Carcinoma, Mucoepidermoid
Carcinoma
Salivary Glands, Minor
Adenolymphoma
Mucoepidermoid Tumor
Carcinoma, Adenoid Cystic
Tracheal Neoplasms
Adenoma, Pleomorphic
Carcinoma, Squamous Cell
Carcinoma, Acinar Cell
Carcinoma, Hepatocellular
Palatal Neoplasms
Jaw Cysts
Carcinoma in Situ
Immunohistochemistry
Tumor Markers, Biological
Gene Fusion
Maxillary Sinus
Radiography, Panoramic
Carcinoma, Papillary
Neoplasm Staging
Prognosis
Oncogene Proteins, Fusion
Sclerosis
Carcinoma, Ductal, Breast
Carcinoma, Basal Cell
Regulation of human airway mucins by acrolein and inflammatory mediators. (1/163)
Bronchitis, asthma, and cystic fibrosis, marked by inflammation and mucus hypersecretion, can be caused or exacerbated by airway pathogens or irritants including acrolein, an aldehyde present in tobacco smoke. To determine whether acrolein and inflammatory mediators alter mucin gene expression, steady-state mRNA levels of two airway mucins, MUC5AC and MUC5B, were measured (by RT-PCR) in human lung carcinoma cells (NCI-H292). MUC5AC mRNA levels increased after >/=0.01 nM acrolein, 10 microM prostaglandin E2 or 15-hydroxyeicosatetraenoic acid, 1.0 nM tumor necrosis factor-alpha (TNF-alpha), or 10 nM phorbol 12-myristate 13-acetate (a protein kinase C activator). In contrast, MUC5B mRNA levels, although easily detected, were unaffected by these agonists, suggesting that irritants and associated inflammatory mediators increase mucin biosynthesis by inducing MUC5AC message levels, whereas MUC5B is constitutively expressed. When transcription was inhibited, TNF-alpha exposure increased MUC5AC message half-life compared with control level, suggesting that transcript stabilization is a major mechanism controlling increased MUC5AC message levels. Together, these findings imply that irritants like acrolein can directly and indirectly (via inflammatory mediators) increase airway mucin transcripts in epithelial cells. (+info)Sclerosing Mucoepidermoid carcinoma with eosinophilia of the thyroid glands: a case report with clinical manifestation of recurrent neck mass. (2/163)
Sclerosing mucoepidermoid carcinoma with eosinophilia (SMECE) is a recently recognized malignant neoplasm of the thyroid gland. About 14 cases of SMECE have been reported and this is the first reported case in Korea. A 57-year-old woman presented with right neck mass for 20 years. Total thyroidectomy was performed under the impression of thyroid carcinoma. The resected thyroid gland showed a poorly circumscribed hard mass. Histologically, the tumor consisted of solid nests of large atypical cells with dense fibrous stroma. The tumor cells showed squamoid appearance with abundant eosinophilic cytoplasm. There were also rare mucin-containing cells within the nests. Within the hyalinized stroma, numerous eosinophils were found. The surrounding thyroid parenchyma displayed Hashimoto's thyroiditis. There was metastasis in a regional lymph node. Two years after initial surgery, she underwent a modified radical neck dissection due to recurrent neck mass. After the radiation therapy for eight weeks, laryngectomy and esophagectomy were performed due to a recurrent carcinoma in the esophageal wall. We report an additional case of SMECE, with metastasis to regional lymph nodes and esophagus. The tumor appears to be more aggressive than previously reported and a correct diagnosis can be rendered by just examining the metastatic lesions. (+info)Characterization of CFTR expression in a human pulmonary mucoepidermoid carcinoma cell line, NCI-H292 cells. (3/163)
The NCI-H292 cell, a human pulmonary mucoepidermoid carcinoma cell line, is commonly used for studying bacterial and viral infections of airway epithelial cells. Dysfunction of the cystic fibrosis transmembrane conductance regulator (CFTR) is the main cause of fetal lung infection in cystic fibrosis patients. In this study, we examined CFTR expression in NCI-H292 cells to determine whether NCI-H292 cells possess sufficient, normally functioning CFTR. The results of RT-PCR and Northern blotting analysis indicated that the CFTR gene expression level was much lower in NCI-H292 cells than in T84 cells. However, Western blotting analysis showed that protein expression in NCI-H292 cells was comparable to that in T84 cells. Furthermore, whole-cell and cell-attached patch clamp electrophysiological techniques indicated that the Cl- current induced by intracellular cAMP elevation in NCI-H292 cells was comparable to that in T84 cells. These findings suggest that NCI-H292 cells with a low level of CFTR gene expression possess enough functional CFTR to show a physiological response. (+info)Salivary gland tumors in Jordan: a retrospective study of 221 patients. (4/163)
AIM: To evaluate the types and clinical outcome of salivary gland tumors in Jordan. METHODS: Hospital records of 221 patients (85 women and 136 men) with salivary gland tumors, diagnosed from January 1988 to December 1997 were reviewed. The patients were analyzed according to sex, age, histopathological type and site of the tumor. Survival curves for patients with malignant tumors were constructed using Kaplan-Meier's method. RESULTS: Of the total 221 salivary gland tumors, 155 (70.2%) were parotid tumors, 42 (19%) minor salivary gland tumors, 23 (10.4%) submandibular gland tumors, and a single (0.4%) sublingual gland tumor. Most of the tumors (151, or 68.4%) were classified as benign and 70 (31.6%) were malignant. Men to women ratio was 1.6:1, and the age of the patients ranged from 2 to 81 years. The overall 5 and 10 year-survival rates for the 70 malignant tumors were 67% and 53%, respectively, for all tumor stages. Mucoepidermoid carcinoma had the best, and squamous cell carcinoma the worst 10-year survival rate. Patients treated with surgery and subsequent radiation therapy had better survival rates than those treated with surgery or radiation therapy alone. CONCLUSION: The principal site for salivary gland tumors in Jordan population was the parotid, and the pleo- morphic adenoma the most common pathological finding. Tumor characteristics and survival data for the Jordanian population are comparable to those from western countries. (+info)Detection of circulating anti-p53 antibodies in esophageal cancer patients. (5/163)
It has been reported that circulating anti-p53 antibodies (p53-Ab) in the serum are detected in some cancers. To investigate the usefulness of detecting p53-Ab, we measured the circulating p53-Ab in comparison with squamous cell carcinoma antigen (SCC-Ag) in patients with esophageal carcinoma. Serum specimens from 46 esophageal cancer patients (42 squamous cell carcinomas, 3 mucoepidermoid carcinomas and 1 basaloid squamous carcinoma) and 13 healthy subjects were studied. Serum p53-Ab was measured by an enzyme-linked immunosorbent assay. Surgically resected specimens from 43 patients were immunohistochemically stained for p53. Serum SCC-Ag was measured by a radioimmunoassay. The results were analyzed with the clinical data and outcome. Serum p53-Ab was detected in 13 (28%) of the 46 patients, but not in any of the healthy subjects. The positive rate was 0% (0/6) in stage I, 60% (3/5) in stage IIA, 30% (3/10) in stage IIB, 29% (7/24) in stage III and 0% (0/1) in stage IV. There was no difference in the outcome between the p53-Ab-positive and p53-Ab-negative patients. Immunohistochemically, 30 (70%) of the 43 specimens stained positively for p53. Serum p53-Ab was detected in 43% (13/30) of the patients with tumors which stained positively for p53. There was a close correlation between positivity for p53 immunostaining and positivity for p53-Ab (p<0.01). An elevated level of SCC-Ag was found in only 13%of the patients, and most patients positive for SCC-Ag already had advanced disease with lymph node metastasis and invasion to the adventitia. In conclusion, serum p53-Ab was detected in Japanese esophageal cancer patients at a frequency similar to that reported in Western countries. Serum p53-Ab may be a potentially useful molecular marker for detection and screening of esophageal cancer. Further studies of a large population may be required to elucidate the true diagnostic usefulness of measuring the serum p53-Ab. (+info)Failure patterns and factors affecting prognosis of salivary gland carcinoma: retrospective study. (6/163)
OBJECTIVES: To investigate the failure patterns and the prognostic factors following postoperative radiotherapy for salivary gland carcinoma. DESIGN: Retrospective study. SETTING: University teaching hospital, Hong Kong. PATIENTS: Fifty patients who had non-disseminated salivary gland carcinoma and who received primary treatment from 1984 through 1993. MAIN OUTCOME MEASURES: Demographic data, cancer T- and N-stages, histological type, site of origin, completeness of surgery, whether postoperative radiotherapy was given, and the clinical outcome. RESULTS: Two (4%) patients had been treated with radiotherapy alone, six (12%) had undergone radical resection alone, and 42 (84%) had been radically treated by using both modalities. The 5-year overall survival and relapse-free survival rates were 78.4% and 63.1%, respectively. The free from local failure and free from distant metastasis rates at 5 years were 77.2% and 72.8%, respectively. The N-stage was a significant prognostic factor. The site of the primary tumour, T-stage, completeness of surgery, and use of postoperative radiotherapy were not significant independent prognosticators; however, among the T-stage tumours, the b-substage carcinomas had significantly fewer local failures (P=0.040) and better survival rates (P=0.038) than the a-substage carcinomas. There were seven (14%) locoregional failures without distant metastasis, seven (14%) cases of distant metastasis without locoregional failures, and four (8%) locoregional failures preceding distant metastasis; isolated regional relapse was rare (1/50; 2%). All regional failures (5/50; 10%) occurred ipsilateral to the primary lesion. There were no deaths due to lymphoepithelioma-like carcinoma or acinic cell carcinoma. CONCLUSIONS: The N-stage is the main prognostic factor of overall survival, relapse- and metastasis-free recovery, and success of treatment for salivary gland carcinoma. Optimal locoregional treatment can help reduce distant metastasis, and the maximal use of postoperative radiotherapy may contribute to improved locoregional control. Elective ipsilateral neck radiotherapy is indicated for lymphoepithelioma-like carcinoma. (+info)Proliferating cell nuclear antigen expression in mucoepidermoid carcinoma of salivary glands. (7/163)
CONTEXT: Among the cytological and morphological properties of mucoepidermoid carcinoma, one of the most important criteria for measuring its biological behavior and aggressiveness is cell proliferation. In this way, immunohistochemical markers of cell proliferation have been found to be useful in tumor classification and have formed part of the prognostic and therapeutic studies of these pathologies. OBJECTIVE: To analyze 11 cases of mucoepidermoid carcinoma (MEC) using the proliferation activity marker (PCNA) and to determine its relationship to the grade of malignancy of these tumors. DESIGN: Correlation study. SETTING: Head and Neck Surgery Service of Heliopolis Hospital, Sao Paulo, Brazil. SAMPLE: Slides of 11 cases of primary mucoepidermoid carcinomas of salivary glands were prepared according to routine techniques employed in the Oral Pathology Department of the Dentistry Faculty of Sao Paulo University, Brazil. They were fixed in a 10% formaldehyde solution and stained with hematoxylin and eosin. After this preparation the tumors were classified as low, intermediate and high grade of malignancy, according to the criteria established by Seifert & Sobin and Auclair, Goode & Ellis. The slides were sent for immunohistochemical processing to evaluate the positivity of proliferating cell nuclear antigen using the streptavidin biotin technique. MAIN MEASUREMENT: The correlation between proliferating cell nuclear antigen expression and the histological malignancy grade in mucoepidermoid carcinoma of salivary glands. RESULTS: there were 4 cases (36%) of low grade, 4 cases (36%) of intermediate grade and 3 cases (27%) of high grade of malignancy. After a comparative study between histological features and immunohistochemical analysis, significant differences were observed (P < 0.01) for low, intermediate and high grades: 16.04%, 26.98% and 56.98% of proliferating cell nuclear antigen expression in mucoepidermoid carcinoma, respectively. CONCLUSION: The proliferating cell nuclear antigen expression increases with the grade of malignancy in mucoepidermoid carcinoma of salivary glands. (+info)Primary mucoepidermoid carcinoma and sclerosing mucoepidermoid carcinoma with eosinophilia of the thyroid gland: a report of nine cases. (8/163)
Mucoepidermoid carcinoma is a rare primary thyroid tumor with indolent biologic potential. Two types of tumors have been described under this category: mucoepidermoid carcinoma (MEC) and sclerosing mucoepidermoid carcinoma with eosinophilia (SMECE). The MEC shows both squamous and glandular differentiation in a background of a noninflamed gland, whereas SMECE is characterized by extensive sclerosis, squamous and glandular differentiation, a concomitant inflammatory infiltrate rich in eosinophils, and a background of lymphocytic thyroiditis. We present nine cases of these entities: five MEC and four SMECE. All tumors occurred in women (age 27 to 73 years). Five tumors showed extrathyroidal invasion and multiple lymph node metastases. One case of MEC showed a concomitant tall cell variant of papillary carcinoma with vascular invasion, and two cases showed intimately associated areas of usual papillary carcinoma. One of the latter cases also showed areas of transformation to anaplastic carcinoma. In all cases of SMECE and in only one case of MEC, the uninvolved thyroid tissue showed lymphocytic thyroiditis. Follow-up information was available in four of the nine cases (3 months to 7 years). Two patients with SMECE are alive with no evidence of disease. One patient with MEC and tall cell variant of papillary carcinoma died of disease after 3 months, and the patient with anaplastic carcinoma died after 5 months with lung metastasis. Both MEC and SMECE were positive for cytokeratin and negative for calcitonin. All cases of MEC were positive for thyroglobulin, whereas all cases of SMECE were negative. The immunohistochemical findings suggest that both MEC and SMECE have different histogenesis. (+info)Mucoepidermoid carcinoma is a type of cancer that develops in the salivary glands or, less commonly, in other areas such as the lungs or skin. It is called "mucoepidermoid" because it contains two types of cells: mucus-secreting cells and squamous (or epidermoid) cells.
Mucoepidermoid carcinomas can vary in their behavior, ranging from low-grade tumors that grow slowly and rarely spread to other parts of the body, to high-grade tumors that are aggressive and can metastasize. The treatment and prognosis for mucoepidermoid carcinoma depend on several factors, including the grade and stage of the tumor, as well as the patient's overall health.
It is important to note that while I strive to provide accurate and up-to-date information, this definition may not capture all the nuances of this medical condition. Therefore, it is always best to consult with a healthcare professional for medical advice.
Salivary gland neoplasms refer to abnormal growths or tumors that develop in the salivary glands. These glands are responsible for producing saliva, which helps in digestion, lubrication of food and maintaining oral health. Salivary gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms are slow-growing and typically do not spread to other parts of the body. They may cause symptoms such as swelling, painless lumps, or difficulty swallowing if they grow large enough to put pressure on surrounding tissues.
Malignant neoplasms, on the other hand, can be aggressive and have the potential to invade nearby structures and metastasize (spread) to distant organs. Symptoms of malignant salivary gland neoplasms may include rapid growth, pain, numbness, or paralysis of facial nerves.
Salivary gland neoplasms can occur in any of the major salivary glands (parotid, submandibular, and sublingual glands) or in the minor salivary glands located throughout the mouth and throat. The exact cause of these neoplasms is not fully understood, but risk factors may include exposure to radiation, certain viral infections, and genetic predisposition.
Carcinoma is a type of cancer that develops from epithelial cells, which are the cells that line the inner and outer surfaces of the body. These cells cover organs, glands, and other structures within the body. Carcinomas can occur in various parts of the body, including the skin, lungs, breasts, prostate, colon, and pancreas. They are often characterized by the uncontrolled growth and division of abnormal cells that can invade surrounding tissues and spread to other parts of the body through a process called metastasis. Carcinomas can be further classified based on their appearance under a microscope, such as adenocarcinoma, squamous cell carcinoma, and basal cell carcinoma.
Minor salivary glands are numerous small exocrine glands that produce saliva and are distributed throughout the oral cavity, nasal cavity, pharynx, larynx, and paranasal sinuses. They are classified as "minor" due to their smaller size compared to the three pairs of major salivary glands (parotid, submandibular, and sublingual). The minor salivary glands are primarily mucous glands, although some contain serous cells. They are responsible for producing approximately 5-10% of the total saliva in the mouth. These glands help moisten the oral cavity, protect the mucosal lining, and facilitate speaking, chewing, and swallowing.
Parotid neoplasms refer to abnormal growths or tumors in the parotid gland, which is the largest of the salivary glands and is located in front of the ear and extends down the neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parotid neoplasms are typically slow-growing, painless masses that may cause facial asymmetry or difficulty in chewing or swallowing if they become large enough to compress surrounding structures. The most common type of benign parotid tumor is a pleomorphic adenoma.
Malignant parotid neoplasms, on the other hand, are more aggressive and can invade nearby tissues and spread to other parts of the body. They may present as rapidly growing masses that are firm or fixed to surrounding structures. Common types of malignant parotid tumors include mucoepidermoid carcinoma, adenoid cystic carcinoma, and squamous cell carcinoma.
The diagnosis of parotid neoplasms typically involves a thorough clinical evaluation, imaging studies such as CT or MRI scans, and fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Treatment options depend on the type, size, and location of the neoplasm but may include surgical excision, radiation therapy, and chemotherapy.
Adenolymphoma is a rare, benign tumor that arises from the lymphoid tissue found in glandular structures, such as the salivary glands. It is also known as Warthin's tumor or cystic papillary adenolymphoma.
The tumor is composed of multiple cyst-like spaces lined by columnar epithelial cells and surrounded by lymphoid tissue, which may contain lymphocytes, plasma cells, and occasionally, germinal centers. The etiology of adenolymphoma is unclear, but it has been associated with smoking and genetic factors.
Adenolymphomas are typically slow-growing and painless, although they can cause discomfort or facial asymmetry if they become large enough. They are usually diagnosed through imaging studies such as ultrasound, CT scan, or MRI, followed by a biopsy to confirm the diagnosis.
Treatment of adenolymphoma typically involves surgical excision, which is usually curative. Recurrence after surgery is rare, but long-term follow-up is recommended due to the potential for malignant transformation into squamous cell carcinoma or other malignancies.
A mucoepidermoid tumor is a type of salivary gland neoplasm (abnormal growth) that can occur in the major or minor salivary glands. These tumors are characterized by the presence of mucus-secreting cells, epidermoid cells (which resemble skin cells), and intermediate cells.
Mucoepidermoid tumors are classified into three grades based on their histological features: low grade, intermediate grade, and high grade. Low-grade mucoepidermoid tumors tend to grow slowly and have a better prognosis compared to higher-grade tumors, which are more aggressive and have a higher risk of recurrence and metastasis (spread to other parts of the body).
Treatment for mucoepidermoid tumors typically involves surgical excision. The extent of surgery depends on the location, size, and grade of the tumor. Radiation therapy may also be recommended in some cases, particularly for high-grade tumors or when there is a high risk of residual tumor after surgery.
Adenoid cystic carcinoma (AdCC) is a rare type of cancer that can occur in various glands and tissues of the body, most commonly in the salivary glands. AdCC is characterized by its slow growth and tendency to spread along nerves. It typically forms solid, cystic, or mixed tumors with distinct histological features, including epithelial cells arranged in tubular, cribriform, or solid patterns.
The term "carcinoma" refers to a malignant tumor originating from the epithelial cells lining various organs and glands. In this case, adenoid cystic carcinoma is a specific type of carcinoma that arises in the salivary glands or other glandular tissues.
The primary treatment options for AdCC include surgical resection, radiation therapy, and sometimes chemotherapy. Despite its slow growth, adenoid cystic carcinoma has a propensity to recur locally and metastasize to distant sites such as the lungs, bones, and liver. Long-term follow-up is essential due to the risk of late recurrences.
Tracheal neoplasms refer to abnormal growths or tumors in the trachea, which is the windpipe that carries air from the nose and throat to the lungs. These growths can be benign (non-cancerous) or malignant (cancerous). Malignant tracheal neoplasms are relatively rare and can be primary (originating in the trachea) or secondary (spreading from another part of the body, such as lung cancer). Primary tracheal cancers can be squamous cell carcinoma, adenoid cystic carcinoma, mucoepidermoid carcinoma, or sarcomas. Symptoms may include cough, difficulty breathing, wheezing, or chest pain. Treatment options depend on the type, size, and location of the neoplasm and can include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
A pleomorphic adenoma is a type of benign (non-cancerous) tumor that typically develops in the salivary glands, although they can also occur in other areas such as the nasopharynx and skin. "Pleomorphic" refers to the diverse appearance of the cells within the tumor, which can vary in size, shape, and arrangement.
Pleomorphic adenomas are composed of a mixture of epithelial and mesenchymal cells, which can form glandular structures, squamous (scale-like) cells, and areas that resemble cartilage or bone. These tumors tend to grow slowly and usually do not spread to other parts of the body.
While pleomorphic adenomas are generally not dangerous, they can cause problems if they become large enough to press on surrounding tissues or structures. In some cases, these tumors may also undergo malignant transformation, leading to a cancerous growth known as carcinoma ex pleomorphic adenoma. Surgical removal is the standard treatment for pleomorphic adenomas, and the prognosis is generally good with proper management.
Squamous cell carcinoma is a type of skin cancer that begins in the squamous cells, which are flat, thin cells that form the outer layer of the skin (epidermis). It commonly occurs on sun-exposed areas such as the face, ears, lips, and backs of the hands. Squamous cell carcinoma can also develop in other areas of the body including the mouth, lungs, and cervix.
This type of cancer usually develops slowly and may appear as a rough or scaly patch of skin, a red, firm nodule, or a sore or ulcer that doesn't heal. While squamous cell carcinoma is not as aggressive as some other types of cancer, it can metastasize (spread) to other parts of the body if left untreated, making early detection and treatment important.
Risk factors for developing squamous cell carcinoma include prolonged exposure to ultraviolet (UV) radiation from the sun or tanning beds, fair skin, a history of sunburns, a weakened immune system, and older age. Prevention measures include protecting your skin from the sun by wearing protective clothing, using a broad-spectrum sunscreen with an SPF of at least 30, avoiding tanning beds, and getting regular skin examinations.
Carcinoma, acinar cell is a type of pancreatic cancer that originates in the acinar cells of the pancreas. The acinar cells are responsible for producing digestive enzymes. This type of cancer is relatively rare and accounts for less than 5% of all pancreatic cancers. It typically presents with symptoms such as abdominal pain, weight loss, and jaundice. Treatment options may include surgery, chemotherapy, and radiation therapy.
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer in adults. It originates from the hepatocytes, which are the main functional cells of the liver. This type of cancer is often associated with chronic liver diseases such as cirrhosis caused by hepatitis B or C virus infection, alcohol abuse, non-alcoholic fatty liver disease (NAFLD), and aflatoxin exposure.
The symptoms of HCC can vary but may include unexplained weight loss, lack of appetite, abdominal pain or swelling, jaundice, and fatigue. The diagnosis of HCC typically involves imaging tests such as ultrasound, CT scan, or MRI, as well as blood tests to measure alpha-fetoprotein (AFP) levels. Treatment options for Hepatocellular carcinoma depend on the stage and extent of the cancer, as well as the patient's overall health and liver function. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or liver transplantation.
Papillary cystadenoma is a type of benign (non-cancerous) tumor that arises from the glandular cells in various organs. It is characterized by the growth of finger-like projections (papillae) inside the cysts. These tumors can occur in different parts of the body, including the ovaries, pancreas, and the lining of the abdominal cavity (peritoneum).
In general, papillary cystadenomas are slow-growing and do not typically spread to other organs. However, they can cause symptoms such as pain or discomfort if they become large enough to press on surrounding tissues. Treatment usually involves surgical removal of the tumor. It is important to note that while papillary cystadenomas are generally benign, there is a small risk that they may undergo malignant transformation and develop into cancerous tumors over time. Regular follow-up with a healthcare provider is recommended to monitor for any changes in the tumor or the development of new symptoms.
Maxillary neoplasms refer to abnormal growths or tumors in the maxilla, which is the upper jaw bone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and spread to distant sites.
Maxillary neoplasms can cause various symptoms such as swelling, pain, numbness, loose teeth, or difficulty in chewing or swallowing. They may also cause nasal congestion, nosebleeds, or visual changes if they affect the eye or orbit. The diagnosis of maxillary neoplasms usually involves a combination of clinical examination, imaging studies such as CT or MRI scans, and biopsy to determine the type and extent of the tumor.
Treatment options for maxillary neoplasms depend on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and preferences. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis and ensure optimal outcomes.
Bronchial neoplasms refer to abnormal growths or tumors in the bronchi, which are the large airways that lead into the lungs. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Malignant bronchial neoplasms are often referred to as lung cancer and can be further classified into small cell lung cancer and non-small cell lung cancer, depending on the type of cells involved.
Benign bronchial neoplasms are less common than malignant ones and may include growths such as papillomas, hamartomas, or chondromas. While benign neoplasms are not cancerous, they can still cause symptoms and complications if they grow large enough to obstruct the airways or if they become infected.
Treatment for bronchial neoplasms depends on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Palatal neoplasms refer to abnormal growths or tumors that occur on the palate, which is the roof of the mouth. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slower growing and less likely to spread, while malignant neoplasms are more aggressive and can invade nearby tissues and organs.
Palatal neoplasms can have various causes, including genetic factors, environmental exposures, and viral infections. They may present with symptoms such as mouth pain, difficulty swallowing, swelling or lumps in the mouth, bleeding, or numbness in the mouth or face.
The diagnosis of palatal neoplasms typically involves a thorough clinical examination, imaging studies, and sometimes biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or spread of the neoplasm.
A jaw cyst is a pathological cavity filled with fluid or semi-fluid material, which forms within the jaw bones. They are typically classified as odontogenic (developing from tooth-forming tissues) or non-odontogenic (developing from other tissues). The most common types of odontogenic jaw cysts include dentigerous cysts (formed around the crown of an unerupted tooth) and follicular cysts (formed from the inflammation of a developing tooth's tissue). Non-odontogenic cysts, such as nasopalatine duct cysts and keratocystic odontogenic tumors, can also occur in the jaw bones. Jaw cysts may cause symptoms like swelling, pain, or displacement of teeth, but some may not present any symptoms until they grow large enough to be detected on a radiographic examination. Treatment typically involves surgical removal of the cyst and, if necessary, reconstruction of the affected bone.
Sublingual gland neoplasms refer to the abnormal growths or tumors that develop in the sublingual salivary glands, which are located beneath the tongue in the floor of the mouth. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign sublingual gland neoplasms are typically slow-growing and cause little to no discomfort, although they may become large enough to interfere with speaking, swallowing, or breathing. Malignant sublingual gland neoplasms, on the other hand, can grow rapidly, invade surrounding tissues, and potentially spread (metastasize) to other parts of the body.
The most common type of benign sublingual gland neoplasm is a pleomorphic adenoma, while malignant tumors may include mucoepidermoid carcinoma, adenoid cystic carcinoma, or squamous cell carcinoma. Treatment options for sublingual gland neoplasms depend on the type, size, location, and stage of the tumor but often involve surgical excision, with or without radiation therapy or chemotherapy. Regular follow-up care is essential to monitor for recurrence or metastasis.
Carcinoma in situ is a medical term used to describe the earliest stage of cancer, specifically a type of cancer that begins in the epithelial tissue, which is the tissue that lines the outer surfaces of organs and body structures. In this stage, the cancer cells are confined to the layer of cells where they first developed and have not spread beyond that layer into the surrounding tissues or organs.
Carcinoma in situ can occur in various parts of the body, including the skin, cervix, breast, lung, prostate, bladder, and other areas. It is often detected through routine screening tests, such as Pap smears for cervical cancer or mammograms for breast cancer.
While carcinoma in situ is not invasive, it can still be a serious condition because it has the potential to develop into an invasive cancer if left untreated. Treatment options for carcinoma in situ may include surgery, radiation therapy, or other forms of treatment, depending on the location and type of cancer. It is important to consult with a healthcare provider to determine the best course of action for each individual case.
Mandibular neoplasms refer to abnormal growths or tumors that develop in the mandible, which is the lower jawbone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and rarely spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and may metastasize (spread) to distant sites.
Mandibular neoplasms can have various causes, including genetic mutations, exposure to certain chemicals or radiation, and infection with certain viruses. The symptoms of mandibular neoplasms may include swelling or pain in the jaw, difficulty chewing or speaking, numbness in the lower lip or chin, loose teeth, and/or a lump or mass in the mouth or neck.
The diagnosis of mandibular neoplasms typically involves a thorough clinical examination, imaging studies such as X-rays, CT scans, or MRI scans, and sometimes a biopsy to confirm the type and extent of the tumor. Treatment options depend on the type, stage, and location of the neoplasm, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or metastasis.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
Tumor markers are substances that can be found in the body and their presence can indicate the presence of certain types of cancer or other conditions. Biological tumor markers refer to those substances that are produced by cancer cells or by other cells in response to cancer or certain benign (non-cancerous) conditions. These markers can be found in various bodily fluids such as blood, urine, or tissue samples.
Examples of biological tumor markers include:
1. Proteins: Some tumor markers are proteins that are produced by cancer cells or by other cells in response to the presence of cancer. For example, prostate-specific antigen (PSA) is a protein produced by normal prostate cells and in higher amounts by prostate cancer cells.
2. Genetic material: Tumor markers can also include genetic material such as DNA, RNA, or microRNA that are shed by cancer cells into bodily fluids. For example, circulating tumor DNA (ctDNA) is genetic material from cancer cells that can be found in the bloodstream.
3. Metabolites: Tumor markers can also include metabolic products produced by cancer cells or by other cells in response to cancer. For example, lactate dehydrogenase (LDH) is an enzyme that is released into the bloodstream when cancer cells break down glucose for energy.
It's important to note that tumor markers are not specific to cancer and can be elevated in non-cancerous conditions as well. Therefore, they should not be used alone to diagnose cancer but rather as a tool in conjunction with other diagnostic tests and clinical evaluations.
Lacrimal apparatus diseases refer to conditions that affect the structure and function of the lacrimal system, which is responsible for producing, storing, and draining tears. The lacrimal apparatus includes the lacrimal glands, lacrimal canaliculi, lacrimal sac, and nasolacrimal duct.
Diseases of the lacrimal apparatus can cause a range of symptoms, including watery eyes, redness, pain, swelling, and discharge. Some common conditions that affect the lacrimal apparatus include:
1. Dry eye syndrome: A condition in which the lacrimal glands do not produce enough tears or the tears are of poor quality, leading to dryness, irritation, and inflammation of the eyes.
2. Dacryocystitis: An infection of the lacrimal sac that can cause pain, swelling, redness, and discharge from the eye.
3. Nasolacrimal duct obstruction: A blockage in the nasolacrimal duct that can cause watery eyes, discharge, and recurrent infections.
4. Epiphora: Excessive tearing or watering of the eyes due to overflow of tears from the eye because of blocked tear ducts or increased production of tears.
5. Canaliculitis: An infection of the lacrimal canaliculi that can cause swelling, redness, and discharge from the eye.
6. Lacrimal gland tumors: Rare tumors that can affect the lacrimal glands and cause symptoms such as pain, swelling, and protrusion of the eyeball.
Treatment for lacrimal apparatus diseases depends on the specific condition and its severity. Treatment options may include medications, surgery, or a combination of both.
A gene fusion, also known as a chromosomal translocation or fusion gene, is an abnormal genetic event where parts of two different genes combine to create a single, hybrid gene. This can occur due to various mechanisms such as chromosomal rearrangements, deletions, or inversions, leading to the formation of a chimeric gene with new and often altered functions.
Gene fusions can result in the production of abnormal fusion proteins that may contribute to cancer development and progression by promoting cell growth, inhibiting apoptosis (programmed cell death), or activating oncogenic signaling pathways. In some cases, gene fusions are specific to certain types of cancer and serve as valuable diagnostic markers and therapeutic targets for personalized medicine.
The maxillary sinuses, also known as the antrums of Highmore, are the largest of the four pairs of paranasal sinuses located in the maxilla bones. They are air-filled cavities that surround the nasolacrimal duct and are situated superior to the upper teeth and lateral to the nasal cavity. Each maxillary sinus is lined with a mucous membrane, which helps to warm, humidify, and filter the air we breathe. Inflammation or infection of the maxillary sinuses can result in conditions such as sinusitis, leading to symptoms like facial pain, headaches, and nasal congestion.
Panoramic radiography is a specialized type of dental X-ray imaging that captures a panoramic view of the entire mouth, including the teeth, upper and lower jaws, and surrounding structures. It uses a special machine that rotates around the head, capturing images as it moves. This technique provides a two-dimensional image that is helpful in diagnosing and planning treatment for various dental conditions such as impacted teeth, bone abnormalities, and jaw disorders.
The panoramic radiograph can also be used to assess the development and positioning of wisdom teeth, detect cysts or tumors in the jaws, and evaluate the effects of trauma or injury to the mouth. It is a valuable tool for dental professionals as it allows them to see a comprehensive view of the oral structures, which may not be visible with traditional X-ray techniques.
It's important to note that while panoramic radiography provides valuable information, it should be used in conjunction with other diagnostic tools and clinical examinations to ensure accurate diagnosis and treatment planning.
Carcinoma, papillary is a type of cancer that begins in the cells that line the glandular structures or the lining of organs. In a papillary carcinoma, the cancerous cells grow and form small finger-like projections, called papillae, within the tumor. This type of cancer most commonly occurs in the thyroid gland, but can also be found in other organs such as the lung, breast, and kidney. Papillary carcinoma of the thyroid gland is usually slow-growing and has a good prognosis, especially when it is diagnosed at an early stage.
Neoplasm staging is a systematic process used in medicine to describe the extent of spread of a cancer, including the size and location of the original (primary) tumor and whether it has metastasized (spread) to other parts of the body. The most widely accepted system for this purpose is the TNM classification system developed by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC).
In this system, T stands for tumor, and it describes the size and extent of the primary tumor. N stands for nodes, and it indicates whether the cancer has spread to nearby lymph nodes. M stands for metastasis, and it shows whether the cancer has spread to distant parts of the body.
Each letter is followed by a number that provides more details about the extent of the disease. For example, a T1N0M0 cancer means that the primary tumor is small and has not spread to nearby lymph nodes or distant sites. The higher the numbers, the more advanced the cancer.
Staging helps doctors determine the most appropriate treatment for each patient and estimate the patient's prognosis. It is an essential tool for communication among members of the healthcare team and for comparing outcomes of treatments in clinical trials.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
Liver neoplasms refer to abnormal growths in the liver that can be benign or malignant. Benign liver neoplasms are non-cancerous tumors that do not spread to other parts of the body, while malignant liver neoplasms are cancerous tumors that can invade and destroy surrounding tissue and spread to other organs.
Liver neoplasms can be primary, meaning they originate in the liver, or secondary, meaning they have metastasized (spread) to the liver from another part of the body. Primary liver neoplasms can be further classified into different types based on their cell of origin and behavior, including hepatocellular carcinoma, cholangiocarcinoma, and hepatic hemangioma.
The diagnosis of liver neoplasms typically involves a combination of imaging studies, such as ultrasound, CT scan, or MRI, and biopsy to confirm the type and stage of the tumor. Treatment options depend on the type and extent of the neoplasm and may include surgery, radiation therapy, chemotherapy, or liver transplantation.
A mouth neoplasm refers to an abnormal growth or tumor in the oral cavity, which can be benign (non-cancerous) or malignant (cancerous). Malignant mouth neoplasms are also known as oral cancer. They can develop on the lips, gums, tongue, roof and floor of the mouth, inside the cheeks, and in the oropharynx (the middle part of the throat at the back of the mouth).
Mouth neoplasms can have various causes, including genetic factors, tobacco use, alcohol consumption, and infection with human papillomavirus (HPV). Symptoms may include a lump or thickening in the oral soft tissues, white or red patches, persistent mouth sores, difficulty swallowing or speaking, and numbness in the mouth. Early detection and treatment of mouth neoplasms are crucial for improving outcomes and preventing complications.
Prognosis is a medical term that refers to the prediction of the likely outcome or course of a disease, including the chances of recovery or recurrence, based on the patient's symptoms, medical history, physical examination, and diagnostic tests. It is an important aspect of clinical decision-making and patient communication, as it helps doctors and patients make informed decisions about treatment options, set realistic expectations, and plan for future care.
Prognosis can be expressed in various ways, such as percentages, categories (e.g., good, fair, poor), or survival rates, depending on the nature of the disease and the available evidence. However, it is important to note that prognosis is not an exact science and may vary depending on individual factors, such as age, overall health status, and response to treatment. Therefore, it should be used as a guide rather than a definitive forecast.
An oncogene protein fusion is a result of a genetic alteration in which parts of two different genes combine to create a hybrid gene that can contribute to the development of cancer. This fusion can lead to the production of an abnormal protein that promotes uncontrolled cell growth and division, ultimately resulting in a malignant tumor. Oncogene protein fusions are often caused by chromosomal rearrangements such as translocations, inversions, or deletions and are commonly found in various types of cancer, including leukemia and sarcoma. These genetic alterations can serve as potential targets for cancer diagnosis and therapy.
Sclerosis is a medical term that refers to the abnormal hardening or scarring of body tissues, particularly in the context of various degenerative diseases affecting the nervous system. The term "sclerosis" comes from the Greek word "skleros," which means hard. In these conditions, the normally flexible and adaptable nerve cells or their protective coverings (myelin sheath) become rigid and inflexible due to the buildup of scar tissue or abnormal protein deposits.
There are several types of sclerosis, but one of the most well-known is multiple sclerosis (MS). In MS, the immune system mistakenly attacks the myelin sheath surrounding nerve fibers in the brain and spinal cord, leading to scarring and damage that disrupts communication between the brain and the rest of the body. This results in a wide range of symptoms, such as muscle weakness, numbness, vision problems, balance issues, and cognitive impairment.
Other conditions that involve sclerosis include:
1. Amyotrophic lateral sclerosis (ALS): Also known as Lou Gehrig's disease, ALS is a progressive neurodegenerative disorder affecting motor neurons in the brain and spinal cord, leading to muscle weakness, stiffness, and atrophy.
2. Systemic sclerosis: A rare autoimmune connective tissue disorder characterized by thickening and hardening of the skin and internal organs due to excessive collagen deposition.
3. Plaque psoriasis: A chronic inflammatory skin condition marked by red, scaly patches (plaques) resulting from rapid turnover and accumulation of skin cells.
4. Adhesive capsulitis: Also known as frozen shoulder, this condition involves stiffening and thickening of the shoulder joint's capsule due to scarring or inflammation, leading to limited mobility and pain.
Carcinoma, ductal, breast is a type of breast cancer that begins in the milk ducts (the tubes that carry milk from the lobules of the breast to the nipple). It is called "ductal" because it starts in the cells that line the milk ducts. Ductal carcinoma can be further classified as either non-invasive or invasive, based on whether the cancer cells are confined to the ducts or have spread beyond them into the surrounding breast tissue.
Non-invasive ductal carcinoma (also known as intraductal carcinoma or ductal carcinoma in situ) is a condition where abnormal cells have been found in the lining of the milk ducts, but they have not spread outside of the ducts. These cells have the potential to become invasive and spread to other parts of the breast or body if left untreated.
Invasive ductal carcinoma (IDC) is a type of breast cancer that starts in a milk duct and then grows into the surrounding breast tissue. From there, it can spread to other parts of the body through the bloodstream and lymphatic system. IDC is the most common form of breast cancer, accounting for about 80% of all cases.
Symptoms of ductal carcinoma may include a lump or thickening in the breast, changes in the size or shape of the breast, dimpling or puckering of the skin on the breast, nipple discharge (especially if it is clear or bloody), and/or redness or scaling of the nipple or breast skin. However, many cases of ductal carcinoma are detected through mammography before any symptoms develop.
Treatment for ductal carcinoma depends on several factors, including the stage and grade of the cancer, as well as the patient's overall health and personal preferences. Treatment options may include surgery (such as a lumpectomy or mastectomy), radiation therapy, chemotherapy, hormone therapy, and/or targeted therapies.
Carcinoma, basal cell is a type of skin cancer that arises from the basal cells, which are located in the lower part of the epidermis (the outermost layer of the skin). It is also known as basal cell carcinoma (BCC) and is the most common form of skin cancer.
BCC typically appears as a small, shiny, pearly bump or nodule on the skin, often in sun-exposed areas such as the face, ears, neck, hands, and arms. It may also appear as a scar-like area that is white, yellow, or waxy. BCCs are usually slow growing and rarely spread (metastasize) to other parts of the body. However, they can be locally invasive and destroy surrounding tissue if left untreated.
The exact cause of BCC is not known, but it is thought to be related to a combination of genetic and environmental factors, including exposure to ultraviolet (UV) radiation from the sun or tanning beds. People with fair skin, light hair, and blue or green eyes are at increased risk of developing BCC.
Treatment for BCC typically involves surgical removal of the tumor, along with a margin of healthy tissue. Other treatment options may include radiation therapy, topical chemotherapy, or photodynamic therapy. Prevention measures include protecting your skin from UV radiation by wearing protective clothing, using sunscreen, and avoiding tanning beds.
Neoplastic gene expression regulation refers to the processes that control the production of proteins and other molecules from genes in neoplastic cells, or cells that are part of a tumor or cancer. In a normal cell, gene expression is tightly regulated to ensure that the right genes are turned on or off at the right time. However, in cancer cells, this regulation can be disrupted, leading to the overexpression or underexpression of certain genes.
Neoplastic gene expression regulation can be affected by a variety of factors, including genetic mutations, epigenetic changes, and signals from the tumor microenvironment. These changes can lead to the activation of oncogenes (genes that promote cancer growth and development) or the inactivation of tumor suppressor genes (genes that prevent cancer).
Understanding neoplastic gene expression regulation is important for developing new therapies for cancer, as targeting specific genes or pathways involved in this process can help to inhibit cancer growth and progression.
 Mucoepidermoid carcinoma
Mucoepidermoid carcinoma
Index of oral health and dental articles
Ramesh C. Deka
Glandular odontogenic cyst
Salivary gland
CRTC1
MAML2
Ceruminous gland
Parotidectomy
Dentigerous cyst
CTNNAL1
Human betaherpesvirus 5
Adenoid cystic carcinoma
Ceruminous adenocarcinoma
Parotid gland
Mastermind-like 3 (drosophila)
Head and neck cancer
Salivary gland tumour
Sebaceous lymphadenoma
Mucinous cystadenocarcinoma of the lung
Hyalinizing clear cell carcinoma
Oncovirus
Epithelial-myoepithelial carcinoma of the lung
Cysts of the jaws
Mucicarmine stain
Hidradenocarcinoma
Odontogenic cyst
List of MeSH codes (C04)
Pleural disease
Salivary gland-like carcinoma of the lung
Mucoepidermoid carcinoma - Wikipedia
 Scholarship@Western - Western Student Research Conference: Selective Upregulation of Kallikreins in Mucoepidermoid Carcinoma
Scholarship@Western - Western Student Research Conference: Selective Upregulation of Kallikreins in Mucoepidermoid Carcinoma
Carcinoma, Mucoepidermoid | Profiles RNS
 The Challenge of 'Monomorphic' Mucoepidermoid Carcinoma-Report of a Rare Case with Pure Spindle-Clear Cell Morphology. | Read...
The Challenge of 'Monomorphic' Mucoepidermoid Carcinoma-Report of a Rare Case with Pure Spindle-Clear Cell Morphology. | Read...
 Bronchial Adenoma: Practice Essentials, Pathophysiology, Etiology
Bronchial Adenoma: Practice Essentials, Pathophysiology, Etiology
 Mucoepidermoid Lung Carcinoma in Child | 2675
Mucoepidermoid Lung Carcinoma in Child | 2675
Short description of cell lines. Tumor: carcinoma, mucoepidermoid
 Juvenile mucoepidermoid carcinoma: a case report and literature review
Juvenile mucoepidermoid carcinoma: a case report and literature review
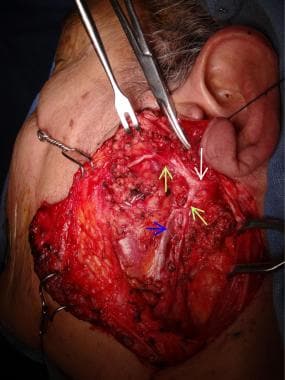
 High-Grade Mucoepidermoid Carcinoma Ex-Pleomorphic Adenoma of the Parotid Gland: Case Report and Review of Literature
High-Grade Mucoepidermoid Carcinoma Ex-Pleomorphic Adenoma of the Parotid Gland: Case Report and Review of Literature
 Bronchial mucoepidermoid carcinoma (Radiopaedia 57023-63895 Sagittal) - NC Commons
Bronchial mucoepidermoid carcinoma (Radiopaedia 57023-63895 Sagittal) - NC Commons
Conjunctival mucoepidermoid carcinoma: Clear cell variant<...
 View of Mucoepidermoid carcinoma of the palate: a rare case report
View of Mucoepidermoid carcinoma of the palate: a rare case report
 IRUCAA@TDC : A case of mucoepidermoid carcinoma associated with maxillary cyst.
IRUCAA@TDC : A case of mucoepidermoid carcinoma associated with maxillary cyst.
 LINE-1 and Alu hypomethylation in mucoepidermoid carcinoma | BMC Clinical Pathology | Full Text
LINE-1 and Alu hypomethylation in mucoepidermoid carcinoma | BMC Clinical Pathology | Full Text
 Surgical technique and results of tracheal and carinal replacement with aortic allografts for salivary gland-type carcinoma
Surgical technique and results of tracheal and carinal replacement with aortic allografts for salivary gland-type carcinoma
Radiation treatment to a postresection primary mucoepidermoid carcinoma (MEC) of the conjunctiva with positive margins at the...
 Cervical Cancers: Varieties and the Lower Anogenital Squamous Terminology - CytoJournal
Cervical Cancers: Varieties and the Lower Anogenital Squamous Terminology - CytoJournal
 Select Diagnosis | A Firm Palatal Nodule Select diagonosis | DentalCare.com
Select Diagnosis | A Firm Palatal Nodule Select diagonosis | DentalCare.com
 Mass in Parotid Gland of 39-Year-Old Patient
Mass in Parotid Gland of 39-Year-Old Patient
 André Fehr | Göteborgs universitet
André Fehr | Göteborgs universitet
 Tamara Giorgadze, MD, PhD | Medical College of Wisconsin
Tamara Giorgadze, MD, PhD | Medical College of Wisconsin
 Amifostine Plus Chemotherapy and Radiation Therapy in Treating Patients With Advanced, Unresectable Head and Neck Cancer
Amifostine Plus Chemotherapy and Radiation Therapy in Treating Patients With Advanced, Unresectable Head and Neck Cancer
 Thieme E-Journals - Klinische Monatsblätter für Augenheilkunde / Abstract
Thieme E-Journals - Klinische Monatsblätter für Augenheilkunde / Abstract
Hicham Jalal - Articles - Scientific Research Publishing
 Salivary gland cancer | Cancer Research UK
Salivary gland cancer | Cancer Research UK
 The Effect of Monocyte Count on Disease-Free Survival in Esophageal Cancer Patients | Research Square
The Effect of Monocyte Count on Disease-Free Survival in Esophageal Cancer Patients | Research Square
 Volume 44 Issue 2 | Acta Cytologica | Karger Publishers
Volume 44 Issue 2 | Acta Cytologica | Karger Publishers
 Paraffin Tissue Section - Human Lung Tumor, EGFR/KRAS Characterized | BioChain Institute Inc.
Paraffin Tissue Section - Human Lung Tumor, EGFR/KRAS Characterized | BioChain Institute Inc.
Malignant Tumors of the Palate: Practice Essentials, Etiology, Pathophysiology
 Journal Articles - ecancer
Journal Articles - ecancer
Tumor7
- Warthin tumor (WT)-like mucoepidermoid carcinoma (WT MEC) resembles the histologic pattern of WT, and pathologists unaware of this possibility may misdiagnose it as squamous and mucoepithelial WT or WT malignant transfer into MEC (MEC ex WT). (researchsquare.com)
- Mucoepidermoid carcinoma (MEC) is a rare pulmonary tumor that occurs for 0.1 to 0.2% of all pulmonary tumors [1] . (madridge.org)
- 7. Mucoepidermoid carcinoma of the hard palate: a rare cause of hypervascular tumor. (nih.gov)
- 11. Infarcted Warthin tumor with mucoepidermoid carcinoma-like metaplasia: a case report and review of the literature. (nih.gov)
- 15. A study of MECT1-MAML2 in mucoepidermoid carcinoma and Warthin's tumor of salivary glands. (nih.gov)
- The most common malignant tumor is mucoepidermoid carcinoma . (wikidoc.org)
- Clear cell carcinoma, NOS, is a rare form of salivary gland tumor and involves mostly minor salivary glands, especially those of the palate. (ispub.com)
Salivary glands3
- I'm a survivor (3.5 years) of low/intermediate grade mucoepidermoid carcinoma of the minor salivary glands in the base of my tongue. (cancer.org)
- The Evaluation and Management of Carcinoma of the Minor Salivary Glands. (nih.gov)
- Adenoid cystic carcinomas and actinic cell carcinomas - These develop in the salivary glands in the neck. (tgh.org)
Tumors5
- Relative incidence of parotid tumors, showing mucoepidermoid carcinoma at top right. (wikipedia.org)
- Adenoid cystic carcinoma behaves very similarly to major and minor salivary gland tumors. (medscape.com)
- Mucoepidermoid carcinomas account for about 21% of the malignant tumors of the parotid gland and 10% of the sublingual gland. (bvsalud.org)
- Epithelial tumors, like pleomorphic adenomas and adenoid cystic carcinomas, tend to occur in patients with an average age of 40 years. (eyewiki.org)
- Thymic neuroendocrine tumors are even less common than thymomas and thymic carcinomas. (itmig.org)
Adenoid6
- In cases of adenoid cystic carcinoma, the risk of lymph node metastasis is low, and the neck is not treated electively. (medscape.com)
- Adenoid cystic carcinoma (ACC), which commonly arises in a salivary gland, accounts for 10% of bronchial adenomas (0.04-0.2% of all lung cancers). (medscape.com)
- MEC and adenoid cystic carcinoma are considered to be salivary gland-type neoplasms. (madridge.org)
- Hemoptysis, while uncommon, more often occurs with a squamous cell carcinoma and can potentially lead to earlier diagnosis, whereas wheezing or stridor occurs more often with the adenoid cystic variant. (msdmanuals.com)
- A fusion oncogene between MYB and NFIB along with a translocation between chromosome 6q22-23 and chromosome 9pq23-24 has been associated with adenoid cystic carcinoma. (eyewiki.org)
- Adenoid cystic carcinoma (ACC) is characterized by solid areas or cords of bland-appearing malignant epithelial cells. (eyewiki.org)
Hard palate7
- Mucoepidermoid carcinoma of hard palate. (nih.gov)
- Juvenile mucoepidermoid carcinoma is a rare disease that occurs most often in the minor glands of the hard palate. (bvsalud.org)
- We report the case of a 12-year-old female with mucoepidermoid carcinoma of the hard palate with adjuvant radiotherapy. (bvsalud.org)
- 19. Calcifications in a clear cell mucoepidermoid carcinoma of the hard palate. (nih.gov)
- 20. Mucoepidermoid Carcinoma of the Hard Palate in a Young Patient. (nih.gov)
- Half of all hard palate cancers are squamous cell carcinomas (SCCs) as seen in the image below. (medscape.com)
- Squamous cell carcinoma of the hard palate. (medscape.com)
Histological2
- Salivary mucoepidermoid carcinoma: histological variants, grading systems, CRTC1/3-MAML2 fusions, and clinicopathological features. (nih.gov)
- Mucoepidermoid carcinoma (MEC) of the lung is a rare form of lung cancer that is classified into low grade andhigh grade based on histological features. (madridge.org)
Neoplasm3
- Mucoepidermoid carcinoma (MEC), characterized as the most common malignant salivary gland neoplasm, is histologically defined by a mixture of three cell types: epidermal cells, intermediate cells, and mucous cells, which may be present in different proportions. (researchsquare.com)
- Hyalinizing clear cell carcinoma (HCCC) is a neoplasm that predominantly affects the oral cavity in adult females. (ispub.com)
- Pleomorphic adenocarcinoma or carcinoma-ex-PA is a neoplasm resulting from the malignant transformation of a PA. (eyewiki.org)
Palate3
- 3. Atypical clinical manifestation of mucoepidermoid carcinoma in the palate. (nih.gov)
- 10. Mucoepidermoid carcinoma of the palate in a child. (nih.gov)
- Only 4 cases of clear cell carcinoma arising in pleomorphic adenoma have been reported so far, 2 in submandibular glands and 2 in a minor salivary gland of the palate 2 , 3 , 4 , 5 . (ispub.com)
Anaplastic1
- The most common type is papillary thyroid carcinoma (90%), mainly classic variant, sometimes follicular and tall cell variant ( J Clin Endocrinol Metab 2011;96:2684 ), and rarely anaplastic and mucoepidermoid carcinoma ( Thyroid FNA Cytology 2019:143 ). (pathologyoutlines.com)
Benign1
- They are characterized by a clinical course that is usually more benign than that of bronchogenic carcinoma. (medscape.com)
Adenosquamous2
- A 40-year-old woman with mucoepidermoid variant of adenosquamous carcinoma arising in dermoid cyst in left ovary is presented. (bmj.com)
- To our best knowledge, this is 12th case of adenosquamous carcinoma in dermoid cyst and third case of mucoepidermoid variant of adenosquamous carcinoma in the literature. (bmj.com)
Squamous cell10
- Four out of 21 patients had malignant melanoma (MM), while 17 had squamous cell carcinoma (SCC) of the conjunctiva. (karger.com)
- Frucht-Pery J, Rozenman Y, Pe'er J: Topical mitomycin-C for partially excised conjunctival squamous cell carcinoma. (karger.com)
- Shields CL, Demirci H, Marr BP, Masheyekhi A, Mathein M, Shields JA: Chemoreduction with topical mitomycin C prior to resection of extensive squamous cell carcinoma of the conjunctiva. (karger.com)
- Squamous cell carcinomas tend to metastasize to regional lymph nodes and directly invade mediastinal structures, leading to high local and regional recurrence rates. (msdmanuals.com)
- Squamous cell carcinomas - These develop in the thin, flat cells that make up the top layer of skin, as well as the lining on the inside of the esophagus and windpipe. (tgh.org)
- A history of prior squamous cell carcinoma , malignant melanoma , or malignant fibrous histiocytoma suggests intraglandular metastasis or metastasis to parotid lymph nodes. (medscape.com)
- They are classified according to their histomorphologic appearance with squamous cell carcinoma being the most common subtype. (itmig.org)
- Some thymic carcinoma subtypes such as well differentiated squamous cell carcinoma and mucoepidermoid carcinoma have a more favorable prognosis than others such as NUT carcinoma or lymphoepithelioma-like carcinoma which have a worse outcome. (itmig.org)
- Squamous cell carcinoma (5%) is derived from the actual cyst lining. (pathologyoutlines.com)
- Basal and squamous cell carcinomas of non-mucoepidermoid sites of the skin are not reportable. (getscreenedsd.org)
Pleomorphic Adenoma3
- We report the first case of hyalinizing clear cell carcinoma arising in a recurrent pleomorphic adenoma of the parotid gland in a 44 year-old female. (ispub.com)
- A definite diagnosis of HCCC arising in recurrent pleomorphic adenoma was rendered (carcinoma e-pleomorphic adenoma). (ispub.com)
- We report the first case of hyalinizing clear cell carcinoma arising in recurrent pleomorphic adenoma. (ispub.com)
Prognosis1
- Thyroglossal duct carcinoma has an excellent prognosis similar to conventional papillary thyroid carcinoma. (pathologyoutlines.com)
Lesions2
- 18. Mucoepidermoid carcinoma misdiagnosed as palatal odontogenic infection: an overview on the differential diagnosis of palatal lesions. (nih.gov)
- The differential diagnosis of lesions with prominent clear cells involving the parotid gland is extensive and includes clear cell myoepithelial carcinoma, clear cell epithelial-myoepithelial carcinoma, hyalinizing clear cell carcinoma, clear cell variant of acinic cell carcinoma and oncocytoma, mucoepidermoid carcinoma, and metastatic lesions especially carcinomas from kidney and thyroid, and from balloon cell melanomas. (ispub.com)
Form of salivary1
- Researchers at the University of Michigan Rogel Cancer Center and School of Dentistry found that certain drugs can change the fundamental makeup of cancer stem cells in mouse models of mucoepidermoid carcinoma - a lethal form of salivary gland cancer that currently has no treatment options. (rogelcancercenter.org)
Major salivary gland2
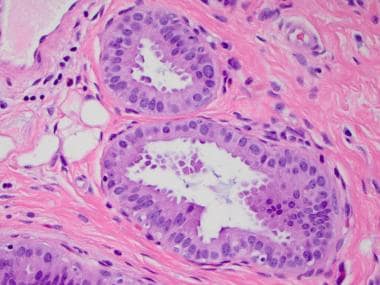
- Histopathologic image of mucoepidermoid carcinoma of the major salivary gland. (wikipedia.org)
- H & E stain Histopathologic image of mucoepidermoid carcinoma of the major salivary gland. (wikipedia.org)
Malignancy3
- Mucoepidermoid carcinoma (MEC) is the most common type of minor salivary gland malignancy in adults. (wikipedia.org)
- Introduction: Mucoepidermoid carcinoma (MEC) of the upper aerodigestive tract (UADT) is an uncommon malignancy, with limited literature available on its clinical and pathologic characteristics. (utmb.edu)
- Thyroglossal duct carcinoma is a rare malignancy arising from thyroid follicular cells of the thyroglossal duct. (pathologyoutlines.com)
Clear Cell Variant1
- 14. A clear cell variant of mucoepidermoid carcinoma harboring CRTC1-MAML2 fusion gene found in buccal mucosa: report of a case showing a large clear cell component and lacking typical epidermoid cells and intermediate cells. (nih.gov)
MECT1-MAML22
- Alcian blue-PAS stain Mucoepidermoid carcinomas of the salivary and bronchial glands are characterized by a recurrent t(11;19)(q21;p13) chromosomal translocation resulting in a MECT1-MAML2 fusion gene. (wikipedia.org)
- 12. MECT1-MAML2 fusion transcript defines a favorable subset of mucoepidermoid carcinoma. (nih.gov)
Translocation1
- t(11;19)(q21;p13) translocation in mucoepidermoid carcinoma creates a novel fusion product that disrupts a Notch signaling pathway. (nih.gov)
Adenocarcinoma1
- Primary adenocarcinoma also is characterized by glandular differentiation but does not have features that identify more specific carcinoma types. (eyewiki.org)
Clinical1
- This is a patient with surgical stage T1, clinical N0, low-grade parotid mucoepidermoid carcinoma. (medscape.com)
Primary4
- Genotypic characterization of a primary mucoepidermoid carcinoma of the parotid gland by cytogenetic, fluorescence in situ hybridization, and DNA ploidy analysis. (nih.gov)
- Primary mucoepidermoid carcinoma of the intrahepatic bile duct: a case report with review of literature. (nih.gov)
- 9. Clinicopathologic and genetic features of primary bronchopulmonary mucoepidermoid carcinoma: the MD Anderson Cancer Center experience and comprehensive review of the literature. (nih.gov)
- Secondary metastasis to the lacrimal gland are quite rare but are mostly found to be associated to primary breast and lung carcinomas. (eyewiki.org)
Common malignant salivary1
- Mucoepidermoid carcinoma is the most common malignant salivary gland cancer with very limited therapeutic options. (rogelcancercenter.org)
Bronchial1
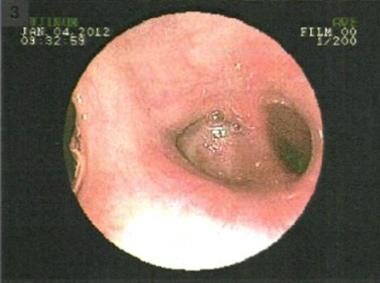
- High-resolution CT scan of the thorax obtained during inspiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (arrow). (medscape.com)
Medullary1
- Medullary carcinoma cannot develop in the thyroglossal duct because C cells are absent in this structure. (pathologyoutlines.com)
CRTC1-MAML21
- The CRTC1-MAML2 fusion is the major oncogenic driver in mucoepidermoid carcinoma. (ufl.edu)
Cystic1
- A carcinoma morphologically characterized the presence of cuboidal mucous cells, goblet-like mucous cells, squamoid cells, cystic changes, and a fibrotic stromal formation. (nih.gov)
Epithelial1
- Prickle cells, keratin forma i) Mucoepidermoid carcinoma is a tumour having tion and epithelial pearls are generally seen. (ehd.org)
Metastases1
- Lawlor CM, Nelson RE, Doucet ME and Friedlander PL. A rare case of mucoepidermoid carcinoma of the lingual tonsil with cervical lymph node metastases . (hoajonline.com)
Lacrimal2
- Mucoepidermoid carcinoma can also be found in other organs, such as bronchi, lacrimal sac, and thyroid gland. (wikipedia.org)
- In this study, we evaluated the clinicopathologic and molecular characteristics of lacrimal apparatus mucoepidermoid carcinoma (MEC) to define its typical diagnostic features. (nih.gov)
Lung2
- In this report, we describe the case of a 44 year-old woman who incidentally found endobronchial lesion at left upper lobe bronchus which was diagnosed as mucoepidermoid carcinoma of the lung. (madridge.org)
- Staging Lung carcinoma is the leading cause of cancer-related death in men and women worldwide. (msdmanuals.com)
Mucous1
- Mucoepidermoid carcinomas - These develop in the cells that produce mucous for the larynx and thyroid gland. (tgh.org)
Metastasis1
- I'm looking for anyone who has beaten the survival odds (about 12 months) with mucoepidermoid carcinoma of the salivary gland WITH significant distant metastasis. (cancer.org)
Cells5
- Hyalinizing clear cell carcinoma shows groups and trabeculae of polygonal, glycogen-rich cells separated by dense collagen bands. (ispub.com)
- Clear cell myoepithelial carcinoma shows sheets of clear cells sometimes admixed with spindle shaped and other myoepithelial cells. (ispub.com)
- Clear-cell variants of acinic cell carcinoma are usually never pure and cells with periodic acid Schiff positive and diastase resistant cytoplasmic zymogen granules are also present. (ispub.com)
- To review this, a MTT assay was performed using several concentrations of 6-MP in mucoepidermoid carcinoma NCI-H292 cells. (exposed-skin-care.net)
- In a thymic carcinoma, the cells no longer look like normal thymic cells. (itmig.org)
Tumour2
- Mucoepidermoid carcinoma (MEC) is the most common tumour of salivary gland. (oraljournal.com)
- Similarly, under Carcinoma, specific renamed or deleted in later revisions of tumour classifications. (who.int)
Cancer4
- In the Brownell Lab, she is involved in the study of merkel cell carcinoma (MCC), a rare and aggressive skin cancer. (nih.gov)
- Assessment of cancer cell line representativeness using microarrays for Merkel cell carcinoma. (nih.gov)
- Une étude rétrospective descriptive en milieu hospitalier a été menée sur tous les cas de cancer de la tête et du cou dans deux hôpitaux de Damas pendant une période de trois ans (2008-2010). (who.int)
- Thymic carcinomas grow in general more quickly than thymomas and sometimes have spread to other parts of the body when the cancer is found. (itmig.org)
Cysts1
- Carcinoma develops in less than 1% of thyroglossal duct cysts, with a F:M ratio = 2:1 and a mean age of 40 years ( Thyroid FNA Cytology 2019:143 ). (pathologyoutlines.com)
Lesion2
Adenocystic1
- Adenocystic carcinoma. (indiasurgerytour.com)
Nasopharyngeal1
- 1. To determine the prognostic implication of plasma Epstein-Bar Virus (EBV) DNA concentrations, as measured by quantitative polymerase chain reaction (PCR) in patients with nasopharyngeal carcinoma (NPC). (stanford.edu)
Molecular1
- Telomere length assessment and molecular characterization of TERT gene promoter in periampullary carcinomas. (who.int)
Merkel2
- Merkel cell carcinoma. (indiasurgerytour.com)
- Hedgehog Signaling Inhibitors Fail to Reduce Merkel Cell Carcinoma Viability. (nih.gov)