Middle Ear Ventilation
Otitis Media with Effusion
Myringoplasty
Ketoprofen
Tonsillitis
Tympanoplasty
Sulfisoxazole
Ambulatory Surgical Procedures
Palatine Tonsil
Endoscopy
Effects of anticholinergics on postoperative vomiting, recovery, and hospital stay in children undergoing tonsillectomy with or without adenoidectomy. (1/168)
BACKGROUND: Nausea and vomiting are the most frequent problems after minor ambulatory surgical procedures. The agents used to induce and maintain anesthesia may modify the incidence of emesis. When neuromuscular blockade is antagonized with anticholinesterases, atropine or glycopyrrolate is used commonly to prevent bradycardia and excessive oral secretions. This study was designed to evaluate the effect of atropine and glycopyrrolate on postoperative vomiting in children. METHODS: Ninety-three patients undergoing tonsillectomy with or without adenoidectomy were studied. After inhalation induction of anesthesia with nitrous oxide, oxygen, and halothane, anesthesia was maintained with a nitrous oxide-oxygen mixture, halothane, morphine, and atracurium. Patients were randomized to receive, in a double-blinded manner, either 15 microg/kg atropine or 10 microg/kg glycopyrrolate with 60 microg/kg neostigmine to reverse neuromuscular blockade. Patient recovery, the incidence of postoperative emesis, antiemetic therapy, and the duration of postoperative hospital stay were assessed. RESULTS: There were no significant differences in age, gender, weight, or discharge time from the postanesthesia care unit or the hospital between the groups. Twenty-four hours after operation, the incidence of vomiting in the atropine group (56%) was significantly less than in the glycopyrrolate group (81%; P<0.05). There was no significant difference between the atropine and glycopyrrolate groups in the number of patients who required antiemetics or additional analgesics. CONCLUSIONS: In children undergoing tonsillectomy with or without adenoidectomy, reversal of neuromuscular blockade with atropine and neostigmine is associated with a lesser incidence of postoperative emesis compared with glycopyrrolate and neostigmine. (+info)I.v. intraoperative ketoprofen in small children during adenoidectomy: a dose-finding study. (2/168)
We have investigated if a low dose of ketoprofen (0.3 mg kg-1) i.v., provided as good analgesia with less adverse effects than higher doses (1.0 and 3.0 mg kg-1) in 220 children, aged 1-7 yr, undergoing adenoidectomy, in a prospective, randomized, double-blind, placebo-controlled, parallel group study. The postoperative analgesic effect was notable even after the lowest dose of ketoprofen. However, the higher doses seemed to provide better analgesia with no increase in adverse events or intraoperative bleeding. None of the children experienced postoperative bleeding which would have required intervention or delayed discharge from hospital. This study confirms the efficacy and safety of intraoperative ketoprofen in children during adenoidectomy. (+info)Recovery after halothane anaesthesia induced with thiopental, propofol-alfentanil or halothane for day-case adenoidectomy in small children. (3/168)
We studied recovery from halothane anaesthesia in 93 children, aged 1-3 yr, undergoing day-case adenoidectomy. Children were allocated randomly to receive thiopental 5 mg kg-1 (group TH), alfentanil 10 micrograms kg-1 and propofol 3 mg kg-1 (group PAH) or 5% halothane (group HH) for induction of anaesthesia. In group TH, tracheal intubation was facilitated with succinylcholine (suxamethonium) 1.5 mg kg-1. In groups PAH and HH, tracheal intubation was performed without neuromuscular block, and succinylcholine was used only if required. Anaesthesia was maintained with 1-3% halothane during spontaneous respiration. Times to achieving predetermined recovery end-points were recorded. Quality of recovery was assessed using a score of 1-9 (best to worst) for sedation, crying, restlessness and agitation. A postoperative questionnaire was used to determine the well-being of the child at home, 24 h after operation. Emergence from anaesthesia (response to non-painful stimuli) occurred earlier in group HH (mean 9 (SD 6) min) than in groups PAH (13 (6) min, P < 0.01) and TH (18 (14) min, P < 0.01). Sitting up, walking and home readiness were achieved earlier in groups PAH and HH than in group TH (P < 0.05 for each variable). Children in group TH were more sedated during the first 30 min after anaesthesia than those in the two other groups (P < 0.05) while emergence-related delirium was more common in group HH than in group TH (P < 0.01). Well-being at home was similar in all groups. We conclude that induction of halothane anaesthesia with propofol-alfentanil or halothane provided more rapid recovery and earlier discharge than that with thiopental. (+info)Postoperative pain after adenoidectomy in children. (4/168)
We have investigated if pain intensity or analgesic requirements in hospital predicted pain intensity, pain duration or analgesic requirements at home in 611 children, aged 1-7 yr, after day-case adenoidectomy. We also investigated if ketoprofen 0.3-3.0 mg kg-1, administered pre-emptively i.v. during operation, modified pain at home. In hospital, a prospective, randomized, double-blind, placebo-controlled study design was performed. A standard anaesthetic technique was used in all children and fentanyl i.v. was available for rescue analgesia. After discharge, the study design was open, experimental, prospective and longitudinal. On return home, children were prescribed ketoprofen tablets 5 mg kg-1 day-1. Parents were asked to complete an analgesia diary; non-responders were contacted by telephone. The response rate was 91%. The number of doses of fentanyl given in hospital correlated with pain intensity at home (P < 0.001). There were no other correlations and no pre-emptive effect of ketoprofen. (+info)Double-blind comparison of sevofluran vs propofol and succinylcholine for tracheal intubation in children. (5/168)
We have studied intubating conditions in 64 healthy children, aged 3-10 yr, undergoing adenotonsillectomy, in a double-blind, randomized study. Intubation was performed 150 s after induction using either 8% sevoflurane in nitrous oxide and oxygen or propofol 3-4 mg kg-1 with succinylcholine 2 mg kg-1. An anaesthetist blinded to the technique performed intubation and scored intubating conditions using Krieg and Copenhagen Consensus Conference (CCC) scores. The trachea was intubated successfully at the first attempt in all patients under clinically acceptable conditions, although scores were significantly better with propofol and succinylcholine. The sevoflurane technique cost 3.62 +/- 0.55 Pounds to completion of tracheal intubation, significantly more (P < 0.001) than the cost of propofol-succinylcholine and isoflurane (2.04 +/- 0.54 Pounds) when based on actual amount of drug used. This cost increased to 4.38 +/- 0.05 Pounds when based on whole ampoules, which is significantly more than the cost of sevoflurane (P < 0.001). (+info)Comparison of intravenous and oral ketoprofen for postoperative pain after adenoidectomy in children. (6/168)
One hundred children, aged 1-9 yr, undergoing adenoidectomy were randomized to receive ketoprofen 1 mg kg-1 either i.v. with an oral placebo (n = 40) or ketoprofen 1 mg kg-1 orally with an i.v. placebo (n = 40), or both oral and i.v. placebo (n = 20). The study design was prospective and double blind with parallel groups. The pain was assessed at rest and during swallowing using the Maunuksela pain scale (0 = no pain, 10 = worst possible pain) after surgery for 3 h. Fentanyl 0.5 microgram kg-1 i.v. was given for rescue analgesia. Children in the i.v. group needed significantly less doses (1, 1-3; median and 10th/90th percentiles) of rescue analgesic compared with the oral group (2, 1-3; P = 0.024). Of those who needed rescue analgesic, three out of 30 children in the i.v. group required three or more doses of fentanyl compared with 10 out of 28 children in the oral group. There were no differences between the groups with respect to pain scores, operation times, perioperative bleeding or frequency of adverse events. (+info)PCR-based detection, restriction endonuclease analysis, and transcription of tonB in Haemophilus influenzae and Haemophilus parainfluenzae isolates obtained from children undergoing tonsillectomy and adenoidectomy. (7/168)
We developed and evaluated a PCR-based-restriction endonuclease analysis method to detect and analyze the tonB gene of Haemophilus influenzae and Haemophilus parainfluenzae from pediatric patients undergoing tonsillectomy and adenoidectomy. Multiple sites from the same patient, including the surface of adenoids and tonsils, as well as the core of tonsils, were cultured on chocolate agar and identified using standard procedures and the API NH Kit. A total of 55 H. influenzae isolates were recovered from different sites of 20 patients, and 32 H. parainfluenzae isolates were recovered from various sites of 12 patients. DNA was extracted from American Type Culture Collection strains and test isolates by the PureGene kit. Two primers, G1 (21-mer) and G2 (23-mer), were designed by us to amplify by PCR the tonB gene that consists of an 813-bp fragment. A nested PCR using primers T1 (23-mer) and T2 (24-mer) that flank an internal sequence to the gene of the order of 257 bp and restriction endonuclease digestion using XhoI and BglII were done to detect whether heterogeneity within the gene exists between the two species. Reverse transcription-PCR (RT-PCR) was finally done to detect transcription of the gene in both species. Our data have shown that the tonB gene was detected in both species. It is known to encode a virulent protein, TonB, in H. influenzae; however, demonstration of its presence in H. parainfluenzae is novel. Nested-PCR and restriction endonuclease analysis have shown that the tonB gene is apparently structurally the same in both species, with possible differences that may exist in certain H. parainfluenzae isolates. RT-PCR done on selected numbers of H. influenzae and H. parainfluenzae have shown that the tonB gene was transcribed in both species. This shows that the TonB protein, if expressed, may play a different role in the virulence in H. parainfluenzae since it is not needed for heme or heme complexes uptake as with H. influenzae. (+info)Long-term follow-up of obstructive sleep apnea syndrome following surgery in children and adults. (8/168)
Obstructive sleep apnea syndrome (OSAS) is characterized by recurrent apneas during sleep, resulting in repetitive hypoxemia. The present study retrospectively analyzed subjective and objective assessments of the patients with OSAS in a relatively long-term follow-up. From February 1986 to August 1996, 53 patients received surgical treatment for OSAS and snoring. Thirty-seven (27 males and 10 females) out of 53 patients completed the questionnaire and postoperative sleep study was obtained in 6 patients. In 20 children (<15 years), snoring, sleep apnea, and daytime sleepiness completely disappeared in 12, 19, and 16, and improved in 8, 1, and 4, respectively. These findings confirm that tonsillectomy and/or adenoidectomy in children may be the first selection for treatment. In 17 adults, snoring, sleep apnea, and daytime sleepiness completely disappeared in 2, 5, and 8, improved in 11, 8, and 7, and was unchanged in 4, 4, and 1, respectively. The apnea index in adults was significantly decreased in both early and late postoperative periods. These results suggest that surgery is a satisfactory alternative for adult patients if performed accurate preoperative diagnosis of the localization of the airway collapse and careful long-term follow-up. (+info)Adenoidectomy is a surgical procedure in which the adenoids are removed. The adenoids are a patch of tissue located behind the nasal cavity, near the roof of the mouth. They help to filter out germs that are breathed in through the nose. However, sometimes the adenoids can become enlarged or infected, leading to problems such as difficulty breathing through the nose, recurrent ear infections, and sleep apnea. In these cases, an adenoidectomy may be recommended to remove the adenoids and alleviate these symptoms.
The procedure is typically performed on an outpatient basis, which means that the patient can go home the same day as the surgery. The surgeon will use a special instrument to remove the adenoids through the mouth, without making any external incisions. After the surgery, the patient may experience some discomfort, sore throat, and difficulty swallowing for a few days. However, these symptoms usually resolve within a week or two.
It is important to note that an adenoidectomy is not the same as a tonsillectomy, which is the surgical removal of the tonsils. While the tonsils and adenoids are both part of the immune system and located in the same area of the mouth, they serve different functions and may be removed separately or together depending on the individual's medical needs.
A tonsillectomy is a surgical procedure in which the tonsils, two masses of lymphoid tissue located on both sides of the back of the throat, are removed. This procedure is typically performed to treat recurrent or severe cases of tonsillitis (inflammation of the tonsils), sleep-disordered breathing such as obstructive sleep apnea, and other conditions where the tonsils are causing problems or complications. The surgery can be done under general anesthesia, and there are various methods for removing the tonsils, including traditional scalpel excision, electrocautery, and laser surgery. After a tonsillectomy, patients may experience pain, swelling, and difficulty swallowing, but these symptoms typically improve within 1-2 weeks post-surgery.
Adenoids are a pair of masses of lymphoid tissue located in the nasopharynx, which is the upper part of the throat behind the nose. They are part of the immune system and help to protect against infection. Adenoids are largest in children and tend to shrink in size as people get older. In some cases, adenoids can become enlarged or infected, leading to problems such as breathing difficulties, ear infections, and sleep disorders. Treatment for enlarged or infected adenoids may include antibiotics, medications to reduce swelling, or surgical removal of the adenoids (adenoidectomy).
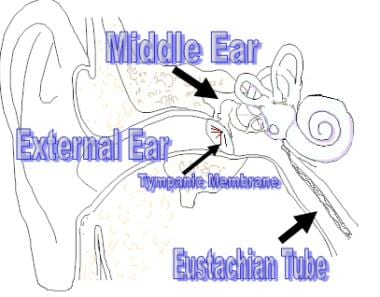
Middle ear ventilation refers to the normal process of air movement between the middle ear and the back of the nose (nasopharynx) through the eustachian tube. This tube is a narrow canal that connects the middle ear to the nasopharynx and helps to regulate air pressure in the middle ear, preventing its accumulation and subsequent negative pressure or fluid build-up, which can lead to conditions such as otitis media (middle ear infection) or serous otitis media (fluid in the middle ear).
The eustachian tube opens during activities such as swallowing, yawning, or chewing, allowing fresh air to enter the middle ear and any accumulated fluid or gas to be drained out. Abnormalities in middle ear ventilation can result from dysfunction of the eustachian tube, leading to various middle ear disorders.
Otitis media with effusion (OME), also known as serous otitis media or glue ear, is a medical condition characterized by the presence of fluid in the middle ear without signs or symptoms of acute ear infection. The fluid accumulation occurs due to the dysfunction of the Eustachian tube, which results in negative pressure and subsequent accumulation of sterile fluid within the middle ear space.
OME can lead to hearing difficulties, especially in children, as the fluid buildup impairs sound conduction through the ossicles in the middle ear. Symptoms may include mild hearing loss, tinnitus (ringing in the ears), and a sensation of fullness or pressure in the affected ear. In some cases, OME can resolve on its own within a few weeks or months; however, persistent cases might require medical intervention, such as placement of tympanostomy tubes (ear tubes) to drain the fluid and restore hearing.
Myringoplasty is a surgical procedure that involves reconstructing or repairing the tympanic membrane (eardrum) in the middle ear. The eardrum is the thin, delicate tissue that separates the outer ear from the inner ear. It plays a crucial role in hearing by vibrating in response to sound waves and transmitting these vibrations to the bones of the middle ear.
Myringoplasty is typically performed to treat chronic perforations or holes in the eardrum that have not healed on their own or with medical management. These perforations can result from various causes, such as infection, trauma, or congenital defects. By closing the perforation, myringoplasty helps prevent the risk of middle ear infections and improves hearing function.
The procedure involves harvesting a small piece of tissue, often from the patient's own body (such as the fascia surrounding a muscle), to use as a graft to cover the eardrum perforation. The graft is placed through an incision made in the ear canal or, less commonly, via an external approach through the mastoid bone behind the ear.
Myringoplasty is typically performed under general anesthesia and requires a short hospital stay for observation and monitoring. Following surgery, patients may need to avoid water exposure, heavy lifting, and strenuous activities for a few weeks to allow proper healing. The success rate of myringoplasty is generally high, with most patients experiencing improved hearing and reduced symptoms of ear infections.
Ketoprofen is a non-steroidal anti-inflammatory drug (NSAID) that is commonly used to treat pain, fever, and inflammation in the body. It works by inhibiting the production of prostaglandins, which are hormone-like substances that cause pain and inflammation in the body.
Ketoprofen has analgesic, anti-inflammatory, and antipyretic properties, making it a useful medication for managing various conditions such as arthritis, menstrual cramps, muscle pain, dental pain, and migraines. It is available in various forms, including oral capsules, tablets, suppositories, and topical creams or gels.
Like other NSAIDs, ketoprofen can cause side effects such as stomach ulcers, bleeding, and kidney damage if used in high doses or for extended periods. It is essential to follow the recommended dosage and consult with a healthcare provider before using this medication.
Tonsillitis is a medical condition characterized by inflammation and infection of the tonsils, which are two masses of lymphoid tissue located on either side of the back of the throat. The tonsils serve as a defense mechanism against inhaled or ingested pathogens; however, they can become infected themselves, leading to tonsillitis.
The inflammation of the tonsils is often accompanied by symptoms such as sore throat, difficulty swallowing, fever, swollen and tender lymph nodes in the neck, cough, headache, and fatigue. In severe or recurrent cases, a tonsillectomy (surgical removal of the tonsils) may be recommended to alleviate symptoms and prevent complications.
Tonsillitis can be caused by both viral and bacterial infections, with group A streptococcus being one of the most common bacterial causes. It is typically diagnosed based on a physical examination and medical history, and sometimes further confirmed through laboratory tests such as a throat swab or rapid strep test. Treatment may include antibiotics for bacterial tonsillitis, pain relievers, and rest to aid in recovery.
Tympanoplasty is a surgical procedure performed to reconstruct or repair the tympanic membrane (eardrum) and/or the small bones of the middle ear (ossicles). The primary goal of this surgery is to restore hearing, but it can also help manage chronic middle ear infections, traumatic eardrum perforations, or cholesteatoma (a skin growth in the middle ear).
During the procedure, a surgeon may use various techniques such as grafting tissue from another part of the body to rebuild the eardrum or using prosthetic materials to reconstruct the ossicles. The choice of technique depends on the extent and location of the damage. Tympanoplasty is typically an outpatient procedure, meaning patients can return home on the same day of the surgery.
Sulfisoxazole is an antibacterial drug, specifically a sulfonamide. It is defined as a synthetic, short-acting, bacteriostatic antibiotic that inhibits the growth of certain bacteria by interfering with their ability to synthesize folic acid, an essential component for their survival. Sulfisoxazole is used to treat various infections caused by susceptible bacteria, including respiratory tract infections, urinary tract infections, and skin infections.
It's important to note that the use of sulfonamides like sulfisoxazole has declined over time due to the emergence of bacterial resistance and the availability of alternative antibiotics with better safety profiles. Additionally, adverse reactions such as rashes, allergies, and blood disorders have been associated with their use, so they should be prescribed with caution and only when necessary.
Nasopharyngeal diseases refer to conditions that affect the nasopharynx, which is the uppermost part of the pharynx (throat) located behind the nose. The nasopharynx is lined with mucous membrane and contains the opening of the Eustachian tubes, which connect to the middle ear.
There are several types of nasopharyngeal diseases, including:
1. Nasopharyngitis: Also known as a "common cold," this is an inflammation of the nasopharynx caused by a viral infection. Symptoms may include a runny nose, sore throat, cough, and fever.
2. Nasopharyngeal cancer: A malignant tumor that develops in the nasopharynx. It is relatively rare but more common in certain populations, such as those of Southeast Asian or Southern Chinese descent. Symptoms may include a lump in the neck, nosebleeds, hearing loss, and difficulty swallowing.
3. Nasopharyngeal stenosis: A narrowing of the nasopharynx that can be congenital or acquired. Acquired stenosis may result from trauma, infection, or inflammation. Symptoms may include difficulty breathing through the nose and snoring.
4. Nasopharyngeal abscess: A collection of pus in the nasopharynx that can be caused by a bacterial infection. Symptoms may include fever, difficulty swallowing, and neck pain or stiffness.
5. Nasopharyngitis allergica: Also known as "hay fever," this is an inflammation of the nasopharynx caused by an allergic reaction to substances such as pollen, dust mites, or pet dander. Symptoms may include a runny nose, sneezing, and itchy eyes.
Treatment for nasopharyngeal diseases depends on the specific condition and its severity. Treatment options may include medications, surgery, or radiation therapy.
Ambulatory surgical procedures, also known as outpatient or same-day surgery, refer to medical operations that do not require an overnight hospital stay. These procedures are typically performed in a specialized ambulatory surgery center (ASC) or in a hospital-based outpatient department. Patients undergoing ambulatory surgical procedures receive anesthesia, undergo the operation, and recover enough to be discharged home on the same day of the procedure.
Examples of common ambulatory surgical procedures include:
1. Arthroscopy (joint scope examination and repair)
2. Cataract surgery
3. Colonoscopy and upper endoscopy
4. Dental surgery, such as wisdom tooth extraction
5. Gallbladder removal (cholecystectomy)
6. Hernia repair
7. Hysteroscopy (examination of the uterus)
8. Minor skin procedures, like biopsies and lesion removals
9. Orthopedic procedures, such as carpal tunnel release or joint injections
10. Pain management procedures, including epidural steroid injections and nerve blocks
11. Podiatric (foot and ankle) surgery
12. Tonsillectomy and adenoidectomy
Advancements in medical technology, minimally invasive surgical techniques, and improved anesthesia methods have contributed to the growth of ambulatory surgical procedures, offering patients a more convenient and cost-effective alternative to traditional inpatient surgeries.
The palatine tonsils, also known as the "tonsils," are two masses of lymphoid tissue located on either side of the oropharynx, at the back of the throat. They are part of the immune system and play a role in protecting the body from inhaled or ingested pathogens. Each tonsil has a surface covered with crypts and follicles that contain lymphocytes, which help to filter out bacteria and viruses that enter the mouth and nose.
The palatine tonsils are visible through the mouth and can be seen during a routine physical examination. They vary in size, but typically are about the size of a large olive or almond. Swelling or inflammation of the tonsils is called tonsillitis, which can cause symptoms such as sore throat, difficulty swallowing, fever, and swollen lymph nodes in the neck. In some cases, enlarged tonsils may need to be removed through a surgical procedure called a tonsillectomy.
Otitis media is an inflammation or infection of the middle ear. It can occur as a result of a cold, respiratory infection, or allergy that causes fluid buildup behind the eardrum. The buildup of fluid can lead to infection and irritation of the middle ear, causing symptoms such as ear pain, hearing loss, and difficulty balancing. There are two types of otitis media: acute otitis media (AOM), which is a short-term infection that can cause fever and severe ear pain, and otitis media with effusion (OME), which is fluid buildup in the middle ear without symptoms of infection. In some cases, otitis media may require medical treatment, including antibiotics or the placement of ear tubes to drain the fluid and relieve pressure on the eardrum.
Endoscopy is a medical procedure that involves the use of an endoscope, which is a flexible tube with a light and camera at the end, to examine the interior of a body cavity or organ. The endoscope is inserted through a natural opening in the body, such as the mouth or anus, or through a small incision. The images captured by the camera are transmitted to a monitor, allowing the physician to visualize the internal structures and detect any abnormalities, such as inflammation, ulcers, or tumors. Endoscopy can also be used for diagnostic purposes, such as taking tissue samples for biopsy, or for therapeutic purposes, such as removing polyps or performing minimally invasive surgeries.
Postoperative pain is defined as the pain or discomfort experienced by patients following a surgical procedure. It can vary in intensity and duration depending on the type of surgery performed, individual pain tolerance, and other factors. The pain may be caused by tissue trauma, inflammation, or nerve damage resulting from the surgical intervention. Proper assessment and management of postoperative pain is essential to promote recovery, prevent complications, and improve patient satisfaction.
An earache is defined as a pain or discomfort in the ear. It can occur in either the outer, middle, or inner ear. The pain may be sharp, dull, constant, or intermittent and can vary in intensity from mild to severe. Earaches are often accompanied by other symptoms such as hearing loss, ringing in the ears (tinnitus), and feelings of pressure or fullness in the ear. In some cases, an earache may be a symptom of an underlying medical condition, such as an ear infection, swimmer's ear, or a ruptured eardrum. If you are experiencing an earache that is severe or persistent, it is important to seek medical attention from a healthcare professional.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
 Adenoidectomy
Adenoidectomy Adenoids and Adenoidectomies (for Kids) - Nemours (XML)
Adenoids and Adenoidectomies (for Kids) - Nemours (XML) Adenoidectomy versus chemoprophylaxis and placebo for recurrent acute otitis media in children aged under 2 years: randomised...
Adenoidectomy versus chemoprophylaxis and placebo for recurrent acute otitis media in children aged under 2 years: randomised... quote Oh, MY"e in Tonsillectomy and Adenoidectomy Loving Healing Press eBook v. Laurie Zelinger | Weltbild
quote Oh, MY"e in Tonsillectomy and Adenoidectomy Loving Healing Press eBook v. Laurie Zelinger | Weltbild What causes bad taste in mouth after tonsillectomy and adenoidectomy? | HealthTap Online Doctor
What causes bad taste in mouth after tonsillectomy and adenoidectomy? | HealthTap Online Doctor Endoscopic Septoplasty & Endoscopic Transnasal Adenoidectomy | In the Media | ENT & Allergy Assocaites
Endoscopic Septoplasty & Endoscopic Transnasal Adenoidectomy | In the Media | ENT & Allergy Assocaites Adenoidectomy - EasyHeals
Adenoidectomy - EasyHeals Tonsillectomy & Adenoidectomy Surgery
Tonsillectomy & Adenoidectomy Surgery Adenoidectomy - Adenoidectomy Procedure
Adenoidectomy - Adenoidectomy Procedure Chronic ear infection: Symptoms, causes, treatment, and prevention
Chronic ear infection: Symptoms, causes, treatment, and prevention Adenoidectomy | Rockwall, TX | Lakeside Allergy ENT
Adenoidectomy | Rockwall, TX | Lakeside Allergy ENT Adenoidectomy Cost In Thailand | Adenoidectomy in Thailand
Adenoidectomy Cost In Thailand | Adenoidectomy in Thailand Videos and Animations of PEAK PlasmaBlade Procedures and Techniques | Spinal Surgery
Videos and Animations of PEAK PlasmaBlade Procedures and Techniques | Spinal Surgery Adenoidectomy in Guwahati: cost, best hospitals and doctors
Adenoidectomy in Guwahati: cost, best hospitals and doctors Adenoidectomy Surgery in Delhi (India) - ORL International Hospital
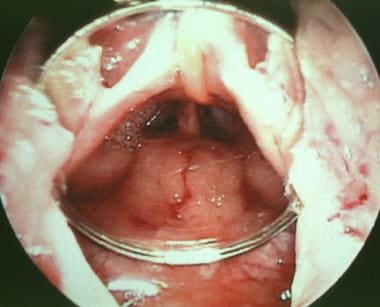
Adenoidectomy Surgery in Delhi (India) - ORL International Hospital A NEW SOFT PALATE RETRACTOR PERMITTING ADENOIDECTOMY UNDER DIRECT VISION | JAMA Otolaryngology-Head & Neck Surgery | JAMA...
A NEW SOFT PALATE RETRACTOR PERMITTING ADENOIDECTOMY UNDER DIRECT VISION | JAMA Otolaryngology-Head & Neck Surgery | JAMA...![10 Best Clinics for Adenoidectomy in Bucharova [2023 Prices]](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAA7VBMVEVHcEwrodw3p95goc2e0u4qrOMkot0WZqJsjaNQhbAzr+QtqOA9WHtkyfMiaaQdl9Yoq+ImquIvQWMmm9iByuQnq+Izr+RIY4UrcqxLoc8AACZFuOs6TWzN5eg3sON0WmUnqOEdmNc9s+UhmdcfmdceZJym3PMZOWB/ip89frUTJk0sbKMmbaczRmUjOl5AUnA/XH42odtSueciHj44t+w8QFw/U3MrVXw9WHoWQmseSHE5caQ3r+QfOF5XY35uosUcPGRNaooxQmIxS20fmdc/qN9tfpoemNclqeIEMFoAGkMAH0gAV5YFXZwmm9jSTIdTAAAAR3RSTlMAMJBTA/5c+g5y+aSEQNHjQWunvCCzwmymFmuZnRLoHbvM3/GmZQnSQH703rTik4p2zX9cfnpNsVX92YrV2WF1+YDB9VBtNmSKSzQAAADZSURBVBiVPY7XcsIwEEWvq2Tjggu9d9ITSkIqKYDkpv//HBDJ5Lzc2Z3dOReQTHdBUMY/tM+NYdfg6t9c5m+xTNfmVKbCFngtCkLqqHK5YCq0nHje9cUc3QpgCnhWTnQQKw07vIFI7eTb/ArQLrO0NwwwcieF1Ti96vQma7ZKYMqkqP/q7rLmqgJfo9bT/QZ4vG2ny9PFuISX2vMn8J45KWwTikAtcb7iw0/SXruyyOABTiL5/oBdPTeL0Atns5DqI27o0ueL/RSIVcYYN8++3YAJwSLFHPv9I8hRG0SWb3LsAAAAAElFTkSuQmCC) 10 Best Clinics for Adenoidectomy in Bucharova [2023 Prices]
10 Best Clinics for Adenoidectomy in Bucharova [2023 Prices] Glue Ear (Otitis Media with Effusion): Symptoms & Causes
Glue Ear (Otitis Media with Effusion): Symptoms & Causes Tonsillectomy and Adenoidectomy for Modern Management | Children's Hospital Colorado Continuing Education
Tonsillectomy and Adenoidectomy for Modern Management | Children's Hospital Colorado Continuing Education Conditions And Treatments | Otolaryngology And Communication Enhancement | Boston Children's Hospital
Conditions And Treatments | Otolaryngology And Communication Enhancement | Boston Children's Hospital What An Adenoidectomy Treats - Georgetown Ear, Nose and Throat Center P.A.
What An Adenoidectomy Treats - Georgetown Ear, Nose and Throat Center P.A. Tonsillectomy and Adenoidectomy for Obstructive Sleep Apnea and Snoring - ENT of Georgia North
Tonsillectomy and Adenoidectomy for Obstructive Sleep Apnea and Snoring - ENT of Georgia North Division of Otolaryngology (Ear, Nose and Throat) Resources | Children's Hospital of Philadelphia
Division of Otolaryngology (Ear, Nose and Throat) Resources | Children's Hospital of Philadelphia