Endolymphatic Duct
Endolymphatic Sac
Meniere Disease
Endolymphatic Hydrops
Ear Neoplasms
Vestibular Aqueduct
Ear, Inner
Hearing Loss, Sensorineural
von Hippel-Lindau Disease
3D MRI of the membranous labyrinth. An age related comparison of MR findings in patients with labyrinthine fibrosis and in persons without inner ear symptoms. (1/29)
PURPOSE: We compared MRI of the membranous labyrinth in patients with chronic non-neoplastic inner ear disease and MR signs of labyrinthine fibrosis and controls depending on their age, in order to establish whether there were any MR differences regarding patient age groups, control age groups and between the patients and controls themselves. MATERIALS AND METHODS: Clinical ENT examinations as well as a T2* weighted 3D CISS (Constructive Interference in Steady State) sequence with a slice thickness of 0.7 mm were performed. Our collective was subdivided as follows: 0-19 years (10 controls, 3 patients with chronic non-neoplastic inner ear disease), 20-49 years (55 controls, 8 patients), 50 years and older (40 controls, 22 patients). Detectability of labyrinthine structures (e.g. cochlea, vestibule, semicircular canals) and filling defects were evaluated. RESULTS: In the 3 age-groups of the control collective no significant differences were observed in the membranous labyrinth. However differences concerning labyrinthine detectability emerged between controls and patients in both the 20-49 years and 50 years and older age groups. In the patient collective the 3 age groups showed no significant discrepancy in the mean number of lesions. CONCLUSION: Filling defects of the membranous labyrinth on 3D CISS MR images are pathological even in older persons. We would therefore recommend high resolution T2* weighted MRI in the case of suspected labyrinthine fibrosis. (+info)MR evaluation of vestibulocochlear anomalies associated with large endolymphatic duct and sac. (2/29)
BACKGROUND AND PURPOSE: Large endolymphatic duct and sac (LEDS) is one of the most common anomalies seen in patients with congenital sensorineural hearing loss (SNHL), and is known to occur with other inner ear findings. Our purpose was to use high-resolution T2-weighted fast spin-echo (FSE) MR imaging to describe the features and prevalence of specific anomalies that occur in association with LEDS. METHODS: We retrospectively reviewed MR images of the inner ear obtained in 63 patients with LEDS and in 60 control subjects. We evaluated each image for features of cochlear and vestibular dysplasia, including deficiency of the cochlear modiolus, gross cochlear dysmorphism, asymmetry of the cochlear scalar chambers, enlargement of the membranous vestibule, gross vestibular dysmorphism, and abnormality of the semicircular canals (SCC). RESULTS: Cochlear anomalies were present in 76% of ears with LEDS. Modiolar deficiency, gross dysmorphism, and scalar asymmetry were seen in 94%, 71%, and 65% of abnormal cochleas, respectively. Vestibular abnormalities were present in 40% of ears with LEDS. Simple enlargement, gross dysmorphism, and distortion of the lateral SCC were seen in 84%, 16%, and 32% of abnormal vestibules, respectively. CONCLUSION: Coexistent cochlear anomalies, vestibular anomalies, or both are present in most ears with LEDS, and appear as a spectrum of lesions, ranging from subtle dymorphism to overt dysplasia. The presence of coexistent anomalies in LEDS affects treatment decisions and prognosis. Newer techniques of high-resolution FSE MR imaging provide a means of exquisite characterization of LEDS, as well as more sensitive detection of associated vestibulocochlear anomalies. (+info)MR imaging of the enlarged endolymphatic duct and sac syndrome by use of a 3D fast asymmetric spin-echo sequence: volume and signal-intensity measurement of the endolymphatic duct and sac and area measurement of the cochlear modiolus. (3/29)
BACKGROUND AND PURPOSE: In enlarged endolymphatic duct (EED) and sac (EES) syndrome, deformity of the EED and EES is congenital; however, hearing loss is acquired. To investigate the pathophysiology of progressive sensorineural hearing loss in EED and EES syndrome, we measured the volume of the EED and EES, the diameter of the EED and EES, the area of the cochlear modiolus, and the signal intensity of the EES and compared our findings against degree of hearing loss. METHODS: Thin-section MR images of 33 ears in 17 patients with EED and EES syndrome were studied. All studies were obtained on a 1.5-T MR unit using a quadrature surface phased-array coil. Heavily T2-weighted 3D fast asymmetric spin-echo images were obtained with a voxel size of 0.3 x 0.3 x 0.8 mm without zero-fill interpolation. Two radiologists traced the areas of the EED and EES manually, and the volume was calculated. The area of the cochlear modiolus, diameter of the EED and EES, and signal intensity of the EES were also measured by drawing regions of interest manually. The signal intensity ratio of EES/CSF was calculated. These measured values were compared against audiographic data, and the degree of linear correlation was determined. RESULTS: The volume of the EED and EES, the area of the modiolus, the diameter of the EED and EES, and the signal intensity of the EES did not show significant correlation with degree of hearing loss. CONCLUSION: These findings suggest that there is a microscopic area of damage or fragility in the inner ear not visible even with thin-section heavily T2-weighted MR imaging. (+info)Phenotypes associated with replacement of His by Arg in the Pendred syndrome gene. (4/29)
BACKGROUND: Pendred syndrome is often associated with inner ear malformations, especially enlarged vestibular aqueduct (EVA). Recently, mutations in the Pendred syndrome gene (PDS) have been reported in patients with EVA, in addition to those with classical Pendred syndrome. OBJECTIVE: The aim of this study was to investigate the genotype-phenotype correlations of PDS. METHODS: Each of the 21 exons and flanking splice regions of PDS was analysed by direct DNA sequencing in nine patients with EVA; allele-specific amplification was performed to confirm the mutation. Genetic analyses were compared with thyroid function tests, perchlorate discharge tests, thyroid volume and pure-tone audiogram. Magnetic resonance imaging was used to determine the volume of the endolymphatic duct and sac of each patient. RESULTS: A missense mutation, H723R, was identified in the homozygous state in three patients and in the heterozygous state in another three. Although none of the patients had goitre, increased serum thyroglobulin and an abnormal degree of iodide release were correlated with the number of mutant alleles identified. However, there was no relationship between the degree of hearing loss and the number of mutant alleles. CONCLUSION: The present study reveals that the number of mutant alleles correlates with the degree of subclinical thyroid abnormality, but not with the degree of hearing loss in Japanese patients with the PDS missense mutation H723R. (+info)Network organization of interstitial connective tissue cells in the human endolymphatic duct. (5/29)
The human endolymphatic duct (ED) and sac of the inner ear have been suggested to control endolymph volume and pressure. However, the physiological mechanisms for these processes remain obscure. We investigated the organization of the periductal interstitial connective tissue cells and extracellular matrix (ECM) in four freshly fixed human EDs by transmission electron microscopy and by immunohistochemistry. The unique surgical material allowed a greatly improved structural and epitopic preservation of tissue. Periductal connective tissue cells formed frequent intercellular contacts and focally occurring electron-dense contacts to ECM structures, creating a complex tissue network. The connective tissue cells also formed contacts with the basal lamina of the ED epithelium and the bone matrix, connecting the ED with the surrounding bone of the vestibular aqueduct. The interstitial connective tissue cells were non-endothelial and non-smooth muscle fibroblastoid cells. We suggest that the ED tissue network forms a functional mechanical entity that takes part in the control of inner ear fluid pressure and endolymph resorption. (+info)DAN directs endolymphatic sac and duct outgrowth in the avian inner ear. (6/29)
Bone morphogenetic proteins (BMPs) are expressed in the developing vertebrate inner ear and participate in inner ear axial patterning and the development of its sensory epithelium. BMP antagonists, such as noggin, chordin, gremlin, cerberus, and DAN (differential screening-selected gene aberrative in neuroblastoma) inhibit BMP activity and establish morphogenetic gradients during the patterning of many developing tissues and organs. In this study, the role of the BMP antagonist DAN in inner ear development was investigated. DAN-expressing cell pellets were implanted into the otocyst and the periotic mesenchyme to determine the effects of exogenous DAN on otic development. Similar to the effects on the inner ear seen after exposure of otocysts to the BMP4 antagonist noggin, semicircular canals were truncated or eliminated based upon the site of pellet implantation. Unique to the DAN implantations, however, were effects on the developing endolymphatic duct and sac. In DAN-treated inner ears, endolymphatic ducts and sacs were merged with the crus or grew into the superior semicircular canal. Both the canal and endolymphatic duct and sac effects were rescued by joint implantation of BMP4-expressing cells. Electroporation of DAN antisense morpholinos into the epithelium of stage 15-17 otocysts, blocking DAN protein synthesis, resulted in enlarged endolymphatic ducts and sacs as well as smaller semicircular canals in some cases. Taken together, these data suggest a role for DAN both in helping to regulate BMP activity spatially and temporally and in patterning and partitioning of the medial otic tissue between the endolymphatic duct/sac and medially derived inner ear structures. (+info)3-T imaging of the cochlear nerve and labyrinth in cochlear-implant candidates: 3D fast recovery fast spin-echo versus 3D constructive interference in the steady state techniques. (7/29)
BACKGROUND AND PURPOSE: High-resolution imaging of the internal auditory canal and labyrinth at 1.5 T is often performed by using three-dimensional (3D) fast spin-echo or T2* techniques. We evaluated both techniques at 3 T in the preoperative assessment of patients being considered for cochlear implants. METHODS: Sagittal 3D fast recovery fast spin-echo (FRFSE) and 3D constructive interference in the steady state (CISS) images were acquired in eight patients at 3.0 T by using dual surface coils. Contrast-to-noise ratios (CNRs) for the intracanalicular nerve and CSF were measured in the internal auditory canal. Two neuroradiologists reviewed the images to determine whether the techniques provided images of diagnostic quality. RESULTS: CNRs for 3D CISS were twice those obtained with 3D FRFSE. Both techniques provided images of diagnostic quality, though spurious signal intensity loss at the apex of the superior semicircular canals was encountered on 3D FRFSE images in four of eight patients. CONCLUSION: Both 3D FRFSE and 3D CISS provide high-resolution images of the internal auditory canal and labyrinth at 3.0 T. We predict that the superior CNRs obtained with 3D CISS will prove advantageous as we move to smaller fields of view at higher field strength. (+info)The role of Pax2 in mouse inner ear development. (8/29)
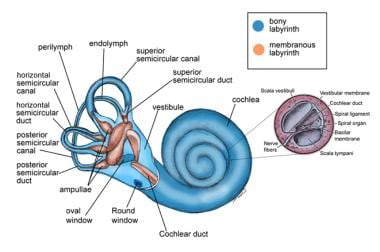
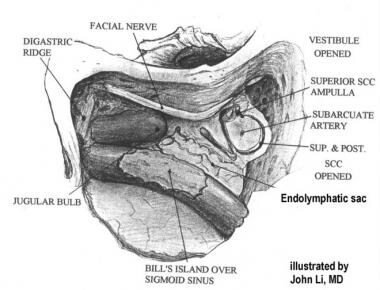
The paired box transcription factor, Pax2, is important for cochlear development in the mouse inner ear. Two mutant alleles of Pax2, a knockout and a frameshift mutation (Pax21Neu), show either agenesis or severe malformation of the cochlea, respectively. In humans, mutations in the PAX2 gene cause renal coloboma syndrome that is characterized by kidney abnormalities, optic nerve colobomas and mild sensorineural deafness. To better understand the role of Pax2 in inner ear development, we examined the inner ear phenotype in the Pax2 knockout mice using paint-fill and gene expression analyses. We show that Pax2-/- ears often lack a distinct saccule, and the endolymphatic duct and common crus are invariably fused. However, a rudimentary cochlea is always present in all Pax2 knockout inner ears. Cochlear outgrowth in the mutants is arrested at an early stage due to apoptosis of cells that normally express Pax2 in the cochlear anlage. Lack of Pax2 affects tissue specification within the cochlear duct, particularly regions between the sensory tissue and the stria vascularis. Because the cochlear phenotypes observed in Pax2 mutants are more severe than those observed in mice lacking Otx1 and Otx2, we postulate that Pax2 plays a key role in regulating the differential growth within the cochlear duct and thus, its proper outgrowth and coiling. (+info)The endolymphatic duct is a narrow canal in the inner ear that is part of the membranous labyrinth. It connects the utricle and saccule (two sensory structures in the vestibular system responsible for detecting changes in head position and movement) to the endolymphatic sac (a dilated portion of the duct that helps regulate the volume and pressure of endolymph, a fluid found within the membranous labyrinth).
The endolymphatic duct plays a crucial role in maintaining the balance and homeostasis of the inner ear by allowing the absorption and circulation of endolymph. Disorders or abnormalities in this region can lead to various vestibular and hearing dysfunctions, such as Meniere's disease, endolymphatic hydrops, and other inner ear disorders.
The endolymphatic sac is a small, fluid-filled structure that is part of the inner ear. It is located near the vestibular aqueduct and is responsible for maintaining the balance of fluids in the inner ear. The endolymphatic sac also plays a role in the resorption of endolymph, which is the fluid that fills the membranous labyrinth of the inner ear. Disorders of the endolymphatic sac can lead to conditions such as Meniere's disease, which is characterized by vertigo, hearing loss, and tinnitus.
Menière disease is an inner ear disorder that is characterized by episodes of vertigo (a spinning sensation), tinnitus (ringing or buzzing in the ear), hearing loss, and aural fullness (a feeling of pressure or blockage in the ear). It is caused by an abnormal accumulation of endolymphatic fluid in the inner ear, which can lead to damage of the vestibular system and cochlea. The exact cause of this fluid buildup is not known, but it may be related to genetics, allergies, or autoimmune disorders. Menière disease is typically a chronic condition, with symptoms that can vary in frequency and severity over time. Treatment options include dietary modifications, diuretics, vestibular rehabilitation therapy, and, in some cases, surgery.
Endolymphatic hydrops is a term used to describe the abnormal accumulation of fluid (endolymph) within the inner ear. This condition is most commonly associated with Meniere's disease, but can also be seen in other disorders that affect the inner ear.
The inner ear is made up of two main parts: the cochlea, which is responsible for hearing, and the vestibular system, which helps to control balance. Both of these systems are filled with fluid, including endolymph, which is a watery fluid that bathes the sensory hair cells in these structures.
In endolymphatic hydrops, there is an overproduction or decreased absorption of endolymph, leading to an abnormal buildup of fluid within the inner ear. This can cause a variety of symptoms, including vertigo (a spinning sensation), tinnitus (ringing in the ears), hearing loss, and a feeling of fullness or pressure in the affected ear.
The exact cause of endolymphatic hydrops is not fully understood, but it is thought to be related to changes in the inner ear's fluid balance. Treatment options may include medications to help control symptoms, as well as surgical procedures to relieve pressure on the inner ear.
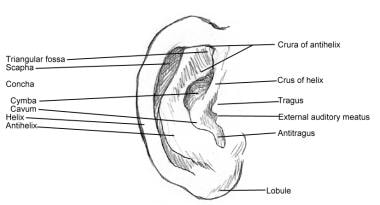
Ear neoplasms refer to abnormal growths or tumors that occur in the ear. These growths can be benign (non-cancerous) or malignant (cancerous) and can affect any part of the ear, including the outer ear, middle ear, inner ear, and the ear canal.
Benign ear neoplasms are typically slow-growing and do not spread to other parts of the body. Examples include exostoses, osteomas, and ceruminous adenomas. These types of growths are usually removed surgically for cosmetic reasons or if they cause discomfort or hearing problems.
Malignant ear neoplasms, on the other hand, can be aggressive and may spread to other parts of the body. Examples include squamous cell carcinoma, basal cell carcinoma, and adenoid cystic carcinoma. These types of tumors often require more extensive treatment, such as surgery, radiation therapy, and chemotherapy.
It is important to note that any new growth or change in the ear should be evaluated by a healthcare professional to determine the nature of the growth and develop an appropriate treatment plan.
The vestibular aqueduct is a bony canal that runs from the inner ear to the brain. It contains a membranous duct, called the endolymphatic duct, which is filled with a fluid called endolymph. The vestibular aqueduct plays a role in the maintenance of balance and hearing by regulating the pressure and composition of the endolymph. Abnormalities or damage to the vestibular aqueduct can lead to conditions such as endolymphatic hydrops, which can cause symptoms like vertigo, dizziness, and hearing loss.
The inner ear is the innermost part of the ear that contains the sensory organs for hearing and balance. It consists of a complex system of fluid-filled tubes and sacs called the vestibular system, which is responsible for maintaining balance and spatial orientation, and the cochlea, a spiral-shaped organ that converts sound vibrations into electrical signals that are sent to the brain.
The inner ear is located deep within the temporal bone of the skull and is protected by a bony labyrinth. The vestibular system includes the semicircular canals, which detect rotational movements of the head, and the otolith organs (the saccule and utricle), which detect linear acceleration and gravity.
Damage to the inner ear can result in hearing loss, tinnitus (ringing in the ears), vertigo (a spinning sensation), and balance problems.
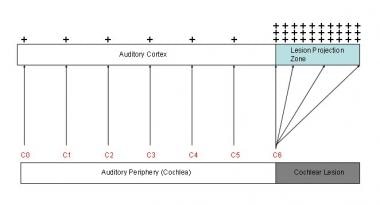
Sensorineural hearing loss (SNHL) is a type of hearing impairment that occurs due to damage to the inner ear (cochlea) or to the nerve pathways from the inner ear to the brain. It can be caused by various factors such as aging, exposure to loud noises, genetics, certain medical conditions (like diabetes and heart disease), and ototoxic medications.
SNHL affects the ability of the hair cells in the cochlea to convert sound waves into electrical signals that are sent to the brain via the auditory nerve. As a result, sounds may be perceived as muffled, faint, or distorted, making it difficult to understand speech, especially in noisy environments.
SNHL is typically permanent and cannot be corrected with medication or surgery, but hearing aids or cochlear implants can help improve communication and quality of life for those affected.
Von Hippel-Lindau (VHL) disease is a rare genetic disorder characterized by the development of tumors and cysts in various parts of the body. It is caused by mutations in the VHL gene, which leads to the abnormal growth of blood vessels, resulting in the formation of these tumors.
The tumors associated with VHL disease can develop in several organs, including the eyes (in the form of retinal hemangioblastomas), the brain and spinal cord (in the form of cerebellar hemangioblastomas and spinal cord hemangioblastomas), the adrenal glands (in the form of pheochromocytomas or paragangliomas), the kidneys (in the form of clear cell renal cell carcinomas), and the pancreas (in the form of serous cystadenomas or neuroendocrine tumors).
Individuals with VHL disease are at risk for developing multiple tumors over their lifetime, and the severity of the disease can vary widely from person to person. The diagnosis of VHL disease is typically made through genetic testing, family history, and imaging studies to detect the presence of tumors. Treatment may involve surgical removal of the tumors, radiation therapy, or other interventions depending on the location and size of the tumors. Regular monitoring and follow-up are essential for individuals with VHL disease to manage their condition effectively.
 Endolymphatic duct
Endolymphatic duct abnormal endolymphatic duct morphology - Ontology Browser - Rat Genome Database
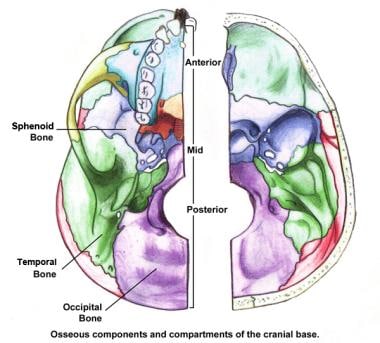
abnormal endolymphatic duct morphology - Ontology Browser - Rat Genome Database Skull Base Anatomy: Overview, Anterior Skull Base, Middle Skull Base
Skull Base Anatomy: Overview, Anterior Skull Base, Middle Skull Base The internal cranial anatomy of Romundina stellina Ørvig, 1975 (Vertebrata, Placodermi, Acanthothoraci) and the origin of jawed...
The internal cranial anatomy of Romundina stellina Ørvig, 1975 (Vertebrata, Placodermi, Acanthothoraci) and the origin of jawed...![Blom HM[au] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Blom HM[au] - Search Results - PubMed
Blom HM[au] - Search Results - PubMed Interactive Prenatal Development Timeline - Advanced
Interactive Prenatal Development Timeline - Advanced head and neck anatomy.ppt
head and neck anatomy.ppt Apaf1-dependent programmed cell death is required for inner ear morphogenesis and growth | Development | The Company of...
Apaf1-dependent programmed cell death is required for inner ear morphogenesis and growth | Development | The Company of... Descriptive anatomy of the largest known specimen of Protoichthyosaurus prostaxalis (Reptilia: Ichthyosauria) including...
Descriptive anatomy of the largest known specimen of Protoichthyosaurus prostaxalis (Reptilia: Ichthyosauria) including... Medifocus Guidebook on Meniere's Disease
Medifocus Guidebook on Meniere's Disease Buy Alprazolam 0.5 Mg - kitchentablecult.com
Buy Alprazolam 0.5 Mg - kitchentablecult.com American Academy of Otolaryngology-Head and Neck Surgery Annual Meeting 2021 - Course Medical Shop
American Academy of Otolaryngology-Head and Neck Surgery Annual Meeting 2021 - Course Medical Shop Best Cheats Library | Executor, Triggerbot, Updated - Restaurante o Jardim
Best Cheats Library | Executor, Triggerbot, Updated - Restaurante o Jardim Pesquisa | Prevenção e Controle de Câncer
Pesquisa | Prevenção e Controle de Câncer The association between tinnitus, the neck and TMJ - MSK Neurology
The association between tinnitus, the neck and TMJ - MSK Neurology Ear: Anatomy | Concise Medical Knowledge
Ear: Anatomy | Concise Medical Knowledge Stapedius muscle | Radiology Reference Article | Radiopaedia.org
Stapedius muscle | Radiology Reference Article | Radiopaedia.org "Recent surgical advances and continued controversies in medically refr" by Jacob C Lucas and Robert S. Hong
"Recent surgical advances and continued controversies in medically refr" by Jacob C Lucas and Robert S. Hong Morphological analysis of sigmoid sinus anatomy: clinical applications to neurotological surgery | Journal of Otolaryngology -...
Morphological analysis of sigmoid sinus anatomy: clinical applications to neurotological surgery | Journal of Otolaryngology -... Large Vestibular Aqueduct Syndrome
Large Vestibular Aqueduct Syndrome SDB CoRe - Inner Ear Development
SDB CoRe - Inner Ear Development