Frontal Bone
Frontal Lobe
Frontal Sinus
Bone and Bones
Parietal Bone
Sex Reassignment Surgery
Ethmoid Bone
Hyperostosis Frontalis Interna
MSX1 Transcription Factor
Bone Remodeling
Craniosynostoses
Eosinophilic Granuloma
Bone Density
Neural Crest
The interfrontal bone and mutant genes in the mouse. (1/162)
The relationship between corrected skull width and the presence and size of an interfrontal bone is discussed with regard to the effect of certain mutant genes in the mouse known to affect the development of the neural tube. All genes reviewed which increase the incidence of the interfrontal bone and affect the neural tube also change the proportions of the adult skull. (+info)Frontal bone windows for transcranial color-coded duplex sonography. (2/162)
BACKGROUND AND PURPOSE: The use of the conventional temporal bone window for transcranial color-coded duplex sonography (TCCS) often results in difficulties in obtaining angle-corrected flow velocity measurements of the A2 segment of the anterior cerebral artery, the posterior communicating artery, and the midline venous vasculature because of the unfavorable insonation angle. The same applies to B-mode imaging of the frontal parenchyma. However, transorbital TCCS raises problems with the insonation of the orbital lens. To overcome these drawbacks, we studied the feasibility of frontal bone windows for TCCS examinations. METHODS: In 75 healthy volunteers (mean age, 45.3+/-17.0 years; age range, 17 to 77 years), the circle of Willis and the venous midline vasculature were insonated through a lateral and paramedian frontal bone window. Insonation quality of parenchymal structures (B-mode) was graded on a 3-point scale depending on the visibility of typical parenchymal landmarks. In a similar manner, the quality of the color-/Doppler-mode imaging of the arteries of the circle of Willis and the internal cerebral veins was assessed. In 15 patients (mean age, 62.7+/-13.7 years; age range, 33 to 83 years), the color-/Doppler-mode imaging quality of the intracranial vessels before and after application of an ultrasound contrast-enhancing agent was compared. RESULTS: B-mode insonation quality was optimal to fair in 73.3% of cases using the lateral and in 52.0% of cases using the paramedian frontal bone window, with defined parenchymal structures used as reference. Insonation quality decreased in those older than 60 years. In those younger than 60 years, angle-corrected flow velocity measurements of the A2 segment of the anterior cerebral artery and the internal cerebral vein were possible in 73.6% and 60.0%, respectively. Contrast enhancement resulted in a highly significant improvement in the imaging quality of the intracranial vessels. CONCLUSIONS: The transfrontal bone windows offer new possibilities for TCCS examinations, although the insonation quality is inferior to the conventional temporal bone window in terms of failure of an acoustic window. This can be compensated for by application of an ultrasound contrast-enhancing agent. (+info)Comparing frontal cranial profiles in archaic and modern homo by morphometric analysis. (3/162)
Archaic and modern human frontal bones are known to be quite distinct externally, by both conventional visual and metric evaluation. Internally this area of the skull has been considerably less well-studied. Here we present results from a comparison of interior, as well as exterior, frontal bone profiles from CT scans of five mid-Pleistocene and Neanderthal crania and 16 modern humans. Analysis was by a new morphometric method, Procrustes analysis of semi-landmarks, that permits the statistical comparison of curves between landmarks. As expected, we found substantial external differences between archaic and modern samples, differences that are mainly confined to the region around the brow ridge. However, in the inner median-sagittal profile, the shape remained remarkably stable over all 21 specimens. This implies that no significant alteration in this region has taken place over a period of a half-million years or more of evolution, even as considerable external change occurred within the hominid clade spanning several species. This confirms that the forms of the inner and outer aspects of the human frontal bone are determined by entirely independent factors, and further indicates unexpected stability in anterior brain morphology over the period during which modern human cognitive capacities emerged. Anat Rec (New Anat): 257:217-224, 1999. (+info)Fetal acalvaria with amniotic band syndrome. (4/162)
A case of amniotic band syndrome (ABS) presenting with acalvaria is reported. ABS includes a spectrum of non-genetic anomalies, varying from simple digital band constriction to major craniofacial and visceral defects, and even fetal death. Acalvaria is a rare congenital malformation characterised by the absence of the dome-like superior portion of the cranium comprising the frontal, parietal, and occipital bones and dura mater, in the presence of a normal skull base and facial bones with complete cranial contents. No two cases are the same. Acrania or absence of the flat skull bones with disorganised cerebral hemispheres have been reported in the presence of amniotic bands. ABS is an aetiological factor in acalvaria. Appropriate counselling for affected families needs to be given after prenatal diagnosis. (+info)Location of the glenoid fossa after a period of unilateral masticatory function in young rabbits. (5/162)
Changes in glenoid fossa position and skull morphology after a period of unilateral masticatory function were studied. The right-side maxillary and mandibular molars in twenty-seven 10-day-old rabbits were ground down under general anaesthesia. The procedure was repeated twice a week, until the rabbits were 50 days old. Fourteen rabbits were then killed and 13 left to grow to age 100 days. Nine 50-day-old and sixteen 100-day-old rabbits with unmodified occlusions served as controls. Three-dimensional measurements were made using a machine-vision technique and a video-imaging camera. The glenoid fossa position become more anterior in both groups of animals subjected to molar grinding as compared with controls (P < 0.01 in the 50-day-old group and P < 0.05 in 100-day-old group). In the 100-day-old group the right-side fossa was also in a more inferior position (P < 0.01). The glenoid fossa was more anteriorly located on the right than on the left side of individual animals in the group in which the right-side molars had been ground down (P < 0.001). (+info)Trigonocephaly in rabbits with familial interfrontal suture synostosis: the multiple effects of premature single-suture fusion. (6/162)
Previous studies from our laboratory have characterized the craniofacial morphology and growth patterns of an inbred strain of rabbits with autosomal dominant coronal suture synostosis. A number of rabbit perinates from this colony have been collected sporadically over a 5-year period with premature interfrontal suture synostosis. The present study describes the very early onset of craniofacial dysmorphology of these rabbits and compares them to similar-aged normal control rabbits. A total of 40 perinatal New Zealand White rabbits were used in the present study. Twenty-one comprised the sample with interfrontal suture synostosis and ranged in age from 27 to 38 days postconception (term = 31 days) with a mean age of 33.53 days (+/-2.84 days). Nineteen rabbits served as age-matched, normal controls (mean age = 33.05 days +/-2.79 days). Lateral and dorsoventral radiographs were collected from each rabbit. The radiographs were traced, computer digitized, and 12 craniofacial measurements, angles, and indices were obtained. Mean measures were compared using an unpaired Student's t-test. All synostosed rabbits were stillborn or died shortly after birth. Grossly, these rabbits exhibited extreme frontal bossing, trigonocephaly with sagittal keeling, and midfacial shortening. No somatic anomalies were noted. Radiographically, rabbits with interfrontal suture synostosis had significantly (P < 0.05) narrower bifrontal widths, shorter cranial vault lengths, kyphotic cranial base angles, and different cranial vault indices (shapes) compared to controls. Results reveal severe and early pathological and compensatory cranial vault changes associated with premature interfrontal suture synostosis in this rabbit model. The 100% mortality rate noted in this condition may be related to the inheritance of a lethal genetic mutation or to neural compression from reduced intracranial volume. Results are discussed in light of current pathogenic hypotheses for human infants with premature metopic suture synostosis. (+info)Bilateral fronto-orbito-zygomatic craniotomy--a combined extended frontal and orbitozygomatic approach. (7/162)
In extensive skull base lesions involving the spheno-ethmoido-clival region and extending into both the cavernous sinuses and infratemporal regions, a combination of approaches is usually required, either in the same operation or at a second stage. The bilateral fronto-orbito-zygomatic craniotomy described in this report is a combination of an extended frontal approach and fronto-orbito-zygomatic craniotomy. This gives a wide exposure of the spheno-ethmoido-clival regions of both the cavernous sinuses and both the infratemporal regions. The exposure is thus greatly improved with minimal frontal lobe retraction. The single bone piece can be speedily replaced obviating the need for a complicated reconstruction technique and gives a superior cosmetic result. The operative technique is described in detail. (+info)Bone defect associated with middle meningeal arteriovenous fistula treated by embolization--case report. (8/162)
A 57-year-old male presented with a frontal bone defect associated with a middle meningeal arteriovenous fistula (AVF) manifesting as headache. The patient had a history of head injury 19 years previously. Skull radiography and computed tomography demonstrated a left frontal bone defect. Left external carotid angiography demonstrated a middle meningeal AVF at the frontal region, at the same location as the bone defect. The AVF was fed by the bilateral middle meningeal and left deep temporal arteries, and drained by the superior sagittal and ipsilateral cavernous sinuses. The minor feeding artery, the left deep temporal artery, was embolized with polyvinyl alcohol particles, then 0.4 ml of a 1:3 mixture of n-butyl cyanoacrylate and lipiodol was injected from the left middle meningeal artery. Follow-up angiography 3 months after the embolization revealed complete obliteration of the fistula. The bone defect may have been caused by erosion of the frontal bone by the pulsating effect of the feeding and draining vessels of the fistula, or by inadequate nutrition to the bone tissue because of the arteriovenous shunt. (+info)The frontal bone is the bone that forms the forehead and the upper part of the eye sockets (orbits) in the skull. It is a single, flat bone that has a prominent ridge in the middle called the superior sagittal sinus, which contains venous blood. The frontal bone articulates with several other bones, including the parietal bones at the sides and back, the nasal bones in the center of the face, and the zygomatic (cheek) bones at the lower sides of the orbits.
Cranial sutures are the fibrous joints that connect and hold together the bones of the skull (cranium) in humans and other animals. These sutures provide flexibility for the skull during childbirth and growth, allowing the skull to expand as the brain grows in size, especially during infancy and early childhood.
There are several cranial sutures in the human skull, including:
1. The sagittal suture, which runs along the midline of the skull, connecting the two parietal bones.
2. The coronal suture, which connects the frontal bone to the two parietal bones.
3. The lambdoid suture, which connects the occipital bone to the two parietal bones.
4. The squamosal suture, which connects the temporal bone to the parietal bone.
5. The frontosphenoidal and sphenoethmoidal sutures, which connect the frontal bone, sphenoid bone, and ethmoid bone in the anterior cranial fossa.
These sutures are typically made up of a specialized type of connective tissue called Sharpey's fibers, which interdigitate with each other to form a strong yet flexible joint. Over time, as the skull bones fully fuse together, these sutures become less prominent and eventually ossify (turn into bone). In some cases, abnormalities in cranial suture development or fusion can lead to medical conditions such as craniosynostosis.
Skull neoplasms refer to abnormal growths or tumors that develop within the skull. These growths can be benign (non-cancerous) or malignant (cancerous). They can originate from various types of cells, such as bone cells, nerve cells, or soft tissues. Skull neoplasms can cause various symptoms depending on their size and location, including headaches, seizures, vision problems, hearing loss, and neurological deficits. Treatment options include surgery, radiation therapy, and chemotherapy. It is important to note that a neoplasm in the skull can also refer to metastatic cancer, which has spread from another part of the body to the skull.
The frontal lobe is the largest lobes of the human brain, located at the front part of each cerebral hemisphere and situated in front of the parietal and temporal lobes. It plays a crucial role in higher cognitive functions such as decision making, problem solving, planning, parts of social behavior, emotional expressions, physical reactions, and motor function. The frontal lobe is also responsible for what's known as "executive functions," which include the ability to focus attention, understand rules, switch focus, plan actions, and inhibit inappropriate behaviors. It is divided into five areas, each with its own specific functions: the primary motor cortex, premotor cortex, Broca's area, prefrontal cortex, and orbitofrontal cortex. Damage to the frontal lobe can result in a wide range of impairments, depending on the location and extent of the injury.
A frontal sinus is a paired, air-filled paranasal sinus located in the frontal bone of the skull, above the eyes and behind the forehead. It is one of the four pairs of sinuses found in the human head. The frontal sinuses are lined with mucous membrane and are interconnected with the nasal cavity through small openings called ostia. They help to warm, humidify, and filter the air we breathe, and contribute to the resonance of our voice. Variations in size, shape, and asymmetry of frontal sinuses are common among individuals.
"Bone" is the hard, dense connective tissue that makes up the skeleton of vertebrate animals. It provides support and protection for the body's internal organs, and serves as a attachment site for muscles, tendons, and ligaments. Bone is composed of cells called osteoblasts and osteoclasts, which are responsible for bone formation and resorption, respectively, and an extracellular matrix made up of collagen fibers and mineral crystals.
Bones can be classified into two main types: compact bone and spongy bone. Compact bone is dense and hard, and makes up the outer layer of all bones and the shafts of long bones. Spongy bone is less dense and contains large spaces, and makes up the ends of long bones and the interior of flat and irregular bones.
The human body has 206 bones in total. They can be further classified into five categories based on their shape: long bones, short bones, flat bones, irregular bones, and sesamoid bones.
The parietal bone is one of the four flat bones that form the skull's cranial vault, which protects the brain. There are two parietal bones in the skull, one on each side, located posterior to the frontal bone and temporal bone, and anterior to the occipital bone. Each parietal bone has a squamous part, which forms the roof and sides of the skull, and a smaller, wing-like portion called the mastoid process. The parietal bones contribute to the formation of the coronal and lambdoid sutures, which are fibrous joints that connect the bones in the skull.
The skull is the bony structure that encloses and protects the brain, the eyes, and the ears. It is composed of two main parts: the cranium, which contains the brain, and the facial bones. The cranium is made up of several fused flat bones, while the facial bones include the upper jaw (maxilla), lower jaw (mandible), cheekbones, nose bones, and eye sockets (orbits).
The skull also provides attachment points for various muscles that control chewing, moving the head, and facial expressions. Additionally, it contains openings for blood vessels, nerves, and the spinal cord to pass through. The skull's primary function is to protect the delicate and vital structures within it from injury and trauma.
Maxillary fractures, also known as Le Fort fractures, are complex fractures that involve the upper jaw or maxilla. Named after the French surgeon René Le Fort who first described them in 1901, these fractures are categorized into three types (Le Fort I, II, III) based on the pattern and level of bone involvement.
1. Le Fort I fracture: This type of maxillary fracture involves a horizontal separation through the lower part of the maxilla, just above the teeth's roots. It often results from direct blows to the lower face or chin.
2. Le Fort II fracture: A Le Fort II fracture is characterized by a pyramidal-shaped fracture pattern that extends from the nasal bridge through the inferior orbital rim and maxilla, ending at the pterygoid plates. This type of fracture usually results from forceful impacts to the midface or nose.
3. Le Fort III fracture: A Le Fort III fracture is a severe craniofacial injury that involves both the upper and lower parts of the face. It is also known as a "craniofacial dysjunction" because it separates the facial bones from the skull base. The fracture line extends through the nasal bridge, orbital rims, zygomatic arches, and maxilla, ending at the pterygoid plates. Le Fort III fractures typically result from high-impact trauma to the face, such as car accidents or assaults.
These fractures often require surgical intervention for proper alignment and stabilization of the facial bones.
Sex reassignment surgery (SRS), also known as gender confirmation surgery, is a surgical procedure (or series of procedures) that an individual may undergo as part of the process to change their physical sex to match their gender identity. It involves the alteration and reconstruction of the genitalia and secondary sex characteristics to resemble those of the desired sex.
For individuals transitioning from male to female, SRS typically includes orchiectomy (removal of the testicles), penectomy (removal of the penis), and vaginoplasty (creation of a vagina). For individuals transitioning from female to male, SRS may involve hysterectomy (removal of the uterus and ovaries), salpingo-oophorectomy (removal of the fallopian tubes and ovaries), vaginectomy (removal of the vagina), metoidioplasty or phalloplasty (creation of a penis), and scrotoplasty (creation of a scrotum).
It is important to note that SRS is just one aspect of gender affirming care, which may also include hormone therapy, mental health support, and social transition. The decision to undergo SRS is highly personal and depends on various factors, including the individual's physical and mental health, personal goals, and financial resources.
The ethmoid bone is a paired, thin, and lightweight bone that forms part of the skull's anterior cranial fossa and contributes to the formation of the orbit and nasal cavity. It is located between the frontal bone above and the maxilla and palatine bones below. The ethmoid bone has several important features:
1. Cribriform plate: This is the horizontal, sieve-like portion that forms part of the anterior cranial fossa and serves as the roof of the nasal cavity. It contains small openings (foramina) through which olfactory nerves pass.
2. Perpendicular plate: The perpendicular plate is a vertical structure that projects downward from the cribriform plate, forming part of the nasal septum and separating the left and right nasal cavities.
3. Superior and middle nasal conchae: These are curved bony projections within the lateral walls of the nasal cavity that help to warm, humidify, and filter incoming air.
4. Lacrimal bone: The ethmoid bone articulates with the lacrimal bone, forming part of the medial wall of the orbit.
5. Frontal process: This is a thin, vertical plate that articulates with the frontal bone above the orbit.
6. Sphenoidal process: The sphenoidal process connects the ethmoid bone to the sphenoid bone posteriorly.
The ethmoid bone plays a crucial role in protecting the brain and providing structural support for the eyes, as well as facilitating respiration by warming, humidifying, and filtering incoming air.
Hyperostosis Frontalis Interna (HFI) is a medical condition characterized by an abnormal thickening or overgrowth of the inner table of the frontal bone, which is the bone that forms the forehead. This condition most commonly affects middle-aged to older women. The exact cause of HFI is not known, but it may be associated with hormonal factors, as it is more common in women who have gone through menopause.
In HFI, the overgrowth of bone can cause a raised, bumpy, or irregular appearance on the forehead, and can sometimes lead to headaches or other symptoms. However, many people with HFI do not experience any symptoms at all. The diagnosis of HFI is typically made based on imaging studies such as X-rays or CT scans, which show the characteristic thickening of the frontal bone.
While HFI is not a life-threatening condition, it can cause cosmetic concerns and may require treatment in some cases. Treatment options for HFI include medication to manage symptoms such as headaches, as well as surgical removal of the excess bone in severe cases.
MSX1 (Homeobox protein MSX-1) is a transcription factor that belongs to the muscle segment homebox gene family, also known as the msh homeobox genes. These genes are involved in the development and differentiation of various tissues, including muscle, bone, and neural crest derivatives.
MSX1 plays crucial roles during embryonic development, such as regulating cell proliferation, differentiation, and apoptosis. It is widely expressed in the developing embryo, particularly in the oral ectoderm, neural crest, and mesenchyme. In the oral region, MSX1 helps control tooth development by interacting with other transcription factors and signaling molecules.
As a transcription factor, MSX1 binds to specific DNA sequences called homeobox response elements (HREs) in the promoter regions of its target genes. This binding either activates or represses gene expression, depending on the context and interacting partners. Dysregulation of MSX1 has been implicated in various developmental disorders and diseases, such as tooth agenesis, cleft lip/palate, and cancer.
Bone remodeling is the normal and continuous process by which bone tissue is removed from the skeleton (a process called resorption) and new bone tissue is formed (a process called formation). This ongoing cycle allows bones to repair microdamage, adjust their size and shape in response to mechanical stress, and maintain mineral homeostasis. The cells responsible for bone resorption are osteoclasts, while the cells responsible for bone formation are osteoblasts. These two cell types work together to maintain the structural integrity and health of bones throughout an individual's life.
During bone remodeling, the process can be divided into several stages:
1. Activation: The initiation of bone remodeling is triggered by various factors such as microdamage, hormonal changes, or mechanical stress. This leads to the recruitment and activation of osteoclast precursor cells.
2. Resorption: Osteoclasts attach to the bone surface and create a sealed compartment called a resorption lacuna. They then secrete acid and enzymes that dissolve and digest the mineralized matrix, creating pits or cavities on the bone surface. This process helps remove old or damaged bone tissue and releases calcium and phosphate ions into the bloodstream.
3. Reversal: After resorption is complete, the osteoclasts undergo apoptosis (programmed cell death), and mononuclear cells called reversal cells appear on the resorbed surface. These cells prepare the bone surface for the next stage by cleaning up debris and releasing signals that attract osteoblast precursors.
4. Formation: Osteoblasts, derived from mesenchymal stem cells, migrate to the resorbed surface and begin producing a new organic matrix called osteoid. As the osteoid mineralizes, it forms a hard, calcified structure that gradually replaces the resorbed bone tissue. The osteoblasts may become embedded within this newly formed bone as they differentiate into osteocytes, which are mature bone cells responsible for maintaining bone homeostasis and responding to mechanical stress.
5. Mineralization: Over time, the newly formed bone continues to mineralize, becoming stronger and more dense. This process helps maintain the structural integrity of the skeleton and ensures adequate calcium storage.
Throughout this continuous cycle of bone remodeling, hormones, growth factors, and mechanical stress play crucial roles in regulating the balance between resorption and formation. Disruptions to this delicate equilibrium can lead to various bone diseases, such as osteoporosis, where excessive resorption results in weakened bones and increased fracture risk.
Craniosynostosis is a medical condition that affects the skull of a developing fetus or infant. It is characterized by the premature closure of one or more of the fibrous sutures between the bones of the skull (cranial sutures). These sutures typically remain open during infancy to allow for the growth and development of the brain.
When a suture closes too early, it can restrict the growth of the surrounding bones and cause an abnormal shape of the head. The severity of craniosynostosis can vary depending on the number of sutures involved and the extent of the premature closure. In some cases, craniosynostosis can also lead to increased pressure on the brain, which can cause a range of neurological symptoms.
There are several types of craniosynostoses, including:
1. Sagittal synostosis: This is the most common type and involves the premature closure of the sagittal suture, which runs from front to back along the top of the head. This can cause the skull to grow long and narrow, a condition known as scaphocephaly.
2. Coronal synostosis: This type involves the premature closure of one or both of the coronal sutures, which run from the temples to the front of the head. When one suture is affected, it can cause the forehead to bulge and the eye socket on that side to sink in (anterior plagiocephaly). When both sutures are affected, it can cause a flattened appearance of the forehead and a prominent back of the head (brachycephaly).
3. Metopic synostosis: This type involves the premature closure of the metopic suture, which runs from the top of the forehead to the bridge of the nose. It can cause a triangular shape of the forehead and a prominent ridge along the midline of the skull (trigonocephaly).
4. Lambdoid synostosis: This is the least common type and involves the premature closure of the lambdoid suture, which runs along the back of the head. It can cause an asymmetrical appearance of the head and face, as well as possible neurological symptoms.
In some cases, multiple sutures may be affected, leading to more complex craniofacial abnormalities. Treatment for craniosynostosis typically involves surgery to release the fused suture(s) and reshape the skull. The timing of the surgery depends on the type and severity of the condition but is usually performed within the first year of life. Early intervention can help prevent further complications, such as increased intracranial pressure and developmental delays.
Eosinophilic granuloma is a term used in pathology to describe a specific type of inflammatory lesion that is characterized by the accumulation of eosinophils, a type of white blood cell, and the formation of granulomas. A granuloma is a small nodular structure formed by the accumulation of immune cells, typically including macrophages, lymphocytes, and other inflammatory cells.
Eosinophilic granulomas can occur in various organs of the body, but they are most commonly found in the lungs, skin, and bones. In the lungs, eosinophilic granulomas are often associated with hypersensitivity reactions to inhaled antigens, such as dust mites or fungal spores. They can also be seen in association with certain diseases, such as Langerhans cell histiocytosis, an uncommon disorder characterized by the abnormal proliferation of a type of immune cell called Langerhans cells.
The symptoms of eosinophilic granuloma depend on the location and extent of the lesion. In the lungs, eosinophilic granulomas may cause cough, chest pain, or shortness of breath. In the skin, they may present as nodules, plaques, or ulcers. In the bones, they can cause pain, swelling, and fractures.
The diagnosis of eosinophilic granuloma is typically made based on a combination of clinical, radiological, and pathological findings. Treatment may include avoidance of known antigens, corticosteroids, or other immunosuppressive medications, depending on the severity and location of the lesion.
Osteogenesis is the process of bone formation or development. It involves the differentiation and maturation of osteoblasts, which are bone-forming cells that synthesize and deposit the organic matrix of bone tissue, composed mainly of type I collagen. This organic matrix later mineralizes to form the inorganic crystalline component of bone, primarily hydroxyapatite.
There are two primary types of osteogenesis: intramembranous and endochondral. Intramembranous osteogenesis occurs directly within connective tissue, where mesenchymal stem cells differentiate into osteoblasts and form bone tissue without an intervening cartilage template. This process is responsible for the formation of flat bones like the skull and clavicles.
Endochondral osteogenesis, on the other hand, involves the initial development of a cartilaginous model or template, which is later replaced by bone tissue. This process forms long bones, such as those in the limbs, and occurs through several stages involving chondrocyte proliferation, hypertrophy, and calcification, followed by invasion of blood vessels and osteoblasts to replace the cartilage with bone tissue.
Abnormalities in osteogenesis can lead to various skeletal disorders and diseases, such as osteogenesis imperfecta (brittle bone disease), achondroplasia (a form of dwarfism), and cleidocranial dysplasia (a disorder affecting skull and collarbone development).
Bone density refers to the amount of bone mineral content (usually measured in grams) in a given volume of bone (usually measured in cubic centimeters). It is often used as an indicator of bone strength and fracture risk. Bone density is typically measured using dual-energy X-ray absorptiometry (DXA) scans, which provide a T-score that compares the patient's bone density to that of a young adult reference population. A T-score of -1 or above is considered normal, while a T-score between -1 and -2.5 indicates osteopenia (low bone mass), and a T-score below -2.5 indicates osteoporosis (porous bones). Regular exercise, adequate calcium and vitamin D intake, and medication (if necessary) can help maintain or improve bone density and prevent fractures.
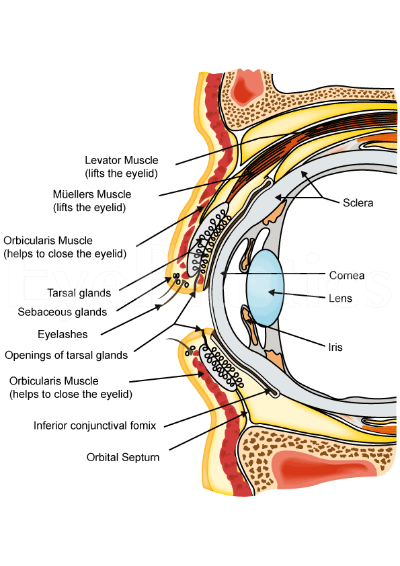
In medical terms, the orbit refers to the bony cavity or socket in the skull that contains and protects the eye (eyeball) and its associated structures, including muscles, nerves, blood vessels, fat, and the lacrimal gland. The orbit is made up of several bones: the frontal bone, sphenoid bone, zygomatic bone, maxilla bone, and palatine bone. These bones form a pyramid-like shape that provides protection for the eye while also allowing for a range of movements.
The neural crest is a transient, multipotent embryonic cell population that originates from the ectoderm (outermost layer) of the developing neural tube (precursor to the central nervous system). These cells undergo an epithelial-to-mesenchymal transition and migrate throughout the embryo, giving rise to a diverse array of cell types and structures.
Neural crest cells differentiate into various tissues, including:
1. Peripheral nervous system (PNS) components: sensory neurons, sympathetic and parasympathetic ganglia, and glial cells (e.g., Schwann cells).
2. Facial bones and cartilage, as well as connective tissue of the skull.
3. Melanocytes, which are pigment-producing cells in the skin.
4. Smooth muscle cells in major blood vessels, heart, gastrointestinal tract, and other organs.
5. Secretory cells in endocrine glands (e.g., chromaffin cells of the adrenal medulla).
6. Parts of the eye, such as the cornea and iris stroma.
7. Dental tissues, including dentin, cementum, and dental pulp.
Due to their wide-ranging contributions to various tissues and organs, neural crest cells play a crucial role in embryonic development and organogenesis. Abnormalities in neural crest cell migration or differentiation can lead to several congenital disorders, such as neurocristopathies.
Bone resorption is the process by which bone tissue is broken down and absorbed into the body. It is a normal part of bone remodeling, in which old or damaged bone tissue is removed and new tissue is formed. However, excessive bone resorption can lead to conditions such as osteoporosis, in which bones become weak and fragile due to a loss of density. This process is carried out by cells called osteoclasts, which break down the bone tissue and release minerals such as calcium into the bloodstream.
 Frontal bone - Wikipedia
Frontal bone - Wikipedia Frontal Bone Fracture Management in the ED: Practice Essentials, Pathophysiology, Epidemiology
Frontal Bone Fracture Management in the ED: Practice Essentials, Pathophysiology, Epidemiology Frontal bone
Frontal bone Frontal bone Archives - Open Source Cranio
Frontal bone Archives - Open Source Cranio Radiology case: Fissure of frontal bone
Radiology case: Fissure of frontal bone Acervo Digital: Reconstruction of the anterior wall of the frontal sinus using bovine bone matrix: histological study with...
Acervo Digital: Reconstruction of the anterior wall of the frontal sinus using bovine bone matrix: histological study with... October 2019 - Volume 30 - Issue 7 : Journal of Craniofacial Surgery
October 2019 - Volume 30 - Issue 7 : Journal of Craniofacial Surgery New Arrival - 300% Density Bone Straight lace Frontal Wig 350 Gram
- naijabeautyhair
New Arrival - 300% Density Bone Straight lace Frontal Wig 350 Gram
- naijabeautyhair Surgical management of osteoma in the frontal bone: a case report
Surgical management of osteoma in the frontal bone: a case report Cranberry 613 Blonde 13x4 Transparent Lace Frontal Wig Bone Straight H
- Cranberry Hair
Cranberry 613 Blonde 13x4 Transparent Lace Frontal Wig Bone Straight H
- Cranberry Hair Blue Wig 13x4 HD Lace Frontal Wig Bone Straight Human Hair Colored Wig
- Hairsmarket
Blue Wig 13x4 HD Lace Frontal Wig Bone Straight Human Hair Colored Wig
- Hairsmarket 2020-2021 BCSC Basic and Clinical Science Course™
2020-2021 BCSC Basic and Clinical Science Course™ Cranial sutures: MedlinePlus Medical Encyclopedia
Cranial sutures: MedlinePlus Medical Encyclopedia Cranial Bones: Function and Anatomy, Diagram, Conditions, Health Tips
Cranial Bones: Function and Anatomy, Diagram, Conditions, Health Tips "Intraosseous Hemangioma of the Frontal Bone. Report of a Case and Revi" by Joshua S. Brandner, Yeshwant B. Rawal et al.
"Intraosseous Hemangioma of the Frontal Bone. Report of a Case and Revi" by Joshua S. Brandner, Yeshwant B. Rawal et al. Angelbella Glory Virgin Hair 13X4 Bone Straight 613 Raw Human Hair HD Lace Frontal Extensions Wigs from China manufacturer -...
Angelbella Glory Virgin Hair 13X4 Bone Straight 613 Raw Human Hair HD Lace Frontal Extensions Wigs from China manufacturer -... Search Results
Search Results What is the definition of Frontal? | Dictionary.net
What is the definition of Frontal? | Dictionary.net Hamamelis Virginica - ABC Homeopathy
Hamamelis Virginica - ABC Homeopathy Anatomy, Head and Neck, Nasal Cavity - StatPearls - NCBI Bookshelf
Anatomy, Head and Neck, Nasal Cavity - StatPearls - NCBI Bookshelf Metopic craniosynostosis: Types, treatment, and more
Metopic craniosynostosis: Types, treatment, and more PDF) A new species of Cyrtodactylus (Squamata: Gekkonidae) and the first record of C. otai from Son La Province, Vietnam
PDF) A new species of Cyrtodactylus (Squamata: Gekkonidae) and the first record of C. otai from Son La Province, Vietnam Veterinary Screw Targeting Clamp (STC)
Veterinary Screw Targeting Clamp (STC)