Peptic Ulcer Hemorrhage
Peptic Ulcer
Peptic Ulcer Perforation
Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. (1/305)
BACKGROUND AND METHODS: After endoscopic treatment to control bleeding of peptic ulcers, bleeding recurs in 15 to 20 percent of patients. In a prospective, randomized study, we compared endoscopic retreatment with surgery after initial endoscopy. Over a 40-month period, 1169 of 3473 adults who were admitted to our hospital with bleeding peptic ulcers underwent endoscopy to reestablish hemostasis. Of 100 patients with recurrent bleeding, 7 patients with cancer and 1 patient with cardiac arrest were excluded from the study; 48 patients were randomly assigned to undergo immediate endoscopic retreatment and 44 were assigned to undergo surgery. The type of operation used was left to the surgeon. Bleeding was considered to have recurred in the event of any one of the following: vomiting of fresh blood, hypotension and melena, or a requirement for more than four units of blood in the 72-hour period after endoscopic treatment. RESULTS: Of the 48 patients who were assigned to endoscopic retreatment, 35 had long-term control of bleeding. Thirteen underwent salvage surgery, 11 because retreatment failed and 2 because of perforations resulting from thermocoagulation. Five patients in the endoscopy group died within 30 days, as compared with eight patients in the surgery group (P=0.37). Seven patients in the endoscopy group (including 6 who underwent salvage surgery) had complications, as compared with 16 in the surgery group (P=0.03). The duration of hospitalization, the need for hospitalization in the intensive care unit and the resultant duration of that stay, and the number of blood transfusions were similar in the two groups. In multivariate analysis, hypotension at randomization (P=0.01) and an ulcer size of at least 2 cm (P=0.03) were independent factors predictive of the failure of endoscopic retreatment. CONCLUSIONS: In patients with peptic ulcers and recurrent bleeding after initial endoscopic control of bleeding, endoscopic retreatment reduces the need for surgery without increasing the risk of death and is associated with fewer complications than is surgery. (+info)Prevalence and cost of hospitalization for gastrointestinal complications related to peptic ulcers with bleeding or perforation: comparison of two national databases. (2/305)
The purpose of this study was to determine the prevalence and cost of hospitalization for upper gastrointestinal complications, including peptic ulcers with hemorrhage or perforation. Upper gastrointestinal complications and corresponding economic data were obtained from two sources. The first was a 20% sample of all community hospital discharges (about 6 million per year) from 11 states for 1991 and 1992 Hospital Cost Utilization Project; HCUP-3). The second source of data was a claims database for employees of large US corporations and their dependents for 1992, 1993, and 1994 (about 3.5 million covered lives per year; MarketScan). A group of ICD-9 codes for the diagnosis of peptic and gastroduodenal ulcers with bleeding or perforation were used to identify hospital admissions because of upper gastrointestinal complications. Similar patterns were observed across the MarketScan and HCUP-3 databases regarding hospitalization with diagnoses related to gastrointestinal complications identified according to the ICD-9 codes. The average age of patients with upper gastrointestinal complications was 66 years in the HCUP-3 database and 52 years in the MarketScan database. The average annual rates of upper gastrointestinal complications as a primary or secondary diagnosis were 6.4 and 6.7 per 1000 discharges for 1991 and 1992, respectively (HCUP-3), and 4.3, 4.2, and 4.9 per 1000 admissions for 1992, 1993, and 1994, respectively (MarketScan). The average length of stay for upper gastrointestinal complications as a primary diagnosis was 7.8 days in 1991 and 7.5 days in 1992 (HCUP-3) and 6.1, 5.1, and 5.1 days in 1992, 1993, and 1994, respectively (MarketScan). The national average total charge for hospitalization for gastrointestinal problems as a primary diagnosis was $12,970 in 1991 and $14,294 in 1992 (HCUP-3). The average total reimbursement for hospitalizations related to upper gastrointestinal problems was $15,309 in 1992, $12,987 in 1993, and $13,150 in 1994 (MarketScan). Hospital admissions for upper gastrointestinal complications are expensive. The rate and cost per admission are higher for the older population. The results on the elements covered by both databases are consistent. Therefore the databases complement each other on the type of information abstracted. (+info)Comparison of adrenaline injection and bipolar electrocoagulation for the arrest of peptic ulcer bleeding. (3/305)
BACKGROUND: Peptic ulcers with active bleeding or a non-bleeding visible vessel require aggressive endoscopic treatment. AIMS: To determine whether endoscopic adrenaline injection alone or contact probe therapy following injection is a suitable treatment for peptic ulcer bleeding. METHODS: A total of 96 patients with active bleeding or non-bleeding visible vessels received adrenaline alone, bipolar electrocoagulation alone, or combined treatment (n=32 in each group). RESULTS: Initial haemostasis was not achieved in one patient in the adrenaline group, two in the gold probe group, and two in the injection gold probe group (p>0.1). Rebleeding episodes were fewer in the injection gold probe group (2/30, 6.7%) than in the gold probe group (9/30, 30%, p=0.04) and in the adrenaline group (11/31, 35.5%, p=0.01). Treatment failure (other therapy required) was rarer in the injection gold probe group (4/32, 12.5%) than in the adrenaline group (12/32, 37.5%, p=0.04). The volume of blood transfused after entry of the study was less in the injection gold probe group (mean 491 ml) than in the adrenaline group (1548 ml, p<0. 0001) and the gold probe group (1105 ml, p<0.01). Duration of hospital stay, numbers of patients requiring urgent surgery, and death rate were not statistically different among the three groups. CONCLUSIONS: For patients with peptic ulcer bleeding, combined adrenaline injection and gold probe treatment offers an advantage in preventing rebleeding and decreasing the need for blood transfusion. (+info)Helicobacter pylori infection is a protective factor for bleeding gastric ulcers but not for bleeding duodenal ulcers in NSAID users. (4/305)
BACKGROUND: The effect of Helicobacter pylori infection on NSAID-induced gastroduodenal damage is unclear. AIM: To determine the role of H. pylori and NSAID use in complicated peptic ulcers. METHODS: A total of 185 consecutive patients with bleeding peptic ulcers and 185 hospitalized matched controls were studied prospectively. Additionally, 75 consecutive uncomplicated peptic ulcers and 75 community controls were also studied. Active H. pylori infection was determined by urea breath test and/or both urease test and histology. Serum CagA and VacA status were determined at random in 135 infected patients and 82 controls. NSAID use was determined by structured data collection. RESULTS: H. pylori (odds ratio [OR]=5. 98; 2.9-12.3) and NSAID use (OR=5.74; 3.4-9.7) were independent risk factors for duodenal ulcer bleeding, whereas NSAID use was the main risk factor for bleeding gastric ulcers (OR=12.4; 5.5-27.9). Interaction of both factors was associated with reduced risk for bleeding gastric ulcers (OR=0.19; 0.04-0.88) but not for bleeding duodenal ulcers, which showed a similar risk to any one factor alone. This was observed for all types of NSAID use, including low-dose aspirin, and infection by CagA positive strains. H. pylori was the only factor involved in common uncomplicated duodenal ulcers. CONCLUSION: Interaction of both H. pylori infection and NSAID use decreases the risk of bleeding due to gastric ulcers, but not that due to duodenal ulcers. (+info)Peptic ulcer bleeding: accessory risk factors and interactions with non-steroidal anti-inflammatory drugs. (5/305)
AIMS: To determine risk factors for peptic ulcer bleeding other than non-steroidal anti-inflammatory drugs (NSAIDs). Methods-Data on possible antecedent risk factors obtained in a large case control study of 1121 patients admitted to hospitals in Glasgow, Newcastle, Nottingham, Oxford, and Portsmouth with bleeding peptic ulcers were compared with the same information obtained in 989 population controls. Data were analysed by logistic regression with the calculation of odds ratios (OR) and 95% confidence intervals (CI). RESULTS: From a logistic regression model, oral anticoagulants (OR 7. 8; 95% CI 2.8-21.5), previous peptic ulcer (3.8; 2.6-4.9), treatment for heart failure (5.9; 2.3-13.1), oral corticosteroid use (2.7; 1. 3-4.5), treatment for diabetes (3.1; 1.2-4.3), and current smoking (1.6; 1.2-2.0) were all independent risk factors. No association was found with use of calcium channel antagonists. Odds ratios for concomitant NSAID usage were multiplicative with the exception of current smoking. CONCLUSIONS: Some 45% of admissions for peptic ulcer bleeding in England and Wales in those aged 60 or more are calculated to be attributable to, or associated with, these accessory risk factors, which, together with those associated with aspirin or other NSAID use will account for over 80% of predisposing factors to ulcer bleeding. (+info)Risk of ulcer bleeding in patients infected with Helicobacter pylori taking non-steroidal anti-inflammatory drugs. (6/305)
OBJECTIVE: To determine whether Helicobacter pylori is an independent risk factor for bleeding peptic ulcer in users of non-steroidal anti-inflammatory drugs (NSAIDs), including aspirin. DESIGN: A prospective matched case-control study. SETTING: Odense University Hospital, Denmark. SUBJECTS: 132 patients with a bleeding peptic ulcer (n=124) or haemorrhagic gastritis (n=8) at endoscopy who had taken an NSAID in the previous week and 136 controls who had taken NSAIDs without gastrointestinal complications. The controls were recruited from rheumatology and geriatric outpatient clinics. MEASUREMENTS: H pylori status assessed by serology and 13C-urea breath test and regarded as positive if either test was positive. Data on potential confounding factors including smoking and alcohol were collected by interview. MAIN RESULT: H pylori was present in 57% of cases and 43% of controls. The adjusted odds ratio of bleeding from a peptic ulcer owing to H pylori infection in NSAID users was 1.81 (95% CI 1.02 to 3.21) and was similar in aspirin and non-aspirin NSAID users. Peptic ulcer bleeding was also statistically significantly associated with a history of previous ulcer bleeding, dyspepsia within the previous 3 months, drinking alcohol but not with smoking. About 16% of bleeding peptic ulcers in NSAID users could be attributed to H pylori infection. CONCLUSION: NSAID users infected with H pylori have an almost doubled risk of bleeding peptic ulcer compared with uninfected NSAID users. (+info)Low sensitivity of invasive tests for the detection of Helicobacter pylori infection in patients with bleeding ulcer. (7/305)
BACKGROUND: A high false negative rate for antral infection with Helicobacter pylori when assessed by rapid urease test has recently been reported in patients with bleeding ulcer. This result could partly explain the differing prevalence of H. pylori infection in bleeding and non-bleeding ulcers. AIMS: To evaluate the accuracy of a rapid urease test (UT), histology and culture for detection of H. pylori in antral biopsies from acute bleeding peptic ulcer patients using a serological test as reference. PATIENTS AND METHODS: All consecutive patients with active bleeding gastric or duodenal ulcer at endoscopic examination admitted in six university hospitals in France were considered for inclusion. Five antral biopsies were taken during the diagnostic endoscopy for UT, culture and histology. A blood sample was taken for H. pylori serology. RESULTS: One hundred and eighty one patients were included and 129 (71%) had a positive serology. The sensitivity of UT, histology and culture for detection of H. pylori infection were 41%, 33% and 34%, respectively. The sensitivity and specificity of the combination of the three invasive tests were 48.8% (95% CI: 40.2-57.4) and 90.6% (95% CI: 82. 6-99) respectively. In the 52 serologically negative patients, only 5 had at least one invasive positive test. The sensitivity of the invasive tests decreased significantly with age but was not influenced by NSAIDs intake. Of 80 patients with a positive serological test and negative histological evaluation for H. pylori, chronic antral inflammation was found in 70 patients (87%). In 46 patients with both negative serological test and H. pylori negative test according to histology, only 13 (28%) had chronic antral inflammation. CONCLUSIONS: The sensitivity of invasive tests for detection of H. pylori is low during acute ulcer bleeding, and they should be used with caution in this condition. A serological test is recommended to identify patients with H. pylori infection in spite of negative invasive tests. (+info)Overall mortality among patients surviving an episode of peptic ulcer bleeding. (8/305)
STUDY OBJECTIVE: The authors investigated whether patients who have survived an acute episode of peptic ulcer bleeding (PUB) have an excess long term all cause mortality compared with the general population free of PUB. DESIGN: Follow up study of previously identified cohort of patients with a PUB episode and a general population cohort. SETTING: The source population included all people aged 30 to 89 years, registered with general practitioners in the United Kingdom. PATIENTS: All patients alive one month after the PUB episode constituted the cohort of PUB patients (n = 978). A control group of 5000 people was randomly sampled from the source population. The same eligibility criteria as for patients with PUB were applied to the control series. Also, controls had to be free of PUB before start date. MAIN RESULTS: Relative risk of mortality among PUB patients was 2.1, 95% CI: 1.7, 2.6) compared with the general population. This increased mortality risk occurred mainly in the patients less than 60 years old. No difference was observed between men and women. The excess mortality was not only circumscribed to deaths attributable to recurrent gastrointestinal bleed, but also cardiovascular, cancer and other causes. CONCLUSIONS: People who have survived an acute episode of PUB have a reduced long term survival compared with the general population. This reduction was stronger among middle age patients than in the elderly. (+info)Peptic ulcer hemorrhage is a medical condition characterized by bleeding in the gastrointestinal tract due to a peptic ulcer. Peptic ulcers are open sores that develop on the lining of the stomach, lower esophagus, or small intestine. They are usually caused by infection with the bacterium Helicobacter pylori or long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs).
When a peptic ulcer bleeds, it can cause symptoms such as vomiting blood or passing black, tarry stools. In severe cases, the bleeding can lead to shock, which is a life-threatening condition characterized by a rapid heartbeat, low blood pressure, and confusion. Peptic ulcer hemorrhage is a serious medical emergency that requires immediate treatment. Treatment may include medications to reduce stomach acid, antibiotics to eliminate H. pylori infection, and endoscopic procedures to stop the bleeding. In some cases, surgery may be necessary to repair the ulcer or remove damaged tissue.
A peptic ulcer is a sore or erosion in the lining of your stomach and the first part of your small intestine (duodenum). The most common causes of peptic ulcers are bacterial infection and long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin, ibuprofen, or naproxen.
The symptoms of a peptic ulcer include abdominal pain, often in the upper middle part of your abdomen, which can be dull, sharp, or burning and may come and go for several days or weeks. Other symptoms can include bloating, burping, heartburn, nausea, vomiting, loss of appetite, and weight loss. Severe ulcers can cause bleeding in the digestive tract, which can lead to anemia, black stools, or vomit that looks like coffee grounds.
If left untreated, peptic ulcers can result in serious complications such as perforation (a hole through the wall of the stomach or duodenum), obstruction (blockage of the digestive tract), and bleeding. Treatment for peptic ulcers typically involves medications to reduce acid production, neutralize stomach acid, and kill the bacteria causing the infection. In severe cases, surgery may be required.
Peptic ulcer perforation is a serious and sightful gastrointestinal complication characterized by the penetration or erosion of an acid-peptic ulcer through the full thickness of the stomach or duodenal wall, resulting in spillage of gastric or duodenal contents into the peritoneal cavity. This leads to chemical irritation and/or bacterial infection of the abdominal cavity, causing symptoms such as sudden severe abdominal pain, tenderness, rigidity, and potentially life-threatening sepsis if not promptly diagnosed and treated with surgical intervention, antibiotics, and supportive care.
A stomach ulcer, also known as a gastric ulcer, is a sore that forms in the lining of the stomach. It's caused by a breakdown in the mucous layer that protects the stomach from digestive juices, allowing acid to come into contact with the stomach lining and cause an ulcer. The most common causes are bacterial infection (usually by Helicobacter pylori) and long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs). Stomach ulcers may cause symptoms such as abdominal pain, bloating, heartburn, and nausea. If left untreated, they can lead to more serious complications like internal bleeding, perforation, or obstruction.
 Recent trends in admissions and mortality due to peptic ulcer in England: increasing frequency of haemorrhage among older...
Recent trends in admissions and mortality due to peptic ulcer in England: increasing frequency of haemorrhage among older... High-Dose Pantoprazole Continuous Infusion and Patients With Peptic Ulcer
High-Dose Pantoprazole Continuous Infusion and Patients With Peptic Ulcer Peptic ulcer: MedlinePlus Medical Encyclopedia
Peptic ulcer: MedlinePlus Medical Encyclopedia K27.4 - Chronic or unspecified peptic ulcer, site unspecified, with hemorrhage - ICD List 2023
K27.4 - Chronic or unspecified peptic ulcer, site unspecified, with hemorrhage - ICD List 2023 Peptic Ulcer Disease - Gastrointestinal Disorders - MSD Manual Professional Edition
Peptic Ulcer Disease - Gastrointestinal Disorders - MSD Manual Professional Edition DailyMed - PROPAFENONE- propafenone hydrochloride capsule, extended release
DailyMed - PROPAFENONE- propafenone hydrochloride capsule, extended release Astringent - Wikipedia
Astringent - Wikipedia Chapter 15: Peptic Ulcer Disease - NIDDK
Chapter 15: Peptic Ulcer Disease - NIDDK IndexCat
IndexCat Peptic Ulcer II - Subacute Ulcer of Stomach
Peptic Ulcer II - Subacute Ulcer of Stomach Increased mortality in prostate carcinoma and smoking-related disease after parietal cell vagotomy: A long-term follow-up study...
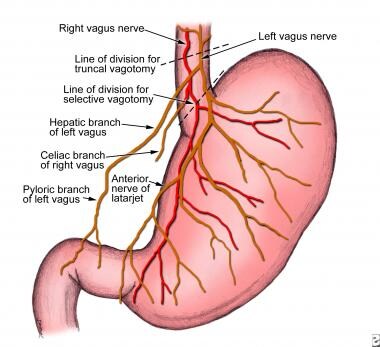
Increased mortality in prostate carcinoma and smoking-related disease after parietal cell vagotomy: A long-term follow-up study... ZONTIVITY Dosage & Rx Info | Uses, Side Effects
ZONTIVITY Dosage & Rx Info | Uses, Side Effects Molecules | Free Full-Text | Preventative and Therapeutic Potential of Flavonoids in Peptic Ulcers
Molecules | Free Full-Text | Preventative and Therapeutic Potential of Flavonoids in Peptic Ulcers Correspondence - The British Journal of Cardiology
Correspondence - The British Journal of Cardiology Zilretta (Triamcinolone Acetonide Extended-Release Injectable Suspension): Uses, Dosage, Side Effects, Interactions, Warning
Zilretta (Triamcinolone Acetonide Extended-Release Injectable Suspension): Uses, Dosage, Side Effects, Interactions, Warning Virtual Clinic - The patient with peptic ulcer disease - PCSG
Virtual Clinic - The patient with peptic ulcer disease - PCSG National Nursing Home Survey, 1977
National Nursing Home Survey, 1977 Iron deficiency symptoms: Tinnitus - ringing in the ear - could indicate the condition | Express.co.uk
Iron deficiency symptoms: Tinnitus - ringing in the ear - could indicate the condition | Express.co.uk DeCS
DeCS