Juxtaglomerular Apparatus
Renin
Kidney Tubules, Distal
Loop of Henle
Arterioles
Kidney
Kidney Tubules
Kidney Glomerulus
Angiotensin II
Golgi Apparatus
Intrarenal site of action of calcium on renin secretion in dogs. (1/269)
We studied the effects of intrarenal calcium infusion on renin secretion in sodium-depleted dogs in an attempt to elucidate the major site of calcium-induced inhibition of renin release. Both calcium chloride and calcium gluconate reduced renal blood flow and renin secretion while renal perfusion pressure was unchanged. These data indicate that calcium inhibition of renin secretion did not occur primarily at the renal vascular receptor; decreased renal blood flow is usually associated with increased renin secretion. Calcium chloride infusion increased urinary chloride excretion without affecting sodium excretion, and calcium gluconate failed to increase either sodium or chloride excretion. Also, the filtered loads of sodium and chloride were unchanged during the calcium infusions. These results give no indication that calcium inhibited renin secretion by increasing the sodium or chloride load at the macula densa. The effects of intrarenal calcium infusion on renin release were also assessed in dogs with a nonfiltering kidney in which renal tubular mechanisms could not influence renin secretion. The observation that calcium still suppressed renin release in these dogs provides additional evidence that the the major effect of calcium involved nontubular mechanisms. Thus, it appears likely that calcium acted directly on the juxtaglomerular cells to inhibit renin secretion. (+info)Direct demonstration of exocytosis and endocytosis in single mouse juxtaglomerular cells. (2/269)
The rate of renin secretion from renal juxtaglomerular (JG) cells is the major determinant of the activity of the renin-angiotensin system. However, the mechanisms involved in the excretion and turnover of secretory granules in the JG cells remain obscure. Therefore, in the present study, the whole-cell patch-clamp technique was applied to single JG cells from the mouse kidney to measure changes in cell membrane capacitance (Cm) as an index of secretory activity. Resting JG cell Cm was stable, on average 3. 13+/-0.13 pF (SEM, n=106). In isotonic solutions, Cm was unaffected by [Cl-]i. Cm was consistently increased (7.0+/-1.3% and 7.2+/-3.1%) by intracellular cAMP (1 to 10 micromol/L). This effect was mimicked by extracellular application of the beta-agonist isoproterenol to the JG cells (9.4+/-3.1%). At 100 micromol/L, cAMP induced a paradoxical decrease in Cm of +info)Tubuloglomerular feedback in ACE-deficient mice. (3/269)
In these experiments, we used a strain of angiotensin converting enzyme (ACE) germline null mutant mice, generated by J. H. Krege and co-workers (J. H. Krege, S. W. M. John, L. L. Langenbach, J. B. Hodgin, J. R. Hagaman, E. S. Bachman, J. C. Jennette, D. A. O'Brien, and O. Smithies. Nature 375: 146-148, 1995), to examine the effect of chronic ACE deficiency on the magnitude of tubuloglomerular feedback (TGF) responses. The genotype was determined by PCR on DNA extracted from the tail and was verified after each experiment by assessment of the blood pressure response to an injection of ANG I. To assess TGF responsiveness, we determined the change in stop-flow pressure (PSF) caused by increasing NaCl concentration at the macula densa by using micropuncture techniques. When loop of Henle flow rate was increased from 0 to 40 nl/min, PSF fell from a mean of 42.3 +/- 1.95 to 33.6 +/- 2.09 mmHg (n = 6, P = 0.005) in wild-type mice (+/+), fell from 40.6 +/- 2.35 to 38.6 +/- 1.93 mmHg in heterozygous (+/-) mice (n = 7, P = 0.014), and did not change in homozygous ACE (-/-) mice [36.7 +/- 2.02 mmHg vs. 36.4 +/- 2.01 mmHg; n = 4, P = not significant (NS)]. During an infusion of ANG II at a dose that did not significantly elevate blood pressure (70 ng. kg-1. min-1), TGF response magnitude (PSF 0 - PSF 40) increased from 6.5 +/- 1.4 to 9.8 +/- 1.19 mmHg in +/+ (P = 0.006), from 1.14 +/- 0.42 to 4.6 +/- 1.3 mmHg in +/- (P = 0.016), and from 0.42 +/- 0.25 to 4.02 +/- 1.06 in -/- mice (P = 0.05). Absence of TGF responses in ACE null mutant mice and restoration of near-normal responses during an acute infusion of ANG II supports previous conclusions that ANG II is an essential component in the signal transmission pathway that links the macula densa with the glomerular vascular pole. (+info)Thromboxane A2 contributes to the enhanced tubuloglomerular feedback activity in young SHR. (4/269)
We performed micropuncture studies to determine the role of thromboxane A2 in the exaggerated tubuloglomerular feedback (TGF) activity in young spontaneously hypertensive rats (SHR). Glomerular function was assessed by changes in proximal tubular stop-flow pressure (SFP) produced by different rates of orthograde perfusion through Henle's loop. Seven-week-old SHR exhibited an exaggerated TGF activity compared with Wistar-Kyoto rats (WKY) during euvolemia, confirming earlier studies. During control periods, the feedback-induced maximal SFP response (DeltaSFP) was greater in SHR (18-19 vs. 12-13 mmHg in WKY), whereas basal SFP and proximal tubular free-flow pressure were similar in both strains. In one series, the thromboxane A2 agonist U-46619 was added to the tubular perfusate for a final concentration of 10(-6) M. In WKY, DeltaSFP was increased by 100% to 26 mmHg. In contrast, DeltaSFP in young SHR was unaffected by the thromboxane A2 agonist. In other animals, the thromboxane synthase inhibitor pirmagrel (50 mg/kg) was injected intravenously to inhibit thromboxane production. In SHR, pirmagrel decreased DeltaSFP by 8.5 mmHg and reduced reactivity. Less attenuation was observed in WKY; DeltaSFP was reduced by 3 mmHg, whereas reactivity was unchanged. In other studies, tubular perfusion with the thromboxane receptor inhibitor SQ-29548 (10(-6) M) reduced DeltaSFP more in SHR (7 vs. 3 mmHg in WKY) and also decreased reactivity more in SHR (2.3 vs. 0.5 mmHg. nl-1. min-1). Coperfusion of SQ-29548 and U-46619 resulted in an 85% block of the effect of U-46619 on DeltaSFP. Tubular perfusion with the agonist U-46619 during thromboxane synthase inhibition markedly enhanced DeltaSFP in both strains, with a greater effect in WKY. These results suggest that elevated levels of thromboxane A2 in young SHR contribute to the exaggerated TGF control of glomerular function in SHR during the developmental phase of hypertension. (+info)Experimental model of renovascular hypertension. (5/269)
OBJECTIVE: To establish a model of renovascular hypertension. METHODS: A 4/0 resorbable chromic catgut ligature was used to ligate subtotally the renal arteries of 18 dogs, forming experimental renovascular hypertension steadily. Blood pressure, plasma renin activity, the ultrastructural changes of juxtaglomerular apparatus and renal artery wall were studied after the constriction. RESULTS: It was reasonable that renal blood flow measured with an electromagnetic flowmeter was reduced by 30% after the constriction. The pathological changes of the induced renal artery stenosis were similar to those of fibromuscular dysphasia. CONCLUSION: The findings provide valuable evidence for the treatment of renovascular hypertension. (+info)Transmural pressure inhibits prorenin processing in juxtaglomerular cell. (6/269)
Pressure control of renin secretion involves a complex integration of shear stress, stretch, and transmural pressure (TP). This study was designed to delineate TP control of renin secretion with minimal influence of shear stress or stretch and to determine its mechanism. Rat juxtaglomerular (JG) cells were applied to a TP-loading apparatus for 12 h. In cells conditioned with atmospheric pressure or atmospheric pressure + 40 mmHg, renin secretion rate (RSR) averaged 29.6 +/- 3.7 and 14.5 +/- 3.3% (P < 0.05, n = 8 cultures), respectively, and active renin content (ARC) averaged 47.3 +/- 4.6 and 38.4 +/- 3.4 ng of ANG I. h(-1). million cells(-1) (P < 0.05, n = 10 cultures), respectively. Total renin content and renin mRNA levels were unaffected by TP. The TP-induced decrease in RSR was prevented by Ca(2+)-free medium and the Ca(2+) channel blocker verapamil and was attenuated by thapsigargin and caffeine, which deplete intracellular Ca(2+) stores. Thapsigargin and caffeine, but not Ca(2+)-free medium or verapamil, prevented TP-induced decreases in ARC. The adenylate cyclase activator forskolin did not modulate TP-induced decreases in RSR or ARC. These findings suggest that TP not only stimulates Ca(2+) influx but also inhibits prorenin processing through an intracellular Ca(2+) store-dependent mechanism and thus inhibits active renin secretion by JG cells. (+info)Differential regulation of renal prostaglandin receptor mRNAs by dietary salt intake in the rat. (7/269)
BACKGROUND: In this study, we tested the hypothesis that prostaglandin (PG) receptor expression in the rat kidney is subject to physiological regulation by dietary salt intake. METHODS: Rats were fed diets with 0.02 or 4% NaCl for two weeks. PG receptor expression was assayed in kidney regions and cells by ribonuclease protection assay and reverse transcription-polymerase chain reaction analysis. Functional correlates were studied by measurement of PGE2-induced cAMP formation and renin secretion in juxtaglomerular (JG) cells isolated from animals on various salt intakes. RESULTS: EP1 and EP3 receptors were predominantly expressed, and the EP2 receptor was exclusively expressed in the rat kidney medulla. The EP4 receptor was strongly expressed in glomeruli and in renin-secreting JG granular cells. IP receptor transcripts were found mainly in cortex. Maintaining rats on a low- or high-NaCl diet did not affect the expression of EP1 or IP receptors, whereas EP4 transcripts in glomeruli were increased twofold by salt deprivation. Consistent with this, we found that PGE2-evoked cAMP production and renin secretion by JG cells from salt-deprived animals were significantly higher compared with cells obtained from salt-loaded animals. In the outer medulla, EP3 transcripts correlated directly with salt intake, and mRNA abundance was increased twofold by a high-NaCl diet. CONCLUSIONS: Our results suggest that subtype-specific, regional changes in PG receptor expression are involved in the renal adaptation to changes in salt intake. The results are in accord with the general concept that renocortical PGE2 stimulates renin secretion and maintains renal blood flow during low-salt states, whereas medullary PGE2 promotes salt excretion in response to a high salt intake. (+info)Regulation of in vitro renin secretion by ANG II feedback manipulation in vivo in the ovine fetus. (8/269)
The renin-angiotensin system is critically important to fetal cardiovascular function and organ development. The feedback regulation of renin secretion by ANG II develops early in gestation yet does not linearly progress from fetal life to adulthood. Renin secretion is elevated in late gestation compared with earlier or postnatal time periods, which suggests that some component of the negative feedback regulation of renin secretion is less sensitive in late gestation. We examined in fetal sheep the age-related consequence of chronic in vivo manipulation of ANG II on renal renin secretion measured in vitro. Immature (101-103 days of gestation) and mature (130-133 days of gestation) fetuses were treated for 72 h with enalaprilat, ANG II or vehicle. Content and basal and isoproterenol-stimulated secretion of prorenin (PR) and active renin (AR) from fetal kidney cortical slices were determined. Enalaprilat pretreatment in vivo increased renal renin content and basal and stimulated secretion of PR and AR in vitro even in immature animals. Immunohistochemical localization showed that enalaprilat treatment caused an age-related recruitment of renin-containing juxtaglomerular cells. Conversely, ANG II pretreatment decreased basal and stimulated PR and AR secretion from immature fetal kidneys, but only inhibited PR secretion from mature kidneys. It also caused an age-related decrease in the percentage of renin-containing juxtaglomerular cells. These results suggest that ANG II feedback modulates not only the synthesis and content of renin, but the sensitivity of the coupling between stimulus and secretion. A critical observation of our study is that the higher renal tissue concentrations of prorenin and active renin in late gestation may be a consequence of reduced sensitivity to ANG II feedback; this is consistent with the increased plasma concentrations of renin found in near-term mammals. (+info)The Juxtaglomerular Apparatus (JGA) is a specialized region located at the junction between the afferent arteriole and the distal convoluted tubule in the nephron of the kidney. It plays a crucial role in regulating blood pressure and fluid balance within the body through the renin-angiotensin-aldosterone system (RAAS).
The JGA consists of three main components:
1. Juxtaglomerular Cells: These are specialized smooth muscle cells found in the media layer of the afferent arteriole. They have the ability to synthesize and release renin, an enzyme that initiates the RAAS cascade. When blood pressure decreases or when sodium levels in the distal convoluted tubule are low, these cells are stimulated to release renin.
2. Macula Densa: This is a group of specialized epithelial cells located within the wall of the distal convoluted tubule at its point of contact with the afferent arteriole. These cells monitor the concentration and flow rate of filtrate in the tubule and provide feedback to the juxtaglomerular cells regarding sodium levels and pressure changes in the nephron.
3. Lacis Cells: Also known as extraglomerular mesangial cells, lacis cells are located within the connective tissue surrounding the JGA. They help regulate blood flow to the glomerulus by contracting or relaxing in response to various stimuli.
In summary, the Juxtaglomerular Apparatus is a critical structure involved in maintaining homeostasis through its role in regulating blood pressure and fluid balance via the renin-angiotensin-aldosterone system.
Renin is a medically recognized term and it is defined as:
"A protein (enzyme) that is produced and released by specialized cells (juxtaglomerular cells) in the kidney. Renin is a key component of the renin-angiotensin-aldosterone system (RAAS), which helps regulate blood pressure and fluid balance in the body.
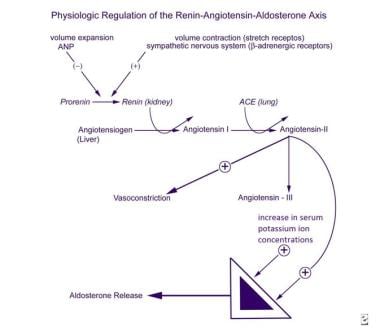
When the kidney detects a decrease in blood pressure or a reduction in sodium levels, it releases renin into the bloodstream. Renin then acts on a protein called angiotensinogen, converting it to angiotensin I. Angiotensin-converting enzyme (ACE) subsequently converts angiotensin I to angiotensin II, which is a potent vasoconstrictor that narrows blood vessels and increases blood pressure.
Additionally, angiotensin II stimulates the adrenal glands to release aldosterone, a hormone that promotes sodium reabsorption in the kidneys and increases water retention, further raising blood pressure.
Therefore, renin plays a critical role in maintaining proper blood pressure and electrolyte balance in the body."
Distal kidney tubules are the final segment of the renal tubule in the nephron of the kidney. The nephron is the basic unit of the kidney that filters blood and produces urine. After the filtrate leaves the glomerulus, it enters the proximal tubule where most of the reabsorption of water, electrolytes, and nutrients occurs.
The filtrate then moves into the loop of Henle, which is divided into a thin and thick descending limb and a thin and thick ascending limb. The loop of Henle helps to establish a concentration gradient in the medullary interstitium, allowing for the reabsorption of water in the collecting ducts.
The distal tubule is the last segment of the renal tubule before the filtrate enters the collecting duct. It is a relatively short structure that receives filtrate from the thick ascending limb of the loop of Henle. The distal tubule plays an important role in regulating electrolyte and water balance by actively transporting ions such as sodium, potassium, and chloride.
The distal tubule also contains specialized cells called principal cells and intercalated cells that are responsible for secreting or reabsorbing hydrogen and potassium ions to maintain acid-base balance. Additionally, the distal tubule is a site of action for several hormones, including aldosterone, which stimulates sodium reabsorption and potassium excretion, and vasopressin (antidiuretic hormone), which promotes water reabsorption in the collecting ducts.
The Loop of Henle, also known as the Henle's loop or nephron loop, is a hairpin-shaped structure in the nephrons of the mammalian kidney. It is a part of the renal tubule and plays a crucial role in concentrating urine and maintaining water-electrolyte balance in the body.
The Loop of Henle consists of two main segments: the thin descending limb, which dips into the medulla of the kidney, and the thick ascending limb, which returns to the cortex. The loop is responsible for creating a concentration gradient in the medullary interstitium, allowing for the reabsorption of water from the filtrate in the collecting ducts under the influence of antidiuretic hormone (ADH).
In summary, the Loop of Henle is a vital component of the kidney's nephron that facilitates urine concentration and helps regulate fluid balance in the body.
Arterioles are small branches of arteries that play a crucial role in regulating blood flow and blood pressure within the body's circulatory system. They are the smallest type of blood vessels that have muscular walls, which allow them to contract or dilate in response to various physiological signals.
Arterioles receive blood from upstream arteries and deliver it to downstream capillaries, where the exchange of oxygen, nutrients, and waste products occurs between the blood and surrounding tissues. The contraction of arteriolar muscles can reduce the diameter of these vessels, causing increased resistance to blood flow and leading to a rise in blood pressure upstream. Conversely, dilation of arterioles reduces resistance and allows for greater blood flow at a lower pressure.
The regulation of arteriolar tone is primarily controlled by the autonomic nervous system, local metabolic factors, and various hormones. This fine-tuning of arteriolar diameter enables the body to maintain adequate blood perfusion to vital organs while also controlling overall blood pressure and distribution.
A kidney, in medical terms, is one of two bean-shaped organs located in the lower back region of the body. They are essential for maintaining homeostasis within the body by performing several crucial functions such as:
1. Regulation of water and electrolyte balance: Kidneys help regulate the amount of water and various electrolytes like sodium, potassium, and calcium in the bloodstream to maintain a stable internal environment.
2. Excretion of waste products: They filter waste products from the blood, including urea (a byproduct of protein metabolism), creatinine (a breakdown product of muscle tissue), and other harmful substances that result from normal cellular functions or external sources like medications and toxins.
3. Endocrine function: Kidneys produce several hormones with important roles in the body, such as erythropoietin (stimulates red blood cell production), renin (regulates blood pressure), and calcitriol (activated form of vitamin D that helps regulate calcium homeostasis).
4. pH balance regulation: Kidneys maintain the proper acid-base balance in the body by excreting either hydrogen ions or bicarbonate ions, depending on whether the blood is too acidic or too alkaline.
5. Blood pressure control: The kidneys play a significant role in regulating blood pressure through the renin-angiotensin-aldosterone system (RAAS), which constricts blood vessels and promotes sodium and water retention to increase blood volume and, consequently, blood pressure.
Anatomically, each kidney is approximately 10-12 cm long, 5-7 cm wide, and 3 cm thick, with a weight of about 120-170 grams. They are surrounded by a protective layer of fat and connected to the urinary system through the renal pelvis, ureters, bladder, and urethra.
Kidney tubules are the structural and functional units of the kidney responsible for reabsorption, secretion, and excretion of various substances. They are part of the nephron, which is the basic unit of the kidney's filtration and reabsorption process.
There are three main types of kidney tubules:
1. Proximal tubule: This is the initial segment of the kidney tubule that receives the filtrate from the glomerulus. It is responsible for reabsorbing approximately 65% of the filtrate, including water, glucose, amino acids, and electrolytes.
2. Loop of Henle: This U-shaped segment of the tubule consists of a thin descending limb, a thin ascending limb, and a thick ascending limb. The loop of Henle helps to concentrate urine by creating an osmotic gradient that allows water to be reabsorbed in the collecting ducts.
3. Distal tubule: This is the final segment of the kidney tubule before it empties into the collecting duct. It is responsible for fine-tuning the concentration of electrolytes and pH balance in the urine by selectively reabsorbing or secreting substances such as sodium, potassium, chloride, and hydrogen ions.
Overall, kidney tubules play a critical role in maintaining fluid and electrolyte balance, regulating acid-base balance, and removing waste products from the body.
A kidney glomerulus is a functional unit in the nephron of the kidney. It is a tuft of capillaries enclosed within a structure called Bowman's capsule, which filters waste and excess fluids from the blood. The glomerulus receives blood from an afferent arteriole and drains into an efferent arteriole.
The process of filtration in the glomerulus is called ultrafiltration, where the pressure within the glomerular capillaries drives plasma fluid and small molecules (such as ions, glucose, amino acids, and waste products) through the filtration membrane into the Bowman's space. Larger molecules, like proteins and blood cells, are retained in the blood due to their larger size. The filtrate then continues down the nephron for further processing, eventually forming urine.
Angiotensin II is a potent vasoactive peptide hormone that plays a critical role in the renin-angiotensin-aldosterone system (RAAS), which is a crucial regulator of blood pressure and fluid balance in the body. It is formed from angiotensin I through the action of an enzyme called angiotensin-converting enzyme (ACE).
Angiotensin II has several physiological effects on various organs, including:
1. Vasoconstriction: Angiotensin II causes contraction of vascular smooth muscle, leading to an increase in peripheral vascular resistance and blood pressure.
2. Aldosterone release: Angiotensin II stimulates the adrenal glands to release aldosterone, a hormone that promotes sodium reabsorption and potassium excretion in the kidneys, thereby increasing water retention and blood volume.
3. Sympathetic nervous system activation: Angiotensin II activates the sympathetic nervous system, leading to increased heart rate and contractility, further contributing to an increase in blood pressure.
4. Thirst regulation: Angiotensin II stimulates the hypothalamus to increase thirst, promoting water intake and helping to maintain intravascular volume.
5. Cell growth and fibrosis: Angiotensin II has been implicated in various pathological processes, such as cell growth, proliferation, and fibrosis, which can contribute to the development of cardiovascular and renal diseases.
Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are two classes of medications commonly used in clinical practice to target the RAAS by blocking the formation or action of angiotensin II, respectively. These drugs have been shown to be effective in managing hypertension, heart failure, and chronic kidney disease.
The Golgi apparatus, also known as the Golgi complex or simply the Golgi, is a membrane-bound organelle found in the cytoplasm of most eukaryotic cells. It plays a crucial role in the processing, sorting, and packaging of proteins and lipids for transport to their final destinations within the cell or for secretion outside the cell.
The Golgi apparatus consists of a series of flattened, disc-shaped sacs called cisternae, which are stacked together in a parallel arrangement. These stacks are often interconnected by tubular structures called tubules or vesicles. The Golgi apparatus has two main faces: the cis face, which is closest to the endoplasmic reticulum (ER) and receives proteins and lipids directly from the ER; and the trans face, which is responsible for sorting and dispatching these molecules to their final destinations.
The Golgi apparatus performs several essential functions in the cell:
1. Protein processing: After proteins are synthesized in the ER, they are transported to the cis face of the Golgi apparatus, where they undergo various post-translational modifications, such as glycosylation (the addition of sugar molecules) and sulfation. These modifications help determine the protein's final structure, function, and targeting.
2. Lipid modification: The Golgi apparatus also modifies lipids by adding or removing different functional groups, which can influence their properties and localization within the cell.
3. Protein sorting and packaging: Once proteins and lipids have been processed, they are sorted and packaged into vesicles at the trans face of the Golgi apparatus. These vesicles then transport their cargo to various destinations, such as lysosomes, plasma membrane, or extracellular space.
4. Intracellular transport: The Golgi apparatus serves as a central hub for intracellular trafficking, coordinating the movement of vesicles and other transport carriers between different organelles and cellular compartments.
5. Cell-cell communication: Some proteins that are processed and packaged in the Golgi apparatus are destined for secretion, playing crucial roles in cell-cell communication and maintaining tissue homeostasis.
In summary, the Golgi apparatus is a vital organelle involved in various cellular processes, including post-translational modification, sorting, packaging, and intracellular transport of proteins and lipids. Its proper functioning is essential for maintaining cellular homeostasis and overall organismal health.
 Juxtaglomerular apparatus - Wikipedia
Juxtaglomerular apparatus - Wikipedia Juxtaglomerular-apparatus Definition & Meaning | YourDictionary
Juxtaglomerular-apparatus Definition & Meaning | YourDictionary Juxtaglomerular Apparatus
Juxtaglomerular Apparatus Hyperchloremic Acidosis: Practice Essentials, Etiology, Patient Education
Hyperchloremic Acidosis: Practice Essentials, Etiology, Patient Education Mir125b1 (microRNA 125b-1) - Rat Genome Database
Mir125b1 (microRNA 125b-1) - Rat Genome Database JCI Insight -
Inhibition of the renin-angiotensin system causes concentric hypertrophy of renal arterioles in mice and humans
JCI Insight -
Inhibition of the renin-angiotensin system causes concentric hypertrophy of renal arterioles in mice and humans Nitrite (JECFA Food Additives Series 50)
Nitrite (JECFA Food Additives Series 50) Primary Aldosteronism: Screening and Confirmatory Testing | myADLM.org
Primary Aldosteronism: Screening and Confirmatory Testing | myADLM.org DailyMed - CAPTOPRIL tablet
DailyMed - CAPTOPRIL tablet β-Adrenoceptors
β-Adrenoceptors 10/22/2020 - Swirlzcupcakes.com
10/22/2020 - Swirlzcupcakes.com SciELO - Brazil - Natural products inhibitors of the angiotensin converting enzyme (ACE): a review between 1980 - 2000 Natural...
SciELO - Brazil - Natural products inhibitors of the angiotensin converting enzyme (ACE): a review between 1980 - 2000 Natural... Flashcards - A&P 202 Study Guide Exam 4
Flashcards - A&P 202 Study Guide Exam 4![LOINC 100820-0 Renin [Mass/volume] in Plasma --3rd specimen post XXX challenge](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAASFBMVEVHcEwAnt4Cot////////////8AoN7g8fr///////8UpeBZuObD4/UlqOHR6ff0+/5JsuR/xuuZ0O623fM1reNmvOiu2fLn9PtK62mFAAAACnRSTlMAVf//l9cS3qgk43SAKwAAAKZJREFUGJUtj0mWxCAMQymZNMEDc8j9b9quVLTC31hPCsGVY1JNMYdX50brvWGcv/loVyVX3ZqefRv0qDao/8lbnvFW4auMHOKqpZAugM26xZDq943FOpwghXLdcrHc6ENgrA6owtC/PhMOktFmc0q9UPOTaPdmVgLppOamefo9D5oermB7/FNGZy5uoZAn/CEihiUMOd5y06MAa56fvx/x+qW89f8BsVYIw+NPTI8AAAAASUVORK5CYII=) LOINC 100820-0 Renin [Mass/volume] in Plasma --3rd specimen post XXX challenge
LOINC 100820-0 Renin [Mass/volume] in Plasma --3rd specimen post XXX challenge DeCS 2020 - June 23, 2020 version
DeCS 2020 - June 23, 2020 version Renin - Structure, Enzyme, Hormone, and FAQs
Renin - Structure, Enzyme, Hormone, and FAQs