Actinomycosis, Cervicofacial
Actinomyces
Mycobacterium haemophilum
Pelvic Inflammatory Disease
Face
Vascular Malformations
Granuloma, Foreign-Body
Bronchial Diseases
Oophoritis
Actinomyces viscosus
Colon, Ascending
Tomography, X-Ray Computed
Penicillins
Cervicofacial actinomycosis: CT and MR imaging findings in seven patients. (1/14)
BACKGROUND AND PURPOSE: Cervicofacial actinomycosis is uncommon, but without proper treatment it causes extensive tissue destruction. Early diagnosis is critical but usually difficult with cultures or imaging. Our aim was to identify characteristic imaging features that facilitated diagnosis in seven patients with cervicofacial actinomycosis. METHODS: We retrospectively reviewed the CT and MR findings in seven patients with pathologically proved actinomycosis. Histologic diagnosis was made by means of surgical excision or biopsy in seven patients. Culturing was performed in two patients. Enhanced CT scans (n=7) and MR images (n=2) were evaluated for the location, margin, infiltrative nature, enhancement pattern, and presence of lymphadenopathy. RESULTS: CT and MR images showed either a well-defined (n=2) or ill-defined (n=5) mass. Involved areas included the nasal cavity (n=2), buccal space (n=1), pyriform sinus (n=1), aryepiglottic fold (n=1), oro- and hypopharynx (n=1) and tongue (n=1). Imaging confirmed the infiltrative nature, showing the tendency of the lesion to invade across tissue planes and boundaries (n=6). Moderate homogeneous contrast enhancement was seen on CT scans in six patients with several small low-attenuating foci (n=2). T1- and T2-weighted MR images showed intermediate signal intensity with moderate contrast enhancement (n=2). Reactive lymphadenopathy was associated in three patients. CONCLUSION: Although cervicofacial actinomycosis occurs infrequently, it should be included in the differential diagnosis when images show a soft-tissue mass with inflammatory changes and an infiltrative nature in the cervicofacial area. (+info)Human cervicofacial actinomycoses: microbiological data for 1997 cases. (2/14)
Actinomycoses are sporadically occurring endogenous polymicrobial inflammatory processes, in which fermentative actinomycetes of the genera Actinomyces, Propionibacterium, or Bifidobacterium act as the principal pathogens. Difficulties in diagnosing the disease in a timely and reliable fashion have led clinicians and microbiologists to grossly underestimate its medical importance. Therefore, we evaluated microbiological and selected clinical data derived from 1997 culture-positive cases of human cervicofacial actinomycoses examined in our laboratories during 1972-1999. The causative actinomycetes belonged to at least 9 different species, among which Actinomyces israelii and Actinomyces gerencseriae predominated. The well-known predisposition of male patients to acquire the disease varied with age and appeared to be especially pronounced in patients aged 20-60 years, the highest incidence being found in female patients aged 11-40 years and in male patients aged 21-50 years. The relevant procedures necessary for diagnosing human actinomycoses reliably, as well as details of their complex etiology, are discussed. (+info)Histopathologic examination to confirm diagnosis of periapical lesions: a review. (3/14)
Most periapical lesions are represented by inflammatory cysts, granulomas, abscesses or fibrous scars. These inflammatory conditions are often termed "endodontic lesions" because pulpal necrosis is the initiating event in their pathogenesis. Although rare, other clinically confusing periapical lesions have been extensively documented in numerous case reports and short case series. These lesions represent a wide range of pathosis, including various developmental cysts, infections, benign but locally aggressive lesions, and malignancies. The literature describing these lesions and the value of a histopathologic examination in diagnosis is reviewed. (+info)Short-term treatment of actinomycosis: two cases and a review. (4/14)
Recommendations for prolonged penicillin treatment of actinomycosis date from the early antibiotic era, when patients often presented with neglected, advanced disease and received interrupted therapy at suboptimal dosages. This report describes cases of esophageal and of cervicofacial actinomycosis treated successfully with short-term antibiotic therapy and reviews the literature. Many patients are cured with <6 months of antibiotic therapy. If short-term antibiotic treatment is attempted, the clinical and radiological response should be closely monitored. Cervicofacial actinomycosis is especially responsive to brief courses of antibiotic treatment. (+info)Fine-needle aspiration cytology in the diagnosis of cervicofacial actinomycosis: report of 15 cases. (5/14)
OBJECTIVES: Actinomycosis is quite an infrequent bacterial infection nowadays. However it can be considered in cases with a persistent cervicofacial disease. Although it is a bacterial infection, microbiologic cultures are frequently not diagnoses, therefore histopathologic studies and image studies are essential. Our interest is to explain our experience with cervicofacial actinomycosis; the clinical behaviour, evolution and treatment, always assisted by their elected diagnostic technique: the FNAC. STUDY DESIGN: In the last 16 years, 15 patients have been diagnosed with cervicofacial actinomycosis by FNAC, treated by Maxillofacial, Internal Medicine and Paediatrics units. Clinical course, evolution, anatomical space situation, antibiotic treatment, and surgical treatment have been studied. RESULTS AND CONCLUSIONS: The fine-needle aspiration cytology (FNAC) is an easy, safe and rapid method, with a high effect, that has made the final diagnosis in 15 cases in our Hospital. All the patients have had a good clinical evolution, only in one case did we need a new treatment for recidive. In all the cases treatment has been definitive. Our interest is to explain our experience in the treatment of cervicofacial actinomycosis, its clinical presentation and evolution, together with its elected method of diagnosis, FNAC. (+info)Cervicofacial actinomycosis: still a difficult differential diagnosis. (6/14)
Cervicofacial actinomycosis, a rare chronic infectious disease, is, however, an important clinical entity, due to the difficulties involved, still today, in its diagnosis. Following personal experience in a case referred to our Department, and in agreement with reports in the literature, attention is drawn to the presenting clinical manifestations, stressing that these are often confusing since they mimic those of other diseases, Moreover, many pre-operative investigations (radiological scans, incisional biopsy, fine-needle aspiration) are generally nonspecific. Finally, surgical excision of the mass is now the last essential step to make a definitive diagnosis and define the appropriate antibiotic therapy. (+info)Two unusual presentations of cervicofacial actinomycosis and review of the literature. (7/14)
Cervicofacial actinomycosis is the most common clinical form of actinomycosis. This bacterial infection is rare. Diagnosis is difficult, often it is definitive only after surgical excision of the cervicofacial mass. Personal experience is reported concerning two cases of cervicoactinomycosis. Diagnosis, in both cases, has been based on histological findings, not on clinical symptoms. A review of the literature shows that mainly males are affected by this condition and, in fact, both patients described here are males. Symptoms of acute infection were absent. Both patients denied any history of oromaxillofacial trauma or recent dental extraction or oral manipulations. Imaging techniques--ultrasonography and computerized tomography--were not effective in making the diagnosis, in either of these patients. Furthermore, fine needle aspiration cytology did not provide a definitive diagnosis. Both patients underwent surgical excision of the mass. Penicillin was the drug of choice in post-operative long-term treatment (one month). In one of the two men, intravenous steroids were administered. As in several reports in the literature, the definitive diagnosis was histological and not clinical. (+info)Actinomycotic pseudo-tumour of the mid-cervical region (a case report). (8/14)
Cervicofacial actinomycosis is today a rare disease in our country. Isolated actinomycotic neck masses are extremely rare. A case of young man with an isolated midcervical tumour like actinomycotic granuloma without sinuses or discharging granules is reported here. (+info)Actinomycosis is a type of infection caused by bacteria that are normally found in the mouth, intestines, and female genital tract. These bacteria can cause abscesses or chronic inflammation if they infect body tissues, often after trauma or surgery. The infection typically affects the face, neck, or chest, and can spread to other parts of the body over time. Symptoms may include swelling, redness, pain, and the formation of pus-filled abscesses that may discharge a characteristic yellowish granular material called "sulfur granules." Treatment typically involves long-term antibiotic therapy, often requiring high doses and intravenous administration. Surgical drainage or removal of infected tissue may also be necessary in some cases.
Cervicofacial actinomycosis is a form of actinomycosis, which is a type of infection caused by the Actinomyces species of bacteria. These bacteria are normally found in the mouth, throat, and digestive system and are usually harmless. However, they can cause an infection if they are able to penetrate the mucosal lining of these areas, such as through trauma or injury.
Cervicofacial actinomycosis specifically affects the head and neck region. It often presents as a slowly progressive, painful, indurated (hardened) mass in the cervicofacial area, which can be accompanied by symptoms such as fever, weight loss, and fatigue. The infection can spread to surrounding tissues, including bone and muscle, and can form abscesses or fistulas that drain pus.
Cervicofacial actinomycosis is typically treated with high-dose antibiotics for an extended period of time, often several months. Surgical intervention may also be necessary to remove any areas of necrotic (dead) tissue or to drain abscesses. The prognosis for cervicofacial actinomycosis is generally good with appropriate treatment, although the infection can recur if not fully treated.
Actinomyces is a genus of gram-positive, rod-shaped bacteria that are normal inhabitants of the human mouth, colon, and urogenital tract. Under certain conditions, such as poor oral hygiene or tissue trauma, these bacteria can cause infections known as actinomycosis. These infections often involve the formation of abscesses or granulomas and can affect various tissues, including the lungs, mouth, and female reproductive organs. Actinomyces species are also known to form complex communities called biofilms, which can contribute to their ability to cause infection.
"Mycobacterium haemophilum" is a slow-growing, gram-positive, acid-fast bacterium that is a member of the Mycobacteriaceae family. It is an opportunistic pathogen that primarily causes skin and soft tissue infections in immunocompromised individuals, such as those with HIV/AIDS or organ transplant recipients. The bacterium requires enriched media containing hemoglobin or hemin for growth, which is why it is named "haemophilum." Infections caused by this bacterium can be difficult to diagnose and treat due to its slow growth rate and resistance to many first-line anti-tuberculosis drugs.
An Intrauterine Device (IUD) is a long-acting, reversible contraceptive device that is inserted into the uterus to prevent pregnancy. It is a small T-shaped piece of flexible plastic with strings attached to it for removal. There are two types of IUDs available: hormonal and copper. Hormonal IUDs release progestin, which thickens cervical mucus and thins the lining of the uterus, preventing sperm from reaching and fertilizing an egg. Copper IUDs, on the other hand, produce an inflammatory reaction in the uterus that is toxic to sperm and eggs, preventing fertilization.
IUDs are more than 99% effective at preventing pregnancy and can remain in place for several years, depending on the type. They are easily removable by a healthcare provider if a woman wants to become pregnant or choose another form of contraception. IUDs do not protect against sexually transmitted infections (STIs), so it is important to use condoms in addition to an IUD for protection against STIs.
In summary, Intrauterine Devices are small, T-shaped plastic devices that are inserted into the uterus to prevent pregnancy. They come in two types: hormonal and copper, both of which work by preventing fertilization. IUDs are highly effective, long-acting, and reversible forms of contraception.
Lymphadenitis is a medical term that refers to the inflammation of one or more lymph nodes, which are small, bean-shaped glands that are part of the body's immune system. Lymph nodes contain white blood cells called lymphocytes, which help fight infection and disease.
Lymphadenitis can occur as a result of an infection in the area near the affected lymph node or as a result of a systemic infection that has spread through the bloodstream. The inflammation causes the lymph node to become swollen, tender, and sometimes painful to the touch.
The symptoms of lymphadenitis may include fever, fatigue, and redness or warmth in the area around the affected lymph node. In some cases, the overlying skin may also appear red and inflamed. Lymphadenitis can occur in any part of the body where there are lymph nodes, including the neck, armpits, groin, and abdomen.
The underlying cause of lymphadenitis must be diagnosed and treated promptly to prevent complications such as the spread of infection or the formation of an abscess. Treatment may include antibiotics, pain relievers, and warm compresses to help reduce swelling and discomfort.
A "cheek" is the fleshy, muscular area of the face that forms the side of the face below the eye and above the jaw. It contains the buccinator muscle, which helps with chewing by moving food to the back teeth for grinding and also assists in speaking and forming facial expressions. The cheek also contains several sensory receptors that allow us to perceive touch, temperature, and pain in this area of the face. Additionally, there is a mucous membrane lining inside the mouth cavity called the buccal mucosa which covers the inner surface of the cheek.
The dental high-speed technique is a method used in dentistry that involves the use of an air-driven handpiece, also known as a "high-speed" handpiece, to remove tooth structure quickly and efficiently during various procedures such as cavity preparation or tooth reduction for restorations. The term "high-speed" refers to the rotation speed of the bur (cutting tool) in the handpiece, which can reach up to 400,000 revolutions per minute (RPM). This technique allows dentists to complete treatments more efficiently and with greater precision compared to using slower-speed handpieces.
The high-speed technique is commonly used for:
1. Removing decayed tooth structure during cavity preparation
2. Reducing tooth size or shape prior to placing restorations, such as crowns, veneers, or inlays/onlays
3. Smoothing rough surfaces on teeth or restorations
4. Trimming or shaping excess material from dental restorations
5. Sectioning teeth for easier removal or extraction
When performing high-speed techniques, dentists must exercise caution to avoid damaging healthy tooth structure, pulp exposure, or causing patient discomfort. They typically use water coolant and/or air to reduce heat generation and minimize potential damage to the tooth. Additionally, high-speed handpieces are often equipped with a built-in spray system that helps wash away debris and maintain visibility during procedures.
In summary, the dental high-speed technique is a valuable tool in modern dentistry for efficiently and precisely removing tooth structure or shaping restorations using an air-driven high-speed handpiece.
In medical terms, the "neck" is defined as the portion of the body that extends from the skull/head to the thorax or chest region. It contains 7 cervical vertebrae, muscles, nerves, blood vessels, lymphatic vessels, and glands (such as the thyroid gland). The neck is responsible for supporting the head, allowing its movement in various directions, and housing vital structures that enable functions like respiration and circulation.
Pelvic Inflammatory Disease (PID) is a medical condition characterized by inflammation of the reproductive organs in women, specifically the uterus, fallopian tubes, and/or ovaries. It is often caused by an infection that ascends from the cervix or vagina into the upper genital tract. The infectious agents are usually sexually transmitted bacteria such as Neisseria gonorrhoeae and Chlamydia trachomatis, but other organisms can also be responsible.
Symptoms of PID may include lower abdominal pain, irregular menstrual bleeding, vaginal discharge with an unpleasant odor, fever, painful sexual intercourse, or pain in the lower back. However, some women with PID may not experience any symptoms at all. If left untreated, PID can lead to serious complications such as infertility, ectopic pregnancy, and chronic pelvic pain.
Diagnosis of PID is typically based on a combination of clinical findings, physical examination, and laboratory tests. Treatment usually involves antibiotics to eradicate the infection and may also include pain management and other supportive measures. In some cases, hospitalization may be necessary for more intensive treatment or if complications arise.
In medical terms, the face refers to the front part of the head that is distinguished by the presence of the eyes, nose, and mouth. It includes the bones of the skull (frontal bone, maxilla, zygoma, nasal bones, lacrimal bones, palatine bones, inferior nasal conchae, and mandible), muscles, nerves, blood vessels, skin, and other soft tissues. The face plays a crucial role in various functions such as breathing, eating, drinking, speaking, seeing, smelling, and expressing emotions. It also serves as an important identifier for individuals, allowing them to be recognized by others.
Vascular malformations are abnormalities in the development and growth of blood vessels and lymphatic vessels that can occur anywhere in the body. They can be present at birth or develop later in life, and they can affect both the form and function of the affected tissues and organs. Vascular malformations can involve arteries, veins, capillaries, and/or lymphatic vessels, and they can range from simple, localized lesions to complex, multifocal disorders.
Vascular malformations are typically classified based on their location, size, flow characteristics, and the type of blood or lymphatic vessels involved. Some common types of vascular malformations include:
1. Capillary malformations (CMs): These are characterized by abnormal dilated capillaries that can cause red or pink discoloration of the skin, typically on the face or neck.
2. Venous malformations (VMs): These involve abnormal veins that can cause swelling, pain, and disfigurement in the affected area.
3. Lymphatic malformations (LMs): These involve abnormal lymphatic vessels that can cause swelling, infection, and other complications.
4. Arteriovenous malformations (AVMs): These involve a tangled mass of arteries and veins that can cause high-flow lesions, bleeding, and other serious complications.
5. Combined vascular malformations: These involve a combination of different types of blood or lymphatic vessels, such as capillary-lymphatic-venous malformations (CLVMs) or arteriovenous-lymphatic malformations (AVLMs).
The exact cause of vascular malformations is not fully understood, but they are believed to result from genetic mutations that affect the development and growth of blood vessels and lymphatic vessels. Treatment options for vascular malformations depend on the type, size, location, and severity of the lesion, as well as the patient's age and overall health. Treatment may include medication, compression garments, sclerotherapy, surgery, or a combination of these approaches.
A granuloma is a type of organized immune response that occurs when the body encounters a foreign substance that it cannot eliminate. A "foreign-body" granuloma specifically refers to this reaction in response to an exogenous material, such as a splinter, suture, or other types of medical implants.
Foreign-body granulomas are characterized by the formation of a collection of immune cells, including macrophages and lymphocytes, which surround and attempt to isolate the foreign material. Over time, this collection of immune cells can become walled off and form a well-circumscribed mass or nodule.
Foreign-body granulomas may cause localized symptoms such as pain, swelling, or inflammation, depending on their location and size. In some cases, they may also lead to complications such as infection or tissue damage. Treatment typically involves removing the foreign body, if possible, followed by anti-inflammatory therapy to manage any residual symptoms or complications.
Bronchial diseases refer to medical conditions that affect the bronchi, which are the large airways that lead into the lungs. These diseases can cause inflammation, narrowing, or obstruction of the bronchi, leading to symptoms such as coughing, wheezing, chest tightness, and difficulty breathing.
Some common bronchial diseases include:
1. Asthma: A chronic inflammatory disease of the airways that causes recurring episodes of wheezing, breathlessness, chest tightness, and coughing.
2. Chronic Bronchitis: A long-term inflammation of the bronchi that leads to a persistent cough and excessive mucus production.
3. Bronchiectasis: A condition in which the bronchi become damaged and widened, leading to chronic infection and inflammation.
4. Bronchitis: An inflammation of the bronchi that can cause coughing, wheezing, and chest tightness.
5. Emphysema: A lung condition that causes shortness of breath due to damage to the air sacs in the lungs. While not strictly a bronchial disease, it is often associated with chronic bronchitis and COPD (Chronic Obstructive Pulmonary Disease).
Treatment for bronchial diseases may include medications such as bronchodilators, corticosteroids, or antibiotics, as well as lifestyle changes such as quitting smoking and avoiding irritants. In severe cases, oxygen therapy or surgery may be necessary.
Oophoritis is a medical term that refers to the inflammation of one or both ovaries. It is often caused by an infection, which can be bacterial, viral, or fungal in nature. The infection can spread to the ovaries from other parts of the reproductive system, such as the fallopian tubes or the uterus.
Oophoritis can cause symptoms such as pelvic pain, abdominal cramping, irregular menstrual bleeding, and fever. In some cases, it may lead to complications such as infertility or chronic pelvic pain. Treatment typically involves antibiotics to clear the infection, as well as pain relief medications and anti-inflammatory drugs to manage symptoms.
It is important to note that oophoritis can be a serious condition, especially if left untreated. If you are experiencing any symptoms of oophoritis, it is important to seek medical attention promptly.
A pelvic infection, also known as pelvic inflammatory disease (PID), is a medical condition characterized by inflammation of the reproductive organs in females, including the uterus, fallopian tubes, ovaries, and surrounding tissues. It is often caused by an ascending infection from the cervix or vagina, commonly due to sexually transmitted bacteria such as Neisseria gonorrhoeae and Chlamydia trachomatis. However, other organisms can also cause pelvic infections.
Symptoms of pelvic infections may include lower abdominal pain, irregular menstrual bleeding, vaginal discharge with an unpleasant odor, fever, painful intercourse, and difficulty urinating. In some cases, pelvic infections may not cause any noticeable symptoms, making it challenging to diagnose the condition promptly.
If left untreated, pelvic infections can lead to serious complications such as chronic pelvic pain, infertility, ectopic pregnancy, and abscess formation in the reproductive organs. Treatment typically involves antibiotics to eradicate the infection, and in severe cases, hospitalization and surgical intervention may be necessary.
Actinomyces viscosus is a gram-positive, anaerobic, rod-shaped bacterium that is commonly found in the oral cavity and upper respiratory tract of humans. It is a normal resident of the human microbiota but can cause infections in immunocompromised individuals or when it gains access to deeper tissues, such as the pulp of teeth or the soft tissues of the head and neck.
Actinomyces viscosus has been associated with dental caries, periodontal disease, and endodontic infections. It can also cause actinomycosis, a chronic suppurative and granulomatous infection that typically affects the cervicofacial region, thorax, or abdomen.
The name "viscosus" refers to the sticky, mucoid appearance of the bacterial colonies when grown in culture. Actinomyces viscosus is closely related to other species of Actinomyces, such as A. israelii and A. gerencseriae, which can also cause actinomycosis.
Bacterial skin diseases are a type of infectious skin condition caused by various species of bacteria. These bacteria can multiply rapidly on the skin's surface when given the right conditions, leading to infection and inflammation. Some common bacterial skin diseases include:
1. Impetigo: A highly contagious superficial skin infection that typically affects exposed areas such as the face, hands, and feet. It is commonly caused by Staphylococcus aureus or Streptococcus pyogenes bacteria.
2. Cellulitis: A deep-skin infection that can spread rapidly and involves the inner layers of the skin and underlying tissue. It is often caused by Group A Streptococcus or Staphylococcus aureus bacteria.
3. Folliculitis: An inflammation of hair follicles, usually caused by an infection with Staphylococcus aureus or other bacteria.
4. Furuncles (boils) and carbuncles: Deep infections that develop from folliculitis when the infection spreads to surrounding tissue. A furuncle is a single boil, while a carbuncle is a cluster of boils.
5. Erysipelas: A superficial skin infection characterized by redness, swelling, and warmth in the affected area. It is typically caused by Group A Streptococcus bacteria.
6. MRSA (Methicillin-resistant Staphylococcus aureus) infections: Skin infections caused by a strain of Staphylococcus aureus that has developed resistance to many antibiotics, making it more difficult to treat.
7. Leptospirosis: A bacterial infection transmitted through contact with contaminated water or soil and characterized by flu-like symptoms and skin rashes.
Treatment for bacterial skin diseases usually involves the use of topical or oral antibiotics, depending on the severity and location of the infection. In some cases, drainage of pus-filled abscesses may be necessary to promote healing. Proper hygiene and wound care can help prevent the spread of these infections.
The ascending colon is the first part of the large intestine, which is the portion of the digestive system that follows the small intestine. It is called "ascending" because it travels upward from the right side of the abdomen toward the underside of the liver. The primary function of the ascending colon is to absorb water and electrolytes from digested food and prepare waste for elimination.
Lung diseases refer to a broad category of disorders that affect the lungs and other structures within the respiratory system. These diseases can impair lung function, leading to symptoms such as coughing, shortness of breath, chest pain, and wheezing. They can be categorized into several types based on the underlying cause and nature of the disease process. Some common examples include:
1. Obstructive lung diseases: These are characterized by narrowing or blockage of the airways, making it difficult to breathe out. Examples include chronic obstructive pulmonary disease (COPD), asthma, bronchiectasis, and cystic fibrosis.
2. Restrictive lung diseases: These involve stiffening or scarring of the lungs, which reduces their ability to expand and take in air. Examples include idiopathic pulmonary fibrosis, sarcoidosis, and asbestosis.
3. Infectious lung diseases: These are caused by bacteria, viruses, fungi, or parasites that infect the lungs. Examples include pneumonia, tuberculosis, and influenza.
4. Vascular lung diseases: These affect the blood vessels in the lungs, impairing oxygen exchange. Examples include pulmonary embolism, pulmonary hypertension, and chronic thromboembolic pulmonary hypertension (CTEPH).
5. Neoplastic lung diseases: These involve abnormal growth of cells within the lungs, leading to cancer. Examples include small cell lung cancer, non-small cell lung cancer, and mesothelioma.
6. Other lung diseases: These include interstitial lung diseases, pleural effusions, and rare disorders such as pulmonary alveolar proteinosis and lymphangioleiomyomatosis (LAM).
It is important to note that this list is not exhaustive, and there are many other conditions that can affect the lungs. Proper diagnosis and treatment of lung diseases require consultation with a healthcare professional, such as a pulmonologist or respiratory therapist.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Penicillins are a group of antibiotics derived from the Penicillium fungus. They are widely used to treat various bacterial infections due to their bactericidal activity, which means they kill bacteria by interfering with the synthesis of their cell walls. The first penicillin, benzylpenicillin (also known as penicillin G), was discovered in 1928 by Sir Alexander Fleming. Since then, numerous semi-synthetic penicillins have been developed to expand the spectrum of activity and stability against bacterial enzymes that can inactivate these drugs.
Penicillins are classified into several groups based on their chemical structure and spectrum of activity:
1. Natural Penicillins (e.g., benzylpenicillin, phenoxymethylpenicillin): These have a narrow spectrum of activity, mainly targeting Gram-positive bacteria such as streptococci and staphylococci. However, they are susceptible to degradation by beta-lactamase enzymes produced by some bacteria.
2. Penicillinase-resistant Penicillins (e.g., methicillin, oxacillin, nafcillin): These penicillins resist degradation by certain bacterial beta-lactamases and are primarily used to treat infections caused by staphylococci, including methicillin-susceptible Staphylococcus aureus (MSSA).
3. Aminopenicillins (e.g., ampicillin, amoxicillin): These penicillins have an extended spectrum of activity compared to natural penicillins, including some Gram-negative bacteria such as Escherichia coli and Haemophilus influenzae. However, they are still susceptible to degradation by many beta-lactamases.
4. Antipseudomonal Penicillins (e.g., carbenicillin, ticarcillin): These penicillins have activity against Pseudomonas aeruginosa and other Gram-negative bacteria with increased resistance to other antibiotics. They are often combined with beta-lactamase inhibitors such as clavulanate or tazobactam to protect them from degradation.
5. Extended-spectrum Penicillins (e.g., piperacillin): These penicillins have a broad spectrum of activity, including many Gram-positive and Gram-negative bacteria. They are often combined with beta-lactamase inhibitors to protect them from degradation.
Penicillins are generally well-tolerated antibiotics; however, they can cause allergic reactions in some individuals, ranging from mild skin rashes to life-threatening anaphylaxis. Cross-reactivity between different penicillin classes and other beta-lactam antibiotics (e.g., cephalosporins) is possible but varies depending on the specific drugs involved.
 Actinomycosis: Background, Pathophysiology, Epidemiology
Actinomycosis: Background, Pathophysiology, Epidemiology
 Cervicofacial actinomycosis: a case report
Cervicofacial actinomycosis: a case report
Actinomycosis: Background, Pathophysiology, Epidemiology
Pediatric Actinomycosis: Background, Pathophysiology, Etiology
 DailyMed - PENICILLIN G POTASSIUM- penicillin g injection, solution
DailyMed - PENICILLIN G POTASSIUM- penicillin g injection, solution
Dermatologic Aspects of Actinomycosis Workup: Approach Considerations, Laboratory Studies, Imaging Studies
 Penicillin G - GlobalRPH
Penicillin G - GlobalRPH
 Actinomycosis - Infections - MSD Manual Consumer Version
Actinomycosis - Infections - MSD Manual Consumer Version
 Cutaneous actinomycosis - Wikipedia
Cutaneous actinomycosis - Wikipedia
 IndexCat
IndexCat
 Osteomyelitis - References | BMJ Best Practice US
Osteomyelitis - References | BMJ Best Practice US
 Human actinomycosis. A study of 181 subjects - PubMed
Human actinomycosis. A study of 181 subjects - PubMed
 Clindamycin in the treatment of serious anaerobic infections - PubMed
Clindamycin in the treatment of serious anaerobic infections - PubMed
Pfizerpen, penicillin G potassium (penicillin G aqueous) dosing, indications, interactions, adverse effects, and more
Biomarkers Search
 PROC FORMAT for International Classification of Diseases, 10th Revision (ICD-10) codes
PROC FORMAT for International Classification of Diseases, 10th Revision (ICD-10) codes
Actinomycosis: Background, Pathophysiology, Epidemiology
 DeCS
DeCS
Code System Concept
 MeSH Browser
MeSH Browser
MeSH Browser
and
 Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS
Subjects: Zoonoses - Digital Collections - National Library of Medicine Search Results
 1,361 results in SearchWorks catalog
1,361 results in SearchWorks catalog
Actinomyces Odontolyticus Bacteremia - Volume 9, Number 12-December 2003 - Emerging Infectious Diseases journal - CDC
IndexCat
 Actinomycetes and Non Sporing Anaerobes MCQ Questions & Answers - Dapzoi
Actinomycetes and Non Sporing Anaerobes MCQ Questions & Answers - Dapzoi
 List of Publications
List of PublicationsThoracic8
- The most common clinical forms of actinomycosis are cervicofacial (ie, lumpy jaw), thoracic, and abdominal. (medscape.com)
- Thoracic actinomycosis accounts for 15-20% of cases. (medscape.com)
- Occasionally, thoracic actinomycosis results from the introduction of organisms via esophageal perforation, by direct spread from an actinomycotic process of the neck or abdomen, or via hematogenous spread from a distant lesion. (medscape.com)
- Thoracic actinomycosis commonly presents as a pulmonary infiltrate or mass, which, if left untreated, can spread to involve the pleura, pericardium, and chest wall, ultimately leading to the formation of sinuses that discharge sulfur granules. (medscape.com)
- Cervicofacial, pulmonary/thoracic and gastrointestinal forms exist, yet cervicofacial disease accounts for two-thirds of reported infections. (wikipedia.org)
- Actinomycosis, with infective arthritis and was given treat- on the other hand, affects the cervicofacial, ment but there was no improvement after 6 thoracic and abdominal regions. (who.int)
- Actinomycosis takes place most often in the cervicofacial place (50%-65%), followed by your thoracic (15%-30%) and abdominopelvic (20%) parts, yet rarely requires the neurological system. (syksignal.com)
- Thoracic manifestations include parenchymal, bronchiectatic, along with endobronchial actinomycosis. (syksignal.com)
Actinomyces5
- Gram-positive, pleomorphic non-spore-forming, non-acid-fast anaerobic or microaerophilic bacilli of the genus Actinomyces and the order Actinomycetales cause actinomycosis. (medscape.com)
- Actinomyces israelii , Actinomyces naeslundii, Actinomyces odontolyticus, Actinomyces viscosus, and Actinomyces meyeri most frequently cause human actinomycosis. (medscape.com)
- Actinomycosis is a chronic infection caused mainly by the anaerobic bacteria Actinomyces israelii . (msdmanuals.com)
- In 1877, Bollinger and Harz ( 3 ) named the genus Actinomyces when they described the etiologic agent of bovine actinomycosis ("lumpy jaw") and called it Actinomyces bovis . (cdc.gov)
- Bottom line: Our files suggest that cystatin C is quite a bit heritable as well as connected with arterial firmness amongst Afro-Caribbeans.Actinomycosis can be a long-term suppurative infection a result of Actinomyces kinds. (syksignal.com)
Pulmonary2
- Acute disseminated actinomycosis presenting as pneumonia with bilateral pulmonary nodules and pelvic osteomyelitis in an immunocompetent patient. (nih.gov)
- From worked out tomography, pulmonary actinomycosis usually looks like chronic segmental airspace loan consolidation made up of necrotic low-attenuation areas using side-line development. (syksignal.com)
Infection5
- Actinomycosis is a subacute-to-chronic bacterial infection caused by filamentous, gram-positive, non-acid-fast, anaerobic-to-microaerophilic bacteria. (medscape.com)
- Furthermore, actinomycosis is generally a polymicrobial infection, with isolates numbering as many as 5-10 bacterial species. (medscape.com)
- Cervicofacial actinomycosis is the most common type of the infection, comprising 50-70% of reported cases. (medscape.com)
- The radiologic findings of actinomycosis are variable and depend on the primary site involved by the infection, extension, and duration of disease. (medscape.com)
- Actinomycosis, an infection difficult to diagnose and requiring extremely prolonged antibiotic therapy]. (nih.gov)
Lumpy1
- A form of ACTINOMYCOSIS characterized by slow-growing inflammatory lesions of the lymph nodes that drain the mouth (lumpy jaw), reddening of the overlying skin, and intraperitoneal abscesses. (bvsalud.org)
Pelvic2
- In women, pelvic actinomycosis is possible. (medscape.com)
- Pelvic actinomycosis most commonly ascends from the uterus in association with intrauterine contraceptive devices (IUCDs). (medscape.com)
Diagnosis5
- The purpose of the present article is to report a case of cervicofacial actinomycosis, describing and discussing its methods of diagnosis, clinical course and treatment. (bvsalud.org)
- This clinical case of cervicofacial actinomycosis reported here emphasizes the importance of this condition and the need for an early diagnosis with a view to improving the quality of life of patients affected. (bvsalud.org)
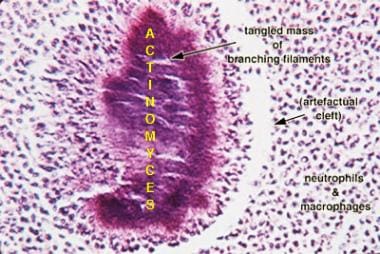
- This is not an exclusive finding of actinomycosis, and its absence does not rule out the diagnosis. (medscape.com)
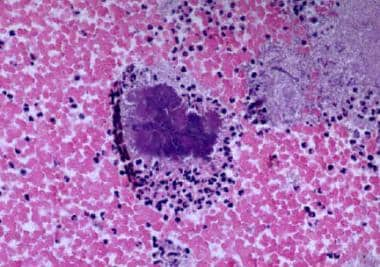
- Microscopic examination for the diagnosis of actinomycosis has been a major tool for years. (medscape.com)
- And related organisms in cervicofacial infections: Pathomechanism, diagnosis and therapeutic aspects. (u-szeged.hu)
Clinical1
- High clinical suspicion of actinomycosis should be followed by concurrent histological and microbiological evaluation of tissue, diagnostic imaging, and antibiotic treatment. (medscape.com)
Chronic2
- Actinomycosis is a chronic bacterial disease. (medscape.com)
- Cutaneous actinomycosis is a chronic disease that affects the deep subcutaneous tissue of the skin. (wikipedia.org)
Organism1
- However, this organism has never been convincingly proven to cause actinomycosis in humans ( 4 ), nor has it ever been isolated from human mucosa or other human sources. (cdc.gov)
Nocardia1
- Bacteria that masquerade as fungi: actinomycosis/nocardia. (nih.gov)
Lesion2
- Mandibular Actinomycosis Disguised as a Periapical Lesion. (nih.gov)
- In the serious type, cervicofacial condition may show itself together with soft-tissue puffiness, an excruciating pyogenic abscess, or perhaps a bulk lesion. (syksignal.com)
Dermatology1
- For additional information on actinomycosis, see the articles Actinomycosis (dermatology focus), Actinomycosis (pediatrics focus), and Actinomycosis (ophthalmology focus). (medscape.com)
Infectious1
- Actinomycosis is the most common infectious disease of kangaroos ( 7 ). (cdc.gov)
Disease1
- Actinomycosis is a disease of antiquity, having most likely infected the jaw of a fossil rhinoceros ( 1 ) and the ribs of a man discovered in southeastern Ontario, Canada, who by radiocarbon dating lived 230 A.D. + 55 ( 2 ). (cdc.gov)
Organs1
- Hematogenous dissemination to distant organs may occur in any stage of actinomycosis, whereas lymphatic dissemination is unusual. (medscape.com)
Manifestations1
- Specifically, they may be responsible for the early manifestations of actinomycosis and for treatment failures. (medscape.com)
Commonly1
- Oral and cervicofacial diseases are commonly associated with dental procedures, trauma, oral surgery, or dental sepsis. (medscape.com)
Intrauterine1
- Numerous reports have linked the use of intrauterine contraceptive devices to the development of actinomycosis of the female genital tract. (medscape.com)
Lymph1
- 10. [Cervicofacial actinomycosis in a patient treated by surgery of the lymph node due to laryngeal cancer: case report]. (nih.gov)
Soft-tissue1
- Cervicofacial actinomycosis is characterized in the initial stages by soft-tissue swelling of the perimandibular area. (medscape.com)
Generally2
- Many cases associated with cervicofacial actinomycosis are generally odontogenic throughout origin. (syksignal.com)
- Generally, actinomycosis reacts well in order to prescription antibiotic treatment, nevertheless long-term follow-up following treatment is required because of frequent goes back. (syksignal.com)
Treatment1
- Morphocycline in treatment of patients with actinomycoses]. (nih.gov)
Patients2
- Vandeplas et al presented a case series of six patients who developed cervicofacial actinomycosis following third molar extraction. (medscape.com)
- The major human pathogen for actinomycosis, A. israelii, was identified in two patients in 1878 and fully delineated by Israel ( 5 ). (cdc.gov)
Cases1
- Actinomycosis of the abdomen and pelvis accounts for 10-20% of reported cases. (medscape.com)
Human1
- Human actinomycosis. (nih.gov)
Forms1
- Actinomycosis has several forms. (msdmanuals.com)
Oral2
- Artroscopia operativa y apertura oral en el trastorno interno de la ATM. (ajman.ac.ae)
- Linfoma de Burkitt primario de la cavidad oral en una paciente con sida. (ajman.ac.ae)
Small1
- The particular image studies favoring abdominopelvic actinomycosis incorporate strong enhancement from the sound element of the size soon after comparison substance administration, small rim-enhancing abscesses from the size, and also extensive inflamation related extensions. (syksignal.com)
Patient1
- A case of actinomycosis and pseudo-actinomycosis in the same patient]. (nih.gov)