Biliopancreatic Diversion
Obesity, Morbid
Vagotomy, Truncal
Bariatric Surgery
Gastric Bypass
Urinary Diversion
Jejunoileal Bypass
Triglyceride-induced diabetes associated with familial lipoprotein lipase deficiency. (1/54)
Raised plasma triglycerides (TGs) and nonesterified fatty acid (NEFA) concentrations are thought to play a role in the pathogenesis of insulin-resistant diabetes. We report on two sisters with extreme hypertriglyceridemia and overt diabetes, in whom surgical normalization of TGs cured the diabetes. In all of the family members (parents, two affected sisters, ages 18 and 15 years, and an 11-year-old unaffected sister), we measured oral glucose tolerance, insulin sensitivity (by the euglycemic-hyperinsulinemic clamp technique), substrate oxidation (indirect calorimetry), endogenous glucose production (by the [6,6-2H2]glucose technique), and postheparin plasma lipoprotein lipase (LPL) activity. In addition, GC-clamped polymerase chain reaction-amplified DNA from the promoter region and the 10 coding LPL gene exons were screened for nucleotide substitution. Two silent mutations were found in the father's exon 4 (Glu118 Glu) and in the mother's exon 8 (Thr361 Thr), while a nonsense mutation (Ser447 Ter) was detected in the mother's exon 9. Mutations in exons 4 and 8 were inherited by the two affected girls. At 1-2 years after the appearance of hyperchylomicronemia, both sisters developed hyperglycemia with severe insulin resistance. Because medical therapy (including high-dose insulin) failed to reduce plasma TGs or control glycemia, lipid malabsorption was surgically induced by a modified biliopancreatic diversion. Within 3 weeks of surgery, plasma TGs and NEFA and cholesterol levels were drastically lowered. Concurrently, fasting plasma glucose levels fell from 17 to 5 mmol/l (with no therapy), while insulin-stimulated glucose uptake, oxidation, and storage were all markedly improved. Throughout the observation period, plasma TG levels were closely correlated with both plasma glucose and insulin concentrations, as measured during the oral glucose tolerance test. These cases provide evidence that insulin-resistant diabetes can be caused by extremely high levels of TGs. (+info)Luminal dietary protein, not amino acids, induces pancreatic protease via CCK in pancreaticobiliary-diverted rats. (2/54)
We determined whether pancreatic adaptation to a high-protein diet depends on ingested protein in the intestinal lumen and whether such adaptation depends on a CCK or capsaicin-sensitive vagal afferent pathway in pancreaticobiliary-diverted (PBD) rats. Feeding a high-casein (60%) diet but not a high-amino acid diet to PBD rats increased pancreatic trypsin and chymotrypsin activities compared with those after feeding a 25% casein diet. In contrast, feeding both the high-nitrogen diets induced pancreatic hypertrophy in PBD rats. These pancreatic changes by the diets were abolished by treatment with devazepide, a CCK-A receptor antagonist. Protease zymogen mRNA abundance in the PBD rat was not increased by feeding the high-casein diet and was decreased by devazepide. Perivagal capsaicin treatment did not influence the values of any pancreatic variables in PBD rats fed the normal or high-casein diet. We concluded that luminal protein or peptides were responsible for the bile pancreatic juice-independent induction of pancreatic proteases on feeding a high-protein diet. The induction was found to be dependent on the direct action of CCK on the pancreas. Pancreatic growth induced by high-protein feeding in PBD rats may depend at least partly on absorbed amino acids. (+info)Vitamin A deficiency in a newborn resulting from maternal hypovitaminosis A after biliopancreatic diversion for the treatment of morbid obesity. (3/54)
BACKGROUND: Biliopancreatic diversion (BPD) has been advocated for the treatment of morbid obesity. This procedure has the theoretical advantage that patients retain normal eating capacity and lose weight irrespective of their eating habits. However, vitamin deficiencies may develop because BPD causes malabsorption. OBJECTIVE: This report describes a 40-y-old mother and her newborn infant, who developed vitamin A deficiency as a result of iatrogenic maternal malabsorption after BPD. Our primary objective is to show that BPD patients need close follow-up and lifelong micronutrient supplementation to prevent nutrient deficiencies in themselves and their offspring. DESIGN: The medical records of the mother and infant were reviewed, and their clinical course was followed until 10 mo postpartum. The mother was also interviewed on several occasions about her medical care, follow-up, and supplemental vitamin use. RESULTS: The mother developed night blindness with undetectable serum vitamin A concentrations in the third trimester of her pregnancy. Her vitamin A deficiency was untreated until she delivered her infant. At delivery, the infant also had vitamin A deficiency. He may have permanent retinal damage, but this is still unclear because the ophthalmologic examination performed at 2 mo of age was inconclusive. CONCLUSIONS: Complications of BPD may take many years to develop, and the signs and symptoms may be subtle. Because of the malabsorption that results from BPD, patients need lifelong follow-up and appropriate vitamin supplementation to prevent deficiencies. These nutrient deficiencies can also affect the offspring of female BPD patients. (+info)Potential of surgery for curing type 2 diabetes mellitus. (4/54)
OBJECTIVE: To review the effect of morbid obesity surgery on type 2 diabetes mellitus, and to analyze data that might explain the mechanisms of action of these surgeries and that could answer the question of whether surgery for morbid obesity can represent a cure for type 2 diabetes in nonobese patients as well. SUMMARY BACKGROUND DATA: Diabetes mellitus type 2 affects more than 150 million people worldwide. Although the incidence of complications of type 2 diabetes can be reduced with tight control of hyperglycemia, current therapies do not achieve a cure. Some operations for morbid obesity not only induce significant and lasting weight loss but also lead to improvements in or resolution of comorbid disease states, especially type 2 diabetes. METHODS: The authors reviewed data from the literature to address what is known about the effect of surgery for obesity on glucose metabolism and the endocrine changes that follow this surgery. RESULTS: Series with long-term follow-up show that gastric bypass and biliopancreatic diversion achieve durable normal levels of plasma glucose, plasma insulin, and glycosylated hemoglobin in 80% to 100% of severely obese diabetic patients, usually within days after surgery. Available data show a significant change in the pattern of secretion of gastrointestinal hormones. Case reports have also documented remission of type 2 diabetes in nonmorbidly obese individuals undergoing biliopancreatic diversion for other indications. CONCLUSIONS: Gastric bypass and biliopancreatic diversion seem to achieve control of diabetes as a primary and independent effect, not secondary to the treatment of overweight. Although controlled trials are needed to verify the effectiveness on nonobese individuals, gastric bypass surgery has the potential to change the current concepts of the pathophysiology of type 2 diabetes and, possibly, the management of this disease. (+info)Reduced expression of uncoupling proteins-2 and -3 in adipose tissue in post-obese patients submitted to biliopancreatic diversion. (5/54)
OBJECTIVE: Little is known about the physiological role and the regulation of uncoupling proteins-2 and -3 (UCP-2 and -3) in adipose tissue. We investigated whether the expression of UCP-2 and -3 in adipose tissue was affected by weight loss due to a biliopancreatic diversion (BPD) and related to the daily energy expenditure (24-h EE). DESIGN: Ten morbidly obese subjects (mean body mass index +/- s.e.m.=49.80 +/- 2.51 kg/m(2)) were studied before and 18+/-2 Months after BPD. METHODS: We determined body composition using tritiated water and 24-h EE in a respiratory chamber. Adipose tissue UCP-2 and -3 mRNA, plasma insulin, glucose, free fatty acids (NEFA), free triiodothyronine (FT3), free thyroxine (FT4) and leptin were assayed before and after BPD. RESULTS: BPD treatment resulted in a marked weight loss (P<0.001) mainly due to a fat mass reduction. A significant decrease in 24-h EE/fat-free mass (FFM) (P<0.05) and in UCP-2 (P<0.05) and UCP-3 (P<0.05) mRNA was observed. A significant reduction in plasma insulin, glucose, NEFA, FT3, FT4 and leptin was seen after BPD. The decline in plasma leptin and FFA was tightly correlated with the decrease in both UCP-2 and -3. A significant correlation was found between changes in FT3 and variations in 24-h EE (r=0.64, P<0.05). In a multiple-regression analysis changes in 24-h EE/FFM after BPD were significantly correlated with changes in UCP-3 expression (P<0.05). CONCLUSION: These findings suggest that UCPs in adipose tissue may play a role in the reduction in 24-h EE observed in post-obese individuals. (+info)The duodenal switch operation for the treatment of morbid obesity. (6/54)
OBJECTIVE: To determine the safety and efficacy of the duodenal switch procedure as surgical treatment of morbid obesity. SUMMARY BACKGROUND DATA: The longitudinal gastrectomy and duodenal switch procedure as performed for morbid obesity involves a 75% subtotal greater curvature gastrectomy and long limb suprapapillary Roux-en-Y duodenoenterostomy. This results in a restricted caloric intake and diversion of bile and pancreatic secretions to induce fat malabsorption. Broad acceptance of this procedure has been impeded because of concerns that the malabsorptive component may produce serious nutritional complications. METHODS: Review of data collected prospectively from all patients who underwent duodenal switch as the primary surgical treatment of morbid obesity at a single institution during the 10-year period beginning September 1992. Operative morbidity and mortality, weight loss, volume of food intake, and bowel function were recorded. Sequential measurements of serum albumin, hemoglobin, and calcium levels were obtained to assess metabolic function and nutrient absorption. RESULTS: Duodenal switch was performed as the primary operation in 701 (81%) of a total 863 patients undergoing bariatric surgery during the period of study. The average body mass index (BMI) was 52.8 (range, 34-95). Perioperative mortality was 1.4%, and morbidity (including leaks, wound dehiscence, splenectomy, and postoperative hemorrhage) occurred in 21 patients (2.9%). Weight loss averaged 127 pounds at 1 year, 131 at 3 years, and 118 at 5 or more years (% EBWL of 69%, 73%, and 66%, respectively). The mean number of bowel movements was fewer than 3 per day. Patients reported and maintained a mean restriction of 63% of their preoperative intake (approximately 1600 calories), with no specific food intolerance, at 3 or more years follow-up. At 3 years, serum albumin remained at normal levels in 98% of patients, hemoglobin in 52%, and calcium in 71%. No patients reported dumping, and marginal ulcers were not seen. CONCLUSIONS: The longitudinal gastrectomy with duodenal switch is a safe and effective primary procedure for the treatment of morbid obesity. It has the advantage of allowing acceptable alimentation with a minimum of side effects while producing and maintaining significant weight loss. These results are achieved without developing significant dietary restrictions or clinical metabolic or nutritional complications. (+info)Surgical treatment of obesity: a review. (7/54)
Obesity is a chronic disease due to excess fat storage, a genetic predisposition, and strong environmental contributions. This problem is worldwide, and the incidence is increasing daily. There are medical, physical, social, economic, and psychological comorbid conditions associated with obesity. There is no cure for obesity except possibly prevention. Nonsurgical treatment has been inadequate in providing sustained weight loss. Currently, surgery offers the only viable treatment option with longterm weight loss and maintenance for the morbidly obese. Surgeries for weight loss are called bariatric surgeries. There is no one operation that is effective for all patients. Gastric bypass operations are the most common operations currently used. Because there are inherent complications from surgeries, bariatric surgeries should be performed in a multidisciplinary setting. The laparoscopic approach is being used by some surgeons in performing the various operations. The success rate--usually defined as >50% excess weight loss that is maintained for at least five years from bariatric surgery--ranges from 40% in the simple to >70% in the complex operations. The weight loss from surgical treatment results in significant improvements and, in some cases, complete resolution of comorbid conditions associated with obesity. Patients undergoing surgery for obesity need lifelong nutritional supplements and medical monitoring. (+info)Biliopancreatic tumors: patient survival and quality of life after palliative treatment. (8/54)
OBJECTIVES: to analyse survival and quality of life of patients with malignant obstructive jaundice after palliative treatment, comparing endoscopic stent insertion and palliative surgical (palliative resection and bypass surgical). PATIENTS AND METHOD: eighty and seven patients were included in a trial. They were distributed to endoscopic stent (50) and palliative surgical (37). It analysed survival, quality of life and comfort index of jaundiced patients. The good quality of life was defined by absence of jaundice, pruritus and cholangitis after the initial treatment. RESULTS: the median survival of the patients treated to endoscopic stent was 9,6 months whereas the patients to surgical treatment survived a median of 17 months. The time free of disease was 4 months in stented patients and 10,5 months in surgical patients. There was no significant difference in comfort index between the two groups (stented 34%, surgical 42,5%) Neither was there significant difference in survival and quality of life between palliative resection and bypass surgery. CONCLUSIONS: despite the survival and time free of disease being better in surgical patients, there was no significant difference in overall quality of life between the two groups. The survival and quality of life are the same after palliative resection as after bypass surgery, for this should not be performed routinely or to justify resection as a debulking procedure. (+info)Biliopancreatic diversion is a surgical procedure for the treatment of morbid obesity. It involves creating a small pouch from the lower part of the stomach and connecting it directly to the last portion of the small intestine (ileum), bypassing the majority of the stomach and duodenum. This results in a significant reduction in food intake, as well as malabsorption of nutrients such as fats, proteins, and vitamins.
The procedure is designed to promote weight loss through restriction and malabsorption. The small pouch restricts the amount of food that can be consumed at one time, while the bypassed portion of the intestine reduces the absorption of calories from food. This results in a significant reduction in calorie intake, leading to weight loss.
However, due to the malabsorption of nutrients, patients who undergo biliopancreatic diversion are at risk for nutrient deficiencies and require lifelong supplementation with vitamins and minerals. The procedure also carries a higher risk of complications such as dumping syndrome, ulcers, and malnutrition compared to other weight loss surgeries.
It is important to note that biliopancreatic diversion should only be considered in patients who are severely obese (with a body mass index or BMI greater than 50) and have not been successful with non-surgical weight loss methods. The decision to undergo this procedure should be made in consultation with a team of healthcare professionals, including a bariatric surgeon, dietitian, and mental health professional.
Morbid obesity is a severe form of obesity, defined by a body mass index (BMI) of 40 or higher or a BMI of 35 or higher in the presence of at least one serious obesity-related health condition, such as diabetes, high blood pressure, or sleep apnea. It is called "morbid" because it significantly increases the risk of various life-threatening health problems and reduces life expectancy.
Morbid obesity is typically associated with significant excess body weight, often characterized by a large amount of abdominal fat, that can strain the body's organs and lead to serious medical complications, such as:
* Type 2 diabetes
* High blood pressure (hypertension)
* Heart disease
* Stroke
* Sleep apnea and other respiratory problems
* Nonalcoholic fatty liver disease (NAFLD)
* Osteoarthritis
* Certain types of cancer, such as breast, colon, and endometrial cancer
Morbid obesity can also have significant negative impacts on a person's quality of life, including mobility issues, difficulty with daily activities, and increased risk of mental health problems, such as depression and anxiety. Treatment for morbid obesity typically involves a combination of lifestyle changes, medication, and in some cases, surgery.
A truncal vagotomy is a surgical procedure that involves the selective or complete division of the trunks of the vagus nerves. The vagus nerves are pairs of nerves that originate in the brainstem and extend down to the abdomen, providing parasympathetic nerve supply to various organs. In a truncal vagotomy, the vagus nerves are cut above the level of the diaphragm, which results in denervation of the stomach and parts of the digestive tract.
This procedure is typically performed as a treatment for peptic ulcers, as it reduces acid secretion in the stomach by interrupting the nerve supply that stimulates acid production. However, truncal vagotomy can also have side effects such as altered gastric motility and decreased intestinal secretions, which may lead to symptoms like bloating, diarrhea, or dumping syndrome.
It's important to note that there are different types of vagotomy procedures, including selective vagotomy and highly selective vagotomy, which aim to preserve some of the nerve supply to the stomach and minimize side effects. The choice of procedure depends on various factors, such as the location and severity of the ulcer, patient's overall health, and individual preferences.
Bariatric surgery is a branch of medicine that involves the surgical alteration of the stomach, intestines, or both to induce weight loss in individuals with severe obesity. The primary goal of bariatric surgery is to reduce the size of the stomach, leading to decreased food intake and absorption, which ultimately results in significant weight loss.
There are several types of bariatric surgeries, including:
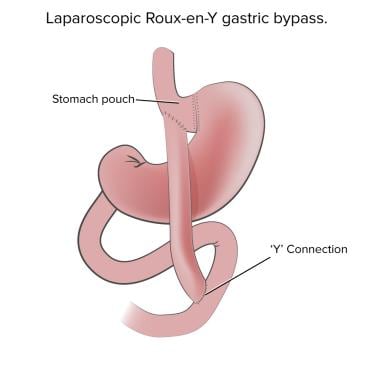
1. Roux-en-Y gastric bypass (RYGB): This procedure involves creating a small pouch at the top of the stomach and connecting it directly to the middle portion of the small intestine, bypassing the rest of the stomach and the upper part of the small intestine.
2. Sleeve gastrectomy: In this procedure, a large portion of the stomach is removed, leaving behind a narrow sleeve-shaped pouch that restricts food intake.
3. Adjustable gastric banding (AGB): This surgery involves placing an adjustable band around the upper part of the stomach to create a small pouch and limit food intake.
4. Biliopancreatic diversion with duodenal switch (BPD/DS): This is a more complex procedure that involves both restricting the size of the stomach and rerouting the small intestine to reduce nutrient absorption.
Bariatric surgery can lead to significant weight loss, improvement in obesity-related health conditions such as diabetes, high blood pressure, sleep apnea, and reduced risk of mortality. However, it is not without risks and complications, including infection, bleeding, nutrient deficiencies, and dumping syndrome. Therefore, careful consideration and evaluation by a multidisciplinary team are necessary before undergoing bariatric surgery.
Gastric bypass is a surgical procedure that involves creating a small pouch in the stomach and rerouting the small intestine to connect to this pouch, thereby bypassing the majority of the stomach and the first part of the small intestine (duodenum). This procedure is typically performed as a treatment for morbid obesity and related health conditions such as type 2 diabetes, sleep apnea, and high blood pressure.
The smaller stomach pouch restricts food intake, while the rerouting of the small intestine reduces the amount of calories and nutrients that are absorbed, leading to weight loss. Gastric bypass can also result in hormonal changes that help regulate appetite and metabolism, further contributing to weight loss and improved health outcomes.
There are different types of gastric bypass procedures, including Roux-en-Y gastric bypass and laparoscopic gastric bypass. The choice of procedure depends on various factors such as the patient's overall health, medical history, and personal preferences. Gastric bypass is generally considered a safe and effective treatment for morbid obesity, but like any surgical procedure, it carries risks and requires careful consideration and preparation.
Urinary diversion is a surgical procedure that involves the creation of a new way for urine to leave the body, bypassing the native urinary system. This is typically performed in individuals who have damaged or removed urinary systems due to conditions such as cancer, severe trauma, or congenital abnormalities.
There are several types of urinary diversions, including:
1. Ileal Conduit: A segment of the small intestine (ileum) is used to create a passageway for urine to flow from the ureters to an external collection bag or pouch worn on the abdomen.
2. Continent Urinary Reservoir: A pouch-like reservoir is created using a segment of the intestine, which is then connected to the ureters. The patient periodically empties the reservoir through a stoma (opening) in the abdominal wall using a catheter.
3. Orthotopic Neobladder: A pouch-like reservoir is created using a segment of the intestine, which is then connected to the urethra, allowing for normal urination through the native urethral opening.
These procedures can significantly improve the quality of life for patients with severe urinary system damage or disease, although they do come with potential complications such as infections, stone formation, and electrolyte imbalances.
Weight loss is a reduction in body weight attributed to loss of fluid, fat, muscle, or bone mass. It can be intentional through dieting and exercise or unintentional due to illness or disease. Unintentional weight loss is often a cause for concern and should be evaluated by a healthcare professional to determine the underlying cause and develop an appropriate treatment plan. Rapid or significant weight loss can also have serious health consequences, so it's important to approach any weight loss plan in a healthy and sustainable way.
A jejunoileal bypass is a surgical procedure that was once used to treat morbid obesity, but it is now rarely performed due to the high risk of serious complications. This procedure involves dividing the small intestine into two parts: the proximal jejunum and the distal ileum. The proximal jejunum is then connected to the colon, bypassing a significant portion of the small intestine where nutrient absorption occurs.
The goal of this surgery was to reduce the amount of food and nutrients that could be absorbed, leading to weight loss. However, it was found that patients who underwent jejunoileal bypass were at risk for developing severe malnutrition, vitamin deficiencies, bone disease, kidney stones, and liver problems. Additionally, many patients experienced unpleasant side effects such as diarrhea, bloating, and foul-smelling stools. Due to these significant risks and limited benefits, jejunoileal bypass has largely been replaced by other weight loss surgeries such as gastric bypass and sleeve gastrectomy.
Extrahepatic bile ducts refer to the portion of the biliary system that lies outside the liver. The biliary system is responsible for producing, storing, and transporting bile, a digestive fluid produced by the liver.
The extrahepatic bile ducts include:
1. The common hepatic duct: This duct is formed by the union of the right and left hepatic ducts, which drain bile from the corresponding lobes of the liver.
2. The cystic duct: This short duct connects the gallbladder to the common hepatic duct, allowing bile to flow into the gallbladder for storage and concentration.
3. The common bile duct: This is the result of the fusion of the common hepatic duct and the cystic duct. It transports bile from the liver and gallbladder to the duodenum, the first part of the small intestine, where it aids in fat digestion.
4. The ampulla of Vater (or hepatopancreatic ampulla): This is a dilated area where the common bile duct and the pancreatic duct join and empty their contents into the duodenum through a shared opening called the major duodenal papilla.
Extrahepatic bile ducts can be affected by various conditions, such as gallstones, inflammation (cholangitis), strictures, or tumors, which may require medical or surgical intervention.
 Intestinal bypass
Intestinal bypass
Bowel-associated dermatosis-arthritis syndrome
Bariatric surgery
Duodenal switch
Gastric bypass surgery
Obesity and fertility
Adjustable gastric band
BPD
List of MeSH codes (E04)
 Laparoscopic Conversion of Roux-en-Y Gastric Bypass to Biliopancreatic Diversion with Duodenal Switch from the SAGES Video...
Laparoscopic Conversion of Roux-en-Y Gastric Bypass to Biliopancreatic Diversion with Duodenal Switch from the SAGES Video...
 BilioPancreatic Diversion | International Federation for the Surgery of Obesity and Metabolic Disorders
BilioPancreatic Diversion | International Federation for the Surgery of Obesity and Metabolic Disorders
Robotically-Assisted Laparoscopic Biliopancreatic Diversion with Duodenal Switch. Learning Curve and Progress in Five Years of...
 How to Choose The Best Type of Weight Loss Surgery for You
How to Choose The Best Type of Weight Loss Surgery for You
 Biliopancreatic diversion with duodenal switch
Biliopancreatic diversion with duodenal switch
 Safety and efficacy of Biliopancreatic Diversion - FitForMe Research
Safety and efficacy of Biliopancreatic Diversion - FitForMe Research
 Biliopancreatic Diversion With Duodenal Switch - Green Valley Orthopedics
Biliopancreatic Diversion With Duodenal Switch - Green Valley Orthopedics
 Biliopancreatic Diversion With A Duodenal Switch | Andre Sny
Biliopancreatic Diversion With A Duodenal Switch | Andre Sny
 Biliopancreatic Diversion
Biliopancreatic Diversion
Biliopancreatic Diversion Surgery in Virginia - USWLS | Advanced Bariatric Services
 Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery
Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery
 Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery
Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery
 Biliopancreatic diversion with duodenal switch<...
Biliopancreatic diversion with duodenal switch<...
Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery
 Biliopancreatic Diversion with Duodenal Switch - Valhalla, NY & Carmel, NY: Advanced Surgeons
Biliopancreatic Diversion with Duodenal Switch - Valhalla, NY & Carmel, NY: Advanced Surgeons
 Bariatric Surgery and Diabetes Reversal | UPMC
Bariatric Surgery and Diabetes Reversal | UPMC
 Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery - ECU Health
Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery - ECU Health
 The four types of bariatric surgeries performed at Richmond Metabolic and Bariatric Surgery Clinic | Vancouver Coastal Health
The four types of bariatric surgeries performed at Richmond Metabolic and Bariatric Surgery Clinic | Vancouver Coastal Health
 Mid-Life Weight Gain Anne Collins
Mid-Life Weight Gain Anne Collins
NYP-CADC-Services-Weight Management-Surgery for Weight Loss and Metabolic Diseases | NYP
 Dr. med. Thomas Köstler in Zurich, Switzerland
Dr. med. Thomas Köstler in Zurich, Switzerland
 Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery | UCLA Health Library, Los Angeles, CA
Biliopancreatic Diversion with Duodenal Switch (BPD-DS) Weight-Loss Surgery | UCLA Health Library, Los Angeles, CA
 Treating the Obese Diabetic
Treating the Obese Diabetic
Obesity Treatment & Management: Approach Considerations, Patient Screening, Assessment, and Expectations, Weight-Loss Goals
 Clinics for Biliopancreatic Diversion with Duodenal Switch (BPD/DS) in Czech: Cost, Reviews in Top 1 Clinics | MediGlobus
Clinics for Biliopancreatic Diversion with Duodenal Switch (BPD/DS) in Czech: Cost, Reviews in Top 1 Clinics | MediGlobus
Intestinal bypass - Wikipedia
 NCA - Bariatric Surgery for the Treatment of Morbid Obesity (CAG-00250R) - Decision Memo
NCA - Bariatric Surgery for the Treatment of Morbid Obesity (CAG-00250R) - Decision Memo
 Circadian rhythms of GIP and GLP1 in glucose-tolerant and in type 2 diabetic patients after biliopancreatic diversion.<...
Circadian rhythms of GIP and GLP1 in glucose-tolerant and in type 2 diabetic patients after biliopancreatic diversion.<...
![Martín-Duce A[Author] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Martín-Duce A[Author] - Search Results - PubMed
Martín-Duce A[Author] - Search Results - PubMed
 Weighing the options for bariatric surgery | ACP Internist
Weighing the options for bariatric surgery | ACP InternistDuodenal17
- The biliopancreatic diversion with duodenal switch (BPD-DS), known simply as "Duodenal Switch (DS)" was created in 1988 by Douglas Hess, Bowling Green, Ohio, [2] and was first published by Picard Marceau, Québec, Canada [3] in 1993. (ifso.com)
- Robotically-Assisted Laparoscopic Biliopancreatic Diversion with Duodenal Switch. (sages.org)
- Laparoscopic biliopancreatic diversion with duodenal switch (BPD/DS) is the most technically challenging procedure in bariatric surgery. (sages.org)
- A Biliopancreatic Bypass with Duodenal Switch is a less common weight loss procedure that involves two major steps. (tunisie-esthetic.com)
- In a biliopancreatic diversion with duodenal switch, a portion of the stomach is removed but the pylorus remains intact. (gvortho.com)
- Background: This paper evaluates biliopancreatic diversion combined with the duodenal switch, forming a hybrid procedure which is a mixture of malabsorption and restriction. (andresny.com)
- The biliopancreatic diversion with a duodenal switch (BPD-DS) is a less commonly performed but very effective bariatric procedure that has been in existence for more than 20 years. (utmb.edu)
- Biliopancreatic diversion with duodenal switch (BPD/DS) is a type of surgery to cause weight loss. (franciscanhealth.org)
- Biliopancreatic Diversion with Duodenal Switch (BPD/DS): A Malabsorptive Procedure. (nygetfit.com)
- There are three malabsorptive procedures: Biliopancreatic Diversion with Duodenal Switch, Biliopancreatic Diversion, and Extended Roux-en-Y gastric bypass surgery . (nygetfit.com)
- Biliopancreatic Diversion with Duodenal Switch In this version of BPD, stomach removal is limited to the outer margin, creating a sleeve of stomach. (nygetfit.com)
- Biliopancreatic diversion with duodenal switch (BPD/DS) or simply duodenal switch (DS) is a bariatric surgery that can help patients lose up to 80% of their excess body weight. (vch.ca)
- Less common bariatric surgeries include gastric banding and biliopancreatic diversion with duodenal switch (BPD-DS). (medscape.com)
- There are several weight loss surgeries available, including gastric pass, sleeve gastrectomy, gastric banding, and biliopancreatic diversion with duodenal switch. (thedietchannel.com)
- Gastric pass, sleeve gastrectomy, and biliopancreatic diversion with duodenal switch are restrictive and malabsorptive surgeries. (thedietchannel.com)
- Bariatric surgery guidelines state that laparoscopic adjustable gastric banding (LAGB), laparoscopic sleeve gastrectomy, laparoscopic Roux-en-Y gastric bypass, and laparoscopic biliopancreatic diversion without/with duodenal switch, or related procedures, should be considered as primary bariatric and metabolic procedures performed in patients requiring weight loss and/or amelioration of obesity-related complications. (medscape.com)
- as a modification of the biliopancreatic diversion with duodenal switch. (bvsalud.org)
Bypass12
- These operations often resulted in a high degree of patient satisfaction because patients were able to eat larger meals than with a purely restrictive or standard Roux-en-Y gastric bypass procedure. (nygetfit.com)
- What Is Biliopancreatic Diversion Bypass (BPD)? (annecollins.com)
- They are jejunocolic bypass, end-to-side jejunoileal bypass, end-to-end jejunoileal bypass, and biliopancreatic diversion, respectively. (wikipedia.org)
- First appeared in 1980, biliopancreatic diversion involves two parts: gastrectomy and intestinal bypass. (wikipedia.org)
- Roux-en-Y Gastric Bypass in the Elderly: a Systematic Review. (nih.gov)
- Currently, the two most common types of weight loss surgery performed include sleeve gastrectomy and Roux-en-Y gastric bypass (RYGB). (medscape.com)
- In the new study analysing the prolonged benefits of weight loss surgery, diabetic patients aged 30-60 were randomly assigned to have standard medical treatment for Type 2 diabetes or weight loss surgery in the form of either a gastric bypass (shrinking the size of the stomach and rerouting the upper part of the small intestine) or biliopancreatic diversion (a more extensive bypassing of the intestine). (huffingtonpost.co.uk)
- The study found that 50% of patients who had weight loss surgery - from either gastric bypass or biliopancreatic diversion - had maintained diabetes remission for at least five years, compared with none of the 15 patients who had received standard medical treatment. (huffingtonpost.co.uk)
- Man who underwent Roux-en-Y gastric bypass at age 26, subsequently diagnosed with Crohn's disease, involving jejunum, ileum and colon, at age 42 when he presented with large volume diarrhoea and rectal bleeding. (medscape.com)
- Woman who underwent Roux-en-Y gastric bypass at age 38 and was subsequently diagnosed with ulcerative proctosigmoiditis at age 44. (medscape.com)
- Woman with IBD-U (pancolitis), who underwent Roux-en-Y gastric bypass at age 53 and was subsequently diagnosed with IBD at age 55. (medscape.com)
- Woman who underwent Roux-en-Y gastric bypass at age 40, although was subsequently reversed 1 year later. (medscape.com)
Procedure1
- A biliopancreatic diversion is a lesser-known weight-loss procedure. (blkmaxhospital.com)
Scopinaro1
- The Biliopancreatic Diversion (BPD) was developed in the 1970s by Nicola Scopinaro from Genoa, Italy [1]. (ifso.com)
Intestine2
- The bypassed portion of the intestine (biliopancreatic limb) delivers bile and pancreatic juices to the anastomosis at the ileum, where it meets the alimentary limb (proximal duodenum, through which food passes) to form the common channel. (vch.ca)
- BPD-DS includes sleeve gastrectomy, resection of a large section of the small intestine, and diversion of the pancreatic and biliary duct to a point below the junction of the ends of the resected gut. (medscape.com)
Pancreatic1
- Effects of bilio-pancreatic diversion on diabetic complications: a 10-year follow-up. (cnr.it)
Diabetic1
- Circadian rhythms of GIP and GLP1 in glucose-tolerant and in type 2 diabetic patients after biliopancreatic diversion. (unicatt.it)
Surgery3
- Biliopancreatic diversion is a major surgery that has certain risk factors associated with it. (blkmaxhospital.com)
- Recovery after biliopancreatic diversion may take up to three to six weeks, depending upon your condition, but the real recovery after this surgery remains for a lifetime. (blkmaxhospital.com)
- Most cases were women, had Roux-en-Y surgery years prior to diagnosis and few IBD-related complications. (medscape.com)
Limits2
- A biliopancreatic diversion limits food consumption and reduces the absorption of nutrients, proteins and fats. (blkmaxhospital.com)
- This diversion limits the time that food mixes with digestive juices and reduces the number of calories that can be absorbed, leading to weight loss. (vch.ca)
Type1
- biliopancreatic diversion ( n =8) type. (endocrine-abstracts.org)
Links1
- Find out more about Biliopancreatic Diversion BPD with the following links. (ifso.com)
Common1
- The longer pathway (biliopancreatic channel) carries bile from the liver to the common channel. (vch.ca)
Sleeve gastrectomy3
- 13 Peterli R, Wolnerhanssen BK, Peters T. et al Effect of laparoscopic sleeve gastrectomy vs. laparoscopic roux-en-y-gastric bypass on weight loss in patients with morbid obesity: The SM-BOSS Randomized Clinical Trial. (thieme-connect.com)
- 16 Salminen P, Helmiö M, Ovaska J. et al Effect of laparoscopic sleeve gastrectomy vs. laparoscopic Roux-en-Y gastric bypass on weight loss at 5 years among patients with morbid obesity. (thieme-connect.com)
- 17 Wölnerhanssen B, Peterli R, Hurme S.. Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: 5-year outcomes of merged data from two randomized clinical trials (SLEEVEPASS and SM-BOSS). (thieme-connect.com)
Laparoscopic4
- The Roux-en-Y Gastric Bypass, often called the "gastric bypass", has now been performed for more than 50 years and the laparoscopic approach has been refined since 1993. (utmbhealth.com)
- Laparoscopic Gastric Bypass, Roux-en-Y: Preliminary Report of Five Cases. (medscape.com)
- Laparoscopic Roux-en-Y gastric bypass: technique and 3-year follow-up. (medscape.com)
- Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. (medscape.com)
Bypass15
- What Is Biliopancreatic Diversion Bypass (BPD)? (annecollins.com)
- Biliopancreatic Diversion combines a certain amount of restriction with a high degree of malabsorption, and was originally designed to reduce the health complications associated with the discontinued jejuno-ileal bypass procedure. (annecollins.com)
- How Does Biliopancreatic Diversion Bypass Work? (annecollins.com)
- What Happens During A Biliopancreatic Diversion Bypass Operation? (annecollins.com)
- After Roux-en-Y gastric bypass the stomach is roughly 30 ml in capacity. (annecollins.com)
- Biliopancreatic diversion patients typically lose 60-80 percent of their initial excess weight, compared to 50-70 percent weight loss for Roux-en-Y gastric bypass patients. (annecollins.com)
- The principal health danger of biliopancreatic diversion stomach bypass is malnutrition, which is a lifelong and constant health risk. (annecollins.com)
- A Billiopancreatic Diversion bypass carries all the normal perioperative and post-operative health risks of any major surgical operation. (annecollins.com)
- Who Can Qualify For Biliopancreatic Diversion Bypass Surgery? (annecollins.com)
- Diabetes remission is greater after biliopancreatic diversion (BPD) than Roux-en-Y gastric bypass (RYGB) surgery. (unicatt.it)
- They are jejunocolic bypass, end-to-side jejunoileal bypass, end-to-end jejunoileal bypass, and biliopancreatic diversion, respectively. (wikipedia.org)
- First appeared in 1980, biliopancreatic diversion involves two parts: gastrectomy and intestinal bypass. (wikipedia.org)
- 7 Yan Y, Sha Y, Yao G. et al Roux-en-Y gastric bypass versus medical treatment for type 2 diabetes mellitus in obese patients: a systematic review and meta-analysis of randomized controlled trials. (thieme-connect.com)
- 18 Robert M, Espalieu P, Pelascini E. et al Efficacy and safety of one anastomosis gastric bypass versus Roux-en-Y gastric bypass for obesity (YOMEGA): a multicentre, randomized, openlabel, non-inferiority trial. (thieme-connect.com)
- Lack of association between 11 gene polymorphisms on weight loss 1 year after Roux-en-y gastric bypass surgery in woman. (cdc.gov)
Malabsorptive1
- Malabsorptive operations, such as biliopancreatic diversion (BPD), restrict both food intake and the amount of calories and nutrients the body absorbs. (medlineplus.gov)
Patients3
- Individual differences in calcium absorption determine chronic secondary hyperparathyroidism after biliopancreatic diversion in half of the patients who have normal levels of 25-hydroxyvitamin D. We aimed to evaluate if certain vitamin D receptor polymorphisms may be responsible for the latter. (nih.gov)
- Cases and controls study including 57 patients after biliopancreatic diversion with a mean serum 25-hydroxyvitamin D above 20 ng/mL, separated into those with secondary hyperparathyroidism (n = 26, cases) and those without it (n = 31, controls). (nih.gov)
- The aim of the present study was to assess the role of preoperative eating behavior in patients' selection for biliopancreatic diversion.Sixty-one consecutive patients who underwent BPD were evaluated for the present study. (unifi.it)
Surgical1
- Influence of -55CT polymorphism of UCP3 gene on surgical results of biliopancreatic diversion. (cdc.gov)
Complications1
- Effects of bilio-pancreatic diversion on diabetic complications: a 10-year follow-up. (cnr.it)
Results1
- Results of biliopancreatic diversion after five years. (bvsalud.org)
Study1
- The study was funded by the Fonds de la Recherche en Santé du Quebec. (medscape.com)