Lingual Nerve Injuries
Lingual Nerve
Mandibular Nerve
Foramen Ovale
Trigeminal Nerve Injuries
Tongue
Links between anaesthetic modality and nerve damage during lower third molar surgery. (1/19)
OBJECTIVE: To investigate the relationships between eruption status, gender, social class, grade of operator, anaesthetic modality and nerve damage during third molar surgery. DESIGN: Two centre prospective longitudinal study. SETTING: The department of oral and maxillofacial surgery, University Hospital Birmingham NHS Trust and oral surgery outpatient clinics at Birmingham Dental Hospital. SUBJECTS: A total of 391 patients had surgical removal of lower third molars. Sensory disturbance was recorded at one week post operatively. Patients with altered sensation were followed up at one month, three months and six months following surgery. RESULTS: 614 lower third molars in 391 patients were removed. Forty-six procedures (7.5%) were associated with altered sensation at one week with three procedures (0.49%) showing persistent symptoms at six months. Of these 46 nerve injuries, 26 (4.23%) involved the lingual nerve and 20 (3.25%) the inferior dental nerve (IDN). All three persistent sensations were IDN related. A logistic regression model found that the use ofa lingual retractor chi2 = 11.559, p = 0.003 was more significant than eruption status chi2 = 12.935, p = 0.007. There was no significant relationship between anaesthetic modality, age, social class, sex and seniority of operator. CONCLUSIONS: There was no link between the choices of local or general anaesthesia and nerve damage during lower third molar removal when difficulty of surgery was taken into account. (+info)Iatrogenic paresthesia in the third division of the trigeminal nerve: 12 years of clinical experience. (2/19)
BACKGROUND: Iatrogenic paresthesia in the third division of the trigeminal nerve remains a complex clinical problem with major medicolegal implications. However, most lawsuits can be prevented through better planning of procedures and by obtaining informed consent. The purpose of this article is to present the authors" clinical experience over the past 12 years, to review the principles of prevention and management of trigeminal paresthesia and to highlight the resulting medicolegal implications. METHODS: The files of all 165 patients referred to the oral and maxillofacial surgery department for evaluation of iatrogenic paresthesia in the third division of the trigeminal nerve were reviewed. The characteristics of the subgroup of patients who had taken an attending dentist to court were compared with those of the other patients. RESULTS: Surgical extraction of impacted molars was the main cause of paresthesia in 109 (66%) of the 165 subjects. The alveolar nerve was affected in 89 (54%) subjects, the lingual nerve in 67 (41%) subjects, and both nerves were affected in 9 (5%) subjects. There were more female than male patients (ratio 2.2:1). Lawsuits were initiated in 33 (20%) of the cases; patients who initiated lawsuits were younger, were more likely to have experienced anesthesia and were more likely to need microsurgery (all p < 0.001). Poor surgical planning and lack of informed consent were the most common errors on the part of the dentists. CONCLUSIONS: An accurate evaluation of surgical indications and risk, good surgical technique, preoperative informed consent and sufficient postoperative follow-up should help to reduce the frequency of neurosensory deficits after dental treatment and attendant lawsuits. (+info)Lingual nerve injury associated with the ProSeal laryngeal mask airway: a case report and review of the literature. (3/19)
We present a case of lingual nerve injury that was associated with use of the ProSeal laryngeal mask airway during shoulder replacement in a 61-yr-old male. We also review other cases of cranial nerve injury, most of which were associated with use of the classic laryngeal mask airway. In principle, the frequency of cranial nerve injuries can be reduced by avoiding insertion trauma, using appropriate sizes, minimizing cuff volume, and early identification and correction of malposition. (+info)Morbidity of third molar extraction in patients between 12 and 18 years of age. (4/19)
OBJECTIVE: An analysis is made of the incidence of complications following third molar surgical extraction in patients between 12 and 18 years of age. PATIENTS AND METHOD: A retrospective study was conducted of 390 surgical extractions of upper and lower third molars in 173 patients operated upon under locoregional anesthesia during the year 2000 in the Master in Oral Surgery and Implantology of Barcelona University Dental School (Spain). The patients were divided into three age groups (A: 12-14 years, B: 15-16 years, C: 17-18 years). The reason for extraction, the degree of dental development, and third molar position, angle and impaction were recorded. Finally, the association of these variables to the appearance of postoperative complications was analyzed. RESULTS: Most patients were females (66.9%), and the age group in which most extractions were carried out (62.8%) corresponded to Group C (17-18 years). The main reason for extraction was orthodontist indication (40.5%), closely followed by prophylaxis (39.5%). The existence of clinical manifestations was an indication for extraction in 20% of cases. The postoperative complications rate after the extraction of the global 390 molars was 15.6%. In Groups A, B and C the complication risks were 17.4%, 19% and 13.7%, respectively. All complications were reversible and of short duration. One case each of inferior alveolar nerve paresthesia and lingual nerve paresthesia was recorded, which subsided after one and two months, respectively. CONCLUSIONS: There were no significant differences in complications between the three age groups. An increased tendency towards complications was observed in females, and the percentage of postoperative problems increased. (+info)Nerve injuries after dental injection: a review of the literature. (5/19)
Prolonged and possibly permanent change in sensation due to nerve damage can occur after dental injections. Although the condition is rare, many practitioners will see this form of nerve injury during their careers. The exact mechanism of the injury has yet to be determined, and little can be done to prevent its occurrence. This type of injury carries with it many functional and psychological implications, and referral to both dental and medical specialists may be necessary for continued follow-up and possible treatment. (+info)Comparison of morbidity following the removal of mandibular third molar by lingual split, surgical bur and simplified split bone technique. (6/19)
BACKGROUND: The methods frequently used for surgical removal of impacted third molars are bur technique, lingual split and simplified split bone technique. The morbidity rates following the use of these different surgical techniques are not completely resolved. The use of a surgical method with minimum postoperative complication is needed. AIM: This study was conducted to compare the morbidity rates of the three different surgical techniques and their efficacy with regard to postoperative pain, swelling, labial and lingual sensation. MATERIALS AND METHODS: Ninety patients with a symptomatic impacted mandibular third molar with the age range of 14-62 years were divided into three groups of 30 patients each for surgical bur technique, lingual split technique and simplified split bone technique. All patients were operated by the same surgeon under local anesthesia (2% lignocaine) in the dental chair. The severity of pain and swelling was recorded on a visual analogue scale and the presence or absence of sensory disturbance at 6, 24, 48 hours and seven days after operation. The pain was scored according to a visual analogue 4-point scale. Patients were asked to indicate which side was more swollen and to record this assessment on the swelling scale. RESULTS: Lingual split technique was more painful than the other two techniques. Surgical bur technique had more swelling than the other two techniques. Labial and lingual sensations were not altered in all the techniques. CONCLUSION: The simplified split bone technique had the least morbidity than the lingual split and surgical bur technique. (+info)Extra-laryngeal complications of suspension laryngoscopy. (7/19)
Although suspension laryngoscopy is routinely used in laryngeal surgery, there are only few studies on the complications of this procedure. AIM: to evaluate the complications outside the larynx following suspension laryngoscopy and analyze their relation with surgery duration. MATERIALS AND METHODS: Thirty-seven procedures were prospectively analyzed for intervention-related complications. The study included patient preoperative and postoperative assessment, focusing on dental, mucosal and nerve status (hypoglossal and lingual nerves). RESULTS: Most procedures (27/37) were associated to some kind of complication, and mucosal injuries were the most common; temporary nerve lesions were observed in five cases and dental injuries in one case. Statistic significance was found between surgery duration and mucosal injury (lesions smaller than 1 centimeter), showing that longer procedure pose higher risks for these complications. CONCLUSION: These findings suggest that suspension laryngoscopy is frequently associated with complications outside the larynx. Although these injuries represent a low risk of significant morbidity, they can be avoided if more accurate techniques are used. (+info)Retrospective review of voluntary reports of nonsurgical paresthesia in dentistry. (8/19)
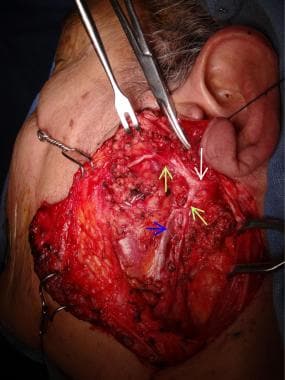
OBJECTIVE: Paresthesia is an adverse event that may be associated with the administration of local anesthetics in dentistry. The purpose of this retrospective study was to analyze cases of paresthesia associated with local anesthetic injection that were voluntarily reported to Ontario"s Professional Liability Program (PLP) from 1999 to 2008 inclusive, to see if the findings were consistent with those from 1973 to 1998 from this same source. MATERIALS AND METHODS: All cases of nonsurgical paresthesia reported from 1999 to 2008 were reviewed; cases involving surgical procedures were excluded. Variables examined included patient age and gender, type and volume of local anesthetic, anatomic site of nerve injury, affected side and pain on injection or any other symptoms. RESULTS: During the study period, 182 PLP reports of paresthesia following nonsurgical procedures were made; all but 2 were associated with mandibular block injection. There was no significant gender predilection, but the lingual nerve was affected more than twice as frequently as the inferior alveolar nerve. During 2006-2008 alone, 64 cases of nonsurgical paresthesia were reported to PLP, a reported incidence of 1 in 609,000 injections. For the 2 local anesthetic drugs available in dental cartridges as 4% solutions, i.e., articaine and prilocaine, the frequencies of reporting of paresthesia were significantly greater than expected (chi2, exact binomial distribution; p < 0.01) based on their level of use by Ontario dentists. These data suggest that local anesthetic neurotoxicity may be at least partly involved in the development of postinjection paresthesia. (+info)A lingual nerve injury refers to damage or trauma to the lingual nerve, which is a branch of the mandibular nerve (itself a branch of the trigeminal nerve). The lingual nerve provides sensation to the anterior two-thirds of the tongue and the floor of the mouth. It also contributes to taste perception on the front two-thirds of the tongue through its connection with the chorda tympani nerve.
Lingual nerve injuries can result from various causes, such as surgical procedures (e.g., dental extractions, implant placements, or third molar surgeries), pressure from tumors or cysts, or direct trauma to the mouth and tongue area. The injury may lead to symptoms like numbness, altered taste sensation, pain, or difficulty speaking and swallowing. Treatment for lingual nerve injuries typically involves a combination of symptom management and possible surgical intervention, depending on the severity and cause of the injury.
The lingual nerve is a branch of the mandibular division of the trigeminal nerve (cranial nerve V). It provides general sensory innervation to the anterior two-thirds of the tongue, including taste sensation from the same region. It also supplies sensory innervation to the floor of the mouth and the lingual gingiva (gum tissue). The lingual nerve is closely associated with the submandibular and sublingual salivary glands and their ducts.
The mandibular nerve is a branch of the trigeminal nerve (the fifth cranial nerve), which is responsible for sensations in the face and motor functions such as biting and chewing. The mandibular nerve provides both sensory and motor innervation to the lower third of the face, below the eye and nose down to the chin.
More specifically, it carries sensory information from the lower teeth, lower lip, and parts of the oral cavity, as well as the skin over the jaw and chin. It also provides motor innervation to the muscles of mastication (chewing), which include the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles.
Damage to the mandibular nerve can result in numbness or loss of sensation in the lower face and mouth, as well as weakness or difficulty with chewing and biting.
The foramen ovale is a fetal cardiovascular structure that usually closes after birth. It's a flap-like opening between the right and left atria (the upper chambers) of the heart. This opening allows oxygen-rich blood from the mother to bypass the fetal lungs and go directly to the fetal brain and body.
After birth, when the newborn starts breathing and blood pressure in the lungs increases, the pressure in the left atrium also rises, causing the flap to close and seal the foramen ovale. In about 25% of adults, this flap doesn't close completely, resulting in a condition known as a patent foramen ovale (PFO), which is usually asymptomatic but can rarely lead to complications such as stroke or migraine with aura.
Trigeminal nerve injuries refer to damages or traumas affecting the trigeminal nerve, also known as the fifth cranial nerve. This nerve is responsible for sensations in the face and motor functions such as biting and chewing. Trigeminal nerve injuries can result in various symptoms depending on the severity and location of the injury, including:
1. Loss or reduction of sensation in the face, lips, gums, teeth, or tongue.
2. Pain, often described as burning, aching, or stabbing, in the affected areas.
3. Numbness or tingling sensations.
4. Difficulty with biting, chewing, or performing other motor functions.
5. Impaired taste sensation.
6. Headaches or migraines.
7. Eye dryness or excessive tearing.
Trigeminal nerve injuries can occur due to various reasons, such as trauma during facial surgeries, accidents, tumors, infections, or neurological conditions like multiple sclerosis. Treatment options depend on the cause and severity of the injury and may include medication, physical therapy, surgical intervention, or pain management strategies.
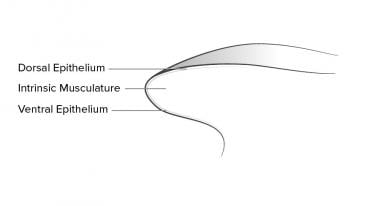
In medical terms, the tongue is a muscular organ in the oral cavity that plays a crucial role in various functions such as taste, swallowing, and speech. It's covered with a mucous membrane and contains papillae, which are tiny projections that contain taste buds to help us perceive different tastes - sweet, salty, sour, and bitter. The tongue also assists in the initial process of digestion by moving food around in the mouth for chewing and mixing with saliva. Additionally, it helps in forming words and speaking clearly by shaping the sounds produced in the mouth.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
 Dental extraction
Dental extraction Lingual Nerve Injury
Lingual Nerve Injury Lingual nerve injury following the use of an i-gel™ laryngeal mask | Teleflex® | LMA®
Lingual nerve injury following the use of an i-gel™ laryngeal mask | Teleflex® | LMA® Reconstructive Options for Inferior Alveolar and Lingual Nerve Injuries After Dental and Oral Surgery: An Evidence-Based Review...
Reconstructive Options for Inferior Alveolar and Lingual Nerve Injuries After Dental and Oral Surgery: An Evidence-Based Review... Extremely Rare Form of Impaction Bilateral Kissing Molars: Report of a Case and Review of the Literature
Extremely Rare Form of Impaction Bilateral Kissing Molars: Report of a Case and Review of the Literature Browsing Centre for Teaching and Innovation (CTI) by Issue Date
Browsing Centre for Teaching and Innovation (CTI) by Issue Date raid1/www/Hosts/bankrupt/CAR Public/001219.MBX
raid1/www/Hosts/bankrupt/CAR Public/001219.MBX Neurophysiology and genetics of burning mouth syndrome - PubMed
Neurophysiology and genetics of burning mouth syndrome - PubMed MeSH Browser
MeSH Browser Oral and Maxillofacial Surgery Archives - UW School of Dentistry
Oral and Maxillofacial Surgery Archives - UW School of Dentistry Rare disease
Rare disease DeCS
DeCS Fort Lauderdale Hospital Negligence Attorney | Hospital Errors Lawyer Weston
Fort Lauderdale Hospital Negligence Attorney | Hospital Errors Lawyer Weston IndexCat
IndexCat Searching for "arthroscopy" - Nucleus Medical Art Library
Searching for "arthroscopy" - Nucleus Medical Art Library Journal of Audiology & Otology
Journal of Audiology & Otology 875,000 Dental Malpractice Settlement - Atlanta Injury Lawyers Blog - June 30, 2015
875,000 Dental Malpractice Settlement - Atlanta Injury Lawyers Blog - June 30, 2015 Negligent Extraction of Wisdom Teeth | Dental Negligence Team | Dental Negligence Team Blog
Negligent Extraction of Wisdom Teeth | Dental Negligence Team | Dental Negligence Team Blog Nerve Injury & Repair<...
Nerve Injury & Repair<... Abnormality of mylohyoid muscle (Concept Id: C4073217)
- MedGen - NCBI
Abnormality of mylohyoid muscle (Concept Id: C4073217)
- MedGen - NCBI