Pancreatic Neoplasms
Neoplasms
Neoplasms, Cystic, Mucinous, and Serous
Neoplasms, Multiple Primary
Neoplasms, Second Primary
Adenocarcinoma, Mucinous
Myeloproliferative Disorders
Cystadenoma
Neoplasms, Connective and Soft Tissue
Neoplasms, Plasma Cell
Cystadenoma, Mucinous
Ovarian Neoplasms
Gastrointestinal Neoplasms
Carcinoma, Pancreatic Ductal
Neoplasms, Experimental
Neoplasms, Vascular Tissue
Immunohistochemistry
Neoplasms, Radiation-Induced
Adenocarcinoma, Papillary
Carcinoma, Papillary
Testicular Neoplasms
Neoplasms, Muscle Tissue
Neoplasms, Glandular and Epithelial
Cystadenocarcinoma, Mucinous
Alterations of Rb pathway (Rb-p16INK4-cyclin D1) in preinvasive bronchial lesions. (1/530)
Lung cancer results from a stepwise accumulation of genetic and molecular abnormalities with unknown temporal relationships to precursor bronchial lesions. In a search for biomarkers of malignant progression, we analyzed the expression of the tumor suppressor gene Rb and of the proteins regulating its phosphorylation and function in G1 arrest, p16INK4A and cyclin D1, in preinvasive bronchial lesions accompanying cancer in 75 patients, in comparison with similar lesions in 22 patients with no cancer history. Rb was constantly expressed in preinvasive lesions, including carcinoma in situ (CIS). In contrast, p16 expression was lost in moderate dysplasia (12%) and in CIS (30%) in patients with lung cancer. p16 loss occurred exclusively in patients who displayed loss of p16 expression in their related invasive carcinoma. Loss of p16 expression was not seen in nine patients with dysplasia but no cancer progression. Cyclin D1 overexpression was seen in hyperplasia and metaplasia (6%), mild dysplasia (17%), moderate dysplasia (46%), and CIS (38%) in patients with cancer but was lost in 5% of the patients during the process of invasion; it was also observed in patients with no cancer progression (14%). Our results indicate that Rb protein function can be invalidated before invasion through alteration of the Rb phosphorylation pathway, by p16 inhibition, and/or by cyclin D1 overexpression and suggest a role for p16 and cyclin D1 deregulation in progression of preinvasive bronchial lesions to invasive carcinoma. (+info)Differential responses of normal, premalignant, and malignant human bronchial epithelial cells to receptor-selective retinoids. (2/530)
Using an in vitro lung carcinogenesis model consisting of normal, premalignant, and malignant human bronchial epithelial (HBE) cells, we analyzed the growth inhibitory effects of 26 novel synthetic retinoic acid receptor (RAR)- and retinoid X receptor (RXR)-selective retinoids. RAR-selective retinoids such as CD271, CD437, CD2325, and SR11364 showed potent activity in inhibiting the growth of either normal or premalignant and malignant HBE cells (IC50s mostly <1 microM) and were much more potent than RXR-selective retinoids. Nonetheless, the combination of RAR- and RXR-selective retinoids exhibited additive effects in HBE cells. As the HBE cells became progressively more malignant, they exhibited decreased or lost sensitivity to many retinoids. The activity of the RAR-selective retinoids, with the exception of the most potent retinoid, CD437, could be suppressed by an RAR panantagonist. These results suggest that: (a) RAR/RXR heterodimers play an important role in mediating the growth inhibitory effects of most retinoids in HBE cells; (b) CD437 may act through an RAR-independent pathway; (c) some of the RAR-selective retinoids may have the potential to be used in the clinic as chemopreventive and chemotherapeutic agents for lung cancer; and (d) early stages of lung carcinogenesis may be responsive targets for chemoprevention by retinoids, as opposed to later stages. (+info)Cyclin D1 proteolysis: a retinoid chemoprevention signal in normal, immortalized, and transformed human bronchial epithelial cells. (3/530)
BACKGROUND: Retinoids (derivatives of vitamin A) are reported to reduce the occurrence of some second primary cancers, including aerodigestive tract tumors. In contrast, beta-carotene does not reduce the occurrence of primary aerodigestive tract cancers. Mechanisms explaining these effective retinoid and ineffective carotenoid chemoprevention results are poorly defined. Recently, the all-trans-retinoic acid (RA)-induced proteolysis of cyclin D1 that leads to the arrest of cells in G1 phase of the cell cycle was described in human bronchial epithelial cells and is a promising candidate for such a mechanism. In this study, we have investigated this proteolysis as a common signal used by carotenoids or receptor-selective and receptor-nonselective retinoids. METHODS: We treated cultured normal human bronchial epithelial cells, immortalized human bronchial epithelial cells (BEAS-2B), and transformed human bronchial epithelial cells (BEAS-2BNNK) with receptor-selective or receptor-nonselective retinoids or with carotenoids and studied the effects on cell proliferation by means of tritiated thymidine incorporation and on cyclin D1 expression by means of immunoblot analysis. We also examined whether calpain inhibitor I, an inhibitor of the 26S proteasome degradation pathway, affected the decline (i.e., proteolysis) of cyclin D1. RESULTS: Receptor-nonselective retinoids were superior to the carotenoids studied in mediating the decline in cyclin D1 expression and in suppressing the growth of bronchial epithelial cells. Retinoids that activated retinoic acid receptor beta or retinoid X receptor pathways preferentially led to a decrease in the amount of cyclin D1 protein and a corresponding decline in growth. The retinoid-mediated degradation of cyclin D1 was blocked by cotreatment with calpain inhibitor I. CONCLUSIONS: Retinoid-dependent cyclin D1 proteolysis is a common chemoprevention signal in normal and neoplastic human bronchial epithelial cells. In contrast, carotenoids did not affect cyclin D1 expression. Thus, the degradation of cyclin D1 is a candidate intermediate marker for effective retinoid-mediated cancer chemoprevention in the aerodigestive tract. (+info)Survey of outpatient sputum cytology: influence of written instructions on sample quality and who benefits from investigation. (4/530)
OBJECTIVES: To evaluated quality of outpatient sputum cytology and whether written instructions to patients improve sample quality and to identify variables that predict satisfactory samples. DESIGN: Prospective randomised study. SETTING: Outpatient department of a district general hospital. PATIENTS: 224 patients recruited over 18 months whenever their clinicians requested sputum cytology, randomized to receive oral or oral and written advice. INTERVENTIONS: Oral advice from nurse on producing a sputum sample (114 patients); oral advice plus written instructions (110). MAIN MEASURES: Percentages of satisfactory sputum samples and of patients who produced more than one satisfactory sample; clinical or radiological features identified from subsequent review of patients' notes and radiographs associated with satisfactory samples; final diagnosis of bronchial cancer. RESULTS: 588 sputum samples were requested and 477 received. Patients in the group receiving additional written instructions produced 75(34%) satisfactory samples and 43(39%) of them one or more sets of satisfactory samples. Corresponding figures for the group receiving only oral advice (80(31%) and 46(40%) respectively)were not significantly different. Logistic regression showed that radiological evidence of collapse or consolidation (p<0.01) and hilar mass (p<0.05) were significant predictors of the production of satisfactory samples. Sputum cytology confirmed the diagnosis in only 9(17%) patients with bronchial carcinoma. CONCLUSIONS: The quality of outpatients' sputum samples was poor and was not improved by written instructions. Sputum cytology should be limited to patients with probable bronchial cancer unsuitable for surgery. IMPLICATIONS: Collection of samples and requests for sputum cytology should be reviewed in other hospitals. (+info)Sex-related differences in bronchial epithelial changes associated with tobacco smoking. (5/530)
BACKGROUND: Lung cancer is the most common cause of cancer death in North American women. Because smoking-related changes in the bronchial epithelium and in lung function have not been studied in detail in women, we used fluorescence bronchoscopy-directed biopsy to determine the prevalence of high-grade preinvasive lesions in former and current smokers of both sexes. METHODS: Spirometry, white-light bronchoscopy, and fluorescence bronchoscopy were performed in 189 women and 212 men older than 40 years of age who had smoked 20 pack-years or more (pack-years = number of packs of cigarettes smoked per day x number of years of smoking). RESULTS: Carcinoma in situ was found in 1.8% of the subjects, severe dysplasia was found in 6.5%, and moderate dysplasia was found in 14% (all preinvasive lesions). Compared with men, women had a lower prevalence of high-grade preinvasive lesions in the observed airways (14% versus 31%; odds ratio = 0.18; 95% confidence interval = 0.04-0.88), and women with preinvasive lesions had fewer such lesions (two-sided P = .048). The prevalence of preinvasive lesions did not change substantially for more than 10 years after cessation of smoking. Lung function was associated with the prevalence of preinvasive lesions, but the association was weaker in women than in men. If the presence of airflow obstruction was defined by an FEV1/FVC (forced expiratory volume in 1 second/forced vital capacity) value of 70% or less, only 56% of the men and 44% of the women with preinvasive lesions had abnormal lung function. CONCLUSION: In developing strategies for chemoprevention or early detection of lung cancer in high-risk populations, it is important to consider the effect of sex and arbitrarily chosen lung function values on the prevalence of preinvasive airway lesions. (+info)Malignant tumors of the liver and lungs in an area with a PVC industry. (6/530)
The incidence of malignant tumors of the lung and bronchus and of cytologically confirmed primary malignant tumor of the liver was analyzed for a 4-yr period in a city with several factories, including a PVC industry. Prior to the study two cases of angio-sarcoma of the liver were diagnosed in workers employed in PVC production. The total incidence of analyzed tumors was only slightly higher than predicted. The tumors of the liver recorded did not show any dependence on place of work or residence. During the period of observation, malignant tumors of the bronchus (lung) were not recorded in the PVC industry. Their rate in the area in which the PVC industry is situated was approximately the same as that for the entire city area. The study does not indicate that the occurrence of malignant tumors other than angiosarcoma is associated with exposure to vinyl chloride. (+info)Overexpression of cyclins D1 and E is frequent in bronchial preneoplasia and precedes squamous cell carcinoma development. (7/530)
Increased protein expression of the G1 cyclins D1 and E is reported in invasive non-small cell lung carcinoma. However, during transformation of the bronchial epithelium, overexpression of these species occurs, and their relationship to aberrant expression of p53 and retinoblastoma (Rb) has not been described previously. To determine the expression of these cell cycle regulators during the development of invasive squamous cell carcinoma (SCC) of the lung, the immunohistochemical expression patterns in normal bronchial epithelium (n = 36), squamous metaplasia (SM; n = 28), and epithelial atypia (n = 34) were compared with that in low-grade dysplasia (LGD; n = 17), high-grade bronchial dysplasia (HGD; n = 30), and SCC (n = 36). Monoclonal anti-p53 Pab1801, polyclonal anti-cyclin D1 DCS6, monoclonal anti-cyclin E HE12, and monoclonal anti-Rb OP-66 antibodies were used. Cyclin D1 was not expressed in normal bronchial epithelium but was detected in 7% of SMs, 15% of atypias; 18% of LGDs, 47% of HGDs, and 42% of SCCs. Cyclin E was not detected in normal epithelium (n = 24), SM (n = 16), or LGD (n = 12), but it was found in 9% of atypias (2 of 22), 33% of HGDs (7 of 21), and 54% of SCCs (13 of 24). p53 was not expressed in normal epithelium, SM, and LGD, but it was overexpressed in 6% of atypias, 53% of HGDs, and 61% of SCCs. Abnormal Rb expression was found only in 2 of 36 cases of SCC. A total of 91% of HGDs and 92% of SCCs exhibited overexpression of at least one of the p53, cyclin D1, or cyclin E species. However, no link was observed between overexpression of p53 and the overexpressed G1 cyclins in preneoplastic lesions. Overexpression of cyclin D1, cyclin E, and p53 occurs frequently and independently in pulmonary SCC and is detected in lesions before the development of invasive carcinoma. In contrast, altered Rb expression is a late and infrequent event in squamous cell carcinogenesis. (+info)Bronchial capillary hemangioma in adults. (8/530)
Two cases with capillary hemangioma of the trachea and the left upper lobe bronchus are presented. The adult patients were referred to the hospital because of hemoptysis and cough. The chest radiographs were normal in both cases. The bronchoscopic examination revealed circumscribed lesions with a capillarized surface protruding into the lumen of the trachea and the left upper lobe bronchus, respectively. The lesions were excised in toto with flexible bronchoscopic forceps. The specimens contained typical capillary hemangiomas without any signs of malignancy. Capillary hemangioma in the bronchial tree is an extremely rare benign lesion in adults. Nevertheless, it should be considered as a possible cause of hemoptysis and cough. (+info)Bronchial neoplasms refer to abnormal growths or tumors in the bronchi, which are the large airways that lead into the lungs. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Malignant bronchial neoplasms are often referred to as lung cancer and can be further classified into small cell lung cancer and non-small cell lung cancer, depending on the type of cells involved.
Benign bronchial neoplasms are less common than malignant ones and may include growths such as papillomas, hamartomas, or chondromas. While benign neoplasms are not cancerous, they can still cause symptoms and complications if they grow large enough to obstruct the airways or if they become infected.
Treatment for bronchial neoplasms depends on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
Neoplasms: Neoplasms refer to abnormal growths of tissue that can be benign (non-cancerous) or malignant (cancerous). They occur when the normal control mechanisms that regulate cell growth and division are disrupted, leading to uncontrolled cell proliferation.
Cystic Neoplasms: Cystic neoplasms are tumors that contain fluid-filled sacs or cysts. These tumors can be benign or malignant and can occur in various organs of the body, including the pancreas, ovary, and liver.
Mucinous Neoplasms: Mucinous neoplasms are a type of cystic neoplasm that is characterized by the production of mucin, a gel-like substance produced by certain types of cells. These tumors can occur in various organs, including the ovary, pancreas, and colon. Mucinous neoplasms can be benign or malignant, and malignant forms are often aggressive and have a poor prognosis.
Serous Neoplasms: Serous neoplasms are another type of cystic neoplasm that is characterized by the production of serous fluid, which is a thin, watery fluid. These tumors commonly occur in the ovary and can be benign or malignant. Malignant serous neoplasms are often aggressive and have a poor prognosis.
In summary, neoplasms refer to abnormal tissue growths that can be benign or malignant. Cystic neoplasms contain fluid-filled sacs and can occur in various organs of the body. Mucinous neoplasms produce a gel-like substance called mucin and can also occur in various organs, while serous neoplasms produce thin, watery fluid and commonly occur in the ovary. Both mucinous and serous neoplasms can be benign or malignant, with malignant forms often being aggressive and having a poor prognosis.
Skin neoplasms refer to abnormal growths or tumors in the skin that can be benign (non-cancerous) or malignant (cancerous). They result from uncontrolled multiplication of skin cells, which can form various types of lesions. These growths may appear as lumps, bumps, sores, patches, or discolored areas on the skin.
Benign skin neoplasms include conditions such as moles, warts, and seborrheic keratoses, while malignant skin neoplasms are primarily classified into melanoma, squamous cell carcinoma, and basal cell carcinoma. These three types of cancerous skin growths are collectively known as non-melanoma skin cancers (NMSCs). Melanoma is the most aggressive and dangerous form of skin cancer, while NMSCs tend to be less invasive but more common.
It's essential to monitor any changes in existing skin lesions or the appearance of new growths and consult a healthcare professional for proper evaluation and treatment if needed.
Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
Kidney neoplasms refer to abnormal growths or tumors in the kidney tissues that can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various types of kidney cells, including the renal tubules, glomeruli, and the renal pelvis.
Malignant kidney neoplasms are also known as kidney cancers, with renal cell carcinoma being the most common type. Benign kidney neoplasms include renal adenomas, oncocytomas, and angiomyolipomas. While benign neoplasms are generally not life-threatening, they can still cause problems if they grow large enough to compromise kidney function or if they undergo malignant transformation.
Early detection and appropriate management of kidney neoplasms are crucial for improving patient outcomes and overall prognosis. Regular medical check-ups, imaging studies, and urinalysis can help in the early identification of these growths, allowing for timely intervention and treatment.
A "second primary neoplasm" is a distinct, new cancer or malignancy that develops in a person who has already had a previous cancer. It is not a recurrence or metastasis of the original tumor, but rather an independent cancer that arises in a different location or organ system. The development of second primary neoplasms can be influenced by various factors such as genetic predisposition, environmental exposures, and previous treatments like chemotherapy or radiation therapy.
It is important to note that the definition of "second primary neoplasm" may vary slightly depending on the specific source or context. In general medical usage, it refers to a new, separate cancer; however, in some research or clinical settings, there might be more precise criteria for defining and diagnosing second primary neoplasms.
Adenocarcinoma, mucinous is a type of cancer that begins in the glandular cells that line certain organs and produce mucin, a substance that lubricates and protects tissues. This type of cancer is characterized by the presence of abundant pools of mucin within the tumor. It typically develops in organs such as the colon, rectum, lungs, pancreas, and ovaries.
Mucinous adenocarcinomas tend to have a distinct appearance under the microscope, with large pools of mucin pushing aside the cancer cells. They may also have a different clinical behavior compared to other types of adenocarcinomas, such as being more aggressive or having a worse prognosis in some cases.
It is important to note that while a diagnosis of adenocarcinoma, mucinous can be serious, the prognosis and treatment options may vary depending on several factors, including the location of the cancer, the stage at which it was diagnosed, and the individual's overall health.
Thyroid neoplasms refer to abnormal growths or tumors in the thyroid gland, which can be benign (non-cancerous) or malignant (cancerous). These growths can vary in size and may cause a noticeable lump or nodule in the neck. Thyroid neoplasms can also affect the function of the thyroid gland, leading to hormonal imbalances and related symptoms. The exact causes of thyroid neoplasms are not fully understood, but risk factors include radiation exposure, family history, and certain genetic conditions. It is important to note that most thyroid nodules are benign, but a proper medical evaluation is necessary to determine the nature of the growth and develop an appropriate treatment plan.
Myeloproliferative disorders (MPDs) are a group of rare, chronic blood cancers that originate from the abnormal proliferation or growth of one or more types of blood-forming cells in the bone marrow. These disorders result in an overproduction of mature but dysfunctional blood cells, which can lead to serious complications such as blood clots, bleeding, and organ damage.
There are several subtypes of MPDs, including:
1. Chronic Myeloid Leukemia (CML): A disorder characterized by the overproduction of mature granulocytes (a type of white blood cell) in the bone marrow, leading to an increased number of these cells in the blood. CML is caused by a genetic mutation that results in the formation of the BCR-ABL fusion protein, which drives uncontrolled cell growth and division.
2. Polycythemia Vera (PV): A disorder characterized by the overproduction of all three types of blood cells - red blood cells, white blood cells, and platelets - in the bone marrow. This can lead to an increased risk of blood clots, bleeding, and enlargement of the spleen.
3. Essential Thrombocythemia (ET): A disorder characterized by the overproduction of platelets in the bone marrow, leading to an increased risk of blood clots and bleeding.
4. Primary Myelofibrosis (PMF): A disorder characterized by the replacement of normal bone marrow tissue with scar tissue, leading to impaired blood cell production and anemia, enlargement of the spleen, and increased risk of infections and bleeding.
5. Chronic Neutrophilic Leukemia (CNL): A rare disorder characterized by the overproduction of neutrophils (a type of white blood cell) in the bone marrow, leading to an increased number of these cells in the blood. CNL can lead to an increased risk of infections and organ damage.
MPDs are typically treated with a combination of therapies, including chemotherapy, targeted therapy, immunotherapy, and stem cell transplantation. The choice of treatment depends on several factors, including the subtype of MPD, the patient's age and overall health, and the presence of any comorbidities.
The term "DNA, neoplasm" is not a standard medical term or concept. DNA refers to deoxyribonucleic acid, which is the genetic material present in the cells of living organisms. A neoplasm, on the other hand, is a tumor or growth of abnormal tissue that can be benign (non-cancerous) or malignant (cancerous).
In some contexts, "DNA, neoplasm" may refer to genetic alterations found in cancer cells. These genetic changes can include mutations, amplifications, deletions, or rearrangements of DNA sequences that contribute to the development and progression of cancer. Identifying these genetic abnormalities can help doctors diagnose and treat certain types of cancer more effectively.
However, it's important to note that "DNA, neoplasm" is not a term that would typically be used in medical reports or research papers without further clarification. If you have any specific questions about DNA changes in cancer cells or neoplasms, I would recommend consulting with a healthcare professional or conducting further research on the topic.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
Parotid neoplasms refer to abnormal growths or tumors in the parotid gland, which is the largest of the salivary glands and is located in front of the ear and extends down the neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parotid neoplasms are typically slow-growing, painless masses that may cause facial asymmetry or difficulty in chewing or swallowing if they become large enough to compress surrounding structures. The most common type of benign parotid tumor is a pleomorphic adenoma.
Malignant parotid neoplasms, on the other hand, are more aggressive and can invade nearby tissues and spread to other parts of the body. They may present as rapidly growing masses that are firm or fixed to surrounding structures. Common types of malignant parotid tumors include mucoepidermoid carcinoma, adenoid cystic carcinoma, and squamous cell carcinoma.
The diagnosis of parotid neoplasms typically involves a thorough clinical evaluation, imaging studies such as CT or MRI scans, and fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Treatment options depend on the type, size, and location of the neoplasm but may include surgical excision, radiation therapy, and chemotherapy.
Cystadenoma is a type of benign tumor (not cancerous), which arises from glandular epithelial cells and is covered by a thin layer of connective tissue. These tumors can develop in various locations within the body, including the ovaries, pancreas, and other organs that contain glands.
There are two main types of cystadenomas: serous and mucinous. Serous cystadenomas are filled with a clear or watery fluid, while mucinous cystadenomas contain a thick, gelatinous material. Although they are generally not harmful, these tumors can grow quite large and cause discomfort or other symptoms due to their size or location. In some cases, cystadenomas may undergo malignant transformation and develop into cancerous tumors, known as cystadenocarcinomas. Regular medical follow-up and monitoring are essential for individuals diagnosed with cystadenomas to ensure early detection and treatment of any potential complications.
Neoplasms of connective and soft tissue are abnormal growths or tumors that develop in the body's supportive tissues, such as cartilage, tendons, ligaments, fascia, and fat. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign connective and soft tissue neoplasms include:
- Lipomas: slow-growing, fatty tumors that develop under the skin.
- Fibromas: firm, benign tumors that develop in connective tissue such as tendons or ligaments.
- Nevi (plural of nevus): benign growths made up of cells called melanocytes, which produce pigment.
Malignant connective and soft tissue neoplasms include:
- Sarcomas: a type of cancer that develops in the body's supportive tissues such as muscle, bone, fat, cartilage, or blood vessels. There are many different types of sarcomas, including liposarcoma (fatty tissue), rhabdomyosarcoma (muscle), and osteosarcoma (bone).
- Desmoid tumors: a rare type of benign tumor that can become aggressive and invade surrounding tissues. While not considered cancerous, desmoid tumors can cause significant morbidity due to their tendency to grow and infiltrate nearby structures.
Connective and soft tissue neoplasms can present with various symptoms depending on their location and size. Treatment options include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis (spread) of the tumor.
Plasma cell neoplasms are a type of cancer that originates from plasma cells, which are a type of white blood cell found in the bone marrow. These cells are responsible for producing antibodies to help fight off infections. When plasma cells become cancerous and multiply out of control, they can form a tumor called a plasmacytoma.
There are two main types of plasma cell neoplasms: solitary plasmacytoma and multiple myeloma. Solitary plasmacytoma is a localized tumor that typically forms in the bone, while multiple myeloma is a systemic disease that affects multiple bones and can cause a variety of symptoms such as bone pain, fatigue, and anemia.
Plasma cell neoplasms are diagnosed through a combination of tests, including blood tests, imaging studies, and bone marrow biopsy. Treatment options depend on the stage and extent of the disease, but may include radiation therapy, chemotherapy, and stem cell transplantation.
Appendiceal neoplasms refer to various types of tumors that can develop in the appendix, a small tube-like structure attached to the large intestine. These neoplasms can be benign or malignant and can include:
1. Adenomas: These are benign tumors that arise from the glandular cells lining the appendix. They are usually slow-growing and may not cause any symptoms.
2. Carcinoids: These are neuroendocrine tumors that arise from the hormone-producing cells in the appendix. They are typically small and slow-growing, but some can be aggressive and spread to other parts of the body.
3. Mucinous neoplasms: These are tumors that produce mucin, a slippery substance that can cause the appendix to become distended and filled with mucus. They can be low-grade (less aggressive) or high-grade (more aggressive) and may spread to other parts of the abdomen.
4. Adenocarcinomas: These are malignant tumors that arise from the glandular cells lining the appendix. They are relatively rare but can be aggressive and spread to other parts of the body.
5. Pseudomyxoma peritonei: This is a condition in which mucin produced by an appendiceal neoplasm leaks into the abdominal cavity, causing a jelly-like accumulation of fluid and tissue. It can be caused by both benign and malignant tumors.
Treatment for appendiceal neoplasms depends on the type and stage of the tumor, as well as the patient's overall health. Treatment options may include surgery, chemotherapy, or radiation therapy.
Liver neoplasms refer to abnormal growths in the liver that can be benign or malignant. Benign liver neoplasms are non-cancerous tumors that do not spread to other parts of the body, while malignant liver neoplasms are cancerous tumors that can invade and destroy surrounding tissue and spread to other organs.
Liver neoplasms can be primary, meaning they originate in the liver, or secondary, meaning they have metastasized (spread) to the liver from another part of the body. Primary liver neoplasms can be further classified into different types based on their cell of origin and behavior, including hepatocellular carcinoma, cholangiocarcinoma, and hepatic hemangioma.
The diagnosis of liver neoplasms typically involves a combination of imaging studies, such as ultrasound, CT scan, or MRI, and biopsy to confirm the type and stage of the tumor. Treatment options depend on the type and extent of the neoplasm and may include surgery, radiation therapy, chemotherapy, or liver transplantation.
Mucinous cystadenoma is a type of benign tumor that arises from the epithelial cells lining the mucous membranes of the body. It is most commonly found in the ovary, but can also occur in other locations such as the pancreas or appendix.
Mucinous cystadenomas are characterized by the production of large amounts of mucin, a slippery, gel-like substance that accumulates inside the tumor and causes it to grow into a cystic mass. These tumors can vary in size, ranging from a few centimeters to over 20 centimeters in diameter.
While mucinous cystadenomas are generally benign, they have the potential to become cancerous (mucinous cystadenocarcinoma) if left untreated. Symptoms of mucinous cystadenoma may include abdominal pain or swelling, bloating, and changes in bowel movements or urinary habits. Treatment typically involves surgical removal of the tumor.
Ovarian neoplasms refer to abnormal growths or tumors in the ovary, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various cell types within the ovary, including epithelial cells, germ cells, and stromal cells. Ovarian neoplasms are often classified based on their cell type of origin, histological features, and potential for invasive or metastatic behavior.
Epithelial ovarian neoplasms are the most common type and can be further categorized into several subtypes, such as serous, mucinous, endometrioid, clear cell, and Brenner tumors. Some of these epithelial tumors have a higher risk of becoming malignant and spreading to other parts of the body.
Germ cell ovarian neoplasms arise from the cells that give rise to eggs (oocytes) and can include teratomas, dysgerminomas, yolk sac tumors, and embryonal carcinomas. Stromal ovarian neoplasms develop from the connective tissue cells supporting the ovary and can include granulosa cell tumors, thecomas, and fibromas.
It is essential to diagnose and treat ovarian neoplasms promptly, as some malignant forms can be aggressive and potentially life-threatening if not managed appropriately. Regular gynecological exams, imaging studies, and tumor marker tests are often used for early detection and monitoring of ovarian neoplasms. Treatment options may include surgery, chemotherapy, or radiation therapy, depending on the type, stage, and patient's overall health condition.
Endocrine gland neoplasms refer to abnormal growths (tumors) that develop in the endocrine glands. These glands are responsible for producing hormones, which are chemical messengers that regulate various functions and processes in the body. Neoplasms can be benign or malignant (cancerous). Benign neoplasms tend to grow slowly and do not spread to other parts of the body. Malignant neoplasms, on the other hand, can invade nearby tissues and organs and may also metastasize (spread) to distant sites.
Endocrine gland neoplasms can occur in any of the endocrine glands, including:
1. Pituitary gland: located at the base of the brain, it produces several hormones that regulate growth and development, as well as other bodily functions.
2. Thyroid gland: located in the neck, it produces thyroid hormones that regulate metabolism and calcium balance.
3. Parathyroid glands: located near the thyroid gland, they produce parathyroid hormone that regulates calcium levels in the blood.
4. Adrenal glands: located on top of each kidney, they produce hormones such as adrenaline, cortisol, and aldosterone that regulate stress response, metabolism, and blood pressure.
5. Pancreas: located behind the stomach, it produces insulin and glucagon, which regulate blood sugar levels, and digestive enzymes that help break down food.
6. Pineal gland: located in the brain, it produces melatonin, a hormone that regulates sleep-wake cycles.
7. Gonads (ovaries and testicles): located in the pelvis (ovaries) and scrotum (testicles), they produce sex hormones such as estrogen, progesterone, and testosterone that regulate reproductive function and secondary sexual characteristics.
Endocrine gland neoplasms can cause various symptoms depending on the type and location of the tumor. For example, a pituitary gland neoplasm may cause headaches, vision problems, or hormonal imbalances, while an adrenal gland neoplasm may cause high blood pressure, weight gain, or mood changes.
Diagnosis of endocrine gland neoplasms typically involves a combination of medical history, physical examination, imaging studies such as CT or MRI scans, and laboratory tests to measure hormone levels. Treatment options may include surgery, radiation therapy, chemotherapy, or hormonal therapy, depending on the type and stage of the tumor.
Gastrointestinal (GI) neoplasms refer to abnormal growths in the gastrointestinal tract, which can be benign or malignant. The gastrointestinal tract includes the mouth, esophagus, stomach, small intestine, large intestine, rectum, and anus.
Benign neoplasms are non-cancerous growths that do not invade nearby tissues or spread to other parts of the body. They can sometimes be removed completely and may not cause any further health problems.
Malignant neoplasms, on the other hand, are cancerous growths that can invade nearby tissues and organs and spread to other parts of the body through the bloodstream or lymphatic system. These types of neoplasms can be life-threatening if not diagnosed and treated promptly.
GI neoplasms can cause various symptoms, including abdominal pain, bloating, changes in bowel habits, nausea, vomiting, weight loss, and anemia. The specific symptoms may depend on the location and size of the neoplasm.
There are many types of GI neoplasms, including adenocarcinomas, gastrointestinal stromal tumors (GISTs), lymphomas, and neuroendocrine tumors. The diagnosis of GI neoplasms typically involves a combination of medical history, physical examination, imaging studies, and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or immunotherapy.
Pancreatic ductal carcinoma (PDC) is a specific type of cancer that forms in the ducts that carry digestive enzymes out of the pancreas. It's the most common form of exocrine pancreatic cancer, making up about 90% of all cases.
The symptoms of PDC are often vague and can include abdominal pain, jaundice (yellowing of the skin and eyes), unexplained weight loss, and changes in bowel movements. These symptoms can be similar to those caused by other less serious conditions, which can make diagnosis difficult.
Pancreatic ductal carcinoma is often aggressive and difficult to treat. The prognosis for PDC is generally poor, with a five-year survival rate of only about 9%. Treatment options may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. However, because PDC is often not detected until it has advanced, treatment is frequently focused on palliative care to relieve symptoms and improve quality of life.
Experimental neoplasms refer to abnormal growths or tumors that are induced and studied in a controlled laboratory setting, typically in animals or cell cultures. These studies are conducted to understand the fundamental mechanisms of cancer development, progression, and potential treatment strategies. By manipulating various factors such as genetic mutations, environmental exposures, and pharmacological interventions, researchers can gain valuable insights into the complex processes underlying neoplasm formation and identify novel targets for cancer therapy. It is important to note that experimental neoplasms may not always accurately represent human cancers, and further research is needed to translate these findings into clinically relevant applications.
A neoplasm of vascular tissue is an abnormal growth or mass of cells in the blood vessels or lymphatic vessels. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms, such as hemangiomas and lymphangiomas, are typically not harmful and may not require treatment. However, they can cause symptoms if they grow large enough to press on nearby organs or tissues. Malignant neoplasms, such as angiosarcomas, are cancerous and can invade and destroy surrounding tissue, as well as spread (metastasize) to other parts of the body. Treatment for vascular tissue neoplasms depends on the type, size, location, and stage of the growth, and may include surgery, radiation therapy, chemotherapy, or a combination of these.
Eye neoplasms, also known as ocular tumors or eye cancer, refer to abnormal growths of tissue in the eye. These growths can be benign (non-cancerous) or malignant (cancerous). Eye neoplasms can develop in various parts of the eye, including the eyelid, conjunctiva, cornea, iris, ciliary body, choroid, retina, and optic nerve.
Benign eye neoplasms are typically slow-growing and do not spread to other parts of the body. They may cause symptoms such as vision changes, eye pain, or a noticeable mass in the eye. Treatment options for benign eye neoplasms include monitoring, surgical removal, or radiation therapy.
Malignant eye neoplasms, on the other hand, can grow and spread rapidly to other parts of the body. They may cause symptoms such as vision changes, eye pain, floaters, or flashes of light. Treatment options for malignant eye neoplasms depend on the type and stage of cancer but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
It is important to note that early detection and treatment of eye neoplasms can improve outcomes and prevent complications. Regular eye exams with an ophthalmologist are recommended for early detection and prevention of eye diseases, including eye neoplasms.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
Nose neoplasms refer to abnormal growths or tumors in the nasal cavity or paranasal sinuses. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and have the potential to metastasize.
Nose neoplasms can cause various symptoms such as nasal congestion, nosebleeds, difficulty breathing through the nose, loss of smell, facial pain or numbness, and visual changes if they affect the eye. The diagnosis of nose neoplasms usually involves a combination of physical examination, imaging studies (such as CT or MRI scans), and biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Salivary gland neoplasms refer to abnormal growths or tumors that develop in the salivary glands. These glands are responsible for producing saliva, which helps in digestion, lubrication of food and maintaining oral health. Salivary gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms are slow-growing and typically do not spread to other parts of the body. They may cause symptoms such as swelling, painless lumps, or difficulty swallowing if they grow large enough to put pressure on surrounding tissues.
Malignant neoplasms, on the other hand, can be aggressive and have the potential to invade nearby structures and metastasize (spread) to distant organs. Symptoms of malignant salivary gland neoplasms may include rapid growth, pain, numbness, or paralysis of facial nerves.
Salivary gland neoplasms can occur in any of the major salivary glands (parotid, submandibular, and sublingual glands) or in the minor salivary glands located throughout the mouth and throat. The exact cause of these neoplasms is not fully understood, but risk factors may include exposure to radiation, certain viral infections, and genetic predisposition.
Radiation-induced neoplasms are a type of cancer or tumor that develops as a result of exposure to ionizing radiation. Ionizing radiation is radiation with enough energy to remove tightly bound electrons from atoms or molecules, leading to the formation of ions. This type of radiation can damage DNA and other cellular structures, which can lead to mutations and uncontrolled cell growth, resulting in the development of a neoplasm.
Radiation-induced neoplasms can occur after exposure to high levels of ionizing radiation, such as that received during radiation therapy for cancer treatment or from nuclear accidents. The risk of developing a radiation-induced neoplasm depends on several factors, including the dose and duration of radiation exposure, the type of radiation, and the individual's genetic susceptibility to radiation-induced damage.
Radiation-induced neoplasms can take many years to develop after initial exposure to ionizing radiation, and they often occur at the site of previous radiation therapy. Common types of radiation-induced neoplasms include sarcomas, carcinomas, and thyroid cancer. It is important to note that while ionizing radiation can increase the risk of developing cancer, the overall risk is still relatively low, especially when compared to other well-established cancer risk factors such as smoking and exposure to certain chemicals.
Adenocarcinoma, papillary is a type of cancer that begins in the glandular cells and grows in a finger-like projection (called a papilla). This type of cancer can occur in various organs, including the lungs, pancreas, thyroid, and female reproductive system. The prognosis and treatment options for papillary adenocarcinoma depend on several factors, such as the location and stage of the tumor, as well as the patient's overall health. It is important to consult with a healthcare professional for an accurate diagnosis and personalized treatment plan.
Carcinoma, papillary is a type of cancer that begins in the cells that line the glandular structures or the lining of organs. In a papillary carcinoma, the cancerous cells grow and form small finger-like projections, called papillae, within the tumor. This type of cancer most commonly occurs in the thyroid gland, but can also be found in other organs such as the lung, breast, and kidney. Papillary carcinoma of the thyroid gland is usually slow-growing and has a good prognosis, especially when it is diagnosed at an early stage.
Testicular neoplasms are abnormal growths or tumors in the testicle that can be benign (non-cancerous) or malignant (cancerous). They are a type of genitourinary cancer, which affects the reproductive and urinary systems. Testicular neoplasms can occur in men of any age but are most commonly found in young adults between the ages of 15 and 40.
Testicular neoplasms can be classified into two main categories: germ cell tumors and non-germ cell tumors. Germ cell tumors, which arise from the cells that give rise to sperm, are further divided into seminomas and non-seminomas. Seminomas are typically slow-growing and have a good prognosis, while non-seminomas tend to grow more quickly and can spread to other parts of the body.
Non-germ cell tumors are less common than germ cell tumors and include Leydig cell tumors, Sertoli cell tumors, and lymphomas. These tumors can have a variety of clinical behaviors, ranging from benign to malignant.
Testicular neoplasms often present as a painless mass or swelling in the testicle. Other symptoms may include a feeling of heaviness or discomfort in the scrotum, a dull ache in the lower abdomen or groin, and breast enlargement (gynecomastia).
Diagnosis typically involves a physical examination, imaging studies such as ultrasound or CT scan, and blood tests to detect tumor markers. Treatment options depend on the type and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular self-examinations of the testicles are recommended for early detection and improved outcomes.
Neoplasms in muscle tissue refer to abnormal and excessive growths of muscle cells that can be benign or malignant. These growths can arise from any of the three types of muscle tissue: skeletal, cardiac, or smooth muscle. Neoplasms in muscle tissue are classified based on their origin, behavior, and histological features.
Benign neoplasms in muscle tissue include leiomyomas (smooth muscle), rhabdomyomas (skeletal muscle), and myxomas (cardiac muscle). These tumors are usually slow-growing and do not invade surrounding tissues or spread to other parts of the body.
Malignant neoplasms in muscle tissue, also known as sarcomas, include leiomyosarcoma (smooth muscle), rhabdomyosarcoma (skeletal muscle), and angiosarcoma (cardiac muscle). These tumors are aggressive, invasive, and have the potential to metastasize to other parts of the body.
Symptoms of neoplasms in muscle tissue depend on their location, size, and type. They may include a painless or painful mass, weakness, fatigue, weight loss, and difficulty swallowing or breathing. Treatment options for neoplasms in muscle tissue include surgery, radiation therapy, chemotherapy, and targeted therapy. The choice of treatment depends on the type, stage, location, and patient's overall health condition.
Neoplasms are abnormal growths of cells or tissues that serve no purpose and can be benign (non-cancerous) or malignant (cancerous). Glandular and epithelial neoplasms refer to specific types of tumors that originate from the glandular and epithelial tissues, respectively.
Glandular neoplasms arise from the glandular tissue, which is responsible for producing and secreting substances such as hormones, enzymes, or other fluids. These neoplasms can be further classified into adenomas (benign) and adenocarcinomas (malignant).
Epithelial neoplasms, on the other hand, develop from the epithelial tissue that lines the outer surfaces of organs and the inner surfaces of cavities. These neoplasms can also be benign or malignant and are classified as papillomas (benign) and carcinomas (malignant).
It is important to note that while both glandular and epithelial neoplasms can become cancerous, not all of them do. However, if they do, the malignant versions can invade surrounding tissues and spread to other parts of the body, making them potentially life-threatening.
Mucinous cystadenocarcinoma is a type of cancer that arises from the mucin-producing cells in the lining of a cyst. It is a subtype of cystadenocarcinoma, which is a malignant tumor that develops within a cyst. Mucinous cystadenocarcinomas are typically found in the ovary or pancreas but can also occur in other organs such as the appendix and the respiratory tract.
These tumors are characterized by the production of large amounts of mucin, a gel-like substance that can accumulate within the cyst and cause it to grow. Mucinous cystadenocarcinomas tend to grow slowly but can become quite large and may eventually spread (metastasize) to other parts of the body if left untreated.
Symptoms of mucinous cystadenocarcinoma depend on the location and size of the tumor, but they may include abdominal pain or discomfort, bloating, changes in bowel movements, or vaginal bleeding. Treatment typically involves surgical removal of the tumor, followed by chemotherapy or radiation therapy to kill any remaining cancer cells. The prognosis for mucinous cystadenocarcinoma depends on several factors, including the stage of the disease at diagnosis and the patient's overall health.
An adenoma is a benign (noncancerous) tumor that develops from glandular epithelial cells. These types of cells are responsible for producing and releasing fluids, such as hormones or digestive enzymes, into the surrounding tissues. Adenomas can occur in various organs and glands throughout the body, including the thyroid, pituitary, adrenal, and digestive systems.
Depending on their location, adenomas may cause different symptoms or remain asymptomatic. Some common examples of adenomas include:
1. Colorectal adenoma (also known as a polyp): These growths occur in the lining of the colon or rectum and can develop into colorectal cancer if left untreated. Regular screenings, such as colonoscopies, are essential for early detection and removal of these polyps.
2. Thyroid adenoma: This type of adenoma affects the thyroid gland and may result in an overproduction or underproduction of hormones, leading to conditions like hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid).
3. Pituitary adenoma: These growths occur in the pituitary gland, which is located at the base of the brain and controls various hormonal functions. Depending on their size and location, pituitary adenomas can cause vision problems, headaches, or hormonal imbalances that affect growth, reproduction, and metabolism.
4. Liver adenoma: These rare benign tumors develop in the liver and may not cause any symptoms unless they become large enough to press on surrounding organs or structures. In some cases, liver adenomas can rupture and cause internal bleeding.
5. Adrenal adenoma: These growths occur in the adrenal glands, which are located above the kidneys and produce hormones that regulate stress responses, metabolism, and blood pressure. Most adrenal adenomas are nonfunctioning, meaning they do not secrete excess hormones. However, functioning adrenal adenomas can lead to conditions like Cushing's syndrome or Conn's syndrome, depending on the type of hormone being overproduced.
It is essential to monitor and manage benign tumors like adenomas to prevent potential complications, such as rupture, bleeding, or hormonal imbalances. Treatment options may include surveillance with imaging studies, medication to manage hormonal issues, or surgical removal of the tumor in certain cases.
 Bronchial leiomyoma
Bronchial leiomyoma
Lambert-Eaton myasthenic syndrome
Acinic cell carcinoma of the lung
Multiple endocrine neoplasia
Subcutaneous emphysema
Fetal adenocarcinoma
International Classification of Diseases for Oncology
Bovhyaluronidase azoximer
Neuroendocrine tumor
List of cancer types
Comorbidity
Giant-cell carcinoma of the lung
Basaloid squamous cell lung carcinoma
Small-cell carcinoma
Lymphangioleiomyomatosis
Sialadenitis
Mucoepidermoid carcinoma
Peptide receptor radionuclide therapy
Stem cell marker
List of MeSH codes (C23)
Somatic evolution in cancer
Non-small-cell lung cancer
Carcinogenesis
Treatment of lung cancer
Glossary of medicine
Bronchial leiomyoma - Wikipedia
 Diaphragmatic Injury Imaging: Practice Essentials, Radiography, Computed Tomography
Diaphragmatic Injury Imaging: Practice Essentials, Radiography, Computed Tomography
 Occult carcinoma of the bronchus
Occult carcinoma of the bronchus
NIOSHTIC-2 Search Results - Full View
 Comprehensive analysis of HE4 expression in normal and malignant human tissues | Modern Pathology
Comprehensive analysis of HE4 expression in normal and malignant human tissues | Modern Pathology
 E-Pilo-2 - Side Effects, Uses, Dosage, Overdose, Pregnancy, Alcohol | RxWiki
E-Pilo-2 - Side Effects, Uses, Dosage, Overdose, Pregnancy, Alcohol | RxWiki
Figure - Cryptosporidium baileyi Pulmonary Infection in Immunocompetent Woman with Benign Neoplasm - Volume 26, Number 8-August...
Gigantism and Acromegaly: Practice Essentials, Background, Pathophysiology and Etiology
Abstract Search
 Gary Hartman - Stanford Medicine Children's Health
Gary Hartman - Stanford Medicine Children's Health
Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine | Journal of Nuclear Medicine
 A Study to Evaluate the Efficacy and Safety of Multiple Targeted Therapies as Treatments for Participants With Non-Small Cell...
A Study to Evaluate the Efficacy and Safety of Multiple Targeted Therapies as Treatments for Participants With Non-Small Cell...
 Impingement Syndrome - Shoulder | KLINIK am RING
Impingement Syndrome - Shoulder | KLINIK am RING
 Clinical and Economic Consequences of Inhaled Corticosteroid Doses and | COPD
Clinical and Economic Consequences of Inhaled Corticosteroid Doses and | COPD
 Namespace
Namespace
Human Genome Epidemiology Literature Finder|Home|PHGKB
 Paediatric Surgery
Paediatric Surgery
 Atlas of Vascular Anatomy: An Angiographic Approach - Google Books
Atlas of Vascular Anatomy: An Angiographic Approach - Google Books
 Pulm III: Neoplasms Cheat Sheet by ksellybelly - Download free from Cheatography - Cheatography.com: Cheat Sheets For Every...
Pulm III: Neoplasms Cheat Sheet by ksellybelly - Download free from Cheatography - Cheatography.com: Cheat Sheets For Every...
 Alan W. Katz, M.D., M.P.H. | UR Medicine
Alan W. Katz, M.D., M.P.H. | UR Medicine
 Pancreatic ductal adenocarcinoma can be detected by analysis of volatile organic compounds (VOCs) in alveolar air | BMC Cancer ...
Pancreatic ductal adenocarcinoma can be detected by analysis of volatile organic compounds (VOCs) in alveolar air | BMC Cancer ...
 DeCS
DeCS
 An unusual cause of acromegaly | HKMJ
An unusual cause of acromegaly | HKMJ
Suppression of Tumorigenicity of a Human Lung Carcinoma Line by Nontumorigenic Bronchial Epithelial Cells in Somatic Cell...
 Neoplasm staging. Medical search. Definitions
Neoplasm staging. Medical search. Definitions
 SIADH- Syndrome of Inappropriate ADH - NEET PG - www.MedicalTalk.Net the Best Medical Forum for Medical Students and Doctors...
SIADH- Syndrome of Inappropriate ADH - NEET PG - www.MedicalTalk.Net the Best Medical Forum for Medical Students and Doctors...
 Global Anatomic Pathology Equipment And Consumables Opportunities And Strategies Market Report
Global Anatomic Pathology Equipment And Consumables Opportunities And Strategies Market Report
 Neuroendocrine Tumors Clinical Trial Pipeline Insights | 55+ Key Companies Investigating Their Lead Candidates to Improve the...
Neuroendocrine Tumors Clinical Trial Pipeline Insights | 55+ Key Companies Investigating Their Lead Candidates to Improve the...
Tumors5
- Bronchopulmonary endocrine tumors represent 25 30% of lung neoplasms. (endocrine-abstracts.org)
- Bronchial carcinoid tumors are rare, accounting for up to 2.5% of all pulmonary neoplasms and for 12-15% of carcinoid tumors overall. (medscape.com)
- Bronchial carcinoid tumors appear in the images below. (medscape.com)
- Bronchial carcinoids belong to a group of neuroendocrine tumors, which range from bronchial carcinoid tumors at one end of the spectrum to, at the other end, small cell carcinomas or, possibly, large cell neuroendocrine tumors. (medscape.com)
- Neuroendocrine neoplasms (NENs) include all tumors derived from the diffuse endocrine system. (springeropen.com)
Typical and atypical carcinoids1
- In the huge spectrum of lung neuroendocrine neoplasms, typical and atypical carcinoids should be considered as a separate biological entity from poorly differentiated forms, harboring peculiar molecular alterations. (springeropen.com)
Carcinoma5
- Pathological evidence indicates that bronchial carcinoma at this occult stage can be diagnosed cytologically, is rarely multifocal and, as a localized neoplasm, is amenable to curative therapy. (nih.gov)
- 1) Squamous cell carcinoma: 25-35% of cases, hemopt-ysis, bronchial in origin. (cheatography.com)
- Tracheal reconstruction and replacement is a complex and vital surgical procedure with several indications, including primary tracheal neoplasm (adenoid cystic carcinoma and squamous cell carcinoma), thyroid cancer, extensive tracheoesophageal fistulas, unsuccessful previous surgery for benign tracheal diseases (re-stenosis, long-term stenosis that has been dilated or been non-surgically repaired) and, rarely, congenital tracheal stenosis. (ersjournals.com)
- What's the difference between a carcinoma and neoplasms? (imperial.ac.uk)
- The term neoplasm includes both benign and malignant "new growths) A carcinoma is a malignant neoplasm of epithelial cells. (imperial.ac.uk)
Pulmonary neoplasms1
- It is the commonest of all pulmonary neoplasms. (jdshospital.com)
Carcinomas2
- 18 With the exception of the ovarian neoplasms, the same carcinomas analyzed for gene expression were also examined for HE4 by immunohistochemistry on tissue microarrays (see below). (nature.com)
- It represents approximately 15% of all bronchial carcinomas, and this percentage is usually tending to decrease recently. (thetechnoant.info)
Skin Neoplasms1
- Skin Neoplasms Malignant And Unspec. (drugcite.com)
Benign neoplasm1
- Findings from a 51-year-old immunocompetent woman with a benign neoplasm and Cryptosporidium baileyi pulmonary infection, Poland, 2015. (cdc.gov)
Malignant neoplasm2
- Salivary gland type malignant neoplasm arising from bronchial seromucinous glands. (cancerhealthcenter.com)
- INTRODUCTION Small cell lung malignancy (SCLC) is highly malignant neoplasm, derived from neuroendocrine cells. (thetechnoant.info)
Neuroendocrine neoplasms1
- Since the pioneering use of 131 I in differentiated thyroid cancer in the 1940s, remarkable achievements in nuclear medicine endoradiotherapy have been demonstrated, mainly in the treatment of neuroendocrine neoplasms by using 177 Lu-labeled somatostatin analogs or in the treatment of advanced prostate cancer using prostate-specific membrane antigen-directed radionuclide therapy. (snmjournals.org)
Lung cancer1
- Bronchial carcinoids are not associated with smoking, whereas small cell lung cancer (neuroendocrine type 3) has a definite relationship to smoking. (medscape.com)
Diseases1
- Of course, from a differential diagnosis point of view it is important to consider that in addition to the impingement syndrome numerous other causes such as internal diseases (CHD, liver, bronchial CA etc.) or neurogenic disorders (cervical disc prolapse, neoplasms, etc.) may be responsible for shoulder pain. (klinik-am-ring.de)
Histological type1
- The second neoplasm may have the same or different histological type and can occur in the same or different organs as the previous neoplasm but in all cases arises from an independent oncogenic event. (lookformedical.com)
Adenoma1
- Also, see eMedicineHealth's patient education article Bronchial Adenoma . (medscape.com)
Leiomyoma2
- A bronchial leiomyoma is a relatively rare form of lung tumours. (wikipedia.org)
- The first bronchial leiomyoma was described by in 1909. (wikipedia.org)
Pneumonia1
- 50 years of age with slow sociation with underlying neoplasm or less or non-resolving pneumonia [ 5 ]. (who.int)
Pancreatic1
- The detection and statistical rendering of alveolar VOC composition can be useful for the clinical diagnostic approach of pancreatic neoplasms with excellent sensitivity and specificity. (biomedcentral.com)
Mucinous2
- RESULTS: On pathological evaluation, a peribronchial mucinous neoplasm with a unique morphology was found. (bvsalud.org)
- RNA NGS analysis showed anETV6-NTRK3 translocation in a low-grade mucinous bronchial adenocarcinoma. (bvsalud.org)
Cysts1
- Abdominal & Intestinal surgeries for mesenteric/omental cysts, duplication cysts, irreducible intussusceptions & neoplasms. (klehospital.org)
Histologically2
- Although growth hormone-releasing hormone (GHRH) level was not available, the patient most likely suffered from a GHRH-secreting bronchial carcinoid as suggested by the presence of a histologically confirmed bronchial carcinoid tumour, and normalisation of serum IGF-1 level and normal GH response following an OGTT upon complete removal of his lung tumour. (hkmj.org)
- The neoplasms may be histologically the same or different, and may be found in the same or different sites. (lookformedical.com)
Bronchopulmonary1
- In this work, we extensively reviewed scientific literature exploring available therapeutic options, new molecular targets and future perspectives in the management of well differentiated neoplasms of bronchopulmonary tree. (springeropen.com)
Tumour4
- We report a rare case of acromegaly due to a growth hormone releasing hormone-secreting bronchial carcinoid tumour. (hkmj.org)
- Right lower lobectomy was performed, and the tumour was confirmed to be a bronchial carcinoid tumour on histology. (hkmj.org)
- Histology confirmed the tumour to be an atypical bronchial carcinoid. (hkmj.org)
- This is a malignant tumour arising from the bronchial epithelium. (jdshospital.com)
Peribronchial1
- These arteries (except the thyroid artery) form a peribronchial plexus that follows the bronchial tree deep into the lung parenchyma to supply blood also to the visceral pleura and the walls of the pulmonary arteries and veins (vasa vasorum). (medscape.com)
Metastases2
- Abnormal growths of tissue that follow a previous neoplasm but are not metastases of the latter. (lookformedical.com)
- Bronchial carcinoids are now classed as low-grade malignant neoplasms because of their potential to cause local invasion, their tendency for local recurrence, and their occasional metastases to extrathoracic sites. (medscape.com)
Systemic1
- Malignant neoplasms (both for systemic use and for local external exposure). (macrocosmscience.com)
Abnormal1
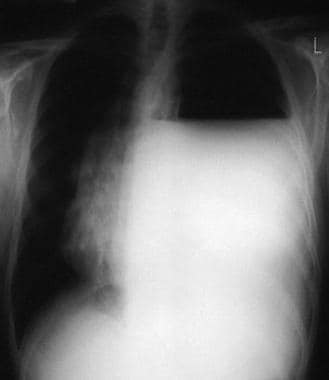
- Chest radiographs (CXRs) are abnormal in 90% of patients with bronchial carcinoid. (medscape.com)
Cancer1
- A neuroendocrine cancer, also known as a neuroendocrine tumor (NET) or neuroendocrine neoplasm, starts in the body's neuroendocrine system's specialized cells. (medgadget.com)
Metastasis1
- Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms . (lookformedical.com)
Serum1
- Neoplasms containing cyst-like formations or producing mucin or serum. (lookformedical.com)
Primary1
- Transfer of a neoplasm from its primary site to lymph nodes or to distant parts of the body by way of the lymphatic system. (lookformedical.com)
Syndrome1
- In light of the co-existence of bronchial carcinoid and a history of a pituitary lesion, multiple endocrine neoplasia type 1 (MEN-1) syndrome was suspected, but genetic testing could not detect any mutations. (hkmj.org)
Methods2
- The possibility of identifying subjects affected by different kinds of neoplasms requires the use of various analytic methods with very different characteristics. (biomedcentral.com)
- Methods which attempt to express in replicable terms the extent of the neoplasm in the patient. (lookformedical.com)
Factors1
- The development of the second neoplasm may or may not be related to the treatment for the previous neoplasm since genetic risk or predisposing factors may actually be the cause. (lookformedical.com)
Thyroid1
- The vascular supply of the trachea and bronchial tree depends on branches from the inferior thyroid arteries, intercostal arteries, and bronchial arteries (aortic branches). (medscape.com)
Term1
- They originate from the neurosecretory cells of bronchial mucosa and were previously classified as bronchial adenomas, a term no longer used. (medscape.com)
Spectrum2
- D) Cryptosporidium oocyst detected in patient's bronchial washings after immunofluorescent labeling with excitation and emission spectrum peak wave lengths of 495 nm/519 nm. (cdc.gov)
- In the huge spectrum of lung NENs, the most important distinction split between well differentiated and poorly differentiated neoplasms. (springeropen.com)
Tree2
- Bronchial tree with nomenclature. (medscape.com)
- Different systems of nomenclature have been applied to the bronchial tree over the years. (medscape.com)
Type1
- But de l'etude : rapporter un cas clinique de neurofibromatose de type 1 (NF1) en service de chirurgie generale complique de volumineuses tumeurs royales invalidantes. (bvsalud.org)