The genetic modifications can include knockout or knock-in mutations, transgenic expression of specific genes, or RNA interference techniques. The animals may also be exposed to environmental factors such as chemicals, radiation, or infectious agents to induce the disease state.
Examples of animal disease models include:
1. Mouse models of cancer: Genetically engineered mice that develop various types of tumors, allowing researchers to study cancer initiation, progression, and metastasis.
2. Alzheimer's disease models: Transgenic mice expressing mutant human genes associated with Alzheimer's disease, which exhibit amyloid plaque formation and cognitive decline.
3. Diabetes models: Obese and diabetic mouse strains like the NOD (non-obese diabetic) or db/db mice, used to study the development of type 1 and type 2 diabetes, respectively.
4. Cardiovascular disease models: Atherosclerosis-prone mice, such as ApoE-deficient or LDLR-deficient mice, that develop plaque buildup in their arteries when fed a high-fat diet.
5. Inflammatory bowel disease models: Mice with genetic mutations affecting intestinal barrier function and immune response, such as IL-10 knockout or SAMP1/YitFc mice, which develop colitis.
Animal disease models are essential tools in preclinical research, but it is important to recognize their limitations. Differences between species can affect the translatability of results from animal studies to human patients. Therefore, researchers must carefully consider the choice of model and interpret findings cautiously when applying them to human diseases.
Heart rate is the number of heartbeats per unit of time, often expressed as beats per minute (bpm). It can vary significantly depending on factors such as age, physical fitness, emotions, and overall health status. A resting heart rate between 60-100 bpm is generally considered normal for adults, but athletes and individuals with high levels of physical fitness may have a resting heart rate below 60 bpm due to their enhanced cardiovascular efficiency. Monitoring heart rate can provide valuable insights into an individual's health status, exercise intensity, and response to various treatments or interventions.
Coronary angiography is a medical procedure that uses X-ray imaging to visualize the coronary arteries, which supply blood to the heart muscle. During the procedure, a thin, flexible catheter is inserted into an artery in the arm or groin and threaded through the blood vessels to the heart. A contrast dye is then injected through the catheter, and X-ray images are taken as the dye flows through the coronary arteries. These images can help doctors diagnose and treat various heart conditions, such as blockages or narrowing of the arteries, that can lead to chest pain or heart attacks. It is also known as coronary arteriography or cardiac catheterization.
Emission-Computed Tomography, Single-Photon (SPECT) is a type of nuclear medicine imaging procedure that generates detailed, three-dimensional images of the distribution of radioactive pharmaceuticals within the body. It uses gamma rays emitted by a radiopharmaceutical that is introduced into the patient's body, and a specialized gamma camera to detect these gamma rays and create tomographic images. The data obtained from the SPECT imaging can be used to diagnose various medical conditions, evaluate organ function, and guide treatment decisions. It is commonly used to image the heart, brain, and bones, among other organs and systems.
Myocardial contraction refers to the rhythmic and forceful shortening of heart muscle cells (myocytes) in the myocardium, which is the muscular wall of the heart. This process is initiated by electrical signals generated by the sinoatrial node, causing a wave of depolarization that spreads throughout the heart.
During myocardial contraction, calcium ions flow into the myocytes, triggering the interaction between actin and myosin filaments, which are the contractile proteins in the muscle cells. This interaction causes the myofilaments to slide past each other, resulting in the shortening of the sarcomeres (the functional units of muscle contraction) and ultimately leading to the contraction of the heart muscle.
Myocardial contraction is essential for pumping blood throughout the body and maintaining adequate circulation to vital organs. Any impairment in myocardial contractility can lead to various cardiac disorders, such as heart failure, cardiomyopathy, and arrhythmias.
Cardiac arrhythmias are abnormal heart rhythms that result from disturbances in the electrical conduction system of the heart. The heart's normal rhythm is controlled by an electrical signal that originates in the sinoatrial (SA) node, located in the right atrium. This signal travels through the atrioventricular (AV) node and into the ventricles, causing them to contract and pump blood throughout the body.
An arrhythmia occurs when there is a disruption in this electrical pathway or when the heart's natural pacemaker produces an abnormal rhythm. This can cause the heart to beat too fast (tachycardia), too slow (bradycardia), or irregularly.
There are several types of cardiac arrhythmias, including:
1. Atrial fibrillation: A rapid and irregular heartbeat that starts in the atria (the upper chambers of the heart).
2. Atrial flutter: A rapid but regular heartbeat that starts in the atria.
3. Supraventricular tachycardia (SVT): A rapid heartbeat that starts above the ventricles, usually in the atria or AV node.
4. Ventricular tachycardia: A rapid and potentially life-threatening heart rhythm that originates in the ventricles.
5. Ventricular fibrillation: A chaotic and disorganized electrical activity in the ventricles, which can be fatal if not treated immediately.
6. Heart block: A delay or interruption in the conduction of electrical signals from the atria to the ventricles.
Cardiac arrhythmias can cause various symptoms, such as palpitations, dizziness, shortness of breath, chest pain, and fatigue. In some cases, they may not cause any symptoms and go unnoticed. However, if left untreated, certain types of arrhythmias can lead to serious complications, including stroke, heart failure, or even sudden cardiac death.
Treatment for cardiac arrhythmias depends on the type, severity, and underlying causes. Options may include lifestyle changes, medications, cardioversion (electrical shock therapy), catheter ablation, implantable devices such as pacemakers or defibrillators, and surgery. It is essential to consult a healthcare professional for proper evaluation and management of cardiac arrhythmias.
Reperfusion, in medical terms, refers to the restoration of blood flow to tissues or organs that have been deprived of adequate oxygen supply, usually as a result of ischemia (lack of blood flow). This process is often initiated through therapeutic interventions such as thrombolysis (breaking up blood clots), angioplasty (opening narrowed or blocked blood vessels using a balloon or stent), or surgical procedures.
Reperfusion aims to salvage the affected tissues and prevent further damage; however, it can also lead to reperfusion injury. This injury occurs when the return of oxygen-rich blood to previously ischemic tissues results in the overproduction of free radicals and inflammatory mediators, which can cause additional cellular damage and organ dysfunction.
Managing reperfusion injury involves using various strategies such as antioxidants, anti-inflammatory agents, and other protective treatments to minimize its negative impact on the recovering tissues or organs.
Sprague-Dawley rats are a strain of albino laboratory rats that are widely used in scientific research. They were first developed by researchers H.H. Sprague and R.C. Dawley in the early 20th century, and have since become one of the most commonly used rat strains in biomedical research due to their relatively large size, ease of handling, and consistent genetic background.
Sprague-Dawley rats are outbred, which means that they are genetically diverse and do not suffer from the same limitations as inbred strains, which can have reduced fertility and increased susceptibility to certain diseases. They are also characterized by their docile nature and low levels of aggression, making them easier to handle and study than some other rat strains.
These rats are used in a wide variety of research areas, including toxicology, pharmacology, nutrition, cancer, and behavioral studies. Because they are genetically diverse, Sprague-Dawley rats can be used to model a range of human diseases and conditions, making them an important tool in the development of new drugs and therapies.
Myocardial perfusion imaging (MPI) is a non-invasive nuclear medicine test used to assess the blood flow to the heart muscle (myocardium). It typically involves the injection of a radioactive tracer, such as thallium-201 or technetium-99m sestamibi, into a vein. The tracer is taken up by healthy heart muscle in proportion to blood flow. A special camera then takes images of the distribution of the tracer within the heart, providing information about areas of reduced or blocked blood flow (ischemia) or scarred tissue (infarction). MPI can help diagnose coronary artery disease, assess the effectiveness of treatments, and determine prognosis.
Left ventricular function refers to the ability of the left ventricle (the heart's lower-left chamber) to contract and relax, thereby filling with and ejecting blood. The left ventricle is responsible for pumping oxygenated blood to the rest of the body. Its function is evaluated by measuring several parameters, including:
1. Ejection fraction (EF): This is the percentage of blood that is pumped out of the left ventricle with each heartbeat. A normal ejection fraction ranges from 55% to 70%.
2. Stroke volume (SV): The amount of blood pumped by the left ventricle in one contraction. A typical SV is about 70 mL/beat.
3. Cardiac output (CO): The total volume of blood that the left ventricle pumps per minute, calculated as the product of stroke volume and heart rate. Normal CO ranges from 4 to 8 L/minute.
Assessment of left ventricular function is crucial in diagnosing and monitoring various cardiovascular conditions such as heart failure, coronary artery disease, valvular heart diseases, and cardiomyopathies.
Creatine kinase (CK) is a muscle enzyme that is normally present in small amounts in the blood. It is primarily found in tissues that require a lot of energy, such as the heart, brain, and skeletal muscles. When these tissues are damaged or injured, CK is released into the bloodstream, causing the levels to rise.
Creatine kinase exists in several forms, known as isoenzymes, which can be measured in the blood to help identify the location of tissue damage. The three main isoenzymes are:
1. CK-MM: Found primarily in skeletal muscle
2. CK-MB: Found primarily in heart muscle
3. CK-BB: Found primarily in the brain
Elevated levels of creatine kinase, particularly CK-MB, can indicate damage to the heart muscle, such as occurs with a heart attack. Similarly, elevated levels of CK-BB may suggest brain injury or disease. Overall, measuring creatine kinase levels is a useful diagnostic tool for assessing tissue damage and determining the severity of injuries or illnesses.
Ischemic preconditioning is a phenomenon in which brief, non-lethal episodes of ischemia (restriction or interruption of blood supply to an organ or tissue) render the tissue more resistant to subsequent prolonged ischemia and reperfusion injury. This adaptive response involves a complex series of cellular and molecular changes that protect the myocardium, brain, kidney, or other organs from ischemic damage. The underlying mechanisms include the activation of various signaling pathways, such as adenosine, opioid, and kinase pathways, which lead to the production of protective factors and the modulation of cellular responses to ischemia and reperfusion injury. Ischemic preconditioning has been extensively studied in the context of cardiovascular medicine, where it has been shown to reduce infarct size and improve cardiac function after myocardial infarction. However, this protective phenomenon has also been observed in other organs and systems, including the brain, kidney, liver, and skeletal muscle.
A Transient Ischemic Attack (TIA), also known as a "mini-stroke," is a temporary period of symptoms similar to those you'd get if you were having a stroke. A TIA doesn't cause permanent damage and is often caused by a temporary decrease in blood supply to part of your brain, which may last as little as five minutes.
Like an ischemic stroke, a TIA occurs when a clot or debris blocks blood flow to part of your nervous system. However, unlike a stroke, a TIA doesn't leave lasting damage because the blockage is temporary.
Symptoms of a TIA can include sudden onset of weakness, numbness or paralysis in your face, arm or leg, typically on one side of your body. You could also experience slurred or garbled speech, or difficulty understanding others. Other symptoms can include blindness in one or both eyes, dizziness, or a severe headache with no known cause.
Even though TIAs usually last only a few minutes, they are a serious condition and should not be ignored. If you suspect you or someone else is experiencing a TIA, seek immediate medical attention. TIAs can be a warning sign that a full-blown stroke is imminent.
"Wistar rats" are a strain of albino rats that are widely used in laboratory research. They were developed at the Wistar Institute in Philadelphia, USA, and were first introduced in 1906. Wistar rats are outbred, which means that they are genetically diverse and do not have a fixed set of genetic characteristics like inbred strains.
Wistar rats are commonly used as animal models in biomedical research because of their size, ease of handling, and relatively low cost. They are used in a wide range of research areas, including toxicology, pharmacology, nutrition, cancer, cardiovascular disease, and behavioral studies. Wistar rats are also used in safety testing of drugs, medical devices, and other products.
Wistar rats are typically larger than many other rat strains, with males weighing between 500-700 grams and females weighing between 250-350 grams. They have a lifespan of approximately 2-3 years. Wistar rats are also known for their docile and friendly nature, making them easy to handle and work with in the laboratory setting.
Warm ischemia, also known as warm injury or warm hypoxia, refers to the damage that occurs to tissues when there is an inadequate blood supply at body temperature. This can happen during surgical procedures, trauma, or other medical conditions that restrict blood flow to a specific area of the body. The lack of oxygen and nutrients, combined with the buildup of waste products, can cause cells to become damaged or die, leading to tissue dysfunction or failure.
The term "warm" is used to distinguish this type of ischemia from cold ischemia, which occurs when tissues are cooled and blood flow is restricted. Cold ischemia is often used in organ transplantation to preserve the organ until it can be transplanted. Warm ischemia is generally more damaging to tissues than cold ischemia because the metabolic demands of the cells are not being met, leading to a more rapid onset of cellular damage.
The severity and duration of warm ischemia can affect the extent of tissue damage and the likelihood of recovery. In some cases, warm ischemia may be reversible if blood flow is restored quickly enough, but in other cases it may lead to permanent tissue damage or loss of function. Treatment for warm ischemia typically involves restoring blood flow to the affected area as soon as possible, along with supportive care to manage any complications that may arise.
Dipyridamole is a medication that belongs to a class of drugs called antiplatelet agents. It works by preventing platelets in your blood from sticking together to form clots. Dipyridamole is often used in combination with aspirin to prevent stroke and other complications in people who have had a heart valve replacement or a type of irregular heartbeat called atrial fibrillation.
Dipyridamole can also be used as a stress agent in myocardial perfusion imaging studies, which are tests used to evaluate blood flow to the heart. When used for this purpose, dipyridamole is given intravenously and works by dilating the blood vessels in the heart, allowing more blood to flow through them and making it easier to detect areas of reduced blood flow.
The most common side effects of dipyridamole include headache, dizziness, and gastrointestinal symptoms such as diarrhea, nausea, and vomiting. In rare cases, dipyridamole can cause more serious side effects, such as allergic reactions, abnormal heart rhythms, or low blood pressure. It is important to take dipyridamole exactly as directed by your healthcare provider and to report any unusual symptoms or side effects promptly.
Myocardial stunning is a condition in cardiovascular medicine where the heart muscle (myocardium) temporarily loses its ability to contract effectively after being exposed to a brief, severe episode of ischemia (restriction of blood supply) or reperfusion injury (damage that occurs when blood flow is restored to an organ or tissue after a period of ischemia). This results in a reduction in the heart's pumping function, which can be detected using imaging techniques such as echocardiography.
The stunning phenomenon is believed to be caused by complex biochemical and cellular processes that occur during ischemia-reperfusion injury, including the generation of free radicals, calcium overload, inflammation, and activation of various signaling pathways. These changes can lead to the dysfunction of contractile proteins, mitochondrial damage, and altered gene expression in cardiomyocytes (heart muscle cells).
Myocardial stunning is often observed following procedures such as coronary angioplasty or bypass surgery, where blood flow is temporarily interrupted and then restored to the heart. It can also occur during episodes of unstable angina, acute myocardial infarction, or cardiac arrest. Although the stunning itself is usually reversible within a few days to several weeks, it may contribute to short-term hemodynamic instability and increased risk of adverse events such as heart failure, arrhythmias, or even death.
Management of myocardial stunning typically involves supportive care, optimizing hemodynamics, and addressing any underlying conditions that may have contributed to the ischemic episode. In some cases, medications like inotropes or vasopressors might be used to support cardiac function temporarily. Preventive strategies, such as maintaining adequate blood pressure, heart rate, and oxygenation during procedures, can help reduce the risk of myocardial stunning.
Perfusion, in medical terms, refers to the process of circulating blood through the body's organs and tissues to deliver oxygen and nutrients and remove waste products. It is a measure of the delivery of adequate blood flow to specific areas or tissues in the body. Perfusion can be assessed using various methods, including imaging techniques like computed tomography (CT) scans, magnetic resonance imaging (MRI), and perfusion scintigraphy.
Perfusion is critical for maintaining proper organ function and overall health. When perfusion is impaired or inadequate, it can lead to tissue hypoxia, acidosis, and cell death, which can result in organ dysfunction or failure. Conditions that can affect perfusion include cardiovascular disease, shock, trauma, and certain surgical procedures.
Blood pressure is the force exerted by circulating blood on the walls of the blood vessels. It is measured in millimeters of mercury (mmHg) and is given as two figures:
1. Systolic pressure: This is the pressure when the heart pushes blood out into the arteries.
2. Diastolic pressure: This is the pressure when the heart rests between beats, allowing it to fill with blood.
Normal blood pressure for adults is typically around 120/80 mmHg, although this can vary slightly depending on age, sex, and other factors. High blood pressure (hypertension) is generally considered to be a reading of 130/80 mmHg or higher, while low blood pressure (hypotension) is usually defined as a reading below 90/60 mmHg. It's important to note that blood pressure can fluctuate throughout the day and may be affected by factors such as stress, physical activity, and medication use.
Thallium radioisotopes are radioactive isotopes or variants of the element thallium (Tl), which decays and emits radiation. Thallium has several radioisotopes, with the most commonly used being thallium-201 (^201Tl). This radioisotope is used in medical imaging, specifically in myocardial perfusion scintigraphy, to evaluate blood flow to the heart muscle. It decays by electron capture and emits gamma radiation with a half-life of 73 hours, making it suitable for diagnostic procedures.
It's important to note that handling and using radioisotopes require proper training and safety measures due to their ionizing radiation properties.
Adenosine is a purine nucleoside that is composed of a sugar (ribose) and the base adenine. It plays several important roles in the body, including serving as a precursor for the synthesis of other molecules such as ATP, NAD+, and RNA.
In the medical context, adenosine is perhaps best known for its use as a pharmaceutical agent to treat certain cardiac arrhythmias. When administered intravenously, it can help restore normal sinus rhythm in patients with paroxysmal supraventricular tachycardia (PSVT) by slowing conduction through the atrioventricular node and interrupting the reentry circuit responsible for the arrhythmia.
Adenosine can also be used as a diagnostic tool to help differentiate between narrow-complex tachycardias of supraventricular origin and those that originate from below the ventricles (such as ventricular tachycardia). This is because adenosine will typically terminate PSVT but not affect the rhythm of VT.
It's worth noting that adenosine has a very short half-life, lasting only a few seconds in the bloodstream. This means that its effects are rapidly reversible and generally well-tolerated, although some patients may experience transient symptoms such as flushing, chest pain, or shortness of breath.
Coronary artery disease (CAD) is a medical condition in which the coronary arteries, which supply oxygen-rich blood to the heart muscle, become narrowed or blocked due to the buildup of cholesterol, fatty deposits, and other substances, known as plaque. Over time, this buildup can cause the arteries to harden and narrow (a process called atherosclerosis), reducing blood flow to the heart muscle.
The reduction in blood flow can lead to various symptoms and complications, including:
1. Angina (chest pain or discomfort) - This occurs when the heart muscle doesn't receive enough oxygen-rich blood, causing pain, pressure, or discomfort in the chest, arms, neck, jaw, or back.
2. Shortness of breath - When the heart isn't receiving adequate blood flow, it can't pump blood efficiently to meet the body's demands, leading to shortness of breath during physical activities or at rest.
3. Heart attack - If a piece of plaque ruptures or breaks off in a coronary artery, a blood clot can form and block the artery, causing a heart attack (myocardial infarction). This can damage or destroy part of the heart muscle.
4. Heart failure - Chronic reduced blood flow to the heart muscle can weaken it over time, leading to heart failure, a condition in which the heart can't pump blood efficiently to meet the body's needs.
5. Arrhythmias - Reduced blood flow and damage to the heart muscle can lead to abnormal heart rhythms (arrhythmias), which can be life-threatening if not treated promptly.
Coronary artery disease is typically diagnosed through a combination of medical history, physical examination, and diagnostic tests such as electrocardiograms (ECGs), stress testing, cardiac catheterization, and imaging studies like coronary computed tomography angiography (CCTA). Treatment options for CAD include lifestyle modifications, medications, medical procedures, and surgery.
Collateral circulation refers to the alternate blood supply routes that bypass an obstructed or narrowed vessel and reconnect with the main vascular system. These collateral vessels can develop over time as a result of the body's natural adaptation to chronic ischemia (reduced blood flow) caused by various conditions such as atherosclerosis, thromboembolism, or vasculitis.
The development of collateral circulation helps maintain adequate blood flow and oxygenation to affected tissues, minimizing the risk of tissue damage and necrosis. In some cases, well-developed collateral circulations can help compensate for significant blockages in major vessels, reducing symptoms and potentially preventing the need for invasive interventions like revascularization procedures. However, the extent and effectiveness of collateral circulation vary from person to person and depend on factors such as age, overall health status, and the presence of comorbidities.
Dobutamine is a synthetic catecholamine used in medical treatment, specifically as a positive inotrope and vasodilator. It works by stimulating the beta-1 adrenergic receptors of the heart, thereby increasing its contractility and stroke volume. This results in an improved cardiac output, making dobutamine beneficial in treating heart failure, cardiogenic shock, and other conditions where heart function is compromised.
It's important to note that dobutamine should be administered under strict medical supervision due to its potential to cause adverse effects such as arrhythmias, hypotension, or hypertension. The dosage, frequency, and duration of administration are determined by the patient's specific condition and response to treatment.
Cardiac myocytes are the muscle cells that make up the heart muscle, also known as the myocardium. These specialized cells are responsible for contracting and relaxing in a coordinated manner to pump blood throughout the body. They differ from skeletal muscle cells in several ways, including their ability to generate their own electrical impulses, which allows the heart to function as an independent rhythmical pump. Cardiac myocytes contain sarcomeres, the contractile units of the muscle, and are connected to each other by intercalated discs that help coordinate contraction and ensure the synchronous beating of the heart.
"Swine" is a common term used to refer to even-toed ungulates of the family Suidae, including domestic pigs and wild boars. However, in a medical context, "swine" often appears in the phrase "swine flu," which is a strain of influenza virus that typically infects pigs but can also cause illness in humans. The 2009 H1N1 pandemic was caused by a new strain of swine-origin influenza A virus, which was commonly referred to as "swine flu." It's important to note that this virus is not transmitted through eating cooked pork products; it spreads from person to person, mainly through respiratory droplets produced when an infected person coughs or sneezes.
Intraoperative complications refer to any unforeseen problems or events that occur during the course of a surgical procedure, once it has begun and before it is completed. These complications can range from minor issues, such as bleeding or an adverse reaction to anesthesia, to major complications that can significantly impact the patient's health and prognosis.
Examples of intraoperative complications include:
1. Bleeding (hemorrhage) - This can occur due to various reasons such as injury to blood vessels or organs during surgery.
2. Infection - Surgical site infections can develop if the surgical area becomes contaminated during the procedure.
3. Anesthesia-related complications - These include adverse reactions to anesthesia, difficulty maintaining the patient's airway, or cardiovascular instability.
4. Organ injury - Accidental damage to surrounding organs can occur during surgery, leading to potential long-term consequences.
5. Equipment failure - Malfunctioning surgical equipment can lead to complications and compromise the safety of the procedure.
6. Allergic reactions - Patients may have allergies to certain medications or materials used during surgery, causing an adverse reaction.
7. Prolonged operative time - Complications may arise if a surgical procedure takes longer than expected, leading to increased risk of infection and other issues.
Intraoperative complications require prompt identification and management by the surgical team to minimize their impact on the patient's health and recovery.
Vasodilator agents are pharmacological substances that cause the relaxation or widening of blood vessels by relaxing the smooth muscle in the vessel walls. This results in an increase in the diameter of the blood vessels, which decreases vascular resistance and ultimately reduces blood pressure. Vasodilators can be further classified based on their site of action:
1. Systemic vasodilators: These agents cause a generalized relaxation of the smooth muscle in the walls of both arteries and veins, resulting in a decrease in peripheral vascular resistance and preload (the volume of blood returning to the heart). Examples include nitroglycerin, hydralazine, and calcium channel blockers.
2. Arterial vasodilators: These agents primarily affect the smooth muscle in arterial vessel walls, leading to a reduction in afterload (the pressure against which the heart pumps blood). Examples include angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), and direct vasodilators like sodium nitroprusside.
3. Venous vasodilators: These agents primarily affect the smooth muscle in venous vessel walls, increasing venous capacitance and reducing preload. Examples include nitroglycerin and other organic nitrates.
Vasodilator agents are used to treat various cardiovascular conditions such as hypertension, heart failure, angina, and pulmonary arterial hypertension. It is essential to monitor their use carefully, as excessive vasodilation can lead to orthostatic hypotension, reflex tachycardia, or fluid retention.
Chest pain is a discomfort or pain that you feel in the chest area. The pain can be sharp, dull, burning, crushing, heaviness, or tightness. It may be accompanied by other symptoms such as shortness of breath, sweating, nausea, dizziness, or pain that radiates to the arm, neck, jaw, or back.
Chest pain can have many possible causes, including heart-related conditions such as angina or a heart attack, lung conditions such as pneumonia or pleurisy, gastrointestinal problems such as acid reflux or gastritis, musculoskeletal issues such as costochondritis or muscle strain, and anxiety or panic attacks.
It is important to seek immediate medical attention if you experience chest pain that is severe, persistent, or accompanied by other concerning symptoms, as it may be a sign of a serious medical condition. A healthcare professional can evaluate your symptoms, perform tests, and provide appropriate treatment.
Echocardiography is a medical procedure that uses sound waves to produce detailed images of the heart's structure, function, and motion. It is a non-invasive test that can help diagnose various heart conditions, such as valve problems, heart muscle damage, blood clots, and congenital heart defects.
During an echocardiogram, a transducer (a device that sends and receives sound waves) is placed on the chest or passed through the esophagus to obtain images of the heart. The sound waves produced by the transducer bounce off the heart structures and return to the transducer, which then converts them into electrical signals that are processed to create images of the heart.
There are several types of echocardiograms, including:
* Transthoracic echocardiography (TTE): This is the most common type of echocardiogram and involves placing the transducer on the chest.
* Transesophageal echocardiography (TEE): This type of echocardiogram involves passing a specialized transducer through the esophagus to obtain images of the heart from a closer proximity.
* Stress echocardiography: This type of echocardiogram is performed during exercise or medication-induced stress to assess how the heart functions under stress.
* Doppler echocardiography: This type of echocardiogram uses sound waves to measure blood flow and velocity in the heart and blood vessels.
Echocardiography is a valuable tool for diagnosing and managing various heart conditions, as it provides detailed information about the structure and function of the heart. It is generally safe, non-invasive, and painless, making it a popular choice for doctors and patients alike.
Cold ischemia is a medical term that refers to the loss of blood flow and subsequent lack of oxygen delivery to an organ or tissue, which is then cooled and stored in a solution at temperatures between 0-4°C (32-39°F) for the purpose of transplantation. The term "cold" indicates the temperature range, while "ischemia" refers to the lack of blood flow and oxygen delivery to the tissue.
During cold ischemia, the metabolic activity of the organ or tissue slows down significantly, which helps to reduce the rate of cellular damage that would otherwise occur due to the absence of oxygen and nutrients. However, even with cold storage, there is still some degree of injury to the organ or tissue, and this can affect its function after transplantation.
The duration of cold ischemia time is an important factor in determining the success of a transplant procedure. Prolonged cold ischemia times are associated with increased risk of poor organ function and rejection, as well as decreased graft survival rates. Therefore, it is essential to minimize the cold ischemia time as much as possible during organ transplantation to ensure optimal outcomes for the recipient.
Stress echocardiography is a medical test that uses ultrasound imaging to assess how well your heart muscles are pumping blood and how well they respond to stress. It can help diagnose and evaluate coronary artery disease, valvular heart disease, and other cardiac conditions.
During the test, you will be asked to exercise on a treadmill or stationary bike while your heart rate and blood pressure are monitored. At peak exercise, a healthcare professional will take ultrasound images of your heart to evaluate its structure and function. If you are unable to exercise, medication may be given to simulate the effects of exercise on your heart.
The test can help identify areas of your heart that aren't receiving enough oxygen-rich blood due to blocked or narrowed arteries. It can also assess how well your heart valves are functioning and whether there are any structural abnormalities in your heart. Your healthcare provider will use the results of the test to develop a treatment plan tailored to your individual needs.
Troponin I is a protein that is found in the cardiac muscle cells (myocytes) of the heart. It is a component of the troponin complex, which also includes troponin C and troponin T, that regulates the calcium-mediated interaction between actin and myosin filaments during muscle contraction.
Troponin I is specific to the cardiac muscle tissue, making it a useful biomarker for detecting damage to the heart muscle. When there is injury or damage to the heart muscle cells, such as during a heart attack (myocardial infarction), troponin I is released into the bloodstream.
Measurement of cardiac troponin I levels in the blood is used in the diagnosis and management of acute coronary syndrome (ACS) and other conditions that cause damage to the heart muscle. Elevated levels of troponin I in the blood are indicative of myocardial injury, and the degree of elevation can help determine the severity of the injury.
I believe there may be some confusion in your question. "Rabbits" is a common name used to refer to the Lagomorpha species, particularly members of the family Leporidae. They are small mammals known for their long ears, strong legs, and quick reproduction.
However, if you're referring to "rabbits" in a medical context, there is a term called "rabbit syndrome," which is a rare movement disorder characterized by repetitive, involuntary movements of the fingers, resembling those of a rabbit chewing. It is also known as "finger-chewing chorea." This condition is usually associated with certain medications, particularly antipsychotics, and typically resolves when the medication is stopped or adjusted.
The heart ventricles are the two lower chambers of the heart that receive blood from the atria and pump it to the lungs or the rest of the body. The right ventricle pumps deoxygenated blood to the lungs, while the left ventricle pumps oxygenated blood to the rest of the body. Both ventricles have thick, muscular walls to generate the pressure necessary to pump blood through the circulatory system.
Ischemic postconditioning is a medical/physiological term that refers to a cardioprotective strategy used to mitigate the damage caused by ischemia-reperfusion injury, which occurs during myocardial infarction (heart attack) or other conditions involving restricted blood flow to the heart muscle.
The technique involves applying brief, intermittent periods of reduced blood flow (ischemia) and reflow (reperfusion) to the heart immediately after a prolonged period of ischemia. This process triggers a complex intracellular signaling cascade that helps protect the heart tissue from further damage during reperfusion.
The protective effects of ischemic postconditioning are attributed to various cellular and molecular mechanisms, such as reducing oxidative stress, inhibiting inflammation, preserving mitochondrial function, and modulating calcium homeostasis. These combined actions help minimize the infarct size (area of damaged heart tissue) and improve overall cardiac function following an ischemic event.
Ischemic postconditioning has been explored as a potential therapeutic approach to treat ischemia-reperfusion injuries in various clinical settings, including heart attacks, cardiac surgery, and organ transplantation. However, its translation into clinical practice has been challenging due to the complexity of the intervention and the need for precise timing and control over the ischemic and reperfusion periods.
Gerbillinae is a subfamily of rodents that includes gerbils, jirds, and sand rats. These small mammals are primarily found in arid regions of Africa and Asia. They are characterized by their long hind legs, which they use for hopping, and their long, thin tails. Some species have adapted to desert environments by developing specialized kidneys that allow them to survive on minimal water intake.
Spinal cord ischemia refers to a reduction or interruption of blood flow to the spinal cord, leading to insufficient oxygen and nutrient supply. This condition can cause damage to the spinal cord tissue, potentially resulting in neurological deficits, such as muscle weakness, sensory loss, or autonomic dysfunction. Spinal cord ischemia may be caused by various factors, including atherosclerosis, embolism, spinal artery stenosis, or complications during surgery. The severity and extent of the neurological impairment depend on the duration and location of the ischemic event in the spinal cord.
Ventricular Fibrillation (VF) is a type of cardiac arrhythmia, which is an abnormal heart rhythm. In VF, the ventricles, which are the lower chambers of the heart, beat in a rapid and unorganized manner. This results in the heart being unable to pump blood effectively to the rest of the body, leading to immediate circulatory collapse and cardiac arrest if not treated promptly. It is often caused by underlying heart conditions such as coronary artery disease, structural heart problems, or electrolyte imbalances. VF is a medical emergency that requires immediate defibrillation to restore a normal heart rhythm.
Troponin T is a subunit of the troponin complex, which is a protein complex that plays a crucial role in muscle contraction. In particular, Troponin T is responsible for binding the troponin complex to tropomyosin, another protein that helps regulate muscle contraction.
In the context of medical diagnostics, Troponin T is often measured as a biomarker for heart damage. When heart muscle cells are damaged or die, such as in a myocardial infarction (heart attack), troponin T is released into the bloodstream. Therefore, measuring the levels of Troponin T in the blood can help diagnose and assess the severity of heart damage.
It's important to note that Troponin T is specific to cardiac muscle cells, which makes it a more reliable biomarker for heart damage than other markers that may also be found in skeletal muscle cells. However, it's worth noting that Troponin T levels can also be elevated in conditions other than heart attacks, such as heart failure, myocarditis, and pulmonary embolism, so clinical context is important when interpreting test results.
An acute disease is a medical condition that has a rapid onset, develops quickly, and tends to be short in duration. Acute diseases can range from minor illnesses such as a common cold or flu, to more severe conditions such as pneumonia, meningitis, or a heart attack. These types of diseases often have clear symptoms that are easy to identify, and they may require immediate medical attention or treatment.
Acute diseases are typically caused by an external agent or factor, such as a bacterial or viral infection, a toxin, or an injury. They can also be the result of a sudden worsening of an existing chronic condition. In general, acute diseases are distinct from chronic diseases, which are long-term medical conditions that develop slowly over time and may require ongoing management and treatment.
Examples of acute diseases include:
* Acute bronchitis: a sudden inflammation of the airways in the lungs, often caused by a viral infection.
* Appendicitis: an inflammation of the appendix that can cause severe pain and requires surgical removal.
* Gastroenteritis: an inflammation of the stomach and intestines, often caused by a viral or bacterial infection.
* Migraine headaches: intense headaches that can last for hours or days, and are often accompanied by nausea, vomiting, and sensitivity to light and sound.
* Myocardial infarction (heart attack): a sudden blockage of blood flow to the heart muscle, often caused by a buildup of plaque in the coronary arteries.
* Pneumonia: an infection of the lungs that can cause coughing, chest pain, and difficulty breathing.
* Sinusitis: an inflammation of the sinuses, often caused by a viral or bacterial infection.
It's important to note that while some acute diseases may resolve on their own with rest and supportive care, others may require medical intervention or treatment to prevent complications and promote recovery. If you are experiencing symptoms of an acute disease, it is always best to seek medical attention to ensure proper diagnosis and treatment.
I'm happy to help! However, it seems like there are two terms combined into one request: "Mitochondria" and "Heart." I will provide separate definitions for each.
Mitochondrion (singular) or Mitochondria (plural): These are specialized structures found in the cytoplasm of most eukaryotic cells (cells with a true nucleus), including human cells. They are often referred to as the "powerhouse" of the cell because they generate energy in the form of ATP (adenosine triphosphate) through a process called oxidative phosphorylation. Mitochondria contain their own DNA, which is distinct from the nuclear DNA, and are believed to have originated from ancient bacteria that established a symbiotic relationship with primitive eukaryotic cells.
Heart: In human anatomy, the heart is a muscular organ responsible for pumping blood throughout the body. It is located in the thoracic cavity, slightly left of the center, and is enclosed by the pericardium, a double-walled sac that provides protection and lubrication for the heart's movement. The human heart is divided into four chambers: two atria on the top and two ventricles on the bottom. The right side of the heart receives deoxygenated blood from the body and pumps it to the lungs, while the left side receives oxygenated blood from the lungs and pumps it to the rest of the body. The heart's pumping action is regulated by electrical signals that originate in a group of specialized cardiac muscle cells called the sinoatrial node (SA node).
Nitroglycerin, also known as glyceryl trinitrate, is a medication used primarily for the treatment of angina pectoris (chest pain due to coronary artery disease) and hypertensive emergencies (severe high blood pressure). It belongs to a class of drugs called nitrates or organic nitrites.
Nitroglycerin works by relaxing and dilating the smooth muscle in blood vessels, which leads to decreased workload on the heart and increased oxygen delivery to the myocardium (heart muscle). This results in reduced symptoms of angina and improved cardiac function during hypertensive emergencies.
The drug is available in various forms, including sublingual tablets, sprays, transdermal patches, ointments, and intravenous solutions. The choice of formulation depends on the specific clinical situation and patient needs. Common side effects of nitroglycerin include headache, dizziness, and hypotension (low blood pressure).
Anesthesia is a medical term that refers to the loss of sensation or awareness, usually induced by the administration of various drugs. It is commonly used during surgical procedures to prevent pain and discomfort. There are several types of anesthesia, including:
1. General anesthesia: This type of anesthesia causes a complete loss of consciousness and is typically used for major surgeries.
2. Regional anesthesia: This type of anesthesia numbs a specific area of the body, such as an arm or leg, while the patient remains conscious.
3. Local anesthesia: This type of anesthesia numbs a small area of the body, such as a cut or wound, and is typically used for minor procedures.
Anesthesia can be administered through various routes, including injection, inhalation, or topical application. The choice of anesthesia depends on several factors, including the type and duration of the procedure, the patient's medical history, and their overall health. Anesthesiologists are medical professionals who specialize in administering anesthesia and monitoring patients during surgical procedures to ensure their safety and comfort.
Lactic acid, also known as 2-hydroxypropanoic acid, is a chemical compound that plays a significant role in various biological processes. In the context of medicine and biochemistry, lactic acid is primarily discussed in relation to muscle metabolism and cellular energy production. Here's a medical definition for lactic acid:
Lactic acid (LA): A carboxylic acid with the molecular formula C3H6O3 that plays a crucial role in anaerobic respiration, particularly during strenuous exercise or conditions of reduced oxygen availability. It is formed through the conversion of pyruvate, catalyzed by the enzyme lactate dehydrogenase (LDH), when there is insufficient oxygen to complete the final step of cellular respiration in the Krebs cycle. The accumulation of lactic acid can lead to acidosis and muscle fatigue. Additionally, lactic acid serves as a vital intermediary in various metabolic pathways and is involved in the production of glucose through gluconeogenesis in the liver.
Coronary stenosis is a medical condition that refers to the narrowing of the coronary arteries, which supply oxygen-rich blood to the heart muscle. This narrowing is typically caused by the buildup of plaque, made up of fat, cholesterol, and other substances, on the inner walls of the arteries. Over time, as the plaque hardens and calcifies, it can cause the artery to become narrowed or blocked, reducing blood flow to the heart muscle.
Coronary stenosis can lead to various symptoms and complications, including chest pain (angina), shortness of breath, irregular heart rhythms (arrhythmias), and heart attacks. Treatment options for coronary stenosis may include lifestyle changes, medications, medical procedures such as angioplasty or bypass surgery, or a combination of these approaches. Regular check-ups and diagnostic tests, such as stress testing or coronary angiography, can help detect and monitor coronary stenosis over time.
Unstable angina is a term used in cardiology to describe chest pain or discomfort that occurs suddenly and unexpectedly, often at rest or with minimal physical exertion. It is caused by an insufficient supply of oxygen-rich blood to the heart muscle due to reduced blood flow, typically as a result of partial or complete blockage of the coronary arteries.
Unlike stable angina, which tends to occur predictably during physical activity and can be relieved with rest or nitroglycerin, unstable angina is more severe, unpredictable, and may not respond to traditional treatments. It is considered a medical emergency because it can be a sign of an impending heart attack or other serious cardiac event.
Unstable angina is often treated in the hospital with medications such as nitroglycerin, beta blockers, calcium channel blockers, and antiplatelet agents to improve blood flow to the heart and prevent further complications. In some cases, more invasive treatments such as coronary angioplasty or bypass surgery may be necessary to restore blood flow to the affected areas of the heart.
Cardiovascular agents are a class of medications that are used to treat various conditions related to the cardiovascular system, which includes the heart and blood vessels. These agents can be further divided into several subcategories based on their specific mechanisms of action and therapeutic effects. Here are some examples:
1. Antiarrhythmics: These drugs are used to treat abnormal heart rhythms or arrhythmias. They work by stabilizing the electrical activity of the heart and preventing irregular impulses from spreading through the heart muscle.
2. Antihypertensives: These medications are used to lower high blood pressure, also known as hypertension. There are several classes of antihypertensive drugs, including diuretics, beta-blockers, calcium channel blockers, and angiotensin-converting enzyme (ACE) inhibitors.
3. Anticoagulants: These drugs are used to prevent blood clots from forming or growing larger. They work by interfering with the coagulation cascade, which is a series of chemical reactions that lead to the formation of a blood clot.
4. Antiplatelet agents: These medications are used to prevent platelets in the blood from sticking together and forming clots. They work by inhibiting the aggregation of platelets, which are small cells in the blood that help form clots.
5. Lipid-lowering agents: These drugs are used to lower cholesterol and other fats in the blood. They work by reducing the production or absorption of cholesterol in the body or increasing the removal of cholesterol from the bloodstream. Examples include statins, bile acid sequestrants, and PCSK9 inhibitors.
6. Vasodilators: These medications are used to widen blood vessels and improve blood flow. They work by relaxing the smooth muscle in the walls of blood vessels, causing them to dilate or widen. Examples include nitrates, calcium channel blockers, and ACE inhibitors.
7. Inotropes: These drugs are used to increase the force of heart contractions. They work by increasing the sensitivity of heart muscle cells to calcium ions, which are necessary for muscle contraction.
These are just a few examples of cardiovascular medications that are used to treat various conditions related to the heart and blood vessels. It is important to note that these medications can have side effects and should be taken under the guidance of a healthcare provider.
Prospective studies, also known as longitudinal studies, are a type of cohort study in which data is collected forward in time, following a group of individuals who share a common characteristic or exposure over a period of time. The researchers clearly define the study population and exposure of interest at the beginning of the study and follow up with the participants to determine the outcomes that develop over time. This type of study design allows for the investigation of causal relationships between exposures and outcomes, as well as the identification of risk factors and the estimation of disease incidence rates. Prospective studies are particularly useful in epidemiology and medical research when studying diseases with long latency periods or rare outcomes.
"Miniature Swine" is not a medical term per se, but it is commonly used in the field of biomedical research to refer to certain breeds or types of pigs that are smaller in size compared to traditional farm pigs. These miniature swine are often used as animal models for human diseases due to their similarities with humans in terms of anatomy, genetics, and physiology. Examples of commonly used miniature swine include the Yucatan, Sinclair, and Göttingen breeds. It is important to note that while these animals are often called "miniature," they can still weigh between 50-200 pounds depending on the specific breed or age.
The Predictive Value of Tests, specifically the Positive Predictive Value (PPV) and Negative Predictive Value (NPV), are measures used in diagnostic tests to determine the probability that a positive or negative test result is correct.
Positive Predictive Value (PPV) is the proportion of patients with a positive test result who actually have the disease. It is calculated as the number of true positives divided by the total number of positive results (true positives + false positives). A higher PPV indicates that a positive test result is more likely to be a true positive, and therefore the disease is more likely to be present.
Negative Predictive Value (NPV) is the proportion of patients with a negative test result who do not have the disease. It is calculated as the number of true negatives divided by the total number of negative results (true negatives + false negatives). A higher NPV indicates that a negative test result is more likely to be a true negative, and therefore the disease is less likely to be present.
The predictive value of tests depends on the prevalence of the disease in the population being tested, as well as the sensitivity and specificity of the test. A test with high sensitivity and specificity will generally have higher predictive values than a test with low sensitivity and specificity. However, even a highly sensitive and specific test can have low predictive values if the prevalence of the disease is low in the population being tested.
Heart function tests are a group of diagnostic exams that are used to evaluate the structure and functioning of the heart. These tests help doctors assess the pumping efficiency of the heart, the flow of blood through the heart, the presence of any heart damage, and the overall effectiveness of the heart in delivering oxygenated blood to the rest of the body.
Some common heart function tests include:
1. Echocardiogram (Echo): This test uses sound waves to create detailed images of the heart's structure and functioning. It can help detect any damage to the heart muscle, valves, or sac surrounding the heart.
2. Nuclear Stress Test: This test involves injecting a small amount of radioactive substance into the patient's bloodstream and taking images of the heart while it is at rest and during exercise. The test helps evaluate blood flow to the heart and detect any areas of reduced blood flow, which could indicate coronary artery disease.
3. Cardiac Magnetic Resonance Imaging (MRI): This test uses magnetic fields and radio waves to create detailed images of the heart's structure and function. It can help detect any damage to the heart muscle, valves, or other structures of the heart.
4. Electrocardiogram (ECG): This test measures the electrical activity of the heart and helps detect any abnormalities in the heart's rhythm or conduction system.
5. Exercise Stress Test: This test involves walking on a treadmill or riding a stationary bike while being monitored for changes in heart rate, blood pressure, and ECG readings. It helps evaluate exercise capacity and detect any signs of coronary artery disease.
6. Cardiac Catheterization: This is an invasive procedure that involves inserting a catheter into the heart to measure pressures and take samples of blood from different parts of the heart. It can help diagnose various heart conditions, including heart valve problems, congenital heart defects, and coronary artery disease.
Overall, heart function tests play an essential role in diagnosing and managing various heart conditions, helping doctors provide appropriate treatment and improve patient outcomes.
"Random allocation," also known as "random assignment" or "randomization," is a process used in clinical trials and other research studies to distribute participants into different intervention groups (such as experimental group vs. control group) in a way that minimizes selection bias and ensures the groups are comparable at the start of the study.
In random allocation, each participant has an equal chance of being assigned to any group, and the assignment is typically made using a computer-generated randomization schedule or other objective methods. This process helps to ensure that any differences between the groups are due to the intervention being tested rather than pre-existing differences in the participants' characteristics.
Necrosis is the premature death of cells or tissues due to damage or injury, such as from infection, trauma, infarction (lack of blood supply), or toxic substances. It's a pathological process that results in the uncontrolled and passive degradation of cellular components, ultimately leading to the release of intracellular contents into the extracellular space. This can cause local inflammation and may lead to further tissue damage if not treated promptly.
There are different types of necrosis, including coagulative, liquefactive, caseous, fat, fibrinoid, and gangrenous necrosis, each with distinct histological features depending on the underlying cause and the affected tissues or organs.
In medical terms, constriction refers to the narrowing or tightening of a body part or passageway. This can occur due to various reasons such as spasms of muscles, inflammation, or abnormal growths. It can lead to symptoms like difficulty in breathing, swallowing, or blood flow, depending on where it occurs. For example, constriction of the airways in asthma, constriction of blood vessels in hypertension, or constriction of the esophagus in certain digestive disorders.
Angina pectoris, variant (also known as Prinzmetal's angina or vasospastic angina) is a type of chest pain that results from reduced blood flow to the heart muscle due to spasms in the coronary arteries. These spasms cause the arteries to narrow, temporarily reducing the supply of oxygen-rich blood to the heart. This can lead to symptoms such as chest pain, shortness of breath, and fatigue.
Variant angina is typically more severe than other forms of angina and can occur at rest or with minimal physical exertion. It is often treated with medications that help relax the coronary arteries and prevent spasms, such as calcium channel blockers and nitrates. In some cases, additional treatments such as angioplasty or bypass surgery may be necessary to improve blood flow to the heart.
It's important to note that chest pain can have many different causes, so it is essential to seek medical attention if you experience any symptoms of angina or other types of chest pain. A healthcare professional can help determine the cause of your symptoms and develop an appropriate treatment plan.
Coronary vessel anomalies refer to abnormalities in the structure, origin, or course of the coronary arteries or veins. These vessels are responsible for delivering oxygenated blood to the heart muscle. Some common types of coronary vessel anomalies include:
1. Anomalous Origin of the Coronary Artery (AOCA): This occurs when one or both of the coronary arteries originate from an abnormal location in the aorta. The left coronary artery may arise from the right sinus of Valsalva, while the right coronary artery may arise from the left sinus of Valsalva. This can lead to ischemia (reduced blood flow) and potentially life-threatening complications such as sudden cardiac death.
2. Coronary Artery Fistula: A fistula is an abnormal connection between a coronary artery and another chamber or vessel in the heart. Blood flows directly from the high-pressure coronary artery into a low-pressure chamber, bypassing the capillaries and leading to a steal phenomenon where oxygenated blood is diverted away from the heart muscle.
3. Coronary Artery Aneurysm: An aneurysm is a localized dilation or bulging of the coronary artery wall. This can lead to complications such as thrombosis (blood clot formation), embolism (blockage caused by a clot that travels to another location), or rupture, which can be life-threatening.
4. Myocardial Bridge: In this condition, a segment of the coronary artery passes between the muscle fibers of the heart, instead of running along its surface. This can cause compression of the artery during systole (contraction) and lead to ischemia.
5. Kawasaki Disease: Although not strictly an anomaly, Kawasaki disease is a pediatric illness that can result in coronary artery aneurysms and other complications if left untreated.
Coronary vessel anomalies may be asymptomatic or present with symptoms such as chest pain, shortness of breath, palpitations, or syncope (fainting). Diagnosis typically involves imaging techniques such as coronary angiography, computed tomography (CT) angiography, or magnetic resonance angiography. Treatment depends on the specific anomaly and may involve medications, percutaneous interventions, or surgical correction.
Neuroprotective agents are substances that protect neurons or nerve cells from damage, degeneration, or death caused by various factors such as trauma, inflammation, oxidative stress, or excitotoxicity. These agents work through different mechanisms, including reducing the production of free radicals, inhibiting the release of glutamate (a neurotransmitter that can cause cell damage in high concentrations), promoting the growth and survival of neurons, and preventing apoptosis (programmed cell death). Neuroprotective agents have been studied for their potential to treat various neurological disorders, including stroke, traumatic brain injury, Parkinson's disease, Alzheimer's disease, and multiple sclerosis. However, more research is needed to fully understand their mechanisms of action and to develop effective therapies.
Lactates, also known as lactic acid, are compounds that are produced by muscles during intense exercise or other conditions of low oxygen supply. They are formed from the breakdown of glucose in the absence of adequate oxygen to complete the full process of cellular respiration. This results in the production of lactate and a hydrogen ion, which can lead to a decrease in pH and muscle fatigue.
In a medical context, lactates may be measured in the blood as an indicator of tissue oxygenation and metabolic status. Elevated levels of lactate in the blood, known as lactic acidosis, can indicate poor tissue perfusion or hypoxia, and may be seen in conditions such as sepsis, cardiac arrest, and severe shock. It is important to note that lactates are not the primary cause of acidemia (low pH) in lactic acidosis, but rather a marker of the underlying process.
L-Lactate Dehydrogenase (LDH) is an enzyme found in various tissues within the body, including the heart, liver, kidneys, muscles, and brain. It plays a crucial role in the process of energy production, particularly during anaerobic conditions when oxygen levels are low.
In the presence of the coenzyme NADH, LDH catalyzes the conversion of pyruvate to lactate, generating NAD+ as a byproduct. Conversely, in the presence of NAD+, LDH can convert lactate back to pyruvate using NADH. This reversible reaction is essential for maintaining the balance between lactate and pyruvate levels within cells.
Elevated blood levels of LDH may indicate tissue damage or injury, as this enzyme can be released into the circulation following cellular breakdown. As a result, LDH is often used as a nonspecific biomarker for various medical conditions, such as myocardial infarction (heart attack), liver disease, muscle damage, and certain types of cancer. However, it's important to note that an isolated increase in LDH does not necessarily pinpoint the exact location or cause of tissue damage, and further diagnostic tests are usually required for confirmation.
A biological marker, often referred to as a biomarker, is a measurable indicator that reflects the presence or severity of a disease state, or a response to a therapeutic intervention. Biomarkers can be found in various materials such as blood, tissues, or bodily fluids, and they can take many forms, including molecular, histologic, radiographic, or physiological measurements.
In the context of medical research and clinical practice, biomarkers are used for a variety of purposes, such as:
1. Diagnosis: Biomarkers can help diagnose a disease by indicating the presence or absence of a particular condition. For example, prostate-specific antigen (PSA) is a biomarker used to detect prostate cancer.
2. Monitoring: Biomarkers can be used to monitor the progression or regression of a disease over time. For instance, hemoglobin A1c (HbA1c) levels are monitored in diabetes patients to assess long-term blood glucose control.
3. Predicting: Biomarkers can help predict the likelihood of developing a particular disease or the risk of a negative outcome. For example, the presence of certain genetic mutations can indicate an increased risk for breast cancer.
4. Response to treatment: Biomarkers can be used to evaluate the effectiveness of a specific treatment by measuring changes in the biomarker levels before and after the intervention. This is particularly useful in personalized medicine, where treatments are tailored to individual patients based on their unique biomarker profiles.
It's important to note that for a biomarker to be considered clinically valid and useful, it must undergo rigorous validation through well-designed studies, including demonstrating sensitivity, specificity, reproducibility, and clinical relevance.
Left ventricular dysfunction (LVD) is a condition characterized by the impaired ability of the left ventricle of the heart to pump blood efficiently during contraction. The left ventricle is one of the four chambers of the heart and is responsible for pumping oxygenated blood to the rest of the body.
LVD can be caused by various underlying conditions, such as coronary artery disease, cardiomyopathy, valvular heart disease, or hypertension. These conditions can lead to structural changes in the left ventricle, including remodeling, hypertrophy, and dilation, which ultimately impair its contractile function.
The severity of LVD is often assessed by measuring the ejection fraction (EF), which is the percentage of blood that is pumped out of the left ventricle during each contraction. A normal EF ranges from 55% to 70%, while an EF below 40% is indicative of LVD.
LVD can lead to various symptoms, such as shortness of breath, fatigue, fluid retention, and decreased exercise tolerance. It can also increase the risk of complications, such as heart failure, arrhythmias, and cardiac arrest. Treatment for LVD typically involves managing the underlying cause, along with medications to improve contractility, reduce fluid buildup, and control heart rate. In severe cases, devices such as implantable cardioverter-defibrillators (ICDs) or left ventricular assist devices (LVADs) may be required.
Middle Cerebral Artery (MCA) infarction is a type of ischemic stroke that occurs when there is an obstruction in the blood supply to the middle cerebral artery, which is one of the major blood vessels that supplies oxygenated blood to the brain. The MCA supplies blood to a large portion of the brain, including the motor and sensory cortex, parts of the temporal and parietal lobes, and the basal ganglia.
An infarction is the death of tissue due to the lack of blood supply, which can lead to damage or loss of function in the affected areas of the brain. Symptoms of MCA infarction may include weakness or numbness on one side of the body, difficulty speaking or understanding speech, vision problems, and altered levels of consciousness.
MCA infarctions can be caused by various factors, including embolism (a blood clot that travels to the brain from another part of the body), thrombosis (a blood clot that forms in the MCA itself), or stenosis (narrowing of the artery due to atherosclerosis or other conditions). Treatment for MCA infarction may include medications to dissolve blood clots, surgery to remove the obstruction, or rehabilitation to help regain lost function.
C57BL/6 (C57 Black 6) is an inbred strain of laboratory mouse that is widely used in biomedical research. The term "inbred" refers to a strain of animals where matings have been carried out between siblings or other closely related individuals for many generations, resulting in a population that is highly homozygous at most genetic loci.
The C57BL/6 strain was established in 1920 by crossing a female mouse from the dilute brown (DBA) strain with a male mouse from the black strain. The resulting offspring were then interbred for many generations to create the inbred C57BL/6 strain.
C57BL/6 mice are known for their robust health, longevity, and ease of handling, making them a popular choice for researchers. They have been used in a wide range of biomedical research areas, including studies of cancer, immunology, neuroscience, cardiovascular disease, and metabolism.
One of the most notable features of the C57BL/6 strain is its sensitivity to certain genetic modifications, such as the introduction of mutations that lead to obesity or impaired glucose tolerance. This has made it a valuable tool for studying the genetic basis of complex diseases and traits.
Overall, the C57BL/6 inbred mouse strain is an important model organism in biomedical research, providing a valuable resource for understanding the genetic and molecular mechanisms underlying human health and disease.
Peroxidase is a type of enzyme that catalyzes the chemical reaction in which hydrogen peroxide (H2O2) is broken down into water (H2O) and oxygen (O2). This enzymatic reaction also involves the oxidation of various organic and inorganic compounds, which can serve as electron donors.
Peroxidases are widely distributed in nature and can be found in various organisms, including bacteria, fungi, plants, and animals. They play important roles in various biological processes, such as defense against oxidative stress, breakdown of toxic substances, and participation in metabolic pathways.
The peroxidase-catalyzed reaction can be represented by the following chemical equation:
H2O2 + 2e- + 2H+ → 2H2O
In this reaction, hydrogen peroxide is reduced to water, and the electron donor is oxidized. The peroxidase enzyme facilitates the transfer of electrons between the substrate (hydrogen peroxide) and the electron donor, making the reaction more efficient and specific.
Peroxidases have various applications in medicine, industry, and research. For example, they can be used for diagnostic purposes, as biosensors, and in the treatment of wastewater and medical wastes. Additionally, peroxidases are involved in several pathological conditions, such as inflammation, cancer, and neurodegenerative diseases, making them potential targets for therapeutic interventions.
Coronary vasospasm refers to a sudden constriction (narrowing) of the coronary arteries, which supply oxygenated blood to the heart muscle. This constriction can reduce or block blood flow, leading to symptoms such as chest pain (angina) or, in severe cases, a heart attack (myocardial infarction). Coronary vasospasm can occur spontaneously or be triggered by various factors, including stress, smoking, and certain medications. It is also associated with conditions such as coronary artery disease and variant angina. Prolonged or recurrent vasospasms can cause damage to the heart muscle and increase the risk of cardiovascular events.
Adenosine Triphosphate (ATP) is a high-energy molecule that stores and transports energy within cells. It is the main source of energy for most cellular processes, including muscle contraction, nerve impulse transmission, and protein synthesis. ATP is composed of a base (adenine), a sugar (ribose), and three phosphate groups. The bonds between these phosphate groups contain a significant amount of energy, which can be released when the bond between the second and third phosphate group is broken, resulting in the formation of adenosine diphosphate (ADP) and inorganic phosphate. This process is known as hydrolysis and can be catalyzed by various enzymes to drive a wide range of cellular functions. ATP can also be regenerated from ADP through various metabolic pathways, such as oxidative phosphorylation or substrate-level phosphorylation, allowing for the continuous supply of energy to cells.
Adrenergic beta-antagonists, also known as beta blockers, are a class of medications that block the effects of adrenaline and noradrenaline (also known as epinephrine and norepinephrine) on beta-adrenergic receptors. These receptors are found in various tissues throughout the body, including the heart, lungs, and blood vessels.
Beta blockers work by binding to these receptors and preventing the activation of certain signaling pathways that lead to increased heart rate, force of heart contractions, and relaxation of blood vessels. As a result, beta blockers can lower blood pressure, reduce heart rate, and decrease the workload on the heart.
Beta blockers are used to treat a variety of medical conditions, including hypertension (high blood pressure), angina (chest pain), heart failure, irregular heart rhythms, migraines, and certain anxiety disorders. Some common examples of beta blockers include metoprolol, atenolol, propranolol, and bisoprolol.
It is important to note that while beta blockers can have many benefits, they can also cause side effects such as fatigue, dizziness, and shortness of breath. Additionally, sudden discontinuation of beta blocker therapy can lead to rebound hypertension or worsening chest pain. Therefore, it is important to follow the dosing instructions provided by a healthcare provider carefully when taking these medications.
Coronary artery bypass surgery, also known as coronary artery bypass grafting (CABG), is a surgical procedure used to improve blood flow to the heart in patients with severe coronary artery disease. This condition occurs when the coronary arteries, which supply oxygen-rich blood to the heart muscle, become narrowed or blocked due to the buildup of fatty deposits, called plaques.
During CABG surgery, a healthy blood vessel from another part of the body is grafted, or attached, to the coronary artery, creating a new pathway for oxygen-rich blood to flow around the blocked or narrowed portion of the artery and reach the heart muscle. This bypass helps to restore normal blood flow and reduce the risk of angina (chest pain), shortness of breath, and other symptoms associated with coronary artery disease.
There are different types of CABG surgery, including traditional on-pump CABG, off-pump CABG, and minimally invasive CABG. The choice of procedure depends on various factors, such as the patient's overall health, the number and location of blocked arteries, and the presence of other medical conditions.
It is important to note that while CABG surgery can significantly improve symptoms and quality of life in patients with severe coronary artery disease, it does not cure the underlying condition. Lifestyle modifications, such as regular exercise, a healthy diet, smoking cessation, and medication therapy, are essential for long-term management and prevention of further progression of the disease.
Apoptosis is a programmed and controlled cell death process that occurs in multicellular organisms. It is a natural process that helps maintain tissue homeostasis by eliminating damaged, infected, or unwanted cells. During apoptosis, the cell undergoes a series of morphological changes, including cell shrinkage, chromatin condensation, and fragmentation into membrane-bound vesicles called apoptotic bodies. These bodies are then recognized and engulfed by neighboring cells or phagocytic cells, preventing an inflammatory response. Apoptosis is regulated by a complex network of intracellular signaling pathways that involve proteins such as caspases, Bcl-2 family members, and inhibitors of apoptosis (IAPs).
Microvascular angina, also known as cardiac syndrome X or microvascular ischemia, is a type of angina (chest pain) that results from reduced blood flow to the heart muscle due to dysfunction in the small coronary arteries (microvasculature). These vessels are too small to be visualized during conventional diagnostic tests like coronary angiography.
The medical definition of microvascular angina is:
A clinical syndrome characterized by the presence of anginal chest pain, often accompanied by evidence of myocardial ischemia (insufficient blood flow to the heart muscle), in the absence of obstructive coronary artery disease on conventional diagnostic imaging. The underlying mechanism involves dysfunction and impaired regulation of the microvasculature, leading to reduced vasodilatory capacity, increased vasoconstriction, and ultimately, inadequate oxygen supply to meet the metabolic demands of the heart muscle.
Microvascular angina is more prevalent in women, especially those with risk factors such as hypertension, diabetes, hyperlipidemia, and smoking. Diagnosis often requires specialized testing like coronary flow reserve assessment using positron emission tomography (PET) or cardiac magnetic resonance imaging (MRI). Treatment typically involves a combination of lifestyle modifications, medications to improve blood vessel function and reduce chest pain, and sometimes, invasive treatments such as transmyocardial laser revascularization.
Oxygen consumption, also known as oxygen uptake, is the amount of oxygen that is consumed or utilized by the body during a specific period of time, usually measured in liters per minute (L/min). It is a common measurement used in exercise physiology and critical care medicine to assess an individual's aerobic metabolism and overall health status.
In clinical settings, oxygen consumption is often measured during cardiopulmonary exercise testing (CPET) to evaluate cardiovascular function, pulmonary function, and exercise capacity in patients with various medical conditions such as heart failure, chronic obstructive pulmonary disease (COPD), and other respiratory or cardiac disorders.
During exercise, oxygen is consumed by the muscles to generate energy through a process called oxidative phosphorylation. The amount of oxygen consumed during exercise can provide important information about an individual's fitness level, exercise capacity, and overall health status. Additionally, measuring oxygen consumption can help healthcare providers assess the effectiveness of treatments and rehabilitation programs in patients with various medical conditions.
Ergonovine is a medication that belongs to a class of drugs called ergot alkaloids. It is derived from the ergot fungus and is used in medical settings as a uterotonic agent, which means it causes the uterus to contract. Ergonovine is often used after childbirth to help the uterus return to its normal size and reduce bleeding.
Ergonovine works by binding to specific receptors in the smooth muscle of the uterus, causing it to contract. It has a potent effect on the uterus and can also cause vasoconstriction (narrowing of blood vessels) in other parts of the body. This is why ergonovine is sometimes used to treat severe bleeding caused by conditions such as uterine fibroids or ectopic pregnancy.
Like other ergot alkaloids, ergonovine can have serious side effects if not used carefully. It should be administered under the close supervision of a healthcare provider and should not be used in women with certain medical conditions, such as high blood pressure or heart disease. Ergonovine can also interact with other medications, so it's important to inform your healthcare provider of all medications you are taking before receiving this drug.
Diltiazem is a calcium channel blocker medication that is used to treat hypertension (high blood pressure), angina (chest pain), and certain heart rhythm disorders. It works by relaxing the muscles of the blood vessels, which lowers blood pressure and improves blood flow to the heart. Diltiazem may also be used to reduce the risk of heart attack in patients with coronary artery disease.
The medication is available in various forms, including immediate-release tablets, extended-release tablets, and extended-release capsules. It is usually taken orally, one to three times a day, depending on the formulation and the individual patient's needs. Diltiazem may cause side effects such as dizziness, headache, nausea, and constipation.
It is important to follow the dosage instructions provided by your healthcare provider and to inform them of any other medications you are taking, as well as any medical conditions you have, before starting diltiazem.
Medical Definition:
"Risk factors" are any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury. They can be divided into modifiable and non-modifiable risk factors. Modifiable risk factors are those that can be changed through lifestyle choices or medical treatment, while non-modifiable risk factors are inherent traits such as age, gender, or genetic predisposition. Examples of modifiable risk factors include smoking, alcohol consumption, physical inactivity, and unhealthy diet, while non-modifiable risk factors include age, sex, and family history. It is important to note that having a risk factor does not guarantee that a person will develop the disease, but rather indicates an increased susceptibility.
Phosphocreatine (PCr) is a high-energy phosphate compound found in the skeletal muscles, cardiac muscle, and brain. It plays a crucial role in energy metabolism and storage within cells. Phosphocreatine serves as an immediate energy reserve that helps regenerate ATP (adenosine triphosphate), the primary source of cellular energy, during short bursts of intense activity or stress. This process is facilitated by the enzyme creatine kinase, which catalyzes the transfer of a phosphate group from phosphocreatine to ADP (adenosine diphosphate) to form ATP.
In a medical context, phosphocreatine levels may be assessed in muscle biopsies or magnetic resonance spectroscopy (MRS) imaging to evaluate muscle energy metabolism and potential mitochondrial dysfunction in conditions such as muscular dystrophies, mitochondrial disorders, and neuromuscular diseases. Additionally, phosphocreatine depletion has been implicated in various pathological processes, including ischemia-reperfusion injury, neurodegenerative disorders, and heart failure.
Technetium Tc 99m Sestamibi is a radiopharmaceutical compound used in medical imaging, specifically in myocardial perfusion scintigraphy. It is a technetium-labeled isonitrile chelate that is taken up by mitochondria in cells with high metabolic activity, such as cardiomyocytes (heart muscle cells).
Once injected into the patient's body, Technetium Tc 99m Sestamibi emits gamma rays, which can be detected by a gamma camera. This allows for the creation of images that reflect the distribution and function of the radiopharmaceutical within the heart muscle. The images can help identify areas of reduced blood flow or ischemia, which may indicate coronary artery disease.
The uptake of Technetium Tc 99m Sestamibi in other organs, such as the breast and thyroid, can also be used for imaging purposes, although its primary use remains in cardiac imaging.
Coronary balloon angioplasty is a minimally invasive medical procedure used to widen narrowed or obstructed coronary arteries (the blood vessels that supply oxygen-rich blood to the heart muscle) and improve blood flow to the heart. This procedure is typically performed in conjunction with the insertion of a stent, a small mesh tube that helps keep the artery open.
During coronary balloon angioplasty, a thin, flexible catheter with a deflated balloon at its tip is inserted into a blood vessel, usually through a small incision in the groin or arm. The catheter is then guided to the narrowed or obstructed section of the coronary artery. Once in position, the balloon is inflated to compress the plaque against the artery wall and widen the lumen (the inner space) of the artery. This helps restore blood flow to the heart muscle.
The procedure is typically performed under local anesthesia and conscious sedation to minimize discomfort. Coronary balloon angioplasty is a relatively safe and effective treatment for many people with coronary artery disease, although complications such as bleeding, infection, or re-narrowing of the artery (restenosis) can occur in some cases.
Sensitivity and specificity are statistical measures used to describe the performance of a diagnostic test or screening tool in identifying true positive and true negative results.
* Sensitivity refers to the proportion of people who have a particular condition (true positives) who are correctly identified by the test. It is also known as the "true positive rate" or "recall." A highly sensitive test will identify most or all of the people with the condition, but may also produce more false positives.
* Specificity refers to the proportion of people who do not have a particular condition (true negatives) who are correctly identified by the test. It is also known as the "true negative rate." A highly specific test will identify most or all of the people without the condition, but may also produce more false negatives.
In medical testing, both sensitivity and specificity are important considerations when evaluating a diagnostic test. High sensitivity is desirable for screening tests that aim to identify as many cases of a condition as possible, while high specificity is desirable for confirmatory tests that aim to rule out the condition in people who do not have it.
It's worth noting that sensitivity and specificity are often influenced by factors such as the prevalence of the condition in the population being tested, the threshold used to define a positive result, and the reliability and validity of the test itself. Therefore, it's important to consider these factors when interpreting the results of a diagnostic test.
Nitric oxide (NO) is a molecule made up of one nitrogen atom and one oxygen atom. In the body, it is a crucial signaling molecule involved in various physiological processes such as vasodilation, immune response, neurotransmission, and inhibition of platelet aggregation. It is produced naturally by the enzyme nitric oxide synthase (NOS) from the amino acid L-arginine. Inhaled nitric oxide is used medically to treat pulmonary hypertension in newborns and adults, as it helps to relax and widen blood vessels, improving oxygenation and blood flow.
Cerebrovascular circulation refers to the network of blood vessels that supply oxygenated blood and nutrients to the brain tissue, and remove waste products. It includes the internal carotid arteries, vertebral arteries, circle of Willis, and the intracranial arteries that branch off from them.
The internal carotid arteries and vertebral arteries merge to form the circle of Willis, a polygonal network of vessels located at the base of the brain. The anterior cerebral artery, middle cerebral artery, posterior cerebral artery, and communicating arteries are the major vessels that branch off from the circle of Willis and supply blood to different regions of the brain.
Interruptions or abnormalities in the cerebrovascular circulation can lead to various neurological conditions such as stroke, transient ischemic attack (TIA), and vascular dementia.
Physiologic neovascularization is the natural and controlled formation of new blood vessels in the body, which occurs as a part of normal growth and development, as well as in response to tissue repair and wound healing. This process involves the activation of endothelial cells, which line the interior surface of blood vessels, and their migration, proliferation, and tube formation to create new capillaries. Physiologic neovascularization is tightly regulated by a balance of pro-angiogenic and anti-angiogenic factors, ensuring that it occurs only when and where it is needed. It plays crucial roles in various physiological processes, such as embryonic development, tissue regeneration, and wound healing.
The pericardium is the double-walled sac that surrounds the heart. It has an outer fibrous layer and an inner serous layer, which further divides into two parts: the parietal layer lining the fibrous pericardium and the visceral layer (epicardium) closely adhering to the heart surface.
The space between these two layers is filled with a small amount of lubricating serous fluid, allowing for smooth movement of the heart within the pericardial cavity. The pericardium provides protection, support, and helps maintain the heart's normal position within the chest while reducing friction during heart contractions.
Thallium is a chemical element with the symbol Tl and atomic number 81. It is a soft, malleable, silver-like metal that is highly toxic. In the context of medicine, thallium may be used as a component in medical imaging tests, such as thallium stress tests, which are used to evaluate blood flow to the heart and detect coronary artery disease. Thallium-201 is a radioactive isotope of thallium that is used as a radiopharmaceutical in these tests. When administered to a patient, it is taken up by heart muscle tissue in proportion to its blood flow, allowing doctors to identify areas of the heart that may not be receiving enough oxygen-rich blood. However, due to concerns about its potential toxicity and the availability of safer alternatives, thallium stress tests are less commonly used today than they were in the past.
"Cat" is a common name that refers to various species of small carnivorous mammals that belong to the family Felidae. The domestic cat, also known as Felis catus or Felis silvestris catus, is a popular pet and companion animal. It is a subspecies of the wildcat, which is found in Europe, Africa, and Asia.
Domestic cats are often kept as pets because of their companionship, playful behavior, and ability to hunt vermin. They are also valued for their ability to provide emotional support and therapy to people. Cats are obligate carnivores, which means that they require a diet that consists mainly of meat to meet their nutritional needs.
Cats are known for their agility, sharp senses, and predatory instincts. They have retractable claws, which they use for hunting and self-defense. Cats also have a keen sense of smell, hearing, and vision, which allow them to detect prey and navigate their environment.
In medical terms, cats can be hosts to various parasites and diseases that can affect humans and other animals. Some common feline diseases include rabies, feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), and toxoplasmosis. It is important for cat owners to keep their pets healthy and up-to-date on vaccinations and preventative treatments to protect both the cats and their human companions.
Organotechnetium compounds are chemical substances that contain carbon-technetium bonds, where technetium is an element with the symbol Tc and atomic number 43. These types of compounds are primarily used in medical imaging as radioactive tracers due to the ability of technetium-99m to emit gamma rays. The organotechnetium compounds help in localizing specific organs, tissues, or functions within the body, making them useful for diagnostic purposes in nuclear medicine.
It is important to note that most organotechnetium compounds are synthesized from technetium-99m, which is generated from the decay of molybdenum-99. The use of these compounds requires proper handling and administration by trained medical professionals due to their radioactive nature.
Oxygen is a colorless, odorless, tasteless gas that constitutes about 21% of the earth's atmosphere. It is a crucial element for human and most living organisms as it is vital for respiration. Inhaled oxygen enters the lungs and binds to hemoglobin in red blood cells, which carries it to tissues throughout the body where it is used to convert nutrients into energy and carbon dioxide, a waste product that is exhaled.
Medically, supplemental oxygen therapy may be provided to patients with conditions such as chronic obstructive pulmonary disease (COPD), pneumonia, heart failure, or other medical conditions that impair the body's ability to extract sufficient oxygen from the air. Oxygen can be administered through various devices, including nasal cannulas, face masks, and ventilators.
Arterial occlusive diseases are medical conditions characterized by the blockage or narrowing of the arteries, which can lead to a reduction in blood flow to various parts of the body. This reduction in blood flow can cause tissue damage and may result in serious complications such as tissue death (gangrene), organ dysfunction, or even death.
The most common cause of arterial occlusive diseases is atherosclerosis, which is the buildup of plaque made up of fat, cholesterol, calcium, and other substances in the inner lining of the artery walls. Over time, this plaque can harden and narrow the arteries, restricting blood flow. Other causes of arterial occlusive diseases include blood clots, emboli (tiny particles that travel through the bloodstream and lodge in smaller vessels), inflammation, trauma, and certain inherited conditions.
Symptoms of arterial occlusive diseases depend on the location and severity of the blockage. Common symptoms include:
* Pain, cramping, or fatigue in the affected limb, often triggered by exercise and relieved by rest (claudication)
* Numbness, tingling, or weakness in the affected limb
* Coldness or discoloration of the skin in the affected area
* Slow-healing sores or wounds on the toes, feet, or legs
* Erectile dysfunction in men
Treatment for arterial occlusive diseases may include lifestyle changes such as quitting smoking, exercising regularly, and eating a healthy diet. Medications to lower cholesterol, control blood pressure, prevent blood clots, or manage pain may also be prescribed. In severe cases, surgical procedures such as angioplasty, stenting, or bypass surgery may be necessary to restore blood flow.
Hydroxy acids are a class of chemical compounds that contain both a carboxylic acid group and a hydroxyl group. They are commonly used in dermatology and cosmetic products for their exfoliating, moisturizing, and anti-aging properties. The two main types of hydroxy acids used in skincare are alpha-hydroxy acids (AHAs) and beta-hydroxy acids (BHAs).
Alpha-hydroxy acids include compounds such as glycolic acid, lactic acid, malic acid, tartaric acid, and citric acid. They work by breaking down the "glue" that holds dead skin cells together, promoting cell turnover and helping to improve the texture and tone of the skin. AHAs are also known for their ability to improve the appearance of fine lines, wrinkles, and age spots.
Beta-hydroxy acids, on the other hand, are primarily represented by salicylic acid. BHAs are oil-soluble, which allows them to penetrate deeper into the pores and exfoliate dead skin cells and excess sebum that can lead to clogged pores and acne breakouts.
It is important to note that hydroxy acids can cause skin irritation and sensitivity to sunlight, so it is recommended to use sunscreen and start with lower concentrations when first incorporating them into a skincare routine.
The endocardium is the innermost layer of tissue that lines the chambers of the heart and the valves between them. It is a thin, smooth membrane that is in contact with the blood within the heart. This layer helps to maintain the heart's internal environment, facilitates the smooth movement of blood through the heart, and provides a protective barrier against infection and other harmful substances. The endocardium is composed of simple squamous epithelial cells called endothelial cells, which are supported by a thin layer of connective tissue.
Ventricular pressure refers to the pressure within the ventricles, which are the lower chambers of the heart. In the left ventricle, the pressure measures the force that the blood exerts on the walls as it is pumped out to the rest of the body. In the right ventricle, the pressure measures the force of the blood being pumped into the pulmonary artery and ultimately to the lungs for oxygenation.
Normally, the left ventricular pressure ranges from 8-12 mmHg at rest when the heart is relaxed (diastolic pressure) and can increase up to 120-140 mmHg during contraction (systolic pressure). The right ventricular pressure is lower than the left, with a normal diastolic pressure of 0-6 mmHg and a systolic pressure ranging from 15-30 mmHg.
Abnormal ventricular pressures can indicate various heart conditions, such as heart failure, hypertension, or valvular heart disease. Regular monitoring of ventricular pressure is essential in managing these conditions and ensuring proper heart function.
The term "asymptomatic disease" refers to a medical condition or infection that does not cause any obvious symptoms in an affected individual. Some people with asymptomatic diseases may never develop any signs or symptoms throughout their lives, while others may eventually go on to develop symptoms at a later stage. In some cases, asymptomatic diseases may still be detected through medical testing or screening, even if the person feels completely well. A classic example of an asymptomatic disease is a person who has a positive blood test for a latent viral infection, such as HIV or HSV (herpes simplex virus), but does not have any symptoms related to the infection at that time.
Iodobenzenes are organic compounds that contain a iodine atom (I) attached to a benzene ring. The general formula for iodobenzenes is C6H5I. They can be considered as aryl halides and can undergo various chemical reactions such as nucleophilic substitution, electrophilic aromatic substitution, and reduction. Iodobenzenes are less reactive than other aryl halides due to the larger size and lower electronegativity of iodine compared to other halogens. They are used in organic synthesis as building blocks or reagents for various chemical transformations.
Creatine kinase (CK) is an enzyme found in various cells throughout the body, including heart muscle cells and skeletal muscle fibers. The CK enzyme exists in different forms, depending on the type of tissue where it is found. One such form is creatine kinase MB (CK-MB), which is primarily found in cardiac muscle cells.
An increase in the levels of CK-MB in the blood can indicate damage to the heart muscle, such as that caused by a heart attack or myocardial infarction. When heart muscle cells are damaged, they release their contents, including CK-MB, into the bloodstream. Therefore, measuring CK-MB levels is a useful diagnostic tool for detecting and monitoring heart muscle damage.
It's important to note that while an elevated CK-MB level can suggest heart muscle damage, it is not specific to the heart and can also be elevated in other conditions such as skeletal muscle damage or certain muscle disorders. Therefore, CK-MB levels should be interpreted in conjunction with other clinical findings and diagnostic tests.
Anti-arrhythmia agents are a class of medications used to treat abnormal heart rhythms or arrhythmias. These drugs work by modifying the electrical activity of the heart to restore and maintain a normal heart rhythm. There are several types of anti-arrhythmia agents, including:
1. Sodium channel blockers: These drugs slow down the conduction of electrical signals in the heart, which helps to reduce rapid or irregular heartbeats. Examples include flecainide, propafenone, and quinidine.
2. Beta-blockers: These medications work by blocking the effects of adrenaline on the heart, which helps to slow down the heart rate and reduce the force of heart contractions. Examples include metoprolol, atenolol, and esmolol.
3. Calcium channel blockers: These drugs block the entry of calcium into heart muscle cells, which helps to slow down the heart rate and reduce the force of heart contractions. Examples include verapamil and diltiazem.
4. Potassium channel blockers: These medications work by prolonging the duration of the heart's electrical cycle, which helps to prevent abnormal rhythms. Examples include amiodarone and sotalol.
5. Digoxin: This drug increases the force of heart contractions and slows down the heart rate, which can help to restore a normal rhythm in certain types of arrhythmias.
It's important to note that anti-arrhythmia agents can have significant side effects and should only be prescribed by a healthcare professional who has experience in managing arrhythmias. Close monitoring is necessary to ensure the medication is working effectively and not causing any adverse effects.
Decanoic acids are a type of medium-chain fatty acid with a chain length of 10 carbon atoms. The most common decanoic acid is decanoic acid or capric acid. It is found in various animal and plant sources, such as coconut oil and cow's milk. Decanoic acids have a variety of uses, including as ingredients in cosmetics and food products, and as a potential treatment for medical conditions such as epilepsy and bacterial infections. In the body, decanoic acids are metabolized in the liver and used for energy production.
The heart conduction system is a group of specialized cardiac muscle cells that generate and conduct electrical impulses to coordinate the contraction of the heart chambers. The main components of the heart conduction system include:
1. Sinoatrial (SA) node: Also known as the sinus node, it is located in the right atrium near the entrance of the superior vena cava and functions as the primary pacemaker of the heart. It sets the heart rate by generating electrical impulses at regular intervals.
2. Atrioventricular (AV) node: Located in the interatrial septum, near the opening of the coronary sinus, it serves as a relay station for electrical signals between the atria and ventricles. The AV node delays the transmission of impulses to allow the atria to contract before the ventricles.
3. Bundle of His: A bundle of specialized cardiac muscle fibers that conducts electrical impulses from the AV node to the ventricles. It divides into two main branches, the right and left bundle branches, which further divide into smaller Purkinje fibers.
4. Right and left bundle branches: These are extensions of the Bundle of His that transmit electrical impulses to the respective right and left ventricular myocardium. They consist of specialized conducting tissue with large diameters and minimal resistance, allowing for rapid conduction of electrical signals.
5. Purkinje fibers: Fine, branching fibers that arise from the bundle branches and spread throughout the ventricular myocardium. They are responsible for transmitting electrical impulses to the working cardiac muscle cells, triggering coordinated ventricular contraction.
In summary, the heart conduction system is a complex network of specialized muscle cells responsible for generating and conducting electrical signals that coordinate the contraction of the atria and ventricles, ensuring efficient blood flow throughout the body.
Blood flow velocity is the speed at which blood travels through a specific part of the vascular system. It is typically measured in units of distance per time, such as centimeters per second (cm/s) or meters per second (m/s). Blood flow velocity can be affected by various factors, including cardiac output, vessel diameter, and viscosity of the blood. Measuring blood flow velocity is important in diagnosing and monitoring various medical conditions, such as heart disease, stroke, and peripheral vascular disease.
Cerebral infarction, also known as a "stroke" or "brain attack," is the sudden death of brain cells caused by the interruption of their blood supply. It is most commonly caused by a blockage in one of the blood vessels supplying the brain (an ischemic stroke), but can also result from a hemorrhage in or around the brain (a hemorrhagic stroke).
Ischemic strokes occur when a blood clot or other particle blocks a cerebral artery, cutting off blood flow to a part of the brain. The lack of oxygen and nutrients causes nearby brain cells to die. Hemorrhagic strokes occur when a weakened blood vessel ruptures, causing bleeding within or around the brain. This bleeding can put pressure on surrounding brain tissues, leading to cell death.
Symptoms of cerebral infarction depend on the location and extent of the affected brain tissue but may include sudden weakness or numbness in the face, arm, or leg; difficulty speaking or understanding speech; vision problems; loss of balance or coordination; and severe headache with no known cause. Immediate medical attention is crucial for proper diagnosis and treatment to minimize potential long-term damage or disability.
Acetanilides are a group of chemical compounds that consist of an acetic acid molecule (CH3COO-) linked to aniline (C6H5NH2) through an amide bond (-CONH-). The most well-known member of this class is acetanilide itself (N-phenylacetamide, C8H9NO), which has been used historically as a pain reliever and fever reducer. However, its use in medicine has largely been abandoned due to the discovery of serious side effects, including the potential for causing methemoglobinemia, a condition that can lead to tissue hypoxia and even death.
Acetanilides have also been used as intermediates in the synthesis of other chemical compounds, such as dyes and pharmaceuticals. Some derivatives of acetanilide continue to be used in medicine today, including certain antipyretic and analgesic agents. However, these drugs are carefully designed and tested to minimize the risk of adverse effects associated with acetanilide itself.
The brain is the central organ of the nervous system, responsible for receiving and processing sensory information, regulating vital functions, and controlling behavior, movement, and cognition. It is divided into several distinct regions, each with specific functions:
1. Cerebrum: The largest part of the brain, responsible for higher cognitive functions such as thinking, learning, memory, language, and perception. It is divided into two hemispheres, each controlling the opposite side of the body.
2. Cerebellum: Located at the back of the brain, it is responsible for coordinating muscle movements, maintaining balance, and fine-tuning motor skills.
3. Brainstem: Connects the cerebrum and cerebellum to the spinal cord, controlling vital functions such as breathing, heart rate, and blood pressure. It also serves as a relay center for sensory information and motor commands between the brain and the rest of the body.
4. Diencephalon: A region that includes the thalamus (a major sensory relay station) and hypothalamus (regulates hormones, temperature, hunger, thirst, and sleep).
5. Limbic system: A group of structures involved in emotional processing, memory formation, and motivation, including the hippocampus, amygdala, and cingulate gyrus.
The brain is composed of billions of interconnected neurons that communicate through electrical and chemical signals. It is protected by the skull and surrounded by three layers of membranes called meninges, as well as cerebrospinal fluid that provides cushioning and nutrients.
A dose-response relationship in the context of drugs refers to the changes in the effects or symptoms that occur as the dose of a drug is increased or decreased. Generally, as the dose of a drug is increased, the severity or intensity of its effects also increases. Conversely, as the dose is decreased, the effects of the drug become less severe or may disappear altogether.
The dose-response relationship is an important concept in pharmacology and toxicology because it helps to establish the safe and effective dosage range for a drug. By understanding how changes in the dose of a drug affect its therapeutic and adverse effects, healthcare providers can optimize treatment plans for their patients while minimizing the risk of harm.
The dose-response relationship is typically depicted as a curve that shows the relationship between the dose of a drug and its effect. The shape of the curve may vary depending on the drug and the specific effect being measured. Some drugs may have a steep dose-response curve, meaning that small changes in the dose can result in large differences in the effect. Other drugs may have a more gradual dose-response curve, where larger changes in the dose are needed to produce significant effects.
In addition to helping establish safe and effective dosages, the dose-response relationship is also used to evaluate the potential therapeutic benefits and risks of new drugs during clinical trials. By systematically testing different doses of a drug in controlled studies, researchers can identify the optimal dosage range for the drug and assess its safety and efficacy.
A hindlimb, also known as a posterior limb, is one of the pair of extremities that are located distally to the trunk in tetrapods (four-legged vertebrates) and include mammals, birds, reptiles, and amphibians. In humans and other primates, hindlimbs are equivalent to the lower limbs, which consist of the thigh, leg, foot, and toes.
The primary function of hindlimbs is locomotion, allowing animals to move from one place to another. However, they also play a role in other activities such as balance, support, and communication. In humans, the hindlimbs are responsible for weight-bearing, standing, walking, running, and jumping.
In medical terminology, the term "hindlimb" is not commonly used to describe human anatomy. Instead, healthcare professionals use terms like lower limbs or lower extremities to refer to the same region of the body. However, in comparative anatomy and veterinary medicine, the term hindlimb is still widely used to describe the corresponding structures in non-human animals.
Regional blood flow (RBF) refers to the rate at which blood flows through a specific region or organ in the body, typically expressed in milliliters per minute per 100 grams of tissue (ml/min/100g). It is an essential physiological parameter that reflects the delivery of oxygen and nutrients to tissues while removing waste products. RBF can be affected by various factors such as metabolic demands, neural regulation, hormonal influences, and changes in blood pressure or vascular resistance. Measuring RBF is crucial for understanding organ function, diagnosing diseases, and evaluating the effectiveness of treatments.
The double-blind method is a study design commonly used in research, including clinical trials, to minimize bias and ensure the objectivity of results. In this approach, both the participants and the researchers are unaware of which group the participants are assigned to, whether it be the experimental group or the control group. This means that neither the participants nor the researchers know who is receiving a particular treatment or placebo, thus reducing the potential for bias in the evaluation of outcomes. The assignment of participants to groups is typically done by a third party not involved in the study, and the codes are only revealed after all data have been collected and analyzed.
Artificial cardiac pacing is a medical procedure that involves the use of an artificial device to regulate and stimulate the contraction of the heart muscle. This is often necessary when the heart's natural pacemaker, the sinoatrial node, is not functioning properly and the heart is beating too slowly or irregularly.
The artificial pacemaker consists of a small generator that produces electrical impulses and leads that are positioned in the heart to transmit the impulses. The generator is typically implanted just under the skin in the chest, while the leads are inserted into the heart through a vein.
There are different types of artificial cardiac pacing systems, including single-chamber pacemakers, which stimulate either the right atrium or right ventricle, and dual-chamber pacemakers, which stimulate both chambers of the heart. Some pacemakers also have additional features that allow them to respond to changes in the body's needs, such as during exercise or sleep.
Artificial cardiac pacing is a safe and effective treatment for many people with abnormal heart rhythms, and it can significantly improve their quality of life and longevity.
Analysis of Variance (ANOVA) is a statistical technique used to compare the means of two or more groups and determine whether there are any significant differences between them. It is a way to analyze the variance in a dataset to determine whether the variability between groups is greater than the variability within groups, which can indicate that the groups are significantly different from one another.
ANOVA is based on the concept of partitioning the total variance in a dataset into two components: variance due to differences between group means (also known as "between-group variance") and variance due to differences within each group (also known as "within-group variance"). By comparing these two sources of variance, ANOVA can help researchers determine whether any observed differences between groups are statistically significant, or whether they could have occurred by chance.
ANOVA is a widely used technique in many areas of research, including biology, psychology, engineering, and business. It is often used to compare the means of two or more experimental groups, such as a treatment group and a control group, to determine whether the treatment had a significant effect. ANOVA can also be used to compare the means of different populations or subgroups within a population, to identify any differences that may exist between them.
Isosorbide dinitrate is a medication that belongs to a class of drugs called nitrates. It is primarily used in the prevention and treatment of angina pectoris, which is chest pain caused by reduced blood flow to the heart muscle.
The medical definition of Isosorbide dinitrate is:
A soluble nitrate ester used in the prevention and treatment of anginal attacks. It acts by dilating coronary and peripheral arteries and veins, thereby reducing cardiac workload and increasing oxygen delivery to the heart muscle. Its therapeutic effects are attributed to its conversion to nitric oxide, a potent vasodilator, in the body. Isosorbide dinitrate is available in various forms, including tablets, capsules, and oral solutions, and is typically taken 2-3 times daily for optimal effect.
Microcirculation is the circulation of blood in the smallest blood vessels, including arterioles, venules, and capillaries. It's responsible for the delivery of oxygen and nutrients to the tissues and the removal of waste products. The microcirculation plays a crucial role in maintaining tissue homeostasis and is regulated by various physiological mechanisms such as autonomic nervous system activity, local metabolic factors, and hormones.
Impairment of microcirculation can lead to tissue hypoxia, inflammation, and organ dysfunction, which are common features in several diseases, including diabetes, hypertension, sepsis, and ischemia-reperfusion injury. Therefore, understanding the structure and function of the microcirculation is essential for developing new therapeutic strategies to treat these conditions.
Oxidative stress is defined as an imbalance between the production of reactive oxygen species (free radicals) and the body's ability to detoxify them or repair the damage they cause. This imbalance can lead to cellular damage, oxidation of proteins, lipids, and DNA, disruption of cellular functions, and activation of inflammatory responses. Prolonged or excessive oxidative stress has been linked to various health conditions, including cancer, cardiovascular diseases, neurodegenerative disorders, and aging-related diseases.
Prognosis is a medical term that refers to the prediction of the likely outcome or course of a disease, including the chances of recovery or recurrence, based on the patient's symptoms, medical history, physical examination, and diagnostic tests. It is an important aspect of clinical decision-making and patient communication, as it helps doctors and patients make informed decisions about treatment options, set realistic expectations, and plan for future care.
Prognosis can be expressed in various ways, such as percentages, categories (e.g., good, fair, poor), or survival rates, depending on the nature of the disease and the available evidence. However, it is important to note that prognosis is not an exact science and may vary depending on individual factors, such as age, overall health status, and response to treatment. Therefore, it should be used as a guide rather than a definitive forecast.
Radiopharmaceuticals are defined as pharmaceutical preparations that contain radioactive isotopes and are used for diagnosis or therapy in nuclear medicine. These compounds are designed to interact specifically with certain biological targets, such as cells, tissues, or organs, and emit radiation that can be detected and measured to provide diagnostic information or used to destroy abnormal cells or tissue in therapeutic applications.
The radioactive isotopes used in radiopharmaceuticals have carefully controlled half-lives, which determine how long they remain radioactive and how long the pharmaceutical preparation remains effective. The choice of radioisotope depends on the intended use of the radiopharmaceutical, as well as factors such as its energy, range of emission, and chemical properties.
Radiopharmaceuticals are used in a wide range of medical applications, including imaging, cancer therapy, and treatment of other diseases and conditions. Examples of radiopharmaceuticals include technetium-99m for imaging the heart, lungs, and bones; iodine-131 for treating thyroid cancer; and samarium-153 for palliative treatment of bone metastases.
The use of radiopharmaceuticals requires specialized training and expertise in nuclear medicine, as well as strict adherence to safety protocols to minimize radiation exposure to patients and healthcare workers.
Follow-up studies are a type of longitudinal research that involve repeated observations or measurements of the same variables over a period of time, in order to understand their long-term effects or outcomes. In medical context, follow-up studies are often used to evaluate the safety and efficacy of medical treatments, interventions, or procedures.
In a typical follow-up study, a group of individuals (called a cohort) who have received a particular treatment or intervention are identified and then followed over time through periodic assessments or data collection. The data collected may include information on clinical outcomes, adverse events, changes in symptoms or functional status, and other relevant measures.
The results of follow-up studies can provide important insights into the long-term benefits and risks of medical interventions, as well as help to identify factors that may influence treatment effectiveness or patient outcomes. However, it is important to note that follow-up studies can be subject to various biases and limitations, such as loss to follow-up, recall bias, and changes in clinical practice over time, which must be carefully considered when interpreting the results.
Acidosis is a medical condition that occurs when there is an excess accumulation of acid in the body or when the body loses its ability to effectively regulate the pH level of the blood. The normal pH range of the blood is slightly alkaline, between 7.35 and 7.45. When the pH falls below 7.35, it is called acidosis.
Acidosis can be caused by various factors, including impaired kidney function, respiratory problems, diabetes, severe dehydration, alcoholism, and certain medications or toxins. There are two main types of acidosis: metabolic acidosis and respiratory acidosis.
Metabolic acidosis occurs when the body produces too much acid or is unable to eliminate it effectively. This can be caused by conditions such as diabetic ketoacidosis, lactic acidosis, kidney failure, and ingestion of certain toxins.
Respiratory acidosis, on the other hand, occurs when the lungs are unable to remove enough carbon dioxide from the body, leading to an accumulation of acid. This can be caused by conditions such as chronic obstructive pulmonary disease (COPD), asthma, and sedative overdose.
Symptoms of acidosis may include fatigue, shortness of breath, confusion, headache, rapid heartbeat, and in severe cases, coma or even death. Treatment for acidosis depends on the underlying cause and may include medications, oxygen therapy, fluid replacement, and dialysis.
Anoxia is a medical condition that refers to the absence or complete lack of oxygen supply in the body or a specific organ, tissue, or cell. This can lead to serious health consequences, including damage or death of cells and tissues, due to the vital role that oxygen plays in supporting cellular metabolism and energy production.
Anoxia can occur due to various reasons, such as respiratory failure, cardiac arrest, severe blood loss, carbon monoxide poisoning, or high altitude exposure. Prolonged anoxia can result in hypoxic-ischemic encephalopathy, a serious condition that can cause brain damage and long-term neurological impairments.
Medical professionals use various diagnostic tests, such as blood gas analysis, pulse oximetry, and electroencephalography (EEG), to assess oxygen levels in the body and diagnose anoxia. Treatment for anoxia typically involves addressing the underlying cause, providing supplemental oxygen, and supporting vital functions, such as breathing and circulation, to prevent further damage.
Stroke volume is a term used in cardiovascular physiology and medicine. It refers to the amount of blood that is pumped out of the left ventricle of the heart during each contraction (systole). Specifically, it is the difference between the volume of blood in the left ventricle at the end of diastole (when the ventricle is filled with blood) and the volume at the end of systole (when the ventricle has contracted and ejected its contents into the aorta).
Stroke volume is an important measure of heart function, as it reflects the ability of the heart to pump blood effectively to the rest of the body. A low stroke volume may indicate that the heart is not pumping efficiently, while a high stroke volume may suggest that the heart is working too hard. Stroke volume can be affected by various factors, including heart disease, high blood pressure, and physical fitness level.
The formula for calculating stroke volume is:
Stroke Volume = End-Diastolic Volume - End-Systolic Volume
Where end-diastolic volume (EDV) is the volume of blood in the left ventricle at the end of diastole, and end-systolic volume (ESV) is the volume of blood in the left ventricle at the end of systole.
A Severity of Illness Index is a measurement tool used in healthcare to assess the severity of a patient's condition and the risk of mortality or other adverse outcomes. These indices typically take into account various physiological and clinical variables, such as vital signs, laboratory values, and co-morbidities, to generate a score that reflects the patient's overall illness severity.
Examples of Severity of Illness Indices include the Acute Physiology and Chronic Health Evaluation (APACHE) system, the Simplified Acute Physiology Score (SAPS), and the Mortality Probability Model (MPM). These indices are often used in critical care settings to guide clinical decision-making, inform prognosis, and compare outcomes across different patient populations.
It is important to note that while these indices can provide valuable information about a patient's condition, they should not be used as the sole basis for clinical decision-making. Rather, they should be considered in conjunction with other factors, such as the patient's overall clinical presentation, treatment preferences, and goals of care.
The endothelium is a thin layer of simple squamous epithelial cells that lines the interior surface of blood vessels, lymphatic vessels, and heart chambers. The vascular endothelium, specifically, refers to the endothelial cells that line the blood vessels. These cells play a crucial role in maintaining vascular homeostasis by regulating vasomotor tone, coagulation, platelet activation, inflammation, and permeability of the vessel wall. They also contribute to the growth and repair of the vascular system and are involved in various pathological processes such as atherosclerosis, hypertension, and diabetes.
Glyburide is a medication that falls under the class of drugs known as sulfonylureas. It is primarily used to manage type 2 diabetes by lowering blood sugar levels. Glyburide works by stimulating the release of insulin from the pancreas, thereby increasing the amount of insulin available in the body to help glucose enter cells and decrease the level of glucose in the bloodstream.
The medical definition of Glyburide is:
A second-generation sulfonylurea antidiabetic drug (oral hypoglycemic) used in the management of type 2 diabetes mellitus. It acts by stimulating pancreatic beta cells to release insulin and increases peripheral glucose uptake and utilization, thereby reducing blood glucose levels. Glyburide may also decrease glucose production in the liver.
It is important to note that Glyburide should be used as part of a comprehensive diabetes management plan that includes proper diet, exercise, regular monitoring of blood sugar levels, and other necessary lifestyle modifications. As with any medication, it can have side effects and potential interactions with other drugs, so it should only be taken under the supervision of a healthcare provider.
Tissue survival, in the context of medical and surgical sciences, refers to the ability of tissues to maintain their structural and functional integrity after being subjected to various stressors such as injury, surgery, ischemia (restriction in blood supply), or disease. The maintenance of tissue survival is crucial for ensuring proper healing, reducing the risk of complications, and preserving organ function.
Factors that contribute to tissue survival include adequate blood flow, sufficient oxygen and nutrient supply, removal of waste products, maintenance of a healthy cellular environment (pH, temperature, etc.), and minimal exposure to harmful substances or damaging agents. In some cases, therapeutic interventions such as hypothermia, pharmacological treatments, or tissue engineering strategies may be employed to enhance tissue survival in challenging clinical scenarios.
A "knockout" mouse is a genetically engineered mouse in which one or more genes have been deleted or "knocked out" using molecular biology techniques. This allows researchers to study the function of specific genes and their role in various biological processes, as well as potential associations with human diseases. The mice are generated by introducing targeted DNA modifications into embryonic stem cells, which are then used to create a live animal. Knockout mice have been widely used in biomedical research to investigate gene function, disease mechanisms, and potential therapeutic targets.
Malondialdehyde (MDA) is a naturally occurring organic compound that is formed as a byproduct of lipid peroxidation, a process in which free radicals or reactive oxygen species react with polyunsaturated fatty acids. MDA is a highly reactive aldehyde that can modify proteins, DNA, and other biomolecules, leading to cellular damage and dysfunction. It is often used as a marker of oxidative stress in biological systems and has been implicated in the development of various diseases, including cancer, cardiovascular disease, and neurodegenerative disorders.
A chronic disease is a long-term medical condition that often progresses slowly over a period of years and requires ongoing management and care. These diseases are typically not fully curable, but symptoms can be managed to improve quality of life. Common chronic diseases include heart disease, stroke, cancer, diabetes, arthritis, and COPD (chronic obstructive pulmonary disease). They are often associated with advanced age, although they can also affect children and younger adults. Chronic diseases can have significant impacts on individuals' physical, emotional, and social well-being, as well as on healthcare systems and society at large.
Cardiac catheterization is a medical procedure used to diagnose and treat cardiovascular conditions. In this procedure, a thin, flexible tube called a catheter is inserted into a blood vessel in the arm or leg and threaded up to the heart. The catheter can be used to perform various diagnostic tests, such as measuring the pressure inside the heart chambers and assessing the function of the heart valves.
Cardiac catheterization can also be used to treat certain cardiovascular conditions, such as narrowed or blocked arteries. In these cases, a balloon or stent may be inserted through the catheter to open up the blood vessel and improve blood flow. This procedure is known as angioplasty or percutaneous coronary intervention (PCI).
Cardiac catheterization is typically performed in a hospital cardiac catheterization laboratory by a team of healthcare professionals, including cardiologists, radiologists, and nurses. The procedure may be done under local anesthesia with sedation or general anesthesia, depending on the individual patient's needs and preferences.
Overall, cardiac catheterization is a valuable tool in the diagnosis and treatment of various heart conditions, and it can help improve symptoms, reduce complications, and prolong life for many patients.
Cell death is the process by which cells cease to function and eventually die. There are several ways that cells can die, but the two most well-known and well-studied forms of cell death are apoptosis and necrosis.
Apoptosis is a programmed form of cell death that occurs as a normal and necessary process in the development and maintenance of healthy tissues. During apoptosis, the cell's DNA is broken down into small fragments, the cell shrinks, and the membrane around the cell becomes fragmented, allowing the cell to be easily removed by phagocytic cells without causing an inflammatory response.
Necrosis, on the other hand, is a form of cell death that occurs as a result of acute tissue injury or overwhelming stress. During necrosis, the cell's membrane becomes damaged and the contents of the cell are released into the surrounding tissue, causing an inflammatory response.
There are also other forms of cell death, such as autophagy, which is a process by which cells break down their own organelles and proteins to recycle nutrients and maintain energy homeostasis, and pyroptosis, which is a form of programmed cell death that occurs in response to infection and involves the activation of inflammatory caspases.
Cell death is an important process in many physiological and pathological processes, including development, tissue homeostasis, and disease. Dysregulation of cell death can contribute to the development of various diseases, including cancer, neurodegenerative disorders, and autoimmune diseases.
Vascular surgical procedures are operations that are performed to treat conditions and diseases related to the vascular system, which includes the arteries, veins, and capillaries. These procedures can be invasive or minimally invasive and are often used to treat conditions such as peripheral artery disease, carotid artery stenosis, aortic aneurysms, and venous insufficiency.
Some examples of vascular surgical procedures include:
* Endarterectomy: a procedure to remove plaque buildup from the inside of an artery
* Bypass surgery: creating a new path for blood to flow around a blocked or narrowed artery
* Angioplasty and stenting: using a balloon to open a narrowed artery and placing a stent to keep it open
* Aneurysm repair: surgically repairing an aneurysm, a weakened area in the wall of an artery that has bulged out and filled with blood
* Embolectomy: removing a blood clot from a blood vessel
* Thrombectomy: removing a blood clot from a vein
These procedures are typically performed by vascular surgeons, who are trained in the diagnosis and treatment of vascular diseases.
Enzyme inhibitors are substances that bind to an enzyme and decrease its activity, preventing it from catalyzing a chemical reaction in the body. They can work by several mechanisms, including blocking the active site where the substrate binds, or binding to another site on the enzyme to change its shape and prevent substrate binding. Enzyme inhibitors are often used as drugs to treat various medical conditions, such as high blood pressure, abnormal heart rhythms, and bacterial infections. They can also be found naturally in some foods and plants, and can be used in research to understand enzyme function and regulation.
An animal model in medicine refers to the use of non-human animals in experiments to understand, predict, and test responses and effects of various biological and chemical interactions that may also occur in humans. These models are used when studying complex systems or processes that cannot be easily replicated or studied in human subjects, such as genetic manipulation or exposure to harmful substances. The choice of animal model depends on the specific research question being asked and the similarities between the animal's and human's biological and physiological responses. Examples of commonly used animal models include mice, rats, rabbits, guinea pigs, and non-human primates.
Signal transduction is the process by which a cell converts an extracellular signal, such as a hormone or neurotransmitter, into an intracellular response. This involves a series of molecular events that transmit the signal from the cell surface to the interior of the cell, ultimately resulting in changes in gene expression, protein activity, or metabolism.
The process typically begins with the binding of the extracellular signal to a receptor located on the cell membrane. This binding event activates the receptor, which then triggers a cascade of intracellular signaling molecules, such as second messengers, protein kinases, and ion channels. These molecules amplify and propagate the signal, ultimately leading to the activation or inhibition of specific cellular responses.
Signal transduction pathways are highly regulated and can be modulated by various factors, including other signaling molecules, post-translational modifications, and feedback mechanisms. Dysregulation of these pathways has been implicated in a variety of diseases, including cancer, diabetes, and neurological disorders.
Systole is the phase of the cardiac cycle during which the heart muscle contracts to pump blood out of the heart. Specifically, it refers to the contraction of the ventricles, the lower chambers of the heart. This is driven by the action of the electrical conduction system of the heart, starting with the sinoatrial node and passing through the atrioventricular node and bundle branches to the Purkinje fibers.
During systole, the pressure within the ventricles increases as they contract, causing the aortic and pulmonary valves to open and allowing blood to be ejected into the systemic and pulmonary circulations, respectively. The duration of systole is typically shorter than that of diastole, the phase during which the heart muscle relaxes and the chambers fill with blood.
In clinical settings, the terms "systolic" and "diastolic" are often used to describe blood pressure measurements, with the former referring to the pressure exerted on the artery walls when the ventricles contract and eject blood, and the latter referring to the pressure when the ventricles are relaxed and filling with blood.
Cardiac-gated single-photon emission computer-assisted tomography (SPECT) is a medical imaging technique used to evaluate the function and perfusion of the heart. This technique combines the principles of cardiac gating, SPECT imaging, and computed tomography (CT) to produce detailed, three-dimensional images of the heart.
In this procedure, a small amount of radioactive tracer is injected into the patient's bloodstream. The tracer accumulates in the heart muscle according to its blood flow, allowing for the assessment of regional myocardial perfusion and function. A specialized gamma camera then captures images of the distribution of this tracer within the heart.
Cardiac gating is a technique that synchronizes image acquisition with the patient's electrocardiogram (ECG) signal, ensuring that data are collected only during specific phases of the cardiac cycle. This allows for the accurate assessment of regional wall motion and thickening, which can help identify areas of the heart affected by ischemia or scarring.
The acquired images are then reconstructed using computer algorithms to create detailed, three-dimensional representations of the heart's structure and function. These images can aid in the diagnosis and management of various cardiac conditions, such as coronary artery disease, cardiomyopathies, and heart failure.
Myocardial revascularization is a medical term that refers to the restoration of blood flow to the heart muscle (myocardium), typically through a surgical or interventional procedure. This is often performed in patients with coronary artery disease, where the buildup of plaque in the coronary arteries restricts blood flow to the heart muscle, causing symptoms such as chest pain (angina) or shortness of breath, and increasing the risk of a heart attack (myocardial infarction).
There are two main types of myocardial revascularization:
1. Coronary artery bypass grafting (CABG): This is a surgical procedure in which a healthy blood vessel from another part of the body is used to create a detour around the blocked or narrowed coronary artery, allowing blood to flow more freely to the heart muscle.
2. Percutaneous coronary intervention (PCI), also known as angioplasty and stenting: This is a minimally invasive procedure in which a thin catheter is inserted into an artery in the groin or arm and threaded up to the blocked or narrowed coronary artery. A balloon is then inflated to widen the artery, and a stent may be placed to keep it open.
Both procedures aim to improve symptoms, reduce the risk of heart attack, and prolong survival in appropriately selected patients with coronary artery disease.
Vectorcardiography (VCG) is a type of graphical recording that depicts the vector magnitude and direction of the electrical activity of the heart over time. It provides a three-dimensional view of the electrical activation pattern of the heart, as opposed to the one-dimensional view offered by a standard electrocardiogram (ECG).
In VCG, the electrical potentials are recorded using a special array of electrodes placed on the body surface. These potentials are then mathematically converted into vectors and plotted on a vector loop or a series of loops that represent different planes of the heart's electrical activity. The resulting tracing provides information about the magnitude, direction, and timing of the electrical activation of the heart, which can be helpful in diagnosing various cardiac arrhythmias, ischemic heart disease, and other cardiac conditions.
Overall, vectorcardiography offers a more detailed and comprehensive view of the heart's electrical activity than traditional ECG, making it a valuable tool in clinical cardiology.
Physiological monitoring is the continuous or intermittent observation and measurement of various body functions or parameters in a patient, with the aim of evaluating their health status, identifying any abnormalities or changes, and guiding clinical decision-making and treatment. This may involve the use of specialized medical equipment, such as cardiac monitors, pulse oximeters, blood pressure monitors, and capnographs, among others. The data collected through physiological monitoring can help healthcare professionals assess the effectiveness of treatments, detect complications early, and make timely adjustments to patient care plans.
The sympathetic nervous system (SNS) is a part of the autonomic nervous system that operates largely below the level of consciousness, and it functions to produce appropriate physiological responses to perceived danger. It's often associated with the "fight or flight" response. The SNS uses nerve impulses to stimulate target organs, causing them to speed up (e.g., increased heart rate), prepare for action, or otherwise respond to stressful situations.
The sympathetic nervous system is activated due to stressful emotional or physical situations and it prepares the body for immediate actions. It dilates the pupils, increases heart rate and blood pressure, accelerates breathing, and slows down digestion. The primary neurotransmitter involved in this system is norepinephrine (also known as noradrenaline).
Energy metabolism is the process by which living organisms produce and consume energy to maintain life. It involves a series of chemical reactions that convert nutrients from food, such as carbohydrates, fats, and proteins, into energy in the form of adenosine triphosphate (ATP).
The process of energy metabolism can be divided into two main categories: catabolism and anabolism. Catabolism is the breakdown of nutrients to release energy, while anabolism is the synthesis of complex molecules from simpler ones using energy.
There are three main stages of energy metabolism: glycolysis, the citric acid cycle (also known as the Krebs cycle), and oxidative phosphorylation. Glycolysis occurs in the cytoplasm of the cell and involves the breakdown of glucose into pyruvate, producing a small amount of ATP and nicotinamide adenine dinucleotide (NADH). The citric acid cycle takes place in the mitochondria and involves the further breakdown of pyruvate to produce more ATP, NADH, and carbon dioxide. Oxidative phosphorylation is the final stage of energy metabolism and occurs in the inner mitochondrial membrane. It involves the transfer of electrons from NADH and other electron carriers to oxygen, which generates a proton gradient across the membrane. This gradient drives the synthesis of ATP, producing the majority of the cell's energy.
Overall, energy metabolism is a complex and essential process that allows organisms to grow, reproduce, and maintain their bodily functions. Disruptions in energy metabolism can lead to various diseases, including diabetes, obesity, and neurodegenerative disorders.
Coronary occlusion is the medical term used to describe a complete blockage in one or more of the coronary arteries, which supply oxygenated blood to the heart muscle. This blockage is usually caused by the buildup of fatty deposits, called plaques, inside the artery walls, a condition known as atherosclerosis. Over time, these plaques can rupture, leading to the formation of blood clots that completely obstruct the flow of blood through the coronary artery.
Coronary occlusion can lead to serious complications, such as a heart attack (myocardial infarction), angina (chest pain), or even sudden cardiac death, depending on the severity and duration of the blockage. Immediate medical attention is required in case of coronary occlusion to restore blood flow to the affected areas of the heart and prevent further damage. Treatment options may include medications, minimally invasive procedures like angioplasty and stenting, or surgical interventions such as coronary artery bypass grafting (CABG).
Diastole is the phase of the cardiac cycle during which the heart muscle relaxes and the chambers of the heart fill with blood. It follows systole, the phase in which the heart muscle contracts and pumps blood out to the body. In a normal resting adult, diastole lasts for approximately 0.4-0.5 seconds during each heartbeat. The period of diastole is divided into two phases: early diastole and late diastole. During early diastole, the ventricles fill with blood due to the pressure difference between the atria and ventricles. During late diastole, the atrioventricular valves close, and the ventricles continue to fill with blood due to the relaxation of the ventricular muscle and the compliance of the ventricular walls. The duration and pressure changes during diastole are important for maintaining adequate cardiac output and blood flow to the body.
Cardioplegic solutions are specially formulated liquids used in medical procedures to induce cardiac arrest and protect the heart muscle during open-heart surgery. These solutions typically contain a combination of electrolytes, such as potassium and magnesium, which stop the heart from beating by interrupting its electrical activity. They may also include energy substrates, buffers, and other components to maintain the health and function of the heart cells during the period of arrest. The specific formulation of cardioplegic solutions can vary depending on the needs of the patient and the preferences of the medical team.
Ligation, in the context of medical terminology, refers to the process of tying off a part of the body, usually blood vessels or tissue, with a surgical suture or another device. The goal is to stop the flow of fluids such as blood or other substances within the body. It is commonly used during surgeries to control bleeding or to block the passage of fluids, gases, or solids in various parts of the body.
Microspheres are tiny, spherical particles that range in size from 1 to 1000 micrometers in diameter. They are made of biocompatible and biodegradable materials such as polymers, glass, or ceramics. In medical terms, microspheres have various applications, including drug delivery systems, medical imaging, and tissue engineering.
In drug delivery, microspheres can be used to encapsulate drugs and release them slowly over time, improving the efficacy of the treatment while reducing side effects. They can also be used for targeted drug delivery, where the microspheres are designed to accumulate in specific tissues or organs.
In medical imaging, microspheres can be labeled with radioactive isotopes or magnetic materials and used as contrast agents to enhance the visibility of tissues or organs during imaging procedures such as X-ray, CT, MRI, or PET scans.
In tissue engineering, microspheres can serve as a scaffold for cell growth and differentiation, promoting the regeneration of damaged tissues or organs. Overall, microspheres have great potential in various medical applications due to their unique properties and versatility.
Risk assessment in the medical context refers to the process of identifying, evaluating, and prioritizing risks to patients, healthcare workers, or the community related to healthcare delivery. It involves determining the likelihood and potential impact of adverse events or hazards, such as infectious diseases, medication errors, or medical devices failures, and implementing measures to mitigate or manage those risks. The goal of risk assessment is to promote safe and high-quality care by identifying areas for improvement and taking action to minimize harm.
Histamine H3 receptors are a type of G protein-coupled receptor (GPCR) that are widely distributed throughout the central and peripheral nervous system. They are activated by the neurotransmitter histamine and function as autoreceptors, inhibiting the release of histamine from presynaptic nerve terminals. Histamine H3 receptors also modulate the activity of other neurotransmitters, such as acetylcholine, dopamine, norepinephrine, and serotonin, by regulating their synthesis, release, and uptake.
Histamine H3 receptors have been identified as potential targets for the treatment of various neurological and psychiatric disorders, including sleep disorders, attention deficit hyperactivity disorder (ADHD), schizophrenia, and drug addiction. Antagonists or inverse agonists of Histamine H3 receptors may enhance the release of neurotransmitters in the brain, leading to improved cognitive function, mood regulation, and reward processing. However, further research is needed to fully understand the therapeutic potential and safety profile of Histamine H3 receptor modulators.
Postoperative complications refer to any unfavorable condition or event that occurs during the recovery period after a surgical procedure. These complications can vary in severity and may include, but are not limited to:
1. Infection: This can occur at the site of the incision or inside the body, such as pneumonia or urinary tract infection.
2. Bleeding: Excessive bleeding (hemorrhage) can lead to a drop in blood pressure and may require further surgical intervention.
3. Blood clots: These can form in the deep veins of the legs (deep vein thrombosis) and can potentially travel to the lungs (pulmonary embolism).
4. Wound dehiscence: This is when the surgical wound opens up, which can lead to infection and further complications.
5. Pulmonary issues: These include atelectasis (collapsed lung), pneumonia, or respiratory failure.
6. Cardiovascular problems: These include abnormal heart rhythms (arrhythmias), heart attack, or stroke.
7. Renal failure: This can occur due to various reasons such as dehydration, blood loss, or the use of certain medications.
8. Pain management issues: Inadequate pain control can lead to increased stress, anxiety, and decreased mobility.
9. Nausea and vomiting: These can be caused by anesthesia, opioid pain medication, or other factors.
10. Delirium: This is a state of confusion and disorientation that can occur in the elderly or those with certain medical conditions.
Prompt identification and management of these complications are crucial to ensure the best possible outcome for the patient.
"Inbred strains of rats" are genetically identical rodents that have been produced through many generations of brother-sister mating. This results in a high degree of homozygosity, where the genes at any particular locus in the genome are identical in all members of the strain.
Inbred strains of rats are widely used in biomedical research because they provide a consistent and reproducible genetic background for studying various biological phenomena, including the effects of drugs, environmental factors, and genetic mutations on health and disease. Additionally, inbred strains can be used to create genetically modified models of human diseases by introducing specific mutations into their genomes.
Some commonly used inbred strains of rats include the Wistar Kyoto (WKY), Sprague-Dawley (SD), and Fischer 344 (F344) rat strains. Each strain has its own unique genetic characteristics, making them suitable for different types of research.
Perioperative care is a multidisciplinary approach to the management of patients before, during, and after surgery with the goal of optimizing outcomes and minimizing complications. It encompasses various aspects such as preoperative evaluation and preparation, intraoperative monitoring and management, and postoperative recovery and rehabilitation. The perioperative period begins when a decision is made to pursue surgical intervention and ends when the patient has fully recovered from the procedure. This care is typically provided by a team of healthcare professionals including anesthesiologists, surgeons, nurses, physical therapists, and other specialists as needed.
Potassium channels are membrane proteins that play a crucial role in regulating the electrical excitability of cells, including cardiac, neuronal, and muscle cells. These channels facilitate the selective passage of potassium ions (K+) across the cell membrane, maintaining the resting membrane potential and shaping action potentials. They are composed of four or six subunits that assemble to form a central pore through which potassium ions move down their electrochemical gradient. Potassium channels can be modulated by various factors such as voltage, ligands, mechanical stimuli, or temperature, allowing cells to fine-tune their electrical properties and respond to different physiological demands. Dysfunction of potassium channels has been implicated in several diseases, including cardiac arrhythmias, epilepsy, and neurodegenerative disorders.
Norepinephrine, also known as noradrenaline, is a neurotransmitter and a hormone that is primarily produced in the adrenal glands and is released into the bloodstream in response to stress or physical activity. It plays a crucial role in the "fight-or-flight" response by preparing the body for action through increasing heart rate, blood pressure, respiratory rate, and glucose availability.
As a neurotransmitter, norepinephrine is involved in regulating various functions of the nervous system, including attention, perception, motivation, and arousal. It also plays a role in modulating pain perception and responding to stressful or emotional situations.
In medical settings, norepinephrine is used as a vasopressor medication to treat hypotension (low blood pressure) that can occur during septic shock, anesthesia, or other critical illnesses. It works by constricting blood vessels and increasing heart rate, which helps to improve blood pressure and perfusion of vital organs.
Mesenteric vascular occlusion refers to the blockage or obstruction of the blood vessels that supply the intestines, specifically the mesenteric arteries and veins. This condition can result in insufficient blood flow to the intestines, leading to ischemia (inadequate oxygen supply) and potential necrosis (tissue death).
There are two primary types of mesenteric vascular occlusion:
1. Mesenteric arterial occlusion: This occurs when the mesenteric artery, which carries oxygenated blood from the heart to the intestines, becomes blocked. The most common causes include atherosclerosis (plaque buildup in the arteries), embolism (a clot or particle that travels from another part of the body and lodges in the artery), and thrombosis (a blood clot forming directly in the artery).
2. Mesenteric venous occlusion: This happens when the mesenteric vein, which returns deoxygenated blood from the intestines to the heart, becomes obstructed. The most common causes include thrombophlebitis (inflammation and clot formation in the vein), tumors, or abdominal trauma.
Symptoms of mesenteric vascular occlusion may include severe abdominal pain, nausea, vomiting, diarrhea, and bloody stools. Rapid diagnosis and treatment are crucial to prevent intestinal tissue damage and potential life-threatening complications such as sepsis or shock. Treatment options typically involve surgical intervention, anticoagulation therapy, or endovascular procedures to restore blood flow.
Cardiovascular models are simplified representations or simulations of the human cardiovascular system used in medical research, education, and training. These models can be physical, computational, or mathematical and are designed to replicate various aspects of the heart, blood vessels, and blood flow. They can help researchers study the structure and function of the cardiovascular system, test new treatments and interventions, and train healthcare professionals in diagnostic and therapeutic techniques.
Physical cardiovascular models may include artificial hearts, blood vessels, or circulation systems made from materials such as plastic, rubber, or silicone. These models can be used to study the mechanics of heart valves, the effects of different surgical procedures, or the impact of various medical devices on blood flow.
Computational and mathematical cardiovascular models use algorithms and equations to simulate the behavior of the cardiovascular system. These models may range from simple representations of a single heart chamber to complex simulations of the entire circulatory system. They can be used to study the electrical activity of the heart, the biomechanics of blood flow, or the distribution of drugs in the body.
Overall, cardiovascular models play an essential role in advancing our understanding of the human body and improving patient care.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
'Sus scrofa' is the scientific name for the wild boar, a species of suid that is native to much of Eurasia and North Africa. It is not a medical term or concept. If you have any questions related to medical terminology or health-related topics, I would be happy to help with those instead!
Myocardial bridging is a congenital cardiovascular anomaly where a segment of a major epicardial coronary artery, usually the left anterior descending (LAD) coronary artery, passes between the muscle fibers of the heart (myocardium) instead of running over the surface. This results in the coronary artery being compressed or "bridged" by the contracting myocardium during systole (contraction phase of the heart cycle), which can lead to a decrease in blood flow to the affected area of the heart muscle.
Myocardial bridging is usually asymptomatic and discovered incidentally during coronary angiography or autopsy. However, in some cases, it may cause symptoms such as angina (chest pain), shortness of breath, or arrhythmias (irregular heartbeats) due to the compromised blood flow. The severity of the symptoms depends on the length and depth of the myocardial bridge and the degree of compression during systole.
While myocardial bridging is a benign condition in most cases, it can increase the risk of ischemia (reduced blood supply to the heart muscle) and adverse cardiac events such as myocardial infarction (heart attack) or sudden cardiac death in rare instances. Treatment options for symptomatic myocardial bridging include medications, lifestyle modifications, and invasive procedures such as percutaneous coronary intervention or coronary artery bypass grafting.
In situ nick-end labeling (ISEL, also known as TUNEL) is a technique used in pathology and molecular biology to detect DNA fragmentation, which is a characteristic of apoptotic cells (cells undergoing programmed cell death). The method involves labeling the 3'-hydroxyl termini of double or single stranded DNA breaks in situ (within tissue sections or individual cells) using modified nucleotides that are coupled to a detectable marker, such as a fluorophore or an enzyme. This technique allows for the direct visualization and quantification of apoptotic cells within complex tissues or cell populations.
Intraoperative monitoring (IOM) is the practice of using specialized techniques to monitor physiological functions or neural structures in real-time during surgical procedures. The primary goal of IOM is to provide continuous information about the patient's status and the effects of surgery on neurological function, allowing surgeons to make informed decisions and minimize potential risks.
IOM can involve various methods such as:
1. Electrophysiological monitoring: This includes techniques like somatosensory evoked potentials (SSEP), motor evoked potentials (MEP), and electroencephalography (EEG) to assess the integrity of neural pathways and brain function during surgery.
2. Neuromonitoring: Direct electrical stimulation of nerves or spinal cord structures can help identify critical neuroanatomical structures, evaluate their functional status, and guide surgical interventions.
3. Hemodynamic monitoring: Measuring blood pressure, heart rate, cardiac output, and oxygen saturation helps assess the patient's overall physiological status during surgery.
4. Imaging modalities: Intraoperative imaging techniques like ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI) can provide real-time visualization of anatomical structures and surgical progress.
The specific IOM methods employed depend on the type of surgery, patient characteristics, and potential risks involved. Intraoperative monitoring is particularly crucial in procedures where there is a risk of neurological injury, such as spinal cord or brain surgeries, vascular interventions, or tumor resections near critical neural structures.
Tachycardia is a medical term that refers to an abnormally rapid heart rate, often defined as a heart rate greater than 100 beats per minute in adults. It can occur in either the atria (upper chambers) or ventricles (lower chambers) of the heart. Different types of tachycardia include supraventricular tachycardia (SVT), atrial fibrillation, atrial flutter, and ventricular tachycardia.
Tachycardia can cause various symptoms such as palpitations, shortness of breath, dizziness, lightheadedness, chest discomfort, or syncope (fainting). In some cases, tachycardia may not cause any symptoms and may only be detected during a routine physical examination or medical test.
The underlying causes of tachycardia can vary widely, including heart disease, electrolyte imbalances, medications, illicit drug use, alcohol abuse, smoking, stress, anxiety, and other medical conditions. In some cases, the cause may be unknown. Treatment for tachycardia depends on the underlying cause, type, severity, and duration of the arrhythmia.
The intraoperative period is the phase of surgical treatment that refers to the time during which the surgery is being performed. It begins when the anesthesia is administered and the patient is prepared for the operation, and it ends when the surgery is completed, the anesthesia is discontinued, and the patient is transferred to the recovery room or intensive care unit (ICU).
During the intraoperative period, the surgical team, including surgeons, anesthesiologists, nurses, and other healthcare professionals, work together to carry out the surgical procedure safely and effectively. The anesthesiologist monitors the patient's vital signs, such as heart rate, blood pressure, oxygen saturation, and body temperature, throughout the surgery to ensure that the patient remains stable and does not experience any complications.
The surgeon performs the operation, using various surgical techniques and instruments to achieve the desired outcome. The surgical team also takes measures to prevent infection, control bleeding, and manage pain during and after the surgery.
Overall, the intraoperative period is a critical phase of surgical treatment that requires close collaboration and communication among members of the healthcare team to ensure the best possible outcomes for the patient.
Neurons, also known as nerve cells or neurocytes, are specialized cells that constitute the basic unit of the nervous system. They are responsible for receiving, processing, and transmitting information and signals within the body. Neurons have three main parts: the dendrites, the cell body (soma), and the axon. The dendrites receive signals from other neurons or sensory receptors, while the axon transmits these signals to other neurons, muscles, or glands. The junction between two neurons is called a synapse, where neurotransmitters are released to transmit the signal across the gap (synaptic cleft) to the next neuron. Neurons vary in size, shape, and structure depending on their function and location within the nervous system.
Intra-arterial injection is a type of medical procedure where a medication or contrast agent is delivered directly into an artery. This technique is used for various therapeutic and diagnostic purposes.
For instance, intra-arterial chemotherapy may be used to deliver cancer drugs directly to the site of a tumor, while intra-arterial thrombolysis involves the administration of clot-busting medications to treat arterial blockages caused by blood clots. Intra-arterial injections are also used in diagnostic imaging procedures such as angiography, where a contrast agent is injected into an artery to visualize the blood vessels and identify any abnormalities.
It's important to note that intra-arterial injections require precise placement of the needle or catheter into the artery, and are typically performed by trained medical professionals using specialized equipment.
Mucocutaneous Lymph Node Syndrome is also known as Kawasaki Disease. It is a type of vasculitis that primarily affects young children, usually those under the age of 5. The disease is named after Dr. Tomisaku Kawasaki, who first described it in Japan in 1967.
The condition is characterized by inflammation of the mucous membranes (mucosa), skin (cutaneous), and lymph nodes. The symptoms typically include fever, rash, red eyes, swollen lips and tongue, strawberry tongue, and swollen lymph nodes in the neck. In addition, children with Kawasaki disease may also experience joint pain, diarrhea, vomiting, and abdominal pain.
In severe cases, Kawasaki disease can lead to complications such as coronary artery aneurysms, which can increase the risk of heart attacks and other cardiovascular problems. The exact cause of Kawasaki disease is unknown, but it is thought to be triggered by an infection or other environmental factor in genetically susceptible children. Treatment typically involves administering high doses of intravenous immunoglobulin (IVIG) and aspirin to reduce inflammation and prevent complications.
Cell hypoxia, also known as cellular hypoxia or tissue hypoxia, refers to a condition in which the cells or tissues in the body do not receive an adequate supply of oxygen. Oxygen is essential for the production of energy in the form of ATP (adenosine triphosphate) through a process called oxidative phosphorylation. When the cells are deprived of oxygen, they switch to anaerobic metabolism, which produces lactic acid as a byproduct and can lead to acidosis.
Cell hypoxia can result from various conditions, including:
1. Low oxygen levels in the blood (hypoxemia) due to lung diseases such as chronic obstructive pulmonary disease (COPD), pneumonia, or high altitude.
2. Reduced blood flow to tissues due to cardiovascular diseases such as heart failure, peripheral artery disease, or shock.
3. Anemia, which reduces the oxygen-carrying capacity of the blood.
4. Carbon monoxide poisoning, which binds to hemoglobin and prevents it from carrying oxygen.
5. Inadequate ventilation due to trauma, drug overdose, or other causes that can lead to respiratory failure.
Cell hypoxia can cause cell damage, tissue injury, and organ dysfunction, leading to various clinical manifestations depending on the severity and duration of hypoxia. Treatment aims to correct the underlying cause and improve oxygen delivery to the tissues.
Neutrophils are a type of white blood cell that are part of the immune system's response to infection. They are produced in the bone marrow and released into the bloodstream where they circulate and are able to move quickly to sites of infection or inflammation in the body. Neutrophils are capable of engulfing and destroying bacteria, viruses, and other foreign substances through a process called phagocytosis. They are also involved in the release of inflammatory mediators, which can contribute to tissue damage in some cases. Neutrophils are characterized by the presence of granules in their cytoplasm, which contain enzymes and other proteins that help them carry out their immune functions.
Atenolol is a beta-blocker medication that is primarily used to treat hypertension (high blood pressure), angina (chest pain), and certain types of heart rhythm disorders. It works by blocking the action of certain hormones in the body, such as adrenaline, on the heart and blood vessels. This helps to reduce the heart's workload, lower its rate and force of contractions, and improve blood flow.
Beta-blockers like atenolol are also sometimes used to prevent migraines or to treat symptoms of anxiety, such as rapid heartbeat or tremors. Atenolol is available in immediate-release and extended-release forms, and it is typically taken orally once or twice a day. As with any medication, atenolol can have side effects, including dizziness, fatigue, and gastrointestinal symptoms, and it may interact with other medications or medical conditions. It is important to use atenolol only under the supervision of a healthcare provider.
Cytoprotection refers to the protection of cells, particularly from harmful agents or damaging conditions. This can be achieved through various mechanisms, such as:
1. Activation of cellular defense pathways that help cells resist damage.
2. Inhibition of oxidative stress and inflammation, which can cause cellular damage.
3. Enhancement of cell repair processes, enabling cells to recover from damage more effectively.
4. Prevention of apoptosis (programmed cell death) or promotion of cell survival signals.
In the medical context, cytoprotective agents are often used to protect tissues and organs from injury due to various factors like chemotherapy, radiation therapy, ischemia-reperfusion injury, or inflammation. These agents can include antioxidants, anti-inflammatory drugs, growth factors, and other compounds that help maintain cellular integrity and function.
Bradykinin is a naturally occurring peptide in the human body, consisting of nine amino acids. It is a potent vasodilator and increases the permeability of blood vessels, causing a local inflammatory response. Bradykinin is formed from the breakdown of certain proteins, such as kininogen, by enzymes called kininases or proteases, including kallikrein. It plays a role in several physiological processes, including pain transmission, blood pressure regulation, and the immune response. In some pathological conditions, such as hereditary angioedema, bradykinin levels can increase excessively, leading to symptoms like swelling, redness, and pain.
Isoflurane is a volatile halogenated ether used for induction and maintenance of general anesthesia. It is a colorless liquid with a pungent, sweet odor. Isoflurane is an agonist at the gamma-aminobutyric acid type A (GABAA) receptor and inhibits excitatory neurotransmission in the brain, leading to unconsciousness and immobility. It has a rapid onset and offset of action due to its low blood solubility, allowing for quick adjustments in anesthetic depth during surgery. Isoflurane is also known for its bronchodilator effects, making it useful in patients with reactive airway disease. However, it can cause dose-dependent decreases in heart rate and blood pressure, so careful hemodynamic monitoring is required during its use.
Premedication is the administration of medication before a medical procedure or surgery to prevent or manage pain, reduce anxiety, minimize side effects of anesthesia, or treat existing medical conditions. The goal of premedication is to improve the safety and outcomes of the medical procedure by preparing the patient's body in advance. Common examples of premedication include administering antibiotics before surgery to prevent infection, giving sedatives to help patients relax before a procedure, or providing medication to control acid reflux during surgery.
Calcium is an essential mineral that is vital for various physiological processes in the human body. The medical definition of calcium is as follows:
Calcium (Ca2+) is a crucial cation and the most abundant mineral in the human body, with approximately 99% of it found in bones and teeth. It plays a vital role in maintaining structural integrity, nerve impulse transmission, muscle contraction, hormonal secretion, blood coagulation, and enzyme activation.
Calcium homeostasis is tightly regulated through the interplay of several hormones, including parathyroid hormone (PTH), calcitonin, and vitamin D. Dietary calcium intake, absorption, and excretion are also critical factors in maintaining optimal calcium levels in the body.
Hypocalcemia refers to low serum calcium levels, while hypercalcemia indicates high serum calcium levels. Both conditions can have detrimental effects on various organ systems and require medical intervention to correct.
Reproducibility of results in a medical context refers to the ability to obtain consistent and comparable findings when a particular experiment or study is repeated, either by the same researcher or by different researchers, following the same experimental protocol. It is an essential principle in scientific research that helps to ensure the validity and reliability of research findings.
In medical research, reproducibility of results is crucial for establishing the effectiveness and safety of new treatments, interventions, or diagnostic tools. It involves conducting well-designed studies with adequate sample sizes, appropriate statistical analyses, and transparent reporting of methods and findings to allow other researchers to replicate the study and confirm or refute the results.
The lack of reproducibility in medical research has become a significant concern in recent years, as several high-profile studies have failed to produce consistent findings when replicated by other researchers. This has led to increased scrutiny of research practices and a call for greater transparency, rigor, and standardization in the conduct and reporting of medical research.
Fractional Flow Reserve (Myocardial) is a medical term used to describe the ratio of maximum blood flow through a stenosed (narrowed) coronary artery to the maximum flow that could be achieved if the artery were completely normal. It is a pressure-based index, which is measured during cardiac catheterization using a special wire that can measure pressure differences across a stenosis.
The FFR value ranges from 0 (no flow) to 1 (normal flow). An FFR value less than or equal to 0.80 is generally considered indicative of functionally significant coronary artery disease, which may benefit from revascularization (such as angioplasty or bypass surgery).
FFR is used in clinical practice to help guide decisions regarding the management of patients with coronary artery disease and has been shown to improve patient outcomes.
Brain edema is a medical condition characterized by the abnormal accumulation of fluid in the brain, leading to an increase in intracranial pressure. This can result from various causes, such as traumatic brain injury, stroke, infection, brain tumors, or inflammation. The swelling of the brain can compress vital structures, impair blood flow, and cause neurological symptoms, which may range from mild headaches to severe cognitive impairment, seizures, coma, or even death if not treated promptly and effectively.
Diabetic angiopathies refer to a group of vascular complications that occur due to diabetes mellitus. Prolonged exposure to high blood sugar levels can damage the blood vessels, leading to various types of angiopathies such as:
1. Diabetic retinopathy: This is a condition where the small blood vessels in the retina get damaged due to diabetes, leading to vision loss or blindness if left untreated.
2. Diabetic nephropathy: In this condition, the kidneys' glomeruli (the filtering units) become damaged due to diabetes, leading to protein leakage and eventually kidney failure if not managed properly.
3. Diabetic neuropathy: This is a type of nerve damage caused by diabetes that can affect various parts of the body, including the legs, feet, and hands, causing numbness, tingling, or pain.
4. Diabetic cardiomyopathy: This is a condition where the heart muscle becomes damaged due to diabetes, leading to heart failure.
5. Diabetic peripheral arterial disease (PAD): In this condition, the blood vessels that supply the legs and feet become narrowed or blocked due to diabetes, leading to pain, cramping, or even gangrene in severe cases.
Overall, diabetic angiopathies are serious complications of diabetes that can significantly impact a person's quality of life and overall health. Therefore, it is crucial for individuals with diabetes to manage their blood sugar levels effectively and undergo regular check-ups to detect any early signs of these complications.
Western blotting is a laboratory technique used in molecular biology to detect and quantify specific proteins in a mixture of many different proteins. This technique is commonly used to confirm the expression of a protein of interest, determine its size, and investigate its post-translational modifications. The name "Western" blotting distinguishes this technique from Southern blotting (for DNA) and Northern blotting (for RNA).
The Western blotting procedure involves several steps:
1. Protein extraction: The sample containing the proteins of interest is first extracted, often by breaking open cells or tissues and using a buffer to extract the proteins.
2. Separation of proteins by electrophoresis: The extracted proteins are then separated based on their size by loading them onto a polyacrylamide gel and running an electric current through the gel (a process called sodium dodecyl sulfate-polyacrylamide gel electrophoresis or SDS-PAGE). This separates the proteins according to their molecular weight, with smaller proteins migrating faster than larger ones.
3. Transfer of proteins to a membrane: After separation, the proteins are transferred from the gel onto a nitrocellulose or polyvinylidene fluoride (PVDF) membrane using an electric current in a process called blotting. This creates a replica of the protein pattern on the gel but now immobilized on the membrane for further analysis.
4. Blocking: The membrane is then blocked with a blocking agent, such as non-fat dry milk or bovine serum albumin (BSA), to prevent non-specific binding of antibodies in subsequent steps.
5. Primary antibody incubation: A primary antibody that specifically recognizes the protein of interest is added and allowed to bind to its target protein on the membrane. This step may be performed at room temperature or 4°C overnight, depending on the antibody's properties.
6. Washing: The membrane is washed with a buffer to remove unbound primary antibodies.
7. Secondary antibody incubation: A secondary antibody that recognizes the primary antibody (often coupled to an enzyme or fluorophore) is added and allowed to bind to the primary antibody. This step may involve using a horseradish peroxidase (HRP)-conjugated or alkaline phosphatase (AP)-conjugated secondary antibody, depending on the detection method used later.
8. Washing: The membrane is washed again to remove unbound secondary antibodies.
9. Detection: A detection reagent is added to visualize the protein of interest by detecting the signal generated from the enzyme-conjugated or fluorophore-conjugated secondary antibody. This can be done using chemiluminescent, colorimetric, or fluorescent methods.
10. Analysis: The resulting image is analyzed to determine the presence and quantity of the protein of interest in the sample.
Western blotting is a powerful technique for identifying and quantifying specific proteins within complex mixtures. It can be used to study protein expression, post-translational modifications, protein-protein interactions, and more. However, it requires careful optimization and validation to ensure accurate and reproducible results.
"Cells, cultured" is a medical term that refers to cells that have been removed from an organism and grown in controlled laboratory conditions outside of the body. This process is called cell culture and it allows scientists to study cells in a more controlled and accessible environment than they would have inside the body. Cultured cells can be derived from a variety of sources, including tissues, organs, or fluids from humans, animals, or cell lines that have been previously established in the laboratory.
Cell culture involves several steps, including isolation of the cells from the tissue, purification and characterization of the cells, and maintenance of the cells in appropriate growth conditions. The cells are typically grown in specialized media that contain nutrients, growth factors, and other components necessary for their survival and proliferation. Cultured cells can be used for a variety of purposes, including basic research, drug development and testing, and production of biological products such as vaccines and gene therapies.
It is important to note that cultured cells may behave differently than they do in the body, and results obtained from cell culture studies may not always translate directly to human physiology or disease. Therefore, it is essential to validate findings from cell culture experiments using additional models and ultimately in clinical trials involving human subjects.
Troponin is a protein complex found in cardiac and skeletal muscle cells that plays a critical role in muscle contraction. It consists of three subunits: troponin C, which binds calcium ions; troponin I, which inhibits the interaction between actin and myosin in the absence of calcium; and troponin T, which binds to tropomyosin and helps anchor the complex to the muscle filament.
In clinical medicine, "troponin" usually refers to cardiac-specific isoforms of these proteins (cTnI and cTnT) that are released into the bloodstream following damage to the heart muscle, such as occurs in myocardial infarction (heart attack). Measurement of troponin levels in the blood is a sensitive and specific biomarker for the diagnosis of acute myocardial infarction.
Antioxidants are substances that can prevent or slow damage to cells caused by free radicals, which are unstable molecules that the body produces as a reaction to environmental and other pressures. Antioxidants are able to neutralize free radicals by donating an electron to them, thus stabilizing them and preventing them from causing further damage to the cells.
Antioxidants can be found in a variety of foods, including fruits, vegetables, nuts, and grains. Some common antioxidants include vitamins C and E, beta-carotene, and selenium. Antioxidants are also available as dietary supplements.
In addition to their role in protecting cells from damage, antioxidants have been studied for their potential to prevent or treat a number of health conditions, including cancer, heart disease, and age-related macular degeneration. However, more research is needed to fully understand the potential benefits and risks of using antioxidant supplements.
Reactive Oxygen Species (ROS) are highly reactive molecules containing oxygen, including peroxides, superoxide, hydroxyl radical, and singlet oxygen. They are naturally produced as byproducts of normal cellular metabolism in the mitochondria, and can also be generated by external sources such as ionizing radiation, tobacco smoke, and air pollutants. At low or moderate concentrations, ROS play important roles in cell signaling and homeostasis, but at high concentrations, they can cause significant damage to cell structures, including lipids, proteins, and DNA, leading to oxidative stress and potential cell death.
Nitric Oxide Synthase (NOS) is a group of enzymes that catalyze the production of nitric oxide (NO) from L-arginine. There are three distinct isoforms of NOS, each with different expression patterns and functions:
1. Neuronal Nitric Oxide Synthase (nNOS or NOS1): This isoform is primarily expressed in the nervous system and plays a role in neurotransmission, synaptic plasticity, and learning and memory processes.
2. Inducible Nitric Oxide Synthase (iNOS or NOS2): This isoform is induced by various stimuli such as cytokines, lipopolysaccharides, and hypoxia in a variety of cells including immune cells, endothelial cells, and smooth muscle cells. iNOS produces large amounts of NO, which functions as a potent effector molecule in the immune response, particularly in the defense against microbial pathogens.
3. Endothelial Nitric Oxide Synthase (eNOS or NOS3): This isoform is constitutively expressed in endothelial cells and produces low levels of NO that play a crucial role in maintaining vascular homeostasis by regulating vasodilation, inhibiting platelet aggregation, and preventing smooth muscle cell proliferation.
Overall, NOS plays an essential role in various physiological processes, including neurotransmission, immune response, cardiovascular function, and respiratory regulation. Dysregulation of NOS activity has been implicated in several pathological conditions such as hypertension, atherosclerosis, neurodegenerative diseases, and inflammatory disorders.
In medical terms, the leg refers to the lower portion of the human body that extends from the knee down to the foot. It includes the thigh (femur), lower leg (tibia and fibula), foot, and ankle. The leg is primarily responsible for supporting the body's weight and enabling movements such as standing, walking, running, and jumping.
The leg contains several important structures, including bones, muscles, tendons, ligaments, blood vessels, nerves, and joints. These structures work together to provide stability, support, and mobility to the lower extremity. Common medical conditions that can affect the leg include fractures, sprains, strains, infections, peripheral artery disease, and neurological disorders.
Vasodilation is the widening or increase in diameter of blood vessels, particularly the involuntary relaxation of the smooth muscle in the tunica media (middle layer) of the arteriole walls. This results in an increase in blood flow and a decrease in vascular resistance. Vasodilation can occur due to various physiological and pathophysiological stimuli, such as local metabolic demands, neural signals, or pharmacological agents. It plays a crucial role in regulating blood pressure, tissue perfusion, and thermoregulation.
Intravenous (IV) infusion is a medical procedure in which liquids, such as medications, nutrients, or fluids, are delivered directly into a patient's vein through a needle or a catheter. This route of administration allows for rapid absorption and distribution of the infused substance throughout the body. IV infusions can be used for various purposes, including resuscitation, hydration, nutrition support, medication delivery, and blood product transfusion. The rate and volume of the infusion are carefully controlled to ensure patient safety and efficacy of treatment.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Medical Definition:
Superoxide dismutase (SOD) is an enzyme that catalyzes the dismutation of superoxide radicals (O2-) into oxygen (O2) and hydrogen peroxide (H2O2). This essential antioxidant defense mechanism helps protect the body's cells from damage caused by reactive oxygen species (ROS), which are produced during normal metabolic processes and can lead to oxidative stress when their levels become too high.
There are three main types of superoxide dismutase found in different cellular locations:
1. Copper-zinc superoxide dismutase (CuZnSOD or SOD1) - Present mainly in the cytoplasm of cells.
2. Manganese superoxide dismutase (MnSOD or SOD2) - Located within the mitochondrial matrix.
3. Extracellular superoxide dismutase (EcSOD or SOD3) - Found in the extracellular spaces, such as blood vessels and connective tissues.
Imbalances in SOD levels or activity have been linked to various pathological conditions, including neurodegenerative diseases, cancer, and aging-related disorders.
Sarcolemma is the medical term for the cell membrane that surrounds a muscle fiber or a skeletal muscle cell. It is responsible for providing protection and structure to the muscle fiber, as well as regulating the movement of ions and other molecules in and out of the cell. The sarcolemma plays a crucial role in the excitation-contraction coupling process that allows muscles to contract and relax.
The sarcolemma is composed of two main layers: the outer plasma membrane, which is similar to the cell membranes of other cells, and the inner basal lamina, which provides structural support and helps to anchor the muscle fiber to surrounding tissues. The sarcolemma also contains various ion channels, receptors, and transporters that are involved in regulating muscle function and communication with other cells.
Damage to the sarcolemma can lead to a variety of muscle disorders, including muscular dystrophy and myasthenia gravis.
The term "lower extremity" is used in the medical field to refer to the portion of the human body that includes the structures below the hip joint. This includes the thigh, lower leg, ankle, and foot. The lower extremities are responsible for weight-bearing and locomotion, allowing individuals to stand, walk, run, and jump. They contain many important structures such as bones, muscles, tendons, ligaments, nerves, and blood vessels.
Heart disease is a broad term for a class of diseases that involve the heart or blood vessels. It's often used to refer to conditions that include:
1. Coronary artery disease (CAD): This is the most common type of heart disease. It occurs when the arteries that supply blood to the heart become hardened and narrowed due to the buildup of cholesterol and other substances, which can lead to chest pain (angina), shortness of breath, or a heart attack.
2. Heart failure: This condition occurs when the heart is unable to pump blood efficiently to meet the body's needs. It can be caused by various conditions, including coronary artery disease, high blood pressure, and cardiomyopathy.
3. Arrhythmias: These are abnormal heart rhythms, which can be too fast, too slow, or irregular. They can lead to symptoms such as palpitations, dizziness, and fainting.
4. Valvular heart disease: This involves damage to one or more of the heart's four valves, which control blood flow through the heart. Damage can be caused by various conditions, including infection, rheumatic fever, and aging.
5. Cardiomyopathy: This is a disease of the heart muscle that makes it harder for the heart to pump blood efficiently. It can be caused by various factors, including genetics, viral infections, and drug abuse.
6. Pericardial disease: This involves inflammation or other problems with the sac surrounding the heart (pericardium). It can cause chest pain and other symptoms.
7. Congenital heart defects: These are heart conditions that are present at birth, such as a hole in the heart or abnormal blood vessels. They can range from mild to severe and may require medical intervention.
8. Heart infections: The heart can become infected by bacteria, viruses, or parasites, leading to various symptoms and complications.
It's important to note that many factors can contribute to the development of heart disease, including genetics, lifestyle choices, and certain medical conditions. Regular check-ups and a healthy lifestyle can help reduce the risk of developing heart disease.
Vascular Endothelial Growth Factor A (VEGFA) is a specific isoform of the vascular endothelial growth factor (VEGF) family. It is a well-characterized signaling protein that plays a crucial role in angiogenesis, the process of new blood vessel formation from pre-existing vessels. VEGFA stimulates the proliferation and migration of endothelial cells, which line the interior surface of blood vessels, thereby contributing to the growth and development of new vasculature. This protein is essential for physiological processes such as embryonic development and wound healing, but it has also been implicated in various pathological conditions, including cancer, age-related macular degeneration, and diabetic retinopathy. The regulation of VEGFA expression and activity is critical to maintaining proper vascular function and homeostasis.
Nitric Oxide Synthase Type III (NOS-III), also known as endothelial Nitric Oxide Synthase (eNOS), is an enzyme responsible for the production of nitric oxide (NO) in the endothelium, the lining of blood vessels. This enzyme catalyzes the conversion of L-arginine to L-citrulline, producing NO as a byproduct. The release of NO from eNOS plays an important role in regulating vascular tone and homeostasis, including the relaxation of smooth muscle cells in the blood vessel walls, inhibition of platelet aggregation, and modulation of immune function. Mutations or dysfunction in NOS-III can contribute to various cardiovascular diseases such as hypertension, atherosclerosis, and erectile dysfunction.
Peroxynitrous acid (ONOOH) is a highly reactive nitrogen species formed from the reaction between nitric oxide (NO) and superoxide radical (O2-). It is an unstable compound that quickly decomposes to form other reactive species, such as nitrogen dioxide (NO2) and hydroxyl radical (HO•), which can cause significant damage to biological molecules, including proteins, lipids, and DNA. Peroxynitrous acid has been implicated in the pathogenesis of various diseases, including neurodegenerative disorders, cardiovascular disease, and cancer.
Hydrogen-ion concentration, also known as pH, is a measure of the acidity or basicity of a solution. It is defined as the negative logarithm (to the base 10) of the hydrogen ion activity in a solution. The standard unit of measurement is the pH unit. A pH of 7 is neutral, less than 7 is acidic, and greater than 7 is basic.
In medical terms, hydrogen-ion concentration is important for maintaining homeostasis within the body. For example, in the stomach, a high hydrogen-ion concentration (low pH) is necessary for the digestion of food. However, in other parts of the body such as blood, a high hydrogen-ion concentration can be harmful and lead to acidosis. Conversely, a low hydrogen-ion concentration (high pH) in the blood can lead to alkalosis. Both acidosis and alkalosis can have serious consequences on various organ systems if not corrected.
Exercise is defined in the medical context as a physical activity that is planned, structured, and repetitive, with the primary aim of improving or maintaining one or more components of physical fitness. Components of physical fitness include cardiorespiratory endurance, muscular strength, muscular endurance, flexibility, and body composition. Exercise can be classified based on its intensity (light, moderate, or vigorous), duration (length of time), and frequency (number of times per week). Common types of exercise include aerobic exercises, such as walking, jogging, cycling, and swimming; resistance exercises, such as weightlifting; flexibility exercises, such as stretching; and balance exercises. Exercise has numerous health benefits, including reducing the risk of chronic diseases, improving mental health, and enhancing overall quality of life.
Balloon occlusion is a medical procedure that involves the use of a small, deflated balloon at the end of a catheter, which can be inserted into a blood vessel or other tubular structure in the body. Once the balloon is in position, it is inflated with a fluid or gas to create a blockage or obstruction in the vessel. This can be used for various medical purposes, such as:
1. Controlling bleeding: By inflating the balloon in a blood vessel, doctors can temporarily stop the flow of blood to a specific area, allowing them to treat injuries or abnormalities that are causing excessive bleeding.
2. Vessel narrowing or blockage assessment: Balloon occlusion can be used to assess the severity of narrowing or blockages in blood vessels. By inflating the balloon and measuring the pressure differences upstream and downstream, doctors can determine the extent of the obstruction and plan appropriate treatment.
3. Embolization therapy: In some cases, balloon occlusion is used to deliver embolic agents (such as coils, particles, or glue) that block off blood flow to specific areas. This can be useful in treating conditions like tumors, arteriovenous malformations, or aneurysms.
4. Temporary vessel occlusion during surgery: During certain surgical procedures, it may be necessary to temporarily stop the flow of blood to a specific area. Balloon occlusion can be used to achieve this quickly and safely.
5. Assisting in the placement of stents or other devices: Balloon occlusion can help position and deploy stents or other medical devices by providing temporary support or blocking off blood flow during the procedure.
It is important to note that balloon occlusion procedures carry potential risks, such as vessel injury, infection, or embolism (the blockage of a blood vessel by a clot or foreign material). These risks should be carefully weighed against the benefits when considering this type of treatment.
In the context of medicine and toxicology, protective agents are substances that provide protection against harmful or damaging effects of other substances. They can work in several ways, such as:
1. Binding to toxic substances: Protective agents can bind to toxic substances, rendering them inactive or less active, and preventing them from causing harm. For example, activated charcoal is sometimes used in the emergency treatment of certain types of poisoning because it can bind to certain toxins in the stomach and intestines and prevent their absorption into the body.
2. Increasing elimination: Protective agents can increase the elimination of toxic substances from the body, for example by promoting urinary or biliary excretion.
3. Reducing oxidative stress: Antioxidants are a type of protective agent that can reduce oxidative stress caused by free radicals and reactive oxygen species (ROS). These agents can protect cells and tissues from damage caused by oxidation.
4. Supporting organ function: Protective agents can support the function of organs that have been damaged by toxic substances, for example by improving blood flow or reducing inflammation.
Examples of protective agents include chelating agents, antidotes, free radical scavengers, and anti-inflammatory drugs.
Neutrophil infiltration is a pathological process characterized by the accumulation of neutrophils, a type of white blood cell, in tissue. It is a common feature of inflammation and occurs in response to infection, injury, or other stimuli that trigger an immune response. Neutrophils are attracted to the site of tissue damage by chemical signals called chemokines, which are released by damaged cells and activated immune cells. Once they reach the site of inflammation, neutrophils help to clear away damaged tissue and microorganisms through a process called phagocytosis. However, excessive or prolonged neutrophil infiltration can also contribute to tissue damage and may be associated with various disease states, including cancer, autoimmune disorders, and ischemia-reperfusion injury.
"Recovery of function" is a term used in medical rehabilitation to describe the process in which an individual regains the ability to perform activities or tasks that were previously difficult or impossible due to injury, illness, or disability. This can involve both physical and cognitive functions. The goal of recovery of function is to help the person return to their prior level of independence and participation in daily activities, work, and social roles as much as possible.
Recovery of function may be achieved through various interventions such as physical therapy, occupational therapy, speech-language therapy, and other rehabilitation strategies. The specific approach used will depend on the individual's needs and the nature of their impairment. Recovery of function can occur spontaneously as the body heals, or it may require targeted interventions to help facilitate the process.
It is important to note that recovery of function does not always mean a full return to pre-injury or pre-illness levels of ability. Instead, it often refers to the person's ability to adapt and compensate for any remaining impairments, allowing them to achieve their maximum level of functional independence and quality of life.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Induced heart arrest, also known as controlled cardiac arrest or planned cardiac arrest, is a deliberate medical intervention where cardiac activity is temporarily stopped through the use of medications or electrical disruption. This procedure is typically carried out during a surgical procedure, such as open-heart surgery, where the heart needs to be stilled to allow surgeons to work on it safely.
The most common method used to induce heart arrest is by administering a medication called potassium chloride, which stops the heart's electrical activity. Alternatively, an electrical shock may be delivered to the heart to achieve the same effect. Once the procedure is complete, the heart can be restarted using various resuscitation techniques, such as defibrillation or medication administration.
It's important to note that induced heart arrest is a carefully monitored and controlled medical procedure carried out by trained healthcare professionals in a hospital setting. It should not be confused with sudden cardiac arrest, which is an unexpected and often unpredictable event that occurs outside of a medical setting.
Purinergic P1 receptors are a type of G-protein coupled receptor that bind to nucleotides such as adenosine. These receptors are involved in a variety of physiological processes, including modulation of neurotransmitter release, cardiovascular function, and immune response. There are four subtypes of P1 receptors (A1, A2A, A2B, and A3) that have different signaling pathways and functions. Activation of these receptors can lead to a variety of cellular responses, including inhibition or stimulation of adenylyl cyclase activity, changes in intracellular calcium levels, and activation of various protein kinases. They play important roles in the central nervous system, cardiovascular system, respiratory system, gastrointestinal system, and immune system.
An action potential is a brief electrical signal that travels along the membrane of a nerve cell (neuron) or muscle cell. It is initiated by a rapid, localized change in the permeability of the cell membrane to specific ions, such as sodium and potassium, resulting in a rapid influx of sodium ions and a subsequent efflux of potassium ions. This ion movement causes a brief reversal of the electrical potential across the membrane, which is known as depolarization. The action potential then propagates along the cell membrane as a wave, allowing the electrical signal to be transmitted over long distances within the body. Action potentials play a crucial role in the communication and functioning of the nervous system and muscle tissue.
Free radicals are molecules or atoms that have one or more unpaired electrons in their outermost shell, making them highly reactive. They can be formed naturally in the body through processes such as metabolism and exercise, or they can come from external sources like pollution, radiation, and certain chemicals. Free radicals can cause damage to cells and contribute to the development of various diseases, including cancer, cardiovascular disease, and neurodegenerative disorders. Antioxidants are substances that can neutralize free radicals and help protect against their harmful effects.
Vascular resistance is a measure of the opposition to blood flow within a vessel or a group of vessels, typically expressed in units of mmHg/(mL/min) or sometimes as dynes*sec/cm^5. It is determined by the diameter and length of the vessels, as well as the viscosity of the blood flowing through them. In general, a decrease in vessel diameter, an increase in vessel length, or an increase in blood viscosity will result in an increase in vascular resistance, while an increase in vessel diameter, a decrease in vessel length, or a decrease in blood viscosity will result in a decrease in vascular resistance. Vascular resistance is an important concept in the study of circulation and cardiovascular physiology because it plays a key role in determining blood pressure and blood flow within the body.
Glucose is a simple monosaccharide (or single sugar) that serves as the primary source of energy for living organisms. It's a fundamental molecule in biology, often referred to as "dextrose" or "grape sugar." Glucose has the molecular formula C6H12O6 and is vital to the functioning of cells, especially those in the brain and nervous system.
In the body, glucose is derived from the digestion of carbohydrates in food, and it's transported around the body via the bloodstream to cells where it can be used for energy. Cells convert glucose into a usable form through a process called cellular respiration, which involves a series of metabolic reactions that generate adenosine triphosphate (ATP)—the main currency of energy in cells.
Glucose is also stored in the liver and muscles as glycogen, a polysaccharide (multiple sugar) that can be broken down back into glucose when needed for energy between meals or during physical activity. Maintaining appropriate blood glucose levels is crucial for overall health, and imbalances can lead to conditions such as diabetes mellitus.
Caspase-3 is a type of protease enzyme that plays a central role in the execution-phase of cell apoptosis, or programmed cell death. It's also known as CPP32 (CPP for ced-3 protease precursor) or apopain. Caspase-3 is produced as an inactive protein that is activated when cleaved by other caspases during the early stages of apoptosis. Once activated, it cleaves a variety of cellular proteins, including structural proteins, enzymes, and signal transduction proteins, leading to the characteristic morphological and biochemical changes associated with apoptotic cell death. Caspase-3 is often referred to as the "death protease" because of its crucial role in executing the cell death program.
Messenger RNA (mRNA) is a type of RNA (ribonucleic acid) that carries genetic information copied from DNA in the form of a series of three-base code "words," each of which specifies a particular amino acid. This information is used by the cell's machinery to construct proteins, a process known as translation. After being transcribed from DNA, mRNA travels out of the nucleus to the ribosomes in the cytoplasm where protein synthesis occurs. Once the protein has been synthesized, the mRNA may be degraded and recycled. Post-transcriptional modifications can also occur to mRNA, such as alternative splicing and addition of a 5' cap and a poly(A) tail, which can affect its stability, localization, and translation efficiency.
The hippocampus is a complex, curved formation in the brain that resembles a seahorse (hence its name, from the Greek word "hippos" meaning horse and "kampos" meaning sea monster). It's part of the limbic system and plays crucial roles in the formation of memories, particularly long-term ones.
This region is involved in spatial navigation and cognitive maps, allowing us to recognize locations and remember how to get to them. Additionally, it's one of the first areas affected by Alzheimer's disease, which often results in memory loss as an early symptom.
Anatomically, it consists of two main parts: the Ammon's horn (or cornu ammonis) and the dentate gyrus. These structures are made up of distinct types of neurons that contribute to different aspects of learning and memory.
Oxprenolol is a non-selective beta blocker and partial agonist of beta-adrenergic receptors. It works by blocking the effects of certain chemicals on the heart and blood vessels, which can help to reduce heart rate, blood pressure, and strain on the heart. Oxprenolol is used to treat angina (chest pain), high blood pressure, irregular heartbeats, and tremors. It may also be used for other purposes not listed here.
It's important to note that oxprenolol should only be taken under the supervision of a medical professional, as it can have significant interactions with other medications and medical conditions. Additionally, sudden discontinuation of oxprenolol should be avoided, as it can lead to rebound effects such as increased heart rate and blood pressure.
Beta-endorphins are naturally occurring opioid peptides that are produced in the brain and other parts of the body. They are synthesized from a larger precursor protein called proopiomelanocortin (POMC) and consist of 31 amino acids. Beta-endorphins have potent analgesic effects, which means they can reduce the perception of pain. They also play a role in regulating mood, emotions, and various physiological processes such as immune function and hormonal regulation.
Beta-endorphins bind to opioid receptors in the brain and other tissues, leading to a range of effects including pain relief, sedation, euphoria, and reduced anxiety. They are released in response to stress, physical activity, and certain physiological conditions such as pregnancy and lactation. Beta-endorphins have been studied for their potential therapeutic uses in the treatment of pain, addiction, and mood disorders. However, more research is needed to fully understand their mechanisms of action and potential side effects.
Induced hypothermia is a medically controlled lowering of the core body temperature to around 89.6-93.2°F (32-34°C) for therapeutic purposes. It is intentionally induced to reduce the metabolic rate and oxygen demand of organs, thereby offering protection during periods of low blood flow or inadequate oxygenation, such as during cardiac bypass surgery, severe trauma, or after a cardiac arrest. The deliberate induction and maintenance of hypothermia can help minimize tissue damage and improve outcomes in specific clinical scenarios. Once the risk has passed, the body temperature is gradually rewarmed to normal levels under controlled conditions.
Technetium Tc 99m Pyrophosphate (Tc-99m PYP) is a radiopharmaceutical agent used in nuclear medicine imaging, specifically myocardial perfusion imaging. It is a complex of technetium-99m, a metastable isotope of technetium, with pyrophosphate, a molecule that accumulates in damaged heart muscle tissue.
When injected into the patient's bloodstream, Tc-99m PYP is taken up by the heart muscle in proportion to its blood flow and the degree of damage or scarring (fibrosis). This allows for the detection and evaluation of conditions such as myocardial infarction (heart attack), cardiomyopathy, and heart transplant rejection.
The imaging procedure involves the injection of Tc-99m PYP, followed by the acquisition of images using a gamma camera, which detects the gamma rays emitted by the technetium-99m isotope. The resulting images provide information about the distribution and extent of heart muscle damage, helping physicians to make informed decisions regarding diagnosis and treatment planning.
Adrenergic fibers are a type of nerve fiber that releases neurotransmitters known as catecholamines, such as norepinephrine (noradrenaline) and epinephrine (adrenaline). These neurotransmitters bind to adrenergic receptors in various target organs, including the heart, blood vessels, lungs, glands, and other tissues, and mediate the "fight or flight" response to stress.
Adrenergic fibers can be classified into two types based on their neurotransmitter content:
1. Noradrenergic fibers: These fibers release norepinephrine as their primary neurotransmitter and are widely distributed throughout the autonomic nervous system, including the sympathetic and some parasympathetic ganglia. They play a crucial role in regulating cardiovascular function, respiration, metabolism, and other physiological processes.
2. Adrenergic fibers with dual innervation: These fibers contain both norepinephrine and epinephrine as neurotransmitters and are primarily located in the adrenal medulla. They release epinephrine into the bloodstream, which acts on distant target organs to produce a more widespread and intense "fight or flight" response than norepinephrine alone.
Overall, adrenergic fibers play a critical role in maintaining homeostasis and responding to stress by modulating various physiological functions through the release of catecholamines.
Purinergic P1 receptor antagonists are a class of pharmaceutical drugs that block the activity of purinergic P1 receptors, which are a type of G-protein coupled receptor found in many tissues throughout the body. These receptors are activated by extracellular nucleotides such as adenosine and ATP, and play important roles in regulating a variety of physiological processes, including cardiovascular function, neurotransmission, and immune response.
Purinergic P1 receptor antagonists work by binding to these receptors and preventing them from being activated by nucleotides. This can have various therapeutic effects, depending on the specific receptor subtype that is targeted. For example, A1 receptor antagonists have been shown to improve cardiac function in heart failure, while A2A receptor antagonists have potential as anti-inflammatory and neuroprotective agents.
However, it's important to note that the use of purinergic P1 receptor antagonists is still an area of active research, and more studies are needed to fully understand their mechanisms of action and therapeutic potential.
A feasibility study is a preliminary investigation or analysis conducted to determine the viability of a proposed project, program, or product. In the medical field, feasibility studies are often conducted before implementing new treatments, procedures, equipment, or facilities. These studies help to assess the practicality and effectiveness of the proposed intervention, as well as its potential benefits and risks.
Feasibility studies in healthcare typically involve several steps:
1. Problem identification: Clearly define the problem that the proposed project, program, or product aims to address.
2. Objectives setting: Establish specific, measurable, achievable, relevant, and time-bound (SMART) objectives for the study.
3. Literature review: Conduct a thorough review of existing research and best practices related to the proposed intervention.
4. Methodology development: Design a methodology for data collection and analysis that will help answer the research questions and achieve the study's objectives.
5. Resource assessment: Evaluate the availability and adequacy of resources, including personnel, time, and finances, required to carry out the proposed intervention.
6. Risk assessment: Identify potential risks and challenges associated with the implementation of the proposed intervention and develop strategies to mitigate them.
7. Cost-benefit analysis: Estimate the costs and benefits of the proposed intervention, including direct and indirect costs, as well as short-term and long-term benefits.
8. Stakeholder engagement: Engage relevant stakeholders, such as patients, healthcare providers, administrators, and policymakers, to gather their input and support for the proposed intervention.
9. Decision-making: Based on the findings of the feasibility study, make an informed decision about whether or not to proceed with the proposed project, program, or product.
Feasibility studies are essential in healthcare as they help ensure that resources are allocated efficiently and effectively, and that interventions are evidence-based, safe, and beneficial for patients.
Adenosine A3 receptor (A3R) is a type of G-protein coupled receptor that binds to adenosine, a purine nucleoside, and plays a role in various physiological processes. The activation of A3R leads to the inhibition of adenylate cyclase activity, which results in decreased levels of intracellular cAMP. This, in turn, modulates several downstream signaling pathways that are involved in anti-inflammatory and neuroprotective effects.
A3R is widely expressed in various tissues, including the brain, heart, lungs, liver, kidneys, and immune cells. In the central nervous system, A3R activation has been shown to have neuroprotective effects, such as reducing glutamate release, protecting against excitotoxicity, and modulating neuroinflammation. Additionally, A3R agonists have been investigated for their potential therapeutic benefits in various pathological conditions, including pain management, ischemia-reperfusion injury, and neurodegenerative diseases.
Overall, the Adenosine A3 receptor is an important target for drug development due to its role in modulating inflammation and cellular responses in various tissues and diseases.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Fentanyl is a potent synthetic opioid analgesic, which is similar to morphine but is 50 to 100 times more potent. It is a schedule II prescription drug, typically used to treat patients with severe pain or to manage pain after surgery. It works by binding to the body's opioid receptors, which are found in the brain, spinal cord, and other areas of the body.
Fentanyl can be administered in several forms, including transdermal patches, lozenges, injectable solutions, and tablets that dissolve in the mouth. Illegally manufactured and distributed fentanyl has also become a major public health concern, as it is often mixed with other drugs such as heroin, cocaine, and counterfeit pills, leading to an increase in overdose deaths.
Like all opioids, fentanyl carries a risk of dependence, addiction, and overdose, especially when used outside of medical supervision or in combination with other central nervous system depressants such as alcohol or benzodiazepines. It is important to use fentanyl only as directed by a healthcare provider and to be aware of the potential risks associated with its use.
Nicorandil is a medication that belongs to a class of drugs known as potassium channel activators. It works by relaxing and widening blood vessels, which improves blood flow and reduces the workload on the heart. Nicorandil is primarily used to treat chronic stable angina, a type of chest pain caused by reduced blood flow to the heart muscle.
The medical definition of Nicorandil can be described as:
A synthetic derivative of nicotinamide with vasodilatory properties, acting as an opener of ATP-sensitive potassium channels in vascular smooth muscle and cardiomyocytes. It is used in the management of chronic stable angina, providing both antianginal and antiischemic effects through a dual mechanism that includes coronary and peripheral vasodilation. By reducing afterload and preload, Nicorandil decreases myocardial oxygen demand while increasing supply, leading to improved exercise tolerance and reduced frequency of anginal episodes.
Electroacupuncture is a form of acupuncture where a small electric current is passed between pairs of acupuncture needles. This technique is used to stimulate the acupoints more strongly and consistently than with manual acupuncture. The intensity of the electrical impulses can be adjusted depending on the patient's comfort level and the desired therapeutic effect. Electroacupuncture is often used to treat conditions such as chronic pain, muscle spasms, and paralysis. It may also be used in the treatment of addiction, weight loss, and stroke rehabilitation.
Acute Coronary Syndrome (ACS) is a term used to describe a range of conditions associated with sudden, reduced blood flow to the heart muscle. This reduction in blood flow, commonly caused by blood clots forming in coronary arteries, can lead to damage or death of the heart muscle and is often characterized by symptoms such as chest pain, shortness of breath, and fatigue.
There are three main types of ACS:
1. Unstable Angina: This occurs when there is reduced blood flow to the heart muscle, causing chest pain or discomfort, but the heart muscle is not damaged. It can be a warning sign for a possible future heart attack.
2. Non-ST Segment Elevation Myocardial Infarction (NSTEMI): This type of heart attack occurs when there is reduced blood flow to the heart muscle, causing damage or death of some of the muscle cells. However, the electrical activity of the heart remains relatively normal.
3. ST Segment Elevation Myocardial Infarction (STEMI): This is a serious and life-threatening type of heart attack that occurs when there is a complete blockage in one or more of the coronary arteries, causing extensive damage to the heart muscle. The electrical activity of the heart is significantly altered, which can lead to dangerous heart rhythms and even cardiac arrest.
Immediate medical attention is required for anyone experiencing symptoms of ACS, as prompt treatment can help prevent further damage to the heart muscle and reduce the risk of complications or death. Treatment options may include medications, lifestyle changes, and procedures such as angioplasty or bypass surgery.
Edema, cardiac is a type of edema (swelling) that occurs due to the accumulation of fluid in the body tissues as a result of heart failure. When the heart is not able to pump blood efficiently, it can cause blood to back up in the veins and increase pressure in the capillaries. This increased pressure forces fluid out of the blood vessels and into the surrounding tissues, causing edema.
Cardiac edema most commonly affects the lower extremities, such as the legs, ankles, and feet, but it can also occur in other parts of the body, including the lungs (pulmonary edema). Symptoms of cardiac edema may include swelling, weight gain, shortness of breath, and coughing. Treatment typically involves addressing the underlying heart condition through medications, lifestyle changes, or medical procedures.
Ventricular function, in the context of cardiac medicine, refers to the ability of the heart's ventricles (the lower chambers) to fill with blood during the diastole phase and eject blood during the systole phase. The ventricles are primarily responsible for pumping oxygenated blood out to the body (left ventricle) and deoxygenated blood to the lungs (right ventricle).
There are several ways to assess ventricular function, including:
1. Ejection Fraction (EF): This is the most commonly used measure of ventricular function. It represents the percentage of blood that is ejected from the ventricle during each heartbeat. A normal left ventricular ejection fraction is typically between 55% and 70%.
2. Fractional Shortening (FS): This is another measure of ventricular function, which calculates the change in size of the ventricle during contraction as a percentage of the original size. A normal FS for the left ventricle is typically between 25% and 45%.
3. Stroke Volume (SV): This refers to the amount of blood that is pumped out of the ventricle with each heartbeat. SV is calculated by multiplying the ejection fraction by the end-diastolic volume (the amount of blood in the ventricle at the end of diastole).
4. Cardiac Output (CO): This is the total amount of blood that the heart pumps in one minute. It is calculated by multiplying the stroke volume by the heart rate.
Impaired ventricular function can lead to various cardiovascular conditions, such as heart failure, cardiomyopathy, and valvular heart disease. Assessing ventricular function is crucial for diagnosing these conditions, monitoring treatment response, and guiding clinical decision-making.
A coronary aneurysm is a localized dilation or bulging of a portion of the wall of a coronary artery, which supplies blood to the muscle tissue of the heart. It's similar to a bubble or balloon-like structure that forms within the artery wall due to weakness in the arterial wall, leading to abnormal enlargement or widening.
Coronary aneurysms can vary in size and may be classified as true or false aneurysms based on their structure. True aneurysms involve all three layers of the artery wall, while false aneurysms (also known as pseudoaneurysms) only have one or two layers involved, with the remaining layer disrupted.
These aneurysms can lead to complications such as blood clots forming inside the aneurysm sac, which can then dislodge and cause blockages in smaller coronary arteries (embolism). Additionally, coronary aneurysms may rupture, leading to severe internal bleeding and potentially life-threatening situations.
Coronary aneurysms are often asymptomatic but can present with symptoms such as chest pain, shortness of breath, or palpitations, especially if the aneurysm causes a significant narrowing (stenosis) in the affected artery. They can be diagnosed through imaging techniques like coronary angiography, computed tomography (CT), or magnetic resonance imaging (MRI). Treatment options include medications to manage symptoms and prevent complications, as well as surgical interventions such as stenting or bypass grafting to repair or reroute the affected artery.
Trimetazidine is a medication that belongs to the class of drugs known as anti-ischemic agents. It is primarily used in the management of angina pectoris, a type of chest pain caused by reduced blood flow to the heart muscle.
Trimetazidine works by improving the efficiency of heart muscle cells in utilizing energy and reducing the production of harmful oxygen free radicals during periods of reduced oxygen supply, such as during angina attacks. This helps to preserve the function of the heart muscle and reduce the severity and frequency of angina episodes.
It is important to note that Trimetazidine should only be used under the supervision of a healthcare provider, and it is not recommended for individuals with severe liver or kidney impairment.
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic technique that uses a strong magnetic field and radio waves to create detailed cross-sectional images of the body's internal structures. In MRI, Cine is a specific mode of imaging that allows for the evaluation of moving structures, such as the heart, by acquiring and displaying a series of images in rapid succession. This technique is particularly useful in cardiac imaging, where it can help assess heart function, valve function, and blood flow. The term "Cine" refers to the continuous playback of these images, similar to watching a movie, allowing doctors to evaluate motion and timing within the heart.
Gated Blood-Pool Imaging (GBPI) is a type of nuclear medicine test that uses radioactive material and a specialized camera to create detailed images of the heart and its function. In this procedure, a small amount of radioactive tracer is injected into the patient's bloodstream, which then accumulates in the heart muscle and the blood pool within the heart chambers.
The term "gated" refers to the use of an electrocardiogram (ECG) signal to synchronize the image acquisition with the heart's contractions. This allows for the visualization of the heart's motion during different phases of the cardiac cycle, providing valuable information about the size, shape, and contraction of the heart chambers, as well as the movement of the walls of the heart.
GBPI is often used to assess patients with known or suspected heart disease, such as valvular abnormalities, cardiomyopathies, or congenital heart defects. It can help diagnose and evaluate the severity of these conditions, guide treatment decisions, and monitor the effectiveness of therapy.
Sudden cardiac death (SCD) is a sudden, unexpected natural death caused by the cessation of cardiac activity. It is often caused by cardiac arrhythmias, particularly ventricular fibrillation, and is often associated with underlying heart disease, although it can occur in people with no known heart condition. SCD is typically defined as a natural death due to cardiac causes that occurs within one hour of the onset of symptoms, or if the individual was last seen alive in a normal state of health, it can be defined as occurring within 24 hours.
It's important to note that sudden cardiac arrest (SCA) is different from SCD, although they are related. SCA refers to the sudden cessation of cardiac activity, which if not treated immediately can lead to SCD.
Amputation is defined as the surgical removal of all or part of a limb or extremity such as an arm, leg, foot, hand, toe, or finger. This procedure is typically performed to remove damaged or dead tissue due to various reasons like severe injury, infection, tumors, or chronic conditions that impair circulation, such as diabetes or peripheral arterial disease. The goal of amputation is to alleviate pain, prevent further complications, and improve the patient's quality of life. Following the surgery, patients may require rehabilitation and prosthetic devices to help them adapt to their new physical condition.
I must clarify that the term "Guinea Pigs" is not typically used in medical definitions. However, in colloquial or informal language, it may refer to people who are used as the first to try out a new medical treatment or drug. This is known as being a "test subject" or "in a clinical trial."
In the field of scientific research, particularly in studies involving animals, guinea pigs are small rodents that are often used as experimental subjects due to their size, cost-effectiveness, and ease of handling. They are not actually pigs from Guinea, despite their name's origins being unclear. However, they do not exactly fit the description of being used in human medical experiments.
Physical exertion is defined as the act of applying energy to physically demandable activities or tasks, which results in various body systems working together to produce movement and maintain homeostasis. It often leads to an increase in heart rate, respiratory rate, and body temperature, among other physiological responses. The level of physical exertion can vary based on the intensity, duration, and frequency of the activity.
It's important to note that engaging in regular physical exertion has numerous health benefits, such as improving cardiovascular fitness, strengthening muscles and bones, reducing stress, and preventing chronic diseases like obesity, diabetes, and heart disease. However, it is also crucial to balance physical exertion with adequate rest and recovery time to avoid overtraining or injury.
P-Selectin is a type of cell adhesion molecule, specifically a member of the selectin family, that is involved in the inflammatory response. It is primarily expressed on the surface of activated platelets and endothelial cells. P-Selectin plays a crucial role in the initial interaction between leukocytes (white blood cells) and the vascular endothelium, which is an essential step in the recruitment of leukocytes to sites of inflammation or injury. This process helps to mediate the rolling and adhesion of leukocytes to the endothelial surface, facilitating their extravasation into the surrounding tissue. P-Selectin's function is regulated by its interaction with specific ligands on the surface of leukocytes, such as PSGL-1 (P-Selectin Glycoprotein Ligand-1).
Purinergic P1 receptor agonists are substances that bind to and activate purinergic P1 receptors, which are a type of G protein-coupled receptor found in many tissues throughout the body. These receptors are activated by endogenous nucleotides such as adenosine and its metabolites.
Purinergic P1 receptors include four subtypes: A1, A2A, A2B, and A3. Each of these subtypes has distinct signaling pathways and physiological roles. For example, A1 receptor activation can lead to vasodilation, bradycardia, and anti-inflammatory effects, while A2A receptor activation can increase cyclic AMP levels and have anti-inflammatory effects.
Purinergic P1 receptor agonists are used in various therapeutic applications, including as cardiovascular drugs, antiplatelet agents, and anti-inflammatory agents. Some examples of purinergic P1 receptor agonists include adenosine, regadenoson, and dipyridamole.
It's important to note that the use of these substances should be under medical supervision due to their potential side effects and interactions with other medications.
Potassium is a essential mineral and an important electrolyte that is widely distributed in the human body. The majority of potassium in the body (approximately 98%) is found within cells, with the remaining 2% present in blood serum and other bodily fluids. Potassium plays a crucial role in various physiological processes, including:
1. Regulation of fluid balance and maintenance of normal blood pressure through its effects on vascular tone and sodium excretion.
2. Facilitation of nerve impulse transmission and muscle contraction by participating in the generation and propagation of action potentials.
3. Protein synthesis, enzyme activation, and glycogen metabolism.
4. Regulation of acid-base balance through its role in buffering systems.
The normal serum potassium concentration ranges from 3.5 to 5.0 mEq/L (milliequivalents per liter) or mmol/L (millimoles per liter). Potassium levels outside this range can have significant clinical consequences, with both hypokalemia (low potassium levels) and hyperkalemia (high potassium levels) potentially leading to serious complications such as cardiac arrhythmias, muscle weakness, and respiratory failure.
Potassium is primarily obtained through the diet, with rich sources including fruits (e.g., bananas, oranges, and apricots), vegetables (e.g., leafy greens, potatoes, and tomatoes), legumes, nuts, dairy products, and meat. In cases of deficiency or increased needs, potassium supplements may be recommended under the guidance of a healthcare professional.
Calcium channel blockers (CCBs) are a class of medications that work by inhibiting the influx of calcium ions into cardiac and smooth muscle cells. This action leads to relaxation of the muscles, particularly in the blood vessels, resulting in decreased peripheral resistance and reduced blood pressure. Calcium channel blockers also have anti-arrhythmic effects and are used in the management of various cardiovascular conditions such as hypertension, angina, and certain types of arrhythmias.
Calcium channel blockers can be further classified into two main categories based on their chemical structure: dihydropyridines (e.g., nifedipine, amlodipine) and non-dihydropyridines (e.g., verapamil, diltiazem). Dihydropyridines are more selective for vascular smooth muscle and have a greater effect on blood pressure than heart rate or conduction. Non-dihydropyridines have a more significant impact on cardiac conduction and contractility, in addition to their vasodilatory effects.
It is important to note that calcium channel blockers may interact with other medications and should be used under the guidance of a healthcare professional. Potential side effects include dizziness, headache, constipation, and peripheral edema.
Ventricular remodeling is a structural adaptation process of the heart in response to stress or injury, such as myocardial infarction (heart attack) or pressure overload. This process involves changes in size, shape, and function of the ventricles (the lower chambers of the heart).
In ventricular remodeling, the heart muscle may thicken, enlarge, or become more stiff, leading to alterations in the pumping ability of the heart. These changes can ultimately result in cardiac dysfunction, heart failure, and an increased risk of arrhythmias (irregular heart rhythms).
Ventricular remodeling is often classified into two types:
1. Concentric remodeling: This occurs when the ventricular wall thickens (hypertrophy) without a significant increase in chamber size, leading to a decrease in the cavity volume and an increase in the thickness of the ventricular wall.
2. Eccentric remodeling: This involves an increase in both the ventricular chamber size and wall thickness due to the addition of new muscle cells (hyperplasia) or enlargement of existing muscle cells (hypertrophy). As a result, the overall shape of the ventricle becomes more spherical and less elliptical.
Both types of remodeling can negatively impact heart function and contribute to the development of heart failure. Close monitoring and appropriate treatment are essential for managing ventricular remodeling and preventing further complications.
Allopurinol is a medication used to treat chronic gout and certain types of kidney stones. It works by reducing the production of uric acid in the body, which is the substance that can cause these conditions when it builds up in high levels. Allopurinol is a xanthine oxidase inhibitor, meaning it blocks an enzyme called xanthine oxidase from converting purines into uric acid. By doing this, allopurinol helps to lower the levels of uric acid in the body and prevent the formation of new kidney stones or gout attacks.
It is important to note that allopurinol can have side effects, including rash, stomach upset, and liver or kidney problems. It may also interact with other medications, so it is essential to inform your healthcare provider of any other drugs you are taking before starting allopurinol. Your healthcare provider will determine the appropriate dosage and monitoring schedule based on your individual needs and medical history.
Laser-Doppler flowmetry (LDF) is a non-invasive, investigative technique used to measure microcirculatory blood flow in real time. It is based on the principle of the Doppler effect, which describes the change in frequency or wavelength of light or sound waves as they encounter a moving object or reflect off a moving surface.
In LDF, a low-power laser beam is directed at the skin or other transparent tissue. The light penetrates the tissue and scatters off the moving red blood cells within the microvasculature. As the light scatters, it undergoes a slight frequency shift due to the movement of the red blood cells. This frequency shift is then detected by a photodetector, which converts it into an electrical signal. The magnitude of this signal is directly proportional to the speed and concentration of the moving red blood cells, providing a measure of microcirculatory blood flow.
LDF has various clinical applications, including the assessment of skin perfusion in patients with peripheral arterial disease, burn injuries, and flaps used in reconstructive surgery. It can also be used to study the effects of drugs or other interventions on microcirculation in research settings.
The cerebral cortex is the outermost layer of the brain, characterized by its intricate folded structure and wrinkled appearance. It is a region of great importance as it plays a key role in higher cognitive functions such as perception, consciousness, thought, memory, language, and attention. The cerebral cortex is divided into two hemispheres, each containing four lobes: the frontal, parietal, temporal, and occipital lobes. These areas are responsible for different functions, with some regions specializing in sensory processing while others are involved in motor control or associative functions. The cerebral cortex is composed of gray matter, which contains neuronal cell bodies, and is covered by a layer of white matter that consists mainly of myelinated nerve fibers.
Guanidines are organic compounds that contain a guanidino group, which is a functional group with the formula -NH-C(=NH)-NH2. Guanidines can be found in various natural sources, including some animals, plants, and microorganisms. They also occur as byproducts of certain metabolic processes in the body.
In a medical context, guanidines are most commonly associated with the treatment of muscle weakness and neuromuscular disorders. The most well-known guanidine compound is probably guanidine hydrochloride, which has been used as a medication to treat conditions such as myasthenia gravis and Eaton-Lambert syndrome.
However, the use of guanidines as medications has declined in recent years due to their potential for toxicity and the development of safer and more effective treatments. Today, guanidines are mainly used in research settings to study various biological processes, including protein folding and aggregation, enzyme inhibition, and cell signaling.
Cardiac output is a measure of the amount of blood that is pumped by the heart in one minute. It is defined as the product of stroke volume (the amount of blood pumped by the left ventricle during each contraction) and heart rate (the number of contractions per minute). Normal cardiac output at rest for an average-sized adult is about 5 to 6 liters per minute. Cardiac output can be increased during exercise or other conditions that require more blood flow, such as during illness or injury. It can be measured noninvasively using techniques such as echocardiography or invasively through a catheter placed in the heart.
A stroke, also known as cerebrovascular accident (CVA), is a serious medical condition that occurs when the blood supply to part of the brain is interrupted or reduced, leading to deprivation of oxygen and nutrients to brain cells. This can result in the death of brain tissue and cause permanent damage or temporary impairment to cognitive functions, speech, memory, movement, and other body functions controlled by the affected area of the brain.
Strokes can be caused by either a blockage in an artery that supplies blood to the brain (ischemic stroke) or the rupture of a blood vessel in the brain (hemorrhagic stroke). A transient ischemic attack (TIA), also known as a "mini-stroke," is a temporary disruption of blood flow to the brain that lasts only a few minutes and does not cause permanent damage.
Symptoms of a stroke may include sudden weakness or numbness in the face, arm, or leg; difficulty speaking or understanding speech; vision problems; loss of balance or coordination; severe headache with no known cause; and confusion or disorientation. Immediate medical attention is crucial for stroke patients to receive appropriate treatment and prevent long-term complications.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Metoprolol is a type of medication known as a beta blocker. According to the US National Library of Medicine's MedlinePlus, metoprolol is used to treat high blood pressure, angina (chest pain), and heart conditions that may occur after a heart attack. It works by blocking the action of certain natural chemicals in your body, such as epinephrine, on the heart and blood vessels. This helps to reduce the heart's workload, lower its blood pressure, and regulate its rhythm.
Metoprolol is available under various brand names, including Lopressor and Toprol-XL. It can be taken orally as a tablet or an extended-release capsule. As with any medication, metoprolol should be used under the supervision of a healthcare provider, who can monitor its effectiveness and potential side effects.
It is important to note that this definition is intended to provide a general overview of the medical use of metoprolol and should not be considered a substitute for professional medical advice.
Hypertrophic cardiomyopathy (HCM) is a genetic disorder characterized by the thickening of the heart muscle, specifically the ventricles (the lower chambers of the heart that pump blood out to the body). This thickening can make it harder for the heart to pump blood effectively, which can lead to symptoms such as shortness of breath, chest pain, and fatigue. In some cases, HCM can also cause abnormal heart rhythms (arrhythmias) and may increase the risk of sudden cardiac death.
The thickening of the heart muscle in HCM is caused by an overgrowth of the cells that make up the heart muscle, known as cardiomyocytes. This overgrowth can be caused by mutations in any one of several genes that encode proteins involved in the structure and function of the heart muscle. These genetic mutations are usually inherited from a parent, but they can also occur spontaneously in an individual with no family history of the disorder.
HCM is typically diagnosed using echocardiography (a type of ultrasound that uses sound waves to create images of the heart) and other diagnostic tests such as electrocardiogram (ECG) and cardiac magnetic resonance imaging (MRI). Treatment for HCM may include medications to help manage symptoms, lifestyle modifications, and in some cases, surgical procedures or implantable devices to help prevent or treat arrhythmias.
The Chi-square distribution is a continuous probability distribution that is often used in statistical hypothesis testing. It is the distribution of a sum of squares of k independent standard normal random variables. The resulting quantity follows a chi-square distribution with k degrees of freedom, denoted as χ²(k).
The probability density function (pdf) of the Chi-square distribution with k degrees of freedom is given by:
f(x; k) = (1/ (2^(k/2) * Γ(k/2))) \* x^((k/2)-1) \* e^(-x/2), for x > 0 and 0, otherwise.
Where Γ(k/2) is the gamma function evaluated at k/2. The mean and variance of a Chi-square distribution with k degrees of freedom are k and 2k, respectively.
The Chi-square distribution has various applications in statistical inference, including testing goodness-of-fit, homogeneity of variances, and independence in contingency tables.
Premature cardiac complexes, also known as premature heartbeats or premature ventricular contractions (PVCs), refer to extra or early heartbeats that originate in the lower chambers of the heart (the ventricles). These extra beats disrupt the normal rhythm and sequence of heartbeats, causing the heart to beat earlier than expected.
Premature cardiac complexes can occur in healthy individuals as well as those with heart disease. They are usually harmless and do not cause any symptoms, but in some cases, they may cause palpitations, skipped beats, or a fluttering sensation in the chest. In rare cases, frequent premature cardiac complexes can lead to more serious heart rhythm disorders or decreased heart function.
The diagnosis of premature cardiac complexes is usually made through an electrocardiogram (ECG) or Holter monitoring, which records the electrical activity of the heart over a period of time. Treatment is typically not necessary unless the premature complexes are frequent, symptomatic, or associated with underlying heart disease. In such cases, medications, cardioversion, or catheter ablation may be recommended.
Thromboxane B2 (TXB2) is a stable metabolite of thromboxane A2 (TXA2), which is a potent vasoconstrictor and platelet aggregator synthesized by activated platelets. TXA2 has a very short half-life, quickly undergoing spontaneous conversion to the more stable TXB2.
TXB2 itself does not have significant biological activity but serves as a marker for TXA2 production in various physiological and pathophysiological conditions, such as thrombosis, inflammation, and atherosclerosis. It can be measured in blood or other bodily fluids to assess platelet activation and the status of hemostatic and inflammatory processes.
Nitric Oxide Synthase Type II (NOS2), also known as Inducible Nitric Oxide Synthase (iNOS), is an enzyme that catalyzes the production of nitric oxide (NO) from L-arginine. Unlike other isoforms of NOS, NOS2 is not constitutively expressed and its expression can be induced by various stimuli such as cytokines, lipopolysaccharides, and bacterial products. Once induced, NOS2 produces large amounts of NO, which plays a crucial role in the immune response against invading pathogens. However, excessive or prolonged production of NO by NOS2 has been implicated in various pathological conditions such as inflammation, septic shock, and neurodegenerative disorders.
Isoenzymes, also known as isoforms, are multiple forms of an enzyme that catalyze the same chemical reaction but differ in their amino acid sequence, structure, and/or kinetic properties. They are encoded by different genes or alternative splicing of the same gene. Isoenzymes can be found in various tissues and organs, and they play a crucial role in biological processes such as metabolism, detoxification, and cell signaling. Measurement of isoenzyme levels in body fluids (such as blood) can provide valuable diagnostic information for certain medical conditions, including tissue damage, inflammation, and various diseases.
Acetylcholine is a neurotransmitter, a type of chemical messenger that transmits signals across a chemical synapse from one neuron (nerve cell) to another "target" neuron, muscle cell, or gland cell. It is involved in both peripheral and central nervous system functions.
In the peripheral nervous system, acetylcholine acts as a neurotransmitter at the neuromuscular junction, where it transmits signals from motor neurons to activate muscles. Acetylcholine also acts as a neurotransmitter in the autonomic nervous system, where it is involved in both the sympathetic and parasympathetic systems.
In the central nervous system, acetylcholine plays a role in learning, memory, attention, and arousal. Disruptions in cholinergic neurotransmission have been implicated in several neurological disorders, including Alzheimer's disease, Parkinson's disease, and myasthenia gravis.
Acetylcholine is synthesized from choline and acetyl-CoA by the enzyme choline acetyltransferase and is stored in vesicles at the presynaptic terminal of the neuron. When a nerve impulse arrives, the vesicles fuse with the presynaptic membrane, releasing acetylcholine into the synapse. The acetylcholine then binds to receptors on the postsynaptic membrane, triggering a response in the target cell. Acetylcholine is subsequently degraded by the enzyme acetylcholinesterase, which terminates its action and allows for signal transduction to be repeated.
The extracellular space is the region outside of cells within a tissue or organ, where various biological molecules and ions exist in a fluid medium. This space is filled with extracellular matrix (ECM), which includes proteins like collagen and elastin, glycoproteins, and proteoglycans that provide structural support and biochemical cues to surrounding cells. The ECM also contains various ions, nutrients, waste products, signaling molecules, and growth factors that play crucial roles in cell-cell communication, tissue homeostasis, and regulation of cell behavior. Additionally, the extracellular space includes the interstitial fluid, which is the fluid component of the ECM, and the lymphatic and vascular systems, through which cells exchange nutrients, waste products, and signaling molecules with the rest of the body. Overall, the extracellular space is a complex and dynamic microenvironment that plays essential roles in maintaining tissue structure, function, and homeostasis.
Potassium channel blockers are a class of medications that work by blocking potassium channels, which are proteins in the cell membrane that control the movement of potassium ions into and out of cells. By blocking these channels, potassium channel blockers can help to regulate electrical activity in the heart, making them useful for treating certain types of cardiac arrhythmias (irregular heart rhythms).
There are several different types of potassium channel blockers, including:
1. Class III antiarrhythmic drugs: These medications, such as amiodarone and sotalol, are used to treat and prevent serious ventricular arrhythmias (irregular heart rhythms that originate in the lower chambers of the heart).
2. Calcium channel blockers: While not strictly potassium channel blockers, some calcium channel blockers also have effects on potassium channels. These medications, such as diltiazem and verapamil, are used to treat hypertension (high blood pressure), angina (chest pain), and certain types of arrhythmias.
3. Non-selective potassium channel blockers: These medications, such as 4-aminopyridine and tetraethylammonium, have a broader effect on potassium channels and are used primarily in research settings to study the electrical properties of cells.
It's important to note that potassium channel blockers can have serious side effects, particularly when used in high doses or in combination with other medications that affect heart rhythms. They should only be prescribed by a healthcare provider who is familiar with their use and potential risks.
Propranolol is a medication that belongs to a class of drugs called beta blockers. Medically, it is defined as a non-selective beta blocker, which means it blocks the effects of both epinephrine (adrenaline) and norepinephrine (noradrenaline) on the heart and other organs. These effects include reducing heart rate, contractility, and conduction velocity, leading to decreased oxygen demand by the myocardium. Propranolol is used in the management of various conditions such as hypertension, angina pectoris, arrhythmias, essential tremor, anxiety disorders, and infants with congenital heart defects. It may also be used to prevent migraines and reduce the risk of future heart attacks. As with any medication, it should be taken under the supervision of a healthcare provider due to potential side effects and contraindications.
A kidney, in medical terms, is one of two bean-shaped organs located in the lower back region of the body. They are essential for maintaining homeostasis within the body by performing several crucial functions such as:
1. Regulation of water and electrolyte balance: Kidneys help regulate the amount of water and various electrolytes like sodium, potassium, and calcium in the bloodstream to maintain a stable internal environment.
2. Excretion of waste products: They filter waste products from the blood, including urea (a byproduct of protein metabolism), creatinine (a breakdown product of muscle tissue), and other harmful substances that result from normal cellular functions or external sources like medications and toxins.
3. Endocrine function: Kidneys produce several hormones with important roles in the body, such as erythropoietin (stimulates red blood cell production), renin (regulates blood pressure), and calcitriol (activated form of vitamin D that helps regulate calcium homeostasis).
4. pH balance regulation: Kidneys maintain the proper acid-base balance in the body by excreting either hydrogen ions or bicarbonate ions, depending on whether the blood is too acidic or too alkaline.
5. Blood pressure control: The kidneys play a significant role in regulating blood pressure through the renin-angiotensin-aldosterone system (RAAS), which constricts blood vessels and promotes sodium and water retention to increase blood volume and, consequently, blood pressure.
Anatomically, each kidney is approximately 10-12 cm long, 5-7 cm wide, and 3 cm thick, with a weight of about 120-170 grams. They are surrounded by a protective layer of fat and connected to the urinary system through the renal pelvis, ureters, bladder, and urethra.
Anesthetics are medications that are used to block or reduce feelings of pain and sensation, either locally in a specific area of the body or generally throughout the body. They work by depressing the nervous system, interrupting the communication between nerves and the brain. Anesthetics can be administered through various routes such as injection, inhalation, or topical application, depending on the type and the desired effect. There are several classes of anesthetics, including:
1. Local anesthetics: These numb a specific area of the body and are commonly used during minor surgical procedures, dental work, or to relieve pain from injuries. Examples include lidocaine, prilocaine, and bupivacaine.
2. Regional anesthetics: These block nerve impulses in a larger area of the body, such as an arm or leg, and can be used for more extensive surgical procedures. They are often administered through a catheter to provide continuous pain relief over a longer period. Examples include spinal anesthesia, epidural anesthesia, and peripheral nerve blocks.
3. General anesthetics: These cause a state of unconsciousness and are used for major surgical procedures or when the patient needs to be completely immobile during a procedure. They can be administered through inhalation or injection and affect the entire body. Examples include propofol, sevoflurane, and isoflurane.
Anesthetics are typically safe when used appropriately and under medical supervision. However, they can have side effects such as drowsiness, nausea, and respiratory depression. Proper dosing and monitoring by a healthcare professional are essential to minimize the risks associated with anesthesia.
Verapamil is a calcium channel blocker medication that is primarily used to treat hypertension (high blood pressure), angina (chest pain), and certain types of cardiac arrhythmias (irregular heart rhyats). It works by relaxing the smooth muscle cells in the walls of blood vessels, which causes them to dilate or widen, reducing the resistance to blood flow and thereby lowering blood pressure. Verapamil also slows down the conduction of electrical signals within the heart, which can help to regulate the heart rate and rhythm.
In addition to its cardiovascular effects, verapamil is sometimes used off-label for the treatment of other conditions such as migraine headaches, Raynaud's phenomenon, and certain types of tremors. It is available in various forms, including immediate-release tablets, extended-release capsules, and intravenous (IV) injection.
It is important to note that verapamil can interact with other medications, so it is essential to inform your healthcare provider about all the drugs you are taking before starting this medication. Additionally, verapamil should be used with caution in people with certain medical conditions, such as heart failure, liver disease, and low blood pressure.
Enoximone is a medication that belongs to a class of drugs called phosphodiesterase inhibitors. It works by increasing the levels of cyclic adenosine monophosphate (cAMP) in the heart, which leads to relaxation of the heart muscle and improved pumping ability. Enoximone is used to treat chronic heart failure and is often given intravenously in a hospital setting.
The medical definition of 'Enoximone' is:
A selective inhibitor of type III phosphodiesterase, which increases the concentration of cyclic adenosine monophosphate (cAMP) in the heart muscle, leading to vasodilation and positive inotropic effects. Enoximone is used in the treatment of congestive heart failure.
Intravenous injections are a type of medical procedure where medication or fluids are administered directly into a vein using a needle and syringe. This route of administration is also known as an IV injection. The solution injected enters the patient's bloodstream immediately, allowing for rapid absorption and onset of action. Intravenous injections are commonly used to provide quick relief from symptoms, deliver medications that are not easily absorbed by other routes, or administer fluids and electrolytes in cases of dehydration or severe illness. It is important that intravenous injections are performed using aseptic technique to minimize the risk of infection.
Counterpulsation is a medical treatment used in critical care medicine, particularly in the management of cardiovascular conditions. It refers to a technique that involves delivering therapies that counter or oppose the patient's own cardiac cycle. The most common form of counterpulsation is through the use of an intra-aortic balloon pump (IABP).
During IABP, a catheter with a sausage-shaped balloon at its tip is inserted into the patient's aorta, usually through the femoral artery in the groin. The balloon is then connected to a console that controls its inflation and deflation. The console is programmed to detect the patient's cardiac cycle using either the ECG or arterial pressure waveform.
During diastole (when the heart muscle relaxes and fills with blood), the balloon inflates, increasing the volume of blood in the aorta and improving coronary artery perfusion. This helps to increase oxygen delivery to the myocardium (heart muscle) and reduce its workload.
During systole (when the heart muscle contracts and ejects blood), the balloon deflates, reducing afterload (the resistance against which the heart must pump). This reduces the workload of the left ventricle, allowing it to fill more easily during diastole and improving overall cardiac output.
In summary, counterpulsation is a medical intervention that uses therapies, such as intra-aortic balloon pumps, to counter or oppose the patient's own cardiac cycle. This technique aims to improve coronary artery perfusion, reduce afterload, and enhance overall cardiac function.
The prosencephalon is a term used in the field of neuroembryology, which refers to the developmental stage of the forebrain in the embryonic nervous system. It is one of the three primary vesicles that form during the initial stages of neurulation, along with the mesencephalon (midbrain) and rhombencephalon (hindbrain).
The prosencephalon further differentiates into two secondary vesicles: the telencephalon and diencephalon. The telencephalon gives rise to structures such as the cerebral cortex, basal ganglia, and olfactory bulbs, while the diencephalon develops into structures like the thalamus, hypothalamus, and epithalamus.
It is important to note that 'prosencephalon' itself is not used as a medical term in adult neuroanatomy, but it is crucial for understanding the development of the human brain during embryogenesis.
ATP-sensitive potassium (KATP) channels are a type of ion channel found in the membranes of cells, including those in the heart, muscle, and pancreas. These channels are unique because their opening and closing are regulated by the levels of adenosine triphosphate (ATP) and adenosine diphosphate (ADP) in the cell.
Under normal conditions, when ATP levels are high and ADP levels are low, the KATP channels are closed, which allows the cells to maintain their normal electrical activity. However, during times of metabolic stress or ischemia (a lack of blood flow), the levels of ATP in the cell decrease while the levels of ADP increase. This change in the ATP-to-ADP ratio causes the KATP channels to open, which allows potassium ions to flow out of the cell. The efflux of potassium ions then leads to hyperpolarization of the cell membrane, which helps to protect the cells from damage.
In the pancreas, KATP channels play a crucial role in regulating insulin secretion. In the beta cells of the pancreas, an increase in blood glucose levels leads to an increase in ATP production and a decrease in ADP levels, which causes the KATP channels to close. This closure of the KATP channels leads to depolarization of the cell membrane, which triggers the release of insulin.
Overall, KATP channels are important regulators of cellular electrical activity and play a critical role in protecting cells from damage during times of metabolic stress or ischemia.
Telemetry is the automated measurement and wireless transmission of data from remote or inaccessible sources to receiving stations for monitoring and analysis. In a medical context, telemetry is often used to monitor patients' vital signs such as heart rate, blood pressure, oxygen levels, and other important physiological parameters continuously and remotely. This technology allows healthcare providers to track patients' conditions over time, detect any abnormalities or trends, and make informed decisions about their care, even when they are not physically present with the patient. Telemetry is commonly used in hospitals, clinics, and research settings to monitor patients during procedures, after surgery, or during extended stays in intensive care units.
Tiopronin is a medication that belongs to a class of drugs called mucolytic agents. It works by breaking down mucus in the respiratory tract, making it easier to cough up and clear the airways. Tiopronin is also known as tiopronin sodium or Thiola®.
In addition to its use as a mucolytic agent, tiopronin has been found to be effective in reducing the formation of cystine kidney stones in patients with a rare genetic disorder called cystinuria. It works by binding to cystine in the urine and preventing it from forming into crystals or stones.
Tiopronin is available as a tablet or oral solution and is typically taken several times a day, with dosing adjusted based on the patient's individual needs and response to treatment. Common side effects of tiopronin include stomach upset, loss of appetite, and rash.
Brain Natriuretic Peptide (BNP) is a type of natriuretic peptide that is primarily produced in the heart, particularly in the ventricles. Although it was initially identified in the brain, hence its name, it is now known that the cardiac ventricles are the main source of BNP in the body.
BNP is released into the bloodstream in response to increased stretching or distension of the heart muscle cells due to conditions such as heart failure, hypertension, and myocardial infarction (heart attack). Once released, BNP binds to specific receptors in the kidneys, causing an increase in urine production and excretion of sodium, which helps reduce fluid volume and decrease the workload on the heart.
BNP also acts as a hormone that regulates various physiological functions, including blood pressure, cardiac remodeling, and inflammation. Measuring BNP levels in the blood is a useful diagnostic tool for detecting and monitoring heart failure, as higher levels of BNP are associated with more severe heart dysfunction.
Cardiomyopathies are a group of diseases that affect the heart muscle, leading to mechanical and/or electrical dysfunction. The American Heart Association (AHA) defines cardiomyopathies as "a heterogeneous group of diseases of the myocardium associated with mechanical and/or electrical dysfunction that usually (but not always) exhibit inappropriate ventricular hypertrophy or dilatation and frequently lead to heart failure."
There are several types of cardiomyopathies, including:
1. Dilated cardiomyopathy (DCM): This is the most common type of cardiomyopathy, characterized by an enlarged left ventricle and impaired systolic function, leading to heart failure.
2. Hypertrophic cardiomyopathy (HCM): In this type, there is abnormal thickening of the heart muscle, particularly in the septum between the two ventricles, which can obstruct blood flow and increase the risk of arrhythmias.
3. Restrictive cardiomyopathy (RCM): This is a rare form of cardiomyopathy characterized by stiffness of the heart muscle, impaired relaxation, and diastolic dysfunction, leading to reduced filling of the ventricles and heart failure.
4. Arrhythmogenic right ventricular cardiomyopathy (ARVC): In this type, there is replacement of the normal heart muscle with fatty or fibrous tissue, primarily affecting the right ventricle, which can lead to arrhythmias and sudden cardiac death.
5. Unclassified cardiomyopathies: These are conditions that do not fit into any of the above categories but still significantly affect the heart muscle and function.
Cardiomyopathies can be caused by genetic factors, acquired conditions (e.g., infections, toxins, or autoimmune disorders), or a combination of both. The diagnosis typically involves a comprehensive evaluation, including medical history, physical examination, electrocardiogram (ECG), echocardiography, cardiac magnetic resonance imaging (MRI), and sometimes genetic testing. Treatment depends on the type and severity of the condition but may include medications, lifestyle modifications, implantable devices, or even heart transplantation in severe cases.
The postoperative period is the time following a surgical procedure during which the patient's response to the surgery and anesthesia is monitored, and any complications or adverse effects are managed. This period can vary in length depending on the type of surgery and the individual patient's needs, but it typically includes the immediate recovery phase in the post-anesthesia care unit (PACU) or recovery room, as well as any additional time spent in the hospital for monitoring and management of pain, wound healing, and other aspects of postoperative care.
The goals of postoperative care are to ensure the patient's safety and comfort, promote optimal healing and rehabilitation, and minimize the risk of complications such as infection, bleeding, or other postoperative issues. The specific interventions and treatments provided during this period will depend on a variety of factors, including the type and extent of surgery performed, the patient's overall health and medical history, and any individualized care plans developed in consultation with the patient and their healthcare team.
Recurrence, in a medical context, refers to the return of symptoms or signs of a disease after a period of improvement or remission. It indicates that the condition has not been fully eradicated and may require further treatment. Recurrence is often used to describe situations where a disease such as cancer comes back after initial treatment, but it can also apply to other medical conditions. The likelihood of recurrence varies depending on the type of disease and individual patient factors.
Hydrogen sulfide (H2S) is a colorless, flammable, and extremely toxic gas with a strong odor of rotten eggs. It is a naturally occurring compound that is produced in various industrial processes and is also found in some natural sources like volcanoes, hot springs, and swamps.
In the medical context, hydrogen sulfide is known to have both toxic and therapeutic effects on the human body. At high concentrations, it can cause respiratory failure, unconsciousness, and even death. However, recent studies have shown that at low levels, hydrogen sulfide may act as a signaling molecule in the human body, playing a role in various physiological processes such as regulating blood flow, reducing inflammation, and protecting against oxidative stress.
It's worth noting that exposure to high levels of hydrogen sulfide can be life-threatening, and immediate medical attention is required in case of exposure.
Hyperemia is a medical term that refers to an increased flow or accumulation of blood in certain capillaries or vessels within an organ or tissue, resulting in its redness and warmth. This can occur due to various reasons such as physical exertion, emotional excitement, local injury, or specific medical conditions.
There are two types of hyperemia: active and passive. Active hyperemia is a physiological response where the blood flow increases as a result of the metabolic demands of the organ or tissue. For example, during exercise, muscles require more oxygen and nutrients, leading to an increase in blood flow. Passive hyperemia, on the other hand, occurs when there is a blockage in the venous outflow, causing the blood to accumulate in the affected area. This can result from conditions like thrombosis or vasoconstriction.
It's important to note that while hyperemia itself is not a disease, it can be a symptom of various underlying medical conditions and should be evaluated by a healthcare professional if it persists or is accompanied by other symptoms.
Vagus nerve stimulation (VNS) is a medical treatment that involves the use of a device to send electrical signals to the vagus nerve, which is a key part of the body's autonomic nervous system. The autonomic nervous system controls various automatic functions of the body, such as heart rate and digestion.
In VNS, a small generator is implanted in the chest, and thin wires are routed under the skin to the vagus nerve in the neck. The generator is programmed to send electrical signals to the vagus nerve at regular intervals. These signals can help regulate certain body functions and have been found to be effective in treating a number of conditions, including epilepsy and depression.
The exact mechanism by which VNS works is not fully understood, but it is thought to affect the release of neurotransmitters, chemicals that transmit signals in the brain. This can help reduce seizure activity in people with epilepsy and improve mood and other symptoms in people with depression.
VNS is typically used as a last resort for people who have not responded to other treatments. It is generally considered safe, but like any medical procedure, it does carry some risks, such as infection, bleeding, and damage to the vagus nerve or surrounding tissues.
Contrast media are substances that are administered to a patient in order to improve the visibility of internal body structures or processes in medical imaging techniques such as X-rays, CT scans, MRI scans, and ultrasounds. These media can be introduced into the body through various routes, including oral, rectal, or intravenous administration.
Contrast media work by altering the appearance of bodily structures in imaging studies. For example, when a patient undergoes an X-ray examination, contrast media can be used to highlight specific organs, tissues, or blood vessels, making them more visible on the resulting images. In CT and MRI scans, contrast media can help to enhance the differences between normal and abnormal tissues, allowing for more accurate diagnosis and treatment planning.
There are several types of contrast media available, each with its own specific properties and uses. Some common examples include barium sulfate, which is used as a contrast medium in X-ray studies of the gastrointestinal tract, and iodinated contrast media, which are commonly used in CT scans to highlight blood vessels and other structures.
While contrast media are generally considered safe, they can sometimes cause adverse reactions, ranging from mild symptoms such as nausea or hives to more serious complications such as anaphylaxis or kidney damage. As a result, it is important for healthcare providers to carefully evaluate each patient's medical history and individual risk factors before administering contrast media.
Inflammation is a complex biological response of tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. It is characterized by the following signs: rubor (redness), tumor (swelling), calor (heat), dolor (pain), and functio laesa (loss of function). The process involves the activation of the immune system, recruitment of white blood cells, and release of inflammatory mediators, which contribute to the elimination of the injurious stimuli and initiation of the healing process. However, uncontrolled or chronic inflammation can also lead to tissue damage and diseases.
Capillaries are the smallest blood vessels in the body, with diameters that range from 5 to 10 micrometers. They form a network of tiny tubes that connect the arterioles (small branches of arteries) and venules (small branches of veins), allowing for the exchange of oxygen, carbon dioxide, nutrients, and waste products between the blood and the surrounding tissues.
Capillaries are composed of a single layer of endothelial cells that surround a hollow lumen through which blood flows. The walls of capillaries are extremely thin, allowing for easy diffusion of molecules between the blood and the surrounding tissue. This is essential for maintaining the health and function of all body tissues.
Capillaries can be classified into three types based on their structure and function: continuous, fenestrated, and sinusoidal. Continuous capillaries have a continuous layer of endothelial cells with tight junctions that restrict the passage of large molecules. Fenestrated capillaries have small pores or "fenestrae" in the endothelial cell walls that allow for the passage of larger molecules, such as proteins and lipids. Sinusoidal capillaries are found in organs with high metabolic activity, such as the liver and spleen, and have large, irregular spaces between the endothelial cells that allow for the exchange of even larger molecules.
Overall, capillaries play a critical role in maintaining the health and function of all body tissues by allowing for the exchange of nutrients, oxygen, and waste products between the blood and surrounding tissues.
Phosphorylation is the process of adding a phosphate group (a molecule consisting of one phosphorus atom and four oxygen atoms) to a protein or other organic molecule, which is usually done by enzymes called kinases. This post-translational modification can change the function, localization, or activity of the target molecule, playing a crucial role in various cellular processes such as signal transduction, metabolism, and regulation of gene expression. Phosphorylation is reversible, and the removal of the phosphate group is facilitated by enzymes called phosphatases.
Genetic therapy, also known as gene therapy, is a medical intervention that involves the use of genetic material, such as DNA or RNA, to treat or prevent diseases. It works by introducing functional genes into cells to replace missing or faulty ones caused by genetic disorders or mutations. The introduced gene is incorporated into the recipient's genome, allowing for the production of a therapeutic protein that can help manage the disease symptoms or even cure the condition.
There are several approaches to genetic therapy, including:
1. Replacing a faulty gene with a healthy one
2. Inactivating or "silencing" a dysfunctional gene causing a disease
3. Introducing a new gene into the body to help fight off a disease, such as cancer
Genetic therapy holds great promise for treating various genetic disorders, including cystic fibrosis, muscular dystrophy, hemophilia, and certain types of cancer. However, it is still an evolving field with many challenges, such as efficient gene delivery, potential immune responses, and ensuring the safety and long-term effectiveness of the therapy.
Thromboxane A2 (TXA2) is a potent prostanoid, a type of lipid compound derived from arachidonic acid. It is primarily produced and released by platelets upon activation during the process of hemostasis (the body's response to stop bleeding). TXA2 acts as a powerful vasoconstrictor, causing blood vessels to narrow, which helps limit blood loss at the site of injury. Additionally, it promotes platelet aggregation, contributing to the formation of a stable clot and preventing further bleeding. However, uncontrolled or excessive production of TXA2 can lead to thrombotic events such as heart attacks and strokes. Its effects are balanced by prostacyclin (PGI2), which is produced by endothelial cells and has opposing actions, acting as a vasodilator and inhibiting platelet aggregation. The balance between TXA2 and PGI2 helps maintain vascular homeostasis.
Blood substitutes, also known as artificial blood or blood surrogates, are fluids that are designed to mimic some of the properties and functions of human blood. They are used as a replacement for blood transfusions in situations where blood is not available or when it is not safe to use. Blood substitutes can be divided into two main categories: oxygen-carrying and non-oxygen-carrying.
Oxygen-carrying blood substitutes contain artificial molecules called hemoglobin-based oxygen carriers (HBOCs) that are designed to carry oxygen from the lungs to the body's tissues. These HBOCs can be derived from human or animal hemoglobin, or they can be synthetically produced.
Non-oxygen-carrying blood substitutes, on the other hand, do not contain hemoglobin and are used primarily to restore intravascular volume and maintain blood pressure in cases of hypovolemia (low blood volume) caused by bleeding or dehydration. These products include crystalloids, such as saline solution and lactated Ringer's solution, and colloids, such as albumin and hydroxyethyl starch solutions.
It is important to note that while blood substitutes can be useful in certain situations, they are not a perfect substitute for human blood. They do not provide all of the functions of blood, such as immune defense and clotting, and their use is associated with some risks, including allergic reactions, kidney damage, and increased oxygen free radical production. Therefore, they should only be used when there is no suitable alternative available.
Benzophenanthridines are a class of chemical compounds that contain a benzophenanthrene skeleton, which is a polycyclic aromatic hydrocarbon structure made up of three benzene rings fused together. Benzophenanthridine alkaloids are naturally occurring compounds found in plants and have various biological activities, including anti-inflammatory, antimicrobial, and antitumor properties. Some well-known benzophenanthridine alkaloids include sanguinarine, chelerythrine, and berberine. These compounds are known to interact with various biological targets such as enzymes, receptors, and DNA, making them of interest in pharmaceutical research and development.
Enzyme activation refers to the process by which an enzyme becomes biologically active and capable of carrying out its specific chemical or biological reaction. This is often achieved through various post-translational modifications, such as proteolytic cleavage, phosphorylation, or addition of cofactors or prosthetic groups to the enzyme molecule. These modifications can change the conformation or structure of the enzyme, exposing or creating a binding site for the substrate and allowing the enzymatic reaction to occur.
For example, in the case of proteolytic cleavage, an inactive precursor enzyme, known as a zymogen, is cleaved into its active form by a specific protease. This is seen in enzymes such as trypsin and chymotrypsin, which are initially produced in the pancreas as inactive precursors called trypsinogen and chymotrypsinogen, respectively. Once they reach the small intestine, they are activated by enteropeptidase, a protease that cleaves a specific peptide bond, releasing the active enzyme.
Phosphorylation is another common mechanism of enzyme activation, where a phosphate group is added to a specific serine, threonine, or tyrosine residue on the enzyme by a protein kinase. This modification can alter the conformation of the enzyme and create a binding site for the substrate, allowing the enzymatic reaction to occur.
Enzyme activation is a crucial process in many biological pathways, as it allows for precise control over when and where specific reactions take place. It also provides a mechanism for regulating enzyme activity in response to various signals and stimuli, such as hormones, neurotransmitters, or changes in the intracellular environment.
The refractory period, electrophysiological, refers to the time interval during which a cardiac or neural cell is unable to respond to a new stimulus immediately after an action potential has been generated. This period is divided into two phases: the absolute refractory period and the relative refractory period.
During the absolute refractory period, the cell cannot be re-stimulated, regardless of the strength of the stimulus, due to the rapid inactivation of voltage-gated sodium channels that are responsible for the rapid depolarization during an action potential. This phase is crucial for maintaining the unidirectional conduction of electrical impulses and preventing the occurrence of re-entry circuits, which can lead to life-threatening arrhythmias in the heart or hyperexcitability in neural tissue.
The relative refractory period follows the absolute refractory period and is characterized by a reduced excitability of the cell. During this phase, a stronger than normal stimulus is required to elicit an action potential due to the slower recovery of voltage-gated sodium channels and the partial activation of potassium channels, which promote repolarization. The duration of both the absolute and relative refractory periods varies depending on the cell type, its physiological state, and other factors such as temperature and pH.
In summary, the electrophysiological refractory period is a fundamental property of excitable cells that ensures proper electrical signaling and prevents uncontrolled excitation or re-entry circuits.
Glycolysis is a fundamental metabolic pathway that occurs in the cytoplasm of cells, consisting of a series of biochemical reactions. It's the process by which a six-carbon glucose molecule is broken down into two three-carbon pyruvate molecules. This process generates a net gain of two ATP molecules (the main energy currency in cells), two NADH molecules, and two water molecules.
Glycolysis can be divided into two stages: the preparatory phase (or 'energy investment' phase) and the payoff phase (or 'energy generation' phase). During the preparatory phase, glucose is phosphorylated twice to form glucose-6-phosphate and then converted to fructose-1,6-bisphosphate. These reactions consume two ATP molecules but set up the subsequent breakdown of fructose-1,6-bisphosphate into triose phosphates in the payoff phase. In this second stage, each triose phosphate is further oxidized and degraded to produce one pyruvate molecule, one NADH molecule, and one ATP molecule through substrate-level phosphorylation.
Glycolysis does not require oxygen to proceed; thus, it can occur under both aerobic (with oxygen) and anaerobic (without oxygen) conditions. In the absence of oxygen, the pyruvate produced during glycolysis is further metabolized through fermentation pathways such as lactic acid fermentation or alcohol fermentation to regenerate NAD+, which is necessary for glycolysis to continue.
In summary, glycolysis is a crucial process in cellular energy metabolism, allowing cells to convert glucose into ATP and other essential molecules while also serving as a starting point for various other biochemical pathways.
Inhalational anesthetics are a type of general anesthetic that is administered through the person's respiratory system. They are typically delivered in the form of vapor or gas, which is inhaled through a mask or breathing tube. Commonly used inhalational anesthetics include sevoflurane, desflurane, isoflurane, and nitrous oxide. These agents work by depressing the central nervous system, leading to a loss of consciousness and an inability to feel pain. They are often used for their rapid onset and offset of action, making them useful for both induction and maintenance of anesthesia during surgical procedures.
Transesophageal echocardiography (TEE) is a type of echocardiogram, which is a medical test that uses sound waves to create detailed images of the heart. In TEE, a special probe containing a transducer is passed down the esophagus (the tube that connects the mouth to the stomach) to obtain views of the heart from behind. This allows for more detailed images of the heart structures and function compared to a standard echocardiogram, which uses a probe placed on the chest. TEE is often used in patients with poor image quality from a standard echocardiogram or when more detailed images are needed to diagnose or monitor certain heart conditions. It is typically performed by a trained cardiologist or sonographer under the direction of a cardiologist.
Mannitol is a type of sugar alcohol (a sugar substitute) used primarily as a diuretic to reduce brain swelling caused by traumatic brain injury or other causes that induce increased pressure in the brain. It works by drawing water out of the body through the urine. It's also used before surgeries in the heart, lungs, and kidneys to prevent fluid buildup.
In addition, mannitol is used in medical laboratories as a medium for growing bacteria and other microorganisms, and in some types of chemical research. In the clinic, it is also used as an osmotic agent in eye drops to reduce the pressure inside the eye in conditions such as glaucoma.
It's important to note that mannitol should be used with caution in patients with heart or kidney disease, as well as those who are dehydrated, because it can lead to electrolyte imbalances and other complications.
Nitrates are chemical compounds that consist of a nitrogen atom bonded to three oxygen atoms (NO3-). In the context of medical science, nitrates are often discussed in relation to their use as medications or their presence in food and water.
As medications, nitrates are commonly used to treat angina (chest pain) caused by coronary artery disease. Nitrates work by relaxing and widening blood vessels, which improves blood flow and reduces the workload on the heart. Some examples of nitrate medications include nitroglycerin, isosorbide dinitrate, and isosorbide mononitrate.
In food and water, nitrates are naturally occurring compounds that can be found in a variety of vegetables, such as spinach, beets, and lettuce. They can also be present in fertilizers and industrial waste, which can contaminate groundwater and surface water sources. While nitrates themselves are not harmful, they can be converted into potentially harmful compounds called nitrites under certain conditions, particularly in the digestive system of young children or in the presence of bacteria such as those found in unpasteurized foods. Excessive levels of nitrites can react with hemoglobin in the blood to form methemoglobin, which cannot transport oxygen effectively and can lead to a condition called methemoglobinemia.
Physiological stress is a response of the body to a demand or threat that disrupts homeostasis and activates the autonomic nervous system and hypothalamic-pituitary-adrenal (HPA) axis. This results in the release of stress hormones such as adrenaline, cortisol, and noradrenaline, which prepare the body for a "fight or flight" response. Increased heart rate, rapid breathing, heightened sensory perception, and increased alertness are some of the physiological changes that occur during this response. Chronic stress can have negative effects on various bodily functions, including the immune, cardiovascular, and nervous systems.
Transgenic mice are genetically modified rodents that have incorporated foreign DNA (exogenous DNA) into their own genome. This is typically done through the use of recombinant DNA technology, where a specific gene or genetic sequence of interest is isolated and then introduced into the mouse embryo. The resulting transgenic mice can then express the protein encoded by the foreign gene, allowing researchers to study its function in a living organism.
The process of creating transgenic mice usually involves microinjecting the exogenous DNA into the pronucleus of a fertilized egg, which is then implanted into a surrogate mother. The offspring that result from this procedure are screened for the presence of the foreign DNA, and those that carry the desired genetic modification are used to establish a transgenic mouse line.
Transgenic mice have been widely used in biomedical research to model human diseases, study gene function, and test new therapies. They provide a valuable tool for understanding complex biological processes and developing new treatments for a variety of medical conditions.
NG-Nitroarginine Methyl Ester (L-NAME) is not a medication, but rather a research chemical used in scientific studies. It is an inhibitor of nitric oxide synthase, an enzyme that synthesizes nitric oxide, a molecule involved in the relaxation of blood vessels.
Therefore, L-NAME is often used in experiments to investigate the role of nitric oxide in various physiological and pathophysiological processes. It is important to note that the use of L-NAME in humans is not approved for therapeutic purposes due to its potential side effects, which can include hypertension, decreased renal function, and decreased cerebral blood flow.
Vasoconstriction is a medical term that refers to the narrowing of blood vessels due to the contraction of the smooth muscle in their walls. This process decreases the diameter of the lumen (the inner space of the blood vessel) and reduces blood flow through the affected vessels. Vasoconstriction can occur throughout the body, but it is most noticeable in the arterioles and precapillary sphincters, which control the amount of blood that flows into the capillary network.
The autonomic nervous system, specifically the sympathetic division, plays a significant role in regulating vasoconstriction through the release of neurotransmitters like norepinephrine (noradrenaline). Various hormones and chemical mediators, such as angiotensin II, endothelin-1, and serotonin, can also induce vasoconstriction.
Vasoconstriction is a vital physiological response that helps maintain blood pressure and regulate blood flow distribution in the body. However, excessive or prolonged vasoconstriction may contribute to several pathological conditions, including hypertension, stroke, and peripheral vascular diseases.
Halothane is a general anesthetic agent, which is a volatile liquid that evaporates easily and can be inhaled. It is used to produce and maintain general anesthesia (a state of unconsciousness) during surgical procedures. Halothane is known for its rapid onset and offset of action, making it useful for both induction and maintenance of anesthesia.
The medical definition of Halothane is:
Halothane (2-bromo-2-chloro-1,1,1-trifluoroethane) is a volatile liquid general anesthetic agent with a mild, sweet odor. It is primarily used for the induction and maintenance of general anesthesia in surgical procedures due to its rapid onset and offset of action. Halothane is administered via inhalation and acts by depressing the central nervous system, leading to a reversible loss of consciousness and analgesia.
It's important to note that Halothane has been associated with rare cases of severe liver injury (hepatotoxicity) and anaphylaxis (a severe, life-threatening allergic reaction). These risks have led to the development and use of alternative general anesthetic agents with better safety profiles.
Exercise tolerance is a term used to describe the ability of an individual to perform physical activity or exercise without experiencing symptoms such as shortness of breath, chest pain, or undue fatigue. It is often used as a measure of cardiovascular fitness and can be assessed through various tests, such as a stress test or a six-minute walk test. Exercise intolerance may indicate the presence of underlying medical conditions, such as heart disease, lung disease, or deconditioning.
Angiography is a medical procedure in which an x-ray image is taken to visualize the internal structure of blood vessels, arteries, or veins. This is done by injecting a radiopaque contrast agent (dye) into the blood vessel using a thin, flexible catheter. The dye makes the blood vessels visible on an x-ray image, allowing doctors to diagnose and treat various medical conditions such as blockages, narrowing, or malformations of the blood vessels.
There are several types of angiography, including:
* Cardiac angiography (also called coronary angiography) - used to examine the blood vessels of the heart
* Cerebral angiography - used to examine the blood vessels of the brain
* Peripheral angiography - used to examine the blood vessels in the limbs or other parts of the body.
Angiography is typically performed by a radiologist, cardiologist, or vascular surgeon in a hospital setting. It can help diagnose conditions such as coronary artery disease, aneurysms, and peripheral arterial disease, among others.
Magnetic Resonance Spectroscopy (MRS) is a non-invasive diagnostic technique that provides information about the biochemical composition of tissues, including their metabolic state. It is often used in conjunction with Magnetic Resonance Imaging (MRI) to analyze various metabolites within body tissues, such as the brain, heart, liver, and muscles.
During MRS, a strong magnetic field, radio waves, and a computer are used to produce detailed images and data about the concentration of specific metabolites in the targeted tissue or organ. This technique can help detect abnormalities related to energy metabolism, neurotransmitter levels, pH balance, and other biochemical processes, which can be useful for diagnosing and monitoring various medical conditions, including cancer, neurological disorders, and metabolic diseases.
There are different types of MRS, such as Proton (^1^H) MRS, Phosphorus-31 (^31^P) MRS, and Carbon-13 (^13^C) MRS, each focusing on specific elements or metabolites within the body. The choice of MRS technique depends on the clinical question being addressed and the type of information needed for diagnosis or monitoring purposes.
A Sodium-Hydrogen Antiporter (NHA) is a type of membrane transport protein that exchanges sodium ions (Na+) and protons (H+) across a biological membrane. It is also known as a Na+/H+ antiporter or exchanger. This exchange mechanism plays a crucial role in regulating pH, cell volume, and intracellular sodium concentration within various cells and organelles, including the kidney, brain, heart, and mitochondria.
In general, NHA transporters utilize the energy generated by the electrochemical gradient of sodium ions across a membrane to drive the uphill transport of protons from inside to outside the cell or organelle. This process helps maintain an optimal intracellular pH and volume, which is essential for proper cellular function and homeostasis.
There are several isoforms of Sodium-Hydrogen Antiporters found in different tissues and organelles, each with distinct physiological roles and regulatory mechanisms. Dysfunction or alterations in NHA activity have been implicated in various pathophysiological conditions, such as hypertension, heart failure, neurological disorders, and cancer.
Protein-kinase B, also known as AKT, is a group of intracellular proteins that play a crucial role in various cellular processes such as glucose metabolism, apoptosis, cell proliferation, transcription, and cell migration. The AKT family includes three isoforms: AKT1, AKT2, and AKT3, which are encoded by the genes PKBalpha, PKBbeta, and PKBgamma, respectively.
Proto-oncogene proteins c-AKT refer to the normal, non-mutated forms of these proteins that are involved in the regulation of cell growth and survival under physiological conditions. However, when these genes are mutated or overexpressed, they can become oncogenes, leading to uncontrolled cell growth and cancer development.
Activation of c-AKT occurs through a signaling cascade that begins with the binding of extracellular ligands such as insulin-like growth factor 1 (IGF-1) or epidermal growth factor (EGF) to their respective receptors on the cell surface. This triggers a series of phosphorylation events that ultimately lead to the activation of c-AKT, which then phosphorylates downstream targets involved in various cellular processes.
In summary, proto-oncogene proteins c-AKT are normal intracellular proteins that play essential roles in regulating cell growth and survival under physiological conditions. However, their dysregulation can contribute to cancer development and progression.
Single-domain antibodies (sdAbs), also known as nanobodies or VHHs, are antigen-binding fragments derived from the heavy-chain only antibodies found in camelids (camels, llamas, and alpacas) and some shark species. These unique antibodies lack light chains and consist of a single variable domain (VHH) that can bind to specific antigens with high affinity and stability. The small size (12-15 kDa), robustness, and solubility make sdAbs attractive for various biotechnological and therapeutic applications, including diagnostics, targeted drug delivery, and protein engineering.
Cell survival refers to the ability of a cell to continue living and functioning normally, despite being exposed to potentially harmful conditions or treatments. This can include exposure to toxins, radiation, chemotherapeutic drugs, or other stressors that can damage cells or interfere with their normal processes.
In scientific research, measures of cell survival are often used to evaluate the effectiveness of various therapies or treatments. For example, researchers may expose cells to a particular drug or treatment and then measure the percentage of cells that survive to assess its potential therapeutic value. Similarly, in toxicology studies, measures of cell survival can help to determine the safety of various chemicals or substances.
It's important to note that cell survival is not the same as cell proliferation, which refers to the ability of cells to divide and multiply. While some treatments may promote cell survival, they may also inhibit cell proliferation, making them useful for treating diseases such as cancer. Conversely, other treatments may be designed to specifically target and kill cancer cells, even if it means sacrificing some healthy cells in the process.
Brain infarction, also known as cerebral infarction, is a type of stroke that occurs when blood flow to a part of the brain is blocked, often by a blood clot. This results in oxygen and nutrient deprivation to the brain tissue, causing it to become damaged or die. The effects of a brain infarction depend on the location and extent of the damage, but can include weakness, numbness, paralysis, speech difficulties, memory loss, and other neurological symptoms.
Brain infarctions are often caused by underlying medical conditions such as atherosclerosis, atrial fibrillation, or high blood pressure. Treatment typically involves addressing the underlying cause of the blockage, administering medications to dissolve clots or prevent further clotting, and providing supportive care to manage symptoms and prevent complications.
Emission computed tomography (ECT) is a type of tomographic imaging technique in which an emission signal from within the body is detected to create cross-sectional images of that signal's distribution. In Emission-Computed Tomography (ECT), a radionuclide is introduced into the body, usually through injection, inhalation or ingestion. The radionuclide emits gamma rays that are then detected by external gamma cameras.
The data collected from these cameras is then used to create cross-sectional images of the distribution of the radiopharmaceutical within the body. This allows for the identification and quantification of functional information about specific organs or systems within the body, such as blood flow, metabolic activity, or receptor density.
One common type of Emission-Computed Tomography is Single Photon Emission Computed Tomography (SPECT), which uses a single gamma camera that rotates around the patient to collect data from multiple angles. Another type is Positron Emission Tomography (PET), which uses positron-emitting radionuclides and detects the coincident gamma rays emitted by the annihilation of positrons and electrons.
Overall, ECT is a valuable tool in medical imaging for diagnosing and monitoring various diseases, including cancer, heart disease, and neurological disorders.
Microvessels are the smallest blood vessels in the body, including capillaries, venules, and arterioles. They form a crucial part of the circulatory system, responsible for delivering oxygen and nutrients to tissues and organs while removing waste products. Capillaries, the tiniest microvessels, facilitate the exchange of substances between blood and tissue cells through their thin walls. Overall, microvessels play a vital role in maintaining proper organ function and overall health.
Hypoxia-Ischemia, Brain refers to a condition characterized by a reduced supply of oxygen (hypoxia) and blood flow (ischemia) to the brain. This can lead to serious damage or death of brain cells, depending on the severity and duration of the hypoxic-ischemic event.
Hypoxia occurs when there is insufficient oxygen available to meet the metabolic needs of the brain tissue. Ischemia results from a decrease in blood flow, which can be caused by various factors such as cardiac arrest, stroke, or severe respiratory distress. When both hypoxia and ischemia occur together, they can have a synergistic effect, leading to more severe brain damage.
Brain Hypoxia-Ischemia can result in neurological deficits, cognitive impairment, and physical disabilities, depending on the area of the brain affected. Treatment typically focuses on addressing the underlying cause of the hypoxia-ischemia and providing supportive care to minimize secondary damage. In some cases, therapeutic hypothermia may be used to reduce metabolic demands and protect vulnerable brain tissue.
Desipramine is a tricyclic antidepressant (TCA) that is primarily used to treat depression. It works by increasing the levels of certain neurotransmitters, such as norepinephrine and serotonin, in the brain. These neurotransmitters are important for maintaining mood, emotion, and behavior.
Desipramine is also sometimes used off-label to treat other conditions, such as anxiety disorders, chronic pain, and attention deficit hyperactivity disorder (ADHD). It is available in oral form and is typically taken one to three times a day.
Like all medications, desipramine can cause side effects, which can include dry mouth, blurred vision, constipation, dizziness, and drowsiness. More serious side effects are rare but can include heart rhythm problems, seizures, and increased suicidal thoughts or behavior in some people, particularly children and adolescents.
It is important to take desipramine exactly as prescribed by a healthcare provider and to report any bothersome or unusual symptoms promptly. Regular follow-up appointments with a healthcare provider are also recommended to monitor the effectiveness and safety of the medication.
Ventricular Tachycardia (VT) is a rapid heart rhythm that originates from the ventricles, the lower chambers of the heart. It is defined as three or more consecutive ventricular beats at a rate of 120 beats per minute or greater in a resting adult. This abnormal heart rhythm can cause the heart to pump less effectively, leading to inadequate blood flow to the body and potentially life-threatening conditions such as hypotension, shock, or cardiac arrest.
VT can be classified into three types based on its duration, hemodynamic stability, and response to treatment:
1. Non-sustained VT (NSVT): It lasts for less than 30 seconds and is usually well tolerated without causing significant symptoms or hemodynamic instability.
2. Sustained VT (SVT): It lasts for more than 30 seconds, causes symptoms such as palpitations, dizziness, shortness of breath, or chest pain, and may lead to hemodynamic instability.
3. Pulseless VT: It is a type of sustained VT that does not produce a pulse, blood pressure, or adequate cardiac output, requiring immediate electrical cardioversion or defibrillation to restore a normal heart rhythm.
VT can occur in people with various underlying heart conditions such as coronary artery disease, cardiomyopathy, valvular heart disease, congenital heart defects, and electrolyte imbalances. It can also be triggered by certain medications, substance abuse, or electrical abnormalities in the heart. Prompt diagnosis and treatment of VT are crucial to prevent complications and improve outcomes.
Doppler echocardiography is a type of ultrasound test that uses high-frequency sound waves to produce detailed images of the heart and its blood vessels. It measures the direction and speed of blood flow in the heart and major blood vessels leading to and from the heart. This helps to evaluate various conditions such as valve problems, congenital heart defects, and heart muscle diseases.
In Doppler echocardiography, a small handheld device called a transducer is placed on the chest, which emits sound waves that bounce off the heart and blood vessels. The transducer then picks up the returning echoes, which are processed by a computer to create moving images of the heart.
The Doppler effect is used to measure the speed and direction of blood flow. This occurs when the frequency of the sound waves changes as they bounce off moving objects, such as red blood cells. By analyzing these changes, the ultrasound machine can calculate the velocity and direction of blood flow in different parts of the heart.
Doppler echocardiography is a non-invasive test that does not require any needles or dyes. It is generally safe and painless, although patients may experience some discomfort from the pressure applied by the transducer on the chest. The test usually takes about 30 to 60 minutes to complete.
Pulmonary wedge pressure, also known as pulmonary capillary wedge pressure (PCWP) or left heart filling pressure, is a measurement obtained during right heart catheterization. It reflects the pressure in the left atrium, which is an estimate of the diastolic pressure in the left ventricle. Normal PCWP ranges from 4 to 12 mmHg. Increased pulmonary wedge pressure can indicate heart failure or other cardiac disorders that affect the left side of the heart.
Thrombolytic therapy, also known as thrombolysis, is a medical treatment that uses medications called thrombolytics or fibrinolytics to dissolve or break down blood clots (thrombi) in blood vessels. These clots can obstruct the flow of blood to vital organs such as the heart, lungs, or brain, leading to serious conditions like myocardial infarction (heart attack), pulmonary embolism, or ischemic stroke.
The goal of thrombolytic therapy is to restore blood flow as quickly and efficiently as possible to prevent further damage to the affected organ and potentially save lives. Commonly used thrombolytic drugs include alteplase (tPA), reteplase, and tenecteplase. It's essential to administer these medications as soon as possible after the onset of symptoms for optimal treatment outcomes. However, there are risks associated with thrombolytic therapy, such as an increased chance of bleeding complications, which must be carefully weighed against its benefits in each individual case.
Electrophysiology is a branch of medicine that deals with the electrical activities of the body, particularly the heart. In a medical context, electrophysiology studies (EPS) are performed to assess abnormal heart rhythms (arrhythmias) and to evaluate the effectiveness of certain treatments, such as medication or pacemakers.
During an EPS, electrode catheters are inserted into the heart through blood vessels in the groin or neck. These catheters can record the electrical activity of the heart and stimulate it to help identify the source of the arrhythmia. The information gathered during the study can help doctors determine the best course of treatment for each patient.
In addition to cardiac electrophysiology, there are also other subspecialties within electrophysiology, such as neuromuscular electrophysiology, which deals with the electrical activity of the nervous system and muscles.
Nifedipine is an antihypertensive and calcium channel blocker medication. It works by relaxing the muscles of the blood vessels, which helps to lower blood pressure and improve the supply of oxygen and nutrients to the heart. Nifedipine is used to treat high blood pressure (hypertension), angina (chest pain), and certain types of heart rhythm disorders.
In medical terms, nifedipine can be defined as: "A dihydropyridine calcium channel blocker that is used in the treatment of hypertension, angina pectoris, and Raynaud's phenomenon. It works by inhibiting the influx of calcium ions into vascular smooth muscle and cardiac muscle, which results in relaxation of the vascular smooth muscle and decreased workload on the heart."
Cerebral arteries refer to the blood vessels that supply oxygenated blood to the brain. These arteries branch off from the internal carotid arteries and the vertebral arteries, which combine to form the basilar artery. The major cerebral arteries include:
1. Anterior cerebral artery (ACA): This artery supplies blood to the frontal lobes of the brain, including the motor and sensory cortices responsible for movement and sensation in the lower limbs.
2. Middle cerebral artery (MCA): The MCA is the largest of the cerebral arteries and supplies blood to the lateral surface of the brain, including the temporal, parietal, and frontal lobes. It is responsible for providing blood to areas involved in motor function, sensory perception, speech, memory, and vision.
3. Posterior cerebral artery (PCA): The PCA supplies blood to the occipital lobe, which is responsible for visual processing, as well as parts of the temporal and parietal lobes.
4. Anterior communicating artery (ACoA) and posterior communicating arteries (PComAs): These are small arteries that connect the major cerebral arteries, forming an important circulatory network called the Circle of Willis. The ACoA connects the two ACAs, while the PComAs connect the ICA with the PCA and the basilar artery.
These cerebral arteries play a crucial role in maintaining proper brain function by delivering oxygenated blood to various regions of the brain. Any damage or obstruction to these arteries can lead to serious neurological conditions, such as strokes or transient ischemic attacks (TIAs).
Theophylline is a medication that belongs to a class of drugs called methylxanthines. It is used in the management of respiratory diseases such as asthma, chronic obstructive pulmonary disease (COPD), and other conditions that cause narrowing of the airways in the lungs.
Theophylline works by relaxing the smooth muscle around the airways, which helps to open them up and make breathing easier. It also acts as a bronchodilator, increasing the flow of air into and out of the lungs. Additionally, theophylline has anti-inflammatory effects that can help reduce swelling in the airways and relieve symptoms such as coughing, wheezing, and shortness of breath.
Theophylline is available in various forms, including tablets, capsules, and liquid solutions. It is important to take this medication exactly as prescribed by a healthcare provider, as the dosage may vary depending on individual factors such as age, weight, and liver function. Regular monitoring of blood levels of theophylline is also necessary to ensure safe and effective use of the medication.
Radionuclide ventriculography (RVG), also known as multiple-gated acquisition scan (MUGA) or nuclear ventriculography, is a non-invasive diagnostic test used to evaluate the function and pumping efficiency of the heart's lower chambers (ventricles). The test involves the use of radioactive tracers (radionuclides) that are injected into the patient's bloodstream. A specialized camera then captures images of the distribution of the radionuclide within the heart, which allows for the measurement of ventricular volumes and ejection fraction (EF), an important indicator of cardiac function.
During the test, the patient lies on a table while the camera takes pictures of their heart as it beats. The images are captured in "gates" or intervals, corresponding to different phases of the cardiac cycle. This allows for the calculation of ventricular volumes and EF at each phase of the cycle, providing detailed information about the heart's pumping ability.
RVG is commonly used to assess patients with known or suspected heart disease, including those who have had a heart attack, heart failure, valvular heart disease, or cardiomyopathy. It can also be used to monitor the effectiveness of treatment and to evaluate changes in cardiac function over time.
Up-regulation is a term used in molecular biology and medicine to describe an increase in the expression or activity of a gene, protein, or receptor in response to a stimulus. This can occur through various mechanisms such as increased transcription, translation, or reduced degradation of the molecule. Up-regulation can have important functional consequences, for example, enhancing the sensitivity or response of a cell to a hormone, neurotransmitter, or drug. It is a normal physiological process that can also be induced by disease or pharmacological interventions.
A circadian rhythm is a roughly 24-hour biological cycle that regulates various physiological and behavioral processes in living organisms. It is driven by the body's internal clock, which is primarily located in the suprachiasmatic nucleus (SCN) of the hypothalamus in the brain.
The circadian rhythm controls many aspects of human physiology, including sleep-wake cycles, hormone secretion, body temperature, and metabolism. It helps to synchronize these processes with the external environment, particularly the day-night cycle caused by the rotation of the Earth.
Disruptions to the circadian rhythm can have negative effects on health, leading to conditions such as insomnia, sleep disorders, depression, bipolar disorder, and even increased risk of chronic diseases like cancer, diabetes, and cardiovascular disease. Factors that can disrupt the circadian rhythm include shift work, jet lag, irregular sleep schedules, and exposure to artificial light at night.
Reference values, also known as reference ranges or reference intervals, are the set of values that are considered normal or typical for a particular population or group of people. These values are often used in laboratory tests to help interpret test results and determine whether a patient's value falls within the expected range.
The process of establishing reference values typically involves measuring a particular biomarker or parameter in a large, healthy population and then calculating the mean and standard deviation of the measurements. Based on these statistics, a range is established that includes a certain percentage of the population (often 95%) and excludes extreme outliers.
It's important to note that reference values can vary depending on factors such as age, sex, race, and other demographic characteristics. Therefore, it's essential to use reference values that are specific to the relevant population when interpreting laboratory test results. Additionally, reference values may change over time due to advances in measurement technology or changes in the population being studied.
Diabetes complications refer to a range of health issues that can develop as a result of poorly managed diabetes over time. These complications can affect various parts of the body and can be classified into two main categories: macrovascular and microvascular.
Macrovascular complications include:
* Cardiovascular disease (CVD): People with diabetes are at an increased risk of developing CVD, including coronary artery disease, peripheral artery disease, and stroke.
* Peripheral arterial disease (PAD): This condition affects the blood vessels that supply oxygen and nutrients to the limbs, particularly the legs. PAD can cause pain, numbness, or weakness in the legs and may increase the risk of amputation.
Microvascular complications include:
* Diabetic neuropathy: This is a type of nerve damage that can occur due to prolonged high blood sugar levels. It commonly affects the feet and legs, causing symptoms such as numbness, tingling, or pain.
* Diabetic retinopathy: This condition affects the blood vessels in the eye and can cause vision loss or blindness if left untreated.
* Diabetic nephropathy: This is a type of kidney damage that can occur due to diabetes. It can lead to kidney failure if not managed properly.
Other complications of diabetes include:
* Increased risk of infections, particularly skin and urinary tract infections.
* Slow healing of wounds, which can increase the risk of infection and amputation.
* Gum disease and other oral health problems.
* Hearing impairment.
* Sexual dysfunction.
Preventing or managing diabetes complications involves maintaining good blood sugar control, regular monitoring of blood glucose levels, following a healthy lifestyle, and receiving routine medical care.
Aspirin is the common name for acetylsalicylic acid, which is a medication used to relieve pain, reduce inflammation, and lower fever. It works by inhibiting the activity of an enzyme called cyclooxygenase (COX), which is involved in the production of prostaglandins, hormone-like substances that cause inflammation and pain. Aspirin also has an antiplatelet effect, which means it can help prevent blood clots from forming. This makes it useful for preventing heart attacks and strokes.
Aspirin is available over-the-counter in various forms, including tablets, capsules, and chewable tablets. It is also available in prescription strengths for certain medical conditions. As with any medication, aspirin should be taken as directed by a healthcare provider, and its use should be avoided in children and teenagers with viral infections due to the risk of Reye's syndrome, a rare but serious condition that can affect the liver and brain.
Protein Kinase C-epsilon (PKCε) is a serine-threonine protein kinase that belongs to the family of Protein Kinase C (PKC) enzymes. These enzymes play crucial roles in various cellular processes, including signal transduction, cell survival, differentiation, and apoptosis.
PKCε is specifically involved in regulating several signaling pathways related to inflammation, proliferation, and carcinogenesis. It can be activated by different stimuli such as diacylglycerol (DAG) and phorbol esters, which lead to its translocation from the cytosol to the plasma membrane, where it phosphorylates and modulates the activity of various target proteins.
Abnormal regulation or expression of PKCε has been implicated in several diseases, including cancer, cardiovascular diseases, and neurodegenerative disorders. Therefore, PKCε is considered a potential therapeutic target for these conditions, and inhibitors of this enzyme are being developed and tested in preclinical and clinical studies.
Limb salvage is a medical term used to describe the surgical procedures and treatments aimed at preserving and restoring the functionality of a severely injured or diseased limb, rather than amputating it. The goal of limb salvage is to improve the patient's quality of life by maintaining their mobility, independence, and overall well-being.
Limb salvage may involve various surgical techniques such as vascular reconstruction, bone realignment, muscle flap coverage, and external fixation. These procedures aim to restore blood flow, stabilize bones, cover exposed tissues, and prevent infection. Additionally, adjuvant therapies like hyperbaric oxygen treatment, physical therapy, and pain management may be employed to support the healing process and improve functional outcomes.
Limb salvage is typically considered when a limb is threatened by conditions such as severe trauma, tumors, infections, or peripheral arterial disease. The decision to pursue limb salvage over amputation depends on factors like the patient's overall health, age, and personal preferences, as well as the extent of the injury or disease, potential for recovery, and likelihood of successful rehabilitation.
Free radical scavengers, also known as antioxidants, are substances that neutralize or stabilize free radicals. Free radicals are highly reactive atoms or molecules with unpaired electrons, capable of causing damage to cells and tissues in the body through a process called oxidative stress. Antioxidants donate an electron to the free radical, thereby neutralizing it and preventing it from causing further damage. They can be found naturally in foods such as fruits, vegetables, and nuts, or they can be synthesized and used as dietary supplements. Examples of antioxidants include vitamins C and E, beta-carotene, and selenium.
Vascular patency is a term used in medicine to describe the state of a blood vessel (such as an artery or vein) being open, unobstructed, and allowing for the normal flow of blood. It is an important concept in the treatment and management of various cardiovascular conditions, such as peripheral artery disease, coronary artery disease, and deep vein thrombosis.
Maintaining vascular patency can help prevent serious complications like tissue damage, organ dysfunction, or even death. This may involve medical interventions such as administering blood-thinning medications to prevent clots, performing procedures to remove blockages, or using devices like stents to keep vessels open. Regular monitoring of vascular patency is also crucial for evaluating the effectiveness of treatments and adjusting care plans accordingly.
Endothelin-1 is a small peptide (21 amino acids) and a potent vasoconstrictor, which means it narrows blood vessels. It is primarily produced by the endothelial cells that line the interior surface of blood vessels. Endothelin-1 plays a crucial role in regulating vascular tone, cell growth, and inflammation. Its dysregulation has been implicated in various cardiovascular diseases, such as hypertension and heart failure. It exerts its effects by binding to specific G protein-coupled receptors (ETA and ETB) on the surface of target cells.
Heart failure is a pathophysiological state in which the heart is unable to pump sufficient blood to meet the metabolic demands of the body or do so only at the expense of elevated filling pressures. It can be caused by various cardiac disorders, including coronary artery disease, hypertension, valvular heart disease, cardiomyopathy, and arrhythmias. Symptoms may include shortness of breath, fatigue, and fluid retention. Heart failure is often classified based on the ejection fraction (EF), which is the percentage of blood that is pumped out of the left ventricle during each contraction. A reduced EF (less than 40%) is indicative of heart failure with reduced ejection fraction (HFrEF), while a preserved EF (greater than or equal to 50%) is indicative of heart failure with preserved ejection fraction (HFpEF). There is also a category of heart failure with mid-range ejection fraction (HFmrEF) for those with an EF between 40-49%.
Molsidomine is a medication that belongs to a class of drugs called vasodilators. It works by relaxing and widening blood vessels, which helps to improve blood flow and reduce the workload on the heart. Molsidomine is used to treat chronic stable angina (chest pain caused by reduced blood flow to the heart) and has been found to be effective in reducing the frequency and severity of anginal attacks.
When molsidomine is absorbed into the body, it is converted into its active metabolite, SIN-1, which is responsible for its vasodilatory effects. SIN-1 causes smooth muscle relaxation by increasing the levels of nitric oxide in the blood vessels, leading to their dilation and improved blood flow.
Molsidomine is available in tablet form and is typically taken two to three times a day, with or without food. Common side effects of molsidomine include headache, dizziness, flushing, and palpitations. It should be used with caution in patients with low blood pressure, heart failure, or impaired kidney function.
I'm sorry for any confusion, but "pilot projects" is not a medical term per se. Instead, it is a general term used in various fields, including healthcare and medicine, to describe a small-scale initiative that is implemented on a temporary basis to evaluate its feasibility, effectiveness, or impact before deciding whether to expand or continue it.
In the context of healthcare, pilot projects might involve testing new treatment protocols, implementing innovative care models, or introducing technology solutions in a limited setting to assess their potential benefits and drawbacks. The results of these projects can help inform decisions about broader implementation and provide valuable insights for improving the quality and efficiency of healthcare services.
General anesthesia is a state of controlled unconsciousness, induced by administering various medications, that eliminates awareness, movement, and pain sensation during medical procedures. It involves the use of a combination of intravenous and inhaled drugs to produce a reversible loss of consciousness, allowing patients to undergo surgical or diagnostic interventions safely and comfortably. The depth and duration of anesthesia are carefully monitored and adjusted throughout the procedure by an anesthesiologist or certified registered nurse anesthetist (CRNA) to ensure patient safety and optimize recovery. General anesthesia is typically used for more extensive surgical procedures, such as open-heart surgery, major orthopedic surgeries, and neurosurgery.
Methyl ethers are a type of organic compound where a methyl group (CH3-) is attached to an oxygen atom, which in turn is connected to another carbon atom. They are formed by the process of methylation, where a methyl group replaces a hydrogen atom in another molecule.
Methyl ethers can be found in various natural and synthetic substances. For example, dimethyl ether (CH3-O-CH3) is a common fuel used in refrigeration systems and as a propellant in aerosol sprays. Anisole (CH3-O-C6H5), another methyl ether, is found in anise oil and is used as a flavoring agent and solvent.
It's worth noting that some methyl ethers have been associated with potential health risks, particularly when they are volatile and can be inhaled or ingested. For example, exposure to high levels of dimethyl ether can cause respiratory irritation, headaches, and dizziness. Therefore, it's important to handle these substances with care and follow appropriate safety guidelines.
The superior mesenteric artery (SMA) is a major artery that supplies oxygenated blood to the intestines, specifically the lower part of the duodenum, jejunum, ileum, cecum, ascending colon, and the first and second parts of the transverse colon. It originates from the abdominal aorta, located just inferior to the pancreas, and passes behind the neck of the pancreas before dividing into several branches to supply the intestines. The SMA is an essential vessel in the digestive system, providing blood flow for nutrient absorption and overall gut function.
Angioplasty, balloon refers to a medical procedure used to widen narrowed or obstructed blood vessels, particularly the coronary arteries that supply blood to the heart muscle. This procedure is typically performed using a catheter-based technique, where a thin, flexible tube called a catheter is inserted into an artery, usually through the groin or wrist, and guided to the site of the narrowing or obstruction in the coronary artery.
Once the catheter reaches the affected area, a small balloon attached to the tip of the catheter is inflated, which compresses the plaque against the artery wall and stretches the artery, thereby restoring blood flow. The balloon is then deflated and removed, along with the catheter.
Balloon angioplasty is often combined with the placement of a stent, a small metal mesh tube that helps to keep the artery open and prevent it from narrowing again. This procedure is known as percutaneous coronary intervention (PCI) or coronary angioplasty and stenting.
Overall, balloon angioplasty is a relatively safe and effective treatment for coronary artery disease, although complications such as bleeding, infection, or re-narrowing of the artery can occur in some cases.
Endothelial cells are the type of cells that line the inner surface of blood vessels, lymphatic vessels, and heart chambers. They play a crucial role in maintaining vascular homeostasis by controlling vasomotor tone, coagulation, platelet activation, and inflammation. Endothelial cells also regulate the transport of molecules between the blood and surrounding tissues, and contribute to the maintenance of the structural integrity of the vasculature. They are flat, elongated cells with a unique morphology that allows them to form a continuous, nonthrombogenic lining inside the vessels. Endothelial cells can be isolated from various tissues and cultured in vitro for research purposes.
Propanolamines are a class of pharmaceutical compounds that contain a propan-2-olamine functional group, which is a secondary amine formed by the replacement of one hydrogen atom in an ammonia molecule with a propan-2-ol group. They are commonly used as decongestants and bronchodilators in medical treatments.
Examples of propanolamines include:
* Phenylephrine: a decongestant used to relieve nasal congestion.
* Pseudoephedrine: a decongestant and stimulant used to treat nasal congestion and sinus pressure.
* Ephedrine: a bronchodilator, decongestant, and stimulant used to treat asthma, nasal congestion, and low blood pressure.
It is important to note that propanolamines can have side effects such as increased heart rate, elevated blood pressure, and insomnia, so they should be used with caution and under the supervision of a healthcare professional.
A Receiver Operating Characteristic (ROC) curve is a graphical representation used in medical decision-making and statistical analysis to illustrate the performance of a binary classifier system, such as a diagnostic test or a machine learning algorithm. It's a plot that shows the tradeoff between the true positive rate (sensitivity) and the false positive rate (1 - specificity) for different threshold settings.
The x-axis of an ROC curve represents the false positive rate (the proportion of negative cases incorrectly classified as positive), while the y-axis represents the true positive rate (the proportion of positive cases correctly classified as positive). Each point on the curve corresponds to a specific decision threshold, with higher points indicating better performance.
The area under the ROC curve (AUC) is a commonly used summary measure that reflects the overall performance of the classifier. An AUC value of 1 indicates perfect discrimination between positive and negative cases, while an AUC value of 0.5 suggests that the classifier performs no better than chance.
ROC curves are widely used in healthcare to evaluate diagnostic tests, predictive models, and screening tools for various medical conditions, helping clinicians make informed decisions about patient care based on the balance between sensitivity and specificity.
Catecholamines are a group of hormones and neurotransmitters that are derived from the amino acid tyrosine. The most well-known catecholamines are dopamine, norepinephrine (also known as noradrenaline), and epinephrine (also known as adrenaline). These hormones are produced by the adrenal glands and are released into the bloodstream in response to stress. They play important roles in the "fight or flight" response, increasing heart rate, blood pressure, and alertness. In addition to their role as hormones, catecholamines also function as neurotransmitters, transmitting signals in the nervous system. Disorders of catecholamine regulation can lead to a variety of medical conditions, including hypertension, mood disorders, and neurological disorders.
Pituitary hormones refer to the chemical messengers produced and released by the pituitary gland, which is a small endocrine gland located at the base of the brain. The pituitary gland is divided into two main parts: the anterior lobe (also known as the adenohypophysis) and the posterior lobe (also known as the neurohypophysis).
Posterior pituitary hormones are those that are produced by the hypothalamus, a region of the brain located above the pituitary gland, and stored in the posterior pituitary before being released. There are two main posterior pituitary hormones:
1. Oxytocin: This hormone plays a role in social bonding, sexual reproduction, and childbirth. During childbirth, oxytocin stimulates uterine contractions to help facilitate delivery of the baby. After delivery, oxytocin continues to be released to stimulate milk production and letdown during breastfeeding.
2. Vasopressin (also known as antidiuretic hormone or ADH): This hormone helps regulate water balance in the body by controlling the amount of urine that is produced by the kidneys. When vasopressin is released, it causes the kidneys to retain water and increase blood volume, which can help to maintain blood pressure.
Together, these posterior pituitary hormones play important roles in regulating various physiological processes in the body.
'Rats, Nude' is not a standard medical term or condition. The term 'nude' in the context of laboratory animals like rats usually refers to a strain of rats that are hairless due to a genetic mutation. This can make them useful for studies involving skin disorders, wound healing, and other conditions where fur might interfere with observations or procedures. However, 'Rats, Nude' is not a recognized or established term in medical literature or taxonomy.
Pathological constriction refers to an abnormal narrowing or tightening of a body passage or organ, which can interfere with the normal flow of blood, air, or other substances through the area. This constriction can occur due to various reasons such as inflammation, scarring, or abnormal growths, and can affect different parts of the body, including blood vessels, airways, intestines, and ureters. Pathological constriction can lead to a range of symptoms and complications depending on its location and severity, and may require medical intervention to correct.
Hypothermia is a medically defined condition where the core body temperature drops below 35°C (95°F). It is often associated with exposure to cold environments, but can also occur in cases of severe illness, injury, or immersion in cold water. Symptoms may include shivering, confusion, slowed heart rate and breathing, and if not treated promptly, can lead to unconsciousness, cardiac arrest, and even death.
Superoxides are partially reduced derivatives of oxygen that contain one extra electron, giving them an overall charge of -1. They are highly reactive and unstable, with the most common superoxide being the hydroxyl radical (•OH-) and the superoxide anion (O2-). Superoxides are produced naturally in the body during metabolic processes, particularly within the mitochondria during cellular respiration. They play a role in various physiological processes, but when produced in excess or not properly neutralized, they can contribute to oxidative stress and damage to cells and tissues, potentially leading to the development of various diseases such as cancer, atherosclerosis, and neurodegenerative disorders.
Organophosphorus compounds are a class of chemical substances that contain phosphorus bonded to organic compounds. They are used in various applications, including as plasticizers, flame retardants, pesticides (insecticides, herbicides, and nerve gases), and solvents. In medicine, they are also used in the treatment of certain conditions such as glaucoma. However, organophosphorus compounds can be toxic to humans and animals, particularly those that affect the nervous system by inhibiting acetylcholinesterase, an enzyme that breaks down the neurotransmitter acetylcholine. Exposure to these compounds can cause symptoms such as nausea, vomiting, muscle weakness, and in severe cases, respiratory failure and death.
Sulfones are a group of medications that contain a sulfur atom bonded to two oxygen atoms and one other group, typically a hydrogen or carbon atom. They have various medical uses, including as antibacterial, antifungal, and anti-inflammatory agents. One example of a sulfone is dapsone, which is used to treat bacterial infections such as leprosy and Pneumocystis jirovecii pneumonia (PJP), as well as some inflammatory skin conditions. It's important to note that sulfones can have significant side effects and should only be used under the supervision of a healthcare professional.
The Autonomic Nervous System (ANS) is a part of the peripheral nervous system that operates largely below the level of consciousness and controls visceral functions. It is divided into two main subdivisions: the sympathetic and parasympathetic nervous systems, which generally have opposing effects and maintain homeostasis in the body.
The Sympathetic Nervous System (SNS) prepares the body for stressful or emergency situations, often referred to as the "fight or flight" response. It increases heart rate, blood pressure, respiratory rate, and metabolic rate, while also decreasing digestive activity. This response helps the body respond quickly to perceived threats.
The Parasympathetic Nervous System (PNS), on the other hand, promotes the "rest and digest" state, allowing the body to conserve energy and restore itself after the stress response has subsided. It decreases heart rate, blood pressure, and respiratory rate, while increasing digestive activity and promoting relaxation.
These two systems work together to maintain balance in the body by adjusting various functions based on internal and external demands. Disorders of the Autonomic Nervous System can lead to a variety of symptoms, such as orthostatic hypotension, gastroparesis, and cardiac arrhythmias, among others.
Intra-arterial infusion is a medical procedure in which a liquid medication or fluid is delivered directly into an artery. This technique is used to deliver drugs directly to a specific organ or region of the body, bypassing the usual systemic circulation and allowing for higher concentrations of the drug to reach the target area. It is often used in cancer treatment to deliver chemotherapeutic agents directly to tumors, as well as in other conditions such as severe infections or inflammation.
Intra-arterial infusions are typically administered through a catheter that is inserted into an artery, usually under the guidance of imaging techniques such as fluoroscopy, CT, or MRI. The procedure requires careful monitoring and precise control to ensure proper placement of the catheter and accurate delivery of the medication.
It's important to note that intra-arterial infusions are different from intra venous (IV) infusions, where medications are delivered into a vein instead of an artery. The choice between intra-arterial and intra-venous infusion depends on various factors such as the type of medication being used, the location of the target area, and the patient's overall medical condition.
Preclinical drug evaluation refers to a series of laboratory tests and studies conducted to determine the safety and effectiveness of a new drug before it is tested in humans. These studies typically involve experiments on cells and animals to evaluate the pharmacological properties, toxicity, and potential interactions with other substances. The goal of preclinical evaluation is to establish a reasonable level of safety and understanding of how the drug works, which helps inform the design and conduct of subsequent clinical trials in humans. It's important to note that while preclinical studies provide valuable information, they may not always predict how a drug will behave in human subjects.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Microdialysis is a minimally invasive technique used in clinical and research settings to continuously monitor the concentration of various chemicals, such as neurotransmitters, drugs, or metabolites, in biological fluids (e.g., extracellular fluid of tissues, blood, or cerebrospinal fluid). This method involves inserting a small, flexible catheter with a semipermeable membrane into the region of interest. A physiological solution is continuously perfused through the catheter, allowing molecules to diffuse across the membrane based on their concentration gradient. The dialysate that exits the catheter is then collected and analyzed for target compounds using various analytical techniques (e.g., high-performance liquid chromatography, mass spectrometry).
In summary, microdialysis is a valuable tool for monitoring real-time changes in chemical concentrations within biological systems, enabling better understanding of physiological processes or pharmacokinetic properties of drugs.
Cardiac arrest, also known as heart arrest, is a medical condition where the heart suddenly stops beating or functioning properly. This results in the cessation of blood flow to the rest of the body, including the brain, leading to loss of consciousness and pulse. Cardiac arrest is often caused by electrical disturbances in the heart that disrupt its normal rhythm, known as arrhythmias. If not treated immediately with cardiopulmonary resuscitation (CPR) and defibrillation, it can lead to death or permanent brain damage due to lack of oxygen supply. It's important to note that a heart attack is different from cardiac arrest; a heart attack occurs when blood flow to a part of the heart is blocked, often by a clot, causing damage to the heart muscle, but the heart continues to beat. However, a heart attack can sometimes trigger a cardiac arrest.
Vascular Endothelial Growth Factors (VEGFs) are a family of signaling proteins that stimulate the growth and development of new blood vessels, a process known as angiogenesis. They play crucial roles in both physiological and pathological conditions, such as embryonic development, wound healing, and tumor growth. Specifically, VEGFs bind to specific receptors on the surface of endothelial cells, which line the interior surface of blood vessels, triggering a cascade of intracellular signaling events that promote cell proliferation, migration, and survival. Dysregulation of VEGF signaling has been implicated in various diseases, including cancer, age-related macular degeneration, and diabetic retinopathy.
I'm happy to help! "Rats, Inbred Lew" is a specific strain of laboratory rats that have been inbred for research purposes. The "Lew" part of the name refers to the location where they were first developed, the Lewis Institute in Lake Bluff, Illinois, USA.
Inbreeding is a process of mating closely related individuals over many generations to create a genetically homogeneous population. This results in a high degree of genetic similarity among members of the strain, making them ideal for use as experimental models because any differences observed between individuals are more likely to be due to the experimental manipulation rather than genetic variation.
Inbred Lew rats have been widely used in biomedical research, particularly in studies related to hypertension and cardiovascular disease. They exhibit a number of unique characteristics that make them useful for these types of studies, including their susceptibility to developing high blood pressure when fed a high-salt diet or given certain drugs.
It's important to note that while inbred strains like Lew rats can be very useful tools for researchers, they are not perfect models for human disease. Because they have been bred in a controlled environment and selected for specific traits, they may not respond to experimental manipulations in the same way that humans or other animals would. Therefore, it's important to interpret findings from these studies with caution and consider multiple lines of evidence before drawing any firm conclusions.
Blood gas analysis is a medical test that measures the levels of oxygen and carbon dioxide in the blood, as well as the pH level, which indicates the acidity or alkalinity of the blood. This test is often used to evaluate lung function, respiratory disorders, and acid-base balance in the body. It can also be used to monitor the effectiveness of treatments for conditions such as chronic obstructive pulmonary disease (COPD), asthma, and other respiratory illnesses. The analysis is typically performed on a sample of arterial blood, although venous blood may also be used in some cases.
Magnetic Resonance Angiography (MRA) is a non-invasive medical imaging technique that uses magnetic fields and radio waves to create detailed images of the blood vessels or arteries within the body. It is a type of Magnetic Resonance Imaging (MRI) that focuses specifically on the circulatory system.
MRA can be used to diagnose and evaluate various conditions related to the blood vessels, such as aneurysms, stenosis (narrowing of the vessel), or the presence of plaques or tumors. It can also be used to plan for surgeries or other treatments related to the vascular system. The procedure does not use radiation and is generally considered safe, although people with certain implants like pacemakers may not be able to have an MRA due to safety concerns.
Stable angina is a type of chest pain or discomfort that typically occurs during physical exertion or emotional stress. It is caused by reduced blood flow to the heart muscle, which can occur when the coronary arteries become narrowed or blocked due to the buildup of cholesterol and other substances (a condition known as atherosclerosis).
The symptoms of stable angina are usually predictable and may include chest pain or discomfort that is:
* Described as a squeezing, pressure, heaviness, or tightness in the chest
* Typically located in the center of the chest, but may radiate to the shoulders, arms, neck, jaw, or back
* Lasts for a few minutes and is usually relieved by rest or nitroglycerin
Stable angina is considered "stable" because the symptoms tend to occur predictably and can be managed with medication, lifestyle changes, and sometimes medical procedures such as angioplasty or bypass surgery. However, it is still a serious condition that requires proper diagnosis and treatment to prevent complications such as heart attack or stroke.
A cross-over study is a type of experimental design in which participants receive two or more interventions in a specific order. After a washout period, each participant receives the opposite intervention(s). The primary advantage of this design is that it controls for individual variability by allowing each participant to act as their own control.
In medical research, cross-over studies are often used to compare the efficacy or safety of two treatments. For example, a researcher might conduct a cross-over study to compare the effectiveness of two different medications for treating high blood pressure. Half of the participants would be randomly assigned to receive one medication first and then switch to the other medication after a washout period. The other half of the participants would receive the opposite order of treatments.
Cross-over studies can provide valuable insights into the relative merits of different interventions, but they also have some limitations. For example, they may not be suitable for studying conditions that are chronic or irreversible, as it may not be possible to completely reverse the effects of the first intervention before administering the second one. Additionally, carryover effects from the first intervention can confound the results if they persist into the second treatment period.
Overall, cross-over studies are a useful tool in medical research when used appropriately and with careful consideration of their limitations.
Body Surface Potential Mapping (BSPM) is a non-invasive medical technique used to record and analyze the electrical activity of the heart from the surface of the body. It involves placing multiple electrodes on the skin of the chest, back, and limbs to measure the potential differences between these points during each heartbeat. This information is then used to create a detailed, visual representation of the electrical activation pattern of the heart, which can help in the diagnosis and evaluation of various cardiac disorders such as arrhythmias, myocardial infarction, and ventricular hypertrophy.
The BSPM technique provides high-resolution spatial and temporal information about the cardiac electrical activity, making it a valuable tool for both clinical and research purposes. It can help identify the origin and spread of abnormal electrical signals in the heart, which is crucial for determining appropriate treatment strategies. Overall, Body Surface Potential Mapping is an important diagnostic modality that offers unique insights into the electrical functioning of the heart.
A tourniquet is a device or material used to apply pressure around an extremity, typically an arm or leg, with the goal of controlling severe bleeding (hemorrhage) by compressing blood vessels and limiting arterial flow. Tourniquets are usually applied as a last resort when direct pressure and elevation have failed to stop life-threatening bleeding. They should be used cautiously because they can cause tissue damage, nerve injury, or even amputation if left on for too long. In a medical setting, tourniquets are often applied by healthcare professionals in emergency situations; however, there are also specialized tourniquets available for use by trained individuals in the military, first responder communities, and civilians who have undergone proper training.
In the context of medicine, and specifically in physiology and respiratory therapy, partial pressure (P or p) is a measure of the pressure exerted by an individual gas in a mixture of gases. It's commonly used to describe the concentrations of gases in the body, such as oxygen (PO2), carbon dioxide (PCO2), and nitrogen (PN2).
The partial pressure of a specific gas is calculated as the fraction of that gas in the total mixture multiplied by the total pressure of the mixture. This concept is based on Dalton's law, which states that the total pressure exerted by a mixture of gases is equal to the sum of the pressures exerted by each individual gas.
For example, in room air at sea level, the partial pressure of oxygen (PO2) is approximately 160 mmHg (mm of mercury), which represents about 21% of the total barometric pressure (760 mmHg). This concept is crucial for understanding gas exchange in the lungs and how gases move across membranes, such as from alveoli to blood and vice versa.
Ventricular dysfunction is a term that refers to the impaired ability of the ventricles, which are the lower chambers of the heart, to fill with blood or pump it efficiently to the rest of the body. This condition can lead to reduced cardiac output and may cause symptoms such as shortness of breath, fatigue, and fluid retention.
There are two types of ventricular dysfunction:
1. Systolic dysfunction: This occurs when the ventricles cannot contract forcefully enough to eject an adequate amount of blood out of the heart during each beat. This is often due to damage to the heart muscle, such as that caused by a heart attack or cardiomyopathy.
2. Diastolic dysfunction: This happens when the ventricles are unable to relax and fill properly with blood between beats. This can be caused by stiffening of the heart muscle, often due to aging, high blood pressure, or diabetes.
Both types of ventricular dysfunction can lead to heart failure, a serious condition in which the heart is unable to pump blood effectively to meet the body's needs. Treatment for ventricular dysfunction may include medications, lifestyle changes, and in some cases, medical procedures or surgery.
An injection is a medical procedure in which a medication, vaccine, or other substance is introduced into the body using a needle and syringe. The substance can be delivered into various parts of the body, including into a vein (intravenous), muscle (intramuscular), under the skin (subcutaneous), or into the spinal canal (intrathecal or spinal).
Injections are commonly used to administer medications that cannot be taken orally, have poor oral bioavailability, need to reach the site of action quickly, or require direct delivery to a specific organ or tissue. They can also be used for diagnostic purposes, such as drawing blood samples (venipuncture) or injecting contrast agents for imaging studies.
Proper technique and sterile conditions are essential when administering injections to prevent infection, pain, and other complications. The choice of injection site depends on the type and volume of the substance being administered, as well as the patient's age, health status, and personal preferences.
"Pyrroles" is not a medical term in and of itself, but "pyrrole" is an organic compound that contains one nitrogen atom and four carbon atoms in a ring structure. In the context of human health, "pyrroles" often refers to a group of compounds called pyrrol derivatives or pyrrole metabolites.
In clinical settings, "pyrroles" is sometimes used to refer to a urinary metabolite called "pyrrole-protein conjugate," which contains a pyrrole ring and is excreted in the urine. Elevated levels of this compound have been associated with certain psychiatric and behavioral disorders, such as schizophrenia and mood disorders. However, the relationship between pyrroles and these conditions is not well understood, and more research is needed to establish a clear medical definition or diagnostic criteria for "pyrrole disorder" or "pyroluria."
Arginine is an α-amino acid that is classified as a semi-essential or conditionally essential amino acid, depending on the developmental stage and health status of the individual. The adult human body can normally synthesize sufficient amounts of arginine to meet its needs, but there are certain circumstances, such as periods of rapid growth or injury, where the dietary intake of arginine may become necessary.
The chemical formula for arginine is C6H14N4O2. It has a molecular weight of 174.20 g/mol and a pKa value of 12.48. Arginine is a basic amino acid, which means that it contains a side chain with a positive charge at physiological pH levels. The side chain of arginine is composed of a guanidino group, which is a functional group consisting of a nitrogen atom bonded to three methyl groups.
In the body, arginine plays several important roles. It is a precursor for the synthesis of nitric oxide, a molecule that helps regulate blood flow and immune function. Arginine is also involved in the detoxification of ammonia, a waste product produced by the breakdown of proteins. Additionally, arginine can be converted into other amino acids, such as ornithine and citrulline, which are involved in various metabolic processes.
Foods that are good sources of arginine include meat, poultry, fish, dairy products, nuts, seeds, and legumes. Arginine supplements are available and may be used for a variety of purposes, such as improving exercise performance, enhancing wound healing, and boosting immune function. However, it is important to consult with a healthcare provider before taking arginine supplements, as they can interact with certain medications and have potential side effects.
Radionuclide angiography (RNA) is a type of nuclear medicine imaging procedure used to evaluate the heart's function, specifically the pumping ability of the lower chambers of the heart (the ventricles). It involves the use of radioactive material (radionuclide or radiopharmaceutical) that is injected into the patient's bloodstream. A special camera then captures images of the distribution and accumulation of this radioactive material within the heart, providing information about blood flow, ventricular function, and any potential abnormalities in the heart muscle.
During a RNA procedure, the radiopharmaceutical is usually injected into a vein in the patient's arm. As the tracer circulates through the bloodstream, it accumulates in the heart tissue. The gamma camera captures images of the distribution and accumulation of the radionuclide within the heart at different time points. These images are then used to assess various aspects of heart function, such as ejection fraction (the percentage of blood that is pumped out of the ventricles with each beat), wall motion abnormalities, and any potential areas of reduced blood flow or damage in the heart muscle.
Radionuclide angiography can be used to diagnose and monitor various cardiac conditions, including coronary artery disease, heart failure, cardiomyopathy, and valvular heart disease. It is a non-invasive procedure that does not require catheterization or the use of contrast agents, making it a safer alternative for patients with kidney problems or allergies to contrast materials. However, as with any medical procedure involving radiation exposure, the benefits of RNA must be weighed against the potential risks.
Methylergonovine is a medication that belongs to a class of drugs called ergot alkaloids. It is primarily used to prevent and treat uterine bleeding after childbirth. Medically, it is defined as a semi-synthetic ergopeptide analog with oxytocic properties, which stimulates myometrial contractions and reduces postpartum hemorrhage.
Methylergonovine works by stimulating the smooth muscle of the uterus, causing it to contract. This helps to return the uterus to its pre-pregnancy size and also helps to control bleeding after childbirth. It is important to note that methylergonovine should only be used under the supervision of a healthcare provider, as it can have serious side effects if not used properly.
Heme Oxygenase-1 (HO-1) is an inducible enzyme that catalyzes the degradation of heme into biliverdin, iron, and carbon monoxide. It is a rate-limiting enzyme in the oxidative degradation of heme. HO-1 is known to play a crucial role in cellular defense against oxidative stress and inflammation. It is primarily located in the microsomes of many tissues, including the spleen, liver, and brain. Induction of HO-1 has been shown to have cytoprotective effects, while deficiency in HO-1 has been associated with several pathological conditions, such as vascular diseases, neurodegenerative disorders, and cancer.
'Gene expression regulation' refers to the processes that control whether, when, and where a particular gene is expressed, meaning the production of a specific protein or functional RNA encoded by that gene. This complex mechanism can be influenced by various factors such as transcription factors, chromatin remodeling, DNA methylation, non-coding RNAs, and post-transcriptional modifications, among others. Proper regulation of gene expression is crucial for normal cellular function, development, and maintaining homeostasis in living organisms. Dysregulation of gene expression can lead to various diseases, including cancer and genetic disorders.
Lipid peroxidation is a process in which free radicals, such as reactive oxygen species (ROS), steal electrons from lipids containing carbon-carbon double bonds, particularly polyunsaturated fatty acids (PUFAs). This results in the formation of lipid hydroperoxides, which can decompose to form a variety of compounds including reactive carbonyl compounds, aldehydes, and ketones.
Malondialdehyde (MDA) is one such compound that is commonly used as a marker for lipid peroxidation. Lipid peroxidation can cause damage to cell membranes, leading to changes in their fluidity and permeability, and can also result in the modification of proteins and DNA, contributing to cellular dysfunction and ultimately cell death. It is associated with various pathological conditions such as atherosclerosis, neurodegenerative diseases, and cancer.
Radionuclide imaging, also known as nuclear medicine, is a medical imaging technique that uses small amounts of radioactive material, called radionuclides or radiopharmaceuticals, to diagnose and treat various diseases and conditions. The radionuclides are introduced into the body through injection, inhalation, or ingestion and accumulate in specific organs or tissues. A special camera then detects the gamma rays emitted by these radionuclides and converts them into images that provide information about the structure and function of the organ or tissue being studied.
Radionuclide imaging can be used to evaluate a wide range of medical conditions, including heart disease, cancer, neurological disorders, gastrointestinal disorders, and bone diseases. The technique is non-invasive and generally safe, with minimal exposure to radiation. However, it should only be performed by qualified healthcare professionals in accordance with established guidelines and regulations.
Histamine agonists are substances that bind to and activate histamine receptors, leading to the initiation or enhancement of various physiological responses. Histamine is a naturally occurring molecule that plays a key role in the body's immune and allergic responses, as well as in the regulation of sleep, wakefulness, and appetite.
There are four main types of histamine receptors (H1, H2, H3, and H4), each with distinct functions and signaling pathways. Histamine agonists can be selective for one or more of these receptor subtypes, depending on their pharmacological properties.
For example, H1 agonists are commonly used as decongestants and antihistamines to treat allergies, while H2 agonists are used to treat gastroesophageal reflux disease (GERD) and peptic ulcers. H3 agonists have been investigated for their potential therapeutic use in the treatment of neurological disorders such as Parkinson's disease and schizophrenia, while H4 agonists are being studied for their role in inflammation and immune regulation.
It is important to note that histamine agonists can also have adverse effects, particularly if they are not selective for a specific receptor subtype or if they are used at high doses. These effects may include increased heart rate, blood pressure, and bronchodilation (opening of the airways), as well as gastrointestinal symptoms such as nausea, vomiting, and diarrhea.
Multivariate analysis is a statistical method used to examine the relationship between multiple independent variables and a dependent variable. It allows for the simultaneous examination of the effects of two or more independent variables on an outcome, while controlling for the effects of other variables in the model. This technique can be used to identify patterns, associations, and interactions among multiple variables, and is commonly used in medical research to understand complex health outcomes and disease processes. Examples of multivariate analysis methods include multiple regression, factor analysis, cluster analysis, and discriminant analysis.
Hypertension is a medical term used to describe abnormally high blood pressure in the arteries, often defined as consistently having systolic blood pressure (the top number in a blood pressure reading) over 130 mmHg and/or diastolic blood pressure (the bottom number) over 80 mmHg. It is also commonly referred to as high blood pressure.
Hypertension can be classified into two types: primary or essential hypertension, which has no identifiable cause and accounts for about 95% of cases, and secondary hypertension, which is caused by underlying medical conditions such as kidney disease, hormonal disorders, or use of certain medications.
If left untreated, hypertension can lead to serious health complications such as heart attack, stroke, heart failure, and chronic kidney disease. Therefore, it is important for individuals with hypertension to manage their condition through lifestyle modifications (such as healthy diet, regular exercise, stress management) and medication if necessary, under the guidance of a healthcare professional.
Endothelin is a type of peptide (small protein) that is produced by the endothelial cells, which line the interior surface of blood vessels. Endothelins are known to be potent vasoconstrictors, meaning they cause the narrowing of blood vessels, and thus increase blood pressure. There are three major types of endothelin molecules, known as Endothelin-1, Endothelin-2, and Endothelin-3. These endothelins bind to specific receptors (ETA, ETB) on the surface of smooth muscle cells in the blood vessel walls, leading to contraction and subsequent vasoconstriction. Additionally, endothelins have been implicated in various physiological and pathophysiological processes such as regulation of cell growth, inflammation, and fibrosis.
The Autonomic Nervous System (ANS) is a part of the nervous system that controls involuntary actions, such as heart rate, digestion, respiratory rate, pupillary response, urination, and sexual arousal. It consists of two subdivisions: the sympathetic and parasympathetic nervous systems, which generally have opposing effects and maintain homeostasis in the body.
Autonomic Nervous System Diseases (also known as Autonomic Disorders or Autonomic Neuropathies) refer to a group of conditions that affect the functioning of the autonomic nervous system. These diseases can cause damage to the nerves that control automatic functions, leading to various symptoms and complications.
Autonomic Nervous System Diseases can be classified into two main categories:
1. Primary Autonomic Nervous System Disorders: These are conditions that primarily affect the autonomic nervous system without any underlying cause. Examples include:
* Pure Autonomic Failure (PAF): A rare disorder characterized by progressive loss of autonomic nerve function, leading to symptoms such as orthostatic hypotension, urinary retention, and constipation.
* Multiple System Atrophy (MSA): A degenerative neurological disorder that affects both the autonomic nervous system and movement coordination. Symptoms may include orthostatic hypotension, urinary incontinence, sexual dysfunction, and Parkinsonian features like stiffness and slowness of movements.
* Autonomic Neuropathy associated with Parkinson's Disease: Some individuals with Parkinson's disease develop autonomic symptoms such as orthostatic hypotension, constipation, and urinary dysfunction due to the degeneration of autonomic nerves.
2. Secondary Autonomic Nervous System Disorders: These are conditions that affect the autonomic nervous system as a result of an underlying cause or disease. Examples include:
* Diabetic Autonomic Neuropathy: A complication of diabetes mellitus that affects the autonomic nerves, leading to symptoms such as orthostatic hypotension, gastroparesis (delayed gastric emptying), and sexual dysfunction.
* Autoimmune-mediated Autonomic Neuropathies: Conditions like Guillain-Barré syndrome or autoimmune autonomic ganglionopathy can cause autonomic symptoms due to the immune system attacking the autonomic nerves.
* Infectious Autonomic Neuropathies: Certain infections, such as HIV or Lyme disease, can lead to autonomic dysfunction as a result of nerve damage.
* Toxin-induced Autonomic Neuropathy: Exposure to certain toxins, like heavy metals or organophosphate pesticides, can cause autonomic neuropathy.
Autonomic nervous system disorders can significantly impact a person's quality of life and daily functioning. Proper diagnosis and management are crucial for improving symptoms and preventing complications. Treatment options may include lifestyle modifications, medications, and in some cases, devices or surgical interventions.
In epidemiology, the incidence of a disease is defined as the number of new cases of that disease within a specific population over a certain period of time. It is typically expressed as a rate, with the number of new cases in the numerator and the size of the population at risk in the denominator. Incidence provides information about the risk of developing a disease during a given time period and can be used to compare disease rates between different populations or to monitor trends in disease occurrence over time.
Diabetes Mellitus, Type 2 is a metabolic disorder characterized by high blood glucose (or sugar) levels resulting from the body's inability to produce sufficient amounts of insulin or effectively use the insulin it produces. This form of diabetes usually develops gradually over several years and is often associated with older age, obesity, physical inactivity, family history of diabetes, and certain ethnicities.
In Type 2 diabetes, the body's cells become resistant to insulin, meaning they don't respond properly to the hormone. As a result, the pancreas produces more insulin to help glucose enter the cells. Over time, the pancreas can't keep up with the increased demand, leading to high blood glucose levels and diabetes.
Type 2 diabetes is managed through lifestyle modifications such as weight loss, regular exercise, and a healthy diet. Medications, including insulin therapy, may also be necessary to control blood glucose levels and prevent long-term complications associated with the disease, such as heart disease, nerve damage, kidney damage, and vision loss.
Preoperative care refers to the series of procedures, interventions, and preparations that are conducted before a surgical operation. The primary goal of preoperative care is to ensure the patient's well-being, optimize their physical condition, reduce potential risks, and prepare them mentally and emotionally for the upcoming surgery.
Preoperative care typically includes:
1. Preoperative assessment: A thorough evaluation of the patient's overall health status, including medical history, physical examination, laboratory tests, and diagnostic imaging, to identify any potential risk factors or comorbidities that may impact the surgical procedure and postoperative recovery.
2. Informed consent: The process of ensuring the patient understands the nature of the surgery, its purpose, associated risks, benefits, and alternative treatment options. The patient signs a consent form indicating they have been informed and voluntarily agree to undergo the surgery.
3. Preoperative instructions: Guidelines provided to the patient regarding their diet, medication use, and other activities in the days leading up to the surgery. These instructions may include fasting guidelines, discontinuing certain medications, or arranging for transportation after the procedure.
4. Anesthesia consultation: A meeting with the anesthesiologist to discuss the type of anesthesia that will be used during the surgery and address any concerns related to anesthesia risks, side effects, or postoperative pain management.
5. Preparation of the surgical site: Cleaning and shaving the area where the incision will be made, as well as administering appropriate antimicrobial agents to minimize the risk of infection.
6. Medical optimization: Addressing any underlying medical conditions or correcting abnormalities that may negatively impact the surgical outcome. This may involve adjusting medications, treating infections, or managing chronic diseases such as diabetes.
7. Emotional and psychological support: Providing counseling, reassurance, and education to help alleviate anxiety, fear, or emotional distress related to the surgery.
8. Preoperative holding area: The patient is transferred to a designated area near the operating room where they are prepared for surgery by changing into a gown, having intravenous (IV) lines inserted, and receiving monitoring equipment.
By following these preoperative care guidelines, healthcare professionals aim to ensure that patients undergo safe and successful surgical procedures with optimal outcomes.
Leukocytes, also known as white blood cells (WBCs), are a crucial component of the human immune system. They are responsible for protecting the body against infections and foreign substances. Leukocytes are produced in the bone marrow and circulate throughout the body in the bloodstream and lymphatic system.
There are several types of leukocytes, including:
1. Neutrophils - These are the most abundant type of leukocyte and are primarily responsible for fighting bacterial infections. They contain enzymes that can destroy bacteria.
2. Lymphocytes - These are responsible for producing antibodies and destroying virus-infected cells, as well as cancer cells. There are two main types of lymphocytes: B-lymphocytes and T-lymphocytes.
3. Monocytes - These are the largest type of leukocyte and help to break down and remove dead or damaged tissues, as well as microorganisms.
4. Eosinophils - These play a role in fighting parasitic infections and are also involved in allergic reactions and inflammation.
5. Basophils - These release histamine and other chemicals that cause inflammation in response to allergens or irritants.
An abnormal increase or decrease in the number of leukocytes can indicate an underlying medical condition, such as an infection, inflammation, or a blood disorder.
A single-blind method in medical research is a study design where the participants are unaware of the group or intervention they have been assigned to, but the researchers conducting the study know which participant belongs to which group. This is done to prevent bias from the participants' expectations or knowledge of their assignment, while still allowing the researchers to control the study conditions and collect data.
In a single-blind trial, the participants do not know whether they are receiving the active treatment or a placebo (a sham treatment that looks like the real thing but has no therapeutic effect), whereas the researcher knows which participant is receiving which intervention. This design helps to ensure that the participants' responses and outcomes are not influenced by their knowledge of the treatment assignment, while still allowing the researchers to assess the effectiveness or safety of the intervention being studied.
Single-blind methods are commonly used in clinical trials and other medical research studies where it is important to minimize bias and control for confounding variables that could affect the study results.
Papillary muscles are specialized muscle structures located in the heart, specifically in the ventricles (the lower chambers of the heart). They are attached to the tricuspid and mitral valves' leaflets via tendinous cords, also known as chordae tendineae. The main function of papillary muscles is to prevent the backflow of blood during contraction by providing tension to the valve leaflets through these tendinous cords.
There are two sets of papillary muscles in the heart:
1. Anterior and posterior papillary muscles in the left ventricle, which are attached to the mitral (bicuspid) valve.
2. Three smaller papillary muscles in the right ventricle, which are attached to the tricuspid valve.
These muscle structures play a crucial role in maintaining proper blood flow through the heart and ensuring efficient cardiac function.
Imidazoles are a class of heterocyclic organic compounds that contain a double-bonded nitrogen atom and two additional nitrogen atoms in the ring. They have the chemical formula C3H4N2. In a medical context, imidazoles are commonly used as antifungal agents. Some examples of imidazole-derived antifungals include clotrimazole, miconazole, and ketoconazole. These medications work by inhibiting the synthesis of ergosterol, a key component of fungal cell membranes, leading to increased permeability and death of the fungal cells. Imidazoles may also have anti-inflammatory, antibacterial, and anticancer properties.
Plasmalogens are a type of complex lipid called glycerophospholipids, which are essential components of cell membranes. They are characterized by having a unique chemical structure that includes a vinyl ether bond at the sn-1 position of the glycerol backbone and an ester bond at the sn-2 position, with the majority of them containing polyunsaturated fatty acids. The headgroup attached to the sn-3 position is typically choline or ethanolamine.
Plasmalogens are abundant in certain tissues, such as the brain, heart, and skeletal muscle. They have been suggested to play important roles in cellular functions, including membrane fluidity, signal transduction, and protection against oxidative stress. Reduced levels of plasmalogens have been associated with various diseases, including neurological disorders, cardiovascular diseases, and aging-related conditions.
Glycogen is a complex carbohydrate that serves as the primary form of energy storage in animals, fungi, and bacteria. It is a polysaccharide consisting of long, branched chains of glucose molecules linked together by glycosidic bonds. Glycogen is stored primarily in the liver and muscles, where it can be quickly broken down to release glucose into the bloodstream during periods of fasting or increased metabolic demand.
In the liver, glycogen plays a crucial role in maintaining blood glucose levels by releasing glucose when needed, such as between meals or during exercise. In muscles, glycogen serves as an immediate energy source for muscle contractions during intense physical activity. The ability to store and mobilize glycogen is essential for the proper functioning of various physiological processes, including athletic performance, glucose homeostasis, and overall metabolic health.
"Newborn animals" refers to the very young offspring of animals that have recently been born. In medical terminology, newborns are often referred to as "neonates," and they are classified as such from birth until about 28 days of age. During this time period, newborn animals are particularly vulnerable and require close monitoring and care to ensure their survival and healthy development.
The specific needs of newborn animals can vary widely depending on the species, but generally, they require warmth, nutrition, hydration, and protection from harm. In many cases, newborns are unable to regulate their own body temperature or feed themselves, so they rely heavily on their mothers for care and support.
In medical settings, newborn animals may be examined and treated by veterinarians to ensure that they are healthy and receiving the care they need. This can include providing medical interventions such as feeding tubes, antibiotics, or other treatments as needed to address any health issues that arise. Overall, the care and support of newborn animals is an important aspect of animal medicine and conservation efforts.
Thiourea is not a medical term, but a chemical compound. It's a colorless crystalline solid with the formula SC(NH2)2. Thiourea is used in some industrial processes and can be found in some laboratory reagents. It has been studied for its potential effects on certain medical conditions, such as its ability to protect against radiation damage, but it is not a medication or a treatment that is currently in clinical use.
Tumor Necrosis Factor-alpha (TNF-α) is a cytokine, a type of small signaling protein involved in immune response and inflammation. It is primarily produced by activated macrophages, although other cell types such as T-cells, natural killer cells, and mast cells can also produce it.
TNF-α plays a crucial role in the body's defense against infection and tissue injury by mediating inflammatory responses, activating immune cells, and inducing apoptosis (programmed cell death) in certain types of cells. It does this by binding to its receptors, TNFR1 and TNFR2, which are found on the surface of many cell types.
In addition to its role in the immune response, TNF-α has been implicated in the pathogenesis of several diseases, including autoimmune disorders such as rheumatoid arthritis, inflammatory bowel disease, and psoriasis, as well as cancer, where it can promote tumor growth and metastasis.
Therapeutic agents that target TNF-α, such as infliximab, adalimumab, and etanercept, have been developed to treat these conditions. However, these drugs can also increase the risk of infections and other side effects, so their use must be carefully monitored.
Isosorbide is a type of sugar alcohol (a sugary-tasting substance that is not actually sugar) used as a low-calorie sweetener and sugar substitute in various food and pharmaceutical products. It is also used as an active ingredient in some medications for treating chest pain (angina) and heart failure.
Medically, isosorbide can exist in two forms: isosorbide dinitrate and isosorbide mononitrate. These are both vasodilators, meaning they relax and widen blood vessels, improving blood flow and reducing the workload on the heart. Isosorbide dinitrate is often used to prevent angina attacks, while isosorbide mononitrate is used for both prevention and treatment of angina.
It's important to note that overuse of sugar alcohols like isosorbide can lead to digestive issues such as bloating, diarrhea, and gas due to their incomplete absorption in the gut.
Nonparametric statistics is a branch of statistics that does not rely on assumptions about the distribution of variables in the population from which the sample is drawn. In contrast to parametric methods, nonparametric techniques make fewer assumptions about the data and are therefore more flexible in their application. Nonparametric tests are often used when the data do not meet the assumptions required for parametric tests, such as normality or equal variances.
Nonparametric statistical methods include tests such as the Wilcoxon rank-sum test (also known as the Mann-Whitney U test) for comparing two independent groups, the Wilcoxon signed-rank test for comparing two related groups, and the Kruskal-Wallis test for comparing more than two independent groups. These tests use the ranks of the data rather than the actual values to make comparisons, which allows them to be used with ordinal or continuous data that do not meet the assumptions of parametric tests.
Overall, nonparametric statistics provide a useful set of tools for analyzing data in situations where the assumptions of parametric methods are not met, and can help researchers draw valid conclusions from their data even when the data are not normally distributed or have other characteristics that violate the assumptions of parametric tests.
Primary headache disorders are a group of headaches that are not caused by an underlying medical condition or structural problem. They are considered to be separate medical entities and include:
1. Migraine: A recurring headache that typically causes moderate to severe throbbing pain, often on one side of the head. It is commonly accompanied by nausea, vomiting, and sensitivity to light and sound.
2. Tension-type headache (TTH): The most common type of headache, characterized by a pressing or tightening sensation around the forehead or back of the head and neck. It is usually not aggravated by physical activity and does not cause nausea or vomiting.
3. Cluster headache: A rare but extremely painful type of headache that occurs in clusters, meaning they happen several times a day for weeks or months, followed by periods of remission. The pain is usually one-sided, centered around the eye and often accompanied by redness, tearing, and nasal congestion.
4. New daily persistent headache (NDPH): A type of headache that starts suddenly and persists every day for weeks or months. It can be similar to tension-type headaches or migraines but is not caused by an underlying medical condition.
5. Trigeminal autonomic cephalalgias (TACs): A group of primary headache disorders characterized by severe pain on one side of the head, often accompanied by symptoms such as redness, tearing, and nasal congestion. Cluster headaches are a type of TAC.
6. Other primary headache disorders: These include rare conditions such as hemicrania continua, paroxysmal hemicrania, and short-lasting unilateral neuralgiform headache attacks.
Primary headache disorders can significantly impact a person's quality of life and ability to function. Treatment typically involves medication, lifestyle changes, and behavioral therapies.
A stent is a small mesh tube that's used to treat narrow or weak arteries. Arteries are blood vessels that carry blood away from your heart to other parts of your body. A stent is placed in an artery as part of a procedure called angioplasty. Angioplasty restores blood flow through narrowed or blocked arteries by inflating a tiny balloon inside the blocked artery to widen it.
The stent is then inserted into the widened artery to keep it open. The stent is usually made of metal, but some are coated with medication that is slowly and continuously released to help prevent the formation of scar tissue in the artery. This can reduce the chance of the artery narrowing again.
Stents are also used in other parts of the body, such as the neck (carotid artery) and kidneys (renal artery), to help maintain blood flow and prevent blockages. They can also be used in the urinary system to treat conditions like ureteropelvic junction obstruction or narrowing of the urethra.
Voltage-gated sodium channel blockers are a class of pharmaceutical drugs or toxins that work by inhibiting the function of voltage-gated sodium channels. These channels are crucial for the initiation and propagation of action potentials in excitable cells, such as neurons and muscle fibers. By blocking these channels, the drug reduces the flow of sodium ions into the cell, which stabilizes the membrane potential and prevents or reduces the generation of action potentials.
This class of drugs is used to treat a variety of medical conditions, including cardiac arrhythmias, neuropathic pain, and epilepsy. Examples of voltage-gated sodium channel blockers include Class I antiarrhythmics such as lidocaine, flecainide, and propafenone, as well as some antiepileptic drugs like carbamazepine and lamotrigine. Some toxins, such as those found in certain types of cone snails and spiders, also act as voltage-gated sodium channel blockers.
Angiogenesis inducing agents are substances or drugs that stimulate the growth of new blood vessels, a process known as angiogenesis. This process is essential for the growth and development of tissues and organs in the body, including wound healing and the formation of blood vessels in the placenta during pregnancy. However, abnormal angiogenesis can also contribute to various diseases, such as cancer, diabetic retinopathy, and age-related macular degeneration.
Angiogenesis inducing agents are being studied for their potential therapeutic benefits in a variety of medical conditions. For example, they may be used to promote wound healing or tissue repair after injury or surgery. In cancer treatment, angiogenesis inhibitors are often used to block the growth of new blood vessels and prevent tumors from growing and spreading. However, angiogenesis inducing agents can have the opposite effect and may potentially be used to enhance the delivery of drugs to tumors or improve the effectiveness of other cancer treatments.
Examples of angiogenesis inducing agents include certain growth factors, such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and platelet-derived growth factor (PDGF). These substances can be administered as drugs to stimulate angiogenesis in specific contexts. Other substances, such as hypoxia-inducible factors (HIFs) and prostaglandins, can also induce angiogenesis under certain conditions.
Fibrinolytic agents are medications that dissolve or break down blood clots by activating plasminogen, which is converted into plasmin. Plasmin is a proteolytic enzyme that degrades fibrin, the structural protein in blood clots. Fibrinolytic agents are used medically to treat conditions such as acute ischemic stroke, deep vein thrombosis, pulmonary embolism, and myocardial infarction (heart attack) by restoring blood flow in occluded vessels. Examples of fibrinolytic agents include alteplase, reteplase, and tenecteplase. It is important to note that these medications carry a risk of bleeding complications and should be administered with caution.
The vagus nerve, also known as the 10th cranial nerve (CN X), is the longest of the cranial nerves and extends from the brainstem to the abdomen. It has both sensory and motor functions and plays a crucial role in regulating various bodily functions such as heart rate, digestion, respiratory rate, speech, and sweating, among others.
The vagus nerve is responsible for carrying sensory information from the internal organs to the brain, and it also sends motor signals from the brain to the muscles of the throat and voice box, as well as to the heart, lungs, and digestive tract. The vagus nerve helps regulate the body's involuntary responses, such as controlling heart rate and blood pressure, promoting relaxation, and reducing inflammation.
Dysfunction in the vagus nerve can lead to various medical conditions, including gastroparesis, chronic pain, and autonomic nervous system disorders. Vagus nerve stimulation (VNS) is a therapeutic intervention that involves delivering electrical impulses to the vagus nerve to treat conditions such as epilepsy, depression, and migraine headaches.
The femoral artery is the major blood vessel that supplies oxygenated blood to the lower extremity of the human body. It is a continuation of the external iliac artery and becomes the popliteal artery as it passes through the adductor hiatus in the adductor magnus muscle of the thigh.
The femoral artery is located in the femoral triangle, which is bound by the sartorius muscle anteriorly, the adductor longus muscle medially, and the biceps femoris muscle posteriorly. It can be easily palpated in the groin region, making it a common site for taking blood samples, measuring blood pressure, and performing surgical procedures such as femoral artery catheterization and bypass grafting.
The femoral artery gives off several branches that supply blood to the lower limb, including the deep femoral artery, the superficial femoral artery, and the profunda femoris artery. These branches provide blood to the muscles, bones, skin, and other tissues of the leg, ankle, and foot.
Sufentanil is a potent, synthetic opioid analgesic that is approximately 5-10 times more potent than fentanyl and 1000 times more potent than morphine. It is primarily used for the treatment of moderate to severe pain in surgical settings, as an adjunct to anesthesia, or for obstetrical analgesia during labor and delivery.
Sufentanil works by binding to opioid receptors in the brain and spinal cord, which inhibits the transmission of pain signals to the brain. It has a rapid onset of action and a short duration of effect, making it useful for procedures that require intense analgesia for brief periods.
Like other opioids, sufentanil can cause respiratory depression, sedation, nausea, vomiting, and constipation. It should be used with caution in patients with compromised respiratory function or those who are taking other central nervous system depressants.
Oxidation-Reduction (redox) reactions are a type of chemical reaction involving a transfer of electrons between two species. The substance that loses electrons in the reaction is oxidized, and the substance that gains electrons is reduced. Oxidation and reduction always occur together in a redox reaction, hence the term "oxidation-reduction."
In biological systems, redox reactions play a crucial role in many cellular processes, including energy production, metabolism, and signaling. The transfer of electrons in these reactions is often facilitated by specialized molecules called electron carriers, such as nicotinamide adenine dinucleotide (NAD+/NADH) and flavin adenine dinucleotide (FAD/FADH2).
The oxidation state of an element in a compound is a measure of the number of electrons that have been gained or lost relative to its neutral state. In redox reactions, the oxidation state of one or more elements changes as they gain or lose electrons. The substance that is oxidized has a higher oxidation state, while the substance that is reduced has a lower oxidation state.
Overall, oxidation-reduction reactions are fundamental to the functioning of living organisms and are involved in many important biological processes.
Endothelin A (ETA) receptor is a type of G protein-coupled receptor that is activated by the peptide hormone endothelin-1, endothelin-2, and endothelin-3. It is widely expressed in various tissues and organs, including vascular smooth muscle cells, cardiac myocytes, fibroblasts, and kidney cells. Activation of ETA receptor leads to vasoconstriction, increased cell proliferation, and fibrosis, which contribute to the development of hypertension, heart failure, and chronic kidney disease. Therefore, ETA receptor antagonists have been developed as potential therapeutic agents for these conditions.
Endothelial growth factors (ECGFs or EGFs) are a group of signaling proteins that stimulate the growth, proliferation, and survival of endothelial cells, which line the interior surface of blood vessels. These growth factors play crucial roles in various physiological processes, including angiogenesis (the formation of new blood vessels), wound healing, and vascular development during embryogenesis.
One of the most well-studied EGFs is the vascular endothelial growth factor (VEGF) family, which consists of several members like VEGFA, VEGFB, VEGFC, VEGFD, and placental growth factor (PlGF). These factors bind to specific receptors on the surface of endothelial cells, leading to a cascade of intracellular signaling events that ultimately result in cell proliferation, migration, and survival.
Other EGFs include fibroblast growth factors (FGFs), hepatocyte growth factor (HGF), platelet-derived growth factor (PDGF), and transforming growth factor-beta (TGF-β). Dysregulation of endothelial growth factors has been implicated in various pathological conditions, such as cancer, diabetic retinopathy, age-related macular degeneration, and cardiovascular diseases. Therefore, understanding the functions and regulation of EGFs is essential for developing novel therapeutic strategies to treat these disorders.
Xanthine oxidase is an enzyme that catalyzes the oxidation of xanthine to uric acid, which is the last step in purine metabolism. It's a type of molybdenum-containing oxidoreductase that generates reactive oxygen species (ROS) during its reaction mechanism.
The enzyme exists in two interconvertible forms: an oxidized state and a reduced state. The oxidized form, called xanthine oxidase, reduces molecular oxygen to superoxide and hydrogen peroxide, while the reduced form, called xanthine dehydrogenase, reduces NAD+ to NADH.
Xanthine oxidase is found in various tissues, including the liver, intestines, and milk. An overproduction of uric acid due to increased activity of xanthine oxidase can lead to hyperuricemia, which may result in gout or kidney stones. Some medications and natural compounds are known to inhibit xanthine oxidase, such as allopurinol and febuxostat, which are used to treat gout and prevent the formation of uric acid stones in the kidneys.
Observer variation, also known as inter-observer variability or measurement agreement, refers to the difference in observations or measurements made by different observers or raters when evaluating the same subject or phenomenon. It is a common issue in various fields such as medicine, research, and quality control, where subjective assessments are involved.
In medical terms, observer variation can occur in various contexts, including:
1. Diagnostic tests: Different radiologists may interpret the same X-ray or MRI scan differently, leading to variations in diagnosis.
2. Clinical trials: Different researchers may have different interpretations of clinical outcomes or adverse events, affecting the consistency and reliability of trial results.
3. Medical records: Different healthcare providers may document medical histories, physical examinations, or treatment plans differently, leading to inconsistencies in patient care.
4. Pathology: Different pathologists may have varying interpretations of tissue samples or laboratory tests, affecting diagnostic accuracy.
Observer variation can be minimized through various methods, such as standardized assessment tools, training and calibration of observers, and statistical analysis of inter-rater reliability.
Retinal vessels refer to the blood vessels that are located in the retina, which is the light-sensitive tissue that lines the inner surface of the eye. The retina contains two types of blood vessels: arteries and veins.
The central retinal artery supplies oxygenated blood to the inner layers of the retina, while the central retinal vein drains deoxygenated blood from the retina. These vessels can be visualized during a routine eye examination using an ophthalmoscope, which allows healthcare professionals to assess their health and any potential abnormalities.
Retinal vessels are essential for maintaining the health and function of the retina, and any damage or changes to these vessels can affect vision and lead to various eye conditions such as diabetic retinopathy, retinal vein occlusion, and hypertensive retinopathy.
Cardiopulmonary bypass (CPB) is a medical procedure that temporarily takes over the functions of the heart and lungs during major heart surgery. It allows the surgeon to operate on a still, bloodless heart.
During CPB, the patient's blood is circulated outside the body with the help of a heart-lung machine. The machine pumps the blood through a oxygenator, where it is oxygenated and then returned to the body. This bypasses the heart and lungs, hence the name "cardiopulmonary bypass."
CPB involves several components, including a pump, oxygenator, heat exchanger, and tubing. The patient's blood is drained from the heart through cannulas (tubes) and passed through the oxygenator, where it is oxygenated and carbon dioxide is removed. The oxygenated blood is then warmed to body temperature in a heat exchanger before being pumped back into the body.
While on CPB, the patient's heart is stopped with the help of cardioplegia solution, which is infused directly into the coronary arteries. This helps to protect the heart muscle during surgery. The surgeon can then operate on a still and bloodless heart, allowing for more precise surgical repair.
After the surgery is complete, the patient is gradually weaned off CPB, and the heart is restarted with the help of electrical stimulation or medication. The patient's condition is closely monitored during this time to ensure that their heart and lungs are functioning properly.
While CPB has revolutionized heart surgery and allowed for more complex procedures to be performed, it is not without risks. These include bleeding, infection, stroke, kidney damage, and inflammation. However, with advances in technology and technique, the risks associated with CPB have been significantly reduced over time.
Chinese herbal drugs, also known as traditional Chinese medicine (TCM), refer to a system of medicine that has been practiced in China for thousands of years. It is based on the belief that the body's vital energy, called Qi, must be balanced and flowing freely for good health. TCM uses various techniques such as herbal therapy, acupuncture, dietary therapy, and exercise to restore balance and promote healing.
Chinese herbal drugs are usually prescribed in the form of teas, powders, pills, or tinctures and may contain one or a combination of herbs. The herbs used in Chinese medicine are typically derived from plants, minerals, or animal products. Some commonly used Chinese herbs include ginseng, astragalus, licorice root, and cinnamon bark.
It is important to note that the use of Chinese herbal drugs should be under the guidance of a qualified practitioner, as some herbs can interact with prescription medications or have side effects. Additionally, the quality and safety of Chinese herbal products can vary widely depending on the source and manufacturing process.
Papaverine is defined as a smooth muscle relaxant and a non-narcotic alkaloid derived from the opium poppy. It works by blocking the phosphodiesterase enzyme, leading to an increase in cyclic adenosine monophosphate (cAMP) levels within the cells, which in turn results in muscle relaxation.
It is used medically for its vasodilatory effects to treat conditions such as cerebral or peripheral vascular spasms and occlusive diseases, Raynaud's phenomenon, and priapism. Papaverine can also be used as an anti-arrhythmic agent in the management of certain types of cardiac arrhythmias.
It is important to note that papaverine has a narrow therapeutic index, and its use should be closely monitored due to the potential for adverse effects such as hypotension, reflex tachycardia, and gastrointestinal disturbances.
Brain hypoxia is a medical condition characterized by a reduced supply of oxygen to the brain. The brain requires a continuous supply of oxygen to function properly, and even a brief period of hypoxia can cause significant damage to brain cells.
Hypoxia can result from various conditions, such as cardiac arrest, respiratory failure, carbon monoxide poisoning, or high altitude exposure. When the brain is deprived of oxygen, it can lead to a range of symptoms, including confusion, disorientation, seizures, loss of consciousness, and ultimately, brain death.
Brain hypoxia is a medical emergency that requires immediate treatment to prevent long-term neurological damage or death. Treatment typically involves addressing the underlying cause of hypoxia, such as administering oxygen therapy, resuscitating the heart, or treating respiratory failure. In some cases, more invasive treatments, such as therapeutic hypothermia or mechanical ventilation, may be necessary to prevent further brain damage.
The Stellate Ganglion is a part of the sympathetic nervous system. It's a collection of nerve cells (a ganglion) located in the neck, more specifically at the level of the sixth and seventh cervical vertebrae. The stellate ganglion is formed by the fusion of the inferior cervical ganglion and the first thoracic ganglion.
This ganglion plays a crucial role in the body's "fight or flight" response, providing sympathetic innervation to the head, neck, upper extremities, and heart. It's responsible for various functions including regulation of blood flow, sweat gland activity, and contributing to the sensory innervation of the head and neck.
Stellate ganglion block is a medical procedure used to diagnose or treat certain conditions like pain disorders, by injecting local anesthetic near the stellate ganglion to numb the area and interrupt nerve signals.
Naloxone is a medication used to reverse the effects of opioids, both illicit and prescription. It works by blocking the action of opioids on the brain and restoring breathing in cases where opioids have caused depressed respirations. Common brand names for naloxone include Narcan and Evzio.
Naloxone is an opioid antagonist, meaning that it binds to opioid receptors in the body without activating them, effectively blocking the effects of opioids already present at these sites. It has no effect in people who have not taken opioids and does not reverse the effects of other sedatives or substances.
Naloxone can be administered via intranasal, intramuscular, intravenous, or subcutaneous routes. The onset of action varies depending on the route of administration but generally ranges from 1 to 5 minutes when given intravenously and up to 10-15 minutes with other methods.
The duration of naloxone's effects is usually shorter than that of most opioids, so multiple doses or a continuous infusion may be necessary in severe cases to maintain reversal of opioid toxicity. Naloxone has been used successfully in emergency situations to treat opioid overdoses and has saved many lives.
It is important to note that naloxone does not reverse the effects of other substances or address the underlying causes of addiction, so it should be used as part of a comprehensive treatment plan for individuals struggling with opioid use disorders.
Hypotension is a medical term that refers to abnormally low blood pressure, usually defined as a systolic blood pressure less than 90 millimeters of mercury (mm Hg) or a diastolic blood pressure less than 60 mm Hg. Blood pressure is the force exerted by the blood against the walls of the blood vessels as the heart pumps blood.
Hypotension can cause symptoms such as dizziness, lightheadedness, weakness, and fainting, especially when standing up suddenly. In severe cases, hypotension can lead to shock, which is a life-threatening condition characterized by multiple organ failure due to inadequate blood flow.
Hypotension can be caused by various factors, including certain medications, medical conditions such as heart disease, endocrine disorders, and dehydration. It is important to seek medical attention if you experience symptoms of hypotension, as it can indicate an underlying health issue that requires treatment.
Protein Kinase C (PKC) is a family of serine-threonine kinases that play crucial roles in various cellular signaling pathways. These enzymes are activated by second messengers such as diacylglycerol (DAG) and calcium ions (Ca2+), which result from the activation of cell surface receptors like G protein-coupled receptors (GPCRs) and receptor tyrosine kinases (RTKs).
Once activated, PKC proteins phosphorylate downstream target proteins, thereby modulating their activities. This regulation is involved in numerous cellular processes, including cell growth, differentiation, apoptosis, and membrane trafficking. There are at least 10 isoforms of PKC, classified into three subfamilies based on their second messenger requirements and structural features: conventional (cPKC; α, βI, βII, and γ), novel (nPKC; δ, ε, η, and θ), and atypical (aPKC; ζ and ι/λ). Dysregulation of PKC signaling has been implicated in several diseases, such as cancer, diabetes, and neurological disorders.
Calcitonin gene-related peptide (CGRP) receptors are a type of cell surface receptor found in various tissues and cells, including the nervous system and blood vessels. CGRP is a neuropeptide that plays a role in regulating vasodilation, inflammation, and nociception (the sensation of pain).
The CGRP receptor is a complex of two proteins: calcitonin receptor-like receptor (CLR) and receptor activity-modifying protein 1 (RAMP1). When CGRP binds to the CLR-RAMP1 complex, it activates a signaling pathway that leads to vasodilation and increased pain sensitivity.
CGRP receptors have been identified as important targets for the treatment of migraine headaches, as CGRP levels are known to increase during migraine attacks. Several drugs that target CGRP receptors have been developed and approved for the prevention and acute treatment of migraines.
Sulfinpyrazone is a medication that belongs to the class of drugs known as uricosurics. It works by increasing the amount of uric acid that is removed from the body through urine, which helps to lower the levels of uric acid in the blood. This makes it useful for the treatment of conditions such as gout and kidney stones that are caused by high levels of uric acid.
In addition to its uricosuric effects, sulfinpyrazone also has antiplatelet properties, which means that it can help to prevent blood clots from forming. This makes it useful for the prevention of heart attacks and strokes in people who are at risk.
Sulfinpyrazone is available by prescription and is typically taken by mouth in the form of tablets. It may be used alone or in combination with other medications, depending on the individual patient's needs and medical condition. As with any medication, sulfinpyrazone should be used under the supervision of a healthcare provider, and patients should follow their provider's instructions carefully to ensure safe and effective use.
The abdominal aorta is the portion of the aorta, which is the largest artery in the body, that runs through the abdomen. It originates from the thoracic aorta at the level of the diaphragm and descends through the abdomen, where it branches off into several smaller arteries that supply blood to the pelvis, legs, and various abdominal organs. The abdominal aorta is typically divided into four segments: the suprarenal, infrarenal, visceral, and parietal portions. Disorders of the abdominal aorta can include aneurysms, atherosclerosis, and dissections, which can have serious consequences if left untreated.
Thromboxanes are a type of lipid compound that is derived from arachidonic acid, a type of fatty acid found in the cell membranes of many organisms. They are synthesized in the body through the action of an enzyme called cyclooxygenase (COX).
Thromboxanes are primarily produced by platelets, a type of blood cell that plays a key role in clotting. Once formed, thromboxanes act as powerful vasoconstrictors, causing blood vessels to narrow and blood flow to decrease. They also promote the aggregation of platelets, which can lead to the formation of blood clots.
Thromboxanes are involved in many physiological processes, including hemostasis (the process by which bleeding is stopped) and inflammation. However, excessive production of thromboxanes has been implicated in a number of pathological conditions, such as heart attacks, strokes, and pulmonary hypertension.
There are several different types of thromboxanes, including thromboxane A2 (TXA2) and thromboxane B2 (TXB2). TXA2 is the most biologically active form and has a very short half-life, while TXB2 is a more stable metabolite that can be measured in the blood to assess thromboxane production.
 Myocardial Ischaemia National Audit Project
Myocardial Ischaemia National Audit Project