Hydatidiform Mole
Hydatidiform Mole, Invasive
Trophoblastic Neoplasms
Choriocarcinoma
Gestational Trophoblastic Disease
Pregnancy Complications, Neoplastic
Moles
Pregnancy
Placenta
Abortion, Spontaneous
Chorionic Villi
Cyclin-Dependent Kinase Inhibitor p57
Chorionic Gonadotropin
Hydrops Fetalis
Pregnancy-Specific beta 1-Glycoproteins
Chorionic Gonadotropin, beta Subunit, Human
Pregnancy Trimester, First
Abortion, Threatened
Trophoblasts
Genomic Imprinting
Intrauterine Devices, Copper
Intrauterine Device Migration
Uterine Perforation
Coagulation and fibrinolysis in intact hydatidiform molar pregnancy. (1/227)
Tests of coagulation, fibrinolysis, and platelet function were performed in 17 patients with intact molar pregnancies. Women with intact molar pregnancies had higher fibrinogen factor VIII, and fibrinogen degradation products, concentrations and lower prothrombin, factor X, plasminogen, and plasminogen activator concentrations than controls with normal pregnancies. They also had reduced platelet counts and thromboelastographic values, which indicated hypocoagulability. These results suggest that intravascular coagulation occurs in intact hydatidiform molar pregnancies. (+info)Genetic mapping of a maternal locus responsible for familial hydatidiform moles. (2/227)
Hydatidiform mole (HM) is the product of an aberrant human pregnancy in which there is an abnormal embryonic development and proliferation of placental villi. The incidence of HM varies between ethnic groups, and occurs in 1 in every 1500 pregnancies in the USA. All HM cases are sporadic, except for extremely rare familial cases. The exact mechanisms leading to molar pregnancies are unknown. We previously postulated that women with recurrent hydatidiform moles are homozygous for an autosomal recessive defective gene. To map this gene genetically, we initiated a genome-wide scan with highly polymorphic short tandem repeats in individuals from two families with recurrent HM. Here, we demonstrate that a defective maternal gene is responsible for recurrent HM. This gene resides on chromosome 19q13.3-13.4 in a 15.2 cM interval flanked by D19S924 and D19S890. The identification of a gene for HM adds new insights into the molecular genetics of early embryogenesis and may be relevant to the large number of patients with sporadic HM. (+info)Delivery of a severely anaemic fetus after partial molar pregnancy: clinical and ultrasonographic findings. (3/227)
The incidence of a normal live fetus and a partial molar placenta is extremely rare. Although triploidy is the most frequent association, a fetus with normal karyotype can survive in cases of partial molar pregnancy. We report a case of partial molar placenta in which a live female baby was delivered at 32 weeks gestation by a 30-year-old woman. At the 18th week, ultrasonographic examination revealed a normal fetus with a huge, multicystic placenta. Chromosomal evaluation by amniocentesis revealed a normal female karyotype (46,XX), and serial biometric measurement of the fetus showed normal growth during pregnancy. There were no obstetric complications until the 32nd gestational week when preterm rupture of the membranes occurred. The electronic fetal heart beat tracing showed a repeated sinusoid pattern and late deceleration after admission. The patient underwent emergency Caesarean section and delivered a 1551-g, anaemic female baby with an Apgar score of 1, 4 and 6 at 1, 5 and 10 min, respectively. The baby recovered within 2 weeks after respiratory support and transfusion of packed red blood cells. Although anaemia is one of the risk factors that jeopardize the fetus in the case of partial molar pregnancy, termination is not indicated when the fetus is normal and no complications have occurred. (+info)The contribution of maternal serum markers in the early prenatal diagnosis of molar pregnancies. (4/227)
The aim of this study was to evaluate the usefulness of maternal serum markers in the early prenatal diagnosis of molar pregnancies. The ultrasound features, cytogenetic and histopathological findings of 10 cases of molar pregnancy diagnosed at 11-13 weeks of gestation were compared retrospectively with the maternal serum concentrations of human chorionic gonadotrophin (HCG), alpha fetoprotein (AFP), pregnancy-associated plasma protein A (PAPP-A) and pregnancy-specific beta1-glycoprotein (SP1). Free beta-HCG and intact HCG concentrations were very high [> or = 2.5 multiples of the median (MoM)] in all cases. AFP concentrations were extremely low in all cases of singleton complete moles (< or = 0.5 MoM) and were high in one case of twin complete mole, in one case of triploid partial mole and two cases of euploid partial mole (> or = 2.5 MoM). Serum PAPP-A and SP1 were high in complete moles. The combined use of ultrasound features, maternal serum proteins and fetal cytogenetic findings should enable the early differential diagnosis in utero and perinatal management of those molar pregnancies presenting with an anatomically normal fetus. (+info)Efficient approach to unique single-nucleotide polymorphism discovery. (5/227)
Single-nucleotide polymorphisms (SNPs) are the most frequently found DNA sequence variations in the human genome. It has been argued that a dense set of SNP markers can be used to identify genetic factors associated with complex disease traits. Because all high-throughput genotyping methods require precise sequence knowledge of the SNPs, any SNP discovery approach must involve both the determination of DNA sequence and allele frequencies. Furthermore, high-throughput genotyping also requires a genomic DNA amplification step, making it necessary to develop sequence-tagged sites (STSs) that amplify only the DNA fragment containing the SNP and nothing else from the rest of the genome. In this report, we demonstrate the utility of a SNP-screening approach that yields the DNA sequence and allele frequency information while screening out duplications with minimal cost and effort. Our approach is based on the use of a homozygous complete hydatidiform mole (CHM) as the reference. With this homozygous reference, one can identify and estimate the allele frequencies of common SNPs with a pooled DNA-sequencing approach (rather than having to sequence numerous individuals as is commonly done). More importantly, the CHM reference is preferable to a single individual reference because it reveals readily any duplicated regions of the genome amplified by the PCR assay before the duplicated sequences are found in GenBank. This approach reduces the cost of SNP discovery by 60% and eliminates the costly development of SNP markers that cannot be amplified uniquely from the genome. (+info)DNA flow cytometric quantification and DNA polymorphism analysis in the case of a complete mole with a coexisting fetus. (6/227)
PURPOSE: Our purpose was to investigate whether DNA flow cytometric quantification and DNA polymorphism analysis are useful for cytogenetic diagnosis in the case of a complete hydatidiform mole that coexists with a living fetus. METHODS: Flow cytometric analysis of the nuclear DNA content and polymerase chain reaction (PCR) amplification of the minisatellite locus with the MCT118 probe were performed on the tissues (fetus, placenta and mole) obtained at the initial evacuation. RESULTS: DNA histograms of placental, fetal, and molar tissues showed diploid peaks. PCR products demonstrated that the allele of the mole was homozygous and inherited solely from the husband and that the mole differed genetically from the fetus and the placenta. CONCLUSIONS: These results suggested that DNA flow cytometry and DNA polymorphism analysis may be useful for the cytogenetic diagnosis of a complete hydatidiform mole and a coexisting fetus. (+info)Sonographic appearance of early complete molar pregnancies. (7/227)
Since our anecdotal experience indicates that the classically described "snowstorm" appearance on ultrasonography of early molar pregnancies is often not present and that theca-lutein cysts are also rare, we examined the ultrasonographic appearance of early complete molar pregnancies. We reviewed the ultrasonographic reports and clinical data of 21 cases of histologically diagnosed complete molar pregnancies with a mean gestational age at sonography of 10.5 weeks (range, 4 to 18 weeks). The diagnosis of molar pregnancy was made on ultrasonography in 12 (57%) cases, was second in the differential diagnosis of one (4.8%) case, and was not considered in eight (38%) cases. No theca-lutein cysts were identified. Five of five (100%) molar pregnancies of 13 weeks or over were diagnosed prospectively, while only eight of 16 (50%) earlier pregnancies were correctly diagnosed prospectively. In a retrospective review of the available images of 16 patients, only nine of 16 (56%) images demonstrated the classic appearance, and no theca-lutein cysts were seen. We conclude that the classic appearance of complete moles on ultrasonography is seen in less than two thirds of cases and even less commonly in the first trimester. The prevalence of theca-lutein cysts is very low. (+info)Purification and characterization of urinary choriogonadotropin from patients with hydatidiform mole. (8/227)
Human choriogonadotropin was isolated from urine of patients with hydatidiform mole by acid and salt precipitation, immunoaffinity, and DEAE-Sephadex chromatography. Polyacrylamide gel electrophoresis, immunodiffusion, immunoelectrophoresis, and NH2-terminal amino acid analysis showed that the product obtained is essentially homogeneous. This choriogonadotropin was found to resemble the choriogonadotropin from urine of normal pregnant women in amino acid composition but to differ from it in having a lower content of N-acetylglucosamine and mannose. (+info)A hydatidiform mole, also known as a molar pregnancy, is a type of gestational trophoblastic disease (GTD), which is a group of rare disorders that involve abnormal growth of the placental tissue.
In a hydatidiform mole, there is an abnormal fertilization event leading to the growth of a mass of grapelike cysts in the uterus instead of a normal pregnancy. The chromosomes from the sperm and egg do not combine properly, resulting in an extra set of chromosomes, which leads to the development of the mole.
Hydatidiform moles can be complete or partial:
* Complete hydatidiform mole (CHM): This type arises when an egg without a nucleus is fertilized by one or two sperm, leading to the growth of abnormal placental tissue with no embryo. The chromosomes come from the father only, and there are typically 46 chromosomes, all of paternal origin.
* Partial hydatidiform mole (PHM): This type occurs when an egg is fertilized by two sperm or a single sperm that duplicates itself, resulting in an abnormal placenta with some fetal tissue. The chromosomes are of both maternal and paternal origin, and the placental tissue has a mix of normal and abnormal cells.
Hydatidiform moles can cause vaginal bleeding, rapid uterine enlargement, and high levels of human chorionic gonadotropin (hCG) hormone in the blood. They are usually detected during an ultrasound exam and require medical treatment to prevent complications such as gestational trophoblastic neoplasia, a malignant form of GTD that can spread to other organs.
An invasive hydatidiform mole (IHM) is a rare and aggressive complication of a gestational trophoblastic disease (GTD), which itself originates from the abnormal proliferation of trophoblastic cells, the tissue that normally develops into the placenta during pregnancy. IHMs are characterized by the invasion of molar villi into the myometrium (the muscular layer of the uterus) and can potentially spread to other organs through the bloodstream, leading to distant metastases.
IHMs usually arise from a complete hydatidiform mole (CHM), which is an abnormal conceptus with no embryonic or fetal development. CHMs are typically diploid and originate from the fertilization of an egg without genetic material (an empty egg or an egg with two sets of paternal chromosomes) by one or two sperm cells. This results in a conceptus with only paternal chromosomes, which leads to uncontrolled proliferation of trophoblastic tissue and the formation of grapelike vesicles filled with fluid (hydatidiform moles).
Invasive hydatidiform moles can cause various symptoms, such as vaginal bleeding, pelvic pain, or the presence of an enlarged uterus. They also pose a risk for developing choriocarcinoma, another type of gestational trophoblastic neoplasia (GTN), which is a malignant tumor that can metastasize and spread to other organs. Proper diagnosis and timely treatment are crucial to prevent severe complications and improve the prognosis for patients with IHMs. Treatment usually involves surgical removal of the mole, followed by chemotherapy to eliminate any residual disease and reduce the risk of GTN development.
Uterine neoplasms refer to abnormal growths in the uterus, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from different types of cells within the uterus, leading to various types of uterine neoplasms. The two main categories of uterine neoplasms are endometrial neoplasms and uterine sarcomas.
Endometrial neoplasms develop from the endometrium, which is the inner lining of the uterus. Most endometrial neoplasms are classified as endometrioid adenocarcinomas, arising from glandular cells in the endometrium. Other types include serous carcinoma, clear cell carcinoma, and mucinous carcinoma.
Uterine sarcomas, on the other hand, are less common and originate from the connective tissue (stroma) or muscle (myometrium) of the uterus. Uterine sarcomas can be further divided into several subtypes, such as leiomyosarcoma, endometrial stromal sarcoma, and undifferentiated uterine sarcoma.
Uterine neoplasms can cause various symptoms, including abnormal vaginal bleeding or discharge, pelvic pain, and difficulty urinating or having bowel movements. The diagnosis typically involves a combination of imaging tests (such as ultrasound, CT, or MRI scans) and tissue biopsies to determine the type and extent of the neoplasm. Treatment options depend on the type, stage, and patient's overall health but may include surgery, radiation therapy, chemotherapy, or hormone therapy.
Trophoblastic neoplasms are a group of rare tumors that originate from the trophoblast, which is the outer layer of cells that surrounds a developing embryo and helps to form the placenta during pregnancy. These tumors can be benign or malignant and are characterized by their ability to produce human chorionic gonadotropin (hCG), a hormone that is normally produced during pregnancy.
There are several types of trophoblastic neoplasms, including:
1. Hydatidiform mole: A benign growth that forms in the uterus when a fertilized egg implants but does not develop into a normal embryo. There are two types of hydatidiform moles: complete and partial. Complete moles have no fetal tissue, while partial moles have some fetal tissue.
2. Invasive mole: A malignant form of hydatidiform mole that invades the uterine wall and may spread to other parts of the body.
3. Choriocarcinoma: A rapidly growing and highly invasive malignant tumor that can arise from a hydatidiform mole, a normal pregnancy, or an ectopic pregnancy. It can spread quickly to other parts of the body, such as the lungs, liver, and brain.
4. Placental site trophoblastic tumor (PSTT): A rare type of trophoblastic neoplasm that arises from the cells that attach the placenta to the uterine wall. It is usually slow-growing but can be aggressive in some cases.
5. Epithelioid trophoblastic tumor (ETT): Another rare type of trophoblastic neoplasm that arises from the cells that form the placental villi. It is typically low-grade and has a good prognosis, but it can recur in some cases.
The treatment for trophoblastic neoplasms depends on the type and stage of the tumor. Treatment options may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. Regular monitoring of hCG levels is also important to ensure that the tumor has been completely removed and to detect any recurrence early.
Choriocarcinoma is a rapidly growing and invasive type of gestational trophoblastic disease (GTD), which are abnormal growths that develop in the tissues that are supposed to become the placenta during pregnancy. It occurs when a malignant tumor develops from trophoblast cells, which are normally found in the developing embryo and help to form the placenta.
Choriocarcinoma can occur after any type of pregnancy, including normal pregnancies, molar pregnancies (a rare mass that forms inside the uterus after conception), or ectopic pregnancies (when a fertilized egg implants outside the uterus). It is characterized by the presence of both trophoblastic and cancerous cells, which can produce human chorionic gonadotropin (hCG) hormone.
Choriocarcinoma can spread quickly to other parts of the body, such as the lungs, liver, brain, or vagina, through the bloodstream. It is important to diagnose and treat choriocarcinoma early to prevent serious complications and improve the chances of a successful treatment outcome. Treatment typically involves surgery, chemotherapy, or radiation therapy.
Gestational Trophoblastic Disease (GTD) is a group of rare pregnancy-related disorders that involve abnormal growth of cells inside a woman's uterus. These cells are part of the placenta, which provides nutrients to the developing fetus. GTD occurs when some of these cells grow in an uncontrolled way, forming tumors or tumor-like growths.
There are several types of GTD:
1. Hydatidiform Mole (HM): Also known as a molar pregnancy, this is the most common type of GTD. It occurs when an egg that has no genetic information is fertilized by a sperm and then divides into multiple copies. This results in a growth that resembles a cluster of grapes, rather than a developing fetus. There are two types of HMs: complete and partial. A complete HM forms when an empty egg is fertilized by two sperms, resulting in no fetal tissue. A partial HM forms when a normal egg is fertilized by two sperm or an abnormal egg with two sets of genetic material, resulting in some fetal tissue.
2. Invasive Mole: This type of GTD occurs when cells from a molar pregnancy invade the uterine wall and surrounding tissues. It can also spread to other parts of the body, such as the lungs or brain.
3. Choriocarcinoma: This is a rare form of GTD that develops from trophoblastic cells and forms a malignant tumor. It can grow rapidly and spread quickly to other organs.
4. Placental Site Trophoblastic Tumor (PSTT): This is an even rarer type of GTD that forms in the tissue where the placenta attaches to the uterus. PSTTs are usually slow-growing but can sometimes spread to other parts of the body.
5. Epithelioid Trophoblastic Tumor (ETT): This is a very rare type of GTD that forms in the tissue where the placenta attaches to the uterus. ETTs are usually slow-growing and have a good prognosis.
It's important to note that most molar pregnancies do not develop into more serious forms of GTD, but regular follow-up care is necessary to monitor for any signs of progression. Treatment options depend on the type and stage of GTD and may include surgery, chemotherapy, or radiation therapy.
Neoplastic pregnancy complications refer to the abnormal growth of cells (neoplasia) that can occur during pregnancy. These growths can be benign or malignant and can arise from any type of tissue in the body. However, when they occur in pregnant women, they can pose unique challenges due to the potential effects on the developing fetus and the changes in the mother's body.
Some common neoplastic pregnancy complications include:
1. Gestational trophoblastic disease (GTD): This is a group of rare tumors that occur in the uterus during pregnancy. GTD can range from benign conditions like hydatidiform mole to malignant forms like choriocarcinoma.
2. Breast cancer: Pregnancy-associated breast cancer (PABC) is a type of breast cancer that occurs during pregnancy or within one year after delivery. It can be aggressive and challenging to diagnose due to the changes in the breast tissue during pregnancy.
3. Cervical cancer: Cervical cancer can occur during pregnancy, and its management depends on the stage of the disease and the gestational age. In some cases, treatment may need to be delayed until after delivery.
4. Lung cancer: Pregnancy does not increase the risk of lung cancer, but it can make diagnosis and treatment more challenging.
5. Melanoma: Melanoma is the most common malignant skin cancer during pregnancy. It can spread quickly and requires prompt treatment.
The management of neoplastic pregnancy complications depends on several factors, including the type and stage of the tumor, gestational age, and the patient's wishes. In some cases, surgery, chemotherapy, or radiation therapy may be necessary. However, these treatments can have potential risks to the developing fetus, so a multidisciplinary team of healthcare providers is often involved in the care of pregnant women with neoplastic complications.
A mole (nevus) is a benign growth on the skin that is usually brown or black. Moles can appear anywhere on the body, alone or in groups. Most adults have between 10 and 40 moles. They typically appear during childhood and adolescence. Some moles may change over time, possibly becoming raised and/or changing color. It's important to keep an eye on moles and see a healthcare provider if any changes are noticed, as melanoma, a type of skin cancer, can develop from moles.
It is also worth noting that there are different types of moles including congenital nevi (moles present at birth), dysplastic nevi (atypical moles) and acquired nevi (moles that appear after birth). Dysplastic nevi are larger than average and irregular in shape, with color variations. They are more likely to develop into melanoma than regular moles.
Pregnancy is a physiological state or condition where a fertilized egg (zygote) successfully implants and grows in the uterus of a woman, leading to the development of an embryo and finally a fetus. This process typically spans approximately 40 weeks, divided into three trimesters, and culminates in childbirth. Throughout this period, numerous hormonal and physical changes occur to support the growing offspring, including uterine enlargement, breast development, and various maternal adaptations to ensure the fetus's optimal growth and well-being.
A "missed abortion" is a medical term used to describe a pregnancy in which the fetus has died or failed to develop, but the products of conception (i.e., the placenta and gestational sac) remain in the uterus. This condition is also sometimes referred to as a "silent miscarriage" or "delayed miscarriage." In a missed abortion, there may be no symptoms or only very mild ones, such as vaginal bleeding or the passing of tissue. The diagnosis is typically made through an ultrasound exam that shows an empty gestational sac or a non-viable fetus. Treatment options include waiting for the body to expel the products of conception naturally, taking medication to induce expulsion, or undergoing a surgical procedure to remove the products of conception.
The placenta is an organ that develops in the uterus during pregnancy and provides oxygen and nutrients to the growing baby through the umbilical cord. It also removes waste products from the baby's blood. The placenta attaches to the wall of the uterus, and the baby's side of the placenta contains many tiny blood vessels that connect to the baby's circulatory system. This allows for the exchange of oxygen, nutrients, and waste between the mother's and baby's blood. After the baby is born, the placenta is usually expelled from the uterus in a process called afterbirth.
Spontaneous abortion, also known as miscarriage, is the unintentional expulsion of a nonviable fetus from the uterus before the 20th week of gestation. It is a common complication of early pregnancy, with most miscarriages occurring during the first trimester. Spontaneous abortion can have various causes, including chromosomal abnormalities, maternal health conditions, infections, hormonal imbalances, and structural issues of the uterus or cervix. In many cases, the exact cause may remain unknown.
The symptoms of spontaneous abortion can vary but often include vaginal bleeding, which may range from light spotting to heavy bleeding; abdominal pain or cramping; and the passing of tissue or clots from the vagina. While some miscarriages occur suddenly and are immediately noticeable, others may progress slowly over several days or even weeks.
In medical practice, healthcare providers often use specific terminology to describe different stages and types of spontaneous abortion. For example:
* Threatened abortion: Vaginal bleeding during early pregnancy, but the cervix remains closed, and there is no evidence of fetal demise or passing of tissue.
* Inevitable abortion: Vaginal bleeding with an open cervix, indicating that a miscarriage is imminent or already in progress.
* Incomplete abortion: The expulsion of some but not all products of conception from the uterus, requiring medical intervention to remove any remaining tissue.
* Complete abortion: The successful passage of all products of conception from the uterus, often confirmed through an ultrasound or pelvic examination.
* Missed abortion: The death of a fetus in the uterus without any expulsion of the products of conception, which may be discovered during routine prenatal care.
* Septic abortion: A rare and life-threatening complication of spontaneous abortion characterized by infection of the products of conception and the surrounding tissues, requiring prompt medical attention and antibiotic treatment.
Healthcare providers typically monitor patients who experience a spontaneous abortion to ensure that all products of conception have been expelled and that there are no complications, such as infection or excessive bleeding. In some cases, medication or surgical intervention may be necessary to remove any remaining tissue or address other issues related to the miscarriage. Counseling and support services are often available for individuals and couples who experience a spontaneous abortion, as they may face emotional challenges and concerns about future pregnancies.
Chorionic villi are finger-like projections of the chorion, which is the outermost extraembryonic membrane in a developing embryo. These structures are composed of both fetal and maternal tissues and play a crucial role in the early stages of pregnancy by providing a site for exchange of nutrients and waste products between the mother and the developing fetus.
Chorionic villi contain fetal blood vessels that are surrounded by stromal cells, trophoblasts, and connective tissue. They are formed during the process of implantation, when the fertilized egg attaches to the uterine wall. The chorionic villi continue to grow and multiply as the placenta develops, eventually forming a highly vascular and specialized organ that supports fetal growth and development throughout pregnancy.
One important function of chorionic villi is to serve as the site for the production of human chorionic gonadotropin (hCG), a hormone that can be detected in the mother's blood and urine during early pregnancy. This hormone plays a critical role in maintaining pregnancy by signaling the corpus luteum to continue producing progesterone, which helps to prevent menstruation and support fetal growth.
Abnormalities in chorionic villi can lead to various pregnancy complications, such as miscarriage, stillbirth, or intrauterine growth restriction. For this reason, chorionic villus sampling (CVS) is a diagnostic procedure that may be performed during early pregnancy to obtain fetal cells for genetic testing and diagnosis of chromosomal abnormalities or other genetic disorders.
Cyclin-dependent kinase inhibitor p57, also known as CDKN1C or p57KIP2, is a protein that regulates the cell cycle and acts as a tumor suppressor. It inhibits the activity of cyclin-dependent kinases (CDKs), which are enzymes that play crucial roles in regulating the cell cycle and transitioning from one phase to another.
The p57 protein is encoded by the CDKN1C gene, which is located on chromosome 11p15.5. This region is known as an imprinted gene cluster, meaning that only one copy of the gene is active, depending on whether it is inherited from the mother or father. In the case of p57, the paternal allele is usually silenced, and only the maternal allele is expressed.
Mutations in the CDKN1C gene can lead to several developmental disorders, including Beckwith-Wiedemann syndrome (BWS), a condition characterized by overgrowth, abdominal wall defects, and an increased risk of childhood tumors. Loss of function mutations in CDKN1C have also been associated with an increased risk of cancer, particularly Wilms' tumor, a type of kidney cancer that typically affects children.
In summary, cyclin-dependent kinase inhibitor p57 is a protein that regulates the cell cycle and acts as a tumor suppressor by inhibiting the activity of CDKs. Mutations in the CDKN1C gene can lead to developmental disorders and an increased risk of cancer.
Chorionic Gonadotropin (hCG) is a hormone that is produced during pregnancy. It is produced by the placenta after implantation of the fertilized egg in the uterus. The main function of hCG is to prevent the disintegration of the corpus luteum, which is a temporary endocrine structure that forms in the ovary after ovulation and produces progesterone during early pregnancy. Progesterone is essential for maintaining the lining of the uterus and supporting the pregnancy.
hCG can be detected in the blood or urine as early as 10 days after conception, and its levels continue to rise throughout the first trimester of pregnancy. In addition to its role in maintaining pregnancy, hCG is also used as a clinical marker for pregnancy and to monitor certain medical conditions such as gestational trophoblastic diseases.
Hydrops Fetalis is a serious condition characterized by the accumulation of excessive fluid in two or more fetal compartments, including the abdomen (ascites), around the heart (pericardial effusion), and/or within the lungs (pleural effusion). This accumulation can also affect the skin, causing it to become edematous. Hydrops Fetalis is often associated with various underlying causes, such as chromosomal abnormalities, congenital infections, genetic disorders, and structural defects that impair the fetus's ability to maintain fluid balance. In some cases, the cause may remain unknown. The prognosis for Hydrops Fetalis is generally poor, with a high mortality rate, although early detection and appropriate management can improve outcomes in certain situations.
Pregnancy-specific beta-1 glycoproteins (PSBGs), also known as SP1 or SP-1, are a group of proteins that are produced in large quantities by the placenta during pregnancy. They were first discovered in 1974 and are found in the serum of pregnant women. These proteins belong to the immunoglobulin superfamily and are involved in various physiological processes during pregnancy, such as implantation, placentation, and fetal development.
PSBGs have been identified as potential markers for early pregnancy diagnosis, as their levels start to rise shortly after conception and can be detected in the maternal bloodstream within days of implantation. They also play a role in the regulation of immune responses during pregnancy, helping to prevent the mother's immune system from attacking the developing fetus.
There are several isoforms of PSBGs, including PSBG1, PSBG2, and PSBG3, which differ in their molecular weight and other biochemical properties. The function of these different isoforms is not fully understood, but they may have distinct roles in the regulation of pregnancy-related processes.
It's worth noting that while PSBGs are produced during pregnancy, they can also be found in non-pregnant individuals, albeit at much lower levels. The exact role of PSBGs outside of pregnancy is not well understood and requires further research.
Chorionic Gonadotropin, beta Subunit, Human (β-hCG) is a protein that is produced by the placenta during pregnancy. It is a component of human chorionic gonadotropin (hCG), which is a hormone that is composed of two subunits: alpha and beta. The β-hCG subunit is specific to hCG and is not found in other hormones, making it a useful marker for pregnancy and certain medical conditions.
During early pregnancy, the levels of β-hCG increase rapidly and can be detected in the blood and urine. This has led to the development of pregnancy tests that detect the presence of β-hCG to confirm pregnancy. In addition to its role in pregnancy, β-hCG is also used as a tumor marker for certain types of cancer, such as germ cell tumors and choriocarcinoma.
Elevated levels of β-hCG may indicate the presence of a molar pregnancy, a condition in which a fertilized egg implants in the uterus but does not develop properly. In some cases, a molar pregnancy can become cancerous and require treatment. Therefore, monitoring β-hCG levels during pregnancy is important for detecting any potential complications.
The first trimester of pregnancy is defined as the period of gestational development that extends from conception (fertilization of the egg by sperm) to the end of the 13th week. This critical phase marks significant transformations in both the mother's body and the growing embryo/fetus.
During the first trimester, the fertilized egg implants into the uterine lining (implantation), initiating a series of complex interactions leading to the formation of the placenta - an organ essential for providing nutrients and oxygen to the developing fetus while removing waste products. Simultaneously, the embryo undergoes rapid cell division and differentiation, giving rise to various organs and systems. By the end of the first trimester, most major structures are present, although they continue to mature and grow throughout pregnancy.
The mother may experience several physiological changes during this time, including:
- Morning sickness (nausea and vomiting)
- Fatigue
- Breast tenderness
- Frequent urination
- Food aversions or cravings
- Mood swings
Additionally, hormonal shifts can cause various symptoms and prepare the body for potential changes in lactation, posture, and pelvic alignment as pregnancy progresses. Regular prenatal care is crucial during this period to monitor both maternal and fetal wellbeing, identify any potential complications early on, and provide appropriate guidance and support throughout the pregnancy.
A "threatened abortion" is a medical term used to describe a situation in which there are symptoms that suggest an impending miscarriage, such as vaginal bleeding and/or cramping during early pregnancy, but the cervix remains closed and the fetal heartbeat is still present. This condition is estimated to occur in up to 20-30% of all pregnancies, and while it can be a source of anxiety for pregnant individuals, it does not necessarily mean that a miscarriage will definitely occur.
It's important to note that if you are experiencing any symptoms of a threatened abortion, you should contact your healthcare provider right away for evaluation and guidance on how to manage the situation. They may recommend bed rest, pelvic rest, or other treatments to help support the pregnancy and reduce the risk of miscarriage.
Trophoblasts are specialized cells that make up the outer layer of a blastocyst, which is a hollow ball of cells that forms in the earliest stages of embryonic development. In humans, this process occurs about 5-6 days after fertilization. The blastocyst consists of an inner cell mass (which will eventually become the embryo) and an outer layer of trophoblasts.
Trophoblasts play a crucial role in implantation, which is the process by which the blastocyst attaches to and invades the lining of the uterus. Once implanted, the trophoblasts differentiate into two main layers: the cytotrophoblasts (which are closer to the inner cell mass) and the syncytiotrophoblasts (which form a multinucleated layer that is in direct contact with the maternal tissues).
The cytotrophoblasts proliferate and fuse to form the syncytiotrophoblasts, which have several important functions. They secrete enzymes that help to degrade and remodel the extracellular matrix of the uterine lining, allowing the blastocyst to implant more deeply. They also form a barrier between the maternal and fetal tissues, helping to protect the developing embryo from the mother's immune system.
Additionally, trophoblasts are responsible for the formation of the placenta, which provides nutrients and oxygen to the developing fetus and removes waste products. The syncytiotrophoblasts in particular play a key role in this process by secreting hormones such as human chorionic gonadotropin (hCG), which helps to maintain pregnancy, and by forming blood vessels that allow for the exchange of nutrients and waste between the mother and fetus.
Abnormalities in trophoblast development or function can lead to a variety of pregnancy-related complications, including preeclampsia, intrauterine growth restriction, and gestational trophoblastic diseases such as hydatidiform moles and choriocarcinomas.
Genomic imprinting is a epigenetic process that leads to the differential expression of genes depending on their parental origin. It involves the methylation of certain CpG sites in the DNA, which results in the silencing of one of the two copies of a gene, either the maternal or paternal allele. This means that only one copy of the gene is active and expressed, while the other is silent.
This phenomenon is critical for normal development and growth, and it plays a role in the regulation of genes involved in growth and behavior. Genomic imprinting is also associated with certain genetic disorders, such as Prader-Willi and Angelman syndromes, which occur when there are errors in the imprinting process that lead to the absence or abnormal expression of certain genes.
It's important to note that genomic imprinting is a complex and highly regulated process that is not yet fully understood. Research in this area continues to provide new insights into the mechanisms underlying gene regulation and their impact on human health and disease.
An Intrauterine Device (IUD) is a long-acting, reversible contraceptive device that is inserted into the uterus to prevent pregnancy. It is a small T-shaped piece of flexible plastic with strings attached to it for removal. There are two types of IUDs available: hormonal and copper. Hormonal IUDs release progestin, which thickens cervical mucus and thins the lining of the uterus, preventing sperm from reaching and fertilizing an egg. Copper IUDs, on the other hand, produce an inflammatory reaction in the uterus that is toxic to sperm and eggs, preventing fertilization.
IUDs are more than 99% effective at preventing pregnancy and can remain in place for several years, depending on the type. They are easily removable by a healthcare provider if a woman wants to become pregnant or choose another form of contraception. IUDs do not protect against sexually transmitted infections (STIs), so it is important to use condoms in addition to an IUD for protection against STIs.
In summary, Intrauterine Devices are small, T-shaped plastic devices that are inserted into the uterus to prevent pregnancy. They come in two types: hormonal and copper, both of which work by preventing fertilization. IUDs are highly effective, long-acting, and reversible forms of contraception.
An Intrauterine Device (IUD) is a small, T-shaped device that is inserted into the uterus to prevent pregnancy. The copper IUD is a type of long-acting reversible contraception (LARC) that releases copper ions, which are toxic to sperm and egg, preventing fertilization. It is one of the most effective forms of birth control available, with a failure rate of less than 1%.
The copper IUD can be used by women who have previously given birth as well as those who have not. It can be inserted up to five days after unprotected intercourse as emergency contraception to prevent pregnancy. Once inserted, the copper IUD can remain in place for up to ten years, although it can be removed at any time if a woman wants to become pregnant or for other reasons.
Copper IUDs are also used as an effective treatment for heavy menstrual bleeding and can be used to manage endometriosis-associated pain. Common side effects of copper IUDs include heavier and longer menstrual periods, cramping during insertion, and irregular periods during the first few months after insertion. However, these side effects usually subside over time.
It is important to note that while copper IUDs are highly effective at preventing pregnancy, they do not protect against sexually transmitted infections (STIs). Therefore, it is still recommended to use condoms or other barrier methods of protection during sexual activity to reduce the risk of STIs.
An intrauterine device (IUD) is a small, T-shaped birth control device that is inserted into the uterus to prevent pregnancy. A medicated IUD is a type of IUD that contains hormones, which are released slowly over time to provide additional benefits beyond just contraception.
There are two types of medicated IUDs available in the US market: levonorgestrel-releasing intrauterine system (LNG-IUS) and the copper intrauterine device (Cu-IUD). The LNG-IUS releases a progestin hormone called levonorgestrel, which thickens cervical mucus to prevent sperm from reaching the egg, thins the lining of the uterus to make it less likely for a fertilized egg to implant, and can also inhibit ovulation in some women. The Cu-IUD is non-hormonal and works by releasing copper ions that create a toxic environment for sperm, preventing them from reaching the egg.
Medicated IUDs are highly effective at preventing pregnancy, with typical use failure rates of less than 1% per year. They can remain in place for several years, depending on the brand, and can be removed at any time by a healthcare provider if a woman wants to become pregnant or experience side effects. Common side effects of medicated IUDs may include irregular menstrual bleeding, cramping, and spotting between periods, although these tend to improve over time.
Intrauterine Device (IUD) expulsion is a medical condition that refers to the unintentional and partial or complete removal of an IUD from the uterus after its initial insertion. This can occur spontaneously or as a result of manipulation, and it may happen soon after insertion or even several months or years later.
IUD expulsion is more common in women who have not previously given birth, and it can increase the risk of unintended pregnancy and other complications. Symptoms of IUD expulsion may include irregular menstrual bleeding, pelvic pain, or the absence of the IUD strings in the vagina. If a woman suspects that her IUD has been expelled, she should contact her healthcare provider for further evaluation and management.
Intrauterine Device (IUD) migration is a medical condition where the IUD, a long-acting reversible contraceptive device placed inside the uterus, moves from its original position. Normally, an IUD is designed to remain in the uterus, with the vertical strings attached to it trailing down through the cervix into the vagina, allowing for easy removal or checking of its position.
IUD migration refers to the unintended movement of the device, either partially or completely, outside the uterine cavity. This may occur due to various reasons such as a weakened uterus, infection, or anatomical abnormalities. The migration can lead to complications like perforation of the uterus, damage to nearby organs, and difficulty in removing or locating the IUD. Regular check-ups with healthcare providers are essential to ensure that the IUD remains in its proper place and to address any potential issues early on.
Uterine perforation is a medical condition that refers to the piercing or puncturing of the uterine wall. This can occur during various medical procedures such as dilatation and curettage (D&C), insertion of an intrauterine device (IUD), or during childbirth. It can also be caused by trauma or infection. Uterine perforation can lead to serious complications, such as bleeding, infection, and damage to surrounding organs. If left untreated, it can be life-threatening. Symptoms of uterine perforation may include severe abdominal pain, heavy vaginal bleeding, fever, and signs of shock. Immediate medical attention is required for proper diagnosis and treatment.
Contraceptive agents, female, are medications or devices specifically designed to prevent pregnancy in women. They work by interfering with the normal process of ovulation, fertilization, or implantation of a fertilized egg in the uterus. Some common examples of female contraceptive agents include:
1. Hormonal methods: These include combined oral contraceptives (COCs), progestin-only pills, patches, vaginal rings, and hormonal implants. They contain synthetic forms of the female hormones estrogen and/or progesterone, which work by preventing ovulation, thickening cervical mucus to make it harder for sperm to reach the egg, or thinning the lining of the uterus to prevent implantation of a fertilized egg.
2. Intrauterine devices (IUDs): These are small, T-shaped devices made of plastic or copper that are inserted into the uterus by a healthcare provider. They release hormones or copper ions that interfere with sperm movement and prevent fertilization or implantation.
3. Barrier methods: These include condoms, diaphragms, cervical caps, and sponges. They work by physically preventing sperm from reaching the egg.
4. Emergency contraception: This includes medications such as Plan B or Ella, which can be taken up to 5 days after unprotected sex to prevent pregnancy. They work by delaying ovulation or preventing fertilization of the egg.
5. Fertility awareness-based methods (FABMs): These involve tracking a woman's menstrual cycle and avoiding sexual intercourse during her fertile window. Some FABMs also involve using barrier methods during this time.
It is important to note that different contraceptive agents have varying levels of effectiveness, side effects, and risks. Women should consult with their healthcare provider to determine the best method for their individual needs and circumstances.
 Invasive hydatidiform mole
Invasive hydatidiform mole
Molar pregnancy
List of OMIM disorder codes
Trophoblast
Gestational choriocarcinoma
Polyploidy
Gestational trophoblastic disease
Sylvia Lawler
NLRP7
John William Magarey Lawton
Cyclin-dependent kinase inhibitor 1C
Theca lutein cyst
Pregnancy-specific beta-1-glycoprotein 1
PSG2
Pre-embryo
Occludin
Anne Hutchinson
PSG6
Eclampsia
PSG10
Breus' mole
PHLDA2
Cytotrophoblast
HYMAI
List of ICD-9 codes 630-679: complications of pregnancy, childbirth, and the puerperium
Goitre
Sentinel Returns
Choriocarcinoma
Gynaecology
Placental disease
Invasive hydatidiform mole - Wikipedia
 Hydatidiform mole: MedlinePlus Medical Encyclopedia
Hydatidiform mole: MedlinePlus Medical Encyclopedia
 Hydatidiform Mole: Practice Essentials, Background, Pathophysiology
Hydatidiform Mole: Practice Essentials, Background, Pathophysiology
 Hydatidiform mole
Hydatidiform mole
 hydatidiform mole - definition and meaning
hydatidiform mole - definition and meaning
 A distinct pattern in the DNA ploidy histograms of hydatidiform moles and nonmolar abortuses is caused by accumulation of...
A distinct pattern in the DNA ploidy histograms of hydatidiform moles and nonmolar abortuses is caused by accumulation of...
Genetic refinement and physical mapping of a biparental complete hydatidiform mole locus on chromosome 19q13.4. | Journal of...
Corrigendum to 'Reprogramming of human peripheral blood mononuclear cells from a patient suffering from recurrent hydatidiform...
 Is Ki-67 of Diagnostic Value in Distinguishing Between Partial and Complete Hydatidiform Moles? A Systematic Review and Meta...
Is Ki-67 of Diagnostic Value in Distinguishing Between Partial and Complete Hydatidiform Moles? A Systematic Review and Meta...
Hydatidiform Mole Imaging: Overview, Computed Tomography, Magnetic Resonance Imaging
A case of a hydatidiform mole in a 56-year-old woman | International Journal of Gynecologic Cancer
 What are the signs and symptoms of hydatidiform mole? - Studybuff.com
What are the signs and symptoms of hydatidiform mole? - Studybuff.com
 CMU Intellectual Repository: Heuristic neural network approach in histological sections detection of hydatidiform mole
CMU Intellectual Repository: Heuristic neural network approach in histological sections detection of hydatidiform mole
 Gestational Trophoblastic Disease | Choose the Right Test
Gestational Trophoblastic Disease | Choose the Right Test
 Role of paternal and maternal genomes in mouse development | Nature
Role of paternal and maternal genomes in mouse development | Nature
 The Danish Mole Project - Forskning - Aarhus Universitet
The Danish Mole Project - Forskning - Aarhus Universitet
Centralized surveillance of hydatidiform mole: 7-year experience from a regional hospital in China | International Journal of...
View of Transient hyperthyroidism in a woman with hydatidiform mole: a case report on unusual clinical presentation and...
 A complete hydatidiform mole and coexisting viable fetus in a twin pregnancy: a case report with literature review. | J Matern...
A complete hydatidiform mole and coexisting viable fetus in a twin pregnancy: a case report with literature review. | J Matern...
 8 Early Signs And Symptoms Of Pregnancy Implantation
8 Early Signs And Symptoms Of Pregnancy Implantation
 Lack of involvement of known DNA methyltransferases in familial hydatidiform mole implies the involvement of other factors in...
Lack of involvement of known DNA methyltransferases in familial hydatidiform mole implies the involvement of other factors in...
Gestational Trophoblastic Neoplasia Medication: Antineoplastics, Chemotherapy modulating agent
 British Medical Journal: 2 (617) | The BMJ
British Medical Journal: 2 (617) | The BMJ
Correction | The BMJ
 Additional file 2 of miR-30a targets STOX2 to increase cell proliferation and metastasis in hydatidiform moles via ERK, AKT,...
Additional file 2 of miR-30a targets STOX2 to increase cell proliferation and metastasis in hydatidiform moles via ERK, AKT,...
 Lainie P. Martin, MD profile | PennMedicine.org
Lainie P. Martin, MD profile | PennMedicine.org
 Home - Professor Michael Seckl
Home - Professor Michael Seckl
 Yes, IUDs Are Abortifacients. Here's Why.
Yes, IUDs Are Abortifacients. Here's Why.
 A-Z fact sheets | The Royal Women's Hospital
A-Z fact sheets | The Royal Women's Hospital
 Block 7 Reproduction Creighton Univ W Xpl Pt 4 - ProProfs Quiz
Block 7 Reproduction Creighton Univ W Xpl Pt 4 - ProProfs Quiz
Choriocarcinoma8
- In very few cases of complete HM, moles develop into a choriocarcinoma. (medlineplus.gov)
- 2000) Choriocarcinoma and partial hydatidiform moles. (imperial.ac.uk)
- Robbins states that 1 in 40 hydatidiform moles will give rise to choriocarcinoma (7th ed pg 1113). (proprofs.com)
- In 1929, Aschheim (using the A-Z bioassay) reported greatly elevated urine hCG results in two forms of gestational trophoblastic disease (GTD), choriocarcinoma and hydatidiform mole, and in these cases urines often required 1/200 dilution (5). (ibms.org)
- To study the expression of nuclear β-catenin and Ki-67 in patients with normal gestation products (NGP), complete hydatidiform moles (CHM), and choriocarcinoma to elucidate their roles in carcinogenesis and their interrelations. (bmj.com)
- Gestational trophoblastic diseases are a heterogenous group of conditions ranging from the benign hydatidiform mole to the malignant choriocarcinoma. (annals.edu.sg)
- In many cases a hydatiform mole , another term for choriocarcinoma, may spontaneously dissolve on its own and be expelled. (nethealthbook.com)
- Cancerous tumors located in the placenta: These tumors (called gestational trophoblastic neoplasia) include placental-site trophoblastic tumor, epithelioid trophoblastic tumor, choriocarcinoma, and invasive mole. (msdmanuals.com)
Recurrent hydatidiform mole5
- p.W195X) in a patient that appears to be associated with recurrent hydatidiform mole. (medscape.com)
- Corrigendum to 'Reprogramming of human peripheral blood mononuclear cells from a patient suffering from recurrent hydatidiform mole to an iPSC line FAHZUi001-A carrying a homozygous p.Gln421Ter mutation in NLRP7 gene' [Stem Cell Res. (stembook.org)
- Recurrent hydatidiform mole is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell have mutations. (studybuff.com)
- The risk is increased significantly after two molar pregnancies, and familial recurrent hydatidiform mole syndrome (caused by NLRP7 or KHDC3L gene variants) should be suspected. (arupconsult.com)
- We have previously shown in humans that an analogous inherited failure to establish imprinting at multiple loci in the female germline underlies a rare phenotype of recurrent hydatidiform mole. (biomedcentral.com)
Partial and Complete Hydatidiform Moles3
- Is Ki-67 of Diagnostic Value in Distinguishing Between Partial and Complete Hydatidiform Moles? (iiarjournals.org)
- Background/Aim: To demonstrate the value of Ki-67 in distinguishing between partial and complete hydatidiform moles. (iiarjournals.org)
- Updated diagnostic criteria for partial and complete hydatidiform moles in early pregnancy. (jabfm.org)
Malignant1
- Gestational trophoblastic neoplasia (GTN) is a malignant disorder that includes invasive moles, choriocarcinomas, placental site trophoblastic tumors, and epithelioid trophoblastic tumors. (arupconsult.com)
Pregnancy14
- Hydatidiform mole (HM) is a rare mass or growth that forms inside the womb (uterus) at the beginning of a pregnancy. (medlineplus.gov)
- A hydatidiform mole (molar pregnancy) is a gestational trophoblastic disease. (medscape.com)
- By studying elective pregnancy terminations, hydatidiform moles were determined to occur in approximately 1 in 1200 pregnancies. (medscape.com)
- A case of a 56-year-old woman with a mole pregnancy and a human chorionic gonadotropin (HCG)-induced thyreotoxicosis is presented. (bmj.com)
- A molar pregnancy (also called a hydatidiform mole or HM) is a tumor (growth) that develops in the uterus (womb) at the beginning of pregnancy. (studybuff.com)
- Hydatidiform moles result in greatly increased production of hCG, and hCG testing should be performed when a molar pregnancy is suspected and may help differentiate between a PHM and a CHM. (arupconsult.com)
- Hydatidiform mole (HM) is an abnormal pregnancy, characterized by trophoblastic hyperplasia, vesicular swelling of the chorionic villi, and without a viable fetus. (au.dk)
- A complete hydatidiform mole and coexisting viable fetus in a twin pregnancy: a case report with literature review. (bvsalud.org)
- A twin pregnancy involving a hydatidiform mole (HM) coexisting with a developing fetus is an extremely rare obstetric complication, which typically presents as a complete hydatidiform mole with a coexisting fetus (CHMCF) or a partial hydatidiform mole with a coexisting fetus (PHMCF). (bvsalud.org)
- Gestational trophoblastic disease (GTD) is usually identified as a hydatidiform mole (a molar pregnancy) or as gestational trophoblastic neoplasia (GTN). (cancercenter.com)
- Invasive mole , which is a type of molar pregnancy that has the potential to metastasize . (cancercenter.com)
- A molar pregnancy (hydatidiform mole) and other types of gestational trophoblastic disease are growth of an abnormal fertilized egg or an overgrowth of tissue from the placenta. (msdmanuals.com)
- Most often, a molar pregnancy is an abnormal fertilized egg that develops into a hydatidiform mole rather than a fetus. (msdmanuals.com)
- Women who have a molar pregnancy (hydatidiform mole) feel as if they are pregnant. (msdmanuals.com)
Fetus1
- The partial hydatidiform mole is characterized by a diandric triploid conceptus, accompanying focal trophoblastic hyperplasia and villous hydrops, and an ascertainable fetus. (iiarjournals.org)
Choriocarcinomas3
- These include complete and partial moles, placental site trophoblastic tumors, choriocarcinomas, and invasive moles. (medscape.com)
- Approximately 2 to 3% of hydatidiform moles develop into choriocarcinomas. (msdmanuals.com)
- The World Health Organization (WHO) prognostic scoring system is important in the medical management of patients with complete hydatidiform moles, partial hydatidiform moles, and choriocarcinomas. (medscape.com)
Gestational trophobla3
- Clinically, complete moles show a much higher incidence (18-29%) of developing into gestational trophoblastic neoplasia, whereas persistent trophoblastic neoplasia occurs only in 1.0-5.6% of partial mole cases ( 3 , 4 ). (iiarjournals.org)
- Therefore, the possibility of progressing to gestational trophoblastic neoplasia and the need for clinical processing and follow-up of the patient emphasizes the importance of differentiating between complete and partial hydatidiform moles. (iiarjournals.org)
- Conclusions A centralized hydatidiform mole surveillance program is feasible and effective and may improve the prognosis of patients with post-molar gestational trophoblastic neoplasia. (bmj.com)
Diploid2
- The complete hydatidiform mole is a diploid androgenetic conceptus with indiscriminate hyperplasia of the villous trophoblast and generalized swelling of the hydatidiform villous without detectable fetal tissues. (iiarjournals.org)
- Most hydatidiform moles are diploid or triploid, with a surplus of paternally inherited genes, however a number of other genetic variants have been observed. (au.dk)
Complete25
- Complete mole. (medscape.com)
- Patients with partial mole do not have the same clinical features as those with complete mole. (medscape.com)
- The following discussion is limited to hydatidiform moles (complete and partial). (medscape.com)
- A complete mole contains no fetal tissue. (medscape.com)
- These account for 85-90% of complete moles, with two identical paternal chromosome complements, derived from duplication of the paternal haploid chromosomes. (medscape.com)
- These account for 10-15% of complete moles. (medscape.com)
- The biparental complete mole is rare. (medscape.com)
- As in a complete mole, hyperplastic trophoblastic tissue and swelling of the chorionic villi occur. (medscape.com)
- DNA ploidy analysis is a useful tool to distinguish the partial hydatidiform moles (PMs) from complete hydatidiform moles (CMs) and nonmolar abortuses (NAs). (nih.gov)
- Genetic refinement and physical mapping of a biparental complete hydatidiform mole locus on chromosome 19q13.4. (bmj.com)
- Conclusion: The Ki-67 expression was higher in complete than in partial hydatidiform moles. (iiarjournals.org)
- Resulting from the earlier clinical evaluation and management of hydatidiform moles, the histopathological features which were regarded as diagnostic evidence of distinguishing complete moles from partial moles are more subtle and less readily identifiable ( 3 , 6 ). (iiarjournals.org)
- During routine clinical practice, misdiagnosis of complete and partial moles is not a new story ( 9 , 10 ). (iiarjournals.org)
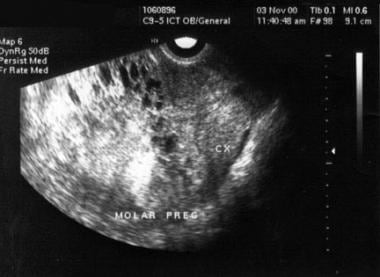
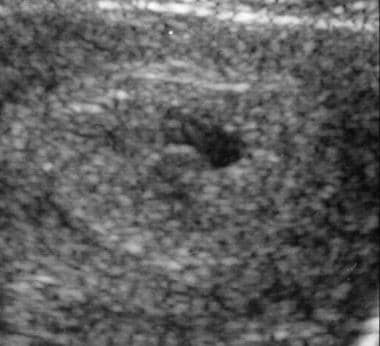
- Magnified transverse sonogram shows a complete hydatidiform mole (CHM) at 7 weeks of menstrual age with a small anembryonic gestational sac. (medscape.com)
- Sagittal endovaginal sonogram of a complete hydatidiform mole (CHM) at 12 weeks of menstrual age demonstrates an enlarged endometrium containing an anembryonic gestational sac with adjacent hyperechoic material containing tiny anechoic spaces. (medscape.com)
- Transverse endovaginal sonogram of a second-trimester complete hydatidiform mole (CHM) demonstrates a distended endometrial cavity containing innumerable, variably sized anechoic cysts with intervening hyperechoic material. (medscape.com)
- Transverse endovaginal sonogram of a second-trimester complete hydatidiform mole (CHM). (medscape.com)
- The major imaging feature distinguishing PHM from complete hydatidiform mole (CHM) is the presence of fetal tissue on the left side of the image (mother's right side). (medscape.com)
- Second-trimester complete hydatidiform mole (CHM) can be confused with retained products of conception. (medscape.com)
- Benign GTD includes molar pregnancies, both partial hydatidiform moles (PHMs) and complete hydatidiform moles (CHMs). (arupconsult.com)
- Complete hydatidiform moles (CHMs), or molar pregnancies, are more common in individuals younger than 21 years and older than 35 years. (arupconsult.com)
- Objective To assess the strategy and value of centralized surveillance of hydatidiform mole at a regional hospital in China and to investigate the necessity of prophylactic chemotherapy for high-risk complete hydatidiform mole. (bmj.com)
- Women with complete hydatidiform mole were categorized into low-risk and high-risk groups according to the criteria from Song Hongzhao's trophoblastic neoplasia. (bmj.com)
- Prophylactic chemotherapy is not recommended for women with high-risk complete hydatidiform mole with adequate surveillance. (bmj.com)
- 2002) Outcome of twin pregnancies with complete hydatidiform mole and healthy co-twin. (imperial.ac.uk)
Sonographic appearance1
- The sonographic appearance of a first-trimester hydatidiform mole can be indistinguishable from that of an anembryonic gestation, specifically blighted ovum. (medscape.com)
Familial2
- A recurrent form of biparental mole, which is familial and appears to be inherited as an autosomal recessive trait, has been described. (medscape.com)
- Mutation of the known DNMT genes does not underlie familial hydatidiform mole, at least in the family under study. (biomedcentral.com)
Diagnosis4
- Ultrasonography is the imaging investigation of choice (see the images below) to confirm the diagnosis of hydatidiform mole . (medscape.com)
- MRI has no established role in the initial diagnosis of hydatidiform moles. (medscape.com)
- CT presents a risk of ionizing radiation, and it has no role in the diagnosis of hydatidiform mole. (medscape.com)
- Hydatidiform Moles: Genetic Basis and Precision Diagnosis. (bvsalud.org)
Trophoblastic diseases1
- In the Danish Mole Project We are collecting samples from hydatidiform moles and other trophoblastic diseases. (au.dk)
Phenotype1
- The phenotype hydatidiform mole seems always to be caused by abnormalities involviong genes regulated by parental imprinting. (au.dk)
Cancerous2
- Is a hydatidiform mole cancerous? (studybuff.com)
- Noncancerous tumors that may become cancerous: These tumors include hydatidiform mole, exaggerated placental site, and placental site nodule. (msdmanuals.com)
Clinical3
- This mole can be classified into two subsidiary sets based on clinical, morphological and genetic characteristics ( 2 ). (iiarjournals.org)
- On the other hand, the recognition that the different subsidiary sets have different clinical management and prognosis has made the precise subdivision of hydatidiform moles essential. (iiarjournals.org)
- Clinical features of hydatidiform mole in patients 40 years or older may differ from those in younger patients. (medscape.com)
Uterus4
- Invasive hydatidiform mole is a type of neoplasia that grows into the muscular wall of the uterus. (wikipedia.org)
- Instead, a cluster of grape-like cysts (known as a hydatidiform mole) grows in the uterus. (studybuff.com)
- A hydatidiform mole is a growing mass of tissue inside your womb (uterus) that will not develop into a baby. (studybuff.com)
- Benign moles are treated surgically with evacuation of the uterus or hysterectomy. (annals.edu.sg)
Fetal tissue1
- With a partial mole, fetal tissue is often present. (medscape.com)
Ultrasonography1
- Of 155 cases of hydatidiform mole, only 53 (34%) were correctly diagnosed as hydatidiform mole with ultrasonography. (medscape.com)
Tissue2
- A hydatidiform mole is growth of an abnormal fertilized egg or an overgrowth of tissue from the placenta. (studybuff.com)
- On the other hand, if a mole comes back or it does not dissolve spontaneously, the doctor has to remove it with suction curettage , where all of the hydatidiform tissue is removed from the uterine cavity. (nethealthbook.com)
Cysts1
- A hydatidiform mole contains many cysts (sacs of fluid). (studybuff.com)
Clinically2
- No angiographic studies are clinically useful for assessing hydatidiform mole. (medscape.com)
- In a multicenter study, many proven cases of hydatidiform mole were not clinically or sonographically evident. (medscape.com)
Occur2
- Partial moles with a 69,XYY complement are rarely seen, and 69,YYY does not occur. (medscape.com)
- Hydatidiform moles occur at a rate of 1 per 1000 pregnancies in the US. (proprofs.com)
Genetic1
- Petignat P, Billieux M, Blouin J, Dahoun S, Vassilakos P. Is genetic analysis useful in the routine management of hydatidiform mole? (jabfm.org)
Trophoblasts1
- The hydatidiform mole encompasses a heterogeneous group of lesions that feature an abnormal non-neoplastic proliferation of trophoblasts ( 1 ). (iiarjournals.org)
Tissues1
- It is usually benign (not cancer) but it may spread to nearby tissues (invasive mole). (studybuff.com)
Uterine1
- These moles can grow deep into the uterine wall and cause bleeding or other complications. (medlineplus.gov)
Types1
- However, this is rather difficult and the two mole types are easily mistaken ( 5 ). (iiarjournals.org)
Methods1
- Methods Between February 2013 and February 2020, all women with hydatidiform mole in Dalian Women's and Children's Medical Center (Group) were registered for surveillance and treatment when indicated. (bmj.com)