Arachnoid Cysts
Arachnoid
Cysts
Syringomyelia
Arachnoiditis
Central Nervous System Cysts
Subarachnoid Space
Cranial Fossa, Middle
Hematoma, Subdural
Cranial Fossa, Posterior
Subdural Effusion
Dura Mater
Spinal Cord Compression
Hernia
Magnetic Resonance Imaging
Neuroendoscopy
Cerebral Ventriculography
Decompression, Surgical
Laminectomy
Iophendylate
Spinal Cord Diseases
Headache
Cerebrospinal Fluid Shunts
Hypothalamic Diseases
Epidermal Cyst
Cisterna Magna
Petrous Bone
Sella Turcica
Hydrocephalus
Hematoma, Subdural, Chronic
Cerebellar Diseases
Tomography, X-Ray Computed
Ventriculoperitoneal Shunt
Cranial Nerve Diseases
Barotrauma
Paroxysmal kinesigenic choreoathetosis associated with frontotemporal arachnoid cyst--case report. (1/167)
A 17-year-old male presented with paroxysmal kinesigenic choreoathetosis (PKC) associated with frontotemporal arachnoid cyst. Xenon-133 single photon emission computed tomography detected a slight but equivocal decrease in regional cerebral blood flow in the vicinity of basal ganglia associated with the PKC episodes. PKC continued after surgical removal of the cyst but was well controlled by oral administration of carbamazepine. Whether the pathogenesis of symptomatic PKC was associated with the cortical lesion could not be determined in the present case. (+info)Heading injury precipitating subdural hematoma associated with arachnoid cysts--two case reports. (2/167)
A 14-year-old boy and a 11-year-old boy presented with subdural hematomas as complications of preexisting arachnoid cysts in the middle cranial fossa, manifesting as symptoms of raised intracranial pressure. Both had a history of heading the ball in a soccer game about 7 weeks and 2 days before the symptom occurred. There was no other head trauma, so these cases could be described as "heading injury." Arachnoid cysts in the middle cranial fossa are often associated with subdural hematomas. We emphasize that mild trauma such as heading of the ball in a soccer game may cause subdural hematomas in patients with arachnoid cysts. (+info)Lumbosacral extradural arachnoid cysts: diagnostic and indication for surgery. (3/167)
No critical discussion of the indication for the surgical treatment of lumbosacral extradural arachnoid cysts is found in the literature. Therefore, we want to compare the results in patients with operative and conservative treatment to define standards for a good surgical result. Over a period of 9 years, we operated on eight patients with a lumbosacral extradural arachnoid cyst and treated eight others conservatively. Only three of the operated patients experienced a postoperative relief of pain, but none was symptom free. The only one with continuing success had a preoperative history of 1 year only. MRI scans without contrast agent were misinterpreted in one included and one excluded case. The results of conservative treatment were nearly the same as those of operative treatment. MRI is the best diagnostic tool, but a variety of sequences must be used. Patients with a short pain history and a clear neurological deficit profited most from surgery. Patients with slight and not clearly related uncharacteristic symptoms should be excluded from surgery. (+info)Intracerebral cystic meningioma--case report. (4/167)
A 46-year-old female presented with persistent bifrontal headache. Computed tomography revealed a large cystic tumor in the right temporoparietal area, which included a solid component. The tumor had no attachment to the dura. There was no peritumoral edema or mass effect usually found around cystic meningiomas. The solid component was totally removed. Histological examination indicated that the tumor was a fibrous meningioma. Intracerebral meningioma with a large cystic component without dural attachment should be considered in the differential diagnosis of cystic cerebral tumors. (+info)Intracystic hemorrhage of the middle fossa arachnoid cyst and subdural hematoma caused by ruptured middle cerebral artery aneurysm. (5/167)
We report a case of a cerebral aneurysm arising from the bifurcation of the left middle cerebral artery that ruptured into a left middle cranial fossa arachnoid cyst, associated with acute subdural hematoma. We discuss the relationships of aneurysm, arachnoid cyst, and subdural hematoma. (+info)The role of endoscopic fenestration procedures for cerebral arachnoid cysts. (6/167)
Recently, endoscopic procedures have been recommended as the first surgical option for cerebral arachnoid cyst (AC). The author reports seven ACs treated endoscopically and discuss the role of endoscopic fenestration. The age of the patients ranged from two to 62 years. Three ACs were located in the posterior cranial fossa, two in the suprasellar area, one in the middle cranial fossa, and one in the convexity. All cases were examined by cine magnetic resonance (MR) flow study. The patient's symptoms included headache, vomiting, dizziness, problems in balance, visual disturbance, and seizure. The author performed a cysto-cisternostomy or cysto-ventriculostomy via a single burr hole. The follow-up periods ranged from six to 18 months. There was no mortality or morbidity except one case of intracisternal bleeding during endoscopic procedure. Symptoms were relieved in all seven patients. Follow-up imaging studies revealed a decrease in the size or disappearance of the cysts. The results support that the minimal fenestration procedure as possibly as preserving the internal environment is valuable for the management of ACs. (+info)Neurodevelopmental outcome after antenatal diagnosis of posterior fossa abnormalities. (7/167)
Posterior fossa abnormalities are sonographically diagnosable in the fetus. Anomalies of this region include Dandy-Walker malformation, enlarged cisterna magna, and arachnoid cyst. Despite prenatal diagnosis, the uncertainties related to natural history and neurodevelopmental outcome in survivors make patient counseling difficult. The purposes of this study were to determine the accuracy of prenatal diagnosis of these lesions and elucidate long-term neurodevelopmental outcome in survivors in prenatally diagnosed posterior fossa abnormalities. Fifteen cases of posterior fossa abnormalities were reviewed. Antenatal diagnoses of Dandy-Walker malformation was made in 13 of these cases, arachnoid cyst in one case, and enlarged cisterna magna in one case. Hydrocephalus was present in 66% of patients. The sonographic diagnosis was concordant with the pathologic or neonatal radiologic diagnosis in 13 of 15 cases. Seven fetuses (47%) exhibited additional cranial or extracranial anomalies. A karyotypic abnormality (trisomy 18) was found in one of 15 cases of posterior fossa abnormalities. Neurodevelopmental delay was present in 80% of survivors with follow-up study to 4 years of age. Prenatal diagnosis of posterior fossa abnormalities is highly accurate, yet the differential diagnosis can be challenging. Cognitive and psychomotor developmental delays remain commonplace despite early diagnosis and treatment. The approach with families in cases of prenatal diagnosis of posterior fossa abnormalities should include a search for additional central nervous system and extra-central nervous system anomalies in the fetus and counseling of parents regarding potential adverse outcome for survivors. (+info)Dandy-Walker syndrome successfully treated with cystoperitoneal shunting--case report. (8/167)
A neonate presented with Dandy-Walker syndrome manifesting as a large posterior cranial fossa cyst, aplasia of the lower cerebellar vermis, and elevation of the confluence of the sinuses but without hydrocephalus. A cystoperitoneal shunt was placed at one month after birth. The cyst diminished in size, and marked development of the cerebellar hemispheres and descent of the confluence of sinuses were observed, but not vermis development. The primary pathology of Dandy-Walker syndrome is posterior cranial fossa cyst formation due to passage obstruction in the fourth ventricle exit area and aplasia of the lower cerebellar vermis. The first choice of treatment in patients with Dandy-Walker syndrome in whom the cerebral aqueduct is open is cystoperitoneal shunt surgery, regardless of the presence or absence of hydrocephalus. (+info)An Arachnoid cyst is a type of abnormal fluid-filled sac that develops between the brain or spinal cord and the arachnoid membrane, which is one of the three layers that cover and protect the central nervous system. These cysts are filled with cerebrospinal fluid (CSF), which is the same fluid that surrounds and cushions the brain and spinal cord.
Arachnoid cysts can vary in size and may be present at birth or develop later in life due to trauma, infection, or other factors. While many arachnoid cysts are asymptomatic and do not cause any problems, larger cysts or those that grow or shift over time can put pressure on the brain or spinal cord, leading to a range of neurological symptoms such as headaches, seizures, hearing or vision changes, balance or coordination difficulties, and cognitive impairments.
Treatment for arachnoid cysts depends on their size, location, and associated symptoms. In some cases, observation and monitoring may be sufficient, while in others, surgical intervention may be necessary to drain the cyst or create a connection between it and the surrounding CSF space to relieve pressure.
The arachnoid is one of the three membranes that cover the brain and the spinal cord, known as the meninges. It is located between the dura mater (the outermost layer) and the pia mater (the innermost layer). The arachnoid is a thin, delicate membrane that is filled with cerebrospinal fluid, which provides protection and nutrition to the central nervous system.
The arachnoid has a spider-web like appearance, hence its name, and it is composed of several layers of collagen fibers and elastic tissue. It is highly vascularized, meaning that it contains many blood vessels, and it plays an important role in regulating the flow of cerebrospinal fluid around the brain and spinal cord.
In some cases, the arachnoid can become inflamed or irritated, leading to a condition called arachnoiditis. This can cause a range of symptoms, including pain, muscle weakness, and sensory changes, and it may require medical treatment to manage.
A cyst is a closed sac, having a distinct membrane and division between the sac and its surrounding tissue, that contains fluid, air, or semisolid material. Cysts can occur in various parts of the body, including the skin, internal organs, and bones. They can be caused by various factors, such as infection, genetic predisposition, or blockage of a duct or gland. Some cysts may cause symptoms, such as pain or discomfort, while others may not cause any symptoms at all. Treatment for cysts depends on the type and location of the cyst, as well as whether it is causing any problems. Some cysts may go away on their own, while others may need to be drained or removed through a surgical procedure.
Syringomyelia is a medical condition characterized by the formation of a fluid-filled cavity or cavities (syrinx) within the spinal cord. This syrinx can lead to various symptoms depending on its size and location, which may include pain, muscle weakness, numbness, and stiffness in the neck, back, shoulders, arms, or legs. In some cases, it may also affect bladder and bowel function, sexual performance, and the ability to maintain normal body temperature. Syringomyelia is often associated with Chiari malformation, a condition where the lower part of the brain extends into the spinal canal. However, other conditions such as spinal cord injuries, tumors, or infections may also cause syringomyelia.
The subdural space is a potential space between the dura mater, which is the outermost of the three meninges covering the brain and spinal cord, and the arachnoid mater, which is the middle meningeal layer. This space normally contains a thin film of fluid, but when it becomes filled with blood (subdural hematoma) or pus (subdural empyema), it can cause significant neurological problems due to increased pressure on the brain. The subdural space can also become widened in certain conditions such as dementia or hydrocephalus, leading to a condition called subdural hygroma.
Arachnoiditis is a medical condition that affects the arachnoid, one of the membranes that surround and protect the nerves of the central nervous system (the brain and spinal cord). The arachnoid becomes inflamed, often as a result of infection, direct injury, or complications from spinal surgery or chronic exposure to irritants such as steroids or contrast dyes.
The inflammation can cause the formation of scar tissue, which can lead to a variety of symptoms including:
1. Chronic pain in the back, legs, or arms
2. Numbness, tingling, or weakness in the limbs
3. Muscle cramps and spasms
4. Bladder and bowel dysfunction
5. Sexual dysfunction
In severe cases, arachnoiditis can cause permanent nerve damage and disability. Treatment typically focuses on managing symptoms and improving quality of life, as there is no cure for the condition.
Central nervous system (CNS) cysts are abnormal fluid-filled sacs that develop in the brain or spinal cord. These cysts can be congenital, meaning they are present at birth and develop as a result of abnormal embryonic development, or they can be acquired later in life due to injury, infection, or disease.
CNS cysts can vary in size and may cause symptoms depending on their location and the amount of pressure they place on surrounding brain or spinal cord tissue. Symptoms may include headaches, seizures, weakness, numbness, or difficulty with coordination and balance. In some cases, CNS cysts may not cause any symptoms and may be discovered incidentally during imaging studies performed for other reasons.
There are several types of CNS cysts, including:
1. Arachnoid cysts: These are the most common type of CNS cyst and occur between the layers of the arachnoid membrane that covers the brain and spinal cord.
2. Colloid cysts: These cysts typically develop at the junction of the third and fourth ventricles in the brain and can obstruct the flow of cerebrospinal fluid (CSF), leading to increased intracranial pressure.
3. Ependymal cysts: These cysts arise from the ependymal cells that line the ventricular system of the brain and can cause symptoms by compressing surrounding brain tissue.
4. Neuroglial cysts: These cysts are composed of glial cells, which support and protect nerve cells in the CNS.
5. Pineal cysts: These cysts develop in the pineal gland, a small endocrine gland located near the center of the brain.
Treatment for CNS cysts depends on their size, location, and symptoms. In some cases, observation and monitoring may be all that is necessary. However, if the cyst is causing significant symptoms or is at risk of rupturing or obstructing CSF flow, surgical intervention may be required to remove or reduce the size of the cyst.
The subarachnoid space is the area between the arachnoid mater and pia mater, which are two of the three membranes covering the brain and spinal cord (the third one being the dura mater). This space is filled with cerebrospinal fluid (CSF), which provides protection and cushioning to the central nervous system. The subarachnoid space also contains blood vessels that supply the brain and spinal cord with oxygen and nutrients. It's important to note that subarachnoid hemorrhage, a type of stroke, can occur when there is bleeding into this space.
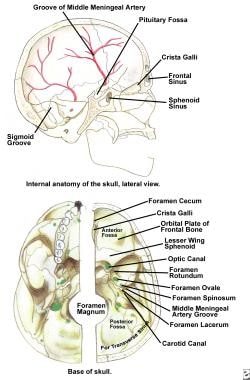
The middle cranial fossa is a depression or hollow in the skull that forms the upper and central portion of the cranial cavity. It is located between the anterior cranial fossa (which lies anteriorly) and the posterior cranial fossa (which lies posteriorly). The middle cranial fossa contains several important structures, including the temporal lobes of the brain, the pituitary gland, the optic chiasm, and the cavernous sinuses. It is also where many of the cranial nerves pass through on their way to the brain.
The middle cranial fossa can be further divided into two parts: the anterior and posterior fossae. The anterior fossa contains the optic chiasm and the pituitary gland, while the posterior fossa contains the temporal lobes of the brain and the cavernous sinuses.
The middle cranial fossa is formed by several bones of the skull, including the sphenoid bone, the temporal bone, and the parietal bone. The shape and size of the middle cranial fossa can vary from person to person, and abnormalities in its structure can be associated with various medical conditions, such as pituitary tumors or aneurysms.
A subdural hematoma is a type of hematoma (a collection of blood) that occurs between the dura mater, which is the outermost protective covering of the brain, and the brain itself. It is usually caused by bleeding from the veins located in this potential space, often as a result of a head injury or trauma.
Subdural hematomas can be classified as acute, subacute, or chronic based on their rate of symptom progression and the time course of their appearance on imaging studies. Acute subdural hematomas typically develop and cause symptoms rapidly, often within hours of the head injury. Subacute subdural hematomas have a more gradual onset of symptoms, which can occur over several days to a week after the trauma. Chronic subdural hematomas may take weeks to months to develop and are often seen in older adults or individuals with chronic alcohol abuse, even after minor head injuries.
Symptoms of a subdural hematoma can vary widely depending on the size and location of the hematoma, as well as the patient's age and overall health. Common symptoms include headache, altered mental status, confusion, memory loss, weakness or numbness, seizures, and in severe cases, coma or even death. Treatment typically involves surgical evacuation of the hematoma, along with management of any underlying conditions that may have contributed to its development.
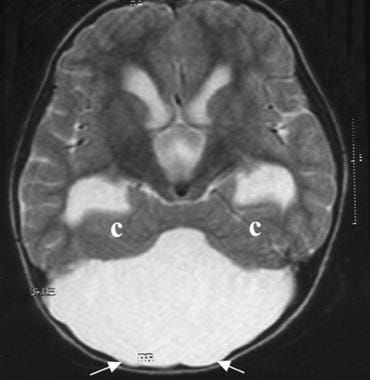
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
The foramen magnum is the largest opening in the human skull, located at the base of the skull, through which the spinal cord connects to the brain. It is a crucial structure for the transmission of nerve impulses between the brain and the rest of the body. The foramen magnum also provides passage for blood vessels that supply the brainstem and upper spinal cord.
A craniotomy is a surgical procedure where a bone flap is temporarily removed from the skull to access the brain. This procedure is typically performed to treat various neurological conditions, such as brain tumors, aneurysms, arteriovenous malformations, or traumatic brain injuries. After the underlying brain condition is addressed, the bone flap is usually replaced and secured back in place with plates and screws. The purpose of a craniotomy is to provide access to the brain for diagnostic or therapeutic interventions while minimizing potential damage to surrounding tissues.
A subdural effusion is an abnormal accumulation of fluid in the potential space between the dura mater (the outermost layer of the meninges that covers the brain and spinal cord) and the arachnoid membrane (one of the three layers of the meninges that surround the brain and spinal cord) in the subdural space.
Subdural effusions can occur due to various reasons, including head trauma, infection, or complications from neurosurgical procedures. The fluid accumulation may result from bleeding (subdural hematoma), inflammation, or increased cerebrospinal fluid pressure. Depending on the underlying cause and the amount of fluid accumulated, subdural effusions can cause various symptoms, such as headaches, altered mental status, or neurological deficits.
Subdural effusions are often asymptomatic and may resolve independently; however, in some cases, medical intervention might be necessary to alleviate the pressure on the brain or address the underlying condition. Imaging techniques like computed tomography (CT) or magnetic resonance imaging (MRI) scans are typically used to diagnose and monitor subdural effusions.
Cyst fluid refers to the fluid accumulated within a cyst, which is a closed sac-like or capsular structure, typically filled with liquid or semi-solid material. Cysts can develop in various parts of the body for different reasons, and the composition of cyst fluid may vary depending on the type of cyst and its location.
In some cases, cyst fluid might contain proteins, sugars, hormones, or even cells from the surrounding tissue. Infected cysts may have pus-like fluid, while cancerous or precancerous cysts might contain abnormal cells or tumor markers. The analysis of cyst fluid can help medical professionals diagnose and manage various medical conditions, including infections, inflammatory diseases, genetic disorders, and cancers.
It is important to note that the term 'cyst fluid' generally refers to the liquid content within a cyst, but the specific composition and appearance of this fluid may vary significantly depending on the underlying cause and type of cyst.
Dura Mater is the thickest and outermost of the three membranes (meninges) that cover the brain and spinal cord. It provides protection and support to these delicate structures. The other two layers are called the Arachnoid Mater and the Pia Mater, which are thinner and more delicate than the Dura Mater. Together, these three layers form a protective barrier around the central nervous system.
Neurosurgical procedures are operations that are performed on the brain, spinal cord, and peripheral nerves. These procedures are typically carried out by neurosurgeons, who are medical doctors with specialized training in the diagnosis and treatment of disorders of the nervous system. Neurosurgical procedures can be used to treat a wide range of conditions, including traumatic injuries, tumors, aneurysms, vascular malformations, infections, degenerative diseases, and congenital abnormalities.
Some common types of neurosurgical procedures include:
* Craniotomy: A procedure in which a bone flap is temporarily removed from the skull to gain access to the brain. This type of procedure may be performed to remove a tumor, repair a blood vessel, or relieve pressure on the brain.
* Spinal fusion: A procedure in which two or more vertebrae in the spine are fused together using bone grafts and metal hardware. This is often done to stabilize the spine and alleviate pain caused by degenerative conditions or spinal deformities.
* Microvascular decompression: A procedure in which a blood vessel that is causing pressure on a nerve is repositioned or removed. This type of procedure is often used to treat trigeminal neuralgia, a condition that causes severe facial pain.
* Deep brain stimulation: A procedure in which electrodes are implanted in specific areas of the brain and connected to a battery-operated device called a neurostimulator. The neurostimulator sends electrical impulses to the brain to help alleviate symptoms of movement disorders such as Parkinson's disease or dystonia.
* Stereotactic radiosurgery: A non-invasive procedure that uses focused beams of radiation to treat tumors, vascular malformations, and other abnormalities in the brain or spine. This type of procedure is often used for patients who are not good candidates for traditional surgery due to age, health status, or location of the lesion.
Neurosurgical procedures can be complex and require a high degree of skill and expertise. Patients considering neurosurgical treatment should consult with a qualified neurosurgeon to discuss their options and determine the best course of action for their individual situation.
The sacrococcygeal region is the lower part of the back where the spine ends, specifically referring to the area where the sacrum (a triangular bone at the base of the spine formed by the fusion of several vertebrae) meets the coccyx (also known as the tailbone). This region is located at the very bottom of the spine and is susceptible to injury or trauma due to its position and role in supporting the body's weight. It is also a common site for birth defects, particularly in newborns.
Spinal cord compression is a medical condition that refers to the narrowing of the spinal canal, which puts pressure on the spinal cord and the nerves that branch out from it. This can occur due to various reasons such as degenerative changes in the spine, herniated discs, bone spurs, tumors, or fractures. The compression can lead to a range of symptoms including pain, numbness, tingling, weakness, or loss of bladder and bowel control. In severe cases, it can cause paralysis. Treatment options depend on the underlying cause and may include physical therapy, medication, surgery, or radiation therapy.
A hernia is a protrusion of an organ or tissue through a weakened area in the abdominal wall, often appearing as a bulge beneath the skin. This condition can occur in various parts of the body such as the groin (inguinal hernia), navel (umbilical hernia), or site of a previous surgical incision (incisional hernia). Hernias may cause discomfort or pain, especially when straining, lifting heavy objects, or during bowel movements. In some cases, they may lead to serious complications like intestinal obstruction or strangulation, requiring immediate medical attention.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Neuroendoscopy is a minimally invasive surgical technique that involves the use of an endoscope to access and treat various conditions within the brain and spinal column. An endoscope is a long, flexible tube with a light and camera at its tip, which allows surgeons to view and operate on internal structures through small incisions or natural openings in the body.
In neuroendoscopy, the surgeon uses the endoscope to navigate through the brain's ventricular system (fluid-filled spaces) or other narrow spaces within the skull or spine to diagnose and treat conditions such as hydrocephalus, brain tumors, arachnoid cysts, and intraventricular hemorrhage.
The benefits of neuroendoscopy include reduced trauma to surrounding tissues, shorter hospital stays, faster recovery times, and improved outcomes compared to traditional open surgical approaches. However, neuroendoscopic procedures require specialized training and expertise due to the complexity of the anatomy involved.
Cerebral ventriculography is a medical imaging technique that involves the injection of a contrast material into the cerebral ventricles, which are fluid-filled spaces within the brain. The purpose of this procedure is to produce detailed images of the ventricular system and the surrounding structures in order to diagnose and evaluate various neurological conditions, such as hydrocephalus (excessive accumulation of cerebrospinal fluid in the ventricles), tumors, or other abnormalities that may be causing obstruction or compression of the ventricular system.
The procedure typically involves inserting a thin, flexible tube called a catheter into the lateral ventricle of the brain through a small hole drilled in the skull. The contrast material is then injected through the catheter and X-ray images are taken as the contrast material flows through the ventricular system. These images can help to identify any abnormalities or blockages that may be present.
Cerebral ventriculography has largely been replaced by non-invasive imaging techniques, such as computed tomography (CT) and magnetic resonance imaging (MRI), which provide similar information without the need for invasive procedures. However, cerebral ventriculography may still be used in certain cases where these other methods are not sufficient to make a definitive diagnosis.
Surgical decompression is a medical procedure that involves relieving pressure on a nerve or tissue by creating additional space. This is typically accomplished through the removal of a portion of bone or other tissue that is causing the compression. The goal of surgical decompression is to alleviate symptoms such as pain, numbness, tingling, or weakness caused by the compression.
In the context of spinal disorders, surgical decompression is often used to treat conditions such as herniated discs, spinal stenosis, or bone spurs that are compressing nerves in the spine. The specific procedure used may vary depending on the location and severity of the compression, but common techniques include laminectomy, discectomy, and foraminotomy.
It's important to note that surgical decompression is a significant medical intervention that carries risks such as infection, bleeding, and injury to surrounding tissues. As with any surgery, it should be considered as a last resort after other conservative treatments have been tried and found to be ineffective. A thorough evaluation by a qualified medical professional is necessary to determine whether surgical decompression is appropriate in a given case.
An ovarian cyst is a sac or pouch filled with fluid that forms on the ovary. Ovarian cysts are quite common in women during their childbearing years, and they often cause no symptoms. In most cases, ovarian cysts disappear without treatment over a few months. However, larger or persistent cysts may require medical intervention, including surgical removal.
There are various types of ovarian cysts, such as functional cysts (follicular and corpus luteum cysts), which develop during the menstrual cycle due to hormonal changes, and non-functional cysts (dermoid cysts, endometriomas, and cystadenomas), which can form due to different causes.
While many ovarian cysts are benign, some may have malignant potential or indicate an underlying medical condition like polycystic ovary syndrome (PCOS). Regular gynecological check-ups, including pelvic examinations and ultrasounds, can help detect and monitor ovarian cysts.
A laminectomy is a surgical procedure that involves the removal of the lamina, which is the back part of the vertebra that covers the spinal canal. This procedure is often performed to relieve pressure on the spinal cord or nerves caused by conditions such as herniated discs, spinal stenosis, or tumors. By removing the lamina, the surgeon can access the affected area and alleviate the compression on the spinal cord or nerves, thereby reducing pain, numbness, or weakness in the back, legs, or arms.
Laminectomy may be performed as a standalone procedure or in combination with other surgical techniques such as discectomy, foraminotomy, or spinal fusion. The specific approach and extent of the surgery will depend on the patient's individual condition and symptoms.
Iophendylate is not typically referred to as a medical definition, but it is the chemical name for a contrast agent that is used in radiology procedures. It is a type of oil-based contrast medium that is injected into the cerebrospinal fluid (CSF) during myelography, which is an imaging test used to visualize the spinal cord and surrounding structures.
Iophendylate, also known as Pantopaque, is a heavy oily substance that outlines the spinal canal and nerve roots on X-ray images, allowing radiologists to diagnose various conditions such as herniated discs, spinal stenosis, or tumors. However, due to the risks associated with its use, including chemical meningitis and potential neurological complications, it has largely been replaced by water-soluble contrast agents in current clinical practice.
Spinal cord diseases refer to a group of conditions that affect the spinal cord, which is a part of the central nervous system responsible for transmitting messages between the brain and the rest of the body. These diseases can cause damage to the spinal cord, leading to various symptoms such as muscle weakness, numbness, pain, bladder and bowel dysfunction, and difficulty with movement and coordination.
Spinal cord diseases can be congenital or acquired, and they can result from a variety of causes, including infections, injuries, tumors, degenerative conditions, autoimmune disorders, and genetic factors. Some examples of spinal cord diseases include multiple sclerosis, spina bifida, spinal cord injury, herniated discs, spinal stenosis, and motor neuron diseases such as amyotrophic lateral sclerosis (ALS).
The treatment for spinal cord diseases varies depending on the underlying cause and severity of the condition. Treatment options may include medication, physical therapy, surgery, and rehabilitation. In some cases, the damage to the spinal cord may be irreversible, leading to permanent disability or paralysis.
A headache is defined as pain or discomfort in the head, scalp, or neck. It can be a symptom of various underlying conditions such as stress, sinus congestion, migraine, or more serious issues like meningitis or concussion. Headaches can vary in intensity, ranging from mild to severe, and may be accompanied by other symptoms such as nausea, vomiting, or sensitivity to light and sound. There are over 150 different types of headaches, including tension headaches, cluster headaches, and sinus headaches, each with their own specific characteristics and causes.
Cerebrospinal fluid (CSF) shunts are medical devices used to divert the flow of excess CSF from the brain and spinal cord to another part of the body, usually the abdominal cavity. The shunt consists of a catheter, a valve, and a reservoir.
The catheter is inserted into one of the ventricles in the brain or the subarachnoid space surrounding the spinal cord to drain the excess CSF. The valve regulates the flow of CSF to prevent over-drainage, which can cause complications such as low CSF pressure and brain sagging. The reservoir is a small chamber that allows for easy access to the shunt system for monitoring and adjusting the pressure settings.
CSF shunts are typically used to treat conditions associated with increased production or impaired absorption of CSF, such as hydrocephalus, communicating hydrocephalus, normal pressure hydrocephalus, and pseudotumor cerebri. By reducing the buildup of CSF in the brain, shunts can help alleviate symptoms such as headaches, nausea, vomiting, vision problems, and cognitive impairment.
It is important to note that while CSF shunts are effective in managing these conditions, they also carry risks of complications such as infection, obstruction, malfunction, and over-drainage. Regular monitoring and follow-up care are necessary to ensure proper functioning and minimize the risk of complications.
Hypothalamic diseases refer to conditions that affect the hypothalamus, a small but crucial region of the brain responsible for regulating many vital functions in the body. The hypothalamus helps control:
1. Body temperature
2. Hunger and thirst
3. Sleep cycles
4. Emotions and behavior
5. Release of hormones from the pituitary gland
Hypothalamic diseases can be caused by genetic factors, infections, tumors, trauma, or other conditions that damage the hypothalamus. Some examples of hypothalamic diseases include:
1. Hypothalamic dysfunction syndrome: A condition characterized by various symptoms such as obesity, sleep disturbances, and hormonal imbalances due to hypothalamic damage.
2. Kallmann syndrome: A genetic disorder that affects the development of the hypothalamus and results in a lack of sexual maturation and a decreased sense of smell.
3. Prader-Willi syndrome: A genetic disorder that causes obesity, developmental delays, and hormonal imbalances due to hypothalamic dysfunction.
4. Craniopharyngiomas: Tumors that develop near the pituitary gland and hypothalamus, often causing visual impairment, hormonal imbalances, and growth problems.
5. Infiltrative diseases: Conditions such as sarcoidosis or histiocytosis can infiltrate the hypothalamus, leading to various symptoms related to hormonal imbalances and neurological dysfunction.
6. Traumatic brain injury: Damage to the hypothalamus due to head trauma can result in various hormonal and neurological issues.
7. Infections: Bacterial or viral infections that affect the hypothalamus, such as encephalitis or meningitis, can cause damage and lead to hypothalamic dysfunction.
Treatment for hypothalamic diseases depends on the underlying cause and may involve medications, surgery, hormone replacement therapy, or other interventions to manage symptoms and improve quality of life.
An epidermal cyst is a common benign skin condition characterized by the growth of a sac-like structure filled with keratin, a protein found in the outermost layer of the skin (epidermis). These cysts typically appear as round, firm bumps just under the surface of the skin, often on the face, neck, trunk, or scalp. They can vary in size from a few millimeters to several centimeters in diameter.
Epidermal cysts usually develop as a result of the accumulation of dead skin cells that become trapped within a hair follicle or a pilosebaceous unit (a structure that contains a hair follicle and an oil gland). The keratin produced by the skin cells then collects inside the sac, causing it to expand gradually.
These cysts are generally slow-growing, painless, and rarely cause any symptoms. However, they may become infected or inflamed, leading to redness, tenderness, pain, or pus formation. In such cases, medical attention might be necessary to drain the cyst or administer antibiotics to treat the infection.
Epidermal cysts can be removed surgically if they cause cosmetic concerns or become frequently infected. The procedure typically involves making an incision in the skin and removing the entire sac along with its contents to prevent recurrence.
The term "cisterna magna" is derived from Latin, where "cisterna" means "reservoir" or "receptacle," and "magna" means "large." In medical anatomy, the cisterna magna refers to a large, sac-like space located near the lower part of the brainstem. It is a subarachnoid cistern, which means it is a space that contains cerebrospinal fluid (CSF) between the arachnoid and pia mater membranes covering the brain and spinal cord.
More specifically, the cisterna magna is situated between the cerebellum (the lower part of the brain responsible for coordinating muscle movements and maintaining balance) and the occipital bone (the bone at the back of the skull). This space contains a significant amount of CSF, which serves as a protective cushion for the brain and spinal cord, helps regulate intracranial pressure, and facilitates the circulation of nutrients and waste products.
The cisterna magna is an essential structure in neurosurgical procedures and diagnostic imaging techniques like lumbar puncture (spinal tap) or myelograms, where contrast agents are introduced into the CSF to visualize the spinal cord and surrounding structures. Additionally, it serves as a crucial landmark for various surgical approaches to the posterior fossa (the lower part of the skull that houses the cerebellum and brainstem).
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
Firesetting behavior is not a medical diagnosis itself, but it is a term used to describe the act of deliberately starting fires. It is often associated with certain mental health conditions, developmental disorders, or substance abuse problems. Firesetting behavior can range from minor incidents, such as lighting candles or matches, to more serious offenses, like arson.
Firesetting behavior can be a symptom of various psychiatric disorders, including conduct disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder, and personality disorders. It can also be associated with substance abuse, cognitive impairments, and traumatic brain injuries. In some cases, firesetting behavior may indicate a cry for help or a maladaptive coping mechanism.
It is essential to assess the underlying causes of firesetting behavior to develop an appropriate treatment plan. This may involve individual therapy, family therapy, cognitive-behavioral therapy, and/or medication management. In severe cases, hospitalization or residential treatment may be necessary. Additionally, fire safety education and community resources can help prevent future incidents.
The Sella Turcica, also known as the Turkish saddle, is a depression or fossa in the sphenoid bone located at the base of the skull. It forms a housing for the pituitary gland, which is a small endocrine gland often referred to as the "master gland" because it controls other glands and makes several essential hormones. The Sella Turcica has a saddle-like shape, with its anterior and posterior clinoids forming the front and back of the saddle, respectively. This region is of significant interest in neuroimaging and clinical settings, as various conditions such as pituitary tumors or other abnormalities may affect the size, shape, and integrity of the Sella Turcica.
Hydrocephalus is a medical condition characterized by an abnormal accumulation of cerebrospinal fluid (CSF) within the brain, leading to an increase in intracranial pressure and potentially causing damage to the brain tissues. This excessive buildup of CSF can result from either overproduction or impaired absorption of the fluid, which typically causes the ventricles (fluid-filled spaces) inside the brain to expand and put pressure on surrounding brain structures.
The condition can be congenital, present at birth due to genetic factors or abnormalities during fetal development, or acquired later in life as a result of injuries, infections, tumors, or other disorders affecting the brain's ability to regulate CSF flow and absorption. Symptoms may vary depending on age, severity, and duration but often include headaches, vomiting, balance problems, vision issues, cognitive impairment, and changes in behavior or personality.
Treatment for hydrocephalus typically involves surgically implanting a shunt system that diverts the excess CSF from the brain to another part of the body where it can be absorbed, such as the abdominal cavity. In some cases, endoscopic third ventriculostomy (ETV) might be an alternative treatment option, creating a new pathway for CSF flow within the brain. Regular follow-ups with neurosurgeons and other healthcare professionals are essential to monitor the condition and make any necessary adjustments to the treatment plan.
Trephination, also known as trepanation or burr hole surgery, is a surgical procedure that involves making a circular hole in the skull. This ancient medical practice was used in various cultures throughout history for various purposes, such as relieving pressure on the brain, treating mental disorders, or releasing evil spirits. In modern medicine, it is rarely performed and usually reserved for severe conditions like subdural hematomas or infection inside the skull.
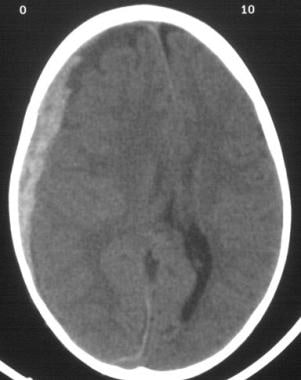
A subdural hematoma (SDH) is a type of intracranial hemorrhage that occurs between the dura mater and the brain. When it becomes chronic, it means that the bleeding has occurred slowly over time, often over the course of several weeks or months. The blood gradually collects in the potential space between the dura and the arachnoid membrane, forming a clot.
A chronic subdural hematoma (CSDH) is typically characterized by the presence of liquefied blood, which can form a loculated collection that may exert mass effect on the underlying brain tissue. This can lead to symptoms such as headache, confusion, weakness, or even seizures, depending on the size and location of the hematoma.
CSDHs are often associated with underlying brain atrophy, which can create a larger potential space for blood to collect. They may also be seen in patients who are taking anticoagulant medications or have a bleeding disorder. Treatment typically involves surgical evacuation of the hematoma, although smaller CSDHs may be managed conservatively with close monitoring and repeat imaging.
Cerebellar diseases refer to a group of medical conditions that affect the cerebellum, which is the part of the brain located at the back of the head, below the occipital lobe and above the brainstem. The cerebellum plays a crucial role in motor control, coordination, balance, and some cognitive functions.
Cerebellar diseases can be caused by various factors, including genetics, infections, tumors, stroke, trauma, or degenerative processes. These conditions can result in a wide range of symptoms, such as:
1. Ataxia: Loss of coordination and unsteady gait
2. Dysmetria: Inability to judge distance and force while performing movements
3. Intention tremors: Shaking or trembling that worsens during purposeful movements
4. Nystagmus: Rapid, involuntary eye movement
5. Dysarthria: Speech difficulty due to muscle weakness or incoordination
6. Hypotonia: Decreased muscle tone
7. Titubation: Rhythmic, involuntary oscillations of the head and neck
8. Cognitive impairment: Problems with memory, attention, and executive functions
Some examples of cerebellar diseases include:
1. Ataxia-telangiectasia
2. Friedrich's ataxia
3. Multiple system atrophy (MSA)
4. Spinocerebellar ataxias (SCAs)
5. Cerebellar tumors, such as medulloblastomas or astrocytomas
6. Infarctions or hemorrhages in the cerebellum due to stroke or trauma
7. Infections, such as viral encephalitis or bacterial meningitis
8. Autoimmune disorders, like multiple sclerosis (MS) or paraneoplastic syndromes
9. Metabolic disorders, such as Wilson's disease or phenylketonuria (PKU)
10. Chronic alcoholism and withdrawal
Treatment for cerebellar diseases depends on the underlying cause and may involve medications, physical therapy, surgery, or supportive care to manage symptoms and improve quality of life.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
A Ventriculoperitoneal (VP) shunt is a surgical procedure that involves the insertion of a long, flexible tube (shunt) into the cerebral ventricles of the brain to drain excess cerebrospinal fluid (CSF). The other end of the shunt is directed into the peritoneal cavity, where the CSF can be absorbed.
The VP shunt is typically used to treat hydrocephalus, a condition characterized by an abnormal accumulation of CSF within the ventricles of the brain, which can cause increased intracranial pressure and damage to the brain. By diverting the excess CSF from the ventricles into the peritoneal cavity, the VP shunt helps to relieve the symptoms of hydrocephalus and prevent further neurological damage.
The shunt system consists of several components, including a ventricular catheter that is placed in the ventricle, a one-way valve that regulates the flow of CSF, and a distal catheter that is directed into the peritoneal cavity. The valve helps to prevent backflow of CSF into the brain and ensures that the fluid flows in only one direction, from the ventricles to the peritoneal cavity.
VP shunts are generally safe and effective, but they can be associated with complications such as infection, obstruction, or malfunction of the shunt system. Regular follow-up with a healthcare provider is necessary to monitor the function of the shunt and ensure that any potential issues are addressed promptly.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
Barotrauma is a type of injury that occurs when there is a difference in pressure between the external environment and the internal body, leading to damage to body tissues. It commonly affects gas-filled spaces in the body, such as the lungs, middle ear, or sinuses.
In medical terms, barotrauma refers to the damage caused by changes in pressure that occur rapidly, such as during scuba diving, flying in an airplane, or receiving treatment in a hyperbaric chamber. These rapid changes in pressure can cause the gas-filled spaces in the body to expand or contract, leading to injury.
For example, during descent while scuba diving, the pressure outside the body increases, and if the diver does not equalize the pressure in their middle ear by swallowing or yawning, the increased pressure can cause the eardrum to rupture, resulting in barotrauma. Similarly, rapid ascent while flying can cause the air in the lungs to expand, leading to lung overexpansion injuries such as pneumothorax or arterial gas embolism.
Prevention of barotrauma involves equalizing pressure in the affected body spaces during changes in pressure and avoiding diving or flying with respiratory infections or other conditions that may increase the risk of injury. Treatment of barotrauma depends on the severity and location of the injury and may include pain management, antibiotics, surgery, or hyperbaric oxygen therapy.
A meningocele is a type of neural tube defect that results in the herniation of the meninges (the protective membranes covering the brain and spinal cord) through a defect in the vertebral column. The meninges protrude as a sac-like structure, which may be covered by skin or a thin layer of tissue. Meningoceles usually do not contain neural tissue, but cerebrospinal fluid is present within the sac. They are typically asymptomatic unless there is compression of surrounding structures or infection. Treatment generally involves surgical repair to prevent potential complications such as meningitis or neurological damage.
 Arachnoid cyst
Arachnoid cyst