Colitis, Ulcerative
Proctocolectomy, Restorative
Ileostomy
Colonic Diseases
Laparoscopy
Diverticulitis, Colonic
Adenomatous Polyposis Coli
Colonic Pouches
Sigmoid Diseases
Megacolon, Toxic
Anastomosis, Surgical
Ileum
Pouchitis
Colon, Transverse
Megacolon
Postoperative Complications
Gastrointestinal Agents
Emergency Treatment
Emergencies
Diverticulosis, Colonic
Intestinal Polyps
Gardner Syndrome
Crohn Disease
Intestinal Obstruction
Rectal Diseases
Colon
Constipation
Enterocolitis, Pseudomembranous
Flatulence
Fibromatosis, Abdominal
Anal Canal
Colorectal Surgery
Ileus
Clostridium difficile
Surgical Stapling
Pirinitramide
Cholangitis, Sclerosing
Treatment Outcome
Retrospective Studies
Colon, Ascending
Colonic Pseudo-Obstruction
Sodium Acetate
Intestinal Polyposis
Surgical Procedures, Elective
Ischaemic enterocolitis complicating idiopathic dysautonomia. (1/863)
A previously fit 23 year old adult male who presented with a sudden onset of profound autonomic neuropathy, for which no cause could be found, is described. The patient subsequently developed ischaemic enterocolitis that ultimately necessitated colectomy and subtotal enterectomy. Potential neural and humoral mechanisms are discussed. (+info)Laparoscopic-assisted colectomy: a comparison of dissection techniques. (2/863)
BACKGROUND AND OBJECTIVES: Mobilization of the colon and dissection of the mesentery are difficult laparoscopic techniques. Traditional methods have been used for this dissection, but often with great difficulty. The ultrasonically activated shears, when introduced in 1993, had the possibility to make this dissection less technically difficult. This is a retrospective review of the use of these shears for these techniques during laparoscopic-assisted colectomy. MATERIALS AND METHODS: Eighty-five patients underwent a laparoscopic-assisted right hemicolectomy or sigmoid resection. Colon mobilization and mesenteric dissection were completed intracorporeally. Complications, operative time, estimated blood loss, and length of stay were compared for resections completed with and without the ultrasonically activated shears. RESULTS: Thirty-six patients had laparoscopic-assisted colectomy without the shears, and 49 patients had the procedure with the shears. There were no complications due to the ultrasonic energy. Use of the shears resulted in shorter operative times (170 min. vs. 187 min., p=0.1989), similar median blood loss (98 mL vs. 95 mL, p=0.7620), and shorter lengths of stay (4.3 days vs. 6.9 days, p=0.0018). CONCLUSIONS: The ultrasonically activated shears are safe and effective for colon mobilization and mesenteric division. The use of the shears may result in shorter operative times and shorter lengths of stay. (+info)Laparoscopic colon surgery for benign disease: a comparison to open surgery. (3/863)
BACKGROUNDS AND OBJECTIVES: There remains a debate in the literature about the advisability of laparoscopic surgery for malignant disease of the colon. Current prospective studies will hopefully answer this question. However, for benign diseases of the colon, we believe laparoscopic surgery offers many advantages including decreased postoperative pain, early discharge from the hospital, and early return to normal activities. We retrospectively reviewed our experience with laparoscopic colectomies for benign disease to see whether these procedures could be done safely and if the proposed advantages could be realized. METHODS: Thirty-eight laparoscopic colon resections performed for benign disease were compared to 39 open colon resections with respect to operating times, length of hospital stay, estimated blood loss, days until first postoperative bowel movement, and complications. RESULTS: The laparoscopic colon resection group had decreased length of stay, less blood loss, earlier return of bowel function, and an equivalent number of complications. Laparoscopic cases did take an average of 24 minutes longer. CONCLUSION: The use of laparoscopic colon surgery for benign disease not only affords the patient the advantage of the laparoscopic approach, but also allows the surgeon to gain experience while awaiting the results of ongoing trials for laparoscopic colon surgery in malignant disease. (+info)Transmesenteric hernia after laparoscopic-assisted sigmoid colectomy. (4/863)
BACKGROUND AND OBJECTIVES: Laparoscopic-assisted surgery has been applied for a variety of colonic surgery. The objective of this paper is to demonstrate a possible and avoidable complication of laparoscopic colonic surgery. CASE PRESENTATION: A 47-year-old woman underwent gasless laparoscopic-assisted sigmoid colectomy. On the 20th postoperative day, she developed bowel obstruction. Decompression with a long tube failed to resolve the bowel obstruction. Open laparotomy was performed. Abdominal exploration revealed a loop of the small bowel incarcerated in the mesenteric defect caused by the previous operation. Adhesiolysis was performed, and the postoperative course was uneventful. DISCUSSION: Despite technical difficulty, complete closure of the mesentery after bowel resection is strongly recommended for prevention of transmesenteric incarcerated hernia after laparoscopic surgery. (+info)Changes in plasma potassium concentration during carbon dioxide pneumoperitoneum. (5/863)
Hyperkalaemia with ECG changes had been noted during prolonged carbon dioxide pneumoperitoneum in pigs. We have compared plasma potassium concentrations during surgery in 11 patients allocated randomly to undergo either laparoscopic or open appendectomy and in another 17 patients allocated randomly to either carbon dioxide pneumoperitoneum or abdominal wall lifting for laparoscopic colectomy. Despite an increasing metabolic acidosis, prolonged carbon dioxide pneumoperitoneum resulted in only a slight increase in plasma potassium concentrations, which was both statistically and clinically insignificant. Thus hyperkalaemia is unlikely to develop in patients with normal renal function undergoing carbon dioxide pneumoperitoneum for laparoscopic surgery. (+info)External beam radiotherapy for pelvic node recurrence after curative resection of colon cancer: report of a case. (6/863)
The role of radiotherapy in locally advanced or recurrent colon cancer has not yet been determined. A 59-year-old man undergoing curative resection for advanced descending colon cancer had pelvic lymph node metastasis detected by computed tomography 5 months postoperatively. Intravenous chemotherapy using 5-fluorouracil and CDDP was repeated bimonthly for 7 months; however, his condition deteriorated progressively. External beam radiotherapy (50 Gy) was started thereafter. His serum carcinoembryonic antigen level decreased promptly and abdominal computed tomography showed apparent shrinkage of the metastatic pelvic node with calcification. The patient maintained a partial response for at least 12 months. Radiotherapy has a more crucial role in the treatment of a subgroup of recurrent colorectal tumors. (+info)A case of amyloid goiter secondary to Crohn's disease. (7/863)
We herewith report a case of amyloid goiter secondary to Crohn's disease. The patient had been diagnosed as having Crohn's disease at the age of 15, and underwent right hemicolectomy at age 20. When he was 26 years old he complained of swelling of the anterior neck. Both TSH and thyroid hormones were within the normal range, and anti-thyroglobulin and anti-microsomal antibodies were negative. Only thyroglobulin was noticeably above the normal range. During the next year his goiter enlarged further and because he had a feeling of pressure he underwent total thyroidectomy. The presence of amyloid A protein in his surgical specimen led to the diagnosis of amyloid goiter. Although most cases of secondary amyloidosis are known to develop in neoplasms or chronic inflammatory diseases, our patient had no illness other than Crohn's disease. Perusal of literature revealed that Crohn's disease is rarely a cause of amyloid goiter. (+info)The changes of ventilatory parameters in laparoscopic colecystectomy. (8/863)
We investigated the ventilatory changes in healthy patients without cardiopulmonary pathology during elective laparoscopic cholecystectomy in the head-up position. During surgery, intraabdominal pressure was maintained at 15 mmHg by a CO2 insufflator, and minute ventilation was controlled with a constant tidal volume and fixed respiratory rate. PETCO2 was monitored continuously and recorded every minute. Basic hemodynamic and ventilatory parameters were measured before anesthesia; after induction of anesthesia; at 5 min, 10 min and 30 min after peritoneal insufflation; and 5 min and 10 min after exsufflation. Arterial blood samples were obtained 3 times to calculate D(a-A)CO2, VD/VT, and Vco2. The latent period of PETCO2 change was 2.9 min, the ascending period was 12.6 min, and the descending period was 12.2 min. During the 71.5 min of pneumoperitoneum, V(I), VE, peak and plateau Paw increased, while Cdyn decreased significantly. Peritoneal insufflation or exsufflation also resulted in a significant change of D(a-A)CO2, D(a-A)O2, and Vco2. The anesthesiologist must be aware of both hemodynamic and ventilatory changes and must be ready to respond promptly and adequately. (+info)A colectomy is a surgical procedure in which all or part of the large intestine (colon) is removed. This surgery may be performed to treat or prevent various medical conditions, including colon cancer, inflammatory bowel disease, diverticulitis, and severe obstructions or injuries of the colon.
There are several types of colectomies, depending on how much of the colon is removed:
* Total colectomy: Removal of the entire colon.
* Partial colectomy: Removal of a portion of the colon.
* Hemicolectomy: Removal of one half of the colon.
* Sigmoidectomy: Removal of the sigmoid colon, which is the part of the colon that is closest to the rectum.
After the affected portion of the colon is removed, the remaining ends of the intestine are reconnected, allowing stool to pass through the digestive system as usual. In some cases, a temporary or permanent colostomy may be necessary, in which a surgical opening (stoma) is created in the abdominal wall and the end of the colon is attached to it, allowing stool to be collected in a pouch outside the body.
Colectomies are major surgeries that require general anesthesia and hospitalization. The recovery time can vary depending on the type of colectomy performed and the individual's overall health, but typically ranges from several weeks to a few months. Complications of colectomy may include bleeding, infection, leakage from the surgical site, bowel obstruction, and changes in bowel habits or function.
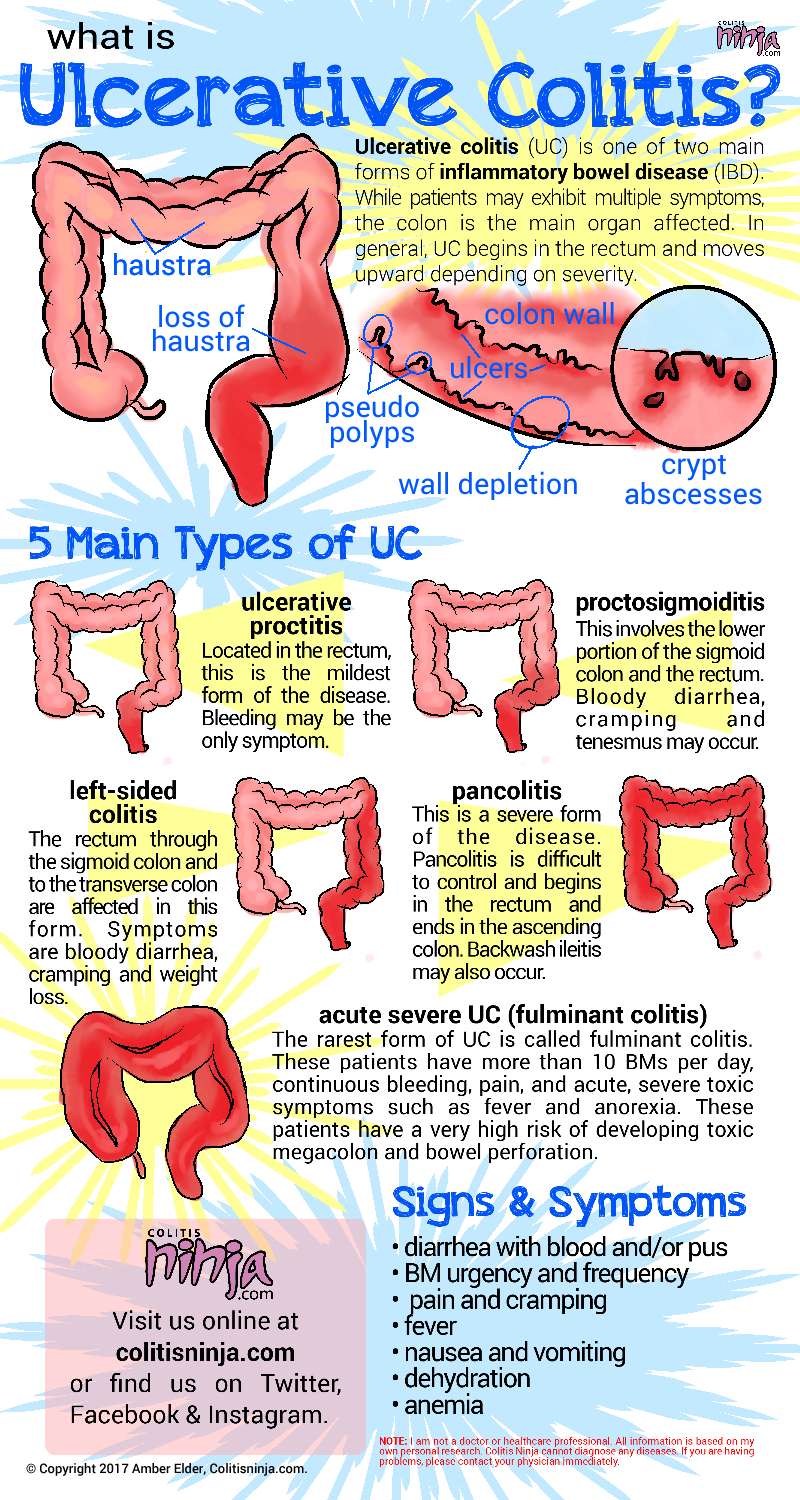
Ulcerative colitis is a type of inflammatory bowel disease (IBD) that affects the lining of the large intestine (colon) and rectum. In ulcerative colitis, the lining of the colon becomes inflamed and develops ulcers or open sores that produce pus and mucous. The symptoms of ulcerative colitis include diarrhea, abdominal pain, and rectal bleeding.
The exact cause of ulcerative colitis is not known, but it is thought to be related to an abnormal immune response in which the body's immune system attacks the cells in the digestive tract. The inflammation can be triggered by environmental factors such as diet, stress, and infections.
Ulcerative colitis is a chronic condition that can cause symptoms ranging from mild to severe. It can also lead to complications such as anemia, malnutrition, and colon cancer. There is no cure for ulcerative colitis, but treatment options such as medications, lifestyle changes, and surgery can help manage the symptoms and prevent complications.
Restorative proctocolectomy, also known as ileal pouch-anal anastomosis (IPAA), is a surgical procedure used to treat ulcerative colitis and familial adenomatous polyposis. This procedure involves the removal of the colon, rectum, and anal canal while preserving the sphincter muscles that control fecal continence.
After removing the diseased tissues, the surgeon creates a pouch from the end of the small intestine (ileum) and attaches it to the anus, restoring the continuity of the gastrointestinal tract. The pouch serves as a reservoir for stool, allowing for more normal bowel movements compared to having a permanent ileostomy.
Restorative proctocolectomy can be performed in one or two stages, depending on the patient's condition and the surgeon's preference. In the two-stage procedure, an initial total colectomy with ileostomy is performed, followed by the creation of the pouch and closure of the ileostomy in a second operation. The single-stage procedure involves removing the colon, creating the pouch, and performing the anastomosis in one surgical setting.
While restorative proctocolectomy significantly improves quality of life for many patients with ulcerative colitis and familial adenomatous polyposis, potential complications include pouchitis (inflammation of the ileal pouch), anastomotic leakage, small bowel obstruction, and pelvic sepsis. Regular follow-up care is essential to monitor for these and other potential issues.
An ileostomy is a surgical procedure in which the end of the small intestine, called the ileum, is brought through an opening in the abdominal wall (stoma) to create a path for waste material to leave the body. This procedure is typically performed when there is damage or removal of the colon, rectum, or anal canal due to conditions such as inflammatory bowel disease (Crohn's disease or ulcerative colitis), cancer, or trauma.
After an ileostomy, waste material from the small intestine exits the body through the stoma and collects in a pouch worn outside the body. The patient needs to empty the pouch regularly, typically every few hours, as the output is liquid or semi-liquid. Ileostomies can be temporary or permanent, depending on the underlying condition and the planned course of treatment. Proper care and management of the stoma and pouch are essential for maintaining good health and quality of life after an ileostomy.
Colonic diseases refer to a group of medical conditions that affect the colon, also known as the large intestine or large bowel. The colon is the final segment of the digestive system, responsible for absorbing water and electrolytes, and storing and eliminating waste products.
Some common colonic diseases include:
1. Inflammatory bowel disease (IBD): This includes conditions such as Crohn's disease and ulcerative colitis, which cause inflammation and irritation in the lining of the digestive tract.
2. Diverticular disease: This occurs when small pouches called diverticula form in the walls of the colon, leading to symptoms such as abdominal pain, bloating, and changes in bowel movements.
3. Colorectal cancer: This is a type of cancer that develops in the colon or rectum, often starting as benign polyps that grow and become malignant over time.
4. Irritable bowel syndrome (IBS): This is a functional gastrointestinal disorder characterized by abdominal pain, bloating, and changes in bowel movements, but without any underlying structural or inflammatory causes.
5. Constipation: This is a common condition characterized by infrequent bowel movements, difficulty passing stools, or both.
6. Infectious colitis: This occurs when the colon becomes infected with bacteria, viruses, or parasites, leading to symptoms such as diarrhea, abdominal cramps, and fever.
Treatment for colonic diseases varies depending on the specific condition and its severity. Treatment options may include medications, lifestyle changes, surgery, or a combination of these approaches.
Laparoscopy is a surgical procedure that involves the insertion of a laparoscope, which is a thin tube with a light and camera attached to it, through small incisions in the abdomen. This allows the surgeon to view the internal organs without making large incisions. It's commonly used to diagnose and treat various conditions such as endometriosis, ovarian cysts, infertility, and appendicitis. The advantages of laparoscopy over traditional open surgery include smaller incisions, less pain, shorter hospital stays, and quicker recovery times.
The rectum is the lower end of the digestive tract, located between the sigmoid colon and the anus. It serves as a storage area for feces before they are eliminated from the body. The rectum is about 12 cm long in adults and is surrounded by layers of muscle that help control defecation. The mucous membrane lining the rectum allows for the detection of stool, which triggers the reflex to have a bowel movement.
Diverticulitis, Colonic is a medical condition characterized by the inflammation or infection of one or more diverticula in the colon. Diverticula are small, bulging pouches that form in the wall of the colon, usually in older adults. They are caused by increased pressure on weakened areas of the colon wall, resulting in the formation of these sac-like protrusions.
When diverticula become inflamed or infected, it leads to the condition known as diverticulitis. Symptoms of colonic diverticulitis may include abdominal pain, fever, nausea, vomiting, constipation or diarrhea, and a decreased appetite. In severe cases, complications such as perforation, abscess formation, or peritonitis (inflammation of the lining of the abdominal cavity) may occur, requiring hospitalization and surgical intervention.
The exact cause of diverticulitis is not fully understood, but it is believed to be associated with a low-fiber diet, obesity, smoking, and lack of exercise. Treatment typically involves antibiotics to clear the infection, a liquid diet to allow the colon to rest, and over-the-counter or prescription pain medications to manage discomfort. In severe cases or in patients who experience recurrent episodes of diverticulitis, surgery may be necessary to remove the affected portion of the colon.
Adenomatous Polyposis Coli (APC) is a genetic disorder characterized by the development of numerous adenomatous polyps in the colon and rectum. APC is caused by mutations in the APC gene, which is a tumor suppressor gene that helps regulate cell growth and division. When the APC gene is mutated, it can lead to uncontrolled cell growth and the development of polyps, which can eventually become cancerous.
Individuals with APC typically develop hundreds to thousands of polyps in their colon and rectum, usually beginning in adolescence or early adulthood. If left untreated, APC can lead to colorectal cancer in nearly all affected individuals by the age of 40.
APC is an autosomal dominant disorder, which means that a person has a 50% chance of inheriting the mutated gene from an affected parent. However, some cases of APC may also occur spontaneously due to new mutations in the APC gene. Treatment for APC typically involves surgical removal of the colon and rectum (colectomy) to prevent the development of colorectal cancer. Regular surveillance with colonoscopy is also recommended to monitor for the development of new polyps.
The sigmoid colon is a part of the large intestine that forms an "S"-shaped curve before it joins the rectum. It gets its name from its unique shape, which resembles the Greek letter sigma (σ). The main function of the sigmoid colon is to store stool temporarily and assist in the absorption of water and electrolytes from digestive waste before it is eliminated from the body.
Colonic pouches, also known as pouch colon or reservoir, refer to an artificial structure created during a surgical procedure called restorative proctocolectomy. This is often performed in patients with certain types of inflammatory bowel disease like ulcerative colitis or familial adenomatous polyposis.
During the surgery, the entire colon and rectum are removed. A pouch is then created using the patient's own small intestine, which is folded back on itself and sewn together to form a reservoir. This pouch is connected to the anus, allowing the patient to have relatively normal bowel movements.
The most common type of colonic pouch is the J-pouch, so named because of its J-shaped design. Other types include the S-pouch and the W-pouch. The choice of pouch depends on various factors, including the patient's anatomy and the surgeon's preference.
The purpose of creating a colonic pouch is to restore intestinal continuity and function after removing the diseased colon and rectum, thereby improving the patient's quality of life. However, it's important to note that living with a colonic pouch also requires significant lifestyle adjustments and ongoing medical management.
"Sigmoid diseases" is not a widely recognized medical term. However, the sigmoid colon is a part of the large intestine, and it can be affected by various conditions such as:
1. Sigmoid diverticulitis: Inflammation or infection of small pouches (diverticula) that form on the wall of the sigmoid colon.
2. Sigmoid volvulus: Twisting of the sigmoid colon on itself, which can lead to obstruction and ischemia.
3. Sigmoid cancer: Malignant tumor arising from the epithelial cells lining the sigmoid colon.
4. Inflammatory bowel disease (IBD): Chronic inflammation of the intestine, including the sigmoid colon, that can lead to symptoms such as diarrhea, abdominal pain, and weight loss.
5. Irritable bowel syndrome (IBS): Functional gastrointestinal disorder characterized by abdominal pain, bloating, and altered bowel habits, which can affect the sigmoid colon.
Therefore, "sigmoid diseases" could refer to any of these conditions or others that specifically affect the sigmoid colon.
Toxic megacolon is a serious complication of colon inflammation that is characterized by non-obstructive dilation of the colon (diameter greater than 6 cm) and systemic toxicity. It is often associated with conditions such as inflammatory bowel disease (e.g., ulcerative colitis, Crohn's disease), infections (e.g., Clostridioides difficile infection), and ischemic colitis.
The dilation of the colon can lead to decreased blood flow, impaired motility, and increased risk of perforation, which can result in sepsis and even death if not promptly treated. The systemic toxicity may manifest as fever, tachycardia, hypotension, electrolyte imbalances, and mental status changes.
Toxic megacolon requires immediate medical attention, often involving hospitalization, intravenous fluids, antibiotics, and possibly surgical intervention to remove the affected portion of the colon.
Surgical anastomosis is a medical procedure that involves the connection of two tubular structures, such as blood vessels or intestines, to create a continuous passage. This technique is commonly used in various types of surgeries, including vascular, gastrointestinal, and orthopedic procedures.
During a surgical anastomosis, the ends of the two tubular structures are carefully prepared by removing any damaged or diseased tissue. The ends are then aligned and joined together using sutures, staples, or other devices. The connection must be secure and leak-free to ensure proper function and healing.
The success of a surgical anastomosis depends on several factors, including the patient's overall health, the location and condition of the structures being joined, and the skill and experience of the surgeon. Complications such as infection, bleeding, or leakage can occur, which may require additional medical intervention or surgery.
Proper postoperative care is also essential to ensure the success of a surgical anastomosis. This may include monitoring for signs of complications, administering medications to prevent infection and promote healing, and providing adequate nutrition and hydration.
The ileum is the third and final segment of the small intestine, located between the jejunum and the cecum (the beginning of the large intestine). It plays a crucial role in nutrient absorption, particularly for vitamin B12 and bile salts. The ileum is characterized by its thin, lined walls and the presence of Peyer's patches, which are part of the immune system and help surveil for pathogens.
Pouchitis is a condition characterized by inflammation of the ileal pouch, a surgically created reservoir that is connected to the patient's anus in individuals who have undergone proctocolectomy with ileal pouch-anal anastomosis (IPAA). This procedure is often performed in patients with ulcerative colitis or familial adenomatous polyposis.
Pouchitis can present with symptoms such as diarrhea, abdominal cramps, urgency, and fecal incontinence. The exact cause of pouchitis remains unclear, but it is thought to be related to changes in the microbiota or an overactive immune response in the ileal pouch.
The diagnosis of pouchitis typically involves a combination of clinical symptoms, endoscopic findings, and histopathological examination of biopsies taken during endoscopy. Treatment options for pouchitis include antibiotics, anti-inflammatory medications, and probiotics, depending on the severity and frequency of the condition.
The transverse colon is the section of the large intestine that runs horizontally across the abdomen, located between the ascending colon and the descending colon. It receives digested food material from the left side of the cecum via the transverse mesocolon, a double-layered fold of peritoneum that attaches it to the posterior abdominal wall.
The transverse colon is responsible for absorbing water, electrolytes, and vitamins from the digested food material before it moves into the distal sections of the large intestine. It also contains a large number of bacteria that help in the breakdown of complex carbohydrates and the production of certain vitamins, such as vitamin K and biotin.
The transverse colon is highly mobile and can change its position within the abdomen depending on factors such as respiration, digestion, and posture. It is also prone to various pathological conditions, including inflammation (colitis), diverticulosis, and cancer.
Megacolon is a medical condition characterized by an abnormal dilation and/or hypomotility (decreased ability to move) of the colon, resulting in a significantly enlarged colon. It can be congenital or acquired. Congenital megacolon, also known as Hirschsprung's disease, is present at birth and occurs due to the absence of ganglion cells in the distal portion of the colon. Acquired megacolon, on the other hand, can develop in adults due to various causes such as chronic constipation, neurological disorders, or certain medications.
In both cases, the affected individual may experience symptoms like severe constipation, abdominal distention, and fecal impaction. If left untreated, megacolon can lead to complications such as perforation of the colon, sepsis, and even death. Treatment options depend on the underlying cause but may include medication, surgery, or a combination of both.
Postoperative complications refer to any unfavorable condition or event that occurs during the recovery period after a surgical procedure. These complications can vary in severity and may include, but are not limited to:
1. Infection: This can occur at the site of the incision or inside the body, such as pneumonia or urinary tract infection.
2. Bleeding: Excessive bleeding (hemorrhage) can lead to a drop in blood pressure and may require further surgical intervention.
3. Blood clots: These can form in the deep veins of the legs (deep vein thrombosis) and can potentially travel to the lungs (pulmonary embolism).
4. Wound dehiscence: This is when the surgical wound opens up, which can lead to infection and further complications.
5. Pulmonary issues: These include atelectasis (collapsed lung), pneumonia, or respiratory failure.
6. Cardiovascular problems: These include abnormal heart rhythms (arrhythmias), heart attack, or stroke.
7. Renal failure: This can occur due to various reasons such as dehydration, blood loss, or the use of certain medications.
8. Pain management issues: Inadequate pain control can lead to increased stress, anxiety, and decreased mobility.
9. Nausea and vomiting: These can be caused by anesthesia, opioid pain medication, or other factors.
10. Delirium: This is a state of confusion and disorientation that can occur in the elderly or those with certain medical conditions.
Prompt identification and management of these complications are crucial to ensure the best possible outcome for the patient.
Gastrointestinal agents are a class of pharmaceutical drugs that affect the gastrointestinal (GI) tract, which includes the organs involved in digestion such as the mouth, esophagus, stomach, small intestine, large intestine, and anus. These agents can have various effects on the GI tract, including:
1. Increasing gastric motility (promoting bowel movements) - laxatives, prokinetics
2. Decreasing gastric motility (reducing bowel movements) - antidiarrheal agents
3. Neutralizing gastric acid - antacids
4. Reducing gastric acid secretion - H2-blockers, proton pump inhibitors
5. Protecting the mucosal lining of the GI tract - sucralfate, misoprostol
6. Relieving symptoms associated with GI disorders such as bloating, abdominal pain, and nausea - antispasmodics, antiemetics
Examples of gastrointestinal agents include:
* Laxatives (e.g., psyllium, docusate)
* Prokinetics (e.g., metoclopramide)
* Antacids (e.g., calcium carbonate, aluminum hydroxide)
* H2-blockers (e.g., ranitidine, famotidine)
* Proton pump inhibitors (e.g., omeprazole, lansoprazole)
* Sucralfate
* Misoprostol
* Antispasmodics (e.g., hyoscyamine, dicyclomine)
* Antiemetics (e.g., ondansetron, promethazine)
It is important to note that gastrointestinal agents can have both therapeutic and adverse effects, and their use should be based on a careful evaluation of the patient's condition and medical history.
Emergency treatment refers to the urgent medical interventions and care provided to individuals who are experiencing a severe injury, illness, or life-threatening condition. The primary aim of emergency treatment is to stabilize the patient's condition, prevent further harm, and provide immediate medical attention to save the patient's life or limb.
Emergency treatment may include various medical procedures, such as cardiopulmonary resuscitation (CPR), airway management, administering medications, controlling bleeding, treating burns, immobilizing fractures, and providing pain relief. The specific emergency treatment provided will depend on the nature and severity of the patient's condition.
Emergency treatment is typically delivered in an emergency department (ED) or a similar setting, such as an urgent care center, ambulance, or helicopter transport. Healthcare professionals who provide emergency treatment include emergency physicians, nurses, paramedics, and other specialists trained in emergency medicine.
It's important to note that emergency treatment is different from routine medical care, which is usually provided on a scheduled basis and focuses on preventing, diagnosing, and managing chronic or ongoing health conditions. Emergency treatment, on the other hand, is provided in response to an acute event or crisis that requires immediate attention and action.
An emergency is a sudden, unexpected situation that requires immediate medical attention to prevent serious harm, permanent disability, or death. Emergencies can include severe injuries, trauma, cardiac arrest, stroke, difficulty breathing, severe allergic reactions, and other life-threatening conditions. In such situations, prompt medical intervention is necessary to stabilize the patient's condition, diagnose the underlying problem, and provide appropriate treatment.
Emergency medical services (EMS) are responsible for providing emergency care to patients outside of a hospital setting, such as in the home, workplace, or public place. EMS personnel include emergency medical technicians (EMTs), paramedics, and other first responders who are trained to assess a patient's condition, provide basic life support, and transport the patient to a hospital for further treatment.
In a hospital setting, an emergency department (ED) is a specialized unit that provides immediate care to patients with acute illnesses or injuries. ED staff includes physicians, nurses, and other healthcare professionals who are trained to handle a wide range of medical emergencies. The ED is equipped with advanced medical technology and resources to provide prompt diagnosis and treatment for critically ill or injured patients.
Overall, the goal of emergency medical care is to stabilize the patient's condition, prevent further harm, and provide timely and effective treatment to improve outcomes and save lives.
Diverticulosis, colonic is a medical condition characterized by the presence of small sacs or pouches (diverticula) that form on the outer wall of the large intestine (colon). These sacs are usually found in the sigmoid colon, which is the part of the colon that is closest to the rectum.
Diverticulosis occurs when the inner layer of the colon's muscle pushes through weak spots in the outer layer of the colon wall, creating small pockets or sacs. The exact cause of diverticulosis is not known, but it may be associated with a low-fiber diet, aging, and increased pressure in the colon.
Most people with diverticulosis do not experience any symptoms, and the condition is often discovered during routine screening exams or when complications arise. However, some people may experience cramping, bloating, and changes in bowel habits.
Diverticulosis can lead to complications such as inflammation (diverticulitis), bleeding, and infection. It is important to seek medical attention if you experience symptoms such as severe abdominal pain, fever, or rectal bleeding, as these may be signs of a more serious condition.
Treatment for diverticulosis typically involves making dietary changes, increasing fiber intake, and taking medications to manage symptoms. In some cases, surgery may be necessary to remove affected portions of the colon.
Colonic neoplasms refer to abnormal growths in the large intestine, also known as the colon. These growths can be benign (non-cancerous) or malignant (cancerous). The two most common types of colonic neoplasms are adenomas and carcinomas.
Adenomas are benign tumors that can develop into cancer over time if left untreated. They are often found during routine colonoscopies and can be removed during the procedure.
Carcinomas, on the other hand, are malignant tumors that invade surrounding tissues and can spread to other parts of the body. Colorectal cancer is the third leading cause of cancer-related deaths in the United States, and colonic neoplasms are a significant risk factor for developing this type of cancer.
Regular screenings for colonic neoplasms are recommended for individuals over the age of 50 or those with a family history of colorectal cancer or other risk factors. Early detection and removal of colonic neoplasms can significantly reduce the risk of developing colorectal cancer.
Intestinal polyps are abnormal growths that protrude from the lining of the intestines. They can occur in any part of the digestive tract, including the colon and rectum (colorectal polyps), small intestine, or stomach. These growths vary in size, shape, and number. Most intestinal polyps are benign, meaning they are not cancerous. However, some types of polyps, such as adenomatous polyps, can become cancerous over time if left untreated.
Intestinal polyps can be asymptomatic or cause symptoms like rectal bleeding, abdominal pain, changes in bowel habits, or anemia (in cases where there is chronic, slow bleeding). The exact cause of intestinal polyps is not fully understood, but factors such as age, family history, and certain genetic conditions can increase the risk of developing them. Regular screening exams, like colonoscopies, are essential for early detection and removal of polyps to prevent potential complications, including colorectal cancer.
Cecal neoplasms refer to abnormal growths in the cecum, which is the first part of the large intestine or colon. These growths can be benign (non-cancerous) or malignant (cancerous). Common types of cecal neoplasms include adenomas (benign tumors that can become cancerous over time), carcinoids (slow-growing tumors that usually don't spread), and adenocarcinomas (cancers that start in the glands that line the inside of the cecum).
Symptoms of cecal neoplasms may include changes in bowel habits, such as diarrhea or constipation; abdominal pain or cramping; blood in the stool; and unexplained weight loss. Treatment options depend on the type and stage of the neoplasm but may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. Regular screening is recommended for people at high risk for developing colorectal cancer, including those with a family history of the disease or certain genetic mutations.
Gardner Syndrome is a rare inherited condition associated with a mutation in the APC gene, which also causes Familial Adenomatous Polyposis (FAP). This syndrome is characterized by the development of multiple benign tumors called adenomas in the colon and rectum. Additionally, individuals with Gardner Syndrome often develop various types of non-cancerous growths outside the gastrointestinal tract, such as osteomas (benign bone tumors), dental abnormalities, and epidermoid cysts on the skin.
Individuals with this syndrome have an increased risk of developing colorectal cancer at a young age, typically before 40 years old, if not monitored and treated appropriately. Other cancers that may develop in association with Gardner Syndrome include duodenal cancer, thyroid cancer, brain tumors (particularly cerebellar medulloblastomas), and adrenal gland tumors.
Regular surveillance through colonoscopies and other diagnostic tests is crucial for early detection and management of potential malignancies in individuals with Gardner Syndrome.
Crohn's disease is a type of inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract, from the mouth to the anus. It is characterized by chronic inflammation of the digestive tract, which can lead to symptoms such as abdominal pain, diarrhea, fatigue, weight loss, and malnutrition.
The specific causes of Crohn's disease are not fully understood, but it is believed to be related to a combination of genetic, environmental, and immune system factors. The disease can affect people of any age, but it is most commonly diagnosed in young adults between the ages of 15 and 35.
There is no cure for Crohn's disease, but treatments such as medications, lifestyle changes, and surgery can help manage symptoms and prevent complications. Treatment options depend on the severity and location of the disease, as well as the individual patient's needs and preferences.
Intestinal obstruction, also known as bowel obstruction, is a medical condition characterized by a blockage that prevents the normal flow of contents through the small intestine or large intestine (colon). This blockage can be caused by various factors such as tumors, adhesions (scar tissue), hernias, inflammation, or impacted feces.
The obstruction can be mechanical, where something physically blocks the intestinal lumen, or functional, where the normal muscular contractions of the bowel are impaired. Mechanical obstructions are more common than functional ones.
Symptoms of intestinal obstruction may include abdominal pain and cramping, nausea and vomiting, bloating, inability to pass gas or have a bowel movement, and abdominal distention. If left untreated, intestinal obstruction can lead to serious complications such as tissue death (necrosis), perforation of the intestine, and sepsis. Treatment typically involves hospitalization, intravenous fluids, nasogastric decompression, and possibly surgery to remove the obstruction.
Rectal diseases refer to conditions that affect the structure or function of the rectum, which is the lower end of the large intestine, just above the anus. The rectum serves as a storage area for stool before it is eliminated from the body. Some common rectal diseases include:
1. Hemorrhoids: Swollen veins in the rectum or anus that can cause pain, itching, bleeding, and discomfort.
2. Rectal cancer: Abnormal growth of cells in the rectum that can invade and destroy nearby tissue and spread to other parts of the body.
3. Anal fissures: Small tears in the lining of the anus that can cause pain, bleeding, and itching.
4. Rectal prolapse: A condition where the rectum slips outside the anus, causing discomfort, fecal incontinence, and other symptoms.
5. Inflammatory bowel disease (IBD): A group of chronic inflammatory conditions that affect the digestive tract, including the rectum, such as Crohn's disease and ulcerative colitis.
6. Rectal abscess: A collection of pus in the rectum caused by an infection, which can cause pain, swelling, and fever.
7. Fistula-in-ano: An abnormal connection between the rectum and the skin around the anus, which can cause drainage of pus or stool.
8. Rectal foreign bodies: Objects that are accidentally or intentionally inserted into the rectum and can cause injury, infection, or obstruction.
These are just a few examples of rectal diseases, and there are many other conditions that can affect the rectum. If you experience any symptoms related to the rectum, it is important to seek medical attention from a healthcare professional for proper diagnosis and treatment.
The colon, also known as the large intestine, is a part of the digestive system in humans and other vertebrates. It is an organ that eliminates waste from the body and is located between the small intestine and the rectum. The main function of the colon is to absorb water and electrolytes from digested food, forming and storing feces until they are eliminated through the anus.
The colon is divided into several regions, including the cecum, ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anus. The walls of the colon contain a layer of muscle that helps to move waste material through the organ by a process called peristalsis.
The inner surface of the colon is lined with mucous membrane, which secretes mucus to lubricate the passage of feces. The colon also contains a large population of bacteria, known as the gut microbiota, which play an important role in digestion and immunity.
Constipation is a condition characterized by infrequent bowel movements or difficulty in passing stools that are often hard and dry. The medical definition of constipation varies, but it is generally defined as having fewer than three bowel movements in a week. In addition to infrequent bowel movements, other symptoms of constipation can include straining during bowel movements, feeling like you haven't completely evacuated your bowels, and experiencing hard or lumpy stools.
Constipation can have many causes, including a low-fiber diet, dehydration, certain medications, lack of physical activity, and underlying medical conditions such as irritable bowel syndrome or hypothyroidism. In most cases, constipation can be treated with lifestyle changes, such as increasing fiber intake, drinking more water, and getting regular exercise. However, if constipation is severe, persistent, or accompanied by other symptoms, it's important to seek medical attention to rule out any underlying conditions that may require treatment.
Pseudomembranous enterocolitis is a medical condition characterized by inflammation of the inner lining of the small intestine (enteritis) and large intestine (colitis), resulting in the formation of pseudomembranes – raised, yellowish-white plaques composed of fibrin, mucus, and inflammatory cells. The condition is most commonly caused by a toxin produced by the bacterium Clostridioides difficile (C. difficile), which can overgrow in the gut following disruption of the normal gut microbiota, often after antibiotic use. Symptoms may include diarrhea, abdominal cramps, fever, nausea, and dehydration. Severe cases can lead to complications such as sepsis, toxic megacolon, or even death if left untreated. Treatment typically involves discontinuing the offending antibiotic, administering oral metronidazole or vancomycin to eliminate C. difficile, and managing symptoms with supportive care. In some cases, fecal microbiota transplantation (FMT) may be considered as a treatment option.
Flatulence is the medical term for the release of intestinal gas from the rectum, commonly known as passing gas or farting. It is a normal bodily function that occurs when the body digests food in the stomach and intestines.
During digestion, the body breaks down food into nutrients that can be absorbed into the bloodstream. However, not all food particles can be fully broken down, and some of them reach the large intestine, where they are fermented by bacteria. This fermentation process produces gases such as nitrogen, oxygen, carbon dioxide, hydrogen, and methane.
The buildup of these gases in the digestive tract can cause discomfort, bloating, and the urge to pass gas. The average person passes gas about 10-20 times a day, although this can vary widely from person to person.
While flatulence is a normal bodily function, excessive or frequent passing of gas can be a sign of an underlying digestive issue such as irritable bowel syndrome (IBS), lactose intolerance, or gastrointestinal infections. If you are experiencing persistent or severe symptoms, it is recommended to consult with a healthcare professional for further evaluation and treatment.
The descending colon is a part of the large intestine in the human digestive system. It is called "descending" because it is located inferiorly and posteriorly to the transverse colon, and its direction goes downward as it continues toward the rectum. The descending colon receives digested food material from the transverse colon via the splenic flexure, also known as the left colic flexure.
The primary function of the descending colon is to absorb water, electrolytes, and any remaining nutrients from the undigested food materials that have passed through the small intestine. The descending colon also stores this waste material temporarily before it moves into the rectum for eventual elimination from the body.
The descending colon's wall contains a layer of smooth muscle, which helps propel the waste material along the gastrointestinal tract via peristalsis. Additionally, the inner mucosal lining of the descending colon contains numerous goblet cells that produce and secrete mucus to lubricate the passage of stool and protect the intestinal wall from irritation or damage caused by waste materials.
In summary, the medical definition of 'Colon, Descending' refers to a section of the large intestine responsible for absorbing water and electrolytes while storing and eliminating waste materials through peristaltic movements and mucus secretion.
Abdominal fibromatosis, also known as aggressive abdominal wall fibromatosis or desmoid tumors, are rare, non-cancerous (benign) growths that originate from the connective tissue in the abdominal wall. These tumors can be invasive and grow into surrounding tissues, causing discomfort, pain, or complications such as bowel obstruction. They can occur spontaneously or following surgical trauma, pregnancy, or familial adenomatous polyposis (FAP), a genetic disorder that increases the risk of colorectal cancer. Treatment options include surgery, radiation therapy, and medical management with anti-inflammatory drugs or chemotherapeutic agents. Regular follow-up is necessary due to the possibility of recurrence.
The anal canal is the terminal portion of the digestive tract, located between the rectum and the anus. It is a short tube-like structure that is about 1 to 1.5 inches long in adults. The main function of the anal canal is to provide a seal for the elimination of feces from the body while also preventing the leakage of intestinal contents.
The inner lining of the anal canal is called the mucosa, which is kept moist by the production of mucus. The walls of the anal canal contain specialized muscles that help control the passage of stool during bowel movements. These muscles include the internal and external sphincters, which work together to maintain continence and allow for the voluntary release of feces.
The anal canal is an important part of the digestive system and plays a critical role in maintaining bowel function and overall health.
A colonoscopy is a medical procedure used to examine the large intestine, also known as the colon and rectum. It is performed using a flexible tube with a tiny camera on the end, called a colonoscope, which is inserted into the rectum and gently guided through the entire length of the colon.
The procedure allows doctors to visually inspect the lining of the colon for any abnormalities such as polyps, ulcers, inflammation, or cancer. If any polyps are found during the procedure, they can be removed immediately using special tools passed through the colonoscope. Colonoscopy is an important tool in the prevention and early detection of colorectal cancer, which is one of the leading causes of cancer-related deaths worldwide.
Patients are usually given a sedative to help them relax during the procedure, which is typically performed on an outpatient basis in a hospital or clinic setting. The entire procedure usually takes about 30-60 minutes to complete, although patients should plan to spend several hours at the medical facility for preparation and recovery.
Colorectal surgery is a medical specialty that deals with the diagnosis and treatment of disorders affecting the colon, rectum, and anus. This can include conditions such as colorectal cancer, inflammatory bowel disease (such as Crohn's disease or ulcerative colitis), diverticulitis, and anal fistulas or fissures.
The surgical procedures performed by colorectal surgeons may involve minimally invasive techniques, such as laparoscopic or robotic-assisted surgery, or more traditional open surgery. These procedures can range from removing polyps during a colonoscopy to complex resections of the colon, rectum, or anus.
Colorectal surgeons also work closely with other medical specialists, such as gastroenterologists, oncologists, and radiologists, to provide comprehensive care for their patients.
"Length of Stay" (LOS) is a term commonly used in healthcare to refer to the amount of time a patient spends receiving care in a hospital, clinic, or other healthcare facility. It is typically measured in hours, days, or weeks and can be used as a metric for various purposes such as resource planning, quality assessment, and reimbursement. The length of stay can vary depending on the type of illness or injury, the severity of the condition, the patient's response to treatment, and other factors. It is an important consideration in healthcare management and can have significant implications for both patients and providers.
Ileus is a condition characterized by a lack of intestinal motility or paralysis of the bowel, leading to obstruction of the digestive tract. It is not caused by a physical blockage but rather by a disruption of the normal muscular contractions (peristalsis) that move food through the intestines. This can result in abdominal distention, vomiting, and absence of bowel movements or gas passage. Ileus can be a complication of various surgical procedures, intra-abdominal infections, or other medical conditions. It is essential to diagnose and treat ileus promptly to prevent further complications such as tissue damage, sepsis, or even death.
Defecation is the medical term for the act of passing stools (feces) through the anus. It is a normal bodily function that involves the contraction of muscles in the colon and anal sphincter to release waste from the body. Defecation is usually a regular and daily occurrence, with the frequency varying from person to person.
The stool is made up of undigested food, bacteria, and other waste products that are eliminated from the body through the rectum and anus. The process of defecation is controlled by the autonomic nervous system, which regulates involuntary bodily functions such as heart rate and digestion.
Difficulties with defecation can occur due to various medical conditions, including constipation, irritable bowel syndrome, and inflammatory bowel disease. These conditions can cause symptoms such as hard or painful stools, straining during bowel movements, and a feeling of incomplete evacuation. If you are experiencing any problems with defecation, it is important to speak with your healthcare provider for proper diagnosis and treatment.
'Clostridium difficile' (also known as 'C. difficile' or 'C. diff') is a type of Gram-positive, spore-forming bacterium that can be found in the environment, including in soil, water, and human and animal feces. It is a common cause of healthcare-associated infections, particularly in individuals who have recently received antibiotics or have other underlying health conditions that weaken their immune system.
C. difficile produces toxins that can cause a range of symptoms, from mild diarrhea to severe colitis (inflammation of the colon) and potentially life-threatening complications such as sepsis and toxic megacolon. The most common toxins produced by C. difficile are called TcdA and TcdB, which damage the lining of the intestine and cause inflammation.
C. difficile infections (CDIs) can be difficult to treat, particularly in severe cases or in patients who have recurrent infections. Treatment typically involves discontinuing any unnecessary antibiotics, if possible, and administering specific antibiotics that are effective against C. difficile, such as metronidazole, vancomycin, or fidaxomicin. In some cases, fecal microbiota transplantation (FMT) may be recommended as a last resort for patients with recurrent or severe CDIs who have not responded to other treatments.
Preventing the spread of C. difficile is critical in healthcare settings, and includes measures such as hand hygiene, contact precautions, environmental cleaning, and antibiotic stewardship programs that promote the appropriate use of antibiotics.
Sigmoid neoplasms refer to abnormal growths or tumors in the sigmoid colon, which is the lower portion of the large intestine that extends from the descending colon to the rectum. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms, such as adenomas, are typically removed through a polypectomy during a colonoscopy to prevent their potential transformation into malignant tumors. Malignant neoplasms, on the other hand, are often referred to as sigmoid colon cancers and can be classified into different types based on their cellular origin, such as adenocarcinomas, lymphomas, carcinoids, or sarcomas.
Adenocarcinomas are the most common type of sigmoid neoplasm, accounting for more than 95% of all cases. These tumors originate from the glandular cells lining the colon's inner surface and can invade surrounding tissues, leading to local spread or distant metastasis if left untreated. Early detection and removal of sigmoid neoplasms significantly improve treatment outcomes and overall prognosis.
Surgical stapling is a medical technique that uses specialized staplers to place linear staple lines to close surgical incisions, connect or remove organs and tissues during surgical procedures. Surgical staples are made of titanium or stainless steel and can be absorbable or non-absorbable. They provide secure, fast, and accurate wound closure, reducing the risk of infection and promoting faster healing compared to traditional suturing methods.
The surgical stapler consists of a handle, an anvil, and a cartridge containing multiple staples. The device is loaded with staple cartridges and used to approximate tissue edges before deploying the staples. Once the staples are placed, the stapler is removed, leaving the staple line in place.
Surgical stapling has various applications, including gastrointestinal anastomosis, lung resection, vascular anastomosis, and skin closure. It is widely used in different types of surgeries, such as open, laparoscopic, and robotic-assisted procedures. The use of surgical stapling requires proper training and expertise to ensure optimal patient outcomes.
I'm sorry for any confusion, but "Pirinitramide" doesn't seem to be a recognized term in medical literature or pharmacology. It's possible that there may be a spelling error or it could be a term specific to certain contexts or regions. If you have more information or if there's another term you'd like me to look up, please let me know!
Sclerosing cholangitis is a chronic progressive disease characterized by inflammation and scarring (fibrosis) of the bile ducts, leading to their narrowing or obstruction. This results in impaired bile flow from the liver to the small intestine, which can cause damage to the liver cells and eventually result in cirrhosis and liver failure.
The condition often affects both the intrahepatic (within the liver) and extrahepatic (outside the liver) bile ducts. The exact cause of sclerosing cholangitis is not known, but it is believed to involve an autoimmune response, genetic predisposition, and environmental factors.
Symptoms of sclerosing cholangitis may include jaundice (yellowing of the skin and eyes), itching, abdominal pain, fatigue, weight loss, dark urine, and light-colored stools. The diagnosis is typically made through imaging tests such as magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP), which can visualize the bile ducts and detect any abnormalities.
Treatment for sclerosing cholangitis is aimed at managing symptoms, preventing complications, and slowing down the progression of the disease. This may include medications to relieve itching, antibiotics to treat infections, and drugs to reduce inflammation and improve bile flow. In severe cases, a liver transplant may be necessary.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Rectal neoplasms refer to abnormal growths in the tissues of the rectum, which can be benign or malignant. They are characterized by uncontrolled cell division and can invade nearby tissues or spread to other parts of the body (metastasis). The most common type of rectal neoplasm is rectal cancer, which often begins as a small polyp or growth in the lining of the rectum. Other types of rectal neoplasms include adenomas, carcinoids, and gastrointestinal stromal tumors (GISTs). Regular screenings are recommended for early detection and treatment of rectal neoplasms.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
The ascending colon is the first part of the large intestine, which is the portion of the digestive system that follows the small intestine. It is called "ascending" because it travels upward from the right side of the abdomen toward the underside of the liver. The primary function of the ascending colon is to absorb water and electrolytes from digested food and prepare waste for elimination.
Ileitis is a medical term that refers to inflammation of the ileum, which is the last part of the small intestine. The condition can have various causes, including infections, autoimmune disorders, and inflammatory bowel diseases such as Crohn's disease.
The symptoms of ileitis may include abdominal pain, diarrhea, fever, weight loss, and nausea or vomiting. The diagnosis of ileitis typically involves a combination of medical history, physical examination, laboratory tests, and imaging studies such as CT scans or MRI.
Treatment for ileitis depends on the underlying cause of the inflammation. In cases of infectious ileitis, antibiotics may be used to treat the infection. For autoimmune or inflammatory causes, medications that suppress the immune system may be necessary to reduce inflammation and manage symptoms.
In severe cases of ileitis, surgery may be required to remove damaged portions of the intestine or to drain abscesses. It is important to seek medical attention if you experience symptoms of ileitis, as early diagnosis and treatment can help prevent complications and improve outcomes.
Colonic pseudo-obstruction, also known as Ogilvie's syndrome, is a medical condition characterized by the absence of an actual physical obstruction in the colon, but with symptoms and radiologic findings that mimic a mechanical intestinal obstruction. It is caused by a dysfunction of the nervous system or muscles in the colon, leading to severe dilation and potential perforation if not treated promptly.
The condition is often associated with underlying medical conditions such as surgery, trauma, infection, electrolyte imbalances, neurologic disorders, and certain medications. The symptoms may include abdominal pain, distention, nausea, vomiting, constipation, and in severe cases, fever and sepsis.
Treatment typically involves decompression of the colon using a nasogastric tube or colonoscopy, as well as addressing any underlying causes. In some cases, surgery may be necessary to remove the excess gas and stool from the colon or to repair a perforation.
Sodium acetate is an ionic compound with the formula NaC2H3O2. It is formed by the combination of sodium ions (Na+) and acetate ions (C2H3O2-). Sodium acetate is a white, crystalline solid that is highly soluble in water. It is commonly used as a buffer in laboratory settings to help maintain a stable pH level in solutions.
In the body, sodium acetate can be produced as a byproduct of metabolism and is also found in some foods and medications. It is quickly converted to bicarbonate in the body, which helps to regulate the acid-base balance and maintain a normal pH level in the blood. Sodium acetate is sometimes used as a source of sodium and acetate ions in intravenous (IV) fluids to help treat dehydration or metabolic acidosis, a condition in which the body has too much acid.
It's important to note that while sodium acetate is generally considered safe when used as directed, it can cause side effects if taken in large amounts or in combination with certain medications. It is always best to consult with a healthcare provider before using any new medication or supplement.
Intestinal polyposis is a condition characterized by the presence of multiple polyps in the inner lining (mucosa) of the intestines. These polyps are abnormal growths that protrude from the intestinal wall and can vary in size, number, and type. Some common types of polyps include adenomatous, hyperplastic, and inflammatory polyps.
Intestinal polyposis can occur throughout the gastrointestinal tract, including the stomach, small intestine, and large intestine (colon). The condition can be inherited or acquired, and it is often associated with various genetic syndromes such as familial adenomatous polyposis (FAP), Peutz-Jeghers syndrome, juvenile polyposis syndrome, and Lynch syndrome.
Depending on the type, size, and number of polyps, intestinal polyposis can increase the risk of developing colorectal cancer and other gastrointestinal malignancies. Regular surveillance, monitoring, and removal of polyps are essential for managing this condition and preventing complications.
Elective surgical procedures are operations that are scheduled in advance because they do not involve a medical emergency. These surgeries are chosen or "elective" based on the patient's and doctor's decision to improve the patient's quality of life or to treat a non-life-threatening condition. Examples include but are not limited to:
1. Aesthetic or cosmetic surgery such as breast augmentation, rhinoplasty, etc.
2. Orthopedic surgeries like knee or hip replacements
3. Cataract surgery
4. Some types of cancer surgeries where the tumor is not spreading or causing severe symptoms
5. Gastric bypass for weight loss
It's important to note that while these procedures are planned, they still require thorough preoperative evaluation and preparation, and carry risks and benefits that need to be carefully considered by both the patient and the healthcare provider.
 Colectomy - Wikipedia
Colectomy - Wikipedia
 Total abdominal colectomy: MedlinePlus Medical Encyclopedia
Total abdominal colectomy: MedlinePlus Medical Encyclopedia
 Ileocolectomy and Right Colectomy and Colorectal Cancer
Ileocolectomy and Right Colectomy and Colorectal Cancer
 Fewer Colectomy Procedures Performed Among Ulcerative Colitis Patients | MedPage Today
Fewer Colectomy Procedures Performed Among Ulcerative Colitis Patients | MedPage Today
 Single incision right colectomy from the SAGES Video Library
Single incision right colectomy from the SAGES Video Library
Single Port Laparoscopic Colectomy: the Learning Curve - SAGES Abstract Archives
 Intravenous Acetaminophen Has Only Limited Benefit for Colectomy Patients, Mount Sinai Study Finds
Intravenous Acetaminophen Has Only Limited Benefit for Colectomy Patients, Mount Sinai Study Finds
Vesalius Clinical Folios: Total Colectomy and J-Pouch for Ulcerative Colitis
 Colon Resection Technique: Approach Considerations, Laparoscopic Left and Sigmoid Colectomy, Low Anterior Resection, and...
Colon Resection Technique: Approach Considerations, Laparoscopic Left and Sigmoid Colectomy, Low Anterior Resection, and...
 Outcomes in Laparoscopic Colectomy for Colorectal Cancer in the Obese | OMICS International | Abstract
Outcomes in Laparoscopic Colectomy for Colorectal Cancer in the Obese | OMICS International | Abstract
 Colon Cancer Surgery - Laparoscopic Colectomy in Bangkok, Thailand
Colon Cancer Surgery - Laparoscopic Colectomy in Bangkok, Thailand
Elective colectomy for severe ulcerative colitis may reduce mortality more than medical therapy | BMJ Evidence-Based Medicine
 Long-term risk of cardiovascular and cerebrovascular disease after removal of the colonic microbiota by colectomy: a cohort...
Long-term risk of cardiovascular and cerebrovascular disease after removal of the colonic microbiota by colectomy: a cohort...
 Colectomy | Colon Resection Surgery - UChicago Medicine
Colectomy | Colon Resection Surgery - UChicago Medicine
HIE Multimedia - Total colectomy or proctocolectomy - discharge
 Colectomy in patients with ulcerative colitis is not associated to future diagnosis of primary sclerosing cholangitis | Lund...
Colectomy in patients with ulcerative colitis is not associated to future diagnosis of primary sclerosing cholangitis | Lund...
 SURGERY OF ACUTE SEVERE ULCERATIVE COLITIS, SUBTOTAL COLECTOMY: WHEN AND HOW TO DO IT?| Abstract
SURGERY OF ACUTE SEVERE ULCERATIVE COLITIS, SUBTOTAL COLECTOMY: WHEN AND HOW TO DO IT?| Abstract
 European Crohn´s and Colitis Organisation - ECCO - P231 Emergency Colectomy for IBD Is Not Associated with Increased Risk of...
European Crohn´s and Colitis Organisation - ECCO - P231 Emergency Colectomy for IBD Is Not Associated with Increased Risk of...
 Subtotal Colectomy with Ileostomy, Surgical Management of Ischemic Colitis: A Case Study
Subtotal Colectomy with Ileostomy, Surgical Management of Ischemic Colitis: A Case Study
 colectomy | GlobeHealer
colectomy | GlobeHealer
 Colorectal cancer: Symptoms, treatment, risk factors, and more
Colorectal cancer: Symptoms, treatment, risk factors, and more
 Colectomy - Regional Clinic
Colectomy - Regional Clinic
IOS Press Ebooks - Surgery simulation using patient-specific models for laparoscopic colectomy
Preventive Oncology: Overview, Risk Assessment, Modifiable Risk Factors
Achieving the High-Value Colectomy: Preventing Complications or Improving Efficiency - Fingerprint - Experts@Syracuse
 Crohn's Disease Surgery: Types, After, and More
Crohn's Disease Surgery: Types, After, and More
 Single incision laparoscopic right colectomy
Single incision laparoscopic right colectomy
 Colon Cancer Surgery Johannesburg | Colectomy
Colon Cancer Surgery Johannesburg | Colectomy
 during-surgery-colectomy-1 - Beranisehat
during-surgery-colectomy-1 - Beranisehat Colorectal Cancer surgery in Surat : Laparoscopic Colectomy
Colorectal Cancer surgery in Surat : Laparoscopic ColectomyRight colectomy11
- What Is a Laparoscopic Ileocolectomy and Right Colectomy? (webmd.com)
- In a right colectomy, the surgeon removes the ascending colon, but leaves the ileum. (webmd.com)
- In the right colectomy, the ascending colon must be freed from its supporting structure. (webmd.com)
- In a right colectomy, only the ascending colon will be freed from the mesentery. (webmd.com)
- This study was designed to describe the surgical technique for single-incision laparoscopic right colectomy and present preliminary short-term results. (uninsubria.it)
- The patient underwent laparoscopic right colectomy with ileocolic anastomosis to remove both lesions. (jomi.com)
- This patient underwent a laparoscopic right colectomy with ileocolic anastomosis as a curative procedure that removed both an unresectable polyp that was found in his ascending colon as well as a carcinoid tumor that was incidentally found at his ileocecal valve. (jomi.com)
- Due to the nature of these two masses, a laparoscopic right colectomy with ileocolic anastomosis was performed. (jomi.com)
- Larson, DW 2008, Right Colectomy: Open and Laparoscopic . (elsevierpure.com)
- No clear consensus on the need to perform an intracorporeal anastomosis (IA) after laparoscopic right colectomy is currently available. (unina.it)
- Based on these results, surgical stress and metabolic response to IA justify advocating the adoption of a totally laparoscopic approach when performing a right colectomy for cancer. (unina.it)
Colorectal cancer7
- Bowel infarction, which may be a complication of ischemic colitis Typhlitis Hirschsprung's disease Prophylactic colectomy can be indicated in some forms of polyposis, Lynch syndrome and certain cases of inflammatory bowel disease because of high risk for development of colorectal cancer. (wikipedia.org)
- LAS VEGAS -- Treatment advancements appear to have helped cut colectomy rates to treat colorectal cancer among patients with ulcerative colitis (UC), according to a presentation here. (medpagetoday.com)
- With emerging advances in treatment and surveillance, colectomy rates in Canada's Alberta province declined 8.6% annually from 2003 to 2015 for colorectal cancer, reported Sherman Picardo, MBBS, of University of Calgary in Alberta, at the Crohn's & Colitis Congress . (medpagetoday.com)
- The analysis was based on provincial registry data, allowing researchers to identify UC patients who had colorectal cancer diagnoses and colectomies, as well as their histories of colonoscopy. (medpagetoday.com)
- Picardo and his colleagues identified 112 colorectal cancer cases among UC patients, of whom 86 had colonoscopy in the year preceding colectomy and 26 did not. (medpagetoday.com)
- Picardo S, et al "A significant decline in colectomy rates for colorectal cancer in patients with ulcerative colitis" CCC 2019. (medpagetoday.com)
- Garcia JS, Dasilva G (2013) Outcomes in Laparoscopic Colectomy for Colorectal Cancer in the Obese. (omicsonline.org)
Ulcerative5
- Some of the most common indications for colectomy are: Colon cancer Diverticulitis and diverticular disease of the large intestine Trauma Inflammatory bowel disease such as ulcerative colitis or Crohn's disease. (wikipedia.org)
- A colectomy is considered a "cure" for ulcerative colitis because the disease attacks only the large intestine and therefore will not be able to flare up again if the entire large intestine (cecum, ascending colon, transverse colon, descending colon and sigmoid colon) and rectum are removed. (wikipedia.org)
- Colectomy is used as a treatment for a variety of diseases, including colon or rectal cancer , large polyps (growths that arise on the lining of the colon), diverticular disease , inflammatory bowel disease (Crohn's disease or ulcerative colitis), or intestinal bleeding that cannot be stopped. (uchicagomedicine.org)
- Occurrence of Crohn's disease in children after total colectomy for ulcerative colitis. (childrensmercy.org)
- BACKGROUND: Colectomy is the definitive treatment for ulcerative colitis (UC) to remove the inflammatory burden. (childrensmercy.org)
Left colectomy2
- Left colectomy. (medscape.com)
- One contraindication for left colectomy is metastatic colon cancer without complications. (medscape.com)
Open colectomy4
- The Mount Sinai team analyzed data of 181,640 patients undergoing open colectomy surgery in 602 hospitals across the United States from 2011-2016. (newswise.com)
- An open colectomy uses a long incision down the center of the abdomen. (uchicagomedicine.org)
- The exact same operation is performed on the inside as with an open colectomy. (uchicagomedicine.org)
- The advantages of a laparoscopic colectomy include reduced postoperative pain due to a shorter incision and decreased exposure of the intra-abdominal viscera to air, compared to an open colectomy. (uchicagomedicine.org)
Elective colectomy3
- This study aims to assess whether patients with severe UC have improved survival after elective colectomy compared to those being treated with certain immunosuppressive therapies. (bmj.com)
- We utilized the NSQIP PUF IBD Cohort 2005-2019 to assess 30-day outcomes in adult IBD patients undergoing emergency vs elective colectomy. (ecco-ibd.eu)
- A study by Roulin et al comparing patients who underwent elective colectomy and urgent colectomy found that most of the ERAS elements could be applied to emergency colectomy. (medscape.com)
Subtotal colectomy with ileostomy2
- Conclusions: The best possible treatment is represented by subtotal colectomy with ileostomy and preservation of a long rectal stump. (alliedacademies.org)
- This case report will discuss clinical presentations, risk factors, diagnosis, and surgical treatment (subtotal colectomy with ileostomy) in a 50-year-old female patient with IC. (heraldopenaccess.us)
Resection8
- Colectomy (col- + -ectomy) is bowel resection of the large bowel (colon). (wikipedia.org)
- It consists of the surgical removal of any extent of the colon, usually segmental resection (partial colectomy). (wikipedia.org)
- For example, if a patient with Crohn's disease has a transverse colectomy, their Crohn's will usually reappear at the resection site of the ascending and descending colons. (wikipedia.org)
- Subtotal colectomy is resection of part of the colon or a resection of all of the colon without complete resection of the colon. (wikipedia.org)
- Discussion: Single incision laparoscopic right hemicolectomy can be safely performed as an oncologic resection for patients who were candidates for conventional laparoscopic or hand-assisted partial colectomy. (sages.org)
- A colectomy is a surgical procedure that entails the resection of all or sections of the colon. (dramishamaraj.co.za)
- Colectomy, also known as a colon resection, is a surgical procedure in which all or part of the colon is removed. (usinsuranceagents.com)
- Therefore, he required right hemi-colectomy for completion of oncological resection and staging. (surgicaloasis.com)
Large intestine6
- In extreme cases where the entire large intestine is removed, it is called total colectomy, and proctocolectomy (procto- + colectomy) denotes that the rectum is included. (wikipedia.org)
- Colectomy neither cures nor eliminates Crohn's disease, instead only removing part of the entire diseased large intestine. (wikipedia.org)
- i.e., no colectomy surgery can cure Crohn's disease, because the disease usually recurs at the site where the healthy sections of the large intestine were joined. (wikipedia.org)
- Total abdominal colectomy is the removal of the large intestine from the lowest part of the small intestine (ileum) to the rectum. (medlineplus.gov)
- A colectomy is the removal of part or all of the colon, also known as the large intestine. (uchicagomedicine.org)
- A colectomy involves removing the damaged portion of the bowel, including the small intestine, large intestine, or rectum. (healthline.com)
Urgent colectomy1
- In the event that there has been no response to medical rescue therapy after 4-7 days, the patient must undergo urgent colectomy surgery. (alliedacademies.org)
Sigmoid Colectomy2
- sigmoid colectomy is the surgical removal of the sigmoid colon (see the second figure below). (medscape.com)
- Sigmoid colectomy. (medscape.com)
Abdominal6
- Traditionally, colectomy is performed via an abdominal incision (laparotomy), though minimally invasive colectomy, by means of laparoscopy, is growing both in scope of indications and popularity, and is a well-established procedure as of 2006[update] in many medical centers. (wikipedia.org)
- Total abdominal colectomy is most often safe. (medlineplus.gov)
- Colectomies can be performed either laparoscopically or via an open abdominal incision. (medscape.com)
- therefore, a total abdominal colectomy with ileorectal anastomosis was performed. (jomi.com)
- Therefore, after much discussion, we decided to proceed with a subtotal colectomy or total abdominal colectomy with an ileorectal anastomosis rather than an ileoanal J-pouch operation. (jomi.com)
- After total abdominal colectomy, 68 patients went on to ileal pouch anal anastomosis by either a two-stage or three-stage approach. (childrensmercy.org)
Partial2
- When only part of the bowel is removed, it is called a partial colectomy. (healthline.com)
- This video demonstrates the application of the robotic platform for medial to lateral approach for partial colectomy with primary intra-corporeal anastomosis. (surgicaloasis.com)
Surgery9
- Background: Single port laparoscopic colectomy is described as a new technique in laparoscopic colorectal surgery. (sages.org)
- What are the costs for colon cancer surgery with laparoscopic colectomy and can my insurance cover this? (samitivejhospitals.com)
- The aim was therefore to investigate the risk of CVD in patients after a total colectomy compared with patients undergoing other types of surgery, which are not expected to alter the gut microbiota or the CVD risk. (bmj.com)
- Participants Patients (n=1530) aged 45 years and above and surviving 1000 days after total colectomy without CVDs were selected and matched with five control patients who were also free of CVD 1000 days after other types of surgery. (bmj.com)
- The major strength of the study is based on the availability of information in the entire Danish Patient Register from 1996 to 2014, which allows historical prospective assessment of the risk of new occurrences of cardiovascular and cerebrovascular diseases (CVDs) during long-term, essentially complete follow-up in patients after colectomy by comparison with matched patients that had undergone other types of surgery. (bmj.com)
- Patients who have a colectomy for cancer will meet with a medical oncologist soon after they have recovered from surgery to determine if further treatment such as chemotherapy is required. (uchicagomedicine.org)
- As with any major surgery, the cost of colectomy can be significant, raising questions about whether health insurance will cover this procedure. (usinsuranceagents.com)
- Laparoscopic colectomies require 3-5 smaller incisions, typically require an in-hospital stay between 2-5 days and help limit scar tissue after surgery. (atlsurgery.com)
- By definition, a colectomy is a surgery removing either a portion or all of the colon. (arizonapremiersurgery.com)
Anastomosis was performed1
- CASE PRESENTATION A 36-year-old man underwent a periodic medical examination for early colon cancer originating from FAP for which laparoscopic-assisted subtotal colectomy with a J-shaped ileal pouch-rectal anastomosis was performed 3 years earlier. (bvsalud.org)
Minimally3
- Contrarily, a laparoscopic colectomy is a minimally invasive procedure that results in reduced post-operative pain and a faster recovery time. (samitivejhospitals.com)
- As a minimally invasive procedure, a laparoscopic colectomy is performed under general anesthesia. (samitivejhospitals.com)
- With a laparoscopic or minimally invasive colectomy, the surgeon uses several very small incisions and specialized instruments to perform the operation. (uchicagomedicine.org)
Complications1
- The potential complications after colectomy include bleeding and infection, injury to nearby structures including the intestines, the bladder, blood vessels and the ureter (a tube that carries urine from the kidney to the bladder). (uchicagomedicine.org)
Diverticulitis1
- In the case of diverticulitis or inflammatory bowel disease , colectomy is used to remove a segment that is affected by severe inflammation or infection. (uchicagomedicine.org)
Patients14
- From about 2.8 per 1,000 UC patients at risk in 2003, colectomy rates in Alberta dipped to 0.5 per 1,000 in 2015, Picardo said. (medpagetoday.com)
- As a laparoscopic colectomy is performed under general anesthesia, patients will be unconscious for the duration of the procedure. (samitivejhospitals.com)
- Results Estimated by Cox proportional hazard models, the HRs of the composite CVD end point for patients with colectomy compared with the control patients were not significantly reduced (HR=0.94, 95% confidence limits 0.85 to 1.04). (bmj.com)
- Below is a list of frequently asked questions we provide to help patients prepare for their colectomies. (uchicagomedicine.org)
- In PSC patients, colectomy has been linked to improved prognosis, especially following liver transplantation. (lu.se)
- Within the UC cohort (n = 61,993 patients), we matched 5577 patients with colectomy to 15,078 without colectomy. (lu.se)
- Conclusions: In UC patients, colectomy was not associated with a decreased risk of subsequent PSC. (lu.se)
- We then aimed to determine if postoperative outcomes are worse in matched patients undergoing elective vs emergency colectomy. (ecco-ibd.eu)
- Laparoscopic colectomy is an option for many patients with colon disease. (atlsurgery.com)
- The surgeon connects the remaining portions of the colon so that bowel movements can occur as before for most patients who undergo a subtotal colectomy. (arizonapremiersurgery.com)
- Some patients may need a temporary colostomy after a subtotal colectomy until the surgical site heals fully. (arizonapremiersurgery.com)
- While a surgeon may perform an emergency colectomy, most patients have time to prepare for the procedure. (arizonapremiersurgery.com)
- Therefore, we reviewed all of our patients who underwent colectomy for inflammatory bowel disease to evaluate the risk of subsequent Crohn's manifestations and to document the outcomes. (childrensmercy.org)
- RESULTS: We identified 70 patients who underwent colectomy for UC. (childrensmercy.org)
Procedure4
- A colectomy is the medical term used to describe the procedure of removing either a part of, or the entire colon. (samitivejhospitals.com)
- In this article, we will explore the various factors that determine whether health insurance will cover colectomy, as well as how to check if your insurance policy includes coverage for this procedure. (usinsuranceagents.com)
- If a patient needs the entire colon removed, the surgeon performs a procedure known as a total colectomy. (arizonapremiersurgery.com)
- If the surgeon removes only part of the colon, the procedure is a subtotal colectomy. (arizonapremiersurgery.com)
Mesentery1
- As a result, the surgical maneuvers involved in laparoscopic colectomy, such as pushing and grasping of the mesentery and its vessels, were effectively simulated in real-time. (iospress.nl)
Conclusions1
- Conclusions Colectomy did not reduce the general risk of CVD, but reduced the risk of hypertensive disorders, most likely due to salt and water depletion induced by colectomy. (bmj.com)
Emergency1
- Emergency colectomy is characterized by high morbidity and low mortality rates. (alliedacademies.org)
Total6
- citation needed] When the entire colon is removed, this is called a total colectomy, also known as Lane's Operation. (wikipedia.org)
- Objectives The hypothesis of the study was that if the gut microbiota is involved in the development of atherosclerotic cardiovascular and cerebrovascular diseases (CVDs), total colectomy may reduce the long-term risk of CVDs. (bmj.com)
- Total and subtotal colectomies can treat a wide variety of digestive issues. (arizonapremiersurgery.com)
- However, if it continues to grow and spread, a total colectomy may be necessary. (arizonapremiersurgery.com)
- The patient required surgical management for total colectomy. (ageb.be)
- Occurrence of Crohn's disease in children after total colectomy for ul" by Vincent E. Mortellaro, Jonathan Green et al. (childrensmercy.org)
Specimen1
- In one patient, Crohn's was intraoperatively diagnosed from the operative colectomy specimen. (childrensmercy.org)
Crohn's1
- Manifestations of Crohn's after colectomy can be devastating because the ileum is needed for restoration of continuity. (childrensmercy.org)
Restorative1
- A restorative pouch was created after colectomy in 46% using a two-stage approach while, 53% were managed with an initial colectomy and three-stage approach. (childrensmercy.org)
Diagnosis1
- Method: Through nationwide registers, we identified all adults diagnosed with UC in Sweden 1990-2018 and retrieved information on PSC diagnosis and colectomy. (lu.se)
Procedures2
- Home » Understanding Health Insurance » Health Insurance Coverage for Medical Procedures » Will health insurance cover Colectomy? (usinsuranceagents.com)
- MyMediTravel currently has no pricing information available for Colectomy procedures in Philippines. (mymeditravel.com)
Retrospective1
- METHODS: A two-center retrospective review of children who underwent colectomy for IBD from January 2000 to July 2010 was performed. (childrensmercy.org)
Treatment1
- When certain medical conditions or diseases affect the colon, colectomy may be recommended as a treatment option. (usinsuranceagents.com)