Carcinoma, Squamous Cell
Carcinoma
Head and Neck Neoplasms
Carcinoma, Hepatocellular
Neoplasms, Squamous Cell
Carcinoma in Situ
Carcinoma, Basal Cell
Immunohistochemistry
Laryngeal Neoplasms
Carcinoma, Papillary
Tumor Markers, Biological
Prognosis
Neoplasm Staging
Gene Expression Regulation, Neoplastic
Carcinoma, Ductal, Breast
Lymphatic Metastasis
Carcinoma, Small Cell
Carcinoma, Bronchogenic
Carcinoma, Verrucous
Carcinoma, Transitional Cell
Tumor Cells, Cultured
Precancerous Conditions
Carcinoma, Adenoid Cystic
Neoplasm Recurrence, Local
Papillomavirus Infections
Neoplasm Proteins
Carcinoma, Intraductal, Noninfiltrating
Papillomaviridae
Carcinoma, Neuroendocrine
Retrospective Studies
Survival Rate
Mouth Mucosa
Mice, Nude
Carcinoma, Medullary
Immunoenzyme Techniques
Cisplatin
Survival Analysis
Carcinoma, Lobular
Neoplasm Metastasis
Combined Modality Therapy
Neoplasms, Multiple Primary
Tumor Suppressor Protein p53
Keratoacanthoma
Antigens, Neoplasm
Treatment Outcome
Reverse Transcriptase Polymerase Chain Reaction
Carcinoma, Mucoepidermoid
RNA, Messenger
Carcinoma, Large Cell
Papilloma
Keratins
Keratosis, Actinic
Neoplasm Transplantation
Disease Progression
Carcinoma, Non-Small-Cell Lung
Carcinoma, Basosquamous
Genes, p53
Neck Dissection
Carcinoma, Merkel Cell
Disease-Free Survival
Tissue Array Analysis
Carcinoma, Endometrioid
Case-Control Studies
Apoptosis
Gingival Neoplasms
Cell Transformation, Neoplastic
Receptor, Epidermal Growth Factor
Ovarian Neoplasms
Carcinoma, Embryonal
Leukoplakia, Oral
Follow-Up Studies
Esophagus
Loss of Heterozygosity
Biopsy
Cyclin-Dependent Kinase Inhibitor p16
Kaplan-Meier Estimate
Carcinoma, Ductal
Human papillomavirus 16
Adrenocortical Carcinoma
Mutation
Carcinoma, Signet Ring Cell
Fatal Outcome
Ki-67 Antigen
Blotting, Western
Risk Factors
Antineoplastic Combined Chemotherapy Protocols
Fluorouracil
Cell Division
Keratinocytes
Sensitivity and Specificity
Chromosomes, Human, Pair 3
Cervical Intraepithelial Neoplasia
Genes, Tumor Suppressor
Bowen's Disease
Tumor Suppressor Proteins
Tomography, X-Ray Computed
Gene Expression Profiling
Serpins
Gene Amplification
Leukoplakia
Neovascularization, Pathologic
Tumor Virus Infections
Palatal Neoplasms
Lymph Nodes
Down-Regulation
Base Sequence
Cadherins
Tumor Burden
Adenocarcinoma, Follicular
Otorhinolaryngologic Neoplasms
Tracheal Neoplasms
Signal Transduction
Vaginal Smears
Predictive Value of Tests
Xenograft Model Antitumor Assays
In Situ Hybridization
Neoplasms, Second Primary
Adenocarcinoma, Mucinous
Neoplasms, Experimental
Gene Expression
Neoplasm Grading
Carcinogens
4-Nitroquinoline-1-oxide
Embryonal Carcinoma Stem Cells
Up-Regulation
Multivariate Analysis
Radiotherapy, Adjuvant
Maxillary Sinus Neoplasms
Endometrial Neoplasms
Cyclin D1
Epithelium
alpha-Fetoproteins
Carcinoembryonic Antigen
Carcinosarcoma
Carcinoma, Papillary, Follicular
Hyperplasia
Oligonucleotide Array Sequence Analysis
Mucous Membrane
Pancreatic Neoplasms
Polymorphism, Single-Stranded Conformational
Colorectal Neoplasms
Skin
Cell Movement
Promoter Regions, Genetic
Alphapapillomavirus
In Situ Hybridization, Fluorescence
Transfection
Molecular Sequence Data
RNA, Small Interfering
Microsatellite Repeats
Adenocarcinoma, Clear Cell
DNA-Binding Proteins
Keratin-19
Neoplasms, Radiation-Induced
Keratin-5
Immunohistochemical expression of mdm2 and p21WAF1 in invasive cervical cancer: correlation with p53 protein and high risk HPV infection. (1/13224)
AIM: To investigate the immunocytochemical staining pattern of mdm2 and p21WAF1 proteins in invasive cervical cancer and to determine its relation with the expression of p53 and with the high risk HPV infection. METHODS: Immunocytochemistry for p53, mdm2, and p21WAF1 was performed in 31 paraffin embedded sections of invasive cervical cancer. The results were assessed by image analysis, evaluating for each protein the optical density of the immunostained area, scored as percentage of the total nuclear area. The presence of high risk human papillomavirus (HPV) infection was detected by using the polymerase chain reaction. RESULTS: Immunostaining for both mdm2 and p21WAF1 was correlated with p53 expression; however, the correlation between p53 and mdm2 (R = 0.49; p < 0.01) was more significant than between p53 and p21WAF1 (R = 0.31; p < 0.05); the less stringent correlation between p53 and p21WAF1 might reflect the p53 independent mechanisms of p21WAF1 induction. Similar average levels of p53, mdm2, and p21WAF1 immunostaining were found in the presence or absence of high risk HPV-DNA, without significant differences between the two groups. CONCLUSIONS: These data suggest that mdm2 and p21WAF1 proteins are expressed in invasive cervical cancer and that their immunocytochemical staining pattern is not abrogated by the presence of high risk HPV genomic sequences. (+info)Expression of vascular endothelial growth factor in human oral squamous cell carcinoma: its association with tumour progression and p53 gene status. (2/13224)
AIMS: To correlate vascular endothelial growth factor (VEGF) expression in oral squamous cell carcinoma with the clinicopathological characteristics and prognosis; and to assess whether p53 gene status is associated with VEGF expression in human cancers. METHODS: Tumour specimens from 45 patients with oral squamous cell carcinomas were examined. Expression of VEGF was determined using an immunohistochemical method, and a tumour was considered positive when more than 5% of the neoplastic cells showed VEGF immunoreactivity. The p53 gene status was screened using a polymerase chain reaction--single strand conformation polymorphism analysis. RESULTS: VEGF positive staining was detected in 19 (42.2%) of the 45 cases. VEGF immunoreactivity did not correlate with the histological degree of tumour differentiation, clinical stages, or lymph node metastasis. The patients with VEGF positive tumours had a significantly worse prognosis than those with VEGF negative tumours. The five year overall survival rate of the VEGF negative patients was 76.5%, as compared with 48.8% for the VEGF positive patients. No significant association between VEGF expression and the p53 gene status of the tumours was found. CONCLUSIONS: VEGF is a good prognostic indicator of the survival of patients with oral squamous cell carcinoma. The p53 gene status does not seem to be associated with VEGF expression in these cancers. (+info)Expression of extracellular matrix proteins in cervical squamous cell carcinoma--a clinicopathological study. (3/13224)
AIM: To evaluate the intracellular and peritumoral expression of matrix proteins in squamous cell carcinoma of the uterine cervix using immunohistochemistry. METHODS: 71 squamous cell carcinomas and 10 controls were stained for laminin, fibronectin, and collagen IV. Cytoplasmic staining in tumour cells and peritumoral deposition of matrix proteins were evaluated. The association between staining results and patient age, tumour stage, histological grade, and survival was studied. RESULTS: Positive cytoplasmic staining for laminin, fibronectin, and collagen IV was observed in 17 (23.9%), 27 (38%), and 10 (14.1%) cases, respectively. Staining for laminin was most pronounced in the invasive front of tumour islands, while for fibronectin and collagen IV it appeared to be diffuse. Peritumoral staining for laminin and collagen IV was detected in 12 cases (16.9%). Early stage (Ia1-Ia2) tumours were uniformly negative for all three proteins. Cytoplasmic staining for laminin correlated with positive staining for fibronectin and collagen IV, and with the presence of a peritumoral deposition of collagen IV and laminin. There was no correlation with any of the three markers between staining results and patient age, stage, grade, or survival. CONCLUSIONS: Expression of extracellular matrix proteins in some cervical squamous cell carcinomas might reflect the enhanced ability of these tumours to modify the peritumoral stroma. This ability seems to be absent in early stage tumours. The correlation between intracytoplasmic and peritumoral expression of matrix proteins supports the evidence of their synthesis by tumour cells. However, this property did not correlate with disease outcome in this study. (+info)Regulation and function of family 1 and family 2 UDP-glucuronosyltransferase genes (UGT1A, UGT2B) in human oesophagus. (4/13224)
Human UDP-glucuronosyltransferases (UGTs) are expressed in a tissue-specific fashion in hepatic and extrahepatic tissues [Strassburg, Manns and Tukey (1998) J. Biol. Chem. 273, 8719-8726]. Previous work suggests that these enzymes play a protective role in chemical carcinogenesis [Strassburg, Manns and Tukey (1997) Cancer Res. 57, 2979-2985]. In this study, UGT1 and UGT2 gene expression was investigated in human oesophageal epithelium and squamous-cell carcinoma in addition to the characterization of individual UGT isoforms using recombinant protein. UGT mRNA expression was characterized by duplex reverse transcriptase-PCR analysis and revealed the expression of UGT1A7, UGT1A8, UGT1A9 and UGT1A10 mRNAs. UGT1A1, UGT1A3, UGT1A4, UGT1A5 and UGT1A6 transcripts were not detected. UGT2 expression included UGT2B7, UGT2B10 and UGT2B15, but UGT2B4 mRNA was absent. UGT2 mRNA was present at significantly lower levels than UGT1 transcripts. This observation was in agreement with the analysis of catalytic activities in oesophageal microsomal protein, which was characterized by high glucuronidation rates for phenolic xenobiotics, all of which are classical UGT1 substrates. Whereas UGT1A9 was not regulated, differential regulation of UGT1A7 and UGT1A10 mRNA was observed between normal oesophageal epithelium and squamous-cell carcinoma. Expression and analysis in vitro of recombinant UGT1A7, UGT1A9, UGT1A10, UGT2B7 and UGT2B15 demonstrated that UGT1A7, UGT1A9 and UGT1A10 catalysed the glucuronidation of 7-hydroxybenzo(alpha)pyrene, as well as other environmental carcinogens, such as 2-hydroxyamino-1-methyl-6-phenylimidazo-(4, 5-beta)-pyridine. Although UGT1A9 was not regulated in the carcinoma tissue, the five-fold reduction in 7-hydroxybenzo(alpha)pyrene glucuronidation could be attributed to regulation of UGT1A7 and UGT1A10. These data elucidate an individual regulation of human UGT1A and UGT2B genes in human oesophagus and provide evidence for specific catalytic activities of individual human UGT isoforms towards environmental carcinogens that have been implicated in cellular carcinogenesis. (+info)Syndecan-1 expression has prognostic significance in head and neck carcinoma. (5/13224)
The syndecans are a family of cell-surface heparan sulphate proteoglycans that regulate cell behaviour by binding extracellular matrix molecules such as growth factors. The syndecan family has four members, of which syndecan-1 is the most studied and best characterized. We have studied the prognostic significance of syndecan-1 expression in squamous cell carcinoma (SCC) of the head and neck treated with surgery and post-operative radiotherapy. Paraffin-embedded tissue samples taken from 175 patients with primary SCC, followed up from 2 to 15 years after surgery, were studied for expression of syndecan-1 by immunohistochemistry. A low number (< or =50%, the median value) of syndecan-1-positive tumour cells was associated with low histological grade of differentiation (P<0.0001), a large primary tumour size (T1-2 vs. T3-4, P = 0.02), positive nodal status (NO vs. N1-3, P = 0.0006), and high clinical stage (stage I or II vs. III or IV, P<0.0001). Low syndecan-1 expression was also associated with unfavourable overall survival in a univariate analysis (P = 0.001). In a multivariate survival analysis, the clinical stage and syndecan-1 expression were the only independent prognostic factors. We conclude that syndecan-1 is a novel prognostic factor in SCC of the head and neck treated with surgery and post-operative radiotherapy. (+info)A possible involvement of aberrant expression of the FHIT gene in the carcinogenesis of squamous cell carcinoma of the uterine cervix. (6/13224)
To investigate involvement of an aberrant expression of the FHIT (fragile histidine triad) gene in the process of carcinogenesis and progression in cervical carcinoma, we examined its expression by the reverse transcriptase polymerase chain reaction (RT-PCR) and cDNA sequence method in 32 cervical invasive carcinomas (25 squamous cell carcinomas and seven adeno- or adenosquamous carcinomas) and 18 of its precursor lesions [four low-grade and 14 high-grade cervical intraepithelial neoplasias (CINs)]. We also examined a link between the occurrence of the aberrant expression and human papillomavirus (HPV). We detected the aberrant FHIT transcripts in 11 of 25 (44%) cervical invasive squamous cell carcinomas and in 5 of 14 (36%) high-grade CINs (CIN 2 or 3), whereas they were not found in seven non-squamous type and four low-grade CINs (CIN 1). The alteration patterns of the FHIT gene expression in high-grade CINs were virtually similar to those found in invasive carcinomas, such that the exons 5-7 were consistently deleted associated or unassociated with loss of the exon 4 and/or 8. The incidence of the aberrant expression was not related to the presence of HPV and its type. These data indicate that the aberrant expression of the FHIT gene is observed in precursor lesions of cervical carcinoma as well as invasive carcinomas, with its incidence not increasing with advance of clinical stage. Given the squamous cell type dominant expression, the aberrant expression may play a critical role in the generation of squamous cell carcinoma of the uterine cervix, but not the consequence of the progression of the cancer. (+info)Collagenase-3 (MMP-13) is expressed by tumor cells in invasive vulvar squamous cell carcinomas. (7/13224)
Collagenase-3 (MMP-13) is a human matrix metalloproteinase specifically expressed by invading tumor cells in squamous cell carcinomas (SCCs) of the head and neck. Here, we have further elucidated the role of MMP-13 in tumor invasion by examining its expression in invasive malignant tumors of the female genital tract. Using in situ hybridization, expression of MMP-13 mRNA was detected in 9 of 12 vulvar SCCs, primarily in tumor cells, but not in intact vulvar epithelium, in cervical SCCs (n = 12), or in endometrial (n = 11) or ovarian adenocarcinomas (n = 8). MMP-13 expression was especially abundant in vulvar carcinomas showing metastasis to lymph nodes and was associated with expression of membrane type 1 MMP by tumor cells and gelatinase-A (MMP-2) by stromal cells, as detected by immunohistochemistry. MMP-13 mRNAs were detected in 9 of 11 cell lines established from vulvar carcinomas and in 4 of 6 cell lines from cervical carcinomas, whereas endometrial (n = 10) and ovarian (n = 9) carcinoma cell lines were negative for MMP-13 mRNA. No correlation was detected between MMP-13 expression and p53 gene mutations in vulvar SCC cell lines. However, MMP-13 expression was detected in 5 of 6 vulvar and cervical SCC cell lines harboring HPV 16 or 68 DNA. These results show that MMP-13 is specifically expressed by malignantly transformed squamous epithelial cells, including vulvar SCC cells, and appears to serve as a marker for their invasive capacity. (+info)[3H]gemcitabine uptake by nucleoside transporters in a human head and neck squamous carcinoma cell line. (8/13224)
Cellular uptake of many chemotherapeutic nucleoside analogs is dependent on the activity of a family of nucleoside transport proteins located in the cell plasma membrane. In the present study, we examined the role of these transporters in the accumulation of gemcitabine by a human head and neck squamous carcinoma cell line. The uptake of [3H]gemcitibine was compared with that of [3H]uridine and [3H]formycin B in the parent cell line (HN-5a) and in a gemcitabine-resistant variant (GEM-8e). The HN-5a and GEM-8e cells were similar in their transport characteristics and expressed predominantly the es (equilibrative, inhibitor-sensitive) transporter subtype; less than 10% of the influx of [3H]formycin B or [3H]uridine was mediated by the ei (equilibrative inhibitor-resistant) system, and there was no evidence for Na+-dependent nucleoside transporters. [3H]Gemcitabine (10 microM) entered these cells via both the es and ei transporters with an initial rate of uptake similar to that seen with the use of [3H]formycin B or [3H]uridine. In addition, ATP-replete cells accumulated significantly less [3H]gemcitabine than did ATP-depleted cells, which is indicative of an active efflux mechanism for gemcitabine. These results show that gemcitabine is a substrate for both the es and ei nucleoside transporters of HN-5a and GEM-8e cells and that gemcitabine resistance of the GEM-8e cells cannot be attributed to changes in transporter activity. Further studies to define the characteristics of the putative efflux mechanism are clearly warranted because this system has the potential to significantly affect the clinical efficacy of gemcitabine. (+info)Squamous cell carcinoma is a type of skin cancer that begins in the squamous cells, which are flat, thin cells that form the outer layer of the skin (epidermis). It commonly occurs on sun-exposed areas such as the face, ears, lips, and backs of the hands. Squamous cell carcinoma can also develop in other areas of the body including the mouth, lungs, and cervix.
This type of cancer usually develops slowly and may appear as a rough or scaly patch of skin, a red, firm nodule, or a sore or ulcer that doesn't heal. While squamous cell carcinoma is not as aggressive as some other types of cancer, it can metastasize (spread) to other parts of the body if left untreated, making early detection and treatment important.
Risk factors for developing squamous cell carcinoma include prolonged exposure to ultraviolet (UV) radiation from the sun or tanning beds, fair skin, a history of sunburns, a weakened immune system, and older age. Prevention measures include protecting your skin from the sun by wearing protective clothing, using a broad-spectrum sunscreen with an SPF of at least 30, avoiding tanning beds, and getting regular skin examinations.
Carcinoma is a type of cancer that develops from epithelial cells, which are the cells that line the inner and outer surfaces of the body. These cells cover organs, glands, and other structures within the body. Carcinomas can occur in various parts of the body, including the skin, lungs, breasts, prostate, colon, and pancreas. They are often characterized by the uncontrolled growth and division of abnormal cells that can invade surrounding tissues and spread to other parts of the body through a process called metastasis. Carcinomas can be further classified based on their appearance under a microscope, such as adenocarcinoma, squamous cell carcinoma, and basal cell carcinoma.
Head and neck neoplasms refer to abnormal growths or tumors in the head and neck region, which can be benign (non-cancerous) or malignant (cancerous). These tumors can develop in various sites, including the oral cavity, nasopharynx, oropharynx, larynx, hypopharynx, paranasal sinuses, salivary glands, and thyroid gland.
Benign neoplasms are slow-growing and generally do not spread to other parts of the body. However, they can still cause problems if they grow large enough to press on surrounding tissues or structures. Malignant neoplasms, on the other hand, can invade nearby tissues and organs and may also metastasize (spread) to other parts of the body.
Head and neck neoplasms can have various symptoms depending on their location and size. Common symptoms include difficulty swallowing, speaking, or breathing; pain in the mouth, throat, or ears; persistent coughing or hoarseness; and swelling or lumps in the neck or face. Early detection and treatment of head and neck neoplasms are crucial for improving outcomes and reducing the risk of complications.
A mouth neoplasm refers to an abnormal growth or tumor in the oral cavity, which can be benign (non-cancerous) or malignant (cancerous). Malignant mouth neoplasms are also known as oral cancer. They can develop on the lips, gums, tongue, roof and floor of the mouth, inside the cheeks, and in the oropharynx (the middle part of the throat at the back of the mouth).
Mouth neoplasms can have various causes, including genetic factors, tobacco use, alcohol consumption, and infection with human papillomavirus (HPV). Symptoms may include a lump or thickening in the oral soft tissues, white or red patches, persistent mouth sores, difficulty swallowing or speaking, and numbness in the mouth. Early detection and treatment of mouth neoplasms are crucial for improving outcomes and preventing complications.
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer in adults. It originates from the hepatocytes, which are the main functional cells of the liver. This type of cancer is often associated with chronic liver diseases such as cirrhosis caused by hepatitis B or C virus infection, alcohol abuse, non-alcoholic fatty liver disease (NAFLD), and aflatoxin exposure.
The symptoms of HCC can vary but may include unexplained weight loss, lack of appetite, abdominal pain or swelling, jaundice, and fatigue. The diagnosis of HCC typically involves imaging tests such as ultrasound, CT scan, or MRI, as well as blood tests to measure alpha-fetoprotein (AFP) levels. Treatment options for Hepatocellular carcinoma depend on the stage and extent of the cancer, as well as the patient's overall health and liver function. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or liver transplantation.
Squamous cell neoplasms are abnormal growths or tumors that originate from squamous cells, which are flat, scale-like cells that make up the outer layer of the skin and the lining of mucous membranes. These neoplasms can be benign (noncancerous) or malignant (cancerous). When malignant, they are called squamous cell carcinomas.
Squamous cell carcinomas often develop in areas exposed to excessive sunlight or ultraviolet radiation, such as the skin, lips, and mouth. They can also occur in other areas of the body, including the cervix, anus, and lungs. Risk factors for developing squamous cell carcinoma include fair skin, a history of sunburns, exposure to certain chemicals or radiation, and a weakened immune system.
Symptoms of squamous cell carcinomas may include rough or scaly patches on the skin, a sore that doesn't heal, a wart-like growth, or a raised bump with a central depression. Treatment for squamous cell carcinomas typically involves surgical removal of the tumor, along with radiation therapy or chemotherapy in some cases. Early detection and treatment can help prevent the spread of the cancer to other parts of the body.
Esophageal neoplasms refer to abnormal growths in the tissue of the esophagus, which is the muscular tube that connects the throat to the stomach. These growths can be benign (non-cancerous) or malignant (cancerous). Malignant esophageal neoplasms are typically classified as either squamous cell carcinomas or adenocarcinomas, depending on the type of cell from which they originate.
Esophageal cancer is a serious and often life-threatening condition that can cause symptoms such as difficulty swallowing, chest pain, weight loss, and coughing. Risk factors for esophageal neoplasms include smoking, heavy alcohol consumption, gastroesophageal reflux disease (GERD), and Barrett's esophagus. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Carcinoma in situ is a medical term used to describe the earliest stage of cancer, specifically a type of cancer that begins in the epithelial tissue, which is the tissue that lines the outer surfaces of organs and body structures. In this stage, the cancer cells are confined to the layer of cells where they first developed and have not spread beyond that layer into the surrounding tissues or organs.
Carcinoma in situ can occur in various parts of the body, including the skin, cervix, breast, lung, prostate, bladder, and other areas. It is often detected through routine screening tests, such as Pap smears for cervical cancer or mammograms for breast cancer.
While carcinoma in situ is not invasive, it can still be a serious condition because it has the potential to develop into an invasive cancer if left untreated. Treatment options for carcinoma in situ may include surgery, radiation therapy, or other forms of treatment, depending on the location and type of cancer. It is important to consult with a healthcare provider to determine the best course of action for each individual case.
Carcinoma, basal cell is a type of skin cancer that arises from the basal cells, which are located in the lower part of the epidermis (the outermost layer of the skin). It is also known as basal cell carcinoma (BCC) and is the most common form of skin cancer.
BCC typically appears as a small, shiny, pearly bump or nodule on the skin, often in sun-exposed areas such as the face, ears, neck, hands, and arms. It may also appear as a scar-like area that is white, yellow, or waxy. BCCs are usually slow growing and rarely spread (metastasize) to other parts of the body. However, they can be locally invasive and destroy surrounding tissue if left untreated.
The exact cause of BCC is not known, but it is thought to be related to a combination of genetic and environmental factors, including exposure to ultraviolet (UV) radiation from the sun or tanning beds. People with fair skin, light hair, and blue or green eyes are at increased risk of developing BCC.
Treatment for BCC typically involves surgical removal of the tumor, along with a margin of healthy tissue. Other treatment options may include radiation therapy, topical chemotherapy, or photodynamic therapy. Prevention measures include protecting your skin from UV radiation by wearing protective clothing, using sunscreen, and avoiding tanning beds.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
Skin neoplasms refer to abnormal growths or tumors in the skin that can be benign (non-cancerous) or malignant (cancerous). They result from uncontrolled multiplication of skin cells, which can form various types of lesions. These growths may appear as lumps, bumps, sores, patches, or discolored areas on the skin.
Benign skin neoplasms include conditions such as moles, warts, and seborrheic keratoses, while malignant skin neoplasms are primarily classified into melanoma, squamous cell carcinoma, and basal cell carcinoma. These three types of cancerous skin growths are collectively known as non-melanoma skin cancers (NMSCs). Melanoma is the most aggressive and dangerous form of skin cancer, while NMSCs tend to be less invasive but more common.
It's essential to monitor any changes in existing skin lesions or the appearance of new growths and consult a healthcare professional for proper evaluation and treatment if needed.
Laryngeal neoplasms refer to abnormal growths or tumors in the larynx, also known as the voice box. These growths can be benign (non-cancerous) or malignant (cancerous). Laryngeal neoplasms can affect any part of the larynx, including the vocal cords, epiglottis, and the area around the vocal cords called the ventricle.
Benign laryngeal neoplasms may include papillomas, hemangiomas, or polyps. Malignant laryngeal neoplasms are typically squamous cell carcinomas, which account for more than 95% of all malignant laryngeal tumors. Other types of malignant laryngeal neoplasms include adenocarcinoma, sarcoma, and lymphoma.
Risk factors for developing laryngeal neoplasms include smoking, alcohol consumption, exposure to industrial chemicals, and a history of acid reflux. Symptoms may include hoarseness, difficulty swallowing, sore throat, ear pain, or a lump in the neck. Treatment options depend on the type, size, location, and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
Tongue neoplasms refer to abnormal growths or tumors that develop in the tongue tissue. These growths can be benign (non-cancerous) or malignant (cancerous).
Benign tongue neoplasms may include entities such as papillomas, fibromas, or granular cell tumors. They are typically slow growing and less likely to spread to other parts of the body.
Malignant tongue neoplasms, on the other hand, are cancers that can invade surrounding tissues and spread to other parts of the body. The most common type of malignant tongue neoplasm is squamous cell carcinoma, which arises from the thin, flat cells (squamous cells) that line the surface of the tongue.
Tongue neoplasms can cause various symptoms such as a lump or thickening on the tongue, pain or burning sensation in the mouth, difficulty swallowing or speaking, and unexplained bleeding from the mouth. Early detection and treatment are crucial for improving outcomes and preventing complications.
Carcinoma, papillary is a type of cancer that begins in the cells that line the glandular structures or the lining of organs. In a papillary carcinoma, the cancerous cells grow and form small finger-like projections, called papillae, within the tumor. This type of cancer most commonly occurs in the thyroid gland, but can also be found in other organs such as the lung, breast, and kidney. Papillary carcinoma of the thyroid gland is usually slow-growing and has a good prognosis, especially when it is diagnosed at an early stage.
Tumor markers are substances that can be found in the body and their presence can indicate the presence of certain types of cancer or other conditions. Biological tumor markers refer to those substances that are produced by cancer cells or by other cells in response to cancer or certain benign (non-cancerous) conditions. These markers can be found in various bodily fluids such as blood, urine, or tissue samples.
Examples of biological tumor markers include:
1. Proteins: Some tumor markers are proteins that are produced by cancer cells or by other cells in response to the presence of cancer. For example, prostate-specific antigen (PSA) is a protein produced by normal prostate cells and in higher amounts by prostate cancer cells.
2. Genetic material: Tumor markers can also include genetic material such as DNA, RNA, or microRNA that are shed by cancer cells into bodily fluids. For example, circulating tumor DNA (ctDNA) is genetic material from cancer cells that can be found in the bloodstream.
3. Metabolites: Tumor markers can also include metabolic products produced by cancer cells or by other cells in response to cancer. For example, lactate dehydrogenase (LDH) is an enzyme that is released into the bloodstream when cancer cells break down glucose for energy.
It's important to note that tumor markers are not specific to cancer and can be elevated in non-cancerous conditions as well. Therefore, they should not be used alone to diagnose cancer but rather as a tool in conjunction with other diagnostic tests and clinical evaluations.
Prognosis is a medical term that refers to the prediction of the likely outcome or course of a disease, including the chances of recovery or recurrence, based on the patient's symptoms, medical history, physical examination, and diagnostic tests. It is an important aspect of clinical decision-making and patient communication, as it helps doctors and patients make informed decisions about treatment options, set realistic expectations, and plan for future care.
Prognosis can be expressed in various ways, such as percentages, categories (e.g., good, fair, poor), or survival rates, depending on the nature of the disease and the available evidence. However, it is important to note that prognosis is not an exact science and may vary depending on individual factors, such as age, overall health status, and response to treatment. Therefore, it should be used as a guide rather than a definitive forecast.
Adenocarcinoma is a type of cancer that arises from glandular epithelial cells. These cells line the inside of many internal organs, including the breasts, prostate, colon, and lungs. Adenocarcinomas can occur in any of these organs, as well as in other locations where glands are present.
The term "adenocarcinoma" is used to describe a cancer that has features of glandular tissue, such as mucus-secreting cells or cells that produce hormones. These cancers often form glandular structures within the tumor mass and may produce mucus or other substances.
Adenocarcinomas are typically slow-growing and tend to spread (metastasize) to other parts of the body through the lymphatic system or bloodstream. They can be treated with surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these treatments. The prognosis for adenocarcinoma depends on several factors, including the location and stage of the cancer, as well as the patient's overall health and age.
Neoplasm staging is a systematic process used in medicine to describe the extent of spread of a cancer, including the size and location of the original (primary) tumor and whether it has metastasized (spread) to other parts of the body. The most widely accepted system for this purpose is the TNM classification system developed by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC).
In this system, T stands for tumor, and it describes the size and extent of the primary tumor. N stands for nodes, and it indicates whether the cancer has spread to nearby lymph nodes. M stands for metastasis, and it shows whether the cancer has spread to distant parts of the body.
Each letter is followed by a number that provides more details about the extent of the disease. For example, a T1N0M0 cancer means that the primary tumor is small and has not spread to nearby lymph nodes or distant sites. The higher the numbers, the more advanced the cancer.
Staging helps doctors determine the most appropriate treatment for each patient and estimate the patient's prognosis. It is an essential tool for communication among members of the healthcare team and for comparing outcomes of treatments in clinical trials.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
Liver neoplasms refer to abnormal growths in the liver that can be benign or malignant. Benign liver neoplasms are non-cancerous tumors that do not spread to other parts of the body, while malignant liver neoplasms are cancerous tumors that can invade and destroy surrounding tissue and spread to other organs.
Liver neoplasms can be primary, meaning they originate in the liver, or secondary, meaning they have metastasized (spread) to the liver from another part of the body. Primary liver neoplasms can be further classified into different types based on their cell of origin and behavior, including hepatocellular carcinoma, cholangiocarcinoma, and hepatic hemangioma.
The diagnosis of liver neoplasms typically involves a combination of imaging studies, such as ultrasound, CT scan, or MRI, and biopsy to confirm the type and stage of the tumor. Treatment options depend on the type and extent of the neoplasm and may include surgery, radiation therapy, chemotherapy, or liver transplantation.
A cell line that is derived from tumor cells and has been adapted to grow in culture. These cell lines are often used in research to study the characteristics of cancer cells, including their growth patterns, genetic changes, and responses to various treatments. They can be established from many different types of tumors, such as carcinomas, sarcomas, and leukemias. Once established, these cell lines can be grown and maintained indefinitely in the laboratory, allowing researchers to conduct experiments and studies that would not be feasible using primary tumor cells. It is important to note that tumor cell lines may not always accurately represent the behavior of the original tumor, as they can undergo genetic changes during their time in culture.
Neoplasm invasiveness is a term used in pathology and oncology to describe the aggressive behavior of cancer cells as they invade surrounding tissues and organs. This process involves the loss of cell-to-cell adhesion, increased motility and migration, and the ability of cancer cells to degrade the extracellular matrix (ECM) through the production of enzymes such as matrix metalloproteinases (MMPs).
Invasive neoplasms are cancers that have spread beyond the original site where they first developed and have infiltrated adjacent tissues or structures. This is in contrast to non-invasive or in situ neoplasms, which are confined to the epithelial layer where they originated and have not yet invaded the underlying basement membrane.
The invasiveness of a neoplasm is an important prognostic factor in cancer diagnosis and treatment, as it can indicate the likelihood of metastasis and the potential effectiveness of various therapies. In general, more invasive cancers are associated with worse outcomes and require more aggressive treatment approaches.
Oropharyngeal neoplasms refer to abnormal growths or tumors in the oropharynx, which is the middle part of the pharynx (throat) that includes the back one-third of the tongue, the soft palate, the side and back walls of the throat, and the tonsils. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Oropharyngeal cancer is a significant global health concern, with squamous cell carcinoma being the most common type of malignant neoplasm in this region. The primary risk factors for oropharyngeal cancers include tobacco use, alcohol consumption, and human papillomavirus (HPV) infection. Early detection and treatment are crucial for improving outcomes and survival rates.
Neoplastic gene expression regulation refers to the processes that control the production of proteins and other molecules from genes in neoplastic cells, or cells that are part of a tumor or cancer. In a normal cell, gene expression is tightly regulated to ensure that the right genes are turned on or off at the right time. However, in cancer cells, this regulation can be disrupted, leading to the overexpression or underexpression of certain genes.
Neoplastic gene expression regulation can be affected by a variety of factors, including genetic mutations, epigenetic changes, and signals from the tumor microenvironment. These changes can lead to the activation of oncogenes (genes that promote cancer growth and development) or the inactivation of tumor suppressor genes (genes that prevent cancer).
Understanding neoplastic gene expression regulation is important for developing new therapies for cancer, as targeting specific genes or pathways involved in this process can help to inhibit cancer growth and progression.
Uterine cervical neoplasms, also known as cervical cancer or cervical dysplasia, refer to abnormal growths or lesions on the lining of the cervix that have the potential to become cancerous. These growths are usually caused by human papillomavirus (HPV) infection and can be detected through routine Pap smears.
Cervical neoplasms are classified into different grades based on their level of severity, ranging from mild dysplasia (CIN I) to severe dysplasia or carcinoma in situ (CIN III). In some cases, cervical neoplasms may progress to invasive cancer if left untreated.
Risk factors for developing cervical neoplasms include early sexual activity, multiple sexual partners, smoking, and a weakened immune system. Regular Pap smears and HPV testing are recommended for early detection and prevention of cervical cancer.
Carcinoma, ductal, breast is a type of breast cancer that begins in the milk ducts (the tubes that carry milk from the lobules of the breast to the nipple). It is called "ductal" because it starts in the cells that line the milk ducts. Ductal carcinoma can be further classified as either non-invasive or invasive, based on whether the cancer cells are confined to the ducts or have spread beyond them into the surrounding breast tissue.
Non-invasive ductal carcinoma (also known as intraductal carcinoma or ductal carcinoma in situ) is a condition where abnormal cells have been found in the lining of the milk ducts, but they have not spread outside of the ducts. These cells have the potential to become invasive and spread to other parts of the breast or body if left untreated.
Invasive ductal carcinoma (IDC) is a type of breast cancer that starts in a milk duct and then grows into the surrounding breast tissue. From there, it can spread to other parts of the body through the bloodstream and lymphatic system. IDC is the most common form of breast cancer, accounting for about 80% of all cases.
Symptoms of ductal carcinoma may include a lump or thickening in the breast, changes in the size or shape of the breast, dimpling or puckering of the skin on the breast, nipple discharge (especially if it is clear or bloody), and/or redness or scaling of the nipple or breast skin. However, many cases of ductal carcinoma are detected through mammography before any symptoms develop.
Treatment for ductal carcinoma depends on several factors, including the stage and grade of the cancer, as well as the patient's overall health and personal preferences. Treatment options may include surgery (such as a lumpectomy or mastectomy), radiation therapy, chemotherapy, hormone therapy, and/or targeted therapies.
Lymphatic metastasis is the spread of cancer cells from a primary tumor to distant lymph nodes through the lymphatic system. It occurs when malignant cells break away from the original tumor, enter the lymphatic vessels, and travel to nearby or remote lymph nodes. Once there, these cancer cells can multiply and form new tumors, leading to further progression of the disease. Lymphatic metastasis is a common way for many types of cancer to spread and can have significant implications for prognosis and treatment strategies.
Carcinoma, small cell is a type of lung cancer that typically starts in the bronchi (the airways that lead to the lungs). It is called "small cell" because the cancer cells are small and appear round or oval in shape. This type of lung cancer is also sometimes referred to as "oat cell carcinoma" due to the distinctive appearance of the cells, which can resemble oats when viewed under a microscope.
Small cell carcinoma is a particularly aggressive form of lung cancer that tends to spread quickly to other parts of the body. It is strongly associated with smoking and is less common than non-small cell lung cancer (NSCLC), which accounts for about 85% of all lung cancers.
Like other types of lung cancer, small cell carcinoma may not cause any symptoms in its early stages. However, as the tumor grows and spreads, it can cause a variety of symptoms, including coughing, chest pain, shortness of breath, hoarseness, and weight loss. Treatment for small cell carcinoma typically involves a combination of chemotherapy, radiation therapy, and sometimes surgery.
Carcinoma, bronchogenic is a medical term that refers to a type of lung cancer that originates in the bronchi, which are the branching tubes that carry air into the lungs. It is the most common form of lung cancer and can be further classified into different types based on the specific cell type involved, such as squamous cell carcinoma, adenocarcinoma, or large cell carcinoma.
Bronchogenic carcinomas are often associated with smoking and exposure to environmental pollutants, although they can also occur in non-smokers. Symptoms may include coughing, chest pain, shortness of breath, wheezing, hoarseness, or unexplained weight loss. Treatment options depend on the stage and location of the cancer, as well as the patient's overall health and may include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these approaches.
Carcinoma, verrucous is a type of slow-growing, well-differentiated squamous cell carcinoma that has a exophytic, papillary, and warty appearance. It typically occurs in the oral cavity, larynx, and genital regions. The tumor often has a long clinical course and is locally invasive but has low potential for metastasis.
It's also known as Ackerman's tumor or Buschke-Lowenstein tumor when it occurs in the genital region. It can be caused by long-standing irritation, chronic inflammation, or infection with certain types of human papillomavirus (HPV). The diagnosis is usually made through a biopsy and imaging studies may be used to determine the extent of the tumor. Treatment typically involves surgical excision, but radiation therapy and chemotherapy may also be used in some cases.
Transitional cell carcinoma (TCC) is a type of cancer that develops in the transitional epithelium, which is the tissue that lines the inner surface of the urinary tract. This includes the renal pelvis, ureters, bladder, and urethra. Transitional cell carcinoma is the most common type of bladder cancer and can also occur in other parts of the urinary system.
Transitional cells are specialized epithelial cells that can stretch and change shape as the organs they line expand or contract. These cells normally have a flat, squamous appearance when at rest but become more cuboidal and columnar when the organ is full. Transitional cell carcinomas typically start in the urothelium, which is the innermost lining of the urinary tract.
Transitional cell carcinoma can be classified as non-invasive (also called papillary or superficial), invasive, or both. Non-invasive TCCs are confined to the urothelium and have not grown into the underlying connective tissue. Invasive TCCs have grown through the urothelium and invaded the lamina propria (a layer of connective tissue beneath the urothelium) or the muscle wall of the bladder.
Transitional cell carcinoma can also be categorized as low-grade or high-grade, depending on how abnormal the cancer cells look under a microscope and how likely they are to grow and spread. Low-grade TCCs tend to have a better prognosis than high-grade TCCs.
Treatment for transitional cell carcinoma depends on the stage and grade of the cancer, as well as other factors such as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or immunotherapy.
'Tumor cells, cultured' refers to the process of removing cancerous cells from a tumor and growing them in controlled laboratory conditions. This is typically done by isolating the tumor cells from a patient's tissue sample, then placing them in a nutrient-rich environment that promotes their growth and multiplication.
The resulting cultured tumor cells can be used for various research purposes, including the study of cancer biology, drug development, and toxicity testing. They provide a valuable tool for researchers to better understand the behavior and characteristics of cancer cells outside of the human body, which can lead to the development of more effective cancer treatments.
It is important to note that cultured tumor cells may not always behave exactly the same way as they do in the human body, so findings from cell culture studies must be validated through further research, such as animal models or clinical trials.
Adenosquamous carcinoma is a rare type of cancer that contains two types of cells: glandular (adeno) and squamous. This mixed composition leads to a unique microscopic appearance and more aggressive behavior compared to other types of carcinomas. Adenosquamous carcinoma can occur in various organs, such as the lung, pancreas, cervix, and skin.
The glandular (adeno) component is made up of columnar epithelial cells that form glands or tubular structures. These cells produce mucus or other secretions. The squamous component consists of flat, scale-like cells that resemble the cells found in the outer layer of the skin.
The presence of both adeno and squamous components in a single tumor can lead to more rapid growth, increased likelihood of metastasis (spreading to other parts of the body), and poorer prognosis compared to carcinomas with only one cell type. Treatment typically involves surgical resection, radiation therapy, chemotherapy, or a combination of these approaches, depending on the location and stage of the cancer.
A precancerous condition, also known as a premalignant condition, is a state of abnormal cellular growth and development that has a higher-than-normal potential to progress into cancer. These conditions are characterized by the presence of certain anomalies in the cells, such as dysplasia (abnormal changes in cell shape or size), which can indicate an increased risk for malignant transformation.
It is important to note that not all precancerous conditions will eventually develop into cancer, and some may even regress on their own. However, individuals with precancerous conditions are often at a higher risk of developing cancer compared to the general population. Regular monitoring and appropriate medical interventions, if necessary, can help manage this risk and potentially prevent or detect cancer at an early stage when it is more treatable.
Examples of precancerous conditions include:
1. Dysplasia in the cervix (cervical intraepithelial neoplasia or CIN)
2. Atypical ductal hyperplasia or lobular hyperplasia in the breast
3. Actinic keratosis on the skin
4. Leukoplakia in the mouth
5. Barrett's esophagus in the digestive tract
Regular medical check-ups, screenings, and lifestyle modifications are crucial for individuals with precancerous conditions to monitor their health and reduce the risk of cancer development.
Adenoid cystic carcinoma (AdCC) is a rare type of cancer that can occur in various glands and tissues of the body, most commonly in the salivary glands. AdCC is characterized by its slow growth and tendency to spread along nerves. It typically forms solid, cystic, or mixed tumors with distinct histological features, including epithelial cells arranged in tubular, cribriform, or solid patterns.
The term "carcinoma" refers to a malignant tumor originating from the epithelial cells lining various organs and glands. In this case, adenoid cystic carcinoma is a specific type of carcinoma that arises in the salivary glands or other glandular tissues.
The primary treatment options for AdCC include surgical resection, radiation therapy, and sometimes chemotherapy. Despite its slow growth, adenoid cystic carcinoma has a propensity to recur locally and metastasize to distant sites such as the lungs, bones, and liver. Long-term follow-up is essential due to the risk of late recurrences.
Local neoplasm recurrence is the return or regrowth of a tumor in the same location where it was originally removed or treated. This means that cancer cells have survived the initial treatment and started to grow again in the same area. It's essential to monitor and detect any local recurrence as early as possible, as it can affect the prognosis and may require additional treatment.
Papillomavirus infections are a group of diseases caused by various types of human papillomaviruses (HPVs). These viruses infect the skin and mucous membranes, and can cause benign growths such as warts or papillomas, as well as malignant growths like cervical cancer.
There are more than 100 different types of HPVs, and they can be classified into low-risk and high-risk types based on their potential to cause cancer. Low-risk HPV types, such as HPV-6 and HPV-11, commonly cause benign genital warts and respiratory papillomas. High-risk HPV types, such as HPV-16 and HPV-18, are associated with an increased risk of developing cancer, including cervical, anal, penile, vulvar, and oropharyngeal cancers.
HPV infections are typically transmitted through sexual contact, and most sexually active individuals will acquire at least one HPV infection during their lifetime. In many cases, the immune system is able to clear the virus without any symptoms or long-term consequences. However, persistent high-risk HPV infections can lead to the development of cancer over time.
Prevention measures for HPV infections include vaccination against high-risk HPV types, safe sex practices, and regular screening for cervical cancer in women. The HPV vaccine is recommended for both boys and girls aged 11-12 years old, and can also be given to older individuals up to age 45 who have not previously been vaccinated or who have not completed the full series of shots.
A neoplasm is a tumor or growth that is formed by an abnormal and excessive proliferation of cells, which can be benign or malignant. Neoplasm proteins are therefore any proteins that are expressed or produced in these neoplastic cells. These proteins can play various roles in the development, progression, and maintenance of neoplasms.
Some neoplasm proteins may contribute to the uncontrolled cell growth and division seen in cancer, such as oncogenic proteins that promote cell cycle progression or inhibit apoptosis (programmed cell death). Others may help the neoplastic cells evade the immune system, allowing them to proliferate undetected. Still others may be involved in angiogenesis, the formation of new blood vessels that supply the tumor with nutrients and oxygen.
Neoplasm proteins can also serve as biomarkers for cancer diagnosis, prognosis, or treatment response. For example, the presence or level of certain neoplasm proteins in biological samples such as blood or tissue may indicate the presence of a specific type of cancer, help predict the likelihood of cancer recurrence, or suggest whether a particular therapy will be effective.
Overall, understanding the roles and behaviors of neoplasm proteins can provide valuable insights into the biology of cancer and inform the development of new diagnostic and therapeutic strategies.
Vulvar neoplasms refer to abnormal growths or tumors in the vulvar region, which is the exterior female genital area including the mons pubis, labia majora, labia minora, clitoris, and the vaginal vestibule. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign vulvar neoplasms may include conditions such as vulvar cysts, fibromas, lipomas, or condylomas (genital warts). They are typically slow-growing and less likely to spread or invade surrounding tissues.
Malignant vulvar neoplasms, on the other hand, are cancers that can invade nearby tissues and potentially metastasize (spread) to distant parts of the body. The most common types of malignant vulvar neoplasms are squamous cell carcinoma, vulvar melanoma, and adenocarcinoma.
Early detection and treatment of vulvar neoplasms are essential for improving prognosis and reducing the risk of complications or recurrence. Regular gynecological examinations, self-examinations, and prompt attention to any unusual symptoms or changes in the vulvar area can help ensure timely diagnosis and management.
Intraductal carcinoma, noninfiltrating is a medical term used to describe a type of breast cancer that is confined to the milk ducts of the breast. It is also sometimes referred to as ductal carcinoma in situ (DCIS). Noninfiltrating means that the cancer cells have not spread beyond the ducts into the surrounding breast tissue or elsewhere in the body.
In this type of cancer, abnormal cells line the milk ducts and fill the inside of the ducts. These abnormal cells may look like cancer cells under a microscope, but they have not grown through the walls of the ducts into the surrounding breast tissue. However, if left untreated, noninfiltrating intraductal carcinoma can progress to an invasive form of breast cancer where the cancer cells spread beyond the milk ducts and invade the surrounding breast tissue.
It is important to note that while noninfiltrating intraductal carcinoma is considered a precancerous condition, it still requires medical treatment to prevent the development of invasive breast cancer. Treatment options may include surgery, radiation therapy, or hormone therapy, depending on the size and location of the tumor and other individual factors.
Nasopharyngeal neoplasms refer to abnormal growths or tumors in the nasopharynx, which is the upper part of the pharynx (throat) behind the nose. These growths can be benign (non-cancerous) or malignant (cancerous).
Malignant nasopharyngeal neoplasms are often referred to as nasopharyngeal carcinoma or cancer. There are different types of nasopharyngeal carcinomas, including keratinizing squamous cell carcinoma, non-keratinizing carcinoma, and basaloid squamous cell carcinoma.
The risk factors for developing nasopharyngeal neoplasms include exposure to the Epstein-Barr virus (EBV), consumption of certain foods, smoking, and genetic factors. Symptoms may include a lump in the neck, nosebleeds, hearing loss, ringing in the ears, and difficulty swallowing or speaking. Treatment options depend on the type, size, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
Papillomaviridae is a family of small, non-enveloped DNA viruses that primarily infect the epithelial cells of mammals, birds, and reptiles. The name "papillomavirus" comes from the Latin word "papilla," which means nipple or small projection, reflecting the characteristic wart-like growths (papillomas) that these viruses can cause in infected host tissues.
The family Papillomaviridae includes more than 200 distinct papillomavirus types, with each type being defined by its specific DNA sequence. Human papillomaviruses (HPVs), which are the most well-studied members of this family, are associated with a range of diseases, from benign warts and lesions to malignant cancers such as cervical, anal, penile, vulvar, and oropharyngeal cancers.
Papillomaviruses have a circular, double-stranded DNA genome that is approximately 8 kbp in size. The viral genome encodes several early (E) proteins involved in viral replication and oncogenesis, as well as late (L) proteins that form the viral capsid. The life cycle of papillomaviruses is tightly linked to the differentiation program of their host epithelial cells, with productive infection occurring primarily in the differentiated layers of the epithelium.
In summary, Papillomaviridae is a family of DNA viruses that infect epithelial cells and can cause a variety of benign and malignant diseases. Human papillomaviruses are a significant public health concern due to their association with several cancer types.
Carcinoma, neuroendocrine is a type of cancer that arises from the neuroendocrine cells, which are specialized cells that have both nerve and hormone-producing functions. These cells are found throughout the body, but neuroendocrine tumors (NETs) most commonly occur in the lungs, gastrointestinal tract, pancreas, and thyroid gland.
Neuroendocrine carcinomas can be classified as well-differentiated or poorly differentiated based on how closely they resemble normal neuroendocrine cells under a microscope. Well-differentiated tumors tend to grow more slowly and are less aggressive than poorly differentiated tumors.
Neuroendocrine carcinomas can produce and release hormones and other substances that can cause a variety of symptoms, such as flushing, diarrhea, wheezing, and heart palpitations. Treatment for neuroendocrine carcinoma depends on the location and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these approaches.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Medical survival rate is a statistical measure used to determine the percentage of patients who are still alive for a specific period of time after their diagnosis or treatment for a certain condition or disease. It is often expressed as a five-year survival rate, which refers to the proportion of people who are alive five years after their diagnosis. Survival rates can be affected by many factors, including the stage of the disease at diagnosis, the patient's age and overall health, the effectiveness of treatment, and other health conditions that the patient may have. It is important to note that survival rates are statistical estimates and do not necessarily predict an individual patient's prognosis.
The mouth mucosa refers to the mucous membrane that lines the inside of the mouth, also known as the oral mucosa. It covers the tongue, gums, inner cheeks, palate, and floor of the mouth. This moist tissue is made up of epithelial cells, connective tissue, blood vessels, and nerve endings. Its functions include protecting the underlying tissues from physical trauma, chemical irritation, and microbial infections; aiding in food digestion by producing enzymes; and providing sensory information about taste, temperature, and texture.
"Nude mice" is a term used in the field of laboratory research to describe a strain of mice that have been genetically engineered to lack a functional immune system. Specifically, nude mice lack a thymus gland and have a mutation in the FOXN1 gene, which results in a failure to develop a mature T-cell population. This means that they are unable to mount an effective immune response against foreign substances or organisms.
The name "nude" refers to the fact that these mice also have a lack of functional hair follicles, resulting in a hairless or partially hairless phenotype. This feature is actually a secondary consequence of the same genetic mutation that causes their immune deficiency.
Nude mice are commonly used in research because their weakened immune system makes them an ideal host for transplanted tumors, tissues, and cells from other species, including humans. This allows researchers to study the behavior of these foreign substances in a living organism without the complication of an immune response. However, it's important to note that because nude mice lack a functional immune system, they must be kept in sterile conditions and are more susceptible to infection than normal mice.
Medullary carcinoma is a type of cancer that develops in the neuroendocrine cells of the thyroid gland. These cells produce hormones that help regulate various bodily functions. Medullary carcinoma is a relatively rare form of thyroid cancer, accounting for about 5-10% of all cases.
Medullary carcinoma is characterized by the presence of certain genetic mutations that cause the overproduction of calcitonin, a hormone produced by the neuroendocrine cells. This overproduction can lead to the formation of tumors in the thyroid gland.
Medullary carcinoma can be hereditary or sporadic. Hereditary forms of the disease are caused by mutations in the RET gene and are often associated with multiple endocrine neoplasia type 2 (MEN 2), a genetic disorder that affects the thyroid gland, adrenal glands, and parathyroid glands. Sporadic forms of medullary carcinoma, on the other hand, are not inherited and occur randomly in people with no family history of the disease.
Medullary carcinoma is typically more aggressive than other types of thyroid cancer and tends to spread (metastasize) to other parts of the body, such as the lymph nodes, lungs, and liver. Symptoms may include a lump or nodule in the neck, difficulty swallowing, hoarseness, and coughing. Treatment options may include surgery, radiation therapy, and chemotherapy. Regular monitoring of calcitonin levels is also recommended to monitor the effectiveness of treatment and detect any recurrence of the disease.
Immunoenzyme techniques are a group of laboratory methods used in immunology and clinical chemistry that combine the specificity of antibody-antigen reactions with the sensitivity and amplification capabilities of enzyme reactions. These techniques are primarily used for the detection, quantitation, or identification of various analytes (such as proteins, hormones, drugs, viruses, or bacteria) in biological samples.
In immunoenzyme techniques, an enzyme is linked to an antibody or antigen, creating a conjugate. This conjugate then interacts with the target analyte in the sample, forming an immune complex. The presence and amount of this immune complex can be visualized or measured by detecting the enzymatic activity associated with it.
There are several types of immunoenzyme techniques, including:
1. Enzyme-linked Immunosorbent Assay (ELISA): A widely used method for detecting and quantifying various analytes in a sample. In ELISA, an enzyme is attached to either the capture antibody or the detection antibody. After the immune complex formation, a substrate is added that reacts with the enzyme, producing a colored product that can be measured spectrophotometrically.
2. Immunoblotting (Western blot): A method used for detecting specific proteins in a complex mixture, such as a protein extract from cells or tissues. In this technique, proteins are separated by gel electrophoresis and transferred to a membrane, where they are probed with an enzyme-conjugated antibody directed against the target protein.
3. Immunohistochemistry (IHC): A method used for detecting specific antigens in tissue sections or cells. In IHC, an enzyme-conjugated primary or secondary antibody is applied to the sample, and the presence of the antigen is visualized using a chromogenic substrate that produces a colored product at the site of the antigen-antibody interaction.
4. Immunofluorescence (IF): A method used for detecting specific antigens in cells or tissues by employing fluorophore-conjugated antibodies. The presence of the antigen is visualized using a fluorescence microscope.
5. Enzyme-linked immunosorbent assay (ELISA): A method used for detecting and quantifying specific antigens or antibodies in liquid samples, such as serum or culture supernatants. In ELISA, an enzyme-conjugated detection antibody is added after the immune complex formation, and a substrate is added that reacts with the enzyme to produce a colored product that can be measured spectrophotometrically.
These techniques are widely used in research and diagnostic laboratories for various applications, including protein characterization, disease diagnosis, and monitoring treatment responses.
Cisplatin is a chemotherapeutic agent used to treat various types of cancers, including testicular, ovarian, bladder, head and neck, lung, and cervical cancers. It is an inorganic platinum compound that contains a central platinum atom surrounded by two chloride atoms and two ammonia molecules in a cis configuration.
Cisplatin works by forming crosslinks between DNA strands, which disrupts the structure of DNA and prevents cancer cells from replicating. This ultimately leads to cell death and slows down or stops the growth of tumors. However, cisplatin can also cause damage to normal cells, leading to side effects such as nausea, vomiting, hearing loss, and kidney damage. Therefore, it is essential to monitor patients closely during treatment and manage any adverse effects promptly.
Hypopharyngeal neoplasms refer to abnormal growths or tumors in the hypopharynx, which is the lower part of the pharynx or throat. These growths can be benign (non-cancerous) or malignant (cancerous). Malignant hypopharyngeal neoplasms are often squamous cell carcinomas and are aggressive with a poor prognosis due to their location and tendency to spread early. They can cause symptoms such as difficulty swallowing, pain when swallowing, sore throat, ear pain, and neck masses. Risk factors for hypopharyngeal cancer include smoking, heavy alcohol consumption, and poor nutrition.
Survival analysis is a branch of statistics that deals with the analysis of time to event data. It is used to estimate the time it takes for a certain event of interest to occur, such as death, disease recurrence, or treatment failure. The event of interest is called the "failure" event, and survival analysis estimates the probability of not experiencing the failure event until a certain point in time, also known as the "survival" probability.
Survival analysis can provide important information about the effectiveness of treatments, the prognosis of patients, and the identification of risk factors associated with the event of interest. It can handle censored data, which is common in medical research where some participants may drop out or be lost to follow-up before the event of interest occurs.
Survival analysis typically involves estimating the survival function, which describes the probability of surviving beyond a certain time point, as well as hazard functions, which describe the instantaneous rate of failure at a given time point. Other important concepts in survival analysis include median survival times, restricted mean survival times, and various statistical tests to compare survival curves between groups.
Carcinoma, lobular is a type of breast cancer that begins in the milk-producing glands (lobules) of the breast. It can be either invasive or non-invasive (in situ). Invasive lobular carcinoma (ILC) occurs when the cancer cells break through the wall of the lobule and invade the surrounding breast tissue, and can potentially spread to other parts of the body. Non-invasive lobular carcinoma (LCIS), on the other hand, refers to the presence of abnormal cells within the lobule that have not invaded nearby breast tissue.
ILC is usually detected as a mass or thickening in the breast, and it may not cause any symptoms or show up on mammograms until it has grown quite large. It tends to grow more slowly than some other types of breast cancer, but it can still be serious and require extensive treatment. LCIS does not typically cause any symptoms and is usually found during a biopsy performed for another reason.
Treatment options for carcinoma, lobular depend on several factors, including the stage of the cancer, the patient's overall health, and their personal preferences. Treatment may include surgery, radiation therapy, chemotherapy, hormone therapy, or targeted therapy. Regular follow-up care is essential to monitor for recurrence or the development of new cancers.
Pharyngeal neoplasms refer to abnormal growths or tumors in the pharynx, which is the part of the throat that lies behind the nasal cavity and mouth, and above the esophagus and larynx. These growths can be benign (non-cancerous) or malignant (cancerous).
Pharyngeal neoplasms can occur in any part of the pharynx, which is divided into three regions: the nasopharynx, oropharynx, and hypopharynx. The most common type of pharyngeal cancer is squamous cell carcinoma, which arises from the flat cells that line the mucosal surface of the pharynx.
Risk factors for developing pharyngeal neoplasms include tobacco use, heavy alcohol consumption, and infection with human papillomavirus (HPV). Symptoms may include sore throat, difficulty swallowing, ear pain, neck masses, and changes in voice or speech. Treatment options depend on the type, size, location, and stage of the neoplasm, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Neoplasm metastasis is the spread of cancer cells from the primary site (where the original or primary tumor formed) to other places in the body. This happens when cancer cells break away from the original (primary) tumor and enter the bloodstream or lymphatic system. The cancer cells can then travel to other parts of the body and form new tumors, called secondary tumors or metastases.
Metastasis is a key feature of malignant neoplasms (cancers), and it is one of the main ways that cancer can cause harm in the body. The metastatic tumors may continue to grow and may cause damage to the organs and tissues where they are located. They can also release additional cancer cells into the bloodstream or lymphatic system, leading to further spread of the cancer.
The metastatic tumors are named based on the location where they are found, as well as the type of primary cancer. For example, if a patient has a primary lung cancer that has metastasized to the liver, the metastatic tumor would be called a liver metastasis from lung cancer.
It is important to note that the presence of metastases can significantly affect a person's prognosis and treatment options. In general, metastatic cancer is more difficult to treat than cancer that has not spread beyond its original site. However, there are many factors that can influence a person's prognosis and response to treatment, so it is important for each individual to discuss their specific situation with their healthcare team.
The term "DNA, neoplasm" is not a standard medical term or concept. DNA refers to deoxyribonucleic acid, which is the genetic material present in the cells of living organisms. A neoplasm, on the other hand, is a tumor or growth of abnormal tissue that can be benign (non-cancerous) or malignant (cancerous).
In some contexts, "DNA, neoplasm" may refer to genetic alterations found in cancer cells. These genetic changes can include mutations, amplifications, deletions, or rearrangements of DNA sequences that contribute to the development and progression of cancer. Identifying these genetic abnormalities can help doctors diagnose and treat certain types of cancer more effectively.
However, it's important to note that "DNA, neoplasm" is not a term that would typically be used in medical reports or research papers without further clarification. If you have any specific questions about DNA changes in cancer cells or neoplasms, I would recommend consulting with a healthcare professional or conducting further research on the topic.
Antineoplastic agents are a class of drugs used to treat malignant neoplasms or cancer. These agents work by inhibiting the growth and proliferation of cancer cells, either by killing them or preventing their division and replication. Antineoplastic agents can be classified based on their mechanism of action, such as alkylating agents, antimetabolites, topoisomerase inhibitors, mitotic inhibitors, and targeted therapy agents.
Alkylating agents work by adding alkyl groups to DNA, which can cause cross-linking of DNA strands and ultimately lead to cell death. Antimetabolites interfere with the metabolic processes necessary for DNA synthesis and replication, while topoisomerase inhibitors prevent the relaxation of supercoiled DNA during replication. Mitotic inhibitors disrupt the normal functioning of the mitotic spindle, which is essential for cell division. Targeted therapy agents are designed to target specific molecular abnormalities in cancer cells, such as mutated oncogenes or dysregulated signaling pathways.
It's important to note that antineoplastic agents can also affect normal cells and tissues, leading to various side effects such as nausea, vomiting, hair loss, and myelosuppression (suppression of bone marrow function). Therefore, the use of these drugs requires careful monitoring and management of their potential adverse effects.
Breast neoplasms refer to abnormal growths in the breast tissue that can be benign or malignant. Benign breast neoplasms are non-cancerous tumors or growths, while malignant breast neoplasms are cancerous tumors that can invade surrounding tissues and spread to other parts of the body.
Breast neoplasms can arise from different types of cells in the breast, including milk ducts, milk sacs (lobules), or connective tissue. The most common type of breast cancer is ductal carcinoma, which starts in the milk ducts and can spread to other parts of the breast and nearby structures.
Breast neoplasms are usually detected through screening methods such as mammography, ultrasound, or MRI, or through self-examination or clinical examination. Treatment options for breast neoplasms depend on several factors, including the type and stage of the tumor, the patient's age and overall health, and personal preferences. Treatment may include surgery, radiation therapy, chemotherapy, hormone therapy, or targeted therapy.
Thyroid neoplasms refer to abnormal growths or tumors in the thyroid gland, which can be benign (non-cancerous) or malignant (cancerous). These growths can vary in size and may cause a noticeable lump or nodule in the neck. Thyroid neoplasms can also affect the function of the thyroid gland, leading to hormonal imbalances and related symptoms. The exact causes of thyroid neoplasms are not fully understood, but risk factors include radiation exposure, family history, and certain genetic conditions. It is important to note that most thyroid nodules are benign, but a proper medical evaluation is necessary to determine the nature of the growth and develop an appropriate treatment plan.
Combined modality therapy (CMT) is a medical treatment approach that utilizes more than one method or type of therapy simultaneously or in close succession, with the goal of enhancing the overall effectiveness of the treatment. In the context of cancer care, CMT often refers to the combination of two or more primary treatment modalities, such as surgery, radiation therapy, and systemic therapies (chemotherapy, immunotherapy, targeted therapy, etc.).
The rationale behind using combined modality therapy is that each treatment method can target cancer cells in different ways, potentially increasing the likelihood of eliminating all cancer cells and reducing the risk of recurrence. The specific combination and sequence of treatments will depend on various factors, including the type and stage of cancer, patient's overall health, and individual preferences.
For example, a common CMT approach for locally advanced rectal cancer may involve preoperative (neoadjuvant) chemoradiation therapy, followed by surgery to remove the tumor, and then postoperative (adjuvant) chemotherapy. This combined approach allows for the reduction of the tumor size before surgery, increases the likelihood of complete tumor removal, and targets any remaining microscopic cancer cells with systemic chemotherapy.
It is essential to consult with a multidisciplinary team of healthcare professionals to determine the most appropriate CMT plan for each individual patient, considering both the potential benefits and risks associated with each treatment method.
Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
Tumor suppressor protein p53, also known as p53 or tumor protein p53, is a nuclear phosphoprotein that plays a crucial role in preventing cancer development and maintaining genomic stability. It does so by regulating the cell cycle and acting as a transcription factor for various genes involved in apoptosis (programmed cell death), DNA repair, and cell senescence (permanent cell growth arrest).
In response to cellular stress, such as DNA damage or oncogene activation, p53 becomes activated and accumulates in the nucleus. Activated p53 can then bind to specific DNA sequences and promote the transcription of target genes that help prevent the proliferation of potentially cancerous cells. These targets include genes involved in cell cycle arrest (e.g., CDKN1A/p21), apoptosis (e.g., BAX, PUMA), and DNA repair (e.g., GADD45).
Mutations in the TP53 gene, which encodes p53, are among the most common genetic alterations found in human cancers. These mutations often lead to a loss or reduction of p53's tumor suppressive functions, allowing cancer cells to proliferate uncontrollably and evade apoptosis. As a result, p53 has been referred to as "the guardian of the genome" due to its essential role in preventing tumorigenesis.
Tonsillar neoplasms refer to abnormal growths or tumors that develop in the tonsils, which are two masses of lymphoid tissue located on either side of the back of the throat (oropharynx). These growths can be benign or malignant (cancerous), and their symptoms may include difficulty swallowing, sore throat, ear pain, and swollen lymph nodes in the neck.
Tonsillar neoplasms are relatively rare, but they can occur at any age. The most common type of malignant tonsillar neoplasm is squamous cell carcinoma, which accounts for about 90% of all cases. Other types of malignant tonsillar neoplasms include lymphomas and sarcomas.
The diagnosis of tonsillar neoplasms typically involves a physical examination, imaging studies such as CT or MRI scans, and sometimes a biopsy to confirm the type of tumor. Treatment options depend on the stage and location of the tumor, as well as the patient's overall health. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence and manage any long-term effects of treatment.
Keratoacanthoma is a rapidly growing, dome-shaped, skin tumor that typically arises on sun-exposed areas such as the face, arms, and legs. It is considered a low-grade squamous cell carcinoma (a type of skin cancer) because it shares some characteristics with both benign and malignant tumors.
Keratoacanthomas usually develop over a period of several weeks to months, growing rapidly in size before eventually stabilizing and then gradually regressing on their own within a few months to a year. However, the regression process can take years, and some lesions may not regress completely, leading to cosmetic concerns or even local invasion.
Histologically, keratoacanthomas are characterized by a central keratin-filled crater surrounded by a well-differentiated layer of squamous epithelial cells. The tumor's growth pattern and histological features can make it difficult to distinguish from other types of skin cancer, such as squamous cell carcinoma.
Treatment options for keratoacanthomas include surgical excision, cryosurgery, curettage and electrodesiccation, and topical therapies like imiquimod or 5-fluorouracil. The choice of treatment depends on various factors such as the size, location, and number of lesions, as well as patient preferences and overall health status.
Neoplasm antigens, also known as tumor antigens, are substances that are produced by cancer cells (neoplasms) and can stimulate an immune response. These antigens can be proteins, carbohydrates, or other molecules that are either unique to the cancer cells or are overexpressed or mutated versions of normal cellular proteins.
Neoplasm antigens can be classified into two main categories: tumor-specific antigens (TSAs) and tumor-associated antigens (TAAs). TSAs are unique to cancer cells and are not expressed by normal cells, while TAAs are present at low levels in normal cells but are overexpressed or altered in cancer cells.
TSAs can be further divided into viral antigens and mutated antigens. Viral antigens are produced when cancer is caused by a virus, such as human papillomavirus (HPV) in cervical cancer. Mutated antigens are the result of genetic mutations that occur during cancer development and are unique to each patient's tumor.
Neoplasm antigens play an important role in the immune response against cancer. They can be recognized by the immune system, leading to the activation of immune cells such as T cells and natural killer (NK) cells, which can then attack and destroy cancer cells. However, cancer cells often develop mechanisms to evade the immune response, allowing them to continue growing and spreading.
Understanding neoplasm antigens is important for the development of cancer immunotherapies, which aim to enhance the body's natural immune response against cancer. These therapies include checkpoint inhibitors, which block proteins that inhibit T cell activation, and therapeutic vaccines, which stimulate an immune response against specific tumor antigens.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) is a laboratory technique used in molecular biology to amplify and detect specific DNA sequences. This technique is particularly useful for the detection and quantification of RNA viruses, as well as for the analysis of gene expression.
The process involves two main steps: reverse transcription and polymerase chain reaction (PCR). In the first step, reverse transcriptase enzyme is used to convert RNA into complementary DNA (cDNA) by reading the template provided by the RNA molecule. This cDNA then serves as a template for the PCR amplification step.
In the second step, the PCR reaction uses two primers that flank the target DNA sequence and a thermostable polymerase enzyme to repeatedly copy the targeted cDNA sequence. The reaction mixture is heated and cooled in cycles, allowing the primers to anneal to the template, and the polymerase to extend the new strand. This results in exponential amplification of the target DNA sequence, making it possible to detect even small amounts of RNA or cDNA.
RT-PCR is a sensitive and specific technique that has many applications in medical research and diagnostics, including the detection of viruses such as HIV, hepatitis C virus, and SARS-CoV-2 (the virus that causes COVID-19). It can also be used to study gene expression, identify genetic mutations, and diagnose genetic disorders.
Mucoepidermoid carcinoma is a type of cancer that develops in the salivary glands or, less commonly, in other areas such as the lungs or skin. It is called "mucoepidermoid" because it contains two types of cells: mucus-secreting cells and squamous (or epidermoid) cells.
Mucoepidermoid carcinomas can vary in their behavior, ranging from low-grade tumors that grow slowly and rarely spread to other parts of the body, to high-grade tumors that are aggressive and can metastasize. The treatment and prognosis for mucoepidermoid carcinoma depend on several factors, including the grade and stage of the tumor, as well as the patient's overall health.
It is important to note that while I strive to provide accurate and up-to-date information, this definition may not capture all the nuances of this medical condition. Therefore, it is always best to consult with a healthcare professional for medical advice.
Messenger RNA (mRNA) is a type of RNA (ribonucleic acid) that carries genetic information copied from DNA in the form of a series of three-base code "words," each of which specifies a particular amino acid. This information is used by the cell's machinery to construct proteins, a process known as translation. After being transcribed from DNA, mRNA travels out of the nucleus to the ribosomes in the cytoplasm where protein synthesis occurs. Once the protein has been synthesized, the mRNA may be degraded and recycled. Post-transcriptional modifications can also occur to mRNA, such as alternative splicing and addition of a 5' cap and a poly(A) tail, which can affect its stability, localization, and translation efficiency.
Carcinoma, large cell is a type of lung cancer that is characterized by the presence of large, abnormal-looking cells when viewed under a microscope. These cells have a large nucleus and a significant amount of cytoplasm. This type of lung cancer can be further divided into subtypes based on the appearance of the cells and the presence or absence of specific genetic mutations.
Large cell carcinoma is often aggressive and tends to grow and spread quickly. It is typically treated with a combination of surgery, chemotherapy, and/or radiation therapy. The prognosis for large cell carcinoma varies depending on the stage at diagnosis and the individual's overall health.
A papilloma is a benign (noncancerous) tumor that grows on a stalk, often appearing as a small cauliflower-like growth. It can develop in various parts of the body, but when it occurs in the mucous membranes lining the respiratory, digestive, or genitourinary tracts, they are called squamous papillomas. The most common type is the skin papilloma, which includes warts. They are usually caused by human papillomavirus (HPV) infection and can be removed through various medical procedures if they become problematic or unsightly.
Keratins are a type of fibrous structural proteins that constitute the main component of the integumentary system, which includes the hair, nails, and skin of vertebrates. They are also found in other tissues such as horns, hooves, feathers, and reptilian scales. Keratins are insoluble proteins that provide strength, rigidity, and protection to these structures.
Keratins are classified into two types: soft keratins (Type I) and hard keratins (Type II). Soft keratins are found in the skin and simple epithelial tissues, while hard keratins are present in structures like hair, nails, horns, and hooves.
Keratin proteins have a complex structure consisting of several domains, including an alpha-helical domain, beta-pleated sheet domain, and a non-repetitive domain. These domains provide keratin with its unique properties, such as resistance to heat, chemicals, and mechanical stress.
In summary, keratins are fibrous structural proteins that play a crucial role in providing strength, rigidity, and protection to various tissues in the body.
Actinic keratosis, also known as solar keratosis, is a precancerous skin condition that typically develops in areas exposed to excessive sun damage over the years. It presents as rough, scaly, or crusty patches of skin, often with a pink, red, or brownish tint. These lesions usually appear on the face, ears, scalp, neck, back of the hands, and forearms.
Actinic keratosis is caused by the prolonged exposure to ultraviolet (UV) radiation from sunlight or artificial sources like tanning beds. The UV rays damage the skin's DNA, leading to abnormal skin cell growth and the formation of these precancerous lesions.
While most actinic keratoses remain benign, a small percentage can progress into squamous cell carcinoma, a type of skin cancer. Therefore, it is essential to have any suspicious or changing lesions evaluated by a healthcare professional for proper diagnosis and treatment. Prevention measures include protecting the skin from excessive sun exposure, wearing protective clothing, using broad-spectrum sunscreen with an SPF of at least 30, and avoiding tanning beds.
Neoplasm transplantation is not a recognized or established medical procedure in the field of oncology. The term "neoplasm" refers to an abnormal growth of cells, which can be benign or malignant (cancerous). "Transplantation" typically refers to the surgical transfer of living cells, tissues, or organs from one part of the body to another or between individuals.
The concept of neoplasm transplantation may imply the transfer of cancerous cells or tissues from a donor to a recipient, which is not a standard practice due to ethical considerations and the potential harm it could cause to the recipient. In some rare instances, researchers might use laboratory animals to study the transmission and growth of human cancer cells, but this is done for scientific research purposes only and under strict regulatory guidelines.
In summary, there is no medical definition for 'Neoplasm Transplantation' as it does not represent a standard or ethical medical practice.
Disease progression is the worsening or advancement of a medical condition over time. It refers to the natural course of a disease, including its development, the severity of symptoms and complications, and the impact on the patient's overall health and quality of life. Understanding disease progression is important for developing appropriate treatment plans, monitoring response to therapy, and predicting outcomes.
The rate of disease progression can vary widely depending on the type of medical condition, individual patient factors, and the effectiveness of treatment. Some diseases may progress rapidly over a short period of time, while others may progress more slowly over many years. In some cases, disease progression may be slowed or even halted with appropriate medical interventions, while in other cases, the progression may be inevitable and irreversible.
In clinical practice, healthcare providers closely monitor disease progression through regular assessments, imaging studies, and laboratory tests. This information is used to guide treatment decisions and adjust care plans as needed to optimize patient outcomes and improve quality of life.
Carcinoma, non-small-cell lung (NSCLC) is a type of lung cancer that includes several subtypes of malignant tumors arising from the epithelial cells of the lung. These subtypes are classified based on the appearance of the cancer cells under a microscope and include adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. NSCLC accounts for about 85% of all lung cancers and tends to grow and spread more slowly than small-cell lung cancer (SCLC).
NSCLC is often asymptomatic in its early stages, but as the tumor grows, symptoms such as coughing, chest pain, shortness of breath, hoarseness, and weight loss may develop. Treatment options for NSCLC depend on the stage and location of the cancer, as well as the patient's overall health and lung function. Common treatments include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these approaches.
Carcinoma, basosquamous is a rare type of skin cancer that has features of both basal cell carcinoma and squamous cell carcinoma. It is also known as metatypical carcinoma or basaloid squamous cell carcinoma. This cancer typically appears as a firm, shiny, pearly nodule or plaque on the skin, often on sun-exposed areas such as the head, neck, or hands. It can be aggressive and has a higher risk of recurrence and metastasis compared to traditional basal cell carcinomas. Treatment options include surgical excision, radiation therapy, and chemotherapy.
Cell proliferation is the process by which cells increase in number, typically through the process of cell division. In the context of biology and medicine, it refers to the reproduction of cells that makes up living tissue, allowing growth, maintenance, and repair. It involves several stages including the transition from a phase of quiescence (G0 phase) to an active phase (G1 phase), DNA replication in the S phase, and mitosis or M phase, where the cell divides into two daughter cells.
Abnormal or uncontrolled cell proliferation is a characteristic feature of many diseases, including cancer, where deregulated cell cycle control leads to excessive and unregulated growth of cells, forming tumors that can invade surrounding tissues and metastasize to distant sites in the body.
p53 is a tumor suppressor gene that encodes a protein responsible for controlling cell growth and division. The p53 protein plays a crucial role in preventing the development of cancer by regulating the cell cycle and activating DNA repair processes when genetic damage is detected. If the damage is too severe to be repaired, p53 can trigger apoptosis, or programmed cell death, to prevent the propagation of potentially cancerous cells. Mutations in the TP53 gene, which encodes the p53 protein, are among the most common genetic alterations found in human cancers and are often associated with a poor prognosis.
Neck dissection is a surgical procedure that involves the removal of lymph nodes and other tissues from the neck. It is typically performed as part of cancer treatment, particularly in cases of head and neck cancer, to help determine the stage of the cancer, prevent the spread of cancer, or treat existing metastases. There are several types of neck dissections, including radical, modified radical, and selective neck dissection, which vary based on the extent of tissue removal. The specific type of neck dissection performed depends on the location and extent of the cancer.
Stomach neoplasms refer to abnormal growths in the stomach that can be benign or malignant. They include a wide range of conditions such as:
1. Gastric adenomas: These are benign tumors that develop from glandular cells in the stomach lining.
2. Gastrointestinal stromal tumors (GISTs): These are rare tumors that can be found in the stomach and other parts of the digestive tract. They originate from the stem cells in the wall of the digestive tract.
3. Leiomyomas: These are benign tumors that develop from smooth muscle cells in the stomach wall.
4. Lipomas: These are benign tumors that develop from fat cells in the stomach wall.
5. Neuroendocrine tumors (NETs): These are tumors that develop from the neuroendocrine cells in the stomach lining. They can be benign or malignant.
6. Gastric carcinomas: These are malignant tumors that develop from the glandular cells in the stomach lining. They are the most common type of stomach neoplasm and include adenocarcinomas, signet ring cell carcinomas, and others.
7. Lymphomas: These are malignant tumors that develop from the immune cells in the stomach wall.
Stomach neoplasms can cause various symptoms such as abdominal pain, nausea, vomiting, weight loss, and difficulty swallowing. The diagnosis of stomach neoplasms usually involves a combination of imaging tests, endoscopy, and biopsy. Treatment options depend on the type and stage of the neoplasm and may include surgery, chemotherapy, radiation therapy, or targeted therapy.
Merkel cell carcinoma (MCC) is a rare and aggressive type of skin cancer that originates from the uncontrolled growth of Merkel cells, which are specialized nerve cells found in the top layer of the skin (epidermis). These cells are responsible for touch sensation. MCC typically presents as a painless, firm, rapidly growing nodule or mass, often on sun-exposed areas such as the head, neck, and arms of older adults.
The primary risk factors for Merkel cell carcinoma include:
1. Exposure to ultraviolet (UV) radiation from sunlight or tanning beds
2. Advanced age (most commonly occurs in people over 50)
3. A weakened immune system due to conditions like HIV/AIDS, organ transplantation, or long-term use of immunosuppressive medications
4. History of other types of skin cancer, such as melanoma or basal cell carcinoma
5. Fair skin and light eye color
MCC is considered an aggressive cancer because it can spread quickly to nearby lymph nodes and other parts of the body (metastasize). The major prognostic factor for MCC is the presence or absence of lymph node involvement at the time of diagnosis. Early detection and treatment are crucial for improving outcomes.
Standard treatments for Merkel cell carcinoma include surgical excision, radiation therapy, and chemotherapy. Immunotherapy with drugs like avelumab has also shown promising results in treating advanced stages of MCC. Regular follow-up care is essential to monitor for recurrence or metastasis.
Disease-free survival (DFS) is a term used in medical research and clinical practice, particularly in the field of oncology. It refers to the length of time after primary treatment for a cancer during which no evidence of the disease can be found. This means that the patient shows no signs or symptoms of the cancer, and any imaging studies or other tests do not reveal any tumors or other indications of the disease.
DFS is often used as an important endpoint in clinical trials to evaluate the effectiveness of different treatments for cancer. By measuring the length of time until the cancer recurs or a new cancer develops, researchers can get a better sense of how well a particular treatment is working and whether it is improving patient outcomes.
It's important to note that DFS is not the same as overall survival (OS), which refers to the length of time from primary treatment until death from any cause. While DFS can provide valuable information about the effectiveness of cancer treatments, it does not necessarily reflect the impact of those treatments on patients' overall survival.
Anus neoplasms refer to abnormal growths or tumors in the anus, which is the opening at the end of the digestive tract where solid waste leaves the body. These growths can be benign (non-cancerous) or malignant (cancerous). Common types of anus neoplasms include squamous cell carcinoma, adenocarcinoma, and melanoma.
Squamous cell carcinoma is the most common type of anus cancer, accounting for about 80% of all cases. It begins in the squamous cells that line the anal canal and can spread to other parts of the body if left untreated.
Adenocarcinoma is a less common type of anus cancer that arises from glandular cells in the anus. This type of cancer is often associated with long-standing inflammatory conditions, such as anal fistulas or ulcerative colitis.
Melanoma is a rare form of skin cancer that can also occur in the anus. It develops from pigment-producing cells called melanocytes and tends to be aggressive with a high risk of spreading to other parts of the body.
Other less common types of anus neoplasms include basal cell carcinoma, sarcoma, and lymphoma. Treatment options for anus neoplasms depend on the type, stage, and location of the tumor, as well as the patient's overall health.
Tissue Microarray (TMA) analysis is a surgical pathology technique that allows for the simultaneous analysis of multiple tissue samples (known as "cores") from different patients or even different regions of the same tumor, on a single microscope slide. This technique involves the extraction of small cylindrical samples of tissue, which are then arrayed in a grid-like pattern on a recipient paraffin block. Once the TMA is created, sections can be cut and stained with various histochemical or immunohistochemical stains to evaluate the expression of specific proteins or other molecules of interest.
Tissue Array Analysis has become an important tool in biomedical research, enabling high-throughput analysis of tissue samples for molecular markers, gene expression patterns, and other features that can help inform clinical decision making, drug development, and our understanding of disease processes. It's widely used in cancer research to study the heterogeneity of tumors, identify new therapeutic targets, and evaluate patient prognosis.
Urinary Bladder Neoplasms are abnormal growths or tumors in the urinary bladder, which can be benign (non-cancerous) or malignant (cancerous). Malignant neoplasms can be further classified into various types of bladder cancer, such as urothelial carcinoma, squamous cell carcinoma, and adenocarcinoma. These malignant tumors often invade surrounding tissues and organs, potentially spreading to other parts of the body (metastasis), which can lead to serious health consequences if not detected and treated promptly and effectively.
Carcinoma, endometrioid is a type of cancer that arises from the glandular cells of the endometrium, which is the lining of the uterus. This type of cancer is named for its similarity in appearance to the normal endometrial cells, and it is the second most common type of endometrial cancer after serous carcinoma.
Endometrioid carcinomas are typically divided into different grades based on how abnormal the cells look under a microscope. Low-grade tumors tend to grow more slowly and are less likely to spread beyond the uterus than high-grade tumors.
Risk factors for endometrioid carcinoma include obesity, older age, early menstruation, late menopause, never having been pregnant, and a history of taking estrogen hormone replacement therapy without progesterone. Treatment typically involves surgery to remove the uterus, fallopian tubes, ovaries, and nearby lymph nodes, followed by radiation therapy, chemotherapy, or hormonal therapy in some cases.
Lip neoplasms refer to abnormal growths or tumors that occur in the lip tissue. These growths can be benign (non-cancerous) or malignant (cancerous). Benign lip neoplasms include conditions such as papillomas, fibromas, and mucocele, while malignant lip neoplasms are typically squamous cell carcinomas.
Squamous cell carcinoma of the lip is the most common type of lip cancer, accounting for about 90% of all lip cancers. It usually develops on the lower lip, and is often associated with prolonged sun exposure, smoking, and alcohol consumption. Symptoms may include a sore or lump on the lip that does not heal, bleeding, pain, numbness, or difficulty moving the lips.
It's important to note that any abnormal growth or change in the lips should be evaluated by a healthcare professional for proper diagnosis and treatment.
A case-control study is an observational research design used to identify risk factors or causes of a disease or health outcome. In this type of study, individuals with the disease or condition (cases) are compared with similar individuals who do not have the disease or condition (controls). The exposure history or other characteristics of interest are then compared between the two groups to determine if there is an association between the exposure and the disease.
Case-control studies are often used when it is not feasible or ethical to conduct a randomized controlled trial, as they can provide valuable insights into potential causes of diseases or health outcomes in a relatively short period of time and at a lower cost than other study designs. However, because case-control studies rely on retrospective data collection, they are subject to biases such as recall bias and selection bias, which can affect the validity of the results. Therefore, it is important to carefully design and conduct case-control studies to minimize these potential sources of bias.
Apoptosis is a programmed and controlled cell death process that occurs in multicellular organisms. It is a natural process that helps maintain tissue homeostasis by eliminating damaged, infected, or unwanted cells. During apoptosis, the cell undergoes a series of morphological changes, including cell shrinkage, chromatin condensation, and fragmentation into membrane-bound vesicles called apoptotic bodies. These bodies are then recognized and engulfed by neighboring cells or phagocytic cells, preventing an inflammatory response. Apoptosis is regulated by a complex network of intracellular signaling pathways that involve proteins such as caspases, Bcl-2 family members, and inhibitors of apoptosis (IAPs).
Gingival neoplasms refer to abnormal growths or tumors that occur in the gingiva, which are the part of the gums that surround the teeth. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms include conditions such as fibromas, papillomas, and hemangiomas, while malignant neoplasms are typically squamous cell carcinomas.
Gingival neoplasms can present with a variety of symptoms, including swelling, bleeding, pain, and loose teeth. They may also cause difficulty with chewing, speaking, or swallowing. The exact cause of these neoplasms is not always known, but risk factors include tobacco use, alcohol consumption, poor oral hygiene, and certain viral infections.
Diagnosis of gingival neoplasms typically involves a thorough clinical examination, including a dental exam and biopsy. Treatment options depend on the type and stage of the neoplasm, but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular dental check-ups and good oral hygiene practices can help to detect gingival neoplasms at an early stage and improve treatment outcomes.
Neoplastic cell transformation is a process in which a normal cell undergoes genetic alterations that cause it to become cancerous or malignant. This process involves changes in the cell's DNA that result in uncontrolled cell growth and division, loss of contact inhibition, and the ability to invade surrounding tissues and metastasize (spread) to other parts of the body.
Neoplastic transformation can occur as a result of various factors, including genetic mutations, exposure to carcinogens, viral infections, chronic inflammation, and aging. These changes can lead to the activation of oncogenes or the inactivation of tumor suppressor genes, which regulate cell growth and division.
The transformation of normal cells into cancerous cells is a complex and multi-step process that involves multiple genetic and epigenetic alterations. It is characterized by several hallmarks, including sustained proliferative signaling, evasion of growth suppressors, resistance to cell death, enabling replicative immortality, induction of angiogenesis, activation of invasion and metastasis, reprogramming of energy metabolism, and evading immune destruction.
Neoplastic cell transformation is a fundamental concept in cancer biology and is critical for understanding the molecular mechanisms underlying cancer development and progression. It also has important implications for cancer diagnosis, prognosis, and treatment, as identifying the specific genetic alterations that underlie neoplastic transformation can help guide targeted therapies and personalized medicine approaches.
The Epidermal Growth Factor Receptor (EGFR) is a type of receptor found on the surface of many cells in the body, including those of the epidermis or outer layer of the skin. It is a transmembrane protein that has an extracellular ligand-binding domain and an intracellular tyrosine kinase domain.
EGFR plays a crucial role in various cellular processes such as proliferation, differentiation, migration, and survival. When EGF (Epidermal Growth Factor) or other ligands bind to the extracellular domain of EGFR, it causes the receptor to dimerize and activate its intrinsic tyrosine kinase activity. This leads to the autophosphorylation of specific tyrosine residues on the receptor, which in turn recruits and activates various downstream signaling molecules, resulting in a cascade of intracellular signaling events that ultimately regulate gene expression and cell behavior.
Abnormal activation of EGFR has been implicated in several human diseases, including cancer. Overexpression or mutation of EGFR can lead to uncontrolled cell growth and division, angiogenesis, and metastasis, making it an important target for cancer therapy.
Ovarian neoplasms refer to abnormal growths or tumors in the ovary, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various cell types within the ovary, including epithelial cells, germ cells, and stromal cells. Ovarian neoplasms are often classified based on their cell type of origin, histological features, and potential for invasive or metastatic behavior.
Epithelial ovarian neoplasms are the most common type and can be further categorized into several subtypes, such as serous, mucinous, endometrioid, clear cell, and Brenner tumors. Some of these epithelial tumors have a higher risk of becoming malignant and spreading to other parts of the body.
Germ cell ovarian neoplasms arise from the cells that give rise to eggs (oocytes) and can include teratomas, dysgerminomas, yolk sac tumors, and embryonal carcinomas. Stromal ovarian neoplasms develop from the connective tissue cells supporting the ovary and can include granulosa cell tumors, thecomas, and fibromas.
It is essential to diagnose and treat ovarian neoplasms promptly, as some malignant forms can be aggressive and potentially life-threatening if not managed appropriately. Regular gynecological exams, imaging studies, and tumor marker tests are often used for early detection and monitoring of ovarian neoplasms. Treatment options may include surgery, chemotherapy, or radiation therapy, depending on the type, stage, and patient's overall health condition.
Embryonal carcinoma is a rare and aggressive type of cancer that arises from primitive germ cells. It typically occurs in the gonads (ovaries or testicles), but can also occur in other areas of the body such as the mediastinum, retroperitoneum, or sacrococcygeal region.
Embryonal carcinoma is called "embryonal" because the cancerous cells resemble those found in an embryo during early stages of development. These cells are capable of differentiating into various cell types, which can lead to a mix of cell types within the tumor.
Embryonal carcinoma is a highly malignant tumor that tends to grow and spread quickly. It can metastasize to other parts of the body, including the lungs, liver, brain, and bones. Treatment typically involves surgical removal of the tumor, followed by chemotherapy and/or radiation therapy to kill any remaining cancer cells.
Prognosis for embryonal carcinoma depends on several factors, including the stage of the disease at diagnosis, the location of the tumor, and the patient's overall health. In general, this type of cancer has a poor prognosis, with a high risk of recurrence even after treatment.
Colonic neoplasms refer to abnormal growths in the large intestine, also known as the colon. These growths can be benign (non-cancerous) or malignant (cancerous). The two most common types of colonic neoplasms are adenomas and carcinomas.
Adenomas are benign tumors that can develop into cancer over time if left untreated. They are often found during routine colonoscopies and can be removed during the procedure.
Carcinomas, on the other hand, are malignant tumors that invade surrounding tissues and can spread to other parts of the body. Colorectal cancer is the third leading cause of cancer-related deaths in the United States, and colonic neoplasms are a significant risk factor for developing this type of cancer.
Regular screenings for colonic neoplasms are recommended for individuals over the age of 50 or those with a family history of colorectal cancer or other risk factors. Early detection and removal of colonic neoplasms can significantly reduce the risk of developing colorectal cancer.
Leukoplakia, oral is a predominantly white patch or plaque that cannot be characterized clinically or pathologically as any other disease. It is an oral potentially malignant disorder (OPMD) and represents a significant risk for the development of squamous cell carcinoma. The lesions are typically caused by chronic irritation, such as smoking or smokeless tobacco use, and are most commonly found on the tongue, floor of the mouth, and buccal mucosa. The diagnosis is confirmed through a biopsy, and management includes removal of causative factors and close monitoring for any signs of malignant transformation.
Follow-up studies are a type of longitudinal research that involve repeated observations or measurements of the same variables over a period of time, in order to understand their long-term effects or outcomes. In medical context, follow-up studies are often used to evaluate the safety and efficacy of medical treatments, interventions, or procedures.
In a typical follow-up study, a group of individuals (called a cohort) who have received a particular treatment or intervention are identified and then followed over time through periodic assessments or data collection. The data collected may include information on clinical outcomes, adverse events, changes in symptoms or functional status, and other relevant measures.
The results of follow-up studies can provide important insights into the long-term benefits and risks of medical interventions, as well as help to identify factors that may influence treatment effectiveness or patient outcomes. However, it is important to note that follow-up studies can be subject to various biases and limitations, such as loss to follow-up, recall bias, and changes in clinical practice over time, which must be carefully considered when interpreting the results.
The esophagus is the muscular tube that connects the throat (pharynx) to the stomach. It is located in the midline of the neck and chest, passing through the diaphragm to enter the abdomen and join the stomach. The main function of the esophagus is to transport food and liquids from the mouth to the stomach for digestion.
The esophagus has a few distinct parts: the upper esophageal sphincter (a ring of muscle that separates the esophagus from the throat), the middle esophagus, and the lower esophageal sphincter (another ring of muscle that separates the esophagus from the stomach). The lower esophageal sphincter relaxes to allow food and liquids to enter the stomach and then contracts to prevent stomach contents from flowing back into the esophagus.
The walls of the esophagus are made up of several layers, including mucosa (a moist tissue that lines the inside of the tube), submucosa (a layer of connective tissue), muscle (both voluntary and involuntary types), and adventitia (an outer layer of connective tissue).
Common conditions affecting the esophagus include gastroesophageal reflux disease (GERD), Barrett's esophagus, esophageal cancer, esophageal strictures, and eosinophilic esophagitis.
Loss of Heterozygosity (LOH) is a term used in genetics to describe the loss of one copy of a gene or a segment of a chromosome, where there was previously a pair of different genes or chromosomal segments (heterozygous). This can occur due to various genetic events such as mutation, deletion, or mitotic recombination.
LOH is often associated with the development of cancer, as it can lead to the loss of tumor suppressor genes, which normally help to regulate cell growth and division. When both copies of a tumor suppressor gene are lost or inactivated, it can result in uncontrolled cell growth and the formation of a tumor.
In medical terms, LOH is used as a biomarker for cancer susceptibility, progression, and prognosis. It can also be used to identify individuals who may be at increased risk for certain types of cancer, or to monitor patients for signs of cancer recurrence.
A biopsy is a medical procedure in which a small sample of tissue is taken from the body to be examined under a microscope for the presence of disease. This can help doctors diagnose and monitor various medical conditions, such as cancer, infections, or autoimmune disorders. The type of biopsy performed will depend on the location and nature of the suspected condition. Some common types of biopsies include:
1. Incisional biopsy: In this procedure, a surgeon removes a piece of tissue from an abnormal area using a scalpel or other surgical instrument. This type of biopsy is often used when the lesion is too large to be removed entirely during the initial biopsy.
2. Excisional biopsy: An excisional biopsy involves removing the entire abnormal area, along with a margin of healthy tissue surrounding it. This technique is typically employed for smaller lesions or when cancer is suspected.
3. Needle biopsy: A needle biopsy uses a thin, hollow needle to extract cells or fluid from the body. There are two main types of needle biopsies: fine-needle aspiration (FNA) and core needle biopsy. FNA extracts loose cells, while a core needle biopsy removes a small piece of tissue.
4. Punch biopsy: In a punch biopsy, a round, sharp tool is used to remove a small cylindrical sample of skin tissue. This type of biopsy is often used for evaluating rashes or other skin abnormalities.
5. Shave biopsy: During a shave biopsy, a thin slice of tissue is removed from the surface of the skin using a sharp razor-like instrument. This technique is typically used for superficial lesions or growths on the skin.
After the biopsy sample has been collected, it is sent to a laboratory where a pathologist will examine the tissue under a microscope and provide a diagnosis based on their findings. The results of the biopsy can help guide further treatment decisions and determine the best course of action for managing the patient's condition.
Keratosis, in general, refers to a skin condition characterized by the abnormal growth or development of keratin, a protein that forms part of the outer layer of the skin (epidermis). There are several types of keratosis, including:
1. Seborrheic Keratosis: benign, often pigmented, rough, and scaly growths that can appear anywhere on the body. They tend to increase in number with age.
2. Actinic Keratosis: rough, scaly patches or spots on the skin that are caused by long-term exposure to sunlight or artificial UV light. These have the potential to develop into squamous cell carcinoma, a type of skin cancer.
3. Solar Keratosis: another term for actinic keratosis, as it is primarily caused by sun damage.
4. Keratosis Pilaris: a common condition where small, rough bumps appear on the skin, often on the arms, thighs, or cheeks. These are caused by excess keratin blocking hair follicles.
5. Follicular Keratosis: a disorder characterized by the formation of horny plugs within the hair follicles, leading to rough, sandpaper-like bumps on the skin.
6. Intraepidermal Keratosis: a term used to describe the abnormal accumulation of keratin in the epidermis, which can lead to various skin conditions.
It's important to consult with a healthcare professional or dermatologist for proper diagnosis and treatment if you suspect having any form of keratosis.
Cyclin-Dependent Kinase Inhibitor p16, also known as CDKN2A or INK4a, is a protein that regulates the cell cycle. It functions as an inhibitor of cyclin-dependent kinases (CDKs) 4 and 6, which are enzymes that play a crucial role in regulating the progression of the cell cycle.
The p16 protein is produced in response to various signals, including DNA damage and oncogene activation, and its main function is to prevent the phosphorylation and activation of the retinoblastoma protein (pRb) by CDK4/6. When pRb is not phosphorylated, it binds to and inhibits the E2F transcription factor, which results in the suppression of genes required for cell cycle progression.
Therefore, p16 acts as a tumor suppressor protein by preventing the uncontrolled proliferation of cells that can lead to cancer. Mutations or deletions in the CDKN2A gene, which encodes the p16 protein, have been found in many types of human cancers, including lung, breast, and head and neck cancers.
The Kaplan-Meier estimate is a statistical method used to calculate the survival probability over time in a population. It is commonly used in medical research to analyze time-to-event data, such as the time until a patient experiences a specific event like disease progression or death. The Kaplan-Meier estimate takes into account censored data, which occurs when some individuals are lost to follow-up before experiencing the event of interest.
The method involves constructing a survival curve that shows the proportion of subjects still surviving at different time points. At each time point, the survival probability is calculated as the product of the conditional probabilities of surviving from one time point to the next. The Kaplan-Meier estimate provides an unbiased and consistent estimator of the survival function, even when censoring is present.
In summary, the Kaplan-Meier estimate is a crucial tool in medical research for analyzing time-to-event data and estimating survival probabilities over time while accounting for censored observations.
Carcinoma, ductal refers to a type of cancer that begins in the milk ducts (tubes that carry milk from the breast to the nipple). It is most commonly found in the breast and is often referred to as "invasive ductal carcinoma" when it has spread beyond the ducts into the surrounding breast tissue. Ductal carcinoma can also occur in other organs, such as the pancreas, where it is called "pancreatic ductal adenocarcinoma." This type of cancer is usually aggressive and can metastasize (spread) to other parts of the body.
Bronchial neoplasms refer to abnormal growths or tumors in the bronchi, which are the large airways that lead into the lungs. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Malignant bronchial neoplasms are often referred to as lung cancer and can be further classified into small cell lung cancer and non-small cell lung cancer, depending on the type of cells involved.
Benign bronchial neoplasms are less common than malignant ones and may include growths such as papillomas, hamartomas, or chondromas. While benign neoplasms are not cancerous, they can still cause symptoms and complications if they grow large enough to obstruct the airways or if they become infected.
Treatment for bronchial neoplasms depends on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Human papillomavirus 16 (HPV16) is a specific type of human papillomavirus (HPV). HPV is a DNA virus that infects the skin and mucous membranes, and there are over 200 types of HPV. Some types of HPV can cause warts, while others are associated with an increased risk of certain cancers.
HPV16 is one of the high-risk types of HPV and is strongly associated with several types of cancer, including cervical, anal, penile, vulvar, and oropharyngeal (throat) cancers. HPV16 is responsible for about 50% of all cervical cancers and is the most common high-risk type of HPV found in these cancers.
HPV16 is typically transmitted through sexual contact, and most people who are sexually active will acquire at least one type of HPV at some point in their lives. While HPV infections are often harmless and clear up on their own without causing any symptoms or health problems, high-risk types like HPV16 can lead to cancer if left untreated.
Fortunately, there are vaccines available that protect against HPV16 and other high-risk types of HPV. These vaccines have been shown to be highly effective in preventing HPV-related cancers and precancerous lesions. The Centers for Disease Control and Prevention (CDC) recommends routine HPV vaccination for both boys and girls starting at age 11 or 12, although the vaccine can be given as early as age 9. Catch-up vaccinations are also recommended for older individuals who have not yet been vaccinated.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
Adrenocortical carcinoma (ACC) is a rare cancer that develops in the outer layer of the adrenal gland, known as the adrenal cortex. The adrenal glands are small hormone-producing glands located on top of each kidney. They produce important hormones such as cortisol, aldosterone, and sex steroids.
ACC is a malignant tumor that can invade surrounding tissues and organs and may metastasize (spread) to distant parts of the body. Symptoms of ACC depend on the size and location of the tumor and whether it produces excess hormones. Common symptoms include abdominal pain, a mass in the abdomen, weight loss, and weakness. Excessive production of hormones can lead to additional symptoms such as high blood pressure, Cushing's syndrome, virilization (excessive masculinization), or feminization.
The exact cause of ACC is not known, but genetic factors, exposure to certain chemicals, and radiation therapy may increase the risk of developing this cancer. Treatment options for ACC include surgery, chemotherapy, radiation therapy, and targeted therapy. The prognosis for ACC varies depending on the stage and extent of the disease at diagnosis, as well as the patient's overall health.
Esophagectomy is a surgical procedure in which part or all of the esophagus (the muscular tube that connects the throat to the stomach) is removed. This surgery is typically performed as a treatment for esophageal cancer, although it may also be used to treat other conditions such as severe damage to the esophagus from acid reflux or benign tumors.
During an esophagectomy, the surgeon will make incisions in the neck, chest, and/or abdomen to access the esophagus. The affected portion of the esophagus is then removed, and the remaining ends are reconnected, often using a section of the stomach or colon to create a new conduit for food to pass from the throat to the stomach.
Esophagectomy is a complex surgical procedure that requires significant expertise and experience on the part of the surgeon. It carries risks such as bleeding, infection, and complications related to anesthesia. Additionally, patients who undergo esophagectomy may experience difficulty swallowing, chronic pain, and other long-term complications. However, for some patients with esophageal cancer or other serious conditions affecting the esophagus, esophagectomy may be the best available treatment option.
A mutation is a permanent change in the DNA sequence of an organism's genome. Mutations can occur spontaneously or be caused by environmental factors such as exposure to radiation, chemicals, or viruses. They may have various effects on the organism, ranging from benign to harmful, depending on where they occur and whether they alter the function of essential proteins. In some cases, mutations can increase an individual's susceptibility to certain diseases or disorders, while in others, they may confer a survival advantage. Mutations are the driving force behind evolution, as they introduce new genetic variability into populations, which can then be acted upon by natural selection.
Carcinoma, signet ring cell is a type of adenocarcinoma, which is a cancer that begins in glandular cells. In signet ring cell carcinoma, the cancer cells have a characteristic appearance when viewed under a microscope. They contain large amounts of mucin, a substance that causes the nucleus of the cell to be pushed to one side, giving the cell a crescent or "signet ring" shape.
Signet ring cell carcinoma can occur in various organs, including the stomach, colon, rectum, and breast. It is often aggressive and has a poor prognosis, as it tends to grow and spread quickly. Treatment options may include surgery, chemotherapy, and radiation therapy, depending on the location and extent of the cancer.
A fatal outcome is a term used in medical context to describe a situation where a disease, injury, or illness results in the death of an individual. It is the most severe and unfortunate possible outcome of any medical condition, and is often used as a measure of the severity and prognosis of various diseases and injuries. In clinical trials and research, fatal outcome may be used as an endpoint to evaluate the effectiveness and safety of different treatments or interventions.
Penile neoplasms refer to abnormal growths or tumors in the penis. These can be benign (non-cancerous) or malignant (cancerous). The most common type of penile cancer is squamous cell carcinoma, which begins in the flat cells that line the surface of the penis. Other types of penile cancer include melanoma, basal cell carcinoma, and adenocarcinoma.
Benign penile neoplasms include conditions such as papillomas, condylomas, and peyronie's disease. These growths are usually not life-threatening, but they can cause discomfort, pain, or other symptoms that may require medical treatment.
It is important to note that any unusual changes in the penis, such as lumps, bumps, or sores, should be evaluated by a healthcare professional to determine the underlying cause and appropriate treatment.
The Ki-67 antigen is a cellular protein that is expressed in all active phases of the cell cycle (G1, S, G2, and M), but not in the resting phase (G0). It is often used as a marker for cell proliferation and can be found in high concentrations in rapidly dividing cells. Immunohistochemical staining for Ki-67 can help to determine the growth fraction of a group of cells, which can be useful in the diagnosis and prognosis of various malignancies, including cancer. The level of Ki-67 expression is often associated with the aggressiveness of the tumor and its response to treatment.
Western blotting is a laboratory technique used in molecular biology to detect and quantify specific proteins in a mixture of many different proteins. This technique is commonly used to confirm the expression of a protein of interest, determine its size, and investigate its post-translational modifications. The name "Western" blotting distinguishes this technique from Southern blotting (for DNA) and Northern blotting (for RNA).
The Western blotting procedure involves several steps:
1. Protein extraction: The sample containing the proteins of interest is first extracted, often by breaking open cells or tissues and using a buffer to extract the proteins.
2. Separation of proteins by electrophoresis: The extracted proteins are then separated based on their size by loading them onto a polyacrylamide gel and running an electric current through the gel (a process called sodium dodecyl sulfate-polyacrylamide gel electrophoresis or SDS-PAGE). This separates the proteins according to their molecular weight, with smaller proteins migrating faster than larger ones.
3. Transfer of proteins to a membrane: After separation, the proteins are transferred from the gel onto a nitrocellulose or polyvinylidene fluoride (PVDF) membrane using an electric current in a process called blotting. This creates a replica of the protein pattern on the gel but now immobilized on the membrane for further analysis.
4. Blocking: The membrane is then blocked with a blocking agent, such as non-fat dry milk or bovine serum albumin (BSA), to prevent non-specific binding of antibodies in subsequent steps.
5. Primary antibody incubation: A primary antibody that specifically recognizes the protein of interest is added and allowed to bind to its target protein on the membrane. This step may be performed at room temperature or 4°C overnight, depending on the antibody's properties.
6. Washing: The membrane is washed with a buffer to remove unbound primary antibodies.
7. Secondary antibody incubation: A secondary antibody that recognizes the primary antibody (often coupled to an enzyme or fluorophore) is added and allowed to bind to the primary antibody. This step may involve using a horseradish peroxidase (HRP)-conjugated or alkaline phosphatase (AP)-conjugated secondary antibody, depending on the detection method used later.
8. Washing: The membrane is washed again to remove unbound secondary antibodies.
9. Detection: A detection reagent is added to visualize the protein of interest by detecting the signal generated from the enzyme-conjugated or fluorophore-conjugated secondary antibody. This can be done using chemiluminescent, colorimetric, or fluorescent methods.
10. Analysis: The resulting image is analyzed to determine the presence and quantity of the protein of interest in the sample.
Western blotting is a powerful technique for identifying and quantifying specific proteins within complex mixtures. It can be used to study protein expression, post-translational modifications, protein-protein interactions, and more. However, it requires careful optimization and validation to ensure accurate and reproducible results.
Medical Definition:
"Risk factors" are any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury. They can be divided into modifiable and non-modifiable risk factors. Modifiable risk factors are those that can be changed through lifestyle choices or medical treatment, while non-modifiable risk factors are inherent traits such as age, gender, or genetic predisposition. Examples of modifiable risk factors include smoking, alcohol consumption, physical inactivity, and unhealthy diet, while non-modifiable risk factors include age, sex, and family history. It is important to note that having a risk factor does not guarantee that a person will develop the disease, but rather indicates an increased susceptibility.
Antineoplastic combined chemotherapy protocols refer to a treatment plan for cancer that involves the use of more than one antineoplastic (chemotherapy) drug given in a specific sequence and schedule. The combination of drugs is used because they may work better together to destroy cancer cells compared to using a single agent alone. This approach can also help to reduce the likelihood of cancer cells becoming resistant to the treatment.
The choice of drugs, dose, duration, and frequency are determined by various factors such as the type and stage of cancer, patient's overall health, and potential side effects. Combination chemotherapy protocols can be used in various settings, including as a primary treatment, adjuvant therapy (given after surgery or radiation to kill any remaining cancer cells), neoadjuvant therapy (given before surgery or radiation to shrink the tumor), or palliative care (to alleviate symptoms and prolong survival).
It is important to note that while combined chemotherapy protocols can be effective in treating certain types of cancer, they can also cause significant side effects, including nausea, vomiting, hair loss, fatigue, and an increased risk of infection. Therefore, patients undergoing such treatment should be closely monitored and managed by a healthcare team experienced in administering chemotherapy.
Fluorouracil is a antineoplastic medication, which means it is used to treat cancer. It is a type of chemotherapy drug known as an antimetabolite. Fluorouracil works by interfering with the growth of cancer cells and ultimately killing them. It is often used to treat colon, esophageal, stomach, and breast cancers, as well as skin conditions such as actinic keratosis and superficial basal cell carcinoma. Fluorouracil may be given by injection or applied directly to the skin in the form of a cream.
It is important to note that fluorouracil can have serious side effects, including suppression of bone marrow function, mouth sores, stomach and intestinal ulcers, and nerve damage. It should only be used under the close supervision of a healthcare professional.
Cell division is the process by which a single eukaryotic cell (a cell with a true nucleus) divides into two identical daughter cells. This complex process involves several stages, including replication of DNA, separation of chromosomes, and division of the cytoplasm. There are two main types of cell division: mitosis and meiosis.
Mitosis is the type of cell division that results in two genetically identical daughter cells. It is a fundamental process for growth, development, and tissue repair in multicellular organisms. The stages of mitosis include prophase, prometaphase, metaphase, anaphase, and telophase, followed by cytokinesis, which divides the cytoplasm.
Meiosis, on the other hand, is a type of cell division that occurs in the gonads (ovaries and testes) during the production of gametes (sex cells). Meiosis results in four genetically unique daughter cells, each with half the number of chromosomes as the parent cell. This process is essential for sexual reproduction and genetic diversity. The stages of meiosis include meiosis I and meiosis II, which are further divided into prophase, prometaphase, metaphase, anaphase, and telophase.
In summary, cell division is the process by which a single cell divides into two daughter cells, either through mitosis or meiosis. This process is critical for growth, development, tissue repair, and sexual reproduction in multicellular organisms.
RNA (Ribonucleic acid) is a single-stranded molecule similar in structure to DNA, involved in the process of protein synthesis in the cell. It acts as a messenger carrying genetic information from DNA to the ribosomes, where proteins are produced.
A neoplasm, on the other hand, is an abnormal growth of cells, which can be benign or malignant. Benign neoplasms are not cancerous and do not invade nearby tissues or spread to other parts of the body. Malignant neoplasms, however, are cancerous and have the potential to invade surrounding tissues and spread to distant sites in the body through a process called metastasis.
Therefore, an 'RNA neoplasm' is not a recognized medical term as RNA is not a type of growth or tumor. However, there are certain types of cancer-causing viruses known as oncoviruses that contain RNA as their genetic material and can cause neoplasms. For example, human T-cell leukemia virus (HTLV-1) and hepatitis C virus (HCV) are RNA viruses that can cause certain types of cancer in humans.
Keratinocytes are the predominant type of cells found in the epidermis, which is the outermost layer of the skin. These cells are responsible for producing keratin, a tough protein that provides structural support and protection to the skin. Keratinocytes undergo constant turnover, with new cells produced in the basal layer of the epidermis and older cells moving upward and eventually becoming flattened and filled with keratin as they reach the surface of the skin, where they are then shed. They also play a role in the immune response and can release cytokines and other signaling molecules to help protect the body from infection and injury.
Sensitivity and specificity are statistical measures used to describe the performance of a diagnostic test or screening tool in identifying true positive and true negative results.
* Sensitivity refers to the proportion of people who have a particular condition (true positives) who are correctly identified by the test. It is also known as the "true positive rate" or "recall." A highly sensitive test will identify most or all of the people with the condition, but may also produce more false positives.
* Specificity refers to the proportion of people who do not have a particular condition (true negatives) who are correctly identified by the test. It is also known as the "true negative rate." A highly specific test will identify most or all of the people without the condition, but may also produce more false negatives.
In medical testing, both sensitivity and specificity are important considerations when evaluating a diagnostic test. High sensitivity is desirable for screening tests that aim to identify as many cases of a condition as possible, while high specificity is desirable for confirmatory tests that aim to rule out the condition in people who do not have it.
It's worth noting that sensitivity and specificity are often influenced by factors such as the prevalence of the condition in the population being tested, the threshold used to define a positive result, and the reliability and validity of the test itself. Therefore, it's important to consider these factors when interpreting the results of a diagnostic test.
Human chromosome pair 3 consists of two rod-shaped structures present in the nucleus of each cell in the human body. Each member of the pair is a single chromosome, and together they contain the genetic material that is inherited from both parents. Chromosomes are made up of DNA, which contains the instructions for the development and function of all living organisms.
Human chromosomes are numbered from 1 to 22, with an additional two sex chromosomes (X and Y) that determine biological sex. Chromosome pair 3 is one of the autosomal pairs, meaning it contains genes that are not related to sex determination. Each member of chromosome pair 3 is identical in size and shape and contains a single long DNA molecule that is coiled tightly around histone proteins to form a compact structure.
Chromosome pair 3 is associated with several genetic disorders, including Waardenburg syndrome, which affects pigmentation and hearing; Marfan syndrome, which affects the connective tissue; and some forms of retinoblastoma, a rare eye cancer that typically affects young children.
Cervical intraepithelial neoplasia (CIN) is a term used to describe the abnormal growth and development of cells on the surface of the cervix. These changes are usually caused by human papillomavirus (HPV) infection, which is a common sexually transmitted infection. CIN is not cancer, but it can develop into cancer if left untreated.
The term "intraepithelial" refers to the fact that the abnormal cells are found in the epithelium, or the lining of the cervix. The term "neoplasia" means abnormal growth or development of cells. CIN is further classified into three grades based on the severity of the cell changes:
* CIN 1: Mild dysplasia (abnormal cell growth) affecting the lower third of the epithelium.
* CIN 2: Moderate dysplasia affecting the lower two-thirds of the epithelium.
* CIN 3: Severe dysplasia or carcinoma in situ, which means that the abnormal cells are found in the full thickness of the epithelium and have a high risk of progressing to invasive cancer if not treated.
It's important to note that CIN can regress on its own without treatment, especially in younger women. However, some cases may progress to invasive cervical cancer if left untreated. Regular Pap testing is recommended to detect and monitor any abnormal cell changes in the cervix. If CIN is detected, further diagnostic procedures such as a colposcopy or biopsy may be performed to determine the extent of the abnormality and guide treatment decisions.
Tumor suppressor genes are a type of gene that helps to regulate and prevent cells from growing and dividing too rapidly or in an uncontrolled manner. They play a critical role in preventing the formation of tumors and cancer. When functioning properly, tumor suppressor genes help to repair damaged DNA, control the cell cycle, and trigger programmed cell death (apoptosis) when necessary. However, when these genes are mutated or altered, they can lose their ability to function correctly, leading to uncontrolled cell growth and the development of tumors. Examples of tumor suppressor genes include TP53, BRCA1, and BRCA2.
Heterologous transplantation is a type of transplantation where an organ or tissue is transferred from one species to another. This is in contrast to allogeneic transplantation, where the donor and recipient are of the same species, or autologous transplantation, where the donor and recipient are the same individual.
In heterologous transplantation, the immune systems of the donor and recipient are significantly different, which can lead to a strong immune response against the transplanted organ or tissue. This is known as a graft-versus-host disease (GVHD), where the immune cells in the transplanted tissue attack the recipient's body.
Heterologous transplantation is not commonly performed in clinical medicine due to the high risk of rejection and GVHD. However, it may be used in research settings to study the biology of transplantation and to develop new therapies for transplant rejection.
Bowen's disease is a skin condition that is characterized by the growth of abnormal cells on the outermost layer of the skin (the epidermis). It is also known as squamous cell carcinoma in situ. The affected area often appears as a red, scaly patch or plaque, and it can develop anywhere on the body, but it is most commonly found on sun-exposed areas such as the face, hands, arms, and legs.
Bowen's disease is considered a precancerous condition because there is a risk that the abnormal cells could eventually develop into invasive squamous cell carcinoma, a type of skin cancer. However, not all cases of Bowen's disease will progress to cancer, and some may remain stable or even regress on their own.
The exact cause of Bowen's disease is not known, but it is thought to be associated with exposure to certain chemicals, radiation, and human papillomavirus (HPV) infection. Treatment options for Bowen's disease include cryotherapy, topical chemotherapy, photodynamic therapy, curettage and electrodessication, and surgical excision. Regular follow-up with a healthcare provider is recommended to monitor the condition and ensure that it does not progress to cancer.
Monoclonal antibodies are a type of antibody that are identical because they are produced by a single clone of cells. They are laboratory-produced molecules that act like human antibodies in the immune system. They can be designed to attach to specific proteins found on the surface of cancer cells, making them useful for targeting and treating cancer. Monoclonal antibodies can also be used as a therapy for other diseases, such as autoimmune disorders and inflammatory conditions.
Monoclonal antibodies are produced by fusing a single type of immune cell, called a B cell, with a tumor cell to create a hybrid cell, or hybridoma. This hybrid cell is then able to replicate indefinitely, producing a large number of identical copies of the original antibody. These antibodies can be further modified and engineered to enhance their ability to bind to specific targets, increase their stability, and improve their effectiveness as therapeutic agents.
Monoclonal antibodies have several mechanisms of action in cancer therapy. They can directly kill cancer cells by binding to them and triggering an immune response. They can also block the signals that promote cancer growth and survival. Additionally, monoclonal antibodies can be used to deliver drugs or radiation directly to cancer cells, increasing the effectiveness of these treatments while minimizing their side effects on healthy tissues.
Monoclonal antibodies have become an important tool in modern medicine, with several approved for use in cancer therapy and other diseases. They are continuing to be studied and developed as a promising approach to treating a wide range of medical conditions.
Tumor suppressor proteins are a type of regulatory protein that helps control the cell cycle and prevent cells from dividing and growing in an uncontrolled manner. They work to inhibit tumor growth by preventing the formation of tumors or slowing down their progression. These proteins can repair damaged DNA, regulate gene expression, and initiate programmed cell death (apoptosis) if the damage is too severe for repair.
Mutations in tumor suppressor genes, which provide the code for these proteins, can lead to a decrease or loss of function in the resulting protein. This can result in uncontrolled cell growth and division, leading to the formation of tumors and cancer. Examples of tumor suppressor proteins include p53, Rb (retinoblastoma), and BRCA1/2.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Gene expression profiling is a laboratory technique used to measure the activity (expression) of thousands of genes at once. This technique allows researchers and clinicians to identify which genes are turned on or off in a particular cell, tissue, or organism under specific conditions, such as during health, disease, development, or in response to various treatments.
The process typically involves isolating RNA from the cells or tissues of interest, converting it into complementary DNA (cDNA), and then using microarray or high-throughput sequencing technologies to determine which genes are expressed and at what levels. The resulting data can be used to identify patterns of gene expression that are associated with specific biological states or processes, providing valuable insights into the underlying molecular mechanisms of diseases and potential targets for therapeutic intervention.
In recent years, gene expression profiling has become an essential tool in various fields, including cancer research, drug discovery, and personalized medicine, where it is used to identify biomarkers of disease, predict patient outcomes, and guide treatment decisions.
Chemoradiotherapy is a medical treatment that combines chemotherapy and radiotherapy. Chemotherapy involves the use of drugs to kill or damage cancer cells, while radiotherapy uses ionizing radiation to achieve the same goal. In chemoradiotherapy, these two modalities are used simultaneously or sequentially to treat a malignancy.
The aim of chemoradiotherapy is to increase the effectiveness of treatment by targeting cancer cells with both chemotherapy and radiation therapy. This approach can be particularly effective in treating certain types of cancer, such as head and neck cancer, lung cancer, esophageal cancer, cervical cancer, anal cancer, and rectal cancer.
The specific drugs used in chemoradiotherapy and the doses and schedules of both chemotherapy and radiotherapy vary depending on the type and stage of cancer being treated. The side effects of chemoradiotherapy can be significant and may include fatigue, skin reactions, mucositis, nausea, vomiting, diarrhea, and myelosuppression. However, these side effects are usually manageable with appropriate supportive care.
SERPINs are an acronym for "serine protease inhibitors." They are a group of proteins that inhibit serine proteases, which are enzymes that cut other proteins. SERPINs are found in various tissues and body fluids, including blood, and play important roles in regulating biological processes such as inflammation, blood clotting, and cell death. They do this by forming covalent complexes with their target proteases, thereby preventing them from carrying out their proteolytic activities. Mutations in SERPIN genes have been associated with several genetic disorders, including emphysema, cirrhosis, and dementia.
Gene amplification is a process in molecular biology where a specific gene or set of genes are copied multiple times, leading to an increased number of copies of that gene within the genome. This can occur naturally in cells as a response to various stimuli, such as stress or exposure to certain chemicals, but it can also be induced artificially through laboratory techniques for research purposes.
In cancer biology, gene amplification is often associated with tumor development and progression, where the amplified genes can contribute to increased cell growth, survival, and drug resistance. For example, the overamplification of the HER2/neu gene in breast cancer has been linked to more aggressive tumors and poorer patient outcomes.
In diagnostic and research settings, gene amplification techniques like polymerase chain reaction (PCR) are commonly used to detect and analyze specific genes or genetic sequences of interest. These methods allow researchers to quickly and efficiently generate many copies of a particular DNA sequence, facilitating downstream analysis and detection of low-abundance targets.
Leukoplakia is a medical term used to describe a white or gray patch that develops on the mucous membranes lining the inside of the mouth. These patches are typically caused by excessive cell growth and cannot be easily scraped off. Leukoplakia is often associated with long-term tobacco use, including smoking and chewing tobacco, as well as alcohol consumption. While most cases of leukoplakia are benign, a small percentage can develop into oral cancer, so it's essential to have any suspicious patches evaluated by a healthcare professional.
Eyelid neoplasms refer to abnormal growths or tumors that develop in the tissues of the eyelids. These growths can be benign (non-cancerous) or malignant (cancerous). Common types of benign eyelid neoplasms include papillomas, hemangiomas, and nevi. Malignant eyelid neoplasms are typically classified as basal cell carcinomas, squamous cell carcinomas, or melanomas. These malignant tumors can be aggressive and may spread to other parts of the body if left untreated. Treatment options for eyelid neoplasms depend on the type, size, and location of the growth, as well as the patient's overall health. Surgical excision is often the preferred treatment approach, although radiation therapy and chemotherapy may also be used in some cases. Regular follow-up care is important to monitor for recurrence or new growths.
Pathologic neovascularization is the abnormal growth of new blood vessels in previously avascular tissue or excessive growth within existing vasculature, which occurs as a result of hypoxia, inflammation, or angiogenic stimuli. These newly formed vessels are often disorganized, fragile, and lack proper vessel hierarchy, leading to impaired blood flow and increased vascular permeability. Pathologic neovascularization can be observed in various diseases such as cancer, diabetic retinopathy, age-related macular degeneration, and chronic inflammation. This process contributes to disease progression by promoting tumor growth, metastasis, and edema formation, ultimately leading to tissue damage and organ dysfunction.
A tumor virus infection is a condition in which a person's cells become cancerous or transformed due to the integration and disruption of normal cellular functions by a viral pathogen. These viruses are also known as oncoviruses, and they can cause tumors or cancer by altering the host cell's genetic material, promoting uncontrolled cell growth and division, evading immune surveillance, and inhibiting apoptosis (programmed cell death).
Examples of tumor viruses include:
1. DNA tumor viruses: These are double-stranded DNA viruses that can cause cancer in humans. Examples include human papillomavirus (HPV), hepatitis B virus (HBV), and Merkel cell polyomavirus (MCV).
2. RNA tumor viruses: Also known as retroviruses, these single-stranded RNA viruses can cause cancer in humans. Examples include human T-cell leukemia virus type 1 (HTLV-1) and human immunodeficiency virus (HIV).
Tumor virus infections are responsible for approximately 15-20% of all cancer cases worldwide, making them a significant public health concern. Prevention strategies, such as vaccination against HPV and HBV, have been shown to reduce the incidence of associated cancers.
Palatal neoplasms refer to abnormal growths or tumors that occur on the palate, which is the roof of the mouth. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slower growing and less likely to spread, while malignant neoplasms are more aggressive and can invade nearby tissues and organs.
Palatal neoplasms can have various causes, including genetic factors, environmental exposures, and viral infections. They may present with symptoms such as mouth pain, difficulty swallowing, swelling or lumps in the mouth, bleeding, or numbness in the mouth or face.
The diagnosis of palatal neoplasms typically involves a thorough clinical examination, imaging studies, and sometimes biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or spread of the neoplasm.
Gallbladder neoplasms refer to abnormal growths in the tissue of the gallbladder, which can be benign or malignant. Benign neoplasms are non-cancerous and typically do not spread to other parts of the body. Malignant neoplasms, also known as gallbladder cancer, can invade nearby tissues and organs and may metastasize (spread) to distant parts of the body. Gallbladder neoplasms can cause symptoms such as abdominal pain, jaundice, and nausea, but they are often asymptomatic until they have advanced to an advanced stage. The exact causes of gallbladder neoplasms are not fully understood, but risk factors include gallstones, chronic inflammation of the gallbladder, and certain inherited genetic conditions.
Lymph nodes are small, bean-shaped organs that are part of the immune system. They are found throughout the body, especially in the neck, armpits, groin, and abdomen. Lymph nodes filter lymph fluid, which carries waste and unwanted substances such as bacteria, viruses, and cancer cells. They contain white blood cells called lymphocytes that help fight infections and diseases by attacking and destroying the harmful substances found in the lymph fluid. When an infection or disease is present, lymph nodes may swell due to the increased number of immune cells and fluid accumulation as they work to fight off the invaders.
Viral DNA refers to the genetic material present in viruses that consist of DNA as their core component. Deoxyribonucleic acid (DNA) is one of the two types of nucleic acids that are responsible for storing and transmitting genetic information in living organisms. Viruses are infectious agents much smaller than bacteria that can only replicate inside the cells of other organisms, called hosts.
Viral DNA can be double-stranded (dsDNA) or single-stranded (ssDNA), depending on the type of virus. Double-stranded DNA viruses have a genome made up of two complementary strands of DNA, while single-stranded DNA viruses contain only one strand of DNA.
Examples of dsDNA viruses include Adenoviruses, Herpesviruses, and Poxviruses, while ssDNA viruses include Parvoviruses and Circoviruses. Viral DNA plays a crucial role in the replication cycle of the virus, encoding for various proteins necessary for its multiplication and survival within the host cell.
Down-regulation is a process that occurs in response to various stimuli, where the number or sensitivity of cell surface receptors or the expression of specific genes is decreased. This process helps maintain homeostasis within cells and tissues by reducing the ability of cells to respond to certain signals or molecules.
In the context of cell surface receptors, down-regulation can occur through several mechanisms:
1. Receptor internalization: After binding to their ligands, receptors can be internalized into the cell through endocytosis. Once inside the cell, these receptors may be degraded or recycled back to the cell surface in smaller numbers.
2. Reduced receptor synthesis: Down-regulation can also occur at the transcriptional level, where the expression of genes encoding for specific receptors is decreased, leading to fewer receptors being produced.
3. Receptor desensitization: Prolonged exposure to a ligand can lead to a decrease in receptor sensitivity or affinity, making it more difficult for the cell to respond to the signal.
In the context of gene expression, down-regulation refers to the decreased transcription and/or stability of specific mRNAs, leading to reduced protein levels. This process can be induced by various factors, including microRNA (miRNA)-mediated regulation, histone modification, or DNA methylation.
Down-regulation is an essential mechanism in many physiological processes and can also contribute to the development of several diseases, such as cancer and neurodegenerative disorders.
A base sequence in the context of molecular biology refers to the specific order of nucleotides in a DNA or RNA molecule. In DNA, these nucleotides are adenine (A), guanine (G), cytosine (C), and thymine (T). In RNA, uracil (U) takes the place of thymine. The base sequence contains genetic information that is transcribed into RNA and ultimately translated into proteins. It is the exact order of these bases that determines the genetic code and thus the function of the DNA or RNA molecule.
Cadherins are a type of cell adhesion molecule that play a crucial role in the development and maintenance of intercellular junctions. They are transmembrane proteins that mediate calcium-dependent homophilic binding between adjacent cells, meaning that they bind to identical cadherin molecules on neighboring cells.
There are several types of cadherins, including classical cadherins, desmosomal cadherins, and protocadherins, each with distinct functions and localization in tissues. Classical cadherins, also known as type I cadherins, are the most well-studied and are essential for the formation of adherens junctions, which help to maintain cell-to-cell contact and tissue architecture.
Desmosomal cadherins, on the other hand, are critical for the formation and maintenance of desmosomes, which are specialized intercellular junctions that provide mechanical strength and stability to tissues. Protocadherins are a diverse family of cadherin-related proteins that have been implicated in various developmental processes, including neuronal connectivity and tissue patterning.
Mutations in cadherin genes have been associated with several human diseases, including cancer, neurological disorders, and heart defects. Therefore, understanding the structure, function, and regulation of cadherins is essential for elucidating their roles in health and disease.
Tumor burden is a term used to describe the total amount of cancer in the body. It can refer to the number of tumors, the size of the tumors, or the amount of cancer cells in the body. In research and clinical trials, tumor burden is often measured to assess the effectiveness of treatments or to monitor disease progression. High tumor burden can cause various symptoms and complications, depending on the type and location of the cancer. It can also affect a person's prognosis and treatment options.
Adenocarcinoma, follicular is a type of cancer that develops in the follicular cells of the thyroid gland. The thyroid gland is a butterfly-shaped endocrine gland located in the neck that produces hormones responsible for regulating various bodily functions such as metabolism and growth.
Follicular adenocarcinoma arises from the follicular cells, which are responsible for producing thyroid hormones. This type of cancer is typically slow-growing and may not cause any symptoms in its early stages. However, as it progresses, it can lead to a variety of symptoms such as a lump or nodule in the neck, difficulty swallowing, hoarseness, or pain in the neck or throat.
Follicular adenocarcinoma is usually treated with surgical removal of the thyroid gland (thyroidectomy), followed by radioactive iodine therapy to destroy any remaining cancer cells. In some cases, additional treatments such as radiation therapy or chemotherapy may be necessary. The prognosis for follicular adenocarcinoma is generally good, with a five-year survival rate of around 90%. However, this can vary depending on the stage and aggressiveness of the cancer at the time of diagnosis.
Otorhinolaryngologic neoplasms refer to abnormal growths or tumors that occur in the structures related to the head and neck, which are studied and managed by the medical specialty of otorhinolaryngology (also known as ENT - ear, nose, and throat). These neoplasms can be benign or malignant and can develop in various areas such as:
1. The external auditory canal (the ear canal)
2. The middle ear and inner ear
3. The nasal cavity and paranasal sinuses
4. The pharynx (throat), including the nasopharynx, oropharynx, and hypopharynx
5. The larynx (voice box)
The symptoms and treatment options for otorhinolaryngologic neoplasms depend on their location, size, and type (benign or malignant). Common symptoms include:
* A mass or growth in the ear, nose, or throat
* Difficulty swallowing or speaking
* Hearing loss or tinnitus (ringing in the ears)
* Nosebleeds or nasal congestion
* Facial pain or numbness
* Swelling in the neck or face
It is essential to consult an otorhinolaryngologist if any concerning symptoms are present, as early detection and treatment can significantly improve outcomes.
Tracheal neoplasms refer to abnormal growths or tumors in the trachea, which is the windpipe that carries air from the nose and throat to the lungs. These growths can be benign (non-cancerous) or malignant (cancerous). Malignant tracheal neoplasms are relatively rare and can be primary (originating in the trachea) or secondary (spreading from another part of the body, such as lung cancer). Primary tracheal cancers can be squamous cell carcinoma, adenoid cystic carcinoma, mucoepidermoid carcinoma, or sarcomas. Symptoms may include cough, difficulty breathing, wheezing, or chest pain. Treatment options depend on the type, size, and location of the neoplasm and can include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Signal transduction is the process by which a cell converts an extracellular signal, such as a hormone or neurotransmitter, into an intracellular response. This involves a series of molecular events that transmit the signal from the cell surface to the interior of the cell, ultimately resulting in changes in gene expression, protein activity, or metabolism.
The process typically begins with the binding of the extracellular signal to a receptor located on the cell membrane. This binding event activates the receptor, which then triggers a cascade of intracellular signaling molecules, such as second messengers, protein kinases, and ion channels. These molecules amplify and propagate the signal, ultimately leading to the activation or inhibition of specific cellular responses.
Signal transduction pathways are highly regulated and can be modulated by various factors, including other signaling molecules, post-translational modifications, and feedback mechanisms. Dysregulation of these pathways has been implicated in a variety of diseases, including cancer, diabetes, and neurological disorders.
A vaginal smear, also known as a Pap test or Pap smear, is a medical procedure in which a sample of cells is collected from the cervix (the lower part of the uterus that opens into the vagina) and examined under a microscope. The purpose of this test is to detect abnormal cells, including precancerous changes, that may indicate the presence of cervical cancer or other conditions such as infections or inflammation.
During the procedure, a speculum is inserted into the vagina to allow the healthcare provider to visualize the cervix. A spatula or brush is then used to gently scrape cells from the surface of the cervix. The sample is spread onto a microscope slide and sent to a laboratory for analysis.
Regular Pap smears are recommended for women as part of their routine healthcare, as they can help detect abnormalities at an early stage when they are more easily treated. The frequency of Pap smears may vary depending on age, medical history, and other factors. It is important to follow the recommendations of a healthcare provider regarding the timing and frequency of Pap smears.
A laryngectomy is a surgical procedure that involves the removal of the larynx, also known as the voice box. This is typically performed in cases of advanced laryngeal cancer or other severe diseases of the larynx. After the surgery, the patient will have a permanent stoma (opening) in the neck to allow for breathing. The ability to speak after a total laryngectomy can be restored through various methods such as esophageal speech, tracheoesophageal puncture with a voice prosthesis, or electronic devices.
The Predictive Value of Tests, specifically the Positive Predictive Value (PPV) and Negative Predictive Value (NPV), are measures used in diagnostic tests to determine the probability that a positive or negative test result is correct.
Positive Predictive Value (PPV) is the proportion of patients with a positive test result who actually have the disease. It is calculated as the number of true positives divided by the total number of positive results (true positives + false positives). A higher PPV indicates that a positive test result is more likely to be a true positive, and therefore the disease is more likely to be present.
Negative Predictive Value (NPV) is the proportion of patients with a negative test result who do not have the disease. It is calculated as the number of true negatives divided by the total number of negative results (true negatives + false negatives). A higher NPV indicates that a negative test result is more likely to be a true negative, and therefore the disease is less likely to be present.
The predictive value of tests depends on the prevalence of the disease in the population being tested, as well as the sensitivity and specificity of the test. A test with high sensitivity and specificity will generally have higher predictive values than a test with low sensitivity and specificity. However, even a highly sensitive and specific test can have low predictive values if the prevalence of the disease is low in the population being tested.
Salivary gland neoplasms refer to abnormal growths or tumors that develop in the salivary glands. These glands are responsible for producing saliva, which helps in digestion, lubrication of food and maintaining oral health. Salivary gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms are slow-growing and typically do not spread to other parts of the body. They may cause symptoms such as swelling, painless lumps, or difficulty swallowing if they grow large enough to put pressure on surrounding tissues.
Malignant neoplasms, on the other hand, can be aggressive and have the potential to invade nearby structures and metastasize (spread) to distant organs. Symptoms of malignant salivary gland neoplasms may include rapid growth, pain, numbness, or paralysis of facial nerves.
Salivary gland neoplasms can occur in any of the major salivary glands (parotid, submandibular, and sublingual glands) or in the minor salivary glands located throughout the mouth and throat. The exact cause of these neoplasms is not fully understood, but risk factors may include exposure to radiation, certain viral infections, and genetic predisposition.
A xenograft model antitumor assay is a type of preclinical cancer research study that involves transplanting human tumor cells or tissues into an immunodeficient mouse. This model allows researchers to study the effects of various treatments, such as drugs or immune therapies, on human tumors in a living organism.
In this assay, human tumor cells or tissues are implanted into the mouse, typically under the skin or in another organ, where they grow and form a tumor. Once the tumor has established, the mouse is treated with the experimental therapy, and the tumor's growth is monitored over time. The response of the tumor to the treatment is then assessed by measuring changes in tumor size or weight, as well as other parameters such as survival rate and metastasis.
Xenograft model antitumor assays are useful for evaluating the efficacy and safety of new cancer therapies before they are tested in human clinical trials. They provide valuable information on how the tumors respond to treatment, drug pharmacokinetics, and toxicity, which can help researchers optimize dosing regimens and identify potential side effects. However, it is important to note that xenograft models have limitations, such as differences in tumor biology between mice and humans, and may not always predict how well a therapy will work in human patients.
In situ hybridization (ISH) is a molecular biology technique used to detect and localize specific nucleic acid sequences, such as DNA or RNA, within cells or tissues. This technique involves the use of a labeled probe that is complementary to the target nucleic acid sequence. The probe can be labeled with various types of markers, including radioisotopes, fluorescent dyes, or enzymes.
During the ISH procedure, the labeled probe is hybridized to the target nucleic acid sequence in situ, meaning that the hybridization occurs within the intact cells or tissues. After washing away unbound probe, the location of the labeled probe can be visualized using various methods depending on the type of label used.
In situ hybridization has a wide range of applications in both research and diagnostic settings, including the detection of gene expression patterns, identification of viral infections, and diagnosis of genetic disorders.
A "second primary neoplasm" is a distinct, new cancer or malignancy that develops in a person who has already had a previous cancer. It is not a recurrence or metastasis of the original tumor, but rather an independent cancer that arises in a different location or organ system. The development of second primary neoplasms can be influenced by various factors such as genetic predisposition, environmental exposures, and previous treatments like chemotherapy or radiation therapy.
It is important to note that the definition of "second primary neoplasm" may vary slightly depending on the specific source or context. In general medical usage, it refers to a new, separate cancer; however, in some research or clinical settings, there might be more precise criteria for defining and diagnosing second primary neoplasms.
Adenocarcinoma, mucinous is a type of cancer that begins in the glandular cells that line certain organs and produce mucin, a substance that lubricates and protects tissues. This type of cancer is characterized by the presence of abundant pools of mucin within the tumor. It typically develops in organs such as the colon, rectum, lungs, pancreas, and ovaries.
Mucinous adenocarcinomas tend to have a distinct appearance under the microscope, with large pools of mucin pushing aside the cancer cells. They may also have a different clinical behavior compared to other types of adenocarcinomas, such as being more aggressive or having a worse prognosis in some cases.
It is important to note that while a diagnosis of adenocarcinoma, mucinous can be serious, the prognosis and treatment options may vary depending on several factors, including the location of the cancer, the stage at which it was diagnosed, and the individual's overall health.
Experimental neoplasms refer to abnormal growths or tumors that are induced and studied in a controlled laboratory setting, typically in animals or cell cultures. These studies are conducted to understand the fundamental mechanisms of cancer development, progression, and potential treatment strategies. By manipulating various factors such as genetic mutations, environmental exposures, and pharmacological interventions, researchers can gain valuable insights into the complex processes underlying neoplasm formation and identify novel targets for cancer therapy. It is important to note that experimental neoplasms may not always accurately represent human cancers, and further research is needed to translate these findings into clinically relevant applications.
Gene expression is the process by which the information encoded in a gene is used to synthesize a functional gene product, such as a protein or RNA molecule. This process involves several steps: transcription, RNA processing, and translation. During transcription, the genetic information in DNA is copied into a complementary RNA molecule, known as messenger RNA (mRNA). The mRNA then undergoes RNA processing, which includes adding a cap and tail to the mRNA and splicing out non-coding regions called introns. The resulting mature mRNA is then translated into a protein on ribosomes in the cytoplasm through the process of translation.
The regulation of gene expression is a complex and highly controlled process that allows cells to respond to changes in their environment, such as growth factors, hormones, and stress signals. This regulation can occur at various stages of gene expression, including transcriptional activation or repression, RNA processing, mRNA stability, and translation. Dysregulation of gene expression has been implicated in many diseases, including cancer, genetic disorders, and neurological conditions.
Radiotherapy dosage refers to the total amount of radiation energy that is absorbed by tissues or organs, typically measured in units of Gray (Gy), during a course of radiotherapy treatment. It is the product of the dose rate (the amount of radiation delivered per unit time) and the duration of treatment. The prescribed dosage for cancer treatments can range from a few Gray to more than 70 Gy, depending on the type and location of the tumor, the patient's overall health, and other factors. The goal of radiotherapy is to deliver a sufficient dosage to destroy the cancer cells while minimizing damage to surrounding healthy tissues.
Neoplasm grading is a system used by pathologists to classify the degree of abnormality in cells that make up a tumor (neoplasm). It provides an assessment of how quickly the tumor is likely to grow and spread. The grade helps doctors predict the prognosis and determine the best treatment options.
Neoplasm grading typically involves evaluating certain cellular features under a microscope, such as:
1. Differentiation or degree of maturity: This refers to how closely the tumor cells resemble their normal counterparts in terms of size, shape, and organization. Well-differentiated tumors have cells that look more like normal cells and are usually slower growing. Poorly differentiated tumors have cells that appear very abnormal and tend to grow and spread more aggressively.
2. Mitotic count: This is the number of times the tumor cells divide (mitosis) within a given area. A higher mitotic count indicates a faster-growing tumor.
3. Necrosis: This refers to areas of dead tissue within the tumor. A significant amount of necrosis may suggest a more aggressive tumor.
Based on these and other factors, pathologists assign a grade to the tumor using a standardized system, such as the Bloom-Richardson or Scarff-Bloom-Richardson grading systems for breast cancer or the Fuhrman grading system for kidney cancer. The grade usually consists of a number or a range (e.g., G1, G2, G3, or G4) or a combination of grades (e.g., low grade, intermediate grade, and high grade).
In general, higher-grade tumors have a worse prognosis than lower-grade tumors because they are more likely to grow quickly, invade surrounding tissues, and metastasize (spread) to other parts of the body. However, neoplasm grading is just one aspect of cancer diagnosis and treatment planning. Other factors, such as the stage of the disease, location of the tumor, patient's overall health, and specific molecular markers, are also considered when making treatment decisions.
Conjunctival neoplasms refer to abnormal growths or tumors that develop on the conjunctiva, which is the thin, clear mucous membrane that covers the inner surface of the eyelids and the outer surface of the eye. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign conjunctival neoplasms are typically slow-growing and do not spread to other parts of the body. They may include lesions such as conjunctival cysts, papillomas, or naevi (moles). These growths can usually be removed through simple surgical procedures with a good prognosis.
Malignant conjunctival neoplasms, on the other hand, are cancerous and have the potential to invade surrounding tissues and spread to other parts of the body. The most common type of malignant conjunctival neoplasm is squamous cell carcinoma, which arises from the epithelial cells that line the surface of the conjunctiva. Other less common types include melanoma, lymphoma, and adenocarcinoma.
Malignant conjunctival neoplasms typically require more extensive treatment, such as surgical excision, radiation therapy, or chemotherapy. The prognosis for malignant conjunctival neoplasms depends on the type and stage of the cancer at the time of diagnosis, as well as the patient's overall health and age. Early detection and prompt treatment are key to improving outcomes in patients with these conditions.
Carcinogens are agents (substances or mixtures of substances) that can cause cancer. They may be naturally occurring or man-made. Carcinogens can increase the risk of cancer by altering cellular DNA, disrupting cellular function, or promoting cell growth. Examples of carcinogens include certain chemicals found in tobacco smoke, asbestos, UV radiation from the sun, and some viruses.
It's important to note that not all exposures to carcinogens will result in cancer, and the risk typically depends on factors such as the level and duration of exposure, individual genetic susceptibility, and lifestyle choices. The International Agency for Research on Cancer (IARC) classifies carcinogens into different groups based on the strength of evidence linking them to cancer:
Group 1: Carcinogenic to humans
Group 2A: Probably carcinogenic to humans
Group 2B: Possibly carcinogenic to humans
Group 3: Not classifiable as to its carcinogenicity to humans
Group 4: Probably not carcinogenic to humans
This information is based on medical research and may be subject to change as new studies become available. Always consult a healthcare professional for medical advice.
4-Nitroquinoline-1-oxide is a chemical compound that is often used in laboratory research as a carcinogenic agent. Its molecular formula is C6H4N2O3, and it is known to cause DNA damage and mutations, which can lead to the development of cancer. It is primarily used in scientific research to study the mechanisms of carcinogenesis and to test the effectiveness of potential cancer treatments.
It is important to note that 4-Nitroquinoline-1-oxide is not a medication or a treatment for any medical condition, and it should only be handled by trained professionals in a controlled laboratory setting.
Embryonal carcinoma stem cells (ECSCs) are a type of cancer stem cell found in embryonal carcinomas, which are a rare form of germ cell tumor that primarily affect the testicles and ovaries. These stem cells are characterized by their ability to differentiate into various cell types, similar to embryonic stem cells. They are believed to play a key role in the development and progression of embryonal carcinomas, as they can self-renew and generate the heterogeneous population of cancer cells that make up the tumor.
Embryonal carcinoma stem cells have been studied extensively as a model system for understanding the biology of cancer stem cells and developing new therapies for germ cell tumors. They are known to express specific markers, such as Oct-4, Nanog, and Sox2, which are also expressed in embryonic stem cells and are involved in maintaining their pluripotency.
It is important to note that while embryonal carcinoma stem cells share some similarities with embryonic stem cells, they are distinct from them and have undergone malignant transformation, making them a target for cancer therapy.
Up-regulation is a term used in molecular biology and medicine to describe an increase in the expression or activity of a gene, protein, or receptor in response to a stimulus. This can occur through various mechanisms such as increased transcription, translation, or reduced degradation of the molecule. Up-regulation can have important functional consequences, for example, enhancing the sensitivity or response of a cell to a hormone, neurotransmitter, or drug. It is a normal physiological process that can also be induced by disease or pharmacological interventions.
Multivariate analysis is a statistical method used to examine the relationship between multiple independent variables and a dependent variable. It allows for the simultaneous examination of the effects of two or more independent variables on an outcome, while controlling for the effects of other variables in the model. This technique can be used to identify patterns, associations, and interactions among multiple variables, and is commonly used in medical research to understand complex health outcomes and disease processes. Examples of multivariate analysis methods include multiple regression, factor analysis, cluster analysis, and discriminant analysis.
Adjuvant radiotherapy is a type of cancer treatment that uses radiation therapy as an adjunct to a primary surgical procedure. The goal of adjuvant radiotherapy is to eliminate any remaining microscopic cancer cells that may be present in the surrounding tissues after surgery, thereby reducing the risk of local recurrence and improving the chances of cure.
Radiotherapy involves the use of high-energy radiation to destroy cancer cells and shrink tumors. In adjuvant radiotherapy, the radiation is usually delivered to the tumor bed and regional lymph nodes in order to target any potential sites of residual disease. The timing and dosing of adjuvant radiotherapy may vary depending on the type and stage of cancer being treated, as well as other factors such as patient age and overall health status.
Adjuvant radiotherapy is commonly used in the treatment of various types of cancer, including breast, colorectal, lung, head and neck, and gynecologic cancers. Its use has been shown to improve survival rates and reduce the risk of recurrence in many cases, making it an important component of comprehensive cancer care.
Maxillary sinus neoplasms refer to abnormal growths or tumors that develop in the maxillary sinuses, which are located in the upper part of your cheekbones, below your eyes. These growths can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms may include conditions such as an osteoma (a benign bone tumor), a papilloma (a benign growth of the lining of the sinus), or a fibrous dysplasia (a condition where bone is replaced by fibrous tissue).
Malignant neoplasms, on the other hand, can be primary (originating in the maxillary sinuses) or secondary (spreading to the maxillary sinuses from another site in the body). Common types of malignant tumors that arise in the maxillary sinus include squamous cell carcinoma, adenocarcinoma, and mucoepidermoid carcinoma.
Symptoms of maxillary sinus neoplasms may include nasal congestion, nosebleeds, facial pain or numbness, vision changes, and difficulty swallowing or speaking. Treatment options depend on the type, size, and location of the tumor but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Endometrial neoplasms refer to abnormal growths or tumors in the endometrium, which is the innermost lining of the uterus. These neoplasms can be benign (non-cancerous) or malignant (cancerous). The two main types of endometrial cancer are type I, also known as endometrioid adenocarcinoma, and type II, which includes serous carcinoma, clear cell carcinoma, and carcinosarcoma.
Type I endometrial cancers are usually estrogen-dependent and associated with risk factors such as obesity, diabetes, and prolonged exposure to estrogen without progesterone. They tend to grow more slowly and have a better prognosis than type II cancers.
Type II endometrial cancers are less common but more aggressive, often presenting at an advanced stage and having a worse prognosis. They are not typically associated with hormonal factors and may occur in women who have gone through menopause.
Endometrial neoplasms can also include benign growths such as polyps, hyperplasia, and endometriosis. While these conditions are not cancerous, they can increase the risk of developing endometrial cancer and should be monitored closely by a healthcare provider.
Cyclin D1 is a type of cyclin protein that plays a crucial role in the regulation of the cell cycle, which is the process by which cells divide and grow. Specifically, Cyclin D1 is involved in the transition from the G1 phase to the S phase of the cell cycle. It does this by forming a complex with and acting as a regulatory subunit of cyclin-dependent kinase 4 (CDK4) or CDK6, which phosphorylates and inactivates the retinoblastoma protein (pRb). This allows the E2F transcription factors to be released and activate the transcription of genes required for DNA replication and cell cycle progression.
Overexpression of Cyclin D1 has been implicated in the development of various types of cancer, as it can lead to uncontrolled cell growth and division. Therefore, Cyclin D1 is an important target for cancer therapy, and inhibitors of CDK4/6 have been developed to treat certain types of cancer that overexpress Cyclin D1.
Epithelium is the tissue that covers the outer surface of the body, lines the internal cavities and organs, and forms various glands. It is composed of one or more layers of tightly packed cells that have a uniform shape and size, and rest on a basement membrane. Epithelial tissues are avascular, meaning they do not contain blood vessels, and are supplied with nutrients by diffusion from the underlying connective tissue.
Epithelial cells perform a variety of functions, including protection, secretion, absorption, excretion, and sensation. They can be classified based on their shape and the number of cell layers they contain. The main types of epithelium are:
1. Squamous epithelium: composed of flat, scalelike cells that fit together like tiles on a roof. It forms the lining of blood vessels, air sacs in the lungs, and the outermost layer of the skin.
2. Cuboidal epithelium: composed of cube-shaped cells with equal height and width. It is found in glands, tubules, and ducts.
3. Columnar epithelium: composed of tall, rectangular cells that are taller than they are wide. It lines the respiratory, digestive, and reproductive tracts.
4. Pseudostratified epithelium: appears stratified or layered but is actually made up of a single layer of cells that vary in height. The nuclei of these cells appear at different levels, giving the tissue a stratified appearance. It lines the respiratory and reproductive tracts.
5. Transitional epithelium: composed of several layers of cells that can stretch and change shape to accommodate changes in volume. It is found in the urinary bladder and ureters.
Epithelial tissue provides a barrier between the internal and external environments, protecting the body from physical, chemical, and biological damage. It also plays a crucial role in maintaining homeostasis by regulating the exchange of substances between the body and its environment.
Alpha-fetoprotein (AFP) is a protein produced by the yolk sac and the liver during fetal development. In adults, AFP is normally present in very low levels in the blood. However, abnormal production of AFP can occur in certain medical conditions, such as:
* Liver cancer or hepatocellular carcinoma (HCC)
* Germ cell tumors, including non-seminomatous testicular cancer and ovarian cancer
* Hepatitis or liver inflammation
* Certain types of benign liver disease, such as cirrhosis or hepatic adenomas
Elevated levels of AFP in the blood can be detected through a simple blood test. This test is often used as a tumor marker to help diagnose and monitor certain types of cancer, particularly HCC. However, it's important to note that an elevated AFP level alone is not enough to diagnose cancer, and further testing is usually needed to confirm the diagnosis. Additionally, some non-cancerous conditions can also cause elevated AFP levels, so it's important to interpret the test results in the context of the individual's medical history and other diagnostic tests.
Carcinoembryonic antigen (CEA) is a protein that is normally produced in small amounts during fetal development. In adults, low levels of CEA can be found in the blood, but elevated levels are typically associated with various types of cancer, particularly colon, rectal, and breast cancer.
Measurement of CEA levels in the blood is sometimes used as a tumor marker to monitor response to treatment, detect recurrence, or screen for secondary cancers in patients with a history of certain types of cancer. However, it's important to note that CEA is not a specific or sensitive indicator of cancer and can be elevated in various benign conditions such as inflammation, smoking, and some gastrointestinal diseases. Therefore, the test should be interpreted in conjunction with other clinical and diagnostic findings.
Carcinosarcoma is a rare and aggressive type of cancer that occurs when malignant epithelial cells (carcinoma) coexist with malignant mesenchymal cells (sarcoma) in the same tumor. This mixed malignancy can arise in various organs, but it is most commonly found in the female reproductive tract, particularly in the uterus and ovaries.
In a carcinosarcoma, the epithelial component typically forms glands or nests, while the mesenchymal component can differentiate into various tissue types such as bone, cartilage, muscle, or fat. The presence of both malignant components in the same tumor makes carcinosarcomas particularly aggressive and challenging to treat.
Carcinosarcomas are also known by other names, including sarcomatoid carcinoma, spindle cell carcinoma, or pseudosarcoma. The prognosis for patients with carcinosarcoma is generally poor due to its high propensity for local recurrence and distant metastasis. Treatment usually involves a combination of surgery, radiation therapy, and chemotherapy.
Papillary and follicular carcinomas are both types of differentiated thyroid cancer. They are called "differentiated" because the cells still have some features of normal thyroid cells. These cancers tend to grow slowly and usually have a good prognosis, especially if they are treated early.
Papillary carcinoma is the most common type of thyroid cancer, accounting for about 80% of all cases. It tends to grow in finger-like projections called papillae, which give the tumor its name. Papillary carcinoma often spreads to nearby lymph nodes, but it is usually still treatable and curable.
Follicular carcinoma is less common than papillary carcinoma, accounting for about 10-15% of all thyroid cancers. It tends to grow in round clusters called follicles, which give the tumor its name. Follicular carcinoma is more likely to spread to distant parts of the body, such as the lungs or bones, than papillary carcinoma. However, it is still usually treatable and curable if it is caught early.
It's important to note that while these cancers are called "papillary" and "follicular," they are not the same as benign (non-cancerous) tumors called papillomas or follicular adenomas, which do not have the potential to spread or become life-threatening.
Hyperplasia is a medical term that refers to an abnormal increase in the number of cells in an organ or tissue, leading to an enlargement of the affected area. It's a response to various stimuli such as hormones, chronic irritation, or inflammation. Hyperplasia can be physiological, like the growth of breast tissue during pregnancy, or pathological, like in the case of benign or malignant tumors. The process is generally reversible if the stimulus is removed. It's important to note that hyperplasia itself is not cancerous, but some forms of hyperplasia can increase the risk of developing cancer over time.
Oligonucleotide Array Sequence Analysis is a type of microarray analysis that allows for the simultaneous measurement of the expression levels of thousands of genes in a single sample. In this technique, oligonucleotides (short DNA sequences) are attached to a solid support, such as a glass slide, in a specific pattern. These oligonucleotides are designed to be complementary to specific target mRNA sequences from the sample being analyzed.
During the analysis, labeled RNA or cDNA from the sample is hybridized to the oligonucleotide array. The level of hybridization is then measured and used to determine the relative abundance of each target sequence in the sample. This information can be used to identify differences in gene expression between samples, which can help researchers understand the underlying biological processes involved in various diseases or developmental stages.
It's important to note that this technique requires specialized equipment and bioinformatics tools for data analysis, as well as careful experimental design and validation to ensure accurate and reproducible results.
A mucous membrane is a type of moist, protective lining that covers various body surfaces inside the body, including the respiratory, gastrointestinal, and urogenital tracts, as well as the inner surface of the eyelids and the nasal cavity. These membranes are composed of epithelial cells that produce mucus, a slippery secretion that helps trap particles, microorganisms, and other foreign substances, preventing them from entering the body or causing damage to tissues. The mucous membrane functions as a barrier against infection and irritation while also facilitating the exchange of gases, nutrients, and waste products between the body and its environment.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
Single-Stranded Conformational Polymorphism (SSCP) is not a medical condition but rather a laboratory technique used in molecular biology and genetics. It refers to the phenomenon where a single-stranded DNA or RNA molecule can adopt different conformations or shapes based on its nucleotide sequence, even if the difference in the sequence is as small as a single base pair change. This property is used in SSCP analysis to detect mutations or variations in DNA or RNA sequences.
In SSCP analysis, the denatured single-stranded DNA or RNA sample is subjected to electrophoresis on a non-denaturing polyacrylamide gel. The different conformations of the single-stranded molecules migrate at different rates in the gel, creating multiple bands that can be visualized by staining or other detection methods. The presence of additional bands or shifts in band patterns can indicate the presence of a sequence variant or mutation.
SSCP analysis is often used as a screening tool for genetic diseases, cancer, and infectious diseases to identify genetic variations associated with these conditions. However, it has largely been replaced by more sensitive and accurate methods such as next-generation sequencing.
Colorectal neoplasms refer to abnormal growths in the colon or rectum, which can be benign or malignant. These growths can arise from the inner lining (mucosa) of the colon or rectum and can take various forms such as polyps, adenomas, or carcinomas.
Benign neoplasms, such as hyperplastic polyps and inflammatory polyps, are not cancerous but may need to be removed to prevent the development of malignant tumors. Adenomas, on the other hand, are precancerous lesions that can develop into colorectal cancer if left untreated.
Colorectal cancer is a malignant neoplasm that arises from the uncontrolled growth and division of cells in the colon or rectum. It is one of the most common types of cancer worldwide and can spread to other parts of the body through the bloodstream or lymphatic system.
Regular screening for colorectal neoplasms is recommended for individuals over the age of 50, as early detection and removal of precancerous lesions can significantly reduce the risk of developing colorectal cancer.
In medical terms, the skin is the largest organ of the human body. It consists of two main layers: the epidermis (outer layer) and dermis (inner layer), as well as accessory structures like hair follicles, sweat glands, and oil glands. The skin plays a crucial role in protecting us from external factors such as bacteria, viruses, and environmental hazards, while also regulating body temperature and enabling the sense of touch.
Cell movement, also known as cell motility, refers to the ability of cells to move independently and change their location within tissue or inside the body. This process is essential for various biological functions, including embryonic development, wound healing, immune responses, and cancer metastasis.
There are several types of cell movement, including:
1. **Crawling or mesenchymal migration:** Cells move by extending and retracting protrusions called pseudopodia or filopodia, which contain actin filaments. This type of movement is common in fibroblasts, immune cells, and cancer cells during tissue invasion and metastasis.
2. **Amoeboid migration:** Cells move by changing their shape and squeezing through tight spaces without forming protrusions. This type of movement is often observed in white blood cells (leukocytes) as they migrate through the body to fight infections.
3. **Pseudopodial extension:** Cells extend pseudopodia, which are temporary cytoplasmic projections containing actin filaments. These protrusions help the cell explore its environment and move forward.
4. **Bacterial flagellar motion:** Bacteria use a whip-like structure called a flagellum to propel themselves through their environment. The rotation of the flagellum is driven by a molecular motor in the bacterial cell membrane.
5. **Ciliary and ependymal movement:** Ciliated cells, such as those lining the respiratory tract and fallopian tubes, have hair-like structures called cilia that beat in coordinated waves to move fluids or mucus across the cell surface.
Cell movement is regulated by a complex interplay of signaling pathways, cytoskeletal rearrangements, and adhesion molecules, which enable cells to respond to environmental cues and navigate through tissues.
Promoter regions in genetics refer to specific DNA sequences located near the transcription start site of a gene. They serve as binding sites for RNA polymerase and various transcription factors that regulate the initiation of gene transcription. These regulatory elements help control the rate of transcription and, therefore, the level of gene expression. Promoter regions can be composed of different types of sequences, such as the TATA box and CAAT box, and their organization and composition can vary between different genes and species.
Paranasal sinus neoplasms refer to abnormal growths or tumors that develop within the paranasal sinuses, which are air-filled cavities located inside the skull near the nasal cavity. These tumors can be benign (noncancerous) or malignant (cancerous), and they can arise from various types of tissue within the sinuses, such as the lining of the sinuses (mucosa), bone, or other soft tissues.
Paranasal sinus neoplasms can cause a variety of symptoms, including nasal congestion, nosebleeds, facial pain or numbness, and visual disturbances. The diagnosis of these tumors typically involves a combination of imaging studies (such as CT or MRI scans) and biopsy to determine the type and extent of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches, depending on the specific type and stage of the neoplasm.
Alphapapillomavirus is a genus of Papillomaviridae, a family of small, non-enveloped DNA viruses that infect the skin and mucous membranes of humans and other animals. Members of this genus are known to cause various types of benign and malignant tumors in humans, including skin warts, genital warts, and cancers of the cervix, anus, penis, vulva, and oropharynx.
The Alphapapillomavirus genus is further divided into several species, each containing multiple types or strains of the virus. Some of the most well-known and studied types of Alphapapillomavirus include:
* Human papillomavirus (HPV) type 16 and 18, which are associated with a high risk of cervical cancer and other anogenital cancers
* HPV type 6 and 11, which are commonly found in genital warts and recurrent respiratory papillomatosis
* HPV types 31, 33, 45, 52, and 58, which are also associated with an increased risk of cervical cancer and other malignancies.
Preventive measures such as vaccination against high-risk HPV types have been shown to significantly reduce the incidence of cervical cancer and other HPV-related diseases. Regular screening for cervical cancer and other precancerous lesions is also an important part of prevention and early detection.
In situ hybridization, fluorescence (FISH) is a type of molecular cytogenetic technique used to detect and localize the presence or absence of specific DNA sequences on chromosomes through the use of fluorescent probes. This technique allows for the direct visualization of genetic material at a cellular level, making it possible to identify chromosomal abnormalities such as deletions, duplications, translocations, and other rearrangements.
The process involves denaturing the DNA in the sample to separate the double-stranded molecules into single strands, then adding fluorescently labeled probes that are complementary to the target DNA sequence. The probe hybridizes to the complementary sequence in the sample, and the location of the probe is detected by fluorescence microscopy.
FISH has a wide range of applications in both clinical and research settings, including prenatal diagnosis, cancer diagnosis and monitoring, and the study of gene expression and regulation. It is a powerful tool for identifying genetic abnormalities and understanding their role in human disease.
Transfection is a term used in molecular biology that refers to the process of deliberately introducing foreign genetic material (DNA, RNA or artificial gene constructs) into cells. This is typically done using chemical or physical methods, such as lipofection or electroporation. Transfection is widely used in research and medical settings for various purposes, including studying gene function, producing proteins, developing gene therapies, and creating genetically modified organisms. It's important to note that transfection is different from transduction, which is the process of introducing genetic material into cells using viruses as vectors.
Smoking is not a medical condition, but it's a significant health risk behavior. Here is the definition from a public health perspective:
Smoking is the act of inhaling and exhaling the smoke of burning tobacco that is commonly consumed through cigarettes, pipes, and cigars. The smoke contains over 7,000 chemicals, including nicotine, tar, carbon monoxide, and numerous toxic and carcinogenic substances. These toxins contribute to a wide range of diseases and health conditions, such as lung cancer, heart disease, stroke, chronic obstructive pulmonary disease (COPD), and various other cancers, as well as adverse reproductive outcomes and negative impacts on the developing fetus during pregnancy. Smoking is highly addictive due to the nicotine content, which makes quitting smoking a significant challenge for many individuals.
Molecular sequence data refers to the specific arrangement of molecules, most commonly nucleotides in DNA or RNA, or amino acids in proteins, that make up a biological macromolecule. This data is generated through laboratory techniques such as sequencing, and provides information about the exact order of the constituent molecules. This data is crucial in various fields of biology, including genetics, evolution, and molecular biology, allowing for comparisons between different organisms, identification of genetic variations, and studies of gene function and regulation.
Small interfering RNA (siRNA) is a type of short, double-stranded RNA molecule that plays a role in the RNA interference (RNAi) pathway. The RNAi pathway is a natural cellular process that regulates gene expression by targeting and destroying specific messenger RNA (mRNA) molecules, thereby preventing the translation of those mRNAs into proteins.
SiRNAs are typically 20-25 base pairs in length and are generated from longer double-stranded RNA precursors called hairpin RNAs or dsRNAs by an enzyme called Dicer. Once generated, siRNAs associate with a protein complex called the RNA-induced silencing complex (RISC), which uses one strand of the siRNA (the guide strand) to recognize and bind to complementary sequences in the target mRNA. The RISC then cleaves the target mRNA, leading to its degradation and the inhibition of protein synthesis.
SiRNAs have emerged as a powerful tool for studying gene function and have shown promise as therapeutic agents for a variety of diseases, including viral infections, cancer, and genetic disorders. However, their use as therapeutics is still in the early stages of development, and there are challenges associated with delivering siRNAs to specific cells and tissues in the body.
Microsatellite repeats, also known as short tandem repeats (STRs), are repetitive DNA sequences made up of units of 1-6 base pairs that are repeated in a head-to-tail manner. These repeats are spread throughout the human genome and are highly polymorphic, meaning they can have different numbers of repeat units in different individuals.
Microsatellites are useful as genetic markers because of their high degree of variability. They are commonly used in forensic science to identify individuals, in genealogy to trace ancestry, and in medical research to study genetic diseases and disorders. Mutations in microsatellite repeats have been associated with various neurological conditions, including Huntington's disease and fragile X syndrome.
Adenocarcinoma, clear cell is a type of cancer that begins in the glandular cells lining various organs and appears "clear" under the microscope due to its characteristic appearance. These cells produce and release mucus or other fluids. This type of cancer can occur in several parts of the body including the lungs, breasts, ovaries, prostate, and kidneys. Clear cell adenocarcinoma is most commonly found in the ovary and accounts for around 5-10% of all ovarian cancers. It is also associated with endometriosis, a condition where tissue similar to the lining of the uterus grows outside the uterine cavity.
Clear cell adenocarcinoma has unique features that distinguish it from other types of cancer. The cells are often large and have distinct borders, giving them a "clear" appearance under the microscope due to their high lipid or glycogen content. This type of cancer tends to be more aggressive than some other forms of adenocarcinoma and may have a poorer prognosis, particularly if it has spread beyond its original site.
Treatment for clear cell adenocarcinoma typically involves surgery to remove the tumor, followed by chemotherapy or radiation therapy to kill any remaining cancer cells. The specific treatment plan will depend on several factors, including the location and stage of the cancer, as well as the patient's overall health and medical history.
DNA Mutational Analysis is a laboratory test used to identify genetic variations or changes (mutations) in the DNA sequence of a gene. This type of analysis can be used to diagnose genetic disorders, predict the risk of developing certain diseases, determine the most effective treatment for cancer, or assess the likelihood of passing on an inherited condition to offspring.
The test involves extracting DNA from a patient's sample (such as blood, saliva, or tissue), amplifying specific regions of interest using polymerase chain reaction (PCR), and then sequencing those regions to determine the precise order of nucleotide bases in the DNA molecule. The resulting sequence is then compared to reference sequences to identify any variations or mutations that may be present.
DNA Mutational Analysis can detect a wide range of genetic changes, including single-nucleotide polymorphisms (SNPs), insertions, deletions, duplications, and rearrangements. The test is often used in conjunction with other diagnostic tests and clinical evaluations to provide a comprehensive assessment of a patient's genetic profile.
It is important to note that not all mutations are pathogenic or associated with disease, and the interpretation of DNA Mutational Analysis results requires careful consideration of the patient's medical history, family history, and other relevant factors.
DNA-binding proteins are a type of protein that have the ability to bind to DNA (deoxyribonucleic acid), the genetic material of organisms. These proteins play crucial roles in various biological processes, such as regulation of gene expression, DNA replication, repair and recombination.
The binding of DNA-binding proteins to specific DNA sequences is mediated by non-covalent interactions, including electrostatic, hydrogen bonding, and van der Waals forces. The specificity of binding is determined by the recognition of particular nucleotide sequences or structural features of the DNA molecule.
DNA-binding proteins can be classified into several categories based on their structure and function, such as transcription factors, histones, and restriction enzymes. Transcription factors are a major class of DNA-binding proteins that regulate gene expression by binding to specific DNA sequences in the promoter region of genes and recruiting other proteins to modulate transcription. Histones are DNA-binding proteins that package DNA into nucleosomes, the basic unit of chromatin structure. Restriction enzymes are DNA-binding proteins that recognize and cleave specific DNA sequences, and are widely used in molecular biology research and biotechnology applications.
Keratin-19 is a type I acidic keratin that is primarily expressed in simple epithelia, such as the gastrointestinal tract, respiratory tract, and epidermal appendages (e.g., hair follicles, sweat glands). It plays an essential role in maintaining the structure and integrity of these tissues by forming intermediate filaments that provide mechanical support to cells.
Keratin-19 is often used as a marker for simple epithelial differentiation and has been implicated in various pathological conditions, including cancer progression and metastasis. Mutations in the KRT19 gene, which encodes keratin-19, have been associated with certain genetic disorders, such as epidermolysis bullosa simplex, a blistering skin disorder.
In summary, Keratin-19 is an important structural protein expressed in simple epithelia that plays a crucial role in maintaining tissue integrity and has implications in various pathological conditions.
Radiation-induced neoplasms are a type of cancer or tumor that develops as a result of exposure to ionizing radiation. Ionizing radiation is radiation with enough energy to remove tightly bound electrons from atoms or molecules, leading to the formation of ions. This type of radiation can damage DNA and other cellular structures, which can lead to mutations and uncontrolled cell growth, resulting in the development of a neoplasm.
Radiation-induced neoplasms can occur after exposure to high levels of ionizing radiation, such as that received during radiation therapy for cancer treatment or from nuclear accidents. The risk of developing a radiation-induced neoplasm depends on several factors, including the dose and duration of radiation exposure, the type of radiation, and the individual's genetic susceptibility to radiation-induced damage.
Radiation-induced neoplasms can take many years to develop after initial exposure to ionizing radiation, and they often occur at the site of previous radiation therapy. Common types of radiation-induced neoplasms include sarcomas, carcinomas, and thyroid cancer. It is important to note that while ionizing radiation can increase the risk of developing cancer, the overall risk is still relatively low, especially when compared to other well-established cancer risk factors such as smoking and exposure to certain chemicals.
Keratin 5 is a type of keratin protein that is primarily expressed in the basal layer of epithelial tissues, including the skin, hair follicles, and nails. It forms heterodimers with keratin 14 and plays a crucial role in maintaining the structural integrity and stability of these tissues. Mutations in the gene that encodes keratin 5 (KRT5) can lead to several genetic disorders, such as epidermolysis bullosa simplex, which is characterized by blistering of the skin and mucous membranes.
9,10-Dimethyl-1,2-benzanthracene (DMBA) is a synthetic, aromatic hydrocarbon that is commonly used in research as a carcinogenic compound. It is a potent tumor initiator and has been widely used to study chemical carcinogenesis in laboratory animals.
DMBA is a polycyclic aromatic hydrocarbon (PAH) with two benzene rings fused together, and two methyl groups attached at the 9 and 10 positions. This structure allows DMBA to intercalate into DNA, causing mutations that can lead to cancer.
Exposure to DMBA has been shown to cause a variety of tumors in different organs, depending on the route of administration and dose. In animal models, DMBA is often applied to the skin or administered orally to induce tumors in the mammary glands, lungs, or digestive tract.
It's important to note that DMBA is not a natural compound found in the environment and is used primarily for research purposes only. It should be handled with care and appropriate safety precautions due to its carcinogenic properties.
Polymerase Chain Reaction (PCR) is a laboratory technique used to amplify specific regions of DNA. It enables the production of thousands to millions of copies of a particular DNA sequence in a rapid and efficient manner, making it an essential tool in various fields such as molecular biology, medical diagnostics, forensic science, and research.
The PCR process involves repeated cycles of heating and cooling to separate the DNA strands, allow primers (short sequences of single-stranded DNA) to attach to the target regions, and extend these primers using an enzyme called Taq polymerase, resulting in the exponential amplification of the desired DNA segment.
In a medical context, PCR is often used for detecting and quantifying specific pathogens (viruses, bacteria, fungi, or parasites) in clinical samples, identifying genetic mutations or polymorphisms associated with diseases, monitoring disease progression, and evaluating treatment effectiveness.
Transcription factors are proteins that play a crucial role in regulating gene expression by controlling the transcription of DNA to messenger RNA (mRNA). They function by binding to specific DNA sequences, known as response elements, located in the promoter region or enhancer regions of target genes. This binding can either activate or repress the initiation of transcription, depending on the properties and interactions of the particular transcription factor. Transcription factors often act as part of a complex network of regulatory proteins that determine the precise spatiotemporal patterns of gene expression during development, differentiation, and homeostasis in an organism.
Proportional hazards models are a type of statistical analysis used in medical research to investigate the relationship between covariates (predictor variables) and survival times. The most common application of proportional hazards models is in the Cox regression model, which is named after its developer, Sir David Cox.
In a proportional hazards model, the hazard rate or risk of an event occurring at a given time is assumed to be proportional to the hazard rate of a reference group, after adjusting for the covariates. This means that the ratio of the hazard rates between any two individuals remains constant over time, regardless of their survival times.
Mathematically, the hazard function h(t) at time t for an individual with a set of covariates X can be expressed as:
h(t|X) = h0(t) \* exp(β1X1 + β2X2 + ... + βpXp)
where h0(t) is the baseline hazard function, X1, X2, ..., Xp are the covariates, and β1, β2, ..., βp are the regression coefficients that represent the effect of each covariate on the hazard rate.
The assumption of proportionality is crucial in the interpretation of the results from a Cox regression model. If the assumption is violated, then the estimated regression coefficients may be biased and misleading. Therefore, it is important to test for the proportional hazards assumption before interpreting the results of a Cox regression analysis.
Cell survival refers to the ability of a cell to continue living and functioning normally, despite being exposed to potentially harmful conditions or treatments. This can include exposure to toxins, radiation, chemotherapeutic drugs, or other stressors that can damage cells or interfere with their normal processes.
In scientific research, measures of cell survival are often used to evaluate the effectiveness of various therapies or treatments. For example, researchers may expose cells to a particular drug or treatment and then measure the percentage of cells that survive to assess its potential therapeutic value. Similarly, in toxicology studies, measures of cell survival can help to determine the safety of various chemicals or substances.
It's important to note that cell survival is not the same as cell proliferation, which refers to the ability of cells to divide and multiply. While some treatments may promote cell survival, they may also inhibit cell proliferation, making them useful for treating diseases such as cancer. Conversely, other treatments may be designed to specifically target and kill cancer cells, even if it means sacrificing some healthy cells in the process.
In epidemiology, the incidence of a disease is defined as the number of new cases of that disease within a specific population over a certain period of time. It is typically expressed as a rate, with the number of new cases in the numerator and the size of the population at risk in the denominator. Incidence provides information about the risk of developing a disease during a given time period and can be used to compare disease rates between different populations or to monitor trends in disease occurrence over time.
Cell differentiation is the process by which a less specialized cell, or stem cell, becomes a more specialized cell type with specific functions and structures. This process involves changes in gene expression, which are regulated by various intracellular signaling pathways and transcription factors. Differentiation results in the development of distinct cell types that make up tissues and organs in multicellular organisms. It is a crucial aspect of embryonic development, tissue repair, and maintenance of homeostasis in the body.
Cytodiagnosis is the rapid, initial evaluation and diagnosis of a disease based on the examination of individual cells obtained from a body fluid or tissue sample. This technique is often used in cytopathology to investigate abnormalities such as lumps, bumps, or growths that may be caused by cancerous or benign conditions.
The process involves collecting cells through various methods like fine-needle aspiration (FNA), body fluids such as urine, sputum, or washings from the respiratory, gastrointestinal, or genitourinary tracts. The collected sample is then spread onto a microscope slide, stained, and examined under a microscope for abnormalities in cell size, shape, structure, and organization.
Cytodiagnosis can provide crucial information to guide further diagnostic procedures and treatment plans. It is often used as an initial screening tool due to its speed, simplicity, and cost-effectiveness compared to traditional histopathological methods that require tissue biopsy and more extensive processing. However, cytodiagnosis may not always be able to distinguish between benign and malignant conditions definitively; therefore, additional tests or follow-up evaluations might be necessary for a conclusive diagnosis.
Nose neoplasms refer to abnormal growths or tumors in the nasal cavity or paranasal sinuses. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and have the potential to metastasize.
Nose neoplasms can cause various symptoms such as nasal congestion, nosebleeds, difficulty breathing through the nose, loss of smell, facial pain or numbness, and visual changes if they affect the eye. The diagnosis of nose neoplasms usually involves a combination of physical examination, imaging studies (such as CT or MRI scans), and biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Cystadenocarcinoma, serous is a type of cystic tumor that arises from the lining of the abdominal or pelvic cavity (the peritoneum). It is called "serous" because the tumor cells produce a thin, watery fluid similar to serum.
Cystadenocarcinoma is a malignant (cancerous) tumor that can invade surrounding tissues and spread (metastasize) to other parts of the body. It typically affects women over the age of 50 and can cause symptoms such as abdominal pain, bloating, and changes in bowel or bladder habits.
Serous cystadenocarcinoma is a subtype of ovarian cancer that arises from the surface of the ovary. It can also occur in other organs, including the fallopian tubes, peritoneum, and endometrium. This type of tumor tends to grow slowly but can spread widely throughout the abdominal cavity, making it difficult to treat.
Treatment for serous cystadenocarcinoma typically involves surgery to remove the tumor and any affected tissues, followed by chemotherapy to kill any remaining cancer cells. The prognosis for this type of cancer depends on several factors, including the stage of the disease at diagnosis, the patient's age and overall health, and the response to treatment.
Betapapillomavirus is a type of human papillomavirus (HPV) that primarily infects the skin, particularly the flat, dry areas known as the cutaneous epithelium. This genus of HPV is not typically associated with cancers or genital warts, unlike other high-risk HPV types. However, some betapapillomavirus types have been linked to benign skin growths called epidermodysplasia verruciformis (EV) lesions, which can develop into squamous cell carcinomas in immunocompromised individuals.
It is important to note that there are more than 200 known types of HPV, and they are classified into different genera based on their genetic similarities. Betapapillomaviruses belong to the genus Beta-Papillomavirus, which includes at least 49 distinct types. Some common examples of betapapillomaviruses include HPV types 5, 8, 17, 20, 23, and 41.
Research into the epidemiology, risk factors, and clinical implications of various HPV types is ongoing, as understanding the role of these viruses in human health and disease can help inform prevention strategies and treatment approaches.
"Carcinoma, Lewis lung" is a term used to describe a specific type of lung cancer that was first discovered in strain C57BL/6J mice by Dr. Margaret R. Lewis in 1951. It is a spontaneously occurring undifferentiated carcinoma that originates from the lung epithelium and is highly invasive and metastatic, making it a popular model for studying cancer biology and testing potential therapies.
The Lewis lung carcinoma (LLC) cells are typically characterized by their rapid growth rate, ability to form tumors when implanted into syngeneic mice, and high levels of vascular endothelial growth factor (VEGF), which promotes angiogenesis and tumor growth.
It is important to note that while the LLC model has been useful for studying certain aspects of lung cancer, it may not fully recapitulate the complexity and heterogeneity of human lung cancers. Therefore, findings from LLC studies should be validated in more clinically relevant models before being translated into human therapies.
Metaplasia is a term used in pathology to describe the replacement of one differentiated cell type with another differentiated cell type within a tissue or organ. It is an adaptive response of epithelial cells to chronic irritation, inflammation, or injury and can be reversible if the damaging stimulus is removed. Metaplastic changes are often associated with an increased risk of cancer development in the affected area.
For example, in the case of gastroesophageal reflux disease (GERD), chronic exposure to stomach acid can lead to metaplasia of the esophageal squamous epithelium into columnar epithelium, a condition known as Barrett's esophagus. This metaplastic change is associated with an increased risk of developing esophageal adenocarcinoma.
Nuclear proteins are a category of proteins that are primarily found in the nucleus of a eukaryotic cell. They play crucial roles in various nuclear functions, such as DNA replication, transcription, repair, and RNA processing. This group includes structural proteins like lamins, which form the nuclear lamina, and regulatory proteins, such as histones and transcription factors, that are involved in gene expression. Nuclear localization signals (NLS) often help target these proteins to the nucleus by interacting with importin proteins during active transport across the nuclear membrane.
"ErbB-2" is also known as "HER2" or "human epidermal growth factor receptor 2." It is a type of receptor tyrosine kinase (RTK) found on the surface of some cells. ErbB-2 does not bind to any known ligands, but it can form heterodimers with other ErbB family members, such as ErbB-3 and ErbB-4, which do have identified ligands. When a ligand binds to one of these receptors, it causes a conformational change that allows the ErbB-2 receptor to become activated through transphosphorylation. This activation triggers a signaling cascade that regulates cell growth, differentiation, and survival.
Overexpression or amplification of the ERBB2 gene, which encodes the ErbB-2 protein, is observed in approximately 20-30% of breast cancers and is associated with a more aggressive disease phenotype and poorer prognosis. Therefore, ErbB-2 has become an important target for cancer therapy, and several drugs that target this receptor have been developed, including trastuzumab (Herceptin), lapatinib (Tykerb), and pertuzumab (Perjeta).
Radiotherapy, also known as radiation therapy, is a medical treatment that uses ionizing radiation to kill cancer cells, shrink tumors, and prevent the growth and spread of cancer. The radiation can be delivered externally using machines or internally via radioactive substances placed in or near the tumor. Radiotherapy works by damaging the DNA of cancer cells, which prevents them from dividing and growing. Normal cells are also affected by radiation, but they have a greater ability to repair themselves compared to cancer cells. The goal of radiotherapy is to destroy as many cancer cells as possible while minimizing damage to healthy tissue.
Proto-oncogene proteins are normal cellular proteins that play crucial roles in various cellular processes, such as signal transduction, cell cycle regulation, and apoptosis (programmed cell death). They are involved in the regulation of cell growth, differentiation, and survival under physiological conditions.
When proto-oncogene proteins undergo mutations or aberrations in their expression levels, they can transform into oncogenic forms, leading to uncontrolled cell growth and division. These altered proteins are then referred to as oncogene products or oncoproteins. Oncogenic mutations can occur due to various factors, including genetic predisposition, environmental exposures, and aging.
Examples of proto-oncogene proteins include:
1. Ras proteins: Involved in signal transduction pathways that regulate cell growth and differentiation. Activating mutations in Ras genes are found in various human cancers.
2. Myc proteins: Regulate gene expression related to cell cycle progression, apoptosis, and metabolism. Overexpression of Myc proteins is associated with several types of cancer.
3. EGFR (Epidermal Growth Factor Receptor): A transmembrane receptor tyrosine kinase that regulates cell proliferation, survival, and differentiation. Mutations or overexpression of EGFR are linked to various malignancies, such as lung cancer and glioblastoma.
4. Src family kinases: Intracellular tyrosine kinases that regulate signal transduction pathways involved in cell proliferation, survival, and migration. Dysregulation of Src family kinases is implicated in several types of cancer.
5. Abl kinases: Cytoplasmic tyrosine kinases that regulate various cellular processes, including cell growth, differentiation, and stress responses. Aberrant activation of Abl kinases, as seen in chronic myelogenous leukemia (CML), leads to uncontrolled cell proliferation.
Understanding the roles of proto-oncogene proteins and their dysregulation in cancer development is essential for developing targeted cancer therapies that aim to inhibit or modulate these aberrant signaling pathways.
Genetic predisposition to disease refers to an increased susceptibility or vulnerability to develop a particular illness or condition due to inheriting specific genetic variations or mutations from one's parents. These genetic factors can make it more likely for an individual to develop a certain disease, but it does not guarantee that the person will definitely get the disease. Environmental factors, lifestyle choices, and interactions between genes also play crucial roles in determining if a genetically predisposed person will actually develop the disease. It is essential to understand that having a genetic predisposition only implies a higher risk, not an inevitable outcome.
Genotype, in genetics, refers to the complete heritable genetic makeup of an individual organism, including all of its genes. It is the set of instructions contained in an organism's DNA for the development and function of that organism. The genotype is the basis for an individual's inherited traits, and it can be contrasted with an individual's phenotype, which refers to the observable physical or biochemical characteristics of an organism that result from the expression of its genes in combination with environmental influences.
It is important to note that an individual's genotype is not necessarily identical to their genetic sequence. Some genes have multiple forms called alleles, and an individual may inherit different alleles for a given gene from each parent. The combination of alleles that an individual inherits for a particular gene is known as their genotype for that gene.
Understanding an individual's genotype can provide important information about their susceptibility to certain diseases, their response to drugs and other treatments, and their risk of passing on inherited genetic disorders to their offspring.
Keratin-6 is a specific type of keratin protein that is expressed in the epithelial tissues, including the skin and hair follicles. It is a member of the keratin family of intermediate filament proteins, which provide structural support to cells. There are several subtypes of Keratin-6 (A, B, C, and D), each with distinct functions and expression patterns.
Keratin-6A and -6B are expressed in response to injury or stress in the epithelial tissues, where they play a role in wound healing by promoting cell migration and proliferation. They have also been implicated in the development of certain skin disorders, such as psoriasis and epidermolysis bullosa simplex.
Keratin-6C is primarily expressed in the hair follicles, where it helps to regulate the growth and structure of the hair shaft. Mutations in the gene encoding Keratin-6C have been associated with certain forms of hair loss, such as monilethrix and pili torti.
Keratin-6D is also expressed in the hair follicles, where it plays a role in maintaining the integrity of the hair shaft. Mutations in the gene encoding Keratin-6D have been linked to certain forms of wooly hair and hair loss.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
Prospective studies, also known as longitudinal studies, are a type of cohort study in which data is collected forward in time, following a group of individuals who share a common characteristic or exposure over a period of time. The researchers clearly define the study population and exposure of interest at the beginning of the study and follow up with the participants to determine the outcomes that develop over time. This type of study design allows for the investigation of causal relationships between exposures and outcomes, as well as the identification of risk factors and the estimation of disease incidence rates. Prospective studies are particularly useful in epidemiology and medical research when studying diseases with long latency periods or rare outcomes.
DNA primers are short single-stranded DNA molecules that serve as a starting point for DNA synthesis. They are typically used in laboratory techniques such as the polymerase chain reaction (PCR) and DNA sequencing. The primer binds to a complementary sequence on the DNA template through base pairing, providing a free 3'-hydroxyl group for the DNA polymerase enzyme to add nucleotides and synthesize a new strand of DNA. This allows for specific and targeted amplification or analysis of a particular region of interest within a larger DNA molecule.
Adenocarcinoma, papillary is a type of cancer that begins in the glandular cells and grows in a finger-like projection (called a papilla). This type of cancer can occur in various organs, including the lungs, pancreas, thyroid, and female reproductive system. The prognosis and treatment options for papillary adenocarcinoma depend on several factors, such as the location and stage of the tumor, as well as the patient's overall health. It is important to consult with a healthcare professional for an accurate diagnosis and personalized treatment plan.
p16, also known as CDKN2A, is a tumor suppressor gene that encodes the protein p16INK4a. This protein plays a crucial role in regulating the cell cycle by inhibiting the activity of cyclin-dependent kinases (CDKs) 4 and 6, which are essential for the progression from G1 to S phase.
The p16 gene is located on chromosome 9p21 and is often inactivated or deleted in various types of cancer, including lung, breast, and head and neck cancers. Inactivation of the p16 gene leads to uncontrolled cell growth and division, which can contribute to tumor development and progression.
Therefore, the p16 gene is an important tumor suppressor gene that helps prevent cancer by regulating cell growth and division.
'Neoplasms, Unknown Primary' is a medical term used to describe a condition where cancerous growths or tumors are found in the body, but the origin or primary site where the cancer started cannot be identified despite extensive diagnostic tests. This situation can occur when cancer cells spread (metastasize) to other parts of the body and form new tumors before the original (primary) tumor grows large enough to be detected or causes any symptoms. In some cases, the primary tumor may regress or become dormant, making it even more challenging to locate.
Healthcare professionals use various diagnostic techniques, such as imaging tests, biopsies, and laboratory analyses of tumor tissue samples, to identify the origin of metastatic cancer. However, when these methods fail to pinpoint the primary source, the condition is classified as 'Neoplasms, Unknown Primary.' Treatment for this condition typically involves addressing the symptoms and controlling the growth of the metastatic tumors, often involving a combination of surgery, radiation therapy, chemotherapy, or targeted therapies.
Vaginal neoplasms refer to abnormal growths or tumors in the vagina. These growths can be benign (non-cancerous) or malignant (cancerous). The two main types of vaginal neoplasms are:
1. Vaginal intraepithelial neoplasia (VAIN): This is a condition where the cells on the inner lining of the vagina become abnormal but have not invaded deeper tissues. VAIN can be low-grade or high-grade, depending on the severity of the cell changes.
2. Vaginal cancer: This is a malignant tumor that arises from the cells in the vagina. The two main types of vaginal cancer are squamous cell carcinoma and adenocarcinoma. Squamous cell carcinoma is the most common type, accounting for about 85% of all cases.
Risk factors for vaginal neoplasms include human papillomavirus (HPV) infection, smoking, older age, history of cervical cancer or precancerous changes, and exposure to diethylstilbestrol (DES) in utero. Treatment options depend on the type, stage, and location of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
The cardia is a term used in anatomical context to refer to the upper part of the stomach that surrounds and opens into the lower end of the esophagus. It is responsible for controlling the passage of food from the esophagus into the stomach and is also known as the cardiac orifice or cardiac sphincter. Any medical condition that affects this area, such as gastroesophageal reflux disease (GERD), can lead to symptoms like heartburn, difficulty swallowing, and chest pain.
Maxillary neoplasms refer to abnormal growths or tumors in the maxilla, which is the upper jaw bone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and spread to distant sites.
Maxillary neoplasms can cause various symptoms such as swelling, pain, numbness, loose teeth, or difficulty in chewing or swallowing. They may also cause nasal congestion, nosebleeds, or visual changes if they affect the eye or orbit. The diagnosis of maxillary neoplasms usually involves a combination of clinical examination, imaging studies such as CT or MRI scans, and biopsy to determine the type and extent of the tumor.
Treatment options for maxillary neoplasms depend on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and preferences. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis and ensure optimal outcomes.
BALB/c is an inbred strain of laboratory mouse that is widely used in biomedical research. The strain was developed at the Institute of Cancer Research in London by Henry Baldwin and his colleagues in the 1920s, and it has since become one of the most commonly used inbred strains in the world.
BALB/c mice are characterized by their black coat color, which is determined by a recessive allele at the tyrosinase locus. They are also known for their docile and friendly temperament, making them easy to handle and work with in the laboratory.
One of the key features of BALB/c mice that makes them useful for research is their susceptibility to certain types of tumors and immune responses. For example, they are highly susceptible to developing mammary tumors, which can be induced by chemical carcinogens or viral infection. They also have a strong Th2-biased immune response, which makes them useful models for studying allergic diseases and asthma.
BALB/c mice are also commonly used in studies of genetics, neuroscience, behavior, and infectious diseases. Because they are an inbred strain, they have a uniform genetic background, which makes it easier to control for genetic factors in experiments. Additionally, because they have been bred in the laboratory for many generations, they are highly standardized and reproducible, making them ideal subjects for scientific research.
Drug resistance in neoplasms (also known as cancer drug resistance) refers to the ability of cancer cells to withstand the effects of chemotherapeutic agents or medications designed to kill or inhibit the growth of cancer cells. This can occur due to various mechanisms, including changes in the cancer cell's genetic makeup, alterations in drug targets, increased activity of drug efflux pumps, and activation of survival pathways.
Drug resistance can be intrinsic (present at the beginning of treatment) or acquired (developed during the course of treatment). It is a significant challenge in cancer therapy as it often leads to reduced treatment effectiveness, disease progression, and poor patient outcomes. Strategies to overcome drug resistance include the use of combination therapies, development of new drugs that target different mechanisms, and personalized medicine approaches that consider individual patient and tumor characteristics.
Human chromosome pair 9 consists of two rod-shaped structures present in the nucleus of each cell of the human body. Each member of the pair contains thousands of genes and other genetic material, encoded in the form of DNA molecules. The two chromosomes in a pair are identical or very similar to each other in terms of their size, shape, and genetic makeup.
Chromosome 9 is one of the autosomal chromosomes, meaning that it is not a sex chromosome (X or Y) and is present in two copies in all cells of the body, regardless of sex. Chromosome 9 is a medium-sized chromosome, and it is estimated to contain around 135 million base pairs of DNA and approximately 1200 genes.
Chromosome 9 contains several important genes that are associated with various human traits and diseases. For example, mutations in the gene that encodes the protein APOE on chromosome 9 have been linked to an increased risk of developing Alzheimer's disease. Additionally, variations in the gene that encodes the protein EGFR on chromosome 9 have been associated with an increased risk of developing certain types of cancer.
Overall, human chromosome pair 9 plays a critical role in the development and function of the human body, and variations in its genetic makeup can contribute to a wide range of traits and diseases.
Antineoplastic agents, phytogenic, also known as plant-derived anticancer drugs, are medications that are derived from plants and used to treat cancer. These agents have natural origins and work by interfering with the growth and multiplication of cancer cells, helping to slow or stop the spread of the disease. Some examples of antineoplastic agents, phytogenic include paclitaxel (Taxol), vincristine, vinblastine, and etoposide. These drugs are often used in combination with other treatments such as surgery, radiation therapy, and other medications to provide a comprehensive approach to cancer care.
A cell line is a culture of cells that are grown in a laboratory for use in research. These cells are usually taken from a single cell or group of cells, and they are able to divide and grow continuously in the lab. Cell lines can come from many different sources, including animals, plants, and humans. They are often used in scientific research to study cellular processes, disease mechanisms, and to test new drugs or treatments. Some common types of human cell lines include HeLa cells (which come from a cancer patient named Henrietta Lacks), HEK293 cells (which come from embryonic kidney cells), and HUVEC cells (which come from umbilical vein endothelial cells). It is important to note that cell lines are not the same as primary cells, which are cells that are taken directly from a living organism and have not been grown in the lab.
Flow cytometry is a medical and research technique used to measure physical and chemical characteristics of cells or particles, one cell at a time, as they flow in a fluid stream through a beam of light. The properties measured include:
* Cell size (light scatter)
* Cell internal complexity (granularity, also light scatter)
* Presence or absence of specific proteins or other molecules on the cell surface or inside the cell (using fluorescent antibodies or other fluorescent probes)
The technique is widely used in cell counting, cell sorting, protein engineering, biomarker discovery and monitoring disease progression, particularly in hematology, immunology, and cancer research.
Uterine cervical dysplasia is a condition characterized by abnormal cell growth on the lining of the cervix, which is the lower part of the uterus that connects to the vagina. It is also known as cervical intraepithelial neoplasia (CIN).
Cervical dysplasia can be caused by certain strains of human papillomavirus (HPV), a common sexually transmitted infection. The abnormal cells may develop into cancerous cells over time, although not all cases of cervical dysplasia will progress to cancer.
Cervical dysplasia is typically detected through a Pap test or HPV test, which are screening tests used to detect precancerous changes in the cervix. Depending on the severity and extent of the abnormal cells, treatment options may include close monitoring, surgical removal of the affected tissue, or more extensive surgery.
It is important for women to receive regular Pap tests and HPV tests as recommended by their healthcare provider to detect and treat cervical dysplasia early, before it has a chance to progress to cancer.
Bronchioloalveolar carcinoma (BAC) is a subtype of adenocarcinoma, which is a type of lung cancer that originates in the cells that line the alveoli (tiny air sacs) in the lungs. BAC is characterized by the spread of cancerous cells along the alveolar walls, without invading the surrounding tissues. It often appears as multiple nodules or a large mass in the lung and can be difficult to diagnose due to its growth pattern.
BAC is typically associated with a better prognosis compared to other types of lung cancer, but it can still be aggressive and spread to other parts of the body. Treatment options for BAC may include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these approaches. It's important to note that medical definitions and classifications of diseases and conditions are constantly evolving as new research emerges, so it's always a good idea to consult with a healthcare professional for the most up-to-date information.
A dose-response relationship in the context of drugs refers to the changes in the effects or symptoms that occur as the dose of a drug is increased or decreased. Generally, as the dose of a drug is increased, the severity or intensity of its effects also increases. Conversely, as the dose is decreased, the effects of the drug become less severe or may disappear altogether.
The dose-response relationship is an important concept in pharmacology and toxicology because it helps to establish the safe and effective dosage range for a drug. By understanding how changes in the dose of a drug affect its therapeutic and adverse effects, healthcare providers can optimize treatment plans for their patients while minimizing the risk of harm.
The dose-response relationship is typically depicted as a curve that shows the relationship between the dose of a drug and its effect. The shape of the curve may vary depending on the drug and the specific effect being measured. Some drugs may have a steep dose-response curve, meaning that small changes in the dose can result in large differences in the effect. Other drugs may have a more gradual dose-response curve, where larger changes in the dose are needed to produce significant effects.
In addition to helping establish safe and effective dosages, the dose-response relationship is also used to evaluate the potential therapeutic benefits and risks of new drugs during clinical trials. By systematically testing different doses of a drug in controlled studies, researchers can identify the optimal dosage range for the drug and assess its safety and efficacy.
Facial neoplasms refer to abnormal growths or tumors that develop in the tissues of the face. These growths can be benign (non-cancerous) or malignant (cancerous). Facial neoplasms can occur in any of the facial structures, including the skin, muscles, bones, nerves, and glands.
Benign facial neoplasms are typically slow-growing and do not spread to other parts of the body. Examples include papillomas, hemangiomas, and neurofibromas. While these tumors are usually harmless, they can cause cosmetic concerns or interfere with normal facial function.
Malignant facial neoplasms, on the other hand, can be aggressive and invasive. They can spread to other parts of the face, as well as to distant sites in the body. Common types of malignant facial neoplasms include basal cell carcinoma, squamous cell carcinoma, and melanoma.
Treatment for facial neoplasms depends on several factors, including the type, size, location, and stage of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. It is important to seek medical attention promptly if you notice any unusual growths or changes in the skin or tissues of your face.
In medical terms, the "neck" is defined as the portion of the body that extends from the skull/head to the thorax or chest region. It contains 7 cervical vertebrae, muscles, nerves, blood vessels, lymphatic vessels, and glands (such as the thyroid gland). The neck is responsible for supporting the head, allowing its movement in various directions, and housing vital structures that enable functions like respiration and circulation.
Drug screening assays for antitumor agents are laboratory tests used to identify and evaluate the effectiveness of potential drugs or compounds that can inhibit the growth of tumor cells or induce their death. These assays are typically performed in vitro (in a test tube or petri dish) using cell cultures of various types of cancer cells.
The assays measure different parameters such as cell viability, proliferation, apoptosis (programmed cell death), and cytotoxicity to determine the ability of the drug to kill or inhibit the growth of tumor cells. The results of these assays can help researchers identify promising antitumor agents that can be further developed for clinical use in cancer treatment.
There are different types of drug screening assays for antitumor agents, including high-throughput screening (HTS) assays, which allow for the rapid and automated testing of a large number of compounds against various cancer cell lines. Other types of assays include phenotypic screening assays, target-based screening assays, and functional screening assays, each with its own advantages and limitations.
Overall, drug screening assays for antitumor agents play a critical role in the development of new cancer therapies by providing valuable information on the activity and safety of potential drugs, helping to identify effective treatments and reduce the time and cost associated with bringing new drugs to market.
MicroRNAs (miRNAs) are a class of small non-coding RNAs, typically consisting of around 20-24 nucleotides, that play crucial roles in post-transcriptional regulation of gene expression. They primarily bind to the 3' untranslated region (3' UTR) of target messenger RNAs (mRNAs), leading to mRNA degradation or translational repression. MicroRNAs are involved in various biological processes, including development, differentiation, proliferation, and apoptosis, and have been implicated in numerous diseases, such as cancers and neurological disorders. They can be found in various organisms, from plants to animals, and are often conserved across species. MicroRNAs are usually transcribed from DNA sequences located in introns or exons of protein-coding genes or in intergenic regions. After transcription, they undergo a series of processing steps, including cleavage by ribonucleases Drosha and Dicer, to generate mature miRNA molecules capable of binding to their target mRNAs.
A Human Papillomavirus (HPV) DNA test is a molecular diagnostic assay used to detect the presence or absence of DNA from high-risk types of HPV in cervical or anal samples. High-risk HPV types are those most strongly associated with an increased risk for developing cervical cancer and other anogenital cancers.
HPV DNA tests typically use polymerase chain reaction (PCR) or other nucleic acid amplification techniques to detect and quantify the viral DNA in clinical samples. These tests can help identify women at higher risk for cervical precancer or cancer, particularly when combined with cytology results from a Pap test.
HPV DNA testing is recommended as a primary screening method for cervical cancer in certain populations or as a follow-up test to abnormal Pap test results. It's important to note that HPV DNA tests do not diagnose cervical precancer or cancer but rather identify the presence of high-risk HPV types, which may increase the risk of developing these conditions over time.
The cell cycle is a series of events that take place in a cell leading to its division and duplication. It consists of four main phases: G1 phase, S phase, G2 phase, and M phase.
During the G1 phase, the cell grows in size and synthesizes mRNA and proteins in preparation for DNA replication. In the S phase, the cell's DNA is copied, resulting in two complete sets of chromosomes. During the G2 phase, the cell continues to grow and produces more proteins and organelles necessary for cell division.
The M phase is the final stage of the cell cycle and consists of mitosis (nuclear division) and cytokinesis (cytoplasmic division). Mitosis results in two genetically identical daughter nuclei, while cytokinesis divides the cytoplasm and creates two separate daughter cells.
The cell cycle is regulated by various checkpoints that ensure the proper completion of each phase before progressing to the next. These checkpoints help prevent errors in DNA replication and division, which can lead to mutations and cancer.
The term "mouth floor" is not a standard medical terminology. However, it might refer to the floor of the mouth, which is the part of the oral cavity located beneath the tongue and above the hyoid bone, which is a U-shaped bone in the front of the neck that helps support the tongue. The mouth floor contains several salivary glands, muscles, and nerves that are important for functions such as swallowing and speaking.
Carcinoma of the skin appendages refers to a type of cancer that originates in the specialized cells of the skin's sweat glands, hair follicles, or sebaceous glands. These cancers are relatively rare and can present as various subtypes, including eccrine carcinoma, apocrine carcinoma, hidradenocarcinoma, and malignant adnexal tumors.
The symptoms of skin appendage carcinomas may include:
1. A firm, painless lump or nodule under the skin that may be skin-colored, red, or blue.
2. Ulceration, crusting, or bleeding from the lesion.
3. Itching, burning, or pain in the affected area.
4. Lymph node enlargement near the tumor site.
Treatment typically involves surgical excision of the tumor, often followed by radiation therapy and/or chemotherapy to ensure complete removal and reduce the risk of recurrence. Regular follow-up appointments with a dermatologist or oncologist are essential for monitoring and early detection of any potential recurrences or new primary cancers.
Human papillomavirus 18 (HPV-18) is a specific type of human papillomavirus (HPV), which is a group of more than 200 related viruses. HPV is named for the warts (papillomas) some types can cause.
HPV-18 is one of the high-risk types of HPV that are linked to several types of cancer, including cervical, anal, vaginal, vulvar, and oropharyngeal (throat) cancers. HPV-18 along with HPV-16 are responsible for about 70% of all cervical cancers.
HPV is passed from one person to another during skin-to-skin contact, usually during sexual activity. Most sexually active people will have an HPV infection at some point in their lives, but most will never know it because the virus often causes no symptoms and goes away on its own. However, when HPV doesn't go away, it can cause serious health problems, including cancer.
There are vaccines available to protect against HPV-18 and other high-risk types of HPV. The Centers for Disease Control and Prevention (CDC) recommends that all boys and girls get the HPV vaccine at age 11 or 12, but it can be given as early as age 9 and until age 26 for those who have not yet received it. The vaccine is most effective when given before becoming sexually active.
A cohort study is a type of observational study in which a group of individuals who share a common characteristic or exposure are followed up over time to determine the incidence of a specific outcome or outcomes. The cohort, or group, is defined based on the exposure status (e.g., exposed vs. unexposed) and then monitored prospectively to assess for the development of new health events or conditions.
Cohort studies can be either prospective or retrospective in design. In a prospective cohort study, participants are enrolled and followed forward in time from the beginning of the study. In contrast, in a retrospective cohort study, researchers identify a cohort that has already been assembled through medical records, insurance claims, or other sources and then look back in time to assess exposure status and health outcomes.
Cohort studies are useful for establishing causality between an exposure and an outcome because they allow researchers to observe the temporal relationship between the two. They can also provide information on the incidence of a disease or condition in different populations, which can be used to inform public health policy and interventions. However, cohort studies can be expensive and time-consuming to conduct, and they may be subject to bias if participants are not representative of the population or if there is loss to follow-up.
Paclitaxel is a chemotherapeutic agent derived from the bark of the Pacific yew tree (Taxus brevifolia). It is an antimicrotubule agent that promotes the assembly and stabilization of microtubules, thereby interfering with the normal dynamic reorganization of the microtubule network that is essential for cell division.
Paclitaxel is used in the treatment of various types of cancer including ovarian, breast, lung, and pancreatic cancers. It works by inhibiting the disassembly of microtubules, which prevents the separation of chromosomes during mitosis, leading to cell cycle arrest and apoptosis (programmed cell death).
Common side effects of paclitaxel include neutropenia (low white blood cell count), anemia (low red blood cell count), alopecia (hair loss), peripheral neuropathy (nerve damage causing numbness or tingling in the hands and feet), myalgias (muscle pain), arthralgias (joint pain), and hypersensitivity reactions.
Gene silencing is a process by which the expression of a gene is blocked or inhibited, preventing the production of its corresponding protein. This can occur naturally through various mechanisms such as RNA interference (RNAi), where small RNAs bind to and degrade specific mRNAs, or DNA methylation, where methyl groups are added to the DNA molecule, preventing transcription. Gene silencing can also be induced artificially using techniques such as RNAi-based therapies, antisense oligonucleotides, or CRISPR-Cas9 systems, which allow for targeted suppression of gene expression in research and therapeutic applications.
Chromosome aberrations refer to structural and numerical changes in the chromosomes that can occur spontaneously or as a result of exposure to mutagenic agents. These changes can affect the genetic material encoded in the chromosomes, leading to various consequences such as developmental abnormalities, cancer, or infertility.
Structural aberrations include deletions, duplications, inversions, translocations, and rings, which result from breaks and rearrangements of chromosome segments. Numerical aberrations involve changes in the number of chromosomes, such as aneuploidy (extra or missing chromosomes) or polyploidy (multiples of a complete set of chromosomes).
Chromosome aberrations can be detected and analyzed using various cytogenetic techniques, including karyotyping, fluorescence in situ hybridization (FISH), and comparative genomic hybridization (CGH). These methods allow for the identification and characterization of chromosomal changes at the molecular level, providing valuable information for genetic counseling, diagnosis, and research.
Adjuvant chemotherapy is a medical treatment that is given in addition to the primary therapy, such as surgery or radiation, to increase the chances of a cure or to reduce the risk of recurrence in patients with cancer. It involves the use of chemicals (chemotherapeutic agents) to destroy any remaining cancer cells that may not have been removed by the primary treatment. This type of chemotherapy is typically given after the main treatment has been completed, and its goal is to kill any residual cancer cells that may be present in the body and reduce the risk of the cancer coming back. The specific drugs used and the duration of treatment will depend on the type and stage of cancer being treated.
Dose fractionation is a medical term that refers to the practice of dividing the total dose of radiation therapy or chemotherapy into smaller doses, which are given over a longer period. This approach allows for the delivery of a higher total dose of treatment while minimizing damage to healthy tissues and reducing side effects.
In radiation therapy, fractionation is used to target cancer cells while sparing surrounding normal tissues. By delivering smaller doses of radiation over several treatments, healthy tissue has time to recover between treatments, reducing the risk of complications. The number and size of fractions can vary depending on the type and location of the tumor, as well as other factors such as the patient's overall health.
Similarly, in chemotherapy, dose fractionation is used to maximize the effectiveness of the treatment while minimizing toxicity. By administering smaller doses of chemotherapy over time, the body has a chance to recover between treatments, reducing side effects and allowing for higher total doses to be given. The schedule and duration of chemotherapy fractionation may vary depending on the type of drug used, the type and stage of cancer, and other factors.
Overall, dose fractionation is an important technique in both radiation therapy and chemotherapy that allows for more effective treatment while minimizing harm to healthy tissues.
Real-Time Polymerase Chain Reaction (RT-PCR) is a laboratory technique used in molecular biology to amplify and detect specific DNA sequences in real-time. It is a sensitive and specific method that allows for the quantification of target nucleic acids, such as DNA or RNA, through the use of fluorescent reporter molecules.
The RT-PCR process involves several steps: first, the template DNA is denatured to separate the double-stranded DNA into single strands. Then, primers (short sequences of DNA) specific to the target sequence are added and allowed to anneal to the template DNA. Next, a heat-stable enzyme called Taq polymerase adds nucleotides to the annealed primers, extending them along the template DNA until a new double-stranded DNA molecule is formed.
During each amplification cycle, fluorescent reporter molecules are added that bind specifically to the newly synthesized DNA. As more and more copies of the target sequence are generated, the amount of fluorescence increases in proportion to the number of copies present. This allows for real-time monitoring of the PCR reaction and quantification of the target nucleic acid.
RT-PCR is commonly used in medical diagnostics, research, and forensics to detect and quantify specific DNA or RNA sequences. It has been widely used in the diagnosis of infectious diseases, genetic disorders, and cancer, as well as in the identification of microbial pathogens and the detection of gene expression.
Epithelial cells are types of cells that cover the outer surfaces of the body, line the inner surfaces of organs and glands, and form the lining of blood vessels and body cavities. They provide a protective barrier against the external environment, regulate the movement of materials between the internal and external environments, and are involved in the sense of touch, temperature, and pain. Epithelial cells can be squamous (flat and thin), cuboidal (square-shaped and of equal height), or columnar (tall and narrow) in shape and are classified based on their location and function.
Cheilitis is a medical term that refers to inflammation of the lips. It can cause dryness, cracking, and soreness of the lips, as well as redness and swelling. There are several types of cheilitis, including:
1. Actinic cheilitis: This type of cheilitis is caused by excessive exposure to the sun's ultraviolet (UV) rays and affects the lower lip. It can increase the risk of developing squamous cell carcinoma, a type of skin cancer.
2. Angular cheilitis: Also known as perleche, angular cheilitis affects the corners of the mouth and is often caused by a fungal or bacterial infection.
3. Atopic cheilitis: This type of cheilitis is associated with atopic dermatitis (eczema) and causes dry, itchy, and scaly patches on the lips.
4. Contact cheilitis: This type of cheilitis is caused by an allergic reaction to substances that come into contact with the lips, such as lip balm, lipstick, or toothpaste.
5. Exfoliative cheilitis: This is a rare and severe form of cheilitis that causes dryness, scaling, and crusting of the lips, leading to painful sores and ulcers.
6. Granulomatous cheilitis: This type of cheilitis is characterized by the formation of granulomas (small nodules) on the lips and is often associated with other systemic diseases such as Crohn's disease or sarcoidosis.
Treatment for cheilitis depends on the underlying cause, and may include topical creams or ointments, oral medications, lifestyle changes, or avoiding triggers that worsen symptoms.
Cyclooxygenase-2 (COX-2) is an enzyme involved in the synthesis of prostaglandins, which are hormone-like substances that play a role in inflammation, pain, and fever. COX-2 is primarily expressed in response to stimuli such as cytokines and growth factors, and its expression is associated with the development of inflammation.
COX-2 inhibitors are a class of nonsteroidal anti-inflammatory drugs (NSAIDs) that selectively block the activity of COX-2, reducing the production of prostaglandins and providing analgesic, anti-inflammatory, and antipyretic effects. These medications are often used to treat pain and inflammation associated with conditions such as arthritis, menstrual cramps, and headaches.
It's important to note that while COX-2 inhibitors can be effective in managing pain and inflammation, they may also increase the risk of cardiovascular events such as heart attack and stroke, particularly when used at high doses or for extended periods. Therefore, it's essential to use these medications under the guidance of a healthcare provider and to follow their instructions carefully.
Genetic polymorphism refers to the occurrence of multiple forms (called alleles) of a particular gene within a population. These variations in the DNA sequence do not generally affect the function or survival of the organism, but they can contribute to differences in traits among individuals. Genetic polymorphisms can be caused by single nucleotide changes (SNPs), insertions or deletions of DNA segments, or other types of genetic rearrangements. They are important for understanding genetic diversity and evolution, as well as for identifying genetic factors that may contribute to disease susceptibility in humans.
I am not aware of a specific medical definition for the term "China." Generally, it is used to refer to:
1. The People's Republic of China (PRC), which is a country in East Asia. It is the most populous country in the world and the fourth largest by geographical area. Its capital city is Beijing.
2. In a historical context, "China" was used to refer to various dynasties and empires that existed in East Asia over thousands of years. The term "Middle Kingdom" or "Zhongguo" (中国) has been used by the Chinese people to refer to their country for centuries.
3. In a more general sense, "China" can also be used to describe products or goods that originate from or are associated with the People's Republic of China.
If you have a specific context in which you encountered the term "China" related to medicine, please provide it so I can give a more accurate response.
Keratin-7 is not a medical term itself, but it is a specific type of keratin protein that is often used in pathology as a marker for certain types of carcinomas. Keratins are a family of fibrous proteins that make up the structural framework of epithelial cells, which line the surfaces and glands of the body.
Keratin-7 is typically expressed in simple epithelia, such as those found in the gastrointestinal tract, pancreas, bile ducts, and respiratory and genitourinary tracts. It can be used as a marker to help identify carcinomas that arise from these tissues, such as adenocarcinomas of the pancreas or biliary system.
In medical terminology, keratin-7 positivity is often reported in the pathology report of a biopsy or surgical specimen to indicate the presence of this protein in cancer cells. This information can be helpful in determining the origin and behavior of the tumor, as well as guiding treatment decisions.
Proliferating Cell Nuclear Antigen (PCNA) is a protein that plays an essential role in the process of DNA replication and repair in eukaryotic cells. It functions as a cofactor for DNA polymerase delta, enhancing its activity during DNA synthesis. PCNA forms a sliding clamp around DNA, allowing it to move along the template and coordinate the actions of various enzymes involved in DNA metabolism.
PCNA is often used as a marker for cell proliferation because its levels increase in cells that are actively dividing or have been stimulated to enter the cell cycle. Immunostaining techniques can be used to detect PCNA and determine the proliferative status of tissues or cultures. In this context, 'proliferating' refers to the rapid multiplication of cells through cell division.
Mandibular neoplasms refer to abnormal growths or tumors that develop in the mandible, which is the lower jawbone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and rarely spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and may metastasize (spread) to distant sites.
Mandibular neoplasms can have various causes, including genetic mutations, exposure to certain chemicals or radiation, and infection with certain viruses. The symptoms of mandibular neoplasms may include swelling or pain in the jaw, difficulty chewing or speaking, numbness in the lower lip or chin, loose teeth, and/or a lump or mass in the mouth or neck.
The diagnosis of mandibular neoplasms typically involves a thorough clinical examination, imaging studies such as X-rays, CT scans, or MRI scans, and sometimes a biopsy to confirm the type and extent of the tumor. Treatment options depend on the type, stage, and location of the neoplasm, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or metastasis.
A phenotype is the physical or biochemical expression of an organism's genes, or the observable traits and characteristics resulting from the interaction of its genetic constitution (genotype) with environmental factors. These characteristics can include appearance, development, behavior, and resistance to disease, among others. Phenotypes can vary widely, even among individuals with identical genotypes, due to differences in environmental influences, gene expression, and genetic interactions.
Radiation tolerance, in the context of medicine and particularly radiation oncology, refers to the ability of tissues or organs to withstand and recover from exposure to ionizing radiation without experiencing significant damage or loss of function. It is often used to describe the maximum dose of radiation that can be safely delivered to a specific area of the body during radiotherapy treatments.
Radiation tolerance varies depending on the type and location of the tissue or organ. For example, some tissues such as the brain, spinal cord, and lungs have lower radiation tolerance than others like the skin or bone. Factors that can affect radiation tolerance include the total dose of radiation, the fractionation schedule (the number and size of radiation doses), the volume of tissue treated, and the individual patient's overall health and genetic factors.
Assessing radiation tolerance is critical in designing safe and effective radiotherapy plans for cancer patients, as excessive radiation exposure can lead to serious side effects such as radiation-induced injury, fibrosis, or even secondary malignancies.
Lymph node excision is a surgical procedure in which one or more lymph nodes are removed from the body for the purpose of examination. This procedure is often conducted to help diagnose or stage various types of cancer, as malignant cells may spread to the lymphatic system and eventually accumulate within nearby lymph nodes.
During a lymph node excision, an incision is made in the skin overlying the affected lymph node(s). The surgeon carefully dissects the tissue surrounding the lymph node(s) to isolate them from adjacent structures before removing them. In some cases, a sentinel lymph node biopsy may be performed instead, where only the sentinel lymph node (the first lymph node to which cancer cells are likely to spread) is removed and examined.
The excised lymph nodes are then sent to a laboratory for histopathological examination, which involves staining and microscopic evaluation of the tissue to determine whether it contains any malignant cells. The results of this examination can help guide further treatment decisions and provide valuable prognostic information.
Chemoembolization, therapeutic is a medical procedure that involves the delivery of chemotherapy drugs directly to a tumor through its blood supply, followed by the blocking of the blood vessel leading to the tumor. This approach allows for a higher concentration of the chemotherapy drug to be delivered directly to the tumor while minimizing exposure to the rest of the body. The embolization component of the procedure involves blocking the blood vessel with various substances such as microspheres, gel foam, or coils, which can help to starve the tumor of oxygen and nutrients.
Therapeutic chemoembolization is typically used in the treatment of liver cancer, including primary liver cancer (hepatocellular carcinoma) and metastatic liver cancer. It may also be used in other types of cancer that have spread to the liver. The procedure can help to reduce the size of the tumor, relieve symptoms, and improve survival rates in some patients. However, like all medical procedures, it carries a risk of complications such as infection, bleeding, and damage to surrounding tissues.
Vascular Endothelial Growth Factor A (VEGFA) is a specific isoform of the vascular endothelial growth factor (VEGF) family. It is a well-characterized signaling protein that plays a crucial role in angiogenesis, the process of new blood vessel formation from pre-existing vessels. VEGFA stimulates the proliferation and migration of endothelial cells, which line the interior surface of blood vessels, thereby contributing to the growth and development of new vasculature. This protein is essential for physiological processes such as embryonic development and wound healing, but it has also been implicated in various pathological conditions, including cancer, age-related macular degeneration, and diabetic retinopathy. The regulation of VEGFA expression and activity is critical to maintaining proper vascular function and homeostasis.
The cervix uteri, often simply referred to as the cervix, is the lower part of the uterus (womb) that connects to the vagina. It has an opening called the external os through which menstrual blood exits the uterus and sperm enters during sexual intercourse. During childbirth, the cervix dilates or opens to allow for the passage of the baby through the birth canal.
Positron-Emission Tomography (PET) is a type of nuclear medicine imaging that uses small amounts of radioactive material, called a radiotracer, to produce detailed, three-dimensional images. This technique measures metabolic activity within the body, such as sugar metabolism, to help distinguish between healthy and diseased tissue, identify cancerous cells, or examine the function of organs.
During a PET scan, the patient is injected with a radiotracer, typically a sugar-based compound labeled with a positron-emitting radioisotope, such as fluorine-18 (^18^F). The radiotracer accumulates in cells that are metabolically active, like cancer cells. As the radiotracer decays, it emits positrons, which then collide with electrons in nearby tissue, producing gamma rays. A special camera, called a PET scanner, detects these gamma rays and uses this information to create detailed images of the body's internal structures and processes.
PET is often used in conjunction with computed tomography (CT) or magnetic resonance imaging (MRI) to provide both functional and anatomical information, allowing for more accurate diagnosis and treatment planning. Common applications include detecting cancer recurrence, staging and monitoring cancer, evaluating heart function, and assessing brain function in conditions like dementia and epilepsy.
Membrane proteins are a type of protein that are embedded in the lipid bilayer of biological membranes, such as the plasma membrane of cells or the inner membrane of mitochondria. These proteins play crucial roles in various cellular processes, including:
1. Cell-cell recognition and signaling
2. Transport of molecules across the membrane (selective permeability)
3. Enzymatic reactions at the membrane surface
4. Energy transduction and conversion
5. Mechanosensation and signal transduction
Membrane proteins can be classified into two main categories: integral membrane proteins, which are permanently associated with the lipid bilayer, and peripheral membrane proteins, which are temporarily or loosely attached to the membrane surface. Integral membrane proteins can further be divided into three subcategories based on their topology:
1. Transmembrane proteins, which span the entire width of the lipid bilayer with one or more alpha-helices or beta-barrels.
2. Lipid-anchored proteins, which are covalently attached to lipids in the membrane via a glycosylphosphatidylinositol (GPI) anchor or other lipid modifications.
3. Monotopic proteins, which are partially embedded in the membrane and have one or more domains exposed to either side of the bilayer.
Membrane proteins are essential for maintaining cellular homeostasis and are targets for various therapeutic interventions, including drug development and gene therapy. However, their structural complexity and hydrophobicity make them challenging to study using traditional biochemical methods, requiring specialized techniques such as X-ray crystallography, nuclear magnetic resonance (NMR) spectroscopy, and single-particle cryo-electron microscopy (cryo-EM).
I'm sorry for any confusion, but "sunlight" is not a term with a specific medical definition. However, sunlight does have various implications in the field of medicine. It is the light that comes from the sun, which is a star at the center of our solar system. Sunlight is essential for the production of vitamin D in humans, and it can also have effects on mood and sleep patterns due to its influence on circadian rhythms.
In a medical context, sunlight is often discussed in relation to its potential health benefits and risks. For instance, moderate sun exposure can help increase vitamin D levels, which are important for bone health, immune function, and other bodily processes. However, excessive sun exposure can lead to harmful effects, such as sunburn, premature skin aging, and an increased risk of skin cancer.
It's essential to balance the benefits and risks of sunlight exposure by practicing safe sun habits, such as wearing protective clothing, using a broad-spectrum sunscreen with an SPF of at least 30, seeking shade during peak sunlight hours, and avoiding intentional tanning.
Esophagoscopy is a medical procedure that involves the visual examination of the esophagus, which is the tube that connects the throat to the stomach. This procedure is typically carried out using an esophagogastroduodenoscope (EGD), a flexible tube with a camera and light on the end.
During the procedure, the EGD is inserted through the mouth and down the throat into the esophagus, allowing the medical professional to examine its lining for any abnormalities such as inflammation, ulcers, or tumors. The procedure may also involve taking tissue samples (biopsies) for further examination and testing.
Esophagoscopy is commonly used to diagnose and monitor conditions such as gastroesophageal reflux disease (GERD), Barrett's esophagus, esophageal cancer, and other disorders affecting the esophagus. It may also be used to treat certain conditions, such as removing polyps or foreign objects from the esophagus.
'Mammary neoplasms, experimental' is not a recognized medical term. However, I can provide definitions for the individual terms:
1. Mammary: Pertaining to the breast or mammary glands in females, which are responsible for milk production.
2. Neoplasms: Abnormal growths of tissue, also known as tumors or masses, that can be benign (non-cancerous) or malignant (cancerous).
3. Experimental: Relating to a scientific experiment or study, typically conducted in a controlled setting to test hypotheses and gather data.
In the context of medical research, 'experimental mammary neoplasms' may refer to artificially induced breast tumors in laboratory animals (such as rats or mice) for the purpose of studying the development, progression, treatment, and prevention of breast cancer. These studies can help researchers better understand the biology of breast cancer and develop new therapies and strategies for its diagnosis and management.
The Mitotic Index (MI) is a measure of cell proliferation that reflects the percentage of cells in a population or sample that are undergoing mitosis, which is the process of cell division. It is often expressed as the number of mitotic figures (dividing cells) per 100 or 1,000 cells counted in a microscopic field. The Mitotic Index is used in various fields, including pathology and research, to assess the growth fraction of cells in tissues or cultures, and to monitor the effects of treatments that affect cell division, such as chemotherapy or radiation therapy.
Paraffin embedding is a process in histology (the study of the microscopic structure of tissues) where tissue samples are impregnated with paraffin wax to create a solid, stable block. This allows for thin, uniform sections of the tissue to be cut and mounted on slides for further examination under a microscope.
The process involves fixing the tissue sample with a chemical fixative to preserve its structure, dehydrating it through a series of increasing concentrations of alcohol, clearing it in a solvent such as xylene to remove the alcohol, and then impregnating it with melted paraffin wax. The tissue is then cooled and hardened into a block, which can be stored, transported, and sectioned as needed.
Paraffin embedding is a commonly used technique in histology due to its relative simplicity, low cost, and ability to produce high-quality sections for microscopic examination.
The Papanicolaou (Pap) test, also known as the Pap smear, is a screening procedure for detecting precancerous and cancerous cells in the cervix. It involves collecting cells from the cervix and examining them under a microscope to look for any abnormalities. The test is typically recommended for women aged 21-65 as part of routine pelvic exams, with the frequency depending on age and risk factors.
The Pap test was developed by Georgios Papanikolaou in the early 20th century and has since become a widely used and important tool in preventing cervical cancer. The test is usually performed in a healthcare provider's office and takes only a few minutes to complete. It is a relatively simple, safe, and painless procedure that can help detect cervical abnormalities at an early stage, when they are most treatable.
The glottis is a medical term that refers to the opening between the vocal cords (the ligaments in the larynx that produce sound when air passes through them during speech) in the human throat or larynx. It is an important structure for breathing, swallowing, and producing sounds or speech. The glottis opens during inhalation to allow air into the lungs and closes during swallowing to prevent food or liquids from entering the trachea (windpipe) and lungs.
Rectal neoplasms refer to abnormal growths in the tissues of the rectum, which can be benign or malignant. They are characterized by uncontrolled cell division and can invade nearby tissues or spread to other parts of the body (metastasis). The most common type of rectal neoplasm is rectal cancer, which often begins as a small polyp or growth in the lining of the rectum. Other types of rectal neoplasms include adenomas, carcinoids, and gastrointestinal stromal tumors (GISTs). Regular screenings are recommended for early detection and treatment of rectal neoplasms.
Beta-catenin is a protein that plays a crucial role in gene transcription and cell-cell adhesion. It is a key component of the Wnt signaling pathway, which regulates various processes such as cell proliferation, differentiation, and migration during embryonic development and tissue homeostasis in adults.
In the absence of Wnt signals, beta-catenin forms a complex with other proteins, including adenomatous polyposis coli (APC) and axin, which targets it for degradation by the proteasome. When Wnt ligands bind to their receptors, this complex is disrupted, allowing beta-catenin to accumulate in the cytoplasm and translocate to the nucleus. In the nucleus, beta-catenin interacts with T cell factor/lymphoid enhancer-binding factor (TCF/LEF) transcription factors to activate the transcription of target genes involved in cell fate determination, survival, and proliferation.
Mutations in the genes encoding components of the Wnt signaling pathway, including beta-catenin, have been implicated in various human diseases, such as cancer, developmental disorders, and degenerative conditions.
Neoadjuvant therapy is a treatment regimen that is administered to patients before they undergo definitive or curative surgery for their cancer. The main goal of neoadjuvant therapy is to reduce the size and extent of the tumor, making it easier to remove surgically and increasing the likelihood of complete resection. This type of therapy often involves the use of chemotherapy, radiation therapy, or targeted therapy, and it can help improve treatment outcomes by reducing the risk of recurrence and improving overall survival rates. Neoadjuvant therapy is commonly used in the treatment of various types of cancer, including breast, lung, esophageal, rectal, and bladder cancer.
Reproducibility of results in a medical context refers to the ability to obtain consistent and comparable findings when a particular experiment or study is repeated, either by the same researcher or by different researchers, following the same experimental protocol. It is an essential principle in scientific research that helps to ensure the validity and reliability of research findings.
In medical research, reproducibility of results is crucial for establishing the effectiveness and safety of new treatments, interventions, or diagnostic tools. It involves conducting well-designed studies with adequate sample sizes, appropriate statistical analyses, and transparent reporting of methods and findings to allow other researchers to replicate the study and confirm or refute the results.
The lack of reproducibility in medical research has become a significant concern in recent years, as several high-profile studies have failed to produce consistent findings when replicated by other researchers. This has led to increased scrutiny of research practices and a call for greater transparency, rigor, and standardization in the conduct and reporting of medical research.
CD44 is a type of protein found on the surface of some cells in the human body. It is a cell adhesion molecule and is involved in various biological processes such as cell-cell interaction, lymphocyte activation, and migration of cells. CD44 also acts as a receptor for hyaluronic acid, a component of the extracellular matrix.
As an antigen, CD44 can be recognized by certain immune cells, including T cells and B cells, and can play a role in the immune response. There are several isoforms of CD44 that exist due to alternative splicing of its mRNA, leading to differences in its structure and function.
CD44 has been studied in the context of cancer, where it can contribute to tumor growth, progression, and metastasis. In some cases, high levels of CD44 have been associated with poor prognosis in certain types of cancer. However, CD44 also has potential roles in tumor suppression and immune surveillance, making its overall role in cancer complex and context-dependent.
Parotid neoplasms refer to abnormal growths or tumors in the parotid gland, which is the largest of the salivary glands and is located in front of the ear and extends down the neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parotid neoplasms are typically slow-growing, painless masses that may cause facial asymmetry or difficulty in chewing or swallowing if they become large enough to compress surrounding structures. The most common type of benign parotid tumor is a pleomorphic adenoma.
Malignant parotid neoplasms, on the other hand, are more aggressive and can invade nearby tissues and spread to other parts of the body. They may present as rapidly growing masses that are firm or fixed to surrounding structures. Common types of malignant parotid tumors include mucoepidermoid carcinoma, adenoid cystic carcinoma, and squamous cell carcinoma.
The diagnosis of parotid neoplasms typically involves a thorough clinical evaluation, imaging studies such as CT or MRI scans, and fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Treatment options depend on the type, size, and location of the neoplasm but may include surgical excision, radiation therapy, and chemotherapy.
Trans-activators are proteins that increase the transcriptional activity of a gene or a set of genes. They do this by binding to specific DNA sequences and interacting with the transcription machinery, thereby enhancing the recruitment and assembly of the complexes needed for transcription. In some cases, trans-activators can also modulate the chromatin structure to make the template more accessible to the transcription machinery.
In the context of HIV (Human Immunodeficiency Virus) infection, the term "trans-activator" is often used specifically to refer to the Tat protein. The Tat protein is a viral regulatory protein that plays a critical role in the replication of HIV by activating the transcription of the viral genome. It does this by binding to a specific RNA structure called the Trans-Activation Response Element (TAR) located at the 5' end of all nascent HIV transcripts, and recruiting cellular cofactors that enhance the processivity and efficiency of RNA polymerase II, leading to increased viral gene expression.
Quinazolines are not a medical term per se, but they are a class of organic compounds that have been widely used in the development of various pharmaceutical drugs. Therefore, I will provide you with a chemical definition of quinazolines:
Quinazolines are heterocyclic aromatic organic compounds consisting of a benzene ring fused to a pyrazine ring. The structure can be represented as follows:
Quinazoline
They are often used as building blocks in the synthesis of various drugs, including those used for treating cancer, cardiovascular diseases, and microbial infections. Some examples of FDA-approved drugs containing a quinazoline core include the tyrosine kinase inhibitors gefitinib (Iressa) and erlotinib (Tarceva), which are used to treat non-small cell lung cancer, and the calcium channel blocker verapamil (Calan, Isoptin), which is used to treat hypertension and angina.
RNA interference (RNAi) is a biological process in which RNA molecules inhibit the expression of specific genes. This process is mediated by small RNA molecules, including microRNAs (miRNAs) and small interfering RNAs (siRNAs), that bind to complementary sequences on messenger RNA (mRNA) molecules, leading to their degradation or translation inhibition.
RNAi plays a crucial role in regulating gene expression and defending against foreign genetic elements, such as viruses and transposons. It has also emerged as an important tool for studying gene function and developing therapeutic strategies for various diseases, including cancer and viral infections.
Brachytherapy is a type of cancer treatment that involves placing radioactive material directly into or near the tumor site. The term "brachy" comes from the Greek word for "short," which refers to the short distance that the radiation travels. This allows for a high dose of radiation to be delivered directly to the tumor while minimizing exposure to healthy surrounding tissue.
There are two main types of brachytherapy:
1. Intracavitary brachytherapy: The radioactive material is placed inside a body cavity, such as the uterus or windpipe.
2. Interstitial brachytherapy: The radioactive material is placed directly into the tumor or surrounding tissue using needles, seeds, or catheters.
Brachytherapy can be used alone or in combination with other cancer treatments such as surgery, external beam radiation therapy, and chemotherapy. It may be recommended for a variety of cancers, including prostate, cervical, vaginal, vulvar, head and neck, and skin cancers. The specific type of brachytherapy used will depend on the size, location, and stage of the tumor.
The advantages of brachytherapy include its ability to deliver a high dose of radiation directly to the tumor while minimizing exposure to healthy tissue, which can result in fewer side effects compared to other forms of radiation therapy. Additionally, brachytherapy is often a shorter treatment course than external beam radiation therapy, with some treatments lasting only a few minutes or hours.
However, there are also potential risks and side effects associated with brachytherapy, including damage to nearby organs and tissues, bleeding, infection, and pain. Patients should discuss the benefits and risks of brachytherapy with their healthcare provider to determine if it is an appropriate treatment option for them.
Thyroidectomy is a surgical procedure where all or part of the thyroid gland is removed. The thyroid gland is a butterfly-shaped endocrine gland located in the neck, responsible for producing hormones that regulate metabolism, growth, and development.
There are different types of thyroidectomy procedures, including:
1. Total thyroidectomy: Removal of the entire thyroid gland.
2. Partial (or subtotal) thyroidectomy: Removal of a portion of the thyroid gland.
3. Hemithyroidectomy: Removal of one lobe of the thyroid gland, often performed to treat benign solitary nodules or differentiated thyroid cancer.
Thyroidectomy may be recommended for various reasons, such as treating thyroid nodules, goiter, hyperthyroidism (overactive thyroid), or thyroid cancer. Potential risks and complications of the procedure include bleeding, infection, damage to nearby structures like the parathyroid glands and recurrent laryngeal nerve, and hypoparathyroidism or hypothyroidism due to removal of or damage to the parathyroid glands or thyroid gland, respectively. Close postoperative monitoring and management are essential to minimize these risks and ensure optimal patient outcomes.
A "mixed tumor, malignant" is a rare and aggressive type of cancer that contains two or more different types of malignant tissue. It is also known as a "malignant mixed Mullerian tumor" (MMMT) or "carcinosarcoma." This type of tumor most commonly arises in the female reproductive organs, such as the uterus or ovaries, but can also occur in other parts of the body.
The malignant mixed Mullerian tumor is composed of both epithelial and mesenchymal components, which are two different types of tissue. The epithelial component is made up of cancerous glandular or squamous cells, while the mesenchymal component consists of cancerous connective tissue, such as muscle, fat, or bone.
Mixed tumors, malignant can be aggressive and have a high risk of recurrence and metastasis. Treatment typically involves surgical removal of the tumor, followed by radiation therapy and/or chemotherapy to kill any remaining cancer cells. The prognosis for mixed tumors, malignant varies depending on several factors, including the size and location of the tumor, the stage of the disease at diagnosis, and the patient's overall health.
Epithelial-mesenchymal transition (EMT) is a biological process that involves the transformation of epithelial cells into mesenchymal cells. This process is characterized by distinct changes in cell shape, behavior, and molecular markers.
Epithelial cells are typically tightly packed together and have a polarized structure with distinct apical and basal surfaces. In contrast, mesenchymal cells are elongated, spindle-shaped cells that can migrate and invade surrounding tissues.
During EMT, epithelial cells lose their polarity and cell-to-cell adhesion molecules, such as E-cadherin, and acquire mesenchymal markers, such as vimentin and N-cadherin. This transition enables the cells to become more motile and invasive, which is critical for embryonic development, wound healing, and cancer metastasis.
EMT is a complex process that involves various signaling pathways, including TGF-β, Wnt, Notch, and Hedgehog, among others. Dysregulation of EMT has been implicated in several diseases, particularly cancer, where it contributes to tumor progression, metastasis, and drug resistance.
Monoclonal antibodies are laboratory-produced proteins that mimic the immune system's ability to fight off harmful antigens such as viruses and cancer cells. They are created by fusing a single B cell (the type of white blood cell responsible for producing antibodies) with a tumor cell, resulting in a hybrid cell called a hybridoma. This hybridoma can then be cloned to produce a large number of identical cells, all producing the same antibody, hence "monoclonal."
Humanized monoclonal antibodies are a type of monoclonal antibody that have been genetically engineered to include human components. This is done to reduce the risk of an adverse immune response in patients receiving the treatment. In this process, the variable region of the mouse monoclonal antibody, which contains the antigen-binding site, is grafted onto a human constant region. The resulting humanized monoclonal antibody retains the ability to bind to the target antigen while minimizing the immunogenicity associated with murine (mouse) antibodies.
In summary, "antibodies, monoclonal, humanized" refers to a type of laboratory-produced protein that mimics the immune system's ability to fight off harmful antigens, but with reduced immunogenicity due to the inclusion of human components in their structure.
An allele is a variant form of a gene that is located at a specific position on a specific chromosome. Alleles are alternative forms of the same gene that arise by mutation and are found at the same locus or position on homologous chromosomes.
Each person typically inherits two copies of each gene, one from each parent. If the two alleles are identical, a person is said to be homozygous for that trait. If the alleles are different, the person is heterozygous.
For example, the ABO blood group system has three alleles, A, B, and O, which determine a person's blood type. If a person inherits two A alleles, they will have type A blood; if they inherit one A and one B allele, they will have type AB blood; if they inherit two B alleles, they will have type B blood; and if they inherit two O alleles, they will have type O blood.
Alleles can also influence traits such as eye color, hair color, height, and other physical characteristics. Some alleles are dominant, meaning that only one copy of the allele is needed to express the trait, while others are recessive, meaning that two copies of the allele are needed to express the trait.
Gene dosage, in genetic terms, refers to the number of copies of a particular gene present in an organism's genome. Each gene usually has two copies (alleles) in diploid organisms, one inherited from each parent. An increase or decrease in the number of copies of a specific gene can lead to changes in the amount of protein it encodes, which can subsequently affect various biological processes and phenotypic traits.
For example, gene dosage imbalances have been associated with several genetic disorders, such as Down syndrome (trisomy 21), where an individual has three copies of chromosome 21 instead of the typical two copies, leading to developmental delays and intellectual disabilities. Similarly, in certain cases of cancer, gene amplification (an increase in the number of copies of a particular gene) can result in overexpression of oncogenes, contributing to tumor growth and progression.
Microdissection is a surgical technique that involves the use of a microscope to allow for precise, minimalistic dissection of tissue. It is often used in research and clinical settings to isolate specific cells, tissues or structures while minimizing damage to surrounding areas. This technique can be performed using various methods such as laser capture microdissection (LCM) or manual microdissection with microsurgical tools. The size and scale of the dissection required will determine the specific method used. In general, microdissection allows for the examination and analysis of very small and delicate structures that would otherwise be difficult to access and study.
Eye neoplasms, also known as ocular tumors or eye cancer, refer to abnormal growths of tissue in the eye. These growths can be benign (non-cancerous) or malignant (cancerous). Eye neoplasms can develop in various parts of the eye, including the eyelid, conjunctiva, cornea, iris, ciliary body, choroid, retina, and optic nerve.
Benign eye neoplasms are typically slow-growing and do not spread to other parts of the body. They may cause symptoms such as vision changes, eye pain, or a noticeable mass in the eye. Treatment options for benign eye neoplasms include monitoring, surgical removal, or radiation therapy.
Malignant eye neoplasms, on the other hand, can grow and spread rapidly to other parts of the body. They may cause symptoms such as vision changes, eye pain, floaters, or flashes of light. Treatment options for malignant eye neoplasms depend on the type and stage of cancer but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
It is important to note that early detection and treatment of eye neoplasms can improve outcomes and prevent complications. Regular eye exams with an ophthalmologist are recommended for early detection and prevention of eye diseases, including eye neoplasms.
Cocarcinogenesis is a term used in the field of oncology to describe a process where exposure to certain chemicals or physical agents enhances the tumor-forming ability of a cancer-causing agent (carcinogen). A cocarcinogen does not have the ability to initiate cancer on its own, but it can promote the development and progression of cancer when combined with a carcinogen.
In other words, a cocarcinogen is a substance or factor that acts synergistically with a known carcinogen to increase the likelihood or speed up the development of cancer. This process can occur through various mechanisms, such as suppressing the immune system, promoting inflammation, increasing cell proliferation, or inhibiting apoptosis (programmed cell death).
Examples of cocarcinogens include tobacco smoke, alcohol, certain viruses, and radiation. These agents can interact with carcinogens to increase the risk of cancer in individuals who are exposed to them. It is important to note that while cocarcinogens themselves may not directly cause cancer, they can significantly contribute to its development and progression when combined with other harmful substances or factors.
Cell growth processes refer to the series of events that occur within a cell leading to an increase in its size, mass, and number of organelles. These processes are essential for the development, maintenance, and reproduction of all living organisms. The main cell growth processes include:
1. Cell Cycle: It is the sequence of events that a eukaryotic cell goes through from one cell division (mitosis) to the next. The cell cycle consists of four distinct phases: G1 phase (growth and preparation for DNA replication), S phase (DNA synthesis), G2 phase (preparation for mitosis), and M phase (mitosis or meiosis).
2. DNA Replication: It is the process by which a cell makes an identical copy of its DNA molecule before cell division. This ensures that each daughter cell receives an exact replica of the parent cell's genetic material.
3. Protein Synthesis: Cells grow by increasing their protein content, which is achieved through the process of protein synthesis. This involves transcribing DNA into mRNA (transcription) and then translating that mRNA into a specific protein sequence (translation).
4. Cellular Metabolism: It refers to the sum total of all chemical reactions that occur within a cell to maintain life. These reactions include catabolic processes, which break down nutrients to release energy, and anabolic processes, which use energy to build complex molecules like proteins, lipids, and carbohydrates.
5. Cell Signaling: Cells communicate with each other through intricate signaling pathways that help coordinate growth, differentiation, and survival. These signals can come from within the cell (intracellular) or from outside the cell (extracellular).
6. Cell Division: Also known as mitosis, it is the process by which a single cell divides into two identical daughter cells. This ensures that each new cell contains an exact copy of the parent cell's genetic material and allows for growth and repair of tissues.
7. Apoptosis: It is a programmed cell death process that helps maintain tissue homeostasis by eliminating damaged or unnecessary cells. Dysregulation of apoptosis can lead to diseases such as cancer and autoimmune disorders.
According to the medical definition, ultraviolet (UV) rays are invisible radiations that fall in the range of the electromagnetic spectrum between 100-400 nanometers. UV rays are further divided into three categories: UVA (320-400 nm), UVB (280-320 nm), and UVC (100-280 nm).
UV rays have various sources, including the sun and artificial sources like tanning beds. Prolonged exposure to UV rays can cause damage to the skin, leading to premature aging, eye damage, and an increased risk of skin cancer. UVA rays penetrate deeper into the skin and are associated with skin aging, while UVB rays primarily affect the outer layer of the skin and are linked to sunburns and skin cancer. UVC rays are the most harmful but fortunately, they are absorbed by the Earth's atmosphere and do not reach the surface.
Healthcare professionals recommend limiting exposure to UV rays, wearing protective clothing, using broad-spectrum sunscreen with an SPF of at least 30, and avoiding tanning beds to reduce the risk of UV-related health problems.
Niacinamide, also known as nicotinamide, is a form of vitamin B3 (niacin). It is a water-soluble vitamin that is involved in energy production and DNA repair in the body. Niacinamide can be found in various foods such as meat, fish, milk, eggs, green vegetables, and cereal grains.
As a medical definition, niacinamide is a nutritional supplement and medication used to prevent or treat pellagra, a disease caused by niacin deficiency. It can also be used to improve skin conditions such as acne, rosacea, and hyperpigmentation, and has been studied for its potential benefits in treating diabetes, cancer, and Alzheimer's disease.
Niacinamide works by acting as a precursor to nicotinamide adenine dinucleotide (NAD), a coenzyme involved in many cellular processes such as energy metabolism, DNA repair, and gene expression. Niacinamide has anti-inflammatory properties and can help regulate the immune system, making it useful for treating inflammatory skin conditions.
It is important to note that niacinamide should not be confused with niacin (also known as nicotinic acid), which is another form of vitamin B3 that has different effects on the body. Niacin can cause flushing and other side effects at higher doses, while niacinamide does not have these effects.
Mucin-1, also known as MUC1, is a type of protein called a transmembrane mucin. It is heavily glycosylated and found on the surface of many types of epithelial cells, including those that line the respiratory, gastrointestinal, and urogenital tracts.
Mucin-1 has several functions, including:
* Protecting the underlying epithelial cells from damage caused by friction, chemicals, and microorganisms
* Helping to maintain the integrity of the mucosal barrier
* Acting as a receptor for various signaling molecules
* Participating in immune responses
In cancer, MUC1 can be overexpressed or aberrantly glycosylated, which can contribute to tumor growth and metastasis. As a result, MUC1 has been studied as a potential target for cancer immunotherapy.
Phenylurea compounds are a class of chemical compounds that contain a phenyl group (a functional group consisting of a six-membered aromatic ring with a hydrogen atom and a single bond to a carbon atom or other group) linked to a urea moiety. Urea is an organic compound that contains a carbonyl functional group connected to two amine groups.
Phenylurea compounds are commonly used as herbicides, fungicides, and insecticides in agriculture due to their ability to inhibit certain enzymes and disrupt plant growth processes. Some examples of phenylurea compounds include chlorotoluron, diuron, linuron, and monuron.
It is important to note that some phenylurea compounds have been found to be toxic to non-target organisms, including mammals, birds, and fish, and can pose environmental risks if not used properly. Therefore, it is essential to follow the recommended guidelines for their use and disposal to minimize potential health and ecological impacts.
The breast is the upper ventral region of the human body in females, which contains the mammary gland. The main function of the breast is to provide nutrition to infants through the production and secretion of milk, a process known as lactation. The breast is composed of fibrous connective tissue, adipose (fatty) tissue, and the mammary gland, which is made up of 15-20 lobes that are arranged in a radial pattern. Each lobe contains many smaller lobules, where milk is produced during lactation. The milk is then transported through a network of ducts to the nipple, where it can be expressed by the infant.
In addition to its role in lactation, the breast also has important endocrine and psychological functions. It contains receptors for hormones such as estrogen and progesterone, which play a key role in sexual development and reproduction. The breast is also a source of sexual pleasure and can be an important symbol of femininity and motherhood.
It's worth noting that males also have breast tissue, although it is usually less developed than in females. Male breast tissue consists mainly of adipose tissue and does not typically contain functional mammary glands. However, some men may develop enlarged breast tissue due to conditions such as gynecomastia, which can be caused by hormonal imbalances or certain medications.
Fluorodeoxyglucose F18 (FDG-18) is not a medical condition, but a radiopharmaceutical used in medical imaging. It is a type of glucose (a simple sugar) that has been chemically combined with a small amount of a radioactive isotope called fluorine-18.
FDG-18 is used in positron emission tomography (PET) scans to help identify areas of the body where cells are using more energy than normal, such as cancerous tumors. The FDG-18 is injected into the patient's vein and travels throughout the body. Because cancer cells often use more glucose than normal cells, they tend to absorb more FDG-18.
Once inside the body, the FDG-18 emits positrons, which interact with electrons in nearby tissue, producing gamma rays that can be detected by a PET scanner. The resulting images can help doctors locate and assess the size and activity of cancerous tumors, as well as monitor the effectiveness of treatment.
A "Drug Administration Schedule" refers to the plan for when and how a medication should be given to a patient. It includes details such as the dose, frequency (how often it should be taken), route (how it should be administered, such as orally, intravenously, etc.), and duration (how long it should be taken) of the medication. This schedule is often created and prescribed by healthcare professionals, such as doctors or pharmacists, to ensure that the medication is taken safely and effectively. It may also include instructions for missed doses or changes in the dosage.
Gene knockdown techniques are methods used to reduce the expression or function of specific genes in order to study their role in biological processes. These techniques typically involve the use of small RNA molecules, such as siRNAs (small interfering RNAs) or shRNAs (short hairpin RNAs), which bind to and promote the degradation of complementary mRNA transcripts. This results in a decrease in the production of the protein encoded by the targeted gene.
Gene knockdown techniques are often used as an alternative to traditional gene knockout methods, which involve completely removing or disrupting the function of a gene. Knockdown techniques allow for more subtle and reversible manipulation of gene expression, making them useful for studying genes that are essential for cell survival or have redundant functions.
These techniques are widely used in molecular biology research to investigate gene function, genetic interactions, and disease mechanisms. However, it is important to note that gene knockdown can have off-target effects and may not completely eliminate the expression of the targeted gene, so results should be interpreted with caution.
Lichen Sclerosus et Atrophicus (LSEA) is a chronic inflammatory skin condition that can affect both males and females, but it's most commonly found in women after menopause. It can occur at any age, including children. The condition typically affects the genital and anal areas, though it can appear elsewhere on the body as well.
The medical definition of Lichen Sclerosus et Atrophicus is:
A skin disorder characterized by white patches (plaques) that can be smooth or wrinkled, thickened, and easily bruised. These patches may merge to form larger areas of affected skin. The condition can cause itching, burning, pain, and blistering. In women, the vulva is often affected, and sexual intercourse may become painful. In men, it can affect the foreskin and glans penis, leading to difficulty urinating or having sex.
The exact cause of Lichen Sclerosus et Atrophicus remains unknown, but it's believed that hormonal imbalances, genetics, and an overactive immune system may play a role in its development. Treatment usually involves topical corticosteroids to reduce inflammation and alleviate symptoms. In some cases, other medications or phototherapy might be recommended. It is essential to consult with a healthcare professional for proper diagnosis and treatment.
The larynx, also known as the voice box, is a complex structure in the neck that plays a crucial role in protection of the lower respiratory tract and in phonation. It is composed of cartilaginous, muscular, and soft tissue structures. The primary functions of the larynx include:
1. Airway protection: During swallowing, the larynx moves upward and forward to close the opening of the trachea (the glottis) and prevent food or liquids from entering the lungs. This action is known as the swallowing reflex.
2. Phonation: The vocal cords within the larynx vibrate when air passes through them, producing sound that forms the basis of human speech and voice production.
3. Respiration: The larynx serves as a conduit for airflow between the upper and lower respiratory tracts during breathing.
The larynx is located at the level of the C3-C6 vertebrae in the neck, just above the trachea. It consists of several important structures:
1. Cartilages: The laryngeal cartilages include the thyroid, cricoid, and arytenoid cartilages, as well as the corniculate and cuneiform cartilages. These form a framework for the larynx and provide attachment points for various muscles.
2. Vocal cords: The vocal cords are thin bands of mucous membrane that stretch across the glottis (the opening between the arytenoid cartilages). They vibrate when air passes through them, producing sound.
3. Muscles: There are several intrinsic and extrinsic muscles associated with the larynx. The intrinsic muscles control the tension and position of the vocal cords, while the extrinsic muscles adjust the position and movement of the larynx within the neck.
4. Nerves: The larynx is innervated by both sensory and motor nerves. The recurrent laryngeal nerve provides motor innervation to all intrinsic laryngeal muscles, except for one muscle called the cricothyroid, which is innervated by the external branch of the superior laryngeal nerve. Sensory innervation is provided by the internal branch of the superior laryngeal nerve and the recurrent laryngeal nerve.
The larynx plays a crucial role in several essential functions, including breathing, speaking, and protecting the airway during swallowing. Dysfunction or damage to the larynx can result in various symptoms, such as hoarseness, difficulty swallowing, shortness of breath, or stridor (a high-pitched sound heard during inspiration).
SCID mice is an acronym for Severe Combined Immunodeficiency mice. These are genetically modified mice that lack a functional immune system due to the mutation or knockout of several key genes required for immunity. This makes them ideal for studying the human immune system, infectious diseases, and cancer, as well as testing new therapies and treatments in a controlled environment without the risk of interference from the mouse's own immune system. SCID mice are often used in xenotransplantation studies, where human cells or tissues are transplanted into the mouse to study their behavior and interactions with the human immune system.
The cell nucleus is a membrane-bound organelle found in the eukaryotic cells (cells with a true nucleus). It contains most of the cell's genetic material, organized as DNA molecules in complex with proteins, RNA molecules, and histones to form chromosomes.
The primary function of the cell nucleus is to regulate and control the activities of the cell, including growth, metabolism, protein synthesis, and reproduction. It also plays a crucial role in the process of mitosis (cell division) by separating and protecting the genetic material during this process. The nuclear membrane, or nuclear envelope, surrounding the nucleus is composed of two lipid bilayers with numerous pores that allow for the selective transport of molecules between the nucleoplasm (nucleus interior) and the cytoplasm (cell exterior).
The cell nucleus is a vital structure in eukaryotic cells, and its dysfunction can lead to various diseases, including cancer and genetic disorders.
Small Cell Lung Carcinoma (SCLC) is a type of lung cancer that typically originates in the central part of the lungs. It is called "small cell" because the tumor cells appear small and round under a microscope. SCLC is an aggressive form of lung cancer that tends to spread rapidly to other parts of the body, such as the lymph nodes, liver, bones, and brain.
SCLC is strongly associated with smoking and is relatively uncommon in people who have never smoked. It accounts for about 10-15% of all lung cancer cases. SCLC is often diagnosed at a later stage because it can grow quickly and cause symptoms such as coughing, chest pain, shortness of breath, and weight loss.
Treatment for SCLC typically involves a combination of chemotherapy and radiation therapy. Surgery is not usually an option due to the advanced stage of the disease at diagnosis. The prognosis for SCLC is generally poor, with a five-year survival rate of less than 7%. However, early detection and treatment can improve outcomes in some cases.
Benzenesulfonates are organic compounds that contain a benzene ring substituted with a sulfonate group. In chemistry, a sulfonate group is a functional group consisting of a sulfur atom connected to three oxygen atoms (-SO3). Benzenesulfonates are often used as detergents, emulsifiers, and phase transfer catalysts in various chemical reactions. They can also be found in some pharmaceuticals and dyes.
The Chi-square distribution is a continuous probability distribution that is often used in statistical hypothesis testing. It is the distribution of a sum of squares of k independent standard normal random variables. The resulting quantity follows a chi-square distribution with k degrees of freedom, denoted as χ²(k).
The probability density function (pdf) of the Chi-square distribution with k degrees of freedom is given by:
f(x; k) = (1/ (2^(k/2) * Γ(k/2))) \* x^((k/2)-1) \* e^(-x/2), for x > 0 and 0, otherwise.
Where Γ(k/2) is the gamma function evaluated at k/2. The mean and variance of a Chi-square distribution with k degrees of freedom are k and 2k, respectively.
The Chi-square distribution has various applications in statistical inference, including testing goodness-of-fit, homogeneity of variances, and independence in contingency tables.
Acid anhydride hydrolases are a class of enzymes that catalyze the hydrolysis (breakdown) of acid anhydrides, which are chemical compounds formed by the reaction between two carboxylic acids. This reaction results in the formation of a molecule of water and the release of a new carboxylic acid.
Acid anhydride hydrolases play important roles in various biological processes, including the metabolism of lipids, carbohydrates, and amino acids. They are also involved in the regulation of intracellular pH and the detoxification of xenobiotics (foreign substances).
Examples of acid anhydride hydrolases include esterases, lipases, and phosphatases. These enzymes have different substrate specificities and catalytic mechanisms, but they all share the ability to hydrolyze acid anhydrides.
The term "acid anhydride hydrolase" is often used interchangeably with "esterase," although not all esterases are capable of hydrolyzing acid anhydrides.
Radiopharmaceuticals are defined as pharmaceutical preparations that contain radioactive isotopes and are used for diagnosis or therapy in nuclear medicine. These compounds are designed to interact specifically with certain biological targets, such as cells, tissues, or organs, and emit radiation that can be detected and measured to provide diagnostic information or used to destroy abnormal cells or tissue in therapeutic applications.
The radioactive isotopes used in radiopharmaceuticals have carefully controlled half-lives, which determine how long they remain radioactive and how long the pharmaceutical preparation remains effective. The choice of radioisotope depends on the intended use of the radiopharmaceutical, as well as factors such as its energy, range of emission, and chemical properties.
Radiopharmaceuticals are used in a wide range of medical applications, including imaging, cancer therapy, and treatment of other diseases and conditions. Examples of radiopharmaceuticals include technetium-99m for imaging the heart, lungs, and bones; iodine-131 for treating thyroid cancer; and samarium-153 for palliative treatment of bone metastases.
The use of radiopharmaceuticals requires specialized training and expertise in nuclear medicine, as well as strict adherence to safety protocols to minimize radiation exposure to patients and healthcare workers.
Radiation-sensitizing agents are drugs that make cancer cells more sensitive to radiation therapy. These agents work by increasing the ability of radiation to damage the DNA of cancer cells, which can lead to more effective tumor cell death. This means that lower doses of radiation may be required to achieve the same therapeutic effect, reducing the potential for damage to normal tissues surrounding the tumor.
Radiation-sensitizing agents are often used in conjunction with radiation therapy to improve treatment outcomes for patients with various types of cancer. They can be given either systemically (through the bloodstream) or locally (directly to the tumor site). The choice of agent and the timing of administration depend on several factors, including the type and stage of cancer, the patient's overall health, and the specific radiation therapy protocol being used.
It is important to note that while radiation-sensitizing agents can enhance the effectiveness of radiation therapy, they may also increase the risk of side effects. Therefore, careful monitoring and management of potential toxicities are essential during treatment.
Cecal neoplasms refer to abnormal growths in the cecum, which is the first part of the large intestine or colon. These growths can be benign (non-cancerous) or malignant (cancerous). Common types of cecal neoplasms include adenomas (benign tumors that can become cancerous over time), carcinoids (slow-growing tumors that usually don't spread), and adenocarcinomas (cancers that start in the glands that line the inside of the cecum).
Symptoms of cecal neoplasms may include changes in bowel habits, such as diarrhea or constipation; abdominal pain or cramping; blood in the stool; and unexplained weight loss. Treatment options depend on the type and stage of the neoplasm but may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. Regular screening is recommended for people at high risk for developing colorectal cancer, including those with a family history of the disease or certain genetic mutations.
A "cheek" is the fleshy, muscular area of the face that forms the side of the face below the eye and above the jaw. It contains the buccinator muscle, which helps with chewing by moving food to the back teeth for grinding and also assists in speaking and forming facial expressions. The cheek also contains several sensory receptors that allow us to perceive touch, temperature, and pain in this area of the face. Additionally, there is a mucous membrane lining inside the mouth cavity called the buccal mucosa which covers the inner surface of the cheek.
"Age factors" refer to the effects, changes, or differences that age can have on various aspects of health, disease, and medical care. These factors can encompass a wide range of issues, including:
1. Physiological changes: As people age, their bodies undergo numerous physical changes that can affect how they respond to medications, illnesses, and medical procedures. For example, older adults may be more sensitive to certain drugs or have weaker immune systems, making them more susceptible to infections.
2. Chronic conditions: Age is a significant risk factor for many chronic diseases, such as heart disease, diabetes, cancer, and arthritis. As a result, age-related medical issues are common and can impact treatment decisions and outcomes.
3. Cognitive decline: Aging can also lead to cognitive changes, including memory loss and decreased decision-making abilities. These changes can affect a person's ability to understand and comply with medical instructions, leading to potential complications in their care.
4. Functional limitations: Older adults may experience physical limitations that impact their mobility, strength, and balance, increasing the risk of falls and other injuries. These limitations can also make it more challenging for them to perform daily activities, such as bathing, dressing, or cooking.
5. Social determinants: Age-related factors, such as social isolation, poverty, and lack of access to transportation, can impact a person's ability to obtain necessary medical care and affect their overall health outcomes.
Understanding age factors is critical for healthcare providers to deliver high-quality, patient-centered care that addresses the unique needs and challenges of older adults. By taking these factors into account, healthcare providers can develop personalized treatment plans that consider a person's age, physical condition, cognitive abilities, and social circumstances.
The epidermis is the outermost layer of the skin, composed mainly of stratified squamous epithelium. It forms a protective barrier that prevents water loss and inhibits the entry of microorganisms. The epidermis contains no blood vessels, and its cells are nourished by diffusion from the underlying dermis. The bottom-most layer of the epidermis, called the stratum basale, is responsible for generating new skin cells that eventually move up to replace dead cells on the surface. This process of cell turnover takes about 28 days in adults.
The most superficial part of the epidermis consists of dead cells called squames, which are constantly shed and replaced. The exact rate at which this happens varies depending on location; for example, it's faster on the palms and soles than elsewhere. Melanocytes, the pigment-producing cells, are also located in the epidermis, specifically within the stratum basale layer.
In summary, the epidermis is a vital part of our integumentary system, providing not only physical protection but also playing a crucial role in immunity and sensory perception through touch receptors called Pacinian corpuscles.
Histochemistry is the branch of pathology that deals with the microscopic localization of cellular or tissue components using specific chemical reactions. It involves the application of chemical techniques to identify and locate specific biomolecules within tissues, cells, and subcellular structures. This is achieved through the use of various staining methods that react with specific antigens or enzymes in the sample, allowing for their visualization under a microscope. Histochemistry is widely used in diagnostic pathology to identify different types of tissues, cells, and structures, as well as in research to study cellular and molecular processes in health and disease.
Cyclin-dependent kinase inhibitor p21, also known as CDKN1A or p21/WAF1/CIP1, is a protein that regulates the cell cycle. It inhibits the activity of cyclin-dependent kinases (CDKs), which are enzymes that play crucial roles in controlling the progression of the cell cycle.
The binding of p21 to CDKs prevents the phosphorylation and activation of downstream targets, leading to cell cycle arrest. This protein is transcriptionally activated by tumor suppressor protein p53 in response to DNA damage or other stress signals, and it functions as an important mediator of p53-dependent growth arrest.
By inhibiting CDKs, p21 helps to ensure that cells do not proceed through the cell cycle until damaged DNA has been repaired, thereby preventing the propagation of potentially harmful mutations. Additionally, p21 has been implicated in other cellular processes such as apoptosis, differentiation, and senescence. Dysregulation of p21 has been associated with various human diseases, including cancer.
A teratoma is a type of germ cell tumor, which is a broad category of tumors that originate from the reproductive cells. A teratoma contains developed tissues from all three embryonic germ layers: ectoderm, mesoderm, and endoderm. This means that a teratoma can contain various types of tissue such as hair, teeth, bone, and even more complex organs like eyes, thyroid, or neural tissue.
Teratomas are usually benign (non-cancerous), but they can sometimes be malignant (cancerous) and can spread to other parts of the body. They can occur anywhere in the body, but they're most commonly found in the ovaries and testicles. When found in these areas, they are typically removed surgically.
Teratomas can also occur in other locations such as the sacrum, coccyx (tailbone), mediastinum (the area between the lungs), and pineal gland (a small gland in the brain). These types of teratomas can be more complex to treat due to their location and potential to cause damage to nearby structures.
Exons are the coding regions of DNA that remain in the mature, processed mRNA after the removal of non-coding intronic sequences during RNA splicing. These exons contain the information necessary to encode proteins, as they specify the sequence of amino acids within a polypeptide chain. The arrangement and order of exons can vary between different genes and even between different versions of the same gene (alternative splicing), allowing for the generation of multiple protein isoforms from a single gene. This complexity in exon structure and usage significantly contributes to the diversity and functionality of the proteome.
Antimetabolites are a class of antineoplastic (chemotherapy) drugs that interfere with the metabolism of cancer cells and inhibit their growth and proliferation. These agents are structurally similar to naturally occurring metabolites, such as amino acids, nucleotides, and folic acid, which are essential for cellular replication and growth. Antimetabolites act as false analogs and get incorporated into the growing cells' DNA or RNA, causing disruption of the normal synthesis process, leading to cell cycle arrest and apoptosis (programmed cell death).
Examples of antimetabolite drugs include:
1. Folate antagonists: Methotrexate, Pemetrexed
2. Purine analogs: Mercaptopurine, Thioguanine, Fludarabine, Cladribine
3. Pyrimidine analogs: 5-Fluorouracil (5-FU), Capecitabine, Cytarabine, Gemcitabine
These drugs are used to treat various types of cancers, such as leukemias, lymphomas, breast, ovarian, and gastrointestinal cancers. Due to their mechanism of action, antimetabolites can also affect normal, rapidly dividing cells in the body, leading to side effects like myelosuppression (decreased production of blood cells), mucositis (inflammation and ulceration of the gastrointestinal tract), and alopecia (hair loss).
A fine-needle biopsy (FNB) is a medical procedure in which a thin, hollow needle is used to obtain a sample of cells or tissue from a suspicious or abnormal area in the body, such as a lump or mass. The needle is typically smaller than that used in a core needle biopsy, and it is guided into place using imaging techniques such as ultrasound, CT scan, or MRI.
The sample obtained during an FNB can be used to diagnose various medical conditions, including cancer, infection, or inflammation. The procedure is generally considered safe and well-tolerated, with minimal risks of complications such as bleeding, infection, or discomfort. However, the accuracy of the diagnosis depends on the skill and experience of the healthcare provider performing the biopsy, as well as the adequacy of the sample obtained.
Overall, FNB is a valuable diagnostic tool that can help healthcare providers make informed decisions about treatment options and improve patient outcomes.
Oncogene proteins, viral, are cancer-causing proteins that are encoded by the genetic material (DNA or RNA) of certain viruses. These viral oncogenes can be acquired through infection with retroviruses, such as human immunodeficiency virus (HIV), human T-cell leukemia virus (HTLV), and certain types of papillomaviruses and polyomaviruses.
When these viruses infect host cells, they can integrate their genetic material into the host cell's genome, leading to the expression of viral oncogenes. These oncogenes may then cause uncontrolled cell growth and division, ultimately resulting in the formation of tumors or cancers. The process by which viruses contribute to cancer development is complex and involves multiple steps, including the alteration of signaling pathways that regulate cell proliferation, differentiation, and survival.
Examples of viral oncogenes include the v-src gene found in the Rous sarcoma virus (RSV), which causes chicken sarcoma, and the E6 and E7 genes found in human papillomaviruses (HPVs), which are associated with cervical cancer and other anogenital cancers. Understanding viral oncogenes and their mechanisms of action is crucial for developing effective strategies to prevent and treat virus-associated cancers.
Risk assessment in the medical context refers to the process of identifying, evaluating, and prioritizing risks to patients, healthcare workers, or the community related to healthcare delivery. It involves determining the likelihood and potential impact of adverse events or hazards, such as infectious diseases, medication errors, or medical devices failures, and implementing measures to mitigate or manage those risks. The goal of risk assessment is to promote safe and high-quality care by identifying areas for improvement and taking action to minimize harm.
Ploidy is a term used in genetics to describe the number of sets of chromosomes in a cell or an organism. The ploidy level can have important implications for genetic inheritance and expression, as well as for evolutionary processes such as speciation and hybridization.
In most animals, including humans, the normal ploidy level is diploid, meaning that each cell contains two sets of chromosomes - one set inherited from each parent. However, there are also many examples of polyploidy, in which an organism has more than two sets of chromosomes.
Polyploidy can arise through various mechanisms, such as genome duplication or hybridization between different species. In some cases, polyploidy may confer evolutionary advantages, such as increased genetic diversity and adaptability to new environments. However, it can also lead to reproductive isolation and the formation of new species.
In plants, polyploidy is relatively common and has played a significant role in their evolution and diversification. Many crop plants are polyploids, including wheat, cotton, and tobacco. In some cases, artificial induction of polyploidy has been used to create new varieties with desirable traits for agriculture and horticulture.
Overall, ploidy is an important concept in genetics and evolution, with implications for a wide range of biological processes and phenomena.
Uterine neoplasms refer to abnormal growths in the uterus, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from different types of cells within the uterus, leading to various types of uterine neoplasms. The two main categories of uterine neoplasms are endometrial neoplasms and uterine sarcomas.
Endometrial neoplasms develop from the endometrium, which is the inner lining of the uterus. Most endometrial neoplasms are classified as endometrioid adenocarcinomas, arising from glandular cells in the endometrium. Other types include serous carcinoma, clear cell carcinoma, and mucinous carcinoma.
Uterine sarcomas, on the other hand, are less common and originate from the connective tissue (stroma) or muscle (myometrium) of the uterus. Uterine sarcomas can be further divided into several subtypes, such as leiomyosarcoma, endometrial stromal sarcoma, and undifferentiated uterine sarcoma.
Uterine neoplasms can cause various symptoms, including abnormal vaginal bleeding or discharge, pelvic pain, and difficulty urinating or having bowel movements. The diagnosis typically involves a combination of imaging tests (such as ultrasound, CT, or MRI scans) and tissue biopsies to determine the type and extent of the neoplasm. Treatment options depend on the type, stage, and patient's overall health but may include surgery, radiation therapy, chemotherapy, or hormone therapy.
Inhibitor of Apoptosis Proteins (IAPs) are a family of proteins that play a crucial role in regulating programmed cell death, also known as apoptosis. These proteins function by binding to and inhibiting the activity of caspases, which are enzymes that drive the execution phase of apoptosis.
There are eight known human IAPs, including X-linked IAP (XIAP), cellular IAP1 (cIAP1), cIAP2, survivin, melanoma IAP (ML-IAP), ILP-2, NAIP, and Bruce. Each IAP contains at least one baculoviral IAP repeat (BIR) domain, which is responsible for binding to caspases and other regulatory proteins.
In addition to inhibiting caspases, some IAPs have been shown to regulate other cellular processes, such as inflammation, innate immunity, and cell cycle progression. Dysregulation of IAP function has been implicated in various diseases, including cancer, neurodegenerative disorders, and autoimmune diseases. Therefore, IAPs are considered important targets for the development of new therapeutic strategies aimed at modulating apoptosis and other cellular processes.
Experimental liver neoplasms refer to abnormal growths or tumors in the liver that are intentionally created or manipulated in a laboratory setting for the purpose of studying their development, progression, and potential treatment options. These experimental models can be established using various methods such as chemical induction, genetic modification, or transplantation of cancerous cells or tissues. The goal of this research is to advance our understanding of liver cancer biology and develop novel therapies for liver neoplasms in humans. It's important to note that these experiments are conducted under strict ethical guidelines and regulations to minimize harm and ensure the humane treatment of animals involved in such studies.
Pancreatic ductal carcinoma (PDC) is a specific type of cancer that forms in the ducts that carry digestive enzymes out of the pancreas. It's the most common form of exocrine pancreatic cancer, making up about 90% of all cases.
The symptoms of PDC are often vague and can include abdominal pain, jaundice (yellowing of the skin and eyes), unexplained weight loss, and changes in bowel movements. These symptoms can be similar to those caused by other less serious conditions, which can make diagnosis difficult.
Pancreatic ductal carcinoma is often aggressive and difficult to treat. The prognosis for PDC is generally poor, with a five-year survival rate of only about 9%. Treatment options may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. However, because PDC is often not detected until it has advanced, treatment is frequently focused on palliative care to relieve symptoms and improve quality of life.
Tumor-infiltrating lymphocytes (TILs) are a type of immune cell that have migrated from the bloodstream into a tumor. They are primarily composed of T cells, B cells, and natural killer (NK) cells. TILs can be found in various types of solid tumors, and their presence and composition have been shown to correlate with patient prognosis and response to certain therapies.
TILs play a crucial role in the immune response against cancer, as they are able to recognize and kill cancer cells. They can also release cytokines and chemokines that attract other immune cells to the tumor site, enhancing the anti-tumor immune response. However, tumors can develop mechanisms to evade or suppress the immune response, including the suppression of TILs.
TILs have emerged as a promising target for cancer immunotherapy, with adoptive cell transfer (ACT) being one of the most widely studied approaches. In ACT, TILs are isolated from a patient's tumor, expanded in the laboratory, and then reinfused back into the patient to enhance their anti-tumor immune response. This approach has shown promising results in clinical trials for several types of cancer, including melanoma and cervical cancer.
Estrogen receptors (ERs) are a type of nuclear receptor protein that are expressed in various tissues and cells throughout the body. They play a critical role in the regulation of gene expression and cellular responses to the hormone estrogen. There are two main subtypes of ERs, ERα and ERβ, which have distinct molecular structures, expression patterns, and functions.
ERs function as transcription factors that bind to specific DNA sequences called estrogen response elements (EREs) in the promoter regions of target genes. When estrogen binds to the ER, it causes a conformational change in the receptor that allows it to recruit co-activator proteins and initiate transcription of the target gene. This process can lead to a variety of cellular responses, including changes in cell growth, differentiation, and metabolism.
Estrogen receptors are involved in a wide range of physiological processes, including the development and maintenance of female reproductive tissues, bone homeostasis, cardiovascular function, and cognitive function. They have also been implicated in various pathological conditions, such as breast cancer, endometrial cancer, and osteoporosis. As a result, ERs are an important target for therapeutic interventions in these diseases.
Liver cirrhosis is a chronic, progressive disease characterized by the replacement of normal liver tissue with scarred (fibrotic) tissue, leading to loss of function. The scarring is caused by long-term damage from various sources such as hepatitis, alcohol abuse, nonalcoholic fatty liver disease, and other causes. As the disease advances, it can lead to complications like portal hypertension, fluid accumulation in the abdomen (ascites), impaired brain function (hepatic encephalopathy), and increased risk of liver cancer. It is generally irreversible, but early detection and treatment of underlying causes may help slow down its progression.
Taxoids are a class of naturally occurring compounds that are derived from the bark of the Pacific yew tree (Taxus brevifolia) and other species of the genus Taxus. They are known for their antineoplastic (cancer-fighting) properties and have been used in chemotherapy to treat various types of cancer, including ovarian, breast, and lung cancer.
The most well-known taxoid is paclitaxel (also known by the brand name Taxol), which was first discovered in the 1960s and has since become a widely used cancer drug. Paclitaxel works by stabilizing microtubules, which are important components of the cell's skeleton, and preventing them from disassembling. This disrupts the normal function of the cell's mitotic spindle, leading to cell cycle arrest and ultimately apoptosis (programmed cell death).
Other taxoids that have been developed for clinical use include docetaxel (Taxotere), which is a semi-synthetic analogue of paclitaxel, and cabazitaxel (Jevtana), which is a second-generation taxoid. These drugs have similar mechanisms of action to paclitaxel but may have different pharmacokinetic properties or be effective against cancer cells that have developed resistance to other taxoids.
While taxoids have been successful in treating certain types of cancer, they can also cause significant side effects, including neutropenia (low white blood cell count), anemia (low red blood cell count), and peripheral neuropathy (nerve damage). As with all chemotherapy drugs, the use of taxoids must be carefully balanced against their potential benefits and risks.
Melanoma is defined as a type of cancer that develops from the pigment-containing cells known as melanocytes. It typically occurs in the skin but can rarely occur in other parts of the body, including the eyes and internal organs. Melanoma is characterized by the uncontrolled growth and multiplication of melanocytes, which can form malignant tumors that invade and destroy surrounding tissue.
Melanoma is often caused by exposure to ultraviolet (UV) radiation from the sun or tanning beds, but it can also occur in areas of the body not exposed to the sun. It is more likely to develop in people with fair skin, light hair, and blue or green eyes, but it can affect anyone, regardless of their skin type.
Melanoma can be treated effectively if detected early, but if left untreated, it can spread to other parts of the body and become life-threatening. Treatment options for melanoma include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, depending on the stage and location of the cancer. Regular skin examinations and self-checks are recommended to detect any changes or abnormalities in moles or other pigmented lesions that may indicate melanoma.
Adrenal cortex neoplasms refer to abnormal growths (tumors) in the adrenal gland's outer layer, known as the adrenal cortex. These neoplasms can be benign or malignant (cancerous). Benign tumors are called adrenal adenomas, while cancerous tumors are called adrenocortical carcinomas.
Adrenal cortex neoplasms can produce various hormones, leading to different clinical presentations. For instance, they may cause Cushing's syndrome (characterized by excessive cortisol production), Conn's syndrome (caused by aldosterone excess), or virilization (due to androgen excess). Some tumors may not produce any hormones and are discovered incidentally during imaging studies for unrelated conditions.
The diagnosis of adrenal cortex neoplasms typically involves a combination of imaging techniques, such as CT or MRI scans, and hormonal assessments to determine if the tumor is functional or non-functional. In some cases, a biopsy may be necessary to confirm the diagnosis and differentiate between benign and malignant tumors. Treatment options depend on the type, size, location, and hormonal activity of the neoplasm and may include surgical excision, radiation therapy, chemotherapy, or a combination of these approaches.
Urothelium is the specialized type of epithelial tissue that lines the urinary tract, including the renal pelvis, ureters, bladder, and urethra. It is a type of transitional epithelium that can change its shape and size depending on the degree of distension or stretching of the organs it lines.
The main function of urothelium is to provide a barrier against urine, which contains various waste products and potential irritants, while also allowing the exchange of ions and water. The urothelial cells are joined together by tight junctions that prevent the passage of substances through the paracellular space, and they also have the ability to transport ions and water through their cell membranes.
In addition to its barrier function, urothelium is also involved in sensory and immune functions. It contains specialized nerve endings that can detect mechanical and chemical stimuli, such as stretch or irritation, and it expresses various antimicrobial peptides and other defense mechanisms that help protect the urinary tract from infection.
Overall, urothelium plays a critical role in maintaining the health and function of the urinary tract, and its dysfunction has been implicated in various urinary tract disorders, such as interstitial cystitis/bladder pain syndrome and bladder cancer.
Neoplastic stem cells, also known as cancer stem cells (CSCs), are a subpopulation of cells within a tumor that are capable of self-renewal and generating the heterogeneous lineages of cells that comprise the tumor. These cells are believed to be responsible for the initiation, maintenance, and progression of cancer, as well as its recurrence and resistance to therapy.
CSCs share some similarities with normal stem cells, such as their ability to divide asymmetrically and give rise to differentiated progeny. However, they also have distinct characteristics that distinguish them from their normal counterparts, including aberrant gene expression, altered signaling pathways, and increased resistance to apoptosis (programmed cell death).
The existence of CSCs has important implications for cancer diagnosis, treatment, and prevention. Targeting these cells specifically may be necessary to achieve durable remissions and prevent relapse, as they are thought to survive conventional therapies that target the bulk of the tumor. Further research is needed to better understand the biology of CSCs and develop effective strategies for their elimination.
Nucleic acid hybridization is a process in molecular biology where two single-stranded nucleic acids (DNA, RNA) with complementary sequences pair together to form a double-stranded molecule through hydrogen bonding. The strands can be from the same type of nucleic acid or different types (i.e., DNA-RNA or DNA-cDNA). This process is commonly used in various laboratory techniques, such as Southern blotting, Northern blotting, polymerase chain reaction (PCR), and microarray analysis, to detect, isolate, and analyze specific nucleic acid sequences. The hybridization temperature and conditions are critical to ensure the specificity of the interaction between the two strands.
In medical terms, the mouth is officially referred to as the oral cavity. It is the first part of the digestive tract and includes several structures: the lips, vestibule (the space enclosed by the lips and teeth), teeth, gingiva (gums), hard and soft palate, tongue, floor of the mouth, and salivary glands. The mouth is responsible for several functions including speaking, swallowing, breathing, and eating, as it is the initial point of ingestion where food is broken down through mechanical and chemical processes, beginning the digestive process.
Mohs surgery, also known as Mohs micrographic surgery, is a precise surgical technique used to treat common types of skin cancer. It's primarily used for basal cell carcinomas and squamous cell carcinomas that have recurred, are large, aggressive, or in critical areas where preservation of healthy tissue is important, such as the face.
The procedure involves removing the visible tumor along with a thin layer of surrounding tissue. This layer is then processed and examined under a microscope while the patient waits. If cancer cells are found in the margin of the removed tissue, another layer of tissue is taken from that specific area and examined. This process continues until no cancer cells are found in the margins, ensuring complete removal of the tumor while minimizing the removal of healthy tissue.
The main advantage of Mohs surgery is its ability to accurately assess the depth and extent of the cancer, leading to high cure rates and improved cosmetic outcomes. However, it's a specialized procedure that requires extensive training and should be performed by a fellowship-trained Mohs surgeon.
Sebaceous gland neoplasms are abnormal growths or tumors that develop in the sebaceous glands, which are small oil-producing glands found in the skin. These glands are responsible for producing sebum, a natural oil that helps keep the skin and hair moisturized. Sebaceous gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign sebaceous gland neoplasms include:
* Seborrheic keratosis: These are common, harmless growths that appear as rough, scaly patches on the skin. They can be tan, brown, or black in color and vary in size from small to large.
* Sebaceous adenoma: This is a benign tumor that arises from the sebaceous glands. It typically appears as a small, yellowish bump on the skin.
Malignant sebaceous gland neoplasms include:
* Sebaceous carcinoma: This is a rare but aggressive form of skin cancer that arises from the sebaceous glands. It often appears as a hard, painless nodule on the eyelid or other areas of the face and can spread to other parts of the body if left untreated.
* Basal cell carcinoma: While not exclusively a sebaceous gland neoplasm, basal cell carcinomas can sometimes arise from the sebaceous glands. These are slow-growing but invasive skin cancers that typically appear as pearly or flesh-colored bumps on the skin.
It is important to have any new or changing growths on the skin evaluated by a healthcare professional to determine whether they are benign or malignant and to develop an appropriate treatment plan if necessary.
Human chromosome pair 17 consists of two rod-shaped structures present in the nucleus of each human cell. Each chromosome is made up of DNA tightly coiled around histone proteins, forming a complex called chromatin. Chromosomes carry genetic information in the form of genes, which are segments of DNA that contain instructions for the development and function of an organism.
Human cells typically have 23 pairs of chromosomes, for a total of 46 chromosomes. Pair 17 is one of the autosomal pairs, meaning it is not a sex chromosome (X or Y). Chromosome 17 is a medium-sized chromosome and contains an estimated 800 million base pairs of DNA. It contains approximately 1,500 genes that provide instructions for making proteins and regulating various cellular processes.
Chromosome 17 is associated with several genetic disorders, including inherited cancer syndromes such as Li-Fraumeni syndrome and hereditary nonpolyposis colorectal cancer (HNPCC). Mutations in genes located on chromosome 17 can increase the risk of developing various types of cancer, including breast, ovarian, colon, and pancreatic cancer.
Gene deletion is a type of mutation where a segment of DNA, containing one or more genes, is permanently lost or removed from a chromosome. This can occur due to various genetic mechanisms such as homologous recombination, non-homologous end joining, or other types of genomic rearrangements.
The deletion of a gene can have varying effects on the organism, depending on the function of the deleted gene and its importance for normal physiological processes. If the deleted gene is essential for survival, the deletion may result in embryonic lethality or developmental abnormalities. However, if the gene is non-essential or has redundant functions, the deletion may not have any noticeable effects on the organism's phenotype.
Gene deletions can also be used as a tool in genetic research to study the function of specific genes and their role in various biological processes. For example, researchers may use gene deletion techniques to create genetically modified animal models to investigate the impact of gene deletion on disease progression or development.
DNA methylation is a process by which methyl groups (-CH3) are added to the cytosine ring of DNA molecules, often at the 5' position of cytospine phosphate-deoxyguanosine (CpG) dinucleotides. This modification is catalyzed by DNA methyltransferase enzymes and results in the formation of 5-methylcytosine.
DNA methylation plays a crucial role in the regulation of gene expression, genomic imprinting, X chromosome inactivation, and suppression of transposable elements. Abnormal DNA methylation patterns have been associated with various diseases, including cancer, where tumor suppressor genes are often silenced by promoter methylation.
In summary, DNA methylation is a fundamental epigenetic modification that influences gene expression and genome stability, and its dysregulation has important implications for human health and disease.
Phosphorylation is the process of adding a phosphate group (a molecule consisting of one phosphorus atom and four oxygen atoms) to a protein or other organic molecule, which is usually done by enzymes called kinases. This post-translational modification can change the function, localization, or activity of the target molecule, playing a crucial role in various cellular processes such as signal transduction, metabolism, and regulation of gene expression. Phosphorylation is reversible, and the removal of the phosphate group is facilitated by enzymes called phosphatases.
Photosensitivity disorders refer to conditions that cause an abnormal reaction to sunlight or artificial light. This reaction can take the form of various skin changes, such as rashes, inflammation, or pigmentation, and in some cases, it can also lead to systemic symptoms like fatigue, fever, or joint pain.
The two main types of photosensitivity disorders are:
1. Phototoxic reactions: These occur when a substance (such as certain medications, chemicals, or plants) absorbs light energy and transfers it to skin cells, causing damage and inflammation. The reaction typically appears within 24 hours of exposure to the light source and can resemble a sunburn.
2. Photoallergic reactions: These occur when the immune system responds to the combination of light and a particular substance, leading to an allergic response. The reaction may not appear until several days after initial exposure and can cause redness, itching, and blistering.
It is important for individuals with photosensitivity disorders to avoid excessive sun exposure, wear protective clothing, and use broad-spectrum sunscreens with a high SPF rating to minimize the risk of phototoxic or photoallergic reactions.
Ear neoplasms refer to abnormal growths or tumors that occur in the ear. These growths can be benign (non-cancerous) or malignant (cancerous) and can affect any part of the ear, including the outer ear, middle ear, inner ear, and the ear canal.
Benign ear neoplasms are typically slow-growing and do not spread to other parts of the body. Examples include exostoses, osteomas, and ceruminous adenomas. These types of growths are usually removed surgically for cosmetic reasons or if they cause discomfort or hearing problems.
Malignant ear neoplasms, on the other hand, can be aggressive and may spread to other parts of the body. Examples include squamous cell carcinoma, basal cell carcinoma, and adenoid cystic carcinoma. These types of tumors often require more extensive treatment, such as surgery, radiation therapy, and chemotherapy.
It is important to note that any new growth or change in the ear should be evaluated by a healthcare professional to determine the nature of the growth and develop an appropriate treatment plan.
Cell adhesion refers to the binding of cells to extracellular matrices or to other cells, a process that is fundamental to the development, function, and maintenance of multicellular organisms. Cell adhesion is mediated by various cell surface receptors, such as integrins, cadherins, and immunoglobulin-like cell adhesion molecules (Ig-CAMs), which interact with specific ligands in the extracellular environment. These interactions lead to the formation of specialized junctions, such as tight junctions, adherens junctions, and desmosomes, that help to maintain tissue architecture and regulate various cellular processes, including proliferation, differentiation, migration, and survival. Disruptions in cell adhesion can contribute to a variety of diseases, including cancer, inflammation, and degenerative disorders.
Medical Definition:
Matrix metalloproteinase 9 (MMP-9), also known as gelatinase B or 92 kDa type IV collagenase, is a member of the matrix metalloproteinase family. These enzymes are involved in degrading and remodeling the extracellular matrix (ECM) components, playing crucial roles in various physiological and pathological processes such as wound healing, tissue repair, and tumor metastasis.
MMP-9 is secreted as an inactive zymogen and activated upon removal of its propeptide domain. It can degrade several ECM proteins, including type IV collagen, elastin, fibronectin, and gelatin. MMP-9 has been implicated in numerous diseases, such as cancer, rheumatoid arthritis, neurological disorders, and cardiovascular diseases. Its expression is regulated at the transcriptional, translational, and post-translational levels, and its activity can be controlled by endogenous inhibitors called tissue inhibitors of metalloproteinases (TIMPs).
Iodine radioisotopes are radioactive isotopes of the element iodine, which decays and emits radiation in the form of gamma rays. Some commonly used iodine radioisotopes include I-123, I-125, I-131. These radioisotopes have various medical applications such as in diagnostic imaging, therapy for thyroid disorders, and cancer treatment.
For example, I-131 is commonly used to treat hyperthyroidism and differentiated thyroid cancer due to its ability to destroy thyroid tissue. On the other hand, I-123 is often used in nuclear medicine scans of the thyroid gland because it emits gamma rays that can be detected by a gamma camera, allowing for detailed images of the gland's structure and function.
It is important to note that handling and administering radioisotopes require specialized training and safety precautions due to their radiation-emitting properties.
Skin diseases, also known as dermatological conditions, refer to any medical condition that affects the skin, which is the largest organ of the human body. These diseases can affect the skin's function, appearance, or overall health. They can be caused by various factors, including genetics, infections, allergies, environmental factors, and aging.
Skin diseases can present in many different forms, such as rashes, blisters, sores, discolorations, growths, or changes in texture. Some common examples of skin diseases include acne, eczema, psoriasis, dermatitis, fungal infections, viral infections, bacterial infections, and skin cancer.
The symptoms and severity of skin diseases can vary widely depending on the specific condition and individual factors. Some skin diseases are mild and can be treated with over-the-counter medications or topical creams, while others may require more intensive treatments such as prescription medications, light therapy, or even surgery.
It is important to seek medical attention if you experience any unusual or persistent changes in your skin, as some skin diseases can be serious or indicative of other underlying health conditions. A dermatologist is a medical doctor who specializes in the diagnosis and treatment of skin diseases.
Bile duct neoplasms, also known as cholangiocarcinomas, refer to a group of malignancies that arise from the bile ducts. These are the tubes that carry bile from the liver to the gallbladder and small intestine. Bile duct neoplasms can be further classified based on their location as intrahepatic (within the liver), perihilar (at the junction of the left and right hepatic ducts), or distal (in the common bile duct).
These tumors are relatively rare, but their incidence has been increasing in recent years. They can cause a variety of symptoms, including jaundice, abdominal pain, weight loss, and fever. The diagnosis of bile duct neoplasms typically involves imaging studies such as CT or MRI scans, as well as blood tests to assess liver function. In some cases, a biopsy may be necessary to confirm the diagnosis.
Treatment options for bile duct neoplasms depend on several factors, including the location and stage of the tumor, as well as the patient's overall health. Surgical resection is the preferred treatment for early-stage tumors, while chemotherapy and radiation therapy may be used in more advanced cases. For patients who are not candidates for surgery, palliative treatments such as stenting or bypass procedures may be recommended to relieve symptoms and improve quality of life.
A "Giant Cell Carcinoma" is a type of cancer that originates from epithelial cells and is characterized by the presence of large, abnormal cells called giant cells. These giant cells are formed by the fusion of several individual cells, resulting in a single, large cell with multiple nuclei. Giant cell carcinomas can occur in various organs, including the lungs, esophagus, and thyroid gland.
Giant cell carcinoma of the lung is a rare and aggressive form of lung cancer that typically affects smokers. It is characterized by the presence of large, bizarre cells with multiple nuclei, as well as a high degree of cellular pleomorphism (variation in size and shape of cells). This type of lung cancer tends to grow and spread quickly, making it difficult to treat.
Giant cell carcinoma of the esophagus is also a rare and aggressive form of cancer that affects the esophagus. It is characterized by the presence of large, abnormal cells with multiple nuclei, as well as a high degree of cellular pleomorphism. This type of esophageal cancer tends to grow and spread quickly, making it difficult to treat.
Giant cell carcinoma of the thyroid gland is an extremely rare form of thyroid cancer that affects the thyroid gland. It is characterized by the presence of large, abnormal cells with multiple nuclei, as well as a high degree of cellular pleomorphism. This type of thyroid cancer tends to grow and spread quickly, making it difficult to treat.
Overall, giant cell carcinomas are aggressive forms of cancer that can occur in various organs. They are characterized by the presence of large, abnormal cells with multiple nuclei, as well as a high degree of cellular pleomorphism. Due to their aggressive nature and tendency to grow and spread quickly, giant cell carcinomas can be difficult to treat.
Common bile duct neoplasms refer to abnormal growths that can occur in the common bile duct, which is a tube that carries bile from the liver and gallbladder into the small intestine. These growths can be benign or malignant (cancerous).
Benign neoplasms of the common bile duct include papillomas, adenomas, and leiomyomas. Malignant neoplasms are typically adenocarcinomas, which arise from the glandular cells lining the duct. Other types of malignancies that can affect the common bile duct include cholangiocarcinoma, gallbladder carcinoma, and metastatic cancer from other sites.
Symptoms of common bile duct neoplasms may include jaundice (yellowing of the skin and eyes), abdominal pain, dark urine, and light-colored stools. Diagnosis may involve imaging tests such as CT scans or MRCP (magnetic resonance cholangiopancreatography) and biopsy to confirm the type of neoplasm. Treatment options depend on the type and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Urologic neoplasms refer to abnormal growths or tumors in the urinary system, which includes the kidneys, ureters, bladder, prostate, and urethra. These growths can be benign (non-cancerous) or malignant (cancerous). Common types of urologic neoplasms include renal cell carcinoma, transitional cell carcinoma, bladder cancer, prostate cancer, and testicular cancer. It is important to note that early detection and treatment can significantly improve outcomes for patients with urologic neoplasms.
The eyebrows are a set of hairs that grow above the eyes on the forehead. They are an important feature of human facial anatomy, and play several roles in non-verbal communication and self-expression. Eyebrows help to prevent sweat and other moisture from dripping into the eyes, and also serve as a protective barrier against dirt, dust, and other foreign particles that might otherwise irritate or damage the eyes.
In addition, eyebrows play an important role in human social interaction and communication. They can convey a range of emotions and facial expressions, such as surprise, anger, fear, happiness, and sadness. Eyebrows can also help to frame the eyes and enhance their appearance, making them an important aspect of personal grooming and beauty.
The eyebrows are made up of several components, including hair follicles, sebaceous glands, and muscles that control their movement. The hairs themselves are composed of a protein called keratin, which also makes up the hair on the head, as well as nails and skin. The color and thickness of eyebrow hair can vary widely from person to person, and may be influenced by factors such as age, genetics, and hormonal changes.
In medical terms, changes in the appearance or condition of the eyebrows can sometimes be a sign of underlying health issues. For example, thinning or loss of eyebrows can be associated with conditions such as alopecia, thyroid disorders, or nutritional deficiencies. Changes in eyebrow shape or position can also be a symptom of certain neurological conditions, such as Bell's palsy or stroke. As such, any significant changes in the appearance or condition of the eyebrows should be evaluated by a healthcare professional to rule out any underlying medical causes.
"Areca" is the term used to refer to the Areca catechu plant, which is also known as the betel nut palm. The areca nut, which is the seed of the fruit produced by this plant, is commonly chewed with betel leaf for its mild stimulant effects. It contains a number of alkaloids, including arecoline, which has psychoactive properties. Chewing areca nut is a popular habit in many parts of Asia and the Pacific Islands, despite evidence that it can have negative health effects, such as increasing the risk of oral cancer.
Vimentin is a type III intermediate filament protein that is expressed in various cell types, including mesenchymal cells, endothelial cells, and hematopoietic cells. It plays a crucial role in maintaining cell structure and integrity by forming part of the cytoskeleton. Vimentin is also involved in various cellular processes such as cell division, motility, and intracellular transport.
In addition to its structural functions, vimentin has been identified as a marker for epithelial-mesenchymal transition (EMT), a process that occurs during embryonic development and cancer metastasis. During EMT, epithelial cells lose their polarity and cell-cell adhesion properties and acquire mesenchymal characteristics, including increased migratory capacity and invasiveness. Vimentin expression is upregulated during EMT, making it a potential target for therapeutic intervention in cancer.
In diagnostic pathology, vimentin immunostaining is used to identify mesenchymal cells and to distinguish them from epithelial cells. It can also be used to diagnose certain types of sarcomas and carcinomas that express vimentin.
"Frozen sections" is a medical term that refers to the process of quickly preparing and examining a small piece of tissue during surgery. This procedure is typically performed by a pathologist in order to provide immediate diagnostic information to the surgeon, who can then make informed decisions about the course of the operation.
To create a frozen section, the surgical team first removes a small sample of tissue from the patient's body. This sample is then quickly frozen, typically using a special machine that can freeze the tissue in just a few seconds. Once the tissue is frozen, it can be cut into thin slices and stained with dyes to help highlight its cellular structures.
The stained slides are then examined under a microscope by a pathologist, who looks for any abnormalities or signs of disease. The results of this examination are typically available within 10-30 minutes, allowing the surgeon to make real-time decisions about whether to remove more tissue, change the surgical approach, or take other actions based on the findings.
Frozen sections are often used in cancer surgery to help ensure that all of the cancerous tissue has been removed, and to guide decisions about whether additional treatments such as radiation therapy or chemotherapy are necessary. They can also be used in other types of surgeries to help diagnose conditions and make treatment decisions during the procedure.
Mitomycin is an antineoplastic antibiotic derived from Streptomyces caespitosus. It is primarily used in cancer chemotherapy, particularly in the treatment of various carcinomas including gastrointestinal tract malignancies and breast cancer. Mitomycin works by forming cross-links in DNA, thereby inhibiting its replication and transcription, which ultimately leads to cell death.
In addition to its systemic use, mitomycin is also used topically in ophthalmology for the treatment of certain eye conditions such as glaucoma and various ocular surface disorders. The topical application of mitomycin can help reduce scarring and fibrosis by inhibiting the proliferation of fibroblasts.
It's important to note that mitomycin has a narrow therapeutic index, meaning there is only a small range between an effective dose and a toxic one. Therefore, its use should be closely monitored to minimize side effects, which can include myelosuppression, mucositis, alopecia, and potential secondary malignancies.
Oncogenes are genes that have the potential to cause cancer. They can do this by promoting cell growth and division (cellular proliferation), preventing cell death (apoptosis), or enabling cells to invade surrounding tissue and spread to other parts of the body (metastasis). Oncogenes can be formed when normal genes, called proto-oncogenes, are mutated or altered in some way. This can happen as a result of exposure to certain chemicals or radiation, or through inherited genetic mutations. When activated, oncogenes can contribute to the development of cancer by causing cells to divide and grow in an uncontrolled manner.
Tumor-associated carbohydrate antigens (TACAs) are a type of tumor antigen that are expressed on the surface of cancer cells. These antigens are abnormal forms of carbohydrates, also known as glycans, which are attached to proteins and lipids on the cell surface.
TACAs are often overexpressed or expressed in a different form on cancer cells compared to normal cells. This makes them attractive targets for cancer immunotherapy because they can be recognized by the immune system as foreign and elicit an immune response. Some examples of TACAs include gangliosides, fucosylated glycans, and sialylated glycans.
Tumor-associated carbohydrate antigens have been studied as potential targets for cancer vaccines, antibody therapies, and other immunotherapeutic approaches. However, their use as targets for cancer therapy is still in the early stages of research and development.
'Antibodies, Neoplasm' is a medical term that refers to abnormal antibodies produced by neoplastic cells, which are cells that have undergone uncontrolled division and form a tumor or malignancy. These antibodies can be produced in large quantities and may have altered structures or functions compared to normal antibodies.
Neoplastic antibodies can arise from various types of malignancies, including leukemias, lymphomas, and multiple myeloma. In some cases, these abnormal antibodies can interfere with the normal functioning of the immune system and contribute to the progression of the disease.
In addition, neoplastic antibodies can also be used as tumor markers for diagnostic purposes. For example, certain types of monoclonal gammopathy, such as multiple myeloma, are characterized by the overproduction of a single type of immunoglobulin, which can be detected in the blood or urine and used to monitor the disease.
Overall, 'Antibodies, Neoplasm' is a term that encompasses a wide range of abnormal antibodies produced by neoplastic cells, which can have significant implications for both the diagnosis and treatment of malignancies.
A chromosome deletion is a type of genetic abnormality that occurs when a portion of a chromosome is missing or deleted. Chromosomes are thread-like structures located in the nucleus of cells that contain our genetic material, which is organized into genes.
Chromosome deletions can occur spontaneously during the formation of reproductive cells (eggs or sperm) or can be inherited from a parent. They can affect any chromosome and can vary in size, from a small segment to a large portion of the chromosome.
The severity of the symptoms associated with a chromosome deletion depends on the size and location of the deleted segment. In some cases, the deletion may be so small that it does not cause any noticeable symptoms. However, larger deletions can lead to developmental delays, intellectual disabilities, physical abnormalities, and various medical conditions.
Chromosome deletions are typically detected through a genetic test called karyotyping, which involves analyzing the number and structure of an individual's chromosomes. Other more precise tests, such as fluorescence in situ hybridization (FISH) or chromosomal microarray analysis (CMA), may also be used to confirm the diagnosis and identify the specific location and size of the deletion.
The Fluorescent Antibody Technique (FAT) is a type of immunofluorescence assay used in laboratory medicine and pathology for the detection and localization of specific antigens or antibodies in tissues, cells, or microorganisms. In this technique, a fluorescein-labeled antibody is used to selectively bind to the target antigen or antibody, forming an immune complex. When excited by light of a specific wavelength, the fluorescein label emits light at a longer wavelength, typically visualized as green fluorescence under a fluorescence microscope.
The FAT is widely used in diagnostic microbiology for the identification and characterization of various bacteria, viruses, fungi, and parasites. It has also been applied in the diagnosis of autoimmune diseases and certain cancers by detecting specific antibodies or antigens in patient samples. The main advantage of FAT is its high sensitivity and specificity, allowing for accurate detection and differentiation of various pathogens and disease markers. However, it requires specialized equipment and trained personnel to perform and interpret the results.
Thymus neoplasms are abnormal growths in the thymus gland that result from uncontrolled cell division. The term "neoplasm" refers to any new and abnormal growth of tissue, also known as a tumor. Thymus neoplasms can be benign or malignant (cancerous).
Malignant thymus neoplasms are called thymomas or thymic carcinomas. Thymomas are the most common type and tend to grow slowly, invading nearby tissues and organs. They can also spread (metastasize) to other parts of the body. Thymic carcinomas are rarer and more aggressive, growing and spreading more quickly than thymomas.
Symptoms of thymus neoplasms may include coughing, chest pain, difficulty breathing, or swelling in the neck or upper chest. Treatment options for thymus neoplasms depend on the type, size, location, and stage of the tumor, as well as the patient's overall health. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Orbital evisceration is not a medical condition itself, but rather a surgical procedure. In ophthalmology (the branch of medicine dealing with the eye), orbital evisceration refers to the removal of the contents of the eye, leaving the scleral shell, extraocular muscles, and orbital fat intact. This is often performed for therapeutic or cosmetic reasons, such as in cases of painful blind eyes or severely disfigured eyes. The empty eye socket is then often fitted with a prosthetic eye to restore a more natural appearance.
Multimodal imaging is a medical term that refers to the combination of two or more imaging techniques to obtain complementary information about the structure, function, and/or physiology of tissues, organs, or organ systems. This approach allows for a more comprehensive assessment of normal and abnormal processes in the body than can be achieved with any single imaging modality alone.
Commonly used imaging modalities in multimodal imaging include computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), single-photon emission computed tomography (SPECT), ultrasound, and optical imaging techniques. Each modality provides unique information that can be integrated to improve diagnostic accuracy, guide treatment planning, and monitor response to therapy.
For example, a patient with a suspected brain tumor may undergo both MRI and PET scans. The MRI provides detailed anatomical information about the size, shape, and location of the tumor, while the PET scan shows metabolic activity within the tumor, which can help distinguish between benign and malignant lesions.
Multimodal imaging is also used in research settings to study various physiological processes, such as blood flow, oxygenation, and neurotransmission, in both health and disease.
An Enzyme-Linked Immunosorbent Assay (ELISA) is a type of analytical biochemistry assay used to detect and quantify the presence of a substance, typically a protein or peptide, in a liquid sample. It takes its name from the enzyme-linked antibodies used in the assay.
In an ELISA, the sample is added to a well containing a surface that has been treated to capture the target substance. If the target substance is present in the sample, it will bind to the surface. Next, an enzyme-linked antibody specific to the target substance is added. This antibody will bind to the captured target substance if it is present. After washing away any unbound material, a substrate for the enzyme is added. If the enzyme is present due to its linkage to the antibody, it will catalyze a reaction that produces a detectable signal, such as a color change or fluorescence. The intensity of this signal is proportional to the amount of target substance present in the sample, allowing for quantification.
ELISAs are widely used in research and clinical settings to detect and measure various substances, including hormones, viruses, and bacteria. They offer high sensitivity, specificity, and reproducibility, making them a reliable choice for many applications.
Ureteral neoplasms refer to abnormal growths or tumors in the ureters, which are the tubes that carry urine from the kidneys to the bladder. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Benign ureteral neoplasms are rare and usually do not pose a significant health risk, although they may need to be removed if they cause obstructions or other complications.
Malignant ureteral neoplasms, on the other hand, are more serious and can spread to other parts of the body. The most common type of malignant ureteral neoplasm is transitional cell carcinoma (TCC), which arises from the cells that line the inside of the ureters. Other types of malignant ureteral neoplasms include squamous cell carcinoma, adenocarcinoma, and sarcoma.
Symptoms of ureteral neoplasms may include hematuria (blood in the urine), flank pain, weight loss, and fatigue. Diagnosis typically involves imaging tests such as CT scans or MRIs, as well as urine cytology and biopsy to confirm the presence of cancer cells. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Cell cycle proteins are a group of regulatory proteins that control the progression of the cell cycle, which is the series of events that take place in a eukaryotic cell leading to its division and duplication. These proteins can be classified into several categories based on their functions during different stages of the cell cycle.
The major groups of cell cycle proteins include:
1. Cyclin-dependent kinases (CDKs): CDKs are serine/threonine protein kinases that regulate key transitions in the cell cycle. They require binding to a regulatory subunit called cyclin to become active. Different CDK-cyclin complexes are activated at different stages of the cell cycle.
2. Cyclins: Cyclins are a family of regulatory proteins that bind and activate CDKs. Their levels fluctuate throughout the cell cycle, with specific cyclins expressed during particular phases. For example, cyclin D is important for the G1 to S phase transition, while cyclin B is required for the G2 to M phase transition.
3. CDK inhibitors (CKIs): CKIs are regulatory proteins that bind to and inhibit CDKs, thereby preventing their activation. CKIs can be divided into two main families: the INK4 family and the Cip/Kip family. INK4 family members specifically inhibit CDK4 and CDK6, while Cip/Kip family members inhibit a broader range of CDKs.
4. Anaphase-promoting complex/cyclosome (APC/C): APC/C is an E3 ubiquitin ligase that targets specific proteins for degradation by the 26S proteasome. During the cell cycle, APC/C regulates the metaphase to anaphase transition and the exit from mitosis by targeting securin and cyclin B for degradation.
5. Other regulatory proteins: Several other proteins play crucial roles in regulating the cell cycle, such as p53, a transcription factor that responds to DNA damage and arrests the cell cycle, and the polo-like kinases (PLKs), which are involved in various aspects of mitosis.
Overall, cell cycle proteins work together to ensure the proper progression of the cell cycle, maintain genomic stability, and prevent uncontrolled cell growth, which can lead to cancer.
Single Nucleotide Polymorphism (SNP) is a type of genetic variation that occurs when a single nucleotide (A, T, C, or G) in the DNA sequence is altered. This alteration must occur in at least 1% of the population to be considered a SNP. These variations can help explain why some people are more susceptible to certain diseases than others and can also influence how an individual responds to certain medications. SNPs can serve as biological markers, helping scientists locate genes that are associated with disease. They can also provide information about an individual's ancestry and ethnic background.
Carcinogenesis is the process by which normal cells are transformed into cancer cells. It is a complex, multi-step process that involves various genetic and epigenetic alterations in the cell's DNA. These changes can be caused by exposure to carcinogens, such as chemicals, radiation, or viruses, and can lead to the uncontrolled growth and division of cells, resulting in the formation of a tumor.
The process of carcinogenesis typically involves several stages: initiation, promotion, and progression. Initiation is the initial damage to the cell's DNA, which can be caused by exposure to a carcinogen. Promotion is the clonal expansion of the initiated cells due to the stimulation of cell growth and division. Progression is the accumulation of additional genetic changes that lead to the development of invasive cancer.
It is important to note that not all exposures to carcinogens will result in cancer, as the process of carcinogenesis depends on a variety of factors, including the dose and duration of exposure, the individual's genetic susceptibility, and the presence of co-carcinogens or protective factors.
Protein kinase inhibitors (PKIs) are a class of drugs that work by interfering with the function of protein kinases. Protein kinases are enzymes that play a crucial role in many cellular processes by adding a phosphate group to specific proteins, thereby modifying their activity, localization, or interaction with other molecules. This process of adding a phosphate group is known as phosphorylation and is a key mechanism for regulating various cellular functions, including signal transduction, metabolism, and cell division.
In some diseases, such as cancer, protein kinases can become overactive or mutated, leading to uncontrolled cell growth and division. Protein kinase inhibitors are designed to block the activity of these dysregulated kinases, thereby preventing or slowing down the progression of the disease. These drugs can be highly specific, targeting individual protein kinases or families of kinases, making them valuable tools for targeted therapy in cancer and other diseases.
Protein kinase inhibitors can work in various ways to block the activity of protein kinases. Some bind directly to the active site of the enzyme, preventing it from interacting with its substrates. Others bind to allosteric sites, changing the conformation of the enzyme and making it inactive. Still, others target upstream regulators of protein kinases or interfere with their ability to form functional complexes.
Examples of protein kinase inhibitors include imatinib (Gleevec), which targets the BCR-ABL kinase in chronic myeloid leukemia, and gefitinib (Iressa), which inhibits the EGFR kinase in non-small cell lung cancer. These drugs have shown significant clinical benefits in treating these diseases and have become important components of modern cancer therapy.
A pleomorphic adenoma is a type of benign (non-cancerous) tumor that typically develops in the salivary glands, although they can also occur in other areas such as the nasopharynx and skin. "Pleomorphic" refers to the diverse appearance of the cells within the tumor, which can vary in size, shape, and arrangement.
Pleomorphic adenomas are composed of a mixture of epithelial and mesenchymal cells, which can form glandular structures, squamous (scale-like) cells, and areas that resemble cartilage or bone. These tumors tend to grow slowly and usually do not spread to other parts of the body.
While pleomorphic adenomas are generally not dangerous, they can cause problems if they become large enough to press on surrounding tissues or structures. In some cases, these tumors may also undergo malignant transformation, leading to a cancerous growth known as carcinoma ex pleomorphic adenoma. Surgical removal is the standard treatment for pleomorphic adenomas, and the prognosis is generally good with proper management.
'Staining and labeling' are techniques commonly used in pathology, histology, cytology, and molecular biology to highlight or identify specific components or structures within tissues, cells, or molecules. These methods enable researchers and medical professionals to visualize and analyze the distribution, localization, and interaction of biological entities, contributing to a better understanding of diseases, cellular processes, and potential therapeutic targets.
Medical definitions for 'staining' and 'labeling' are as follows:
1. Staining: A process that involves applying dyes or stains to tissues, cells, or molecules to enhance their contrast and reveal specific structures or components. Stains can be categorized into basic stains (which highlight acidic structures) and acidic stains (which highlight basic structures). Common staining techniques include Hematoxylin and Eosin (H&E), which differentiates cell nuclei from the surrounding cytoplasm and extracellular matrix; special stains, such as PAS (Periodic Acid-Schiff) for carbohydrates or Masson's trichrome for collagen fibers; and immunostains, which use antibodies to target specific proteins.
2. Labeling: A process that involves attaching a detectable marker or tag to a molecule of interest, allowing its identification, quantification, or tracking within a biological system. Labels can be direct, where the marker is directly conjugated to the targeting molecule, or indirect, where an intermediate linker molecule is used to attach the label to the target. Common labeling techniques include fluorescent labels (such as FITC, TRITC, or Alexa Fluor), enzymatic labels (such as horseradish peroxidase or alkaline phosphatase), and radioactive labels (such as ³²P or ¹⁴C). Labeling is often used in conjunction with staining techniques to enhance the specificity and sensitivity of detection.
Together, staining and labeling provide valuable tools for medical research, diagnostics, and therapeutic development, offering insights into cellular and molecular processes that underlie health and disease.
A Tumor Stem Cell Assay is not a widely accepted or standardized medical definition. However, in the context of cancer research, a tumor stem cell assay generally refers to an experimental procedure used to identify and isolate cancer stem cells (also known as tumor-initiating cells) from a tumor sample.
Cancer stem cells are a subpopulation of cells within a tumor that are believed to be responsible for driving tumor growth, metastasis, and resistance to therapy. They have the ability to self-renew and differentiate into various cell types within the tumor, making them a promising target for cancer therapies.
A tumor stem cell assay typically involves isolating cells from a tumor sample and subjecting them to various tests to identify those with stem cell-like properties. These tests may include assessing their ability to form tumors in animal models or their expression of specific surface markers associated with cancer stem cells. The goal of the assay is to provide researchers with a better understanding of the biology of cancer stem cells and to develop new therapies that target them specifically.
Hepatectomy is a surgical procedure that involves the removal of part or all of the liver. This procedure can be performed for various reasons, such as removing cancerous or non-cancerous tumors, treating liver trauma, or donating a portion of the liver to another person in need of a transplant (live donor hepatectomy). The extent of the hepatectomy depends on the medical condition and overall health of the patient. It is a complex procedure that requires significant expertise and experience from the surgical team due to the liver's unique anatomy, blood supply, and regenerative capabilities.
Mammary neoplasms in animals refer to abnormal growths or tumors that occur in the mammary glands. These tumors can be benign (non-cancerous) or malignant (cancerous). Benign tumors are slow growing and rarely spread to other parts of the body, while malignant tumors are aggressive, can invade surrounding tissues, and may metastasize to distant organs.
Mammary neoplasms are more common in female animals, particularly those that have not been spayed. The risk factors for developing mammary neoplasms include age, reproductive status, hormonal influences, and genetic predisposition. Certain breeds of dogs, such as poodles, cocker spaniels, and dachshunds, are more prone to developing mammary tumors.
Clinical signs of mammary neoplasms may include the presence of a firm, discrete mass in the mammary gland, changes in the overlying skin such as ulceration or discoloration, and evidence of pain or discomfort in the affected area. Diagnosis is typically made through a combination of physical examination, imaging studies (such as mammography or ultrasound), and biopsy with histopathological evaluation.
Treatment options for mammary neoplasms depend on the type, size, location, and stage of the tumor, as well as the animal's overall health status. Surgical removal is often the primary treatment modality, and may be curative for benign tumors or early-stage malignant tumors. Radiation therapy and chemotherapy may also be used in cases where the tumor has spread to other parts of the body. Regular veterinary check-ups and monitoring are essential to ensure early detection and treatment of any recurrence or new mammary neoplasms.
Carboplatin is a chemotherapeutic agent used to treat various types of cancers, including ovarian, lung, and head and neck cancer. It is a platinum-containing compound that works by forming crosslinks in DNA, which leads to the death of rapidly dividing cells, such as cancer cells. Carboplatin is often used in combination with other chemotherapy drugs and is administered intravenously.
The medical definition of Carboplatin is:
"A platinum-containing antineoplastic agent that forms crosslinks with DNA, inducing cell cycle arrest and apoptosis. It is used to treat a variety of cancers, including ovarian, lung, and head and neck cancer."
There is no medical definition for "dog diseases" as it is too broad a term. However, dogs can suffer from various health conditions and illnesses that are specific to their species or similar to those found in humans. Some common categories of dog diseases include:
1. Infectious Diseases: These are caused by viruses, bacteria, fungi, or parasites. Examples include distemper, parvovirus, kennel cough, Lyme disease, and heartworms.
2. Hereditary/Genetic Disorders: Some dogs may inherit certain genetic disorders from their parents. Examples include hip dysplasia, elbow dysplasia, progressive retinal atrophy (PRA), and degenerative myelopathy.
3. Age-Related Diseases: As dogs age, they become more susceptible to various health issues. Common age-related diseases in dogs include arthritis, dental disease, cancer, and cognitive dysfunction syndrome (CDS).
4. Nutritional Disorders: Malnutrition or improper feeding can lead to various health problems in dogs. Examples include obesity, malnutrition, and vitamin deficiencies.
5. Environmental Diseases: These are caused by exposure to environmental factors such as toxins, allergens, or extreme temperatures. Examples include heatstroke, frostbite, and toxicities from ingesting harmful substances.
6. Neurological Disorders: Dogs can suffer from various neurological conditions that affect their nervous system. Examples include epilepsy, intervertebral disc disease (IVDD), and vestibular disease.
7. Behavioral Disorders: Some dogs may develop behavioral issues due to various factors such as anxiety, fear, or aggression. Examples include separation anxiety, noise phobias, and resource guarding.
It's important to note that regular veterinary care, proper nutrition, exercise, and preventative measures can help reduce the risk of many dog diseases.
Colposcopy is a medical procedure in which a colposcope, which is a type of microscope, is used to examine the cervix, vagina, and vulva for signs of disease or abnormalities. The colposcope allows the healthcare provider to see these areas in greater detail than is possible with the naked eye. During the procedure, the provider may take a small sample of tissue (biopsy) for further examination under a microscope.
Colposcopy is often used to investigate abnormal Pap test results or to follow up on women who have been diagnosed with certain types of cervical dysplasia (abnormal cell growth). It can also be used to diagnose and monitor other conditions, such as genital warts, inflammation, or cancer.
It is important to note that colposcopy is a diagnostic procedure and not a treatment. If abnormalities are found during the exam, additional procedures may be necessary to remove or treat them.
Nephrectomy is a surgical procedure in which all or part of a kidney is removed. It may be performed due to various reasons such as severe kidney damage, kidney cancer, or living donor transplantation. The type of nephrectomy depends on the reason for the surgery - a simple nephrectomy involves removing only the affected portion of the kidney, while a radical nephrectomy includes removal of the whole kidney along with its surrounding tissues like the adrenal gland and lymph nodes.
Carrier proteins, also known as transport proteins, are a type of protein that facilitates the movement of molecules across cell membranes. They are responsible for the selective and active transport of ions, sugars, amino acids, and other molecules from one side of the membrane to the other, against their concentration gradient. This process requires energy, usually in the form of ATP (adenosine triphosphate).
Carrier proteins have a specific binding site for the molecule they transport, and undergo conformational changes upon binding, which allows them to move the molecule across the membrane. Once the molecule has been transported, the carrier protein returns to its original conformation, ready to bind and transport another molecule.
Carrier proteins play a crucial role in maintaining the balance of ions and other molecules inside and outside of cells, and are essential for many physiological processes, including nerve impulse transmission, muscle contraction, and nutrient uptake.
Keratin-14 is a type of keratin protein that is specifically expressed in the suprabasal layers of stratified epithelia, including the epidermis. It is a component of the intermediate filament cytoskeleton and plays an important role in maintaining the structural integrity and stability of epithelial cells. Mutations in the gene encoding keratin-14 have been associated with several genetic skin disorders, such as epidermolysis bullosa simplex and white sponge nevus.
Animal disease models are specialized animals, typically rodents such as mice or rats, that have been genetically engineered or exposed to certain conditions to develop symptoms and physiological changes similar to those seen in human diseases. These models are used in medical research to study the pathophysiology of diseases, identify potential therapeutic targets, test drug efficacy and safety, and understand disease mechanisms.
The genetic modifications can include knockout or knock-in mutations, transgenic expression of specific genes, or RNA interference techniques. The animals may also be exposed to environmental factors such as chemicals, radiation, or infectious agents to induce the disease state.
Examples of animal disease models include:
1. Mouse models of cancer: Genetically engineered mice that develop various types of tumors, allowing researchers to study cancer initiation, progression, and metastasis.
2. Alzheimer's disease models: Transgenic mice expressing mutant human genes associated with Alzheimer's disease, which exhibit amyloid plaque formation and cognitive decline.
3. Diabetes models: Obese and diabetic mouse strains like the NOD (non-obese diabetic) or db/db mice, used to study the development of type 1 and type 2 diabetes, respectively.
4. Cardiovascular disease models: Atherosclerosis-prone mice, such as ApoE-deficient or LDLR-deficient mice, that develop plaque buildup in their arteries when fed a high-fat diet.
5. Inflammatory bowel disease models: Mice with genetic mutations affecting intestinal barrier function and immune response, such as IL-10 knockout or SAMP1/YitFc mice, which develop colitis.
Animal disease models are essential tools in preclinical research, but it is important to recognize their limitations. Differences between species can affect the translatability of results from animal studies to human patients. Therefore, researchers must carefully consider the choice of model and interpret findings cautiously when applying them to human diseases.
Telomerase is an enzyme that adds repetitive DNA sequences (telomeres) to the ends of chromosomes, which are lost during each cell division due to the incomplete replication of the ends of linear chromosomes. Telomerase is not actively present in most somatic cells, but it is highly expressed in germ cells and stem cells, allowing them to divide indefinitely. However, in many types of cancer cells, telomerase is abnormally activated, which leads to the maintenance or lengthening of telomeres, contributing to their unlimited replicative potential and tumorigenesis.
Immunoblotting, also known as western blotting, is a laboratory technique used in molecular biology and immunogenetics to detect and quantify specific proteins in a complex mixture. This technique combines the electrophoretic separation of proteins by gel electrophoresis with their detection using antibodies that recognize specific epitopes (protein fragments) on the target protein.
The process involves several steps: first, the protein sample is separated based on size through sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE). Next, the separated proteins are transferred onto a nitrocellulose or polyvinylidene fluoride (PVDF) membrane using an electric field. The membrane is then blocked with a blocking agent to prevent non-specific binding of antibodies.
After blocking, the membrane is incubated with a primary antibody that specifically recognizes the target protein. Following this, the membrane is washed to remove unbound primary antibodies and then incubated with a secondary antibody conjugated to an enzyme such as horseradish peroxidase (HRP) or alkaline phosphatase (AP). The enzyme catalyzes a colorimetric or chemiluminescent reaction that allows for the detection of the target protein.
Immunoblotting is widely used in research and clinical settings to study protein expression, post-translational modifications, protein-protein interactions, and disease biomarkers. It provides high specificity and sensitivity, making it a valuable tool for identifying and quantifying proteins in various biological samples.
Matrix metalloproteinase 2 (MMP-2), also known as gelatinase A, is an enzyme that belongs to the matrix metalloproteinase family. MMPs are involved in the breakdown of extracellular matrix components, and MMP-2 is responsible for degrading type IV collagen, a major component of the basement membrane. This enzyme plays a crucial role in various physiological processes, including tissue remodeling, wound healing, and angiogenesis. However, its dysregulation has been implicated in several pathological conditions, such as cancer, arthritis, and cardiovascular diseases. MMP-2 is synthesized as an inactive proenzyme and requires activation by other proteases or chemical modifications before it can exert its proteolytic activity.
PTEN phosphohydrolase, also known as PTEN protein or phosphatase and tensin homolog deleted on chromosome ten, is a tumor suppressor protein that plays a crucial role in regulating cell growth and division. It works by dephosphorylating (removing a phosphate group from) the lipid second messenger PIP3, which is involved in signaling pathways that promote cell proliferation and survival. By negatively regulating these pathways, PTEN helps to prevent uncontrolled cell growth and tumor formation. Mutations in the PTEN gene can lead to a variety of cancer types, including breast, prostate, and endometrial cancer.
Northern blotting is a laboratory technique used in molecular biology to detect and analyze specific RNA molecules (such as mRNA) in a mixture of total RNA extracted from cells or tissues. This technique is called "Northern" blotting because it is analogous to the Southern blotting method, which is used for DNA detection.
The Northern blotting procedure involves several steps:
1. Electrophoresis: The total RNA mixture is first separated based on size by running it through an agarose gel using electrical current. This separates the RNA molecules according to their length, with smaller RNA fragments migrating faster than larger ones.
2. Transfer: After electrophoresis, the RNA bands are denatured (made single-stranded) and transferred from the gel onto a nitrocellulose or nylon membrane using a technique called capillary transfer or vacuum blotting. This step ensures that the order and relative positions of the RNA fragments are preserved on the membrane, similar to how they appear in the gel.
3. Cross-linking: The RNA is then chemically cross-linked to the membrane using UV light or heat treatment, which helps to immobilize the RNA onto the membrane and prevent it from washing off during subsequent steps.
4. Prehybridization: Before adding the labeled probe, the membrane is prehybridized in a solution containing blocking agents (such as salmon sperm DNA or yeast tRNA) to minimize non-specific binding of the probe to the membrane.
5. Hybridization: A labeled nucleic acid probe, specific to the RNA of interest, is added to the prehybridization solution and allowed to hybridize (form base pairs) with its complementary RNA sequence on the membrane. The probe can be either a DNA or an RNA molecule, and it is typically labeled with a radioactive isotope (such as ³²P) or a non-radioactive label (such as digoxigenin).
6. Washing: After hybridization, the membrane is washed to remove unbound probe and reduce background noise. The washing conditions (temperature, salt concentration, and detergent concentration) are optimized based on the stringency required for specific hybridization.
7. Detection: The presence of the labeled probe is then detected using an appropriate method, depending on the type of label used. For radioactive probes, this typically involves exposing the membrane to X-ray film or a phosphorimager screen and analyzing the resulting image. For non-radioactive probes, detection can be performed using colorimetric, chemiluminescent, or fluorescent methods.
8. Data analysis: The intensity of the signal is quantified and compared to controls (such as housekeeping genes) to determine the relative expression level of the RNA of interest. This information can be used for various purposes, such as identifying differentially expressed genes in response to a specific treatment or comparing gene expression levels across different samples or conditions.
An oxyphilic adenoma is a type of benign tumor that develops in the endocrine glands, specifically in the parathyroid gland. This type of adenoma is characterized by the presence of cells called oxyphils, which have an abundance of mitochondria and appear pink on histological examination due to their high oxidative enzyme activity. Oxyphilic adenomas are a common cause of primary hyperparathyroidism, a condition in which the parathyroid glands produce too much parathyroid hormone (PTH), leading to an imbalance of calcium and phosphorus metabolism. Symptoms of primary hyperparathyroidism may include fatigue, weakness, bone pain, kidney stones, and psychological disturbances. Treatment typically involves surgical removal of the affected parathyroid gland.
Bone neoplasms are abnormal growths or tumors that develop in the bone. They can be benign (non-cancerous) or malignant (cancerous). Benign bone neoplasms do not spread to other parts of the body and are rarely a threat to life, although they may cause problems if they grow large enough to press on surrounding tissues or cause fractures. Malignant bone neoplasms, on the other hand, can invade and destroy nearby tissue and may spread (metastasize) to other parts of the body.
There are many different types of bone neoplasms, including:
1. Osteochondroma - a benign tumor that develops from cartilage and bone
2. Enchondroma - a benign tumor that forms in the cartilage that lines the inside of the bones
3. Chondrosarcoma - a malignant tumor that develops from cartilage
4. Osteosarcoma - a malignant tumor that develops from bone cells
5. Ewing sarcoma - a malignant tumor that develops in the bones or soft tissues around the bones
6. Giant cell tumor of bone - a benign or occasionally malignant tumor that develops from bone tissue
7. Fibrosarcoma - a malignant tumor that develops from fibrous tissue in the bone
The symptoms of bone neoplasms vary depending on the type, size, and location of the tumor. They may include pain, swelling, stiffness, fractures, or limited mobility. Treatment options depend on the type and stage of the tumor but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
Photochemotherapy is a medical treatment that combines the use of drugs and light to treat various skin conditions. The most common type of photochemotherapy is PUVA (Psoralen + UVA), where the patient takes a photosensitizing medication called psoralen, followed by exposure to ultraviolet A (UVA) light.
The psoralen makes the skin more sensitive to the UVA light, which helps to reduce inflammation and suppress the overactive immune response that contributes to many skin conditions. This therapy is often used to treat severe cases of psoriasis, eczema, and mycosis fungoides (a type of cutaneous T-cell lymphoma). It's important to note that photochemotherapy can increase the risk of skin cancer and cataracts, so it should only be administered under the close supervision of a healthcare professional.
Cell adhesion molecules (CAMs) are a type of protein found on the surface of cells that mediate the attachment or adhesion of cells to either other cells or to the extracellular matrix (ECM), which is the network of proteins and carbohydrates that provides structural and biochemical support to surrounding cells.
CAMs play crucial roles in various biological processes, including tissue development, differentiation, repair, and maintenance of tissue architecture and function. They are also involved in cell signaling, migration, and regulation of the immune response.
There are several types of CAMs, classified based on their structure and function, such as immunoglobulin-like CAMs (IgCAMs), cadherins, integrins, and selectins. Dysregulation of CAMs has been implicated in various diseases, including cancer, inflammation, and neurological disorders.
The odds ratio (OR) is a statistical measure used in epidemiology and research to estimate the association between an exposure and an outcome. It represents the odds that an event will occur in one group versus the odds that it will occur in another group, assuming that all other factors are held constant.
In medical research, the odds ratio is often used to quantify the strength of the relationship between a risk factor (exposure) and a disease outcome. An OR of 1 indicates no association between the exposure and the outcome, while an OR greater than 1 suggests that there is a positive association between the two. Conversely, an OR less than 1 implies a negative association.
It's important to note that the odds ratio is not the same as the relative risk (RR), which compares the incidence rates of an outcome in two groups. While the OR can approximate the RR when the outcome is rare, they are not interchangeable and can lead to different conclusions about the association between an exposure and an outcome.
In the context of medicine, risk is the probability or likelihood of an adverse health effect or the occurrence of a negative event related to treatment or exposure to certain hazards. It is usually expressed as a ratio or percentage and can be influenced by various factors such as age, gender, lifestyle, genetics, and environmental conditions. Risk assessment involves identifying, quantifying, and prioritizing risks to make informed decisions about prevention, mitigation, or treatment strategies.
Inverted papilloma is a specific type of benign (non-cancerous) growth that occurs in the mucosal lining of the nasal cavity or paranasal sinuses. It is also known as schneiderian papilloma or cylindrical cell papilloma.
This condition is characterized by the growth of finger-like projections (papillae) that invert or grow inward into the underlying tissue, hence the name "inverted." The lesions are usually composed of an outer layer of stratified squamous epithelium and an inner core of connective tissue.
Inverted papillomas can cause symptoms such as nasal congestion, nosebleeds, sinus pressure, and difficulty breathing through the nose. In some cases, they may also lead to more serious complications, including recurrence after removal and a small risk of malignant transformation into squamous cell carcinoma.
It is important to note that while inverted papillomas are benign, they can still cause significant problems due to their location and tendency to recur. Therefore, they typically require surgical removal and close follow-up with an otolaryngologist (ear, nose, and throat specialist).
Scirrhous adenocarcinoma is a subtype of adenocarcinoma, which is a type of cancer that begins in glandular cells. "Scirrhous" describes a particularly aggressive and invasive form of the disease, characterized by the rapid growth and spread of cancerous cells, as well as the formation of dense, fibrous scar tissue. This scar tissue can cause the affected organs or tissues to become hardened and thickened, which can lead to organ dysfunction and other serious complications.
Scirrhous adenocarcinoma most commonly affects the stomach and breasts, but it can also occur in other areas of the body, such as the colon, rectum, and lungs. Treatment typically involves a combination of surgery, chemotherapy, and radiation therapy, with the goal of removing as much of the cancerous tissue as possible and preventing the spread of the disease to other parts of the body.
It's important to note that medical terminology can be complex and nuanced, and the specific definition and clinical implications of terms like "scirrhous adenocarcinoma" may vary depending on the context in which they are used. If you have any questions or concerns about a particular medical term or diagnosis, it's always best to consult with a qualified healthcare professional for accurate information and guidance.
Nonparametric statistics is a branch of statistics that does not rely on assumptions about the distribution of variables in the population from which the sample is drawn. In contrast to parametric methods, nonparametric techniques make fewer assumptions about the data and are therefore more flexible in their application. Nonparametric tests are often used when the data do not meet the assumptions required for parametric tests, such as normality or equal variances.
Nonparametric statistical methods include tests such as the Wilcoxon rank-sum test (also known as the Mann-Whitney U test) for comparing two independent groups, the Wilcoxon signed-rank test for comparing two related groups, and the Kruskal-Wallis test for comparing more than two independent groups. These tests use the ranks of the data rather than the actual values to make comparisons, which allows them to be used with ordinal or continuous data that do not meet the assumptions of parametric tests.
Overall, nonparametric statistics provide a useful set of tools for analyzing data in situations where the assumptions of parametric methods are not met, and can help researchers draw valid conclusions from their data even when the data are not normally distributed or have other characteristics that violate the assumptions of parametric tests.
Retinoblastoma Protein (pRb or RB1) is a tumor suppressor protein that plays a critical role in regulating the cell cycle and preventing uncontrolled cell growth. It is encoded by the RB1 gene, located on chromosome 13. The retinoblastoma protein functions as a regulatory checkpoint in the cell cycle, preventing cells from progressing into the S phase (DNA synthesis phase) until certain conditions are met.
When pRb is in its active state, it binds to and inhibits the activity of E2F transcription factors, which promote the expression of genes required for DNA replication and cell cycle progression. Phosphorylation of pRb by cyclin-dependent kinases (CDKs) leads to the release of E2F factors, allowing them to activate their target genes and drive the cell into S phase.
Mutations in the RB1 gene can result in the production of a nonfunctional or reduced amount of pRb protein, leading to uncontrolled cell growth and an increased risk of developing retinoblastoma, a rare form of eye cancer, as well as other types of tumors.
In medical terms, the tongue is a muscular organ in the oral cavity that plays a crucial role in various functions such as taste, swallowing, and speech. It's covered with a mucous membrane and contains papillae, which are tiny projections that contain taste buds to help us perceive different tastes - sweet, salty, sour, and bitter. The tongue also assists in the initial process of digestion by moving food around in the mouth for chewing and mixing with saliva. Additionally, it helps in forming words and speaking clearly by shaping the sounds produced in the mouth.
Gastrointestinal (GI) neoplasms refer to abnormal growths in the gastrointestinal tract, which can be benign or malignant. The gastrointestinal tract includes the mouth, esophagus, stomach, small intestine, large intestine, rectum, and anus.
Benign neoplasms are non-cancerous growths that do not invade nearby tissues or spread to other parts of the body. They can sometimes be removed completely and may not cause any further health problems.
Malignant neoplasms, on the other hand, are cancerous growths that can invade nearby tissues and organs and spread to other parts of the body through the bloodstream or lymphatic system. These types of neoplasms can be life-threatening if not diagnosed and treated promptly.
GI neoplasms can cause various symptoms, including abdominal pain, bloating, changes in bowel habits, nausea, vomiting, weight loss, and anemia. The specific symptoms may depend on the location and size of the neoplasm.
There are many types of GI neoplasms, including adenocarcinomas, gastrointestinal stromal tumors (GISTs), lymphomas, and neuroendocrine tumors. The diagnosis of GI neoplasms typically involves a combination of medical history, physical examination, imaging studies, and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or immunotherapy.
I'm sorry for any confusion, but "Carcinoma, Ehrlich Tumor" is not a recognized medical term or a valid medical definition. The term "Ehrlich tumor" is sometimes used to refer to a type of transplantable tumor that was first developed by the German physician Paul Ehrlich in the early 20th century for cancer research purposes. However, it's important to note that this type of tumor is not a naturally occurring cancer and is typically used only in laboratory experiments.
Carcinoma, on the other hand, is a medical term that refers to a type of cancer that starts in cells that line the inner or outer surfaces of organs. Carcinomas can develop in various parts of the body, including the lungs, breasts, colon, and skin.
If you have any specific questions about cancer or a particular medical condition, I would be happy to try to help answer them for you.
"Hairless mice" is a term used to describe strains of laboratory mice that lack a functional fur coat. This condition is also known as "nude mice." The hairlessness in these mice is caused by a genetic mutation that results in the absence or underdevelopment of hair follicles and a weakened immune system.
Hairless mice are often used in scientific research because their impaired immune systems make them more susceptible to certain diseases, allowing researchers to study the progression and treatment of those conditions in a controlled environment. Additionally, their lack of fur makes it easier to observe and monitor skin conditions and wounds. These mice are also used as models for human diseases such as cancer, AIDS, and autoimmune disorders.
A dose-response relationship in radiation refers to the correlation between the amount of radiation exposure (dose) and the biological response or adverse health effects observed in exposed individuals. As the level of radiation dose increases, the severity and frequency of the adverse health effects also tend to increase. This relationship is crucial in understanding the risks associated with various levels of radiation exposure and helps inform radiation protection standards and guidelines.
The effects of ionizing radiation can be categorized into two types: deterministic and stochastic. Deterministic effects have a threshold dose below which no effect is observed, and above this threshold, the severity of the effect increases with higher doses. Examples include radiation-induced cataracts or radiation dermatitis. Stochastic effects, on the other hand, do not have a clear threshold and are based on probability; as the dose increases, so does the likelihood of the adverse health effect occurring, such as an increased risk of cancer.
Understanding the dose-response relationship in radiation exposure is essential for setting limits on occupational and public exposure to ionizing radiation, optimizing radiation protection practices, and developing effective medical countermeasures in case of radiation emergencies.
Protein-Serine-Threonine Kinases (PSTKs) are a type of protein kinase that catalyzes the transfer of a phosphate group from ATP to the hydroxyl side chains of serine or threonine residues on target proteins. This phosphorylation process plays a crucial role in various cellular signaling pathways, including regulation of metabolism, gene expression, cell cycle progression, and apoptosis. PSTKs are involved in many physiological and pathological processes, and their dysregulation has been implicated in several diseases, such as cancer, diabetes, and neurodegenerative disorders.
Papillary cystadenocarcinoma is a type of cancer that arises from the epithelial cells lining a cyst. It is called "papillary" because the tumor has finger-like projections called papillae, which are made up of fibrovascular cores covered by neoplastic cells.
Cystadenocarcinoma is a malignant tumor that has the potential to invade surrounding tissues and spread (metastasize) to other parts of the body. Papillary cystadenocarcinomas can occur in various organs, including the ovaries, pancreas, and lungs.
The symptoms of papillary cystadenocarcinoma depend on the location of the tumor. For example, an ovarian papillary cystadenocarcinoma may cause abdominal pain or bloating, while a lung papillary cystadenocarcinoma may cause coughing or shortness of breath.
The diagnosis of papillary cystadenocarcinoma typically involves imaging tests such as ultrasound, CT scan, or MRI, followed by a biopsy to confirm the presence of cancer cells. Treatment options include surgery to remove the tumor, chemotherapy, and radiation therapy. The prognosis for papillary cystadenocarcinoma depends on several factors, including the stage of the disease at diagnosis, the location of the tumor, and the patient's overall health.
Papillomavirus E7 proteins are small, viral regulatory proteins encoded by the E7 gene in papillomaviruses (HPVs). These proteins play a crucial role in the life cycle of HPVs and are associated with the development of various types of cancer, most notably cervical cancer.
The E7 protein functions as a transcriptional activator and can bind to and degrade the retinoblastoma protein (pRb), which is a tumor suppressor. By binding to and inactivating pRb, E7 promotes the expression of genes required for cell cycle progression, leading to uncontrolled cell growth and proliferation.
E7 proteins are also capable of inducing genetic alterations, such as chromosomal instability and DNA damage, which can contribute to the development of cancer. Additionally, E7 has been shown to inhibit apoptosis (programmed cell death) and promote angiogenesis (the formation of new blood vessels), further contributing to tumor growth and progression.
Overall, Papillomavirus E7 proteins are important oncogenic factors that play a central role in the development of HPV-associated cancers.
Genetic transcription is the process by which the information in a strand of DNA is used to create a complementary RNA molecule. This process is the first step in gene expression, where the genetic code in DNA is converted into a form that can be used to produce proteins or functional RNAs.
During transcription, an enzyme called RNA polymerase binds to the DNA template strand and reads the sequence of nucleotide bases. As it moves along the template, it adds complementary RNA nucleotides to the growing RNA chain, creating a single-stranded RNA molecule that is complementary to the DNA template strand. Once transcription is complete, the RNA molecule may undergo further processing before it can be translated into protein or perform its functional role in the cell.
Transcription can be either "constitutive" or "regulated." Constitutive transcription occurs at a relatively constant rate and produces essential proteins that are required for basic cellular functions. Regulated transcription, on the other hand, is subject to control by various intracellular and extracellular signals, allowing cells to respond to changing environmental conditions or developmental cues.
Antibiotics are a type of medication used to treat infections caused by bacteria. They work by either killing the bacteria or inhibiting their growth.
Antineoplastics, also known as chemotherapeutic agents, are a class of drugs used to treat cancer. These medications target and destroy rapidly dividing cells, such as cancer cells, although they can also affect other quickly dividing cells in the body, such as those in the hair follicles or digestive tract, which can lead to side effects.
Antibiotics and antineoplastics are two different classes of drugs with distinct mechanisms of action and uses. It is important to use them appropriately and under the guidance of a healthcare professional.
A hysterectomy is a surgical procedure that involves the removal of the uterus (womb). Depending on the specific medical condition and necessity, a hysterectomy may also include the removal of the ovaries, fallopian tubes, and surrounding tissues. There are different types of hysterectomies, including:
1. Total hysterectomy: The uterus and cervix are removed.
2. Supracervical (or subtotal) hysterectomy: Only the upper part of the uterus is removed, leaving the cervix intact.
3. Radical hysterectomy: This procedure involves removing the uterus, cervix, surrounding tissues, and the upper part of the vagina. It is typically performed in cases of cervical cancer.
4. Oophorectomy: The removal of one or both ovaries can be performed along with a hysterectomy depending on the patient's medical condition and age.
5. Salpingectomy: The removal of one or both fallopian tubes can also be performed along with a hysterectomy if needed.
The reasons for performing a hysterectomy may include but are not limited to: uterine fibroids, heavy menstrual bleeding, endometriosis, adenomyosis, pelvic prolapse, cervical or uterine cancer, and chronic pelvic pain. The choice of the type of hysterectomy depends on the patient's medical condition, age, and personal preferences.
The ampulla of Vater, also known as hepatopancreatic ampulla, is a dilated portion of the common bile duct where it joins the main pancreatic duct and empties into the second part of the duodenum. It serves as a conduit for both bile from the liver and digestive enzymes from the pancreas to reach the small intestine, facilitating the digestion and absorption of nutrients. The ampulla of Vater is surrounded by a muscular sphincter, the sphincter of Oddi, which controls the flow of these secretions into the duodenum.
A pneumonectomy is a surgical procedure in which an entire lung is removed. This type of surgery is typically performed as a treatment for certain types of lung cancer, although it may also be used to treat other conditions such as severe damage or infection in the lung that does not respond to other treatments. The surgery requires general anesthesia and can be quite complex, with potential risks including bleeding, infection, pneumonia, and air leaks. Recovery from a pneumonectomy can take several weeks, and patients may require ongoing rehabilitation to regain strength and mobility.
Neoplasms are abnormal growths of cells or tissues that serve no purpose and can be benign (non-cancerous) or malignant (cancerous). Glandular and epithelial neoplasms refer to specific types of tumors that originate from the glandular and epithelial tissues, respectively.
Glandular neoplasms arise from the glandular tissue, which is responsible for producing and secreting substances such as hormones, enzymes, or other fluids. These neoplasms can be further classified into adenomas (benign) and adenocarcinomas (malignant).
Epithelial neoplasms, on the other hand, develop from the epithelial tissue that lines the outer surfaces of organs and the inner surfaces of cavities. These neoplasms can also be benign or malignant and are classified as papillomas (benign) and carcinomas (malignant).
It is important to note that while both glandular and epithelial neoplasms can become cancerous, not all of them do. However, if they do, the malignant versions can invade surrounding tissues and spread to other parts of the body, making them potentially life-threatening.
Isoenzymes, also known as isoforms, are multiple forms of an enzyme that catalyze the same chemical reaction but differ in their amino acid sequence, structure, and/or kinetic properties. They are encoded by different genes or alternative splicing of the same gene. Isoenzymes can be found in various tissues and organs, and they play a crucial role in biological processes such as metabolism, detoxification, and cell signaling. Measurement of isoenzyme levels in body fluids (such as blood) can provide valuable diagnostic information for certain medical conditions, including tissue damage, inflammation, and various diseases.
'Alcohol drinking' refers to the consumption of alcoholic beverages, which contain ethanol (ethyl alcohol) as the active ingredient. Ethanol is a central nervous system depressant that can cause euphoria, disinhibition, and sedation when consumed in small to moderate amounts. However, excessive drinking can lead to alcohol intoxication, with symptoms ranging from slurred speech and impaired coordination to coma and death.
Alcohol is metabolized in the liver by enzymes such as alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH). The breakdown of ethanol produces acetaldehyde, a toxic compound that can cause damage to various organs in the body. Chronic alcohol drinking can lead to a range of health problems, including liver disease, pancreatitis, cardiovascular disease, neurological disorders, and increased risk of cancer.
Moderate drinking is generally defined as up to one drink per day for women and up to two drinks per day for men, where a standard drink contains about 14 grams (0.6 ounces) of pure alcohol. However, it's important to note that there are no safe levels of alcohol consumption, and any level of drinking carries some risk to health.
Membrane glycoproteins are proteins that contain oligosaccharide chains (glycans) covalently attached to their polypeptide backbone. They are integral components of biological membranes, spanning the lipid bilayer and playing crucial roles in various cellular processes.
The glycosylation of these proteins occurs in the endoplasmic reticulum (ER) and Golgi apparatus during protein folding and trafficking. The attached glycans can vary in structure, length, and composition, which contributes to the diversity of membrane glycoproteins.
Membrane glycoproteins can be classified into two main types based on their orientation within the lipid bilayer:
1. Type I (N-linked): These glycoproteins have a single transmembrane domain and an extracellular N-terminus, where the oligosaccharides are predominantly attached via asparagine residues (Asn-X-Ser/Thr sequon).
2. Type II (C-linked): These glycoproteins possess two transmembrane domains and an intracellular C-terminus, with the oligosaccharides linked to tryptophan residues via a mannose moiety.
Membrane glycoproteins are involved in various cellular functions, such as:
* Cell adhesion and recognition
* Receptor-mediated signal transduction
* Enzymatic catalysis
* Transport of molecules across membranes
* Cell-cell communication
* Immunological responses
Some examples of membrane glycoproteins include cell surface receptors (e.g., growth factor receptors, cytokine receptors), adhesion molecules (e.g., integrins, cadherins), and transporters (e.g., ion channels, ABC transporters).
Urethral neoplasms refer to abnormal growths or tumors in the urethra, which is the tube that carries urine from the bladder out of the body. These growths can be benign (non-cancerous) or malignant (cancerous).
Benign urethral neoplasms may include conditions such as urethral polyps or papillomas, which are usually not life-threatening and can often be removed with surgery.
Malignant urethral neoplasms, on the other hand, are cancerous tumors that can invade surrounding tissues and spread to other parts of the body. These include urethral carcinomas, which can be further classified into different types such as squamous cell carcinoma, transitional cell carcinoma, and adenocarcinoma, depending on the type of cells involved.
Urethral neoplasms are relatively rare, but when they do occur, they can cause a variety of symptoms such as difficulty urinating, blood in the urine, pain during urination or sexual intercourse, and discharge from the urethra. Treatment options depend on the type, location, and stage of the neoplasm, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
The Nucleolus Organizer Region (NOR) is a specific region within the chromosomes, primarily in the short arm of the acrocentric chromosomes (chromosomes 13, 14, 15, 21, and 22). It consists of clusters of repetitive DNA sequences that encode ribosomal RNA (rRNA) genes. During interphase, these regions form the nucleolus, a distinct structure within the nucleus where rRNA transcription, processing, and ribosome assembly occur. The number of NORs in an individual can vary, which has implications in certain genetic conditions and aging processes.
I'm sorry for any confusion, but "Japan" is not a medical term. Japan is the name of a country, officially known as Nippon-koku or Nihon-koku in Japanese, and is located in East Asia. It is an island nation in the Pacific Ocean with a population of about 126 million people.
If you have any medical questions or terms that you would like me to define, please let me know!
Protein-kinase B, also known as AKT, is a group of intracellular proteins that play a crucial role in various cellular processes such as glucose metabolism, apoptosis, cell proliferation, transcription, and cell migration. The AKT family includes three isoforms: AKT1, AKT2, and AKT3, which are encoded by the genes PKBalpha, PKBbeta, and PKBgamma, respectively.
Proto-oncogene proteins c-AKT refer to the normal, non-mutated forms of these proteins that are involved in the regulation of cell growth and survival under physiological conditions. However, when these genes are mutated or overexpressed, they can become oncogenes, leading to uncontrolled cell growth and cancer development.
Activation of c-AKT occurs through a signaling cascade that begins with the binding of extracellular ligands such as insulin-like growth factor 1 (IGF-1) or epidermal growth factor (EGF) to their respective receptors on the cell surface. This triggers a series of phosphorylation events that ultimately lead to the activation of c-AKT, which then phosphorylates downstream targets involved in various cellular processes.
In summary, proto-oncogene proteins c-AKT are normal intracellular proteins that play essential roles in regulating cell growth and survival under physiological conditions. However, their dysregulation can contribute to cancer development and progression.
Oral Submucous Fibrosis (OSF) is a chronic, progressive, and potentially disabling disease that affects the oral soft tissues. It is characterized by inflammation and fibrosis (excessive deposition of collagen) of the submucosal tissues, leading to stiffness and limitation of mouth opening, tongue movement, and occasionally swallowing or speaking difficulties. The condition primarily affects individuals with a history of areca nut (betel nut) chewing, although other factors such as smoking, alcohol consumption, and genetic predisposition may also contribute to its development. Symptoms can include burning sensation in the mouth, dryness, and pain during speaking, eating, or swallowing. In severe cases, OSF can lead to significant functional impairment and require surgical intervention.
A codon is a sequence of three adjacent nucleotides in DNA or RNA that specifies the insertion of a particular amino acid during protein synthesis, or signals the beginning or end of translation. In DNA, these triplets are read during transcription to produce a complementary mRNA molecule, which is then translated into a polypeptide chain during translation. There are 64 possible codons in the standard genetic code, with 61 encoding for specific amino acids and three serving as stop codons that signal the termination of protein synthesis.
High-energy radiotherapy, also known as external beam radiation therapy (EBRT), is a type of cancer treatment that uses high-energy radiation beams to destroy cancer cells and shrink tumors. The radiation beams are produced by a machine called a linear accelerator (LINAC) and are directed at the tumor site from outside the body. High-energy radiotherapy can be used to treat many different types of cancer, either alone or in combination with other treatments such as surgery or chemotherapy.
The high-energy radiation beams used in this type of radiotherapy are able to penetrate deep into the body and target large areas, making it an effective treatment for cancers that have spread or are too large to be removed surgically. The dose and duration of treatment will depend on the type and stage of cancer being treated, as well as the patient's overall health.
High-energy radiotherapy works by damaging the DNA of cancer cells, which prevents them from dividing and growing. This ultimately leads to the death of the cancer cells. While radiation therapy can also damage normal cells, they are generally better able to repair themselves compared to cancer cells. Therefore, the goal of high-energy radiotherapy is to deliver a high enough dose to destroy the cancer cells while minimizing harm to surrounding healthy tissue.
It's important to note that high-energy radiotherapy requires careful planning and delivery to ensure that the radiation beams are focused on the tumor site and avoid healthy tissues as much as possible. This is typically done using imaging techniques such as CT, MRI, or PET scans to create a treatment plan that maps out the exact location and shape of the tumor. The patient will then undergo a series of treatments, usually scheduled daily over several weeks.
Transforming Growth Factor-alpha (TGF-α) is a type of growth factor, specifically a peptide growth factor, that plays a role in cell growth, proliferation, and differentiation. It belongs to the epidermal growth factor (EGF) family of growth factors. TGF-α binds to the EGF receptor (EGFR) on the surface of cells and activates intracellular signaling pathways that promote cellular growth and division.
TGF-α is involved in various biological processes, including embryonic development, wound healing, and tissue repair. However, abnormal regulation of TGF-α has been implicated in several diseases, such as cancer. Overexpression or hyperactivation of TGF-α can contribute to uncontrolled cell growth and tumor progression by stimulating the proliferation of cancer cells and inhibiting their differentiation and apoptosis (programmed cell death).
TGF-α is produced by various cell types, including epithelial cells, fibroblasts, and immune cells. It can be secreted in a membrane-bound form (pro-TGF-α) or as a soluble protein after proteolytic cleavage.
A feasibility study is a preliminary investigation or analysis conducted to determine the viability of a proposed project, program, or product. In the medical field, feasibility studies are often conducted before implementing new treatments, procedures, equipment, or facilities. These studies help to assess the practicality and effectiveness of the proposed intervention, as well as its potential benefits and risks.
Feasibility studies in healthcare typically involve several steps:
1. Problem identification: Clearly define the problem that the proposed project, program, or product aims to address.
2. Objectives setting: Establish specific, measurable, achievable, relevant, and time-bound (SMART) objectives for the study.
3. Literature review: Conduct a thorough review of existing research and best practices related to the proposed intervention.
4. Methodology development: Design a methodology for data collection and analysis that will help answer the research questions and achieve the study's objectives.
5. Resource assessment: Evaluate the availability and adequacy of resources, including personnel, time, and finances, required to carry out the proposed intervention.
6. Risk assessment: Identify potential risks and challenges associated with the implementation of the proposed intervention and develop strategies to mitigate them.
7. Cost-benefit analysis: Estimate the costs and benefits of the proposed intervention, including direct and indirect costs, as well as short-term and long-term benefits.
8. Stakeholder engagement: Engage relevant stakeholders, such as patients, healthcare providers, administrators, and policymakers, to gather their input and support for the proposed intervention.
9. Decision-making: Based on the findings of the feasibility study, make an informed decision about whether or not to proceed with the proposed project, program, or product.
Feasibility studies are essential in healthcare as they help ensure that resources are allocated efficiently and effectively, and that interventions are evidence-based, safe, and beneficial for patients.
Drug synergism is a pharmacological concept that refers to the interaction between two or more drugs, where the combined effect of the drugs is greater than the sum of their individual effects. This means that when these drugs are administered together, they produce an enhanced therapeutic response compared to when they are given separately.
Drug synergism can occur through various mechanisms, such as:
1. Pharmacodynamic synergism - When two or more drugs interact with the same target site in the body and enhance each other's effects.
2. Pharmacokinetic synergism - When one drug affects the metabolism, absorption, distribution, or excretion of another drug, leading to an increased concentration of the second drug in the body and enhanced therapeutic effect.
3. Physiochemical synergism - When two drugs interact physically, such as when one drug enhances the solubility or permeability of another drug, leading to improved absorption and bioavailability.
It is important to note that while drug synergism can result in enhanced therapeutic effects, it can also increase the risk of adverse reactions and toxicity. Therefore, healthcare providers must carefully consider the potential benefits and risks when prescribing combinations of drugs with known or potential synergistic effects.
Mucins are high molecular weight, heavily glycosylated proteins that are the major components of mucus. They are produced and secreted by specialized epithelial cells in various organs, including the respiratory, gastrointestinal, and urogenital tracts, as well as the eyes and ears.
Mucins have a characteristic structure consisting of a protein backbone with numerous attached oligosaccharide side chains, which give them their gel-forming properties and provide a protective barrier against pathogens, environmental insults, and digestive enzymes. They also play important roles in lubrication, hydration, and cell signaling.
Mucins can be classified into two main groups based on their structure and function: secreted mucins and membrane-bound mucins. Secreted mucins are released from cells and form a physical barrier on the surface of mucosal tissues, while membrane-bound mucins are integrated into the cell membrane and participate in cell adhesion and signaling processes.
Abnormalities in mucin production or function have been implicated in various diseases, including chronic inflammation, cancer, and cystic fibrosis.
Lichen Planus, Oral is a relatively common inflammatory condition that affects the mucous membranes inside the mouth. It is characterized by the presence of white, lacy patches (called Wickham's striae), papules, or plaques on the oral mucosa, which can be uncomfortable or painful, especially when eating spicy, salty, or acidic foods. The condition can also cause soreness, redness, and ulceration in some cases.
The exact cause of oral lichen planus is not known, but it is believed to be related to an abnormal immune response in which the body's immune system attacks the cells in the oral mucosa. The condition can affect people of any age, but it is most commonly seen in middle-aged adults, and it affects women more often than men.
While there is no cure for oral lichen planus, treatment can help to manage symptoms and prevent complications. Topical corticosteroids are often used to reduce inflammation and relieve pain, while systemic medications may be prescribed in severe cases. It is important to avoid irritants such as tobacco, alcohol, and spicy foods, which can exacerbate symptoms. Regular dental check-ups are also recommended to monitor the condition and prevent any complications.
Urogenital neoplasms refer to abnormal growths or tumors that occur in the urinary and genital organs. These can include various types of cancer, such as bladder cancer, kidney cancer, prostate cancer, testicular cancer, cervical cancer, ovarian cancer, and others. Some urogenital neoplasms may be benign (non-cancerous), while others are malignant (cancerous) and can spread to other parts of the body.
The term "urogenital" refers to the combined urinary and genital systems in the human body. The urinary system includes the kidneys, ureters, bladder, and urethra, which are responsible for filtering waste from the blood and eliminating it as urine. The genital system includes the reproductive organs such as the ovaries, fallopian tubes, uterus, vagina, prostate gland, testicles, and penis.
Urogenital neoplasms can cause various symptoms depending on their location and size. Common symptoms include blood in urine, pain during urination, difficulty urinating, abnormal discharge, lumps or swelling in the genital area, and unexplained weight loss. If you experience any of these symptoms, it is important to consult a healthcare professional for further evaluation and treatment.
A Receiver Operating Characteristic (ROC) curve is a graphical representation used in medical decision-making and statistical analysis to illustrate the performance of a binary classifier system, such as a diagnostic test or a machine learning algorithm. It's a plot that shows the tradeoff between the true positive rate (sensitivity) and the false positive rate (1 - specificity) for different threshold settings.
The x-axis of an ROC curve represents the false positive rate (the proportion of negative cases incorrectly classified as positive), while the y-axis represents the true positive rate (the proportion of positive cases correctly classified as positive). Each point on the curve corresponds to a specific decision threshold, with higher points indicating better performance.
The area under the ROC curve (AUC) is a commonly used summary measure that reflects the overall performance of the classifier. An AUC value of 1 indicates perfect discrimination between positive and negative cases, while an AUC value of 0.5 suggests that the classifier performs no better than chance.
ROC curves are widely used in healthcare to evaluate diagnostic tests, predictive models, and screening tools for various medical conditions, helping clinicians make informed decisions about patient care based on the balance between sensitivity and specificity.
Genetic therapy, also known as gene therapy, is a medical intervention that involves the use of genetic material, such as DNA or RNA, to treat or prevent diseases. It works by introducing functional genes into cells to replace missing or faulty ones caused by genetic disorders or mutations. The introduced gene is incorporated into the recipient's genome, allowing for the production of a therapeutic protein that can help manage the disease symptoms or even cure the condition.
There are several approaches to genetic therapy, including:
1. Replacing a faulty gene with a healthy one
2. Inactivating or "silencing" a dysfunctional gene causing a disease
3. Introducing a new gene into the body to help fight off a disease, such as cancer
Genetic therapy holds great promise for treating various genetic disorders, including cystic fibrosis, muscular dystrophy, hemophilia, and certain types of cancer. However, it is still an evolving field with many challenges, such as efficient gene delivery, potential immune responses, and ensuring the safety and long-term effectiveness of the therapy.
Paraneoplastic syndromes refer to a group of rare disorders that are caused by an abnormal immune system response to a cancerous (malignant) tumor. These syndromes are characterized by symptoms or signs that do not result directly from the growth of the tumor itself, but rather from substances produced by the tumor or the body's immune system in response to the tumor.
Paraneoplastic syndromes can affect various organs and systems in the body, including the nervous system, endocrine system, skin, and joints. Examples of paraneoplastic syndromes include Lambert-Eaton myasthenic syndrome (LEMS), which affects nerve function and causes muscle weakness; cerebellar degeneration, which can cause difficulty with coordination and balance; and dermatomyositis, which is an inflammatory condition that affects the skin and muscles.
Paraneoplastic syndromes can occur in association with a variety of different types of cancer, including lung cancer, breast cancer, ovarian cancer, and lymphoma. Treatment typically involves addressing the underlying cancer, as well as managing the symptoms of the paraneoplastic syndrome.
Carcinogenicity tests are a type of toxicity test used to determine the potential of a chemical or physical agent to cause cancer. These tests are typically conducted on animals, such as rats or mice, and involve exposing the animals to the agent over a long period of time, often for the majority of their lifespan. The animals are then closely monitored for any signs of tumor development or other indicators of cancer.
The results of carcinogenicity tests can be used by regulatory agencies, such as the U.S. Environmental Protection Agency (EPA) and the Food and Drug Administration (FDA), to help determine safe exposure levels for chemicals and other agents. The tests are also used by industry to assess the potential health risks associated with their products and to develop safer alternatives.
It is important to note that carcinogenicity tests have limitations, including the use of animals, which may not always accurately predict the effects of a chemical on humans. Additionally, these tests can be time-consuming and expensive, which has led to the development of alternative test methods, such as in vitro (test tube) assays and computational models, that aim to provide more efficient and ethical alternatives for carcinogenicity testing.
NM23 nucleoside diphosphate kinases are a group of proteins that play a role in regulating cellular functions, including signal transduction, cell proliferation, and differentiation. They are named after the NM23 gene that encodes them, which was initially identified as a potential metastasis suppressor.
NM23 nucleoside diphosphate kinases have the ability to transfer phosphate groups between nucleoside diphosphates (NDPs) and nucleoside triphosphates (NTPs), thereby maintaining the balance of these molecules in cells. This enzymatic activity is important for various cellular processes, such as DNA replication, repair, and transcription.
There are several isoforms of NM23 nucleoside diphosphate kinases, including NM23-H1, NM23-H2, and NM23-H4, which differ in their tissue distribution and functions. While the role of NM23 as a metastasis suppressor has been debated, recent studies suggest that it may be involved in regulating cell motility and invasion through its effects on actin dynamics and microtubule organization.
Overall, NM23 nucleoside diphosphate kinases are important regulators of cellular homeostasis and have been implicated in various physiological and pathological processes, including cancer metastasis, inflammation, and neurodegenerative diseases.
Radiation injuries refer to the damages that occur to living tissues as a result of exposure to ionizing radiation. These injuries can be acute, occurring soon after exposure to high levels of radiation, or chronic, developing over a longer period after exposure to lower levels of radiation. The severity and type of injury depend on the dose and duration of exposure, as well as the specific tissues affected.
Acute radiation syndrome (ARS), also known as radiation sickness, is the most severe form of acute radiation injury. It can cause symptoms such as nausea, vomiting, diarrhea, fatigue, fever, and skin burns. In more severe cases, it can lead to neurological damage, hemorrhage, infection, and death.
Chronic radiation injuries, on the other hand, may not appear until months or even years after exposure. They can cause a range of symptoms, including fatigue, weakness, skin changes, cataracts, reduced fertility, and an increased risk of cancer.
Radiation injuries can be treated with supportive care, such as fluids and electrolytes replacement, antibiotics, wound care, and blood transfusions. In some cases, surgery may be necessary to remove damaged tissue or control bleeding. Prevention is the best approach to radiation injuries, which includes limiting exposure through proper protective measures and monitoring radiation levels in the environment.
Hep G2 cells are a type of human liver cancer cell line that were isolated from a well-differentiated hepatocellular carcinoma (HCC) in a patient with hepatitis C virus (HCV) infection. These cells have the ability to grow and divide indefinitely in culture, making them useful for research purposes. Hep G2 cells express many of the same markers and functions as normal human hepatocytes, including the ability to take up and process lipids and produce bile. They are often used in studies related to hepatitis viruses, liver metabolism, drug toxicity, and cancer biology. It is important to note that Hep G2 cells are tumorigenic and should be handled with care in a laboratory setting.
Transgenic mice are genetically modified rodents that have incorporated foreign DNA (exogenous DNA) into their own genome. This is typically done through the use of recombinant DNA technology, where a specific gene or genetic sequence of interest is isolated and then introduced into the mouse embryo. The resulting transgenic mice can then express the protein encoded by the foreign gene, allowing researchers to study its function in a living organism.
The process of creating transgenic mice usually involves microinjecting the exogenous DNA into the pronucleus of a fertilized egg, which is then implanted into a surrogate mother. The offspring that result from this procedure are screened for the presence of the foreign DNA, and those that carry the desired genetic modification are used to establish a transgenic mouse line.
Transgenic mice have been widely used in biomedical research to model human diseases, study gene function, and test new therapies. They provide a valuable tool for understanding complex biological processes and developing new treatments for a variety of medical conditions.
Ras proteins are a group of small GTPases that play crucial roles as regulators of intracellular signaling pathways in cells. They are involved in various cellular processes, such as cell growth, differentiation, and survival. Ras proteins cycle between an inactive GDP-bound state and an active GTP-bound state to transmit signals from membrane receptors to downstream effectors. Mutations in Ras genes can lead to constitutive activation of Ras proteins, which has been implicated in various human cancers and developmental disorders.
Proteins are complex, large molecules that play critical roles in the body's functions. They are made up of amino acids, which are organic compounds that are the building blocks of proteins. Proteins are required for the structure, function, and regulation of the body's tissues and organs. They are essential for the growth, repair, and maintenance of body tissues, and they play a crucial role in many biological processes, including metabolism, immune response, and cellular signaling. Proteins can be classified into different types based on their structure and function, such as enzymes, hormones, antibodies, and structural proteins. They are found in various foods, especially animal-derived products like meat, dairy, and eggs, as well as plant-based sources like beans, nuts, and grains.
F344 is a strain code used to designate an outbred stock of rats that has been inbreeded for over 100 generations. The F344 rats, also known as Fischer 344 rats, were originally developed at the National Institutes of Health (NIH) and are now widely used in biomedical research due to their consistent and reliable genetic background.
Inbred strains, like the F344, are created by mating genetically identical individuals (siblings or parents and offspring) for many generations until a state of complete homozygosity is reached, meaning that all members of the strain have identical genomes. This genetic uniformity makes inbred strains ideal for use in studies where consistent and reproducible results are important.
F344 rats are known for their longevity, with a median lifespan of around 27-31 months, making them useful for aging research. They also have a relatively low incidence of spontaneous tumors compared to other rat strains. However, they may be more susceptible to certain types of cancer and other diseases due to their inbred status.
It's important to note that while F344 rats are often used as a standard laboratory rat strain, there can still be some genetic variation between individual animals within the same strain, particularly if they come from different suppliers or breeding colonies. Therefore, it's always important to consider the source and history of any animal model when designing experiments and interpreting results.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
"Cells, cultured" is a medical term that refers to cells that have been removed from an organism and grown in controlled laboratory conditions outside of the body. This process is called cell culture and it allows scientists to study cells in a more controlled and accessible environment than they would have inside the body. Cultured cells can be derived from a variety of sources, including tissues, organs, or fluids from humans, animals, or cell lines that have been previously established in the laboratory.
Cell culture involves several steps, including isolation of the cells from the tissue, purification and characterization of the cells, and maintenance of the cells in appropriate growth conditions. The cells are typically grown in specialized media that contain nutrients, growth factors, and other components necessary for their survival and proliferation. Cultured cells can be used for a variety of purposes, including basic research, drug development and testing, and production of biological products such as vaccines and gene therapies.
It is important to note that cultured cells may behave differently than they do in the body, and results obtained from cell culture studies may not always translate directly to human physiology or disease. Therefore, it is essential to validate findings from cell culture experiments using additional models and ultimately in clinical trials involving human subjects.
DNA probes for HPV (Human Papillomavirus) are specific DNA sequences that are used in diagnostic tests to detect and identify the presence of HPV DNA in a sample. HPV is a viral infection that can cause various types of cancer, including cervical, anal, and oropharyngeal cancers.
DNA probes for HPV work by binding to complementary sequences of HPV DNA in the sample. This binding can be detected and measured using various methods, such as hybridization, amplification, or labeling techniques. The use of DNA probes for HPV can help identify the specific type of HPV that is present in a sample, which can inform clinical management and treatment decisions.
It's important to note that not all HPV infections lead to cancer, and most HPV infections resolve on their own without causing any harm. However, certain high-risk types of HPV are more strongly associated with an increased risk of developing cancer, so identifying the presence and type of HPV infection can be useful for monitoring and managing patients who may be at higher risk.
Cell surface receptors, also known as membrane receptors, are proteins located on the cell membrane that bind to specific molecules outside the cell, known as ligands. These receptors play a crucial role in signal transduction, which is the process of converting an extracellular signal into an intracellular response.
Cell surface receptors can be classified into several categories based on their structure and mechanism of action, including:
1. Ion channel receptors: These receptors contain a pore that opens to allow ions to flow across the cell membrane when they bind to their ligands. This ion flux can directly activate or inhibit various cellular processes.
2. G protein-coupled receptors (GPCRs): These receptors consist of seven transmembrane domains and are associated with heterotrimeric G proteins that modulate intracellular signaling pathways upon ligand binding.
3. Enzyme-linked receptors: These receptors possess an intrinsic enzymatic activity or are linked to an enzyme, which becomes activated when the receptor binds to its ligand. This activation can lead to the initiation of various signaling cascades within the cell.
4. Receptor tyrosine kinases (RTKs): These receptors contain intracellular tyrosine kinase domains that become activated upon ligand binding, leading to the phosphorylation and activation of downstream signaling molecules.
5. Integrins: These receptors are transmembrane proteins that mediate cell-cell or cell-matrix interactions by binding to extracellular matrix proteins or counter-receptors on adjacent cells. They play essential roles in cell adhesion, migration, and survival.
Cell surface receptors are involved in various physiological processes, including neurotransmission, hormone signaling, immune response, and cell growth and differentiation. Dysregulation of these receptors can contribute to the development of numerous diseases, such as cancer, diabetes, and neurological disorders.
Cyclin-Dependent Kinase Inhibitor p27, also known as CDKN1B or p27Kip1, is a protein that regulates the cell cycle. It inhibits the activity of certain cyclin-dependent kinases (CDKs), which are enzymes that play key roles in regulating the progression of the cell cycle.
The cell cycle is a series of events that cells undergo as they grow and divide. Cyclins and CDKs help to control the different stages of the cell cycle by activating and deactivating various proteins at specific times. The p27 protein acts as a brake on the cell cycle, preventing cells from dividing too quickly or abnormally.
When p27 binds to a CDK-cyclin complex, it prevents the complex from phosphorylating its target proteins, which are necessary for the progression of the cell cycle. By inhibiting CDK activity, p27 helps to ensure that cells divide only when the proper conditions are met.
Mutations in the CDKN1B gene, which encodes p27, have been associated with several types of cancer, including breast, lung, and prostate cancer. These mutations can lead to decreased levels of p27 or impaired function, allowing cells to divide uncontrollably and form tumors.
Southern blotting is a type of membrane-based blotting technique that is used in molecular biology to detect and locate specific DNA sequences within a DNA sample. This technique is named after its inventor, Edward M. Southern.
In Southern blotting, the DNA sample is first digested with one or more restriction enzymes, which cut the DNA at specific recognition sites. The resulting DNA fragments are then separated based on their size by gel electrophoresis. After separation, the DNA fragments are denatured to convert them into single-stranded DNA and transferred onto a nitrocellulose or nylon membrane.
Once the DNA has been transferred to the membrane, it is hybridized with a labeled probe that is complementary to the sequence of interest. The probe can be labeled with radioactive isotopes, fluorescent dyes, or chemiluminescent compounds. After hybridization, the membrane is washed to remove any unbound probe and then exposed to X-ray film (in the case of radioactive probes) or scanned (in the case of non-radioactive probes) to detect the location of the labeled probe on the membrane.
The position of the labeled probe on the membrane corresponds to the location of the specific DNA sequence within the original DNA sample. Southern blotting is a powerful tool for identifying and characterizing specific DNA sequences, such as those associated with genetic diseases or gene regulation.
The liver is a large, solid organ located in the upper right portion of the abdomen, beneath the diaphragm and above the stomach. It plays a vital role in several bodily functions, including:
1. Metabolism: The liver helps to metabolize carbohydrates, fats, and proteins from the food we eat into energy and nutrients that our bodies can use.
2. Detoxification: The liver detoxifies harmful substances in the body by breaking them down into less toxic forms or excreting them through bile.
3. Synthesis: The liver synthesizes important proteins, such as albumin and clotting factors, that are necessary for proper bodily function.
4. Storage: The liver stores glucose, vitamins, and minerals that can be released when the body needs them.
5. Bile production: The liver produces bile, a digestive juice that helps to break down fats in the small intestine.
6. Immune function: The liver plays a role in the immune system by filtering out bacteria and other harmful substances from the blood.
Overall, the liver is an essential organ that plays a critical role in maintaining overall health and well-being.
Aneuploidy is a medical term that refers to an abnormal number of chromosomes in a cell. Chromosomes are thread-like structures located inside the nucleus of cells that contain genetic information in the form of genes.
In humans, the normal number of chromosomes in a cell is 46, arranged in 23 pairs. Aneuploidy occurs when there is an extra or missing chromosome in one or more of these pairs. For example, Down syndrome is a condition that results from an extra copy of chromosome 21, also known as trisomy 21.
Aneuploidy can arise during the formation of gametes (sperm or egg cells) due to errors in the process of cell division called meiosis. These errors can result in eggs or sperm with an abnormal number of chromosomes, which can then lead to aneuploidy in the resulting embryo.
Aneuploidy is a significant cause of birth defects and miscarriages. The severity of the condition depends on which chromosomes are affected and the extent of the abnormality. In some cases, aneuploidy may have no noticeable effects, while in others it can lead to serious health problems or developmental delays.
Epidermal Growth Factor (EGF) is a small polypeptide that plays a significant role in various biological processes, including cell growth, proliferation, differentiation, and survival. It primarily binds to the Epidermal Growth Factor Receptor (EGFR) on the surface of target cells, leading to the activation of intracellular signaling pathways that regulate these functions.
EGF is naturally produced in various tissues, such as the skin, and is involved in wound healing, tissue regeneration, and maintaining the integrity of epithelial tissues. In addition to its physiological roles, EGF has been implicated in several pathological conditions, including cancer, where it can contribute to tumor growth and progression by promoting cell proliferation and survival.
As a result, EGF and its signaling pathways have become targets for therapeutic interventions in various diseases, particularly cancer. Inhibitors of EGFR or downstream signaling components are used in the treatment of several types of malignancies, such as non-small cell lung cancer, colorectal cancer, and head and neck cancer.
Human chromosome pair 11 consists of two rod-shaped structures present in the nucleus of each cell in the human body. Each member of the pair is a single chromosome, and together they contain the genetic material that is inherited from both parents. They are located on the eleventh position in the standard karyotype, which is a visual representation of the 23 pairs of human chromosomes.
Chromosome 11 is one of the largest human chromosomes and contains an estimated 135 million base pairs. It contains approximately 1,400 genes that provide instructions for making proteins, as well as many non-coding RNA molecules that play a role in regulating gene expression.
Chromosome 11 is known to contain several important genes and genetic regions associated with various human diseases and conditions. For example, it contains the Wilms' tumor 1 (WT1) gene, which is associated with kidney cancer in children, and the neurofibromatosis type 1 (NF1) gene, which is associated with a genetic disorder that causes benign tumors to grow on nerves throughout the body. Additionally, chromosome 11 contains the region where the ABO blood group genes are located, which determine a person's blood type.
It's worth noting that human chromosomes come in pairs because they contain two copies of each gene, one inherited from the mother and one from the father. This redundancy allows for genetic diversity and provides a backup copy of essential genes, ensuring their proper function and maintaining the stability of the genome.
Neoplasms are abnormal growths of cells or tissues in the body that can be benign (non-cancerous) or malignant (cancerous). When referring to "Complex and Mixed Neoplasms," it is typically used in the context of histopathology, where it describes tumors with a mixture of different types of cells or growth patterns.
A complex neoplasm usually contains areas with various architectural patterns, cell types, or both, making its classification challenging. It may require extensive sampling and careful examination to determine its nature and behavior. These neoplasms can be either benign or malignant, depending on the specific characteristics of the tumor cells and their growth pattern.
A mixed neoplasm, on the other hand, is a tumor that contains more than one type of cell or tissue component, often arising from different germ layers (the three primary layers of embryonic development: ectoderm, mesoderm, and endoderm). A common example of a mixed neoplasm is a teratoma, which can contain tissues derived from all three germ layers, such as skin, hair, teeth, bone, and muscle. Mixed neoplasms can also be benign or malignant, depending on the specific components of the tumor.
It's important to note that the classification and behavior of complex and mixed neoplasms can vary significantly based on their location in the body, cellular composition, and other factors. Accurate diagnosis typically requires a thorough examination by an experienced pathologist and may involve additional tests, such as immunohistochemistry or molecular analysis, to determine the appropriate treatment and management strategies.
Laminin is a family of proteins that are an essential component of the basement membrane, which is a specialized type of extracellular matrix. Laminins are large trimeric molecules composed of three different chains: α, β, and γ. There are five different α chains, three different β chains, and three different γ chains that can combine to form at least 15 different laminin isoforms.
Laminins play a crucial role in maintaining the structure and integrity of basement membranes by interacting with other components of the extracellular matrix, such as collagen IV, and cell surface receptors, such as integrins. They are involved in various biological processes, including cell adhesion, differentiation, migration, and survival.
Laminin dysfunction has been implicated in several human diseases, including cancer, diabetic nephropathy, and muscular dystrophy.
Glutathione transferases (GSTs) are a group of enzymes involved in the detoxification of xenobiotics and endogenous compounds. They facilitate the conjugation of these compounds with glutathione, a tripeptide consisting of cysteine, glutamic acid, and glycine, which results in more water-soluble products that can be easily excreted from the body.
GSTs play a crucial role in protecting cells against oxidative stress and chemical injury by neutralizing reactive electrophilic species and peroxides. They are found in various tissues, including the liver, kidneys, lungs, and intestines, and are classified into several families based on their structure and function.
Abnormalities in GST activity have been associated with increased susceptibility to certain diseases, such as cancer, neurological disorders, and respiratory diseases. Therefore, GSTs have become a subject of interest in toxicology, pharmacology, and clinical research.
Tissue distribution, in the context of pharmacology and toxicology, refers to the way that a drug or xenobiotic (a chemical substance found within an organism that is not naturally produced by or expected to be present within that organism) is distributed throughout the body's tissues after administration. It describes how much of the drug or xenobiotic can be found in various tissues and organs, and is influenced by factors such as blood flow, lipid solubility, protein binding, and the permeability of cell membranes. Understanding tissue distribution is important for predicting the potential effects of a drug or toxin on different parts of the body, and for designing drugs with improved safety and efficacy profiles.
ERBB-1, also known as EGFR (Epidermal Growth Factor Receptor), is a gene that provides instructions for making a receptor protein involved in cell growth, division, and survival. This gene belongs to the ERBB family of genes, which encode receptors with intrinsic tyrosine kinase activity.
The erbB-1/EGFR protein spans the cell membrane, with one part (the extracellular domain) extending outside the cell and another part (the intracellular domain) inside the cell. When a specific growth factor binds to the extracellular domain, it triggers a series of reactions that activate the tyrosine kinase activity within the intracellular domain. This activation leads to signal transduction pathways that promote cell growth, division, and survival.
Mutations in the erbB-1/EGFR gene have been associated with various types of cancer, such as lung, colon, breast, and brain cancers. These mutations often result in overactive receptors, leading to uncontrolled cell growth and division, ultimately contributing to tumor formation and progression.
Reference values, also known as reference ranges or reference intervals, are the set of values that are considered normal or typical for a particular population or group of people. These values are often used in laboratory tests to help interpret test results and determine whether a patient's value falls within the expected range.
The process of establishing reference values typically involves measuring a particular biomarker or parameter in a large, healthy population and then calculating the mean and standard deviation of the measurements. Based on these statistics, a range is established that includes a certain percentage of the population (often 95%) and excludes extreme outliers.
It's important to note that reference values can vary depending on factors such as age, sex, race, and other demographic characteristics. Therefore, it's essential to use reference values that are specific to the relevant population when interpreting laboratory test results. Additionally, reference values may change over time due to advances in measurement technology or changes in the population being studied.
Chromosome mapping, also known as physical mapping, is the process of determining the location and order of specific genes or genetic markers on a chromosome. This is typically done by using various laboratory techniques to identify landmarks along the chromosome, such as restriction enzyme cutting sites or patterns of DNA sequence repeats. The resulting map provides important information about the organization and structure of the genome, and can be used for a variety of purposes, including identifying the location of genes associated with genetic diseases, studying evolutionary relationships between organisms, and developing genetic markers for use in breeding or forensic applications.
Anoikis is a medical term that refers to a form of programmed cell death (apoptosis) that occurs when cells are detached from the extracellular matrix (ECM) or the surrounding cells to which they are normally attached. The term "anoikis" comes from the Greek words "an," meaning without, and "oikos," meaning home or house.
In the body, cells are typically anchored to the ECM through integrins and other adhesion molecules. When cells become detached from the ECM, they undergo a series of changes that ultimately lead to apoptosis. This process helps to prevent the spread of cancer cells, as tumor cells that break away from the primary tumor and invade surrounding tissues can be eliminated before they have a chance to form new tumors.
However, some cancer cells are able to evade anoikis and survive in a detached state. These cells may then go on to form metastases in distant organs. Understanding the mechanisms of anoikis and how cancer cells can evade it is an active area of research, as it may lead to new therapies for preventing or treating cancer metastasis.
Oncogene proteins are derived from oncogenes, which are genes that have the potential to cause cancer. Normally, these genes help regulate cell growth and division, but when they become altered or mutated, they can become overactive and lead to uncontrolled cell growth and division, which is a hallmark of cancer. Oncogene proteins can contribute to tumor formation and progression by promoting processes such as cell proliferation, survival, angiogenesis, and metastasis. Examples of oncogene proteins include HER2/neu, EGFR, and BCR-ABL.
Analysis of Variance (ANOVA) is a statistical technique used to compare the means of two or more groups and determine whether there are any significant differences between them. It is a way to analyze the variance in a dataset to determine whether the variability between groups is greater than the variability within groups, which can indicate that the groups are significantly different from one another.
ANOVA is based on the concept of partitioning the total variance in a dataset into two components: variance due to differences between group means (also known as "between-group variance") and variance due to differences within each group (also known as "within-group variance"). By comparing these two sources of variance, ANOVA can help researchers determine whether any observed differences between groups are statistically significant, or whether they could have occurred by chance.
ANOVA is a widely used technique in many areas of research, including biology, psychology, engineering, and business. It is often used to compare the means of two or more experimental groups, such as a treatment group and a control group, to determine whether the treatment had a significant effect. ANOVA can also be used to compare the means of different populations or subgroups within a population, to identify any differences that may exist between them.
Deoxycytidine is a chemical compound that is a component of DNA, one of the nucleic acids in living organisms. It is a nucleoside, consisting of the sugar deoxyribose and the base cytosine. Deoxycytidine pairs with guanine via hydrogen bonds to form base pairs in the double helix structure of DNA.
In biochemistry, deoxycytidine can also exist as a free nucleoside, not bound to other molecules. It is involved in various cellular processes related to DNA metabolism and replication. Deoxycytidine can be phosphorylated to form deoxycytidine monophosphate (dCMP), which is an important intermediate in the synthesis of DNA.
It's worth noting that while deoxycytidine is a component of DNA, its counterpart in RNA is cytidine, which contains ribose instead of deoxyribose as the sugar component.
There are many diseases that can affect cats, and the specific medical definitions for these conditions can be quite detailed and complex. However, here are some common categories of feline diseases and examples of each:
1. Infectious diseases: These are caused by viruses, bacteria, fungi, or parasites. Examples include:
* Feline panleukopenia virus (FPV), also known as feline parvovirus, which can cause severe gastrointestinal symptoms and death in kittens.
* Feline calicivirus (FCV), which can cause upper respiratory symptoms such as sneezing and nasal discharge.
* Feline leukemia virus (FeLV), which can suppress the immune system and lead to a variety of secondary infections and diseases.
* Bacterial infections, such as those caused by Pasteurella multocida or Bartonella henselae, which can cause abscesses or other symptoms.
2. Neoplastic diseases: These are cancerous conditions that can affect various organs and tissues in cats. Examples include:
* Lymphoma, which is a common type of cancer in cats that can affect the lymph nodes, spleen, liver, and other organs.
* Fibrosarcoma, which is a type of soft tissue cancer that can arise from fibrous connective tissue.
* Squamous cell carcinoma, which is a type of skin cancer that can be caused by exposure to sunlight or tobacco smoke.
3. Degenerative diseases: These are conditions that result from the normal wear and tear of aging or other factors. Examples include:
* Osteoarthritis, which is a degenerative joint disease that can cause pain and stiffness in older cats.
* Dental disease, which is a common condition in cats that can lead to tooth loss, gum inflammation, and other problems.
* Heart disease, such as hypertrophic cardiomyopathy (HCM), which is a thickening of the heart muscle that can lead to congestive heart failure.
4. Hereditary diseases: These are conditions that are inherited from a cat's parents and are present at birth or develop early in life. Examples include:
* Polycystic kidney disease (PKD), which is a genetic disorder that causes cysts to form in the kidneys and can lead to kidney failure.
* Hypertrophic cardiomyopathy (HCM), which can be inherited as an autosomal dominant trait in some cats.
* Progressive retinal atrophy (PRA), which is a group of genetic disorders that cause degeneration of the retina and can lead to blindness.
"Intralesional injection" is a medical term that refers to the administration of a medication directly into a lesion or skin abnormality, such as a tumor, cyst, or blister. This technique is used to deliver the medication directly to the site of action, allowing for higher local concentrations and potentially reducing systemic side effects. Common examples include the injection of corticosteroids into inflamed tissues to reduce swelling and pain, or the injection of chemotherapeutic agents directly into tumors to shrink them.
A gene is the basic unit of heredity in living organisms. It is a segment of DNA (deoxyribonucleic acid) that contains the instructions for the development and function of an organism. Genes are passed down from parents to offspring and determine many of an individual's traits, such as eye color and height.
A neoplasm, on the other hand, is a term used to describe an abnormal growth of cells, also known as a tumor. Neoplasms can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are generally not harmful and do not spread to other parts of the body. Malignant neoplasms, however, can invade and destroy nearby tissues and organs, and may also metastasize (spread) to other parts of the body.
In some cases, genetic mutations can lead to the development of neoplasms. These genetic changes can be inherited from parents or can occur spontaneously during a person's lifetime. Some genes are known to play a role in the development of certain types of cancer. For example, mutations in the BRCA1 and BRCA2 genes can increase a person's risk of developing breast and ovarian cancer.
It is important to note that not all neoplasms are caused by genetic mutations. Other factors, such as exposure to certain chemicals or viruses, can also contribute to the development of neoplasms.
Warts are small, rough growths on the skin or mucous membranes caused by one of several types of human papillomavirus (HPV). They can appear anywhere on the body but most often occur on the hands, fingers, and feet. Warts are benign, non-cancerous growths, but they can be unsightly, uncomfortable, or painful, depending on their location and size.
Warts are caused by HPV infecting the top layer of skin, usually through a small cut or scratch. The virus triggers an overproduction of keratin, a protein in the skin, leading to the formation of a hard, rough growth. Warts can vary in appearance depending on their location and type, but they are generally round or irregularly shaped, with a rough surface that may be flat or slightly raised. They may also contain small black dots, which are actually tiny blood vessels that have clotted.
Warts are contagious and can spread from person to person through direct skin-to-skin contact or by sharing personal items such as towels or razors. They can also be spread by touching a wart and then touching another part of the body. Warts may take several months to develop after exposure to HPV, so it may not always be clear when or how they were contracted.
There are several types of warts, including common warts, plantar warts (which occur on the soles of the feet), flat warts (which are smaller and smoother than other types of warts), and genital warts (which are sexually transmitted). While most warts are harmless and will eventually go away on their own, some may require medical treatment if they are causing discomfort or are unsightly. Treatment options for warts include topical medications, cryotherapy (freezing the wart with liquid nitrogen), and surgical removal.
Barrett esophagus is a condition in which the tissue lining of the lower esophagus changes, becoming more like the tissue that lines the intestines (intestinal metaplasia). This change can increase the risk of developing esophageal adenocarcinoma, a type of cancer. The exact cause of Barrett esophagus is not known, but it is often associated with long-term gastroesophageal reflux disease (GERD), also known as chronic acid reflux.
In Barrett esophagus, the normal squamous cells that line the lower esophagus are replaced by columnar epithelial cells. This change is usually detected during an upper endoscopy and biopsy. The diagnosis of Barrett esophagus is confirmed when the biopsy shows intestinal metaplasia in the lower esophagus.
It's important to note that not everyone with GERD will develop Barrett esophagus, and not everyone with Barrett esophagus will develop esophageal cancer. However, if you have been diagnosed with Barrett esophagus, your healthcare provider may recommend regular endoscopies and biopsies to monitor the condition and reduce the risk of cancer. Treatment options for Barrett esophagus include medications to control acid reflux, lifestyle changes, and in some cases, surgery.
Medical Definition of "Herpesvirus 4, Human" (Epstein-Barr Virus)
"Herpesvirus 4, Human," also known as Epstein-Barr virus (EBV), is a member of the Herpesviridae family and is one of the most common human viruses. It is primarily transmitted through saliva and is often referred to as the "kissing disease."
EBV is the causative agent of infectious mononucleosis (IM), also known as glandular fever, which is characterized by symptoms such as fatigue, sore throat, fever, and swollen lymph nodes. The virus can also cause other diseases, including certain types of cancer, such as Burkitt's lymphoma, Hodgkin's lymphoma, and nasopharyngeal carcinoma.
Once a person becomes infected with EBV, the virus remains in the body for the rest of their life, residing in certain white blood cells called B lymphocytes. In most people, the virus remains dormant and does not cause any further symptoms. However, in some individuals, the virus may reactivate, leading to recurrent or persistent symptoms.
EBV infection is diagnosed through various tests, including blood tests that detect antibodies against the virus or direct detection of the virus itself through polymerase chain reaction (PCR) assays. There is no cure for EBV infection, and treatment is generally supportive, focusing on relieving symptoms and managing complications. Prevention measures include practicing good hygiene, avoiding close contact with infected individuals, and not sharing personal items such as toothbrushes or drinking glasses.
Acantholysis is a medical term that refers to the separation of the cells in the upper layer of the skin (the epidermis), specifically between the pickle cell layer (stratum spinosum) and the granular cell layer (stratum granulosum). This separation results in the formation of distinct, round, or oval cells called acantholytic cells, which are typically seen in certain skin conditions.
Acantholysis is a characteristic feature of several skin disorders, including:
1. Pemphigus vulgaris: A rare autoimmune blistering disorder where the immune system produces antibodies against desmoglein-1 and -3 proteins, leading to acantholysis and formation of flaccid blisters.
2. Pemphigus foliaceus: Another autoimmune blistering disorder that specifically targets desmoglein-1 protein, causing superficial blisters and erosions on the skin.
3. Hailey-Hailey disease (familial benign chronic pemphigus): An autosomal dominant genetic disorder affecting ATP2C1 gene, leading to defective calcium transport and abnormal keratinocyte adhesion, resulting in acantholysis and recurrent skin eruptions.
4. Darier's disease (keratosis follicularis): An autosomal dominant genetic disorder affecting ATP2A2 gene, causing dysfunction of calcium transport and abnormal keratinocyte adhesion, resulting in acantholysis and characteristic papular or keratotic skin lesions.
5. Grover's disease (transient acantholytic dermatosis): An acquired skin disorder of unknown cause, characterized by the development of pruritic, red, and scaly papules and vesicles due to acantholysis.
The presence of acantholysis in these conditions can be confirmed through histopathological examination of skin biopsies.
Chemoradiotherapy, adjuvant is a medical treatment approach that involves the use of both chemotherapy and radiotherapy in combination to kill any remaining cancer cells after surgery. The goal of this therapy is to reduce the risk of recurrence or spread of the cancer. Adjuvant chemoradiotherapy may be recommended for certain types of cancers, such as colon, rectal, breast, head and neck, and lung cancer, among others.
Adjuvant chemotherapy involves the use of drugs that kill cancer cells throughout the body, while adjuvant radiotherapy uses high-energy radiation to target specific areas where the cancer was removed during surgery. The combination of these two treatments can be more effective than either treatment alone in preventing cancer recurrence and improving survival rates.
The timing and duration of chemoradiotherapy, as well as the specific drugs and doses used, may vary depending on the type and stage of cancer being treated, as well as the individual patient's overall health and medical history. It is important for patients to discuss their treatment options with their healthcare team to determine the best approach for their particular situation.
Genital neoplasms in males refer to abnormal growths or tumors that develop in the male reproductive organs. These can be benign (non-cancerous) or malignant (cancerous).
Malignant genital neoplasms are often referred to as genital cancers. The most common types of male genital cancers include:
1. Penile Cancer: This occurs when cancer cells form in the tissues of the penis.
2. Testicular Cancer: This forms in the testicles (testes), which are located inside the scrotum.
3. Prostate Cancer: This is a common cancer in men, forming in the prostate gland, which is part of the male reproductive system that helps make semen.
4. Scrotal Cancer: This is a rare form of cancer that forms in the skin or tissue of the scrotum.
5. Penile Intraepithelial Neoplasia (PeIN): This is not cancer, but it is considered a pre-cancerous condition of the penis.
Early detection and treatment of genital neoplasms can significantly improve the prognosis. Regular self-examinations and medical check-ups are recommended, especially for individuals with risk factors such as smoking, HIV infection, or a family history of these cancers.
'Digestive System Neoplasms' refer to new and abnormal growths of tissue in the digestive system that can be benign or malignant. These growths are also known as tumors, and they can occur in any part of the digestive system, including the esophagus, stomach, small intestine, large intestine (colon and rectum), liver, bile ducts, pancreas, and gallbladder. Neoplasms in the digestive system can interfere with normal digestion and absorption of nutrients, cause bleeding, obstruct the digestive tract, and spread to other parts of the body (metastasis) if they are malignant.
Benign neoplasms are not cancerous and do not usually spread to other parts of the body. They can often be removed surgically and may not require further treatment. Malignant neoplasms, on the other hand, are cancerous and can invade nearby tissues and organs and spread to other parts of the body. Treatment for malignant neoplasms in the digestive system typically involves a combination of surgery, radiation therapy, and chemotherapy.
The causes of digestive system neoplasms are varied and include genetic factors, environmental exposures, lifestyle factors (such as diet and smoking), and infectious agents. Prevention strategies may include maintaining a healthy diet, avoiding tobacco and excessive alcohol consumption, practicing safe sex, getting vaccinated against certain viral infections, and undergoing regular screenings for certain types of neoplasms (such as colonoscopies for colorectal cancer).
Apocrine glands are a type of sweat gland found in mammals, including humans. They are most concentrated in areas with dense hair follicles, such as the axillae (armpits) and genital region. These glands release their secretions into the hair follicle, which then reaches the skin surface through the pores.
Apocrine glands become active during puberty and are associated with the production of odorous sweat. The sweat produced by apocrine glands is initially odorless but can acquire a smell when it comes into contact with bacteria on the skin surface, which break down the organic compounds in the sweat. This can contribute to body odor.
It's important to note that while apocrine glands are often associated with body odor, they do not cause body odor directly. The odor is produced when the sweat from apocrine glands mixes with bacteria on the skin surface.
Endoscopy is a medical procedure that involves the use of an endoscope, which is a flexible tube with a light and camera at the end, to examine the interior of a body cavity or organ. The endoscope is inserted through a natural opening in the body, such as the mouth or anus, or through a small incision. The images captured by the camera are transmitted to a monitor, allowing the physician to visualize the internal structures and detect any abnormalities, such as inflammation, ulcers, or tumors. Endoscopy can also be used for diagnostic purposes, such as taking tissue samples for biopsy, or for therapeutic purposes, such as removing polyps or performing minimally invasive surgeries.
Glycoproteins are complex proteins that contain oligosaccharide chains (glycans) covalently attached to their polypeptide backbone. These glycans are linked to the protein through asparagine residues (N-linked) or serine/threonine residues (O-linked). Glycoproteins play crucial roles in various biological processes, including cell recognition, cell-cell interactions, cell adhesion, and signal transduction. They are widely distributed in nature and can be found on the outer surface of cell membranes, in extracellular fluids, and as components of the extracellular matrix. The structure and composition of glycoproteins can vary significantly depending on their function and location within an organism.
PROTEIN B-RAF, also known as serine/threonine-protein kinase B-Raf, is a crucial enzyme that helps regulate the cell growth signaling pathway in the body. It is a type of proto-oncogene protein, which means it has the potential to contribute to cancer development if mutated or overexpressed.
The B-RAF protein is part of the RAS/MAPK signaling pathway, which plays a critical role in controlling cell growth, division, and survival. When activated by upstream signals, B-RAF activates another kinase called MEK, which then activates ERK, leading to the regulation of various genes involved in cell growth and differentiation.
Mutations in the B-RAF gene can lead to constitutive activation of the protein, causing uncontrolled cell growth and division, which can contribute to the development of various types of cancer, including melanoma, colon cancer, and thyroid cancer. The most common mutation in the B-RAF gene is V600E, which affects around 8% of all human cancers.
Therefore, B-RAF inhibitors have been developed as targeted therapies for cancer treatment, particularly for melanoma patients with B-RAF V600E mutations. These drugs work by blocking the activity of the mutated B-RAF protein, thereby preventing uncontrolled cell growth and division.
A point mutation is a type of genetic mutation where a single nucleotide base (A, T, C, or G) in DNA is altered, deleted, or substituted with another nucleotide. Point mutations can have various effects on the organism, depending on the location of the mutation and whether it affects the function of any genes. Some point mutations may not have any noticeable effect, while others might lead to changes in the amino acids that make up proteins, potentially causing diseases or altering traits. Point mutations can occur spontaneously due to errors during DNA replication or be inherited from parents.
CD (cluster of differentiation) antigens are cell-surface proteins that are expressed on leukocytes (white blood cells) and can be used to identify and distinguish different subsets of these cells. They are important markers in the field of immunology and hematology, and are commonly used to diagnose and monitor various diseases, including cancer, autoimmune disorders, and infectious diseases.
CD antigens are designated by numbers, such as CD4, CD8, CD19, etc., which refer to specific proteins found on the surface of different types of leukocytes. For example, CD4 is a protein found on the surface of helper T cells, while CD8 is found on cytotoxic T cells.
CD antigens can be used as targets for immunotherapy, such as monoclonal antibody therapy, in which antibodies are designed to bind to specific CD antigens and trigger an immune response against cancer cells or infected cells. They can also be used as markers to monitor the effectiveness of treatments and to detect minimal residual disease (MRD) after treatment.
It's important to note that not all CD antigens are exclusive to leukocytes, some can be found on other cell types as well, and their expression can vary depending on the activation state or differentiation stage of the cells.
Cytoplasm is the material within a eukaryotic cell (a cell with a true nucleus) that lies between the nuclear membrane and the cell membrane. It is composed of an aqueous solution called cytosol, in which various organelles such as mitochondria, ribosomes, endoplasmic reticulum, Golgi apparatus, lysosomes, and vacuoles are suspended. Cytoplasm also contains a variety of dissolved nutrients, metabolites, ions, and enzymes that are involved in various cellular processes such as metabolism, signaling, and transport. It is where most of the cell's metabolic activities take place, and it plays a crucial role in maintaining the structure and function of the cell.
Recurrence, in a medical context, refers to the return of symptoms or signs of a disease after a period of improvement or remission. It indicates that the condition has not been fully eradicated and may require further treatment. Recurrence is often used to describe situations where a disease such as cancer comes back after initial treatment, but it can also apply to other medical conditions. The likelihood of recurrence varies depending on the type of disease and individual patient factors.
Ras genes are a group of genes that encode for proteins involved in cell signaling pathways that regulate cell growth, differentiation, and survival. Mutations in Ras genes have been associated with various types of cancer, as well as other diseases such as developmental disorders and autoimmune diseases. The Ras protein family includes H-Ras, K-Ras, and N-Ras, which are activated by growth factor receptors and other signals to activate downstream effectors involved in cell proliferation and survival. Abnormal activation of Ras signaling due to mutations or dysregulation can contribute to tumor development and progression.
Keratin-1
p14ARF is a tumor suppressor protein that plays a crucial role in regulating the cell cycle and preventing uncontrolled cell growth, which can lead to cancer. It is encoded by the CDKN2A gene located on chromosome 9p21.3. The p14ARF protein functions by binding to and inhibiting the activity of MDM2, a negative regulator of the tumor suppressor protein p53. By inhibiting MDM2, p14ARF promotes the stabilization and activation of p53, leading to cell cycle arrest or apoptosis in response to oncogenic signals or DNA damage. Mutations or deletions in the CDKN2A gene can result in the loss of p14ARF function, contributing to tumorigenesis.
Palliative care is a type of medical care that focuses on relieving the pain, symptoms, and stress of serious illnesses. The goal is to improve quality of life for both the patient and their family. It is provided by a team of doctors, nurses, and other specialists who work together to address the physical, emotional, social, and spiritual needs of the patient. Palliative care can be provided at any stage of an illness, alongside curative treatments, and is not dependent on prognosis.
The World Health Organization (WHO) defines palliative care as: "an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychological and spiritual."
Repressor proteins are a type of regulatory protein in molecular biology that suppress the transcription of specific genes into messenger RNA (mRNA) by binding to DNA. They function as part of gene regulation processes, often working in conjunction with an operator region and a promoter region within the DNA molecule. Repressor proteins can be activated or deactivated by various signals, allowing for precise control over gene expression in response to changing cellular conditions.
There are two main types of repressor proteins:
1. DNA-binding repressors: These directly bind to specific DNA sequences (operator regions) near the target gene and prevent RNA polymerase from transcribing the gene into mRNA.
2. Allosteric repressors: These bind to effector molecules, which then cause a conformational change in the repressor protein, enabling it to bind to DNA and inhibit transcription.
Repressor proteins play crucial roles in various biological processes, such as development, metabolism, and stress response, by controlling gene expression patterns in cells.
Cell hypoxia, also known as cellular hypoxia or tissue hypoxia, refers to a condition in which the cells or tissues in the body do not receive an adequate supply of oxygen. Oxygen is essential for the production of energy in the form of ATP (adenosine triphosphate) through a process called oxidative phosphorylation. When the cells are deprived of oxygen, they switch to anaerobic metabolism, which produces lactic acid as a byproduct and can lead to acidosis.
Cell hypoxia can result from various conditions, including:
1. Low oxygen levels in the blood (hypoxemia) due to lung diseases such as chronic obstructive pulmonary disease (COPD), pneumonia, or high altitude.
2. Reduced blood flow to tissues due to cardiovascular diseases such as heart failure, peripheral artery disease, or shock.
3. Anemia, which reduces the oxygen-carrying capacity of the blood.
4. Carbon monoxide poisoning, which binds to hemoglobin and prevents it from carrying oxygen.
5. Inadequate ventilation due to trauma, drug overdose, or other causes that can lead to respiratory failure.
Cell hypoxia can cause cell damage, tissue injury, and organ dysfunction, leading to various clinical manifestations depending on the severity and duration of hypoxia. Treatment aims to correct the underlying cause and improve oxygen delivery to the tissues.
STAT3 (Signal Transducer and Activator of Transcription 3) is a transcription factor protein that plays a crucial role in signal transduction and gene regulation. It is activated through phosphorylation by various cytokines and growth factors, which leads to its dimerization, nuclear translocation, and binding to specific DNA sequences. Once bound to the DNA, STAT3 regulates the expression of target genes involved in various cellular processes such as proliferation, differentiation, survival, and angiogenesis. Dysregulation of STAT3 has been implicated in several diseases, including cancer, autoimmune disorders, and inflammatory conditions.
Immunotherapy is a type of medical treatment that uses the body's own immune system to fight against diseases, such as cancer. It involves the use of substances (like vaccines, medications, or immune cells) that stimulate or suppress the immune system to help it recognize and destroy harmful disease-causing cells or agents, like tumor cells.
Immunotherapy can work in several ways:
1. Activating the immune system: Certain immunotherapies boost the body's natural immune responses, helping them recognize and attack cancer cells more effectively.
2. Suppressing immune system inhibitors: Some immunotherapies target and block proteins or molecules that can suppress the immune response, allowing the immune system to work more efficiently against diseases.
3. Replacing or enhancing specific immune cells: Immunotherapy can also involve administering immune cells (like T-cells) that have been genetically engineered or modified to recognize and destroy cancer cells.
Immunotherapies have shown promising results in treating various types of cancer, autoimmune diseases, and allergies. However, they can also cause side effects, as an overactive immune system may attack healthy tissues and organs. Therefore, careful monitoring is necessary during immunotherapy treatment.
Enzyme activation refers to the process by which an enzyme becomes biologically active and capable of carrying out its specific chemical or biological reaction. This is often achieved through various post-translational modifications, such as proteolytic cleavage, phosphorylation, or addition of cofactors or prosthetic groups to the enzyme molecule. These modifications can change the conformation or structure of the enzyme, exposing or creating a binding site for the substrate and allowing the enzymatic reaction to occur.
For example, in the case of proteolytic cleavage, an inactive precursor enzyme, known as a zymogen, is cleaved into its active form by a specific protease. This is seen in enzymes such as trypsin and chymotrypsin, which are initially produced in the pancreas as inactive precursors called trypsinogen and chymotrypsinogen, respectively. Once they reach the small intestine, they are activated by enteropeptidase, a protease that cleaves a specific peptide bond, releasing the active enzyme.
Phosphorylation is another common mechanism of enzyme activation, where a phosphate group is added to a specific serine, threonine, or tyrosine residue on the enzyme by a protein kinase. This modification can alter the conformation of the enzyme and create a binding site for the substrate, allowing the enzymatic reaction to occur.
Enzyme activation is a crucial process in many biological pathways, as it allows for precise control over when and where specific reactions take place. It also provides a mechanism for regulating enzyme activity in response to various signals and stimuli, such as hormones, neurotransmitters, or changes in the intracellular environment.
An epidermal cyst is a common benign skin condition characterized by the growth of a sac-like structure filled with keratin, a protein found in the outermost layer of the skin (epidermis). These cysts typically appear as round, firm bumps just under the surface of the skin, often on the face, neck, trunk, or scalp. They can vary in size from a few millimeters to several centimeters in diameter.
Epidermal cysts usually develop as a result of the accumulation of dead skin cells that become trapped within a hair follicle or a pilosebaceous unit (a structure that contains a hair follicle and an oil gland). The keratin produced by the skin cells then collects inside the sac, causing it to expand gradually.
These cysts are generally slow-growing, painless, and rarely cause any symptoms. However, they may become infected or inflamed, leading to redness, tenderness, pain, or pus formation. In such cases, medical attention might be necessary to drain the cyst or administer antibiotics to treat the infection.
Epidermal cysts can be removed surgically if they cause cosmetic concerns or become frequently infected. The procedure typically involves making an incision in the skin and removing the entire sac along with its contents to prevent recurrence.
The hypopharynx is the lower part of the pharynx, which is the muscular tube that extends from the back of the nasal cavity and mouth to the esophagus and trachea. The hypopharynx lies posterior to the larynx and is divided into three regions: the pyriform (or piriform) sinuses, the postcricoid area, and the posterior pharyngeal wall. It serves as a passageway for both food and air, and any abnormalities or diseases in this region can lead to swallowing difficulties, aspiration, and other serious medical conditions.
Tretinoin is a form of vitamin A that is used in the treatment of acne vulgaris, fine wrinkles, and dark spots caused by aging or sun damage. It works by increasing the turnover of skin cells, helping to unclog pores and promote the growth of new skin cells. Tretinoin is available as a cream, gel, or liquid, and is usually applied to the affected area once a day in the evening. Common side effects include redness, dryness, and peeling of the skin. It is important to avoid sunlight and use sunscreen while using tretinoin, as it can make the skin more sensitive to the sun.
Proto-oncogene proteins c-MET are a group of proteins that play a crucial role in normal cell growth and development. They are encoded by the c-MET gene, which provides instructions for making a receptor protein called MET. This receptor is located on the surface of certain cells and becomes active when it binds to a specific molecule called hepatocyte growth factor (HGF).
Activation of the MET receptor triggers a series of signaling pathways inside the cell that promote cell growth, survival, and motility. Proto-oncogene proteins c-MET help regulate various biological processes, including embryonic development, tissue repair, and angiogenesis (the formation of new blood vessels).
However, when the c-MET gene undergoes mutations or is abnormally activated, it can lead to the production of excessive or constantly active MET receptors. This results in uncontrolled cell growth and division, contributing to the development and progression of various types of cancer, such as carcinomas, sarcomas, and glioblastomas. Therefore, c-MET and its signaling pathways are attractive targets for cancer therapy.
Cytoskeletal proteins are a type of structural proteins that form the cytoskeleton, which is the internal framework of cells. The cytoskeleton provides shape, support, and structure to the cell, and plays important roles in cell division, intracellular transport, and maintenance of cell shape and integrity.
There are three main types of cytoskeletal proteins: actin filaments, intermediate filaments, and microtubules. Actin filaments are thin, rod-like structures that are involved in muscle contraction, cell motility, and cell division. Intermediate filaments are thicker than actin filaments and provide structural support to the cell. Microtubules are hollow tubes that are involved in intracellular transport, cell division, and maintenance of cell shape.
Cytoskeletal proteins are composed of different subunits that polymerize to form filamentous structures. These proteins can be dynamically assembled and disassembled, allowing cells to change their shape and move. Mutations in cytoskeletal proteins have been linked to various human diseases, including cancer, neurological disorders, and muscular dystrophies.
Cyclins are a family of regulatory proteins that play a crucial role in the cell cycle, which is the series of events that take place as a cell grows, divides, and produces two daughter cells. They are called cyclins because their levels fluctuate or cycle during the different stages of the cell cycle.
Cyclins function as subunits of serine/threonine protein kinase complexes, forming an active enzyme that adds phosphate groups to other proteins, thereby modifying their activity. This post-translational modification is a critical mechanism for controlling various cellular processes, including the regulation of the cell cycle.
There are several types of cyclins (A, B, D, and E), each of which is active during specific phases of the cell cycle:
1. Cyclin D: Expressed in the G1 phase, it helps to initiate the cell cycle by activating cyclin-dependent kinases (CDKs) that promote progression through the G1 restriction point.
2. Cyclin E: Active during late G1 and early S phases, it forms a complex with CDK2 to regulate the transition from G1 to S phase, where DNA replication occurs.
3. Cyclin A: Expressed in the S and G2 phases, it associates with both CDK2 and CDK1 to control the progression through the S and G2 phases and entry into mitosis (M phase).
4. Cyclin B: Active during late G2 and M phases, it partners with CDK1 to regulate the onset of mitosis by controlling the breakdown of the nuclear envelope, chromosome condensation, and spindle formation.
The activity of cyclins is tightly controlled through several mechanisms, including transcriptional regulation, protein degradation, and phosphorylation/dephosphorylation events. Dysregulation of cyclin expression or function can lead to uncontrolled cell growth and proliferation, which are hallmarks of cancer.
Hypoxia-Inducible Factor 1 (HIF-1) is a transcription factor that plays a crucial role in the body's response to low oxygen levels, also known as hypoxia. HIF-1 is a heterodimeric protein composed of two subunits: an alpha subunit (HIF-1α) and a beta subunit (HIF-1β).
The alpha subunit, HIF-1α, is the regulatory subunit that is subject to oxygen-dependent degradation. Under normal oxygen conditions (normoxia), HIF-1α is constantly produced in the cell but is rapidly degraded by proteasomes due to hydroxylation of specific proline residues by prolyl hydroxylase domain-containing proteins (PHDs). This hydroxylation reaction requires oxygen as a substrate, and under hypoxic conditions, the activity of PHDs is inhibited, leading to the stabilization and accumulation of HIF-1α.
Once stabilized, HIF-1α translocates to the nucleus, where it heterodimerizes with HIF-1β and binds to hypoxia-responsive elements (HREs) in the promoter regions of target genes. This binding results in the activation of gene transcription programs that promote cellular adaptation to low oxygen levels. These adaptive responses include increased erythropoiesis, angiogenesis, glucose metabolism, and pH regulation, among others.
Therefore, HIF-1α is a critical regulator of the body's response to hypoxia, and its dysregulation has been implicated in various pathological conditions, including cancer, cardiovascular disease, and neurodegenerative disorders.
Molecular targeted therapy is a type of treatment that targets specific molecules involved in the growth, progression, and spread of cancer. These molecules can be proteins, genes, or other molecules that contribute to the development of cancer. By targeting these specific molecules, molecular targeted therapy aims to block the abnormal signals that promote cancer growth and progression, thereby inhibiting or slowing down the growth of cancer cells while minimizing harm to normal cells.
Examples of molecular targeted therapies include monoclonal antibodies, tyrosine kinase inhibitors, angiogenesis inhibitors, and immunotherapies that target specific immune checkpoints. These therapies can be used alone or in combination with other cancer treatments such as chemotherapy, radiation therapy, or surgery. The goal of molecular targeted therapy is to improve the effectiveness of cancer treatment while reducing side effects and improving quality of life for patients.
Sunburn is a cutaneous condition characterized by redness, pain, and sometimes swelling of the skin caused by overexposure to ultraviolet (UV) radiation from the sun or other sources such as tanning beds. The skin may also blister and peel in severe cases. Sunburn is essentially a burn to the skin that can have both immediate and long-term consequences, including increased aging of the skin and an increased risk of skin cancer. It is important to protect the skin from excessive sun exposure by using sunscreen, wearing protective clothing, and seeking shade during peak sunlight hours.
Peritoneal neoplasms refer to tumors or cancerous growths that develop in the peritoneum, which is the thin, transparent membrane that lines the inner wall of the abdomen and covers the organs within it. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Malignant peritoneal neoplasms are often associated with advanced stages of gastrointestinal, ovarian, or uterine cancers and can spread (metastasize) to other parts of the abdomen.
Peritoneal neoplasms can cause various symptoms such as abdominal pain, bloating, nausea, vomiting, loss of appetite, and weight loss. Diagnosis typically involves imaging tests like CT scans or MRIs, followed by a biopsy to confirm the presence of cancerous cells. Treatment options may include surgery, chemotherapy, radiation therapy, or a combination of these approaches, depending on the type, stage, and location of the neoplasm.
An amino acid sequence is the specific order of amino acids in a protein or peptide molecule, formed by the linking of the amino group (-NH2) of one amino acid to the carboxyl group (-COOH) of another amino acid through a peptide bond. The sequence is determined by the genetic code and is unique to each type of protein or peptide. It plays a crucial role in determining the three-dimensional structure and function of proteins.
Caspase-3 is a type of protease enzyme that plays a central role in the execution-phase of cell apoptosis, or programmed cell death. It's also known as CPP32 (CPP for ced-3 protease precursor) or apopain. Caspase-3 is produced as an inactive protein that is activated when cleaved by other caspases during the early stages of apoptosis. Once activated, it cleaves a variety of cellular proteins, including structural proteins, enzymes, and signal transduction proteins, leading to the characteristic morphological and biochemical changes associated with apoptotic cell death. Caspase-3 is often referred to as the "death protease" because of its crucial role in executing the cell death program.
 Squamous-cell carcinoma
Squamous-cell carcinoma
Cutaneous squamous-cell carcinoma
Conjunctival squamous cell carcinoma
Basaloid squamous cell lung carcinoma
Squamous-cell carcinoma of the thyroid
Squamous-cell carcinoma of the vagina
Squamous-cell carcinoma of the lung
Skin cancer in horses
Henrietta Lacks
Oropharyngeal cancer
Tobacco smoking
Betel
Murad Alam
Oncovirus
Smoking cessation
Gardasil
HPV vaccine
Papilloma
Papanicolaou stain
Scottish Terrier
Keratoacanthoma
Perils of Paranoia
Actinic keratosis
Cervical cancer
Hedgehog
KMT2D
Right lymphatic duct
Oral cancer
Dentigerous cyst
Leukotriene B4 receptor 2
Situ9
- Three carcinomas in situ are associated with SCCs of the penis:[citation needed] Bowen's disease presents as leukoplakia on the shaft. (wikipedia.org)
- This condition is called squamous-cell carcinoma in situ, and it is diagnosed when the tumor has not yet penetrated the basement membrane or other delimiting structure to invade adjacent tissues. (wikipedia.org)
- Bowen's disease, also called squamous cell carcinoma in situ, is the earliest form of SCC. (healthline.com)
- Squamous cell carcinoma in situ (formerly called Bowen disease) most commonly occurs on sun-exposed areas of the skin but may occur anywhere. (msdmanuals.com)
- is the standard procedure for confirming the diagnosis of squamous cell carcinoma in situ. (msdmanuals.com)
- The earliest form (squamous cell carcinoma in situ) can appear as a scaly, crusted, and large reddish patch that can be larger than 1 inch (2.5 centimeters). (medlineplus.gov)
- Squamous cell carcinoma in situ (also known as Bowen's disease) is a very early form of skin cancer that hasn't yet spread beyond the top layer of the skin. (panthea.com.au)
- In situ carcinomas may progress to invasive lesions. (medscape.com)
- In situ carcinomas include Bowen disease, erythroplasia of Queyrat, and bowenoid papulosis. (medscape.com)
Head and neck23
- These membranes are made up of squamous cells and the head and neck cancers that grow in these cells are called squamous cell carcinomas. (cancer.gov)
- 1 In 2010, about 36,000 Americans are estimated to have been diagnosed with head and neck cancers and an estimated 7,880 were expected have died of squamous cell carcinomas. (cancer.gov)
- The integration of HPV, a virus harboring oncoproteins E6 and E7 that cause HPV positive head and neck squamous cell carcinomas, is linked to increased somatic copy number variants. (cancer.gov)
- Molecular characteristics may help clinicians improve the specificity of the diagnosis and treatment of head and neck squamous cell carcinomas. (cancer.gov)
- Head and Neck Squamous Cell Carcinoma Study was originally published by the National Cancer Institute. (cancer.gov)
- Cancer stem cells (CSC) drive growth, therapy resistance, and recurrence in head and neck squamous cell carcinoma (HNSCC). (nih.gov)
- SIGNIFICANCE: Inhibiting protein elongation with SVC112 reduces tumor growth in head and neck squamous cell carcinoma and increases the effects of radiation by targeting the cancer stem cell pool. (nih.gov)
- To construct a prognostic signature composed of DNA repair genes to effectively predict the prognosis of patients with head and neck squamous cell carcinoma (HNSCC). (frontiersin.org)
- Head and neck squamous cell carcinoma (HNSCC) is a type of tumor that originates from the squamous epithelium of the head and neck areas, including the mucous membranes of the lips, tongue, pharynx, larynx, and others ( 1 ). (frontiersin.org)
- ABSTRACT: Spindle cell carcinoma of head and neck, a subtype of squamous cell carcinoma is a unique and rare neoplasm. (scirp.org)
- As per DelveInsight analysis, the head and neck squamous cell carcinoma market is expected to grow positively at a significant CAGR during the study period (2019-2032). (advfn.com)
- Head and neck squamous cell carcinoma (HNSCC) is a type of cancer that originates in the squamous cells lining the mucous membranes of the head and neck region. (advfn.com)
- The head and neck squamous cell carcinoma epidemiology section provides insights into the historical and current head and neck squamous cell carcinoma patient pool and forecasted trends for individual seven major countries. (advfn.com)
- GB-263 is under clinical development by Genor BioPharma and currently in Phase II for Head And Neck Cancer Squamous Cell Carcinoma. (pharmaceutical-technology.com)
- According to GlobalData, Phase II drugs for Head And Neck Cancer Squamous Cell Carcinoma have a 26% phase transition success rate (PTSR) indication benchmark for progressing into Phase III. (pharmaceutical-technology.com)
- GB-263 is under development for the treatment of non-small cell lung cancer, gastric cancer, esophageal cancer, head and neck squamous cell carcinoma, metastatic colorectal cancer and other solid tumors. (pharmaceutical-technology.com)
- Advanced head and neck squamous cell carcinoma (HNSCC) is treated with radiotherapy, chemotherapy, targeted therapy or a combination of these treatments. (researchsquare.com)
- Merkel cell carcinoma usually presents as nodule of small size on the skin especially of head and neck regions with a property of changing colors like blue, purple, red, etc. whereas squamous cell carcinoma presents as a shallow ulcerative lesion with elevated margins and presence of plaques marks its configuration. (epainassist.com)
- The aim of this study was to compare diffusion-weighted magnetic resonance imaging (DWI) with computed tomography perfusion (CTP) for preoperative detection of metastases to lymph nodes (LNs) in head and neck squamous cell carcinoma (SCC). (hindawi.com)
- Squamous cell carcinoma (SCC) is the most common malignancy of the head and neck region. (hindawi.com)
- Docetaxel (DTX) combined with cisplatin and 5-fluorouracil has been used as induction chemotherapy for head and neck squamous cell carcinoma (HNSCC). (nih.gov)
- To assess the performance of whole-body MRI for staging patients with squamous cell carcinoma of the head and neck region. (uni-luebeck.de)
- p53 mutation and cyclin D1 amplification correlate with cisplatin sensitivity in xenografted human squamous cell carcinomas from head and neck. (lu.se)
Tumor14
- Oral squamous cell carcinoma (OSCC) is a common tumor in the world. (degruyter.com)
- In conclusion, SCARA5 inhibited the proliferation and EMT and induced the apoptosis of OSCC cells through the inhibition of STAT3 and PI3K/AKT signaling pathways, thereby exerting a tumor suppressor effect. (degruyter.com)
- We also analyzed the tumor-infiltrating immune cells, immune-related gene expression, tumor mutation burden, and drug sensitivity of patients with HNSCC in the high- and low-risk groups. (frontiersin.org)
- and GB223, a RANKL (receptor activator of NF-kappaB ligand) monoclonal antibody to treat giant-cell tumor of bone (GCTB). (pharmaceutical-technology.com)
- Background: The base of tongue squamous cell carcinoma (BOTSCC) is mainly an HPV-related tumor. (lu.se)
- It has been suggested that radiation sensitivity and chemosensitivity of cancer cells may play an important role in the local control of the tumor following these therapies. (researchsquare.com)
- It is a tumor suppressor gene and its suppression can lead to stimulation of oncogenes which are responsible for reducing the cell death. (epainassist.com)
- It ranges from a well-differentiated tumor with EPITHELIAL CELLS indistinguishable from normal HEPATOCYTES to a poorly differentiated neoplasm. (lookformedical.com)
- A lesion with cytological characteristics associated with invasive carcinoma but the tumor cells are confined to the epithelium of origin, without invasion of the basement membrane. (lookformedical.com)
- A cell line derived from cultured tumor cells. (lookformedical.com)
- Sometimes, vets will feel comfortable cutting the tumor itself and analyzing the cells that are inside of it. (innovetpet.com)
- However, four patients were classified as having carcinoma of unknown primary, as the primary tumor was not found with any imaging modality. (uni-luebeck.de)
- Following intravenous bolus administration of 30 units of bleomycin to one patient with a primary germ cell tumor of the brain, a peak CSF level was 40% of the simultaneously-obtained plasma level and was attained in two hours after drug administration. (nih.gov)
- Tumor types included squamous cell carcinomas, bronchoalveolar adenomas, bronchoalveolar carcinomas and scirrhous carcinomas. (cdc.gov)
Metastatic9
- Evidence-based recommendations on nivolumab (Opdivo) with fluoropyrimidine- and platinum-based chemotherapy for untreated unresectable advanced, recurrent, or metastatic oesophageal squamous cell carcinoma in adults. (nice.org.uk)
- Garg N, Stoehr C, Zhao YS, Rojas H and Hsueh CT: Metastatic squamous cell carcinoma of colon from esophageal cancer. (spandidos-publications.com)
- Both the cancers have their treatment of choice is surgical resection of the lesion but the lesion of squamous carcinoma requires more margins to be resected due to ulcerative presentation whereas Merkel cell carcinoma is associated more often with lymph node dissection due to higher metastatic rate. (epainassist.com)
- Although both can be metastatic in nature but Merkel cell cancer is more metastatic and is associated with a poorer prognosis than the squamous carcinoma. (epainassist.com)
- According to the microarray analysis and Western blots, PKM2 expression was up-regulated in TSCC cells with enhanced metastatic potential. (oncotarget.com)
- Metastatic carcinoma. (librepathology.org)
- Real-world Efficacy and Safety of Atezolizumab Plus Bevacizumab, Paclitaxel and Carboplatin for First-line Treatment of Japanese Patients With Metastatic Non-squamous Non-small Cell Lung Cancer. (nih.gov)
- Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: a pooled analysis of two randomised trials. (nih.gov)
- Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. (nih.gov)
Diagnosis8
- citation needed] Medical history, physical examination and medical imaging may suggest a squamous-cell carcinoma, but a biopsy for histopathology generally establishes the diagnosis. (wikipedia.org)
- How does this squamous cell carcinoma diagnosis feel compared to your first one? (mdanderson.org)
- A few years before my squamous cell carcinoma diagnosis, I had a red, painful ulcer-like spot on the side of my tongue. (mdanderson.org)
- Immunohistochemistry along with routine histopathology is essential in establishing the diagnosis of spindle cell carcinoma. (scirp.org)
- To present incisional biopsy importance as an effective clinical approach for the diagnosis of lip squamous cell carcinoma and actinic cheilitis malignancy as well as the professional's lack of knowledge on these two diseases. (bvsalud.org)
- This procedure confirmed the diagnosis of lip squamous cell carcinoma. (bvsalud.org)
- The physician and dentist must be aware of the main clinical features of lip squamous cell carcinoma so that they can establish its correct diagnosis and early treatment. (bvsalud.org)
- As with basal cell carcinoma , definitive diagnosis of SCC is made on histology following a punch, shave or excisional biopsy. (panthea.com.au)
Biopsy8
- SCC well-differentiated, left upper paraspinal back marked for biopsy with adjacent actinic keratosis SCC, left lateral canthus marked for biopsy SCC, left ventral forearm Cancer can be considered a very large and exceptionally heterogeneous family of malignant diseases, with squamous-cell carcinomas comprising one of the largest subsets. (wikipedia.org)
- A biopsy should be performed for any lesion suspected of being a cutaneous neoplasm to rule out basal cell carcinoma and other dermal lesions. (medscape.com)
- The biopsy showed that my tongue cancer - specifically, squamous cell carcinoma of the left lateral tongue - had returned. (mdanderson.org)
- A biopsy was performed on day 3, and the patient was diagnosed with squamous cell carcinoma. (cdc.gov)
- This red, irregular area on the arm was diagnosed as squamous cell carcinoma after a biopsy. (merckmanuals.com)
- It was diagnosed as squamous cell carcinoma after a biopsy. (merckmanuals.com)
- A skin biopsy must be done to confirm squamous cell skin cancer or other skin cancers. (medlineplus.gov)
- But a biopsy after surgery showed that there were no cancer cells remaining on his tongue. (cdc.gov)
Cutaneous squamous cell carcinomas6
- This is a retrospective case series of cutaneous squamous cell carcinomas (SCCs) which were incompletely excised in National Skin Centre, Singapore from 1991 to 1995. (annals.edu.sg)
- Also known as actinic keratosis, cutaneous squamous cell carcinomas are most notably recognizable based on the tumors that arise as a result of the buildup of cutaneous squamous cell carcinoma cells. (innovetpet.com)
- Cutaneous squamous cell carcinomas in dogs are a form of skin cancer that affects the epidermis and dermis layers of the skin. (innovetpet.com)
- As a result, the most common places for cutaneous squamous cell carcinomas to appear are behind the ears, on the back of dogs, in the nail beds, around the nail beds, between the pads of the dog's paws, near the abdominal region, and all around the nose of dogs. (innovetpet.com)
- You might be wondering what the different kinds of cutaneous squamous cell carcinomas are, so let's take a look at some of the most common types of SCC in dogs! (innovetpet.com)
- All types of cutaneous squamous cell carcinomas are marked by tumors on the skin. (innovetpet.com)
Malignant8
- Immunohistochemical analysis show concurrent presence of malignant epithelial and sarcomatoid spindle cell components by co-expression of cytokeratin (CK) and vimentin to various degrees. (scirp.org)
- Lip squamous cell carcinoma is a malignant lesion of aggressive behavior, which must be recognized by health professionals to prevent damage to patient's health. (bvsalud.org)
- A malignant neoplasm made up of epithelial cells tending to infiltrate the surrounding tissues and give rise to metastases. (lookformedical.com)
- A primary malignant neoplasm of epithelial liver cells. (lookformedical.com)
- A malignant neoplasm characterized by the formation of numerous, irregular, finger-like projections of fibrous stroma that is covered with a surface layer of neoplastic epithelial cells. (lookformedical.com)
- An anaplastic, highly malignant, and usually bronchogenic carcinoma composed of small ovoid cells with scanty neoplasm. (lookformedical.com)
- Among malignant neoplasms of the penis, squamous cell carcinoma (SCC) is the most common. (medscape.com)
- SCC of the prostate is a rare malignant epithelial neoplasm arising in the prostate, with squamous differentiation of the neoplastic cells. (medscape.com)
Lesion3
- Once the lesion has grown and progressed to the point where it has breached, penetrated, and infiltrated adjacent structures, it is referred to as "invasive" squamous-cell carcinoma. (wikipedia.org)
- Actinic keratosis is a precancerous skin lesion that may become a squamous cell cancer. (medlineplus.gov)
- However, since all individual cases of cutaneous squamous cell carcinoma in dogs are unique, so what happens after the first lesion appears will depend on the specifics of your dog's situation. (innovetpet.com)
Malignancy3
- Worldwide, cervical carcinoma is the second most frequent malignancy among women and the death rate is 8 per 100,000 [ 1 ]. (medsci.org)
- Esophageal squamous cell carcinoma (ESCC) is a malignancy with poor prognosis that requires extensive treatment. (biomedcentral.com)
- Squamous cell carcinoma is by far the most common malignancy of the tongue, typically having 3 gross morphologic growth patterns: exophytic, ulcerative, and infiltrative. (medscape.com)
Induces Apoptosis1
- TNF-related apoptosis inducing ligand (TRAIL) induces apoptosis through its death receptors (DRs) 4 and/or 5 expressed on the surface of target cells. (oncotarget.com)
Epithelial7
- All SCC lesions are thought to begin via the repeated, uncontrolled division of cancer stem cells of epithelial lineage or characteristics. (wikipedia.org)
- In this study, we found that the SCARA5 expression was lower in CAL-27 and SCC-9 cells than that in human normal oral epithelial keratinocytes. (degruyter.com)
- In addition, SCARA5 repressed OSCC cell epithelial-mesenchymal transformation (EMT), evidenced by increased E-cadherin expression and reduced N-cadherin expression. (degruyter.com)
- The study included SCC-1 human oral cancer cells and EBTr normal embryonic bovine tracheal epithelial cells, which were treated with 0 µM, 5 µM, 10 µM, and 20 µM of xanthoxyletin for 24 hours. (medscimonit.com)
- Squamous cells are flat cells of epithelial origin forming the outermost and uppermost layer of skin and even epidermis. (epainassist.com)
- A carcinoma derived from stratified SQUAMOUS EPITHELIAL CELLS. (lookformedical.com)
- It represents a large group of epithelial lung malignancies which can be divided into two clinical groups: SMALL CELL LUNG CANCER and NON-SMALL-CELL LUNG CARCINOMA . (lookformedical.com)
SCCs4
- citation needed] SCCs arise from squamous cells, which are flat cells that line many areas of the body. (wikipedia.org)
- Approximately 80% of non-melanoma skin cancers are basal cell carcinomas and the rest are squamous cell carcinomas (SCCs). (annals.edu.sg)
- SCCs are characterised by abnormal, accelerated growth of squamous cells. (panthea.com.au)
- Hypercalcemia-leukocytosis syndrome (HLS) as a paraneoplastic syndrome (PNS) of bladder cancers is rare, although it is documented in anaplastic thyroid, lung, and penile squamous cell carcinomas (SCCs) [ 1 , 2 ]. (biomedcentral.com)
ESCC6
- Esophageal cancer may be due to either esophageal squamous-cell carcinoma (ESCC) or adenocarcinoma (EAC). (wikipedia.org)
- Neoadjuvant chemotherapy (NAC) followed by surgery is the standard treatment for locally advanced esophageal squamous cell carcinoma (ESCC). (biomedcentral.com)
- Dysfunction of the Hippo pathway is common in esophageal squamous carcinoma (ESCC). (aging-us.com)
- Here, we demonstrated that chaetocin dramatically inhibited the proliferation in ESCC cells by causing cycle arrest in the M phase and activating the caspase-dependent apoptosis signaling pathway in vitro , and we also found that chaetocin induced the accumulation cellular reactive oxygen species (ROS). (aging-us.com)
- We further revealed that chaetocin triggered the activation of Hippo pathway in ESCC cells, which is characterized by elevated phosphorylation levels of almost all core proteins in Hippo pathway, such as MST1 (Thr183), MST2 (Thr180), MOB1 (Thr35), LAST1 (Thr1079 and Ser909) and YAP (Ser127), ultimately leading to decreased nuclear translocation of YAP. (aging-us.com)
- Moreover, the MST1/2 inhibitor XMU-MP-1 not only partially rescued the inhibitory effect chaetocin-induced proliferation, but also rescued the chaetocin-induced apoptosis in ESCC cells. (aging-us.com)
Prognosis3
- Primary squamous-cell carcinoma of the thyroid shows an aggressive biological phenotype resulting in poor prognosis for patients. (wikipedia.org)
- Actinic keratosis and basal cell carcinoma are easily excised and have a very good prognosis, while cSCC has a poor prognosis, especially if it invades the lymph nodes and adjacent vital structures. (medscape.com)
- Because it is very invasive, the prognosis of oral squamous cell carcinoma (OSCC) is poor ( 5 ). (spandidos-publications.com)
Invasive2
- An invasive (infiltrating) CARCINOMA of the mammary ductal system (MAMMARY GLANDS) in the human BREAST. (lookformedical.com)
- If untreated, these conditions may evolve to invasive carcinomas. (medscape.com)
Basal cell8
- Basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (cSCC) are the first and second most common types of skin cancer, respectively. (medscape.com)
- of those, approximately 80% were basal cell carcinoma (BCC) and 20% were cSCC. (medscape.com)
- Basal Cell Carcinoma Basal cell carcinoma, the most common skin cancer, originates in certain cells of the outer layer of the skin (epidermis). (merckmanuals.com)
- SCC is less common than Basal Cell Carcinoma (BCC), but it is more likely to spread to other body parts if left untreated. (advdermatology.com)
- We offer Mohs surgery to help treat common skin cancers in Gretna, NE, including basal cell carcinoma, squamous cell carcinoma, and some forms of melanoma. (moddermatology.com)
- This surgical treatment for basal cell or squamous cell carcinomas at our clinic in Gretna allows us to verify that we have removed all of the cancer cells, decreasing the need for any additional procedures and allowing you to heal more effectively. (moddermatology.com)
- Mohs surgery, offered in Gretna, for basal cell carcinoma, squamous cell carcinoma, or certain types of melanoma, can provide the help you need. (moddermatology.com)
- With its high success rate, Mohs surgery is one of the best options for skin cancer, like basal cell or squamous cell carcinomas. (moddermatology.com)
Esophageal cancer1
- Squamous cell carcinoma of the esophagus is a relatively uncommon form of esophageal cancer. (librepathology.org)
Penile1
- The cause of penile squamous cell carcinoma (SCC) is unclear, although human papillomavirus (HPV) appears to play a major role. (medscape.com)
Form of squamous1
- Some keratoacanthomas may be a form of squamous cell carcinoma. (merckmanuals.com)
Sign of squamous2
- A patch of skin that doesn't heal in regular time may be a sign of squamous cell carcinoma. (healthline.com)
- A sore that does not heal can be a sign of squamous cell cancer. (medlineplus.gov)
Risk of squamous1
- Protecting your skin from UV light can help reduce the risk of squamous cell carcinoma of the skin and other forms of skin cancer. (mayoclinic.org)
Cancers16
- Cutaneous squamous cell carcinoma (cSCC) is the second most common skin cancer and one of the most common cancers overall in the United States. (medscape.com)
- Cell cycle proteins are altered in differently in HPV-positive and HPV-negative cancers, suggesting that treating these cancers should be treated according to their subtype. (cancer.gov)
- The increased levels of EphA2 and EphrinA-1 in a relative high number of early stage squamous cell carcinomas suggested that these two proteins may play an important role in the development of a subset of early cervical cancers. (medsci.org)
- The unrestricted overgrowth of both the cells due to various factors leads to their respective cancers. (epainassist.com)
- Squamous cell cancers are much more common than Merkel cell cancer. (epainassist.com)
- Squamous cell carcinoma makes 20% of the total skin cancers of non-melanomatous origin whereas, on the other hand, the Merkel cell cancer is quite rare cancer to be found alone [2] . (epainassist.com)
- Since there is more of the incidence of squamous cell carcinoma than the Merkel cell carcinoma, these factors are found commonly associated with squamous cell cancers. (epainassist.com)
- The squamous cell cancers are having a much larger number of cases than Merkel cell cancer because of the strong association with etiological factors. (epainassist.com)
- The selectivity of TRAIL towards cancer cells has promoted clinical evaluation of recombinant human TRAIL (rhTRAIL) and its agonistic antibodies in treating several major human cancers including colon and non-Hodgkin's lymphoma. (oncotarget.com)
- American Cancer Society: What Are Basal and Squamous Cell Skin Cancers? (msdmanuals.com)
- Squamous Cell Carcinomas (SCC) account for at least 20% of all non-melanocytic skin cancers. (peachskinclinic.co.uk)
- Most squamous cell cancers occur on skin that is regularly exposed to sunlight or other ultraviolet radiation. (medlineplus.gov)
- Some squamous cell skin cancers may be more difficult to treat. (medlineplus.gov)
- Some squamous cell cancers may return. (medlineplus.gov)
- Squamous cell carcinoma (SCC) is the second most common type of skin cancer, and accounts for 30% of all non-melanoma skin cancers . (panthea.com.au)
- Non-schistosomiasis-associated squamous cell carcinoma (NSA-SCC) accounts for 2% of all bladder cancers in the Western world [ 3 ]. (biomedcentral.com)
Metastases2
- Wiseman D, Ferri L, Lakatos PL, Fiset PO and Bessissow T: Esophageal squamous cell carcinoma with colonic metastases. (spandidos-publications.com)
- Chen YH, Lin CY, Chen YT, Wu IC and Wang YK: Unusual metastases of esophageal squamous cell carcinoma. (spandidos-publications.com)
Goes untreated1
- Unfortunately, the longer squamous cell carcinoma goes untreated, the higher the chance of the cells affecting the bones as well. (innovetpet.com)
Tongue5
- Base of tongue squamous cell carcinomas, outcome depending on treatment strategy and p16 status. (lu.se)
- However, its role in the development and metastasis of tongue squamous cell carcinoma (TSCC) remains unclear. (oncotarget.com)
- Clinical appearance of a lateral tongue squamous cell carcinoma in an 80-year-old man with a previous history of smoking and regular alcoholic beverage consumption. (medscape.com)
- Indications are that the incidence of squamous cell carcinoma of the mobile tongue has been rising among younger women in industrialized nations. (medscape.com)
- The report found that the incidence of primary mobile tongue squamous cell carcinoma has significantly risen in persons under age 45 years within the populations of Australia and Singapore, with the rate of increase being significantly higher in females. (medscape.com)
Tumors4
- HPV-negative tumors contained novel co-amplifications of 11q13 and 11q22, an event that likely promotes the interaction of BIRC2 and FADD , genes that together work to inhibit cell death. (cancer.gov)
- The expression of genes involved in the migration of T cells and myeloid cells, T cell activation and costimulation, interferon (IFN)-γ signaling, cytotoxicity and apoptosis was higher than in low infiltrated tumors. (bmj.com)
- One of the major differences between these squamous cell skin tumors is their location on the body. (innovetpet.com)
- These melanocytic cells are of neuroectodermal origin, and melanocytic tumors may arise from these cells. (medscape.com)
Epithelium1
- Together with mucus-secreting goblet cells within the stratified epithelium, melanocytic cells are found in the basal layer of the conjunctiva. (medscape.com)
Lymph3
- may be used if squamous cell cancer has spread to organs or lymph nodes or if the cancer cannot be treated with surgery. (medlineplus.gov)
- Subungual squamous cell carcinoma specifically infiltrates the nodes and spreads throughout the body by traveling within infected lymph nodes. (innovetpet.com)
- Other times, it's easier for the professionals to look at the surrounding lymph nodes in order to further understand the situation because it's not uncommon for cancerous cells to infiltrate the nodes around them. (innovetpet.com)
Metastasis5
- The present study reports a rare case of esophageal squamous cell carcinoma (SCC) with rectal metastasis. (spandidos-publications.com)
- Shimada Y, Okumura T, Hojo S, Sukegawa K, Nagata T, Hayashi S and Tsukada K: Synchronous asymptomatic colonic metastasis from primary esophageal squamous cell carcinoma. (spandidos-publications.com)
- Hasegawa H, Oshikiri T, Yasuda T, Sumi Y, Fujino Y, Tominaga M and Kakeji Y: Colonic metastasis after resection of primary esophageal squamous cell carcinoma: report of a case. (spandidos-publications.com)
- Fang N, Wang YL, Zeng L, Wu ZJ and Liu LL: Colonic metastasis from esophageal squamous cell carcinoma demonstrated with 18F-FDG PET/CT. (spandidos-publications.com)
- PKM2 knockdown inhibited cell migration and invasion, reduced SOD2 (manganese superoxide dismutase) activity and the intracellular H 2 O 2 level, and inhibited tumour growth and lung metastasis in vivo . (oncotarget.com)
Keratinocytes1
- Squamous cells (keratinocytes) are the main structural cells of the epidermis (the outer layer of skin). (merckmanuals.com)
Vulvar2
Treatment7
- I have learned so much about squamous cell carcinoma and treatment protocols. (mdanderson.org)
- Surgical excision is the best treatment for squamous cell carcinoma and is usually curative. (advdermatology.com)
- Prevention and early treatment of Squamous Cell Carcinoma (SCC) is essential to reduce the risk of skin cancer and improve overall skin health. (advdermatology.com)
- In addition, cell cycle distribution analysis revealed that G0/G1 phase arrest was induced following pristimerin treatment in CAL‑27 and SCC‑25 cells, which was strongly associated with upregulation of p21 and p27, coupled with downregulation of cyclin D1 and cyclin E. Meanwhile, pristimerin induced significant apoptosis of CAL‑27 and SCC‑25 cells, alongside decreased levels of caspase‑3 and specific cleavage of poly (ADP‑ribose) polymerase. (spandidos-publications.com)
- The chances of treatment and survival are more in squamous cell carcinoma. (epainassist.com)
- First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. (nih.gov)
- Immune checkpoint inhibitors, alone or in combination with chemotherapy, as first-line treatment for advanced non-small cell lung cancer. (nih.gov)
Immunohistochemistry1
- By using immunohistochemistry we investigated the expression of EphA2 and EphrinA-1 in 217 early squamous cell cervical carcinomas and examine their prognostic relevance. (medsci.org)
Cancer39
- Squamous-cell carcinoma (SCC), also known as epidermoid carcinoma, comprises a number of different types of cancer that begin in squamous cells. (wikipedia.org)
- Cutaneous squamous-cell carcinoma is the second most common skin cancer, accounting for over 1 million cases in the United States each year. (wikipedia.org)
- When associated with the lung, it is typically a centrally located large-cell cancer (non-small-cell lung cancer). (wikipedia.org)
- It often has a paraneoplastic syndrome causing ectopic production of parathyroid hormone-related protein, resulting in hypercalcemia, but paraneoplastic syndrome is more commonly associated with small-cell lung cancer. (wikipedia.org)
- Most bladder cancer is transitional cell, but bladder cancer associated with schistosomiasis is often SCC. (wikipedia.org)
- Accumulation of these cancer cells causes a microscopic focus of abnormal cells that are, at least initially, locally confined within the specific tissue in which the progenitor cell resided. (wikipedia.org)
- Squamous cell carcinoma (SCC) is a type of skin cancer that most commonly forms on parts of your body exposed to the sun's rays. (healthline.com)
- Once you've had squamous cell carcinoma, you're at higher risk for a recurrence, even if the cancer is removed successfully. (healthline.com)
- Squamous cell carcinoma of the skin is a type of cancer that starts as a growth of cells on the skin. (mayoclinic.org)
- Squamous cell carcinoma is a common type of skin cancer. (mayoclinic.org)
- Squamous cell carcinoma (SCC) of the skin is the second most common form of skin cancer, with approximately 700,000 people in the United States being diagnosed each year. (tgh.org)
- SVC112 preferentially inhibited cancer cells compared with patient-matched cancer-associated fibroblasts, whereas HHT was equally toxic to both. (nih.gov)
- Squamous cell carcinoma is cancer that begins in the squamous cells of the skin. (merckmanuals.com)
- Squamous cell carcinoma is cancer of these cells. (merckmanuals.com)
- However, people who have had more sun exposure to their skin have a higher risk of developing squamous cell skin cancer. (merckmanuals.com)
- Squamous cell carcinoma (SCC) is the second most common form of skin cancer. (advdermatology.com)
- Squamous Cell Carcinoma (SCC) is a type of skin cancer that affects the squamous cells, which are the cells located in the upper layer of the skin's epidermis. (advdermatology.com)
- This study aimed to investigate the effects of xanthoxyletin, a plant-derived coumarin, on human oral squamous cancer cells in vitro and in mouse xenografts in vivo . (medscimonit.com)
- Xanthoxyletin significantly inhibited the proliferation of oral cancer cells (IC₅₀, 10-30 µM) with lower cytotoxicity for normal cells. (medscimonit.com)
- however, the antitumor effects and underlying mechanisms of pristimerin in oral cancer cells have not yet been identified. (spandidos-publications.com)
- Pristimerin has also been reported to induce apoptosis of various human cancer cells, including in multiple myeloma ( 10 ), breast ( 11 ), liver ( 12 ), pancreatic ( 13 ) and prostate cancer ( 14 ). (spandidos-publications.com)
- The term "oncotarget" encompasses all molecules, pathways, cellular functions, cell types, and even tissues that can be viewed as targets relevant to cancer as well as other diseases. (oncotarget.com)
- PKM2 is encoded by the PKM gene and is expressed in embryonic cells, adult stem cells, and cancer cells [ 3 ]. (oncotarget.com)
- Squamous cell carcinomas is a type of skin cancer that originates in the squamous cells, which form the outer layer of the top layer of skin (epidermis). (healthand.com)
- Squamous cell skin cancer is the second most common type of cancer in the United States. (medlineplus.gov)
- Squamous cell skin cancer affects the epidermis, the top layer of skin. (medlineplus.gov)
- Squamous cell cancer may occur in undamaged skin. (medlineplus.gov)
- A keratoacanthoma is a mild type of squamous cell cancer that grows rapidly. (medlineplus.gov)
- Curettage and electrodessication: Scraping away cancer cells and using electricity to kill any that remain. (medlineplus.gov)
- Freezing the cancer cells, which kills them. (medlineplus.gov)
- Medicines: Skin creams containing imiquimod or 5-fluorouracil for superficial squamous cell cancer. (medlineplus.gov)
- There is also a risk that squamous cell skin cancer may spread to other parts of the body. (medlineplus.gov)
- Macrophage coculture induced expression of intercellular adhesion molecule 1 (ICAM1), which promotes stemness and the formation of polyploid giant cancer cells, thereby reducing the efficacy of DTX. (nih.gov)
- Mohs surgery is a procedure where we remove thin layers of skin that contain cancer cells. (moddermatology.com)
- Workers with low professional qualification are at greater risk ranked the sixth most prevalent cancer in various countries in for developing squamous cell carcinoma (SCC) of the orophar- the world1. (bvsalud.org)
- Sintilimab plus bevacizumab biosimilar IBI305 and chemotherapy for patients with EGFR-mutated non-squamous non-small-cell lung cancer who progressed on EGFR tyrosine-kinase inhibitor therapy (ORIENT-31): first interim results from a randomised, double-blind, multicentre, phase 3 trial. (nih.gov)
- If a cell lives but repair is incomplete, lung cancer can develop (NRCC 1999). (cdc.gov)
- Cancer incidence typically increases with age, but it is not known whether ethnic characteristics influence the age dependence of squamous cell carcinoma of the skin (SCC).Objectives. (bvsalud.org)
- Squamous cell carcinoma con- geal cancer is endemic in some regions other malignancies were considered as stituted 95% and adenocarcinoma 5% of Islamic Republic of Iran [3,4] and exclusion criteria. (who.int)
Chemotherapy2
- Furthermore, pristimerin exhibited a more potent anti‑proliferative activity in CAL‑27 and SCC‑25 cells than the common chemotherapy drugs cisplatin and 5‑fluorouracil. (spandidos-publications.com)
- Currently, surgical removal, chemotherapy and radiotherapy are the most common and effective treatments for patients with oral carcinoma. (spandidos-publications.com)
Atypical2
- The atypical cells are partially covered by benign squamous cells, and there is a very sharp transition between the cells with atypia and those without. (librepathology.org)
- The atypical squamous cells extend into the subepithelial tissue in irregularly shaped nests and cords. (librepathology.org)
Oesophageal carcinoma2
- Integrated genomic characterization of oesophageal carcinoma. (spandidos-publications.com)
- We retrospectively examined the correlation of serum alkaline phosphatase (ALP) levels with several clinicopathological characteristics of 207 cases of oesophageal carcinoma. (who.int)
Oropharyngeal3
- Sex-based differences in outcomes among surgically treated patients with HPV-related oropharyngeal squamous cell carcinoma. (physiciansweekly.com)
- Sex differences in surgically treated HPV-associated oropharyngeal squamous cell carcinoma are not defined due to the low number of affected women. (physiciansweekly.com)
- We explored the oncologic outcomes of men and women with p16-positive oropharyngeal squamous cell carinoma treated with primary surgery. (physiciansweekly.com)
Cervical1
- In our previous study of cervical carcinomas FIGO stage I-IV we found that increase expression of EphA2 and EphrinA-1 was significantly associated with shorter overall survival in multivariate analysis [ 22 ]. (medsci.org)
Thyroid1
- Squamous cells are found on the top layers of skin as well as in various parts of the body such as the lungs, throat and thyroid. (tgh.org)
Primary1
- Methods The type, location, and infiltration pattern of T cells were studied in 109 patients with primary VSCC FIGO stage I-III. (bmj.com)
Radiation3
- Most squamous cell carcinomas of the skin are caused by too much ultraviolet (UV) radiation. (mayoclinic.org)
- SVC112 increased cell-cycle progression delay and slowed DNA repair following radiation, enhancing colony and sphere formation radiation effects. (nih.gov)
- Exposure to the ionizing radiation such as X rays, Gamma rays, etc. can easily propel these mutations in the cells and it could lead to cancerous growth. (epainassist.com)
Bowen's1
- In about 5 percent of cases , Bowen's disease becomes squamous cell carcinoma. (healthline.com)
Cytotoxicity1
- In each category, studies related to growth control genes, cell proliferation, apoptosis, DNA repair genes, antioxidant and drug detoxification genes, genes of drug metabolizing enzymes, tissue remodeling genes and genes of antibody-dependent cellular cytotoxicity were discussed separately. (researchsquare.com)
Subtype1
- Results High intraepithelial infiltration with CD4 or CD8 T cells was associated with longer overall and recurrence-free survival and formed an independent prognostic factor, outperforming molecular subtype and stage of the disease. (bmj.com)
Scaly3
- Squamous cell carcinoma is characterized by its thick, scaly, irregular appearance, but it can have various appearances, and a doctor may be suspicious of any sores on sun-exposed surfaces that do not heal. (merckmanuals.com)
- Squamous cell carcinoma typically begins as a red area with a scaly, crusted surface. (merckmanuals.com)
- Squamous cell carcinoma often appears as scaly red patches, open sores, or thick, warty plaques or bumps on the skin's surface. (advdermatology.com)
Clinical1
- Clinical photograph shows an extensive squamous cell carcinoma (SCC) arising on the distal foot in a patient with a history of previous burn injury. (basicmedicalkey.com)
Common1
- Non-schistosomiasis-associated squamous cell carcinoma of the urinary bladder is less common in the Western world. (biomedcentral.com)
Skin15
- These cells form on the surface of the skin, on the lining of hollow organs in the body, and on the lining of the respiratory and digestive tracts. (wikipedia.org)
- Because squamous cell carcinoma sometimes develops in existing skin lesions, it's important to monitor moles, warts, or skin lesions for changes. (healthline.com)
- Sun-exposed areas such as the lips and ears are especially likely to develop squamous cell carcinoma of the skin. (mayoclinic.org)
- The squamous cells make up the middle and outer layers of the skin. (mayoclinic.org)
- Squamous cell carcinoma of the skin is usually not life-threatening. (mayoclinic.org)
- But if it's not treated, squamous cell carcinoma of the skin can grow large or spread to other parts of the body. (mayoclinic.org)
- Squamous cell carcinomas can be anywhere on the skin. (mayoclinic.org)
- In people with Black and brown skin, squamous cell carcinomas are more likely to be on skin that isn't exposed to sun, such as the genitals. (mayoclinic.org)
- Squamous cell carcinoma of the skin most often occurs on sun-exposed skin. (mayoclinic.org)
- When squamous cell carcinoma of the skin happens in people with Black and brown skin, it tends to happen in places that aren't exposed to the sun. (mayoclinic.org)
- SCC is caused by mutations that occur in skin cell DNA. (tgh.org)
- Squamous cell carcinoma may develop on normal skin but is more likely to develop in damaged skin. (merckmanuals.com)
- This squamous cell carcinoma on the lip shows excess build up of keratin (a protein that forms on the surface of the skin, appearing as a brown crust) that has broken down to form an open sore. (merckmanuals.com)
- The UV rays can lead to mutations in the genetics of the skin cells and the commonly encountered gene to be mutated is the Tp53 gene. (epainassist.com)
- Various immune system defects like inability to do DNA repair in the skin cells known as xeroderma pigmentosum can also lead to accumulation of the mutations in the cells which can trigger the squamous cell carcinoma far more often than Merkel cell carcinoma which is relatively very rare with it. (epainassist.com)




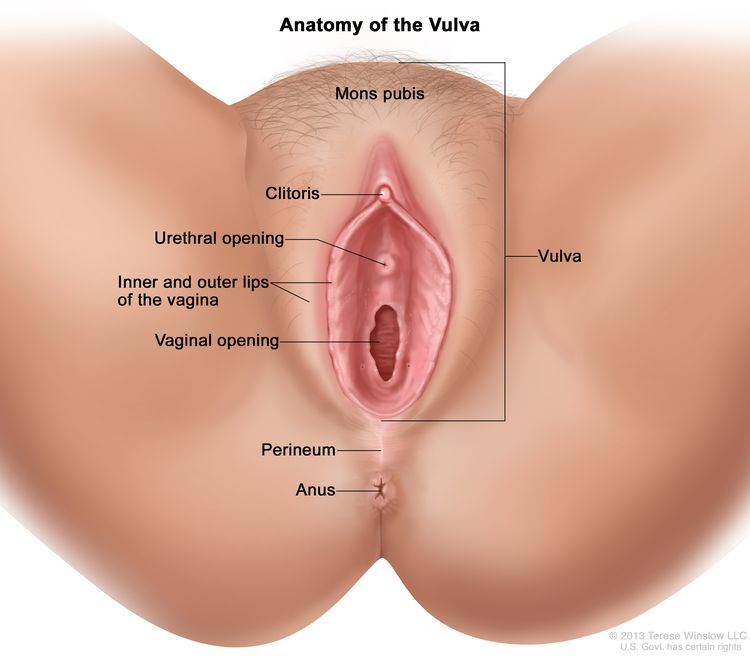
![Recombinant Anti-p53 antibody [E26] KO Tested (ab32389) | Abcam](https://www.abcam.com/ps/products/32/ab32389/Images/ab32389-389819-antip53antibodyimmunocytochemistryimmunofluorescencehap1human.jpg)