Hypersplenism
Splenorenal Shunt, Surgical
Hypertension, Portal
Splenic Artery
Histiocytosis
Splenic Vein
Splenic Diseases
Portasystemic Shunt, Surgical
Embolization, Therapeutic
Esophageal and Gastric Varices
Lymphoproliferative syndrome with autoimmunity: A possible genetic basis for dominant expression of the clinical manifestations. (1/65)
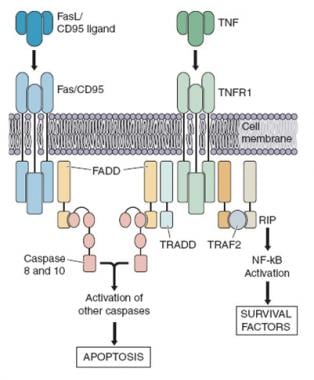
Fas (CD95/Apo-1) mutations were previously reported as the genetic defect responsible for human lymphoproliferative syndrome associated with autoimmune manifestations (also known as autoimmune lymphoproliferative syndrome or Canale-Smith syndrome). We have identified 14 new heterozygous Fas mutations. Analysis of patients and families allow us to further dissect this syndrome with regards to the relationship between Fas mutations, inheritance pattern, and phenotype as observed on long-term follow-up. In vitro studies show that lymphocytes from all Fas mutant carriers exhibit a Fas-antibody-induced apoptosis defect. However, among the 8 inherited mutations, 4 of 4 Fas missense mutations were associated with high clinical penetrance, whereas 3 of 4 mutations leading to a truncated Fas product were associated with variable clinical penetrance. This suggests that a second defect, in another yet undefined factor involved in apoptosis and/or lymphoproliferation control, is necessary to induce full clinical expression of the disease. These results also indicate that the currently available antibody-mediated in vitro apoptosis assay does not necessarily reflect the in vivo ability of abnormal Fas molecules to trigger lymphocyte death. In addition, we found that lymphoproliferative manifestations resolved with age, whereas immunological disorders [ie, hypergammaglobulinemia and detection of TcR alphabeta(+) CD4(-) CD8(-) lymphocytes] persisted. This observation suggests that Fas-mediated apoptosis plays a more important role in lymphocyte homeostasis in early childhood than later on in life. (+info)Thermophilic multidrug-resistant Campylobacter fetus infection with hypersplenism and histiocytic phagocytosis in a patient with acquired immunodeficiency syndrome. (2/65)
We present a case report of a patient who had acquired immunodeficiency syndrome (AIDS) and Campylobacter fetus infection with a number of unusual clinical and microbiological features. The patient had prominent gastrointestinal symptoms, splenic infarction, splenomegaly with hypersplenism, and hemophagocytic histiocytosis in the spleen and lymph nodes; the organism displayed growth on Campy-selective blood agar, thermotolerance, and resistance to quinolones, piperacillin/tazobactam, ceftazidime, and erythromycin. (+info)Recurrent portal hypertension after composite liver/small bowel transplantation. (3/65)
Late technical complications of composite liver/small bowel transplantation procedures are often complex and have not been well defined. Here we describe the unusual presentation and management of two cases of recurrent thrombocytopenia due to hypersplenism resulting from portacaval shunt stenosis. Both patients presented with portal hypertension late after composite liver/small bowel transplantation. One patient presented with recurrent bouts of upper gastrointestinal hemorrhage and was ultimately found to have a stenosis of her native portacaval shunt. After unsuccessful balloon dilatation of the anastomosis, a successful side-to-side distal splenorenal shunt was performed. The second patient presented with severe thrombocytopenia, the etiology of which was determined to be a short segment occlusion of the inferior vena cava between the native portacaval shunt and the piggyback outflow anastomosis of the liver graft. Total caval occlusion prevented balloon dilatation; the patient was relisted for transplantation but died of chronic rejection four months later. Recurrent portal hypertension is challenging in patients who have had combined liver/small bowel transplantation. Surgeons performing intestinal transplantation need to be increasingly aware of these possible late complications. (+info)Partial splenectomy in cystic fibrosis patients with hypersplenism. (4/65)
We report three cystic fibrosis (CF) patients with hypersplenism who underwent partial splenectomy. The postoperative course was uneventful in two patients; one patient developed a complication necessitating resection of the rest of the spleen. Haematological parameters improved and oesophageal varices regressed in all patients. On follow up, one patient showed a normal spleen, the other a normally functioning accessory spleen; the third patient again developed splenomegaly with hypersplenism. Partial splenectomy is a promising therapeutic option for CF patients with hypersplenism. (+info)Experimental study on the feasibility and safety of radiofrequency ablation for secondary splenomagely and hypersplenism. (5/65)
AIM: To assess the feasibility and safety of radiofrequency ablation (RFA) in treatment of secondary splenomagely and hypersplenism. METHODS: Sixteen healthy mongrel dogs were randomly divided into two groups, group I (n=4) and group II (n=12). Congestive splenomegaly was induced by ligation of splenic vein and its collateral branches in both groups. At the end of 3rd week postoperation, RFA in spleen was performed in group II via laparotomy, complications of RFA were observed, CT scan was performed and the spleens were obtained. The radiofrequency (RF) thermal lesions and histopathology of spleen were examined regularly. RESULTS: No complication or death was observed in both groups; CT revealed that the splenomegaly lasted over 2 months after ligation of splenic vein; the segmental RF lesions included hyperintense zone of coagulative necrosis and more extensive peripheral hypointense infarcted zone, the latter was called "bystander effect". The infarcted zone would be absorbed and subsequently disappeared in 4-6 weeks after RFA accompanied with shrinkage of the remnant spleen. The fundamental histopathological changes of splenic lesions caused by RF thermal energy included local coagulative necrosis, peripheral thrombotic infarction zone, subsequent tissue absorption and fibrosis in the zone of thrombotic infarction, the occlusion of vessels in remnant viable spleen, deposition of extensive fibrous protein, and disappearance of congestive splenic sinusoid - "splenic carnification". Those pathologic changes were underline of shrinkage of spleen. CONCLUSION: It is feasible and safe to perform RFA in spleen to treat experimental splenomegaly and hypersplenism. The RFA could be safely performed clinically via laparotomy or laparoscopic procedure while spleen was strictly separated from surrounding organs. (+info)Laparoscopic splenectomy: the latest technical evaluation. (6/65)
AIM: To introduce our latest innovation on technical manipulation of laparoscopic splenectomy. METHODS: Under general anesthesia and carbon dioxide (CO(2)) pneumoperitoneum, 86 cases of laparoscopic splenectomy (LS) were performed. The patients were placed in three different operative positions: 7 cases in the lithotomic position, 31 cases in the right recumbent position and 48 cases in the right lateral position. An ultrasonic scissors was used to dissect the pancreaticosplenic ligament, the splenocolicum ligament, lienorenal ligament and the lienophrenic ligament, respectively. Lastly, the gastrosplenic ligament and short gastric vessels were dissected. The splenic artery and vein were resected at splenic hilum with Endo-GIA. The impact of different operative positions, spleen size and other events during the operation were studied. RESULTS: The laparoscopic splenectomy was successfully performed on all 86 patients from August 1997 to August 2002. No operative complications, such as peritoneal cavity infection, massive bleeding after operation and adjacent organs injured were observed. There was no death related to the operation. The study showed that different operative positions could significantly influence the manipulation of LS. The right lateral position had more advantages than the lithotomic position and the right recumbent position in LS. CONCLUSION: Most cases of LS could be accomplished successfully when patients are placed in the right lateral position. The right lateral position has more advantages than the conventional supine approach by providing a more direct view of the splenic hilum as well as other important anatomies. Regardless of operation positions, the major axis of spleen exceeding 15 cm by B-ultrasound in vitro will surely increase the difficulties of LS and therefore prolong the duration of operation. LS is a safe and feasible modality for splenectomy. (+info)PROGRESSIVE MULTIFOCAL LEUCOENCEPHALOPATHY AND PRIMARY HYPERSPLENISM. WITH A NOTE ON THE ASSOCIATION BETWEEN DISEASE OF THE RETICULOENDOTHELIAL SYSTEM AND PROGRESSIVE MULTIFOCAL LEUCOENCEPHALOPATHY. (7/65)
A patient with progressive multifocal leucoencephalopathy was found to have primary hypersplenism, a benign disorder of the reticuloendothelial system. He failed to respond to conventional doses of corticosteroids. The clinical and pathological manifestations of his illness are described, and the development of the histopathological changes in the nervous system is discussed. Consideration of available data on progressive multifocal leucoencephalopathy reveals a striking association with disease of the reticuloendothelial system, the significance of which is discussed in relation to aetiology and treatment. (+info)Percutaneous splenic embolization of the splenic artery in the treatment of hypersplenism. (8/65)
Percutaneous splenectomy was performed in 6 patients with hypersplenism. Peripheral blood cell counts improved in 5 of the patients. The authors review the indications, technique and complications of percutaneous splenic embolization. It is concluded that medical splenectomy is an effective method particularly to alleviate symptoms of hypersplenism. (+info)Hypersplenism is a condition characterized by an enlarged spleen (splenomegaly) that results in the abnormal removal or destruction of various blood components, such as red blood cells (RBCs), white blood cells (WBCs), and platelets. This leads to peripheral blood cytopenias, which means there is a decrease in one or more types of blood cells in the circulation.
The spleen becomes overactive in hypersplenism, and its increased removal of blood cells can be secondary to various underlying disorders, such as:
1. Infections: e.g., bacterial endocarditis, malaria, or EBV (Epstein-Barr virus) infection
2. Hematologic diseases: e.g., hemolytic anemias, thalassemia, leukemias, lymphomas, or myeloproliferative neoplasms
3. Cirrhosis and portal hypertension
4. Vascular disorders: e.g., splenic vein thrombosis or congestive splenomegaly
5. Storage diseases: e.g., Gaucher's disease, Niemann-Pick disease, or Hurler syndrome
Symptoms of hypersplenism may include fatigue, weakness, pallor (in case of anemia), infections (due to neutropenia), and easy bruising or bleeding (due to thrombocytopenia). Treatment for hypersplenism involves addressing the underlying cause. In some cases, splenectomy (surgical removal of the spleen) may be considered if the benefits outweigh the risks.
A splenectomy is a surgical procedure in which the spleen is removed from the body. The spleen is an organ located in the upper left quadrant of the abdomen, near the stomach and behind the ribs. It plays several important roles in the body, including fighting certain types of infections, removing old or damaged red blood cells from the circulation, and storing platelets and white blood cells.
There are several reasons why a splenectomy may be necessary, including:
* Trauma to the spleen that cannot be repaired
* Certain types of cancer, such as Hodgkin's lymphoma or non-Hodgkin's lymphoma
* Sickle cell disease, which can cause the spleen to enlarge and become damaged
* A ruptured spleen, which can be life-threatening if not treated promptly
* Certain blood disorders, such as idiopathic thrombocytopenic purpura (ITP) or hemolytic anemia
A splenectomy is typically performed under general anesthesia and may be done using open surgery or laparoscopically. After the spleen is removed, the incision(s) are closed with sutures or staples. Recovery time varies depending on the individual and the type of surgery performed, but most people are able to return to their normal activities within a few weeks.
It's important to note that following a splenectomy, individuals may be at increased risk for certain types of infections, so it's recommended that they receive vaccinations to help protect against these infections. They should also seek medical attention promptly if they develop fever, chills, or other signs of infection.
A splenorenal shunt is a surgical procedure that creates a connection between the spleen and the left kidney vein (renal vein). This type of shunt is typically performed to reroute the flow of blood from the spleen when there is an obstruction in the portal vein, which carries blood from the gastrointestinal tract, liver, and spleen. The procedure helps to alleviate portal hypertension (high blood pressure in the portal vein) and its complications, such as variceal bleeding (bleeding from enlarged veins in the esophagus or stomach).
During a surgical splenorenal shunt procedure, the surgeon will make an incision in the left flank region to access both the spleen and the left renal vein. The splenic vein is then divided, and one end is connected to the left renal vein using a synthetic graft or a portion of the patient's own blood vessel (autograft). This connection allows the blood from the spleen to bypass the obstructed portal vein and flow directly into the systemic venous circulation.
It is important to note that splenorenal shunts have been largely replaced by transjugular intrahepatic portosystemic shunts (TIPS) as the first-line treatment for managing portal hypertension due to their lower invasiveness and fewer complications. However, surgical splenorenal shunts may still be considered in specific cases where TIPS is not feasible or has failed.
Portal hypertension is a medical condition characterized by an increased pressure in the portal vein, which is the large blood vessel that carries blood from the intestines, spleen, and pancreas to the liver. Normal portal venous pressure is approximately 5-10 mmHg. Portal hypertension is defined as a portal venous pressure greater than 10 mmHg.
The most common cause of portal hypertension is cirrhosis of the liver, which leads to scarring and narrowing of the small blood vessels in the liver, resulting in increased resistance to blood flow. Other causes include blood clots in the portal vein, inflammation of the liver or bile ducts, and invasive tumors that block the flow of blood through the liver.
Portal hypertension can lead to a number of complications, including the development of abnormal blood vessels (varices) in the esophagus, stomach, and intestines, which are prone to bleeding. Ascites, or the accumulation of fluid in the abdominal cavity, is another common complication of portal hypertension. Other potential complications include encephalopathy, which is a condition characterized by confusion, disorientation, and other neurological symptoms, and an increased risk of bacterial infections.
Treatment of portal hypertension depends on the underlying cause and the severity of the condition. Medications to reduce pressure in the portal vein, such as beta blockers or nitrates, may be used. Endoscopic procedures to band or inject varices can help prevent bleeding. In severe cases, surgery or liver transplantation may be necessary.
Splenomegaly is a medical term that refers to an enlargement or expansion of the spleen beyond its normal size. The spleen is a vital organ located in the upper left quadrant of the abdomen, behind the stomach and below the diaphragm. It plays a crucial role in filtering the blood, fighting infections, and storing red and white blood cells and platelets.
Splenomegaly can occur due to various underlying medical conditions, including infections, liver diseases, blood disorders, cancer, and inflammatory diseases. The enlarged spleen may put pressure on surrounding organs, causing discomfort or pain in the abdomen, and it may also lead to a decrease in red and white blood cells and platelets, increasing the risk of anemia, infections, and bleeding.
The diagnosis of splenomegaly typically involves a physical examination, medical history, and imaging tests such as ultrasound, CT scan, or MRI. Treatment depends on the underlying cause and may include medications, surgery, or other interventions to manage the underlying condition.
The splenic artery is the largest branch of the celiac trunk, which arises from the abdominal aorta. It supplies blood to the spleen and several other organs in the upper left part of the abdomen. The splenic artery divides into several branches that ultimately form a network of capillaries within the spleen. These capillaries converge to form the main venous outflow, the splenic vein, which drains into the hepatic portal vein.
The splenic artery is a vital structure in the human body, and any damage or blockage can lead to serious complications, including splenic infarction (reduced blood flow to the spleen) or splenic rupture (a surgical emergency that can be life-threatening).
Histiocytosis is a term used to describe a group of rare disorders characterized by an abnormal increase in the number of histiocytes, which are a type of white blood cell that helps fight infection and helps in healing processes. These disorders can affect various organs and tissues in the body, leading to different symptoms and severity.
There are several types of histiocytosis, including Langerhans cell histiocytosis (LCH), Erdheim-Chester disease (ECD), and hemophagocytic lymphohistiocytosis (HLH). Each type has its own specific features and diagnostic criteria.
For example, LCH is characterized by the abnormal accumulation of Langerhans cells, a type of histiocyte found in the skin and mucous membranes. These cells can form tumors or lesions in various organs, such as the bones, lungs, liver, and skin.
HLH, on the other hand, is a life-threatening condition that occurs when there is an overactive immune response leading to excessive activation of histiocytes and other immune cells. This can result in fever, enlargement of the liver and spleen, and decreased blood cell counts.
The exact cause of histiocytosis is not fully understood, but it is believed to involve genetic mutations that lead to uncontrolled proliferation and accumulation of histiocytes. Treatment for histiocytosis depends on the type and severity of the disorder and may include chemotherapy, radiation therapy, immunosuppressive drugs, or stem cell transplantation.
The splenic vein is a large, thin-walled vein that carries oxygenated blood from the spleen and pancreas to the liver. It is formed by the union of several smaller veins that drain the upper part of the stomach, the pancreas, and the left side of the colon (splenic flexure). The splenic vein runs along the top border of the pancreas and merges with the superior mesenteric vein to form the portal vein. This venous system allows for the filtration and detoxification of blood by the liver before it is distributed to the rest of the body.
Splenic diseases refer to a range of medical conditions that affect the structure, function, or health of the spleen. The spleen is an organ located in the upper left quadrant of the abdomen, which plays a vital role in filtering the blood and fighting infections. Some common splenic diseases include:
1. Splenomegaly: Enlargement of the spleen due to various causes such as infections, liver disease, blood disorders, or cancer.
2. Hypersplenism: Overactivity of the spleen leading to excessive removal of blood cells from circulation, causing anemia, leukopenia, or thrombocytopenia.
3. Splenic infarction: Partial or complete blockage of the splenic artery or its branches, resulting in tissue death and potential organ dysfunction.
4. Splenic rupture: Traumatic or spontaneous tearing of the spleen capsule, causing internal bleeding and potentially life-threatening conditions.
5. Infections: Bacterial (e.g., sepsis, tuberculosis), viral (e.g., mononucleosis, cytomegalovirus), fungal (e.g., histoplasmosis), or parasitic (e.g., malaria) infections can affect the spleen and cause various symptoms.
6. Hematologic disorders: Conditions such as sickle cell disease, thalassemia, hemolytic anemias, lymphomas, leukemias, or myeloproliferative neoplasms can involve the spleen and lead to its enlargement or dysfunction.
7. Autoimmune diseases: Conditions like rheumatoid arthritis, systemic lupus erythematosus, or vasculitis can affect the spleen and cause various symptoms.
8. Cancers: Primary (e.g., splenic tumors) or secondary (e.g., metastatic cancer from other organs) malignancies can involve the spleen and lead to its enlargement, dysfunction, or rupture.
9. Vascular abnormalities: Conditions such as portal hypertension, Budd-Chiari syndrome, or splenic vein thrombosis can affect the spleen and cause various symptoms.
10. Trauma: Accidental or intentional injuries to the spleen can lead to bleeding, infection, or organ dysfunction.
A platelet count is a laboratory test that measures the number of platelets, also known as thrombocytes, in a sample of blood. Platelets are small, colorless cell fragments that circulate in the blood and play a crucial role in blood clotting. They help to stop bleeding by sticking together to form a plug at the site of an injured blood vessel.
A normal platelet count ranges from 150,000 to 450,000 platelets per microliter (µL) of blood. A lower than normal platelet count is called thrombocytopenia, while a higher than normal platelet count is known as thrombocytosis.
Abnormal platelet counts can be a sign of various medical conditions, including bleeding disorders, infections, certain medications, and some types of cancer. It is important to consult with a healthcare provider if you have any concerns about your platelet count or if you experience symptoms such as easy bruising, prolonged bleeding, or excessive menstrual flow.
A portosystemic shunt is a surgical procedure that creates a connection between the portal vein (the blood vessel that carries blood from the digestive organs to the liver) and another systemic vein (a vein that carries blood away from the liver). This procedure is typically performed in animals, particularly dogs, to treat conditions such as portal hypertension or liver disease.
In a surgical portosystemic shunt, the surgeon creates a connection between the portal vein and a systemic vein, allowing blood from the digestive organs to bypass the liver. This can help to reduce the pressure in the portal vein and improve blood flow to the liver. The specific type of shunt created and the surgical approach used may vary depending on the individual patient's needs and the surgeon's preference.
It is important to note that while a surgical portosystemic shunt can be an effective treatment for certain conditions, it is not without risks and potential complications. As with any surgical procedure, there is always a risk of infection, bleeding, or other complications. Additionally, the creation of a portosystemic shunt can have long-term effects on the liver and overall health of the patient. It is important for pet owners to carefully consider the risks and benefits of this procedure and to discuss any questions or concerns they may have with their veterinarian.
Therapeutic embolization is a medical procedure that involves intentionally blocking or obstructing blood vessels to stop excessive bleeding or block the flow of blood to a tumor or abnormal tissue. This is typically accomplished by injecting small particles, such as microspheres or coils, into the targeted blood vessel through a catheter, which is inserted into a larger blood vessel and guided to the desired location using imaging techniques like X-ray or CT scanning. The goal of therapeutic embolization is to reduce the size of a tumor, control bleeding, or block off abnormal blood vessels that are causing problems.
Esophageal varices and gastric varices are abnormal, enlarged veins in the lower part of the esophagus (the tube that connects the throat to the stomach) and in the stomach lining, respectively. They occur as a result of increased pressure in the portal vein, which is the large blood vessel that carries blood from the digestive organs to the liver. This condition is known as portal hypertension.
Esophageal varices are more common than gastric varices and tend to be more symptomatic. They can cause bleeding, which can be life-threatening if not treated promptly. Gastric varices may also bleed, but they are often asymptomatic until they rupture.
The most common causes of esophageal and gastric varices are cirrhosis (scarring of the liver) and portal hypertension due to other liver diseases such as schistosomiasis or Budd-Chiari syndrome. Treatment options for esophageal and gastric varices include medications to reduce bleeding, endoscopic therapies to treat active bleeding or prevent recurrent bleeding, and surgical procedures to relieve portal hypertension.
Splenic neoplasms refer to abnormal growths or tumors in the spleen, which can be benign (non-cancerous) or malignant (cancerous). These growths can arise from various cell types present within the spleen, including hematopoietic cells (red and white blood cells, platelets), stromal cells (supporting tissue), or lymphoid cells (part of the immune system).
There are several types of splenic neoplasms:
1. Hematologic malignancies: These are cancers that affect the blood and bone marrow, such as leukemias, lymphomas, and multiple myeloma. They often involve the spleen, causing enlargement (splenomegaly) and neoplastic infiltration of splenic tissue.
2. Primary splenic tumors: These are rare and include benign lesions like hemangiomas, lymphangiomas, and hamartomas, as well as malignant tumors such as angiosarcoma, littoral cell angiosarcoma, and primary splenic lymphoma.
3. Metastatic splenic tumors: These occur when cancer cells from other primary sites spread (metastasize) to the spleen. Common sources of metastasis include lung, breast, colon, and ovarian cancers, as well as melanomas and sarcomas.
Symptoms of splenic neoplasms may vary depending on the type and extent of the disease but often include abdominal pain or discomfort, fatigue, weight loss, and anemia. Diagnosis typically involves imaging studies (such as ultrasound, CT, or MRI scans) and sometimes requires a biopsy for confirmation. Treatment options depend on the type of neoplasm and may include surgery, chemotherapy, radiation therapy, targeted therapy, or immunotherapy.
Thrombocytopenia is a medical condition characterized by an abnormally low platelet count (thrombocytes) in the blood. Platelets are small cell fragments that play a crucial role in blood clotting, helping to stop bleeding when a blood vessel is damaged. A healthy adult typically has a platelet count between 150,000 and 450,000 platelets per microliter of blood. Thrombocytopenia is usually diagnosed when the platelet count falls below 150,000 platelets/µL.
Thrombocytopenia can be classified into three main categories based on its underlying cause:
1. Immune thrombocytopenia (ITP): An autoimmune disorder where the immune system mistakenly attacks and destroys its own platelets, leading to a decreased platelet count. ITP can be further divided into primary or secondary forms, depending on whether it occurs alone or as a result of another medical condition or medication.
2. Decreased production: Thrombocytopenia can occur when there is insufficient production of platelets in the bone marrow due to various causes, such as viral infections, chemotherapy, radiation therapy, leukemia, aplastic anemia, or vitamin B12 or folate deficiency.
3. Increased destruction or consumption: Thrombocytopenia can also result from increased platelet destruction or consumption due to conditions like disseminated intravascular coagulation (DIC), thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), or severe bacterial infections.
Symptoms of thrombocytopenia may include easy bruising, prolonged bleeding from cuts, spontaneous nosebleeds, bleeding gums, blood in urine or stools, and skin rashes like petechiae (small red or purple spots) or purpura (larger patches). The severity of symptoms can vary depending on the degree of thrombocytopenia and the presence of any underlying conditions. Treatment for thrombocytopenia depends on the cause and may include medications, transfusions, or addressing the underlying condition.
The portal vein is the large venous trunk that carries blood from the gastrointestinal tract, spleen, pancreas, and gallbladder to the liver. It is formed by the union of the superior mesenteric vein (draining the small intestine and a portion of the large intestine) and the splenic vein (draining the spleen and pancreas). The portal vein then divides into right and left branches within the liver, where the blood flows through the sinusoids and gets enriched with oxygen and nutrients before being drained by the hepatic veins into the inferior vena cava. This unique arrangement allows the liver to process and detoxify the absorbed nutrients, remove waste products, and regulate metabolic homeostasis.
 Hemolysis
Hemolysis Hypersplenism: MedlinePlus Medical Encyclopedia
Hypersplenism: MedlinePlus Medical Encyclopedia Clinical Trials : Hypersplenism
Clinical Trials : Hypersplenism Can Hypersplenism cause leukopenia? - Allclearmister.com
Can Hypersplenism cause leukopenia? - Allclearmister.com Hypersplenism - Hematology and Oncology - MSD Manual Professional Edition
Hypersplenism - Hematology and Oncology - MSD Manual Professional Edition Primary Biliary Cirrhosis & Cholangitis (PBC): Symptoms, Causes & Diagnosis
Primary Biliary Cirrhosis & Cholangitis (PBC): Symptoms, Causes & Diagnosis Imaging of Liver Transplantation Complications: Practice Essentials, Complications, Postoperative Fluid Collections
Imaging of Liver Transplantation Complications: Practice Essentials, Complications, Postoperative Fluid Collections Risk factors for portal vein system thrombosis after partial splenic embolisation in cirrhotic patients with hypersplenism. |...
Risk factors for portal vein system thrombosis after partial splenic embolisation in cirrhotic patients with hypersplenism. |... Thin blood: Causes, symptoms, and treatment
Thin blood: Causes, symptoms, and treatment Distal Splenorenal Shunt: What It Is, Procedure & Complications
Distal Splenorenal Shunt: What It Is, Procedure & Complications Thrombocytopenia Causes
Thrombocytopenia Causes Thieme E-Journals - Digestive Disease Interventions / Abstract
Thieme E-Journals - Digestive Disease Interventions / Abstract SciELO - Brazil - Brazilian Thalassemia Association protocol for iron
chelation therapy in patients under...
SciELO - Brazil - Brazilian Thalassemia Association protocol for iron
chelation therapy in patients under... Lymphocytopenia differential diagnosis - wikidoc
Lymphocytopenia differential diagnosis - wikidoc Partial Splenic Embolization with Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma Accompanied by...
Partial Splenic Embolization with Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma Accompanied by... Hematology - 9780323733885
Hematology - 9780323733885 FR901228 in Treating Patients With Relapsed or Refractory Non-Hodgkin's Lymphoma
FR901228 in Treating Patients With Relapsed or Refractory Non-Hodgkin's Lymphoma FDA approved L-glutamine powder for the treatment of sickle cell disease | FDA
FDA approved L-glutamine powder for the treatment of sickle cell disease | FDA Transfusion Management of Beta (β) Thalassemia: Initiating Regular Transfusions | CDC
Transfusion Management of Beta (β) Thalassemia: Initiating Regular Transfusions | CDC Lymphoma in Ferrets (Mustela putorius furo) - WSAVA2009 - VIN
Lymphoma in Ferrets (Mustela putorius furo) - WSAVA2009 - VIN Consensus guidelines for the management of adult immune thrombocytopenia in Australia and New Zealand | The Medical Journal of...
Consensus guidelines for the management of adult immune thrombocytopenia in Australia and New Zealand | The Medical Journal of... PRIME PubMed | Patterns of pancytopenia patients in a general medical ward and a proposed diagnostic approach
PRIME PubMed | Patterns of pancytopenia patients in a general medical ward and a proposed diagnostic approach Frontiers | Anti-complement Treatment for Paroxysmal Nocturnal Hemoglobinuria: Time for Proximal Complement Inhibition? A...
Frontiers | Anti-complement Treatment for Paroxysmal Nocturnal Hemoglobinuria: Time for Proximal Complement Inhibition? A...