Cholesteatoma, Middle Ear
Cholesteatoma
Ear, Middle
Ear Ossicles
Tympanoplasty
Ear Canal
Tympanic Membrane
Ear
Temporal Bone
Otitis Media with Effusion
Middle Ear Ventilation
Ear Neoplasms
Hearing Loss, Conductive
Ear, Inner
Eustachian Tube
Incus
Chinchilla
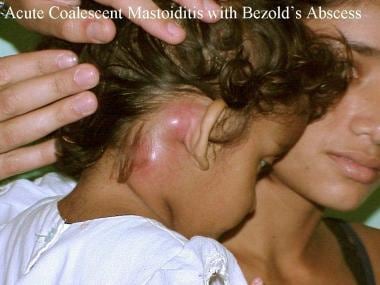
Mastoiditis
Acoustic Impedance Tests
Ear, External
Malleus
Petrous Bone
Cochlear Diseases
Stapes
Cerebrospinal Fluid Otorrhea
Second-Look Surgery
Ossicular Prosthesis
Stapedius
Audiometry, Pure-Tone
Cranial Fossa, Middle
Audiometry
Echo-Planar Imaging
Round Window, Ear
Tensor Tympani
Hearing
Bone Conduction
Gerbillinae
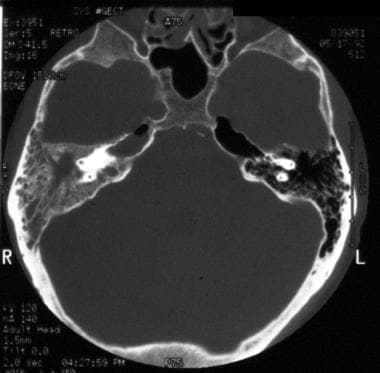
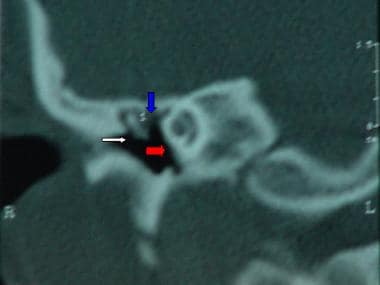
Tomography, X-Ray Computed
Haemophilus influenzae
Semicircular Canals
Fistula
Diffusion Magnetic Resonance Imaging
Optical Imaging
Differentiation characteristics of cholesteatoma epithelium determined by expression of transglutaminase isoenzymes. (1/94)
Transglutaminase (TGase) isoenzymes are involved in the process of the differentiation and cornification of keratinocytes in the epidermis. This study investigates the presence and localization of three TGase isoenzymes to elucidate the nature and differentiation status of the squamous epithelium in human aural cholesteatoma. Twenty cholesteatoma specimens were used. The presence and localization of three TGase isoenzymes were studied by reverse transcription-polymerase chain reaction (RT-PCR) and immunohistochemistry. mRNA expression of three TGase isoenzymes were detected in the tested cholesteatomas with variable levels. The immunohistochemical staining patterns of three TGase isoenzymes showed variations within specimens, relating to keratinizing activity. TGase K is the most abundant among three isoenzymes. Keratinizing epithelium of cholesteatoma have similar expression profiles of TGase isoenzymes with those of epidermis of the skin. Other areas, particularly those showing non-keratinizing epithelium, showed weak immunostaining of TGase E and C, suggesting its different maturation status from keratinizing epithelium. The results of this study indicate that epithelium of cholesteatoma undergoes same direction of maturation and differentiation characteristics as the epidermis of skin, evidenced by similar expressions of TGases both in mRNA level and immunohistochemistry. (+info)Expression of matrix-degrading cysteine proteinase cathepsin K in cholesteatoma. (2/94)
Cholesteatoma is a nonneoplastic lesion of the middle ear space or mastoid that is histologically characterized by a progressive bone erosion of the ossicles and surrounding bone. Several matrix-degrading enzymes have been implicated as mediators of this bone erosion. Because the novel cysteine proteinase cathepsin K has been shown to play a central role in bone resorption, we examined the expression of this enzyme in tissue specimens of cholesteatoma. Tissue specimens of 9 patients with cholesteatoma were obtained during middle-ear surgery. Expression of cathepsin K mRNA was determined by RT-PCR using specific primers. Immunohistochemical analysis of cathepsin K protein expression in tissue sections was performed by using the streptavidin-alkaline phosphatase technique. Expression of both cathepsin K mRNA and protein was detected in areas affected by cholesteatoma, whereas specimens of nonaffected ear cartilage and surrounding tissue were not positive. In addition, cathepsin K was detected in numerous multinucleated giant cells, particularly osteoclasts at the site of bone degradation. In contrast, keratinized squamous epithelium was negative for cathepsin K. These data demonstrate that the matrix-degrading cysteine proteinase cathepsin K may be involved in bone erosion in cholesteatoma. Strong expression of this collagenolytic enzyme in osteoclasts suggests that these cells are mainly involved in cathepsin K-mediated bone destruction. (+info)Diffusion-weighted imaging for differentiating recurrent cholesteatoma from granulation tissue after mastoidectomy: case report. (3/94)
Identification of recurrent cholesteatoma and differentiation from postoperative granulation tissue is important in a patient who has undergone mastoidectomy for cholesteatoma. We describe the diffusion-weighted imaging findings and apparent diffusion coefficient values in a case of recurrent cholesteatoma. This case suggests possible differentiation of cholesteatoma from granulation tissue on the basis of diffusion-weighted imaging findings. (+info)Immunohistochemical investigations of cathepsin D activity in the structures of cholesteatoma. (4/94)
BACKGROUND: Cathepsin D decomposes cytoplasmic proteins, cell organelles, collagen, elastase and proteoglycans. It takes part in angiogenesis and activates osteoclasts, and is thought to play a major role in the destruction of bone tissue by cholesteatoma. The aim of the present study was to evaluate the activity of cathepsin D in the structures of cholesteatoma. MATERIAL/METHODS: Cholesteatomas were collected from 16 patients operated on for chronic inflammation of the middle ear. Specimens were fixed in formalin at pH 7.2, after which parrafin slices were made. Cathepsin D was assayed with a Dako set. Keratin was measured by the Kreyberg method. Normal skin from behind the ear was taken from the patients during the same operation. The samples included a stratified, desquamative epithelium (matrix), a streak containing connective tissue (perimatrix), and a mass of keratin debris. RESULTS: Cathepsin D demonstrates high activity in perimatrix cells adjacent to bone tissue, while it occurs in trace amounts in the matrix. A highly positive reaction was observed within keratin, which was present in the superficial layer of the epithelium. Pseudocathepsin located in desquamative epithelial cells demonstrated a high positive reaction. There were trace amounts of cathepsin D within the dermis. In the control group (the skin samples), there were trace amounts of cathepsin D within the corneous layer of the epithelium. CONCLUSIONS: Cathepsin D places a major role in bone tissue destruction due to cholesteatoma. (+info)Expression patterns of cytokeratins in cholesteatomas: evidence of increased migration and proliferation. (5/94)
Aural cholesteatoma is characterized by invading squamous epithelia with altered growth properties. Cytokeratin (CK) expression is affected in epidermal proliferative diseases and represents the alterations of keratinocyte proliferation, differentiation, and migration. In the present study, the intensity of CK immuno-expression was determined, using densitometry at various sites in experimental cholesteatoma in order to characterize changes of keratinocytes. With cholesteatoma formation, CK4, a marker for non-keratinizing epithelia, increased in the suprabasal layers of the annular external auditory canal (EAC) and at the pars tensa indicating an altered differentiation and migration of keratinocytes. CK5/6, a marker of keratinizing squamous epithelium, increased only at the pars tensa of the tympanic membrane, indicating basal keratinocyte hyperplasia. CK1/10 increased in the suprabasal layer at the annular EAC, and at the peripheral pars tensa, indicating increased terminal differentiation of keratinocytes. CK13/16, markers of differentiation and hyperproliferation, increased in suprabasal layer of the EAC, and at the peripheral pars tensa. However, it decreased in the basal layer of the EAC, indicating hyperproliferation and migration of keratinocytes. The findings of this study support the basal cell hyperplasia hypotheses for the pathogenesis of aural cholesteatoma, with regard to hyperproliferation, migration, and an altered differentiation of keratinocytes. (+info)External auditory canal cholesteatoma: clinical and imaging spectrum. (6/94)
BACKGROUND AND PURPOSE: Cholesteatoma is an inflammatory lesion of the temporal bone that uncommonly involves the external auditory canal (EAC). In this large case series, we aimed to define its imaging features and to determine the characteristics most important to its clinical management. METHODS: Thirteen cases of EAC cholesteatoma (EACC) were retrospectively reviewed. Clinical data were reviewed for the history, presentation, and physical examination findings. High-resolution temporal bone CT scans were examined for a soft-tissue mass in the EAC, erosion of adjacent bone, and bone fragments in the mass. The middle ear cavity, mastoid, facial nerve canal, and tegmen tympani were evaluated for involvement. RESULTS: Patients presented with otorrhea, otalgia, or hearing loss. Eight cases were spontaneous, and five were postsurgical or post-traumatic. CT imaging in all 13 cases showed a soft-tissue mass with adjacent bone erosion. Intramural bone fragments were identified in seven cases. This mass most often arose inferiorly (n = 8) or posteriorly (n = 8), but it was circumferential in two cases. We noted middle ear extension (n = 5), mastoid involvement (n = 4), facial canal erosion (n = 2), and tegmen tympani dehiscence (n = 1). CONCLUSION: Temporal bone CT shows EACC as a soft-tissue mass within the EAC, with adjacent bone erosion. Bone fragments may be present within the mass. The cholesteatoma may extend into the mastoid or middle ear, or it may involve the facial nerve canal or tegmen tympani. Recognition of this entity and its possible extension is important because it may influence clinical management. (+info)Differential diagnosis and treatment of hearing loss. (7/94)
Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be categorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hearing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (+info)Closed tympanoplasty in middle ear cholesteatoma surgery. (8/94)
OBJECTIVE: To determine the effect of closed tympanoplasty surgery for middle ear cholesteatoma and to compare the postoperative results with the outcomes of canal-wall-down mastoidectomy. METHODS: Seventy patients with middle ear cholesteatoma were involved in the study. Pneumo-otoscopy, pure-tone audiometry, anamnestic and clinical data were evaluated before the surgery. Modified radical mastoidectomy was performed for 31 patients. Thirty-nine patients were treated with closed tympanoplasty surgery, including intact canal wall mastoidectomy, endaural atticotomy, lateral attic and aditus wall reconstruction and tympanoplasty. The follow-up examination was carried out 12 months after the surgery. The recurrence of cholesteatoma, otorrhea and hearing level were evaluated postoperatively. RESULTS: Otorrhea was estimated in 4 cases (10.3%) after closed tympanoplasty surgery and in 6 cases (19.4%) after modified radical mastoidectomy. Among the patients who were operated using closed tympanoplasty technique the middle ear cholesteatoma recurrence rate was 12.8% and among those, who underwent modified radical mastoidectomy recurrent disease occurred in 9.7% of the cases. The hearing improvement was found in 15 cases (38.46%) after closed tympanoplasty, while there was no hearing improvement after modified radical mastoidectomy. CONCLUSIONS: We conclude that despite the fact, that cholesteatoma recurrence rate after closed tympanoplasty is relatively high, this surgical method permits to preserve adequate hearing level and releases from postoperative cavity care problems as compared with modified radical mastoidectomy. (+info)Cholesteatoma, middle ear is a medical condition characterized by the abnormal growth of skin cells (keratinizing squamous epithelium) within the middle ear space. This skin cells accumulation forms a pearly, white, or gray mass that can erode and destroy surrounding structures such as the ossicles (the tiny bones in the middle ear), the mastoid process (a bony prominence behind the ear), and even the inner ear or brain.
Cholesteatomas can be congenital (present at birth) or acquired (develop later in life). Acquired cholesteatomas are more common and usually result from repeated middle ear infections that cause a retraction pocket of the eardrum, which then traps skin cells leading to their abnormal growth. Symptoms of cholesteatoma may include hearing loss, ear drainage, ear pain, vertigo, or facial weakness. Treatment typically involves surgical removal of the cholesteatoma and restoration of any damaged structures.
Cholesteatoma is a type of skin growth that occurs in the middle ear behind the eardrum. It is not a cancerous or precancerous growth but can still cause significant damage to the surrounding structures if left untreated. Cholesteatomas typically begin as small collections of dead skin cells, which then accumulate and expand over time, forming a sac-like structure that can erode the bones of the middle ear and lead to hearing loss, balance problems, and even facial paralysis in severe cases.
Cholesteatomas can be congenital (present at birth) or acquired (develop later in life). Acquired cholesteatomas are more common and typically result from repeated ear infections or trauma to the eardrum that causes a pocket or retraction of the eardrum to form, which then traps skin cells and debris. Over time, these cells can multiply and become a cholesteatoma.
Treatment for cholesteatoma typically involves surgical removal of the growth, as well as any damaged bone or tissue. In some cases, additional procedures may be necessary to restore hearing function. Regular follow-up care is also important to monitor for recurrence and ensure proper healing.
The middle ear is the middle of the three parts of the ear, located between the outer ear and inner ear. It contains three small bones called ossicles (the malleus, incus, and stapes) that transmit and amplify sound vibrations from the eardrum to the inner ear. The middle ear also contains the Eustachian tube, which helps regulate air pressure in the middle ear and protects against infection by allowing fluid to drain from the middle ear into the back of the throat.
The mastoid is a term used in anatomy and refers to the bony prominence located at the base of the skull, posterior to the ear. More specifically, it's part of the temporal bone, one of the bones that forms the side and base of the skull. The mastoid process provides attachment for various muscles involved in chewing and moving the head.
In a medical context, "mastoid" can also refer to conditions or procedures related to this area. For example, mastoiditis is an infection of the mastoid process, while a mastoidectomy is a surgical procedure that involves removing part or all of the mastoid process.
The ear ossicles are the three smallest bones in the human body, which are located in the middle ear. They play a crucial role in the process of hearing by transmitting and amplifying sound vibrations from the eardrum to the inner ear. The three ear ossicles are:
1. Malleus (hammer): The largest of the three bones, it is shaped like a hammer and connects to the eardrum.
2. Incus (anvil): The middle-sized bone, it looks like an anvil and connects the malleus to the stapes.
3. Stapes (stirrup): The smallest and lightest bone in the human body, it resembles a stirrup and transmits vibrations from the incus to the inner ear.
Together, these tiny bones work to efficiently transfer sound waves from the air to the fluid-filled cochlea of the inner ear, enabling us to hear.
Tympanoplasty is a surgical procedure performed to reconstruct or repair the tympanic membrane (eardrum) and/or the small bones of the middle ear (ossicles). The primary goal of this surgery is to restore hearing, but it can also help manage chronic middle ear infections, traumatic eardrum perforations, or cholesteatoma (a skin growth in the middle ear).
During the procedure, a surgeon may use various techniques such as grafting tissue from another part of the body to rebuild the eardrum or using prosthetic materials to reconstruct the ossicles. The choice of technique depends on the extent and location of the damage. Tympanoplasty is typically an outpatient procedure, meaning patients can return home on the same day of the surgery.
Ear diseases are medical conditions that affect the ear and its various components, including the outer ear, middle ear, and inner ear. These diseases can cause a range of symptoms, such as hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), ear pain, and discharge. Some common ear diseases include:
1. Otitis externa (swimmer's ear) - an infection or inflammation of the outer ear and ear canal.
2. Otitis media - an infection or inflammation of the middle ear, often caused by a cold or flu.
3. Cholesteatoma - a skin growth that develops in the middle ear behind the eardrum.
4. Meniere's disease - a disorder of the inner ear that can cause vertigo, hearing loss, and tinnitus.
5. Temporomandibular joint (TMJ) disorders - problems with the joint that connects the jawbone to the skull, which can cause ear pain and other symptoms.
6. Acoustic neuroma - a noncancerous tumor that grows on the nerve that connects the inner ear to the brain.
7. Presbycusis - age-related hearing loss.
Treatment for ear diseases varies depending on the specific condition and its severity. It may include medication, surgery, or other therapies. If you are experiencing symptoms of an ear disease, it is important to seek medical attention from a healthcare professional, such as an otolaryngologist (ear, nose, and throat specialist).
The ear canal, also known as the external auditory canal, is the tubular passage that extends from the outer ear (pinna) to the eardrum (tympanic membrane). It is lined with skin and tiny hairs, and is responsible for conducting sound waves from the outside environment to the middle and inner ear. The ear canal is typically about 2.5 cm long in adults and has a self-cleaning mechanism that helps to keep it free of debris and wax.
The tympanic membrane, also known as the eardrum, is a thin, cone-shaped membrane that separates the external auditory canal from the middle ear. It serves to transmit sound vibrations from the air to the inner ear, where they are converted into electrical signals that can be interpreted by the brain as sound. The tympanic membrane is composed of three layers: an outer layer of skin, a middle layer of connective tissue, and an inner layer of mucous membrane. It is held in place by several small bones and muscles and is highly sensitive to changes in pressure.
The ear is the sensory organ responsible for hearing and maintaining balance. It can be divided into three parts: the outer ear, middle ear, and inner ear. The outer ear consists of the pinna (the visible part of the ear) and the external auditory canal, which directs sound waves toward the eardrum. The middle ear contains three small bones called ossicles that transmit sound vibrations from the eardrum to the inner ear. The inner ear contains the cochlea, a spiral-shaped organ responsible for converting sound vibrations into electrical signals that are sent to the brain, and the vestibular system, which is responsible for maintaining balance.
Otoscopy is a medical examination procedure used to evaluate the external auditory canal and tympanic membrane (eardrum). It involves the use of an otoscope, a tool that consists of a lighted speculum attached to a handle. The speculum is inserted into the ear canal, allowing the healthcare provider to visualize and inspect the eardrum for any abnormalities such as perforations, inflammation, fluid accumulation, or foreign bodies. Otoscopy can help diagnose various conditions including ear infections, middle ear disorders, and hearing loss.
The temporal bone is a paired bone that is located on each side of the skull, forming part of the lateral and inferior walls of the cranial cavity. It is one of the most complex bones in the human body and has several important structures associated with it. The main functions of the temporal bone include protecting the middle and inner ear, providing attachment for various muscles of the head and neck, and forming part of the base of the skull.
The temporal bone is divided into several parts, including the squamous part, the petrous part, the tympanic part, and the styloid process. The squamous part forms the lateral portion of the temporal bone and articulates with the parietal bone. The petrous part is the most medial and superior portion of the temporal bone and contains the inner ear and the semicircular canals. The tympanic part forms the lower and anterior portions of the temporal bone and includes the external auditory meatus or ear canal. The styloid process is a long, slender projection that extends downward from the inferior aspect of the temporal bone and serves as an attachment site for various muscles and ligaments.
The temporal bone plays a crucial role in hearing and balance, as it contains the structures of the middle and inner ear, including the oval window, round window, cochlea, vestibule, and semicircular canals. The stapes bone, one of the three bones in the middle ear, is entirely encased within the petrous portion of the temporal bone. Additionally, the temporal bone contains important structures for facial expression and sensation, including the facial nerve, which exits the skull through the stylomastoid foramen, a small opening in the temporal bone.
Otitis media is an inflammation or infection of the middle ear. It can occur as a result of a cold, respiratory infection, or allergy that causes fluid buildup behind the eardrum. The buildup of fluid can lead to infection and irritation of the middle ear, causing symptoms such as ear pain, hearing loss, and difficulty balancing. There are two types of otitis media: acute otitis media (AOM), which is a short-term infection that can cause fever and severe ear pain, and otitis media with effusion (OME), which is fluid buildup in the middle ear without symptoms of infection. In some cases, otitis media may require medical treatment, including antibiotics or the placement of ear tubes to drain the fluid and relieve pressure on the eardrum.
Otitis media with effusion (OME), also known as serous otitis media or glue ear, is a medical condition characterized by the presence of fluid in the middle ear without signs or symptoms of acute ear infection. The fluid accumulation occurs due to the dysfunction of the Eustachian tube, which results in negative pressure and subsequent accumulation of sterile fluid within the middle ear space.
OME can lead to hearing difficulties, especially in children, as the fluid buildup impairs sound conduction through the ossicles in the middle ear. Symptoms may include mild hearing loss, tinnitus (ringing in the ears), and a sensation of fullness or pressure in the affected ear. In some cases, OME can resolve on its own within a few weeks or months; however, persistent cases might require medical intervention, such as placement of tympanostomy tubes (ear tubes) to drain the fluid and restore hearing.
Otologic surgical procedures refer to a range of surgeries performed on the ear or its related structures. These procedures are typically conducted by otologists, who are specialists trained in diagnosing and treating conditions that affect the ears, balance system, and related nerves. The goal of otologic surgery can vary from repairing damaged bones in the middle ear to managing hearing loss, tumors, or chronic infections. Some common otologic surgical procedures include:
1. Stapedectomy/Stapedotomy: These are procedures used to treat otosclerosis, a condition where the stapes bone in the middle ear becomes fixed and causes conductive hearing loss. The surgeon creates an opening in the stapes footplate (stapedotomy) or removes the entire stapes bone (stapedectomy) and replaces it with a prosthetic device to improve sound conduction.
2. Myringoplasty/Tympanoplasty: These are surgeries aimed at repairing damaged eardrums (tympanic membrane). A myringoplasty involves grafting a piece of tissue over the perforation in the eardrum, while a tympanoplasty includes both eardrum repair and reconstruction of the middle ear bones if necessary.
3. Mastoidectomy: This procedure involves removing the mastoid air cells, which are located in the bony prominence behind the ear. A mastoidectomy is often performed to treat chronic mastoiditis, cholesteatoma, or complications from middle ear infections.
4. Ossiculoplasty: This procedure aims to reconstruct and improve the function of the ossicles (middle ear bones) when they are damaged due to various reasons such as infection, trauma, or congenital conditions. The surgeon uses prosthetic devices made from plastic, metal, or even bone to replace or support the damaged ossicles.
5. Cochlear implantation: This is a surgical procedure that involves placing an electronic device inside the inner ear to help individuals with severe to profound hearing loss. The implant consists of an external processor and internal components that directly stimulate the auditory nerve, bypassing the damaged hair cells in the cochlea.
6. Labyrinthectomy: This procedure involves removing the balance-sensing structures (vestibular system) inside the inner ear to treat severe vertigo or dizziness caused by conditions like Meniere's disease when other treatments have failed.
7. Acoustic neuroma removal: An acoustic neuroma is a benign tumor that grows on the vestibulocochlear nerve, which connects the inner ear to the brain. Surgical removal of the tumor is necessary to prevent hearing loss, balance problems, and potential neurological complications.
These are just a few examples of the various surgical procedures performed by otolaryngologists (ear, nose, and throat specialists) to treat conditions affecting the ear and surrounding structures. Each procedure has its specific indications, benefits, risks, and postoperative care requirements. Patients should consult with their healthcare providers to discuss the most appropriate treatment options for their individual needs.
Suppurative Otitis Media is a type of inner ear infection that involves the accumulation of pus (suppuration) in the middle ear space. It can be caused by a bacterial or viral infection and often results from a previous episode of acute otitis media, where fluid builds up behind the eardrum (tympanic membrane).
Suppurative Otitis Media can lead to complications such as hearing loss, damage to the inner ear structures, and spread of infection to nearby areas like the mastoid process or the brain. Treatment typically involves antibiotics to clear the infection and sometimes surgical intervention to drain the pus and relieve pressure on the eardrum.
Middle ear ventilation refers to the normal process of air movement between the middle ear and the back of the nose (nasopharynx) through the eustachian tube. This tube is a narrow canal that connects the middle ear to the nasopharynx and helps to regulate air pressure in the middle ear, preventing its accumulation and subsequent negative pressure or fluid build-up, which can lead to conditions such as otitis media (middle ear infection) or serous otitis media (fluid in the middle ear).
The eustachian tube opens during activities such as swallowing, yawning, or chewing, allowing fresh air to enter the middle ear and any accumulated fluid or gas to be drained out. Abnormalities in middle ear ventilation can result from dysfunction of the eustachian tube, leading to various middle ear disorders.
Ear neoplasms refer to abnormal growths or tumors that occur in the ear. These growths can be benign (non-cancerous) or malignant (cancerous) and can affect any part of the ear, including the outer ear, middle ear, inner ear, and the ear canal.
Benign ear neoplasms are typically slow-growing and do not spread to other parts of the body. Examples include exostoses, osteomas, and ceruminous adenomas. These types of growths are usually removed surgically for cosmetic reasons or if they cause discomfort or hearing problems.
Malignant ear neoplasms, on the other hand, can be aggressive and may spread to other parts of the body. Examples include squamous cell carcinoma, basal cell carcinoma, and adenoid cystic carcinoma. These types of tumors often require more extensive treatment, such as surgery, radiation therapy, and chemotherapy.
It is important to note that any new growth or change in the ear should be evaluated by a healthcare professional to determine the nature of the growth and develop an appropriate treatment plan.
Conductive hearing loss is a type of hearing loss that occurs when there is a problem with the outer or middle ear. Sound waves are not able to transmit efficiently through the ear canal to the eardrum and the small bones in the middle ear, resulting in a reduction of sound that reaches the inner ear. Causes of conductive hearing loss may include earwax buildup, fluid in the middle ear, a middle ear infection, a hole in the eardrum, or problems with the tiny bones in the middle ear. This type of hearing loss can often be treated through medical intervention or surgery.
The inner ear is the innermost part of the ear that contains the sensory organs for hearing and balance. It consists of a complex system of fluid-filled tubes and sacs called the vestibular system, which is responsible for maintaining balance and spatial orientation, and the cochlea, a spiral-shaped organ that converts sound vibrations into electrical signals that are sent to the brain.
The inner ear is located deep within the temporal bone of the skull and is protected by a bony labyrinth. The vestibular system includes the semicircular canals, which detect rotational movements of the head, and the otolith organs (the saccule and utricle), which detect linear acceleration and gravity.
Damage to the inner ear can result in hearing loss, tinnitus (ringing in the ears), vertigo (a spinning sensation), and balance problems.
The Eustachian tube, also known as the auditory tube or pharyngotympanic tube, is a narrow canal that connects the middle ear cavity to the back of the nasopharynx (the upper part of the throat behind the nose). Its function is to maintain equal air pressure on both sides of the eardrum and to drain any fluid accumulation from the middle ear. The Eustachian tube is lined with mucous membrane and contains tiny hair-like structures called cilia that help to move mucus and fluid out of the middle ear. It opens and closes to regulate air pressure and drainage, which typically occurs during swallowing or yawning.
The incus, also known as the anvil, is one of the three smallest bones in the middle ear, located in the ossicular chain. It articulates with the malleus (hammer) and stapes (stirrup). The incus helps transmit and amplify sound vibrations from the eardrum to the inner ear.
## I am not aware of a medical definition for the term "chinchilla."
A chinchilla is actually a type of rodent that is native to South America. They have thick, soft fur and are often kept as exotic pets or used in laboratory research. If you're looking for information about chinchillas in a medical context, such as their use in research or any potential health concerns related to keeping them as pets, I would be happy to help you try to find more information on those topics.
Mastoiditis is a medical condition characterized by an infection and inflammation of the mastoid process, which is the bony prominence located behind the ear. The mastoid process contains air cells that are connected to the middle ear, and an infection in the middle ear (otitis media) can spread to the mastoid process, resulting in mastoiditis.
The symptoms of mastoiditis may include:
* Pain and tenderness behind the ear
* Swelling or redness of the skin behind the ear
* Ear drainage or discharge
* Fever and headache
* Hearing loss or difficulty hearing
Mastoiditis is a serious condition that requires prompt medical attention. Treatment typically involves antibiotics to eliminate the infection, as well as possible surgical intervention if the infection does not respond to medication or if it has caused significant damage to the mastoid process. If left untreated, mastoiditis can lead to complications such as meningitis, brain abscess, or even death.
Acoustic impedance tests are diagnostic procedures used to measure the impedance or resistance of various parts of the ear to sound waves. These tests are often used to assess hearing function and diagnose any issues related to the middle ear, such as fluid buildup or problems with the eardrum.
The most common type of acoustic impedance test is tympanometry, which measures the mobility of the eardrum and the middle ear system by creating variations in air pressure within the ear canal. During this test, a small probe is inserted into the ear canal, and sound waves are generated while the pressure is varied. The resulting measurements provide information about the condition of the middle ear and can help identify any issues that may be affecting hearing.
Another type of acoustic impedance test is acoustic reflex testing, which measures the body's natural response to loud sounds. This involves measuring the contraction of the stapedius muscle in the middle ear, which occurs in response to loud noises. By measuring the strength and timing of this reflex, audiologists can gain additional insights into the functioning of the middle ear and identify any abnormalities that may be present.
Overall, acoustic impedance tests are important tools for diagnosing hearing problems and identifying any underlying issues in the middle ear. They are often used in conjunction with other hearing tests to provide a comprehensive assessment of an individual's hearing function.
The external ear is the visible portion of the ear that resides outside of the head. It consists of two main structures: the pinna or auricle, which is the cartilaginous structure that people commonly refer to as the "ear," and the external auditory canal, which is the tubular passageway that leads to the eardrum (tympanic membrane).
The primary function of the external ear is to collect and direct sound waves into the middle and inner ear, where they can be converted into neural signals and transmitted to the brain for processing. The external ear also helps protect the middle and inner ear from damage by foreign objects and excessive noise.
The Malleus is one of the three smallest bones in the human body, also known as the hammer. It's part of the ossicles in the middle ear, which are responsible for transmitting sound waves from the air to the fluid-filled inner ear. The malleus connects to the eardrum and its base articulates with the incus (anvil), the second of the three ossicles. Together, these bones help amplify and transfer sound vibrations to the inner ear, where they are converted into electrical signals that can be interpreted by the brain as sound.
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
Cochlear diseases refer to conditions that affect the structure or function of the cochlea, which is a part of the inner ear responsible for hearing. These diseases can cause various types and degrees of hearing loss, ranging from mild to profound. Some common cochlear diseases include:
1. Cochlear otosclerosis: A condition where there is abnormal bone growth in the cochlea, which can lead to conductive or sensorineural hearing loss.
2. Cochlear Meniere's disease: A disorder that affects the inner ear and causes vertigo, tinnitus, and fluctuating hearing loss.
3. Cochlear damage due to exposure to loud noises: Prolonged or sudden exposure to loud noises can cause permanent cochlear damage and hearing loss.
4. Presbycusis: Age-related hearing loss that affects the cochlea and other structures of the auditory system.
5. Cochlear nerve tumors: Rare benign or malignant growths on the cochlear nerve can cause hearing loss, tinnitus, and balance problems.
6. Infections: Bacterial or viral infections such as meningitis, labyrinthitis, or otitis media can damage the cochlea and lead to hearing loss.
7. Ototoxicity: Certain medications can be toxic to the cochlea and cause hearing loss, tinnitus, or balance problems.
8. Genetic factors: Inherited genetic mutations can cause various types of cochlear diseases, such as connexin 26 deficiency, Waardenburg syndrome, or Usher syndrome.
It is important to note that early diagnosis and treatment of cochlear diseases can help prevent or minimize hearing loss and other complications.
The stapes is the smallest bone in the human body, which is a part of the middle ear. It is also known as the "stirrup" because of its U-shaped structure. The stapes connects the inner ear to the middle ear, transmitting sound vibrations from the ear drum to the inner ear. More specifically, it is the third bone in the series of three bones (the ossicles) that conduct sound waves from the air to the fluid-filled inner ear.
Proflavine is an antimicrobial agent, specifically a type of dye known as an acridine dye. It is used primarily as a topical antiseptic and disinfectant. Proflavine works by intercalating into DNA, which disrupts the structure of the DNA molecule and prevents bacterial replication.
It's important to note that proflavine has been largely replaced by other more effective and safer antimicrobial agents in clinical practice. It is still used in some research settings and for certain specific applications, such as staining tissues for microscopic examination.
Proflavine should be used with caution, as it can cause skin irritation and may have harmful effects if ingested or absorbed through the skin. As with any medication, it should only be used under the guidance of a healthcare professional.
Ossicular replacement is a surgical procedure in which the damaged or diseased ossicles (the three smallest bones in the middle ear, namely the malleus, incus, and stapes) are replaced with artificial prostheses. This procedure is often performed to correct hearing loss caused by various conditions such as chronic otitis media, cholesteatoma, or ossicular chain discontinuity.
The artificial prostheses used in ossicular replacement can be made of various materials, including ceramic, plastic, or metal. The choice of material depends on several factors, including the patient's individual needs and preferences, the size and shape of the remaining ossicles, and the surgeon's experience and preference.
The goal of ossicular replacement is to improve hearing by restoring the normal function of the ossicular chain, which is responsible for transmitting sound vibrations from the eardrum to the inner ear. By replacing the damaged or missing ossicles with artificial prostheses, the surgeon can help to restore the patient's ability to hear and communicate effectively.
Cerebrospinal fluid (CSF) otorrhea is a condition characterized by the leakage of cerebrospinal fluid from the inner ear into the external auditory canal of the ear. CSF is a clear, colorless fluid that surrounds and protects the brain and spinal cord. It is normally contained within the subarachnoid space, which is a space between the arachnoid membrane and the pia mater that surrounds the brain and spinal cord.
CSF otorrhea can occur as a result of a head injury, skull base fracture, or surgical procedure involving the ear or surrounding structures. It can also be caused by congenital defects or tumors in the area. CSF otorrhea is a serious condition that requires prompt medical attention, as it can lead to meningitis or other complications if left untreated.
Diagnosis of CSF otorrhea typically involves a physical examination and testing of any fluid draining from the ear for beta-2 transferrin, a protein that is present in CSF but not in other bodily fluids. Imaging studies such as CT or MRI scans may also be used to help identify the underlying cause of the CSF leak. Treatment may involve bed rest, hydration, and antibiotics to prevent infection. In some cases, surgery may be necessary to repair the site of the CSF leak.
"Second-look surgery" is a medical term that refers to a second surgical procedure performed after an initial operation, usually to evaluate the effectiveness of treatment or to check for any potential complications. This type of surgery is often used in cancer treatment, where it can help determine if the tumor has responded to chemotherapy or radiation therapy. During the second-look surgery, surgeons may remove additional tissue or tumor cells, or they may perform other procedures to manage any complications that have arisen since the first surgery.
It's worth noting that the use of second-look surgery is not always necessary or appropriate, and the decision to perform this type of procedure will depend on a variety of factors, including the patient's overall health, the type and stage of cancer, and the specific goals of treatment. As with any surgical procedure, there are risks associated with second-look surgery, and patients should discuss these risks thoroughly with their healthcare provider before making a decision about treatment.
An ossicular prosthesis is a medical device used to replace one or more of the small bones (ossicles) in the middle ear that are involved in hearing. These bones, known as the malleus, incus, and stapes, form a chain responsible for transmitting sound vibrations from the eardrum to the inner ear.
An ossicular prosthesis is typically made of biocompatible materials such as ceramic, plastic, or metal. The prosthesis is designed to bypass damaged or missing ossicles and reestablish the connection between the eardrum and the inner ear, thereby improving hearing function. Ossicular prostheses are often used in surgeries aimed at reconstructing the middle ear, such as tympanoplasty or stapedectomy, to treat various types of conductive hearing loss.
The stapedius is a small muscle in the middle ear. It is the smallest striated muscle in the human body, with a mass of about 0.6 mg. The stapedius muscle arises from a pyramidal eminence on the posterior wall of the tympanic cavity and inserts into the neck of the stapes (one of the three ossicles in the middle ear).
The main function of the stapedius muscle is to protect the inner ear from loud sounds. When contracted, it pulls the stapes away from the oval window, reducing its mobility and thus decreasing the transmission of sound vibrations to the inner ear. This reflex action, known as the stapedial reflex or acoustic reflex, helps to prevent damage to the inner ear from excessive noise levels.
The afferent limb of the stapedial reflex is carried by the vestibular branch of the vestibulocochlear nerve (cranial nerve VIII), while the efferent limb is mediated by the facial nerve (cranial nerve VII). The reflex can be elicited by loud sounds, vocalizations, or even mental arithmetic tasks.
Pure-tone audiometry is a hearing test that measures a person's ability to hear different sounds, pitches, or frequencies. During the test, pure tones are presented to the patient through headphones or ear inserts, and the patient is asked to indicate each time they hear the sound by raising their hand, pressing a button, or responding verbally.
The softest sound that the person can hear at each frequency is recorded as the hearing threshold, and a graph called an audiogram is created to show the results. The audiogram provides information about the type and degree of hearing loss in each ear. Pure-tone audiometry is a standard hearing test used to diagnose and monitor hearing disorders.
The middle cranial fossa is a depression or hollow in the skull that forms the upper and central portion of the cranial cavity. It is located between the anterior cranial fossa (which lies anteriorly) and the posterior cranial fossa (which lies posteriorly). The middle cranial fossa contains several important structures, including the temporal lobes of the brain, the pituitary gland, the optic chiasm, and the cavernous sinuses. It is also where many of the cranial nerves pass through on their way to the brain.
The middle cranial fossa can be further divided into two parts: the anterior and posterior fossae. The anterior fossa contains the optic chiasm and the pituitary gland, while the posterior fossa contains the temporal lobes of the brain and the cavernous sinuses.
The middle cranial fossa is formed by several bones of the skull, including the sphenoid bone, the temporal bone, and the parietal bone. The shape and size of the middle cranial fossa can vary from person to person, and abnormalities in its structure can be associated with various medical conditions, such as pituitary tumors or aneurysms.
Audiometry is the testing of a person's ability to hear different sounds, pitches, or frequencies. It is typically conducted using an audiometer, a device that emits tones at varying volumes and frequencies. The person being tested wears headphones and indicates when they can hear the tone by pressing a button or raising their hand.
There are two main types of audiometry: pure-tone audiometry and speech audiometry. Pure-tone audiometry measures a person's ability to hear different frequencies at varying volumes, while speech audiometry measures a person's ability to understand spoken words at different volumes and in the presence of background noise.
The results of an audiometry test are typically plotted on an audiogram, which shows the quietest sounds that a person can hear at different frequencies. This information can be used to diagnose hearing loss, determine its cause, and develop a treatment plan.
Echo-Planar Imaging (EPI) is a type of magnetic resonance imaging (MRI) technique that uses rapidly alternating magnetic field gradients and radiofrequency pulses to acquire multiple images in a very short period of time. This technique allows for the rapid acquisition of images, making it useful for functional MRI (fMRI) studies, diffusion-weighted imaging, and other applications where motion artifacts can be a problem.
In EPI, a single excitation pulse is followed by a series of gradient echoes that are acquired in a rapid succession, with each echo providing information about a different slice or plane of the object being imaged. The resulting images can then be combined to create a 3D representation of the object.
One of the key advantages of EPI is its speed, as it can acquire an entire brain volume in as little as 50 milliseconds. This makes it possible to capture rapid changes in the brain, such as those that occur during cognitive tasks or in response to neural activation. However, the technique can be susceptible to distortions and artifacts, particularly at higher field strengths, which can affect image quality and accuracy.
The round window ( membrana tympani rotunda) is a small, thin membrane-covered opening located in the inner ear between the middle ear and the cochlea. It serves as one of the two openings that lead into the cochlea, with the other being the oval window.
The round window's primary function is to help regulate and dampen the pressure changes within the cochlea that occur when sound waves reach the inner ear. This is accomplished through the movement of the fluid-filled spaces inside the cochlea (the scala vestibuli and scala tympani) caused by vibrations from the stapes bone, which connects to the oval window.
As the stapes bone moves in response to sound waves, it causes a corresponding motion in the perilymph fluid within the cochlea. This movement then creates pressure changes at the round window, causing it to bulge outward or move inward. The flexibility of the round window allows it to absorb and dissipate these pressure changes, which helps protect the delicate structures inside the inner ear from damage due to excessive pressure buildup.
It is important to note that any damage or dysfunction in the round window can negatively impact hearing ability and cause various hearing disorders.
The tensor tympani is a small muscle located in the middle ear of mammals. Its primary function is to tense and dampen the movement of the eardrum (tympanic membrane) in response to loud sounds, protecting the inner ear from potential damage. The tensor tympani is innervated by a branch of the trigeminal nerve (the mandibular nerve).
The term "tensor tympani" refers specifically to this muscle and its associated tendon. It comes from Latin: "tensor," meaning "to stretch or tense," and "tympani," referring to the eardrum or tympanic membrane. Thus, the tensor tympani is the muscle that tenses the eardrum.
Hearing is the ability to perceive sounds by detecting vibrations in the air or other mediums and translating them into nerve impulses that are sent to the brain for interpretation. In medical terms, hearing is defined as the sense of sound perception, which is mediated by the ear and interpreted by the brain. It involves a complex series of processes, including the conduction of sound waves through the outer ear to the eardrum, the vibration of the middle ear bones, and the movement of fluid in the inner ear, which stimulates hair cells to send electrical signals to the auditory nerve and ultimately to the brain. Hearing allows us to communicate with others, appreciate music and sounds, and detect danger or important events in our environment.
Bone conduction is a type of hearing mechanism that involves the transmission of sound vibrations directly to the inner ear through the bones of the skull, bypassing the outer and middle ears. This occurs when sound waves cause the bones in the skull to vibrate, stimulating the cochlea (the spiral cavity of the inner ear) and its hair cells, which convert the mechanical energy of the vibrations into electrical signals that are sent to the brain and interpreted as sound.
Bone conduction is a natural part of the hearing process in humans, but it can also be used artificially through the use of bone-conduction devices, such as hearing aids or headphones, which transmit sound vibrations directly to the skull. This type of transmission can provide improved hearing for individuals with conductive hearing loss, mixed hearing loss, or single-sided deafness, as it bypasses damaged or obstructed outer and middle ears.
Gerbillinae is a subfamily of rodents that includes gerbils, jirds, and sand rats. These small mammals are primarily found in arid regions of Africa and Asia. They are characterized by their long hind legs, which they use for hopping, and their long, thin tails. Some species have adapted to desert environments by developing specialized kidneys that allow them to survive on minimal water intake.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Haemophilus influenzae is a gram-negative, coccobacillary bacterium that can cause a variety of infectious diseases in humans. It is part of the normal respiratory flora but can become pathogenic under certain circumstances. The bacteria are named after their initial discovery in 1892 by Richard Pfeiffer during an influenza pandemic, although they are not the causative agent of influenza.
There are six main serotypes (a-f) based on the polysaccharide capsule surrounding the bacterium, with type b (Hib) being the most virulent and invasive. Hib can cause severe invasive diseases such as meningitis, pneumonia, epiglottitis, and sepsis, particularly in children under 5 years of age. The introduction of the Hib conjugate vaccine has significantly reduced the incidence of these invasive diseases.
Non-typeable Haemophilus influenzae (NTHi) strains lack a capsule and are responsible for non-invasive respiratory tract infections, such as otitis media, sinusitis, and exacerbations of chronic obstructive pulmonary disease (COPD). NTHi can also cause invasive diseases but at lower frequency compared to Hib.
Proper diagnosis and antibiotic susceptibility testing are crucial for effective treatment, as Haemophilus influenzae strains may display resistance to certain antibiotics.
The semicircular canals are part of the vestibular system in the inner ear that contributes to the sense of balance and spatial orientation. They are composed of three fluid-filled tubes, each located in a different plane (anterior, posterior, and horizontal) and arranged at approximately right angles to each other. The semicircular canals detect rotational movements of the head, enabling us to maintain our equilibrium during movement.
When the head moves, the fluid within the semicircular canals moves in response to that motion. At the end of each canal is a structure called the ampulla, which contains hair cells with hair-like projections (stereocilia) embedded in a gelatinous substance. As the fluid moves, it bends the stereocilia, stimulating the hair cells and sending signals to the brain via the vestibular nerve. The brain then interprets these signals to determine the direction and speed of head movement, allowing us to maintain our balance and orientation in space.
A fistula is an abnormal connection or passage between two organs, vessels, or body parts that usually do not connect. It can form as a result of injury, infection, surgery, or disease. A fistula can occur anywhere in the body but commonly forms in the digestive system, genital area, or urinary system. The symptoms and treatment options for a fistula depend on its location and underlying cause.
Diffusion Magnetic Resonance Imaging (MRI) is a non-invasive medical imaging technique that uses magnetic fields and radio waves to produce detailed images of the body's internal structures, particularly the brain and nervous system. In diffusion MRI, the movement of water molecules in biological tissues is measured and analyzed to generate contrast in the images based on the microstructural properties of the tissue.
Diffusion MRI is unique because it allows for the measurement of water diffusion in various directions, which can reveal important information about the organization and integrity of nerve fibers in the brain. This technique has been widely used in research and clinical settings to study a variety of neurological conditions, including stroke, traumatic brain injury, multiple sclerosis, and neurodegenerative diseases such as Alzheimer's disease.
In summary, diffusion MRI is a specialized type of MRI that measures the movement of water molecules in biological tissues to generate detailed images of the body's internal structures, particularly the brain and nervous system. It provides valuable information about the microstructural properties of tissues and has important applications in both research and clinical settings.
Optical imaging is a non-invasive medical imaging technique that uses light to capture images of internal structures and processes within the body. This method often involves the use of endoscopes, microscopes, or specialized cameras to visualize targeted areas, such as organs, tissues, or cells. Optical imaging can be used for various diagnostic and therapeutic purposes, including monitoring disease progression, guiding surgical procedures, and studying biological functions at the cellular level. Different optical imaging techniques include reflectance imaging, fluorescence imaging, bioluminescence imaging, and optical coherence tomography (OCT).
In summary, optical imaging is a versatile and non-ionizing medical imaging technique that utilizes light to visualize internal body structures and processes for diagnostic and therapeutic applications.
Skull neoplasms refer to abnormal growths or tumors that develop within the skull. These growths can be benign (non-cancerous) or malignant (cancerous). They can originate from various types of cells, such as bone cells, nerve cells, or soft tissues. Skull neoplasms can cause various symptoms depending on their size and location, including headaches, seizures, vision problems, hearing loss, and neurological deficits. Treatment options include surgery, radiation therapy, and chemotherapy. It is important to note that a neoplasm in the skull can also refer to metastatic cancer, which has spread from another part of the body to the skull.
 Ear
Ear
Koerner's septum
ICAM2
Muaaz Tarabichi
Hervé Vilard
Endoscopic ear surgery
Prussak's space
Tympanosclerosis
Mastoidectomy
Cholesteatoma
Columella (auditory system)
Middle ear implant
Facial nerve paralysis
Causes of hearing loss
High-resolution computed tomography
James Kennedy (musician)
Otitis media
List of patient-reported quality of life surveys
List of MeSH codes (C17)
Jacob Sadé
Tympanic membrane retraction
Conductive hearing loss
Otic polyp
Labyrinthine fistula
Mastoiditis
Eardrum
Ear canal
List of ICD-9 codes 320-389: diseases of the nervous system and sense organs
Glossary of communication disorders
Neurotology
Inner ear39
- Diseases of the inner ear can cause hearing loss and dizziness or vertigo, but they usually do not cause physical findings which can be photographed or seen. (entusa.com)
- It arises from the eardrum (TYMPANIC MEMBRANE) and grows into the MIDDLE EAR causing erosion of EAR OSSICLES and MASTOID that contains the INNER EAR. (childrensmercy.org)
- In mammals the ear is usually described as having three parts: the outer ear, the middle ear and the inner ear. (wikipedia.org)
- The human ear consists of three parts-the outer ear, middle ear and inner ear. (wikipedia.org)
- The inner ear contains the otolith organs-the utricle and saccule-and the semicircular canals belonging to the vestibular system, as well as the cochlea of the auditory system. (wikipedia.org)
- The middle ear lies between the outer ear and the inner ear. (wikipedia.org)
- The ossicles are three small bones that function together to receive, amplify, and transmit the sound from the eardrum to the inner ear. (wikipedia.org)
- The three ossicles transmit sound from the outer ear to the inner ear. (wikipedia.org)
- A cholesteatoma (kuh-less-tee-uh-TOE-muh) is a growth behind the eardrum, in the middle part of the ear where tiny bones relay sound waves from the eardrum to the inner ear. (kidshealth.org)
- As they grow, they can damage the neighboring structures of the middle ear and even the inner ear and/or brain if left untreated. (stanfordchildrens.org)
- Vertigo stems from a problem with the inner ear, brain, or sensory nerve pathway. (medicalnewstoday.com)
- People with an inner ear disorder, such as Ménière's disease, sometimes also experience vertigo. (medicalnewstoday.com)
- Vertigo can happen when a person looks down from a great height, but the actual term vertigo usually refers to any temporary or ongoing spells of dizziness due to problems in the inner ear or brain. (medicalnewstoday.com)
- Various conditions can lead to vertigo, which usually involves either an imbalance in the inner ear or a problem with the central nervous system (CNS) . (medicalnewstoday.com)
- This disorder can happen when an infection causes inflammation of the inner ear labyrinth. (medicalnewstoday.com)
- This disease causes a buildup of fluid in the inner ear, which can lead to attacks of vertigo with ringing in the ears and hearing loss. (medicalnewstoday.com)
- The ear has three main sections: the outer, middle, and inner ear. (medicalnewstoday.com)
- The eardrum separates the outer ear from the middle ear and helps to transmit sound vibrations to the inner ear. (medicalnewstoday.com)
- The cochlea is a small, curled tube full of liquid that sits in the inner ear. (medicalnewstoday.com)
- The inner ear contains the vestibular system, a part of the body that is largely responsible for spatial orientation and the coordination of movement as they relate to balance. (medicalnewstoday.com)
- Macrophage inflammatory proteins in cytomegalovirus-related inner ear injury. (medscape.com)
- Any disease affecting the eardrum or the three small ear bones may cause a conductive hearing loss by interfering with the transmission of sound to the inner ear. (stvincentmedicalcenter.com)
- Patients with otosclerosis typically have abnormal bone growth around the stapes bone, which must move freely to conduct sound through the middle ear to the inner ear as part of the hearing process. (hearingreview.com)
- In the surgery, they remove the immobilized stapes bone and replace it with a prosthetic device, allowing the bones in the middle ear to resume movement, stimulate fluid in the inner ear, and improve or restore hearing. (hearingreview.com)
- I have conductive hearing loss by the way…in both ears and both sides, the inner ear is totally fine. (hearingreview.com)
- I had prostetic bone replacement done in 2002 however I have had many infections and issues over the years in they middle ear to the point I became very sick and hospitalized after several CT scans the last 3 or 4 years my new ENT finally found my problem somehow the prosthesis went through the middle ear into the inner ear almost to the bone structure of the brain! (hearingreview.com)
- My question is how could this have happened that the prosthesis penetrated the inner ear unbelievable when you see it on the CT scan? (hearingreview.com)
- Or traumatic injuries to the ear abrasions or lacerations , auricular hematoma , traumatic perforation of the TM , disruption of the ossicles , hemotympanum ( blunt or barotrauma ), Basilar skull fracture , associated intracranial injury , Inner ear injury ( blunt or barotrauma ). (wikidoc.org)
- traumatic tympanic membrane perforation , traumatic disruption of the ossicles or inner ear [24] , Basilar skull fracture . (wikidoc.org)
- Inner ear microendoscopy and prosthesis design -- Developing techniques for minimally-invasive imaging of inner ear microanatomy and neural pysiology. (stanford.edu)
- Applications include improved cochlear implant development, inner ear regenerative techniques, inner ear surgery, and auditory physiology. (stanford.edu)
- Her clinical practice focuses on treating both adult and pediatric patients for a variety of middle and inner ear diseases. (yale.edu)
- When you hear sounds, they travel from your outer ear through your middle ear to your inner ear. (medel.com)
- The middle ear carries these sound waves as vibrations to your inner ear. (medel.com)
- Your inner ear turns these sound vibrations into nerve signals that your brain can understand as hearing. (medel.com)
- If there is a problem with your ear canal or the tiny bones (ossicles) in your middle ear, they cannot carry the sound vibrations to your inner ear (cochlea) as well as they should. (medel.com)
- If your child has a hearing loss, your audiologist will also likely test your child's inner ear hearing using a special bone conduction headset. (medel.com)
- Mixed hearing loss is a combination of conductive hearing loss and inner ear hearing loss (sensorineural hearing loss). (medel.com)
- The ear is divided into three parts: the outer, middle, and inner ear. (advocatehealth.com)
Infections39
- The child had highly resistant Streptococcus Pneumonia bacteria and the infection occurred because the standard antibiotics used to treat ear infections were ineffective. (entusa.com)
- Most cholesteatomas happen in kids who've had several ear infections . (kidshealth.org)
- Having a lot of ear infections can make the eardrum pull back into the middle ear space and form a pouch. (kidshealth.org)
- Larger cholesteatomas and those that happen after ear infections are more likely to grow back months or years after surgery. (kidshealth.org)
- Ear infections are more common in children because their eustachian tubes are shorter, narrower, and more horizontal than in adults. (medlineplus.gov)
- Chronic ear infections are much less common than acute ear infections. (medlineplus.gov)
- Chronic ear infections often respond to treatment. (medlineplus.gov)
- Chronic ear infections are not life threatening. (medlineplus.gov)
- Cholesteatomas can result from injury to the eardrum, chronic middle ear infections and/or chronic pressure buildup, which weakens the eardrum until a small pocket forms that stores trapped skin and debris. (stanfordchildrens.org)
- Cholesteatomas can also cause infections in the middle ear that, left untreated, sometimes spread to the brain. (stanfordchildrens.org)
- Infections can be treated with antibiotic ear drops or oral antibiotics as needed before and/or after surgery. (stanfordchildrens.org)
- Chronic ear infections: Dogs who have recurring ear infections are more likely to develop cholesteatoma. (petcarerx.com)
- Allergic reactions: Ear diseases cholesteatoma in dogs is frequently a symptom of a more serious condition, such as allergies or ear infections. (petcarerx.com)
- They may also prescribe an ear cleaner to use at home to avoid recurring infections. (petcarerx.com)
- Whether it's ear infections, a hearing issue, sinusitis, or speech and swallowing our otolaryngology and audiology teams can help. (guthrie.org)
- Cholesteatomas are typically caused by repeated ear infections or a tear in the eardrum, which allows skin cells to accumulate and form a cyst-like growth. (proprofs.com)
- Treatment of suppurative labyrinthitis is aimed at eradicating the underlying infection, providing supportive care to the patient, draining middle ear effusions or mastoid infections, and preventing the spread of infection. (medscape.com)
- Chronic ear infections are medically referred to as chronic otitis media, which means "infection of the middle ear. (stvincentmedicalcenter.com)
- They may also be called middle ear infections. (stvincentmedicalcenter.com)
- Symptoms of chronic ear infections depend upon whether the condition is active or inactive, whether or not there is involvement of the mastoid bone (the bone directly behind the ear) and whether or not there is a hole in the eardrum. (stvincentmedicalcenter.com)
- Middle ear infections often begin with an upper respiratory infection such as a cold or with allergies, which may cause inflammation of the sinuses and auditory tubes. (stvincentmedicalcenter.com)
- This is why children are more susceptible to recurrent ear infections. (stvincentmedicalcenter.com)
- Medical treatment of chronic ear infections frequently will stop ear drainage. (stvincentmedicalcenter.com)
- Ear infections ( otitis media ) are the most common infections requiring treatment in young children. (emedicinehealth.com)
- When a child experiences multiple ear infections, ear tubes (also called tympanostomy tubes, ventilation tubes, or PE [pressure equalization] tubes) may be recommended by an otolaryngologist. (emedicinehealth.com)
- The tube prevents many ear infections by allowing air in the middle ear to exchange freely with the outside air, preventing the formation of a vacuum in the middle ear. (emedicinehealth.com)
- Allergies or asthma , ear infections [32] (first ear infection before six months of age) [33] , and family history of ear infections . (wikidoc.org)
- Dr. Kennedy's research interests include middle ear cholesteatoma, temporal bone fractures, head and neck tumors, head and neck infections, as well as urban and rural outcomes. (choa.org)
- Often these children have a history of ear infections. (luriechildrens.org)
- A child with cholesteatoma may have a history of chronic or recurring ear infections with or without infected liquid draining into the ear canal. (luriechildrens.org)
- I will also be taking goldenseal root extract, which is a natural Antibiotic and recommended for middle ear, sinus infections and tinnitus, as well as olive leaf extract which is antifungal. (curezone.com)
- Eardrum perforations are caused by middle ear infections and injuries. (msdmanuals.com)
- When a perforation is present, people are at risk of chronic middle ear infections, which can cause ear discharge. (msdmanuals.com)
- A patient who needs a mastoidectomy will experience hearing loss, chronic ear infections, and possibly cholesteatoma-an abnormal skin growth in the middle ear. (watsi.org)
- Patients live with hearing loss and chronic ear infections. (watsi.org)
- This treatment will relieve chronic ear infections, hearing loss, and other symptoms caused by the infected mastoid bone. (watsi.org)
- This hearing loss can be temporary or chronic and can have many different causes, such as atresia, microtia, or middle ear infections. (medel.com)
- For children and adults, acquired conductive hearing loss can be caused by infections or disease of the middle ear. (medel.com)
- This can be facilitated in cases where the tympanic membrane has recovered from repeated middle ear infections and its resistance has decreased. (akouson.gr)
OSSICLES7
- The middle ear includes the tympanic cavity and the three ossicles. (wikipedia.org)
- The middle ear contains the three small bones-the ossicles-involved in the transmission of sound, and is connected to the throat at the nasopharynx, via the pharyngeal opening of the Eustachian tube. (wikipedia.org)
- A child whose middle ear bones (called ossicles) are damaged might need more surgery to improve hearing. (kidshealth.org)
- At the time of surgery, anything damaged by the cholesteatoma can be repaired, such as the eardrum or the little hearing bones called the ossicles. (stanfordchildrens.org)
- The Ear Organs of Hearing and Balance Anatomical Chart illustrates ear anatomy including right auricle, right tympanic membrane, middle ear, auditory ossicles, membranous labryinth, membranous. (anatomywarehouse.com)
- This vibration moves the ossicles, transmitting sound further into the ear. (medicalnewstoday.com)
- Cholesteatoma often involves the bone of hearing (ossicles) in the middle ear, even before there is hearing loss. (luriechildrens.org)
Congenital7
- Cholesteatoma can be classified as congenital, primary acquired, or secondary acquired. (medscape.com)
- Small congenital cholesteatomas can be completely removed and usually don't grow back. (kidshealth.org)
- Congenital cholesteatoma happens because sometimes skin cells are present inside the ear that slowly grows. (luriechildrens.org)
- Congenital cholesteatoma is uncommon. (luriechildrens.org)
- In newborns, congenital conductive hearing loss is generally caused by issues with the development of the outer or middle ear. (medel.com)
- Cholesteatoma can be either genetic, known as congenital cholesteatoma, or develop later in life, known as acquired cholesteatoma. (centuryearnosethroat.com)
- Developing congenital cholesteatoma is incredibly rare. (centuryearnosethroat.com)
Cyst12
- The cholesteatoma, strictly speaking a cyst and not a cancer, nevertheless shows expansive and destructive growth patterns that may give rise to serious symptoms and consequences, including fatality, not unlike those seen for malignant neoplasms. (thieme.com)
- A cholesteatoma is a skin cyst in the middle-ear made up of trapped skin cells and debris. (stanfordchildrens.org)
- Cholesteatomas often start as a small skin cyst (Image 1A) in the upper part of the eardrum, but with time can grow into the mastoid, the bony airspace behind the ear canal (Image 1B), as well as lower to involve the hearing bones. (stanfordchildrens.org)
- In this process, the veterinarian examines the ear canal for evidence of the presence of a cyst inside the ear using a specialized tool called an otoscope. (petcarerx.com)
- Dog ear cyst treatment is determined by the size and severity of the cyst. (petcarerx.com)
- Veterinarian consultation: If you feel your dog has an ear cyst, you must seek veterinary attention immediately. (petcarerx.com)
- Cleaning the Ear: If the cyst is minor, your veterinarian may simply wipe the ear to remove any debris or discharge. (petcarerx.com)
- Medication: Your veterinarian may recommend antibiotics or corticosteroids like Prednisone or Dexamethasone to treat the problem if the ear cyst is connected to an underlying infection or inflammation. (petcarerx.com)
- Surgical removal: If the ear cyst is big or intrusive, surgery may be required. (petcarerx.com)
- Fortunately, cholesteatoma presents as a non-cancerous cyst. (centuryearnosethroat.com)
- They can see the cholesteatoma, which often looks like a cyst made of skin cells or a mass of blood vessels. (centuryearnosethroat.com)
- The goal of the treatment is to reduce the chances of an infection occurring, reduce inflammation, and drain the ear of the cyst. (centuryearnosethroat.com)
Infection29
- This is an acute bacterial ear infection which is becoming harder to treat with antibiotics due to the rapidly emerging bacterial resistance. (entusa.com)
- The ear may be affected by disease, including infection and traumatic damage. (wikipedia.org)
- Chronic ear infection is fluid, swelling, or an infection behind the eardrum that does not go away or keeps coming back. (medlineplus.gov)
- A chronic ear infection develops when fluid or an infection behind the eardrum does not go away. (medlineplus.gov)
- Symptoms of a chronic ear infection may be less severe than symptoms of an acute infection. (medlineplus.gov)
- A CT scan of the head or mastoids may show that the infection has spread beyond the middle ear. (medlineplus.gov)
- Getting prompt treatment for an acute ear infection may reduce the risk of developing a chronic ear infection. (medlineplus.gov)
- Have a follow-up exam with your provider after an ear infection has been treated to make sure that it is completely cured. (medlineplus.gov)
- It can occur during pregnancy or as a symptom of an ear infection. (medicalnewstoday.com)
- This noncancerous skin growth develops in the middle ear, usually due to repeated infection. (medicalnewstoday.com)
- Treatment usually involves surgical removal of the cholesteatoma to prevent complications such as hearing loss, infection, or damage to the facial nerve. (proprofs.com)
- Infection or inflammation of the middle ear occurs when the eustachian tube to that ear is blocked. (stvincentmedicalcenter.com)
- Chronic ear infection occurs when the eustachian tube becomes blocked repeatedly or remains blocked for extended periods of time. (stvincentmedicalcenter.com)
- Pain and fullness in the ear are typical symptoms of an ear infection and are often accompanied by fever. (stvincentmedicalcenter.com)
- When an acute infection develops in the middle ear (an abscessed ear), the eardrum may rupture, resulting in a perforation. (stvincentmedicalcenter.com)
- When this trapped fluid becomes infected with bacteria, a middle ear infection is the result. (stvincentmedicalcenter.com)
- Treatment of ear infection is best left in the hands of your physician. (stvincentmedicalcenter.com)
- You should avoid blowing your nose in order to prevent any infection in your nose from spreading to the ear through the eustacian tube. (stvincentmedicalcenter.com)
- This tends to keep the infection from coming to the ear from the back of the nose and causing the ear infection . (emedicinehealth.com)
- The tube then allows the parent to insert medication directly to the site of the infection using antibiotic/steroid ear drops. (emedicinehealth.com)
- This is most often recommended if the patient has had previous ear tube placements or chronic nasal congestion, infection, or obstruction to breathing at night (apnea). (emedicinehealth.com)
- Initially treatment with antibiotics or ear drops may appear to help children with cholesteatoma who are thought to have only infection. (luriechildrens.org)
- Rarely, the first sign of cholesteatoma is weakness or paralysis of muscles that move one side of the face or infection that has spread to the brain. (luriechildrens.org)
- Looking to purchase an El Silverado Zapper in the hopes of it helping get rid of my middle ear infection/Eustachian tube dysfunction. (curezone.com)
- Otitis Media (Acute) Acute otitis media is a bacterial or viral infection of the middle ear. (msdmanuals.com)
- Ear Canal Infection (Swimmer's Ear) Bacteria and sometimes fungi can cause acute infection of the skin of the ear canal. (msdmanuals.com)
- Ear canal infection is caused by bacteria or, less commonly, fungi. (msdmanuals.com)
- One year ago, Ly suffered from an ear infection. (watsi.org)
- This infection caused a cholesteatoma, or abnormal skin growth, to develop in the middle ear behind the ear drum. (watsi.org)
Canal34
- Alternatively, cholesteatomas can be categorized according to location, which could be the external auditory canal, the middle ear cavity, and other pneumatized parts of the temporal bone.Clinically, patients present with foul-smelling otorrhea, earache, and hearing loss. (medscape.com)
- Canal wall-down operations have the highest probability of success with regard to treating cholesteatoma. (medscape.com)
- If the patient has had several episodes of recurrent cholesteatoma and wishes to avoid future operations, the canal wall-down technique is most applicable. (medscape.com)
- Osborn et al reported the results from 420 children who underwent 700 operations and concluded that most children with cholesteatoma can be managed with an intact-canal wall technique. (medscape.com)
- The outer ear consists of the pinna and the ear canal. (wikipedia.org)
- The ear canal of the outer ear is separated from the air-filled tympanic cavity of the middle ear by the eardrum. (wikipedia.org)
- The outer ear is the external portion of the ear and includes the fleshy visible pinna (also called the auricle), the ear canal, and the outer layer of the eardrum (also called the tympanic membrane). (wikipedia.org)
- The pinna consists of the curving outer rim called the helix, the inner curved rim called the antihelix, and opens into the ear canal. (wikipedia.org)
- The tragus protrudes and partially obscures the ear canal, as does the facing antitragus. (wikipedia.org)
- The hollow region in front of the ear canal is called the concha. (wikipedia.org)
- The ear canal stretches for about 1 inch (2.5 cm). (wikipedia.org)
- The skin surrounding the ear canal contains ceruminous and sebaceous glands that produce protective ear wax. (wikipedia.org)
- The ear canal ends at the external surface of the eardrum. (wikipedia.org)
- A view of a normal eardrum at the end of the ear canal (Image 2A) and the normal mastoid space behind the ear drum. (stanfordchildrens.org)
- Non-contrast-enhancing material is present in the right tympanic bulla, with markedly lytic changes affecting the ear canal (arrows) and adjacent brain. (avma.org)
- External sounds then enter a thin passage called the ear canal. (medicalnewstoday.com)
- In the event of ear drainage, the ear canal should be kept clean by means of a small cotton tipped applicator. (stvincentmedicalcenter.com)
- Cotton is placed in the outer ear to catch any discharge but should not be allowed to block the ear canal. (stvincentmedicalcenter.com)
- If a perforation is present, you should not allow water to get into your ear canal. (stvincentmedicalcenter.com)
- This may be avoided when showering or washing the hair by using an ear plug or placing cotton swabs or lambs wool in the external ear canal and covering it with a layer of vaseline. (stvincentmedicalcenter.com)
- The tumors kept returning because doctors couldn't see beyond the curves of her ear canal to remove the entire tumor. (ucf.edu)
- Before being recognized by the brain, sound waves enter the auditory canal, go through the eardrum, and then enter the middle ear. (healthline.com)
- The ear canal, also called the external acoustic meatus, is a passage comprised of bone and skin leading to the eardrum. (healthline.com)
- Normally skin is not present inside the ear, only lining the ear canal and outer surface of the ear drum. (luriechildrens.org)
- It occurs when skin from the eardrum or ear canal grows into the space behind the eardrum. (luriechildrens.org)
- Canal wall cholesteatoma is rare. (luriechildrens.org)
- It begins and usually only involves the ear canal. (luriechildrens.org)
- It is more common in children with very narrow ear canals but may occur within an ear canal of normal size. (luriechildrens.org)
- It also may be difficult for a physician to see because of the presence of fluid in the middle ear or ear canal. (luriechildrens.org)
- The ear canal passes through the base of the skull. (msdmanuals.com)
- Key Points Cerumen impaction is obstruction of the ear canal with ear wax. (advocatehealth.com)
- Insert a probe with a soft flexible tip in the ear canal to obtain a seal. (medscape.com)
- the probes are calibrated differently because of the significant difference in ear canal volume. (medscape.com)
- The smaller ear canal results in a higher effective sound pressure level (SPL), thus a different probe is used to correct for the difference. (medscape.com)
Eustachian tube6
- The middle ear also connects to the upper throat at the nasopharynx via the pharyngeal opening of the Eustachian tube. (wikipedia.org)
- The eustachian tube runs from the middle of each ear to the back of the throat. (medlineplus.gov)
- Pressure buildup can also be the result of a poorly functioning eustachian tube, the small opening that connects the middle ear to the nose and equalizes pressure in our ears. (stanfordchildrens.org)
- COME, often called glue ear, results from chronic eustachian tube dysfunction. (logicalimages.com)
- Sometimes when ear tubes are placed, the surgeon may recommend removal of the adenoid, an area of lymphoid tissue that is located behind the palate near the opening of the Eustachian tube. (emedicinehealth.com)
- Narghile (water-pipe) smoking requires the generation of significant negative intrapharyngeal pressure, which may be transmitted to the middle ear through the Eustachian tube. (who.int)
Tinnitus6
- Diseases of the ear may lead to hearing loss, tinnitus and balance disorders such as vertigo, although many of these conditions may also be affected by damage to the brain or neural pathways leading from the ear. (wikipedia.org)
- Apart from dizziness with vertigo, a person with labyrinthitis may experience hearing loss , tinnitus, headaches, ear pain, and vision changes. (medicalnewstoday.com)
- Chan HBY, Low D , Yuen HW, How CH. Tinnitus - ringing in the ears. (cgh.com.sg)
- If it fails to do so a hearing loss occurs, often associated with head noise (tinnitus) and intermittent or constant ear drainage. (stvincentmedicalcenter.com)
- I have read it has helped some people with tinnitus and ear aches, not to mention sleep, which is a big one for me as well. (curezone.com)
- Ear Ringing or Buzzing Ringing in the ears (tinnitus) is noise originating in the ear rather than in the environment. (msdmanuals.com)
Auditory4
- When the auditory tubes swell, fluid can become trapped in the middle ear behind the eardrum. (stvincentmedicalcenter.com)
- The small size of children's auditory tubes, which are shorter and more narrow than those of adults, increases the chance that inflammation will block the tube completely, trapping fluid in the middle ear. (stvincentmedicalcenter.com)
- This can be caused by problems during childhood, resulting in abnormal function of the auditory tube which leads to significantly reduced pressure in the middle ear and the mastoid antrum. (akouson.gr)
- Pure-tone (PT) audiometry measures throughout the outer ear, middle ear, cochlea, cranial nerve (CN) VIII, and central auditory system. (medscape.com)
Mastoiditis2
- CT scan of the middle ear showed bilateral cholesteatoma and mastoiditis. (cdc.gov)
- Mastoiditis and cholesteatoma are handled best with surgical drainage and debridement by way of a mastoidectomy. (medscape.com)
Mastoidectomy6
- The same view (Image 2B) after a mastoidectomy, which removes bone from the mastoid space in order to remove cholesteatoma. (stanfordchildrens.org)
- Other types of surgery depend on the extent of complications and include removal of infected ear tissue, repair of damaged ear structures, mastoidectomy, ossicular reconstruction, and tympanoplasty. (logicalimages.com)
- On May 9th, she will undergo a mastoidectomy on her right ear at Kien Khleang National Rehabilitation Centre. (watsi.org)
- Simple (or closed) mastoidectomy: The operation is performed through the ear or through an incision behind the ear. (watsi.org)
- Radical mastoidectomy: This procedure removes the most bone and is usually performed for extensive spread of a cholesteatoma. (watsi.org)
- Modified radical mastoidectomy: In this procedure, some middle ear bones are left in place, and the eardrum is rebuilt by tympanoplasty. (watsi.org)
Removal of the cholesteatoma1
- Surgical therapy consists of complete removal of the cholesteatoma. (medscape.com)
High sensitivity and specifi2
- DW MRI can also detect recurrent cholesteatoma with high sensitivity and specificity. (medscape.com)
- We have high sensitivity and specificity for cholesteatoma acquisition with Diffusion TSE. (philips.es)
Tumor5
- Cholesteatoma is a rare condition in dogs that involves the development of a benign tumor in the middle ear. (petcarerx.com)
- It is a particular kind of benign tumor that develops in the middle ear and manifests a variety of symptoms. (petcarerx.com)
- A cholesteatoma is a tumor that originates in the tissues of the eardrum. (proprofs.com)
- Today, she is tumor-free, thanks to a biomedical engineer who designed a special scope that, when inserted, allowed doctors to get a 180-degree view of her ear and better target the tumor. (ucf.edu)
- This growth of skin is where cholesteatoma gets its name, toma being the word for swelling or tumor. (centuryearnosethroat.com)
Otolaryngology1
- Although cholesteatoma is uncommon, we have otolaryngology physicians at Lurie Children's specializing in its diagnosis and treatment in children of all ages. (luriechildrens.org)
Temporal4
- A cholesteatoma , as shown in the images below, consists of an accumulation of desquamated keratin epithelium in the middle ear cleft or any other pneumatized portion of the temporal bone. (medscape.com)
- Because the major changes induced by a cholesteatoma in the temporal bone are produced within the bony framework, MRI has only a supportive role in the evaluation of subjacent extension of disease outside the confines of the temporal bone, intracranial extension, or rare vascular insult that may occur in large, chronic, or relapsing cases. (medscape.com)
- Post-operative healing and long-term stability after mastoid cavity reconstruction using the middle temporal artery and inferior musculoperiosteal flaps. (cgh.com.sg)
- A frequent and potentially dangerous condition that can occur in the middle ear and the mastoid antrum of the temporal bone is called a cholesteatoma. (akouson.gr)
Eardrum and middle ear2
- Loved all the visual aides (pictures of the eardrum and middle ear). (audiologyonline.com)
- The eardrum and middle ear structures may be completely removed. (watsi.org)
Bone6
- The great challenge of therapy is to eradicate the pathologic growth while preserving hearing and other critical functions of the middle ear and petrous bone, respecting the proximity of vital neural and vascular structures, and the intricate three-dimensional relationships involved. (thieme.com)
- Cholesteatoma can dissolve the bone over the facial nerve, which passes by the middle ear bones. (kidshealth.org)
- A diseased ear bone may be replaced by a plastic prosthesis (TORP or PORP), cartilage, or may be repositioned (relocated). (stvincentmedicalcenter.com)
- It is informally referred to as a hammer, owing to it being a hammer-shaped ossicle or small bone that is connected to the ear. (healthline.com)
- In 2018, he received a bone-anchored hearing aid which is a device that captures the sound and uses its physical attachments to the bone to generate the sounds in his head for his brain to interpret, as his ears are struggling to keep up from both his condition and a number of surgeries. (ablegamers.org)
- Treated incorrectly or left untreated, an infected mastoid bone can cause hearing loss, persistent ear discharge, meningitis, temporary dizziness, and temporary loss of taste. (watsi.org)
Sign of cholesteatoma1
- Ear discharge: A continuous and foul-smelling discharge from the ear is a typical sign of cholesteatoma in dogs. (petcarerx.com)
Benign2
- Imaging cholesteatoma, benign tumors of the middle ear, has been a huge challenge," says Dr. Heggelman. (philips.es)
- Cholesteatoma (pronounced co-les-tee-ah-tow-mah) is a benign growth that must be removed because it damages the ear and may cause serious complications. (luriechildrens.org)
Management of cholesteatomas1
- The applicability of using small otoendoscopes as part of the surgical management of cholesteatomas is being explored. (medscape.com)
Diseases3
- Imaging tests: To gain a closer look into the middle ear and confirm the presence of ear diseases cholesteatoma, X-rays or CT scans may be indicated. (petcarerx.com)
- The Department of Otorhinolaryngology/Head and Neck Surgery assesses pathology relating to diseases of the ears, nose and throat, and head and neck. (stvincents.ie)
- study found hearing loss among 13.7% of Clusters started at the level of districts and schoolchildren in Ismailia governorate [5], went down to apartments/place of residence but they used only tympanometry to test for which were considered the end-sampling middle ear diseases. (who.int)
Nose3
- Subscribe to a Mailing List for Ear, Nose & Throat Health Care Providers. (entusa.com)
- Evaluation for a cholesteatoma involves an examination of the eardrum by an Ear Nose and Throat specialist (Otolaryngologist). (stanfordchildrens.org)
- Also our ENT (ear, nose, throat) physicians are excited about the high resolution, the excellent lesion delineation and the sensitivity and specificity. (philips.es)
Complications4
- Ear tubes and complications of ear tubes. (entusa.com)
- Diagnosing cholesteatomas early can prevent many of the complications they can cause. (kidshealth.org)
- The equalization of the middle ear pressure prevents most of the complications to the eardrum that result from the formation of negative pressure in the middle ear. (emedicinehealth.com)
- If cholesteatoma is not removed, it may eventually cause serious complications including meningitis and facial nerve paralysis. (luriechildrens.org)
Structures5
- As it grows behind the eardrum, it can damage the middle ear's bony structures, leading to hearing loss and dizziness. (medicalnewstoday.com)
- It is a non-cancerous growth that can cause damage to the middle ear and surrounding structures if left untreated. (proprofs.com)
- it is passes through ear structures in all population and surgery carries the risk of injuring the facial nerve which causes facial paralysis. (hearingreview.com)
- Ear surgery always involves specializes techniques using either endoscopes and/or a microscope because magnification is necessary to see small structures well. (luriechildrens.org)
- How surgery is done depends upon the size of cholesteatoma and what ear spaces and structures are involved. (luriechildrens.org)
Remove cholesteatoma1
- Surgery is necessary to remove cholesteatoma. (luriechildrens.org)
Symptoms7
- As a result of this Continuing Education Activity, participants will be able to list the symptoms and signs of cholesteatoma. (audiologyonline.com)
- What Are the Signs & Symptoms of a Cholesteatoma? (kidshealth.org)
- present at birth) cholesteatoma can grow for years without causing symptoms. (kidshealth.org)
- Our ENT specialists can find the root of your ear issue by evaluating symptoms, performing tests and creating a treatment plan that's right for you. (guthrie.org)
- feel movable node behind 1 ear 1 cm diameter, been there 3 months.no other symptoms. (healthtap.com)
- Other children may have no symptoms at all, and cholesteatoma is found because a medical professional sees a white mass beneath the ear drum. (luriechildrens.org)
- Because of the severe side effects cholesteatoma might have, it's important for people to get checked out by a doctor should they have any symptoms or risk factors. (centuryearnosethroat.com)
Throat1
- These tubes connect the middle ear to the back of the throat. (medicalnewstoday.com)
Involves3
- If a skull fracture (from a severe head injury) involves that part of the skull, blood and/or cerebrospinal fluid may leak from the ear. (msdmanuals.com)
- Overview of hearing loss Hearing involves several steps as the sound passes from the ear to the brain. (advocatehealth.com)
- Treatment for cholesteatoma often involves surgery for severe cases. (centuryearnosethroat.com)
Facial2
- The ear muscles are supplied by the facial nerve, which also supplies sensation to the skin of the ear itself, as well as to the external ear cavity. (wikipedia.org)
- To innervate these muscles, the facial nerve courses across the region that eventually becomes the middle ear. (medscape.com)
Ossicular chain2
- The typical appearance of a cholesteatoma, with osteolysis of the ossicular chain of the middle ear. (radiopaedia.org)
- In cases of atticoantral disease, an inflammatory disease of the middle ear, the ossicular chain (malleus, incus, and stapes) is often affected by abnormal skin growth, called cholesteatoma. (healthline.com)
Diagnosis5
- To better educate pet owners about cholesteatoma in dogs and how to manage it, this article will go into further detail on the condition's signs, causes, diagnosis, and available treatments. (petcarerx.com)
- Biopsy: A biopsy may be performed to confirm the diagnosis of cholesteatoma. (petcarerx.com)
- The diagnosis of cholesteatoma is made by an otolaryngologist. (luriechildrens.org)
- RESULTS: Parameters that affected the postoperative integrity of TM were age, the time between diagnosis and surgery, the intraoperative status of the middle ear, and secondhand smoke exposure. (bvsalud.org)
- In light of our results, parameters to consider before surgery are age, the time between diagnosis and surgery, the intraoperative status of the middle ear, and secondhand smoke exposure. (bvsalud.org)
Skin growth in the middle1
- The doctor found a cholesteatoma, a skin growth in the middle ear, that he had cleared. (ablegamers.org)
Inflammation2
- Physical examination: The veterinarian will conduct a thorough physical examination, looking for any indications of inflammation, discharge, or abnormal growth in the ears. (petcarerx.com)
- We used to do CT, but then we were unsure if we were looking at an inflammation or a cholesteatoma. (philips.es)
Otitis media with effusion1
- Chronic otitis media is a condition that encompasses a group of chronic inflammatory conditions of the middle ear, including chronic suppurative otitis media (CSOM) and chronic otitis media with effusion (COME). (logicalimages.com)
Outer ear5
- Since the outer ear is the only visible portion of the ear in most animals, the word "ear" often refers to the external part alone. (wikipedia.org)
- Two sets of muscles are associated with the outer ear: the intrinsic and extrinsic muscles. (wikipedia.org)
- The great auricular nerve, auricular nerve, auriculotemporal nerve, and lesser and greater occipital nerves of the cervical plexus all supply sensation to parts of the outer ear and the surrounding skin. (wikipedia.org)
- The outer ear is the visible part, also known as the pinna. (medicalnewstoday.com)
- The outer ear "catches" sounds. (medel.com)
Fluid7
- With CT, it is difficult to differentiate a cholesteatoma from granulation tissue, pus, and fluid, which are present in chronic otitis media without the presence of a cholesteatoma. (medscape.com)
- A child with a cholesteatoma usually has fluid draining from the ear. (kidshealth.org)
- This tube drains fluid made in the middle ear. (medlineplus.gov)
- The tubes can alleviate hearing loss caused by the accumulation of fluid in the middle ear. (emedicinehealth.com)
- The fluid in the middle ear is then aspirated by suction, and the tympanostomy tube is placed in the opening. (emedicinehealth.com)
- This tube allows air to enter the ear and allows fluid to drain. (emedicinehealth.com)
- Sometimes cholesteatoma is found during minor surgery to place a pressure equalizer (PE) tube because it becomes visible when the ear is being cleaned and fluid removed. (luriechildrens.org)
Mastoid4
- The mastoid cavity is a group of air cells behind the ear. (entusa.com)
- Suppurative chronic otitis" is a term used to describe an eardrum that keeps rupturing, draining, or swelling in the middle ear or mastoid area and does not go away. (medlineplus.gov)
- This surgery removes the cholesteatoma from the eardrum and the space behind the eardrum, called the middle ear and mastoid. (stanfordchildrens.org)
- Cholesteatoma is skin that grows inside the ear including the middle ear (behind the ear drum), and mastoid (a space behind and connected to the middle ear). (luriechildrens.org)
Drainage2
- I am recovering but still have drainage and discomfort in the ear. (hearingreview.com)
- Ear discharge (otorrhea) is drainage from the ear. (msdmanuals.com)
Surgical5
- The ear has been adorned by earrings and other jewelry in numerous cultures for thousands of years, and has been subjected to surgical and cosmetic alterations. (wikipedia.org)
- Patterns of middle-ear cholesteatoma and implications for surgical approach. (cgh.com.sg)
- Conclusion: Hearing loss, which is a common way of Cholesteatoma revelation, should be systematically explored and properly treated by using different surgical techniques and prostheses when needed. (remedypublications.com)
- Cholesteatoma requires surgical removal. (luriechildrens.org)
- Surgical Simulation -- Developing immersive environment for simulation of ear and skull base surgery for training, technique assessment, and preoperative planning. (stanford.edu)
Antibiotic4
- If there is a hole in the eardrum, antibiotic ear drops are used. (medlineplus.gov)
- Measures include tympanostomy tube placement and regular aural toilet and quinolone antibiotic ear drops during times of otorrhea. (logicalimages.com)
- Treatment consists of careful cleaning of the ear and, at times, the application of antibiotic powder or eardrops. (stvincentmedicalcenter.com)
- Often antibiotic/steroid ear drops are inserted to prevent blood or secretions from clotting in the tube. (emedicinehealth.com)
Tympanic membrane pe1
- In secondary acquired cholesteatoma, a tympanic membrane perforation is seen in which the epithelium has migrated through the borders and already has reached the middle-ear space. (medscape.com)
Otosclerosis1
- University Hospitals Case Medical Center has announced that a new prosthesis has been developed for use in a traditional middle ear surgery-a stapedectomy -and has been successfully implanted in an otosclerosis patient. (hearingreview.com)
Recurrent1
- nonetheless, there is a risk of persistent and/or recurrent cholesteatomas. (medscape.com)
Hole in the eardrum1
- Such a hearing impairment may be due to a perforation (hole) in the eardrum, partial or total destruction of one or all of the three little ear bones, or scar tissue. (stvincentmedicalcenter.com)
Surgery14
- For example, the absence of hearing in the contralateral ear is a relative contraindication to surgery. (medscape.com)
- However, since cholesteatoma frequently presents a greater risk to residual hearing than surgery, removal usually remains the management option of choice in these clinical situations. (medscape.com)
- [ 35 ] A study by Hunter et al of pediatric patients with cholesteatoma, comparing total endoscopic ear surgery with microscopic surgery and combined endoscopic-microscopic procedures, found that results were similar between the endoscopic and microscopic techniques with regard to hearing outcomes, complication rates, recurrence, and residual disease rates. (medscape.com)
- Description The key reference dedicated to surgery for cholesteatoma. (thieme.com)
- A cholesteatoma is removed with surgery while the child is under general anesthesia . (kidshealth.org)
- Kids will need frequent ear exams and hearing tests for years after surgery to make sure the cholesteatoma doesn't happen again. (kidshealth.org)
- Cholesteatomas are removed with surgery, which is typically done under general anesthesia. (stanfordchildrens.org)
- It is often very difficult to remove all of the skin cells of the cholesteatoma in one surgery, therefore the process requires several procedures separated by months. (stanfordchildrens.org)
- Hearing can be restored or aided with amplification after surgery depending on the extent of damage from the cholesteatoma. (stanfordchildrens.org)
- Also determining if residual cholesteatoma exist after surgery or visualizing recurrence used to be very difficult. (philips.es)
- Cholesteatoma specimens were obtained from six patients undergoing middle ear surgery. (thieme-connect.com)
- Ly said: "After surgery, I will be able to hear and the ear discharge will stop. (watsi.org)
- The treatment of cholesteatoma often requires surgery to bring the ear back to health. (akouson.gr)
- Surgery is perhaps the best way to treat cholesteatomas that won't go away, which is, unfortunately, quite common. (centuryearnosethroat.com)
Abnormal1
- Abnormal growths usually present in the middle ear behind the eardrum. (centuryearnosethroat.com)
Drops3
- Ear drops and nasal spray don't appear to help. (curezone.com)
- Despite using ear drops, Ly has not seen any improvement in her condition, and now she has also developed polyps. (watsi.org)
- However, if caught early, it can be treated through a round of antibiotics, ear drops, and cleaning your ear carefully. (centuryearnosethroat.com)
Effusion2
- Middle ear effusion should be sent for microscopic evaluation, as well as culture and sensitivity. (medscape.com)
- AOM should not be diagnosed without evidence of middle ear effusion on pneumatic otoscopy or tympanometry. (aafp.org)
Hearing loss7
- Hearing loss from damage to the middle ear may slow language and speech development. (medlineplus.gov)
- Hearing loss: The tumor's growth may result in hearing loss in the ear that is being impacted. (petcarerx.com)
- In the United States, 1 in 8 people aged 12 years and older develops hearing loss in both ears. (medicalnewstoday.com)
- Hearing loss is sometimes the reason cholesteatoma is found. (luriechildrens.org)
- Some people also have ear discharge or, rarely, hearing loss. (msdmanuals.com)
- Cholesteatomas cause hearing loss and ear discharge. (watsi.org)
- Think of conductive hearing loss like wearing a pair of ear plugs. (medel.com)
Discharge3
- In June 2006, a 27-year-old immunocompetent man was hospitalized in Campinas (São Paulo, Brazil) for fever, cough with purulent bloody sputum, and discharge from and pain in both ears. (cdc.gov)
- Ear discharge culture grew Proteus mirabilis, sensitive to β-lactams, cephalosporins, and aminoglycosides. (cdc.gov)
- The causative agent may have been undetectable in ear discharge if it was overshadowed by a strain of P. mirabilis, a fastidious organism that also colonizes or co-infects this site. (cdc.gov)
Epithelium2
- A mass of KERATIN-producing squamous EPITHELIUM that resembles an inverted (suck-in) bag of skin in the MIDDLE EAR. (childrensmercy.org)
- In cholesteatoma epithelium, we found a fragmented basement membrane with small amounts of laminin and HSPG showing only occasional positively stained fragments while Collagen IV was almost completely absent. (thieme-connect.com)
Endoscopic1
- Objective: To correlate radiographic evidence of cholesteatoma in the retrotympanum with intraoperative endoscopic findings in cholesteatoma patients and to evaluate the clinical relevance of radiographic evidence of cholesteatoma in the retrotympanum. (researchgate.net)
Recurrence4
- Depending on the selected procedure, approximately 5-40% of cholesteatoma operations are unsuccessful, with cholesteatoma persistence or recurrence manifesting at some point in the postoperative period. (medscape.com)
- Increasing evidence suggests that diffusion-weighted MRI may be able to accurately detect cholesteatoma recurrence and, in some cases, replace a second-look procedure. (medscape.com)
- is the ultimate illustrated guide to complete management of the cholesteatoma, including assessment of the full expansion and degree of destruction caused by the growths, and short- and long-term follow-up to assess and treat for recurrence. (thieme.com)
- Often, two or more surgeries are required for removal and surveillance to check for recurrence of the cholesteatoma, and to rebuild the hearing, if possible. (stanfordchildrens.org)
Bones in the middle2
- The malleus is the outermost and largest of the three small bones in the middle ear, and reaches an average length of about eight millimeters in the typical adult. (healthline.com)
- The cholesteatoma will erode bones in the middle ear and can eventually expose the brain and cause death in complicated, untreated cases. (watsi.org)
Cochlea2
- Coronal high-resolution computed tomography scan shows a cholesteatoma in the posterior epitympanum (blue arrow), erosion of the scutum (white arrow), and rectification of the cochlea (red arrow). (medscape.com)
- The response only emanates from the cochlea, but the outer and middle ear must be able to transmit the emitted sound back to the recording microphone. (medscape.com)