Cranial Nerve Injuries
Cranial Nerves
Cranial Nerve Diseases
Endarterectomy, Carotid
Carotid Stenosis
Cranial Nerve Neoplasms
Sciatic Nerve
Treatment Outcome
Facial Nerve Injuries
Optic Nerve Injuries
Facial Nerve
Wounds and Injuries
Peripheral Nerves
Abducens Nerve Diseases
Spinal Nerves
Encyclopedias as Topic
Outcome Assessment (Health Care)
Retrospective Studies
Pancreatic Neoplasms
Avulsion fracture of the anterior half of the foramen magnum involving the bilateral occipital condyles and the inferior clivus--case report. (1/45)
A 38-year-old male presented with an avulsion fracture of the anterior half of the foramen magnum due to a traffic accident. He had palsy of the bilateral VI, left IX, and left X cranial nerves, weakness of his left upper extremity, and crossed sensory loss. He was treated conservatively and placed in a halo brace for 16 weeks. After immobilization, swallowing, hoarseness, and left upper extremity weakness improved. Hyperextension with a rotatory component probably resulted in strain in the tectorial membrane and alar ligaments, resulting in avulsion fracture at the sites of attachment, the bilateral occipital condyles and the inferior portion of the clivus. Conservative treatment is probably optimum even for this unusual and severe type of occipital condyle fracture. (+info)Extracranial carotid artery aneurysms: Texas Heart Institute experience. (2/45)
BACKGROUND AND PURPOSE: Aneurysms of the extracranial carotid artery (ECA) are rare. Large single-institution series are seldom reported and usually are not aneurysm type-specific. Thus, information about immediate and long-term results of surgical therapy is sparse. This review was conducted to elucidate etiology, presentation, and treatment for ECA aneurysms. METHODS: We retrospectively reviewed the case records of the Texas Heart Institute/St Luke's Episcopal Hospital, Houston, and found 67 cases of ECA aneurysms treated surgically (the largest series to date) between 1960 and 1995: 38 pseudoaneurysms after previous carotid surgery and 29 atherosclerotic or traumatic aneurysms. All aneurysms were surgically explored, and all were repaired except two: a traumatic distal internal carotid artery aneurysm and an infected pseudoaneurysm in which the carotid artery was ligated. RESULTS: Four deaths (three fatal strokes and one myocardial infarction) and two nonfatal strokes were directly attributed to a repaired ECA aneurysm (overall mortality/major stroke incidence, 9%); there was one minor stroke (incidence, 1.5%). The incidence of cranial nerve injury was 6% (four cases). During long-term follow-up (1.5 months-30 years; mean, 5.9 years), 19 patients died, mainly of cardiac causes (11 myocardial infarctions). CONCLUSION: The potential risks of cerebral ischemia and rupture as well as the satisfactory long-term results achieved with surgery strongly argue in favor of surgical treatment of ECA aneurysms. (+info)Cranial and cervical nerve injuries after repeat carotid endarterectomy. (3/45)
BACKGROUND AND PURPOSE: The incidence of cranial and/or cervical nerve injuries after primary carotid endarterectomy (CEA) ranges from 3% to 48%; however, the clinical outcome of these injuries after repeat CEA has not been thoroughly analyzed in the English-language medical literature. This prospective study analyzes the incidence and outcome of cranial nerve injuries after repeat CEA. PATIENTS AND METHODS: This study includes 89 consecutive patients who had repeat CEAs. Preoperative and postoperative cranial nerve evaluations were performed, including clinical examinations (neurologic) and direct laryngoscopy. Patients with vagal or glossopharyngeal nerve injuries also underwent comprehensive speech evaluations, video stroboscopy, fluoroscopy, and methylene blue testing for aspiration. Patients with postoperative cranial nerve injuries were followed up for a long time to assess their recovery. RESULTS: Twenty-five cranial and/or cervical nerve injuries were identified in 19 patients (21%). They included 8 hypoglossal nerves (9%), 11 vagal nerves or branches (12%) (6 recurrent laryngeal nerves [7%], 3 superior laryngeal nerves [3%], and 2 complex vagal nerves [2%]), 3 marginal mandibular nerves (3%), 2 greater auricular nerves (2%), and 1 glossopharyngeal nerve (1%). Twenty-two (88%) of these injuries were transient with a complete healing time ranging from 2 weeks to 28 months (18 of 22 injuries healed within 12 months). The remaining three injuries (12%) were permanent (1 recurrent laryngeal nerve, 1 glossopharyngeal nerve, and 1 complex vagal nerve injury). The recurrent laryngeal nerve injury had a longer healing time than the other cranial nerve injuries. CONCLUSIONS: Repeat CEA is associated with a high incidence of cranial and/or cervical nerve injuries, most of which are transient. However, some of these have a long healing time, and a few can be permanent with significant disability. (+info)Neurological abnormalities associated with CDMA exposure. (4/45)
Dysaesthesiae of the scalp and neurological abnormality after mobile phone use have been reported previously, but the roles of the phone per se or the radiations in causing these findings have been questioned. We report finding a neurological abnormality in a patient after accidental exposure of the left side of the face to mobile phone radiation [code division multiple access (CDMA)] from a down-powered mobile phone base station antenna. He had headaches, unilateral left blurred vision and pupil constriction, unilateral altered sensation on the forehead, and abnormalities of current perception thresholds on testing the left trigeminal ophthalmic nerve. His nerve function recovered during 6 months follow-up. His exposure was 0.015-0.06 mW/cm(2) over 1-2 h. The implications regarding health effects of radiofrequency radiation are discussed. (+info)Redo carotid endarterectomy versus primary carotid endarterectomy. (5/45)
BACKGROUND AND PURPOSE: Several authorities have recently advocated carotid stenting for recurrent carotid stenosis because of the perception that redo surgery has a higher complication rate than primary carotid endarterectomy (CEA). This study compares the early and late results of reoperations versus primary CEA. METHODS: All reoperations for recurrent carotid stenosis performed during a recent 7-year period by a single vascular surgeon were compared with primary CEA. Because all redo CEAs were done with polytetrafluoroethylene (PTFE) or vein patch closure, we only analyzed those primary CEAs that used the same patch closures. A Kaplan-Meier life-table analysis was used to estimate stroke-free survival rates and freedom from >/=50% recurrent stenosis. RESULTS: Of 547 primary CEAs, 265 had PTFE or saphenous vein patch closure, and 124 reoperations had PTFE or vein patch closure during the same period. Both groups had similar demographic characteristics. The indications for reoperation and primary CEA were symptomatic stenosis in 78% and 58% of cases and asymptomatic >/=80% stenosis in 22% and 42% of cases, respectively (P<0.001). The 30-day perioperative stroke and transient ischemic attack rates for reoperation and primary CEA were 4.8% versus 0.8% (P=0.015) and 4% versus 1.1%, respectively, with no perioperative deaths in either group. Cranial nerve injury was noted in 17% of reoperation patients versus 5.3% of primary CEA patients; however, most of these injuries were transient (P<0.001). Mean hospital stay was 1.8 days for reoperation versus 1.6 days for primary CEA. Cumulative rates of stroke-free survival and freedom from >/=50% recurrent stenosis for reoperation and primary CEA at 1, 3, and 5 years were 96%, 91%, and 82% and 98%, 96%, and 95% versus 94%, 92%, and 91% and 98%, 96%, and 96%, respectively (no significant differences). CONCLUSIONS: Reoperation carries higher perioperative stroke and cranial nerve injury rates than primary CEA. However, reoperations are durable and have stroke-free survival rates that are similar to primary CEA. These considerations should be kept in mind when carotid stenting is recommended instead of reoperation. (+info)Long-term outcome after severe head injury. (6/45)
From a consecutive series of 7000 patients with head injuries admitted to the regional accident service, Radcliffe Infirmary, Oxford between 10 and 24 years earlier, every patient was taken who had been amnesic or unconscious for one week or longer. Of these 479 patients, all but ten were traced, and either the cause of death was established or the survivors examined. Ten years after injury 4% were totally disabled, and 14% severely disabled to a degree precluding normal occupational or social life. Of the remainder, 49% had recovered, and the rest were dead. Additionally, a selected series of 64 patients whose unconsciousness had been prolonged for a month or more were studied. Forty of these had survived between three and 25 years after injury and were re-examined. On the basis of age at injury, the worst state of neurological responsiveness, and the duration of posttraumatic amnesia, the outcome of head injury can be predicted reliably in most cases. Patients and relatives need more reassurance and simple psychotherapeutic support, especially in the first few months after injury. Extrapolation from our figures suggests that each year in England and Wales 210 patients survive totally disabled and another 1500 are severely disabled. (+info)Tapia's syndrome following shoulder surgery. (7/45)
Multiple cranial palsy occurred after shoulder surgery in the sitting position. Compression by the tracheal tube, caused by displacement of the head, may have caused the injury. (+info)Perceptual and instrumental evaluation of voice and tongue function after carotid endarterectomy. (8/45)
OBJECTIVE: Laryngeal and tongue function was assessed in 28 patients to evaluate the presence, nature, and resolution of superior recurrent laryngeal and hypoglossal nerve damage resulting from standard open primary carotid endarterectomy (CEA). METHODS: The laryngeal and tongue function in 28 patients who underwent CEA were examined prospectively with various physiologic (Aerophone II, laryngograph, tongue transducer), acoustic (Multi-Dimensional Voice Program), and perceptual speech assessments. Measures were obtained from all participants preoperatively, and at 2 weeks and at 3 months postoperatively. RESULTS: The perceptual speech assessment indicated that the vocal quality of "roughness" was significantly more apparent at the 2-week postoperative assessment than preoperatively. However, by the 3-month postoperative assessment these values had returned to near preoperative levels, with no significant difference detected between preoperative and 3-month postoperative levels or between 2-week and 3-month postoperative levels. Both the instrumental assessments of laryngeal function and the acoustic assessment of vocal quality failed to identify any significant difference on any measure across the three assessment periods. Similarly, no significant impairment in tongue strength, endurance, or rate of repetitive tongue movements was detected at instrumental assessment of tongue function. CONCLUSIONS: No permanent changes to vocal or tongue function occurred in this group of participants after primary CEA. The lack of any significant long-term laryngeal or tongue dysfunction in this group suggests that the standard open CEA procedure is not associated with high rates of superior recurrent and hypoglossal nerve dysfunction, as previously believed. (+info)Cranial nerve injuries refer to damages or trauma to one or more of the twelve cranial nerves (CN I through CN XII). These nerves originate from the brainstem and are responsible for transmitting sensory information (such as vision, hearing, smell, taste, and balance) and controlling various motor functions (like eye movement, facial expressions, swallowing, and speaking).
Cranial nerve injuries can result from various causes, including head trauma, tumors, infections, or neurological conditions. The severity of the injury may range from mild dysfunction to complete loss of function, depending on the extent of damage to the nerve. Treatment options vary based on the type and location of the injury but often involve a combination of medical management, physical therapy, surgical intervention, or rehabilitation.
Hypoglossal nerve injuries refer to damages or impairments to the twelfth cranial nerve, also known as the hypoglossal nerve. This nerve is primarily responsible for controlling the movements of the tongue.
An injury to this nerve can result in various symptoms, depending on the severity and location of the damage. These may include:
1. Deviation of the tongue to one side when protruded (usually away from the side of the lesion)
2. Weakness or paralysis of the tongue muscles
3. Difficulty with speaking, swallowing, and articulation
4. Changes in taste and sensation on the back of the tongue (in some cases)
Hypoglossal nerve injuries can occur due to various reasons, such as trauma, surgical complications, tumors, or neurological disorders like stroke or multiple sclerosis. Treatment for hypoglossal nerve injuries typically focuses on managing symptoms and may involve speech and language therapy, exercises to strengthen the tongue muscles, and, in some cases, surgical intervention.
Laryngeal nerve injuries refer to damages or injuries to the recurrent laryngeal nerve (RLN) and/or the superior laryngeal nerve (SLN), which are the primary nerves that supply the larynx, or voice box. These nerves play crucial roles in controlling the vocal cord movements and protecting the airway during swallowing.
The recurrent laryngeal nerve provides motor function to all intrinsic muscles of the larynx, except for the cricothyroid muscle, which is innervated by the superior laryngeal nerve. The RLN also carries sensory fibers from a small area of the mucous membrane below the vocal folds.
Injuries to these nerves can result in voice changes, breathing difficulties, and swallowing problems. Depending on the severity and location of the injury, patients may experience hoarseness, weak voice, breathy voice, coughing while swallowing, or even complete airway obstruction in severe cases. Laryngeal nerve injuries can occur due to various reasons, such as surgical complications (e.g., thyroid, esophageal, and cardiovascular surgeries), neck trauma, tumors, infections, or iatrogenic causes.
Cranial nerves are a set of twelve pairs of nerves that originate from the brainstem and skull, rather than the spinal cord. These nerves are responsible for transmitting sensory information (such as sight, smell, hearing, and taste) to the brain, as well as controlling various muscles in the head and neck (including those involved in chewing, swallowing, and eye movement). Each cranial nerve has a specific function and is named accordingly. For example, the optic nerve (cranial nerve II) transmits visual information from the eyes to the brain, while the vagus nerve (cranial nerve X) controls parasympathetic functions in the body such as heart rate and digestion.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
Carotid endarterectomy is a surgical procedure to remove plaque buildup (atherosclerosis) from the carotid arteries, which are the major blood vessels that supply oxygen-rich blood to the brain. The surgery involves making an incision in the neck, opening the carotid artery, and removing the plaque from the inside of the artery wall. The goal of the procedure is to restore normal blood flow to the brain and reduce the risk of stroke caused by the narrowing or blockage of the carotid arteries.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
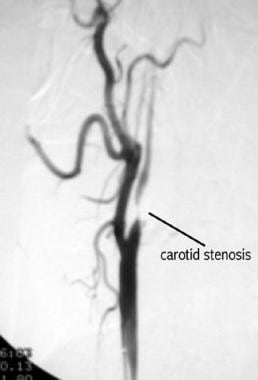
Carotid stenosis is a medical condition that refers to the narrowing or constriction of the lumen (inner space) of the carotid artery. The carotid arteries are major blood vessels that supply oxygenated blood to the head and neck. Carotid stenosis usually results from the buildup of plaque, made up of fat, cholesterol, calcium, and other substances, on the inner walls of the artery. This process is called atherosclerosis.
As the plaque accumulates, it causes the artery to narrow, reducing blood flow to the brain. Severe carotid stenosis can increase the risk of stroke, as a clot or debris from the plaque can break off and travel to the brain, blocking a smaller blood vessel and causing tissue damage or death.
Carotid stenosis is typically diagnosed through imaging tests such as ultrasound, CT angiography, or MRI angiography. Treatment options may include lifestyle modifications (such as quitting smoking, controlling blood pressure, and managing cholesterol levels), medications to reduce the risk of clots, or surgical procedures like endarterectomy or stenting to remove or bypass the blockage.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Facial nerve injuries refer to damages or trauma inflicted on the facial nerve, also known as the seventh cranial nerve (CN VII). This nerve is responsible for controlling the muscles involved in facial expressions, eyelid movement, and taste sensation in the front two-thirds of the tongue.
There are two main types of facial nerve injuries:
1. Peripheral facial nerve injury: This type of injury occurs when damage affects the facial nerve outside the skull base, usually due to trauma from cuts, blunt force, or surgical procedures in the parotid gland or neck region. The injury may result in weakness or paralysis on one side of the face, known as Bell's palsy, and may also impact taste sensation and salivary function.
2. Central facial nerve injury: This type of injury occurs when damage affects the facial nerve within the skull base, often due to stroke, brain tumors, or traumatic brain injuries. Central facial nerve injuries typically result in weakness or paralysis only on the lower half of the face, as the upper motor neurons responsible for controlling the upper face receive innervation from both sides of the brain.
Treatment for facial nerve injuries depends on the severity and location of the damage. For mild to moderate injuries, physical therapy, protective eyewear, and medications like corticosteroids and antivirals may be prescribed. Severe cases might require surgical intervention, such as nerve grafts or muscle transfers, to restore function. In some instances, facial nerve injuries may heal on their own over time, particularly when the injury is mild and there is no ongoing compression or tension on the nerve.
Optic nerve injuries refer to damages or trauma inflicted on the optic nerve, which is a crucial component of the visual system. The optic nerve transmits visual information from the retina to the brain, enabling us to see. Injuries to the optic nerve can result in various visual impairments, including partial or complete vision loss, decreased visual acuity, changes in color perception, and reduced field of view.
These injuries may occur due to several reasons, such as:
1. Direct trauma to the eye or head
2. Increased pressure inside the eye (glaucoma)
3. Optic neuritis, an inflammation of the optic nerve
4. Ischemia, or insufficient blood supply to the optic nerve
5. Compression from tumors or other space-occupying lesions
6. Intrinsic degenerative conditions affecting the optic nerve
7. Toxic exposure to certain chemicals or medications
Optic nerve injuries are diagnosed through a comprehensive eye examination, including visual acuity testing, slit-lamp examination, dilated fundus exam, and additional diagnostic tests like optical coherence tomography (OCT) and visual field testing. Treatment options vary depending on the cause and severity of the injury but may include medications, surgery, or vision rehabilitation.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
A wound is a type of injury that occurs when the skin or other tissues are cut, pierced, torn, or otherwise broken. Wounds can be caused by a variety of factors, including accidents, violence, surgery, or certain medical conditions. There are several different types of wounds, including:
* Incisions: These are cuts that are made deliberately, often during surgery. They are usually straight and clean.
* Lacerations: These are tears in the skin or other tissues. They can be irregular and jagged.
* Abrasions: These occur when the top layer of skin is scraped off. They may look like a bruise or a scab.
* Punctures: These are wounds that are caused by sharp objects, such as needles or knives. They are usually small and deep.
* Avulsions: These occur when tissue is forcibly torn away from the body. They can be very serious and require immediate medical attention.
Injuries refer to any harm or damage to the body, including wounds. Injuries can range from minor scrapes and bruises to more severe injuries such as fractures, dislocations, and head trauma. It is important to seek medical attention for any injury that is causing significant pain, swelling, or bleeding, or if there is a suspected bone fracture or head injury.
In general, wounds and injuries should be cleaned and covered with a sterile bandage to prevent infection. Depending on the severity of the wound or injury, additional medical treatment may be necessary. This may include stitches for deep cuts, immobilization for broken bones, or surgery for more serious injuries. It is important to follow your healthcare provider's instructions carefully to ensure proper healing and to prevent complications.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
The abducens nerve, also known as the sixth cranial nerve, is responsible for controlling the lateral rectus muscle of the eye, which enables the eye to move outward. Abducens nerve diseases refer to conditions that affect this nerve and can result in various symptoms, primarily affecting eye movement.
Here are some medical definitions related to abducens nerve diseases:
1. Abducens Nerve Palsy: A condition characterized by weakness or paralysis of the abducens nerve, causing difficulty in moving the affected eye outward. This results in double vision (diplopia), especially when gazing towards the side of the weakened nerve. Abducens nerve palsy can be congenital, acquired, or caused by various factors such as trauma, tumors, aneurysms, infections, or diseases like diabetes and multiple sclerosis.
2. Sixth Nerve Palsy: Another term for abducens nerve palsy, referring to the weakness or paralysis of the sixth cranial nerve.
3. Internuclear Ophthalmoplegia (INO): A neurological condition affecting eye movement, often caused by a lesion in the medial longitudinal fasciculus (MLF), a bundle of nerve fibers that connects the abducens nucleus with the oculomotor nucleus. INO results in impaired adduction (inward movement) of the eye on the side of the lesion and nystagmus (involuntary eye movements) of the abducting eye on the opposite side when attempting to look towards the side of the lesion.
4. One-and-a-Half Syndrome: A rare neurological condition characterized by a combination of INO and internuclear ophthalmoplegia with horizontal gaze palsy on the same side, caused by damage to both the abducens nerve and the paramedian pontine reticular formation (PPRF). This results in limited or no ability to move the eyes towards the side of the lesion and impaired adduction of the eye on the opposite side.
5. Brainstem Encephalitis: Inflammation of the brainstem, which can affect the abducens nerve and other cranial nerves, leading to various neurological symptoms such as diplopia (double vision), ataxia (loss of balance and coordination), and facial weakness. Brainstem encephalitis can be caused by infectious agents, autoimmune disorders, or paraneoplastic syndromes.
6. Multiple Sclerosis (MS): An autoimmune disorder characterized by inflammation and demyelination of the central nervous system, including the brainstem and optic nerves. MS can cause various neurological symptoms, such as diplopia, nystagmus, and INO, due to damage to the abducens nerve and other cranial nerves.
7. Wernicke's Encephalopathy: A neurological disorder caused by thiamine (vitamin B1) deficiency, often seen in alcoholics or individuals with malnutrition. Wernicke's encephalopathy can affect the brainstem and cause various symptoms such as diplopia, ataxia, confusion, and oculomotor abnormalities.
8. Pontine Glioma: A rare type of brain tumor that arises from the glial cells in the pons (a part of the brainstem). Pontine gliomas can cause various neurological symptoms such as diplopia, facial weakness, and difficulty swallowing due to their location in the brainstem.
9. Brainstem Cavernous Malformation: A benign vascular lesion that arises from the small blood vessels in the brainstem. Brainstem cavernous malformations can cause various neurological symptoms such as diplopia, ataxia, and facial weakness due to their location in the brainstem.
10. Pituitary Adenoma: A benign tumor that arises from the pituitary gland, located at the base of the brain. Large pituitary adenomas can compress the optic nerves and cause various visual symptoms such as diplopia, visual field defects, and decreased vision.
11. Craniopharyngioma: A benign tumor that arises from the remnants of the Rathke's pouch, a structure that gives rise to the anterior pituitary gland. Craniopharyngiomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the optic nerves and pituitary gland.
12. Meningioma: A benign tumor that arises from the meninges, the protective covering of the brain and spinal cord. Meningiomas can cause various neurological symptoms such as diplopia, headaches, and seizures depending on their location in the brain or spinal cord.
13. Chordoma: A rare type of malignant tumor that arises from the remnants of the notochord, a structure that gives rise to the spine during embryonic development. Chordomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the brainstem and spinal cord.
14. Metastatic Brain Tumors: Malignant tumors that spread from other parts of the body to the brain. Metastatic brain tumors can cause various neurological symptoms such as diplopia, headaches, seizures, and cognitive impairment depending on their location in the brain.
15. Other Rare Brain Tumors: There are many other rare types of brain tumors that can cause diplopia or other neurological symptoms, including gliomas, ependymomas, pineal region tumors, and others. These tumors require specialized diagnosis and treatment by neuro-oncologists and neurosurgeons with expertise in these rare conditions.
In summary, diplopia can be caused by various brain tumors, including pituitary adenomas, meningiomas, chordomas, metastatic brain tumors, and other rare types of tumors. It is important to seek medical attention promptly if you experience diplopia or other neurological symptoms, as early diagnosis and treatment can improve outcomes and quality of life.
Spinal nerves are the bundles of nerve fibers that transmit signals between the spinal cord and the rest of the body. There are 31 pairs of spinal nerves in the human body, which can be divided into five regions: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve carries both sensory information (such as touch, temperature, and pain) from the periphery to the spinal cord, and motor information (such as muscle control) from the spinal cord to the muscles and other structures in the body. Spinal nerves also contain autonomic fibers that regulate involuntary functions such as heart rate, digestion, and blood pressure.
A nerve crush injury is a type of peripheral nerve injury that occurs when there is excessive pressure or compression applied to a nerve, causing it to become damaged or dysfunctional. This can happen due to various reasons such as trauma from accidents, surgical errors, or prolonged pressure on the nerve from tight casts, clothing, or positions.
The compression disrupts the normal functioning of the nerve, leading to symptoms such as numbness, tingling, weakness, or pain in the affected area. In severe cases, a nerve crush injury can cause permanent damage to the nerve, leading to long-term disability or loss of function. Treatment for nerve crush injuries typically involves relieving the pressure on the nerve, providing supportive care, and in some cases, surgical intervention may be necessary to repair the damaged nerve.
Nerve regeneration is the process of regrowth and restoration of functional nerve connections following damage or injury to the nervous system. This complex process involves various cellular and molecular events, such as the activation of support cells called glia, the sprouting of surviving nerve fibers (axons), and the reformation of neural circuits. The goal of nerve regeneration is to enable the restoration of normal sensory, motor, and autonomic functions impaired due to nerve damage or injury.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
I'm not aware of any medical definition for the term "Boston." It is a city in the state of Massachusetts, USA, and is widely known for its cultural institutions, such as Boston Symphony Orchestra, Boston Ballet, and The Museum of Fine Arts. Additionally, it is home to many renowned medical institutions, including Massachusetts General Hospital, Brigham and Women's Hospital, and Dana-Farber Cancer Institute. However, "Boston" does not have a specific meaning or definition in the medical field.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Healthcare disparities refer to differences in the quality, accessibility, and outcomes of healthcare that are systematically related to social or economic disadvantage. These disparities may exist between different racial, ethnic, socioeconomic, gender, sexual orientation, geographic, or disability status groups. They can result from a complex interplay of factors including provider bias, patient-provider communication, health system policies, and structural racism, among others. Healthcare disparities often lead to worse health outcomes and reduced quality of life for disadvantaged populations.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
 Surgical Outcomes Analysis and Research
Surgical Outcomes Analysis and Research
Basilar skull fracture
Max Talmey
Carotid endarterectomy
Trapezius
Radiation therapy
Birth trauma (physical)
Cadaveric spasm
Ellen Rae Greenberg
Sixth nerve palsy
Zenon Mariak
Fourth nerve palsy
Esotropia
Marcus Gunn phenomenon
Complications of traumatic brain injury
Cranial nerve disease
Occipital condyles
List of MeSH codes (C21)
Brown-Vialetto-Van Laere syndrome
Gennaro Gattuso
Abducens nerve
Epidural hematoma
Neurological disorder
Obstetrical forceps
List of ICD-9 codes 800-999: injury and poisoning
Harrison's Principles of Internal Medicine
Diabetic neuropathy
Intraoperative neurophysiological monitoring
Neuropathic pain
Orbital blowout fracture
Cranial Nerve Diseases - Facial Nerve Injuries | CU Experts | CU Boulder
 Neck Trauma Management Clinical Presentation: History, Physical Examination
Neck Trauma Management Clinical Presentation: History, Physical Examination
 Optic Nerve Injuries; Optic Nerve Trauma; Optic Neuropathy, Traumatic; Second Cranial Nerve Trauma
Optic Nerve Injuries; Optic Nerve Trauma; Optic Neuropathy, Traumatic; Second Cranial Nerve Trauma
Birth Trauma: Overview, Etiology, Prognosis
Surgical Outcomes Analysis and Research - Wikipedia
 Results of the ROADSTER multicenter trial of transcarotid stenting with dynamic flow reversal
Results of the ROADSTER multicenter trial of transcarotid stenting with dynamic flow reversal
 Anjan K. Chatterjee, MD profile | PennMedicine.org
Anjan K. Chatterjee, MD profile | PennMedicine.org
Complications of Carotid Endarterectomy (CEA) in the Postanesthesia Care Unit (PACU): Practice Essentials, Problem:...
 Carotid Body Tumor: Symptoms, Causes & Treatment
Carotid Body Tumor: Symptoms, Causes & Treatment
Skull Fracture: Practice Essentials, History of the Procedure, Problem
Classification and Complications of Traumatic Brain Injury: Practice Essentials, Epidemiology, Pathophysiology
 Vascular disease | University Hospitals
Vascular disease | University Hospitals
 Head Trauma - WSAVA2008 - VIN
Head Trauma - WSAVA2008 - VIN
 Ying Guo | MD Anderson Cancer Center
Ying Guo | MD Anderson Cancer Center
Plus it
 Research | Division of Plastic and Reconstructive Surgery | UTHSC
Research | Division of Plastic and Reconstructive Surgery | UTHSC
 Neurological Surgery - New York City - Montefiore Medical Center - Facial Pain and Hemifacial Spasm Center
Neurological Surgery - New York City - Montefiore Medical Center - Facial Pain and Hemifacial Spasm Center
 Clinical Characteristics of Recurrent Nasopharyngeal Carcinoma in High-Incidence Area
Clinical Characteristics of Recurrent Nasopharyngeal Carcinoma in High-Incidence Area
2014 ICD-9-CM Diagnosis Codes 767.* : Birth trauma
 Pituitary Surgery | Neurosurgery | Stanford Medicine
Pituitary Surgery | Neurosurgery | Stanford Medicine
 Rick Redett III, M.D., Professor of Plastic and Reconstructive Surgery | Johns Hopkins Medicine
Rick Redett III, M.D., Professor of Plastic and Reconstructive Surgery | Johns Hopkins Medicine
 Scranton Catastrophic Injury Lawyer | Munley Law Personal Injury Attorneys
Scranton Catastrophic Injury Lawyer | Munley Law Personal Injury Attorneys
 View source for Sensorineural hearing loss - wikidoc
View source for Sensorineural hearing loss - wikidoc
 Call Transcript: November 13, 2018 | Clinicians Outreach and Outreach Communication (COCA)
Call Transcript: November 13, 2018 | Clinicians Outreach and Outreach Communication (COCA)
Injury diagnoses | Emergency Medicine Journal
 ICD-10-CM Diagnosis Code S04.21XA - Injury of trochlear nerve, right side, initial encounter
ICD-10-CM Diagnosis Code S04.21XA - Injury of trochlear nerve, right side, initial encounter
Neurosciences | Providence
Traumatic brain in3
- We wrote the book on traumatic brain injuries. (autoaccident.com)
- Traumatic brain injuries can be one of the most devastating events that a family can face. (autoaccident.com)
- Read more below on traumatic brain injuries. (autoaccident.com)
Cognitive Impairment1
- More severe involvement may lead to progressive central neurologic deficits (dysarthria, ataxia, cranial nerve palsies, cognitive impairment) or to ischemic injury to the kidney, intestine, and/or digits. (nih.gov)
Seventh crani1
- During the procedure, she suffered an injury to her seventh cranial nerve resulting in permanent facial paralysis. (mdanational.com.au)
Disorders2
- Disorders that affect myelin interrupt nerve transmission. (msdmanuals.com)
- Clinical neurophysiology of cranial nerve disorders. (beds.ac.uk)
Neuropathy1
- Clinical Utility of Repetitive Nerve Stimulation Test in Differentiating Multifocal Motor Neuropathy From Progressive Muscular Atrophy. (beds.ac.uk)
Trigeminal1
- Injury to your bulldog's cranial nerve 7 (Facial Nerve Paralysis) or CN5 (Trigeminal nerve). (vet4bulldog.com)
Optic5
- Fibrous gliosis develops in plaques that are disseminated throughout the central nervous system (CNS), primarily in white matter, particularly in the lateral and posterior columns (especially in the cervical regions), optic nerves, and periventricular areas. (msdmanuals.com)
- C3671 Injury C99147 Neonatal Research Network Terminology C101036 Retinopathy of Prematurity with Plus Disease Retinopathy of Prematurity with Plus Disease A stage of retinopathy of prematurity characterized by the presence of the following in at least two quadrants around the optic nerve: dilation and tortuosity of major retinal vasculature as a result of increased blood flow. (nih.gov)
- Plus disease is characterized by at least two quadrants around the optic nerve showing evidence of dilation and tortuosity of the major retinal vessels resulting from increased blood flow or neovascularization of the iris or poor view of the retina due to vitreous haze. (nih.gov)
- Optic nerve conditions and visual discomfort/disturbances accounted for more than one-quarter (30.1%) of all ocular and vision-related hospital bed days. (health.mil)
- Neuro-ophthalmic diagnoses (conditions of the optic nerve, visual tract, and cranial nerves responsible for eye movements) accounted for the most hospital bed days. (health.mil)
Diseases1
- Diseases of the eleventh cranial (spinal accessory) nerve. (reference.md)
Carotid2
- Blunt-mechanism facial fracture patterns associated with internal carotid artery injuries: Recommendations for additional screening criteria based on analysis of 4,398 patients. (cns.org)
- Carotid endarterectomy has been the gold standard for the past 50 years, though it does carry risks such as cranial nerve injury, infection, and myocardial infarction (heart attack). (centraljersey.com)
Dysfunction4
- Dysfunction of one or more cranial nerves causally related to a traumatic injury. (nih.gov)
- Traumatic injuries to the RECURRENT LARYNGEAL NERVE that may result in vocal cord dysfunction. (childrensmercy.org)
- Symptomatology seems hyperactive dysfunction syndrome of the cranial nerves. (endocrine-abstracts.org)
- Financial costs of ocular injuries and visual dysfunction resulting from traumatic brain injury have been recently reported and are significant. (health.mil)
Tumors3
- Specialized imaging protocols are utilized for various neurologic indications including brain tumors, seizures, multiple sclerosis, dementia, traumatic brain injury, and cranial nerve imaging. (radnet.com)
- Causes may include nerve injury, vascular compression, tumors. (endocrine-abstracts.org)
- The most common structural complication of these tumors are cranial nerve deficits. (houstonendocrine.com)
Glossopharyngeal nerve1
- Cranial nerve IX is connected to difficulty swallowing (the glossopharyngeal nerve). (practicetestgeeks.com)
Surgical2
- While this technique protects the brain during the procedure, the large incision leaves a visible and lengthy scar across the neck and carries risks of surgical complications including bleeding, infection, heart attack, and cranial nerve injuries that can cause issues with swallowing, speaking, and sensation in the face. (vertical-group.com)
- Microvascular decompression is a surgical procedure that relieves abnormal compression of a cranial nerve. (symptoma.com)
Complications2
- [ 9 , 4 ] In addition to perioperative stroke, serious complications that may develop after CEA include myocardial ischemia and infarction , hemodynamic instability, cranial nerve (CN) injuries, and bleeding resulting in neck hematomas and airway compromise. (medscape.com)
- Birth injuries can range from minor issues like lacerations or bruises to life-threatening complications like spinal cord or brain damage. (lawrencefirm.com)
Fractures2
- 0.001) and lateral impact (ipsilateral temporal and sphenoid sinus fractures) (OR: 3.96, p = 0.028) were identified significant, whereas basilar skull fracture (OR: 1.58, p = 0.300) and injuries to ocular nerves (CN III, IV, and VI) (OR: 1.77, p = 0.055) were insignificant. (cns.org)
- Facial and skull fractures, airway crush or obstruction, penetrating neck trauma, and cranial nerve injuries can all be extremely dangerous. (munley.com)
Catastrophic12
- We help those who have suffered catastrophic injuries. (munley.com)
- Call our Scranton catastrophic injury lawyer today. (munley.com)
- Catastrophic injuries can have a life-changing effect on both an individual and their entire family. (munley.com)
- When a catastrophic injury is caused by the negligence of another, you may be able to pursue compensation for your injuries. (munley.com)
- An experienced Scranton catastrophic injury law firm can help you obtain the compensation you need to care for yourself and your family while you recover from your devastating injuries. (munley.com)
- After a catastrophic injury, you probably have many questions. (munley.com)
- Let a Scranton catastrophic injury lawyer at Munley Law Personal Injury Attorneys help in any way we can. (munley.com)
- What is a Catastrophic Injury? (munley.com)
- A catastrophic injury is considered a physical injury or illness that has a life-altering impact on the accident victim. (munley.com)
- Unlike a serious or minor injury, which can heal in a few weeks or months, a catastrophic injury may be permanent. (munley.com)
- Brain injuries are among the most devastating types of catastrophic injuries. (munley.com)
- Andrew is conducting an examination on a patient undergoing rehabilitation following a catastrophic brain injury. (practicetestgeeks.com)
Compression2
- Introduction: Neurogenic hypertension is associated with unilateral neurovascular compression of the brainstem and cranial nerves V, IX-X, VII, VIII. (endocrine-abstracts.org)
- Compression of cranial nerve 5 can cause pain and numbness in the forehead and nose. (houstonendocrine.com)
Ocular2
- Injury to ocular nerves is not predictive but as an essential differential diagnosis with reversible outcome. (cns.org)
- The current report used an ocular and vision disease classification system and several health care burden measures to quantify the impacts of various ocular and vision-related illnesses and injuries among active component service members of the U.S. Armed Forces during 2018. (health.mil)
Vascular1
- Pituitary adenomas often invade the medial wall of the cavernous sinus, but this structure is generally not surgically removed because of the risk of vascular and cranial nerve injury. (stanford.edu)
Jugular2
- 23. Intraoperative relationship of the spinal accessory nerve to the internal jugular vein: variation from cadaver studies. (nih.gov)
- The two components of the nerve join and exit the skull via the jugular foramen, innervating the sternocleidomastoid and trapezius muscles, which become weak or paralyzed if the nerve is injured. (reference.md)
Risks1
- Dr Biggs recalled his usual practice was to inform the patient of the risks of surgery, including injury to the facial nerve. (mdanational.com.au)
Rehabilitation1
- This glossary provides information and definitions of medical terms associated with brain injury and rehabilitation to help you or your family. (brainline.org)
Structures2
- These structures produce, transmit and interpret nerve impulses. (drugs.com)
- Other advantages include avoidance of general anesthesia, better exposure of structures including muscular process, and rostral position of cranial esophagus: indeed, the dissection of the esophageal ostium from the muscular process is better performed with the patient standing. (ecvs.org)
Wounds1
- Hock and knee injuries vary in severity, ranging from areas of hair loss or broken skin, scabs, or minor swelling to areas with major swelling and/or open wounds with purulent discharge. (merckvetmanual.com)
Clinical2
- Origin and prevalence of the accessory phrenic nerve: A meta-analysis and clinical appraisal. (beds.ac.uk)
- Clinical and Electromyographic Characteristics of Unilateral Vocal Fold Paralysis With Lower Cranial Nerve Injury. (beds.ac.uk)
Disease1
- The nerve is commonly involved in MOTOR NEURON DISEASE, and may be injured by trauma to the posterior triangle of the neck. (reference.md)
Peripheral1
- Injury to the cerebellar germinal matrix may result in peripheral cerebellar bleeds. (ajnr.org)
Head12
- To eliminate the bias, two cohorts were matched according to age, gender, Abbreviated Injury Scale (AIS) of head and face, and Injury Severity Score (ISS). (cns.org)
- Face, neck, and head injuries can be life-threatening. (munley.com)
- The pattern of injury in patients with head and neck pain is remarkably consistent. (hmccentre.com)
- Well, in fact, it is all in your head, the injury pain is real. (hmccentre.com)
- A head injury or traumatic brain injury (TBI) is a common consequence of injury-related accidents. (autoaccident.com)
- The significant forces involved in serious accidents can produce the apparent results of major head trauma and the less obvious but more frequent results of concussions, minor TBIs, and long-term head injury symptoms. (autoaccident.com)
- A brain injury is generally caused by trauma to the head resulting in brain and skull damage. (autoaccident.com)
- Pain and suffering for the emotional and psychological harms caused by a severe head injury. (autoaccident.com)
- Closed head injuries may not produce visible traumas. (autoaccident.com)
- In any injury accident involving a blow to the head, the person and his/her family, friends, and co-workers should be alert for any changes in the injured person's mental or emotional status. (autoaccident.com)
- It has been shown, for example, that acceleration/deceleration injuries can be caused to the brain in cases where rapid speed changes occurred, even if there was no apparent striking of the head on other objects -- the medical evidence is that the brain can be "bruised" in these instances merely by impacting the inside of the skull when a sudden speed change happens. (autoaccident.com)
- The one positioned in the steering wheel protect the neck and head, reducing the possibility of cranial nerves and traumatic spinal cord injuries in an accident. (hyosung.com)
19991
- The figure above shows the rate of traumatic brain injury (TBI)-related deaths among persons aged 0-19 years, by age group, in the United States during 1999-2010, based on data from the National Vital Statistics System. (cdc.gov)
Fibers1
- This swelling results in pressure on the nerve fibers and their blood vessels. (symptoma.com)
Seizures1
- Even those without obvious physical injuries may be left with seizures, behavioral problems, speech and language impairments, learning disabilities, developmental delays, cognitive impairments, or intellectual deficiencies. (lawrencefirm.com)
Unilateral1
- Limperopoulos et al reported unilateral cerebellar atrophy following contralateral cerebral injuries and vice versa in preterm babies. (ajnr.org)
Stroke1
- Then he started walking funny and we thought he had a stroke or cranial nerve injury. (paleomg.com)
Birth injuries8
- Birth injuries can alter the lives of victims and their families forever. (lawrencefirm.com)
- Although some birth injuries are mild and have no long-term consequences, others can cause lifelong impairments that impede the child's cognitive, emotional, and/or physical development. (lawrencefirm.com)
- In many situations, doctors may avoid birth injuries by following a set standard of care, closely monitoring the mother's and child's health, and immediately resolving any suspected concerns that develop throughout pregnancy, labor, and delivery. (lawrencefirm.com)
- Many children who suffer birth injuries may never recover. (lawrencefirm.com)
- However, some birth injuries that cause harm to the brain, nerves, and muscles may not be immediately apparent. (lawrencefirm.com)
- The parents of children suffering from birth injuries are sometimes hesitant to seek the help of a Bolingbrook birth injury malpractice attorney because they are under the impression that their child's injury was their fault. (willenslaw.com)
- Often, birth injuries cause mental or physical life-long disabilities, and can greatly affect the families who must care for the child. (willenslaw.com)
- In almost all cases, families are not aware of birth injuries until after the baby's birth. (willenslaw.com)
Carries signals1
- This nerve carries signals to the brain. (drugs.com)
Results in injuries2
- If the birth results in injuries or even the loss of life, however, this picture-perfect day can quickly turn into a nightmare. (willenslaw.com)
- The hocks and knees rub repeatedly as a cow moves in her stall or transitions between lying and standing, creating friction that results in injuries to these upper-leg regions over time. (merckvetmanual.com)
Mild1
- All of these injuries are seen with mild-to-moderate anoxia. (ajnr.org)
BRAIN INJURY12
- acquired brain injury - the implication of this term is that the individual experienced normal growth and development from conception through birth, until sustaining an insult to the brain at some later time which resulted in impairment of brain function. (brainline.org)
- Do you need help or answers from an experienced Sacramento traumatic brain injury attorney? (autoaccident.com)
- What is a Traumatic Brain Injury? (autoaccident.com)
- Can I Claim Compensation for a Traumatic Brain Injury? (autoaccident.com)
- While every personal injury case for a severe TBI is different, there is a wide array of damages that a Sacramento brain injury lawyer can recover on behalf of an injured person after an accident. (autoaccident.com)
- Lost wages for time missed at work to recover from a traumatic brain injury or attend a medical appointment. (autoaccident.com)
- Loss of consortium for damage to a marital relationship as a result of a brain injury. (autoaccident.com)
- How Long After a Brain Injury Do Symptoms Appear? (autoaccident.com)
- A traumatic brain injury can only be properly evaluated with the input of experienced medical personnel, including neuropsychologists, neurologists, and neuroradiologists. (autoaccident.com)
- In the video below, doctors from the Shirley Ryan Ability Lab discuss how a traumatic brain injury is treated with new technology and treatments. (autoaccident.com)
- For this reason, doctors recommend that those suffering from a brain injury maintain their brain health for the rest of their lives. (autoaccident.com)
- What are the long-term effects of a traumatic brain injury? (autoaccident.com)
Occurs4
- Any sort of damage to a newborn that occurs during or shortly after birth is referred to as a birth injury. (lawrencefirm.com)
- Medical malpractice occurs when a medical provider fails to accomplish these tasks and their carelessness leads to a preventable birth injury. (lawrencefirm.com)
- sh injury occurs when force or pressure is put on a body part. (munley.com)
- During much of this course, the facial nerve is encased in a bony canal, which may make it prone to injury when nerve swelling occurs. (symptoma.com)
Accessory2
- This nerve originates from motor neurons in the lower medulla (accessory portion of nerve) and upper spinal cord (spinal portion of nerve). (reference.md)
- Prevalence of the accessory deep peroneal nerve: A cadaveric study and meta-analysis. (beds.ac.uk)
Lawyer3
- As an Illiniois lawyer handling medical malpractice for 25 plus years now, I have seen many types of birth injury cases. (willenslaw.com)
- Some lawyers may claim to be birth injury lawyers, but the truth probably is that the lawyer is a medical malpractice lawyer or even a personal injury lawyer who happens to have experience with handling birth injury matters. (willenslaw.com)
- This is why families should consult with an experienced Bolingbrook birth injury lawyer to get the help they need. (willenslaw.com)
Muscles1
- The lateral rectus muscles around the eyes are controlled by cranial nerve VI (the abducens nerve), which limits or prevents lateral eye movement if this nerve is damaged. (practicetestgeeks.com)