Berylliosis
Beryllium
HLA-DP Antigens
Chemical Hazard Release
Hantavirus Pulmonary Syndrome
Granuloma, Respiratory Tract
Disasters
Coca
Disaster Planning
Public Health
Communication
Pandemics
Differential susceptibilities to chronic beryllium disease contributed by different Glu69 HLA-DPB1 and -DPA1 alleles. (1/92)
Chronic beryllium disease (CBD) is associated with the allelic substitution of a Glu69 in the HLA-DPB1 gene. Although up to 97% of CBD patients may have the Glu69 marker, about 30-45% of beryllium-exposed, unaffected individuals carry the same marker. Because CBD occurs in only 1-6% of exposed workers, the presence of Glu69 does not appear to be the sole genetic factor underlying the disease development. Using two rounds of direct automated DNA sequencing to precisely assign HLA-DPB1 haplotypes, we have discovered highly significant Glu69-containing allele frequency differences between the CBD patients and a beryllium-exposed, nondiseased control group. Individuals with DPB1 Glu69 in both alleles were almost exclusively found in the CBD group (6/20) vs the control group (1/75). Whereas most Glu69 carriers from the control group had a DPB1 allele *0201 (68%), most Glu69 carriers from the CBD group had a non-*0201 DPB1 Glu69-carrying allele (84%). The DPB1 allele *0201 was almost exclusively (29/30) associated with DPA1 *01 alleles, while the non-*0201 Glu69-containing DPB1 alleles were closely associated with DPA1 *02 alleles (26/29). Relatively rare Glu69-containing alleles *1701, *0901, and *1001 had extremely high frequencies in the CBD group (50%), as compared with the control group (6.7%). Therefore, the most common Glu69-containing DPB1 allele, *0201, does not seem to be a major disease allele. The results suggest that it is not the mere presence of Glu69, per se, but specific Glu69-containing alleles and their copy number (homozygous or heterozygous) that confer the greatest susceptibility to CBD in exposed individuals. (+info)Partial IL-10 inhibition of the cell-mediated immune response in chronic beryllium disease. (2/92)
Chronic beryllium disease (CBD) provides a human disorder in which to study the delayed type IV hypersensitivity response to persistent Ag that leads to noncaseating pulmonary granuloma formation. We hypothesized that, in CBD, failure of IL-10 to modulate the beryllium-specific, cell-mediated immune response would result in persistent, maximal cytokine production and T lymphocyte proliferation, thus contributing to the development of granulomatous lung disease. To test this hypothesis, we used bronchoalveolar lavage cells from control and CBD subjects to evaluate the beryllium salt-specific production of endogenous IL-10 and the effects of exogenous human rIL-10 (rhIL-10) on HLA expression, on the production of IL-2, IFN-gamma, and TNF-alpha, and on T lymphocyte proliferation. Our data demonstrate that beryllium-stimulated bronchoalveolar lavage cells produce IL-10, and the neutralization of endogenous IL-10 does not increase significantly cytokine production, HLA expression, or T lymphocyte proliferation. Second, the addition of excess exogenous rhIL-10 partially inhibited the beryllium-stimulated production of IL-2, IFN-gamma, and TNF-alpha; however, we measured no change in T lymphocyte proliferation or in the percentage of alveolar macrophages expressing HLA-DP. Interestingly, beryllium salts interfered with an IL-10-stimulated decrease in the percentage of alveolar macrophages expressing HLA-DR. We conclude that, in the CBD-derived, beryllium-stimulated cell-mediated immune response, low levels of endogenous IL-10 have no appreciable effect; exogenous rhIL-10 has a limited effect on cytokine production and no effect on T lymphocyte proliferation or HLA expression. (+info)Chronic beryllium disease and cancer risk estimates with uncertainty for beryllium released to the air from the Rocky Flats Plant. (3/92)
Beryllium was released into the air from routine operations and three accidental fires at the Rocky Flats Plant (RFP) in Colorado from 1958 to 1989. We evaluated environmental monitoring data and developed estimates of airborne concentrations and their uncertainties and calculated lifetime cancer risks and risks of chronic beryllium disease to hypothetical receptors. This article discusses exposure-response relationships for lung cancer and chronic beryllium disease. We assigned a distribution to cancer slope factor values based on the relative risk estimates from an occupational epidemiologic study used by the U.S. Environmental Protection Agency (EPA) to determine the slope factors. We used the regional atmospheric transport code for Hanford emission tracking atmospheric transport model for exposure calculations because it is particularly well suited for long-term annual-average dispersion estimates and it incorporates spatially varying meteorologic and environmental parameters. We accounted for model prediction uncertainty by using several multiplicative stochastic correction factors that accounted for uncertainty in the dispersion estimate, the meteorology, deposition, and plume depletion. We used Monte Carlo techniques to propagate model prediction uncertainty through to the final risk calculations. We developed nine exposure scenarios of hypothetical but typical residents of the RFP area to consider the lifestyle, time spent outdoors, location, age, and sex of people who may have been exposed. We determined geometric mean incremental lifetime cancer incidence risk estimates for beryllium inhalation for each scenario. The risk estimates were < 10(-6). Predicted air concentrations were well below the current reference concentration derived by the EPA for beryllium sensitization. (+info)Association of man-made mineral fibre exposure and sarcoidlike granulomas. (4/92)
It is assumed that sarcoidosis is caused by inhalation of air borne agents in susceptible persons triggering the inflammatory reaction. The association of metallic dust exposure, such as beryllium and aluminium, and sarcoidlike pulmonary disorders is well known. The ability of man-made mineral fibres (MMMF) to cause granulomatous lung disease has not been appreciated until now. Recently, we observed the association of sarcoidlike granulomatous reaction and occupational history of glass fibre exposure. We hypothesized that there might be a relationship between MMMF exposure and the development of sarcoidlike granulomas. Therefore, the records of 50 sarcoidosis patients-who visited our outpatient clinic between 1996 and 1999 were reviewed. This revealed that 14 cases recalled a history of exposure to either glass fibres or rock wool, both MMMF fibres. The available obtained tissue specimens (n = 12) were reviewed. In six cases electron microscopy qualitative analysis of small fragments of the tissue revealed among others silica, aluminium and sometimes titanium. A distinct relation between fibre deposits fibre deposits and granulomas was found. These findings indicate that in susceptible people MMMF exposure might be related to a chronic granulomatous disease similar to chronic beryllium disease. (+info)Government laboratory worker with lung cancer: comparing risks from beryllium, asbestos, and tobacco smoke. (5/92)
Occupational medicine physicians are frequently asked to establish cancer causation in patients with both workplace and non-workplace exposures. This is especially difficult in cases involving beryllium for which the data on human carcinogenicity are limited and controversial. In this report we present the case of a 73-year-old former technician at a government research facility who was recently diagnosed with lung cancer. The patient is a former smoker who has worked with both beryllium and asbestos. He was referred to the University of California, San Francisco, Occupational and Environmental Medicine Clinic at San Francisco General Hospital for an evaluation of whether past workplace exposures may have contributed to his current disease. The goal of this paper is to provide an example of the use of data-based risk estimates to determine causation in patients with multiple exposures. To do this, we review the current knowledge of lung cancer risks in former smokers and asbestos workers, and evaluate the controversies surrounding the epidemiologic data linking beryllium and cancer. Based on this information, we estimated that the patient's risk of lung cancer from asbestos was less than his risk from tobacco smoke, whereas his risk from beryllium was approximately equal to his risk from smoking. Based on these estimates, the patient's workplace was considered a probable contributing factor to his development of lung cancer. (+info)Beryllium presentation to CD4+ T cells underlies disease-susceptibility HLA-DP alleles in chronic beryllium disease. (6/92)
Chronic beryllium disease results from beryllium exposure in the workplace and is characterized by CD4(+) T cell-mediated inflammation in the lung. Susceptibility to this disease is associated with particular HLA-DP alleles. We isolated beryllium-specific T cell lines from the lungs of affected patients. These CD4(+) T cell lines specifically responded to beryllium in culture in the presence of antigen-presenting cells that expressed class II MHC molecules HLA-DR, -DQ, and -DP. The response to beryllium was nearly completely and selectively blocked by mAb to HLA-DP. Additional studies showed that only certain HLA-DP alleles allowed presentation of beryllium. Overall, the DP alleles that presented beryllium to disease-specific T cell lines match those implicated in disease susceptibility, providing a mechanism for this association. Based on amino acid residues shared by these restricting and susceptibility DP alleles, our results provide insight into the residues of the DP beta-chain required for beryllium presentation. (+info)HLA-DP allele-specific T cell responses to beryllium account for DP-associated susceptibility to chronic beryllium disease. (7/92)
Occupational exposure to small molecules, such as metals, is frequently associated with hypersensitivity reactions. Chronic beryllium (Be) disease (CBD) is a multisystem granulomatous disease that primarily affects the lung, and occurs in approximately 3% of individuals exposed to this element. Immunogenetic studies have demonstrated a strong association between CBD and possession of alleles of HLA-DP containing glutamic acid (Glu) at position 69 in the HLA-DP beta-chain. T cell clones were raised from three patients with CBD in whom exposure occurred 10 and 30 years previously. Of 25 Be-specific clones that were obtained, all were restricted by HLA-DP alleles with Glu at DP beta69. Furthermore, the proliferative responses of the clones were absolutely dependent upon DP beta Glu(69) in that a single amino acid substitution at this position abolished the response. As befits a disease whose pathogenesis involves a delayed type hypersensitivity response, the large majority of Be-specific clones secreted IFN-gamma (Th1) and little or no IL-4 (Th2) cytokines. This study provides insights into the molecular basis of DP2-associated susceptibility to CBD. (+info)IL-4 fails to regulate in vitro beryllium-induced cytokines in berylliosis. (8/92)
Bronchoalveolar lavage (BAL) cells from patients with chronic beryllium disease (CBD) have been used to evaluate the beryllium-specific immune response and potential immunotherapeutics. Beryllium induces interferon-gamma (IFN-gamma), interleukin-2 (IL-2), tumour necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6) and interleukin-10 (IL-10) from BAL cells. An antibody to IL-2 and recombinant human (rHu) IL-10 is able to partially suppress the beryllium-stimulated immune response. To obtain BAL cells, bronchoscopy is required, providing risk to the patient and a limited number of cells to study the immune response. As a result, the objectives of the study were to determine 1) whether CBD peripheral blood mononuclear cells (PBMNs) stimulated with beryllium would produce a similar cytokine pattern as BAL cells, and 2) whether this response could be modulated by interleukin-4 (IL-4), an immunomodulatory cytokine. CBD and normal individuals' PBMN and BAL cells were stimulated with and without beryllium sulfate. To modulate this antigen-stimulated response, we added rHu IL-4 to the unstimulated and beryllium-stimulated cells. IFN-gamma, IL-2, TNF-alpha, IL-6 and IL-10 cytokine concentrations were determined from cell supernatants by enzyme-linked immunosorbent assays (ELISA), while IL-4 messenger ribonucleic acid (mRNA) was assessed using polymerase chain reaction (PCR). Beryllium did not stimulate any of these cytokines from normal PBMNs. Increasing levels of IL-6 and TNF-alpha were produced constituitively by CBD PBMNs over time. Compared to the unstimulated CBD PBMNs, beryllium stimulated significant IFN-gamma, TNF-alpha, IL-2, IL-6 and IL-10 production. This response was similar to that stimulated from CBD BAL cells, although of a much lower magnitude. Low levels of IL-4 mRNA were found in CBD and control PBMNs, which were not increased with beryllium stimulation. The beryllium-stimulated cytokine levels were not decreased by the addition of IL-4. IL-4 was unable to downregulate any of these beryllium-stimulated cytokines from CBD BAL cells or increase IL-4 mRNA from either CBD PBMN or BAL cells, and thus is an unlikely immunomodulatory agent in CBD. From the data, it was concluded that chronic beryllium disease peripheral blood mononuclear cells provide a model to study the beryllium-stimulated immune response. Interleukin-4's inability to downregulate any of the beryllium-stimulated cytokines makes it an unlikely therapeutic candidate in chronic beryllium disease. (+info)Berylliosis is a chronic inflammatory disease that affects the lungs and, less commonly, other organs. It is caused by exposure to beryllium, a lightweight, strong metal used in various industries such as aerospace, electronics, and nuclear energy. The disease can be categorized into two types: acute and chronic.
Acute berylliosis is a rare form of the disease that occurs after high levels of exposure to beryllium, usually through inhalation. Symptoms typically develop within a few weeks to months after exposure and include cough, chest pain, shortness of breath, and fatigue. Acute berylliosis can be severe and may require hospitalization.
Chronic berylliosis, also known as beryllium sensitization or beryllium disease, is a more common form of the disease that occurs after long-term exposure to low levels of beryllium. It is characterized by the development of an immune response to beryllium, resulting in chronic inflammation and scarring of the lung tissue. Symptoms may not appear for several years after exposure and can include cough, shortness of breath, fatigue, weight loss, and joint pain.
Diagnosis of berylliosis typically involves a combination of medical history, physical examination, chest X-ray or CT scan, pulmonary function tests, and blood tests to detect the presence of beryllium sensitization. Treatment may include corticosteroids and other immunosuppressive medications to manage inflammation and scarring in the lungs. Avoiding further exposure to beryllium is essential to prevent disease progression.
Beryllium is a chemical element with the symbol Be and atomic number 4. It is a steel-gray, hard, brittle alkaline earth metal that is difficult to fabricate because of its high reactivity and toxicity. Beryllium is primarily used as a hardening agent in alloys, such as beryllium copper, and as a moderator and reflector in nuclear reactors due to its ability to efficiently slow down neutrons.
In the medical field, beryllium is most well-known for its potential to cause a chronic allergic lung disease called berylliosis. This condition can occur after prolonged exposure to beryllium-containing dusts or fumes, and can lead to symptoms such as cough, shortness of breath, and fatigue. In severe cases, it can cause scarring and thickening of the lung tissue, leading to respiratory failure.
Healthcare professionals should take appropriate precautions when handling beryllium-containing materials, including using protective equipment and following proper disposal procedures to minimize exposure.
HLA-DP antigens are a type of human leukocyte antigen (HLA) class II molecule that plays a crucial role in the immune system. The HLAs are proteins found on the surface of cells that help the immune system distinguish between the body's own cells and foreign substances, such as viruses and bacteria.
The HLA-DP antigens are composed of two polypeptide chains, alpha and beta, which are encoded by genes located on chromosome 6 in the human genome. These antigens are expressed on the surface of various cells, including B lymphocytes, dendritic cells, and macrophages.
HLA-DP antigens present peptides to CD4+ T cells, which then become activated and help coordinate the immune response. The HLA-DP antigens have a wide range of peptide specificity, meaning they can bind and present a diverse array of peptides to the immune system.
Variation in HLA genes is common, and differences in these genes can affect an individual's susceptibility or resistance to various diseases, including autoimmune disorders, infectious diseases, and cancer. Therefore, understanding the role of HLA-DP antigens in the immune response is important for developing new therapies and treatments for a variety of medical conditions.
A "chemical hazard release" is a situation where there is an uncontrolled or accidental release of chemicals into the environment, which can pose a threat to human health and the ecosystem. This can occur due to various reasons such as equipment failure, human error, natural disasters, or intentional acts. The released chemicals can be in the form of gas, liquid, or solid and can vary in their level of toxicity, flammability, reactivity, and corrosiveness. Examples of chemical hazard releases include leakage from chemical storage tanks, spills during transportation, accidental fires or explosions at industrial facilities, and illegal dumping of chemicals into water bodies or landfills. It is important to have proper safety measures and emergency response plans in place to minimize the risks associated with chemical hazard releases.
HLA-DP beta-chains are proteins that are encoded by the HLA-DPB1 gene in humans. HLA, or Human Leukocyte Antigens, are a group of proteins found on the surface of cells that play an important role in the body's immune system. They help the body recognize and distinguish between its own cells and foreign substances such as viruses and bacteria.
HLA-DP beta-chains are one part of the HLA-DP complex, which is a type of MHC class II molecule. MHC class II molecules present pieces of proteins from outside the cell to T-cells, a type of white blood cell that plays a central role in the immune response. The HLA-DP complex is composed of an alpha and beta chain, and the beta-chain is encoded by the HLA-DPB1 gene.
Variations in the HLA-DPB1 gene can affect an individual's susceptibility to certain diseases, including autoimmune disorders and infectious diseases. Additionally, HLA-DP beta-chains can be used as markers for tissue typing in organ transplantation to help match donors and recipients and reduce the risk of rejection.
Hantavirus Pulmonary Syndrome (HPS) is a severe, sometimes fatal, respiratory disease in humans caused by infection with hantaviruses. These viruses are spread to people through the aerosolized urine, droppings, or saliva of infected rodents. The virus cannot be transmitted between humans unless there is direct contact with an infected person's blood or bodily fluids. Early symptoms include fatigue, fever, and muscle aches, followed by coughing and shortness of breath as the lungs fill with fluid leading to severe respiratory distress. It's crucial to seek immediate medical attention if you suspect HPS because it can progress rapidly to serious illness or death within days.
A granuloma in the respiratory tract refers to a small nodular lesion that forms in the lung tissue due to an ongoing immune response. It is typically composed of macrophages, lymphocytes, and other inflammatory cells that cluster together around a foreign substance or organism that the body cannot eliminate.
Granulomas can form in response to various stimuli, including infectious agents such as mycobacteria (tuberculosis, nontuberculous mycobacteria), fungi, and parasites, as well as non-infectious causes like inhaled particles (e.g., silica, beryllium) or autoimmune diseases (e.g., sarcoidosis).
These lesions can cause damage to the lung tissue over time, leading to symptoms such as cough, shortness of breath, chest pain, and fatigue. Diagnosis often involves imaging studies like chest X-rays or CT scans, followed by biopsy and microscopic examination to confirm the presence of granulomas and identify the underlying cause. Treatment depends on the underlying cause but may include antibiotics, corticosteroids, or other immunosuppressive medications.
A disaster is a serious disruption of the functioning of a community or a society involving widespread human, material, economic or environmental losses and impacts, which exceeds the ability of the affected community or society to cope using its own resources. Disasters can be natural, such as earthquakes, hurricanes, tsunamis, and wildfires, or they can be caused by human activities, such as technological accidents, intentional acts of violence, and complex emergencies.
The medical definition of a disaster focuses on the health impacts and consequences of the event, which can include injury, illness, disability, and death, as well as psychological distress and social disruption. The response to a disaster typically involves a coordinated effort by multiple agencies and organizations, including healthcare providers, emergency responders, public health officials, and government authorities, to address the immediate needs of affected individuals and communities and to restore basic services and infrastructure.
Disasters can have long-term effects on the health and well-being of individuals and populations, including increased vulnerability to future disasters, chronic illness and disability, and mental health problems such as post-traumatic stress disorder (PTSD), depression, and anxiety. Preparedness, mitigation, response, and recovery efforts are critical components of disaster management, with the goal of reducing the risks and impacts of disasters and improving the resilience of communities and societies to withstand and recover from them.
"Coca" is a medication and plant extract that comes from the leaves of the Erythroxylon coca bush, which is native to South America. The active alkaloids in the leaves include cocaine and other related compounds. Coca leaves have been used for centuries by indigenous peoples in the Andean region for their mild stimulant effects and as a remedy for altitude sickness.
However, it's important to note that chewing coca leaves or using coca-based medications is not the same as using illicit forms of cocaine. The concentration of cocaine in coca leaves is relatively low, and traditional use does not typically lead to the severe psychological and physical effects associated with cocaine abuse.
In modern medicine, coca alkaloids are used in the form of purified cocaine for topical anesthesia in eye surgery and other medical procedures. However, the recreational use of cocaine is illegal and highly regulated due to its addictive properties and potential for harm.
Disaster planning in a medical context refers to the process of creating and implementing a comprehensive plan for responding to emergencies or large-scale disasters that can impact healthcare facilities, services, and patient care. The goal of disaster planning is to minimize the impact of such events on the health and well-being of patients and communities, ensure continuity of medical services, and protect healthcare infrastructure and resources.
Disaster planning typically involves:
1. Risk assessment: Identifying potential hazards and assessing their likelihood and potential impact on healthcare facilities and services.
2. Developing a disaster plan: Creating a detailed plan that outlines the steps to be taken before, during, and after a disaster to ensure the safety of patients, staff, and visitors, as well as the continuity of medical care.
3. Training and education: Providing training and education to healthcare personnel on disaster preparedness, response, and recovery.
4. Exercises and drills: Conducting regular exercises and drills to test the effectiveness of the disaster plan and identify areas for improvement.
5. Resource management: Identifying and securing necessary resources, such as medical supplies, equipment, and personnel, to support disaster response efforts.
6. Communication and coordination: Establishing clear communication protocols and coordinating with local emergency responders, public health authorities, and other healthcare facilities to ensure a coordinated response to disasters.
7. Recovery and restoration: Developing plans for restoring medical services and infrastructure after a disaster has occurred.
Disaster planning is an essential component of healthcare delivery and is critical to ensuring the safety and well-being of patients and communities during emergencies or large-scale disasters.
Public health is defined by the World Health Organization (WHO) as "the art and science of preventing disease, prolonging life and promoting human health through organized efforts of society." It focuses on improving the health and well-being of entire communities, populations, and societies, rather than individual patients. This is achieved through various strategies, including education, prevention, surveillance of diseases, and promotion of healthy behaviors and environments. Public health also addresses broader determinants of health, such as access to healthcare, housing, food, and income, which have a significant impact on the overall health of populations.
In the medical context, communication refers to the process of exchanging information, ideas, or feelings between two or more individuals in order to facilitate understanding, cooperation, and decision-making. Effective communication is critical in healthcare settings to ensure that patients receive accurate diagnoses, treatment plans, and follow-up care. It involves not only verbal and written communication but also nonverbal cues such as body language and facial expressions.
Healthcare providers must communicate clearly and empathetically with their patients to build trust, address concerns, and ensure that they understand their medical condition and treatment options. Similarly, healthcare teams must communicate effectively with each other to coordinate care, avoid errors, and provide the best possible outcomes for their patients. Communication skills are essential for all healthcare professionals, including physicians, nurses, therapists, and social workers.
A pandemic is a global outbreak of a disease that spreads easily from person to person across a large region, such as multiple continents or worldwide. It is declared by the World Health Organization (WHO) when the spread of a disease poses a significant threat to the global population due to its severity and transmissibility.
Pandemics typically occur when a new strain of virus emerges that has not been previously seen in humans, for which there is little or no pre-existing immunity. This makes it difficult to control the spread of the disease, as people do not have natural protection against it. Examples of pandemics include the 1918 Spanish flu pandemic and the more recent COVID-19 pandemic caused by the SARS-CoV-2 virus.
During a pandemic, healthcare systems can become overwhelmed, and there may be significant social and economic disruption as governments take measures to slow the spread of the disease, such as travel restrictions, quarantines, and lockdowns. Effective vaccines and treatments are critical in controlling the spread of pandemics and reducing their impact on public health.
Community-institutional relations in a medical context generally refers to the interactions and relationships between healthcare institutions, such as hospitals or clinics, and the communities they serve. This can include initiatives and programs aimed at promoting community health, addressing social determinants of health, and building trust and engagement with community members. It may also involve collaborations and partnerships with other organizations, such as community-based organizations, public health agencies, and local government entities, to address shared health concerns and improve overall community wellbeing. Effective community-institutional relations can help to ensure that healthcare institutions are responsive to the needs of their communities and contribute to positive health outcomes.
 Berylliosis
Berylliosis
Pit (nuclear weapon)
Beryllium
Harriet Louise Hardy
Schaumann body
Period 2 element
MELISA
Beryllium granuloma
Beryllium oxide
Calcitriol
Kveim test
Bhaisajyaguru
Acute beryllium poisoning
Herbert L. Anderson
W. W. Hansen
Jörgen Nielsen Schaumann
Organoberyllium chemistry
Progressive massive fibrosis
Occupational lung disease
List of diseases (C)
Bilateral hilar lymphadenopathy
List of medical mnemonics
Beryllium poisoning
List of MeSH codes (C08)
List of diseases (B)
Pneumoconiosis
Dust Diseases Tribunal of New South Wales
Hypercalcaemia
Interferon gamma
List of hepato-biliary diseases
Berylliosis - Wikipedia
 Berylliosis: Background, Pathophysiology, Etiology
Berylliosis: Background, Pathophysiology, Etiology
 Berylliosis | Health Information Center
Berylliosis | Health Information Center
 Chronic berylliosis | UKF IMS
Chronic berylliosis | UKF IMSBerylliosis - Occupational Respiratory Diseases - Respiratory Diseases - Diseases - McMaster Textbook of Internal Medicine
International Classification of Diseases (ICD) Codes
 Article - Billing and Coding: Vitamin D Assay Testing (A57484)
Article - Billing and Coding: Vitamin D Assay Testing (A57484)
 Prednisone Tablets, USP Rx only
Prednisone Tablets, USP Rx only
DailyMed - PREDNISONE tablet
 Beryllium Disease among Workers in a Spacecraft-
Manufacturing Plant -- California
Beryllium Disease among Workers in a Spacecraft-
Manufacturing Plant -- California
 Beryllium disease | Safety and health at work EU-OSHA
Beryllium disease | Safety and health at work EU-OSHA
NIOSHTIC-2 Search Results - Full View
![Gondouin A[au] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Gondouin A[au] - Search Results - PubMed
Gondouin A[au] - Search Results - PubMed
 Reportable Diseases and Conditions
Reportable Diseases and Conditions
Beryllium Toxicity: Literature Cited | Environmental Medicine | ATSDR
 About Clean Air. Clear Lungs. | Safe Work Australia
About Clean Air. Clear Lungs. | Safe Work Australia
Call Transcript: November 17, 2016|Clinicians Outreach and Outreach Communication (COCA)
Occupational lung disease
 Table of Contents - March 01, 2001, 17 (3) | European Respiratory Society
Table of Contents - March 01, 2001, 17 (3) | European Respiratory Society
Histoplasmosis Imaging: Practice Essentials, Radiography, Computed Tomography
Chronic Beryllium Disease
Diagnosis of Beryllium Disease | Chronic Beryllium Disease
Call Transcript: November 17, 2016|Clinicians Outreach and Outreach Communication (COCA)
 OS2.GURU - Abit KT7-Raid / eComStation / IBM OS/2 Warp
OS2.GURU - Abit KT7-Raid / eComStation / IBM OS/2 Warp
 Beryllium Disease - Lung and Airway Disorders - MSD Manual Consumer Version
Beryllium Disease - Lung and Airway Disorders - MSD Manual Consumer Version
 Baby’s Pregnancy Calendar
Baby’s Pregnancy Calendar
 Pathoma - Respiratory Pathology Flashcards by Jon L | Brainscape
Pathoma - Respiratory Pathology Flashcards by Jon L | Brainscape
 Career Corner: Pitching Your Contributions at the Right Level (Journal Article) | DOE PAGES
Career Corner: Pitching Your Contributions at the Right Level (Journal Article) | DOE PAGESChronic beryllium2
- Berylliosis, or chronic beryllium disease (CBD), is a chronic allergic-type lung response and chronic lung disease caused by exposure to beryllium and its compounds, a form of beryllium poisoning. (wikipedia.org)
- Inhalation of beryllium (Be) has been associated with two pulmonary syndromes, which are an acute chemical pneumonitis and a granulomatous lung disease known as chronic beryllium disease (CBD), or berylliosis. (medscape.com)
Risk of berylliosis1
- The risk of berylliosis is highest in those who work near beryllium. (cvs.com)
Systemic3
- Berylliosis is a systemic disease characterized mainly by inflammatory and granulomatous lesions in the lungs following inhalation of metallic beryllium dust, its alloys, or compounds. (empendium.com)
- Editorial Note: Chronic berylliosis is a pulmonary and systemic granulomatous disease caused by exposure to beryllium. (cdc.gov)
- Berylliosis is a systemic disorder that in its chronic form produces granulomatous disease in the lungs. (nih.gov)
Acute2
Beryllium exposure1
- Berylliosis is a lung disease due to beryllium exposure. (cvs.com)
Exposure2
- In some individuals, a single exposure to beryllium can cause berylliosis. (wikipedia.org)
- The risk of developing berylliosis depends on the level and duration of exposure to beryllium dusts. (empendium.com)
Sarcoidosis4
- Granulomas are seen in other chronic diseases, such as tuberculosis and sarcoidosis, and it can occasionally be hard to distinguish berylliosis from these disorders. (wikipedia.org)
- The differential diagnosis for berylliosis includes: Sarcoidosis Granulomatous lung diseases Tuberculosis Fungal infections (e.g., histoplasmosis) Granulomatosis with polyangiitis Idiopathic pulmonary fibrosis Hypersensitivity pneumonitis Asthma Of these possibilities, berylliosis presents most similarly to sarcoidosis. (wikipedia.org)
- Some studies suggest that up to 6% of all cases of sarcoidosis are actually berylliosis. (wikipedia.org)
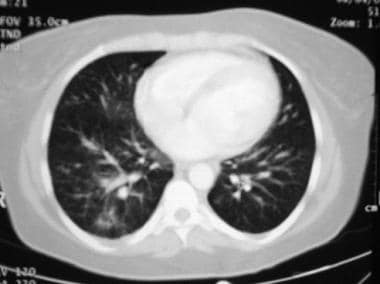
- One study found that ground-glass opacities were more commonly seen on CT scan in berylliosis than in sarcoidosis. (wikipedia.org)
Parenchymal1
- Findings that are common in CT scans of people with berylliosis include parenchymal nodules in early stages. (wikipedia.org)
Granulomatous1
- Definitive diagnosis of berylliosis is based on history of beryllium exposures, documented beryllium sensitivity and granulomatous inflammation on lung biopsy. (wikipedia.org)
Pulmonary1
- Given the invasive nature of a lung biopsy, diagnosis can also be based on clinical history consistent with berylliosis, abnormal chest x-ray or CT scan findings, and abnormalities in pulmonary function tests. (wikipedia.org)
Lungs1
- Chronic berylliosis leads to scarring of the lungs. (cvs.com)
NIOSH1
- From 1977 to 1981, three cases of beryllium disease (berylliosis) among workers in a large spacecraft-manufacturing plant in California, were reported to the Beryllium Case Registry (BCR) of the National Institute for Occupational Safety and Health (NIOSH). (cdc.gov)
Occupational1
- Berylliosis is an occupational lung disease. (wikipedia.org)
Diseases1
- Available at: https://rarediseases.org/rare-diseases/berylliosis. (cvs.com)
Cases1
- Cases of chronic berylliosis were first described in 1946 among workers in plants manufacturing fluorescent lamps in Massachusetts (3). (cdc.gov)
Silicosis4
- Such exposures can lead to an allergic reaction and occupational asthma or other respiratory diseases, including silicosis, berylliosis, rhinitis, sinusitis, byssinosis (brown lung), chronic obstructive airways disease and emphysema. (brachers.co.uk)
- The upper lobes of the lungs are the common site for coal worker pneumoconiosis, similar to the site of berylliosis and silicosis. (picmonic.com)
- AMBOSS says "A syndrome that occurs in individuals with both rheumatoid arthritis and occupational pneumoconiosis (e.g., silicosis, asbestosis, berylliosis, anthracosis). (ankihub.net)
- asbestosis (asbestos dust), silicosis (silica dust), berylliosis (beryllium dust), coal miner's pneumoconiosis / black lung disease (coal dust), siderosis (iron dust) anthracosis (carbon dust). (accident-claim-expert.co.uk)
Chronic8
- Berylliosis, or chronic beryllium disease (CBD), is a chronic allergic-type lung response and chronic lung disease caused by exposure to beryllium and its compounds, a form of beryllium poisoning. (wikipedia.org)
- Sizar O, Talati R. Berylliosis (chronic beryllium disease). (medscape.com)
- A high-resolution CT scan of the chest showing the typical ground glass appearance in a patient with chronic beryllium disease, or berylliosis. (medscape.com)
- A histopathology slide (hematosin and eosin stain) showing the typical well-formed granuloma of chronic beryllium disease, or berylliosis. (medscape.com)
- Although acute beryllium disease occurs rarely today, chronic beryllium disease (CBD, or berylliosis) continues to occur in industries where beryllium and its alloys are smelted, fabricated and machined. (nih.gov)
- There is a disease associated with it called berylliosis and this is a chronic condition affecting the lungs. (highpowermedia.com)
- Chronic Beryllium Disease (CBD), or Berylliosis, is a pulmonary disease caused by beryllium exposure and causes granulomas to form in the lungs, scarring them. (unitedallianceservices.com)
- The commercial use of beryllium requires the use of appropriate dust control equipment and industrial controls at all times because of the toxicity of inhaled beryllium-containing dusts that can cause a chronic life-threatening allergic disease in some people called berylliosis. (periodic-table.org)
Silica dust1
- For example, if an employee suffers from the effects of inhaling asbestos or silica dust or from berylliosis, that employee can file a claim up to three years after the last day he or she was exposed. (gwclaw.com)
Lung3
- Berylliosis is an occupational lung disease. (wikipedia.org)
- Given the invasive nature of a lung biopsy, diagnosis can also be based on clinical history consistent with berylliosis, abnormal chest x-ray or CT scan findings, and abnormalities in pulmonary function tests. (wikipedia.org)
- An overall population 36 berylliosis patients and 38 Be-sensitization without lung granulomas and 86 Be-exposed controls was analysed to assess the role of the individual HLA-class II polymorphisms associated with BH-susceptibility in HLA-DPGlu69 negative subjects by univariate and multivariate analysis. (nih.gov)
People1
- Findings that are common in CT scans of people with berylliosis include parenchymal nodules in early stages. (wikipedia.org)